

SY-02-03
MONITORING OSTEOPOROSIS TREATMENT
T. J. De Villiers
Panorama MediClinic and University of Stellenbosch, Cape Town, South Africa
Osteoporosis treatment is aimed at the prevention of fragility fractures in individuals at high risk of fracture. Poor compliance to therapy is a problem. As osteoporosis is a silent disease, response to treatment is monitored by the measurement of surrogate markers of fracture.
Bone mineral density (BMD) measurement by DXA is well established as a determinant of fracture risk in the untreated patient. The serial measurement of BMD with the aim of monitoring patients on treatment, unfortunately has serious pitfalls:
Serial measurements performed by different operators and different machines are flawed by individual variations in precision. The least significant change in BMD needs to be calculated for individual operators and machines. Typically a change in BMD of at least 3.8% (hip) and 2.4% (spine) is needed to be of any significance. Currently available therapies are not expected to result in significant improvement within 1 year (spine) or 18 months (hip).
Regression to the mean predicts that patients with unusual responses to treatment might represent outliers who are likely to have more typical responses if treatment is continued without change. It has been suggested by Cummings et al that most women who lose BMD during the first year of treatment will gain BMD if the same treatment is continued for a year.
Placebo controlled clinical trials have indicated that absolute changes in BMD do not reflect fracture risk, as the reduction in fracture risk is expressed relative to controls. Even patients who lose bone on treatment have a lower fracture risk compared to patients on no treatment.
BMD does not take into account effects on cortical thickness, cortical porosity or trabecular connectivity.
Different drugs have different effects on BMD.
Bone turnover markers can indicate suppression of bone turnover as early as 3 months, before changes in BMD occur. Although early suppression may correlate with fracture risk reduction, the information is more useful as an indicator of early adherence to therapy and may be used to improve persistence.
Vertebral fracture assessment by DXA is the most meaningful monitoring tool available at present, as an accurate assessment of incident vertebral fractures can be made.
Until new in vivo measurements of bone strength becomes available, monitoring osteoporosis treatment and clinical decisions will have to rely on the integration of surrogate markers with the clinical fracture risk of the individual patient.
SY-02-04
THE DECISION TO TREAT OR NOT TO TREAT
René Rizzoli (Switzerland)
Abstract not available at the time of going to press.
SY-03: Androgens and female sexual dysfunction
Supported by an unrestricted grant from P&G
SY-03-01
ANDROGEN THERAPY IN WOMEN: WHAT DO WE KNOW?
Susan R. Davis
Monash University, Melbourne, Victoria Australia
Published studies suggest that the prevalence of sexual problems among women ranges from 9% to 43%. The most commonly reported sexual problems in women relate to desire, arousal, pleasure and global satisfaction with these symptoms being common after natural menopause and bilateral oophorectomy. This may be due to a mixture of climacteric symptoms and for many women, improvement in general well-being achieved with symptom amelioration by estrogen therapy, will positively influence sexual functioning.
The role of androgens in treatment of female sexual function and dysfunction remains controversial. There is no valid biochemical definition for “androgen deficiency” in women and this has presented a major obstacle for clinicians in this field. Several large randomized placebo-controlled clinical trials involving naturally and surgically postmenopausal women presenting with low libido demonstrate that testosterone therapy, with and without concurrent estrogen therapy, improves the quality of the sexual experience, with preliminary data that this may also apply to premenopausal women.
The assessment of the woman presenting with low sexual wellbeing requires a comprehensive clinical evaluation with a full medical and psycho-social history and physical examination.
A pragmatic concern is which women are suitable candidates for testosterone therapy, as not all women will benefit. As yet no clinically applicable diagnostic algorithm has achieved acceptance. A low serum testosterone level is not predictive of a diagnosis of low libido nor does it predict likelihood of therapeutic response. In most instances, only a trial of therapy will identify responders. However, an analysis of data from a number of clinical studies combined indicates that women with a sex hormone binding globulin (SHBG) level above 160nmol/L or women taking concurrent conjugated equine estrogen (CEE) are unlikely to benefit from testosterone therapy. The former is because testosterone binds SHBG with high affinity, such that having an elevated SHBG results in a very low free or bioavailable testosterone. The interaction between CEE therapy and exogenous testosterone is unclear, but it may be that a component of CEE interferes with the binding of testosterone to the androgen receptor in addition to increasing SHBG.
Testosterone treatment is well tolerated in studies of up to 12 months duration, with the main adverse effects being increased hair growth and acne, and with oral testosterone, suppression of HDL-cholesterol. No long term safety data for the use of testosterone in women is as yet available. Thus consideration of treatment of a woman with testosterone therapy must involve patient education including information that not all women respond to therapy and the uncertainty of the long term safety.
SY-03-02
SAFETY OF ANDROGEN THERAPY IN WOMEN: WHAT DO WE KNOW?
James A. Simon
George Washington University, Washington, DC, USA
Objective: To review the published data concerning the safety of androgen or testosterone administration to postmenopausal women.
Design and Methods: The safety of menopausal androgen therapy has been questioned since these compounds became available 50 years ago. This sentiment has been recently reiterated by the US Food and Drug Administration (FDA, 2004). Although it is acknowledged that androgen excess carries the common cosmetic risks of hirsuitism, and acne, safety concerns over long-term therapy at physiological levels have focused on potential cardiovascular disease, breast cancer and endometrial cancer. The basis for these concerns stems from epidemiological evidence suggesting higher risks of these endpoints in women with endogenous androgen excess syndromes, like polycystic ovary syndrome (PCOS), the earlier risk of cardiovascular disease in men compared with women, and a generalized paranoia over hormone therapy of all kinds arising from the Women's Health Initiative (WHI). This review is based upon the published English language literature identified by a search of standard databases and bibliographies identified as dealing with the topics of androgen or testosterone treatment of postmenopausal women, and a careful analysis of the results of ongoing randomized clinical trials.
Results: These searches identified the major adverse reactions to exogenous androgens to be the expected cosmetic side effects of hirsuitism and acne. While PCOS may serve as a potential model of risk for menopausal androgen therapy, this model suffers from several fundamental deficiencies that do not necessarily affect postmenopausal women. These include: hyperinsulinemia, obesity, hyperlipidemia, and the metabolic syndrome. While men do develop cardiovascular disease at an earlier chronological age than women, many aspects of cardiovascular fitness are actually improved in hypogonadal men by physiological testosterone supplementation. While high-density lipoprotein (HDL) levels may be decreased with oral androgen therapy suggesting increased cardiovascular risk, HDL concentrations appear unaffected by non-oral regimens.
Conclusion: There are currently insufficient long-term safety data regarding cardiovascular disease, breast cancer and endometrial cancer to draw strong conclusions, although the data available to date are extremely reassuring. Testosterone administration to postmenopausal women that result in physiological to slightly supraphysiological serum-free testosterone concentrations appear to be safe for at least 2–3 years. Ongoing randomized clinical trials to definitively address safety concerns will also be reviewed to the degree that data are available at the time of presentation.
SY-03-03
SPECIAL ASPECTS OF BREAST SAFETY WITH ANDROGEN THERAPY
Bo von Schoultz
Department of Obstetrics and Gynaecology, Karolinska Hospital, Stockholm, Sweden
There is increasing interest in the role of androgens in the treatment of women but little is known about the long-term safety. There are also very few studies on testosterone therapy and breast cancer risk. Some observational data suggest postmenopausal women with high plasma levels of testosterone to have an increased risk of breast cancer, while other studies have found no such association. The interpretation of available data is complex and studies differ by e.g. methods for testosterone measurement, calculation of free testosterone and adjustment for estrogen status. Dimitrakakis et al found no increase of breast cancer in a group of postmenopausal women when testosterone was added to HT, during a mean follow-up of 5.8 years. In contrast, recent data from the Nurses Health Study suggest combined estrogen/testosterone to be associated with an increased risk. On the other hand, there are some observations to suggest that androgens may counteract the stimulatory effects of estrogen and progestogen in the mammary gland. Human studies on the effects of testosterone on the breast have been hampered by the lack of preparations suitable for women. However, a transdermal patch releasing 300 μg of testosterone per day, is currently available for clinical trials in postmenopausal women. Mammographic breast density and breast cell proliferation could be regarded as surrogate markers for the risk of breast cancer. In a six months prospective double blind trial postmenopausal women were given continuous combined estradiol 2 mg/norehisterone acetate 1 mg and were equally randomized to receive additional treatment with either the testosterone patch or a placebo patch. Breast cells were collected by fine needle biopsies at baseline and after six months. In the placebo group and in agreement with previous reports there was a more than five-fold increase in total breast cell proliferation from baseline to six months. In contrast, during testosterone addition no significant increase in breast cell proliferation was recorded. The different effects of the two treatments were apparent in both epithelial and stromal breast cells. Further more among women participating in the Aphrodite trial transdermal testosterone therapy over fifty-two weeks was found to have no significant effect on digitally quantified mammographic density. These results indicate that testosterone may not stimulate the breast also in women not using concurrent estrogen.
SY-03-04
FINDING THE RIGHT PATIENT: HSDD IN WOMEN – HOW DO WE KNOW?
Alessandra Graziottin
Director, Center of Gynecology and Medical Sexology, H. San Raffaele Resnati, Milano Italy
Background: Women's sexual desire is dependent on biological, psychosexual, and context-related factors. Epidemiological data indicate that sexual desire decreases gradually with age, from 19% in european women aged 20–49, to 48% in the age cohort 50–70; however, the distress associated with loss ofdesire decreases with age. The menopause has an incremental negative effect on a woman's sexuality separate from the change brought about by aging. Surgical menopause significantly increases the percentage of women with low desire in the age cohort of 20–49 (from 19 to 32%).
The Hypoactive Sexual Desire Disorder (HSDD) is defined by a loss of motivation and/or drive to be sexual, which causes asignificant personal distress. It affects from 5 to 9.5% of women. HSDD is the most frequent complaint in women.
Aim of the presentation: defining the identikit of women affected by HSDD who require clinical help.
Method: literature review plus Author's clinical experience.
Results: women affected by HSDD are usually young (the younger the woman the higher the probability that low desire is distressing to her and her partner); are frequently overstressed, because of the increasing demands on multiple fronts (family, work, children) and chronic shortage of sleep; have undergone premature menopause, either spontaneous (Premature Ovarian Failure, POF) or iatrogenic: surgical, chemotherapeutic or radiotherapeutic; have frequent comorbidities: medical, with depression, anxiety, chronic diseases, urinary incontinence, chronic pelvic pain; sexual, with arousal disorders, orgasmic disorders, sexual pain disorders;contextual, with relational problems, mainly loss of feelings for partner, partner's health and/or sexual problems, andsocial issues, such as poor economic conditions, poor education, poor medical and social support.
Low testosterone levels (lower quartile of, or under, the normal range of free testosterone of the examining lab.) may suggest a biological basis of HSDD., the so called “Androgen Insufficiency Syndrome, AIS”.
Leading symptoms of AIS, although elusive, include low desire, low vital energy, low assertiveness, low mood, lower muscle strength, poor genital arousal, increased orgasmic difficulties, poor orgasm or loss of it.
A critical issue is that many genital conditions causing poor genital arousal (such as vaginal dryness), and/or pain(lichen sclerosus, vulvar vestibulitis, vulvodynia, endometriosis, recurrent or post-coital cystitis, anismus) may secondarily cause loss of desire, unless specifically diagnosed and treated.
Conclusion: HSDD affects a significant proportion of women. It has a multifactorial etiology. Appropriate clinical history, accurate genital exam and minimal lab tests may well identify women with HSDD who need clinical help.
SY-04: Effects of hormone deprivation and hrt on the female brain
SY-04-01
BRAIN STEROIDOGENESIS: IMPLICATIONS FOR HORMONE THERAPY
L. M. Garcia-Segura
Instituto Cajal, CSIC, Madrid, Spain
In addition to the classical reproductive roles of brain aromatase, its activity may also modulate mood, affective status, non-reproductive behaviors and cognition. Under physiological conditions, brain aromatase activity is rapidly regulated by synaptic inputs and in turn the enzyme regulates brain plasticity, synaptic function and the processing of information by neuronal circuits. In addition, under pathological conditions, aromatase expression, estradiol synthesis and estrogen receptor levels are up-regulated in reactive astroglia at sites of neurodegeneration. In rodents, genetic or pharmacological inhibition of brain aromatase results in marked neuronal death after different forms of mild neurodegenerative stimuli that do not compromise neuronal survival under control conditions. This finding strongly suggest that local formation of estradiol in the brain is neuroprotective and that the induction of aromatase and the consecutive increase in the local production of estradiol are part of the program triggered by the neural tissue to cope with neurodegenerative insults. Proteins involved in the intra-mitochondrial trafficking of cholesterol, the first step in steroidogenesis, such as the translocator protein 18kDa (TSPO) and the steroidogenic acute regulatory protein (StAR), are also up-regulated in the brain after injury, together with the first enzyme in the steroidogenic pathway (P450scc). This suggests that brain steroidogenesis may be modified in adaptation to neurodegenerative conditions. Recent studies have shown that TSPO ligands that increase brain steroidogenesis are neuroprotective and reduce reactive gliosis and neurodegeneration. Therefore, StAR, TSPO and aromatase are attractive pharmacological targets to promote brain protection. Furthermore, these findings suggest that the neurological outcome of hormone therapy may be affected by the endogenous steroidogenic activity of the brain. Supported by Ministerio de Educación y Ciencia, Spain (SAF 2005‐00272) and the European Union (EWA project: LSHM-CT‐2005‐518245).
SY-04-02
HORMONE THERAPY AND THE EARLY POSTMENOPAUSE
P. M. Maki
University of Illinois at Chicago, Chicago Illinois USA
Twenty years ago, Barbara Sherwin first reported that surgical menopause leads to declines in verbal memory and estrogen prevents those declines. This presentation provides an overview of how our understanding of estrogen and cognitive function has evolved in the 20 years since that seminal report. A systematic review of clinical trials suggests that early treatment may be necessary to maintain verbal memory, a cognitive ability that favors women over men. There is growing evidence from randomized clinical trials that while estrogen confers cognitive benefits, certain formulations of estrogen and progesterone have a negative impact on verbal memory and other cognitive functions, even early in the menopausal transition. This negative impact on verbal memory is likely due to anti-estrogenic properties of certain progestins in the hippocampus, a brain structure that is critical for memory. Early beneficial effects of estrogen appear to be largely dependent on its beneficial effects on cholinergic function. Animal models and human psychopharmacological studies indicate that the cholinergic mechanism of action depends on the timing of estrogen treatment. Neuroimaging studies in women demonstrate direct effects of estrogen on the hippocampus, prefrontal cortex, and other brain areas that subserve verbal memory. In addition to these direct effects on the brain, estrogen therapy might improve verbal memory by decreasing hot flashes and improving sleep. Women with vasomotor symptoms underreport their symptoms by as much as 45%, and new data from our laboratory provide evidence that verbal memory performance relates to the true number of objective hot flashes women experience but not to the number of hot flashes they report. These findings suggest that physiological rather than psychological correlates of vasomotor symptoms are related to memory decline. Thus, hormone therapy might improve cognition through both indirect (i.e., symptom improvement) and direct mechanisms (i.e., cholinergic function, hippocampal and prefrontal function). Since Sherwin's initial finding, our understanding of estrogen and brain function has evolved considerably, but there is not yet sufficient evidence to promote the use of estrogen for the treatment of cognitive complaints. As the literature evolves, it appears that her initial study identified the clinical group that might most benefit immediately and in the long-term from estrogen therapy. Our attempts to generalize her results to other clinical samples (i.e., naturally menopausal women, older women), other cognitive domains (i.e., attention, non-verbal memory), and other hormone formulations (i.e., certain estrogen plus progestin formulations) might not be as successful.
SY-04-03
ALZHEIMER'S DISEASE AND ESTROGEN REVISITED
V. W. Henderson
Stanford University, Stanford, California, United States
The ability to learn and recall new information (episodic memory) is adversely affected during normal aging. Importantly, impairment in this cognitive domain is associated with increased risk of Alzheimer's disease. Effects of estrogen-containing hormone therapy on this form of memory and on other aspects of cognition have been examined in several large, randomized, double-blind, placebo-controlled trials. Most have involved older, healthy postmenopausal women, and results of this research support the view that hormone therapy initiated after about age 60 does not substantially benefit or harm mean cognitive performance over intervals of up to five years. Key histopathological characteristics of Alzheimer's disease are neurofibrillary tangles and neuritic plaques. However, it is becoming increasingly evident that tangles and plaques are more likely to result in dementia in the presence of other forms of cerebral pathology, particularly including ischemic changes of cerebrovascular disease. Biochemical hallmarks of Alzheimer's disease are the deposition within the brain of beta-amyloid protein and the hyperphosphorylation of tau protein; in animal models estradiol reduces beta-amyloid formation as well as tau phosphorylation. Other hormonal actions (e.g., on coagulation, inflammatory makers and the vasculature) act in ways that might increase dementia risk in some clinical settings. It is not yet possible to reconcile results of the Women's Health Initiative Memory Study trials (increased dementia risk from hormone use after age 64) and observational studies (generally associated with reduced Alzheimer risk from hormone use before this age). It is possible that healthy-user bias and recall bias account for these associations in observational research. However, recent evidence linking coronary heart disease to timing of hormone use in relation to menopause or to age of hormone use raises the possibility of a similar critical window with regard to Alzheimer's disease. Could early hormone use reduce Alzheimer risk in old age (as implied by observational studies) but late use increase dementia risk (as demonstrated in the Women's Health Initiative Memory Study)? Two ongoing clinical trials in the United States (ELITE and KEEPS) will provide additional insight on cognitive consequences of early hormone therapy use. However, neither study is designed to provide clear answers regarding late-life dementia after early hormone use. Because of the extraordinary difficulty in obtaining unbiased data (for example, through a clinical trial of hormone therapy begun during the early postmenopause with a follow-up period of two decades), it is unlike that this important issue can soon be resolved.
SY-04-04
THE PROS AND CONS OF NON-HRT THERAPIES ON THE BRAIN
Frederick Naftolin (USA)
Abstract not available at the time of going to press.
SY-05: Primary cardiovascular prevention in perimenopausal women
Supported by an unrestricted grant from Bayer-Schering.
SY-05-01
ARE WOMEN EXCLUDED FROM THE 2007 ESH/ESC GUIDELINES FOR THE MANAGEMENT OF HYPERTENSION?
Stéphane Laurent
Georges Pompidou European Hospital and INSERM U872, University Paris-Descartes, Paris, France
To the question “Are women excluded from the 2007 ESH/ESC guidelines for the management of hypertension?”, the best answer that the writing committee of the ESH/ESC Guidelines for the Management of Hypertension (Mancia G et al. J Hypertens 2007,25:1105–87) can give is: “Certainly not!”. Indeed, primary cardiovascular prevention in perimenopausal women is of outmost importance. Hypertension is a powerful risk factor for stroke and coronary heart disease in women. The prevalence of coronary heart disease increases markedly in women after the menopause. Mortality from cardiovascular disease has been steadily decreasing for men, but the same is not true for women.
Although women typically have lower systolic blood pressure (BP) levels than men in the 30 to 44 year age groups, their systolic BP rises more steeply with age than in males, which means that at or beyond 60 years of age, women have a higher BP and greater prevalence of hypertension. Between the ages of 40 and 69 years, each difference in systolic BP of 20 mmHg is associated with a two-fold difference in the rate of cardiovascular death. The cardiovascular risk is increased not only at high BP levels, but also at BP levels generally considered by physicians as normal.
The beneficial effect of antihypertensive treatment versus placebo was found to be similar in the two genders, as exemplified in a meta-analysis of individual patients. No gender-based meta-analysis has yet been made of trials comparing different active treatments but most studies have shown similar risk reductions by the various regimens in either gender group, with the exception of the ANBP 2 trial, which reported the benefit of enalapril- over the hydrochlorothiazide- based treatment to be limited to males, and the VALUE trial, which reported amlodipine to be more effective than valsartan in lowering blood pressure and reducing cardiac events in women but not in men.
Successful implementation of guidelines requires awareness of the barriers interposed between recommendations and practice: Doctors who are correctly aware that their task is to manage individuals, so often different from each other, while guidelines, by necessity, are dealing with a medical condition in general; Patients who have to adhere to lifestyle changes and be compliant with long term multiple drugs treatment; And health providers, who sometimes wrongly consider the management of hypertension as the matter of few minute visits, and reimburse doctors accordingly.
SY-05-02
DO WE HAVE A POCKET GUIDE FOR CARDIOVASCULAR PREVENTION IN PERI-AND POSTMENOPAUSAL WOMEN?
Peter Collins
Royal Brompton Hospital and Imperial College London, London, UK
“Gynaecologists and general practitioners are in a unique position to be able to impact on the future risk of CVD, the commonest cause of death of women in the industrialized world.”
Cardiovascular risk is poorly managed in women, especially during the menopausal transition when susceptibility to cardiovascular events increases. Clear gender differences exist in the epidemiology, symptoms, diagnosis, progression, prognosis and management of cardiovascular risk. Key risk factors that need to be managed in the peri-menopausal woman are hypertension, dyslipidaemia, obesity and other components of the metabolic syndrome, with the avoidance or careful control of diabetes. Hypertension is a particularly powerful risk factor and lowering of blood pressure is pivotal. Both gynaecologists and cardiovascular physicians have an important role to play in identifying peri-menopausal women at risk of cardiovascular morbidity and mortality and should work as a team to identify and manage risk factors such as hypertension.
Recently a consensus paper generated by a meeting of European cardiovascular physicians and gynaecologists was published (Collins et al, Management of cardiovascular risk in the peri-menopausal woman: a consensus statement of European cardiologists and gynaecologists. Eur. Heart J. 28 (16):2028–2040, 2007.) It emphasizes the need to identify and manage cardiovascular risk factors in menopausal women at the time of the menopausal transition, often a time before overt cardiovascular disease (CVD) is evident but at a time when timely management and intervention can decrease the long-term risk of developing CVD. The gynaecologist and primary care physician are in a prime position to assess these risk factors, but often they are not adequately addressed and managed, resulting in exposure of this excess risk to women over many years.
As a follow up to this publication a practical guide for menopausal physicians to aid the identification and management of cardiovascular risk in peri- and postmenopausal women has been produced by the same group of cardiovascular and gynaecological physicians in collaboration with the European Society of Cardiology and the International Menopause Society. It is hoped the guide will fill an unmet need for awareness and management strategies that will enable physicians to reduce the burden of CVD in menopausal women.
SY-05-03
IS CARDIOVASCULAR RISK IN POSTMENOPAUSAL WOMEN POORLY ASSESSED?
Santiago Palacios
Objective:The objective of this study was first to understand the current practice in the assessment of the management of cardiovascular risk (CV) factors by gynecologists. Secondly, to evaluate the need for tools to assess CV risk factors and, finally, to have a guide development of these tools by revealing needs, and better understanding the reasons for CV risk assessment and management practice by gynecologists.
Design & Method: It was an on-line survey given to 672 physicians from France, Germany, Italy, Spain, UK and USA. The majority were gynecologists except in the UK, where there were GP's as well. The sample was based on a database of the market research institute and randomly drawn. The screening criteria to choose the physicians, were: to have equal or more than 3 years of experience, to have equal or more than 20 patients with menopausal symptoms per month (except in the UK which was equal or more than 10) and to have equal or more than 5 prescriptions of HRT per month.
Results:Unaided, only 20% of gynecologists mentioned that the measurement of blood pressure is a standard assessment for postmenopausal women. An unspecified examination of cardiac health/CV risk was mentioned by 10%. When questioned about major indicators used to assess CV risk, physicians mentioned blood pressure (56%), patient history (45%), blood lipid panel (42%) and BMI (41%).
More than 1/3 of physicians are not aware of any guidelines from cardiology societies for assessment and management of cardiovascular risks. Only about every second gynaecologists can correctly state the systolic blood pressure levels corresponding to the BP class ‘high normal blood pressure’.
In cases when physicians do not measure factors that are perceived as easy to assess (e.g. diabetes), the main reason is an attitude of not being responsible for these factors.
