
Abstract
Objective
The aim of this study was to clarify the actual status of male climacteric symptoms in rotating night shift workers and how to cope with the symptoms.
Methods
We planned a self-administered questionnaire survey in male rotating night shift workers. Male climacteric symptoms were evaluated by using the Aging Males’ Symptoms (AMS) scale.
Results
Of 1891 questionnaires that were sent, 1561 were collected. There were significant differences in total AMS scores among the age groups. In all age groups, there were high proportions of men with increased need for sleep and often feeling tired (64.9%) and decrease in muscular strength (60.7%). There were significant differences in AMS scores for somatic symptoms between men in their 20 s and those in their 40 s or 50 s and between men in their 30 s and those in their 50 s and in AMS scores for sexual symptoms between men in their 20 s and those in their 30 s, 40 s, 50 s or 60 s, between men in their 30 s and those in their 40 s, 50 s or 60 s and between men in their 40 s and those in their 50 s or 60 s.
Conclusion
Significant age-dependent differences are found in somatic symptoms and sexual symptoms in rotating night shift workers.
Introduction
Late-onset hypogonadism (LOH) syndrome, which causes various symptoms due to a decrease in androgen, is generally called male climacteric symptoms. Recently, LOH syndrome has received much attention worldwide [Citation1]. The onset and duration of LOH syndrome differ greatly among individuals. Various symptoms in LOH syndrome have been classified as somatic symptoms such as general fatigue, psychological symptoms such as decrease in vitality, and sexual symptoms such as decrease in libido. LOH syndrome has been extensively evaluated by using the Aging Males’ Symptoms (AMS) scale. Among 499 men aged from 40 to 90 years who visited a hospital in Indonesia, 54.5% had mild, 39.0% had moderate and 6.5% had severe AMS levels [Citation2]. The effects of hormone treatment in 261 patients with LOH syndrome were investigated by using AMS scale in Germany [Citation3]. Among 103 Iranian men aged 40–76 years, 73.6% of the men experienced symptoms of andropause and the proportions of men who had mild, moderate and severe AMS scores were 38.6%, 27.1% and 7.9%, respectively [Citation4]. In Japan, the actual status of male climacteric symptoms has been examined after medical examinations and treatment for male climacteric symptoms were started in 2000. Ichioka et al. [Citation5] also reported that the proportions of men with a mild AMS score were 42.9% in men in their 30 s, 51.2% in men in their 40 s, 61.7% in men in their 50 s and 72.6% in men in their 60 s among 206 healthy men.
In terms of occupational health, it is important to consider physical health and mental health of workers, particularly night shift workers. Accordance to the United States Bureau of Labor Statistics in 2004, 14.8% of the labor force was shift workers and 70% of the shift workers were night shift workers [Citation6]. According to the Japanese Ministry of Health, Labor and Welfare, the proportion of night shift workers in 2005 was 34.1% (manufacturing: 25.2%), and it increased to 36% in 2010 (manufacturing: 30.4%) in companies in which the number of employees was more than 10 [Citation7]. It has been reported that night shift work was associated with various health problems including cardiovascular diseases, gastrointestinal disturbances and metabolic syndrome [Citation8–12]. Kaneko et al. [Citation13] reported that the proportion of male workers with a depressive state was higher in double shift workers than in day shift workers. Male climacteric symptoms might occur due to androgen deficiency in rotating night shift workers who have mental health disturbances. Physical and psychological management is necessary for shift workers. From the viewpoint of industrial health, Horie [Citation14] reported that the quality of life will decrease for men with LOH syndrome who do not receive treatment. Since the proportion of rotating night shift workers has been increasing, it is important for such workers to voluntarily visit a hospital for examination and treatment of LOH syndrome. However, the actual status of male climacteric symptoms in rotating night shift workers and how the workers cope with the symptoms have not been reported.
The aim of this study was to clarify the actual status of male climacteric symptoms in rotating night shift workers and to determine the relationship between symptoms and age.
Subjects and methods
We planned an unsigned self-administered questionnaire survey in male rotating night shift workers over the age of 20 years, including those working all or some of the hours from 10 pm to 5 am, in manufacturing companies. We asked the managers of general affairs or occupational nurses in 33 companies and distributed the questionnaires to 1891 male rotating night shift workers throughout Japan during the period from March to May in 2017. The questionnaires were collected from collection boxes or by mail.
