
Abstract
Aims
To assess US payers’ per-patient cost of testing associated with next-generation sequencing (NGS) versus polymerase chain reaction (PCR) biomarker testing strategies among patients with metastatic non-small cell lung cancer (mNSCLC), including costs of testing, delayed care, and suboptimal treatment initiation.
Methods
A decision tree model considered biomarker testing for genomic alterations using either NGS, sequential PCR testing, or hotspot panel PCR testing. Literature-based model inputs included time-to-test results, costs for testing/medical care, costs of delaying care, costs of immunotherapy [IO]/chemotherapy [CTX] initiation prior to receiving test results, and costs of suboptimal treatment initiation after test results (i.e. costs of first-line IO/CTX in patients with actionable mutations that were undetected by PCR that would have been identified with NGS). The proportion of patients testing positive for a targetable alteration, time to appropriate therapy initiation, and per-patient costs were estimated for NGS and PCR strategies combined.
Results
In a modeled cohort of 1,000,000 members (25% Medicare, 75% commercial), an estimated 1,119 had mNSCLC and received testing. The proportion of patients testing positive for a targetable alteration was 45.9% for NGS and 40.0% for PCR testing. Mean per-patient costs were lowest for NGS ($8,866) compared to PCR ($18,246), with lower delayed care costs of $1,301 for NGS compared to $3,228 for PCR, and lower costs of IO/CTX initiation prior to receiving test results (NGS: $2,298; PCR:$5,991). Cost savings, reaching $10,496,220 at the 1,000,000-member plan level, were driven by more rapid treatment with appropriate therapy for patients tested with NGS (2.1 weeks) compared to PCR strategies (5.2 weeks).
Limitations
Model inputs/assumptions were based on published literature or expert opinion.
Conclusions
NGS testing was associated with greater cost savings versus PCR, driven by more rapid results, shorter time to appropriate therapy initiation, and minimized use of inappropriate therapies while awaiting and after test results.
Introduction
Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, representing approximately 85% of all diagnosed cases worldwide.Citation1 The prevalence of NSCLC has increased over the last decade, reaching 198.3 per 100,000 individuals in 2016 in the United States (US).Citation2 Non-squamous NSCLC (primarily adenocarcinoma) comprises ∼57% of NSCLC cases, of which ∼50% are classified as advanced, while squamous NSCLC comprises ∼29% of cases, of which ∼40% are classified as advanced.Citation2 Since most patients with NSCLC are diagnosed in advanced stages, the prognosis tends to be poor, with 5-year survival rates estimated at 5.8% for patients with metastatic NSCLC (mNSCLC).Citation1,Citation2 However, survival can be significantly improved among patients with driver mutations for which targeted therapies are available, resulting in response rates as high as 80%.Citation3 Over half of NSCLC adenocarcinomas are positive for an actionable genetic alteration, including EGFR mutations (19%), KRAS G12C mutations (∼12%), and ALK rearrangements (5%).Citation4–6 As such, molecular testing has become an integral aspect of disease management for patients with mNSCLC, with implications for treatment that may include targeted therapies for patients with specific alterations.Citation3 Accordingly, the current clinical practice guidelines recommend comprehensive molecular testing for all patients with non-squamous advanced-stage NSCLC so that they may receive appropriate targeted therapy as needed.Citation7,Citation8 There are no recommendations for routine molecular testing in patients with squamous cell carcinoma, though testing should be performed when clinical features indicate high probability of driver mutations, regardless of NSCLC histology.Citation7
Currently available molecular testing strategies range from simple, single-gene tests like polymerase chain reaction (PCR)-based methods (e.g. sequential or targeted hotspot panel) to complex, multiple-gene assays that can simultaneously detect various types of genetic modifications.Citation8,Citation9 Next-generation sequencing (NGS) is one such broad panel − based strategy that has become the preferred method for comprehensive and parallel testing of multiple clinically relevant genetic modifications, consistent with guideline recommendations.Citation7–9 Relative to hotspot panel testing, NGS allows for a broader assessment of mutations in one test, including alterations that may not be reliably detected by hotspot (e.g. fusions, copy number alterations).Citation9 Additionally, NGS requires less tissue than hotspot testing, especially if multiple genes or genomic regions must be analyzed, and is often associated with a faster turnaround time compared to multiple, sequential single-gene assays.Citation8,Citation9 While NGS testing has traditionally been done via tissue biopsy, the use of liquid biopsy (i.e. plasma-based circulating tumor DNA) may represent a less invasive alternative that also has a shorter turnaround time.Citation9,Citation10 Use of NGS in patients with mNSCLC has been shown to be associated with substantial cost savings relative to single-gene testing strategies in the US, from both Medicare and commercial payer perspectives.Citation11–13 Indeed, in a previous study using a decision tree model by Vanderpoel et al. NGS testing, relative to PCR testing strategies, was associated with a shorter time to appropriate targeted therapy (2 weeks versus 6 weeks) and lower per-patient testing and testing-related medical costs ($4,932 versus $6,605).Citation13
However, given the potential for missed detections and additional time needed for single-gene testing sequences to accurately identify the presence of mutations, patients with mNSCLC who are tested with PCR strategies often experience delays in receiving appropriate treatment and may be initiated on non-targeted treatment instead.Citation14,Citation15 The costs associated with this delayed care and inappropriate treatment initiated either before or after receiving biomarker test results are not well-characterized in the literature. Therefore, the current study was conducted to expand upon the model by Vanderpoel et al. by assessing the total cost of testing associated with NGS versus PCR testing strategies among patients with mNSCLC, including costs of delayed care, treatment initiation before receiving test results, and suboptimal treatment initiation after test results, from Medicare and commercial payer perspectives.
Methods
Model framework
As previously described by Vanderpoel et al.Citation13 a decision tree model was developed with a time horizon spanning from the date of first test collection following mNSCLC diagnosis to appropriate therapy initiation.
