
Abstract
Background
The work participation of young adults with chronic physical conditions lag behind compared to healthy age-mates. ‘At Work’ is a vocational rehabilitation intervention provided by occupational therapists, that supports them for entering the competitive labour market after graduating post-secondary education.
Aim
To evaluate the effects of ‘At Work’ on self-efficacy, work-ability and employment status as compared to usual care.
Materials and methods
In total, 88 young adults were included in a multicentre controlled trial; 49 entered ‘At Work’, 39 received usual care. GEE-analyses were applied.
Results
Scores on all outcome measures substantially improved over time in the intervention group, but no significant effects were found as compared to the control group. The effect on general self-efficacy showed a positive trend in favour of the intervention group.
Conclusions and significance
Unlike previous study results pointing to positive outcomes of At Work’, the current study did not support the effectiveness of this program on work-related self-efficacy, work-ability and paid employment, as compared to usual care. Yet, we did find an indication for positive intervention effect on general self-efficacy, which is known to be an important capacity to achieve social participation.
Introduction
Despite of having both the desire and ability to work, the work participation of young adults with chronic physical conditions lag behind compared to healthy age-mates [Citation1–3]. Young adults with chronic physical conditions experience substantial difficulties when entering the competitive labour market, such as low self-esteem, lack of (life) skills, problems with disability disclosure, limited accessibility of buildings, limited adaptation of workplaces or working conditions, discrimination, and lack of support of manager or colleagues [Citation4–10]. Yet, it is important to promote the work participation of these young adults, since it helps them to get control over their lives and fosters the development of self-identity and achievement of personal occupational goals [Citation11–13].
Several vocational services are developed to support young people with chronic physical conditions in finding and maintaining employment. Occupational therapists are well-placed to deliver evidence based programs and services that promotes their work participation [Citation14]. Most of the present programs for this patient group mainly address the development of general life skills or provide support in finding temporary jobs as a student [Citation15–19]. To our knowledge, none of these programs are primarily focussed on supporting them to enter the competitive labour market after graduating from post-secondary education. To this specific aim, the ‘At Work’ program was developed in the Netherlands and implemented in some rehabilitation centres in the context of transition care [Citation20–23]. ‘At Work’ is a vocational rehabilitation intervention provided by occupational therapists and jobcoaches and supports young adults with chronic physical conditions to find and maintaining suitable competitive employment [Citation20–23]. The program is based on the Model of Human occupation (MOHO) [Citation24] and has an empowerment perspective. MOHO is a commonly used model in occupational therapy. It states that persons generate and modify their occupations in interaction with the environment. The model discerns three main components: motivation, habituation and performance capacity. Accordingly, during the ‘At Work’ intervention motivation for employment, productive roles and routines, and work-related life skills are addressed. The program aims to enhance the self-efficacy at work, knowledge, self-awareness and skills of the individuals, in order to help them solve problems they face in their process to work. Self-efficacy refers to the capacity to take action and deal with life stressors [Citation15]. ‘At Work’ offers a formal curriculum, including group education, peer-mentorship, simulation sessions, coaching and experimental learning [Citation20–23]. These intervention elements are evaluated as useful and appropriate to improve young adults’ (work-related) self-efficacy and life skills and to provide support for their vocational participation [Citation15–19,Citation22,Citation25]. A feasibility study of the ‘At Work’ program showed an increase in paid employment rates from 8.3% to 33.3% after 1 year and to 41.7% after 2 years [Citation20]. In a larger sample we showed that – starting from a disadvantaged position – paid employment rates of former participants increased substantially over time, approaching employment rates of national data of young people with chronic physical conditions [Citation23]. This was especially the case for those with severe physical limitations [Citation23]. The present study aims to evaluate the program’s effects on self-efficacy in solving work- and disease-related problems, self-perceived work-ability and employment status, as compared to usual care. We hypothesised a larger increase in work-related self-efficacy (primary outcome measure) in the intervention group (IG), compared to the control group (CG). The same pattern was expected for the secondary outcome measures addressing general self-efficacy, self- perceived work-ability and employment status. Thus, the study provides insights into the effects of vocational support provided by occupational therapists and jobcoaches.
Materials and methods
Design
We used the Consolidated Standards of Reporting Trials (CONSORT) [Citation26] statement to structure this article. This study was designed as a non-randomized non-blinded multicentre controlled trial (Netherlands Trial Register NL3922/NTR4145) [Citation27]. The IG consisted of participants of the ‘At Work’ program. The CG included young people with chronic physical conditions receiving usual rehabilitation care. All participants provided written consent, and were entered in a lottery to win a tablet as token of appreciation. The Erasmus MC Medical Ethical Review Board approved the study (MEC 2012-381). All participating centres granted local approval.
