
Abstract
Purpose
Up to 30% of women of reproductive age experience HMB, which has a substantial impact on their quality of life. A clinical care pathway for women with HMB is an unmet need, but its development requires better understanding of the factors that characterise current diagnosis and management of the condition.
Materials and methods
This observational, survey-based study assessed the burden, personal experiences, and path through clinical management of women with HMB in Canada, the USA, Brazil, France and Russia using a detailed, semi-structured online questionnaire. After excluding those reporting relevant organic pathology, responses to the questionnaire from 200 women per country were analysed.
Results
Around 75% of women with HMB had actively sought information about heavy periods, mostly through internet research. The mean time from first symptoms until seeking help was 2.9 (Standard deviation, 3.1) years. However, 40% of women had not seen a health care professional about the condition. Furthermore, 54% had never been diagnosed or treated. Only 20% had been diagnosed and received appropriate treatment. Treatment was successful in 69% of those patients currently receiving treatment. Oral contraceptives were the treatment most commonly prescribed for HMB, although the highly effective levonorgestrel-intrauterine system was used by only a small proportion of women.
Conclusions
This study provides insight into the typical journey of a woman with HMB which may help patients and health care professionals improve the path to diagnosis and treatment, although further research with long-term outcomes is needed.
女性月经过多治疗的艰难历程:一项多国调查 摘要
目的:多达30%的育龄女性经历过HMB, 这对她们的生活质量有很大影响。女性HMB的临床路径尚未满足需求, 它的发展需要更好地理解当前疾病诊断和管理的特征因素。材料和方法:这项观察性、基于调查的研究使用了详细的半结构化在线问卷, 评估了加拿大、美国、巴西、法国和俄罗斯的HMB女性负担、个人经历和临床管理路径。在排除了那些报告相关器质性病变的受试者之后, 对每个国家200名女性的答卷进行分析。结果:大约75%患有HMB的女性积极寻求有关月经的信息, 大部分是通过互联网查找。从首次出现症状到寻求帮助的平均时间是2.9年(标准差, 3.1)。然而, 40%的女性没有去看过健康保健专家。此外, 54%受试者从未被诊断或治疗过。只有20%受试者被诊断并接受了适当的治疗。在目前接受治疗的患者中, 69%的患者治疗成功。口服避孕药是HMB最常用的治疗方法, 然而只有一小部分女性使用高效的左炔诺孕酮宫内避孕系统。结论:这项研究提供了对HMB女性典型病史的观察, 这可能有助于患者和医疗保健专业人员改善诊断和治疗的途径。但仍然需要进一步的长期结果研究。
Introduction
Heavy menstrual bleeding (HMB) is defined as excessive menstrual blood loss that affects a woman’s physical, emotional, social, and material quality of life [Citation1]. The prevalence of HMB among women of reproductive age ranges from 10% to 30% and is influenced by the approach to assessment and the clinical setting, as well as cultural, social, and age-driven perceptions of what constitutes ‘normal’ menstruation [Citation2,Citation3]. The condition has a huge impact on the quality of life of those affected and accounts for 20% of all referrals to gynaecology outpatient departments [Citation4]. Moreover, it is the most common cause of iron-deficiency anaemia in healthy fertile women [Citation5].
There are many challenges to gauging what women perceive as HMB [Citation2]. There is a poor correlation between women’s assessment of blood loss during menstruation and their actual blood loss [Citation6]. There is also a low level of awareness of and understanding about HMB, and a tendency to adapt to the condition, which can prevent women seeking medical help [Citation5]. When women do access services, clinicians lack detailed information about the problem, as well as acceptance of and understanding about it [Citation3,Citation7].
Among healthcare professionals (HCPs), the diagnosis of HMB is hampered by a number of clinical factors. It is generally impractical to objectively measure menstrual blood loss (MBL) in routine clinical practice, so diagnosis is based on information provided by the patient [Citation3]. This difficulty has been further compounded by confusing and inconsistent nomenclature and the lack of a standardised approach to investigation [Citation2]. There is also a wide variation in the availability of services for the diagnosis and management of HMB [Citation5,Citation8,Citation9].
Choosing the right treatment for HMB is guided by a number of clinical and patient factors, including effectiveness, safety, tolerability, cost, and the presence of underlying medical conditions or comorbidities [Citation3,Citation10,Citation11]. Treatment choice is also influenced by a woman’s desire for pregnancy and the acceptability of the method proposed [Citation3,Citation11]. When counselling the patient on treatment choice, the suitability, acceptability, availability, and affordability of each option need to be considered.
