
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Erectile dysfunction (ED) is a common diabetes-related complication.
Materials and methods
This study examined the effect of daily low-dose tadalafil (5 mg) on patients’ quality of life (including that of sex life) and blood circulation. Erectile dysfunction questionnaires were administered to 20 patients with type 2 diabetes (T2DM) and ED. The safety and efficacy of tadalafil were evaluated using laboratory tests, and the effect on blood circulation was measured through nail fold capillaroscopy.
Results
Daily tadalafil use by patients with T2DM and ED showed a statistically significant increase in the erectile reliability score from of 1.15 to 3.20 (p < .00012). Capillary blood circulation improvement tests showed a statistically significant increase in apical limb width from 13.1 to 14.64 µm (p = .04829) and flow from 9035 to 11946 μm3/s (p = .04405). Although not significant, increased capillary width and speed (rate of blood flow) confirmed improved blood circulation. There were no significant changes in the cardiac indicators (troponin, prostate-specific antigen, or electrocardiogram tests) before and after tadalafil administration, supporting the safety of its low-dose daily administration.
Conclusions
A small dose of daily tadalafil was shown to safely improve erectile dysfunction and peripheral blood flow in patients with T2DM, in which peripheral arterial diseases should not be considered separately but rather as complex entities.
Introduction
It is estimated that there are 537 million people with diabetes worldwide (20–79 years), accounting for approximately one out of five people aged 65 and above; by 2045, these would have increased to 783 million [Citation1]. Due to westernized eating habits, such as the consumption of fast food, diabetes has become a common lifestyle disease with a prevalence of up to 13.7%. Diabetes, a condition with higher-than-normal blood glucose concentration, is caused by many factors, including aging, stress, obesity, and immune system abnormalities. Ninety percent of adult patients with diabetes have type 2 diabetes (T2DM), which can cause microvascular, macrovascular, and other miscellaneous complications (hyperglycemia, nephropathy, and retinopathy) through various mechanisms. In particular, erectile dysfunction (ED) is common in people with diabetes. A study reported that ED (including unstable erection) affects up to 50% of the diabetic population [Citation2]. ED is attributed to different causes and can be of psychogenic (from psychological factors such as stress) and organic (caused by disabilities in the sex organ, blood vessel, endocrine, and nerve) types. Due to the high risk of complications in diabetes, patients often become psychologically anxious, and its complication, ED, also causes a loss of confidence, psychological frustration, and stress [Citation3,Citation4]. Thus, the patients should be cared for with a focus on this aspect as well.
Although diabetes does not decrease sexual desire, neuroinflammation and vascular arteriosclerosis can cause ED. Men with DM are at a significantly higher risk for ED than those without DM. patients with DM had an approximately 3.5-fold higher prevalence of ED than those without DM. Diabetes and erectile dysfunction share the same risk factors [Citation5]. With diabetes, the physical friction caused by increased blood viscosity on the cavernous vessel walls impairs the vessel walls, leading to endothelial dysfunction and decreased oxygen inflow. Oxidative damage causes arteriosclerosis in the vessel walls, further reducing blood flow. During sexual stimulation, the release of neurotransmitters establishes an erection, but in patients with diabetes with damaged nerves, sensitivity is decreased. The erection phenomenon is the release of nitric oxide (NO) from the penile sponges when sexual excitement is achieved.
It begins with NO increases the activity of an enzyme called guanylate cyclase.
Increase the production of cyclic guanosine monophosphate (cGMP). cGMP relaxes smooth muscles; penis sponges increase the flow of blood to cause an erection.
In diabetic patients, the activity of vascular endothelial nitrogen oxide synthesis (eNOS) in endothelial cells such as spongiform arteries are easily reduced, resulting in erectile dysfunction due to smooth muscle relaxation, that is, spongiform dysfunction [Citation5]. Diabetes influences the overall endocrine system, consequently giving rise to psychological problems from fear of complications [Citation6,Citation7].
Moreover, diabetes is commonly observed in patients with PAD (Peripheral arterial disease). Both diabetes and PAD are complicated by neuropathy and foot ulceration, which are associated with an increased risk of gangrene and lower extremity amputation [Citation8]. PVD, a vascular disease occurring outside the heart and brain, wherein the narrowing of blood vessels leads to abnormal blood circulation, has been associated with vascular reactivity in people with diabetes, including morphological changes in the hands and feet and decreased capillary density in nails [Citation3]. In diabetes, vascular complications are serious conditions, and PAD is dangerous if left untreated. Blockage of arteries can lead to infarctions as well as ED.