Model structure
Patients with mNSCLC insured through Medicare (aged ≥65 years) or a commercial health insurance plan (aged 18–64 years) entered the model, received an initial biopsyCitation12,Citation13,Citation16, and underwent one of the following testing strategies:
NGS testing: a broad spectrum biomarker panel simultaneously testing for all clinical guideline–recommended and/or actionable alterations (EGFR, ALK, ROS1, KRAS, BRAF, MET, HER2, RET, NTRK1, NTRK2, and NTRK3)Citation8; either a tissue or liquid biopsy was used
Sequential testing: a sequence of single-gene tests for clinical guideline–recommended alterations, in the order of EGFR, ALK, and ROS1Citation8; if a positive test result was received, no additional testing was required. If all three alterations tested negative, the following sequence of single-gene tests was conducted, in this order (as reported in clinical guidelines), as long as a negative test result was received for the prior alteration: KRAS, BRAF, MET, HER2, RET, NTRK1, NTRK2, and NTRK3Citation8
Hotspot panel testing: a simultaneous panel test for three clinical guideline–recommended alterations (EGFR, ALK, and ROS1)Citation8; if all three alterations tested negative, an expanded testing panel for other alterations (KRAS, BRAF, MET, HER2, RET, NTRK1, NTRK2, and NTRK3) was conducted
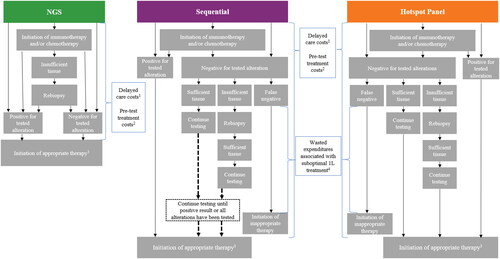
Patients may have initiated immunotherapy and/or chemotherapy while awaiting test results. Depending on the testing strategy received, additional testing and rebiopsy may have been required after the initial test if a genomic alteration was not appropriately identified and there was insufficient tissue sample remaining from the initial biopsy. A terminal node in the decision tree was reached when a genomic alteration was correctly identified and appropriate therapy was initiated, which was defined as targeted therapy for those with an actionable mutation or non-targeted therapy (i.e. immunotherapy and/or chemotherapy) for those without an actionable mutation. Among patients tested with PCR-based sequential and hotspot panel testing, a proportion of patients were classified as false negative when they had actionable mutations that were undetected by PCR that would have been identified with NGS. For each testing strategy, total cost of testing was assessed and included testing costs and testing-related medical costs associated with rebiopsies and related complications, as well as outpatient/specialist visits. Additionally, costs associated with treatment initiated prior to receiving test results, delayed care, and suboptimal first-line (1 L) treatment were included based on the below assumptions ().
Figure 1. Model diagram.
Abbreviations. 1L, first-line; NGS, next-generation sequencing; PCR, polymerase chain reaction.
Notes:
1. The estimated costs associated with delaying treatment were calculated as the time to initiation of appropriate targeted therapy times the estimated weekly cost during the pre-diagnosis phase.
2. The estimated costs associated with the initiation of treatment (i.e. immunotherapy and/or chemotherapy) prior to receiving test results were calculated as the time to initiation of appropriate targeted therapy times the weekly drug and medical costs associated with the treatment regimen.
3. Appropriate therapy was defined as targeted therapy for those with an actionable mutation or non-targeted therapy (i.e. immunotherapy and/or chemotherapy) for those without an actionable mutation. Patients who initiated immunotherapy and/or chemotherapy (i.e. non-targeted therapy) prior to receiving test results who were negative for tested alterations continued to receive non-targeted therapy.
4. Wasted expenditures associated with initiating suboptimal treatment (i.e. immunotherapy and/or chemotherapy) were calculated as the estimated incremental medical costs associated with targeted therapy as second line versus first line, times the average duration for the line of therapy.
Model assumptions
Model assumptions were as described in Vanderpoel et al.Citation13 (Table S1), with the following modifications incorporated:
The proportion of patients receiving each testing strategy was updated to 60% NGSCitation17 (10% liquid, 90% tissue), 10% sequential, and 30% hotspot panel, to reflect recent testing patterns. These testing strategies were mutually exclusive.
A proportion of patients initiated immunotherapy and/or chemotherapy prior to receiving test results; this proportion was assumed to be the same for each testing strategy, based on published literatureCitation18. Patients who tested positive for EGFR ex20ins who initiated immunotherapy monotherapy prior to receiving test results were considered as initiating inappropriate treatment based on current clinical guidelinesCitation19.
Delaying the start of treatment because of longer time to test results was assumed to be associated with monthly costs consistent with the monthly costs of regular care in the 12-month pre-diagnosis phase, referred to as costs of delaying care (details provided in the Model inputs section below).
It was assumed that additional costs (referred to as wasted healthcare expenditures associated with initiating suboptimal 1L treatment) were incurred for patients with actionable mutations that were not detected with a PCR testing strategy, given that they would be initiating suboptimal 1L treatment (i.e. immunotherapy and/or chemotherapy instead of targeted therapy for the actionable mutation that would have been identified with NGS; details provided in the Model inputs section below).
Model inputs
Population inputs
The total population included a hypothetical cohort of 1,000,000 insured adult patients, where 250,000 were covered by Medicare and 750,000 were covered by a commercial health plan. Additional scenarios considered cohorts composed of 100% Medicare-insured or 100% commercially insured patients. Population inputs included the proportion of adults with lung cancer, those with mNSCLC, and those with squamous mNSCLC; full details regarding population inputs are provided in Table S2.
Clinical inputs
Clinical inputs used in the model included the rate of positive genomic identification for each alteration, the proportion of patients requiring or receiving rebiopsy, the proportion of patients initiating immunotherapy and/or chemotherapy prior to receiving test results, and time to test results. Additionally, the proportion of patients inappropriately initiating immunotherapy and/or chemotherapy as 1 L treatment after missed detection of an actionable mutation with a PCR testing strategy (i.e. the difference between the proportion of patients testing positive for an actionable mutation with NGS versus PCR testing) was also included. All clinical inputs were estimated based on targeted literature review and/or expert opinion; full details are provided in Table S2.
