
Abstract
Background
Sick leave due to stress-related mental ill health increases in society. In occupational therapy, occupational balance is considered important for experiencing health and well-being. Thus, knowledge regarding occupational balance and occupational value constitute essential parts of occupational therapists’ work with people suffering from occupational ill health.
Objective
The aim of this study is to analyse the relationships between sociodemographic factors, occupational value, occupational balance and perceived health in people suffering from occupational ill health.
Methods
In a quantitative cross-sectional study data from a total of 218 individuals were included, 192 women, 22 men and 4 individuals who did not specify their gender. Data were collected by means of surveys prior to an occupational therapy intervention. The instruments used included OVal-pd, OBQ, EQ5D and a sociodemographic questionnaire. Data were analysed using regression and decision tree analysis.
Results
The results show that individuals who experience an imbalance in their everyday life and who have few or no experiences of daily occupations imprinted by socio-symbolic occupational value experienced lower perceived health.
Conclusions
Low level of experiences of balance in daily life and occupational value seems to be the main risk factors for the development of occupational ill health, rather than sociodemographic factors.
Introduction
Mental illness is used as an overarching term for both less serious mental health problems, such as anxiety and depression, and more serious mental disorders, such as bipolar disorders and schizophrenia [Citation1]. According to the Swedish Public Health Agency [Citation2], the WHO has estimated that mental illness will be one of the greatest and fastest-growing public health challenges globally. The costs associated with mental illness for individuals, employers and society at large are high. Apart from its impact on people’s well-being, the total costs of mental ill health are estimated to exceed EUR 600 billion – or more than 4% of GDP – across the 28 EU countries [Citation3]. Mental illness continues to be the largest cause of sick leave in Sweden [Citation4], and according to the Swedish Social Insurance Agency [Citation4], it is the cause of half of all sick leave. Already in 2009, the European Commission estimated that 50–60% of lost working days in the European Union were linked to work-related stress [Citation5]. According to OECD, mental health at the workplace is considered a future challenge for the labour market that needs to be prioritized [Citation3].
In Sweden, sick leave due stress-related mental ill health is increasing in society. In the event of sick leave, there always needs to be a diagnosis linked to the individual’s ability to work. From a European and societal perspective, the main purpose of prescribing sick leave is to promote recovery and the individual returning to work [Citation6]. Compared to other European countries, Sweden’s sickness absence rate is found somewhere in the middle, with a higher sick leave rate for women compared to men. Compared to other European countries, however, Swedish women participate in the labour market to a larger extent [Citation7].
The social determinants and indicators related to mental illness concern demographic factors such as gender, age, ethnicity and family structure, economic factors that include income and employment, as well as social and cultural factors, including social participation, education and practical support [Citation2]. In addition to these factors, work-related factors may also contribute to the onset of mental illness [Citation8]. Sick leave due to mental illness in the male population has increased in Sweden. Increased gender equality and a higher level of acceptance regarding mental illness are believed to form the basis of the new sick leave rates [Citation9]. Another study has shown that factors affecting the experience of perceived health differ between women and men [Citation10]. For women, it concerned the experience of having time to perform daily household chores and leisure occupations. The same relationship did not exist in the group of men. The article also highlighted that men experience stressors during paid work, while the stressors for women manifested themselves outside work hours. Hence, strategies aimed at improving health only focussing on wage labour may be ineffective [Citation11].
Sick leave also affects everyday life and health in a secondary process [Citation12]. Not having paid work as an important part of one’s pattern of daily occupations due to illness may lead to a sense of loss of identity [Citation13–15]. As a result, individuals who experience ill health and are on sick leave often suffer from additional ill health referred to as occupational ill health [Citation16]. In such cases, occupational ill health is caused by roles and habits changing and by being excluded from the social context at work. Paid work impact and contribute to perceived health and occupational balance. Its form and function vary in different stages of life. In adulthood, work is both a societal expectation and a right that consolidates social roles [Citation16,Citation17]. Wilkock and Hocking [Citation16] highlight several factors with a focus on what you do, which in themselves pose a risk of developing ill health in everyday life. Occupational problems arise when everyday life becomes too much of a challenge, while occupational imbalance occurs when the person’s participation in occupations does not correspond to his or her unique physical, social and mental needs. Occupational balance is associated with perceived health and wellbeing [Citation18]. It is also important to have a variety of occupational values in the patterns of everyday life to prevent ill health or maintain good health and well-being. Occupational values can be divided into three different dimensions according to the ValMO model: concrete-, socio-symbolic and self-rewarding occupational value. The ValMO model describes the complexity and meaning-creating occupational values involved in all occupations in daily living [Citation19]. The higher amount of perceived occupational value, the greater experience of overall meaning in life which in turn has a strong link to perceived health and wellbeing [Citation20,Citation21].
