
ABSTRACT
An extended professional identity theory is proposed to enhance interprofessional collaboration. The purpose of this study is to investigate whether comparative feedback on interprofessional interaction can decrease the degree of profession-based dominance and general dominance in mixed profession groups. This observational study comprised a randomized double-blind pretest-posttest control group design with 19 mixed profession groups (10 intervention and nine control groups, each with three dental and three dental hygiene students). All groups received reflective feedback during two consecutive two hour team development meetings. Intervention groups also received comparative feedback. Profession-based dominance concerned the sum of three observation items (conversational turn-taking, dominance and contributing ideas) with a three-point scale: −1 = dental dominance, 0 = no dominance, +1 = dental hygiene dominance. Polychoric correlations confirmed positive associations with the latent trait and an unidimensional underlying structure. Observation items were internally consistent (α > .70). General dominance concerned the sum of absolute values of observation items with a minimum value of zero (no dominance) and the maximum value of three (strong dominance). A two-way factorial ANOVA was performed. The results revealed a significant interaction effect with regard to general dominance, F(1,17) = 6.630, p = 0.020 and large effect size (partial eta squared = 0.28). Comparative feedback on interprofessional interaction decreases general dominance in mixed profession groups.
Changing demographics (e.g., Baumgartner, Schimmel, & Müller, Citation2015; Thistlethwaite, Citation2012; WHO, Citation2012), increasing the complexity of work (e.g., Hood, Citation2012; Koné Pefoyo et al., Citation2015; Vettore, Meira, Rebelo, Rebelo Vieira, & Machuca, Citation2016) and fragmentation through increasing specialization (e.g., Agha, Frandsen, & Rebitzer, Citation2017; Teece & Abdulrahman, Citation2011; Tsoukas & Vladimirou, Citation2001) are three important reasons that increase the necessity to integrate services. The challenge of integrating services of different disciplines and organizations is prominent in health care (Hood, Citation2012; Xyrichis, Reeves, & Zwarenstein, Citation2017), social work (e.g., Archibald & Estreet, Citation2017; Bolin, Citation2016) and information technology (e.g., Bryan Jean, Sinkovics, & Kim, Citation2014; Gal, Blegind Jensen, & Lyytinen, Citation2014). Integrated services are the outcome of interprofessional collaboration (Headrick, Wilcock, & Batalden, Citation1998). However, such collaboration can be limited by social psychological processes during which ingroup members favour each other while simultaneously enhancing outgroup derogation which leads to intergroup competition (Tajfel & Turner, Citation1979; Liao, O’Brien, Jimmieson, & Restubog, Citation2015; McNeil, Rebecca, Mitchell & Parker, Citation2013). Between professions, these ingroup-outgroup behaviours become visible in the degree of profession-based dominance (e.g., Morison, Marley, Stevenson, & Milner, Citation2008; Palaganas, Epps, & Raemer, Citation2014; Ross, Turner, & Ibbetson, Citation2009). To overcome this type of intergroup behaviour between members of different professions, intergroup contact is applied as a common educational intervention to enhance positive attitudes between different professional groups (e.g., Hayashi et al., Citation2012; Hertweck et al., Citation2012; Matziou et al., Citation2014; Robben et al., Citation2012). However, only intergroup contact between members from different professions (such as multiprofessional education; MPE) is not enough to produce attitude changes (Carpenter & Dickinson, Citation2016). According to Allport (Citation1954), four conditions are required besides mere intergroup contact: support of authorities (institutional support), working towards common goals, cooperation and equal status within the contact situation are also necessary. Four additional conditions were identified by other researchers: positive expectations, successful joint work, similarities versus differences and the perception that outgroup members are typical representatives of their group (Hewstone & Brown, Citation1986).
During interprofessional education (IPE), students from different professions learn about each other by working together on assignments that enhance interprofessional collaboration (Reeves et al., Citation2016). Several studies report that this collaborative work in mixed profession groups can positively influence interprofessional attitudes, knowledge and skills. A recent study reports that professional identification within a mixed profession group can have a negative effect on interprofessional attitudes of one professional subgroup while having a positive effect on attitudes of another (Sollami, Caricati, & Mancini, Citation2017). The exclusive nature of professional identity can prevent the inclusion of other professionals when working together (Whittington, Citation2003). In addition, several other authors are also convinced that professional identity plays a key role in limiting or enhancing interprofessional collaboration (e.g., Baker, Egan-Lee, Martimianakis, & Reeves, Citation2011; Carpenter & Dickinson, Citation2016; Hammick, Freeth, Copperman, & Goodsman, Citation2009; Khalili, Orchard, Spence Laschinger, & Farah, Citation2013). A professional identity is a social identity that consists of three aspects: belonging, commitment and beliefs (Barbour & Lammers, Citation2015; Liao et al., Citation2015). Just changing the beliefs such as attitudes towards other professions and interprofessional teamwork might not be sufficient. Changing attitudes does not have to change a sense of belonging and commitment to an interprofessional team. Even more so, commitment and attitude are two distinct phenomena (Meyer & Herscovitch, Citation2001). Commitment can influence behaviour even in the absence of extrinsic motivation or positive attitudes. Based on these arguments, changing attitudes towards interprofessional education and collaboration will not be a sufficient predictor of interprofessional communication even though this is a common approach for enhancing interprofessional collaboration (e.g., Hayashi et al., Citation2012; Hertweck et al., Citation2012; Matziou et al., Citation2014; Robben et al., Citation2012).