Vocational rehabilitation program ‘at work’
‘At Work’ is an out-patient multidisciplinary vocational rehabilitation intervention for young people (16–27 years) with chronic physical conditions, aiming to foster (work-related) self-efficacy and life skills and, and to improve sustainable work participation. Participants must have finished post-secondary education, or do so within six months, and wish to enter competitive employment, i.e. not seasonal or temporary employment. According to the model of human occupation (MOHO) [Citation24], motivation for employment, productive roles and routines, and skills are addressed during the ‘At Work’ intervention. In addition, an empowerment perspective is applied, in order to foster the self-efficacy and self-directed behaviour of participants [Citation20–23]. Vocational services provided by jobcoaches of a reintegration agency are integrated with specialised rehabilitation care with a large share of occupational therapy. A rehabilitation physician referred participants for the intervention, including six group-sessions and a one-year individual coaching trajectory. The intervention starts with an individual assessment by an occupational therapist. During this assessment, personal capacities are explored and personal goals for employment are determined using The Canadian Occupational Performance Measure (COPM) and the Occupational Performance History Interview (OPHI) [Citation28,Citation29]. After the individual intake, all participants take part in six group-sessions. These -sessions are facilitated by an occupational therapist and a jobcoach, and a psychologist is involved in those group-sessions addressing mental issues. Group-sessions aim to empower the participants and, thus, increase their self-efficacy, knowledge, work and life skills, and awareness of their own values and needs. Participants are trained in solving work- and disease-related problems, to ask for modifications or adjustment of working conditions, and to disclose their condition to others. Group-sessions entail peer-support, role modelling, experimental learning and education; these intervention elements were evaluated as useful and appropriate to improve young adults’ (work-related) life skills and to provide support for their vocational participation [Citation15–19,Citation22,Citation25]. The subsequent coaching trajectory is provided by the occupational therapist and a jobcoach. The occupational therapist help participants to reach personal goals as defined in the baseline assessment session that were not addressed during the group-sessions, e.g. to use public transport or to perform or organise their self-care activities. The individual coaching sessions provided by the jobcoach, are based on the supported employment methodology [Citation30] and support finding and applying for a suitable job, and dealing with the social and physical work environment, i.e. informing the employer and colleagues about the chronic physical condition, arranging workplace modifications or adjusted working conditions. The content, frequency and duration of individual coaching were adjusted to the participants’ personal needs and goals.
Study setting
‘At Work’ was developed in Rijndam Rehabilitation (Rotterdam), and subsequently implemented in two other rehabilitation centres, Reade Rehabilitation and Rheumatology (Amsterdam), and Basalt Rehabilitation (Leiden). These centres deployed an outpatient Young Adult Team, and collaborated locally with the same jobcoach agency ‘VolZin’. Rehabilitation professionals in these centres completed a ‘train the trainer course’, consisting of two three-hour sessions, aiming to: a) educate about the theoretical base, content and practical organisation of the intervention (including eligibility of participants, multidisciplinary collaboration); b) train interview skills for individual assessments at the start; c) inform and instruct professionals about this trial and data collection. Professionals indicated that the training gave them enough skills to implement and provide the ‘At Work’ Program. Also, engaging the same re-integration agency as part of the intervention in all intervention centres, facilitated a comparable implementation of the intervention across centres. CG-participants were recruited in eight other rehabilitation centres, located in other regions of the Netherlands.
Participants and recruitment
In the IG, a rehabilitation physician referred young adults with chronic physical conditions for the intervention. These conditions include for example cerebral palsy, spina bifida, rheumatoid arthritis, (neuro)muscular disease, or acquired brain injury. Intervention participants were eligible for inclusion in this study if they met each of the following inclusion criteria: a) age 16–27 years; b) not employed, or not suitably employed, defined as employment not consistent with the individual’s education, physical abilities and preferences; c) perceived problems with finding or maintaining competitive employment; d) finished education, or finishing education within 6 months; e) adequate understanding of Dutch language and; f) no severe intellectual impairments. A patient information letter was given to eligible patients.
To recruit participants for the CG, rehabilitation professionals (e.g. nurse, occupational or physical therapist) reviewed patient records in their databases, and compiled a list of candidates with chronic physical conditions who met the inclusion criteria. Employment status (inclusion criterion b) was checked by a self-report 4-item questionnaire enclosed with the patient information letter. Those who were not eligible for inclusion in the study, received an explanation for exclusion.
In order to detect a clinically relevant difference on the primary outcome measure Self-efficacy in solving work- and disease-related problems with a power of 0.8 and alpha of 0.05, 86 participants (43 in each group) would be required. Recruitment was stopped when the predefined number of participants was reached.
Measurements
Procedure
For data collection we used the online application GemsTracker, which has been developed by Erasmus MC and partners for distribution of questionnaires during clinical healthcare research. GemsTracker automatically sent out questionnaires on the date of inclusion (baseline, T0) and one year later (post-intervention, T1). At two-year follow-up (T2), we contacted participants by phone to verify their employment status at that time.
