
Abstract
Objectives: To evaluate the association between handgrip strength and erectile dysfunction (ED) in community-dwelling older men.
Methods: This cross-sectional study included 1771 participants of the Dong-gu Study. Handgrip strength was measured with a handheld dynamometer. ED was assessed with the Korean version of the International Index of Erectile Function (IIEF). ED was categorized as none to mild (IIEF-EF scores of 13–30) and moderate to severe (IIEF-EF scores of 0–12). Multivariable logistic regression was conducted with adjustment for potential confounders.
Results: The proportion of men with moderate to severe ED was 48.8%. The age-adjusted ED score increased with increasing quartile of handgrip strength (11.0, 12.4, 13.4, and 14.0 in the lowest, second, third, and highest quartiles, respectively). After adjustment for potential confounders, greater handgrip strength was associated with a lower risk of ED (odds ratio (OR): 0.82 per 5 kg; 95% confidence interval (CI): 0.74–0.90). In addition, a high level of moderate to vigorous physical activity was associated with a lower risk of ED (OR: 0.75; 95% CI: 0.61–0.93).
Conclusion: In this study, aging men with greater handgrip strength had a lower risk of ED. This result suggests that reduced physical functioning may contribute to ED.
Introduction
Sexual function is an important part of men’s health. Sexual dysfunction, especially erectile dysfunction (ED), can have a significant negative impact on the quality of life of affected men and their female partners [Citation1,Citation2]. There is much epidemiologic evidence demonstrating risk factors for ED, such as cardiovascular disease, diabetes, lower urinary tract symptoms, and other chronic diseases [Citation3,Citation4]. In addition, modifiable lifestyle factors including physical activity, smoking, diabetes control, and obesity are also related to ED [Citation5].
Physical fitness and activity have an important role in preventing chronic disease, including type 2 diabetes, osteoporosis, obesity, depression, and cancer [Citation6]. In the measurement of muscle fitness, handgrip strength is a quick, easy, noninvasive measure [Citation7]. Grip strength provides an indication of an individual’s overall strength and also gives indications of muscle mass, physical function, nutritional status, and health status [Citation8]. Recently, several researchers have focused on the relationship of handgrip strength with diabetes, hypertension, and other metabolic diseases [Citation9–11]. However, few studies have been conducted on the association between physical fitness and ED [Citation12,Citation13]. To our knowledge, the association between handgrip strength and ED has not been evaluated. The aim of this study was to evaluate the association between handgrip strength and ED in community-dwelling older men.
Materials and methods
Subjects
The Dong-gu Study is a population-based cohort study, which has previously been described in detail by Kweon et al. [Citation14]. The study was conducted to investigate the risk factors of chronic diseases such as stroke, myocardial infarction, fracture, and cognitive decline in an urban elderly population aged 50 years and older. The baseline survey was conducted from 2007 to 2010 and 9260 participants (3711 men and 5549 women) aged 50 years or older participated. Of the 9260 subjects, 5704 subjects (2301 males and 3403 females; response rate, 61.6%) participated in the follow-up survey from 2014 to 2016. Of 2301 men, 1875 subjects completed the erectile function questionnaire. A total of 1708 participants were included in the final analysis after excluding 167 subjects for whom information was not available on medical history, lifestyle, body measurements, and blood tests. All study subjects agreed to participate in the study and gave written consent, and the study was conducted in accordance with the guidelines in the Declaration of Helsinki. The study was approved by the Institutional Review Board of Chonnam National University Hospital.
Measurements
The severity of ED was assessed with the Korean version of International Index of Erectile Function (IIEF) [Citation15]. The severity of ED was classified into five diagnostic categories: no ED (EF score 26–30); mild ED (EF score 22–25); mild to moderate (EF score 17–21); moderate (EF score 11–16); and severe (EF score 6–10) [Citation16]. It was previously reported that men with moderate ED perceive the impact of ED on their life satisfaction equally to those with severe ED [Citation2]. Therefore, ED was categorized as none to mild (17–30) and moderate to severe (6–16) on the basis of IIEF-EF scores.