Cost inputs
The Medicare and commercial payer perspectives were evaluated using separate cost estimates. Centers for Medicare & Medicaid Services (CMS) Physician and Clinical Lab Fee SchedulesCitation20,Citation21 and data collected from a targeted literature review were used to derive cost inputs for each specific type of test. Medical costs included PD-L1 testing costs and costs associated with rebiopsy and outpatient/specialist visits. Costs associated with delaying care were based on retrospective claims analyses of patients with lung cancer that reported mean per-patient costs during the pre-diagnosis phaseCitation22,Citation23 and were estimated by multiplying the weekly cost by the time to initiation of appropriate therapy (in weeks) evaluated for each testing strategy. Costs associated with initiating treatment prior to receiving test results (i.e. immunotherapy and/or chemotherapy) were calculated as the weekly drug and medical costs associated with the treatment regimen multiplied by the time to initiation of appropriate therapy evaluated for each testing strategy. Costs of immunotherapy (i.e. pembrolizumab) and chemotherapy (i.e. carboplatin plus paclitaxel for squamous mNSCLC and carboplatin plus pemetrexed for non-squamous mNSCLC) were based on the CMS Drug Fee ScheduleCitation24, as well as a targeted literature review. Wasted healthcare expenditures associated with initiating suboptimal 1 L treatment (i.e. immunotherapy and/or chemotherapy) were evaluated among patients with actionable mutations that were not detected with PCR versus NGS testing, calculated as the literature-based incremental medical costs associated with initiating targeted therapy as second-line versus 1 LCitation25, times the average regimen-based 1 L therapy duration (as a conservative estimate)Citation26,Citation27. Full details on the cost inputs are provided in Table S3.
Model outputs
The proportion of patients testing positive for a mutation with an approved targeted therapy, as well as the time to initiation of appropriate therapy, was reported by testing strategy (i.e. NGS, sequential, hotspot panel, and both PCR options [sequential and hotspot panel] combined). The following actionable mutations were considered to have approved targeted therapies: EGFR, ALK, ROS1, BRAF V600E, KRAS G12C, MET, HER2, RET, NTRK1, NTRK2, and NTRK3.
The total cost of testing for each strategy (i.e. NGS, sequential, hotspot panel, or both PCR options combined) was evaluated both at the per patient and plan level, and included testing costs, testing-related medical costs, estimated costs associated with delaying care, costs of treatment initiated prior to receiving test results, and wasted healthcare expenditures associated with initiating suboptimal 1 L treatment. Total costs were estimated from the Medicare and commercial payer perspectives, separately and combined (i.e. blended). The medical care component of the Consumer Price Index was used to inflate all costs to 2022 US dollarsCitation28.
Budget impact analysis
The proportion of patients tested with NGS was increased from the base case of 60% to 80%, reducing the proportions of patients receiving PCR strategies (5% sequential and 15% hotspot panel), to assess the effect of increased NGS use on health system costs. The budget impact analysis was conducted from the Medicare and commercial payer perspectives, separately and blended.
Sensitivity analysis
A one-way sensitivity analysis (OSA) was conducted, where key model inputs (e.g. testing costs, proportion of patients initiating treatment prior to receiving test results, costs of treatment and delaying treatment) were independently modified to evaluate the robustness of the results. The impact of each parameter on costs was assessed using a “high” and “low” value corresponding to upper and lower bounds identified in a targeted literature review (focusing on publications from the last 5 years) or based on predetermined thresholds (e.g. ± 20% of the base case; Table S4). Separate OSAs were conducted for NGS and both PCR testing strategies combined.
Results
Population and clinical outputs
A total of 1,119 members from the blended Medicare and commercial insurance cohort were estimated to have mNSCLC and received genetic testing. In the 100% Medicare and 100% commercial populations, 3,853 and 207 members, respectively, were estimated to have mNSCLC and received genetic testing. Under base case assumptions for the blended population, a higher proportion of patients tested positive for a mutation with an approved targeted therapy using NGS (45.9%) than PCR testing strategies (total 40.0%; 37.9% for sequential and 40.7% for hotspot panel). NGS was associated with a shorter estimated mean time to initiation of appropriate therapy (2.1 weeks) compared to the PCR strategies (total 5.2 weeks; 10.5 weeks for sequential and 3.5 weeks for hotspot panel; ).
Table 1. Clinical output summary.
Costs associated with NGS versus PCR testing strategies
Under base case assumptions for the blended population, total lifetime costs of testing, delayed care, pre-test treatment, and wasted expenditures of suboptimal 1 L treatment per patient were lowest for NGS testing ($8,866) compared to the PCR strategies (total $18,246; $27,954 for sequential and $15,009 for hotspot panel; ). The population-level cost of testing was $5,949,941 for NGS compared to $8,165,095 for the combined PCR strategies.
Figure 2. Cost of genetic testing, delayed care, and suboptimal treatment, per testing strategy, among the (A) blended population,1 (B) Medicare only population, and (C) commercial only population.
Abbreviations. 1L, first-line; NGS, next-generation sequencing; US, United States.
Notes:
1. The blended population assumed that 25% of members had Medicare coverage and 75% of members had commercial coverage.
2. Wasted expenditures associated with initiating suboptimal treatment (i.e. immunotherapy and/or chemotherapy) were calculated as the estimated incremental medical costs associated with targeted therapy as second line versus first line, times the average duration for the line of therapy.
3. The estimated costs associated with the initiation of treatment (i.e. immunotherapy and/or chemotherapy) prior to receiving test results were calculated as the time to initiation of appropriate targeted therapy times the weekly drug and medical costs associated with the treatment regimen.
4. The estimated costs associated with delaying treatment were calculated as the time to initiation of appropriate targeted therapy times the estimated weekly cost during the pre-diagnosis phase.