Conclusion: Education on assessment and management of CV risk for the gynecologist should be fostered.
Acknowledgments: The survey has been funded by a grant from Bayer Schering Pharma.
SY-05-04
TRANSLATION OF THE GUIDELINES INTO THE CLINICAL PRACTICE
Margaret Rees (United Kingdom)
Abstract not available at the time of going to press.
SY-06: Future trends in menopause management
SY-06-01
LOW DOSE-ULTRA LOW DOSE: WHERE ARE THE LIMITS OF HRT
Marco Gambacciani
Dipartimento di Ostetricia e Ginecologia, Centro della Menopausa, Azienda Ospedaliera Universitaria Pisana, Via Roma 67, 56100 Pisa. Tel 05099238, fax 050 993058, email [email protected]
The limits of HRT are related to the benefit/risk ratio. Estrogen deficiency is a key factor in the pathogenesis of postmenopausal symptoms and osteoporosis. Postmenopausal administration of hormones has been used both to avoid symptoms and to prevent osteoporosis. The use of HRT for is based on biology, epidemiology, animal and preclinical data, observational studies and randomized clinical trials. The minimum effective dose of HRT has been questioned. At present, the regimens containing 1 mg micronized oral 17β estradiol or 0.45 mg conjugated equine estrogens are considered low-dose HRT (LD-HRT). Various studies have assessed the efficacy LD-HRT in the prevention of osteoporosis in postmenopausal women, while providing symptomatic relief from subjective symptoms associated with menopause and improving quality of life (QoL). Recent studies further evaluated the effects of LD-HRT in normal young postmenopausal women receiving low-dose continuous combined HRT (LD-HRT) containing 1 mg 17β estradiol or 0.5 mg of 17β estradiol (Ultra low dose, Ultra-LD-HRT) along with corresponding progestogen doses. Analogous studies have been conducted with preparations containing 0.3 mg conjugated equine estrogens. Menopausal symptoms, bleeding profiles, lipid pattern, bone mineral density (BMD) and bone turnover were assessed. LD-HRT and Ultra-LD-HRT were both effective in reducing menopausal clinical symptoms. BMD showed a significant increases vs placebo/calcium control groups either at the spine and femoral sites. LD-HRT and Ultra-LD-HRT can alleviate subjective symptoms providing an effective protection against the postmenopausal decrease of BMD. The benefit/risk ratio and the continuation rate seem to be more favourable for LD- and Ultra LD-HRT than standard HRT doses. Attention of clinical researchers should focus on the effects of lower dosage estrogen on osteoporotic fractures and other health outcomes.
SY-06-02
SERMS: WHAT'S NEW?
A. Cano
University of Valencia, Valencia, Spain
Selective Estrogen Receptor Modulators (SERMs) bind to the estrogen receptor to achieve a full array of stimulatory or inhibitory effects. The versatility is dependent on the compound as well as on the target tissue. This mutable functional profile is at the base of the concept of the ideal SERM, which should behave as agonistic or antagonistic as a result of the required circumstances. The properties of this ideal molecule are defined by its behaviour in areas where estrogens have demonstrated significant activity, mainly osteoporosis, endocrine cancer, cardiovascular disease, and central nervous system. In fact, the increased knowledge on the mechanisms of the susceptible diseases is being used in structure-activity studies aiming at the optimization of the design of new SERMs. The clinical data obtained with the wide use of tamoxifen, and particularly raloxifene, have been also used as a referent for identifying areas for improvement. The novelty in SERMs, therefore, concentrates in two main fields. Firstly, there are a few compounds that have demonstrated functional profiles of interest in experimental models. This has paved the way for advancing into the clinical step, with trials whose preliminary results are already available. Most of the interest has converged on arzoxifene, bazedoxifene, and lasofoxifene. Given the progress brought about by raloxifene, the new compounds have been challenged for increased power in osteoporosis and for more protective changes in cardiovascular parameters, while still preserving the profile of raloxifene in breast and endometrium. Secondly, there is a considerable interest in a better understanding of the role of raloxifene in areas such as cardiovascular disease. This is an objective close to that recently achieved for estrogens that, under certain conditions, have been confirmed as protective in atherogenesis. Consistent evidence suggests that raloxifene, and probably other SERMs, may exhibit some level of protection too. There is information confirming their role as limiting factors in the oxidative susceptibility of LDL. Moreover, there is a series of findings favouring a protective effect on endothelium, a crucial agent in the initiation of atherosclerosis. There is a potent agonistic effect on the production of nitric oxide and prostacyclin as well as on the promotion of endothelial proliferation, a key factor for endothelial regeneration.
SY-06-03
NEW TREATMENTS FOR MENOPAUSAL SYMPTOMS
M. Hickey
School of Women's and Infants' Health, University of Western Australia, Australia
Finding an effective and safe non-hormonal treatment for menopausal symptoms has been a long-standing goal for breast cancer patients and is increasingly requested by the larger population of women.
Vasomotor symptoms, in particular hot flashes and night sweats affect around 80% of women during the menopause and are the most common reason for women to seek treatment for symptoms. Symptomatic vaginal atrophy affects around 40% of women, and unlike hot flashes may persist or even worsen over time. Sexual dysfunction and depression are also associated with the menopause transition
Estrogen, ± progestogen has been used for many years for the relief of vasomotor symptoms and vaginal dryness and appears highly effective for many women. However, for those who wish to avoid estrogen the options have been limited. Tibolone is an effective alternative but carries similar contraindications to estrogen.
New developments in non-hormonal treatments have indicated that the SSRI paroxetine, the SNRI venlafaxine and the anti-convulsant gabapentin indicate that these medications show moderate efficacy, at least in the short term, in the treatment of vasomotor symptoms. In one study, gabapentin was equally effective as oestrogen in the reducing the frequency and severity of hot flashes. Other SSRI have shown limited efficacy. Each of these therapies is associated with side-effects which may limit their clinical use. Clonidine has shown very limited efficacy and a there is no good evidence that the “natural” therapies tested to date are effective.
Few studies have addressed the role of non-hormonal therapies in the treatment of other menopausal symptoms apart from hot flashes.
It is anticipated that new studies addressing the mechanisms of hot flashes will indicate novel directions for targeted therapies in this rapidly developing area.
SY-06-04
GLOBAL QUALITY OF LIFE AND RISK: BENEFIT OF MENOPAUSAL HORMONE THERAPY
Wulf H. Utian
Executive Director, NAMS; Consultant in Women's Health, the Cleveland Clinic; Professor Emeritus, Reproductive Biology and Obstetrics and Gynecology, Case Western Reserve University; Cleveland, Ohio, USA
Quality of Life (QOL) is the ultimate outcome expected of any successful medical intervention. Unfortunately it is usually not considered, or is not precisely defined or measured. This has resulted in confusing and often misleading conclusions in multiple publications reporting on menopausal hormone therapy (MHT) and QOL, including those coming from the writing groups of large studies such as the Heart and Estrogen Replacement Study (HERS) and the Women's Health Initiative (WHI).
Health-related QOL and global QOL are quite different and are accurately defined in the literature. Moreover, current instruments for measuring them are available. The limited available valid studies relating impact of risk and benefit of MHT on global QOL will be outlined. It can be shown, despite the paucity of directly measured QOL data, that MHT has a benefit on both health related and global QOL, but that the extent of that benefit will vary dependent on the clinical presentation, the population demographics, and the types and combinations of hormones used.
In our future continuing efforts to determine the true risks and benefits of postmenopausal hormone usage, it is absolutely critical that the full spectrum of effects be measured. There is no excuse for future studies on hormone use not to include well-validated instruments for measuring health related and global QOL and for not reporting those effects as part of the rest of the study. Questionnaire instruments can often provide more information than many of the invasive tests that are part of contemporary trials. They also add little cost, yet can be invaluable in the analysis of real cost-effectiveness of interventions in contemporary women's health care. Beyond safety and efficacy evaluation of drug therapies, there is an absolute need to know about the real impact of these therapies on overall quality of life.
It is also strongly recommended that a simple global QOL instrument be administered on an annual basis as part of routine clinical care. Variance in results from a previous assessment is of potential benefit in determining the success or failure of treatments administered or to get a sense of current state of health of our patients.
SY-07: Update and future of treatments in postmenopausal women
SY-07-01
THE LONG CYCLE PRINCIPLE IN HORMONE REPLACEMENT THERAPY: IS IT SAFE?
D. F. Archer
Eastern Virginia Medical School, Norfolk, VA, USA
It is well known that estrogen therapy (ET) in postmenopausal women with an intact uterus increases the risk of endometrial cancer 1. Progestogen added to ET is felt to reduce the incidence of endometrial hyperplasia and endometrial cancer 1. A recommendation to omit the progestogen in hormone therapy has been made 2. The use of estrogen alone for three or more months followed by a progestogen was introduced to reduce the monthly withdrawal bleeding and stillprevent hyperplasia 3. The potential increased incidence of endometrial cancer with a reduce duration ofprogestogen per month is a concern 1,4,5. A prospective randomized clinical trial was stopped because of an increased incidence of endometrial hyperplasia in the women using a progestogen administered every 12 weeks 6. The duration of the progestin not the dose is important in reducing endometrial hyperplasia 1,4,7.
The current findings strongly support the need for a progestogen continuously rather than cyclically when hormone therapy is used for five or more years,to interdict the occurrence of endometrial hyperplasia 5.
SY-07-02
TISSUE SELECTIVE ESTROGEN COMPLEXES (TSECS): A NEW DIRECTION FOR MENOPAUSAL HEALTHCARE
J. H. Pickar
Wyeth Research, Philadelphia, PA, USA
Tissue selective estrogen complexes are a new class of menopausal therapy which partner a selective estrogen receptor modulator (SERM) with other estrogens to achieve optimal clinical results based on their blended tissue selective activity profile. Treating menopausal symptoms, preventing osteoporosis and estrogenic stimulation of the endometrium with a favorable tolerability profile are the targeted clinical results. The TSEC partnering bazedoxifene (BZA) and conjugated estrogens (CE) is the first to demonstrate endometrial protection. Attempts with raloxifene and 17β-estradiol had not succeeded in preventing the estrogenic stimulation of the endometrium1,2.
In randomized, double-blind, placebo-controlled, clinical trials, the TSEC composed of BZA/CE demonstrated efficacy in treating vasomotor symptoms similar to what is commonly seen with menopausal hormone therapy (HT). Additionally, BZA/CE prevented osteoporosis by increasing bone mineral density by over 3.5% compared with placebo in the lumbar spine and over 1.75% in the hip over two years.
Breast tenderness and bleeding are two of the more common complaints of women using HT, leading to discontinuation. Large clinical trials with BZA/CE indicate that the incidence of breast tenderness with this TSEC is not different from placebo. Additionally, cumulative amenorrhea rates were similar to placebo and significantly better than that seen with HT. In the clinical trials, the overall incidence of serious adverse events was generally similar across treatment groups.
This TSEC treats menopausal symptoms, prevents osteoporosis, and offers an approach to the endometrium which prevents the unopposed estrogen mediated increase in the incidence of hyperplasia. Additionally, it maximizes the amenorrhea rate and minimizes the incidence of breast tenderness to a degree not achievable with progestational agents.
Clinical trial results will be presented.
SY-07-03
TIBOLONE, OVERVIEW OF THE EVIDENCE ON EFFICACY AND SAFETY
P. Kenemans
VU University Medical Center, Amsterdam, The Netherlands
Tibolone, is a synthetic steroid with a unique clinical profile that results from the tissue-specific action of its three active metabolites1.
Tibolone relieves climacteric flushes, improves vaginal atrophy and prevents bone loss, with an effectivity highly similar to that of unopposed estrogen therapy (ET) and of estrogen/progestagen therapy (EPT).
However, in contrast to ET, tibolone rarely causes endometrial proliferation and has a low incidence of vaginal bleeding, and, therefore, no additional progestagen is required.
In contrast to EPT, tibolone has a low incidence of breast pain and of increased mammographic density. Absolute numbers of women at increased risk for breast cancer are estimated to be significantly lower with tibolone than with EPT, making tibolone the preferred choice for postmenopausal symptomatic women with a uterus.
In addition, in a subgroup of postmenopausal women, tibolone improves mood and sexual wellbeing.
Various recently finalized prospective randomized controlled clinical trials (the THEBES Trial2, the Total Trial3, the LIFT Trial4 and the STEP Trial5,6), confirm tibolone's unique clinical profile and moreover, allow for a more precise description of tibolone's benefits and risks in early, respectively late postmenopausal women.
SY-07-04
PROGESTERONE RECEPTOR MODULATORS: CLINICAL APPLICATIONS
R. Sitruk-Ware
Rockefeller University and Population Council, NY, USA
Progesterone receptor modulators (PRM) and antiprogestins (AP) recently synthesized exhibit various degrees of agonistic and antagonistic properties to progesterone. The antiproliferative action of antiprogestins (AP) was evidenced on the monkey endometrium as well as in estrogen-treated postmenopausal women and this effect was attributed to a partial agonistic progestational effect of the molecule. More recently Slayden et al testing several PRMs on the monkey's endometrium evidenced the same antiproliferative action of these molecules decreasing thickness as well as markers of cell proliferation. An overexpression of the androgen receptor (AR) was evidenced in the monkey's endometrium treated with different PRMs and it was shown that the antiproliferative effect would be exerted via the AR as a specific AR antagonist blocked the antiestrogenic action of the PRMs on the endometrium. Direct intrauterine administration of new PRMs in the rhesus macaque was also shown to maintain the atrophy of the endometrium. Cell mitosis markers such as Phospho-H3 were shown to decrease after PRMs treatment in the human endometrium.
Results: We studied the delivery of a novel PRM from an intrauterine system that blocked the progestational differentiation in the macaque endometrium as indicated by the reduction in menstrual bleeding over 3.5 cycles. There was no significant spotting or breakthrough bleeding in the treated animals. The most notable histological change was the development of glandular cysts. However, there were no obvious signs of real cystic hyperplasia. There was moderate proliferation suggestive of estrogen action, but there was also glandular degeneration suggestive of endometrial atrophy. Overall, the amount of endometrial tissue was reduced compared to the amount found in a fully estrogenized animal. In long-term studies conducted with different PRMs in women with myomas, similar fibrocystic changes were observed as in the macaque model, with no hyperplastic characteristics and no mitosis.
Conclusion: Selective PRM are antiproliferative on some (endometrium), but not all tissues (vaginal epithelium and bone) and thus treatment with PRMs offers therapeutic options in endometriosis and myoma. By virtue of a partial progesterone agonistic and antiproliferative actions, the PRMs may also have a role in the treatment of dysfunctional uterine bleeding and possibly together with estrogen therapy in PMW. However the extrapolation of animal data to the human and the applicability of using PRM in estrogen-treated PMW deserve further long-term studies.
SY-08: Biopsychocultural influences on menopause and women's health
SY-08-01
PSYCHOLOGICAL CONTRIBUTION TO GYNAECOLOGY IN THE CLINICAL STUDY AND MANAGEMENT OF MENOPAUSE
Carlos Damonte Khoury
ISPOG, Alicante, Spain
Epistemologists show that complex realities, like Menopause, have many variables that may be studied by different theoretical fields or scientific disciplines.
Interdiscipline with Clinical Psychology and Psychoanalysis helps us see the incompleteness of any scientific field, the relationship with uncertainty and death. We can understand the patient is not a mere victim of her condition; she may obtain some unconscious benefits from it, she does not always seek for her own good, nor always asks for what she really wants.
This is included in psychosomatic attitude of listening, helping the patient to be the subject of its consultation, to express her suffering instead of speaking of her body and its disease as if it were an “outer object”.
In nowadays Gynaecology, and in Psychology research, we think it is “scientific” to use questionnaires or scales for assessing subjective issues like “quality of life”, instead of interviews. Some times this is due to the lack of time per patient, or the stimulus of the Medical Societies and the Pharmaceutical Industry, interested in increasing awareness of various issues as menopausal symptoms, sexual complaints, urinary incontinence, etc. Another example is the concept of “risk”. Linear techniques of estimation of risks are insufficient to include such a complex clinical condition as Menopause. Today medical science works with probabilistic risks, very difficult to explain to the patient, who understands it literally or magnified by the press, like in the of the disclosure of WHI study.
Science is a paradigm of thought adapted to every time and it is not “the truth”. Evidence based medicine is supported by RCTs that need to exclude subjective and individual biases to obtain great series of similar cases, and this is necessary for research and quantification.
But denying cultural, and psychological variables in the daily clinic has a high price, namely the dissatisfaction of doctors and patients.
Human beings do seek for Identity and Meaning, they intend to be helped by doctors in this aim, and illness or conditions like symptomatic menopause are a meeting point between organic and symbolic “body”.
In the study and the management of Menopause it is mandatory not to confound biological organism with the body expressed by the patients language.
SY-08-02
CULTURAL ASPECTS OF THE MENOPAUSE, FOR PHYSICIANS
M. Flint
Montclair State University, Montclair, New Jersey, USA
Objective: To help physicians, who are dealing with non-indigenous populations of menopausal women, understand how they can better help these women, bridging the gap between their cultures and the main culture of the physicians.
Design & Method: Using methodologies of anthropological fieldwork, physicians, who treat these non-indigenous menopausal populations, will be advised about improving sensitivity to cultural differences. These include language, values, attitudes, belief systems and material goods of these women.
Results: These methods of improving communication, between physicians and their non-indigenous patients, are expected to foster a milieu of trust, which will result in an improvement in the quality of care that is provided. For physicians, who have a change in populations they have traditionally treated, learning about the cultures of the people they will now treat, is vital to their practices.
Conclusion:As more and more populations continue to migrate to Europe, the United States, Asia and Middle East countries, physicians will be seeing increased non-indigenous populations, including menopausal women. In order to best service these women, physicians need to understand their cultures, to better communicate with them.
SY-08-03
MENOPAUSAL TRANSITION AND PSYCHOLOGICAL DEVELOPMENT
Aila Collins
Karolinska Institute, Stockholm, Sweden
Although research on menopause tends to emphasize negative bodily changes and risk of disease, there is an increasing awareness that menopause also represents a potential for reflection and personal growth and that the challenges experienced during this period may, in fact, serve as precursors of psychological development. Experience of the menopause varies between different cultures, social groups and individuals. Psychological development may be the result of complicated transactions between individual and contextual factors and the same event can either trigger or inhibit development depending on the individual and her psychosocial environment. The aim of a population-based longitudinal study was to investigate the interaction between biological and psychological changes in healthy women during transition to menopause. The study cohort included women aged 49 at study entry living in Stockholm and it suburbs. They participated in a five-year longitudinal follow up study comprising biological and psychological measures. Women completed symptom rating scales and participated in a semi-structured in depth interview including questions about menopausal status, work role, life stress and social relationships. Also, open-ended questions about experience of menopause and current life phase were included. The responses were analyzed qualitatively using grounded theory. The aim was to identify themes in their statements and to trace developmental changes during the menopausal transition. The women's statements were categorized into three main categories: optimistic, pessimistic and neutral. At the study entry most women (56%) had neutral expectations 13% were optimistic and 31% percent were initially pessimistic. The initial appraisals were followed by reappraisal and by the end of the study 67% were optimistic, 16% were neutral and 17% were negative. The pessimistic women reported more frequent menopausal symptoms. In an ongoing longitudinal study we focused on perceived work stress, health risks and appraisals of this phase of life using the same methods as above. The results showed that the dominant theme in the women's experience was “a sense of increased freedom and more personal time” which increased from baseline to follow-up. Our results also suggest that work stress interacts with the increased maturity and sense of new freedom and therefore tends to be perceived as less of a burden over the course of the study. In conclusion, our results showed that menopause is a positive phase for most women. The change toward more positive appraisals suggests that menopause has a developmental potential for women.
SY-08-04
A SYMPTOMATIC APPROACH TO UNDERSTANDING WOMEN'S HEALTH EXPERIENCES
L. Dennerstein1, P. Lehert1,2, P. Koochaki3, A. Graziottin4, S. Leiblum5 and J. Leventhal Alexander6
1The University of Melbourne, Victoria, Australia; 2FUCAM, Louvain Academy, Belgium; 3Procter and Gamble Pharmaceuticals, Mason, Ohio, USA; 4H. San Raffaele Resnati, Milan, Italy; 5UMDNJ Robert Wood Johnson Medical School, Piscataway, New Jersey, USA; 6Kaiser Permanente Medical Group, Oakland, California, USA
Objective: to compare across age groups, country and reproductive stages, factors affecting symptom prevalence and quality of life.
Design and Method: cross-sectional survey carried out from 1999 to 2000 in USA, UK, Germany, France and Italy.
Sample: 4517 women, recruited from large market research panels in all countries except Italy where women were found by random door knock. Inclusion criteria: 20 to 70 years, resident and literate in national language of the country. Response rate 70%.
Measures: self report questionnaires including: general health section, menopausal health section, MenQol. Symptoms were measured on the MenQol.
Statistical analysis: A step-wise least squares estimate was used to assess effects of all possible predictors on each symptom. Results were only considered significant at p < 0.001.
Results: Hierarchical clustering found 6 groups of symptoms. The following symptoms were found related to markers of menopausal hormonal change: hot flashes, night sweats; and poor memory, difficulty sleeping, aches neck, head and shoulders, vaginal dryness, difficulty sexual arousal. Physical and mental morbidity affected perception of all symptoms. Psychological symptoms declined with age from a maximum prevalence before age 40. Certain physical symptoms increased with age and BMI. There were marked differences in prevalence between countries for certain physical and psychological symptoms with 3 groups emerging: US and UK women; French/Italian women; German women.
Conclusions: The 7 symptoms most linked to menopausal hormonal change should form part of any future menopause symptom list. These symptoms need to be distinguished from those related to chronological aging. Physical and mental morbidity affect perception of these symptoms and should be measured.
SY-09: Menopause and the metabolic syndrome
SY-09-01
EFFECTS OF ADIPOSITY ON CARDIOVASCULAR RISK IN POSTMENOPAUSAL WOMEN
Pratima Gupta (UK)
Abstract not available at the time of going to press.
SY-09-02
MENOPAUSE AND INSULIN RESISTANCE
Ulysse Gaspard (Belgium)
Abstract not available at the time of going to press.
SY-09-03
DIFFERENT EFFECTS OF ORAL VERSUS NON-ORAL HORMONE REPLACEMENT THERAPY ON CLOTTING
G. D. O. Lowe
University of Glasgow, Glasgow, Scotland, UK
Observational and prospective studies have clearly established that oral oestrogen replacement therapy induces significant changes in certain circulating haemostatic and inflammatory biomarkers, while non-oral (transdermal) replacement therapy does not. Oral oestrogen replacement increases circulating levels of coagulation factors VII and IX (but not fibrinogen), decreases circulating levels of coagulation inhibitors (antithrombin, protein C, protein S), and increases activated protein C resistance. Presumably as a result of these changes, oral oestrogen replacement increases circulating levels of coagulation activation markers (prothrombin F1 + 2, thrombin-antithrombin complexes, fibrin D-dimer). These systemic changes are similar to those observed with combined oral contraceptives, and probably reflect the “first-pass” effect of oral oestrogens on hepatic synthesis of haemostatic proteins. While oral oestrogen also increases circulating levels of C-reactive protein, changes in haemostatic proteins are unlikely to reflect a generalised inflammatory response, because circulating levels of other inflammatory markers (fibrinogen, interleukin–6) do not increase.
These reversible effects of oral oestrogen replacement therapy on blood coagulation provide a plausible biological explanation for its reversible effects on risk of thrombosis (venous, cerebral and possibly coronary). The “starter effect” may reflect precipitation of thrombosis in susceptible women with thrombophilias. There is increasing evidence that levels of these haemostatic factors are associated with risk of venous thrombosis, and possibly of arterial thrombosis. The supra-additive effects of oral oestrogens, obesity and factor V Leiden on risk of venous thrombosis are consistent with common causal pathways such as activated protein C resistance.
A recent meta-analysis has shown that oral oestrogen replacement therapy carries a higher risk of venous thrombosis than non-oral therapy. While the latter may therefore be preferred in women at increased risk, further studies are required to establish with confidence the risks of venous and arterial thrombosis in users of non-oral therapies; the biological effects and thrombotic risks of low-dose oral and high-dose non-oral oestrogen replacement therapies; and the biological effects and thrombotic risks of androgen replacement therapies.