Interprofessional communication becomes apparent in non-hierarchical behaviours and implies reciprocity between different professions (D’Amour, Ferrada-Videla, San Martin Rodriguez, & Beaulieu, Citation2005; Headrick et al., Citation1998). Profession-based dominance can limit the collaboration between members of different professions (Edmondson, Citation2003) as non-hierarchical groups are more productive in the sense that individuals have a higher identification with their enterprise, feel more committed and consequently work more efficiently and productively (Godard & Delaney, Citation2000; Huselid, Citation1995; Ichniowski, Shaw, & Prennushi, Citation1997; Wenga & Carlsson, Citation2015). Hierarchy is a rank order of individuals or groups on a valued social dimension (Magee & Galinsky, Citation2008) and is common to all social groups including professions (Brown, Citation1991). The degree of profession-based dominance is represented by the relative dominance between professions (Cheng, Tracy, Foulsham, Kingstone, & Henrich, Citation2013; Cheng, Tracy, & Henrich, Citation2010) and is visible in several observable behaviours. It is also visible in asymmetry during conversational turn-taking (Bateson, Citation1972; Corser, Citation1998; West, Citation1979), i.e., dominant individuals tend to talk more often than those that are less dominant. Non-hierarchical behaviour concerns a behavioural pattern characterized by similar behaviour of interacting individuals (Bateson, Citation1972). According to the interaction theory (Gallagher, Citation2008, Citation2005), our understanding of others is based on our interactions and perceptions. It is also inherent to socialization (Clausen, Citation1968). The claim-affirmation model of Holmes (Citation2001) describes the process of professional socialization in which individuals claim or disclaim their professional attributes and affirm or disaffirm other people’s professional attributes. This process reflects the relationship between the members of different professions and is visible in profession-based dominance. Non-hierarchical communication between group members becomes apparent in the willingness to share (Guzzo, Citation1995; Yukelson, Weinberg, & Jackson, Citation1984) and is especially functional when group tasks require a broad range of ideas and perspectives (Anderson & Brown, Citation2010). Intergroup comparison can enhance intragroup collaboration (Böhm & Rockenbach, Citation2013) because it enhances social identification. This identification is associated with perceived intragroup similarity through psychological distinctiveness from another group (Tajfel & Turner, Citation1979). Such intragroup similarity is associated with greater group cohesion. Commitment increases within a group and is a direct determinant of behaviours that benefit ingroup members (Bergami & Bagozzi, Citation2000). When members of different professions identify with an interprofessional group, they are also likely to display ingroup behaviours accordingly. If so, professional subgroups in a mixed profession group are likely to show less profession-based dominance. In addition, mixed profession groups in which interprofessional identification is not facilitated will probably show more profession-based dominance or maintain the same degree of it during mixed profession group formation. This group formation concerns the assembly of a collection of people into a unity or group (Campbell, Citation1958). In order to facilitate interprofessional identification, the professional identity should be “extended” to include interprofessional belonging, commitment and beliefs. The self-categorization theory describes under which circumstances an individual will perceive collections of people as a group and themselves as a group member (Turner, Citation1999, Citation1987). This theory makes a distinction between different levels of abstraction and inclusiveness with regard to personal and social identity. In other words, a professional can also be a member of a larger group like an interprofessional group. The salience of a social category like the interprofessional group depends on a non-conscious process of accentuation. This means that differences between mixed profession groups can be emphasized along with similarities within these social categories. Consistent accentuation can result in depersonalization which concerns a process of self-stereotyping. Individuals will perceive themselves as interchangeable examples of a social category. This way, unique individuals will be inclined to act upon and base their interpretations on the norms, goals and needs of the salient ingroup. The self is redefined in terms of group membership. The context in which a social identity or self-categorization is formed also depends on comparative and normative perceptions. Also, past experiences will influence the readiness to use a particular social category.
The self-categorization theory provides clues for social identity formation through self-categorization. Because of this, it is likely that professionals can identify with an interprofessional group. However, this theory does not provide practical suggestions for how to change specific behaviours and enhance interprofessional collaboration. It also does not take into account that long-term interprofessional socialization is likely to influence a social category of a lower abstraction level: professional identity formation. It is inherent to interprofessional collaboration that any profession should be added value to the interprofessional group. This makes a distinct professional identity also inherent to interprofessional identification and, eventually, interprofessionalism will become a characteristic of professional identity. The self-categorization theory does not describe how to practically enhance accentuation. It describes the process but not how specific (interprofessional) behaviour can be facilitated. So far, no single theory has provided practical clues of how to facilitate interprofessional identification and, ultimately, interprofessional behaviour. For this reason, an extended professional identity theory is proposed as a practical intervention theory that is a special adaptation of self-categorization theory.
Towards an extended professional identity theory
Comparative group feedback as a team process during professionals’ education is a promising strategy for influencing perceptions on interprofessional task distribution (Reinders, Krijnen, Stegenga, & van der Schans, Citation2017). In addition, intergroup comparison enhances intragroup cooperation (Böhm & Rockenbach, Citation2013), and competition between groups can divert internal competition between subgroups (Munkes & Diehl, Citation2003). Furthermore, social identity formation requires psychological distinctiveness or accentuation of differences and similarities. This distinctiveness is only possible when using a comparable reference group (Turner & Reynolds, Citation2010). Therefore, when facilitating competition through comparative group feedback between mixed profession groups, it is likely that professional subgroup members will identify with their mixed profession group. If interprofessional identification is enhanced, it is also likely that the members of the professional subgroups will exhibit a decreased profession-based dominance. On the other hand, reflective group feedback without intergroup comparison is likely to not unify the members of a mixed profession group but will plausibly reinforce the initial relationship between its professional subgroups.
Basic assumptions of the extended professional identity theory
Based on earlier research and the rationale described earlier, the proposed extended professional identity theory has 10 basic assumptions.
1. Social belonging is a common human need that predicts group commitment and group loyalty. People can feel committed to any social group under the right circumstances and have the tendency and desire to belong to a social group (Beal, Cohen, Burke, & McLendon, Citation2003).
2. A group is a social psychological construct and thus a psychological reality. The perception that a collection of individuals is a psychological unity or group, also known as entitativity (Campbell, Citation1958), will depend on three aspects: common fate, similarity and proximity. This is why new groups can be composed and accepted as a social psychological reality. Groups can also include smaller groups because people can have widening circles of group membership (Turner, Citation1987).
3.Social differentiation is essential for creating a strong professional identity. A social identity such as a professional identity is constructed by individuals through differentiation between groups as a result of intergroup comparison (Barnes, Carpenter, & Dickinson, Citation2000; Forgas & Williams, Citation2014). This differentiation enables self-definition as a group member because individuals have a need for psychological distinctiveness.
4. Interprofessionality cannot exist without distinct professional identities. When a professional identity has an interprofessional orientation, the uniqueness of an individual’s own field of expertise becomes emphasized because interprofessional collaboration concerns connecting distinct fields of expertise. Thus, the uniqueness of a professional identity in an interprofessional team is related to the added value of the interprofessional team. When professional uniqueness decreases, so will the added value to the team. Team diversity is only utilized when there is interprofessional commitment. The relationship between team diversity and team effectiveness is moderated by team identity (Mitchell, Parker, & Giles, Citation2011).
5. According to the team development model of Tuckman (Citation1999, Citation1965), internal conflict or competition in a team is a risk after a team is formed. Introducing a comparable outgroup will shift the risk of internal competition to external competition. This way, interprofessional conflict or competition within a mixed profession group can be avoided and will not decrease group cohesion (Munkes & Diehl, Citation2003).
6. Intergroup contact between members of different professions will enhance interprofessional tolerance under the right conditions (Allport, Citation1954; Hewstone & Brown, Citation1986) but not change interprofessional positions or profession-based dominance. Attributions of professional characteristics can deviate from true group characteristics (Baker et al., Citation2011). Therefore, intergroup contact can enhance interprofessional tolerance by discrediting occupational stereotypes. However, it will not enhance interprofessional commitment because there is no sense of belonging to an interprofessional team that does not psychologically exist.
7. The nature of intergroup comparison dimensions will indirectly guide behaviour through professional identity. A professional identity is a mental representation of professional behaviour and, therefore, also interprofessional behaviour. This identity subsequently guides professional and interprofessional behaviour (Owens, Robinson, & Smith-Lovin, Citation2010). When reciprocal behaviours (such as equal conversational turn-taking) between members of different professions are a comparison dimension or performance indicator, beliefs regarding interprofessional relationships will be altered by observational learning (Bandura, Citation1988) and social comparison (Festinger, Citation1954). This way, when such beliefs are developed in a work related context, they will become internalized and initiate interprofessional behaviours.