The demographic characteristics in the questionnaire were age, work experience, length of service in shift work, type of shift, lifestyle (diet, physical activity, smoking habit, alcohol consumption, sleeping status, ways of spending free time), degree of stress, recognition of andropause and awareness of male climacteric symptoms, and coping strategy. Male climacteric symptoms were evaluated by using the AMS scale. The AMS questionnaire, which is a self-administered questionnaire that was developed in Germany, has been used worldwide for assessing male climacteric symptoms [Citation4,Citation15–17]. The questionnaire consists of 17 items including seven items for somatic symptoms, five items for psychological symptoms and five items for sexual symptoms. The AMS scale is a self-rated scale of the degrees of symptoms and each answer is rated with a 5-point Likert-type scale ranging from 1 (none) to 5 (very severe). A total score of less than 26 and less indicates no symptoms, a total score of more than 27 and less than 36 indicates mild symptoms, a total score of more than 37 and less than 49 indicates moderate symptoms, and a total score of 50 or higher indicates severe male climacteric symptoms [Citation15–16]. AMS was translated into Japanese and its reliability has been verified for validity [Citation17].
Statistical analysis
Baseline characteristics were analyzed by descriptive statistics. We classified male climacteric symptoms into four groups according to the degree of symptoms (none, mild, moderate, severe) and performed analysis for five generations (20 s, 30 s, 40 s, 50 s and 60 s). We used the chi-square test for comparing the proportions of subjects with each symptom among the age groups. Assuming that AMS score does not follow the normal distribution, we compared AMS scores among the age groups by using the Kruskal–Wallis test. The Bonferroni test was used for comparison of each pair of variables with a significant difference as a post hoc test. p values less than 0.05 were considered to be statistically significant. All statistical analyses were conducted using SPSS statistics ver.25 (IBM Corp.).
Ethical consideration
This study was approved by the Research Ethics Committee of Tokushima University Hospital (approval number 2745). We firstly distributed an explanation sheet and a consent form to the manager in the company, and we received written informed consent after explanation regarding the study. After that, we recruited participants through the general affairs division in the company and health care center. The subjects were only men who agreed to participate after explanation by using the explanation sheet through the manager in the company. The explanation sheet included an explanation about the respect for autonomy and anonymization of personal data.
Results
Of the total of 1891 questionnaires that were sent, 1561 were collected (response rate of 82.5%). We excluded 26 participants who were under 20 years of age, 11 participants who were fixed night shift workers and 24 participants for whom ages were not known, and we analyzed data for 1500 rotating night shift workers. As can be seen in , the proportion of rotating night shift workers whose occupational duration was less than 10 years was 38.0%, which was the highest proportion, and 74% of the shift workers worked three shifts. Most of the participants (86.7%) were full-time workers.
Table 1. Baseline characteristics.
We showed the proportion of men who reported any symptoms regardless of degrees in . There were high proportions in all age groups for the following symptoms: increased need for sleep and often feeling tired, decrease in muscular strength and physical exhaustion/lacking vitality. In men in their 20 s and 30 s, there were high proportions of men with increased need for sleep and often feeling tired and irritability.
Table 2. Proportion of AMS symptoms according to age.
The proportions of men with somatic symptoms such as decrease in muscular strength, joint and muscular pain and physical exhaustion/lacking vitality prominently increased with advance of age. The proportion of men with decrease in sexual function also increased with advance of age. On the other hand, the proportion of men with symptoms such as increased need for sleep, often feeling tired, irritability and depressive mood were high in the younger age groups as well as the older age groups.
As can be seen in , the median (25–75 percentiles) total AMS score in all of the men was 26 (21–35). The median total AMS scores were 23 in men in their 20 s, 25 in men in their 30 s, 28 in men in their 40 s, 30 in men in their 50 s and 29 in men in their 60 s. There were significant differences in total AMS scores among the age groups (p < 0.001). Significant differences in AMS score were found between men in their 20 s and those in their 40 s or those in their 50 s or those in their 60 s (p < 0.001). There were also significant differences between men in their 30 s and those in their 50 s (p = 0.001) and between men in their 30 s and those in their 60 s (p = 0.035). As can be seen in , the proportions of men with mild, moderate and severe symptoms increased in all ages with advance of age until 60 years.