The effectiveness of clinical care pathways to improve clinical outcomes is well established [Citation12]. Defining a clinical care pathway may enhance the quality of care by increasing patient satisfaction, and can optimise the use of resources (services, possible medications, surgical options, etc.). A patient journey can be used to gain insight into the interactions and barriers in the process for the patient, and allows a better understanding of the entire process in order to improve it. Despite the significant burden of HMB, a pathway for the clinical management of women with this condition has not yet been developed. The aim of this study is therefore to evaluate the journey of women suffering from HMB from the onset of symptoms to any eventual treatment.
Materials and methods
This observational, survey-based study assessed the burden, personal experiences, and path through clinical management (i.e., the journey) of women suffering from HMB. The target group was women with HMB who were aged 18–49 years and based in Canada, the USA, Brazil, France, or Russia.
For the survey, a semi-structured questionnaire was developed that used quality exercises and open-ended questions to address the life experiences and disease management trajectories of women with HMB. The questionnaire was translated by native speakers and tested for comprehension prior to use (see the Supplementary Material for the survey questionnaire in English).
Study design and participants
Existing nursing and medical market research panels were used to identify eligible members who had expressed an interest in participating in research projects. Individuals were selected by random sampling. Each woman was sent an e-mail inviting her to take part in a survey that would on average take 20 min to complete, but did not specify the survey topic. No participant received direct payment for answering the questionnaire, but respondents did receive credits (e.g., account points) from their respective market research panel participation scheme.
The distribution, administration, and data analysis of the survey were undertaken in October 2019 by the independent research organisation Ipsos GmbH (Germany); the study was funded by Bayer AG (Germany).
In an initial screening for HMB, those participating were asked to consider the following seven statements suggested by the Heavy Menstrual Bleeding: Evidence-based Learning for best Practice (HELP) Group, a panel of independent physicians with interest and clinical experience in the management of HMB.
I experience periods that last more than 7 days a month.
I need to change my protection during the night.
I worry about having accidents related to bleeding.
On the heavier days of my period, I have to change my protection more often than every 2 h.
I pass large blood clots during my period.
I feel faint or breathless during my period.
I avoid social activities or plan my clothing around my period.
Women who reported experiencing at least three of these seven descriptors ‒ considered indicative of HMB based on the expert opinion of the HELP Group ‒ were eligible for the study. The International Federation of Gynaecology and Obstetrics (FIGO) working group on menstrual disorders developed a classification system for abnormal uterine bleeding termed PALM–COEIN (polyp; adenomyosis; leiomyoma; malignancy and hyperplasia; coagulopathy; ovulatory dysfunction; endometrial; iatrogenic; and not yet classified) [Citation5]. This study focussed on the COEIN group of aetiologies for HMB; women were excluded if they reported having relevant organic pathology (those with polyps, adenomyosis, endometriosis, uterine fibroids, or endometrial hyperplasia/malignancy were excluded). Women were also excluded if they responded that they did not need help for their heavy periods. Responses to the completed full survey from 1000 of those identified as having HMB were then analysed and are reported here. This sample of 1000 women consisted of the first participants meeting the study criteria to fill the country quotas for age at onset of HMB, totalling 200 per country.
Statistical analysis
Questionnaire responses were analysed overall, by country, and by subgroup according to when in their life HMB began. Respondents were assigned to one of four life-stage-related subgroups (young age; switch or end of contraception; postpartum; or perimenopausal) according to their answer to the question, ‘Please think back to when your heavy periods started. Which of the following statements best describes that time?’:
My periods have always been heavy, already from a young age (i.e. since menarche).
My periods became heavier since I changed my birth control, or
My periods became heavier when I stopped my birth control.
My periods became heavier after giving birth.
My periods became heavier in the last 10 years or when I entered perimenopause.
Analysis of the data was undertaken using IBM SPSS Statistics software, version 20 (SPSS, Chicago, IL, USA). Between-group comparisons used the chi-squared test, and a p value of <0.05 was considered significant.
