
Abstract
Objective: To evaluate requests for legal abortion due to pregnancies resulting from sexual violence (SV) in a reference service, and characterise and compare the outcome groups.
Methods
Retrospective cohort study with review of medical records of women assisted between 2015 and 2020. The variables were socio-demographic and SV characteristics, gestational age, reactions towards pregnancy and outcome. We compared outcome groups using the chi-square test, Fisher’s exact test and the Kruskal–Wallis test. The significance level was 5%.
Results
We evaluated the medical records of 235 women, of which 153(65%) had undergone to abortion; 17(7.2%) had a spontaneous abortion; 19(8%) remained pregnant; 25(10.6%) had an abortion denied; and 21(8.9%) had been lost to follow-up. Out of the total number of women, 44(18.7%) were adolescents, 152(65.2%) were white and 201(88.5%) had an education ≥9 years. Women who remained pregnant had a known aggressor, disclosed the pregnancy (p < 0.001) and were more ambivalent (p < 0.001) than the other groups. Gestational age was higher in the denied abortion group than in the performed abortion group (p < 0.001).
Conclusion
Feelings related to decision-making about abortion affected all groups, with differences. It is important to give women space to be heard, so they can make their own decisions.
SHORT CONDENSATION
Abortion care is possible in places with restrictive laws; however, women with more vulnerable characteristics did not seek the service. Legal restrictions interfere with women’s decision-making about abortion and can promote inequality in gaining access to health services.
Introduction
The global prevalence of sexual violence (SV) against women aged 15 to 49 shows that 30% of women are victimised by intimate partners (IPV) and 7.2% by non-intimate partner perpetrators [Citation1]. Pregnancies resulting from SV are a threat to women’s physical and mental health and a challenge for health services, particularly in countries with restrictive abortion laws.
The lack of data on abortion in most countries makes it necessary for the calculation of global and regional estimates to be based on different methodologies, such as the number of unwanted pregnancies, the use of contraceptives, or different income groups and regions with or without restrictive abortion laws [Citation2]. One study found that 61% of unwanted pregnancies ended in abortion in the period 2015–2020, with a total global occurrence of 73.3 million abortions per year on average, which corresponded to an annual global rate of 39 abortions per 1,000 women aged 15 to 49 [Citation3].
The World Health Organisation (WHO) has categorised termination of pregnancy according to the safety of its execution as safe, less safe and least safe [Citation4]. Safe or legal abortion is conceptualised when the procedure is performed by a trained professional using recommended methods, which covers an estimated proportion of 55% of abortions worldwide. Less safe abortion is defined when the procedure includes only one of the conditions and is estimated to occur in 31% of situations. The unsafe scenario is when the procedure is conducted by untrained persons and when unsafe techniques or methods are used, which is estimated to occur in about 14% of abortions [Citation4].
A systematic review to evaluate unsafe abortion in Brazil, with 50 articles published in the period 2008–2018, estimated the prevalence of induced abortion by the direct method to be 15% in 2010 and 13% in 2016, indicating that abortion is frequently used, especially in less developed regions and by more socially vulnerable women [Citation5], who probably do not use legal abortion services. Brazil is one of the countries with the most restrictive abortion laws in the world; it is legal in cases of SV, saving a woman’s life and, since 2012, in anencephalic foetus situations [Citation6].
Services that respond to abortion requests in countries with restrictive laws must be accessible to all women who request a legal procedure, while also needing to develop processes for supportive care and follow-up for those situations in which the law does not provide for. Knowing the characteristics of women who request legal abortions and the outcome of these requests may clarify the regional view of this health demand and help to improve the quality of care.
The objectives of this study were to evaluate the legal abortion requests due to pregnancy resulting from SV, and the outcomes, in a reference service in the state of São Paulo, Brazil. Socio-demographic and SV characteristics, feelings and attitudes expressed by women regarding pregnancy were compared in different outcome groups.