Normally, problems with erection can be treated with phosphodiesterase-5 (PDE-5) inhibitors (Viagra®_Sildenafil) which inhibit cyclic guanosine monophosphate (cGMP). Several studies exist on the relationship between diabetes and vascular disease. Hatzichristou et al. [Citation9], in a placebo-controlled study, showed that daily therapy with a PED-5 inhibitor is effective in improving the satisfaction associated with sexual intercourse and overall treatment satisfaction in patients with diabetes. Nevertheless, this is the first study to examine its association with capillary blood circulation. By inhibiting PDE-5, cGMP levels are prolonged, and smooth muscle relaxation is improved. Sildenafil, tadalafil, and vardenafil are PDE-5 drugs used in clinical care. PDE5i improves the success of erectile intercourse in patients with diabetic ED [Citation10]. To improve ED, the medication must be taken 1–2 h before sexual activity. dosage should be regulated because the high dosage can lead to side effects. The side effects of PDE-5 inhibitors include flushing, headache, indigestion, congested nose, and diarrhea. Furthermore, MI and heart attack can occur in men who take sildenafil for ED. However, a couple of studies have found these medications to be highly tolerable while being safe and effective for coronary artery disease [Citation11].
Most people are not well-aware of diabetes-related complications. In Asian countries such as the Republic of Korea, it is considered taboo to talk about ED, and thus, treatments are often left undiscussed or ignored. People search for medications for ED on their own, as ED is also commonly thought of as a natural phenomenon related to aging. However, because of other ED causes, including diabetes-related complications, it is crucial to identify the cause and to provide proper treatment before the vascular disease becomes severe.
ED and PAD are closely associated with aging, and diabetes increases the mortality of PAD [Citation12,Citation13]. But diabetes-associated-ED is often devalued as it seems neither life-threatening nor associated with physical pain. However, as ED can cause physical and mental harm, including loss of confidence, psychological frustration, and conflict with one’s partner, appropriate management is important in patients with DM and ED.
This study aimed to compare the status before and after taking tadalafil; the blood flows improvement in diabetes patients with ED. We hypothesized that a low-dosage PDE-5 inhibitor would help improve the blood flow in patients with diabetes and ED.
Materials and methods
Study design
This was a 4-week open-label pilot evaluation of the efficacy of 5 mg once-daily tadalafil. The study included 30 outpatients at Soonchunhyang University Hospital, Republic of Korea. Our thesis is based on the study of Sáenz de Tejada, Anglin, Knight, and Emmick [Citation14]. Considering the study’s relatively high dropout rate, 30 subjects were selected considering the minimum statistical significance probability with a dropout rate of 30% (two-sided alpha = 0.05, beta [1 − power] = 0.1).
Inclusion criteria
Men over 20 years of age, Persons with HbA1C of 6.5 or higher, who have a history of diabetes mellitus and treatment for more than 6 months, and have erectile dysfunction, who voluntarily participated in the preparation of written consent and clinical trials.
Exclusion criteria
Persons with myocardial infarction within the last 90 d, unstable angina, or angina during sexual activities; Persons with heart failure in New York Heart Association Class 2 or more in the last 6 months; Persons with genetic degenerative retinopathy including pigmented retinitis; Persons who taking PDE5i or Guanylate Cyclase Stimulatory; Persons with non-arterial anterior ischemic optic neuropathy; Persons with the genetic disease as like galactose intolerance, lactulose intolerance.
The protocol and informed consent documents were approved by the ethical review board at Soonchunhyang University Hospital (No.2018-01-015), and all patients provided written informed consent before enrolment. The study was conducted in accordance with the protocol and ethical principles stated in the Declaration of Helsinki, revised in 2000, and applicable laws. The Clinical Research Information Service (CRIS) of the Republic of Korea clinical trial registered under NCT 0007552.
Measures of efficacy
The first 4 treatment-free weeks and run-in period were followed by 8 weeks of treatment phases. Eligible patients received tadalafil 5 mg at approximately the same time daily. Treatment compliance was defined as taking at least 80% of the required doses.