People have a need to be sufficiently challenged as well as a need for social interaction. In case of illness or injury, the person’s roles and everyday life change, thus making it more difficult to maintain health and everyday balance. In order to achieve or regain occupational health, the person needs to be able to perform what he or she wants and needs in the environment they inhabit [Citation16]. Taylor [Citation22] describes balance in everyday life as the habits and roles created by the person to maintain a rhythm or balance. These roles entail various occupations organized as habits. He also highlights the importance of having a balance between values, interests, goals and the demands of the environment.
Working women with families have been found to have highly complex patterns of daily occupations [Citation23] causing an imbalance in the present occupations and the experiences related to these. For example, a positive correlation has been found between a low rating of occupational value in daily occupations and a low level of perceived subjective health [Citation20,Citation24]. Another study by Håkansson and Ahlborg [Citation25] involving 2223 individuals showed that several factors related to occupational balance may cause occupational ill health. The results of this study suggest that women need balance in their patterns of everyday life in order to experience good health regarding occupations at work, during leisure time, occupations related to home and family life, recovery and rest. For the men in the study, the experience of stress was the highest when there was an imbalance between rest and work in everyday life [Citation25]. Existing research has found that there is a correlation between, on the one hand, how people experience their occupational values and health and, on the other hand, how they experience their occupational balance and health [Citation20,Citation24,Citation26]. In addition to these relationships, gender, number of hours worked and whether the person is on sick leave have also been found to be related to how people experience their health [Citation1,Citation11,Citation21,Citation25,Citation26].
Thus, there are several predictors affecting our health, but there is a lack of knowledge regarding whether they are related to each other and, if so, how. This knowledge is important in terms of developing new interventions, both preventive and therapeutic, but also when it comes to evaluating the greatest risk factors for developing occupational ill health. The aim of this study was to analyse the relationships between sociodemographic factors, occupational value, occupational balance and perceived health in people suffering from occupational ill health.
Material and methods
The study used a quantitative design [Citation27] and analysed data from two separate studies. Participants from the two databases were compiled into a common database. A total of 218 individuals were subjected to an occupational therapy group intervention – ReDO® [Citation28]. The study was cross-sectional, analysing baseline data, before the intervention was initiated.
Procedure
Data from two similar studies were used. In each study data were collected before the ReDO® intervention started. Written information regarding the intervention and inclusion criteria was provided to everyone invited to participate. Individuals who met the criteria were informed about the specific study and they had to answer two screening questions. If both questions were answered with a yes, the person was offered to receive the intervention and to participate in a study. Database I was generated in the primary care sector in a region in the south of Sweden [Citation29]. Data were collected at individual meetings between an occupational therapist and a participant during the period between September 2014 and March 2016 [Citation29,Citation30]. The instruments were completed by the participant during the individual meeting. Recruiting participants took place either through other staff at the health centres or through referring physicians.
Database II was generated in the primary care sector in three regions in the south of Sweden. Data were gathered through a digital platform developed for the study. Thus, data were collected thorough a digital platform that was accessed by the participants through their bank ID. The participants selected for the intervention received login details and were then asked to answer all the instruments on their own, on the platform. The platform and the procedure were developed to decrease the number of health care appointments for the participants and to make participation in the research project, less demanding. The data collection was going on from November 2017 to December 2019. The total data collection included assessments at baseline, and at 3, 6 and 12 months after the intervention. This study, however, only included data from participants at baseline.
Database I originally consisted of 145 people, 10 of whom were men, while Database II, consisted of 73 people, including 12 men and 4 individuals who did not specify their gender.
