
ABSTRACT
Different clinical medicine programs exist in China, which are mainly the 3-year junior college medical program, the 5-year medical bachelor’s degree program, the 5 + 3 medical master’s degree program, and the 8-year medical doctoral degree program. Medical graduates obtain different degrees from various medical programs, leading to inequality and polarization of the cultivation. The extended length of schooling discourages talented students from pursuing clinical medicine. The current situation has worsened due to the mismatch between clinical competence and promotion, as well as insufficient remuneration. The most critical reform measure is to establish separate degree systems for scientific research skill training and clinical training, which helps clarify the boundaries between these two. Students who receive academic postgraduate education obtain academic degrees, such as the master of medical science and doctor of philosophy; students who take part in the national standardized resident training, specialist training, or general practitioner training obtain professional degrees, such as master of medicine and doctor of medicine. It is imperative to consider shortening the duration of medical education, with an ideal limit of eight years on average. Optimizing the way to promotion and raising the expenditure of remuneration are also crucial. The reform of medical education system in China still has a long way to go and requires gradual adjustment and optimization.
Introduction
Medical education is an important cornerstone of the development of healthcare. China, which has the largest population base in the world, has attached great importance to medical education. China has the largest enrollment in medical majors globally, with over 1.7 million medical students enrolled in 2021 [Citation1]. There are several different types of programs existing in the major of clinical medicine, which mainly are the 3-year junior college medical program, the 5-year medical bachelor’s degree program, the 5 + 3 medical master’s degree program, and the 8-year medical doctoral degree program [Citation2]. Different programs have been set up to meet the needs of national health services at different stages of the country’s development. The report on the 20th National Congress of the Communist Party of China has stressed the importance of promoting the construction of ‘Healthy China’ and ensuring the protection of people’s health as a strategic priority [Citation3]. The Chinese government has carried out policies to adopt measures in optimizing the reform and accelerate the innovative development of medical education system [Citation4,Citation5]. We now present our thinkings on the reform of medical education system in China, advising on improving the path of doctor training and the adjustments to current different clinical medicine programs.
Clinical medicine programs in China
Historical reasons have contributed to the variety of clinical medicine programs in China. In 1912, the first public medical school dedicated to teaching Western medicine was established in Beijing [Citation6]. At the early stage of reform practice in medical education, due to the imbalance of urban-rural development and the shortage of medical practitioners, the Chinese government has made sufficient efforts to ensure the demand for healthcare by expanding the scale of medical education and shortening the cycle of medical education [Citation7]. Steps were taken to improve the quality of medical education in the 21st century via implementing longer-term programs, such as the 5 + 3 and 8-year programs [Citation8]. In recent years, some top institutes launched the 4 + 4 program, enrolling talented college graduates with multidisciplinary academic backgrounds and cultivating them into internationalized medical scientists to meet the increasing need for high healthcare expectations [Citation9]. Nanjing Medical University has taken the first step to launch the 9-year program in 2019, aiming to integrate undergraduate, postgraduate, doctoral education, and standardized resident training (SRT) within nine years and train highly qualified doctors with a doctor of medicine (MD) degree [Citation10]. Since doctors in China must first complete the national SRT, which lasts for three years, the 9-year program that provides both the MD degree and contains the SRT simultaneously is currently the program with the shortest integrated training period in medical education. The main clinical medicine programs in China are presented in [Citation2,Citation11].
Table 1. The main clinical medicine programs in China.
The 3-year secondary school or junior college medical program was set up for primary medical services, training medical students via a lower entry threshold and shorter length of schooling. Students who graduate from these programs may have the chance to receive a further 2-year general practitioner (GP) training, which is so-called the 3 + 2 medical program [Citation12]. Although there is a certain gap between the clinical and scientific research ability of the 3-year program graduates and the graduates of other programs, the 3-year medical program has greatly alleviated the shortage of healthcare service in rural China and has made outstanding contributions to guaranteeing the basic level of medical service. Previous study has shown a descending trend of medical students enrolled in secondary school, which is in accordance with the government’s demand to improve the degree level of medical practitioners [Citation4,Citation13].