For primary efficacy, we determined: (1) the International Erectile Function Index according to the IIEF (a verified self-managed questionnaire that is used worldwide to diagnose ED that has demonstrated a high level of sensitivity and specificity for ED diagnosis) domains [Citation15]. The questionnaire is composed of 15 items spanning the domains of male sexual dysfunction (ED, orgasmic function, sexual desire, ejaculation, intercourse, and overall satisfaction). (2) The International Prostate Symptom Score (IPSS) and Quality of Life (QoL) questionnaire; consisting of seven questions on incomplete bladder emptying, frequency of micturition, intermittency, urgency, weak stream, straining, and nocturia, which are frequently used to assess the symptoms and QoL of men with urethral strictures. (3) Physiologic status of the patients after 8 h of fasting through blood tests, urine test, and electrocardiogram (EKG). The tests included chemistry (HbA1c, troponin, blood urea nitrogen [BUN], creatinine, fasting blood sugar [FBS], aspartate aminotransferase [AST], alanine aminotransferase [ALT], gamma-glutamyl transpeptidase [GGTP], and C-reactive protein [CRP]), complete blood count [CBC] and differentials [Diff] (white blood cell [WBC], hemoglobin [Hb], platelet), lipid (total cholesterol, high-density lipoprotein [HDL], low-density lipoprotein [LDL], triglyceride), routine urine test, prostate-specific antigen (PSA), testosterone level, bone metabolism, and EKG.
In addition to assessing efficacy, an exploratory analysis was conducted on the effect of tadalafil on capillary pressure. Capillary tests can be used to noninvasively observe microvessels [Citation16].
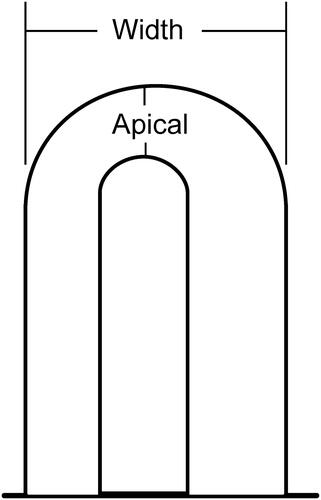
The nail vascular test was used to analyze capillary abnormalities around the nail. It is helpful in assessing the health of blood vessels throughout the body [Citation17]. After placing a drop of immersion oil on the nail to visualize the blood vessels, the second and fourth values on both sides of the nails were observed using a microscope at 200 × magnification. The capillaries of each patient’s fingernails were transferred and stored in a computer using a halo-vision stereomicroscope (digital camera Polaroid, USA) for analyses. Based on the center with the highest resolution on each of the fingers, three apical limbs and capillary widths were measured along with the speed and flow (). The nail fold capillary test is indicated by (1) apical limb width, (2) capillary width, (3) speed, and (4) flow. Capillaroscopy results are effective in evaluating the progression of early, active, and late patterns of sclerosing microangiopathy [Citation18].
Figure 1. Scheme of the capillary loop measurements (×200). Apical limb width and Capillary width.
The awareness of patients on diabetes-related complications was investigated. The responses for the items were “Yes,” “No,” or “Don’t know.”
Safety was assessed by analyzing all reported treatment-emergent adverse events (TEAEs), which were defined as any adverse event that first occurred or worsened after the patient was assigned to treatment.
Statistical analysis
All data are expressed as mean ± standard deviation, and statistical significance was assumed at p < .05. Statistical comparisons of IPSS, IIEF-5, and QoL before and after tadalafil use were made using the paired t-test. A comparison of laboratory tests was also performed using a t-test. The perception of diabetes-related complication responses were divided into three categories: “Yes,” “No,” or “Don’t know” and the percentages were measured. Analyses were conducted using the statistical R software (version 4.0; R Project for Statistical Computing, Vienna, Austria).
Results
Study participant characteristics
Overall, 20 patients (mean age, 51.11 ± 9.01 years; body mass index [BMI], 39.27 ± 15.46 kg/m2; SBP, 137.20 ± 14.09 mmHg; DBP, 84 ± 9.68 mmHg; and pulse, 82.75 ± 11.29) were included () in the study. Six patients whose visit window deviated by ±7 d were excluded and considered as lost-to-follow-up, and additional four patients were excluded due to their own decision. All participants had T2DM and had been on treatment for diabetes for >6 months using only oral medications.
Table 1. Characteristics of studies.