SY-09-04
METABOLIC EFFECTS OF NEW HORMONAL AGENTS
J. C. Stevenson
National Heart & Lung Institute, Imperial College London, London SW3 6NP, UK
Metabolic abnormalities have adverse consequences for the cardiovascular system and coronary heart disease (CHD). Postmenopausal hormone replacement therapy (HRT) may reduce the incidence of CHD through various mechanisms which are important in the development of atheromatous disease. Hence, the metabolic effects of HRT regimens are important and need to be evaluated in all new HRT regimens. HRT affects lipids and lipoproteins; these effects vary according to the dose and type of estrogen or progestogen used, and their route of administration. Reductions in LDL cholesterol and increases in HDL cholesterol are achieved with all HRT, but more so with oral estrogen than transdermal estradiol. The addition of an oral androgenic progestogen prevents the HDL increase, whilst transdermal administration or non-androgenic progestogens have little impact. Oral estrogens result in increases in triglycerides, whereas transdermal estradiol decreases them. The addition of androgenic progestogens decreases triglycerides, whilst the non-androgenic progestogens do not prevent an increase. Oral estrogens, and particularly the androgenic progestogens, reduce lipoprotein (a) levels, a potentially beneficial effect. Small dense LDL particles are thought to be the most atherogenic lipoproteins, and oral estrogen reduces the LDL particle size whereas transdermal estradiol has no such effect. However, oral estrogen also increases the clearance of small dense LDL. In addition, estrogen increases the clearance of other atherogenic lipid particles, such as triglyceride remnants, from the circulation, and also helps protect LDL against oxidative damage. Estrogens also affect glucose and insulin metabolism. Insulin resistance is a pivotal metabolic disturbance underlying CHD development, which is influenced by HRT. High doses of conjugated equine estrogens may have adverse effects on glucose and insulin metabolism, but such effects are probably eliminated with the lower dose preparations. Transdermal estradiol has little effect, but oral estradiol increases pancreatic insulin secretion, insulin sensitivity and insulin elimination. Androgenic progestogens may oppose these effects but non-androgenic progestogens do not. Selective estradiol receptor modulators (SERMs) also have effects on lipids. Raloxifene and toremifine lower total and LDL cholesterol, increase HDL cholesterol, and toremifine reduces triglycerides. There are few other metabolic data for SERMs, but raloxifene appears to have no adverse effect on insulin sensitivity or glucose tolerance. The metabolic effects of newer HRT preparations, such as conjugated equine estrogens and bazedoxifene, are currently being evaluated. It is important to optimize the metabolic effects produced by HRT, and HRT regimens should be tailored to individual patients with metabolic disturbances in order to maximise CHD benefit.
SY-10: Future strategies in the management of Osteoporosis
Unrestricted grant from Amgen
SY-10-01
NEW CONCEPTS IN THE THE PATHOPHISIOLOGY OF OSTEOPOROSIS
Lorenz Hofbauer (Germany)
Abstract not available at the time of going to press.
SY-10-02
THERAPEUTIC POTENTIAL OF RANKL INHIBITION IN PATIENTS WITH POSTMENOPAUSAL OSTEOPOROSIS
A. Diez-Perez
Hospital del Mar. IMIM. RETICEF. Autonomous University of Barcelona, Barcelona, Spain
Osteoporosis is the result of an imbalance between bone formation and resorption because a predominance of the latter. However, the resorbing cell, the osteoclast, works in exquisite coordination with the bone-forming cell, the osteoblast, and the osteocyte, a key element in the signaling mechanisms. A critical pathway has been identified in the cross-talk between these different cells, the RANK (receptor activator of nuclear factor κB) – RANKL (its ligand) – OPG (osteoprotegerin) system. RANKL binds to RANK stimulating the differentiation and activation of the osteoclastic cells. A number of hormones and other local and systemic factors enhancing bone resorption work thru this system that becomes the common final signal in the resorption process in a number of bone diseases. Osteoprotegerin, a decoy receptor, blocks the system by binding to RANKL and, thus, preventing the activation of the RANK receptor. Therefore OPG protects bone from excessive resorption and the ratio RANKL/OPG determines the final bone balance.
This system has emerged as a good target for osteoporosis treatment. OPG could be a good candidate to slow bone resorption and the associated bone loss. However, monoclonal antibodies against RANKL have been developed because a much better pharmacodynamic profile. Denosumab is a fully human antibody to RANKL that mimics the action of OPG but has a much longer half-life. Is highly selective for bone tissue and has been developed to treat bone loss associated to osteoporosis, bone metastases and inflammation-associated bone resorption.
In postmenopausal osteoporosis, denosumab is a powerful antiresorptive that prevents bone loss. Phase I and II clinical trials of up to two years of duration have been published with the drug showing significant differences between bone mineral density increases in treated women compared with those receiving placebo. The effect is apparent at the usual locations, lumbar spine and proximal femur but also, in contradistinction with other antiresorptive drugs, has positive effects on the radius. The administration of the drug is by a single subcutaneous injection every six months and the profile of tolerance and safety of the drug is excellent. Moreover, the decrease in bone resorption, measured by biochemical markers of bone turnover, is very fast and powerful. In addition, the effect of the drug is reversible not lasting in bone tissue for prolonged periods of time. Antifracture efficacy of denosumab is currently being tested in a large phase III trial and, if confirmed, will offer to the clinician a powerful, safe and convenient alternative for the prevention and treatment of postmenopausal osteoporosis.
SY-10-03
HOW TO PREDICT THE FRACTURE RISK
John Kanis (UK)
Abstract not available at the time of going to press.
SY-11: Update in HRT
SY-11-01
LOW DOSE OESTROGENS DELIVERED BY THE VAGINA
Elizabeth Farrell
Monash Medical Centre, Southern Health, Clayton, Victoria, Australia
Symptoms of urogenital atrophy after the menopause may impact significantly in women's life interfering in their normal daily function and relationships.
The most commonly experienced symptoms are vaginal dryness, dyspareunia, itching and discomfort. These symptoms increase through the menopausal transition with about 50% of women experiencing in the post menopausal years and continue on with aging. Urinary dysfunction also appears to increase in the post menopausal years. There is a reluctance to report these symptoms as women are often too embarrassed to talk about them.
There are many changes which occur in the pelvis after the menopause including decreased vaginal blood flow, diminished vaginal secretions, loss of elasticity of the tissues, changes in the connective tissue and thinning of the vaginal epithelium, Sometimes there is increased laxity of the vagina leading to prolapse but conversely in some women narrowing of the introitus and vagina. The vaginal pH becomes less acidic and the bacterial flora change.
Vaginal oestrogen preparations have been found to be very effective in reducing the urogenital atrophic symptoms and recurrent urinary infections. These preparations include creams, pessaries, tablets and a vaginal ring, and contain oestriol and oestradiol.
Overall there are advantages in using these products as they are less likely to cause systemic side effects, increased liver metabolism and may be used in women with a history of cancer. Lower doses than systemic therapy may be used and if used in the recommended doses endometrial stimulation does not occur.
Conjugated equine estrogens in a cream has been associated with dose related systemic absorption and side effects.
Newer preparations have been developed with lower doses which are as effective in reducing symptoms and less likely to cause systemic symptoms or be significantly absorbed.
The vagina has been an effective organ for drug delivery and perhaps in the future we will see newer forms of hormone therapy using this mode of delivery.
SY-11-02
LOW DOSAGE ESTROGEN FOR SYMPTOM RELIEF AND PREVENTION OF BONE LOSS
B. Ettinger
University of California, San Francisco, California, USA
Objective: To summarize potential benefits of low and ultralow dosage postmenopausal estrogen therapy (HT), both for symptom relief and for bone health.
Design & Method: Personal perspective based on review of the literature. For the purpose of this review, 0.3 mg conjugated estrogens or its equivalent (e.g. 0.5 mg oral micronized estradiol or 25 μg transdermal estradiol) is considered low dosage. One half this amount (e.g. 0.25 mg oral micronized estradiol or 14 μg transdermal estradiol) is considered ultra-low.
Results: In numerous placebo-controlled clinical trials low dose estrogens have been shown to reduce hot flashes 60–70%. This reduction is about twice that observed with placebo, but less than the 80–90% reductions typically observed with standard dosage. Recently, ultralow estrogen has proven to relieve vasomotor symptoms better than placebo in clinical trials.
Low dosage is effective in preventing bone loss in early menopause and both low and ultra-low dosages have prevented bone loss in women aged 60 years and older. The Nurses' Health Study observed that women using half strength estrogen obtained the same degree of cardioprotection as those using full strength—while those using higher estrogen dosages had less cardioprotection! In that study, stroke risk appeared strongly related to the dose of estrogen; while half strength estrogen appeared protective, standard or higher doses appear to increase the risk in a dose-proportional manner. Compared to women using standard dosages, those using low-dosages of estrogens are less likely to have unacceptable side effects, such as irregular or heavy bleeding or breast tenderness. Low and ultralow dosage estrogens appear to have lower thromboembolic risk than standard dosage.
When prescribing low dosage estrogen to a woman with a uterus, one can safely use less progestin, either less daily dosage or less frequent cycles.
Conclusions: Low and ultra-low dosage estrogen can relieve vasomotor symptoms and can prevent postmenopausal bone loss. Women taking low-dosages of estrogens are less likely to have unacceptable side effects, such as irregular bleeding, heavy bleeding, or breast tenderness. Moreover, the potential harm caused by standard dosages of estrogen with progestin may be mitigated by use of lower estrogen doses that do not require daily or monthly progestin opposition. Furthermore, it is now appropriate to plan a new generation of low dose estrogen studies to adequately document its risks and benefits.
SY-11-03
ESTROGEN AND SKIN
M. P. Brincat and J. Calleja-Agius
Mater Dei Hospital, B'Kara, Malta
Cutaneous ageing manifests itself as a progressive reduction in maximum function and reserve capacity of skin tissue. There is an increase in skin thickness up to the age of 49, followed by an age-related thinning. Collagen atrophy is a major factor in skin ageing. There is a strong correlation between skin collagen loss and estrogen deficiency due to the menopause. As much as 30% of skin collagen (both type I and type II) is lost in the first five years after the menopause. Skin ageing, especially in the face, is associated with a progressive increase in extensibility and a reduction in elasticity. With increasing age, the skin also becomes more fragile and susceptible to trauma, leading to more lacerations and bruising. Furthermore wound healing is impaired in older women.
A beneficial effect of subcutaneous, topical and oral estrogens has been demonstrated on ageing skin. Estrogen use after the menopause increases collagen content, dermal thickness and elasticity. It also decreases the likelihood of senile dry skin, possibly due to the estrogen-stimulated increase in mucopolysaccharides and hyaluronic acid levels in skin. This correlates with an increase in dermal water content, leading to an increased skin thickness. Sebum secretion decreases with age. Overall, there is a 38% increase in sebum production in postmenopausal women taking hormone replacement therapy.
Large-scale clinical trials are necessary to help make informed recommendations regarding postmenopausal estrogen use and its role in the prevention of skin ageing. Estrogen has profound effects on connective tissue turnover, no matter the site. It has been shown that the menopause has similar effects on the connective tissue of the carotid artery media, bone and intervertebral discs.
SY-11-04
THE EURAS HRT STUDY: OBJECTIVES, STUDY DESIGN, AND INTERIM RESULTS
J. Dinger and A. Assmann
ZEG – Berlin Center for Epidemiology and Health Research, Berlin, Germany
Objective: Progestins used in HRT have substantially distinct pharmacological profiles. The progestin drospirenone (DRSP) has antimineralocorticoid properties which could have beneficial as well as unfavorable effects on cardiovascular outcomes. The study compares incidence rates of serious adverse events – in particular cardiovascular outcomes – in users of DRSP/estradiol and oral continuous combined preparations under routine medical conditions in Europe.
Design & Method: Multi-national, prospective, controlled cohort study with three arms: women using 1) DRSP/estradiol, 2) other oral continuous-combined HRT, and 3) all other oral HRTs. The combined cohorts will include at least 30,000 women aged 40 or older in seven countries who started or switched to an oral HRT at the time of inclusion in the study. At least 90,000 years of observation are expected. Field work started in 2002 and will end around 2010. All patient-reported outcomes of interest are validated by the women's treating physicians. Unbiased classification of adverse events will be ensured by blinded adjudication at the end of the study. A multifaceted 4-level follow-up procedure should result in low loss to follow-up rates. Inferential statistics will be based on Cox regression models comparing the cohorts.
Results: By the end of October 2007 a total of 19,254 users of oral continuous combined HRT preparations – reflecting more than 45,871 WY of observation – was recruited by 1,007 study centers. The prevalence of cardiovascular risk factors among HRT users is higher in northern and central European countries than in Mediterranean countries. Incidence rates for thromboembolic events (e.g., stroke, myocardial infarction, deep venous thrombosis, pulmonary embolism) were 20.1 (95% CI, 8.1–41.4) and 40.9 (95% CI, 32.6–50.6) per 10,000 WY for DRSP/estradiol and other oral continuous-combined HRT, respectively. Updated results will be presented at the meeting.
Conclusion: Results do not indicate a higher cardiovascular risk potential for DRSP/estradiol compared to other oral continuous combined HRT preparations. Preliminary risk estimates for DRSP/estradiol suggest a very low incidence of arterial thromboembolic events. The impact of differences in baseline risk on these estimates needs to be analyzed based on a larger data set.
SY-12: HRT and breast cancer risk
SY-12-01
IS HRT CARCINOGENIC DUE TO GENOTOXIC METABOLITES?
Alfred O. Mueck
University Women's Hospital of Tuebingen, Germany
The ‘International Agency for Research on Cancer’ (IARC), a working-group of the World Health Organization (WHO), recently classified estrogens and estrogen-progestogen combinations as ‘carcinogenic in humans’. One of the main reasons is the production of potential carcinogenic estrogen metabolites. The IARC identifies potential carcinogens associated with nutrition, environment and pharmaceutical products; risk-benefit analyses are outside its scope. They do not quantitate estimates of the age-specific absolute risk, the availability and effectiveness of cancer screening or other health and societal effects. The IARC admits that their statement will not automatically meet the overall net public-health outcome for each different country.
However, the WHO's classification added fuel to the discussion how far estrogens not only act as growth factors in promoting cancers, enhanced by progestogen addition, but also may cause mutations, not only by DNA-replication mistakes (which can be repaired by a huge battery of different systems) but also by certain estrogen metabolites which indeed have been already demonstrated to be genotoxic in experimental studies. In the last years evidence has strongly grown that estradiol metabolites have own biological properties even at very low concentrations which can exceed manifold those of their parent substance.
Certain estrogen metabolites may have carcinogenic potency by inducing long-lasting receptor activation or by oxidative processes leading to DNA strang breaks. Especially the 4-quinones are supposed to play a role in carcinogenesis. However, their toxic effects need special oxidative cell stress to manage a crucial one-electron oxidation from semiquinones to quinones, which can be prevented by various cellular defence mechanisms. We have been able to assess the biological potency of various metabolites and to demonstrate that the pattern of estrogen metabolism during HRT can be influenced by administration route and the type of added progestogen. In addition, life-style factors such as physical activity and smoking as well as genetic polymorphisms of the enzymes involved in the formation and degradation of the catechol estrogens may have a crucial impact.
Our present conclusion is that the clinical importance of potential genotoxic metabolites still awaits further research. In terms of HRT there is no reason to change current clinical practice. However, in the presence of factors, which could influence estradiol metabolism such as smoking or genetic polymorphisms, it seems prudent to use a transdermal HRT to minimize the production of possible toxic metabolites.
SY-12-02
HRT AND STEM CELL ORIGIN OF BREAST CANCER
H. P. G. Schneider and W. Boecker
University of Muenster, Germany
Tumors are proliferatively heterogeneous with only a subfraction of tumor cells able to grow either in vitro or in vivo based on xenograft models. This has been explained by 1st, a stochastic theory which attributes each tumor cell an equal but low probability of initiating tumor growth or 2nd, the stem cell (SC) theory of cancer. The latter predicts that a small number of tumor initiating cells, or cancer <stem cells>, would drive tumor growth and populations of more differentiated non-tumorigenic daughter cells, analogous to the transit amplifying and differentiated cells of the normal tissue.
There is accumulating evidence that breast epithelial stem cells or their progenitors might be the targets for transformation during mammary carcinogenesis. A CD44pos and CD24neg/low phenotype of breast cancer (BC) SCs, when isolated from mammosphere cultures, provides enhanced transplantation capacity in cleared mammary fat pad immunodeficient (cmfi) mice, marks three out of four bone marrow tumor daughter cells and identifies a 186-gene <invasiveness> signature.
Both estrogen receptor (ER) subtypes are found in Ck8/18-stained luminal epithelia contrast to Ck5/6 and Ck14 basal epithelia. Rodent mammary luminal ERpos and ERneg cells could be isolated and specifically marked; their repopulating (SC or progenitor cell) activity in cmfi mice is abundant in the basal cell and rather little in the ERpos luminal cell compartment. Estrogen-induced luminal ER expression apparently signals proliferation to a separate ERneg luminal SC population. The stem cell model may account for the classification of subtypes of BC based on cell of origin: basal epithelia with stem cell properties, thus highly invasive and metastatic or luminal epithelia with more indolent progenitor cells, shorter lived, higher grade and less invasive, and with or without the expression of the gene encoding the estrogen receptor.
This stem cell model predicts that different subsets of BC arise from the transformation of (a) the most primitive ERneg stem or early progenitor cell with a basal phenotype only or (b) with mutations that allow for intermediate differentiation into ERpos cells. Both (a) and (b) subtypes are driven by an ERneg stem cell with unchanged (a) or limited (b) response to HRT and either poor (a) or intermediate (b) prognosis. A third (c) subtype with ERpos and differentiated progenitor cells is characterized by luminal markers only, with good SERM responsiveness. HRT, in our experience, will promote (c) subtype BC, however, with lower mortality and improved disease-free survival.
SY-12-03
DO LOW DOSES OF HRT REDUCE BREAST CANCER?
J.-M. Foidart (Belgium)
Abstract not available at the time of going to press.
SY-12-04
DIFFERENT HRT TYPES AND THE RISK OF BREAST CANCER
A. Gompel and G. Plu-Bureau
Hôtel-Dieu de Paris, APHP, Université Paris V, Paris, France
It is known for years that breast cancer is a hormone dependent disease and that reproductive factors can contribute to increase its incidence. Among the factors, Hormone Therapy (HT) for postmenopausal symptoms appears to be a contributor at least in some women. HT remains to be the most efficient intervention to alleviate the postmenopausal symptoms. However the possible mild increase in the risk of breast cancer remains a limit to its prescription. From one country to another, regimens are different, especially concerning the type of progestin combined with the estrogen. In addition, the estrogens vary between the US and most of the others countries. Indeed, in the US conjugated estrogens are used whereas in the rest of the world, the predominant estrogen is estradiol. The risk shown by most of the studies is mild with the estrogens, does not seem to differ between estradiol and the conjugated estrogens and appears after a long term use in most of the studies. At the opposite, according to observational studies, the magnitude of the risk can vary dependent of the progestogen used. The French cohort observational study,E3N, is the only one to report on the use of estradiol and progesterone and observed no increase in the risk of breast cancer with this HT, but an increase in the patients using either estradiol alone or estradiol and a synthetic progestin. The scientific literature concerning the biological effects of progestins and progesterone does not provide any satisfactory evidence or explanation to understand this strong discrepancy. The literature also provides evidence of a predominant increase in lobular carcinoma compared to pure ductal carcinoma and this increase is observed independently of the countries including the US and France but still no increase with progesterone combined with estradiol. A last question will be discussed which is the importance of continuous versus sequential treatment. A meta-analysis of the existing data suggests that the continuous regimens could be more deleterious than the sequential. However the interpretation of the data is difficult due to the fact that the composition of the HT used continuously or sequentially is not the same suggesting that the difference in the risk could be due to the type of the used progestin. We will review the available information on HT from European and US studies in order to provide an overview of the current knowledge of this important question.
SY-13: HRT and gynecological cancer
SY-13-01
TIBOLONE IN BREAST CANCER PATIENTS: FIRST RESULTS OF THE LIBERATE TRIAL
P. Kenemans1, M. W. Beckmann2, N. J. Bundred3, J.-M. Foidart4, E. Kubista5, B. von Schoultz6, P. Sismondi7, R. Vassilopoulou-Sellin9, C. H. Yip9, J. Egberts10, J. Planellas Gomez10, R. Mulder10 and S. van Os10
1Free Univ, Amsterdam, Netherlands; 2University Clinic, Erlangen, Germany; 3Univ of Manchester, Manchester, United Kingdom; 4Univ of Liege, Liege, Belgium; 5Medical Univ, Vienna, Austria; 6Karolinska Inst, Stockholm, Sweden; 7Univ of Turin, Turin, Italy; 8Univ of Texas, Houston, United States; 9University Malaya Medical Centre, Kuala Lumpur, Malaysia; 10NV Organon, Oss, The Netherlands
Objective: Many patients with a history of breast cancer (BC) will suffer from vasomotor symptoms, which can be induced or exacerbated by treatment with tamoxifen or aromatase inhibitors. LIBERATE was designed as a randomized, double-blind trial to evaluate that tibolone (Livial®) is non-inferior to placebo regarding BC recurrence in women with vasomotor symptoms surgically treated for primary BC within the last 5 years.
Design & Method: Patients with histologically confirmed and surgically treated BC (T1‐3, N0‐2, M0), and complaining of vasomotor symptoms, were randomly assigned to either tibolone 2.5 mg daily or placebo treatment for a maximum of 5 years. The primary endpoint is BC recurrence rate. Secondary outcome variables include overall mortality, menopausal symptoms, bone mineral density and health-related quality of life. Adequate sample size was estimated to be >1500 in each arm, based on an expected yearly BC recurrence rate of 3% and 8% in N− and N+ patients, respectively.
Results: In total, 3148 patients were randomized at 245 centers in 31 countries worldwide between June 2002 and December 2004. Mean age at randomization was 52.6 years, and the mean time since surgery 2.1 years. The mean daily number of hot flushes and sweating episodes was 7.3 and 6.1, respectively. The primary tumour was N + for 58% of the patients and ER + for 78%. Prior to or at study entry, tamoxifen was given to 75% of the patients and aromatase inhibitors to 8%.
Twice-yearly unblinded safety review was performed by an independent DSMB. At their latest review in March 2007, the DSMB found a trend for an excess of BC recurrences in the tibolone group, although the difference did not reach the predefined boundary. Since it seemed highly improbable that the statistical criteria for non-inferiority could be met, the LIBERATE trial was prematurely stopped and reached clinical completion in August 2007. Final statistical analysis is planned for early 2008, focusing primarily on the HR's and 95% CI for BC recurrence and mortality. Special attention will be given to various subgroups of patients.
The results of the LIBERATE trial will be presented at this meeting for the first time.
Conclusion The LIBERATE trial is the largest, well-controlled ever performed study, for treatment of vasomotor symptoms following BC surgery. As it is very unlikely that the safety of tibolone can be shown in this important group of patients, an effective and safe hormonal modality will still be lacking for the relief of vasomotor symptoms in BC patients.
SY-13-02
HRT AND OVARIAN CANCER
Valerie Beral (UK)
Abstract not available at the time of going to press.
SY-13-03
HRT AND ENDOMETRIAL CANCER
L. G. Ulrich
Rigshospitalet – Copenhagen University Hospital, Copenhagen, Denmark
Histopathological features separate endometrial cancers into two main types. Type one cancers are endometrioid adenocarcinomas, generally expressing both estrogen and progestogen receptors (ER and PR), developing from hyperplastic endometria, estrogen dependent and associated with a relatively good prognosis. Endometrioid adenocarcinomas constitute 75–80% of all endometrial cancers, 85–90% of stage one cancers, and two out of three are grade one or two, stage I A or B. With just a simple hysterectomy and bilateral salpingooophorectomy, these patients can expect the same survival as the background population and when occurring in young women, conservative treatment is sometimes feasible. Type two cancers are more malignant types of such as serous adenocarcinomas, clear cell, undifferentiated and carcinosarcomas arising from atrophic endometria and associated with a poorer prognosis. Most express lower levels of ER and PR and are associated with higher p53 values.