8. A professional identity with an interprofessional orientation is context dependent. A social identity is triggered by the context that is relevant to that identity (Finn, Garner, & Sawdon, Citation2010; Ginsburg, Regehr, & Lingard, Citation2003; Lingard, Garwood, Szauter, & Stern, Citation2001). Interprofessional behaviour does not always have to be necessary but is appropriate in dynamic situations and complex patient categories (Donofrio, Spohrer, & Zadeh, Citation2009).
9. Intergroup comparison simultaneously enhances ingroup cohesion and outgroup separation. It is associated with intragroup cooperation (Böhm & Rockenbach, Citation2013), and outgroup derogation is accompanied by ingroup favouritism (Hewstone, Rubin, & Willis, Citation2002).
10. The group cohesion in a mixed profession group can increase through time without developing an interprofessional team culture. According to the team development model of Tuckman (Citation1999, Citation1965), group cohesion will develop after a group has evolved beyond the storming phase during which internal group conflict is at risk. However, this model describes the development of any team and not just an interprofessional team. Team cohesion is distinct from team culture.
Based on these 10 basic assumptions, an extended professional identity is formed when comparative feedback on interprofessional performance between comparable mixed profession groups is facilitated in a professional context (). The extended professional identity theory states that interprofessional collaboration can be enhanced by facilitating intergroup comparison on interprofessional reciprocity between mixed profession groups. In order to do so, comparative feedback between mixed profession groups and regarding professional subgroup interaction should decrease dominance between professional subgroups.
Figure 1. Towards an “extended professional identity theory”.
The purpose of this study is to investigate whether comparative feedback on interprofessional interaction is more effective for decreasing the degree of profession-based dominance and general dominance in mixed profession groups compared to only reflective feedback.
Methods
We conducted a randomized double-blind pretest-posttest control group design with mixed profession groups. Each mixed profession group consisted of six students (three dental and three dental hygiene students) who performed assignments related to team development and interprofessional care.
Participants
Eligible participants were dental students of the University of Groningen and dental hygiene students of the Hanze University of Applied Sciences, Groningen, The Netherlands who were at the midpoint of their undergraduate training. None of the students had previous experience with interprofessional collaboration or clinical practice: they had only received a single-discipline education and were not yet involved in patient care.
Study design
We randomly (alphabetically) assigned 114 dental and dental hygiene students to 19 mixed profession groups, each simulating an oral care practice. Subsequently, the groups were randomly assigned to either an intervention condition or a control condition (). Each mixed profession group received eight team development assignments (e.g., mission statement, business establishment, interior design, practice website, work schedules, protocols) and four virtual patient assignments for shared care planning. The assignment results were entered into a group portfolio after each group meeting. The experiment took four hours divided over two consecutive group meetings of two hours each.
Figure 2. Study design.
Psychologists and psychology master students were trained as observers to score specific communicative behaviours between dental and dental hygiene students (ratio of conversational turn-taking, relative dominance and relative contribution of ideas) during two consecutive group meetings each lasting 15 minutes. Each mixed profession group consisted of two subgroups: a subgroup of three dental and a subgroup of three dental hygiene students. Interprofessional communication between the subgroups of dental and dental hygiene students in each mixed profession group was observed for the purpose of measurement and group-based feedback as well as experimental intervention (intergroup comparison by comparative feedback). Observed dominance between dental and dental hygiene students was recoded and reframed as “interprofessional interaction” before it was communicated as group-based feedback to each group. Both groups received feedback on the degree of relative dominance between professions within their (mixed) group after each session. Only the intervention groups received feedback concerning relative dominance in the other mixed groups. This was distributed through the group portfolio.
Ethical considerations
We informed all of the participants about the study, and they could withdraw at any given time. We guaranteed full anonymity to all participants. The Institutional Review Board of the Hanze University of Applied Sciences approved this study.
Measurement of profession-based dominance and general dominance
Profession-based dominance was defined as the relative dominance of members of one profession over members of another profession (based on Lindemann, Citation2007). This was measured with three observation items (i.e., conversational turn-taking, relative dominance and relative contributing ideas). General dominance was the degree of dominance within a mixed profession group without considering the dominance of one profession over the other.
Observation item 1. Ratio of conversational turn-taking
The ratio of conversational turn-taking was measured by the observers on a group-level between the subgroups of dental and dental hygiene students for 15 minutes at a time. Each initiated verbal response by a dental or dental hygiene student was counted during each collective group meeting (West, Citation1979). A non-participating observer (psychologist of psychology master student) began each observation by identifying participants (dental or dental hygiene students) within a mixed profession group. In order to clearly register the responses of dental and dental hygiene students during the group meeting, the profession and physical position of each student was determined beforehand. Each initiated verbal response of at least three words was counted as a turn. The ratio was calculated by dividing the average turns of dental hygiene students by the average turns of dental students. The value ‘0ʹ (= no dominance) was assigned when the ratio of conversational turn-taking was between 45% and 55%. The profession-based dominance was based on dental domination (−1 = dental dominance) when the ratio of conversational turn-taking was more than 55% and dental hygiene domination (+1 = dental dominance) when it was less than 45% of the time during a team meeting. These turn-taking intervals corresponded with the group-based feedback standard on this communicative behaviour during the simulation. This observation item had a three-point scale: −1 = dental dominance, 0 = no dominance, +1 = dental hygiene dominance.
Observation item 2. Relative dominance
Relative dominance was measured by observers on a group-level between the subgroups of dental and dental hygiene students for 15 minutes at a time. During the observer training, several indicators of dominance were discussed: interruption, questioning, topic control, formulation and amount of talk (e.g., Adelswärd et al., Citation1987; Duff, Citation1986; Kollock, Blumstein, & Schwartz, Citation1985; Linell, Citation1990; Roger & Schumacher, Citation1983; Ten Have, Citation1991). Observers evaluated this relative dominance between dental and dental hygiene students within a mixed profession group using an ordinal scale (to score the perceived image related to dominance): −1 = dental dominance, 0 = no dominance, +1 = dental hygiene dominance.
Observation item 3. Relative contribution of ideas
The relative contribution of ideas was measured by observers on a group-level between the subgroups of dental and dental hygiene students for 15 minutes at a time. The relative contribution of ideas is also considered an indication of dominance in the groups (James, Citation2006). It was defined as the verbal response of a person in bringing about a result by providing a meaningful thought, conception, or notion (Stichler, Citation1995). Verbal responses that were an expression of agreement, understanding, or listening were not considered as the contribution of an idea. Observers evaluated this relative contribution of ideas between dental and dental hygiene students within a mixed profession group using an ordinal scale (to score the perceived image related to the contribution of ideas): −1 = dental dominance, 0 = no dominance, +1 = dental hygiene dominance.
Psychometric properties
Profession-based dominance and general dominance were each applied as an index based on psychometric properties when factorability was sufficient. A non-parametric kernel smoothing IRT (Mazza, Punzo, & McGuire, Citation2014; Ramsay, Citation2000) was applied to determine whether all three observation items represent the same latent variable. For purposes of comparison Cronbach’s alpha was calculated to estimate internal consistency. The internal consistency is considered sufficient when it is higher than .70 (Nunnally, Citation1978; Nunnally & Bernstein, Citation1994).