The 5-year medical bachelor’s degree program is the most common program provided in most medical colleges in China. Graduates can attend the National Medical Licensing Examination (NMLE) after one year of participating in clinical work at medical institutions. It should be noted that most of them need to complete the SRT further to become a doctor. The Chinese government is attempting to establish a medical practitioner training system that contains 5 + 3 (5 years of undergraduate medical education plus 3 years of the SRT or 3 years of postgraduate education with professional degree) medical education as the main body and 3 + 2 (3 years of secondary school or junior college medical education plus 2 years of GP training) medical education as the supplement [Citation14]. The 5-year medical program and the SRT will continue to play essential roles during the period.
Three more years have been added to the 5-year medical program to form the 5 + 3 medical master’s degree program, during which students are required to simultaneously accomplish studies for the master’s degree of medicine (MM), pass the NMLE, and complete the SRT.
The 8-year and 4 + 4 medical doctoral degree programs are set up in top institutes with the best medical colleges in China. Students who graduate from these programs can obtain the degree of doctor of philosophy (PhD). The main difference between these two programs is their enrollment requirements. The 8-year program enrolls senior middle school graduates, while the 4 + 4 program enrolls college graduates with non-medical bachelor’s degrees. The students in the latter program only have four years to study clinical medicine systematically.
In China, the policy has been implemented that graduates of clinical medicine should complete the national SRT to be eligible for employment [Citation15]. It is essential to check if the medical programs mentioned above offer the SRT to students during their training period. Additionally, it is worth noting that different postgraduate programs may offer different degrees. Programs with the SRT typically offer professional degrees, while those without the SRT offer academic degrees. Students who complete 8-year and 4+4 medical programs obtain academic degrees upon graduation. The training period of different medical programs in China is shown in .
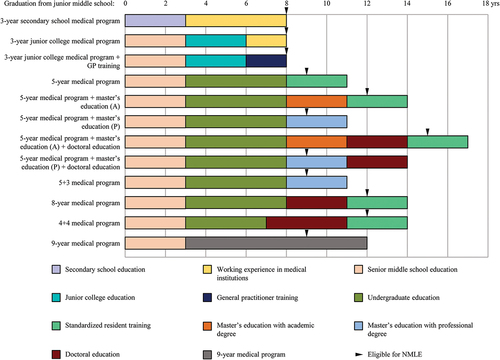
Figure 1. Training period of different medical programs in China. Different medical programs require different lengths of schooling to cultivate medical practitioners. It should be noted that the master’s education with professional degree and the 9-year medical program simultaneously contain the SRT. Abbreviations: GP, general practitioner; A, academic degree; P, professional degree; NMLE, national medical licensing examination.
The existing problems under current medical education system
The chaos in clinical medicine programs
The following three aspects illustrate the chaos of clinical medicine programs. First, the existence of different medical programs has led to confusion. For instance, the 3-year medical program is available for junior middle school graduates; however, the 4 + 4 medical program only enrolls talented college graduates from prestigious universities. The dissimilarity of the source of students is reflected not only in student’s performance on exams, but also in the entrance age, which seriously exacerbates the competence disparity between doctors. Likewise, because students who graduate from the 3-year medical program tend to work in rural areas after graduation, the problem of this chaos will eventually affect or even widen the healthcare disparity between urban and rural areas in China [Citation16,Citation17].
Second, graduates may face inequality as a result of getting various degrees from different medical programs. Graduates of the 8-year and 4 + 4 medical programs obtain a doctoral degree, while graduates of the 5 + 3 medical program obtain a master’s degree after the same eight years of education. In particular, completing the 5-year medical program and further participating in the SRT without pursuing postgraduate education may result in remaining at the bachelor level after eight years of medical education. The time spent on education may be equal, but the type of degree earned differs. Unlike some other countries, employers in China tend to strongly value academic qualifications when hiring employees, which brings inequity in the employment of medical graduates. In countries like Japan and Germany, for instance, medical graduates are awarded different types of degrees. In Japan, graduates obtain a bachelor’s degree, while in Germany, they only obtain a practicing certificate. However, despite the variations, the quality of medical education in these countries is still highly respected [Citation18,Citation19]. The maturity and stability of their medical education can ensure their medical students have adequate clinical competence after six years of education. Therefore, it is worth discussing which degree should be awarded to which part of the students. This will help to meet the needs of medical education reform and ensure that the process is scientific and uniform.