Unopposed estrogen treatment and high endogenous estrogen increase the risk of endometrial hyperplasia and type one cancers. This increased risk persists for several years after estrogen treatment is stopped and is related to estrogen dose as well as to duration of treatment.
Adding progestogen to estrogen treatment reduces the risk dependent upon the number of days of addition per cycle and possibly also on dose and type of progestogen. Use of continuous combined estrogen and progestogen causing an atrophic endometrium may even reduce the risk of endometrial cancer. Progestogen can be administrated systemically or by intrauterine IUD's which result in high endometrial progestogen levels. Tibolone, although inducing endometrial atrophy, in the Million Women Study was associated with an increased risk of endometrial cancer of the same magnitude as unopposed estrogen, but this has not been confirmed in other studies. It is still not known whether cancers arising from atrophic endometria during treatment with continuous combined HRT or Tibolone are of different types than the pure estrogen induced cancers. This is the case with Tamoxiphen which not only increases the risk of endometrial cancer but also is associated with more type two cancers.
The use of HRT after treatment for endometrial cancer is investigated in a number of small studies, but the only large scale study on this topic was terminated early due to poor recruitment following the publication of the WHI study. Based upon the available evidence HRT following treatment for endometrial cancer may be acceptable.
SY-14: Management of premature menopause
SY-14-01
MANAGEMENT OF PREMATURE MENOPAUSE
Margaret Rees (UK)
Abstract not available at the time of going to press.
SY-14-02
DOES PREMATURE MENOPAUSE CAUSE PREMATURE DEATH, AND FROM WHAT CAUSES?
R. A. Lobo
Columbia University, New York, New York, U.S.A.
Premature menopause is defined as the cessation of menses prior to the age of 40 years. It has been estimated that this occurs in approximately 1% of the female population. Etiologies of spontaneous premature menopause are varied, and poorly understood, but include familial/genetic and autoimmune causes. Iatrogenic causes include bilateral oophorectomy for a variety of reasons or chemotherapy and/or radiation therapy for malignancy.
There is a compelling literature that points to premature menopause being related to an increased incidence of CV disease, particularly coronary disease, with an adjusted odds ratio of 1.38 (1.21–1.58) prior to the age of 50 years, and higher ratios for younger women. This also translates into increased mortality: odds ratio 2.10 (1.07–4.1), with women having had bilateral oophorectomy having a relative risk of 4 fold or greater. There is some evidence, mechanistically, that there is an accelerated rate of atherosclerosis, as occurs after natural menopause, and that atherogenic lipoproteins begin to increase in the circulation several years after the cessation of menses. While there is less consistency on this issue, there are also data suggesting an increased rate of cerebrovascular disease and ischemic stroke in women with premature menopause; although the data are much stronger for the association with coronary disease.
An extension of these data, is a study which suggested that bilateral oophorectomy prior to age 55 years increases mortality by 8.6% by the age of 80 years, but goes down progressively thereafter. There are data that hormonal therapy in women with premature menopause decreases the risk of CV disease and mortality, although the data are largely observational.
Apart from CV disease endpoints, it is known that estrogen deficiency increases the risk of osteoporotic fracture as well as affects the quality of life of the women so affected. However there are no data on what the impact of these factors on mortality may be.
Suggested reading:
SY-14-03
PREMATURE OVARIAN FAILURE AND FERTILITY DESIRE
Philippe Bouchard (France)
Abstract not available at the time of going to press.
SY-14-04
DOES PREMATURE MENOPAUSE CAUSE DEMENTIA OR PARKINSONISM?
W. A. Rocca
College of Medicine, Mayo Clinic, Rochester, Minnesota, USA
Background: There is increasing laboratory evidence for a neuroprotective effect of estrogen during aging; however, the clinical and epidemiological evidence remains limited and conflicting. We studied the association of oophorectomy performed before the onset of menopause with the risk of parkinsonism or dementia.
Methods:We included all women who underwent either unilateral or bilateral oophorectomy before the onset of menopause for a non-cancer indication while residing in Olmsted County, MN, from 1950 through 1987. Each member of the oophorectomy cohort was matched by age to a referent woman in the same population who had not undergone oophorectomy. In total, we studied 1,252 women with unilateral oophorectomy, 1,075 women with bilateral oophorectomy, and 2,368 referent women. Women were followed for a median of 25–30 years. Parkinsonism was assessed using screening and examination, through a medical records-linkage system, and through death certificates. Cognitive status was assessed using a structured questionnaire via a direct or proxy telephone interview.
Results: Women who underwent either unilateral or bilateral oophorectomy before menopause had an increased risk of cognitive decline or dementia (hazard ratio [HR] = 1.46; 95% CI, 1.13 to 1.90; P = 0.005) or of parkinsonism (HR = 1.68; 95% CI, 1.06 to 2.67; P = 0.03) compared to referent women. The risk increased with younger age at oophorectomy (test for linear trend of the log HR with decreasing age; P<0.0001 for dementia and P = 0.01 for parkinsonism). These associations were similar regardless of the indication for the oophorectomy, and for women who underwent unilateral or bilateral oophorectomy considered separately. Women who underwent bilateral oophorectomy before age 49 years (first and second tertile of the distribution) but received treatment with estrogen to age 50 years did not experience an increased risk of cognitive impairment or dementia.
Conclusions: Both unilateral oophorectomy and bilateral oophorectomy performed before the onset of menopause are associated with an increased risk of cognitive impairment or dementia or of parkinsonism. The effect is age-dependent. Our findings, combined with previous laboratory and epidemiologic findings, suggest that estrogen may have an age-dependent neuroprotective effect.
SY-15: Women's healthcare needs
SY-15-01
MORTALITY FOLLOWING THE MENOPAUSE – HOW TO AVOID PREMATURE DEATH
Barry G. Wren
Gynaecologist. First President Australian Menopause Society, Assoc. Prof. University NSW – Retired
Objectives: (1) To examine the major causes of death among women following the menopause and determine how hormonal therapy influences the outcome of these diseases.
(2) To propose a scheme which will inform and educate women regarding the influence of postmenopausal hormone therapy on the various causes of premature death.
Method: The major causes of death in women over the age of 50 will be reviewed and particular attention will be given to research papers which implicate hormonal therapy and breast cancer, the cardiovascular system, osteoporosis and dementia. The role that time (“the window of opportunity”) in initiating hormonal therapy after the menopause plays in reducing adverse events as well as the length of time on therapy will be discussed in relation to longevity of life. While women may wish to take hormonal therapy to relieve distressing symptoms and some are aware that oestrogen therapy reduces the risk of cardiovascular disease and osteoporosis, a large number refuse to begin therapy because of fear.
Women fear hormones will induce breast cancer: This fear has been engendered by media publicity surrounding publication of the WHI report in 2002 and the Million Women Study in 2003 (the power of the media!). The fact that the initial WHI Study which reported 8 extra cases in 10,000 in 5.2 years (26% increase) was counterbalanced by the second WHI in 2004 which reported a 23% decrease in breast cancer over 6.8 years, was ignored by the media and therefore by most doctors in clinical practice. In spite of several recent and very different interpretations of the role of oestrogen in initiating breast cancer these fears have persisted. If media publicity can be engendered by dramatising the positive aspects of hormonal therapy these fears will diminish. Following presentation of data from recent studies a scheme will be proposed which, if implemented, will help to educate and reassure women regarding the benefits of oestrogen replacement therapy.
Conclusion: The adverse publicity surrounding the use of HRT can be countered by an effective campaign involving the media being informed and cultivated regarding recent data which supports the use of oestrogen in reducing cardiovascular disease, osteoporosis, and dementia as well as prolonging life for post-menopausal women. The role which oestrogen plays in promotion of breast cancer, as opposed to initiation, will addressed and clarification of the risks and benefits of HRT will be made clear.
SY-15-02
CLINICAL ASPECTS AND RELATIONSHIPS BETWEEN OBESITY AND MENOPAUSE
C. Castelo-Branco
Hospital Clínic, Institut Clínic de Ginecologia, Obstetrícia i Neonatologia, Faculty of Medicine, University of Barcelona, Spain
Obesity has become a major problem of public health in all developed countries being epidemic in the 21st century. The visceral form is associated with increased risk for metabolic syndrome, cardiovascular disease, hypertension and increased mortality. This type of obesity is frequently observed during gynecological practice. This especially concerns women with ovarian hyperandrogenism, in which visceral obesity is one of the main factors in etiology of metabolic and cardiovascular problems. Another group of women in which this type of obesity plays an important role are climacteric women in whom redistribution of adipose tissue with increase in visceral fat deposit occurs. Menopause onset is one of the critical periods during which weight gain and onset or worsening of obesity is favored. However, this weight gain is more related to aging than to hormones being independent of whether women are postmenopausal or not, treated with estrogens or not. At the same time, there is a central redistribution of fat with a decrease in gluteo femoral fat and an increase in intra abdominal fat. Moreover, during climacteric, often appears an associated muscle mass loss. Likewise for weight gain, changes in body composition are related to aging. Different factors (diet – physical activity – GH secretion … ) could be involved.
Obesity, and more precise, this tendency to visceral fat accumulation clearly favors the increased cardiovascular risk observed after menopause. And in addition, central obesity has slightly different connotations in women because, apart from its greater prevalence, low socio-economic level is a risk factor solely for women. As well as a cardiovascular risk factor in women, it is associated with an increased risk of breast and endometrium cancer, ovarian polycystosis and infertility. Weight control in women has a great aesthetic motivation and food intake has considerable emotional components. On the other hand, women consume more drugs (hormonal contraceptives, analgesics, antiinflamatories, migraine treatments, ansiolytics, anti-depressants, antipsychotics … ) which appear to favor obesity. The role played in the pathogenesis of obesity by menstrual cycle, hormonal changes, pregnancy, the consumption of hormonal contraceptives and the menopause remains to be clarified. The effect of replacement hormone therapy as a cause of weight gain is doubtful.
SY-15-03
SARCOPENIA: CLINICAL IMPACT OF MUSCLE HEALTH IN ADULT WOMEN
Morris Notelovitz
Adult Women's Health Alliance Inc, Boca Raton Fl & Washington DC, USA
Sarcopenia is an involuntary loss of skeletal mass which occurs progressively over time at a rate of 1–2% per year, after the age of 50 years. This age related muscle atrophy is associated with decreased muscle strength, significant adverse effects on functionality, QoL and a direct link to morbidity and mortality associated with an increased prevalence in falls, Type II diabetes, cognitive dysfunction, and probably breast cancer.
Advances in the basic sciences have identified a number of factors that are responsible for this muscle loss, and which are both preventable, and in some instances reversible. Included are alterations in muscle protein synthesis; mitochondrial DNA genomic mutations and dysfunction causing apoptosis; muscle specific metabolic receptors such as the PPAR and vitamin D receptors involved in glucose homeostasis; angiotensin-converting enzyme genotype and its relationship to muscle type (fast twitch muscle) and hence muscle power and physical function.
Translation of this and similar related research allows for three practical clinical practice recommendations: the objective screening for advancing muscle deterioration by midlife handgrip strength testing; the maintenance of healthy and functional muscle through nutritional supplementation (leucine, vitamin D); the reversal of mitochondrial induced aging with resistance exercise regimens; and the selection of drugs with relevant complimentary metabolic/pharmacologic pathways; ACE inhibitors for women with hypertension; thiazolinedione drugs for those with insulin resistant Type II diabetes; and protection against obesity associated free fatty acid induced insulin resistance.
Positive exercise associated outcomes include: improved cognition, memory and emotional well-being; decrease in hip fracture; reversal of metabolic changes associated with insulin resistance, obesity and cardiovascular disease; and reduction in the risk for breast cancer in post-menopausal women.
In the future, genomic technology will allow for specific individualization of age and time adjusted prescriptive nutritional and exercise regimens.
SY-15-04
NUTRITION IN THE POSTMENOPAUSAL YEARS: THE ROLE OF THE GYNECOLOGIST
Ronald Bossemeyer (Brasil)
Abstract not available at the time of going to press.
SY-16: “Houston, we have a problem”: the twisted flow of information on HRT
SY-16-01
“TO FEAR OR NOT TO FEAR, THAT IS THE QUESTION” BENEFITS AND RISKS OF HRT: THE CONSUMER'S PERSPECTIVE
Deborah Legorreta
LPA Mexico
Objective: To describe consumer's perspective and knowledge concerning benefits and risks of HRT in the last 4 years according to valid exploratory, open-population studies in different countries.
Method: Systematic review of literature via Internet using BiomedCentral, Pubmed and other specialized research tools with key words: HRT perception, beliefs, attitudes and psychosocial.
Results: Cultural beliefs influence knowledge and attitudes concerning the menopause and its treatment as well as fears and expectations related to HRT. Contrary to popular belief, media impact has not been as important in the acceptance and adherence of women to HRT treatment as doctor-patient relationship and clear information provided by specialized sources to general public even after the much publicized WHI and Million Women studies.
Conclusion: Doctor-patient relationship and the clear explanation of risks and benefits in simple language to consumers is key to ensure acceptance and adherence of menopausal treatments in general and HRT in particular.
SY-16-02
SCIENTIFIC DATA AND CLINICAL PRACTICE: PERCEIVED RISK BY THE PHYSICIAN
Peter H. M. van de Weijer
Gynaecologist, Gelre Teaching Hospital, Apeldoorn, The Netherlands
If I do not fully understand what the news is all about, how can I then communicate that news to my patients or comment on it to the media? But there is more. I have to explain to my patients that certain risks or probabilities are involved in the decisions we make. This turns out to be very time consuming when the media point in another direction. I have the feeling that every time I mention “risk” or “probability,” it is perceived by my patients as a dead certainty that should be eliminated.
But gradually over time a new point of view started to emerge. By solely putting the responsibility on someone else's shoulders, I was disregarding a most important issue: Why did my patients trust newspapers more than my expertise?
SY-16-03
JOURNALS AND THE MEDIA: A SHARED RESPONSIBILITY?
J. H. Pickar
Wyeth Research, Philadelphia, PA, USA
“The fundamental question in medical journalism is how best to identify, process, and report legitimate medical information to the general public … Medical information is part of an ongoing stream of experimentation and data production that typically grows out of past experiments and will undoubtedly change, often very quickly, with future experiments.”1 Additionally, research gains reliability through replication of results and consistency with the existing body of evidence.2
The etiology of investigator bias in scientific research include financial rewards, desire to improve health, peer recognition, funding dependency and hypothesis investment.3 Increasingly, scientists, institutions, and journals are seeking to set the agenda for the press and shape the content of science news.2,4 Although medical journals operate in a genteel environment, competitive forces are present.5 Steinbrook noted, “Press releases, whether the work of universities, manufacturers, organizers of medical meetings, or medical journals, inherently involve self-interest.”6
The impact of a publication on other authors can be measured by how frequently the publication is cited.7 However, the importance given to impact factors can bias manuscript acceptance.5 Recently the editor of the Journal of the American College of Cardiology expressed his concern over the competition between journals and specifically that the competition may be influencing their behavior. His greatest concern related to seeking media exposure. “The ability to attract media attention appears to have become a criterion of a successful journal … this media orientation has the ability to influence the selection of manuscripts and the portrayal of their results.”5 DeMaria viewed the attempt to couple major media coverage with expedited publication of manuscripts as a negative influence, if it was intended to endorse the importance of the paper and the journal.5
A well known journalist recently noted in regard to one prominent clinical trial, that what it really “taught us was a lot more about the media, medical reporting and how women react to health information.”8 There can be little question that journals and the media have a shared responsibility to accurately communicate and place in proper context medical information.
SY-17: Osteoporosis management: state of the art (ESCEO)
SY-17-01
DETERMINANTS OF BONE FRACTURE RISK: BONE STRENGTH VERSUS BONE MASS
Pierre D. Delmas
Inserm Research Unit 831 and University of Lyon, Lyon, France
Bone mass/density is a major determinant of bone strength and of bone fragility in osteoporosis. It is the basis for the diagnosis of osteoporosis based on bone mineral density measurement by dual energy X ray absorptiometry (DXA). The WHO has proposed to define osteoporosis as a T score ≤ −2.5, and that has been endorsed worldwide.
However, several studies have shown in the past five years that half of fragility fractures occur in postmenopausal women that have a bone mineral density T score above −2.5. The majority of them have osteopenia, i.e. a T score between −1 and −2.5. Although their absolute risk of fracture is significantly lower than in osteoporotic women, they are at least three times more numerous, thus contributing significantly to the burden of osteoporotic fractures.
This finding reflects the complexity of fracture risk in postmenopausal women that depends on several parameters that are independent of the level of bone mass/density. For example, women with a history of fractures after the age of 45, as well as women with high levels of bone turnover markers have a significantly greater risk of fracture than women of the same age and BMD level but without these independent risk factors.
A large meta-analysis of 12 prospective cohorts of men and women over the age of 50 has identified a number of clinical risk factors that contribute to skeletal fragility independently of age, sex and BMD. An algorithm has been developed (the FRAX tool) that should be available soon and that allows to estimate the ten-year risk of fracture at the hip and the four major sites (hip, clinical vertebral, wrist and shoulder) by using these risk factors, with or without BMD.
Over the next few years, it is likely that the decision to treat or not will be based on the absolute risk of fracture, rather than on the level of BMD. Studies are in progress to verify that women selected in that way will have the same response to anti-osteoporotic treatments than those selected on the basis of BMD.
SY–17–02
HOW TO DEFINE COST-EFFECTIVENESS OF ANTI-OSTEOPOROSIS TREATMENT?
John Kanis (UK)
Abstract not available at the time of going to press.
SY-17-03
TREATMENT OF POSTMENOPAUSAL OSTEOPOROSIS: WHO, WHEN AND WHY?
René Rizzoli (Switzerland)
Abstract not available at the time of going to press.
SY-17-04
NEW DEVELOPMENTS IN THE MANAGEMENT OF OSTEOPOROSIS
Jean-Yves Reginster
Department of Public Health Sciences, University of Liège, Liège, Belgium
The three main determinants of the success of an anti-osteoporosis treatment are its ability to reduce fractures at spinal and non-spinal sites, its long-term skeletal and non-skeletal positive risk/benefit ratio and the adherence of patients to this particular treatment. Bisphosphonates are the most widely prescribed drugs in osteoporosis, worldwide. However, if their anti-fracture efficacy has been extensively demonstrated, daily and weekly formulations are facing a dramatic lack of long-term adherence with more than 50% of the patient discontinuing treatment within 12 months. Therefore, compounds which potency allows to increase intervals between dosings have been developed. Monthly oral ibandronate, quarterly intravenous ibandronate and yearly intravenous infusions of zoledronic acid are linked to outstanding anti-fracture efficacy. This may just reflect the increase in drug potency and patients' compliance. New SERMs are developed to maintain the spinal anti-fracture efficacy observed with raloxifene, together with an effect on hip fractures and, if possible, no increase in deep venous thrombosis or hot flushes. Bazedoxifene and arzoxifene are the latest candidates, for which phase II are promising, whereas results from phase III are expected in the coming months. Strontium ranelate has a unique mode of action. It is the only compound, so far, which concomitantly reduces bone resorption and stimulates bone formation. This effect translates into an increase in bone density, an improvement of trabecular and cortical micro-architecture, eventually resulting in fracture reduction at the spine, non-vertebral, major non-vertebral and hip sites. This compound is the only one, today, for which 5-year prospective, double-blind, pre-planned studies have shown a reduction of 43% in hip fractures. The scatter of efficacy of this compound ranges from osteopenic to elderly patients. New developments include non-injectable forms of parathyroid hormone (e.g. oral, subcutaneous … ), monoclonal antibody against RANKL (denosumab), non-oral bisphosphonates (e.g. percutaneous … ) and drugs aiming at specifically increase bone formation (e.g. monoclonal antibody against sclerostin) or to uncouple bone formation from bone resorption (inhibitors of chloride channel). The armentarium for the management of osteoporosis has incredibly improved, during the last ten years. However, there is still room for compounds associating a unique mode of action, translating into a high anti-fracture efficacy, coupled with long-term safety and, a mode of administration which is user-friendly enough to ensure long-term adherence to treatment.
SY-18: Urinary incontinence and the role of preventive urogynecology
SY-18-01
URINARY INCONTINENCE AND THE ROLE OF PREVENTIVE UROGYNECOLOGY
Khunying Kobchitt Limpaphayom
President, Thai Menopause Society; Department of Obstetrics & Gynaecology; Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand
Urinary incontinence is an underreported problem for many women. It is a common medical condition. Many women often wait very long before they seek treatment due to misconception that incontinence is normal for ageing. Overall prevalence of urinary incontinence in women is low in Asia Pacific when compared to western world. Age prevalence is between 45–65 years. Thai study in slum area by face-to-face interview found symptom started at average age 58.9 years and only 15.1% of those think it is a problem.
Urinary incontinence is a chronic health complaint that severely reduces quality of life. The impact of incontinence in women interfere with quality of live, sexual and family problem, loss self esteem and lost of opportunity. Prevalence of urge incontinence increases linearly with age especially perimenopause.
Incontinence is not always preventable, but may be able to decrease the risk. Pelvic floor muscle training is effective but not suitable for everyone due to long term compliance and not sure how to perform correctly. Hormone therapy can be both topical and systemic.
SY-18-02
PATIENT CHARACTERISTICS AND QUALITY OF LIFE IN WOMEN WITH URINARY INCONTINENCE
Montserrat Espuña (Spain)
SY-18-03
THERAPEUTIC APPROACHES TO URINARY PROBLEMS
Göran Samsioe
Department of Obstetrics & Gynaecology, Lund University Hospital, Lund Sweden
Impaired control of micturition is reported by almost 40% of postmenopausal women. It could follow or be part of various neurologic diseases and injuries such as stroke. Intensity and severity vary warranting different strategies. Pelvic floor exercise can be recommended to almost all women with urinary problems irrespective of type, intensity and severity. It can also be combined with other modes of treatment be it pharmacologic or non pharmacologic. For more specific treatment modalities a diagnosis as precise as possible is pivotal as treatment could be very different.
Stress incontinence most commonly diagnosed at midlife is best handled by a surgical approach such as TVT even if SNRI analogues have been reported effective in this condition. Special designed vaginal devices with or without electrical stimulation could also be tried. Estrogen therapy, however, may even worsen the condition.
Urge incontinence often diagnosed at a more advanced age is more difficult to treat but anti muscarinic drugs are often considered first choice. Estrogens given systemically or locally are also effective and may work synergistically with other drugs. A low dose local approach is often recommended as it does not require progestogen co medication. This is not simply due to the low dose but also to venous-arterial counter current mechanisms available in vessels adjacent to the vaginal mucosa. Local estrogens are available as cream, vaginal tablets an rings. Alpha adrenoreceptors are also effective. In severe cases botulinum toxin could be attempted. However, it is expensive and may require multiple installations.
Overactive bladder with similar symptoms as urge incontinence is commonly treated likewise.
SY-19: Discussion: This house believes that those women with the greatest increase in breast density with HRT are at the greatest increase in risk of breast cancer
Chairpersons: Malcom Whitehead (UK), Jo Marsden (UK)
Proposer: Bo von Shoultz (Sweden)
Opposer: Jean Michel Foidart (The Netherlands)
SY-20: Guidelines to best practice in menopause medicine
SY-20-01
CLINICAL MANAGEMENT OF ABNORMAL BLEEDING ON HRT
D. W. Sturdee
Solihull Hospital, Solihull, UK
Bleeding during HRT remains an important issue for patient acceptability as well as physician concern about the implications. It is more common around the time of the menopause when underlying ovarian activity may conflict with the HRT regimen, but the possibility of endometrial pathology is also increased at this time. The merits of how to manage and if or when to investigate are constantly debated. Changing of a sequential regimen to one with a more potent progestogen can be helpful. Intrauterine delivery of progestogen is the most logical route of administration and provides a high level of progestogen directly to the endometrium with good endometrial suppression and often no bleeding. This can also be a most satisfactory method of controlling perimenopausal bleeding problems before starting HRT and can be continued through the transition to maintain the endometrial suppression and protection when estrogen is added for menopausal symptom relief.