Figure 1. Total AMS scores according to age. The bottom line, middle line and top line of box-and-whisker plot indicate 25 percentile, median, and 75 percentile, respectively. Crosses show the mean values. *20s vs 40s or 50s or 60s (p < 0.001), **30s vs 50s (p = 0.001) ***30s vs 60s (p = 0.035).
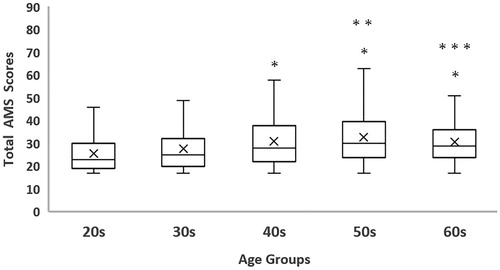
Table 3. Degrees of symptoms according to age.
We categorized the items of AMS into somatic symptoms, psychological symptoms and sexual symptoms, and we compared AMS scores among the age groups (). There were significant differences in AMS scores for somatic symptoms between men in their 20 s and those in their 40 s or 50 s (p < 0.001), between men in their 30 s and those in their 40 s (p = 0.002) and between men in their 30 s and those in their 50 s (p < 0.001). We found no significant difference in the AMS scores for psychological symptoms among the age groups. There were significant differences in AMS scores for sexual symptom between men in their 20 s and those in their 30 s, 40 s, 50 s or 60 s (p < 0.001), between men in their 30 s and those in their 40 s or 50 s or 60 s (p < 0.001) and between men in their 40 s and those in their 50 s or 60 s (p < 0.001).
Table 4. Psychological symptoms, somatic symptoms and sexual symptoms in AMS according to age.
Discussion
The proportions of rotating night shift workers who complained of increased need for sleep and often feeling tired were more than 60% in all age groups. We found that the proportions of men with somatic symptoms such as decrease in muscular strength and joint and muscular pain and the proportions of with sexual symptoms increased with advance of age excluding 60 s. The median AMS scores ranged from 23 to 30, and the score increased with advance of age. Significant differences in AMS scores for somatic symptoms and sexual symptoms were found among the age groups, but a significant difference in the AMS scores for psychological symptoms was not found among the age groups. In 969 men aged 40–80 years in China, somatic and sexual subscores showed significant differences among different age groups [Citation18]. The results of our study for shift workers are consistent with the results of that study.
Symptoms with high frequencies in all workers were increased need for sleep and often feeling tired, suggesting that these symptoms are common male rotating night shift workers. Symptoms with high frequencies in men in their 20 s and 30 s included increased need for sleep, often feeling tired and irritability. The proportion of male respondents who felt that they could not get any rest or could not get sufficient rest from sleeping were 23.2% in men in their 20 s, 27.6% in men in their 30 s, 30.9% in men in their 40 s, 28.4% in men in their 50 s and 15.0% in men in their 60 s in the National Health and Nutrition Examination Survey in 2017 in Japan [Citation19]. Night shift workers in their 20 s, 30 s, and 40 s are likely to need more sleep than other ordinary men. The problem of insufficient sleep that was a complaint made by high proportions of the participants in all age groups may be a common problem for rotating night shift workers, whose lifestyle is not in tune with circadian rhythm. Circadian rhythm has been shown to be disturbed in night shift workers [Citation20]. Previous study showed that melatonin level related to circadian rhythm was associated with levels of reproductive hormones including androgen [Citation21]. Androgen level may be influenced by rotating night shift work [Citation21].
We showed that the proportions of men who had mild, moderate or severe male climacteric symptoms according to AMS scores were 42.0% in men in their 30 s, 53.3% in men in their 40 s and 62.8% in men in their 50 s. The result was similar to the result among men who underwent health examinations in the previous study [Citation6]. Also, we showed that there were significant differences in total AMS scores between men in their 20 s and those in their 40 s or 50 s and between men in their 30 s and those in their 40 s or 50 s. Kobayashi et al.[Citation22] reported that mean total AMS scores were 33.9 in 155 healthy men (mean age, 55.5 years) who received medical checkups and 52.1 in 116 outpatients (mean age, 53.2 years) who complained of male climacteric symptoms at a urology department. Thus, the total AMS score in the present study was similar to that in healthy men in the previous study [Citation22].