5. Costs include rebiopsy, outpatient/specialist visits, and PD-L1 testing costs.
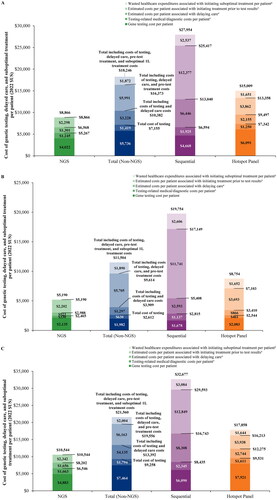
Estimated costs associated with delayed care were the lowest per patient among those tested with NGS ($1,301) relative to both PCR strategies (total $3,228; $6,446 for sequential and $2,155 for hotspot panel), as were per patient costs associated with the initiation of treatment prior to receiving test results (NGS $2,298; total PCR $5,991; $12,377 for sequential and $3,862 for hotspot panel ()). For example, estimated wasted costs per EGFR ex20ins-mutated patient of initiating inappropriate treatment (i.e. immunotherapy monotherapy) prior to receiving a positive genomic alteration test result were $423 for NGS and $1,090 for both PCR testing strategies combined. Among patients tested with PCR testing strategies, 5.9% of patients had an actionable mutation that was not detected by PCR and would have been detected by NGS testing (8.0% for sequential, 5.2% for hotspot panel), resulting in suboptimal 1 L treatment initiation and an associated $1,872 in wasted healthcare expenditures per patient tested with a PCR strategy ($2,537 for sequential, $1,651 for hotspot panel).
NGS was also the least expensive testing strategy per patient when assessed from both a 100% Medicare (NGS $5,190; PCR $11,504; ) and 100% commercial payer perspective (NGS $10,544; PCR $21,560; ).
Budget impact analysis
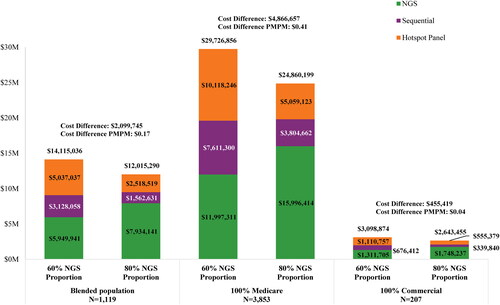
Increasing the proportion of patients tested with NGS from 60% to 80% (and decreasing the proportion tested with PCR strategies from 40% to 20% [sequential from 10% to 5% and hotspot panel from 30% to 15%]) amounted to incremental cost savings of $0.17 per member per month (PMPM) and $2,099,745 annually at the 1 million-member plan level for the blended population (; Table S5). For the 100% Medicare cohort, incremental cost savings amounted to $0.41 PMPM and $4,866,657 annually, while for the Commercial cohort, incremental cost savings were $0.04 PMPM and $455,419 annually. Further extrapolating on the impact of increased NGS adoption, assuming that 100% of the 1,119 members from the blended population were tested with NGS relative to a scenario where 100% were tested with PCR strategies, total plan-level cost savings would amount to $10,496,220 annually, an additional 5.9% of patients would test positive for a mutation with an approved targeted therapy, and the estimated mean time to initiation of appropriate therapy would decrease by 3.1 weeks.
Figure 3. Total budget impact for 60% versus 80% of patients tested with NGS1.
Abbreviations. 1L, first-line; NGS, next-generation sequencing; PMPM, per member per month.
Note:
1. Includes costs of genetic testing, delayed care, pre-test treatment costs, and suboptimal 1L treatment costs.
Sensitivity analysis
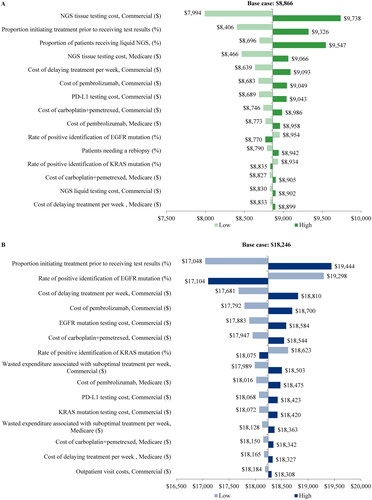
When main model inputs were varied, the total per-patient cost of testing consistently remained lower for patients tested with NGS (range of $7,994 to $9,738) compared with PCR strategies (range of $17,048 to $19,444; ). The model inputs with the largest influence on the total per-patient cost of NGS were the tissue testing costs for commercial and Medicare plans, the proportion of patients initiating treatment prior to receiving test results, and the proportion of patients receiving liquid NGS. Increasing the proportion of patients tested with liquid NGS from 10% to 50% resulted in an increase of $681 in per-patient total costs of testing, delayed care, pre-test treatment, and wasted expenditures of suboptimal 1 L treatment. For both PCR strategies combined, the most impactful model inputs were the proportion of patients initiating treatment prior to receiving test results, rate of positive identification of EGFR mutation, and the cost of delaying treatment per week for the commercial plans.
Figure 4. Sensitivity analysis for (A) NGS and (B) both PCR testing strategies combined.
Abbreviations. NGS, next-generation sequencing; PCR, polymerase chain reaction.
Discussion
In this study, a decision tree model was used to estimate the total cost of biomarker testing for patients with newly diagnosed mNSCLC via NGS or single-gene testing strategies. In addition to medical costs related to testing (e.g. rebiopsies and outpatient/specialist visits), the model incorporated costs associated with non-targeted therapy received while patients were waiting for test results, delayed care, and suboptimal 1 L treatment. Based on the findings, NGS testing resulted in the highest proportion of patients testing positive for an actionable mutation, and it was associated with the shortest time to initiation of appropriate therapy. Accordingly, patients tested with NGS had the lowest total costs of testing relative to sequential or hotspot panel testing strategies in the 100% Medicare, 100% commercial, and blended populations. This finding was driven by the high costs associated with delayed care and immunotherapy and/or chemotherapy initiation prior to receipt of test results for the PCR strategies. Moreover, close to 6% of patients had an actionable mutation that was not detected by PCR and would have been detected by NGS testing, further adding to the higher costs among patients tested with PCR due to wasted healthcare expenditures from suboptimal 1 L treatment initiation. Results remained robust in sensitivity analyses whereby patients tested with NGS continued to have lower costs relative to patients tested with PCR testing strategies as model inputs were varied. This included varying the proportion of patients who received liquid NGS from 10% to 50%, which resulted in an increase of $681 per patient. However, this may be overestimation as liquid NGS is associated with a faster turnaround time relative to tissue NGSCitation10,Citation29 which was not considered in this model and would reduce the estimated costs associated with delayed care.