Primary measure of efficacy
According to the IIEF-5 self-administered questionnaire, there was a statistically significant increase in score from 12.60 to 19.80 (p < .005%). A question in the IIEF-5 questionnaire on erection reliability showed a statistically significant increase in score from 1.15 to 3.20 (p < .00012) (). The IPSS questionnaire on prostate cancer resulted in an improvement from 10.95 to 8.40 (p = .01). The QoL survey measurements changed non-significantly from 2.50 to 2.15.
Table 2. Questionnaire.
Secondary measure of efficacy, laboratory tests
After the daily administration of tadalafil 5 mg to patients with diabetes, laboratory testing showed a non-significant decrease in HbA1c from 7.47% to 7.37% and LDL-cholesterol from 91.30% to 90.85%. AST levels significantly decreased from 35.35 U/L to 23.65 U/L. The blood circulation improvement test at the fingertip capillary showed significantly increased results in the apical limb width from 13.10 to 14.65 µm (p = .04829) and flow from 9035.50 to 11946.65 µm3/s (p = .04405). The width increased non-significantly from 35.40 to 37.55 µm, and the speed from 81.50 124.10 µm/s. Troponin, a cardiac marker, showed no significant change before and after administration at 0.01 ng/mL, respectively (p = .3446). No statistically significant changes pre- and post-measurements occurred for PSA (1.50–1.28 ng/mL), testosterone (482.20–473.85 ng/dL), and EKG (Heart rate: 73.20–73.90 bpm, the Pulse rate: 169.70–172.50, QT: 375.45–385.15), further supporting the safety of the daily administration of low-dose tadalafil ().
Table 3. Laboratory test.
Furthermore, SBP and pulse rate before and after drug administration were stable with no clinical differences. DBP showed a clinically significant decrease from 84.00 to 75.30 mmHg (p = .0073) and was more stable after taking the drug.
The diabetes awareness survey
For the question on the awareness survey regarding whether medications can be used to treat complications, 45% responded with “Don’t Know” and 15% with “No.” These show that approximately >50% of patients with diabetes had inaccurate awareness of diabetes-related complications.
Discussion
This study results showed that patients with diabetes were unaware of the potential complications of the disease. They also showed that a small dose of daily tadalafil was safe and improved ED in patients with diabetes. Daily intake also improved blood flow, indicating the possibility of prevention of vascular injuries.
ED is potentially associated with cardiovascular diseases (CVDs) because of their common risk factors [Citation19]. A meta-analysis revealed associations between diabetes and CVD risk factors, such as fatal coronary heart disease and stroke [Citation20–22]. Therefore, diabetes status must be assessed in the process of identifying CVD [Citation23]. In our study, no changes were observed in either the cardiac biomarker, troponin, or the QT interval in EKG, which graphically illustrates ventricular contraction and relaxation, suggesting that a low dosage of tadalafil is safe as daily therapy.
There are several findings in this study for which we offer potential explanations. The first is the improvement of AST levels, which is a liver enzyme used to represent a liver function. In this study, it showed a significant change from 30.34 ± 18.62 to 23.62 ± 8.86 U/L before and after medication respectively (p < .05). Tadalafil is effective in dilating the arteries and veins, and AST is widely distributed in the mitochondria of the muscle, brain, lung, kidney, and liver [Citation24,Citation25]. One possible reason behind the improvement may be because tadalafil is effective in dilating veins and arteries. This would allow a better supply of blood flow to the hepatic vein and arteries yielding increased hepatic detoxification, which could decrease liver-specific AST measurements. Secondly, tadalafil’s enhancement of cellular metabolism could have also yielded the improvement in AST level. Amylase and isozymes convert polysaccharides into monosaccharides, and excess monosaccharides become triglycerides. Their accumulation can in turn cause fatty liver. However, the use of tadalafil increases cellular metabolism, which decreases triglycerides and fatty liver, leading to increased cellular energy at the biomolecular level, hence, increased metabolism [Citation26]. An increase in metabolism could reduce triglycerides and fatty liver. A previous study described the connection between AST, ALT levels, and coronary artery injury. This study suggested that patients with high AST and ALT levels should undergo periodic follow-up examinations, such as echocardiography. This previous study provides insight into the use of low-dose tadalafil therapy to treat obesity in patients with fatty liver and abdominal obesity and to improve fatty liver with a decrease in liver enzymes such as AST [Citation27].