Third, the current postgraduate education system has been characterized by ‘polarization’, which is not aligned with the needs of national health service and has deviated from the primary objective of training high-level medical practitioners. There are two kinds of postgraduate degrees in China: academic degree and professional degree [Citation20]. Academic postgraduate education focuses on improving scientific research skills, while professional postgraduate education focuses on improving clinical competence [Citation20,Citation21]. In the actual situation, the training process of the academic postgraduates emphasized too much on training for scientific research skills; their time of clinical practice is far from supporting them to work as a doctor after graduation [Citation22]. Potential employment discrimination exists when graduates with an academic degree fail to complete the SRT, a necessary requirement for most hospitals in China to hire new employees. They have to complete the 3-year SRT, significantly delaying their path to becoming a doctor. Furthermore, there is quite a significant duplication of academic graduate education and academic doctoral education in training requirements. This academic training pattern creates experts in experiments; however, most students are still oriented to work in the hospital after graduation. Excessive training for scientific research skills has limited help to their future clinical competence. For professional postgraduates, they typically work in the hospital for a period of three years due to double-track integration. They complete their courses and dissertations during weekends or spare time, having limited opportunities to enhance their scientific research skills, resulting in limited scientific research capabilities.
The extended length of schooling
In parallel comparison, most other majors generally take 9 to 10 years to complete the whole higher education. Since Chinese doctoral students’ graduation is likely to be postponed, the length of schooling has been inevitably extended to over three years [Citation23]. In fact, it takes 11 to 14 years for most medical students to complete the ‘bachelor-master-doctor’ growth curve in China. In comparison, the general length of medical education in other countries is six years. Students who wish to continue their studies can opt for postgraduate education [Citation19]. In China, however, the duration of medical education is considerably extended, which may discourage talented students from choosing clinical medicine. This could ultimately undermine the high-quality advancements and innovations in medical education and practice.
The inconsistency between clinical competence and promotion
Postgraduates who receive academic doctoral education usually lack clinical experience after graduation. However, they are more likely to be promoted to the associate chief doctor or associate professor in a shorter period. Due to the lack of well-established residency education and professional certification, Chinese medical practitioners’ clinical competence is often judged through educational background [Citation24]. Conversely, postgraduates with professional master’s degrees devote almost all their energy to clinical work. It is difficult for them to produce innovative achievements due to their lack of scientific research skills, resulting in difficulty getting promoted, even if their clinical competence is excellent.
The insufficiency of remuneration
As mentioned earlier, the length of schooling in current medical education system is too long. Medical students graduate at a higher age than others and face heavier financial pressure than students in other majors. Therefore, if professional postgraduates’ remuneration is not adequately guaranteed during the SRT, their studies and quality of life will undoubtedly be affected. Financial pressure may force students to abandon the thought of receiving further higher education and choose to work instead. It may even reduce their motivation to participate in medicine in the future [Citation25]. One of the embodiments of this is that only a small percentage of licensed medical professionals choose to register in medical institutions and work as doctors in China [Citation26]. It is a huge waste of funds and resources if medical students do not choose to work as a doctor after years of training.
Although the government stipulated that the remuneration of trainees must be equally paid for equal work as employees in the hospital, most hospitals do not achieve this [Citation27]. Professional postgraduates are treated with little salary and no sound social or medical security. Academic postgraduates are also facing enormous economic pressure due to the long growth path. Relatively low remuneration would decrease the enthusiasm of young medical students for pursuing their future careers [Citation28,Citation29].
Suggestions on the reform of medical education system
Adjust the current different clinical medicine programs
The most critical reform measure is to adjust the current clinical medicine programs. The unified degree and education system makes it feasible to formulate accurate training objectives and evaluation standards [Citation30], and it helps reduce the heterogeneity of medical education, save costs to the healthcare market, and promote equity in the delivery of healthcare services in China [Citation13]. We suggest clarifying the boundaries between scientific research skill training and clinical training by establishing two types of degree systems separately. Students who receive academic postgraduate education obtain academic degrees, such as the master of medical science (MS) and PhD; students who take part in the SRT, specialist training, or GP training obtain professional degrees, which are MM and MD. Medical licenses and certificates of training shall also be awarded to professional postgraduates. After the completion of the SRT, trainees should get the professional title of attending doctor. Further specialist or GP training should be available for those who complete the SRT. The degree of doctor of general practice (DoGP) and the title of associate chief doctor should be offered to those who complete the 2- to 3-year GP training. The degree of MD and the title of associate chief doctor should be offered to those who complete the 3- to 5-year specialist training. Both kinds of medical practitioners are highly qualified with reliable clinical competence through years of solid front-line clinical training. Moreover, academic postgraduates must participate in the SRT to ensure their clinical competence before starting their career as a doctor. Ultimately, doctors prioritize practical clinical competence, which does not align perfectly with academic skills [Citation24].