Results
Demographic information
Of the 15,107 completed questionnaires, 6210 women (41.1%) reported menstrual bleeding characteristics that were indicative of HMB as identified by responses to the HELP Group seven-item screening questionnaire. Of these, 2711 (43.6%) reported a diagnosis of a relevant organic pathology, such as uterine fibroids, adenomyosis, endometriosis, or endometrial hyperplasia/malignancy; these were more common in older women. Approximately one-third (n = 2011) of the women affected by HMB (according to HELP Group questionnaire responses) reported a diagnosis of HMB or menorrhagia.
In the sample of 1000 respondents with signs and/or symptoms consistent with HMB (not due to self-reported disease) who were included in the study analysis, the majority of women (95.3%) fell into the predetermined groups: 273 (27.3%) had had HMB from a young age; 219 (21.9%) experienced the onset of HMB after switching or ending contraception; 238 (23.8%) had HMB that started postpartum; and for 223 (22.3%), the onset of HMB was perimenopausal. The 47 women (4.7%) who could not be allocated to one of the four predefined categories for onset of HMB were included in the analysis as a single heterogeneous ‘other’ group.
Across the complete sample, the mean (standard deviation [SD]) age of women was 34.3 (9.1) years; menarche occurred at a mean (SD) age of 12.7 (1.6) years; and the onset of HMB symptoms was at a mean of 26.5 (10.1) years (Supplementary Table 1). The majority of sample respondents (65%) were parous; and 42% needed contraception.
The characteristics of respondents across the five countries involved were generally similar, but some differences were noted. Compared with the overall sample, women in the USA were older and those in Brazil were younger; menarche occurred later in life for women in Russia; and the average age at onset of HMB symptoms was younger for women in Brazil and older for those in the USA. Average parity was lower for women in Canada and Russia, and higher in the USA. The need for contraception was more frequent in Brazil and less common in Canada and the USA.
Diagnosis and treatment
Respondents identified as being affected by HMB by the initial screening tool included a mix of treated, untreated, diagnosed, and undiagnosed women: 54% had never been diagnosed or treated; 13% had been diagnosed but had never been treated; 14% had received treatment without being diagnosed with HMB (based on the patients’ knowledge); and only 20% had been diagnosed and had received treatment.
Across the predetermined life-stage categories, between 32% and 37% of respondents had been diagnosed with HMB (). When analysed by country, a diagnosis of HMB was significantly more frequent in Brazil (40%), France (39%), the USA (32%), and Russia (32%) than in Canada (23%; p < 0.05) (). Overall, one-third of women had been treated for HMB, and treatment was more common for women whose onset of HMB had been when young (38%) than for perimenopausal women (29%; p < 0.05) (). There were also differences in the frequency of treatment across the countries involved, with the proportion of women receiving treatment being significantly higher in Brazil than in Canada, the USA, France, Russia, or overall ().
Table 1. Diagnosis and treatment of HMB in 1000 women with subjective complaints according to life stage.
Table 2. Diagnosis and treatment of HMB in 1000 women with subjective complaints according to survey country.
Path to action
HMB affected women both socially and medically (): 80% were worried about bleeding-related accidents; 70% avoided social activities because of their heavy periods; 40% had experienced embarrassing situations related to HMB; 69% reported blood clots; 68% reported needing to change sanitary protection more frequently than every 2 h; and 64% suffered from tiredness.
Figure 1. Frequency of difficulties caused by heavy periods for women with heavy menstrual bleeding. Data are frequency of responses to the HELP Group seven-item screening questionnaire in the survey sample of women experiencing at least three of these seven signs or symptoms (n = 1000).

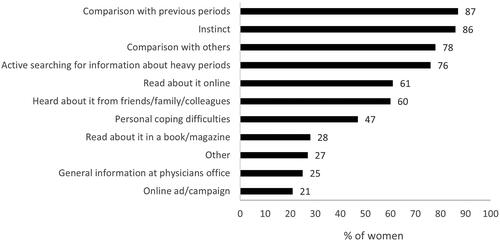
Instinct (86%) and comparison with previous periods (87%) were the main reasons that led many women to question their heavy periods (), particularly among perimenopausal women. Three-quarters of women had actively sought information about HMB (76%), 60% had discussed their heavy periods with family and friends, and 61% had searched the internet for information to try to understand their condition better.
Figure 2. Triggers and information sources that prompted women with heavy menstrual bleeding to understand their condition better. Data are frequency of responses in the complete survey sample of women experiencing at least three signs or symptoms of heavy menstrual bleeding (n = 1000). Respondents were asked to agree with statements describing triggers and/or information sources and were not restricted in the number of statements they could agree with.