Profession-based dominance represented the relative dominance of one profession over the other. Therefore, it was calculated as the sum of the three observation item scores. Profession-based dominance had a minimum value of −3 and a maximum value of +3 since each observation item had a minimum value of −1 and a maximum value of +1.
General dominance represented the degree of dominance within a mixed profession group independent of the profession of either party. Therefore, it was calculated as the sum of absolute values of observation items since each observation item had a minimum value of −1 and a maximum value of +1. Thus, general dominance has a minimum value of 0 (no dominance) and a maximum value of 3 (strong dominance).
Data analyses
A two-way factorial ANOVA was applied to analyse main effects (time or experimental condition) and interaction effects between time and experimental condition. This analysis was performed to separately investigate both profession-based dominance and general dominance.
To determine the effect size, the partial eta squared was used. A partial eta squared of 0.01 is considered small, 0.06 as medium and 0.14 as large (Cohen, Citation1988; Field, Citation2005). Before performing each two-way factorial ANOVA analysis, potential pretest differences of both profession-based dominance and general dominance were tested by an ANOVA. For all of the analyses, we applied a significance level of .05.
Results
Descriptive statistics
The group of students that were eligible for randomization consisted of 114 dental and dental hygiene students. The gender distribution did not differ between experimental conditions (); the majority was female (63.3%, n = 31; 95.7%, n = 44). Dental students were older than dental hygiene students in both the intervention and control conditions (mean = 22.7 years, SD = 1.8 years versus mean = 21.1 years, SD = 1.8 years; p < .001).
Table 1. Descriptive statistics of intervention and control conditions (n=96).
Psychometric properties
Since Cronbach’s alpha seems to be a gross estimate of associations between ordinal observation items (with three levels), a polychoric correlation was used (). With this rating scale with a small number of response options can be tested (Mazza et al., Citation2014; Ramsay, Citation2000). The polychoric correlations were sufficient (between .50 and .94).
Table 2. Polychoric correlations and Cronbach’s alpha’s of observation items.
All the psychometric properties of our measurement were sufficient or more than sufficient (). The three ordinal items were analysed by non-parametric kernel smoothing IRT (Mazza et al., Citation2014; Ramsay, Citation2000), revealing polychoric item trait correlations of .61, .62, .90, respectively (pretest) and .50, .72, .94 respectively (posttest). This provides evidence for strong positive association of the items with the latent trait and a unidimensional underlying structure. For purposes of comparison we also calculated Cronbach’s alpha which was .73 (pretest) and .71 (posttest), respectively, before and after the intervention.
The effect on profession-based dominance
An analysis of pretest differences on profession-based dominance revealed no significant differences between experimental conditions (F(1,17) = .000, p = .988). Therefore, a two-way factorial ANOVA analysis could be performed without having to use baseline scores as a covariate.
shows the means, standard errors and lower and upper bounds (95% confidence interval) at the T0 and T1 measurement moments of the intervention and control condition. The mixed profession groups in the intervention and control conditions display a similar profession-based dominance.
Table 3. Means and standard errors of profession-based dominance of dental and dental hygiene students in mixed profession groups during the experiment (n=19 groups).
illustrates that a trend towards a changed profession-based dominance of dental students was visible but not significant. shows that there is no interaction effect between experimental condition and time, F(1, 17) = 3.441, p = .081. The partial eta squared of this non-significant interaction effect was large since it was 0.17 (Cohen, Citation1988; Field, Citation2005).
Figure 3. Profession-based dominance of dental and dental hygiene students in mixed profession groups before and after the experiment.
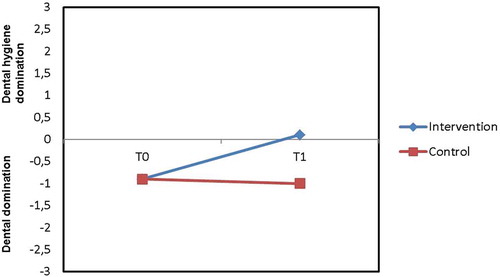
The experimental condition (intervention versus control) as a between-subjects factor did not reveal a main effect F(1,17) = 0.700, p = .415. No main effect was found on time (profession-based dominance before and after the experiment), F(1,17) = 2.202, p = .156.
The effect on general dominance
An analysis of pretest differences on general dominance revealed no significant differences between experimental conditions (F(1,17) = .015, p = .904). Therefore, a two-way factorial ANOVA analysis could be performed without having to use baseline scores as a covariate.
shows the means, standard errors and lower and upper bounds (95% confidence interval) at the T0 and T1 measurement moments of the intervention and control condition. The mixed profession groups in the intervention and control conditions seem to display a similar magnitude of interprofessional hierarchy in both conditions (M = 1.50, SE = 0.31 and M = 1.56, SE = 0.33, respectively).
Table 4. Means and standard errors of general dominance between dental and dental hygiene students in mixed profession groups during the experiment (n=19 groups).
shows a downward trend of general dominance in the intervention condition and an upward trend of general dominance in the control condition. indicates that an interaction effect was determined between experimental condition and time, F(1, 17) = 6.630, p = .020. The partial eta squared of the interaction effect was large since it was 0.28 (Cohen, Citation1988; Field, Citation2005).
Figure 4. General dominance of dental and dental hygiene students in mixed profession groups before and after the experiment.
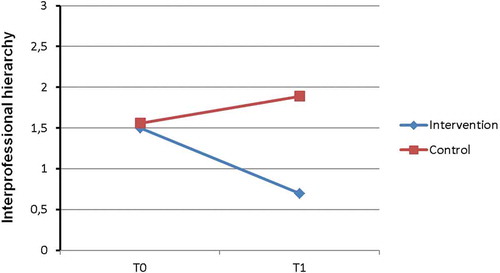
The experimental condition (intervention versus control) as a between-subjects factor did not reveal a main effect F(1,17) = 2.846, p = .110, see and . No main
effect was found for time (general dominance before and after the experiment), F(1,17) = 1.124, p = .304).
Discussion
Comparative feedback on interprofessional interaction in mixed profession groups changes the dominance between different professions. Furthermore, the conventional approach of intergroup contact with reflective but without comparative feedback does not decrease dominance. The results were inconclusive with regard to profession-based dominance. It could not be proven whether one profession was generally more dominant than the other. However, an effect of the intervention on profession-based dominance when considering the magnitude of effect sizes was found.
Intergroup comparison of interprofessional interaction reduces general dominance regardless of profession in mixed profession groups. Thus, dental and dental hygiene students tend to communicate more equally following an intervention based on group identification through comparative feedback on interprofessional interaction. Therefore, these results provide indirect evidence that the proposed extended professional theory seems to be suitable for changing dominance between members of different professions.
Unfortunately, our design does not provide hard evidence that professional group membership is the driver behind group dominance. However, several studies do report that one of the professions involved in this study are generally more dominant compared to the other profession involved (e.g., Morison et al., Citation2008; Palaganas et al., Citation2014; Ross et al., Citation2009). Apart from that, profession-based dominance is not the most desired result but, instead, the ability to decrease dominance in a mixed profession group. Dominance limits interprofessional collaboration independent of profession (D’Amour et al., Citation2005; Headrick et al., Citation1998).