Furthermore, PVDs include all structural or functional abnormalities in the aorta and secretory vessels. Depending on the process of atherosclerosis, various symptoms can arise from intermittent claudication and resting pain in severe cases of skin ulcers and tissue necrosis. CVDs, such as stroke or MI, are particularly common in patients with diabetes and are the main causes of death. In particular, diabetic feet, a diabetic PVD with numbness and pain at the end of the foot, is common in patients with T2DM. Moreover, the underlying risk factor for PVD is diabetes [Citation28].
PVD can cause painless trauma, ulcers, and infection, and can even lead to amputation of the foot due to decreased oxygen, nutrients, and poor blood circulation. In a meta-analysis, patients with diabetic PAD had high mortality and associated CVD with poor prognosis; including increased platelet activity, increased levels of coagulation factors, and inflammatory biomarkers [Citation12]. When comparing the mortality of patients with PAD, the mortality rate was 58% and 29% for patients with and without diabetes, respectively [Citation29]. The results of these studies showed that diabetes-related mortality is associated with peripheral blood vessels. Therefore, since ED, a PVD, is common in patients with diabetes, further studies on the effects of daily low-dose tadalafil therapy on PVD are necessary. Additional studies on the relationship between tadalafil and capillary pressure are also needed.
Previous studies showed the relationship between ED and the prevalence of PAD, and how ED can be used as a marker for coronary artery disease [Citation30]. Furthermore, diabetes is clinically associated with PAD. Therefore, this report extends the spectrum of diabetes-related complications to include blood circulation in ED. Diabetes is a high-risk factor for PVD, and a large-scale study by the National Health and Nutrition Examination Survey found an association between diabetes, high blood pressure, dyslipidemia, smoking, and the prevalence of PAD [Citation31]. In a previous study, 45% of patients with diabetes had ED and 23% had PAD, which was significantly higher for men with than men without ED (32% vs. 16%, p < .01). Of those with PAD, 66% reported no lower extremity symptoms. Moreover, a direct correlation occurred between PAD prevalence and ED severity (28%, 33%, and 40% of men had mild, moderate, and severe ED, respectively, p < .001). In multivariate analysis, ED (odds ratio 1.97; 95% confidence interval, 1.32–2.94; p = .002) was an independent predictor of PAD [Citation32].
In addition, vascular ED can be used as a powerful marker because it is associated with cardiovascular risk [Citation16]. ED should be considered a diabetes-related complication and needs to be discussed during consultation for diabetes. Ultimately, this study was conducted to demonstrate the importance of managing PAD in patients with diabetes with ED.
However, there are several limitations to this study. First, since the research was conducted over the winter, blood circulation, depending on the temperature difference, was not considered. Weather-related fluctuations in blood pressure are common. As the temperature decreases, the sympathetic nerve is stimulated to constrict blood vessels and cause blood circulation disorders; therefore, it was difficult to discern minimal effects [Citation33]. Future studies need to adjust for temperature variations such as by conducting the research during periods of consistent temperatures or after returning to normal body temperature. Second, we could not variate the duration of diabetes treatment. If it had been done, we would have been able to examine in greater detail, the effect of tadalafil on ED depending on the progression of diabetes. Third, it was impossible to completely confirm the possibility and presence of complications based on the duration of diabetes treatment. Fourth, ED in patients with diabetes is related to age, the duration of diabetes treatment, existing disease, compliance with diabetes medications, lifestyle, and smoking; however, this bias was not considered in the study. Finally, our study had a small sample size and was conducted in a single institution. No previous study has confirmed the degree of blood circulation in patients with diabetes and ED; therefore, this study was conducted with a minimum number of samples as a primary study. The drawback is that the magnitude of the association can be overestimated. However, as an initial study to determine the degree of improvement in blood circulation in patients with diabetes and ED, this study may facilitate related studies. To overcome some of these limitations, follow-up studies would be better, in various institutions.
The prevalence of ED is high among patients with diabetes; therefore, it is necessary to plan preventive measures and treatments to raise patient awareness and improve the patients’ QoL. It is important to help patients with diabetes understand the relationship between ED and other severe complications, enhance healthy sexual habits, and improve their QoL by improving their vascular condition with a low dose of medication.