Many women with HMB coped with their symptoms without medical support despite needing help, with 40% not having consulted an HCP about their heavy periods. Nearly half of respondents (48%) thought that their periods were ‘just one of those things’, and more than one-third (36%) felt that it was something they should manage themselves. On the other hand, 60% had sought medical help and advice, and 47% had visited their gynaecologist.
Women endured the burden of their heavy bleeding symptoms for a long time before taking action: the mean (SD) time between onset of symptoms and seeking help was 2.9 (3.1) years. Needing to understand whether their symptoms were normal (66%) or why they were occurring (58%) were the most frequent reasons for women to seek help for their condition; other reasons included embarrassment (40%) and an unacceptably high impact on their social life (32%).
Path to diagnosis
Heavy bleeding was the main reason a woman visited an HCP, but the need for contraception was also important, particularly if the symptoms of HMB started at switch or end of contraception.
There was a strong unmet need for information about heavy periods: 53% of the women would have appreciated more guidance on managing their periods, and others struggled with not knowing whether their periods were normal (40%) and what the cause of the HMB was (41%). In consultations with HCPs, the topics most asked about by women were menstrual pain, length of periods, and frequency of having to change sanitary protection. HCPs typically asked about family history, contraception, and family planning.
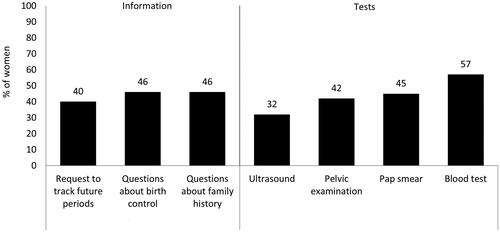
Even if heavy bleeding was discussed with an HCP, not all women were tested or received a formal diagnosis of HMB; the condition was undiagnosed in a mean of 67% of women reporting HMB symptoms (ranging from 60% undiagnosed in Brazil to 78% undiagnosed in Canada). Blood tests and taking a family history or asking about contraception were the most common steps taken by a physician (). Patients were asked to track their future periods by 40% of HCPs, and 32% recommended further investigation by ultrasound scan. Women were, on average, 29 years old (SD 9.9; range 11–47 years) when diagnosed with HMB; this age varied depending on the time of life at onset of HMB ( and ).
Figure 3. Action taken by healthcare providers in response to patients consulting for heavy periods.
A total of 19% of women felt that they were not taken seriously by their HCPs, and 20% were told that their periods were normal. Findings varied between countries however, with 25% of women from Russia reporting that HCPs did not take their complaints seriously, compared to 12% of women from France. Women from France were also more likely to be satisfied with the openness of their discussion with their HCP, with 4% wishing for a more open discussion in comparison to 16–18% of women from the other surveyed countries.
Receiving a diagnosis was generally reassuring, but could cause worry if it was not explained adequately by the HCP; some women still felt that they were coping alone despite visiting their HCP. The proportion of women who were worried by their symptoms was higher among those with a diagnosis of HMB than among those who remained undiagnosed (26% versus 11%). Women with HMB who had visited their HCP but not been formally diagnosed often managed well because serious problems had been excluded and they had found ways of coping with their heavy periods.
Path to treatment
Although 29% of respondents were not aware of any treatments for HMB, 60% knew that oral contraceptives (OCs) were a treatment for it; only 20% were aware of hormonal intrauterine systems (IUSs) as a treatment for HMB.
Some women had tried self-medication (such as non-prescription analgesics [51%]), increased fluid intake (38%), iron supplementation (35%), made changes to their diet or nutrition (34%), or used herbal teas or natural medicines (32%) to manage their HMB. Family and friends were the main influencers in self-medication.
On average, women attended two consultations about their heavy periods, and many had switched physician; the mean (SD) number of different HCPs contacted was 1.5 (1.6) before treatment was initiated. Only 34% of women had received any treatment for their HMB. Overall, 19% of women would have preferred their HCP to provide them with more treatment options; this ranged from 14% in France to 23% in Russia and Brazil.