Ethical considerations
Participation was voluntary in both survey studies and the participants received both oral and written information about the purpose of the study, the meaning of participation and that their anonymised responses were to be used for analysis on group level. Information about confidentiality, free participation and that the individual could leave the studies at any time without being excluded from the intervention, was also given. Both studies follow established rules according to the Act on Ethical Review, and the collection of Database I received approval from the local ethics review team in Lund (Dnr 20l41673 2014/182) and database II received approval from the Regional Ethical Review Association in Lund (Dnr H15 2016/902).
Participants
Health care personnel as physicians, physiotherapists, occupational therapists at primary health care centres could remit their clients to the intervention. Inclusion criteria for both studies meant that the individuals would be on or at risk of developing sick leave, i.e. being in working age and experience one or more of the following problems:
High frequency of health care visits
Complex symptoms
Pain with varied diagnoses or symptoms
Mental illness that may be treated in a primary care setting
Other symptoms/disorders resulting in a perceived occupational imbalance
Individuals who met the criteria were then offered to answer a simple screening instrument when, for example, visiting a physician or other therapists at a health care centre. These questions sought to measure the level of preparedness and motivation to work towards change in their everyday life and answering yes on both, were a prerequisite for being offered the intervention. The first question concerned whether the person experienced imbalance in his or her everyday life, whereas the second question concerned whether he or she was motivated to work towards change in his or her everyday life. Exclusion criteria were (a) not being able to speak or write in Swedish, (b) not having a steady medical treatment, (c) not having cognitive ability to participate in a group and to self-reflect. If the individual fulfilled any of the exclusion criteria they were excluded from the study.
A total of 218 people was added to the database for this study. Sociodemographic data for the sample are described in . The study included a total of 192 women, 22 men and 4 individuals who did not want to declare their gender, aged 25–70 (). The average age of the women was 49 and 46 for the men with a standard deviation of about 9.3 years for both groups. The highest proportion was found in the group aged 50–59.
Table 1. Sociodemographic characteristic of the participants (n = 218).
Measures
Data for the two databases were collected using several instruments. In this study, however, only instruments assessing sociodemographic variables, occupational value, occupational balance and perceived health were used.
Sociodemographic data were collected using a questionnaire developed for the studies, in which participants indicated age, gender, family situation (cohabiting/married or single), number of children living at home, level of education, country of birth and occupational health. Occupational health was measured by one question where the respondent indicating (in percentage) the extent to which he or she was able to work.
Occupational value was measured by means of occupational value pre-defined (OVal-pd) [Citation31], an instrument developed on the basis of the ValMO model in order to measure how often an individual has different value experiences in his or her everyday life [Citation20]. OVal-pd consists of 18 different claims linked to the three occupational value dimensions of ValMO. Respondents estimate how often they have experienced the different aspects of value in their daily occupations in the last month. The various claims are graded on a four-point Likert scale with the different response options (1) ‘not at all’, (2) ‘quite rarely’, (3) ‘quite often’ and (4) ‘very often’. A high total of points indicates that the individual has occupations in his or her everyday life with high value in all three dimensions. The questions can be divided up based on the three occupational value dimensions when the points are calculated as: concrete value 6 questions × 4 = 24 points, socio-symbolic value 4 questions ×4 = 16 points, self-rewarding value 8 questions × 4 = 32 points with a total of 72 possible points [Citation31]. The instrument has shown good reliability and validity [Citation31,Citation32].
To measure occupational balance, the study used the occupational balance questionnaire (OBQ) self-assessment instrument [Citation33], which includes 13 questions regarding occupational balance. The questions are answered on a four-point ordinal scale from 0 to 3: ‘totally disagree’, ‘partly agree’, ‘agree to some extent’, ‘totally agree’ based on the options best corresponding to the participant’s current situation. A high estimate indicates a high self-perceived occupational balance. Analyses can be carried out regarding both individual issues as well as points with a total of 39 possible points [Citation33]. This instrument is based on previous research on the perception of balance in women recovering from stress-related problems [Citation34], what is considered important for life balance [Citation35] and a conceptual analysis of occupational balance [Citation18].