Primary and secondary outcomes
The outcome measures for this study were selected in line with the main goals of the program, and address self-efficacy at work (primary outcome measure), and general self-efficacy, as well as a person’s work ability and employment status (performance) as secondary outcomes. The questionnaire Self-efficacy in solving work- and disease-related problems comprises 14 items, yielding a total score between 14 and 70 (Cronbach’s alpha=.80) [Citation31]. The items of this questionnaire are presented in Box 1. We also assessed general self-efficacy with the 10-item General self-efficacy scale (GSES) as secondary outcome measure. The GSES yields a total score between 10 and 50 (Cronbach’s alpha=.83) [Citation32]. In both measures a higher score indicates the favourable outcome. The Self-efficacy in solving work- and disease-related problems questionnaire was the best available measurement instrument for the present study, since it was validated for persons with chronic conditions in the Netherlands [Citation31,Citation33], and showed good internal consistency of the scales (alpha 0.8) [Citation31,Citation33]. Since the Self-efficacy in solving work- and disease-related problems questionnaire was only used in a limited number of studies so far [Citation31,Citation33] we additionally used the General self-efficacy scale (GSES), which is a valid measure that is broadly used in populations of young adults with chronic physical conditions [Citation32,Citation34, Citation35]. Other secondary outcome measures addressed work ability and employment status, for which the instruments were in line with the previous feasibility study on the intervention [Citation20]. Participants indicated their self-perceived work-ability on the Work Ability Index – Single item (WAS) [Citation20,Citation36]. The WAS is derived from the WAI and consists of one question on the participant’s self-reported current work ability compared to his highest work ability ever (scoring from 0 to 10) [Citation36,Citation37]. Regarding employment status both paid and unpaid employment status (0 = no; 1 = yes) were specifically measured [Citation38]. Paid employment status was defined as performing a paid job for ≥12h/week, in accordance with the definition of Statistics Netherlands at the time of this study [Citation39]. Furthermore, in the intervention group we also distinguished whether the paid employment was in a sheltered or competitive work setting. These secondary outcome measures were validated for use or often used in studies on (young) people with chronic physical conditions [Citation20,Citation36–38,Citation40].
Background characteristics
Background characteristics were assessed at T0. Age, gender, and onset of chronic condition (0 = acquired; 1 = congenital) were recorded. Severity of physical limitations was assessed using the 7-item indicator of the Organisation for Economic Cooperation and Development (OESO) [Citation41], assessing physical limitations (3 items) and limitations in hearing and seeing (4 items) on a 4-point ordinal score (1 = no limitations (score of 1 on all items); 2 = slight limitation (score of 2 on at least one item); 3 = moderate limitation (scored of 3 on at least one item); 4 = severe limitation (score of 4 on at least one item). Educational level was categorised according to International Standard Classification of Education ISCED: 0 = pre-vocational practical education or lower; 1 = pre-vocational theoretical education or upper secondary vocational education; 2 = general secondary education, higher professional education, or university) [Citation42]. We also recorded special education (0 = no; 1 = yes); having an established occupational disability (0 = no; 1 = yes); paid work experience pre-intervention (0 = no; 1 = yes); unpaid work experience at pre-intervention (0 = no; 1 = yes); and length of job search period pre-intervention (1 = not yet searching; 2 = 0–1 year; 3 = 1 year and over). At T1, using a custom-made questionnaire participants in the CG indicated the support for work participation they had received in the past year, and the setting in which the support was provided (1 = jobcoach agencies, 2 = rehabilitation care, 3 = mental health care).
To monitor whether the ‘At Work’ intervention did not result in a decrease in health-related quality of life (HRQoL) due to physical or mental overload, in the IG HRQoL was measured using the 36-item Short-Form health survey (SF-36) [Citation43]. For each domain of the SF-36, sum scores were calculated and transformed to a score of 0–100, with higher scores reflecting better HRQoL. In addition, scores were summarised in the Physical Component Summary (PCS) and Mental Component Summary (MCS), with an expected distribution of 50 (SD = 10) in the general population. The Dutch language version of the SF-36 is validated for use in populations with chronic conditions [Citation44].
Analysis
Statistical analyses were performed with SPSS version 25.0. Demographic characteristics are presented using descriptive statistics. Chi-square-tests for dichotomous variables and one-sample t-tests for continuous variable were applied to test for differences between IG and CG at baseline, to check for selective drop-out of responders at T1, and for paid and unpaid employment also at T2.
General Estimation Equation (GEE) analyses with unstructured correlation structures were performed to determine intervention effects, following an intention-to-treat protocol. Imputation of missing data is not needed, because all available data of the outcomes are used and not only completed cases [Citation45]. A GEE-model was chosen because a) it corrects for dependency of observations within an individual and for missing values; and b) it is robust for relatively small sample sizes [Citation45].