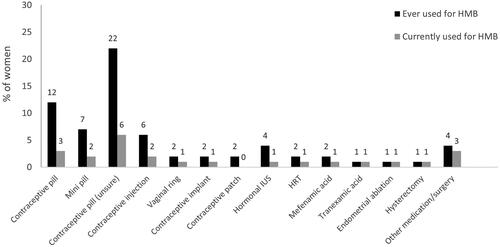
At the time of the survey, 16% of women were using hormonal contraceptives as treatment for HMB. OCs were the treatment most commonly offered: 41% of women had used OCs at some point and 11% were using an OC at the time of the survey (with 3% of women using a combined OC, 2% taking a progestin-only pill and 6% unsure of their OC type). On average, women tried approximately three OCs before finding the best option for them. With regard to the use of other methods of hormonal contraception as a treatment for HMB, 2% had received a contraceptive injection, 1% were using a levonorgestrel-IUS (LNG-IUS), 1% had received a contraceptive implant and 1% were using a vaginal ring. Surgical procedures, such as endometrial ablation and hysterectomy had been used in 1% of cases (). For those who were receiving any treatment for HMB at the time of the survey, treatment was successful in 69% of patients.
Figure 4. Treatment options ever or currently used by women with heavy menstrual bleeding (HMB). IUS: intrauterine system; HRT: hormone replacement treatment; unsure: unsure of type of contraceptive pill.
The journey of women with HMB: an overview
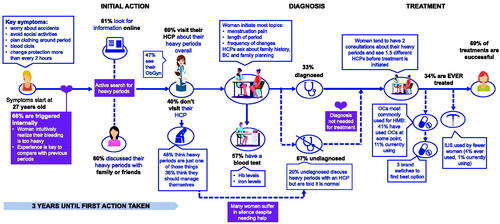
The findings of this survey are summarised and the journey of women with HMB is illustrated in . For many women, the journey from onset of symptoms through diagnosis to treatment of HMB is long and characterised by barriers, delays, misdiagnoses, and missed opportunities for effective treatment with the majority of women remaining undiagnosed and untreated.
Figure 5. An overview of the journey of women with heavy menstrual bleeding from onset to treatment. BC: birth control; Hb: haemoglobin; HCP: healthcare professional; HMB: heavy menstrual bleeding; IUS: intrauterine system; ObGyn: obstetrics and gynaecology professional; OC: oral contraceptives.
Discussion
Findings and interpretation
The most significant result of this survey is the insight it offers into the patient journey from diagnosis to treatment. In the present study, the majority of women intuitively realised that their bleeding was very intense compared with previous periods. The initial step taken by these patients was actively searching for a cause of their heavy periods. Some patients discussed their heavy periods with family and friends, but, in this digital age, people frequently turn to digital resources to find out more about health concerns, as noted elsewhere [Citation13,Citation14], and in this study many respondents did initially look for information on the internet. A wide variety of information sources are available there, some of which may be low quality or unreliable – contributing to the spread of misinformation and a delay in patients seeking help from health services, as well as illustrating the importance of reliable digital resources for patient education.
The lack of information regarding periods and HMB may be a barrier for many women needing access to appropriate treatments for this condition. Many women do not recognise HMB as a problem or realise that a variety of treatment options is available. This study confirms the low levels of awareness, knowledge, and understanding of HMB among women affected by the condition.
Patients need to be encouraged to take action sooner by increasing awareness that treatment is available for HMB. In this survey, although most women did seek medical help, it took an average of nearly 3 years for them to do so. The most common reasons for waiting to consult an HCP were thinking that the blood loss was normal or that they could manage the symptoms themselves.
When women did visit an HCP about their condition, they faced a lack of information, acceptance, or understanding of the issue, as well as diagnostic delays. Women in the present survey were likely to have two consultations about their period symptoms and to have consulted more than one physician before treatment was initiated. The presence of diagnostic delays was apparent in all countries included in the survey and affected patients in multiple ways, including ongoing and progressive symptoms, worsening health and quality of life, and a deterioration in the patient–physician relationship. Factors such as ‘normalization’ of symptoms and misdiagnosis by the HCP are likely to contribute to diagnostic delays and patient frustration.