It is possible that the dominance measured in this study is driven by one or a few individuals’ dominance rather than an entire professional subgroup dominating the other in a mixed profession group. However, based on external evidence, it is more likely that the dental students will display more dominance compared to dental hygiene students (Morison et al., Citation2008; Ross et al., Citation2009). Furthermore, even if one individual is more dominant than all of the other group members will affect group dynamics and, ultimately, the communication style within the mixed profession group. This will subsequently negatively affect the socialization of all of those who are involved.
A limitation of our study is the small sample size of the intervention. This small sample can result in a low statistical power. Therefore, the ability of the statistical test to detect an interaction effect between time and experimental condition becomes less likely even when this specific effect actually exists. However, despite this small sample size, we found a significant effect of our intervention. In addition, independent of sample size, we have found a large effect size.
Researchers should base their inferences on several factors such as the quality of measurements, study design and the external evidence for studied phenomenon. With regard to our study, we used a wide range of external evidence. In addition, we provided a comprehensive theoretical framework to design our intervention and to predict its outcomes. We also used a reliable measurement to analyse the effect of the experimental intervention. Furthermore, we developed a strong study design which is seldom used when investigating the effectiveness of interprofessional education (Reeves et al., Citation2016). Our design has at least five strong design features. In our study, we expected that the profession-based dominance of dental students would change when we facilitated mixed profession group identification. This expectation was based on several studies with many different human subjects. There is no reason to suspect that dental and dental hygiene students would not display similar social behaviours like any other human beings. The only difference is that we applied this external evidence to produce a specific effect between members of different professions. We wanted to change profession-based dominance and reduce dominance between members of different professions in general.
The decreased general dominance corresponds with the theory that intergroup comparison is likely to affect interprofessional identification. Intergroup comparison through comparative feedback is a group process that results in intergroup differentiation on a certain evaluative dimension (Ashfort & Kreiner, Citation1999). The Social Identity Theory (Tajfel & Turner, Citation1979) suggests that similar groups should have increased motivation to distinguish themselves from the others. Perceived ingroup similarity, inherent to social identification, increases because of outgroup distinctiveness. When applied to mixed profession groups, the perceived similarity between the members of a mixed profession group is likely to increase. If so, then mixed profession group identification might influence the formation of an interprofessional identity. Several authors suggest that its formation will enhance interprofessional collaboration (e.g., Baker et al., Citation2011; Carpenter & Dickinson, Citation2016; Hammick et al., Citation2009; Khalili et al., Citation2013). However, even though interprofessional identity formation might have been facilitated during our intervention, only the influence of comparative feedback on interprofessional interaction was measured in our study. It is an indirect indication that interprofessional identification occurred.
In our study, all of the groups were equal in composition and had a similar objective. Therefore, it is likely to assume that their motivation to differentiate between groups was increased when feedback enabled intergroup comparison. Intergroup differentiation is associated with identity formation of which the identity content depends on the content of the evaluative dimension (Ashfort & Kreiner, Citation1999; Hogg, van Knippenberg & Rast III, Citation2012; Kelly, Citation1993). In order to guide the nature of their intergroup differentiation, we controlled the nature of the comparison outcome. The intervention groups compared themselves with other mixed profession groups using interprofessional interaction (non-hierarchical interaction between members of different professions; D’Amour et al., Citation2005) as comparative feedback. Even though interprofessional identification was not measured, the results of the current experiment do correspond with this presumed social psychological mechanism. For this, another indication was found in an experiment regarding a mixed profession group formation intervention and perceived interprofessional task distribution (Reinders et al., Citation2017). In that study, the combination of group-based feedback, intergroup comparison and intergroup competition between mixed profession groups was facilitated. After that intervention, half of all predefined professional tasks became more shared (less dentist-centric) between dental and dental hygiene students. The perceptions of dental students especially became less dentist-centric. The tendency to share with members of one’s own group becomes more likely when people are committed to their group (Guzzo, Citation1995; Yukelson et al., Citation1984). Group commitment is associated with psychological group formation (Beal et al., Citation2003). However, the changed interprofessional communication within the intervention condition does not necessarily have to imply that an interprofessional identity is developed during the group development process. It might just have facilitated a temporary group identity and not have influenced the professional identity formation of the participants. However, a longitudinal application of the intervention might consolidate the group identity as an interprofessional identity and become an integrated part of the professional identity. When comparing this to behavioural change in general, routines are more sustainable when they are consistently displayed over a longer period. For instance, researchers have found proof that, when changed behaviour is consistent for at least six months, it becomes more likely that it becomes a sustainable change (Prochaska, DiClemente, & Norcross, Citation1992). This sustainable change of professional identity is referred to as “internalization” (Yu & Wright, Citation2015). Further research must clarify whether this approach is sustainable and affects professional identity formation.
An alternative explanation of the findings of this study and a former study (Reinders et al., Citation2017) is the contact hypothesis (or intergroup contact theory) of Allport (Citation1954). The premise of his theory states that interpersonal contact can reduce prejudice between groups. By facilitating communication and joint work between members of different groups, such as students in a mixed profession group, a mutual understanding of different viewpoints can be enhanced. However, the contact between students in the control condition did not reduce dominance within the mixed profession groups. Non-hierarchical interaction concerns a behaviour pattern formed from the similar behaviour of interacting individuals (Bateson, Citation1972). Social similarity is inherent to the perception of the ingroup as one entity (Campbell, Citation1958) and inherent to a shared social identity (Gaertner, Rust, Dovidio, Bachman, & Anastasio, Citation1994). Therefore, it is more likely that a shared social identity was developed in the intervention groups and that this shared identity concerns interprofessionality because of the content of the comparative feedback. Further research must substantiate that interprofessional identification can be enhanced by psychological mixed profession group formation with intergroup comparison based on interprofessional behaviour.
The dental students were older in both of the experimental conditions. Age-related status in peer collaboration may play a role in how partners interact (Glachen & Light, Citation1982). Therefore, the general dominance at the beginning of the experiment might have been caused by these age-differences. In small children, such age-differences have a significant impact because of differences in age-related mental development (Feldman & Ruble, Citation1988). These types of age-related developmental differences do not apply to adults and, to a lesser degree, adolescents. Therefore, it is unlikely that a mean age-difference of 1.6 years has a significant impact. However, the age difference could signify an extra year of professional education and training (e.g., 2nd year students and 3rd year students). Therefore, the professional subgroup dominance may be associated with greater knowledge and expertise rather than membership in a professional group. However, none of the students had experience with interprofessional collaboration or with clinical practice. Since clinical practice was the focus of the team development sessions, it is unlikely that differences in experience can account for the outcomes of this study. In addition, age differences and differences in the levels of knowledge and expertise between the professions cannot explain the behavioural differences that were found between the control and intervention conditions.