This study builds upon a prior decision tree model by Vanderpoel et al. that demonstrated faster time to appropriate targeted therapy initiation and lower total costs associated with NGS than PCR testing strategiesCitation13. Importantly, the current study expands the model to incorporate additional costs that patients may incur as part of the testing sequence. Indeed, patients may receive inappropriate therapy (i.e. non-targeted treatment) both before receipt of test results while waiting for accurate resultsCitation15, and after receipt of test results, because of missed detections associated with PCR testing strategiesCitation14. Our results demonstrate that both of these scenarios result in higher costs for PCR-tested patients relative to NGS-tested patients due to delayed care, increased medical visits, and wasted healthcare expenditures related to initiation of suboptimal treatment. These findings are corroborated by the limited existing literature on this topic, which show high costs associated with inappropriate treatment in NSCLCCitation11,Citation14,Citation30. For instance, based on a hypothetical US cohort of 60,502 patients with newly diagnosed mNSCLC, Cheng et al. estimated that using an EGFR molecular test with a 2.3% misclassification rate compared to 1% would result in $7.3 million (2015 USD) higher aggregate treatment costs from a Medicare perspective due to additional drug and adverse event costs among patients who are incorrectly treatedCitation14. A separate model-based study using a simulated population of 89,000 patients with advanced non-squamous NSCLC by Lemmon et al. reported that each incremental 10% increase in the use of NGS versus single-gene testing would produce an average of 2,627 additional life-years gained and cost savings of $75 per life-year gained (USD, published 2023) because of increased rates of mutation detection and targeted therapy use with NGSCitation11. While these studies are not directly comparable to ours, they nonetheless highlight the substantial wasted expenditures incurred when patients with NSCLC receive inappropriate treatment as a result of missed mutation detection. This is particularly important in the context of a recent study by Wong et al. showing that multigene panel tests are not associated with higher costs compared to single-gene tests among commercially insured patients with solid tumors, including advanced NSCLC, and that coverage for multigene panel tests is minimally cost additive to the payers and patient insurance premiumsCitation31.
In addition to high costs, delayed initiation of appropriate targeted therapy for NSCLC can have important clinical implications. Notably, a prior study estimated that if NSCLC treatment was delayed by as little as 1 week, 4% of patients would die while awaiting treatmentCitation32. With regards to targeted therapy specifically, a prior retrospective study of patients with advanced, ALK-positive NSCLC found that a > 3-week delay in initiation of ALK inhibitor treatment was associated with a > 2-fold higher risk of death (adjusted hazard ratio [95% confidence interval] = 2.05 [1.13-3.71])Citation33. Furthermore, in a separate analysis of patients with EGFR- or ALK-positive advanced NSCLC, 18% of patients did not receive treatment with tyrosine kinase inhibitors (TKIs) within 12 months of diagnosis, which was associated with shorter overall survivalCitation34. In fact, use of TKIs was associated with an absolute increase in median overall survival of 10 to 12 months and a relative decrease in risk of death by 42% to 45%, illustrating the importance of timely initiation of appropriate targeted therapy in patients with actionable mutations. With the shortest time to initiation of appropriate therapy relative to PCR testing strategies in the current study, NGS has the potential to minimize treatment delays and subsequently improve survival and economic outcomes for patients with mNSCLC. In fact, findings from a recent real-world evaluation showed that upfront testing with NGS led to better clinical outcomes among patients with advanced NSCLC (median overall survival in months [95% confidence interval] = 20.9 [19.8-21.9]) relative to NGS testing after 1 L therapy initiation (18.2 [16.6-19.4]) or no NGS at all (16.9 [15.3-18.6])Citation35.
In the present study, initiation of non-targeted treatment prior to receiving test results was associated with a considerable cost burden, especially for PCR testing strategies. Despite the poor response rates reported among patients with NSCLC and actionable mutations who are treated with certain systemic, non-targeted therapies (e.g. immunotherapy)Citation36–38, a recent US physician survey study reported that if a patient was initiated on immunotherapy and an actionable mutation was later identified, one-third of physicians would not change the patient’s treatment or would only change it if the initial treatment was intolerable or led to disease progressionCitation15. Additionally, approximately 20%-32% of patients with actionable mutations in the US do not receive targeted therapiesCitation39,Citation40 Since physician choice to maintain patients on non-targeted therapy even after an actionable mutation is discovered was not taken into account in the current study, these findings likely represent a conservative estimate of the wasted healthcare expenditures from suboptimal 1 L treatment initiation.
Taken together, the present study demonstrates the lower costs and improved patient care associated with NGS relative to PCR testing strategies. When considered in the context of the prior literature describing the clinical repercussions of delayed targeted therapy, missed mutation detection, and initiation of suboptimal, non-targeted NSCLC therapy, these findings further emphasize the importance of using efficient and accurate mutation testing strategies that lead to rapid initiation of appropriate targeted therapy. Optimizing biomarker testing becomes increasingly relevant as additional targeted agents enter the NSCLC treatment landscape, including sotorasib (approved for KRAS G12C-mutated NSCLC)Citation41, fam-trastuzumab deruxtecan-nxki (approved for HER2-mutated NSCLC)Citation42, adagrasib (approved for KRAS G12C-mutated NSCLC)Citation43, and amivantamab-vmjw (approved for EGFR ex20ins-mutated advanced NSCLC after chemotherapy, and has demonstrated promising efficacy among patients with common EGFR and ex20ins-mutated EGFR advanced NSCLC in phase III clinical trials)Citation44–48. Real-world studies evaluating these novel targeted agents in clinical practice will provide valuable effectiveness data in the context of the current NSCLC therapeutic landscape. Future research should compare NGS versus PCR testing strategies, costs and clinical outcomes following biomarker testing and throughout the treatment journey to evaluate the longer-term clinical and economic benefits of NGS testing in patients with mNSCLC.