Persistent abnormal bleeding requires investigation by outpatient endometrial biopsy and/or ultrasound scan initially, followed by hysteroscopy if indicated. Bleeding during continuous combined estrogen/progestogen therapy that persists after six months or more from initiation or starts later will usually warrant investigation. The incidence of bleeding is related more to the dose of estrogen than the progestogen and the development of new low dose therapies containing 0.5 mg oral estradiol, 0.3 mg oral conjugated equine estrogens or 14 μg estradiol daily by transdermal patch is associated with less bleeding and thus greater patient acceptability as well as minimal endometrial stimulation.
SY-20-02
NON-RESPONDERS TO HRT: THE CLINICAL CHALLENGES
S. O. Skouby1,2
1Department of Obstetrics and Gynecology, Herlev Hospital, Faculty of Medical Science, University of Copenhagen, Denmark; 2Department for Thrombosis Research, Institute of Public Health, University of Southern Denmark
Since the publication of the Women's Health Initiative (WHI) study and the results from the Million Women Study (MWS), the role of hormonal replacement therapy (HRT) in postmenopausal women has been challenged. For most gynecologists postmenopausal HRT still occupies a clear clinical position in order to attenuate degenerative body changes along with prevention of vasomotor symptoms. Nevertheless, as a result of the adverse publicity, there has been a manifest decline in HRT usage ranging from 40% – 60% with the most outspoken downturn in the US. The question may therefore be raised: How do we manage the clinical challenges in non-responders to HRT? To answer this, it should be emphasized that the epidemiological data have not only been wrongly extrapolated in relation to the clinical settings (age, BMI, co-medication), but also to the whole class of therapies. An example is the various progestogens available for HRT. The compounds exert different partial effects at cellular level according to the biochemical composition. Some have particular antimineralocorticoid effect and some more pronounced antiandrogenic activity while others mimick more closely the effect of natural progesterone. The structural differences the various progestogens result also in a variety of metabolic and hemostatic changes. Moreover, the dose and route of HRT administration translate into differential effects on vascular function. New products are now being developed which maintain benefits and minimize risks. New low- and ultra-low-dose oral appear to maintain benefits for symptom relief and osteoporosis whilst minimizing side-effects and risks. Basic research indicates that both natural estradiol and progesterone may influence physiologic control of eating, basal body energy expenditure and fat disposition. Weight gain tends to occur after the menopause in women whether or not they choose HRT, but untreated women seem to have a threefold higher increase. Estrogen therapy modulates serum leptin levels, reduces the accumulation of fat around the waist by down regulation LPL activity of visceral adipocytes. This may also explain a hypothesized increase in insulin sensitivity. The physiological and the metabolic changes are, however, dependent on the estrogen/progestogen composition and administration form. A non-hormonal option, desvenlafaxine, a serotonin and norepinephrine reuptake inhibitor (SNRI), experienced a significant reduction in moderate to severe vasomotor symptoms and may address some of the clinical challenges in HRT non responders. Additionally, a selective estrogen receptor modulator/conjugated equine estrogen preparation combination is showing encouraging data and should provide a further option for women who will not respond to traditional HRT.
SY-20-03
DO HRT EFFECTS DEPEND MORE ON ROUTE OR ON DOSE?
Tim Hillard
Poole Hospital NHS Foundation Trust, Poole, Dorset, UK
The beneficial effects of HRT, either as estrogen alone or in combination with progestogen, on vasomotor symptoms have been clearly established for over 30 years. As with many other pharmacological treatments, once a “standard” dose becomes established there is a constant background of research to identify whether lower doses may be equally effective with reduced side-effects. Using vasomotor symptoms as the benchmark, the effective dose of HRT has moved from low dose to very low dose and now to ultra low dose, a process given added impetus since the publication of damaging studies on HRT safety. Thus even very small doses of systemic estrogens appear to effectively relieve vasomotor symptoms but the effects of these very small doses on bone and cardiovascular disease health are less clear. Whilst there is no doubt that some estrogen is better than no estrogen for maintaining bone density there are no fracture data to support the use of the lowest doses in women at increased osteoporotic risk. The use of additional progestogen may potentiate the benefits of estrogen on bone but equally may adversely affect cardiovascular disease and breast cancer risk. Although there is an assumption that lower doses will mean lower risks, this has not yet been substantiated in large scale clinical trials.
Different routes of administration have different pharmacokinetic profiles although the clinical relevance of these differences remains uncertain. Some of the differences in the metabolic and haemostatic effects of different routes of administration are potentially clinically important. For instance oral estrogens have greater beneficial effects on lipids and lipoproteins, glucose and insulin metabolism thus women with lipid abnormalities or impaired glucose tolerance should be specifically treated with oral estrogens. In other situations, such as a personal or relevant family history of venous thrombosis, transdermal preparations, which have less effects on coagulation and haemostatic mechanisms, are recommended. For the vast majority of patients the route of administration is not important provided adequate estrogen levels are achieved. The absence of large scale studies on the long-term safety of non-oral HRT does not mean that we can assume that the risks that apply to oral treatment don't equally apply to non-oral.
Ultimately the lowest effective dose of HRT should be prescribed for a specific indication. The choice of route will come down to personal and physician preference but the availability of different routes, doses and combinations of hormones allows HRT to be tailored to the individual.
SY-20-04
HOW TO EVALUATE THE RISK-BENEFIT RATIO?
Henri Rozenbaum
In 2002, the first publication of the Women Health Initiative Study (WHI) showed an overall negative risk-benefit ratio of hormone therapy (HT) with o.625 mg of conjugated estrogens plus 2.5 mg of medroxyprogesterone acetate.
However since 2002, a number of data have challenged the WHI's conclusions:
examination of subgroup analysis of the WHI has demonstrated different effets of HT according to timing of initiation and age of the patients leading to the “critical window” theory: HT stated early after the menopause may slow the progression of coronary atherosclerosis;
as far as breast cancer risk is concerned, the estrogen therapy arm of the WHI has not reported an increased risk; the same applies to a french cohort study showing no increase in risk after 8 years of use of progesterone or dydrogesterone plus estradiol;
a French case-control study has shown no increase on venous thrombo-embolism risk with the cutaneous way of administration of estrogen.
Using low-dose HT and perhaps the cutaneous way of administration of estrogens, at least in women at risk of thrombosis, may definitively improve the risk-benefit ratio of HT if the treatment is used soon after the menopause.
SY-21: Alternatives to HRT for climacteric symptom
SY-21-01
ROLE OF SSRIS/SNRIS ON VASOMOTOR SYMPTOMS
N. Panay
Queen Charlotte's & Chelsea Hospital and Chelsea & Westminster Hospital, London, UK; Honorary Senior Lecturer, Imperial College, London, UK
A significant amount of evidence is accumulating for the efficacy of SSRIs and SNRIs as alternatives to HRT in the treatment of vasomotor symptoms (VMS). Although the exact cause of VMS is unknown, they are thought to result from thermoregulatory dysfunction, initiated at the level of the hypothalamus due to estrogen withdrawal. This estrogen withdrawal is thought to influence the function of the neurotransmitters serotonin and noradrenaline. These neurotransmitters are hypothesized to play an important role in the maintenance of temperature homeostasis.
There are published clinical data for relief of vasomotor symptoms with SSRIs such as fluoxetine and paroxetine and for the SNRI venlafaxine. However, the published studies thus far been of short duration and small magnitude, usually concentrating on breast cancer sufferers. Additionally the relatively high incidence of nausea in these studies has lead to frequent withdrawal from therapy before maximum symptom relief efficacy has been achieved.
DVS is the succinate salt of the major metabolite O-desmethylvenlafaxine of venlafaxine. DVS blocks the reuptake of both serotonin and noradrenaline causing an increase in their levels in the extracellular spaces in the brain. It has been developed with the aim of maximizing the benefits of SNRIs whilst minimizing their side effects. In a recent phase III clinical development programme, postmenopausal women with at least 7 moderate-to-severe hot flushes per day or at least 50 per week were enrolled in 2 multicentre, double-blind, placebo-controlled trials with study durations of 26 and 52 weeks, and in one 12-week, multicenter, double-blind, active comparator and placebo-controlled trial. A total of 1555 subjects who received DVS (n = 986), tibolone (n = 164), or placebo (n = 405) were included in the intention-to-treat population for the efficacy analysis.
In each of the 3 trials, all groups achieved a significant decrease from baseline in the number and severity of moderate-to-severe hot flushes at weeks 4 and 12. DVS 100 mg and 150 mg consistently achieved an approximately 60% to 65% reduction from baseline in the number of moderate-to-severe hot flushes compared with approximately 50% for placebo. DVS had a rapid onset of efficacy consistent across all 3 trials. The main adverse effect was nausea, which usually improved with time. There were also some discontinuation symptoms. Further studies have addressed these issues by up titration of the dosage at the start of therapy and tapering of the dosage at the end of therapy.
SY-21-02
SAFETY AND EFFICACY OF ISOFLAVONES FROM SOY AND RED CLOVER
Stacy Geller (USA)
SY-21-03
THE EFFECT OF FOOD WITH ISOFLAVONES IN CARDIOVASCULAR AND OSTEOPOROSIS PREVENTION
Dimitri Tsangalis1, Gisela Wilcox2, Nagendra Shah1 and Lily Stojanovska1
1Victoria University, Melbourne, Victoria, Australia; 2Monash Medical Centre, Melbourne, Victoria, Australia
Isoflavones found abundantly in soybeans are structurally similar to estrogen and thus able to exert weak estrogenic effects. Epidemiological and clinical studies have associated isoflavones with the prevention of hormone dependent disorders such as in post-menopausal women. Fermentation of soymilk with probiotic bifidobacteria metabolises daidzein into equol. Findings from earlier clinical studies on the potential positive effects of isoflavones on cardiovascular and osteoporosis risk factors in postmenopausal women have been highly variable and inconclusive. The objective of this study was to examine the effects of ingesting a fermented soymilk containing viable bifidobacteria on serum lipid profiles, bone turnover markers and levels of FSH, LH and SHBG in postmenopausal women.
Thirty-six post-menopausal women were involved in a randomised, double-blind, placebo-controlled, parallel study involving a 12-week supplementation of fermented soymilk (FS), non-fermented soymilk (NFS) and casein-milk (CAS). Subjects in the FS and NFS group ingested the same dosage of isoflavone at 80 mg per day. Populations of B. animalis in fermented soymilks were 107 to 108 viable cells per mL. At baseline and endpoint, hormones, lipids, osteocalcin and β-CrossLaps were analysed in serum and deoxypyridinoline in urine.
There was no significant differences in either BMI (P = 0.24) or bodyweight (P = 0.14) between the three groups. After 12 weeks of milk supplementation, there was no significant change in mean bodyweight from baseline measurements for any of the groups. Supplementation of FS and NFS caused a decrease in the levels of FSH and LH (P > 0.05). Moderate rises in SHBG were observed in the groups consuming the NFS and FS. There were no significant differences between baseline and endpoint means of total cholesterol, triglyceride and LDL-cholesterol (P>0.05). Ingestion of FS showed a trend toward a reduction in bone resorption, with urinary DPD decreasing by 2.4 nmol/mmol of CRE, but no significant difference was evident between baseline and endpoint means of the FS group (P = 0.16). In contrast to the increase in DPD excretion shown by women in the NFS and CAS group (10.3% and 3.3%, respectively), women consuming fermented soymilk showed a 17.3% reduction in the urinary excretion of DPD (P = 0.05).
Preliminary findings show that FS may prevent bone loss in postmenopausal women. However, further studies with a larger number of subjects per group are required to evaluate trends showing a positive effect on hormones, bone formation and cardiovascular disease risk.
SY-21-04
WHY SHOULD PHYTOESTROGENS BE OR NOT BE RECOMMENDED?
W. Wuttke
Georg-August-University of Goettingen, Robert-Koch-Str. 40, D–37075 Goettingen, Germany
Objective: Due to negative press reports about classical hormone replacement therapy drug and food additive companies are seeking for alternatives for the treatment of climacteric complaints and postmenopausal diseases such as osteoporosis. Currently two strategies are being pursued.
Design and Methods: Review of the international literature and own results.
Strategy 1: Plant derived substances with estrogenic effects – so called phytoestrogens – are being advertised as selective estrogenic receptor modulators with beneficial effects on climacteric complaints and in the bone but with no effects in the uterus or mammary gland. Recent studies however, raised concern about the safety of soy or red clover containing preparations which contain phytoestrogens, particularly genistein. Genistein was shown to stimulate growth of carcinogen induced mammary tumours as well as uterine tissue in rodents. These effects are typically for estrogen receptor alpha mediated effects. Phytoestrogens have minimal effects on climacteric complaints and on but putatively hazardous effects in the uterus and in the mammary gland. Therefore, most recent reviews conclude that soy/red clover/isoflavones should not be recommended over a longer period of time.
Strategy 2: climacteric complaints are generated in the limbic/hypothalamic structures of the brain where the lack of estrogens cause a derangement of neurotransmitters. Therefore, another approach to ameliorate climacteric, psychosomatic complaints is the use of neurotropic drugs. One plant extract used for decades for the treatment of climacteric complaints and with proven effects is Black cohosh (Cimicifuga racemosa). The best explored extracts are of European origin and a vast amount of literature exists for two German preparations (Klimadynon, Remifemin). For Black cohosh preparations it was shown that they contain serotoninergic as well as dopaminergic components and this is most likely the mechanism by which they ameliorate climacteric complaints. Since all Black cohosh preparations studied so far do not contain estrogenic compounds they stimulated neither mammary gland tissue including carcinogen induced tumours nor did they exert estrogenic effects in the uterus. Surprisingly however, they partially prevented the development of osteoporosis following castration of rats by a mechanism which involved an inhibition of the osteoclast differentiation factor RANKL.
Conclusion: Phytoestrogens have similar effects to classical estrogens used in HRT preparations whereas Black cohosh preparations act primarily via neurotropic mechanisms to ameliorate climacteric complaints.
SY-22: Breast cancer prevention and breast cancer patients
SY-22-01
STRATEGIES TO REDUCE BREAST CANCER RISK
J. Calaf-Alsina
Department of Obstetrics and Gynaecology, Hospital de la Santa Creu I Sant Pau. Barcelona. Spain
Risk reduction implies positive modification of risk factors. Some of them as geneder or genetics imposible to change. Consequently we have to restric our actions to enviromental conditions favorizing epitelial cell progression to neoplasia. Several epidemiologic evidences point to estrogen priming throughout life as a major breast cancer inducer. Consequently interventions shuold focus on reducing exposure to high estrgen levels. Healthy life measures such physical activity, adequate body weight or diet have lend controversial results in several obeservational or randomized controlled trials.
Nuliparity has been shown to be more risky as compared to early first pregnancy and lactation.
The use of hormonal contraception increases non significantly the risk in some subsets of late reproductive age actual users. The real impact of postmenopausal hormone therapy, either with estrogens alone or combined to progestogens is controversial. The use of the lower necessary dose to treat the symptoms will probably decrease the effect of these treatments.
Long periods of amenorrhea, either spontaneous or inducedand early oophorectomy also decreasethe future incidence of breast cancer.
Pharmacological intervention with substances like SERMs competing with estradiol at the receptor level have shown their ability to decrease brest cancer incidence in high risk or general population. Reducing the availability of estrogens to the epitelial mamary cell with aromatase inhibitors has shown to significantly decrease relapse or new primary tumors in women with previous cancers. This family of substances are now under evaluation as prevention tools. However the efficency of these treatments is very much related to the level of risk of the selected population. The side effects are not negligible and include endometrial cancer or cataracts in the case of Tamoxifen, venous thrombotic events for both Tamoxifen and Raloxifene.
Osteoporosis, joint pain and potential impairement of the long term cognitive function are the threats of aromatase inhibitors use.
There are also low quality evidences of a potential protective effect of prostaglandin synthesis inhibitors or statins which need further evaluation.
In cases where a high risk genetic mutation has been detected (BRC 1 and 2) and the reproductive project has been completed prophilactic mastectomy can also be considered.
Also in this subgroup of patients the alternative of pre-implantational genetic diagnosis to avoid the transfer of affected embryos is to be taken into account when counselling on reproduction.
SY-22-02
TREATMENT OF MENOPAUSAL SYMPTOMS IN BREAST CANCER SURVIVORS
J. Marsden
King's Breast Care, King's College Hospital NHS Foundation Trust, London, UK
Oestrogen deficiency symptoms are common in breast cancer survivors. They can arise as a result of a natural menopause, as a side effect of endocrine breast cancer therapy that reduces endogenous oestrogen synthesis or reduces oestrogen activity (i.e. the anti-oestrogen, tamoxifen). In premenopausal women oestrogen synthesis is reduced by ovarian suppression and in postmenopausal women by aromatase inhibition. Chemotherapy has a direct cytotoxic effect and in premenopausal women additionally confers benefit by suppressing ovarian function. This latter mechanism of action is associated with an increased risk of premature ovarian failure.
Vasomotor symptoms (i.e. hot flushes and night sweats) and sexual dysfunction following hormone depletion are particularly difficult clinical problems to manage in breast cancer survivors. This is due to the fact that most cancers are hormone sensitive and the safety of ‘add-back’ hormone replacement in this clinical context is uncertain. HRT may be safe in women with oestrogen receptor (ER) negative disease or those with ER positive cancer who are also using tamoxifen as theoretically this will prevent stimulation of occult malignant disease by blocking the oestrogen receptor. The premature closure of three large randomised trials of hormone replacement therapy (HRT) and most recently the randomised LIBERATE trial of tibolone in symptomatic women with early stage breast cancer due to concerns about the risk of recurrence means that this question will remain unanswered. There is additionally growing concern about systemic absorption from vaginal oestrogens despite an absence of any evidence showing a detrimental impact on survival.
Unfortunately available evidence for alternatives to HRT advocated in this clinical context is disappointing. Whilst sort-duration (i.e. only weeks) use of other prescription medicines such as SSRIs, gabapentin and low-dose progestins appear to confer significant symptom relief compared with placebo, longer-duration evidence is less convincing. Surveys suggest patient preference for complementary therapies. Again there is a lack of data to support any herbal or plant extracts as effective treatments for vasomotor symptoms, some of which exert weak hormonal activity and may not prove to be advisable if used concomitantly with endocrine breast cancer therapies. Non-pharmacological complementary therapies such as homeopathy and acupuncture have yet to be shown to be efficacious in controlled studies. Cognitive behavioural therapy (CBT) however does appear promising with preliminary research suggesting benefit extending beyond the active intervention time.
SY-22-03
RATIONALE FOR CHEMOPREVENTION IN BREAST CANCER
E. Kubista and G. Pfeiler
Adjuvant tamoxifen therapy reduces significantly the risk of contralateral breast cancer, thus indicating that this SERM may be active in prevention of primary breast cancer. Based on the results of the NSABP–1 trial, which evaluated the effect of tamoxifen on the incidence of invasive breast cancer, the FDA approved its use as a chemopreventive agent in women at increased risk according to the Gail's model. Three further trials (Italian trial, Royal Marsden trial, IBIS-I) underlined the efficacy of tamoxifen in preventing breast cancer in high risk women.
In the MORE/CORE trial raloxifene, another SERM, which behaves as an estrogen antagonist in both the breast and the endometrium, has been shown to reduce the incidence of newly diagnosed breast cancer by 66%, without any influence on endometrial cancer incidence. Raloxifene has been evaluated in comparison with tamoxifen in the STAR study, a large primary prevention trial of tamoxifen 20 mg vs raloxifene 60 mg for 5 years.
This lecture will give an overview of chemoprevention trials using SERM's to reduce breast cancer risk and will give an outlook toward aromatase inhibitors as chemopreventive agents.
SY-22-04: Prevention strategies of other diseases in breast cancer patients
Serge Rozenberg (Belgium)
Abstract not available at the time of going to press.
SY-23: Menopause in different cultural environments
SY-23-01
MENOPAUSE IN DIFFERENT CULTURAL ENVIRONMENTS – THE ASIAN PERSPECTIVE
D. A. Tan
United Doctors' Medical Center, Quezon City, Philippines
Menopause is a biological as well as a cultural event. Cross-cultural studies confirm the enormous differences in the experience of menopause among women in different cultures and even in the same culture. There are cross-cultural variations in symptomatology and response to menopause, in the concentrations of reproductive hormones, and in the burden of diseases associated with menopause.
Asia is a huge tapestry of cultural diversity and a singularly ‘Asian’ perspective of menopause is not possible. Not only are Asian women's experience of menopause different from Caucasian and other racial groups of women, there are also significant differences among Asian women themselves.
Several studies have documented the lower incidence of hot flushes among Asian women compared to women in North American, European, African, and Middle Eastern countries. Among nine ethnic groups of Asian women, the Pan-Asia Menopause (PAM) study showed considerable variations in the incidence of hot flushes and in the impact of menopause on quality of life. The most common menopausal symptom reported among Asian women was body aches/joint pains.
In the Study of Women's Health Across the Nation (SWAN), Chinese and Japanese perimenopausal women have lower estradiol and sex hormone binding globulin concentrations compared with Caucasian women and African American women. In the PAM study, levels of follicle-stimulating hormone, luteinizing hormone and particularly of estradiol differ substantially among ethnic groups of postmenopausal Asian women.
Postmenopausal Asian women, particularly Vietnamese, Chinese, and Thai women, compared to Caucasian women, have lower risks for breast cancer. Filipino women have higher prevalence of type 2 diabetes mellitus and the metabolic syndrome compared to Caucasian women. Compared to Caucasian women, the SWAN showed that Chinese and Japanese women have higher lumbar spine and femoral neck bone mineral density measurements and lower bone turnover rates. The incidence of hip fracture is lower in Asian postmenopausal women than Caucasian women.
Because of the diversity of racial and ethnic responses to menopause, no single approach to management will work everywhere. Understanding the interplay of biological and sociocultural factors with menopause will enable the physician to provide medically sound and culturally appropriate care.
SY-23-02
HOW COMPLEX IS MENOPAUSE IN A MULTICULTURAL SOCIETY? AN AFRICAN PERSEPECTIVE
Oscar C. Shimange
Medforum Medi-Clinic. Pretoria, South Africa
The approach to management of menopause was mainly based on a traditional belief that the symptomatology is due to physiological changes. This disregarded other factors which can influence the clinical presentation and hence have a direct influence on compliance to treatment. This paper is designed to look at these factors and also at the methodology that can be used to study these factors:
One to one interviews of perimenopausal, and menopausal patients, traditional healers, and elderly females in different community groups.
Literature search using Medline and Pubmed for articles related to menopause and complexity of presentation associated with cultural differences.
Informal discussion with patients already on treatment for menopause.
Thus subjective experience of menopause can be explained by language differences, culturally shaped expectations about menopausal transition and concerns about female ageing and associated social roles.
Thus it is evident that choosing tools to asses presentation of menopause is complicated by different menopausal symptoms manifesting during different stages of the climacteric. It is therefore vital that caregivers should recognise that variations exists and ask patients specific questions about specific symptoms and their impact on usual functioning.
SY-23-03
MENOPAUSE IN DIFFERENT CULTURAL ENVIRONMENTS – LATIN AMERICAN PERSPECTIVE
Nestor Siseles
University of Buenos Aires, Argentina
We are nowadays witnessing the fastest rate of world population growth in the whole of human history. Still, in the case of Latin America, growth is heterogeneous and there are wide differences across countries and, inside each particular country, there are also differences between urban and rural areas as well as among social classes and ethnic groups. Women make up the majority of the aged population in the countries of the region (1).
In Latin American women, the experience of menopause is determined by a combination of biological and sociocultural factors (2–3). The few studies carried out in several countries of the region disclose different attitudes towards the menopause, and much heterogeneity is observed. From a sociological viewpoint, the climacteric in Latin-American women can be divided into the phenomena observed in middle-and upper-class women from urban areas and those observed in rural areas. The diversity of social backgrounds and roles means that many different situations are encountered. Some women, after a late pregnancy, reach their menopause while still enjoying a clearly defined maternal role; other women define themselves by their role as grandmothers; childless women, or women whose family structure has shrunk, make up their social commitments, and so on. Women living in rural areas are supposed to be clearly aware of the changes they are undergoing, but they must keep silent about them because there is nowhere to discuss them and nobody to listen.