To compare scores on self-efficacy in solving work- and disease-related problems, general self-efficacy and self-perceived work-ability for time interval T0-T1, the moment of measurement and the interaction between group allocation and moment of measurement were added to the GEE model as independent variables. For Paid employment status, which was assessed at T0, T1 and T2, group allocation, baseline values, measurement time and the interaction variable between group allocation and measurement time were added to the GEE model to estimate group differences for different time intervals (T0-T1 and T0-T2). For continuous variables, the regression coefficient (B) is displayed for the group variable (representing between-group differences). For dichotomous variables, between-group differences are indicated as odds ratios (ORs). The CG was specified as the reference group for all analyses. All models were adjusted for gender, onset of the chronic condition, severity of physical limitations, and having attended special education, because the IG and CG differed on these variables at T0. Finally, in order to monitor changes in the HRQoL of the IG, we used descriptive statistics to check whether the HRQoL scores did not decrease during the intervention period in IG participants achieving paid employment at T1 (n = 5), as compared to participants without paid work at T1 (n = 24).
Results
Study sample
Background characteristics of the total study sample, and broken down for the IG and CG, are presented in . In a 5 year period 49 eligible young adults who entered the ‘At Work’ program consented to participate in the study, of whom 30 (61.2%) completed the study at T1. In the same period 39 patients in the control centres consented to participate in the CG, of whom 28 (71.8%) completed the questionnaires at T1.
Table 1. Background characteristics of intervention and control group.
The IG (n = 49) and CG (n = 39) significantly differed for some background characteristics: participants in the IG were more often male (57.1% versus 35.9%), had less often a congenital condition (14.3% versus 43.6%) or severe physical limitations (14.3% versus 43.6%), and had less often attended special education (24.5% versus 46.2%).
Unfortunately, substantial drop-out occurred; the reasons for drop-out are unknown. At T1, drop-outs were younger than completers (respectively 21.46 yrs, SD = 3.28 versus 23.73 yrs, SD = 2.43; p = .004), and at both T1 and T2, drop-outs were more often male (respectively, 78.6%, p = .01; and 62.9%, p = .02). At T2, drop-outs had more often experience with paid work at baseline (60%, p = .04) and were less often looking for employment for more than one year (17%, p = .04). None of these characteristics were significantly correlated with the primary outcome self-efficacy in solving work- and disease-related problems.
Support received in the CG
Completers in the CG (n = 28) received usual care, which in 50% of the cases contained some form of vocational support, consisting of: a) support on work-readiness, e.g. gaining insight into personal interests, physical capacities, and mental capacities; assertiveness training; and education (n = 9); b) job search assistance (n = 9); or c) jobcoaching (n = 5). Seven of them received two or more of these components of vocational support, for example support at work-readiness and job-search assistance or job-search assistance and jobcoaching.
Intervention effects
The data over time are shown in and and ; the corresponding GEE analysis results are presented in . At T0, the IG started from a disadvantaged position as compared with the CG, with significantly lower scores on general self-efficacy (p=.04), self-perceived work-ability (p<.001), and paid employment (p<.001).
Figure 1. Self-efficacy in solving work- and disease related problems, general self-efficacy, and self-perceived work-ability over time. Measurement time: T0 = baseline, T1= post-intervention (at 1 year), T2= two-year follow-up; Scale Scores on outcome measures: A) Self-efficacy in solving work- and disease-related problems questionnaire [Score range 14–70]; B) GSES, General self-efficacy scale [score range 10–50]; C) WAS, Single Work Ability Index – Single item [Score range 1–10]. ^Intervention group significantly differs from control group at T0, p=.04, *Positive trend was found, p=.06, ^^Intervention group significantly differs from control group at T0, p<.001,
![Figure 1. Self-efficacy in solving work- and disease related problems, general self-efficacy, and self-perceived work-ability over time. Measurement time: T0 = baseline, T1= post-intervention (at 1 year), T2= two-year follow-up; Scale Scores on outcome measures: A) Self-efficacy in solving work- and disease-related problems questionnaire [Score range 14–70]; B) GSES, General self-efficacy scale [score range 10–50]; C) WAS, Single Work Ability Index – Single item [Score range 1–10]. ^Intervention group significantly differs from control group at T0, p=.04, *Positive trend was found, p=.06, ^^Intervention group significantly differs from control group at T0, p<.001,](/cms/asset/429fbfd9-59c6-441b-b29c-c18372d2440e/iocc_a_2228019_f0001_b.jpg)
Figure 2. Paid and unpaid employment status over time. Measurement time: T0 = baseline, T1= post-intervention (at 1 year), T2= two-year follow-up. ^Intervention group significantly differs from control group at T0, p<.001.
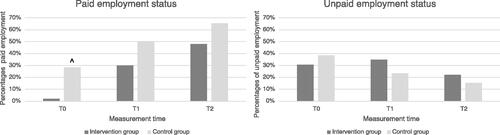
Table 2. Outcome measures for intervention and control groups.
Table 3. Longitudinal generalised equation results for between-group analyses in outcome measure, uncorrected and corrected for gender, onset of the chronic condition, severe physical limitations, and special education.