A limitation of our study is that it was conducted in an educational setting as part of the IPE programme. In such a context, it is more difficult to exert control over experimental conditions since students might have influenced each other between their mixed profession group meetings. However, the occupations involved in this study also work together after graduation and task shifting has resulted in interprofessional tensions and competition between them (e.g., Adams, Citation2004; Knevel, Gussy, Farmer, & Karimi, Citation2017; Northcott et al., Citation2013; Ross & Turner, Citation2015). Therefore, the context of this experiment does approximate the vocational context and makes it more likely that an intervention is required in order to decrease dominance in mixed profession groups. Furthermore, the strengths of this study were its group randomization and double-blind design. This way, the cause and effect relationship in this study can be interpreted with more confidence compared to other designs. First, because of the double-blind design, both the subjects and the observers did not know which group was selected for which experimental condition. Second, the size of each group was the same. Third, dental and dental hygiene students were equally represented in each mixed profession group. Fourth, students were randomly assigned to a mixed profession group. Fifth, all experimental procedures, assignments, tasks and assessments were standardized by protocols. Besides the quality of our measurements and our study design, the intervention derived from our intervention theory was based on comprehensive external evidence.
The results of this study might be reproducible in a work context. In order to do this, the interaction between professionals must be measured in at least two mixed teams. Then, these teams must be able to compare their own interaction with the interprofessional interaction in other teams. It is possible that comparative feedback on other interprofessional behaviours and performance can also produce similar results. However, this must be confirmed by additional studies.
Many other (external) influences can affect collective behaviour in the work context and are less easy to control. The influence of legal issues and liabilities (Colvin et al., Citation2013) or incentives in remuneration systems (Brocklehurst et al., Citation2016) are examples of factors that are likely to influence collaboration between dentists and dental hygienists.
Conclusions and future study
Comparative feedback to facilitate group processes and change dominance in a mixed profession group seems a viable and promising strategy. Even though the results of this study were inconclusive with regard to decreasing profession-based dominance, evidence was found that general dominance in a mixed profession group can be decreased.
Regardless of the study’s limitations and the small sample size, indirect evidence was found that interprofessional identification seems to be facilitated as assumed by the proposed extended professional identity theory. However, additional research must provide direct proof. Apart from that, the intervention based on our intervention theory did enhance interprofessional behaviour. Whether it would produce similar results in the work context is unknown and should be investigated. Future studies might examine whether this approach produces sustainable effects.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Adams, T. L. (2004). Inter-professional conflict and professionalization: Dentistry and dental hygiene in Ontario. Social Science & Medicine, 58, 2243–2252.
- Adelswärd, V., Aronsson, K., Jönsson, L., & Linell, P. (1987). The unequal distribution of interactional space: Dominance and control in courtroom interaction. Text, 7, 313–346.
- Agha, L., Frandsen, B., & Rebitzer, J. B. (2017). Causes and consequences of fragmented care delivery: Theory, evidence, and public policy (NBER working paper no. 23078). National Bureau of Economic Research.
- Allport, G. W. (1954). The nature of prejudice. Cambridge, MA: Perseus Books.
- Anderson, C., & Brown, C. E. (2010). The functions and dysfunctions of hierarchy. Research in Organizational Behavior, 30, 55–89.
- Archibald, P., & Estreet, A. (2017). Utilization of the interprofessional education, practice, and research model in HBCU social work education. Journal of Human Behavior in the Social Environment, 27, 450–462.
- Ashfort, B. E., & Kreiner, G. E. (1999). “How can you do it?”: Dirty work and the challenge of constructing a positive identity. Academy of Management Review, 24, 413–434.
- Baker, L., Egan-Lee, E., Martimianakis, M. A., & Reeves, S. (2011). Relationships of power: Implications for interprofessional education. Journal of Interprofessional Care, 25, 98–104.
- Bandura, A. (1988). Organizational application of social cognitive theory. Australian Journal of Management, 13, 275–302.
- Barbour, J. B., & Lammers, J. C. (2015). Measuring professional identity: A review of the literature and a multilevel confirmatory factor analysis of professional identity constructs. Journal of Professions and Organization, 2, 38–60.
- Barnes, D., Carpenter, J., & Dickinson, C. (2000). Interprofessional education for community mental health: Attitudes to community care and professional stereotypes. Journal of Interprofessional Care, 19, 565–583.
- Bateson, G. (1972). Steps to an ecology of mind. San Francisco: Chandler.
- Baumgartner, W., Schimmel, M., & Müller, F. (2015). Oral health and dental care of elderly adults dependent on care. Swiss Dental Journal, 125, 417–426.
- Beal, D. J., Cohen, R., Burke, M. J., & McLendon, C. L. (2003). Cohesion and performance in groups: A meta-analytic clarification of construct relation. Journal of Applied Psychology, 88, 989–1004.
- Bergami, M., & Bagozzi, R. P. (2000). Self-categorization, affective commitment and group self-esteem as distinct aspects of social identity in the organization. British Journal of Social Psychology, 39, 555–577.
- Böhm, R., & Rockenbach, B. (2013). The inter-group comparison-intra-group cooperation hypothesis: Comparisons between groups increase efficiency in public goods provision. PLoS One, 8, e56152.
- Bolin, A. (2016). Children’s agency in interprofessional collaborative meetings in child welfare work. Child & Family Social Work, 21, 502–511.
- Brocklehurst, P., Birch, S., McDonald, R., Hill, H., O’Malley, L., Macey, R., & Tickle, M. (2016). Determining the optimal model for role substitution in NHS dental services in the UK: A mixed-methods study. Health Services and Delivery Research, 4, 1–118.
- Brown, L. N. (1991). Groups for growth and change. New York: Longman Publishing.
- Bryan Jean, R., Sinkovics, R. R., & Kim, D. (2014). The impact of technological, organizational and environmental characteristics on electronic collaboration and relationship performance in international customer–supplier relationships. Information & Management, 51, 854–864.
- Campbell, D. T. (1958). Common fate, similarity, and other indices of the status of aggregates of person as social entities. Behavioural Science, 3, 14–25.
- Carpenter, J., & Dickinson, H. (2016). Interprofessional education and training. United Kingdom, Bristol: The Policy Press.
- Cheng, J. T., Tracy, J. L., Foulsham, T., Kingstone, A., & Henrich, J. (2013). Two ways to the top: Evidence that dominance and prestige are distinct yet viable avenues to social rank and influence. Journal of Personality and Social Psychology, 104, 103–125.
- Cheng, J. T., Tracy, J. L., & Henrich, J. A. (2010). Pride, personality, and the evolutionary foundations of human social status. Evolution and Human Behavior, 31, 334–347.
- Clausen, J. A. (1968). Socialization and society. Boston: Little Brown and Company.
- Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Earlbaum Associates.
- Colvin, C. J., de Heer, J., Winterton, L., Mellenkamp, M., Glenton, C., Noyes, J., … Rashidian, A. (2013). A systematic review of qualitative evidence on barriers and facilitators to the implementation of task-shifting in midwifery services. Midwifery, 29, 1211–1221.
- Corser, W. D. (1998). A conceptual model of collaborative nurse-physician interactions: The management of traditional influences and personal tendencies. Scholarly Inquiry for Nursing Practice, 12, 325–341.
- D’Amour, D., Ferrada-Videla, M., San Martin Rodriguez, L., & Beaulieu, M. D. (2005). The conceptual basis for interprofessional collaboration: Core concepts and theoretical frameworks. Journal of Interprofessional Care, 19, 116–131.