EQ5D [Citation36] was used to measure perceived health, which is a standardized instrument for measuring and describing a person’s perceived health by means of self-assessment. The first two parts of the instrument have been used in the studies, where the first part is a descriptive questionnaire highlighting five common health problems related to mobility, hygiene, main activities, pains/inconveniences and fear/depressed mood. The participants are then allowed to choose which claim best fits their current health condition. The three available response options are: ‘no problems’, ‘some problems’ and ‘difficult problems’. The second part of the instrument consists of a vertical VAS scale where participants estimate their current perceived health on a scale from 0 to 100, where 0 is by far the worst imaginable and 100 the best imaginable. This instrument provides a health indicator that can easily be displayed in a descriptive profile, as well as an index value that can be used for an economic and clinical evaluation of healthcare [Citation37]. In this study, only the second part of the instrument (i.e. index value based on the VAS scale) was analysed. The psychometric stability of the separated VAS-scale from the EQ5D has been evaluated and found acceptable [Citation38].
Data analysis
Descriptive analyses were conducted in JASP. We used coefficient H as a measure of reliability [Citation39]. Classification and regression trees (CRT) were used to analyse risk factors that may predict the perceived health. In general the CRT analysis is a non-parametric statistical procedure ‘that identifies mutually exclusive and exhaustive subgroups of a population whose members share common characteristic that influence the dependent variables of interest’ [Citation40, p.173]. More specifically, these modelling techniques ‘… allow non-linear interactions among predictors, as well as depict and make use of these interactions, been successful in identifying the subset of risk and predictive factors to explain different outcomes’ [Citation41, p.1312]. In this study the CRT analysis was used to test potential relationships between predictors (in the present study, sociodemographic data, occupational value and occupational balance) and the outcome variable (in this study, perceived health) by identifying the predictors that differ the most with regard to the outcome variable [Citation42]. To increase the power in the results, certain categories were dichotomized to obtain a more even distribution between the groups, while the categories with a continuous scale could remain. The categories that were dichotomized included: country of birth (Sweden or another country), education (university/college or ‘basic education’), marital status (living alone or with another adult), children (children living at home or no children living at home) and occupational health (full-time work or sick leave full or part-time).
In the analysis, a decision tree is generated based on an automatic stepwise variable selection aimed at identifying exclusive subgroups within the population. The analysis classifies the data into subgroups according to the variable that best explains the dependent variable. Each subgroup continues to generate more subgroups based on the most significant predictor until the last stopping rule triggers. In CRT, ‘… splitting stops when the relative reduction in error resulting from the best split falls below a pre-specified threshold known as the complexity parameter. Typical values of this parameter are in the range of 0.001–0.05’ [Citation43, p.5]. Variables that did not reach the pre-specified threshold were not included in the final model. This analysis produces a tree diagram displaying homogenous groups of the individuals in the study based on the observed levels of the predictors and outcome variable. For the analysis, which was performed in SPSS Statistics version 26 (SPSS Inc., Chicago, IL), we used the following criteria [Citation42]: (a) the minimum number of cases in the parent node = 70 (10% of the sample) and (b) the minimum of cases in the terminal nodes = 35 (5% of the sample). To validate the tree, we applied the tenfold cross-validation application. Missing data were treated by surrogated splits. To compare the level of health between the participants within the terminal node, Cohen’s d effect sizes with 95% confidence intervals were calculated.
Results
The results show that on average, the participants exhibited a relatively low level of perceived health. Positive statistically significant correlations were found between the outcome variable of perceived health and all predictors: occupational balance, socio-symbolic occupational value and self-rewarding occupational value, except the total OVal-pd and concrete occupational value (see ).
Table 2. Descriptive and correlations of the study variables.