Materials and methods
This research was a retrospective cohort study carried out at the University Hospital of the Centre for Integral Attention to Women’s Health Prof. Dr José Aristodemo Pinotti, Faculty of Medical Sciences, State University of Campinas, UNICAMP. The project was approved by the Institutional Research Ethics Committee (REC, CAAE number: 50653921.1.0000.5404). Due to the study design, we asked the REC to waive the application of the consent form for this research, which was agreed.
The study setting is a university hospital, which is a reference for tertiary health care in the metropolitan region of Campinas, São Paulo, Brazil, with coverage for a population of around 4.0 million inhabitants. It provides emergency care to women victims of SV and since 1998 has been one of the reference hospitals in the Unified Health System (SUS) for abortion care. After the procedure, the service offers six-month outpatient follow-up carried out by a multidisciplinary team made up of nurses, gynaecologists, psychiatrists, psychologists and social workers [Citation7].
This study was based exclusively on a review of digital and physical medical records that contained the notes of the multidisciplinary team who aided women that sought the service to request a legal abortion in pregnancies resulting from SV in the period from 01-01-2015 to 12-31-2020. All data necessary to study the proposed variables were collected from the medical records in a form designed for the research, categorised and subsequently inserted into the database for analysis.
The variables studied were socio-demographic (origin, age, self-reported skin colour, marital status, education, occupation [employee, student, student and work, at home/no formal occupation], religion, place of residence and monthly family income); obstetric history (number of deliveries and abortions, current gestational age in days); characteristics of violence (known aggressor, any form of intimidation, place of approach [public place, residence, party or workplace]); personal history of any another violence (domestic violence, IPV and sexual violence); feelings expressed about pregnancy (guilt, shame, depression, rage, crying, ambivalence, desire to terminate pregnancy, pregnancy aversion); and attitudes (disclosure about pregnancy, social isolation).
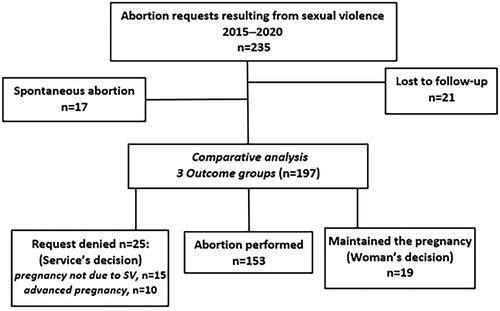
The data collected from the medical records made it possible to identify five outcomes, called ‘outcome groups for the request’, according to the information analysed in relation to the evolution of the pregnancy and considering both the woman’s and the service’s decision (). To better understand the differences in the main outcomes, the spontaneous abortion and loss to follow-up groups were excluded from the comparative analysis.
Figure 1. Flowchart of abortion requests in pregnancies resulting from sexual violence in the period 2015–2020 and outcome groups of comparison.
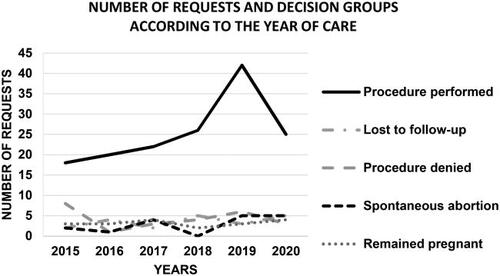
Graphic 1. Number of requests and outcome groups according to the year of care Fisher’s exact test. p = 0.458.
Statistical analysis
Variables were described as number and percentage or mean and standard deviation (SD). For comparison between groups, we used the chi-square and Fisher’s exact tests for the categorical variables, and the Mann–Whitney and Kruskal–Wallis tests for the numerical variables. We used the Statistical Analysis System for Windows, version 9.2 (SAS Institute Inc., 2002–2008, Cary, NC, USA); the level of significance adopted was 5%.