Self-efficacy in solving work- and disease-related problems, general self-efficacy and self-perceived work-ability
In both the IG and CG, participants improved on all outcomes during the intervention period. Corrected for gender, onset of the chronic condition, having severe physical limitations and having attended special education, no significant difference between IG and CG was found on the primary outcome self-efficacy in solving work- and disease-related problems (b = .81; 95%CI= −2.89 to 4.51; p = .67), nor on self-perceived work-ability (b = .14; 95%CI= -,90 to 1.18; p = .63). For general self-efficacy a trend was found (b = 1.78; 95%CI= −.28 to 3.84; p = .06), suggesting a larger increase in the IG as compared to the CG.
Employment status
In both the IC and the CG, the proportions of participants with paid employment increased during the intervention period and further increased up to 2-year follow-up. After correcting for gender, onset of the chronic condition, having severe physical limitations and having prior special education, no significant differences between IG and CG with respect to paid employment status or unpaid employment status were found after one year (T0-T1: respectively b = .34; 95%CI= .09 to 1.25; p = .10 and b = 1.77; 95%CI= .54 to 5.77; p = .35) and after two year (T0-T2: respectively b = .50; 95%CI= .10 to 2.43; p = .39 and b = 1.35; 95%CI= .35 to .53; p = .67).
Health related quality of life
The HRQoL scores in the IG were stable over time or seemed to increase more for participants with paid employment at T1 compared to those without paid employment at T1 (Appendix A).
Discussion
The ‘At Work’ program is – to our knowledge – the first intervention that is specifically developed for young adults with chronic physical conditions facing barriers to enter the competitive labour market. In a previous study we showed that– starting from a disadvantaged position – paid employment rates of intervention participants substantially increased over time, approaching the employment rates of national reference data of persons with chronic physical conditions [Citation23]. Results of a qualitative study indicated that young adults highly appreciated the components of the ‘At Work’ program (e.g. peer-support, skills training, role-playing) and perceived them effective to support their (work-related) self-efficacy and life skills development [Citation22], which was in line with other studies [Citation15–19]. Also for employed persons with chronic physical conditions hampering work participation on-the-job training and job placement assistance were found to be effective to improve their work participation [Citation46–48]. In the present study we compared the effects of the intervention with a control group receiving usual rehabilitation care. In the IG all outcomes improved over time. In the CG, however, similar patterns were seen, albeit it to a lesser extent. As a result, this study did not provide evidence for the intervention’s effectiveness as compared to usual care. The results, however, do suggest a positive effect of the intervention on general self-efficacy, which tended to increase more strongly for participants of the ‘At Work’ program compared to those receiving usual care. Self-efficacy is considered important for youth success and being prepared for several aspects of adult life and independency [Citation15].
Methodological considerations
A clear strength of this study is the two-year follow-up for the outcome paid employment status. This met the expectation that young adults with chronic physical disabilities have to overcome many obstacles to achieve paid employment (e.g. low self-esteem or a lack of life skills, problems with disability disclosure and travelling to work), resulting in longer lead times before effects of an intervention on this outcome can be detected [Citation20]. Also, the long-term follow-up was substantiated by the increasing employment rates of former ‘At Work’ participants until 2 years after the intervention. [Citation23].
Also, some weaknesses should be mentioned. First, the recruitment of participants for the CG in this non-randomized design was difficult and might have resulted in a less comparable CG. In contrast to the intervention centres, most control centres did not provide specialised transition care, and the continuation of rehabilitation care is often hampered between paediatric and adult care. Thus, the control centres might have lost contact with young people in their early twenties with specific needs regarding social participation, including employment, and had to rely on former patient files for the inclusion. The flawed comparability of both groups might have hampered the detection of differences in intervention effects between the two groups. At baseline, the work outcomes of the IG and CG differed substantially, with higher scores on all outcomes in the CG, indicating less severe problems on average or different problems (e.g. overestimation of own abilities). Also, half of the CG did receive some kind of vocational support, which was probably adequate for them to achieve positive outcomes. It is important to further investigate what works for whom, and more specifically which young adults have a need for more intensive vocational support, such as the ‘At Work’ program. Especially occupational therapists can, based on their clinical experience, help to identify subgroups of young adults with specific support needs [Citation14]. These insights may help to further tailor the intensity of vocational support to a person’s needs, and to fine-tune the inclusion criteria for the more intensive ‘At Work’ program.