The results obtained from AMS scores according to the AMS cluster differed from the results obtained from total AMS score. We showed that the proportions of men with decrease in muscular strength and with joint and muscular pain were high in men in their 50 s and 60 s. The proportions of men in their 30 s with decrease in muscular strength and with joint and muscle pain were 1.6–1.8 times higher than the proportions of men in their 20 s, and that proportions gradually increased until 50 s. In addition, there were significant differences in somatic AMS scores between men in their 30 s and those in their 40 s and between men in their 30 s and those in their 50 s, suggesting that there is a difference in each decade of life in that age range. For somatic symptoms, there were marked differences in the decrease in muscular strength among the age groups. The increase in the proportion of men with decrease in muscular strength may be due to testosterone deficiency with advance of age. Kobayashi et al. [Citation22] reported that the mean somatic AMS scores were 8.4 in men who received medical examinations and 14.8 in men with male climacteric symptoms in men in their 50 s in the present study, were similar to the values in men with male climacteric symptoms in that previous study. Rotating night shift workers may have somatic symptoms that are same as those in men with male climacteric symptoms. Testosterone has roles for increasing muscle strength and maintaining sexual function. Decreased testosterone level might be associated with decrease in muscular strength in night shift workers. Recently, sarcopenia in older adults has been focused on as one of the geriatric syndromes, and the importance of bioelectrical impedance analysis for assessment of muscle mass was suggested [Citation23]. Measurement of muscle mass may be needed for rotating night shift workers in a company.
Muscle power of the trunk in rotating night shift workers who are working in the manufacturing industry may be maintained since they stand for long hours and have the same posture in a sitting position, but they may feel a decrease in muscle power in other sites of the body. Asbitt et al. [Citation24] reported that metabolic disturbance in muscles caused by irregular working hours resulted in a decrease in muscle strength.
The proportion of men in the present study who reported sexual symptoms was small, but the proportion increased with advance of age. In addition, there were significant differences in AMS scores for sexual symptoms between men in their 30 s and those in their 40 s and between men in their 40 s and those in their 50 s. Kobayashi et al. [Citation22] reported that mean sexual AMS scores were 12.9 in men who received medical examinations and 15.6 in men with male climacteric symptoms. The mean AMS score for sexual symptom in the present study was 7.5, and this level was lower than that in the previous study [Citation22]. Haider et al. [Citation25] reported that AMS scores decreased in a testosterone-treated group, suggesting that testosterone therapy is effective for improvement of sexual function and quality of life. In addition, Rao et al. [Citation26] reported that treatment with Trigonella foenum-graecum seed extract improved sexual function in middle-aged and older men. Medical treatment should be considered for night shift workers with sexual symptoms.
There were no significant differences among the age groups in psychological symptoms. Notably, there was no significant difference in the mean level of irritability among the age groups. High proportion of men with irritability were found in their 20 s and 30 s. According to Comprehensive Survey of Living Conditions, the proportions of men who had trouble and stress in daily life were 43.6% in men in their 20 s, 48.0% in men in their 30 s, 48.6% in men in their 40 s, 48.6% in men in their 50 s and 38.5% in men in their 60 s [Citation27]. The results showing that the proportion of men with stress was increased in men in their 20 s and 30 s and that there were high proportions of men in the 40 s and 50 s with stress were similar to the results in general men. We could not clarify whether irritability in men in their 20 s and 30 s was due to androgen deficiency or due to job-related stress or stress caused by personal life. Trinick et al. [Citation28] suggested that increase in psychological stress related to occupation may be associated with occurrence of LOH syndrome based on the results in a Web survey by using AMS in 10,896 respondents aged 16–89 years in the USA and in England. Kobayashi et al. reported that mean psychological AMS scores were 13.9 in men who received medical checkups and 22.3 in men with male climacteric symptoms [Citation22]. The mean psychological AMS score, which was 8.3 in the present study, was lower than that in men who received medical checkups and men with male climacteric symptoms in the previous study. The fact that a large number of participants did not give an answer regarding the symptom of feeling burnt out or having hit rock-bottom might have affected the AMS score.