Results
We evaluated the medical records of 235 women aged 10–43; the socio-demographic and obstetric characteristics of the sample of women are shown in . Of the 235 women, 44 (18.7%) were teenagers, while most women were single, lived with their family, worked and/or studied, had ≥9 years of schooling and reported having a religion. About a third of the women were at home/had no formal occupation and self-declared as non-white; only 30 (13%) women lived with a partner, 26 (11.4%) had up to eight years of schooling and the same number lived alone; 28 (12%) women came from cities outside the service’s coverage region. Two-thirds of the women had already given birth and less than 10% had had a previous abortion ().
Table 1. Socio-demographic and obstetric characteristics of women victims of sexual violence who requested legal abortion in the period 2015–2020.
After data collection, women were categorised into outcome groups composed of 153 (65.1%) women who had the abortion procedure performed, 17 (7.2%) who evolved to spontaneous abortion, 19 (8%) who remained pregnant, 25 (10.6%) for whom the abortion was denied and 21 (8.9%) women who were lost to follow-up after the first contact with the service ().
For the group of 153 women who underwent legal abortion, the total time from admission to the procedure had a mean of 15.4 (SD ± 9.9) days (data not shown). Of the 25 women whose requests were denied, 15 had pregnancies that did not correspond to SV and the remainder were of advanced gestational age, ranging from >22 to 32 weeks (data not shown). In this group, 12/25 women were victims of a known aggressor (data not shown). The number of requests distributed by outcome groups was similar during the period 2015 to 2020, as shown in .
The comparative analysis carried out for the three groups showed differences for the education and occupation variables (). When compared to the other groups, the performed procedure group had a higher frequency of women with ≤8 years and with ≥12 years of schooling, while the remained pregnant and abortion denied groups contained a greater number of women with 9–11 years of schooling (p = 0.043) (). The performed procedure and abortion denied groups had a higher frequency of employed women, while the remained pregnant group had a higher number of women at home/no formal occupation (p = 0.048) (). Gestational age was higher for the denied abortion group than for the groups that had the procedure performed and remained pregnant (p < 0.001) ().
Table 2. Comparison between outcome groups in relation to socio-demographic characteristics, obstetric history and gestational age at admission.
There were significant differences between the groups for some variables related to aggression and reactions to pregnancy (). Aggression perpetrated by unknown aggressors was more frequent in the procedure group than in the other groups (p = 0.005) (). The feelings of shame and crying were less frequently expressed by the remained pregnant group than by the other groups, p = 0.034 and p = 0.002, respectively. The remained pregnant group expressed more feelings of ambivalence (p < 0.001) and less desire to terminate the pregnancy (p < 0.001) than the other groups ().
Table 3. Comparison between outcome groups in relation to SV characteristics, personal history, reactions and attitudes related to pregnancy.
In relation to women’s attitudes towards pregnancy, the remained pregnant group had a higher proportion of women who disclosed their pregnancy than the other two groups (p = 0.048). The groups that had the procedure performed and were denied abortion reported social isolation more frequently than the remained pregnant group (p = 0.028) (). The place of approach and the history of previous violence was similar between the groups. Of the women who reported a history of sexual violence, nine (17%) reported a history of child abuse and 44 (83%) reported a history of IPV (data not shown).
Discussion
Findings and interpretation
Women who requested an abortion and had the procedure performed experienced a total time from admission to the procedure of around 15 days, which was compatible with the time described in abortion clinics in regions where abortion is widely legalised [Citation8].
On the other hand, and in line with a previous study, the feelings and attitudes reported by the women reflected suffering [Citation7]. However, we found differences in the behaviour of women in relation to abortion when the aggressor was known. The frequency of a known aggressor was higher in the group of women who remained pregnant by their own decision, while in the performed abortion group the unknown aggressor was more frequent. It is possible that survivors of SV by an unknown aggressor receive greater empathy and have greater encouragement from the people around them to perform the abortion. These results are in line with a study carried out in the city of São Paulo that evaluated 2,418 abortion requests due to SV in the period 1994–2017 and found that known perpetrators were significantly more frequent among the 636 cases in which an abortion was not performed [Citation9].