However, the channel between academic and professional postgraduate education should be preserved. For a minimal number of talented and willing talents, abundant training for scientific research skills should be available through academic postgraduate education. This may lead to a long growth path, but it is suitable for creating compound clinical scientists with enriched academic skills and qualified clinical competence who would possess leadership in the development of their fields.
Shorten the current length of schooling
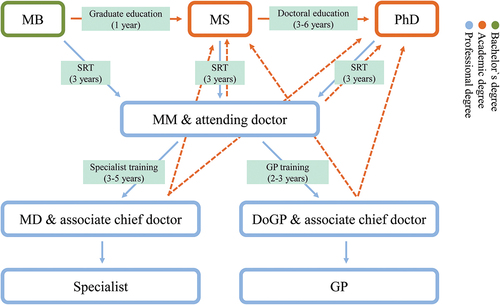
Over half of the medical students in China are experiencing time stress, as reported in the study published by Guo et al. [Citation31] We suggest that the average time of medical education should not exceed 12 years. By shortening the length of schooling for the degree of MS to one year, the consequence of shifting from academic postgraduate education to professional one can become relatively low, which helps shorten the growth curve. This 1-year period is similar to a pre-experiment for doctoral education, where students can acquire basic scientific research skills and select a research direction. If students do not develop an interest or talent for scientific research after one year of academic training, they may feel more acceptable to pursue professional postgraduate education. At the same time, three to six years should be given to doctoral education, allowing students fully improve their scientific research capabilities and produce more valuable and innovative scientific achievements. They can continue to work in scientific research posts after graduation or start the SRT at a younger age. displayed the suggested cultivation process in the medical education system.
Figure 2. The suggested cultivation process in the medical education system. Abbreviations: MB, bachelor of medicine; MS, master of medical science; PhD, doctor of philosophy; SRT, standardized resident training; MM, master of medicine; GP, general practitioner; MD, doctor of medicine; DoGP, doctor of general practice.
Optimize the way to promotion
The methods for evaluating promotion and salary distribution should be based on work performance and contribution to the society, with scientific achievements as only a reference. The government has required that the number of publications should not be used as a precondition or direct criterion for the title assessment [Citation32]. The thesis requirement can be diluted or exempted for those who work at frontline in remote or grassroots regions [Citation33]. This allows doctors to focus on their own work and prevents them from getting involved in pseudo-scientific research that they are not interested in, are not good at, and are not helpful to their clinical work competence.
Raise the expenditure of remuneration
The government should ensure financial security for medical students. Financial concerns are a common source of student stress, which may even influence academic performance and specialty choice [Citation34]. Whether it is during the postgraduate education or the SRT, students should enjoy remuneration and social security appropriate to the intensity of their work. Investment in medical education should be increased, commensurate with the increase in enrollment over the past few years. Extra financial support should be given to economically underdeveloped areas [Citation35,Citation36].
One possible solution is to reduce the enrollment in medical colleges. At home and abroad, medical education is carried out via medical elitism, and the 4 + 4 medical program in China is also modeled on the North American pattern in order to train elite medical scientists. However, to meet the enormous needs of national health service, the 4 + 4 medical program is not applicable everywhere. The feasible way is to reduce the enrollment, especially the enrollment of the 3-year medical program, and further increase investment in every medical student so that high-quality graduates are willing to pursue a career in medicine [Citation37]. In order to ease employment pressure and reduce medical students’ concerns about uncertainty regarding their future careers, raising the expenditure of remuneration may be one of the key points in the reform of medical education system [Citation38,Citation39].
Conclusion
To the government’s conception, by 2050, China will be built into a healthy country compatible with a modern socialist country. A mature, advanced medical education system is undoubtedly one vital part of it [Citation40]. However, different clinical medicine programs exist in China, and the problem still needs to be gradually solved through adjustment and optimization. The reform of medical education system in China still has a long way to go.