Other limitations of this study address the outcome measures used. For work-related self-efficacy we had to use a less-than-ideal measurement instrument for this specific target group that is at the start of a work career, a situation which is inherently different from dropping-out and returning to work. A sensitive outcome measure specifically addressing work-related self-efficacy or work readiness of young adults entering the labour market was not yet available. We selected the ‘self-efficacy in solving work- and disease-related problems questionnaire’ as primary outcome measure, although this was originally developed for adult employees with a chronic physical disease, who experienced problems in their employment [Citation31]. This instrument showed to be less appropriate to measure work-related self-efficacy among young adults with ample work experience and a lack of context to appraise their self-efficacy at work. A possible indication for this problem is a relatively low Cronbach’s alpha for this measure in the present sample (.67). There is a need for age- or developmentally appropriate outcome measures to capture work-related self-efficacy or work readiness in starters entering the labour market. Furthermore, whereas we know from the measurements that paid employment of participants in the IG was all competitive, we assume that the assessed paid employment in the CG also comprised sheltered employment. The latter assumption is based on the observation of relatively high proportions of CG-participants with severe physical limitations and previous special education (). We estimate that about 15% of the paid employment of participants in the CG may refer to sheltered employment, based on the work participation of young adults with cerebral palsy [Citation49]. In future studies on the effects of vocational rehabilitation interventions, it is recommended to distinguish between sheltered employment and regular employment in the assessment of employment status.
Clinical implications
Starting from a disadvantaged position, at least equivalent effects were found in the intervention group as compared to a control group in rehabilitation care. With that and because of the effects of the ‘At Work’ program on sustainable work participation in the long term, it might be worth providing such an intensive program to support young adults with chronic physical conditions who face barriers as starters in the competitive labour market. The results suggest to further tailor the type and intensity of vocational support for young adults with chronic physical conditions entering the labour market.
Conclusion
Unlike several previous study results pointing to positive outcomes of the ‘At Work’ program, the current study did not add to the evidence on its effectiveness on work-related self-efficacy, self-perceived work-ability and employment status as compared to usual care. Yet, we did find an indication for positive intervention effect on general self-efficacy, which is known to be an important capacity to achieve optimal social participation. Challenges to optimise future effectiveness studies on vocational rehabilitation programs in this age group transitioning to adulthood address the comparability of the intervention and control group and the use of a more sensitive outcome measure to capture preparedness for work among starters in the labour market.
Acknowledgements
The authors are grateful to all participants in the study; Joan Verhoef PhD is acknowledged for her valuable contribution to the design, implementation and pilot evaluation of the ‘At Work’ intervention. Rijndam Rehabilitation in Rotterdam (Jetty van Meeteren MD PhD, Monique Floothuis MSc), Reade Rehabilitation and Rheumatology in Amsterdam, Basalt Rehabilitation in Leiden (Winnifred Molenaar, Carin Froberg), and Bureau VolZin (Natasha van Schaardenburgh BA, Theo Blom BA, Jolie Derkx BA) are thanked for their efforts on recruiting participants and providing the ‘At Work’ intervention. Hoogstraat Rehabilitation in Utrecht, Libra Rehabilitation in Tilburg/Eindhoven, Department of Rehabilitation Medicine of Amsterdam University Medical Centres/VU, Revant Rehabilitation in Breda/Goes, Merem Treatment Centre de Trappenberg in Hilversum/Almere, Rehabilitation Centre Roessingh in Enschede, Department of Rehabilitation Medicine/Centre for Rehabilitation of University Medical Centre Groningen and Adelante Rehabilitation in Hoensbroek are thanked for their efforts on recruiting participants for the control group.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Box 1. The items of the self-efficacy in solving work- and disease-related problems questionnaire.
1. I am able to talk to my supervisor about adaptions in working conditions
2. I am able to mention problems that I experience at work
3. I am not able to set my boundaries at work
4. If I need some adjustments at work, then I am able to explain what I need
5. I am able to talk to my colleagues about my chronic condition
6. I am able to find out the work modifications that are available to me
7. I am able to figure out the legislation and regulations
8. I am able to ask the right people for help at work, if I can’t do it by myself.
9. I am able to manage my work in such a way, that I do not get stressed
10. I am not able to negotiate with my supervisor about my tasks at work
11. If my colleagues react negatively to my chronic conditions, then I am able to deal with their reactions.
12. I am able to manage my work in such a way, that I have enough energy in the evening.
13. I am able to ask for help at work, if I can’t do it on my own.
14. I am able to get the attention of my supervisor, when I have to tell something
Additional information
Funding
References
- Experts TANoED. The labour market situation of disabled people in european countries and implementation of employment policies: a summary of evidence from country reports and research studies. Leeds: Academic Network of European Disability Experts (ANED); 2009.
- Eurostat. European social statistics. Luxembourg: European Commission; 2013.
- Yildiz B, Burdorf A, Schuring M. The influence of chronic diseases and multimorbidity on entering paid employment among unemployed persons – a longitudinal register-based study. Scand J Work Environ Health. 2021;47:208–216. doi: 10.5271/sjweh.3942.
- Lindsay S, McPherson AC, Maxwell J. Perspectives of school-work transitions among youth with spina bifida, their parents and health care providers. Disabil Rehabil. 2017;39:641–652. doi: 10.3109/09638288.2016.1153161.
- Achterberg TJ, Wind H, de Boer AG, et al. Factors that promote or hinder young disabled people in work participation: a systematic review. J Occup Rehabil. 2009;19:129–141. doi: 10.1007/s10926-009-9169-0.