The relationships between the risk factors and perceived health
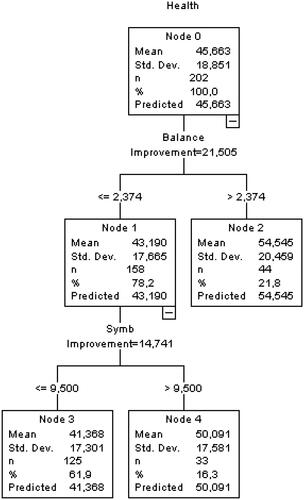
The CRT decision tree analysis showed that the occupational balance variable was found to be the main predictor for how the individuals in this study experience their health. More specifically, participants reporting levels of balance below 2.37 experienced poorer health (Cohen’s d = 0.59, 95% CI = [0.31, 0.88]). Among participants reporting a lower occupational balance, socio-symbolic occupational value was found to be a positive significant predictor of perceived health. A socio-symbolic occupational value above 9.50 was associated with higher levels of perceived health (Cohen’s d = 0.50, 95% CI = [0.18, 0.82]). None of the sociodemographic factors, self-rewarding occupational value nor concrete occupational value were a significant predictor of health. For more information, see .
Figure 1. A CHAID decision CRT used to identify predictors of perceived health.
Discussion
The ambition behind this study was to increase the knowledge regarding whether and if so, how known sociodemographic health predictors are related to perceived health. The specific aim of this study was to analyse the relationships between sociodemographic factors, occupational value, occupational balance – and the outcome variable – perceived health – in a group of individuals experiencing occupational ill health and being subjected to a occupational therapy group intervention. Overall, the key findings of the study indicate that both occupational balance and socio-symbolic occupational value dimension predict the perceived health, where occupational balance was the main predictor. This would suggest that especially an experience of imbalance in the patterns of daily occupations constitutes an important risk for developing ill health. However, the correlational analyses showed that both socio-symbolic and self-rewarding occupational value dimensions were significantly related to the individual’s perceived health. The results indicate that people who experience a good occupational balance in their patterns of daily occupations reported a higher level of perceived health. Furthermore, the results show that experiences of having a higher frequency of daily occupations rich with socio-symbolic occupational value also tends to improve the individual’s experience of health.
The results of this study thus show that occupational balance is associated with perceived health, thereby confirming the results of other studies [Citation20–22]. Furthermore, the experiences of occupational balance and occupational value were interrelated. In a way, the OBQ questioner captures aspects of some occupational value dimensions. The respondent rates experience of balance operationalized as e.g. recovery/sleep, meaningful occupations, the variety of occupations, etc. Aspects recognized also in the descriptions of occupational value dimensions [Citation17]. Thus, the results of this study strengthen the assumption that there is a relationship between a balanced everyday life with varied occupational values and self-perceived health. Furthermore, the results show the importance of having occupations in everyday life enriched with socio-symbolic occupational value to prevent ill health or promoting health. This is in line with previous results supporting the notion that the entire pattern of everyday life including work, and that strategies for promoting health should consider the person’s overall situation [Citation11]. That study concluded that the interplay between risk and health factors is unclear, however, the results showed that a general satisfaction with everyday occupations, a stress-free environment and general control in addition to not having monotonous movements at work explained 46.3% of the participants’ subjective good health and well-being [Citation11].
During this ongoing pandemic when many are urged to work from home and only socialize with our families, mental illness and a lower perceived health have become a greater problem than previously [Citation44], possibly because work and work identity offer experiences of socio-symbolic occupational value. For many people, work has many positive effects on our health, supports participating in society and is not primarily just ‘having something to do’ but promotes personal recovery and helps personal exploration [Citation45]. At the same time another side of the new work from home situation, emerges. A recent report including 2000 officials in Sweden showed that six out of ten that had to work from home during this ongoing pandemic, reported that the puzzle of life, and occupational balance had become easier to maintain [Citation46]. The complexity in the patterns of everyday life decreases in many families that may support experiences of health. Despite this, a result of the restrictions and lockdowns due to the pandemic, humans face new challenges regarding trying to maintain a variation in occupational values in a restricted context within their own home. There is a possibility that the demand for occupational therapists will increase as a result of these growing problems. Occupation is important to promote or maintain health and wellbeing, and to summarize, what we do, singularly or collectively affect our health and wellbeing [Citation16, p.458].