The grip strength of both hands was measured with a hand dynamometer (GRIP-D TKK 5401, Takei Scientific Instruments, Tokyo, Japan) with the subject in a standing position. The range of the grip strength measurement was 5.0–100 kg. We defined handgrip strength as the highest single force recorded during three trials with a 1––2 min rest period between each trial.
Trained interviewers surveyed information on sociodemographic characteristics, lifestyle, medical history, and drug use by use of a standardized questionnaire. Marital status was categorized as married or single (single, divorced, widowed, and separated). Smoking status was classified as current smoker or current nonsmoker. Alcohol consumption was also divided into none, 1–7 drinks per week and eight or more drinks per week. Regular physical activity was defined as either 30 min of moderate-intensity activity five or more days per week or 20 min of vigorous-intensity physical activity three or more days per week. Self-rated health was dichotomized into good (very good with good) and poor (fair with poor).
Body weight and body composition were measured with the subjects in indoor clothing or a light gown without shoes by use of a calibrated Inbody 520 body composition analyzer (Biospace Co., Korea). Waist circumference was measured with a tape measure at the minimum circumference between the iliac crest and the rib cage. Blood pressure was measured by using a mercury sphygmomanometer. After the subject had rested for 5 min, blood pressure was measured three times at one minute intervals. The average was used in the analysis. Brachial-ankle pulse wave velocity (baPWV) and ankle brachial index were measured using a VP-1000 noninvasive screening device (Colin Co. Ltd, Komaki, Japan). Peripheral arterial disease was defined by an ankle brachial blood pressure index <0.9.
Blood was drawn after 12 h of fasting and serum was separated by centrifugation within 30 min. Fasting blood glucose, creatinine, and blood lipids were measured using an enzymatic assay with an automatic analyzer (Hitachi-7600; Hitachi, Tokyo, Japan). Hemoglobin A1c (HbA1c) was measured by high-performance liquid chromatography (Bio-Rad Variant II; Bio-Rad Laboratories, Hercules, CA). Urinary albumin and creatinine were measured in single spot urine specimens and the urinary albumin-to-creatinine ratio was calculated and presented as albumin in milligrams divided by creatinine in grams. Kidney function was assessed by using estimated glomerular filtration rate (eGFR), which was calculated using the Modification of Diet in Renal Disease (MDRD) formula [Citation17].
Statistical analysis
Data are presented as the mean ± standard deviation (SD), or as percentages for categorical variables, according to ED status. Differences in baseline characteristics according to ED status were compared by using t-tests for continuous data and chi-square tests for categorical data. Multivariate logistic regression was conducted to evaluate the association between handgrip strength and ED with adjustment for potential confounders. We constructed three models: (1) unadjusted values, (2) values adjusted for age, and (3) values adjusted for age, marital status, body mass index, systolic blood pressure, diastolic blood pressure, total cholesterol, log triglyceride, High-density lipoprotein (HDL) cholesterol, HbA1c, good self-rated health, current smoking, alcohol consumption, moderate-intensity physical activity, hypertension medication use, diabetes medication use, dyslipidemia medication use, history of coronary heart disease, history of stroke, urinary albumin-to-creatinine ratio, and peripheral arterial disease. Statistical analysis was performed by using the SPSS 23 software package (IBM, Chicago, IL,). A p value less than .05 was considered statistically significant.
Results
The mean age of the study population was 70.7 years old and the prevalence of ED was 91.1%. Of 1708 participants, 13.1% had mild, 14.1% had mild to moderate, 19.4% had moderate, and 44.5% had severe ED. In this study, ED status was divided into two categories; no ED, mild ED, and mild to moderate ED was classified as none to mild ED. Otherwise, moderate ED and severe ED was classified as moderate to severe ED. shows the baseline characteristics of the study population by ED status. The proportion of men with moderate to severe ED was 63.9%. Men with moderate to severe ED tended to be older; to have a lower BMI; to have poorly controlled diabetes; to have a higher proportion of hypertension medication and diabetes medication use; to have a higher proportion of history of coronary heart disease; and to have a lower current alcohol intake and physical activity.
Table 1. Characteristic of the study population.
shows the age-adjusted score of ED according to quartile of handgrip strength. The age-adjusted ED score increased with increasing quartile of handgrip strength (11.0, 12.4, 13.4, and 14.0 in the lowest, second, third, and highest quartile, respectively, p value for the trend was < .001). shows the results of the fully adjusted logistic regression model. In the fully adjusted model, greater handgrip strength was associated with a lower risk of ED (odds ratio (OR): 0.86 per 5 kg; 95% confidence interval (CI): 0.78–0.96). In addition, age (OR, 1.13; 95% CI, 1.11–1.16) and HbA1c levels (OR, 1.29; 95% CI, 1.07–1.56) were associated with a high risk of ED, whereas good self-rated health (OR, 0.56; 95% CI, 0.44–0.72) and a high level of moderate to vigorous physical activity (OR, 0.69; 95% CI, 0.54–0.90) were associated with a lower risk of ED.
Figure 1. Age-adjusted erectile function score according to quartile of handgrip strength (kg).
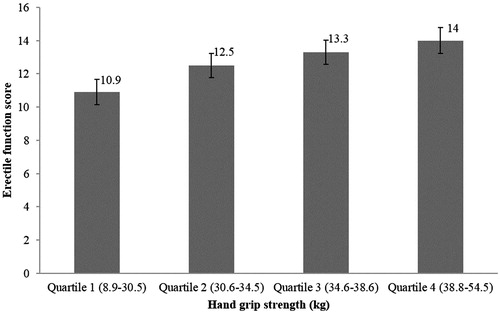
Table 2. Multivariate logistic regression analysis of risk factors for erectile dysfunction (ED).
Discussion
The principal finding of the present study was that men with lower handgrip strength had a higher risk of moderate to severe ED. Also our study demonstrated that ED was significantly associated with age, HbA1c, self-related health, and physical activity in aging men.
Handgrip strength, which is a simple, inexpensive, risk-stratifying method for assessing muscle strength, is easy to use in both clinical and community settings [Citation10]. Goodpaster et al. [Citation18] reported that decline in muscle strength is much more rapid than that in muscle mass and that gaining muscle mass does not prevent aging-related declines in muscle strength. Moreover, low muscle mass does not explain the strong association of strength with mortality, demonstrating that muscle strength as a marker of muscle quality is more important than muscle quantity in estimating mortality risk [Citation19]. These studies indicated that assessing muscle strength may be more appropriate for evaluating the risk of ED than measuring muscle mass. Handgrip strength measured in a sitting position represent the muscle strength of forearm and upper extremities and measured in a standing position can include lower extremities and core muscle strength [Citation9]. We selected handgrip strength as a measure of muscle strength in a standing position and evaluated the association between handgrip strength and ED.
Several studies have reported that handgrip strength is associated with type 2 diabetes, cardiovascular disease, and other metabolic disease [Citation9–11,Citation20]. Lee et al. [Citation9] reported that relative handgrip strength is significantly associated with cardiometabolic risk and that the association was stronger than that using dominant handgrip strength. In a prospective epidemiologic study, Leong et al. [Citation10] reported that handgrip strength is a risk marker for incident cardiovascular disease in some countries and populations. Handgrip strength showed an inverse association with incident type 2 diabetes and HbA1c [Citation11,Citation20]. Low muscle strength was associated with an increased likelihood of metabolic syndrome in men, independent of age, smoking, and alcohol intake [Citation20].
There are several possible reasons for the association of handgrip strength with these diseases. Age-related changes in muscle composition, particularly lipid accumulation in skeletal muscle fibers, contribute to poor muscle quality and cause metabolic disorders, including insulin resistance [Citation21]. Loss of muscle quality and muscle mass appear to be due to the progressive loss of Type II muscle fibers and motor neurons [Citation22,Citation23]. Loss of muscle fiber can lead to the development of diabetes and cardiometabolic disease, because the skeletal muscle is the main site for glucose uptake and deposition [Citation24]. Low handgrip strength in patients with undiagnosed diabetes could be caused by peripheral neuropathy [Citation25].
Many studies have reported on the relationship between ED and age, diabetes, cardiovascular disease, and other metabolic disease [Citation3,Citation4,Citation26]. In the present study, previously well-known, fully adjusted regression analysis showed that men with younger age, well controlled diabetes, good self-related health, and higher physical activity were less likely to suffer from moderate to severe ED.
A randomized controlled trial has proven that physical activity has a protective and therapeutic effect in the treatment of ED [Citation27]. The role of testosterone in ED has been well established in both basic and clinical research [Citation28]. Chin et al. [Citation29] reported that sex hormone status is an important factor in handgrip strength in men. Testosterone supplementation increases muscle strength [Citation30] and also improves ED [Citation28]. In the present study, lower handgrip strength seemed to be related to a higher risk of moderate to severe ED. The biological mechanism linking handgrip strength and ED should be investigated in the future.
There were several limitations in the present study. This study was cross-sectional in nature and it cannot establish a causal relation between handgrip strength and ED. The study can only show that handgrip strength is associated with ED. Further study is warranted to investigate the usefulness of handgrip strength in prevention and recovery of ED. The present study was confined to population from some part of East Asia. Therefore an additional area of future research could provide normative data potentially normed for different ethnic groups. Sexual hormones including testosterone were not assessed, hence its association with both handgrip strength and ED should be analyzed in future. Also, we selected dominant handgrip strength in a standing position as the primary measurement in this study. Future clinical studies are necessary to determine which measurement of handgrip strength may be more appropriate for evaluation of ED risk.
Conclusions
Aging men with greater handgrip strength had a lower risk of moderate to severe ED. Also, men with good self-assessed health and higher physical activity were less likely to suffer from moderate to severe ED. These results suggest that reduced physical functioning may contribute to ED. Further studies are needed to determine whether handgrip strength could be used for evaluation of ED risk.
Acknowledgements
HS Chung contributed to data management and manuscript writing/editing. MH Shin contributed to project development, data collection, and data analysis. K Park contributed to project development, data management, and manuscript editing. We thank Jennifer Holmes for assistance in editing the text.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Fisher WA, Rosen RC, Mollen M, et al. Improving the sexual quality of life of couples affected by erectile dysfunction: a double-blind, randomized, placebo-controlled trial of vardenafil. J Sex Med. 2005;2:699–708.
- Mallis D, Moisidis K, Kirana PS, et al. Moderate and severe erectile dysfunction equally affects life satisfaction. J Sex Med. 2006;3:442–449.
- Braun M, Wassmer G, Klotz T, et al. Epidemiology of erectile dysfunction: results of the 'Cologne Male Survey'. Int J Impot Res. 2000;12:305–311.
- Ho CH, Wu CC, Chen KC, et al. Erectile dysfunction, loss of libido and low sexual frequency increase the risk of cardiovascular disease in men with low testosterone. Aging Male. 2016;19:96–101.
- McCabe MP, Sharlip ID, Lewis R, et al. Risk factors for sexual dysfunction among women and men: a consensus statement from the fourth international consultation on sexual medicine 2015. J Sex Med. 2016;13:153–167.
- Thompson PD, Buchner D, Pina IL, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the council on clinical cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the council on nutrition, physical activity, and metabolism (Subcommittee on Physical Activity). Circulation. 2003; 107:3109–3116.
- Chen LK, Lee WJ, Peng LN, et al. Recent advances in sarcopenia research in Asia: 2016 update from the Asian working group for Sarcopenia. J Am Med Dir Assoc. 2016;17:767.e761–e767.
- Bohannon RW. Muscle strength: clinical and prognostic value of hand-grip dynamometry. Curr Opin Clin Nutr Metab Care. 2015;18:465–470.
- Lee WJ, Peng LN, Chiou ST, et al. Relative handgrip strength is a simple indicator of cardiometabolic risk among middle-aged and older people: a nationwide population-based study in Taiwan. PloS One. 2016;11:0160876.
- Leong DP, Teo KK, Rangarajan S, et al. Prognostic value of grip strength: findings from the prospective urban rural epidemiology (PURE) study. Lancet. 2015;386:266–273.
- Li JJ, Wittert GA, Vincent A, et al. Muscle grip strength predicts incident type 2 diabetes: population-based cohort study. Metab Clin Exp. 2016;65:883–892.
- Agostini LC, Netto JM, Miranda MV Jr, et al. Erectile dysfunction association with physical activity level and physical fitness in men aged 40-75 years. Int J Impot Res. 2011;23:115–121.
- Kalka D, Domagala Z, Dworak J, et al. Association between physical exercise and quality of erection in men with ischaemic heart disease and erectile dysfunction subjected to physical training. Kardiol Pol. 2013;71:573–580.
- Kweon SS, Shin MH, Jeong SK, et al. Cohort profile: the Namwon study and the Dong-gu study. Int J Epidemiol. 2014;43:558–567.
- Chung TG, Chung S, Lee MS, et al. The Korean version of the international index of erectile function(IIEF): reliability and validation study. Korean J Urol. 1999; 40:1334–1343.
- Cappelleri JC, Rosen RC, Smith MD, et al. Diagnostic evaluation of the erectile function domain of the international index of erectile function. Urology. 1999; 54:346–351.
- Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Ann Intern Med. 1999; 130:461–470.
- Goodpaster BH, Park SW, Harris TB, et al. The loss of skeletal muscle strength, mass, and quality in older adults: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci. 2006;61:1059–1064.
- Newman AB, Kupelian V, Visser M, et al. Strength, but not muscle mass, is associated with mortality in the health, aging and body composition study cohort. J Gerontol A Biol Sci Med Sci. 2006;61:72–77.
- Senechal M, McGavock JM, Church TS, et al. Cut points of muscle strength associated with metabolic syndrome in men. Med Sci Sports Exerc. 2014;46:1475–1481.
- Mainous AG 3rd, Tanner RJ, Anton SD, et al. Grip strength as a marker of hypertension and diabetes in healthy weight adults. Am J Prev Med. 2015;49:850–858.
- Faulkner JA, Larkin LM, Claflin DR, et al. Age-related changes in the structure and function of skeletal muscles. Clin Exp Pharmacol Physiol. 2007;34:1091–1096.
- Abe T, Thiebaud RS, Loenneke JP, et al. Association between forearm muscle thickness and age-related loss of skeletal muscle mass, handgrip and knee extension strength and walking performance in old men and women: a pilot study. Ultrasound Med Biol. 2014;40:2069–2075.
- Corcoran MP, Lamon-Fava S, Fielding RA. Skeletal muscle lipid deposition and insulin resistance: effect of dietary fatty acids and exercise. Am J Clin Nutr. 2007;85:662–677.
- Koopman RJ, Mainous AG, Liszka HA, et al. Evidence of nephropathy and peripheral neuropathy in US adults with undiagnosed diabetes. Ann Fam Med. 2006;4:427–432.
- Kaya E, Sikka SC, Gur S. A comprehensive review of metabolic syndrome affecting erectile dysfunction. J Sex Med. 2015;12:856–855.
- Maio G, Saraeb S, Marchiori A. Physical activity and PDE5 inhibitors in the treatment of erectile dysfunction: results of a randomized controlled study. J Sex Med. 2010;7:2201–2208.
- Corona G, Maggi M. The role of testosterone in erectile dysfunction. Nat Rev Urol. 2010;7:46–56.
- Chin KY, Soelaiman IN, Naina Mohamed I, et al. Testosterone is associated with age-related changes in bone health status, muscle strength and body composition in men. Aging Male. 2012;15:240–245.
- Page ST, Amory JK, Bowman FD, et al. Exogenous testosterone (T) alone or with finasteride increases physical performance, grip strength, and lean body mass in older men with low serum T. J Clin Endocrinol Metab. 2005;90:1502–1510.