It has been suggested that various factors such as change in the social environment and psychological factors are involved in the occurrence of male climacteric symptoms [Citation29]. Also, it has been reported that visiting a hospital at an early stage of symptoms and appropriate treatment can improve quality of life [Citation30]. Since the publication of a clinical practice manual for LOH syndrome by the Japanese Urological Association in 2007 [Citation31], male climacteric symptoms have been recognized among medical workers. However, unlike the recognition of female climacteric symptoms, the recognition of male climacteric symptoms in the general population is still poor. Therefore, sufficient efforts are not made to visit a hospital or improve lifestyle habits. It has been reported that the proportion of men who complain of male climacteric symptoms has been increasing with increasing recognition of LOH symptoms and male climacteric symptoms [Citation32]. Medical examinations and educational activities in the workplace are needed since most young to middle-aged men are working.
Since night shift work has harsh working conditions that disturb circadian rhythm, LOH syndrome might occur more frequently in young rotating night shift workers than in young daytime workers. An organization strategy of mental health for rotating night shift workers is needed to prevent LOH syndrome and detect LOH syndrome at an early stage. It has been reported that the degree of awareness of andropause in men over 40 years of age was very low, though they had experienced symptoms of andropause [Citation4]. Occupational health nurses should make a proposal to include an AMS questionnaire in medical checkups and they should recommend employees who have a high AMS score to visit a hospital. Moreover, occupational physicians and occupational health nurses should play important roles for providing information regarding male climacteric symptoms and education for employees regarding knowledge of LOH at a safety and health committee. However, since many small- to medium-sized companies in Japan do not have occupational physicians and nurses, cooperation with health officers and health insurance societies may be necessary. It has been reported that symptoms will get worse if men with LOH syndrome do not receive appropriate treatment [Citation29]. If shift workers recognize their symptoms as male climacteric symptoms and visit a hospital, a beneficial economic effect can be expected due to a reduction in absenteeism and increase in productivity through somatic and psychological health promotion. Assessment by using AMS scores is widely used in various countries as screening for LOH syndrome. Measurement of free testosterone level is necessary for men with high AMS scores [Citation33,Citation34].
The strength of this study is the large sample size. There was no previous study with a sample size as large as that in our study. Previous studies have been conducted using the AMS scale for daytime workers but not for rotating night shift workers. However, this study also has several limitations. First, a causal relationship was not clarified since this study was a cross-sectional design. Secondly, no significant difference was observed between men in their 50 s and those in their 60 s since the number of men in their 60 s was small and the age of men in their 60 s was less than 63 years. The results of our study might be different from the results for men in their 60 s in a previous study [Citation6]. Also, the number of men who do not answer questions regarding sexual symptoms is much that might influence the AMS score. Further study may be needed with large numbers of men in their 50 s and 60 s, who are more likely to have male climacteric symptoms. The generalizability of the obtained results is inconclusive for all shift workers since there are various types of shift work. Questionnaires regarding LOH syndrome have been developed in various countries and their validity and reliability have been examined [Citation33,Citation35–37]. Horie et al. [Citation38] also reported that sexual perceptions were different in Japanese and Caucasian populations. An appropriate questionnaire for each country should be considered.
In conclusion, we found significant age-dependent differences in somatic symptoms and sexual symptoms in rotating night shift workers. More than 60% of the participants reported increased need for sleep and often feeling tired in all age groups. The prevalence of somatic symptoms and sexual symptoms remarkably increased with advance of age. However, the prevalence of psychological symptoms was high in the younger age groups as well as older age groups.
Acknowledgements
The authors would like to show our greatest appreciation to participants, managers of general affairs and occupational nurses. We are also grateful for assistance given by Professor Iwamoto.
Disclosure statement
The authors declare there is no conflicts of interest.
Additional information
Funding
Notes on contributors
Sachiko Kubo
Sachiko Kubo joined Shikoku-University as an Assistant Professor in 2014. She obtained her master`s degree of Nursing Science from Tokushima University Graduate School of Health Sciences in 2013. Her research field is occupational health and adult nursing.
Toshiyuki Yasui
Toshiyuki Yasui is M.D., Ph.D., Professor of Reproductive and Menopause Medicine of Reproductive and Menopause Medicine. In 2019, He was appointed as a dean of Tokushima University Graduate school of Health Sciences. He received his doctorate in Medicine from Tokushima University 1991. His recent research paper includes Different levels of awareness and knowledge of male climacteric in female nurses and female office workers (2015), Associations of endogenous sex hormones and sex hormone-binding globulin with lipid profiles in aged Japanese men and women (2008), Androgen in postmenopausal women (2012). His research field is endocrinology in aging, role of androgen in female, bone and lipid metabolism in postmenopausal medicine, reproductive endocrinology.