However, the concrete occupational value dimension did not show any statistically significant correlation to perceived health. A similar result has been found in other studies [Citation26,Citation47]. Concrete occupational value is linked to occupations that humans need and make sure to perform regardless of how they feel. In other words, occupations that cannot be dodged, such as children, family, bills, housework, etc., are occupations to a large extent performed by women, as demonstrated in another study [Citation48]. The result in this study, however, suggest that gender, being female more precisely, is not necessarily a risk factor for developing occupational imbalance and ill health. Instead, the results indicate that the individual’s patterns of daily occupations and the occupational values he or she embeds in relationship to the demands and conditions in his or her everyday life seem to be the main risk factor, regardless of gender. Given the small number of males within the sample this finding should be evaluated in future studies.
Methodological considerations
A quantitative cross-sectional design was chosen for this study to analyse the relationships between the different predictors used before the individuals embarked on a group treatment programme due to their occupational ill health. However, a cross-sectional study is a snapshot in which one may identify statistical relationships but not determine the direction of the relationship. Hence, more time is needed to follow up on how the different variables affect each other or whether there are additional variables that may have an impact. This could, for example, be done through interview studies or a longitudinal study design [Citation49].
This study included 218 people, 22 of whom were men and four who did not declare their gender. The low number of males might be problematic because we are interested in investigating gender as a potential predictor of health. All data collected with the selected instruments were included in the analyses in order to avoid a large external loss. The total number of potential data points was 8502 (218 * 39). There were no responses to 1028 of these, which resulted in an internal dropout rate of 12.1% (1028/8502), which still indicates a high response rate and thus a high level of reliability in the study [Citation49].
The individuals included in this study mirror Swedish sick leave statistics and are thus considered representative of the population, even though it would have been desirable to include more men, as women made up about 80% of the individuals in the study.
The individuals included answered the questionnaires before initiating an occupational therapy intervention aimed at promoting occupational balance and health in everyday life. The specific occupational therapy intervention, the ReDO® programme [Citation28], is not based on a specific diagnosis but can be used in general for people in need of adjusting their everyday life. This can be seen as a strength and opportunity to capture many people with occupational ill health already at an early stage as well as help reduce medicalization. A consequence of this strategy for inclusion, means that the participants can not clearly be defined by diagnose and the possibility to duplicate the study may decrease. This is, however, only a problem if the diagnoses are in focus for evaluation of the study. If the focus for inclusion is the same as the target for the intervention namely, to improve experiences of health and work ability thorough changes in patterns of daily occupations, the specific medical reason for challenges in everyday life is of less importance.
A consideration, however, involves the difference in the two databases, both in terms of size and data collection. The first database included a larger number of respondents, which could provide a larger range within the data. The data collection was also conducted through a physical meeting with an occupational therapist, and it was possible to ask questions if the participant had a hard time understanding something in the questions. The second database, on the other hand, contained a much smaller number of respondents. Furthermore, the data were collected through an e-platform, which gave the respondents the opportunity to answer the questions from a location of their choice but without anyone to ask in case of uncertainty. Whether the different approaches affected the data in this study is left unsaid.
Conclusion
The results of this study show that what we do, how we do it and why we do it have a positive, statistically significant effect on how we perceive our health. The study also highlights the importance of considering the patterns of daily occupations as a risk factor for developing occupational ill health, rather than the traditional factors of gender, education and work hours. This constitutes key knowledge that needs further research on how to promote health and prevent occupational ill health in society.
Acknowledgements
The authors express their gratitude to all the participants who have contributed with data for this study. We also would like to thank Region Sörmland, Lund University and Halmstad University for funding.
Disclosure statement
The authors report no conflicts of interest.