Limitations
Some limitations should be considered when interpreting these findings. Since the study was based on a modeling approach, some model inputs and assumptions were based on data available in published literature (e.g. rate of positive detection for each mutation) or on expert opinion (e.g. the proportion of patients using liquid NGS), and thus may be subject to a certain level of uncertainty or limited generalizability. For instance, costs associated with delayed care were approximated based on claims analyses evaluating costs in the pre-diagnosis phase among patients with lung cancerCitation22,Citation23 while wasted healthcare expenditures of suboptimal 1 L treatment were approximated based on a claims analysis reporting the incremental costs of initiating targeted therapy as second-line versus 1 LCitation25. While the current study evaluated costs associated with treatment initiated prior to receiving test results, these values may be underestimated as costs for treatment initiated prior to the start of testing were not incorporated, given the model time horizon began at the start of testing. Therefore, future real-world studies confirming these approximations are warranted. Additionally, the amount reimbursed for testing was estimated using either publicly available CMS information or commercial claims, so the results may not be generalizable to payers other than Medicare and commercial insurance or to countries outside of the US. Moreover, dual-eligible patients (with both Medicare and commercial coverage) were not considered in the model.
No restrictions were applied to the study population in terms of type of NSCLC (e.g. squamous or adenocarcinoma) even though guidelines recommend genetic testing in specific subgroupsCitation8; this was done based on expert opinion to avoid excluding patients without a definitive diagnosis of adenocarcinoma, who may still benefit from targeted therapy. In addition, patient smoking history and clinical and pathological information regarding disease histology were not considered in the model. Liquid biopsy was only considered for patients tested with NGS, despite the real-world availability of PCR assays for liquid biopsy for certain biomarkers. Moreover, DNA-based or RNA-based NGS was considered in the model, but not combined DNA- and RNA-based NGS, which may have led to a higher proportion of patients receiving a positive test result and higher costs of testing. Lastly, the sensitivity and specificity of the various testing strategies were not considered in this model.
Conclusion
The results of this model-based study suggest that NGS testing is associated with reduced costs to the health system and more rapid treatment with appropriate therapy relative to PCR testing strategies. Among patients with mNSCLC, the use of NGS resulted in more patients testing positive for a mutation with an approved targeted therapy and a shorter time to initiation of appropriate therapy relative to PCR testing strategies. The use of NGS was associated with cost savings compared to PCR strategies, with lower per-patient total costs of testing for patients tested with NGS regardless of insurance type. Furthermore, increasing the proportion of patients tested with NGS led to greater plan-level cost savings. Importantly, costs of inappropriate immunotherapy and/or chemotherapy initiation prior to receiving test results, as well as wasted expenditures of suboptimal 1 L treatment initiation due to missed detection of actionable mutations, are a significant component of increased costs associated with PCR testing strategies, relative to NGS testing. As such, policies that aim to address barriers associated with the clinical adoption of NGS warrant consideration.
Transparency
Author contributions
All authors were involved in the conception and design, or analysis and interpretation of the data; the drafting of the paper or revising it critically for intellectual content; and the final approval of the version to be published. All authors agree to be accountable for all aspects of the work.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Previous presentations
Part of the material in this manuscript was presented at the American Society of Clinical Oncology (ASCO) Annual Meeting held on June 2-6, 2023 in Chicago, IL, USA as a poster presentation.
Supplemental Material
Download MS Word (103 KB)Acknowledgements
Medical writing support was provided by a professional medical writer, Christine Tam, an employee of Analysis Group, Inc.
Declaration of funding
Financial support for this research was provided by Janssen Scientific Affairs, LLC, a Johnson & Johnson company.
Declaration of financial/other relationships
Christine M. Bestvina reports research funding to the institution from AstraZeneca and BMS, as well as personal consulting from AstraZeneca, BMS, CVS, Daiichi Sankyo, Genentech, Gilead, Jazz, JNJ, Mirati, Regeneron, Sanofi, Takeda, and Tempus. Dexter Waters, Andy He, and Julie Vanderpoel are employees of Janssen Scientific Affairs, LLC, a Johnson & Johnson company, and stockholders of Johnson & Johnson. Laura Morrison, Bruno Emond, Marie-Hélène Lafeuille, Annalise Hilts, and Patrick Lefebvre are employees of Analysis Group, Inc., a consulting company that has provided paid consulting services to Janssen Scientific Affairs, LLC, a Johnson & Johnson company, which funded the development and conduct of this study and manuscript.
Data availability statement
The data underlying this article are available in the article and in its online supplementary materials.
References
- Chevallier M, Borgeaud M, Addeo A, et al. Oncogenic driver mutations in non-small cell lung cancer: past, present and future. World J Clin Oncol. 2021;12(4):217–237. doi: 10.5306/wjco.v12.i4.217.
- Ganti AK, Klein AB, Cotarla I, et al. Update of incidence, prevalence, survival, and initial treatment in patients with non-small cell lung cancer in the US. JAMA Oncol. 2021;7(12):1824–1832. doi: 10.1001/jamaoncol.2021.4932.
- Chen R, Manochakian R, James L, et al. Emerging therapeutic agents for advanced non-small cell lung cancer. J Hematol Oncol. 2020;13(1):58. doi: 10.1186/s13045-020-00881-7.
- Vu P, Patel S. Non-small cell lung cancer targetable mutations: present and future. Precis Cancer Med. 2020;3:5–5. doi: 10.21037/pcm.2019.11.03.
- VanderLaan PA, Rangachari D, Majid A, et al. Tumor biomarker testing in non-small-cell lung cancer: a decade of change. Lung Cancer. 2018;116:90–95. doi: 10.1016/j.lungcan.2018.01.002.