Yukie Matsuura
Yukie Matsuura is an Assistant Professor of Health Science at the Tokushima University. She received her master degree in nursing science from Japanese Red Cross College of Nursing (2008). Her research interests cover wide areas of nursing and health care including maternal and child health, adolescent health, menopausal health, elderly health care etc. Her current research is doing on premenstrual symptoms among young females.
Masahito Tomotake
Masahito Tomotake is M.D., Ph.D., Professor of Mental Health at Tokushima University Graduate school of Health Sciences. In 2019. His recent treatise includes Clinical factors influencing resilience in patients with anorexia nervosa (2018), Relationship between social and cognitive functions in people with schizophrenia (2018). He obtained his doctorate in Medicine from Tokushima University in 1997. His field of study is Etiology of mental disorders, evaluation of mental disorders, prevention against mental disorders.
References
- Basaria S. Male hypogonadism. Lancet. 2014;383:1250–1263.
- Taher A. Proportion and acceptance of andropause symptoms among elderly men: a study in Jakarta. Acta Med Indones. 2005;37:82–86.
- Almehmadi Y, Yassin A, Nettleship E, et al. Testosterone replacement therapy improves the health-related quality of life of men diagnosed with late-onset hypogonadism. Arab J Urol. 2016;14:31–36.
- Samipoor F, Pakseresht S, Rezasoltani P, et al. Awareness and experience of andropause symptoms in men referring to health centers: a cross-sectional study in Iran. Aging Male. 2017;20:153–160.
- Ichioka K, Nishiyama H, Yoshimura K, et al. Aging Males’ Symptoms scale in Japanese men attending a multiphasic health screening clinic. Urology. 2006;67:589–593.
- The United States Department of Labor, Economic News Release, The United States Bureau of Labor Statistics: [Internet]. 2004 [cited 2018 Aug 23]. Available from: http://www.mhlw.go.jp/toukei/list/49-22.html
- Labor safety and health survey. 2010. [Internet]. [cited 2018 Aug 2]. 2018. Available from: https://www.bls.gov/news.release/flex.t05.htm
- Segawa K, Nakazawa S, Tsukamoto Y, et al. Peptic ulcer is prevalent among shift workers. Dig Dis Sci. 1987;32:449–453.
- Pietroiusti A, Forlini A, Magrini A, et al. Shift work increases the frequency of duodenal ulcer in H pylori infected workers. Occup Environ Med. 2006;63:773–775.
- Karlsson B, Knutsson A, Lindahl B. Is there an association between shift work and having a metabolic syndrome? Results from a population based study of 27,485 people. Ann Occup Environ Med. 2001;58:747–752.
- Sookoian S, Gemma C, Fernández Gianotti T, et al. Effects of rotating shift work on biomarkers of metabolic syndrome and inflammation. J Intern Med. 2007;261:285–292.
- Karlsson H, Knutsson K, Lindahl O, et al. Metabolic disturbances in male workers with rotating three shift work. Results of the WOLF study. Int J Environ Health Res. 2003;76:424–430.
- Kaneko S, Maeda T, Sasaki S, et al. Effect of shiftwork on mental state of factory workers. Fukushima J Med Sci. 2004;50:1–9.
- Horie S. Symptoms and treatment of andropause. Japan Med Assoc J. 2006;49:382–384.
- Heinemann J, Zimmermann T, Vermeulen A, et al. A new aging male’s symptoms’ (AMS) rating scale. Aging Male. 1999;2:105–114.
- Daig I, Heinemann LA, Kim S, et al. Aging Malesʼ Symptoms (AMS) scale: review of its methodological characteristics. Health Qual Life Outcomes. 2003;1:77.
- Kobayashi K, Hashimoto K, Kato R, et al. The aging males’ symptoms scale for Japanese men: reliability and applicability of the Japanese version. Int J Impot Res. 2008;20:544–548.