In addition, the group that remained pregnant had a higher frequency of women at home/no occupation, characteristic of financial dependence that may compromise their decision to have an abortion. The lack of support around a woman or her loneliness in facing the request for a legal abortion can also influence the decision to continue the pregnancy.
The variation in feelings and disclosure/social isolation attitudes between the groups was interpreted as resulting from cultural factors that subject women to behaviours of acceptance of the female role, dictated by religion and a conservative society. It has been reported that women internalise society’s prejudices, and that the decision to abort or experience an abortion leads to the breakdown of cultural and religious beliefs and social expectations, which increases suffering [Citation10]. The result of these ‘breaks’ with the sociocultural environment in which a woman is inserted leads to greater social isolation reported by those women who made the decision to have an abortion, as described in other studies [Citation7, Citation10].
In this study, we found a higher proportion of women with ≥9 years of education (88.5%) than that described in the national survey, in which this level of education corresponded to 53.3% of Brazilian women [Citation11]. On the other hand, we found only 81/235 (34.7%) women who self-reported non-white skin colour, contrasting with data from the Brazilian survey, which indicated that 56.1% of the population self-declared as brown or black and 43% as having a white skin colour [Citation11]. It is possible that there are errors in the collection of skin colour data or that the information was not self-reported but noted by a professional inserted in a context of institutional and structural racism. But it is also possible, given the higher education level of this sample, that women belonging to the lowest socio-economic stratum and with greater vulnerability to suffering SV did not have access to this abortion care service. Either they did not have information about the right to legal abortion and about existing services, or they had difficulties in reaching a reference service.
Some women had the procedure denied due to advanced gestational age, above 22 weeks; the abortion denied was the group that least reported intimidation during violence. These results suggest difficulty in asking for help when the aggressor is nearby; in addition, if it is a family member, it may take time for patients to seek medical attention. A study was carried out with 311 adolescents who requested an abortion, 137 victims of incest and 174 victims of unknown aggressors, indicating that a relationship with the aggressor can inhibit the patient’s communication with other people or entities to reveal the situation of violence and/or the diagnosis of pregnancy [Citation12]. On the other hand, in countries with restrictive laws, many women cannot obtain information about specific situations in which abortion is permitted, do not talk or are slow to disclose details about SV and end up contacting services at an advanced gestational age.
Results in the context of what is known
One study carried out to characterise the provision and performance of abortion for medical and legal reasons in Brazil used national health information registries [Citation13]. The 251 services that had registered procedures in 2019 were located in only 3.6% of Brazilian municipalities, mainly in the south-east region (40.5%), with more than 100,000 inhabitants (59.5%) and with a high or very high Human Development Index (77.5%), showing the uneven distribution in the territory. The rate of abortions provided by law among residents of childbearing age in municipalities without abortion care services was 4.8 times lower than that in municipalities that had these services [Citation13].
Another study used official health data from public information systems in Brazil in the period 2008–2015 and reported 200,000 hospitalisations/year for abortion-related procedures, with around 1,600 for medical and legal reasons [Citation14]. From 2006 to 2015, 770 maternal deaths were found with the underlying cause being abortion, highlighting a probable under-reporting of data [Citation14]. The authors pointed out that although it was not possible to estimate the number of abortions in the country, it was possible to draw a profile of women at greater risk of death from abortion: those who are black and indigenous, with low education, aged under 14 and over 40, living in the north, north-east and central-west regions, and without a partner [Citation14].
A qualitative study evaluated women’s routes to, and search for, legal abortion in Brazil and showed that in addition to the psychosocial disorganisation resulting from violence, the obstacles to the right established by law are misinformation, the precariousness of care networks and the conscientious objection of professionals [Citation15]. The lack of information, both in society and in the health and protection network, constitutes one of the main barriers to access to the right to abortion provided for by law in Brazil [Citation7,Citation15].