- Shier M, Graham J, Jones ME. Barriers to employment as experienced by disabled people: a qualitative analysis in calgary and regina, Canada. Disabil Soc. 2009;24:63–75. doi: 10.1080/09687590802535485.
- Roessler R, Neath J, McMahon B, et al. Workplace discrimination outcomes and their predictive factors for adults with multiple sclerosis. Rehabil Couns Bul. 2007;50:139–152. doi: 10.1177/00343552070500030201.
- Lindsay S. Discrimination and other barriers to employment for teens and young adults with disabilities. Disabil Rehabil. 2011;33(15-16):1340–1350. doi: 10.3109/09638288.2010.531372.
- Lindsay S, McDougall C, Menna-Dack D, et al. An ecological approach to understanding barriers to employment for youth with disabilities compared to their typically developing peers: views of youth, employers, and job counselors. Disabil Rehabil. 2015;37:701–711. doi: 10.3109/09638288.2014.939775.
- Lindsay S, Cagliostro E, Carafa G. Disability disclosure and workplace accommodations among youth with disabilities. Disabil Rehabil. 2018;40:2971–2986. doi: 10.1080/09638288.2017.1363824.
- Hall JP, Kurth NK, Hunt SL. Employment as a health determinant for working-age, dually-eligible people with disabilities. Disabil Health J. 2013;6:100–106. doi: 10.1016/j.dhjo.2012.11.001.
- Pawłowska-Cyprysiak K, Konarska M, Zołnierczyk-Zreda D. Self-perceived quality of life of people with physical disabilities and labour force participation. Int J Occup Saf Ergon. 2013;19:185–193. doi: 10.1080/10803548.2013.11076977.
- Liljeholm U, Bejerholm U. Work identity development in young adults with mental health problems. Scand J Occup Ther. 2020;27:431–440. doi: 10.1080/11038128.2019.1609084.
- American occupational therapy association. Occupational therapy in the promotion of health and well-being. Am J Occupat Ther. 2020;74:1–14. doi: 10.5014/ajot.2020.743003.
- King G, McPherson AC, Kingsnorth S, The Ontario Independence Program Research (OIPR) Team., et al. Opportunities, experiences, and outcomes of residential immersive life skills programs for youth with disabilities. Disabil Rehabil. 2021;43:2758–2768. doi: 10.1080/09638288.2020.1716864.
- Kingsnorth S, Healy H, Macarthur C. Preparing for adulthood: a systematic review of life skill programs for youth with physical disabilities. J Adolesc Health. 2007;41:323–332. doi: 10.1016/j.jadohealth.2007.06.007.
- Kingsnorth S, King G, McPherson A, et al. A retrospective study of past graduates of a residential life skills program for youth with physical disabilities. Child Care Health Dev. 2015;41:374–383. doi: 10.1111/cch.12196.
- Lindsay S, Adams T, McDougall C, et al. Skill development in an employment-training program for adolescents with disabilities. Disabil Rehabil. 2012;34:228–237. doi: 10.3109/09638288.2011.603015.
- Lindsay S, Lamptey DL, Cagliostro E, et al. A systematic review of post-secondary transition interventions for youth with disabilities. Disabil Rehabil. 2019;41:2492–2505. doi: 10.1080/09638288.2018.1470260.
- Verhoef JA, Miedema HS, Van Meeteren J, et al. A new intervention to improve work participation of young adults with physical disabilities: a feasibility study. Dev Med Child Neurol. 2013;55:722–728. doi: 10.1111/dmcn.12158.
- Verhoef JA, Roebroeck ME, van Schaardenburgh N, et al. Improved occupational performance of young adults with a physical disability After a vocational rehabilitation intervention. J Occup Rehabil. 2014;24:42–51. doi: 10.1007/s10926-013-9446-9.
- Bal MI, Sattoe JN, van Schaardenburgh NR, et al. A vocational rehabilitation intervention for young adults with physical disabilities: participants’ perception of beneficial attributes. Child Care Health Dev. 2017;43:114–125. doi: 10.1111/cch.12407.
- Bal MI, Roelofs PPDM, Hilberink SR, et al. Entering the labor market: increased employment rates of young adults with chronic physical conditions after a vocational rehabilitation program. Disabil Rehabil. 2021;43:1965–1972. doi: 10.1080/09638288.2019.1687764.
- Kielhofner G, Braveman B, Finlayson M, et al. Outcomes of a vocational program for persons with AIDS. Am J Occup Ther. 2004;58:64–72. doi: 10.5014/ajot.58.1.64.
- Lindsay S, Varahra A. A systematic review of self-determination interventions for children and youth with disabilities. Disab Rehabil. 2022;44:5341–5362. doi: 10.1080/09638288.2021.1928776.
- Campbell MK, Piaggio G, Elbourne DR, for the CONSORT Group, et al. Consort2010 statement: extension to cluster randomised trials. BMJ. 2012;345:e5661. doi: 10.1136/bmj.e5661.