References
- Swedish National Board of Health and Welfare. 2017 [cited 2017 Oct 14]. Available from: www.kunskapsguiden.se/psykiatri/Teman/psykisk-ohalsa-hos-barn-unga/Sidor/Vad-arpsykisk-ohalsa.aspx [Swedish]
- Swedish Public Health Agency. National public health survey. 2020 [cited 2020 Apr 19]. Available from: https://www.folkhalsomyndigheten.se/livsvillkor-levnadsvanor/psykisk-halsa-och-suicidprevention/statistik-psykisk-halsa/ [Swedish]
- OECD. Health at a glance: Europe 2018. 2019 [cited 2019 Mar 17]. Available from: https://doi.org/https://doi.org/10.1787/health_glance_eur-2018-en
- Swedish Social Insurance Agency. Response to government assignments report - follow-up of sick leave development. 2018 [cited 2019 Oct 16]. Available from: https://www.forsakringskassan.se/wps/wcm/connect/d3d2d056-0ae7-46d9-b350-ac87e4696f1c/uppfoljning-av-sjukfranvarons-utveckling-2018.pdf?MOD=AJPERES&CVID [Swedish]
- Milczarek MS. OSH in figures: Stress at work — facts and figures. Luxembourg: European Communities. European Agency for Safety and Health at Work. 2020 [cited 2020 Feb 16]. Available from: https://osha.europa.eu/en/publications/osh-figures-stress-work-facts-and-figures
- Spasova S, Bouget D, Vanhercke B. Sick pay and sickness benefit schemes in the European Union. Background report for the Social Protection Committee’s in-depth review on sickness benefits. Brussels, Belgium: European Commission, European social policy network (ESPN); 2016.
- Eurostatistics. Statistics explained [Website]. EU 2020 [cited 2020 Oct 22]. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php/Genderstatistics
- Harvey S, Modini M, Joyce S, et al. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problem. Ann Occup Environ Med. 2017;74:301–310.
- Prevent. More and more men are suffering from mental illness [cited 2019 Feb 22]. Available from: https://www.prevent.se/Arbetsliv/halsa/2016/allt-fler-man-drabbas-av-psykisk-ohalsa/2016 [Swedish]
- Håkansson C, Ahlborg G. Perceptions of employment, domestic work, and leisure as predictors of health among women and men. J Occup Sci. 2010;17(3):150–157.
- Erlandsson LK, Carlsson G, Horstmann V, et al. Health factors in the everyday life and work of public sector employees in Sweden. Work. 2012;42(13):321–330.
- Holmgren K, Fjällström Lundgren M, Hensing G. Early identification of work-related stress predicted sickness absence in employed women with musculoskeletal or mental disorders: a prospective, longitudinal study in a primary health care setting. Disabil Rehabil. 2013;35(5):418–426.
- Hammell K-W. Dimensions of meaning in the occupations of daily life. Can J Occup Ther. 2004;71(5):296–305.
- Mårtensson L, Andersson C. Reading fiction during sick leave, a multidimensional occupation. Scan J Occup Ther. 2015;22(1):62–71.
- Ullah M, Fossey E, Stuckey R. The meaning of work after spinal cord injury: a scoping review. Spinal Cord. 2018;56(2):92–105.
- Wilkock AA, Hocking C. An occupational perspective on health. 3rd ed. Thorofare (NJ): Slack. 2015.
- Dorsey J, Ehrenfried H, Finch D, Jaegers LA. Work. In: Schell B, Gillen G, editors. Willard & Spackman’s occupational therapy. 13th ed. Philadelphia (PA): Wolters Kluwer; 2019.
- Wagman P, Håkansson C, Björklund A. Occupational balance as used in occupational therapy: a concept analysis. Scan J Occup Ther. 2012;19(4):322–327.
- Erlandsson LK, Persson D. The ValMO-model: occupational therapy for a healthy life by doing. Lund, Sweden: Studentlitteratur; 2020.
- Eklund M, Erlandsson LK, Persson D. Occupational value among individuals with long-term mental illness. Can J Occup Ther. 2003;70(5):276–284.
- Erlandsson LK, Eklund M, Persson D. Occupational value and relationships to meaning and health: Elaborations of the ValMO-model. Scan J Occup Ther. 2011;18(1):72–80.
- Taylor R. Kielhofner’s model of human occupation (theory and application). 5th ed. Philadelphia (PA): Wolters Kluwer Health; 2017.
- Erlandsson LK, Eklund M. The relationships of hassles and uplifts to experience of health in working women. Women Health. 2004;38(4):19–37.
- Erlandsson LK, Eklund M. Levels of complexity in patterns of daily occupations in relation to women’s well-being. J Occu Sci. 2006;13(1):27–36.
- Håkansson C, Ahlborg G. Occupational imbalance and the role of perceived stress in predicting stress-related disorders. Scan J Occu Ther. 2018;25(4):278–287.
- Karlsson L. Experience of occupation and ill health due to everyday life- before entering a ReDO intervention. [Master thesis]. Luleå, Sweden: Luleå University; 2018.