An anthropological research in Havana (Cuba) (4) found that women having to perform a job while also doing household chores showed a high incidence of menopausal symptoms, especially those related to emotional frailness (depression, anxiety, irritability) and diminished libido. In addition, this study concluded that menopausal symptoms ocurred more frequently when the family/couple was dysfunctional. In 1986, Barnett (5) studied a group of peruvian women. His most significant finding was that acceptance of, and adjustment to, the menopause were dependent on the woman's satisfaction with her main role in life. Two main roles stood out: that of the mother and that of the worker. Mothers whose children had not fulfilled their expectations experienced more difficulties during menopause, whereas working women, whose satisfaction depended not only on their children but also on their own achievements in life, responded better.
Thus each society constructs human life culturally, anthropologically, and socially, and each society endows the aging process with its own cultural meaning. Women's longevity appears to be a marked biological advantage, yet in Latin America, it is frequently blurred by the social and cultural disadvantages that women must confront.
We will present the preliminary report of our Study Project of Assessing a Scale of Quality of Life in Latin American Women. This project emphasises the need to consider the sociocultural environment's influence on the well-being experienced by women. The design includes as primary methods qualitative ethonographic and in depth-interviews, and work with focus groups that allow us to approach the categories defined by the women; this means, understand menopause as is understood and told by the protagonists themselves, considering their concepts and what meanings they assign to this vital stage.
SY-23-04
MAORI AND MENOPAUSE IN NEW ZEALAND
Beverley Lawton (New Zealand)
Abstract not available at the time of going to press.
SY-24: Treatment of hormone deficiency in the elderly couple
SY-24-01
THE ELDERLY COUPLE TODAY
M. H. Birkhäuser and C. Bodmer-Hindermann
Div. of Gynaecological Endocrinology and Reproductive Medicine, Dept. Ob/Gyn, Inselspital, University of Bern, Switzerland
Menopausal age did not change in the last 100 years. In contrast, life is still increasing. Today, women spend 1/3 of their lifetime after menopause. Sexuality is an important part of quality of adult life, independent of age. However, the importance of quality of life of the elderly couple, including sexuality, is still largely underestimated, although it is well known that quality of life highly influences the incidence and the duration of somatic and mental diseases, particularly in the elderly. Compared to earlier times, much more men and women start their life after fifty with a new partner, reflected by an increase of their sexual activity. Based on our own experience and on the literature, the following observations can be made for the couple after the age of fifty:
1. Men rate their quality of life better than women and have got a significantly higher self-confidence.
2. Men accept their physical appearance better and are more satisfied with themselves.
3. With increasing age, libido diminishes in both sexes if compared with earlier times, especially in women.
4. However, sexuality remains in the elderly couple an essential part of quality of life.
5. Men continue to put more value on having orgasms than women.
6. Within the elderly couple, men are more satisfied with their sexuality than their female partners.
7. To have a fulfilled sexuality, the importance of tenderness and of mental and spiritual correspondence with a trustworthy and well-known partner increases with age, particularly for women. Men often neglect this aspect.
SY-24-02
TREATMENT OF ANDROGEN IN MALE CLIMACTERIC
Iñigo Sáenz de Tejada (Spain)
Abstract not available at the time of going to press.
SY-24-03
ANDROGENS VS ESTROGENS ON THE ENDOTHELIUM
Tommaso Simoncini
University of Pisa, Pisa, Italy
The large randomized trials on hormone replacement therapy after the menopause have been received by the media as an unexpected failure of hormones to benefit the cardiovascular system. However, when the wealth of knowledge accumulated on how steroids affect vascular cells is taken into consideration, many of the findings of these trials can be more properly interpreted. Estrogen signaling through estrogen receptors is nowadays appreciated as being much more complex than it was once thought. Acting through a rapidly growing number of signaling intermediates estrogen receptor are powerful regulators of vascular cells and tissues and play a relevant role in the modulation of vessels in physiological and pathological conditions. However, relevant differences may exist as to the actions plaid by sex steroids on male or female cells. A growing interest stays in the understanding of the actions of androgens on the cardiovascular system. Recent evidence seems to indicate that androgens are not necessarily dangerous to vascular cells, but rather their effects can be beneficial if used in a right concentration range. This opens a whole new area of investigation, that could expand significantly the relevance of substituting androgens, in addition to estrogens, after the menopause. Overall, these concepts suggest that protective effects of sex steroids on the vessels are likely, but may be limited to a specific “window” of exposure, that is early after the menopause, and possibly to specific hormonal preparations, doses and ways of administration. While the available clinical trials do not address these hypotheses, new studies are currently undergoing that may in the future shed light on this highly controversial clinical field.
SY-24-04
THE CLIMACTERIC IN THE FUTURE …
Manuel Neves-e-Castro
CFH-Clinica de Feminologia Holistica, Lisbon-Portugal. E-mail: [email protected]
The future of the climacteric is aging …
Active and healthy aging are the main objectives that contribute to a good quality of life that everybody desires and deserves no matter the age.
In order to accomplish these goals there are several strategies that must be adopted in order to identify and prevent risks that may lead to future chronic diseases. These must be taken into account at different ages. In what concerns the bone one should attempt to induce a high peak bone mass since the higher it is the lower is the probability of an early osteoporosis. The cardiovascular system must be protected at all times through a rational nutrition, regular exercise, abstention from tobacco smoking, normal body mass index and restriction of alcohol. The central nervous system (brain) must always be active. Stress should be avoided. The breast must be always under regular surveillance.
When the climacteric is felt one must prevent and treat the menstrual irregularities (anovulation) so frequent in the premenopause. Blood pressure and lipid profiles must be kept within the normal range for age. When vasomotor symptoms interfere with the quality of life specific treatments (hormonal) can be safely prescribed, if there are no contraindications, in addition to some other general measures. These treatments can continue as long as they are needed for that purpose; they can offer cardiovascular protection if started early after the menopause up to 60 years of age.
Most of the hormone related symptoms that affect the quality of life in elderly woman are genito-urinary related. Since the vagina, the bladder and the urethra are targets for estrogen action its deficiency is often manifested by vaginal atrophy, atrophic vaginitis, bladder dysfunctions and recurrent cystitis. Local and systemic estrogenic treatment is very effective to relief symptoms and protects the vaginal and the bladder epithelium from infections.
In elderly women (over 70 years of age) vasomotor symptoms are rare although some of them may still feel them, in which case very small and intermittent doses of systemic estrogens are indicated. Other than those conditions, systemic hormone treatments are not indicated.
However other hormone deficiencies should be taken into account, namely hypothyroidism and adrenal hypofunction for which specific treatments are indicated. Type 1 and 2 diabetes and growth hormone deficiency must also be investigated.
The role of the physician should not be confined only to pharmacotherapies. Instead the health care provider must always give all the necessary psychologic support during these difficult years of a woman's life, thus becoming her best friend and counsellor.
SY-25: Menopause and aging, quality of life and sexuality
SY-25-01
FEMALE SEXUALITY AND MENOPAUSE: CONCLUSIONS OF THE 6TH IMS WORKSHOP
Andrea R. Genazzani
University of Pisa, Pisa, Italy
On December 2006, from the 1st to the 4th, the IMS organized a 4-day conference focused on Menopause, Ageing, Quality of Life (QoL) and Sexuality. During the event, prestigious speakers, coming from all over the World, discussed the hot topics of the matter. Briefly, the consensus conference agreed that QoL needs to be considered the gold point of any medical approach. Healthy status represents the major determinant of QoL, in particular in elderly people but sexuality is also an important factor at all ages although it is less often a problem for women than for men. Therefore, QoL is strictly dependent on the gender and ageing status. Hormonal changes associated with ageing, particularly at menopause may deeply affect QoL. Therapeutic intervention such hormonal or non-hormonal treatment, targeting selected disease or components of the ageing process, can improve QoL and sexuality in both sexes. This presentation will review the discussion of the event and highlight the key statements issued during the conference related to: QoL is gender related; Sexuality is a pivotal determinant of QoL; Menopause and ageing deeply influence sexuality and therefore QoL; Therapeutic intervention may positively influence sexuality and QoL in males and females.
SY-25-02
AGING AND SEXUALITY IN WOMEN
R. E. Nappi1,2, F. Albani1,2, V. Santamaria1,2, S. Tonani1,2, C. Pisani1,2, A. Ornati1,2 and F. Polatti1
1Research Center for Reproductive Medicine, Dept of Morphological, Eidological and Clinical Sciences; 2Unit of Gynecological Endocrinology and Menopause, Dept of Internal Medicine and Endocrinology, IRCCS “S Maugeri Foundation”, University of Pavia, Italy
A large number of biological, psycho-relational and socio-cultural factors are related to women's sexual health at any stage of reproductive life and they may negatively affect the entire sexual response cycle inducing significant changes in sexual desire, arousal, orgasm and satisfaction.
In spite of the high prevalence of sexual problems with increasing age, sexual retirement is not an inevitable consequence of the passage of time and a high proportion of men and women remain sexually active well into later life, a result of changing attitudes toward sexuality and of the availability of effective treatments for sexual dysfunction.
A recent comprehensive review of population-based studies reported an age-related decline of sexual functioning and an additional adverse effect of menopausal status. Ageing per se interferes with the level of sexual performance but sexual behaviour of midlife and older women is highly dependent on several factors such as general physical and mental well-being, quality of relationship with the partner and life situation. Level of past sexual functioning, social class, education, employment, stressors, personality factors, socio-cultural environment and negative attitude towards the menopause play also a significant role.
A recent cross-national study of subjective sexual well-being among older women and men outlined that there was a gendered response, with men reporting higher levels of satisfaction than women, regardless of socio-cultural context. Despite substantial cultural variations, several predictors of subjective sexual well-being were consistent across world regions and being sexually satisfied physically, emotionally and relationally significantly correlated with overall happiness in both men and women.
Sex-steroids, mainly low levels of estradiol, are extremely relevant for sexual awareness and vaginal receptivity in naturally menopausal women. Even a significant lack of androgens, as it more frequently occurs in surgically menopausal women, has a negative impact on libido and sexual responsiveness.
At genital levels, estrogen modulate blood flow, peripheral nerve function, vaginal tissue structural integrity and, therefore, the process of lubrication, which is also influenced by testosterone (T). In addition, androgens directly modulate vaginal and clitoral physiology by influencing the muscular tone of erectile tissue and of vaginal walls. Within the central nervous system (CNS), estradiol (E2) plays a permissive role on sexual receptivity, while T contributes to initiation of sexual activity, permission and receptivity for sexual behavior. Finally, progesterone (P) and its metabolites may indirectly influence sexual receptivity by modulating mood and cognition, while the role on peripheral vaginal arousal is poorly understood.
SY-25-03
MENOPAUSE, HORMONES AND DEPRESSION
John Studd
London PMS Menopause Centre, 46 Wimpole Street, London W1G 8SD, UK
Depression is more common in women than men whether measured by hospital admissions, community studies or prescriptions of antidepressants. This excess may be environmental or hormonal. The argument for the hormonal component is that peaks of depression occur in women at times of hormonal fluctuation. This is (1) Puberty (2) Premenstrual (3) Postnatal and (4) Climacteric. Typically women with this propensity for reproductive depression are well during pregnancy, only to develop postnatal depression and then cyclical premenstrual depression when the periods recur. There is also strong evidence that depression in women is linked to an increase in osteoporosis, coronary thrombosis and non-suicidal deaths. There are now several randomised controlled studies to show that transdermal oestrogen will improve the depression in each part of this triad of hormone responsive mood disorders. The usual dose will be 200ug of oestradiol twice weekly. Those women with a uterus will need cyclical progestogen to prevent endometrial hyperplasia but as they are often progestogen-intolerant it is justifiable to decrease the usual duration to 7 days of progestogen each month. Measurement of hormone profiles are not helpful in the diagnosis but a good history is the key to recognition relating episodes of depression to periods, a history of having a good mood during pregnancy, a history of postnatal depression and the change from cyclical depression in young women to more constant depression in women in the two or three years before the cessation of periods. The problems encountered in the hormonal treatment of premenstrual depression, postnatal depression and peri-menopausal depression will be discussed. The tragedy is that psychiatrists have no interest in treatment with oestrogens as they are unfamiliar with the minor side effects of hormone therapy such as mastalgia and irregular bleeding. These can be dealt with by any competent family doctor but in the hands of psychiatrists these women are condemned to antidepressant therapy or worse.
(For further information see: www.studd.co.uk)
SY-25-04
SEX AND SEXAGENARIANS
L. Dennerstein1, J. R. Guthrie1, R. D. Hayes1, L. DeRogatis2 and P. Lehert3
1The University of Melbourne, Victoria, Australia; 2Sheppard Pratt Hospital, Baltimore, MD, USA; 3FUCAM, University of Louvain, Belgium
Objectives: To: (i) describe the change sexual function of women in their sixth decade; (ii) determine the prevalence of sexual distress (and sexual dysfunction) and (iii) the factors associated with and predictive of sexual distress in a population-based sample of mid-aged Australian-born women.
Design & Method: 11-year prospective study of Australian-born women, aged 45–55 years and menstruating at baseline. Validated measure of sexual function (the Personal Experiences Questionnaire [SPEQ] was completed in years 1 to 8 and 11 of follow-up and in the 11th follow-up year the Female Sexual Distress Scale (FSDS). A Total Sex Score of ≤7 from the SPEQ is indicative of low sexual function and a score of ≥15 on the FSDS represents significant sexual distress.
Results: 257 women were interviewed in the 11th year of follow-up. There was a significant decline in all domains of sexual function in the decade studied; women using hormone therapy in year 11 had significantly greater responsivity and higher frequency of sexual activities. 204 women completed both the FSDS and SPEQ questionnaires. 166 (82%) women had an SPEQ score of ≤7 of whom 37 (18%) had an FSDS score of ≥15 and were classified as having female sexual dysfunction. Logistic regression analysis found that female sexual distress was concurrently associated with higher depression scores (OR 1.31, 95%CI 1.10, 1.56) and more negative Feelings for Partner (OR 0.49, 95% CI 0.32, 0.76) and was predicted by prior negative Feelings for Partner (OR 0.31, 95% CI 0.14, 0.70) and a greater decline in Total Sex Score (OR 0.77, 95% CI 0.59, 0.99).
Conclusions: Chronological aging and hormonal levels have negative effects on sexual function. Only a minority of mid-aged postmenopausal women are distressed about low sexual function. Sexual distress is associated with depression and relationship factors.
SY-26: New challenges in menopause
SY-26-01
HORMONAL CHANGES DURING THE MENOPAUSAL TRANSITION: RECENT STUDIES
H. G. Burger1, G. E. Hale2, I. S Fraser2, C. L Hughes3 and D. M. Robertson1
1Prince Henry's Institute of Medical Research, Melbourne, Victoria 3168, Australia; 2University of Sydney, New South Wales 2006, Australia; 3RTI International Research Triangle Park, North Carolina 27709 USA
The progressive decline in follicle numbers and ovulatory function which characterise female reproductive aging are associated with a series of hormonal and physiological events that were classified into a number of stages by The Stages of Reproductive Aging Workshop (STRAW) in 2001. Late in reproductive life, while cycles remain regular, a rise in follicular phase FSH levels is observed in some women, described as Stage ‐3. The menopausal transition starts at STRAW Stage ‐2 (defined when there is a sustained change in menstrual cycle length by ≥7 days), with the initial hormonal event being a fall in the median follicular phase concentration of inhibin B, the major negative feedback regulator of pituitary FSH secretion. In a recent study of 77 menstrual cycles in regularly and irregularly cycling mid life women, FSH, luteinising hormone (LH) and oestradiol in ovulatory cycles increased with each progressive STRAW Stage, while mean luteal phase progesterone levels decreased. The levels of anti-Mullerian hormone (AMH) which reflect ovarian follicle numbers, declined more than 20-fold between STRAW Stages -4 (mid-reproductive age) and -1 (late menopause transition). Further analyses of the hormone changes showed that in some ovulatory cycles, there was a second, mid to late luteal phase rise in oestradiol levels, peaking in the late luteal phase. In about half of these cycles, the rise resulted in an LH peak and progesterone increase early in the subsequent cycle. When such cycles were omitted from the overall analysis of ovulatory cycles, there was no progressive difference in oestradiol or progesterone between the STRAW Stages, although the progressive elevations in FSH and falls in inhibin B and AMH still occurred. Classification of hormone levels in transition ovulatory cycles from this same database suggested that many were endocrinologically similar to those of mid-reproductive age cycle, except that they had significantly lower levels of AMH (cycle type‐1). Other cycles that were similar to the mid-reproductive age cycles showed elevated levels of follicular phase FSH, decreased inhibin B and an increased FSH to inhibin B ratio (type‐2). Such cycles correspond to STRAW Stage ‐3, but also occur at Stages ‐2 and ‐1. A third group showed evidence of a significant fall in luteal phase progesterone and a rise in LH (type‐3). These three cycle types reflect progressive loss of ovarian function associated with reproductive ageing. However, there is no specific pattern of hormonal change characteristic of STRAW stages ‐2 and ‐1 (early and late menopause transition).
SY-26-02
PHARMACOGENETICS IN MENOPAUSE
Irene Lambrinoudaki
University of Athens, Athens, Greece
Pharmacogenetics involves the investigation of the influence of DNA sequence variations on drug response. Pharmacogenetics has received much attention since the publication of the WHI results, as a possible tool for treatment individualization. Selected variants in genes related to the action or metabolism of sex steroids may modulate the risk for adverse events from hormone therapy. Furthermore, polymorphisms in genes involved in bone metabolism, such as the genes for estrogen receptors α and β, the vitamin D receptor or the collagen Iα gene may determine the response to antiosteoporotic treatment. Research is focusing in the post-WHI era towards identifying reliable and cost-effective genetic tests, so as to enable prediction of response to treatment and identification of the high risk patient, prone to develop adverse effects from treatment.
SY-26-03
ENHANCEMENT OF INDIVIDUALIZED HRT BY MOLECULAR MEDICINE
Johannes Huber
Factor V Leiden is the leading cause for constitutional thrombophilia. The relative risk for venous thrombosis is about 3–10 for heterozygotes and 50–100 for homozygote.
Prothrombin 20210A represented the second most frequent prothrombotic polymorphism humans.
Hormone replacement therapy has a partial prothrombotic effect; the knowledge of this polymorphism allows a risk assessment in the treatment of menopausal symptoms. 17-betaestradiol is metabolized in angiogenic (16-hydroxyestron) steroids and in more angiostatic (2-hydroxyestron) compounds. Cytochrom enzymes are involved in this metamorphosis of steroids, the knowledge of human genetic variation in these enzymes makes a modulation of estrogen metabolism possible. Macular degeneration and new neurodegeneration are challenges in the overages population and can be prevented partially also with hormone replacement therapy. Therefore polymorphism, which is associated with macula degeneration and neurodegeneration is important for advising the given patient.
SY-26-04
IMPROVING IMMUNITY IN THE CLIMATERIC YEARS
Farook Al-Azzawi
Gynaecology Research Unit, University Hospitals of Leicester, Leicester, UK
Immunity has evolved to protect the organism from noxious microenvironment. While mechanisms of defence are generally similar between sexes, sexual dimorphism in dealing with pathogens has been widely documented thus implicating gonadal steroids in modulating immune responses. A prime example of the role of oestrogen is the shift from cell destructive Th1 immune response to antibody-mediated Th2 in models of multiple sclerosis. In this presentation the focus is made on the lower generative tract (LGT). The cyclical changes in gonadal steroids influence key immunity-regulating molecules in the LGT, largely to spare an immune attack against spermatozoa. In the climacteric, the changes in LGT involves reduction in blood supply, raised vaginal pH, thinning of epithelial cells, altered composition of the extra-cellular matrix as well changes in tissue constituents of immune defences. This renders the atrophic vagina susceptible to pathogens, but the introduction of oestrogen will restore most of these changes. In treating women with intact uterus the addition of progestogens particularly as a continuous regimen with oestrogen may antagonise the protective effects of oestrogen and such mechanisms will be discussed. Progestagens bind the progesterone receptors but exhibit binding affinities to the glucocorticoid and androgen receptors as well. They also alter immunity to viruses such as HPV and HIV. In conclusion, vaginal immunity should be an important consideration in defining the HRT regimens for postmenopausal women.
SY-27: Breaking news
SY-27-01
FERTILITY IN THE PERIMENOPAUSE: NEW DATA
Rogerio Lobo (USA)
Abstract not available at the time of going to press.
SY-27-02
FERTILITY TREATMENT IN THE POSTMENOPAUSE
Ehud Margalioth
Abstract not available at the time of going to press.
SY-27-03
THE RESTAGE COLLABORATION'S REVISED RECOMMENDATIONS FOR STAGING REPRODUCTIVE AGING
S. D. Harlow1, K. Cain2, S. Crawford3, L. Dennerstein4, N. Fugate-Woods2, R. Little5, E. S. Mitchell2, B. Nan1, J. Randolph1, J. Taffe5 and M. Yosef1
1University of Michigan, Ann Arbor Michigan, USA; 2University of Washington, Seattle Washington, USA; 3University of Massachusetts, Worcester Massachusetts, USA; 4University of Melboune, Melbourne Victoria, Austalia; 5Monash University, Clayton Victoria, Australia
Objective: In July 2001, the Stages of Reproductive Aging Workshop (STRAW) proposed bleeding and hormonal criteria for defining onset of the early and late menopausal transition. STRAW's recommendations reflected expert consensus following review of emerging proposals from several cohort studies but were not verified empirically. STRAW recommended a shorter interval of amenorrhea than the current 90-days amenorrhea for late transition and >7-day change in cycle length for early transition. The ReSTAGE Collaboration (ReSTAGE) conducted a quantitative evaluation of the STRAW recommendations with the aim of reaching a consensusregarding optimal bleeding criteria for staging reproductive aging and ofproviding more precise guidance for use of hormonal criteria.
Design and Method: ReSTAGE used prospective menstrual calendar data from four cohorts (TREMIN (n = 735), Melbourne Women's Midlife Health Project (n = 216), Seattle Midlife Women's Health Study (SMWHS) (n = 279), and Study of Women's Health Across the Nation (SWAN) (n = 2270)) to comparatively assess proposed bleeding criteria for the the early and late menopausal transition. For each proposed bleeding criteria, we assessed frequency of, concordance in age at, time to menopause from and association with serum FSH. For FSH criteria we assessed association with bleeding criteria and FMP.
Results: supported the STRAW recommendation that 60-days of amenorrhea be used to define onset of the late menopausal transition. An annual serum FSH measure > = 40 IU/L is an independent marker of transition (but less predictive than bleeding criteria) and could be incorporated, in conjunction with bleeding markers, into the STRAW paradigm for markers of the late transition. Experience of hot flashes added no information in the presence of hormonal and bleeding criteria. The early transition may be best described by ovarian activity consistent with bleeding criteria of a persistent 7 or more day difference, as recommended by STRAW. Other proposed bleeding criterion for early transition are consistent with changes associated with the late transition.
Conclusion: This empirical assessment supported the STRAW recommendations thata)> = 60-days of amenorrhea be used to define the late menopausal transition and b) that early transition is consistent with a persistent 7 or more day difference in length of consecutive cycles. Serum FSH criterion could be incorporated into the STRAW paradigm to facilitate prediction of proximity of the FMP.
SY-28: Hormonal change and treatment during the menopausal transition
SY-28-01
POLYCYSTIC OVARIAN SYNDROME (PCOS) IN WOMEN IN THEIR FORTIES
Zion Ben-Rafael
Tel-Aviv, Israel
PCOS is one of the most common endocrinopathies that affects between 5 and 7% of the female population. This complex syndrome frequently affects young women who present with anovulation, menstrual disturbances, obesity, hyperandrogenemia, hirsuitism and infertility, all calling for immediate attention and treatment. However, PCOS also affects women later in life, pre and postmenopausal, when the long-term health implications add to the common age-related problem, but this is not as well defined and researched.