Author contributions
Hongtao Tie and Yuxiang Luo searched and collected relevant articles, and drafted the manuscript. Dan Chen conceptualized the paper, reviewed the manuscript, and revised the article. All authors approved the final draft. All authors approved the final draft.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data are available from the corresponding authors upon request.
Additional information
Funding
References
- National Health Commission of the People’s Republic of China.China health statistics yearbook 2022. Peking Union Medical College Press; 2022. http://www.nhc.gov.cn/mohwsbwstjxxzx/tjtjnj/202305/6ef68aac6bd14c1eb9375e01a0faa1fb.shtml
- Liu X, Feng J, Liu C, et al. Medical education systems in China: development, status, and evaluation. Acad Med. 2023;98(1):43–8. doi: 10.1097/ACM.0000000000004919
- Xi J. Report on the 20th national congress of the Communist Party of China 2022. [cited 2023 Apr 11]. Available from: http://www.qstheory.cn/dukan/qs/2022-11/01/c1129089160.htm
- Guiding opinions on accelerating innovation and development of medical education. General office of the state council of the people’s Republic of China. 2020. [cited 2023 Apr 11]. Available from: http://www.gov.cn/zhengce/content/2020-09/23/content_5546373.htm
- The adjustment and optimization reform plan of major settings in general higher education. Ministry of education of the people’s Republic of China. 2023. [cited 2023 Apr 11]. Available from: http://www.moe.gov.cn/srcsite/A08/s7056/202304/t20230404_1054230.html
- History of Peking University Health Science Center. Peking University Health Science Center. [cited 2023 Apr 11]. Available from: https://www.bjmu.edu.cn/xbgk/lsyg/index.htm
- Reynolds TA, Tierney LM Jr. Medical education in modern China. JAMA. 2004;291(17):2141. doi: 10.1001/jama.291.17.2141
- China’s health-care reform: an independent evaluation. Lancet. 2019;394(10204):1113. doi: 10.1016/S0140-6736(19)32210-X
- Wang C, Chen S, Zhu J, et al. China’s new 4 + 4 medical education programme. Lancet. 2019;394(10204):1121–1123. doi: 10.1016/S0140-6736(19)32178-6
- Clinical medicine (a continuous academic project that involves undergraduate, postgraduate and doctoral study). Nanjing Medical University. [cited 2023 Apr 11]. Available from: https://zs.njmu.edu.cn/2019/0624/c3430a149703/page.htm
- Ministry of education of the people’s Republic of China. [cited 2023 Apr 11]. Available from: http://www.moe.gov.cn/
- Lian S, Chen Q, Yao M, et al. Training pathways to working as a general practitioner in China. Fam Med. 2019;51(3):262–270. doi: 10.22454/FamMed.2019.329090
- Hsieh CR, Tang C. The multi-tiered medical education system and its influence on the health care market-China’s Flexner report. Hum Resour Health. 2019;17(1):50. doi: 10.1186/s12960-019-0382-4
- Opinions on deepening the coordination between medicine and education to further promote the reform and development of medical education. General office of the state council of the people’s Republic of China. 2017. [cited 2023 Apr 11]. Available from: https://www.gov.cn/zhengce/content/2017-07/11/content_5209661.htm
- Management measures for the standardized resident training (trial). National health commission of the people’s Republic of China. 2014. [cited 2023 Apr 11]. Available from: http://www.gov.cn/gongbao/content/2015/content_2806023.htm
- Cai J, Coyte PC, Zhao H. Decomposing the causes of socioeconomic-related health inequality among urban and rural populations in China: a new decomposition approach. Int J Equity Health. 2017;16(1):128. doi: 10.1186/s12939-017-0624-9
- Ma C, Song Z, Zong Q. Urban-rural inequality of opportunity in health care: evidence from China. Int J Environ Res Public Health. 2021;18(15):7792. doi: 10.3390/ijerph18157792
- Onishi H. History of Japanese medical education. Korean J Med Educ. 2018;30(4):283–294. doi: 10.3946/kjme.2018.103
- Zavlin D, Jubbal KT, Noé JG, et al. A comparison of medical education in Germany and the United States: from applying to medical school to the beginnings of residency. Ger Med Sci. 2017;15:Doc15. doi: 10.3205/000256
- Jia X, Zhu Y, Zhong X, et al. The attitudes of postgraduate medical students towards the curriculum by degree type: a large-scale questionnaire survey. BMC Med Educ. 2023;23(1):869. doi: 10.1186/s12909-023-04846-5
- Chen Z, Wang L. Reconstruction of a clinician training system in china-A successful “5 + 3” model from Shanghai. Int J Health Plann Manage. 2017;32(3):264–269. doi: 10.1002/hpm.2426
- Wu L, Wang Y, Peng X, et al. Development of a medical academic degree system in China. Med Educ Online. 2014;19(1):23141. doi: 10.3402/meo.v19.23141
- Shi L, Yi W, Zhao L, et al. Analysis of influencing factors of delayed graduation of medical doctoral students. Med Educ Dev. 2021;7(5): 538–544. [in Chinese].