- Ricciut B, Wang C, Rizvi H, et al. Abstract 102: clinicopathological and molecular characteristics, treatment patterns, and outcomes in patients with KRAS p.G12C-mutated metastatic non-small cell lung cancer (NSCLC) in the AACR project GENIE database. Cancer Res. 2021;81(13_Supplement):102–102. doi: 10.1158/1538-7445.AM2021-102.
- Kalemkerian GP, Narula N, Kennedy EB, et al. Molecular testing guideline for the selection of patients with lung cancer for treatment with targeted tyrosine kinase inhibitors: american society of clinical oncology endorsement of the college of American pathologists/international association for the study of lung cancer/association for molecular pathology clinical practice guideline update. J Clin Oncol. 2018;36(9):911–919. doi: 10.1200/JCO.2017.76.7293.
- Lindeman NI, Cagle PT, Aisner DL, et al. Updated molecular testing guideline for the selection of lung cancer patients for treatment with targeted tyrosine kinase inhibitors: guideline from the college of American pathologists, the international association for the study of lung cancer, and the association for molecular pathology. J Mol Diagn. 2018;20(2):129–159. doi: 10.1016/j.jmoldx.2017.11.004.
- Pennell NA, Arcila ME, Gandara DR, et al. Biomarker testing for patients with advanced non-small cell lung cancer: real-world issues and tough choices. Am Soc Clin Oncol Educ Book. 2019;39:531–542. doi: 10.1200/EDBK_237863.
- Raez LE, Brice K, Dumais K, et al. Liquid biopsy versus tissue biopsy to determine front line therapy in metastatic non-small cell lung cancer (NSCLC). Clin Lung Cancer. 2023;24(2):120–129. doi: 10.1016/j.cllc.2022.11.007.
- Lemmon CA, Zhou J, Hobbs B, et al. Modeling costs and life-years gained by population-Wide Next-Generation sequencing or single-gene testing in nonsquamous non-small-cell lung cancer in the United States. J Clin Oncol Precis Oncol. 2023;7:e2200294. doi: 10.1200/PO.22.00294.
- Pennell NA, Mutebi A, Zhou Z-Y, et al. Economic impact of next-generation sequencing versus single-gene testing to detect genomic alterations in metastatic non-small cell luncg cancer using a decision analytic model. J Clin Oncol Precis Oncol. 2019;3:1–9. doi: 10.1200/PO.18.00356.
- Vanderpoel J, Stevens AL, Emond B, et al. Total cost of testing for genomic alterations associated with next-generation sequencing versus polymerase chain reaction testing strategies among patients with metastatic non-small cell lung cancer. J Med Econ. 2022;25(1):457–468. doi: 10.1080/13696998.2022.2053403.
- Cheng MM, Palma JF, Scudder S, et al. The clinical and economic impact of inaccurate EGFR mutation tests in the treatment of metastatic non-small cell lung cancer. J Pers Med. 2017;7(3):5. doi: 10.3390/jpm7030005.
- Mileham KF, Schenkel C, Bruinooge SS, et al. Defining comprehensive biomarker-related testing and treatment practices for advanced non-small-cell lung cancer: results of a survey of U.S. oncologists. Cancer Med. 2022;11(2):530–538. doi: 10.1002/cam4.4459.
- Sheffield BS, Eaton K, Emond B, et al. Cost savings of expedited care with upfront Next-Generation sequencing testing versus single-gene testing among patients with metastatic non-small cell lung cancer based on current Canadian practices. Curr Oncol. 2023;30(2):2348–2365. doi: 10.3390/curroncol30020180.
- Robert NJ, Espirito JL, Chen L, et al. Biomarker testing and tissue journey among patients with metastatic non-small cell lung cancer receiving first-line therapy in the US oncology network. Lung Cancer. 2022;166:197–204. doi: 10.1016/j.lungcan.2022.03.004.
- Smith RE, Johnson ML, Gordan LN, et al. Evaluation of outcomes in patients (pts) with stage 4 non-small cell lung cancer (NSCLC 4) harboring actionable oncogenic drivers (AOD) when treated prior to report of mutation without tyrosine kinase inhibitors (TKI): an integra connect database (ICD) retrospective observational study. J Clin Oncol. 2022;40(16_suppl):1530–1530. doi: 10.1200/JCO.2022.40.16_suppl.1530.
- Metro G, De Giglio A, Ricciuti B, et al. Advanced non-small-cell lung cancer: how to manage EGFR and HER2 exon 20 insertion mutation-positive disease. Drugs Context. 2022;11:1–10. doi: 10.7573/dic.2022-3-9.
- Centers for medicare & medicaid services. Physician Fee Schedule. Baltimore (MD): Centers for Medicare & Medicaid Services; 2022.
- Centers for medicare & medicaid services. Clinical Laboratory Fee Schedule. Baltimore (MD): Centers for Medicare & Medicaid Services; 2022.
- Gildea TR, DaCosta Byfield S, Hogarth DK, et al. A retrospective analysis of delays in the diagnosis of lung cancer and associated costs. Clinicoecon Outcomes Res. 2017;9:261–269. doi: 10.2147/CEOR.S132259.
- Sheehan DF, Criss SD, Chen Y, et al. Lung cancer costs by treatment strategy and phase of care among patients enrolled in medicare. Cancer Med. 2019;8(1):94–103. doi: 10.1002/cam4.1896.
- Centers for Medicare & Medicaid Services. ASP Drug Pricing Files. Baltimore (MD): Centers for Medicare & Medicaid Services; 2022.
- Skinner KE, Fernandes AW, Walker MS, et al. Healthcare costs in patients with advanced non-small cell lung cancer and disease progression during targeted therapy: a real-world observational study. J Med Econ. 2018;21(2):192–200. doi: 10.1080/13696998.2017.1389744.
- Blumenthal G, Gong Y, Kehl K, et al. Analysis of time-to-treatment discontinuation of targeted therapy, immunotherapy, and chemotherapy in clinical trials of patients with non-small-cell lung cancer. Ann Oncol. 2019;30(5):830–838. doi: 10.1093/annonc/mdz060.
- Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non–small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi: 10.1056/NEJMoa1801005.