Polycystic ovaries (PCO), anatomical hallmarks of PCOS, occur 3–4 times more frequently than in PCOS. The prevalence of PCO decreases with age and weight loss. With the decrease in the number of oocytes over time, androgen (androstenedione, not testosterone) levels tend to be lower, cycles more regular and ovarian response to stimulation tends to weaken. The morphology of the ovaries remains typical in about 40% of patients, even after menopause.
During the last decade it became clear that some PCOS women have many features of metabolic syndrome (MS), such as insulin resistance (IR), hyperinsulinemia and hyperandrogenemia.
Whereas during adolescence and the reproductive age, menstrual disorders, hyperandrogenemia and obesity are central features, during menopause, IR, the risk of developing Type–2 diabetes mellitus (T2DM), visceral obesity and risk of cardiovascular disease (CVD) is of greater significance.
The incidence of MS in a population of PCOS patients was two-fold higher (43–46%) than that of the general population, with such patients having higher free testosterone and lower sex hormone-binding globulin levels than the controls.
Long-term epidemiological studies indicate that T2DM can be prevented by adequate lifestyle intervention, such as diet and physical activity. This implies that individual susceptibility to metabolic disorders may be more important than genetic background and that early detection and preventive measures can avert the long-term course of PCOS.
Although many markers of the risk of CVD, such as MS, vessel damage, endothelial dysfunction, proinflammatory state and coagulation factors, frequently aggregate in well-defined women with PCOS, the effect of these risk factors on the development of CVD is still unproven due to lack of longitudinal studies demonstrating that PCOS patients suffer more frequently from myocardial infarctions and strokes in later years.
In summary, PCOS represents a spectrum of clinical features, some of which can be averted by lifestyle or treatment, and some can resolve with age. However, long-range risks have been inadequately studied, and rarely receive the same level of attention as that of the fertile age symptoms, despite the fact that they can, to a certain extent, be prevented!
SY-28-02
MASTALGIA AND BREAST CANCER RISK
Jaen Christopher Thelobard (France)
Abstract not available at the time of going to press.
SY-28-03
BENEFITS VS RISK OF ORAL CONTRACEPTIVES DURING PERIMENOPAUSE
Parra A. Manuel1,2, Burgos S. Nelson1 and Carrasco S. Oriana1,2
1Departamento de Obstetricia y Ginecología, Hospital Clínico de la Universidad de Chile, Facultad de Medicina; 2Clínica Alemana de Santiago; Santiago Chile
Women in perimenopause period decrease their pregnancy rates, associated to a lower use of contraceptives methods, decreasing to a 77% in users between 40–45 years in comparison with a 92% between 25–29 years, with a raise of 70% in not wished pregnancies in women between 40–45 years, also with a raise of abortions in countries that allow it. Major risk of maternal death and of chromosomes pathologies is between 9 and 5 times higher in woman of 45 years.
The population in perimenopause increases especially in developed and under developed countries, which should be helpful to identify and handle the best contraceptive alternatives that suit this group.
In perimenopause, woman experiment a decrease of the ovaric functionality, with anatomical and hormonal changes, a decrease of spontaneous or assisted fertility and with this the appearance of hot flushes, mood changes, changes in the urogenital system and an increase of cardiovascular, osseous and mental diseases.
The question is, what to do during this period with the contraception. The present recommendation is to continue the use of a contraceptive for one year after the last menstrual period among 50 years old women (or older) and for two years in women under 50 years old.
A good contraceptive must carry out these tasks: prevent pregnancy, reduce hormonal fluctuations and provide additional benefits.
When the gynaecologist selects a contraceptive in any of these patients he/she should personalize the advice, educate about other benefits of the use of a contraceptive, and follow up the patient.
Generally the use of oral contraceptives (OC) in low doses have demonstrated benefits in climacteric symptoms, with a non significant effect in number or severity of hot flushes and sexual ambit, but with significant improvement in both physical and mental aspects. The additional benefits of OC in low doses demonstrated a significant increase in the mineral bone density, and a long lasting effect that may reduce the chance of a hip fracture.
New progestins like drospirenone have also additional benefits on premenstrual syndrome, acne and water retention improving the women wellbeing.
The use of OC are also a protection against gynaecological cancer, such as endometrial and ovary cancer. Nevertheless, the use is associated to a higher risk of cervix cancer and an unclear association with the risk of breast cancer. Meta-analysis indicates a very low increase in this risk though.
Finally among OC users the most important risk factors are : age, hypertension and smoking which increase the incidence of heart attacks and strokes. A thrombosis event is infrequent in users of OC. The facts of age and weight are more relevant in these cases than the kind of progestagen that is being used.
SY-28-04
HORMONAL INTRAUTERINE SYSTEM (IUS) FOR USE IN PERI- AND POSTMENOPAUSAL WOMEN
R. Sitruk-Ware
Population Council, and Rockefeller University, New York, NY, USA
The intrauterine system delivering levonorgestrel (Mirena®) initially developed as a long-acting method of contraception, has demonstrated its efficacy and safety in a large number of users all over the world. The local delivery of a small dose of a highly effective progestin in the uterine cavity maintains the endometrium in a non-proliferative state and reduces the number of bleeding days, thus preventing anemia, an important medical benefit, especially in developing countries. In addition, the intrauterine delivery of a progestin allows the treatment of other medical conditions and prevention of endometrial hyperplasia, in postmenopausal women receiving estrogen therapy. During the perimenopausal years, the IUS provides an effective contraception as occasional ovulations occur. In addition by its direct effect on the endometrium it prevents the occurrence of menorrhagia, a frequent condition in the preimenopause. After cessation of the ovarian function, when estrogen therapy may be initiated, the IUS would ensure endometrial protection as a transition to the menopause and as long as hormone therapy is needed. Although the circulating levels of levonorgestrel are very low, minor side effects related to the androgenic properties of LNG have been reported. In addition, the insertion of the system needs a skilled health provider and may be difficult or painful when the uterus is small or atrophic. The development of smaller devices is warranted for these specific situations.
Abstracts of Society Meetings
SM-01: Optimal menopause care – getting it right for women in Europe (organised by the European Menopause and Andropause Society)
SM-01-01
THE MENOPAUSEAL WOMAN AND BONE PROTECTION
David H Barlow
What should a woman at the menopause who wants to avoid osteoporosis be advised to do? We know that accelerated bone loss commences at the menopause; we know that this loss can be prevented by means of therapy and a range of effective therapies is available. There is a very real dilemma to be confronted. To what extent, if any, should drugs be used to prevent bone loss where a woman's bone mass is not yet reduced, even if she is anxious to avoid osteoporosis.
We know that at the early menopausal age range the absolute risk of fracture, the key consequence of osteoporosis, is relatively low even where there has been significant bone loss. Thus where there has not yet been much bone loss in this age range the risk of fracture will be very low indeed. Does this mean that no action is required other than general health measures, such as maintaining a good calcium balance, taking weight bearing exercise and avoiding smoking and excessive alcohol?
Twenty five years later when a woman is about 75 years of age the risk of fracture occurring is much higher and therapy to minimise bone loss can be justified for both women who have developed osteoporosis and for many women who have low bone mass. In discussion with menopause specialists across Europe a common theme can be summarised in the question whether it is right to leave women without therapy at younger postmenopausal ages when they are at low absolute fracture risk when it is possible to help them avoid getting to a state of low bone mass which has such adverse consequences when they are older? Many in the rheumatology/osteoporosis community would argue that the early intervention is not justified because fracture risk is low. A different view is often expressed by European menopause specialists.
How are we to face this dilemma? Where does estrogen therapy fit into this scenario?
SM-01-02
DIFFERENT RISK FACTORS IN BREAST CANCER FOR THE EUROPEAN WOMEN
A. Gompel and G. Plu-Bureau
Hôtel-Dieu Hospital, APHP, University Paris V, Paris, France
The breast cancer incidence and mortality vary within Europe. There is a general dramatic trend to increase in diagnosis and a smaller increase in mortality. The increase in incidence may be due to change in risk factors during the last decades but alos to the increase availability of screening. The trend to decrease in mortality in some of the European countries may rely on the time where the screening began and also to differences in aggressivity of the breast cancer cases or different therapeutic attitudes.
One of the main change in the risk factors can be attributable to major modifications in lifestyle and thus modification in the reproductive characteristics of the women. By example late first full term pregnancy, nulliparity and absence or short breast feeding can account for + 6.7% of additional cases within two decades in France (source: IARC). In addition obesity, alcohol intake, sedentarity, diet and possibly pollutants and other carcinogens are also involved in the rates of breast cancer, mortality and vary greatly among the various European countries and regions. We will take some examples of the available epidemiology to point out major differences within Europe and try to understand how health policies could help to decrease the incidence and mortality in breast cancer.
SM-01-03
EPIDEMIOLOGICAL PERPSECTIVES FOR WOMEN'S HEALTH IN EUROPE
Serge Rosenberg (Belgium)
Abstract not available at the time of going to press.
SM-02: Vaginal health and menopause (organised by the Spanish Menopause Society)
SM-02-01
VAGINAL CHANGES DURING MENOPAUSE
J. Ferrer
Hospital Universitario Central de Asturias, Oviedo, Spain
The first vaginal change after menstruation cessation is vulvo-vaginal ischemia. A sharp decrease in artery flow is quickly detected in pelvic and vulvar vessels as uterine and clitorideal arteries. Consequence of ischemia are the progressive development of vulvar atrophy including clitoris, falling of vulvar hair, reduction of vaginal exudation and finally Paccini corpuscle damage. These changes lead to sexual impairment to some extent.
Secondly the estrogen depletion produces vaginal atrohphy with decrease in vaginal height. Lately, an atrophic epithelium with parabasal cells in surface is established. The outcome usually is dyspareunia and the appearance of macroscopic vaginal changes in the long run as rugar of vaginba loss, flattening of fundus and narrowing of introitus. However these atrophic achanges don't affect all menopasual women and don't correlate with estrogen levels. In fact, sexual coital activity maintains vaginal trhopism to some extent despite of hypoestrogenism.
According to vaginal atrophy changes some clinical symptoms come up: dyspareunia, vaginal dryness and vaginal discomfort no related to sexual activity. Some paprers assess the importance of this problem. 43% of 1280 swedish women over 61 complain of vaginal dryness, and 27% of 2157 dutch women (between 51 and 70) look for medical care due to dyspareunia.
Finally these symptons belong to sexual subscales of Quality of life assessment. So, we must emphasize the importance of evaluation and maintenance of an adequate vaginal health in the postmenopausal women.
SM-02-02
VULVODYNIA
R. Sánchez-Borrego1, M. Manubens2 and N. Mendoza3
1Diatros, Clínica de Atención a la Mujer, Barcelona; 2Institut Universitari Dexeus, Barcelona; 3Clínica Margen, Granada
Vulvodynia is burning, stinging, irritation, or rawness in a normal-appearing vulva. It is not caused by a commonly identifiable infection, inflammation, neoplasia, or neurologic disorder.
Previously termed “vulvodynia” and “vestibulitis”, vulvar pain syndromes have been reclassified by the International Society for the Study of Vulvovaginal Disease (ISSVD) under the common diagnosis of “vulvodynia”. Vulvodynia is now classified as generalized or localized depending on the distribution of the pain and further subtyped based on inciting factors, i.e., provoked pain, unprovoked pain, or mixed (both provoked and unprovoked).
Although numerous etiological factors have been proposed, the etiology or etiologies of PVD are unknown. It is likely that different levels of pathophysiology are involved in the development and maintenance of PVD.
There are many possible causes of vulvodynia (e.g., embryologic abnormalities, increased urinary oxalate levels, genetic or immune factors, hormonal factors, inflammation, infection, neuropathic changes). A thorough history should be taken to determine duration of pain, treatment history, allergies, and sexual history.
To identify painful areas, a cotton swab test should be performed. When pain is present, the patient should be asked to categorize it as mild, moderate, or severe. The vagina should be examined, and tests (e.g., wet mount, vaginal pH, fungal culture, Gram stain) should be performed as indicated.
Most experts treat women with generalized vulvodynia with oral tricyclic antidepressants, suggesting that it may be a systemic problem most manifest to the gynecologist as vulvar pain and dyspareunia. Biofeedback and physical therapy have been useful in some programs in which there is a special interest in these symptoms. Women with localized vulvodynia may have a different pathophysiology (or maybe they have just been diagnosed earlier in the course of the disease). They are more often treated with topical soothing or anesthetic creams. Surgical intervention may be helpful in selected patients, but it is usually best to start with the simple things and establish a good relationship with the patient so that you really understand her problem before recommending a surgical approach.
SM-02-03
TREATMENT OF VULVO-VAGINAL DYSFUCTION
Andrés Forteza (Spain)
Abstract not available at the time of going to press.
SM-02-04
SEXUALITY, VAGINAL HEALTH AND QUALITY OF LIFE
José Villero (Spain)
Abstract not available at the time of going to press.
SM-03: Molecular and cellular effects of sex steroids on ageing (organised by the international society of Gynecological Endocrinology)
SM-03-01
SEX STEROIDS AS FUNDAMENTAL REGULATORS OF CELL MOVEMENT AND MIGRATION
Tommaso Simoncini
University of Pisa, Italy
Through a variety of rapidly recruited intracellular mediators steroid receptors enact quick changes in the function of cells in different settings. Emerging evidence indicates that the interaction with the extracellular environment and cell movement are regulated by sex steroids through such rapid mechanisms. Exposure of different cell types to estrogen, progesterone or other steroids results in swift changes in the morphology of the cells, primarily because of changes in the position and organization of actin fibers. These changes are coupled with the formation of a variety of specialized cell membrane structures that are necessary for the cell interaction with high-molecular weight extracellular proteins or nearby cells, and thus to move around or to cross-talk with neighbor cells. Prominent actions on horizontal cell movement or on the ability to invade matrices are have also been observed during exposure to estrogen or other steroids, which indicate that these steroids are powerful regulators of cell movement. Many of these actions are enacted via the rapid activation on nongenomic signaling cascades of sex steroid receptors that lead to the recruitment of small GTPases such as RhoA or Rac, which therefore drive the changes in actin positioning. These actions of sex steroids are observed in a number of cell types, from vascular cells to neurons, to cancer cells, and may therefore have different relevance based on the tissue where they are recruited. The characterization of these rapid actions of estrogens and other steroids will help to understand some of the effects of these hormones in physiological or pathological settings.
SM-03-02
EFFECTS OF ESTROGEN ON INFLAMMATION AND INFLAMMATORY DISEASES
Frederick Naftolin
Department of Obstetrics and Gynecology, New York University, New York, NY 10016, USA
The role of inflammation in chronic diseases and the possibility of preventive strategies based on agents that regulate inflammation have come to the fore as increasing numbers of women live past the reproductive period. Estrogen and progesterone are natural regulators of the inflammatory system. This is most clearly seen during times of change in ovarian function; puberty, pregnancy and the menopause. Although both cellular and humoral inflammation are always in play, their activity and their effects respond to ovarian hormones. During the reproductive period inflammation underlies the development of disease in many systems, though clinical events may not manifest themselves until some time after the menopause. The progress of immune-based diseases generally accelerates after the menopause. Thus inflammation-related diseases that require more than ten years to develop may only become clinically manifest long after menopause. These include cardiovascular disease, connective tissue disorders and nervous system diseases. Enhanced understanding of these matters has driven better and more active strategies to slow the progress of inflammation-based diseases through the use of hormone replacement therapy and anti-inflammatory drugs. Generally, these are useful for prevention rather than treatment or disease reversal. Moreover, drugs that had previously been thought to have narrow, specific, inflammation-neutral actions, such as estrogen, are now being exploited for their anti-inflammatory actions. All of these developments fit into the newly strengthened interest in prevention and this is an active area of research.
SM-03-03
PROGESTOGENS AND BRAIN
A. R. Genazzani and N. Pluchino
Department of Reproductive Medicine and Child Development, Division of Obstetrics and Gynecology, University of Pisa
The increased use of hormonal therapies over the last years has led to improve the knowledge of pharmacological, biochemical and metabolic properties of several progestins and their effects in target tissues, such as the Central Nervous System (CNS). Progesterone and synthetic progestational agents modulate the synthesis and release of neurotransmitters, neuropeptides and neurotrophin factors in response to specific physiological and pathological stimuli. While these actions may relay on differential activation of steroid receptors or recruitment of intracellular pathways, some of the differences found between progesterone and synthetic progestins may depend on the specific conversion to neuroactive steroids, such as the 3‐α, 5‐α reduced metabolite, allopregnanolone. The addition of certain but not all synthetic progestins to an estrogen molecule, determines a further increase in allopregnanolone levels, suggesting that the metabolism into this reduced product is related to the chemical structure of progestin molecule used. In addition, depending on specific progestin molecule used, different interactions are found with the estradiol-induced beta-endorphin synthesis and release, showing that diverse progestins have specific and divergent actions on the opiatergic system. These results highlight the concept that natural and synthetic progesterone receptor agonists may systematically induce different biological actions in CNS supporting the idea that the progestin has to be clinically selected.
SM-03-04
POSTMENOPAUSE AND BONE
O. Ylikorkala (Finland)
Abstract not available at the time of going to press.
SM-04: Salud Posmenopáusica en la Mujer Mexicana (organised by the Asociación Mexicana para el Estudio del Climaterio
SM-04-01
EPIDEMIOLOGÍA Y CALIDAD DE VIDA
Gilberto Tena (Mexico)
Abstract not available at the time of going to press.
SM-04-02
PRESENT STATE OF OSTEOPOROSIS
Julio Morfín-Martín
Asociación Mexicana para el Estudio del Climaterio, México
The bone mineral density in the adult woman depends on maximum Peak Bone mineral Density (PBD) reached by the late 20s and on the loss of bone mass that can appear, specially after the menopause. In the female population of western and Latin American countries there is a fast increase of the bony mass during the second decade of the life, nevertheless, in the Mexican woman the PBD seems to be reached at 22 years in the lumbar column and at 24 years in femur.
The osteoporosis can get to appear in a 33% of the women in the world and the risk of undergoing some fracture is higher particularly in the postmenopause and the elderly. In our country, luckily, the osteoporosis incidence is smaller to those that have been seen in the rest of the world and even smaller to the caucasian white women of the United States.
In Mexican women older than 20 years the osteopenia prevalence is 37.1% in the lumbar spine, and 40.0% in femoral neck, the osteoporosis prevalence is 7.9% and 7.1% respectively. After the menopause (at 47.4 years average) the osteopenia incidence in lumbar spine and hip is duplicated and the osteoporosis increases five times. There are in our country a 27% of women older than 50 years with normal bone density, 57% with osteopenia and 16% with osteoporosis, respectively 1.8, 3.8 and 1.0 million women approximately.
Existing differences between three different population groups according to three regions in Mexico, founding greater prevalence of osteoporosis in the Southeastern of the country related to smaller weight and hight average, that in the center and still more in relation to the north population.
In México, the annual rate of hip fractures is 169 per 100,000 women. A total of 22,233 hip fracture cases were estimated in México in 2006, which represent a total cost of $ 97,058,159 USD for the healthcare system for the acute treatment alone. The prevalece of vertebral fractures in Mexican women 50 years and older is 19.35%, a lower risk compared with non-Hispanic whites living in USA.
SM-04-03
CÁNCER DE MAMA: UN PROBLEMA EMERGENTE
Cuauhtémoc Célis González (Mexico)
Abstract not available at the time of going to press.
SM-04-04
LA SALUD POSMENOPÁUSICA EN LA MUJER MEXICANA DENTRO DEL CONTEXTO DE AMÉRICA LATINA
Alfonso Murillo (Mexico)
Abstract not available at the time of going to press.
SM-05: Climaterio y menopausia en la población femenina en Bolivia (Asociación Boliviana de Climaterio y Menopausia)
SM-05-01
ESTROGEN BIOMOLECULAR EFFECT IN OSTEOPOROSIS
Teresa Espinoza Flores
Instituto de Endocrinología y Reproducción Humana, Cochabamba, Bolivia
There are big studies that gave us new ideas in the prevention of fractures for osteoporosis. The control of the activity and osteoblast formation has taken us to new drugs that inhibit the bony reabsorption. Mainly by the control of the TNF action, inhibition of the TNF receptors, the osteoprotegerina, the mechanisms of action of the bifosfonates, SERMs, the anabolics that reestablish the structure of the bone and the PTH. The activation of the WNT Freez beta Catenina, shows its importance in the formation, bony reabsorption, hardness and shape of the bone, and also the importance of the control of the hormonal mileu. The control key sees that it resides in the Citokines that influence in the bony cell and its communication that are inter-regulated; we see that the normal bony mass depends on the interaction between osteoblastos and osteoclastos. The constituents of the bony womb and the maintenance of the formation process and reabsorption in good balance depends mainly on the PTH – E2 and D3 interaction. It is important to understand the concepts of the pathogenesis, the number of cells, the osteoclast overproduction and the osteoblast sub-production. Also play a rol the flaw in the precursors or the flaw in the cellular differentiation that are the integral arguments of the cellular biology that determines how the young osteoclasts are recruited and induced to differ in mature osteoclasts. As well as the osteoblasts, instructs to restore the bony mass exactly the quantity that was dug to stuff the same thing. Estrogen is established to have direct effects on bone cells and plays a fundamental rule in skeletal growth and bone homeostasis men and women. Estrogen deficiency causes bone loss and the mechanisms involved have proven to be complex and multifaceted. One major challenge is the integration of a multitude of redundant pathways and cytokines, each apparently capable of playing a relevant role, into a comprehensive model of postmenopausal osteoporosis. Estrogen deficiency is likely to increase T cell reactivity to a pool of self foreign antigens, physiologically present in healthy animals and humans. One cytokine responsible for augmented osteoclastogenesis during estrogen deficiency is TNF. The dominant acute effect of estrogens the blockade of new osteoclast formation. They came from the monocyte precursor that circulate within the hematopoyetic cell pool. Estrogen deficiency leads to dramatic elevations in the number of Basic Multicellular Units through increased activation frequency, which is the number of new remodeling units activated in each unit of time.
SM-05-02
THE METABOLIC SYNDROME IN A SPECIFIC CLIMATERIC BOLIVIAN POPULATION
Javier Saavedra Belmonte
Instituto de Endocrinología y Reproducción Humana; Cochabamba, Bolivia
Atheroesclerotic cardiovascular disease is the number one cause of deaths in adults in western societies. Increase in obesity(OB) as well as in type 2 Diabetes Mellitus(DM2) play a central role in the occurrence of cardiovascular risk. The Metabolic Syndrome (MtbSd) represents a constellation of risk factors as OB, dyslipemia, hyperglycemia and hypertension and predispone to cardiovascular disease (CVD) and DM2. The process of atherosclerosis begins in early childhood and is strongly associated to high Body Mass Index (BMI), Blood Pressure and Lipid Profile. Obesity is believed to be a primary pathogenetic mechanism of both CVD and DM2. Insulin Resistance (I-R) is a condition with a diminished action of Insulin and predisposes hyperinsulinism that carries out a low uptake of glucose by different organs like the muscle. I-R is caused by a genetic predisposition, OB, sedentarism, age, alcohol, smoking and diet. Can cause hyperuricemia, glucose intolerance, inflammatory disease, endothelial impairment, hemodynamic complications, dislipidemia, haemostatic imbalance and reproductive impairment. The Cardiometabolic Risk (CMtb-Rk) is defined as a cluster of modifiable risk factors and markers that identify individuals at increased risk for CVD and DM2. It includes high blood pressure, abdominal adiposity, low HDL-c, elevated triglycerides, elevated blood glucose (ATPIII) plus smoking, elevated LDL-c, insulin resistance and inflammatory markers.
In Bolivia (1998) the Obesity prevalence (IMC > 30) 22.6% (20.9–24.3) men = 15.2% (13–17.5); women = 29.8% (27.4–32.2). Overweight prevalence (IMC = 25–29.9) 59.9%; men = 55.8% and women = 63.9%.