The relation between diabetes and male erectile dysfunction has not been seriously considered in the past, but the latest studies have proven that vascular endothelial cells’ damage as complication of diabetes is associated with the damage on vascular endothelial cells of the male penile cavernous body and can be a major cause of male erectile dysfunction.
Some studies conducted during the SARS-Cov-2 (COVID-19) global pandemic may suggest that male patients infected with COVID-19 are 3.3 times more likely to develop male erectile dysfunction and [Citation34,Citation35] studies confirming that it may have a detrimental effect on male reproductive function, including impaired male erectile dysfunction.
COVID-19 is still a disease that needs further study, but a follow-up study on male sexual dysfunction and infertility in SARS-Cov-2-infected men may also be considered, considering its association with various diseases that cause erectile dysfunction. The progression of PAD can be predicted to some extent at the time of diagnosis of ED in patients with diabetes. Therefore, medical personnel should be aware of the risk of PAD when ED is clinically confirmed in patients with diabetes and be able to offer suggestions for active clinical diagnosis and treatment. However, in cases where patients with diabetes refuse to acknowledge the existence of their own ED, a clinical approach that considers the symptoms of clinically progressive claudication for PAD as objective evidence for accompanying ED is needed.
Conclusions
During treatment, the patient’s life can be improved if more attention is given to improving the QoL and vascular diseases, such as CVD, originating from PAD. Lastly, diabetes, ED, and arterial disease should not be considered as separate diseases but should be viewed as comprehensive diseases using a clinical approach.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, BYW, upon reasonable request.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- International Diabetes Federation. IDF diabetes atlas. 10th ed. Brussels, Belgium: International Diabetes Federation; 2021. Available from: https://diabetesatlas.org/
- Asaduzzaman M, Kamrul-Hasan AB, Islam A, et al. Frequency and risk factors of erectile dysfunction among Bangladeshi adult men with type 2 diabetes mellitus. Mymensingh Med J. 2020;29(1):66–72.
- Meyer MF, Pfohl M, Schatz H. Nachweis diabetischer ikrozirkulationsveranderungen mittels kapillaroskopie und Laser-doppler-Anemometrie. [Assessment of diabetic alterations of microcirculation by means of capillaroscopy and laser-Doppler anemometry]. Med Klin. 2001;96(2):71–77.
- Shabsigh R, Klein LT, Seidman S, et al. Increased incidence of depressive symptoms in men with erectile dysfunction. Urology. 1998;52(5):848–852.
- Giuseppe D, Rossella M, Marta T, et al. Erectile dysfunction and diabetes: a melting pot of circumstances and treatments. Diabetes Metab Res Rev. 2022;38(2):e3494.
- Chu NV, Edelman SV. Diabetes and erectile dysfunction. Clin Diabetes. 2001;19(1):45–47.
- Malavige LS, Levy JC. Erectile dysfunction in diabetes mellitus. J Sex Med. 2009;6(5):1232–1247.
- Dolan NC, Liu K, Criqui MH, et al. Peripheral artery disease, diabetes, and reduced lower extremity functioning. Diabetes Care. 2002;25(1):113–120.
- Hatzichristou D, Haro JM, Martin-Morales A, et al. Patterns of switching phosphodiesterase type 5 inhibitors in the treatment of erectile dysfunction: results from the erectile dysfunction observational study. Int J Clin Pract. 2007;61(11):1850–1862.
- Morano S. Pathophysiology of diabetic sexual dysfunction. J Endocrinol Invest. 2003;26(Suppl 3):65–69.
- Reffelmann T, Kieback A, Kloner RA. The cardiovascular safety of tadalafil. Expert Opin Drug Saf. 2008;7(1):43–52.
- Falkensammer J, Hakaim AG, Falkensammer CE, et al. Prevalence of erectile dysfunction in vascular surgery patients. Vasc Med. 2007;12(1):17–22.
- Vrsalovic M, Vucur K, Vrsalovic Presecki A, et al. Impact of diabetes on mortality in peripheral artery disease: a meta-analysis. Clin Cardiol. 2017;40(5):287–291.
- Sáenz de Tejada I, Anglin G, Knight JR, et al. Effects of tadalafil on erectile dysfunction in men with diabetes. Diabetes Care. 2002;25(12):2159–2164.
- Rosen RC, Riley A, Wagner G, et al. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49(6):822–830.