- U.S. Bureau of Labor Statistics. Consumer Price Index 2023 [cited 2023 April 21]. Available from: https://www.bls.gov/cpi/factsheets/medical-care.htm
- Brice K, Raez LE, Dumais K, et al. Liquid biopsies for the front line therapy decision in non-small cell lung cancer. J Clin Oncol. 2021;39(15_suppl):e21103–e21103. doi: 10.1200/JCO.2021.39.15_suppl.e21103.
- Nesline MK, Knight T, Colman S, et al. Economic burden of checkpoint inhibitor immunotherapy for the treatment of non-small cell lung cancer in US clinical practice. Clin Ther. 2020;42(9):1682–1698 e7. doi: 10.1016/j.clinthera.2020.06.018.
- Wong W, Sheinson D, Liu Y, et al. Costs associated with the use of multigene panel tests in three solid tumor types and the impact on insurance premiums. Future Oncol. 2023;19(10):705–714. doi: 10.2217/fon-2023-0094.
- Stewart DJ, Maziak DE, Moore SM, et al. The need for speed in advanced non-small cell lung cancer: a population kinetics assessment. Cancer Med. 2021;10(24):9040–9046. doi: 10.1002/cam4.4411.
- Sheinson D, Wong WB, Wu N, et al. Impact of delaying initiation of anaplastic lymphoma kinase inhibitor treatment on survival in patients with advanced non-small-cell lung cancer. Lung Cancer. 2020;143:86–92. doi: 10.1016/j.lungcan.2020.03.005.
- Goulart BHL, Chennupati S, Fedorenko CR, et al. Access to tyrosine kinase inhibitors and survival in patients with advanced EGFR(+) and ALK(+) positive non-small-cell lung cancer treated in the real-world. Clin Lung Cancer. 2021;22(5):e723–e733. doi: 10.1016/j.cllc.2021.01.019.
- Levy BP, Nguyen D, Shih Y-H, et al. Association between real-world, upfront, next-generation sequencing and overall survival (OS) in advanced non–small-cell lung cancer (aNSCLC) in the United States. J Clin Oncol. 2023;41(16_suppl):9117–9117. doi: 10.1200/JCO.2023.41.16_suppl.9117.
- Gainor JF, Shaw AT, Sequist LV, et al. EGFR mutations and ALK rearrangements are associated with low response rates to PD-1 pathway blockade in non-small cell lung cancer: a retrospective analysis. Clin Cancer Res. 2016;22(18):4585–4593. doi: 10.1158/1078-0432.CCR-15-3101.
- Lisberg A, Cummings A, Goldman JW, et al. A phase II study of pembrolizumab in EGFR-Mutant, PD-L1+, tyrosine kinase inhibitor naive patients with advanced NSCLC. J Thorac Oncol. 2018;13(8):1138–1145. doi: 10.1016/j.jtho.2018.03.035.
- Scott JA, Lennerz J, Johnson ML, et al. Compromised outcomes in stage IV non-small-cell lung cancer with actionable mutations initially treated without tyrosine kinase inhibitors: a retrospective analysis of real-world data. J Clin Oncol Oncol Pract. 2023;20(1):145–153. doi: 10.1200/op.22.00611.
- Steuten L, Goulart B, Meropol NJ, et al. Cost effectiveness of multigene panel sequencing for patients with advanced non-small-cell lung cancer. J Clin Oncol Clin Cancer Inform. 2019;3:1–10. doi: 10.1200/CCI.19.00002.
- Vashistha V, Armstrong J, Winski D, et al. Barriers to prescribing targeted therapies for patients with NSCLC with highly actionable gene variants in the veterans affairs national precision oncology program. J Clin Oncol Oncol Pract. 2021;17(7):e1012–e1020. doi: 10.1200/OP.20.00703.
- U.S. Food & Drug Administration. FDA grants accelerated approval to sotorasib for KRAS G12C mutated NSCLC 2021 [cited 2023 June 29]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-sotorasib-kras-g12c-mutated-nsclc
- U.S. Food & Drug Administration. FDA grants accelerated approval to fam-trastuzumab deruxtecan-nxki for HER2-mutant non-small cell lung cancer 2022 [cited 2023 June 29]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-fam-trastuzumab-deruxtecan-nxki-her2-mutant-non-small-cell-lung
- U.S. Food & Drug Administration. FDA grants accelerated approval to adagrasib for KRAS G12C-mutated NSCLC 2022 [cited 2023 June 29]. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-adagrasib-kras-g12c-mutated-nsclc.
- Janssen Biotech, Inc. RYBREVANT® (amivantamab-vmjw) Highlights of Prescribing Information 2022 [cited 2023 May 30]. Available from: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/RYBREVANT-pi.pdf.
- Park K, Haura EB, Leighl NB, et al. Amivantamab in EGFR exon 20 Insertion-Mutated non-small-cell lung cancer progressing on platinum chemotherapy: initial results from the CHRYSALIS phase I study. J Clin Oncol. 2021;39(30):3391–3402. doi: 10.1200/JCO.21.00662.
- Girard N, Park K, Tang K, et al. LBA5 amivantamab plus chemotherapy vs chemotherapy as first-line treatment in EGFR exon 20 insertion-mutated advanced non-small cell lung cancer (NSCLC): primary results from PAPILLON, a randomized phase III global study. Annal Oncol. 2023;34: s 1304. doi: 10.1016/j.annonc.2023.10.060.
- Cho BC, Felip E, Spira AI, et al. LBA14 amivantamab plus lazertinib vs osimertinib as first-line treatment in patients with EGFR-mutated, advanced non-small cell lung cancer (NSCLC): primary results from MARIPOSA, a phase III, global, randomized, controlled trial. Annal Oncol. 2023;34: s 1306. doi: 10.1016/j.annonc.2023.10.062.
- Passaro A, Wang J, Wang Y, et al. Amivantamab plus chemotherapy with and without lazertinib in EGFR-mutant advanced NSCLC after disease progression on osimertinib: primary results from the phase 3 MARIPOSA-2 study. Annal Oncol. 2023;35:77–90. doi: 10.1016/j.annonc.2023.10.117.