HMB was undiagnosed in a large proportion of the women in the present study. More than half the undiagnosed patients had discussed their heavy periods with an HCP, but had often been told that they were normal. This indicates that many physicians may not be aware of how to identify HMB, and indeed there are few resources available to HCPs that provide credible, up-to-date information to facilitate effective identification, counselling, and treatment of HMB. This study demonstrates the need for diagnostic criteria that accurately reflect patients’ subjective experiences with HMB, because the prevalence and impact of HMB are high and diagnosis is often delayed. Identification of HMB based on impact on quality of life should be prioritised over identification based on quantification of menstrual blood loss because the latter is hard for patients to relate to and may result in many women who would benefit from treatment remaining undiagnosed. In addition, a lot of women did not discuss their heavy periods because they felt they were not a serious condition. Many of the patients found it difficult to communicate with their physician, and most felt that doctors needed to focus more on symptoms. This highlights the importance of providing education and information for patients so that they may be empowered to openly discuss their condition with their HCP and consider the most suitable treatment option.
In the present study, OCs were most commonly used for HMB treatment, with IUSs being used less frequently. However, the proportion of women receiving any type of hormonal treatment was low, despite nearly half the respondents to the survey requiring effective contraception; a similarly low proportion had received surgical treatment. This indicates that both medical and surgical treatments of HMB are underused, and suggests the need to educate HCPs about the diagnosis, aetiology, impact, and treatment of HMB.
Differences and similarities in relation to other studies
The findings from this survey show that many women do not know that HMB is a treatable condition. Prior studies have also demonstrated this. Indeed, a global study of more than 6000 women found that, of those diagnosed with HMB, 35% knew nothing of the condition, 50% had very little or no knowledge of it, and 39% were unaware that treatment was available [Citation2]. In addition, a previous study indicated that fewer than half the women who have HMB seek treatment, and showed that care is often suboptimal [Citation15]. These findings and the results of our survey demonstrate that women and HCPs must be educated about HMB and the available treatment options.
The present survey demonstrated that most women remain untreated despite the range of medical and surgical treatment options available. Prior studies have shown that oral tranexamic acid 3.9 g/day is able to achieve a 40% reduction in MBL [Citation16]. While OCs in general can achieve reduction of 35–68% [Citation17,Citation18], a quadriphasic combined OC, containing oestradiol valerate and dienogest, can decrease blood loss over seven cycles by a median of 88% and is the only oral contraceptive approved for the treatment of HMB [Citation19]. The 52 mg LNG-IUS is the most effective medical treatment for HMB, achieving a greater reduction in MBL, improved quality of life, and better long-term patient acceptance than OCs [Citation1,Citation4]. The 52 mg LNG-IUS was demonstrated to reduce MBL by around 95% over six cycles [Citation20,Citation21]. For this reason, several studies and guidelines suggest LNG-IUS as the first-line medical therapy for non-structural HMB [Citation22]. The high level of women who had not received treatment in the present survey, and the use of oral contraceptives as the main method among women who were receiving treatment highlights that more must be done to ensure both HCPs and women are aware of the most effective treatment options.
Relevance of the findings: implications for clinicians and policy-makers/health care providers
The present study highlights two things: first, that HMB is generally undertreated despite the available treatment options; and second, the need for educational and counselling materials to support HCPs and patients, facilitate an effective dialogue between HCPs and patients, and help to reduce delay in the diagnosis and treatment of HMB. Appropriate counselling and education can enable patients and clinicians to share in informed decision-making. In a clinical setting, this involves many factors, including prior experience, existing knowledge, trust and confidence in the clinician, personality traits, exposure and access to information, satisfaction with the consultation process, and the influence of family and others [Citation23]. Patients’ involvement in their healthcare has increased in recent years [Citation24,Citation25], and the inclusion of patients’ preferences in the management of HMB is crucial [Citation26].
This study concentrated on the COIEN group of aetiologies for HMB from the PALM-COEIN classification of abnormal uterine bleeding causes because these aetiologies are more prevalent in younger women and are able to be treated medically [Citation5,Citation10]. Thus it is important to raise awareness among HCPs on this issue and the fact that it can be identified and treated relatively easily.
Strengths and weaknesses
To our knowledge, this is the first study to evaluate the experiences of women with HMB from onset of symptoms through to treatment, thus capturing a picture of the whole journey of women with HMB. However, this study also has some limitations. MBL of >80 mL has traditionally been used as the benchmark for HMB [Citation27], but physical assessment of MBL is difficult to achieve outside clinical research settings [Citation22,Citation27]. As a result, the traditional approach of defining HMB on volume of MBL has largely been superseded by the more quality-of-life driven definition developed by the National Institute for Health and Care Excellence [Citation3]. This aspect of HMB has also been captured by items included in the HELP Group questionnaire, which are based on clinical experience, and support its use as an initial screening tool.