- Maldonado G, Guerrero R, Paredes C, et al. Nailfold capillaroscopy in diabetes mellitus. Microvasc Res. 2017;112:41–46.
- Cutolo M, Sulli A, Secchi ME, et al. Nailfold capillaroscopy is useful for the diagnosis and follow-up of autoimmune rheumatic diseases. A future tool for the analysis of microvascular heart involvement? Rheumatology. 2006;45(Suppl 4):iv43–iv46.
- Cutolo M, Grassi W, Matucci Cerinic M. Raynaud’s phenomenon and the role of capillaroscopy. Arthritis Rheum. 2003;48(11):3023–3030.
- Wright AK, Kontopantelis E, Emsley R, et al. Cardiovascular risk and risk factor management in type 2 diabetes mellitus. Circulation. 2019;139(24):2742–2753.
- Huxley R, Barzi F, Woodward M. Excess risk of fatal coronary heart disease associated with diabetes in men and women: meta-analysis of 37 prospective cohort studies. BMJ. 2006;332(7533):73–78.
- Peters SA, Huxley RR, Woodward M. Diabetes as a risk factor for stroke in women compared with men: a systematic review and meta-analysis of 64 cohorts, including 775,385 individuals and 12,539 strokes. Lancet. 2014;383(9933):1973–1980.
- Peters SA, Huxley RR, Woodward M. Diabetes as risk factor for incident coronary heart disease in women compared with men: a systematic review and meta-analysis of 64 cohorts including 858,507 individuals and 28,203 coronary events. Diabetologia. 2014;57(8):1542–1551.
- Cosentino F, Ceriello A, Baeres FMM, et al. Addressing cardiovascular risk in type 2 diabetes mellitus: a report from the European Society of Cardiology Cardiovascular Roundtable. Eur Heart J. 2019;40(34):2907–2919.
- Bocchio M, Pelliccione F, Passaquale G, et al. Inhibition of phosphodiesterase type 5 with tadalafil is associated to an improved activity of circulating angiogenic cells in men with cardiovascular risk factors and erectile dysfunction. Atherosclerosis. 2008;196(1):313–319.
- Rosano GM, Aversa A, Vitale C, et al. Chronic treatment with tadalafil improves endothelial function in men with increased cardiovascular risk. Eur Urol. 2005;47(2):214–220. discussion 220–222.
- Vilela VR, de Oliveira AL, Comar JF, et al. Tadalafil inhibits the cAMP stimulated glucose output in the rat liver. Chem Biol Interact. 2014;220:1–11.
- Wang J, Li J, Ren Y, et al. Association between alanine aminotransferase/aspartate aminotransferase ratio (AST/ALT ratio) and coronary artery injury in children with Kawasaki disease. Cardiol Res Pract. 2020;2020:8743548.
- Hur KY. Diagnosis of peripheral artery disease: focus on the 2016 American Heart Association/American College of Cardiology and 2017 European Society of Cardiology guidelines. J Korean Diabetes. 2019;20(1):17–23.
- Mueller T, Hinterreiter F, Poelz W, et al. Mortality rates at 10 years are higher in diabetic than in non-diabetic patients with chronic lower extremity peripheral arterial disease. Vasc Med. 2016;21(5):445–452.
- Meena BL, Kochar DK, Agarwal TD, et al. Association between erectile dysfunction and cardiovascular risk in individuals with type-2 diabetes without overt cardiovascular disease. Int J Diabetes Dev Ctries. 2009;29(4):150–154.
- Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the national health and nutrition examination survey, 1999–2000. Circulation. 2004;110(6):738–743.
- Polonsky TS, Taillon LA, Sheth H, et al. The association between erectile dysfunction and peripheral arterial disease as determined by screening ankle-brachial index testing. Atherosclerosis. 2009;207(2):440–444.
- Petrofsky JS, Berk L, Alshammari F, et al. The interrelationship between air temperature and humidity as applied locally to the skin: the resultant response on skin temperature and blood flow with age differences. Med Sci Monit. 2012;18(4):CR201–8.
- Mohamed A, Ismail A. Erectile dysfunction: the non-utilized role of exercise rehabilitation for the most embarrassing forgotten post-COVID complication in men. Aging Male. 2022;25(1):217–218.
- Adeyemi DH, Odetayo AF, Hamed MA, et al. Impact of COVID 19 on erectile function. Aging Male. 2022;25(1):202–216.