As several countries have proven, the only approach capable of reducing the number of unwanted pregnancies terminated in abortions and mortality from unsafe abortion in the long term, is to legalise abortion at the request [Citation16,Citation17].
The stigmatisation of women who suffer sexual violence as well as abortion occurs in the most conservative societies and prevents many women from asking for help [Citation10]. However, where individual rights are respected women’s experience of abortion is expressed as more positive; they feel more competent in managing their lives, and they describe a sense of themselves as good women [Citation18].
Clinical implications
Delays in seeking/accessing care may also be associated with the restrictive abortion environment and many women access the health service when their pregnancy is advanced. Recent publications were aimed at facilitating the practical application of clinical recommendation guidelines on abortion care, including in cases of advanced pregnancy [Citation19,Citation20]. But the restrictive abortion environment strongly impacts the adequacy of services to care recommendations, particularly in advanced pregnancy.
Research implications
Despite the higher frequency of women coming from the city of Campinas and cities in the coverage region, we observed 12% from outside, which confirms that, although the SUS organisation system is hierarchical in terms of territorial coverage, abortion services in the country are still admittedly scarce and irregularly distributed and have functional problems [Citation13].
It is important to bear in mind that the characteristics of the women in this study represent only those who were able to seek our service through other services or because they had their own information about it.
Strengths and limitations
The main limitation of this study was evaluating a restricted population, namely women treated in a single service and who did not represent the characteristics of the country’s female population, probably because they live in a region with greater access to services and information. Another limitation of this study was the lack of information on some variables, such as the small proportion of women with a declared family income, which may have generated bias in the analysis.
On the other hand, the strength of this study was understanding the results of assistance with abortion requests in our context and the inequity of this assistance, which may possibly be matched in other legal abortion care services in Brazil.
Conclusions
This study has shown the particularities of abortion health care in situations of restrictive law and its outcomes. The results showed the importance of having a team prepared to accept suffering and ambivalence, while helping the patients in making the decision they consider most appropriate.
Restrictive laws have not resolved inequality of access, even in situations with legal permission.
Acknowledgements
We thank the Special Programme for Research, Development and Training in Research on Human Reproduction (HRP) UNDP-UNFPA-UNICEF-WHO-World Bank, co-sponsored by the World Health Organization (WHO), for supporting PYS (MSc fellow), and the Brazilian National Research Council (CNPq).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data are not available. Data were collected from medical records based on notes from a multidisciplinary team.
References
- World Health Organization. Global and regional estimates of violence against women: prevalence and health effects of intimate partner violence and nonpartner sexual violence. [internet]. Geneva: world Health Organization; 2013. https://www.who.int/publications/i/item/9789241564625
- Singh S, Remez L, Sedgh G, et al. Abortion worldwide: uneven progress and unequal access. New York: Guttmacher Institute; 2018. https://www.guttmacher.org/sites/default/files/report_pdf/abortion-worldwide-2017.pdf.
- Bearak J, Popinchalk A, Ganatra B, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. 2020;8(9):e1152–e1161. doi: 10.1016/S2214-109X(20)30315-6.
- Ganatra B, Gerdts C, Rossier C, et al. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a bayesian hierarchical model. Lancet. 2017;390(10110):2372–2381. doi: 10.1016/S0140-6736(17)31794-4.
- Domingues RMSM, Fonseca SC, Leal MDC, et al. Unsafe abortion in Brazil: a systematic review of the scientific production, 2008–2018. Cad Saude Publica. 2020;36(Suppl 1):e00190418. doi: 10.1590/0102-311X00190418.
- World Health Organization. Abortion care guideline. Geneva: world Health Organization; 2022. https://www.who.int/publications/i/item/9789240039483
- Machado CL, Fernandes AM, Osis MJ, et al. Gravidez após violência sexual: vivências de mulheres em busca da interrupção legal [rape-related pregnancy in Brazil: the experience of women seeking legal abortion]. Cad Saude Publica. 2015;31(2):345–353. doi: 10.1590/0102-311x00051714.