- Donofrio, N., Spohrer, J., & Zadeh, H. S. (2009). Research-driven medical education and practice: A case for T-shaped professionals. MJA Viewpoint, http://www.ceri.msu.edu/wp-content/uploads/2010/06/A-Case-for-T-Shaped-Professionals-20090907-Hossein.pdf, retrieved on March 29th 2018.
- Duff, P. A. (1986). Another look at interlanguage talk: Taking task to task. In R. R. Day (Ed.), Talking to learn: Conversation in second language acquisition (pp. 147–181). Cambridge, MA: Newbury House.
- Edmondson, A. C. (2003). Framing for learning: Lessons in successful technology implementation. California Management Review, 45, 34–54.
- Feldman, A. S., & Ruble, D. N. (1988). The effect of personal relevance on dispositional inference: A developmental analysis. Child Development, 59, 1339–1352.
- Festinger, L. (1954). A theory of social comparison processes. Human Relations, 7, 117–140.
- Field, A. (2005). Discovering statistics using SPSS (2nd ed.). London: Sage.
- Finn, G., Garner, J., & Sawdon, M. (2010). ‘You’re judged all the time!’ Students’ views on professionalism: A multicentre study. Medical Education, 44, 814–825.
- Forgas, J. P., & Williams, K. D. (2014). The social self: Cognitive, interpersonal and intergroup perspectives (Vol. 4). New York: Psychology Press.
- Gaertner, S. L., Rust, M., Dovidio, J. F., Bachman, B. A., & Anastasio, P. A. (1994). The contact hypothesis: The role of common ingroup identity on reducing intergroup bias. Small Group Research, 25, 224–249.
- Gal, U., Blegind Jensen, T., & Lyytinen, K. (2014). Identity orientation, social exchange, and information technology use in interorganizational collaborations. Organization Science, 25, 1372–1390.
- Gallagher, S. (2005). How the body shapes the mind. Oxford: Oxford University Press/Clarendon Press.
- Gallagher, S. (2008). Direct perception in the intersubjective context. Consciousness and Cognition, 17, 535–543.
- Ginsburg, S., Regehr, G., & Lingard, L. (2003). To be and not to be: The paradox of the emerging professional stance. Medical Education, 37, 350–357.
- Glachen, M., & Light, P. (1982). Peer interaction and learning: Can two wrongs make a right? In G. Butterworth & P. Light (Eds.), Social cognition: Studies of the development of understanding (pp. 238–262). Brighton: Harvester.
- Godard, J., & Delaney, J. (2000). Reflections on the “High Performance” paradigm’s implications for industrial relations as a field. Industrial and Labor Relations Review, 53, 482–502.
- Guzzo, R. A. (1995). At the intersection of team effectiveness and decision making. In R. A. Guzzo & E. Salas (Eds.), Team effectiveness and decision making in organizations (pp. 1–8). San Francisco: Jossey-Bass.
- Hammick, M., Freeth, D., Copperman, J., & Goodsman, D. (2009). Being interprofessional. Cambridge: Polity Press.
- Hayashi, T., Shinozaki, H., Makino, T., Ogawara, H., Asakawa, Y., Iwasaki, K., … Watanabe, H. (2012). Changes in attitudes toward interprofessional health care teams and education in the first- and third-year undergraduate students. Journal of Interprofessional Care, 26, 100–107.
- Headrick, L. A., Wilcock, M., & Batalden, B. (1998). Interprofessional working and continuing medical education. BMJ, 316, 771–774.
- Hertweck, M. L., Hawkins, S. R., Bednarek, M. L., Goreczny, A. J., Schreiber, J. L., & Sterrett, S. E. (2012). Attitudes toward interprofessional education: Comparing physician assistant and other health care professions students. Journal of Physician Assistant Education, 23, 8–15.
- Hewstone, M., & Brown, R. (1986). Contact and conflict in intergroup encounters. Oxford: Blackwell.
- Hewstone, M., Rubin, M., & Willis, H. (2002). Intergroup bias. Annual Review of Psychology, 53, 575–604.
- Hogg, M. A., van Knippenberg, D., & Rast, D. E., III. (2012). The social identity theory of leadership: Theoretical origins, research findings, and conceptual developments. European Review of Social Psychology, 23, 258–304.
- Holmes, L. (2001). Reconsidering graduate employability: The `graduate identity’ approach. Quality in Higher Education, 7, 111–119.
- Hood, R. (2012). A critical realist model of complexity for interprofessional working. Journal of Interprofessional Care, 26, 6–12.
- Huselid, M. A. (1995). The impact of human resource management practices on turnover, productivity, and corporate financial performance. Academy of Management Journal, 38, 635–672.
- Ichniowski, C., Shaw, K., & Prennushi, G. (1997). The effects of human resource management practices on productivity: A study of steel finishing lines. American Economic Review, 87, 293–313.
- James, M. C. (2006). The effect of grading incentive on student discourse in peer instruction. American Journal of Physics, 8, 689–691.
- Kelly, C. (1993). Group identification, intergroup perceptions and collective action. European Review of Social Psychology, 4, 59–83.
- Khalili, H., Orchard, C., Spence Laschinger, H. K., & Farah, R. (2013). Interprofessional socialization framework for developing an interprofessional identity among health professions students. Journal of Interprofessional Care, 27, 448–453.
- Knevel, R., Gussy, M. G., Farmer, J., & Karimi, L. (2017). Perception of Nepalese dental hygiene and dentistry students towards the dental hygienists profession. International Journal of Dental Hygiene, 15, 219–228.
- Kollock, P., Blumstein, P., & Schwartz, P. (1985). Sex and power in interaction: Conversational privileges and duties. American Sociological Review, 50, 34–46.
- Koné Pefoyo, A. J., Bronskill, S. E., Gruneir, A., Calzavara, A., Thavorn, K., Petrosyan, Y., … Wodchis, W. P. (2015). The increasing burden and complexity of multimorbidity. BMC Public Health, 15, 415.
- Liao, J., O’Brien, A. T., Jimmieson, N. L., & Restubog, S. L. D. (2015). Predicting transactive memory system in multidisciplinary teams: The interplay between team and professional identities. Journal of Business Research, 68, 965–977.
- Lindemann, K. (2007). The impact of objective characteristics on subjective social position. Trames, 11, 54–68.
- Linell, P. (1990). The power of dialogue dynamics. In I. Marková & K. Foppa (Eds.), The dynamics of dialogue (pp. 147–177). Hemel Hempstead: Harvester Wheatsheaf.
- Lingard, L., Garwood, K., Szauter, K., & Stern, D. (2001). The rhetoric of rationalization: How students grapple with professional dilemmas. Academic Medicine, 76, S45–S47.
- Magee, J. C., & Galinsky, A. D. (2008). Social hierarchy: The self-reinforcing nature of power and status. Academy of Management Annals, 2, 351–398.
- Matziou, V., Vlahioti, E., Perdikaris, P., Matziou, T., Megapanou, E., & Petsios, K. (2014). Physician and nursing perceptions concerning interprofessional communication and collaboration. Journal of Interprofessional Care, 28, 526–533.
- Mazza, A., Punzo, A., & McGuire, B. (2014). KernSmoothIRT: An R package for kernel smoothing in item response theory. Journal of Statistical Software, 58, 1–34.