- Carter RE. Rehabilitation research. Principles and applications. St Louis (MO): Elsevier Saunders; 2011.
- Erlandsson LK. The Designing Daily Occupations (ReDO)-program: supporting women with stress-related disorders to return to work—knowledge base, structure, and content. Occu Ther Ment Health. 2013;29(1):85–101.
- Erlandsson LK, Bohs S, Håkansson C. ReDO-RS; occupational balance and work ability - evaluation of a prevention and rehabilitation method in region Skåne, for people in ongoing or at risk zone for sick leave. Lund, Sweden: Lunds University; 2017. [Unpublished Manucript].
- Olsson A, Erlandsson LK, Håkansson C. The occupation-based intervention REDO™-10: long-term impact on work ability for women at risk for or on sick leave. Scan J Occu Ther. 2020;27(1):47–55.
- Eklund M, Erlandsson LK, Persson D, et al. Rasch analysis of an instrument for measuring occupational value: implications for theory and practice. Scan J Occu Ther. 2009;16:118–128.
- Eakman A, Eklund M. Reliability and structural validity of an assessment of occupational value. Scan J Occu Ther. 2011;18(3):231–240.
- Wagman P, Håkansson C. Introducing the occupational balance questionnaire (OBQ). Scan J Occu Ther. 2014;21(3):227–231.
- Håkansson C, Dahlin-Ivanoff S, Sonn U. Achieving balance in everyday life. J Occu Sci. 2006;13(1):74–82.
- Wagman P, Håkansson C, Jacobsson C, et al. What is considered important for life balance? Similarities and differences among some working adults. Scan J Occu Ther. 2012;19(4):377–384.
- Brooks R. EuroQol: the current state of play. Health Policy. 1996;37(1):53–72.
- EuroQol Research Foundation. EQ-5D-3L user guide. 2018. Available from: https://euroqol.org/publications/user-guides
- Cöster M, Karlsson KM, Nilsson JÅ, et al. Validity, reliability, and responsiveness of a self-reported foot and ankle score (SEFAS). Acta Orthop. 2012;83(2):197–203.
- McNeish D. Thanks coefficient alpha, we’ll take it from here. Psy Met. 2018;23:412–433.
- Lemon SC, Roy J, Clark MA, et al. Classification and regression tree analysis in public health: methodological review and comparison with logistic regression. An Behav Med. 2003;26(3):172–181.
- Bittencourt N, Meeuwisse H, Mendonca D, et al. Complex systems appraoch for sports injuries: moving from risk factor identification to injury pattern recognition - narrative review and new concept. Br J Spo Med. 2016;50:1309–1314.
- Machuca C, Vettore MV, Krasuska M, et al. Using classification and regression tree modelling to investigate response shift patterns in dentine hypersensitivity. BMC Med Res Met. 2017;17:120.
- Venkatasubramaniam A, Wolfson J, Mitchell N, et al. Decision trees in epidemiological research. Emerg Theme Epidemiol. 2017;14:11.
- Panchal N, Kamal R, Orgera K, et al. 2020. KFF. The implications of COVID-19 for mental health and substance use. 2020 [cited 2020 Sep 21]. Available from: https://www.kff.org/coronavirus-covid-19/issue-brief/the-implications-of-covid-19-for-mental-health-and-substance-use/
- Bebout RR, Harris M. Personal myths about work and mental illness: response to Lysaker and Bell. Psychiatry. 1995;58:401–404.
- TCO Sweden. Report: the puzzle of life during the corona pandemic. 2021 [cited 2021 Feb 4]. Available from: https://www.tco.se/globalassets/2021/rapporter/tco_rapport_livspusslet-under-corona-mr.pdf
- Eklund M, Erlandsson LK. Return to work outcomes of the redesigning daily occupations (ReDO) program for women with stress-related disorders—A comparative study. Women Health. 2011;51(7):676–692.
- Björklund C. Occupational patterns and their relation to perceived satisfaction with life in general [Master thesis]. Luleå, Sweden: Luleå University; 2006. [Swedish]
- Polit DF, Beck CT. Nursing research, generating and assessing evidence for nursing practice. 9th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2001.