- Fulcher IR, Neill S, Bharadwa S, et al. State and federal abortion restrictions increase risk of COVID-19 exposure by mandating unnecessary clinic visits. Contraception. 2020;102(6):385–391. doi: 10.1016/j.contraception.2020.08.017.
- Pedroso D, Juliano Y, de Souza PC, et al. Gravidez decorrente de violência sexual: caracterização sociodemográfica das mulheres e desfechos do aborto em um serviço público de referência, são paulo, brasil [pregnancy resulting from sexual violence: socio-demographic characterization of women and outcomes of abortion in a public service of reference, são paulo, Brazil]. Lat Americ J of Develop. 2021;3(3):1455–1471. doi: 10.46814/lajdv3n3-035.
- Adesse L, Jannotti CB, Silva KS, et al. Aborto e estigma: uma análise da produção científica sobre a temática [abortion and stigma: an analysis of the scientific literature on the theme]. Cien Saude Colet. 2016;21(12):3819–3832. doi: 10.1590/1413-812320152112.07282015.
- Brasil. Instituto Brasileiro de Geografia e Estatística – IBGE. Pesquisa Nacional por Amostra de Domicílios Contínua 2012/2021. [Brazilian Institute of Geography and Statistics – IBGE. Continuous National Household Sample Survey 2012/2021]. Brasília: IBGE; 2022. https://biblioteca.ibge.gov.br/visualizacao/livros/liv101957_informativo.pdf.
- Bessa MMM, Drezett J, Adami F, et al. Characterization of adolescent pregnancy and legal abortion in situations involving incest or sexual violence by an unknown aggressor. Medicina (Kaunas). 2019;55(8):474. doi: 10.3390/medicina55080474.
- Jacobs MG, Boing AC. O que os dados nacionais indicam sobre a oferta e a realização de aborto previsto em lei no brasil em 2019? [what do the national data say about the supply and performance of legal abortions in Brazil in 2019?]. Cad Saude Publica. 2021;37(12):e00085321. doi: 10.1590/0102-311X00085321.
- Cardoso BB, Vieira F, Saraceni V. Abortion in Brazil: what do the official data say? Aborto no brasil. Cad Saude Publica. 2020;36(Suppl 1):e00188718. doi: 10.1590/01002-311X00188718.
- Ruschel AE, Machado FV, Giugliani C, et al. Women victims of sexual violence: critical paths in the search for the right to legal abortion. Mulheres vítimas de violência sexual: rotas críticas na busca do direito ao aborto legal. Cad Saude Publica. 2022;38(10):e00105022.) doi: 10.1590/0102-311XPT105022.
- Benson J, Andersen K, Samandari G. Reductions in abortion-related mortality following policy reform: evidence from Romania, South Africa and Bangladesh. Reprod Health. 2011;8(1):39. doi: 10.1186/1742-4755-8-39.
- di Fazio N, Delogu G, La Russa R, et al. Voluntary interruption of pregnancy (VIP) in Italy: interpretation of the current situation according to the report 2019–2020 of the italian ministry of health. Clin Ter. 2022;173(3):235–242. doi: 10.7417/CT.2022.2426.
- Wainer J. Abortion and the struggle to be good in the 1970s. Aust N Z J Psychiatry. 2008;42(1):30–37. doi: 10.1080/00048670701732657.
- World Health Organization. Clinical practice handbook for quality abortion care. Geneva: World Health Organization; 2023. https://www.who.int/publications/i/item/9789240075207
- International Federation of Obstetrics and Gynecology (FIGO). Mifepristone & Misoprostol Dosing Chart. Recommended Regimens. 2023. https://www.figo.org/sites/default/files/2023-10/Mifepristone%20%26%20Misoprostol%20Dosing%20Chart%202023.pdf