Participants in this online survey were identified from market research panels. Although care was taken to ensure that study recruitment was representative, this methodology might have introduced selection bias as a result of including women who were more willing to discuss their HMB and related symptoms and excluding women who did not want to participate in industry-sponsored research or who did not have access to the internet.
The proportion of women using OCs or LNG-IUS was lower than would be expected and probably reflects the fact that women receiving these therapies were being treated effectively and so chose not to report or discuss HMB.
In addition, the questionnaire provided to women asked whether they experienced the onset of HMB after switching birth control, but did not ask them to specify which contraceptive method they had previously been using or which method they switched to. Some methods (for example, a shift from condom use to tubal ligation) do not influence the incidence of HMB, whereas others such as a switch from oral contraception to a copper intrauterine device. Thus, the questionnaire could have been more specific by exploring whether a switch between reversible methods of contraception, excluding barrier methods, was associated with HMB.
Another limitation of this survey is that respondents may not have recalled their experiences accurately, and feelings may be subject to change over time, which could affect the results. Furthermore, respondents self-reported that they had been diagnosed as having HMB with no relevant organic disease present, and the survey might therefore include cases where a diagnosis of organic disease had been misunderstood by a patient; furthermore, diagnoses may vary according to the different standards of care in the countries involved.
Conclusions, unanswered questions and future research
In conclusion, the journey of a woman with HMB is typified by a large burden of suffering, a delay in diagnosis, and a gap in access to therapy. The insight into this journey provided by this study may serve as a basis on which to enhance the quality of care, maximise clinical efficiency, and optimise the use of resources. Further research with long-term outcomes is needed to better understand the condition, to help HCPs improve the path to diagnosis and treatment for HMB, and to have a positive impact on the quality of life of the women affected.
Authors’ roles
A.L.S.F contributed to the critical discussion and analysis of survey data, developed the initial manuscript draft and reviewed all subsequent drafts. C.C. oversaw the design, development and conduct of the survey, was involved in critical discussion of survey data and reviewed all manuscript drafts. A.L. was involved in the design, development and conduct of the survey, critical discussion and analysis of survey data and reviewed all manuscript drafts. G.G. contributed to the critical discussion and analysis of survey data and had input into the initial manuscript draft as well as reviewed all subsequent drafts. R.M.L contributed to the critical discussion and analysis of survey data and had input into the initial manuscript draft as well as reviewed all subsequent drafts. All authors read and approved the final manuscript.
Supplemental Material
Download MS Word (14.3 KB)Acknowledgements
The authors would like to acknowledge Highfield, Oxford, UK for providing medical writing assistance with funding from Bayer AG, Berlin, Germany.
Disclosure statement
A.L.S.F and G.G are members of the HELP Group whose formation and ongoing work is supported by Bayer AG, Berlin, Germany. A.L.S.F and G.G have acted as consultants to Bayer AG and have received consultancy honoraria. C.C is an employee of Bayer Consumer Care AG. A.L is an employee of Bayer AG. R.M.L has no conflict of interest to declare.
Data availability statement
The data on which this article is based will be shared on reasonable request to the corresponding author.
Additional information
Funding
References
- Bofill Rodriguez M, Lethaby A, Jordan V. Progesterone or progestogen-releasing intrauterine systems for heavy menstrual bleeding. Cochrane Database Syst Rev. 2020;6:CD002126.
- Bitzer J, Serrani M, Lahav A. Women’s attitudes towards heavy menstrual bleeding, and their impact on quality of life. Open Access J Contracept. 2013;4:21–28.
- National Institute for Health and Care Excellence. Heavy menstrual bleeding: assessment and management. NICE guideline NG88. London: National Institute for Health and Care Excellence; 2018. (last updated 2020).
- Marjoribanks J, Lethaby A, Farquhar C. Surgery versus medical therapy for heavy menstrual bleeding. Cochrane Database Syst Rev. 2016;2016:CD003855.
- Munro MG, Critchley HO, Broder MS, et al. FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113:3–13.
- Hallberg L, Högdahl AM, Nilsson L, et al. Menstrual blood loss – a population study. Variation at different ages and attempts to define normality. Acta Obstet Gynecol Scand. 1966;45:320–351.
- Byles JE, Hanrahan PF, Schofield MJ. ‘It would be good to know you’re not alone’: the health care needs of women with menstrual symptoms. Fam Pract. 1997;14:249–254.