- Zhu J, Li W, Chen L. Doctors in China: improving quality through modernisation of residency education. Lancet. 2016;388(10054):1922–1929. doi: 10.1016/S0140-6736(16)00582-1
- Pisaniello MS, Asahina AT, Bacchi S, et al. Effect of medical student debt on mental health, academic performance and specialty choice: a systematic review. BMJ Open. 2019;9(7):e029980. doi: 10.1136/bmjopen-2019-029980
- Zeng J, Zeng XX, Tu Q. A gloomy future for medical students in China. Lancet. 2013;382(9908):1878. doi: 10.1016/S0140-6736(13)62624-0
- Notice on the implementation of the “two equal treatment” policy for standardized resident training. General Office of The National Health Commission of The People’s Republic of China. 2021. [cited 2023 Apr 11]. Available from: http://www.nhc.gov.cn/qjjys/s7949/202109/d0801ca57ee44edc97176a9fc1531dab.shtml
- Jingang A. Which future for doctors in China? Lancet. 2013;382(9896):936–937. doi: 10.1016/S0140-6736(13)61928-5
- Xu D, Sun B, Wan X, et al. Reformation of medical education in China. Lancet. 2010;375(9725):1502–1504. doi: 10.1016/S0140-6736(10)60241-3
- Chen C. Reflection on the educational system reform of higher medical education in China. China High Med Edu. 2021;2021(9):6–8. [in Chinese].
- Guo F, Yi M, Sun L, et al. A novel model to predict mental distress among medical graduate students in China. BMC Psychiatry. 2021;21(1):569. doi: 10.1186/s12888-021-03573-9
- Guiding opinions on deepening the reform of the professional title system of health professionals and technicians. Ministry of human resources and social security of the people’s Republic of China. 2021. [cited 2023 Apr 11]. Available from: https://www.gov.cn/zhengce/zhengceku/2021-08/05/content_5629566.htm
- Opinions on deepening the reform of the title system. General office of the state council of the people’s Republic of China. 2017. [cited 2023 Apr 11]. Available from: http://www.gov.cn/xinwen/2017-01/08/content_5157911.htm#1
- Dyrbye LN, Thomas MR, Shanafelt TD. Medical student distress: causes, consequences, and proposed solutions. Mayo Clin Proc. 2005;80(12):1613–1622. doi: 10.4065/80.12.1613
- Li H, Zhou X. Medical education reform in China. Postgrad Med J. 2018;94(1118):673–674. doi: 10.1136/postgradmedj-2018-136145
- Ren X, Yin J, Wang B, et al. A descriptive analysis of medical education in China. Med Teach. 2008;30(7):667–672. doi: 10.1080/01421590802155100
- Yin J. Comparison of academic degree and schooling length of clinical medicine between China and foreign countries. Chin Med Edu Tech. 2016;30(5): 502–507. [in Chinese].
- Yang F, Meng H, Chen H, et al. Influencing factors of mental health of medical students in China. J Huazhong Univ Sci Technolog Med Sci. 2014;34(3):443–449. doi: 10.1007/s11596-014-1298-9
- Zeng W, Chen R, Wang X, et al. Prevalence of mental health problems among medical students in China: a meta-analysis. Medicine (Baltimore). 2019;98(18):e15337. doi: 10.1097/MD.0000000000015337
- Outline of the “healthy China 2030” plan. State council of the people’s Republic of China. 2016. [cited 2023 Apr 11]. Available from: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm