
Abstract
Aim
To find the answer to the question: is a high level of empathy of intensive care nurses effective in increasing organ donation?
Materials and Methods
This study was performed with nurses who had been working in intensive care units for at least 1 year in 17 hospitals in 8 provinces in Turkey. Jefferson Scale of Empathy and the other questionnaire forms were sent to the nurses by email, and completed forms from those who accepted to participate in the study were also received by email.
Results
There was a positive significant relationship between donor declaration and empathy score. An increase was observed in empathy score as donor declaration increased. Cronbach’s alpha coefficient of Jefferson Scale of Empathy (JSE) in general was α = 0.71. JSE is an acceptable tool of measurement in terms of internal consistency. Turkish validation of JSE was provided.
Discussion
There was a direct relationship between empathy levels of intensive care nurses and donor declarations and organ finding. Therefore, it can be assumed that a preference for nurses with a high level of empathy to work in intensive care units would be effective in increasing organ donations. Alternatively, empathy increasing trainings during in-service trainings and seminars for intensive care nurses may increase organ donation and thus provide hope for patients awaiting organ donations.
Introduction
Transplantation is a life-saving treatment option for patients suffering from end stage organ failure. Insufficiency of donor organ quantity with respect to the number of patients waiting for transplantation is one of the major factors restricting the success of transplantation [Citation1,Citation2]. Therefore, optimal management of potential donors in intensive care units gains importance.
This study is based on the basic concepts of empathy, empathy in medicine and the importance of finding donors. First, it would be useful to explain these concepts due to their importance in the study. Although different definitions of empathy have been given, in general terms, it is usually considered to be the ability to understand instinctively how others feel or think. Empathy can be expressed as showing basic feelings such as joy, sadness or anxiety [Citation3]. Empathy is the process of looking at events from another person’s point of view by putting oneself in their place and so understanding correctly the feelings and thoughts of the person and communicating this situation. The importance of empathy is felt much more in professions closely associated with people, such as nursing. Nurses can be affected negatively since they meet suffering people every day, and emotional fatigue can occur, whereas it is known that empathic attitudes both contribute to improvement of patient care results and increase the job satisfaction of health care providers [Citation4]. Additionally, while empathy decreases malpractice, it also increases patient satisfaction by participation and adaptation of the patient to the treatment [Citation5]. Empathy is necessary in all cases where therapeutic communication is needed [Citation4]. Thus, the empathy level of nurses as health care providers is expected to be high.
Cerebral death is the permanent loss of cerebral and brainstem functions [Citation6]. Intra-family communication is one of the most important skills in which all health care providers play a role throughout the whole process of organ transplantation, beginning from the predetermination of brain death and continuing after organ transplantation would be needed and implemented [Citation7,Citation8]. Therefore, it must be expected that all health care workers having a role in any of these steps should exert effort to improve themselves so that they can achieve this skill and empathy level.
The relationship of intensive care nurses with the relatives of donors during their stay in intensive care units is very important for donation decisions. Moreover, the length of stay of the case in the intensive care unit, the reason for going into intensive care, brain death, and the family’s day by day acknowledgement of the patient’s status is important [Citation7,Citation9–11]. The fact that the health care worker interviewing the family shows empathy towards the family and puts himself in the position of the family members facilitates his adoption of an appropriate approach during the family interview [Citation12]. The health system, previous experiences, beliefs, traditions, the intensive care process, opinions about organ donation, comprehension of brain death, and communication with the health team and the media can be listed among factors affecting the organ donation decision of families.
From this point forth, the subject of our study is to analyze the role of empathy levels of intensive care nurses on increasing organ donation from a cadaver. In other words, our aim is to find the answer to the question: is a high level of empathy of intensive care nurses effective in increasing organ donation?
Methods
This study was performed with nurses who had been working in intensive care units for at least 1 year in 17 hospitals in 8 provinces in Turkey. Ethics committee approval for the study was obtained from the local ethics committee. The study was performed in accordance with the Helsinki declaration. Communication with the nurses was established via the Bursa Organ Transplantation Center. Questionnaire forms were sent to the nurses by email, and completed forms from those who accepted to participate in the study were also received by email. While the number of nurses working in intensive care units in related hospitals during the study time was 432, the researcher received 355 completed forms. The response rate was calculated as 82%.
The sociodemographic data form prepared for the study included questions about nurses’ gender, age, professional experience, time of work in the intensive care unit and number of shifts per month. Additionally, they were also asked how many brain deaths occurred during their shifts and how many of these were accepted to be a donor from the cadaver. Similarly, the number of brain deaths occurring in 1 year in the hospitals where the nurses worked and the number of donors among them were also evaluated.
The Jefferson Scale of Empathy (JSE) health professionals’ version was used to evaluate the empathy status of the nurses. The Turkish translation of the Jefferson Scale of Empathy was copyrighted by Jefferson University.
The Jefferson Scale of Empathy consists of 20 questions. The scale consists of three sub-parts and its evaluation is done using the total score.
Statistical analysis
Compatibility of variables to normal distribution was analyzed with Shapiro Wilk test. The total empathy score, in case of compatibility to normal distribution, was expressed with mean, standard deviation, minimum and maximum values, and in case of incompatibility it was expressed with median, minimum and maximum values with the donor declaration variable. Reliability of the JSE was evaluated using item-total correlation and Cronbach’s alpha coefficient. Confirmatory-Factor Analysis was used to evaluate whether or not the Turkish adaptation of the scale validated the factor structure of the original JSE. χ2, χ2/υ, “Root Mean Square Error Approximation (RMSEA)”, Tucker-Lewis Index (TLI) and “Comparative Fit Index” (CFI) values were reported as model goodness of fit criteria. The relationships between total empathy score, donor declaration, age, and years in the profession and shift variables were analyzed with correlation analysis and Spearman correlation coefficient was calculated. Comparisons of total empathy score and donor declaration number among the groups were done using Independent samples t test, Mann Whitney U test and Kruskal Wallis test. Analyses were made with Amos (Arbuckle, 2014). Amos (Version 23.0) [Computer Program]. Chicago: IBM SPSS.) and SPSS (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.) and significance level was taken as α = 0.05.
Results
Item analysis and reliability
Internal consistency of the JSE was analyzed using total item score correlation and Cronbach’s alpha coefficient and the results are given in . Cronbach’s alpha coefficient of the JSE in general was α = 0.71. When Cronbach’s alpha coefficient is considered, it is seen that the JSE is an acceptable tool of measurement in terms of internal consistency. When reliability coefficients of subscales were analyzed, the results were: Cronbach’s alpha value for perspective taking sub-scale α = 0.77, for compassionate subscale α = 0.54 and for standing in the patient’s shoes α = 0.66. Questions 1, 3, 6, 7, 8, 11, 12, 14, 18, and 19 were inversely scored in the JSE scoring algorithm and in our study the answers to the related questions were recoded and total and sub-scale scores were calculated using the converted scores of the related questions. Correlation based item analysis was done in order to determine the representation power of the scale items. When item – total score correlations of the JSE were analyzed, the relation between the answer given to question 1 and the total scale score could not be determined (rs = 0.09; p = .091). It was found that the correlation coefficients of the relations between the total scale score and the scores of the remaining 19 questions of the scale varied between rs = 0.24 – 0.58 and that it was statistically significant (p < .001). When the relations between each subscale score and JSE total scores were analyzed, it was seen that correlation coefficients ranged from rs = 0.44 to 0.73 and this was statistically significant (p < .001) ().
Table 1. Reliability levels of JSE subscales and relationships between scales and mean score values of scales.
The Cronbach’s alpha value was α = 0.77 for the perspective taking subscale, α = 0.54 for the compassionate subscale and α = 0.66 for standing in the patient’s shoes. It was detected that sub-scales of the JSE were associated with each other.
Validity of the scale
Confirmatory factor analysis (CFA) was used to analyze the structural validity of the scale and to evaluate the three-factor model of the original JSE, and goodness of fit criteria were calculated. Byrne [Citation13] indicated that confirmatory factor analysis was applied to test if previously discovered and less factor structured scales were similar with the sample of this research. Twenty items from the Turkish scale and three factor structure were tested with Confirmatory Factor Analysis (CFA). These three structures were “perspective taking”, compassionate care” and “standing in the patient’s shoes” in the study of Hojat et al. and it was attempted to validate the Turkish compatibility of the three structures with CFA. It was seen that confirmatory factor analysis results supported the three structures determined by Hojat et al when goodness of fit criteria were considered. In this study, as goodness of fit criteria, χ2 test statistics were detected as 355.62, υ value as 164, χ2/υ value as 2.17, “Root Mean Square Error Approximation (RMSEA)” value as 0.057, Tucker-Lewis Index (TLI) as 0.801 and “Comparative Fit Index” (CFI) as 0.828. One of the evaluation criteria of the model fit is χ2/υ criteria and values 2 and 3 for this rate show respectively “good” and “acceptable” model fits [Citation13]. While RMSEA values equal to or less than 0.05 are accepted as a good fit, values between 0.05 and 0.08 show an adequate fit, values between 0.08 and 0.10 show a medium fit and values higher than 0.10 show an unacceptable fit [Citation14]. When all these fitting indices are evaluated as a whole it can be said that the three factor structure of the Turkish form determined with explanatory factor analysis is validated with DFA (). The three-factor structure with which the goodness of fit was examined with confirmatory factor analysis in our study is given in . Distributions, percentiles, and descriptive statistics for scores on the Jefferson Scale of Empathy is given in . And, general charactercteristics of the participants are given in .
Figure 1. CFA results of JSE.
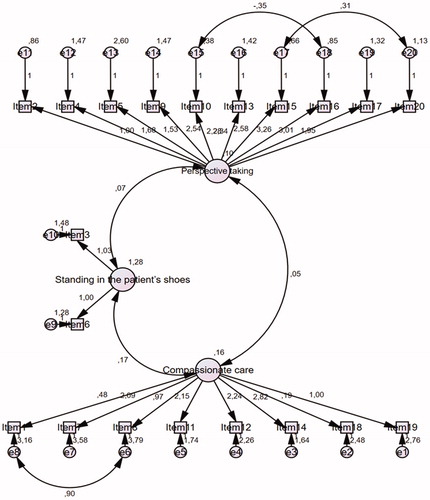
Table 2. Model fit criteria for three factor model of JSE.
Table 3. Scores on the Jefferson empathy scale.
Table 4. General characteristics of the participants.
The relationship between empathy and general charactersitics of the participants are given in .
Table 5. Empathy and the general characteristics of the participants.
We found a positive significant relationship between donor declaration and empathy score. An increase was observed in empathy score as donor declaration increased.
Mean empathy score of females was higher than that of males.
There were differences between hospitals in terms of empathy score. In the sub-group analysis made to determine the hospital(s) causing the difference, the following results were achieved:
Empathy score level of hospital number 12 was lower than hospitals 1, 15, 10, 5, 2, 16, 11, 8, 14, 6, 7 and 9 (respectively, p = .022, p = .014, p = .001, p = .009, p = .004, p = .017, p < .001, p = .030, p = .011, p = .030, p = .003, and p = .006).
Empathy score level of hospital number 17 was lower than hospitals 1, 15, 10, 5, 2, 16, 11, 14 and 9 (respectively, p = .049, p = .031, p = .002, p = .019, p = .009, p = .039, p = .002, p = .006 and p = .012).
Empathy score level of hospital number 3 was lower than hospitals 10, 5, 11, 7 and 9 (respectively, p = .010, p = .046, p = .009, p = .030 and p = .048).
Empathy score level of hospital number 13 was lower than hospitals 10 and 11 (respectively, p = .020 and p = .019).
Factors determining donor declaration are presented in .
Table 6. Relationship between donor declaration and age, gender, professional experience and number of shift.
In our study, a significant relation in the same direction was obtained between total empathy score and donor finding rate (rs =.12; p = .049). An increase in empathy score caused the donor finding rate to increase. Similarly, a decrease in total empathy score caused the donor finding rate to decrease.
There was no relationship between donor declaration and age, professional experience or shift number.
Donor declaration did not vary according to gender.
Discussion
The Cronbach’s alpha coefficient of the JSE in general was α = .71. When the Cronbach’s alpha coefficient is considered, it is seen that the JSE is an acceptable tool of measurement in terms of internal consistency. At the same time, Turkish validation of the JSE was also provided. It was determined that there was a positive significant relationship between donor declaration and empathy score. There was no relationship between donor declaration and age, professional experience or shift number.
In this study that examined the relationship between empathy levels of intensive care unit nurses and obtaining an organ from a cadaver, the JSE mean of the participants was 98.97 ± 12.40. When the highest score of the scale is considered as 140, it can be said that the empathy level was at ‘medium’.
The Jefferson Scale of Empathy was developed by Hojat et al. [Citation15] in 2001 in order to determine the empathy levels of physicians, and subsequently the Turkish adaptation was made. JSE internal consistency was at an acceptable level and the validity of its Turkish form was confirmed.
A positive relationship was found in our study between the empathy scores of intensive care nurses and donor declaration numbers. The fact that the donor declaration increased as empathy score increased is promising in terms of healing of patients waiting for organs since more organs can be found by employing nurses with a high level of empathy in intensive care units.
Empathy score averages showed significant differences among the hospitals. Our study was performed with intensive care nurses in 17 hospitals in 8 provinces in Turkey. Donor declaration rates were high in the hospitals in which empathy score averages were also high.
The mean empathy score of the females was higher than that of the males. Also, in studies run with nursing students, it was shown that empathy score averages of female students were higher than male students [Citation16–18]. No theory was encountered in the literature completely explaining the effect of gender on empathy. However, the effect of gender on empathy can originate from the emotional structure of women or socio-cultural features of the countries where the research studies were run. On the other hand, there are also some studies showing that empathy level does not change according to gender [Citation19,20]. No correlation was detected between the age of the nurses and empathy score averages. Studies also show that age does not have any effect on empathy [Citation16,19,21]. In this context, the result of this study is compatible with the literature.
Donor declaration is not associated with age, gender, professional experience or monthly shift number. There was a significant relationship in the same direction only between total empathy score and donor finding. As our study is the first research study performed in terms of determining the relationship between empathy levels of intensive care unit nurses and their success in finding organs, it was impossible to compare its results with similar studies. However, the effect of the attitudes and behaviors of health professionals on the treatment success in cancer and chronic kidney patients has been shown in many studies [Citation22–24].
Strength and limitations
Our study was limited within Turkey and comprised intensive care unit nurses in 17 hospitals in 8 provinces. When the number of intensive care nurses in Turkey is considered, it is likely to be able to generalize this as a sample.
However, this study was on a national level. It would be possible to achieve different results in different countries due to cultural differences. Thus, it would be useful to run similar studies in different countries on different samples through cooperation.
Additionally, besides nurses, the presence of intensive care physicians and organ transplantation coordinators during the interview with the relatives of the donor at the time of brain death may also affect the donation rate. Evaluation of empathy levels of only nurses can be considered as a limitation of the study.
Conclusions
This study revealed that there was a direct relationship between empathy levels of intensive care nurses and donor declarations and organ finding. Therefore, it can be assumed that a preference for nurses with a high level of empathy to work in intensive care units would be effective in increasing organ donations. Alternatively, empathy increasing trainings during in-service trainings and seminars for intensive care nurses may increase organ donation and thus provide hope for patients awaiting organ donations.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Ojo AO, Heinrichs D, Emond JC, et al. Organ donation and utilization in the USA. Am J Transplant. 2004; 4(Suppl 9):27–37.
- Dare AJ, Bartlett AS, Fraser JF. Critical care of the potential organ donor. Curr Neurol Neurosci Rep. 2012;12:456–465.
- Peterson P, Baker E, McGaw B. International encyclopedia of education. 3rd ed. Oxford: Elsevier; 2010.
- Stephany K. Cultivating empathy: inspiring health professionals to communicate more effectively. Sharjah: Bentham Science Publishers; 2014.
- Hojat M. Empathy in patient care. New York: Springer; 2010.
- Wijdicks EF. The diagnosis of brain death. N Engl J Med. 2001;344:1215–1221.
- Villar CR. Family approach for organ donation. In Valero R, editor. Transplant coordination manual: the new vital cycle. Barcelona; 2007. p. 135–152.
- Santiago C. Family and personal consent to donation. Transplant Proc. 1997; 29:1625–1628.
- Coyle MA. Meeting the needs of the family: the role of the specialist nurse in the management of brain death. Intensive Crit Care Nurs. 2000;16:45–50.
- Meyer K, Bjork IT, Eide H. Intensive care nurses' perceptions of their professional competence in the organ donor process: a national survey. J Adv Nurs. 2012;68:104–115.
- Tamburri LM. The role of critical care nurses in the organ donation breakthrough collaborative. Crit Care Nurse. 2006;26:20, 22, 24.
- Siminoff LA, Gordon N, Hewlett J, et al. Factors influencing families' consent for donation of solid organs for transplantation. JAMA 2001;286:71–77.
- Byrne BM. Structural equation modeling with LISREL, PRELIS and SIMPLIS: basic, concept, applications and programming. New Jersey: Lawrence; 1998.
- Schermelleh-Engel K, Moosbrugger H, Müller H. Evaluating the fit of structural equation models: tests of significance and descriptive goodness-of-fit measures. Methods Psychol Res. 2003;8:23–74.
- Hojat M, Mangione S, Nasca TJ, et al. The Jefferson scale of physician empathy: development and preliminary psychometric data. Educ Psychol Meas. 2001;61:349–365.
- Petrucci C, Cerra CL, Aloisio F, et al. Empathy in healthprofessional students: a comparative cross-sectional study. Nurs Educ Today. 2016;41:1–5.
- Brown T, Boyle M, Williams B, et al. Predictors of empathy in health science students. J Allied Health. 2011;40:143–149.
- Magalhães E, Salgueira AP, Costa P, et al. Empathy in senior year and first year medical students: a cross-sectional study. BMC Med Educ 2011;11:1–7.
- McKenna L, Boyle M, Brown T, et al. Levels of empathy in undergraduate nursing students. Int J Nurs Pract. 2012;18:246–251.
- Yucel H, Acar G. Levels of empathy among undergraduate physiotherapy students: a cross-sectional study at two universities in Istanbul. Pak J Med Sci. 2016;32:85–90.
- Williams B, Boyle M, Earl T. Measurement of empathy levels in undergraduate paramedic students. Prehosp Disaster Med. 2013;28:145–149.
- Munikrishnappa D. Chronic kidney disease (CKD) in the elderly – a geriatrician's perspective. Aging Male. 2007;10:113–137.
- Naccarato AM, Reis LO, Matheus WE, et al. Barriers to prostate cancer screening: psychological aspects and descriptive variables – is there a correlation? Aging Male. 2011;14:66–71.
- Kuzmarov IW, Ferrante A. The development of anti-cancer programs in Canada for the geriatric population: an integrated nursing and medical approach. Aging Male. 2011;14:4–9.