- McNeil, K.A, Rebecca, J, Mitchell, R.J, & Parker, V. (2013). Interprofessional practice and professional identity threat. Health Sociology Review, 22(3), 291-307. doi:10.5172/hesr.2013.22.3.291
- Meyer, J. P., & Herscovitch, L. (2001). Commitment in the workplace: Towards a general model. Human Resources Management Review, 1, 299–326.
- Mitchell, R., Parker, V., & Giles, M. (2011). When do interprofessional teams succeed? Investigating the moderating roles of team and professional identity in interprofessional effectiveness. Human Relations, 64, 1321–1343.
- Morison, S., Marley, J., Stevenson, M., & Milner, S. (2008). Preparing for the dental team: Investigating the views of dental and dental care professional students. European Journal of Dental Education, 12, 23–28.
- Munkes, J., & Diehl, M. (2003). Matching or competition? Performance comparison processes in an idea generation task. Gpir, 6, 305–320.
- Northcott, A., Brocklehurst, P., Jerkovic-Cosic, K., Reinders, J. J., McDermott, I., & Tickle, M. (2013). Direct access: Lessons learnt from the Netherlands. British Dental Journal, 215, 607–610.
- Nunnally, J. (1978). Psychometric theory. New York: McGraw-Hill.
- Nunnally, J., & Bernstein, J. C. (1994). Psychometric theory. New York: McGraw-Hill.
- Owens, T. J., Robinson, D. T., & Smith-Lovin, L. (2010). Three faces of identity. Annual Review of Sociology, 36, 477–499.
- Palaganas, J. C., Epps, C., & Raemer, D. B. (2014). A history of simulation-enhanced interprofessional education. Journal of Interprofessional Care, 28, 110–115.
- Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictive behaviors. American Psychologist, 47, 1102–1114.
- Ramsay, J. O. (2000). TestGraf: A program for the graphical analysis of multiple choice test and questionnaire data. Retrieved January 15, 2018, from http://www.psych.mcgill.ca/faculty/ramsay/ramsay.html
- Reeves, S., Fletcher, S., Barr, H., Birch, I., Boet, S., Davies, N., … Kitto, S. (2016). A BEME systematic review of the effects of interprofessional education: BEME guide no. 39. Medical Teacher, 38, 656–668.
- Reinders, J. J., Krijnen, W. P., Stegenga, B., & van der Schans, C. P. (2017). Perceived dentists and dental hygienist task distribution after a dental and dental hygiene students’ team intervention. Journal of Dental Education, 81, 413–419.
- Robben, S., Perry, M., van Nieuwenhuijzen, L., van Achterberg, T., Rikkert, M. O., Schers, H., … Melis, R. (2012). Impact of interprofessional education on collaboration attitudes, skills, and behavior among primary care professionals. Journal of Continuing Education in the Health Professions, 32, 196–204.
- Roger, D. B., & Schumacher, A. (1983). Effects of individual differences on dyadic conversational strategies. Journal of Personality and Social Psychology, 45, 700–705.
- Ross, M., & Turner, S. (2015). Direct access in the UK: What do dentists really think? British Dental Journal, 218, 641–647.
- Ross, M. K., Turner, S., & Ibbetson, R. J. (2009). The impact of teamworking on the knowledge and attitudes of final year dental students. British Dental Journal, 206, 163–167.
- Sollami, A., Caricati, L. & Mancini, T. (2017). Attitudes towards Interprofessional Education among Medical and Nursing Students: the Role of Professional Identification and Intergroup Contact. Current Psychology, 1-8, Available from: http://link.springer.com/10.1007/s12144-017-9575-y.
- Stichler, J. F. (1995). Professional interdependence: The art of collaboration. Advanced Practice Nursing Quarterly, 1, 53–61.
- Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Monterey, CA: Brooks-Cole.
- Teece, D., & Abdulrahman, A. (2011). Knowledge assets, capabilities and the theory of the firm. In M. Easterby-Smith & M. A. Lyles (Eds.), Handbook of organizational learning and knowledge management (pp. 505–534). New York: Wiley.
- Ten Have, P. (1991). Talk and institution: A reconsideration of the ‘asymmetry’ of doctor-patient interaction. In D. Boden & D. H. Zimmerman (Eds.), Talk and social structure: Studies in ethnomethodology and conversation analysis (pp. 138–163). Cambridge: Polity Press.
- Thistlethwaite, J. (2012). Interprofessional education: A review of context, learning and the research agenda. Medical Education, 46, 58–70.
- Tsoukas, H., & Vladimirou, E. (2001). What is organizational knowledge? Journal of Management Studies, 38, 973–993.
- Tuckman, B. W. (1965). Developmental sequence in small groups. Psychological Bulletin, 63, 384–399.
- Tuckman, B. W. (1999). A tripartite model of motivation for achievement: Attitude/drive/strategy. Paper presented at the annual meeting of the American Psychological Association, Boston.
- Turner, J. C. (1987). A self-categorization theory. In J. C. Turner, M. A. Hogg, P. J. Oakes, S. D. Reicher, & M. S. Wetherell (Eds.), Rediscovering the social group: A self-categorization theory (pp. 42–67). Oxford, UK: Blackwell.
- Turner, J. C. (1999). Some current issues in research on social identity and self-categorization theories. In N. Ellemers, R. Spears, & B. Doosje (Eds.), Social identity (pp. 6–34). Oxford, England: Blackwell.
- Turner, J. C., & Reynolds, K. J. (2010). The story of social identity. In T. Postmes & N. Branscombe (Eds.), rediscovering social identity: Core sources (pp. 13–32). New York: Psychology Press.
- Vettore, M. V., Meira, G. F., Rebelo, M. A. B., Rebelo Vieira, J. M., & Machuca, C. (2016). Multimorbidity patterns of oral clinical conditions, social position, and oral health-related quality of life in a population-based survey of 12-yr-old children. European Journal of Oral Science, 124, 580–590.
- Wenga, Q., & Carlsson, F. (2015). Cooperation in teams: The role of identity, punishment, and endowment distribution. Journal of Public Economics, 126, 25–38.
- West, C. (1979). Against our will: Male interruptions of females in cross-sex conversation. Annals of the New York Academy of Sciences, 327, 81–97.
- Whittington, C. (2003). A model of collaboration. In J. Weinstein, C. Whittington, & T. Leiba T (Eds.), Collaboration in social work practice (pp. 39–62). Londen: Jessica Kingsley.
- WHO. (2012). The health-care challenges posed by population ageing. Bulletin of the World Health Organization, 90, 77–156.
- Xyrichis, A., Reeves, S., & Zwarenstein, M. (2017). Examining the nature of interprofessional practice: An initial framework validation and creation of the InterProfessional Activity Classification Tool (InterPACT). Journal of Interprofessional Care, 13, 1–10.
- Yu, E, & Wright, S.M. (2015). with the end in mind”: imagining personal retirement speeches to promote professionalism. Academic Medicine, 90, 790–793. doi:10.1097/ACM.0000000000000690
- Yukelson, D., Weinberg, R., & Jackson, A. (1984). A multi-dimensional group cohesion instrument for intercollegiate basket-ball teams. Journal of Sport Psychology, 6, 103–117.