- Copher R, Le Nestour E, Law A, et al. Retrospective analysis of variation in heavy menstrual bleeding treatments by age and underlying cause. Curr Med Res Opin. 2013;29(2):127–139.
- Fraser IS, Mansour D, Breymann C, et al. Prevalence of heavy menstrual bleeding and experiences of affected women in a European patient survey. Int J Gynaecol Obstet. 2015;128:196–200.
- Committee on Practice Bulletins—Gynecology. Practice bulletin no. 136: management of abnormal uterine bleeding associated with ovulatory dysfunction. Obstet Gynecol. 2013;122:176–185.
- Singh S, Best C, Dunn S, et al. Abnormal uterine bleeding in pre-menopausal women. J Obstet Gynaecol Can. 2013;35:473–475.
- Schrijvers G, van Hoorn A, Huiskes N. The care pathway: concepts and theories: an introduction. Int J Integr Care. 2012;12:e192.
- Bidmon S, Terlutter R. Gender differences in searching for health information on the internet and the virtual patient–physician relationship in Germany: exploratory results on how men and women differ and why. J Med Internet Res. 2015;17:e156.
- Office for National Statistics. Internet access – households and individuals, Great Britain: 2019. Statistical Bulletin, 12 August 2019. London: Office for National Statistics; 2019. [cited 28 July 2020]. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/householdcharacteristics/homeinternetandsocialmediausage/bulletins/internetaccesshouseholdsandindividuals/2019
- Karlsson TS, Marions LB, Edlund MG. Heavy menstrual bleeding significantly affects quality of life. Acta Obstet Gynecol Scand. 2014;93:52–57.
- Lukes AS, Moore KA, Muse KN, et al. Tranexamic acid treatment for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116(4):865–875.
- Endrikat J, Shapiro H, Lukkari-Lax E, et al. A Canadian, multicentre study comparing the efficacy of a levonorgestrel-releasing intrauterine system to an oral contraceptive in women with idiopathic menorrhagia. J Obstet Gynaecol Can. 2009;31(4):340–347.
- Shabaan MM, Zakherah MS, El-Nashar SA, et al. Levonorgestrel-releasing intrauterine system compared to low dose combined oral contraceptive pills for idiopathic menorrhagia: a randomized clinical trial. Contraception. 2011;83(1):48–54.
- Fraser IS, Parke S, Mellinger U, et al. Effective treatment of heavy and/or prolonged menstrual bleeding without organic cause: pooled analysis of two multinational, randomised, double-blind, placebo-controlled trials of oestradiol valerate and dienogest. Eur J Contracept Reprod Health Care. 2011;16:258–269.
- Reid PC, Virtanen-Kari S. Randomised comparative trial of the levonorgestrel intrauterine system and mefenamic acid for the treatment of idiopathic menorrhagia: a multiple analysis using total menstrual fluid loss, menstrual blood loss and pictorial blood loss assessment charts. BJOG. 2005;112(8):1121–1125.
- Kaunitz AM, Bissonnette F, Monteiro I, et al. Levonorgestrel-releasing intrauterine system or medroxyprogesterone for heavy menstrual bleeding: a randomized controlled trial. Obstet Gynecol. 2010;116(3):625–632. Published correction: Obstet Gynecol. 2010;116:999.
- Lunardi Rocha AL, Cristina França Ferreira M, Mara Lamaita R, et al. Heavy menstrual bleeding: a global survey of health care practitioners’ perceptions. Eur J Contracept Reprod Health Care. 2018;23(4):288–294.
- Schneider CE. The practice of autonomy: patients, doctors, and medical decisions. New York (NY): Oxford University Press; 1998.
- Schivone GB, Glish LL. Contraceptive counseling for continuation and satisfaction. Curr Opin Obstet Gynecol. 2017;29:443–448.
- Christiansen R, Emiliussen J. Manipulation and free will in shared decision making. J Eval Clin Pract. 2020;26:403–408.
- Zandstra D, Busser JAS, Aarts JWM, et al. Interventions to support shared decision-making for women with heavy menstrual bleeding: a systematic review. Eur J Obstet Gynecol Reprod Biol. 2017;211:156–163.
- National Institute for Health and Care Excellence. Heavy menstrual bleeding: assessment and management. Clinical guideline CG44. London: National Institute for Health and Care Excellence; 2007. (last updated 2016; replaced by NICE guideline NG88).