- Yu XH, Zhao J, Zhang SC, et al. The impact of age, BMI and sex hormone on aging males’ symptoms and the international index of erectile function scores. Aging Male. 2017;20:235–240.
- Ministry of Health, Labour and Welfare, Summary of National Health and Nutrition Examination Survey. 2017. [Internet]. [cited 2018 Aug 3]. 2018 Available from: https://www.mhlw.go.jp/content/10904750/000351576.pdf
- Khan S, Duan P, Yao L, et al. Shiftwork-mediated disruptions of circadian rhythms and sleep homeostasis cause serious health problems. Int J Genomics. 2018;2018:1–11.
- Rajmil O, Puig-Domingo M, Tortosa F, et al. Melatonin concentration before and during testosterone replacement in primary hypogonadic men. Eur J Endocrinol. 1997;137:48–52.
- Kobayashi K, Kato R, Hashimoto K, et al. Factor analysis of the Japanese version of the Aging Males’ Symptoms rating scale. Hinyokika Kiyo. 2009;55:475–478.
- Yilmaz O, Bahat G. Suggestions for assessment of muscle mass in primary care setting. Aging Male. 2017;20:168–169.
- Aisbett B, Condo D, Zacharewicz E, et al. The impact of shiftwork on skeletal muscle health. Nutrients. 2017;9:248.
- Haider KS, Haider A, Doros G, et al. Long-term testosterone therapy improves urinary and sexual function, and quality of life in men with hypogonadism: results from a propensity matched subgroup of a controlled registry study. J Urol. 2018;199:257–265.
- Rao A, Steels E, Warrick JI, et al. Testofen, a specialised Trigonella foenum-graecum seed extract reduces age-related symptoms of androgen decrease, increases testosterone levels and improves sexual function in healthy aging males in a double-blind randomised clinical study. Aging Male. 2016;19:1–9.
- Summary Report; Comprehensive Survey of Living Conditions 2016. [Internet]. [cited 2018 July 25]. 2018. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa16/
- Trinick TR, Feneley MR, Welford H, et al. International web survey show high prevalence of symptomatic testosterone deficiency in men. Aging male. 2011;14: 10–15.
- Novak A, Brod M, Elbers J. Andropause and quality of life: Findings from patient focus groups and clinical experts. Maturitas. 2002;43:231–237.
- Okada K, Yamaguchi K, Chiba K, et al. Comprehensive evaluation of androgen replacement therapy in aging Japanese men with late-onset hypogonadism. Aging Male. 2014;17:72–75.
- Namiki M, Akaza H, Shimazui T, et al. Working committee on clinical practice guidelines for late-onset hypogonadism. clinical practice manual for late-onset hypogonadism syndrome. the japanese urological association/japanese society for the study of the aging male. Int J Urol. 2008;5:377–388.
- Giltay E, Tishova Y, Mskhalaya G, et al. Effects of testosterone supplementation on depressive symptoms and sexual dysfunction in hypogonadal men with the metabolic syndrome. J Sex Med. 2010;7:2572–2582.
- Cabral RD, Busin L, Rosito TE, et al. Performance of Massachusetts Male Aging Study (MMAS) and androgen deficiency in the aging male (ADAM) questionnaires in the prediction of free testosterone in patients aged 40 years or older treated in outpatient regimen. Aging Male. 2014;17:147–154.
- Kummer KK, Pope HG, Hudson JI, et al. Aging male symptomatology and eating behavior. Aging Male. 2019;22:55–61.
- Chen W, Liu ZY, Wang LH, et al. Are the Aging Male’s Symptoms (AMS) scale and the Androgen Deficiency in the Aging Male (ADAM) questionnaire suitable for the screening of late-onset hypogonadism in aging Chinese men?. Aging Male. 2013;16:92–96.
- Abootalebi M, Kargar M, Aminsharifi A. Assessment of the validity and reliability of a questionnaire on knowledge and attitude of general practitioners about andropause. Aging Male. 2017;20:60–64.
- Yuen JW, Ng CF, Chiu PK, et al. Aging males’ symptoms and general health of adult males: a cross-sectional study. Aging Male. 2016;19:71–78.
- Horie S, Hisasue S-I, Nakao M, et al. Correlation between the Japanese Aging Male Questionnaire (JAMQ) and Aging Male’s Symptom (AMS) scale in Japanese male. Aging Male. 2014;17:35–41.