- Dutch Trial Register. Find a trial. 2021. https://www.trialregister.nl/trial/3922
- Law M, Baptiste S, Carswell A, et al. N Canadian occupational performance measure. Ottawa: CAOT Publications ACE; 1998
- Kielhofner G, Mallinson T, Crawford C, et al. A user’s manual for the occupational performance history interview (version 2.0). Chicago: The Model of Human Occupation Clearing House; 1998
- Bond GR, Drake RE, Campbell K. Effectiveness of individual placement and support supported employment for young adults. Early Interv Psychiatry. 2016;10:300–307. doi: 10.1111/eip.12175.
- Varekamp I, Verbeek JH, de Boer A, et al. Effect of job maintenance training program for employees with chronic disease - a randomized controlled trial on self-efficacy, job satisfaction, and fatigue. Scand J Work Environ Health. 2011;37:288–297. doi: 10.5271/sjweh.3149.
- Scholz U, Gutiérrez Doña B, Sud S, et al. Is general Self-Efficacy a universal construct. Eur J Psychol Assess. 2002;18:242–251. doi: 10.5271/sjweh.3149.
- Detaille SI, Heerkens YF, Engels JA, et al. Effect evaluation of a self-management program for dutch workers with a chronic somatic disease: a randomized controlled trial. J Occup Rehabil. 2013;23:189–199. doi: 10.1007/s10926-013-9450-0.
- International Consortium for Health Outcomes Measurement. Overall pediatric health. 2023.
- Markwart H, Bomba F, Menrath I, et al. Assessing empowerment as multidimensional outcome of a patient education program for adolescents with chronic conditions: a latent difference score model. PLoS One. 2020;15:e0230659. doi: 10.1371/journal.pone.0230659.
- Ahlstrom L, Grimby-Ekman A, Hagberg M, et al. The work ability index and single-item question: associations with sick leave, symptoms, and health—a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;36:404–412. doi: 10.5271/sjweh.2917.
- Tuomi K, Ilmarinen J, Jahkola A, et al. Work ability index. 2nd rev. ed. Helsinki: Finnish Institute of Occupational Health; 1998.
- Bouwmans C, Krol M, Severens H, et al. The iMTA productivity cost questionnaire: a standardized instrument for measuring and valuing Health-Related productivity losses. Value Health. 2015;18:753–758. doi: 10.1016/j.jval.2015.05.009.
- Statistics Netherlands [internet]. Den Haag: statistics Netherands. 2019. www cbs.nl/en-GB/menu/themas/arbeid-sociale-zekerheid
- Lindsay S. Employment status and work characteristics among adolescents with disabilities. Disab Rehabil. 2011;33:843–854. doi: 10.3109/09638288.2010.514018.
- Botterweck A, Frenken F, Janssen S, et al. Plausibiliteit nieuwe metingen algemene gezondheid en leefstijlen 2001. Heerlen: Central Bureau of Statistics (CBS); 2021. https://www.cbs.nl
- Unesco. International Standard Classification of Education. Montreal: Unesco Institute for statistics; 2021. http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf
- Aaronson NK, Muller M, Cohen PD, et al. Translation, validation, and norming of the dutch language version of the SF-36 health survey in community and chronic disease populations. J Clin Epidemiol. 1998;51:1055–1068. doi: 10.1016/s0895-4356(98)00097-3.
- Slaman J, van den Berg-Emons HJ, van Meeteren J, et al. A lifestyle intervention improves fatigue, mental health and social support among adolescents and young adults with cerebral palsy: focus on mediating effects. Clin Rehabil. 2015;29:717–727. doi: 10.1177/0269215514555136.
- Twisk J, de Vente W. Attrition in longitudinal studies. How to deal with missing data. J Clin Epidemiol. 2002;55:329–337. doi: 10.1016/s0895-4356(01)00476-0.
- Vooijs M, Leensen MC, Hoving JL, et al. Interventions to enhance work participation of workers with a chronic disease: a systematic review of reviews. Occup Environ Med. 2015;72:820–826. doi: 10.1136/oemed-2015-103062.
- Huang IC, Holzbauer JJ, Lee EJ, et al. Vocational rehabilitation services and employment outcomes for adults with cerebral palsy in the United States. Dev Med Child Neurol. 2013;55:1000–1008. doi: 10.1111/dmcn.12224.
- Verhoef JAC, Bal MI, Roelofs PDDM, et al. Effectiveness and characteristics of intervention to improve work participation in adults with chronic physical disabilities: a systematic review. Disabil Rehabil. 2022;44:1007–1022. doi: 10.1080/09638288.2020.1788180.
- Verhoef JA, Bramsen I, Miedema HS, et al. Development of work participation in young adults with cerebral palsy: a longitudinal study. J Rehabil Med. 2014;46:648–655. doi: 10.2340/16501977-1832.