In the REDLINC Study “Prevalence of the Metabolic Syndrome in postmenopausal Latin American women”, the prevalence of Metabolic Syndrome (ATPIII) was 35.1% In Cochabamba Bolivia was 30.4% with abdominal obesity = 23%; Hypertension = 36.1%; Hyperglicemia = 6.9%; Low HDL-C = 65%; High Triglycerides = 60.2%.
Abdominal waist and Blood Pressure best predictors MtbSd. OR:20.57(IC95% = 17.16–24.67); sensibility = 66.7%; Especificity = 91.1%; Predictive Value = 80.3%.
The Endocannabinoid System (ECS) is an endogenous signaling system that plays a role in the regulation of energy homeostasis and lipid and glucose metabolism (feeding behavior)- all of which can influence CMtb-Rk. ECS over activation is associated with obesity and dyslipidemia. The ECS appears to be a promising novel mechanism to modulate important aspects of cardiovascular and metabolic functions. Consists of two types of cellular receptors, CB1 and CB2, and several endogenous ligands, where anandamide and 2-arachidonylglycerol (2-AG) have been the most studied. Endocannabinoids act locally as retrograde messengers in the nervous system. From postsynaptic cells to presynaptic receptors (paracrine action) also in adipose cells, muscle, liver and gastrointestinal tract.
SM-05-03
SEXUALIDAD EN LA MENOPAUSIA
Carmelo Rodríguez (Bolivia)
Abstract not available at the time of going to press.
SM-05-04
THE CERVANTES SCALE®: MEASURING A WOMAN'S QUALITY OF LIFE DURING THE CLIMACTERIC PHASE IN SANTA CRUZ, BOLIVIA
M. Pommier1, D. Mostajo2, J. Villarroel3, S. Carvajal4, J. Mendoza5, C. Rodriguez6 and P. Davalos7
1Clinica Urbarí Santa Cruz-Bolivia; 2Centro Medico Udime Santa Cruz-Bolivia; 3Clinica Urbarí Santa Cruz-Bolivia; 4Caja Nacional Seguro Social Santa Cruz- Bolivia; 5Corporación Social de Seguro Militar Santa Cruz- Bolivia; 6Clinica Sirani Santa Cruz- Bolivia; 7Univ. Gabriel René Moreno Santa Cruz-Bolivia
Objective: To measure the quality of life of women during the climacteric phase by applying the questionnaire of the Cervantes Scale® to a sample of 600 women between 45 and 64 years old in Santa Cruz, Bolivia.
Methodology: Using the single-stage conglomerate sampling method, 600 women between 45 to 64 years old, were selected from several Santa Cruz neighborhoods presenting similar characteristics. The women were mentally and physically capable to answer the questionnaire and accepted to take part in the investigation. They were interviewed over a 4-month period. The internal consistency was validated through Cronbach's α coefficient. For test-retest marking stability, Spearman's non-parametric correlation coefficient was calculated. This objective was achieved by using the statistical processor SPSS 11.5.
Results: Socio-demographic characteristics of the participants:
Age: 45–49 = 31%; 60–64 = 22.5%; Instruction level: high school or more 45.7%; illiterate 6.0% Number of children: none: 6.7%; 3–4 children: 44.5% 5; more than 4 children: 25.4%; Occupation: works outside the house 73.8%; does not work outside the house 26.2%; The aspects measured during the interviews were 1) quality of life, and 2) personality. The quality of life scale consists of four domains: menopause and health, psyche, sexuality, and couple's relationship; and 31 questions were used. The Cronbach α index oscillated between 0.76 and 0.88, with a global Cronbach α index of 0.8766. The personality scale consists of three domains: introversion, emotional instability, and honesty, and 20 questions were used. The Cronbach α index was between 0.80 and 0.83, with a global Cronbach α index of 0.9282.
The Cronbach α index over the total of 51 questions was 0.9392.
Conclusions: The Cervantes Scale allows measuring and acknowledging the deterioration of the quality of life in climacteric women as a function of their age.
SM-06: Menopausia (Fundacion Venezolana de Menopausia y Osteoporosis)
SM-06-01
DEPRESIÓN, ESTRÓGENOS Y MENOPAUSIA
Rafal Molina (Venezuela)
Abstract not available at the time of going to press.
SM-06-02
PENDIENTE DE DEFINIR
Juan Yabur (Venezuela)
Abstract not available at the time of going to press.
SM-06-03
EL ENFOQUE HOLISTICO DE LA MUJER POSMENOPAUSICA A LA LUZ DEL WHI
Manuel Neves-e-Castro
CFH-Clinica de Feminologia Holistica, Lisbon-Portugal (e-mail: [email protected])
A woman is a human being that integrates a body with a mind. It is a psychosomatic unit surrounded by an inner circle and an outer circle.
The inner circle is her home, her family. The outer circle is everything that has to do with where she works, with society, etc.
Holism is the vision of that woman as a complex individual living by herself under the influence of her conditioning surroundings. Therefore the postmenopausal woman must be taken care of as a whole unit and not only as a body.
WHI has cast many doubts among women and physicians. Although this study has internal validity it is devoid of external validity, thus making it impossible to apply its conclusions to the general population of postmenopausal women.
Nevertheless the WHI has been recently reanalyzed. Although hormonal treatments should not be primarily used for preventive purposes, the fact is that when they are used e.g. or the relief of symptoms they may offer protection for cardiovascular diseases in women less than 60 years of age. The risk of breast cancer associated with HTs is extremely small.
None of the usual HTs is better than a proper nutrition, a normal body weight, frequent exercise, moderate alcohol consumption, no smoking and a good psychological support by the attending physician.
SM-07: Composición Corporal en el Climaterio (Sociedad Peruana de Climaterio)
SM-07-01
BODY COMPOSITION IN THE PERUVIAN WOMAN IN TIME
A. Del Castillo1 and P. Crespo2
1Clínica San Pablo, Lima, Perú; 2Instituto de Endocrinología y Metabolismom, Lima, Perú
The body composition of a human being varies according to age and sex. In menopause occur many hormonal and metabolic changes that will influence the anabolic and catabolic aspect of the organism; these hormonal changes can be the beginning of some pathologies that later can origin certain diseases (Hypertension, diabetes mellitus, dyslipidemia, etc.)
In addition to the major changes in skeletal mass, there is redistribution of body fat and lean mass, and by example for the age group from 11 to 17 years with an average tissular weight of 48,646 g ± 11137 (mean ± SD) for a BMI of 21.20, the percentage of total fat is up to 36.27% of which 6800 g are located in the trunk and the content of lean body mass is 30,579 g.
Among 18- 25 years there is an increase of tissular weight to 56,983 ± 9,218 (mean ± SD) with a BMI of 23.02, with a total fat percentage of 38.5%, 8,854 g of fat corresponding to the trunk, and 34.337 g of lean body mass.
Between 26–29 years shows the peak tissular weight of 64,435 ± 14,508 (mean ± SD) with a BMI of 25.18, with a total fat percentage of 39.9% corresponding to the trunk 10,351 g of fat and 37.699 g of lean body mass.
Among those from 30 to 39 years there is a decrease in the tissular weight to 61,461 ± 12,619 (mean ± SD) with a BMI of 24.9 with a total fat percentage of 39.75% corresponding to the trunk 10,154 g of fat and 35.920 grams of lean mass.
Among 40 to 49 years there is an increase of tissular weight to 62,063 ± 11,323 (mean ± SD) with a BMI of 25.12, with a total fat percentage of 38.9% corresponding to the trunk 10297 g of fat and 36,599 g of lean body mass.
Among 50 to 59 years there is a new increase in the tissular weight to 64,876 ± 10,528 (mean ± SD) with a BMI of 26.13, with a total fat percentage of 40.9% corresponding to the trunk 11,296 g of fat and 36,464 g of lean body mass.
The population over 60 years continue increasing the tissular weight to 67,807 ± 15,336 (mean ± SD) with a BMI of 27.3, with a percentage of total fat in 46,145% corresponding to the trunk 12,224 g of fat and 36,450 g of lean body mass.
It is noted that the older must have the greatest increase in percentage of total fat and the greater location is in the trunk, keeping the lean mass from the age of 40.
Obesity is a major cause of morbidity and mortality and exerts a profound negative impact on the quality of life in the woman becoming a public health problem that requires a precautionary approach.
SM-07-02
ASSESSMENT OF THE INSULIN RESISTANCE IN POSTMENOPAUSAL PERUVIAN WOMEN
I. Crespo, A. Stucchi and M. T. Crespo
Instituto de Endocrinología y Metabolismo, Lima, Perú
The hormonal regulation in body weight changes is a complex process and often not clears at all. The center that controls appetite is influenced by a number of substances that have to regulate energy balance. We have seen significant correlation between the increase in fat mass at the trunk associated with age and declining estrogen.
Between 30–50% of women with Polycystic Ovarian Syndrome (PCOS) are obese and there is a close relation in the increase in fat mass and its location at the trunk; while obesity contributes to the emergence of Insulin resistance (IR), in the PCOS the magnitude of the IR exceeds that it would be possible to predict based on the total body mass and even the lean body mass.
In women whose body mass index (BMI) is under 25 have a basal insulin of 10.47 UI in and those whose BMI is over 25 have a basal Insulin of 17 IU.
Menopausal women are more likely to develop diabetes mellitus type II, especially those with more of 10,800 g of fat in the trunk and with a history of PCOS, this group presents pre-diabetes and diabetes, and many of them are labeled as metabolic syndrome. On the other hand these same women are more likely to develop hypertension associated with obesity and insulin resistance.
SM-07-03
BONE MINERAL CONTENT IN DIFFERENT AGES OF PERUVIAN WOMEN
E. Calle1 and I. Crespo2
1Clínica San Pablo, Lima, Perú; 2Instituto de Endocrinología y Metabolismo, Lima, Perú
The Peruvian population exceeds 28 million with a growth rate of 1.5% per annum, of which 49.7% are women. The urban population is up to 72.3%.
The body composition and bone mineral content (BMC) of the human being will vary with respect to age and sex. The bone and muscle mass saved some relationship with age and are of particular importance in the climacteric.
In menopausal women there is a significant negative correlation between age, bone mineral density, bone mineral content and calcium.
The loss of bone tissue is estimated approximately between 0.33 and 0.7% per year from age 30, and increased significantly since the onset of menopause and during the next 10 years.
The BMC and calcium content is variable and depending upon the degree of nutrition from childhood and is directly related to the socio-economic and cultural development. The study population corresponds to a mid-level and high.
Between 11 and 17 years, the average BMC is 2,121 g and calcium content is 813 g.
In the next age group from 18 to 25 years there is an increase in the BMC to 2480 (943 g calcium). The studied group from 26 to 29 years reaches the high BMC, the mean at this age is 2,634 g (1,001 gm. Calcium) considering this age when it reaches the peak bone mass. Between 30 to 39 years begins the fall of BMC to 2599 g (996 g Calcium) and it's similarly maintained between 40 and 49 years. Among the women between 50 to 59 years there is a greater fall (drop) of the BMC until 2415 g (917grs calcium) and then the loss in BMC and Calcium content is kept in similar values in women older than 60 years.
Our data are consistent with those reported in the world literature and allows us to see the important role of estrogen in bone mineral metabolism and maintenance of the bone mass.
SM-07-04
CORPORAL COMPOSITION IN CLIMACTERIC (PERU): CONCLUSIONS
J. Matzumura
Norbert Wiener University. Lima, Peru; Policlínico Peruano Japones (APJ), Lima, Peru
The Peruvian population exceeds 28 million with a growth rate of 1.5% per annum, of which 49.7% are women. The urban population is up to 72.3%.
The body composition and bone mineral content (BMC) of the human being will vary with respect to age and sex. The bone and muscle mass saved some relationship with age and are of particular importance in the climacteric.
The BMC and calcium content is variable and depending upon the degree of nutrition from childhood and is directly related to the socio-economic and cultural development.
In menopausal women there is a significant negative correlation between age, bone mineral density, bone mineral content and calcium.
We have seen significant correlation between the increase in fat mass at the trunk associated with age and declining estrogen.
Among the women between 50 to 59 years there is a greater fall (drop) of the BMC until 2415 (917 g calcium) and then the loss in BMC and Calcium content is kept in similar values in women older than 60 years.
Our data are consistent with those reported in the world literature and allows us to see the important role of estrogen in bone mineral metabolism and maintenance of the bone mass.
In addition:
Between 30–50% of women with Polycystic Ovarian Syndrome (PCOS) are obese and there is a close relation in the increase in fat mass and its location at the trunk; while obesity contributes to the emergence of Insulin resistance (IR), in the PCOS the magnitude of the IR exceeds that it would be possible to predict based on the total body mass and even the lean body mass.
In menopause occur many hormonal and metabolic changes that will influence the anabolic and catabolic aspect of the organism; these hormonal changes can be the beginning of some pathologies that later can origin certain diseases (Hypertension, diabetes mellitus, dyslipidemia, etc.)
Obesity is a major cause of morbidity and mortality and exerts a profound negative impact on the quality of life in the woman becoming a public health problem that requires a precautionary approach.
SM-08: Menopause: Filipino women's and physicians perspectives (organised by the Philippine Society of Climacteric Medicine)
SY-08-01
MENOPAUSE: FILIPINO WOMEN'S AND PHYSICIANS PERSPECTIVES
Lilia Pagtakhan Luna (Philippines)
Abstract not available at the time of going to press.
SY-08-02
THE PREVALENCE OF OSTEOPOROSIS AMONG FILIPINOS BASED ON CALCANEAL QUANTITATIVE ULTRASONOGRAPHY
B. De Guia and K. Lipana
University of the Philippines, Manila
Objectives: To determine the prevalence of osteoporosis and osteopenia among Filipinos based on T-scores using calcaneal quantitative ultrasonography and to correlate the prevalence with age, sex and geographic location.
Design and Method: This is a cross-sectional descriptive study of baseline bone mineral density of Filipino males and females aged 18 years old and above who consulted at the Osteoporosis Advocacy and Screening Initiative Services Testing Center which includes schools, community centers, offices and hospitals. Age at enrollment, race, sex, and geographic location (Luzon, Visayas, or Mindanao) were recorded. Bone mineral density was measured at the calcaneus by quantitative ultrasonography using the Achilles Insight QUS System and T-scores were computed based on WHO criteria.
Results: A total of 20,726 subjects were included with 72.8% of them being females. 74% of the total population had normal T-score, 22% had osteopenia, and 3% had osteoporosis. Most of the osteopenics (46%) belonged to the 46 and above age group, while most of the osteoporotics (46%) belonged to the above 65 years age group. The rest of the osteoporotics (38%) were seen at the age group 46 to 65 years.
Among the male subset, 76% (4,267) had normal T-score, 22% (1,232) were osteopenic and 2% (126) were osteoporotic. Among the female subset, 74% (11,103) had normal T-score, 23% (3,406) were osteopenic, and 4% (718) were osteoporotic.
The prevalence of osteoporosis in the different regions were the same.
Conclusions: The prevalence of osteoporosis among Filipinos was 3%, while that of osteopenia was 22%. Osteoporosis was more prevalent in women and seen most in the 46 years and above age group. Geographic location did not influence the prevalence of the disease in the country.
SY-08-03
EFFECTS OF ESTROGEN VAGINAL CREAM ON THE ENDOMETRIAL THICKNESS OF FILIPINO MENOPAUSAL WOMEN
B. De Guia, C. Cunanan, F. Gonzaga and G. Pastorfide
University of the Philippines, Manila
Objectives: To determine by transvaginal ultrasound changes in endometrial thickness measurement of natural menopausal Filipino women with atrophic vaginitis after 3 months of administration of low-dose estrogen vaginal cream.
Design and Method: This is a before and after study of 36 patients who were recruited at the Menopause Clinic for 3 months. Inclusion criteria were: 1) natural menopausal Filipino women with atrophic vaginitis (dryness, discharge, dyspareunia of burning sensation; 2) such women had a baseline endometrial thickness of ≤4 mm by transvaginal ultrasound; 3) informed consent. Exclusion criteria include any contraindication estrogen use.
All women included in the study underwent baseline transvaginal ultrasound and their endometrial thickness, uterine sizes, and sizes of myoma, if any, were measured. They were given 1 g daily of 0.625 mg estrogen vaginal cream and the same ultrasound parameters measured after. Bleeding patterns during and after treatment were noted. Statistical analysis was done using paired T-test.
Results: There is a significant change in endometrial thickness after 3 months of estrogen vaginal cream (p < .05). The mean endometrial thickness before and after treatment was 2.4 ± 1.2 mm and 4.3 ± 0.6 mm, respectively. The mean increase in endometrial thickness after treatment is 1.7 mm (range 0.6–6.5 mm). There is no change in the sizes of the 4 myomas noted. Bleeding occurred in 2 patients.
Conclusions: There is a significant increase in endometrial thickness of Filipino menopausal women after 3 months of administration of low-dose (0.625 mg) estrogen vaginal cream and close ultrasound monitoring of their endometrium is advised.
SM-09: Jatrogenic menopause (organised by the Polish Gynaecological Society)
SM-09-01
OVARIAN FUNCTION AFTER UTERINE ARTERY EMBOLIZATION FOR FIBROIDS
J. Kotarski, W. Bednarek, I. Wertel and M. Kotarska
Medical University Lublin, Poland
The etiology of uterine fibroids is still unclear, so the preventive and causal treatment of tumors is impossible. Surgery is still a dominant treatment of symptomatic fibroids, but hysterectomy is not acceptable by many patients. In last decade several alternative techniques were adopted for treatment of fibroids. Uterine artery embolization for myomas was introduced into clinics by J.Ravina. The effectiveness of the method in symptomatic women was well documented, but several major and minor complications were observed. One of the side effects observed after treatment was disturbance of ovarian function. This made the method not acceptable for women who planned childbirth.
According to the references following risk factors of ovarian damage can be identified: (1) size of embolization particles, (2) age of patients, (3) type of arterial utero-ovarian connections.
Clinical symptoms of ovarian damage: amenorrhea, oligomenorrhoea and laboratory findings: FSH elevation, decrease of ovarian reserve, decreased perfusion of the ovary (US) and histological identification of polivinyl alcohol particles in gonads.
The ovarian insufficiency after UAE may be permanent or transient. The precentage of amenorrheic patients increases with age. According to Chrisman et al. ovarian failure occured in 43% of women older than 45 years and in none of the younger then 45years.
Not all data confirms these observations. Hovsepian et al did not found difference in impact on ovarian function after UAE, hysterectomy or myomectomy at 6 months. The randomized study done by Hehenkamp at al. compared ovarian reserve, based on the FSH and antiMullerian hormone concentration, after abdominal hysterectomy and UAE. The study documented that both techniques affect ovarian reserve. 24 months after treatment 14 of 80 in UAE group and 17 of 73 in hysterectomy group had FSH concentration >40 IU/l. Concentration of anti-Mullerian hormone decreased in both groups and did not differ between groups.
Conclusion: When choosing UAE as method of treatment of fibroids for patients, risk factors of disturbance of ovarian function should be analyzed.
SM-09-02
THE PRESERVATION OF OVARIES DURING HYSTERECTOMY – SENSE OR NONSENSE
Tomasz Rechberger
II Department of Gynecology, University School of Medicine, Lublin, Poland
Prophylactic oophorectomy is presently, due to lack of highly effective methods of early detection, the only effective method of ovarian cancer prevention. Having accepted the general concept of prophylactic oophorectomy in high-risk women (hereditary predisposition related to mutation in BRCA1, BRCA2 and HNPCC genes) there is still a lot of controversies whether to routinely perform prophylactic oophorectomy during hysterectomy for benign uterine diseases.
According to epidemiological data the lifetime risk of developing ovarian carcinoma is 1.4%. Hysterectomy itself also appears to reduce the risk of ovarian cancer by 40% when compared to its prevalence in general population, however as many as 4 to18% of women with advanced ovarian cancer undergone previously hysterectomy for benign conditions. Clinical data from 31,032 hysterectomy cases from nine series revealed that 400 oophorectomies would be performed during hysterectomy in women over the age of 40 to prevent just one ovarian cancer. The dilemma for the patients and clinician is whether the estimated number of cancer cases prevented (based on US statistics approximately 1000 new cases annually) is worth the number of oophorectomies performed (300,000 procedures). Additionally by performing routinely bilateral salpingo-oophorectomy at the time of hysterectomy decrease the necessity of evaluation abnormal pelvic imaging findings from 50.7% in women with preserved ovaries to only 5.5% among those who underwent oophorectomy during primary surgery. However the ovary is a complex metabolic organ and follicles produce both androgens and estrogens, whereas the stromal tissue synthesizes androgens only. The levels of steroid hormones estradiol, testosterone, and progesterone are different in natural and surgical menopause. In premenopausal women undergoing oophorectomy the mean reduction in serum testosterone is 50% and the mean reduction in serum estradiol concentration is 80% resulting with more frequent and severer symptoms including hot flashes, sexual dysfunction, depression, migraine headaches, vaginal dryness and cardiac symptoms. Recently by means of age specific data for absolute and relative risk, both with and without oophorectomy for ovarian cancer, coronary heart disease, hip fracture, breast cancer and stroke the optimal strategy for maximizing survival rate for women without hereditary predisposition was calculated. It was clearly shown that women who underwent oophorectomy before age of 55 have 8.58% excess mortality by age 80 and those with oophorectomy before age 59 have 3.92% excess mortality. Ovarian preservation at the time of hysterectomy in low risk women outweighs the risk of ovarian cancer development in terms of long term survival rate.
SM-09-03
OVARIAN CYST SURGERY AS A RISK OF GONAD DAMAGE
Wlodzimierz E. Baranowski
Dept. of Gynaecology and Oncological Gynaecology, Military Institute of Health Services, Warsaw, Poland
Population risk of premature ovarian failure (POF) is 5%. The known causes of POF include genetic factors (e.g., chromosome X deletions), autoimmune disorders (autoimmune polyglandular failure syndromes), environmental factors (pollutants, excess of galactose intake) and iatrogenic factors (surgery, chemotherapy, radiation). Postsurgical ovarian failure after classical or laparoscopic surgery due to ovarian cyst (mainly endometriomas) or laparoscopic ovarian drilling (LOD) in PCOS patients is a rare but possible complication. According to data published in literature, iatrogenic (surgical) premature ovarian failure occurs in 2.4% of patients undergoing bilateral endometriomas excision. Scarce data exist on LOD and POF (El-Sheikhah et al. 2004, Cochrane Database 2007).
Approximately 50% of women presenting endometriosis is affected by endometrioma(s), so the scale of the problem is quite large. Ovarian reserve in presence of ovarian cyst may be affected by different ways: damage of ovarian tissue simply by endometrioma, inflammation reaction (white blood cells infiltration) due to endometrioma, surgical damage (excessive excision and coagulation of ovarian tissue, blood supply reduction). According to the guidelines published in 2005 by European Society for Human Reproduction and Endocrinology, laparoscopic cyst excision larger than 4 cm in diameter improves future fertility when compared to drainage and coagulation (laser vaporization) only. In latter case, the risk of cyst recurrence is significantly elevated, even in short-term period. However, Brosens et al. (1996) recommended opening the endometriotic pseudocyst and selective coagulation of endometriotic implants on the exposed inverted cortex. From technical point of view, precise excision of an endometrioma cyst wall without healthy ovarian tissue damage is usually difficult. Additional attention should be paid to avoidance excessive coagulation of ovarian margins to obtain postoperative hemostasis, particularly in area of utero-ovarian ligament (Canis et al. 2001). Some surgeons prefer suturing of ovarian tissue instead of electro-coagulation. Only in few reports published to date (Loh et al. 1999, Somigliana et al. 2003) it was established that responsiveness to hyperstimulation in IVF programme is consistently reduced in ovary undergoing surgery when compared to contralateral intact gonad. This is the only prove that ovarian reserve is affected by surgery. According to literature data repetitive surgeries for ovarian diseases can also lead to POF.
In conclusion it should be said, that in symptomatic patients the benefits of radical (i.e., complete excision) surgical treatment of ovarian cyst clearly overcome the risk of ovarian failure. However, taking into account that scientific data are very limited, this problem needs further, well constructed studies.
SM-09-04
CHEMOTHERAPY AND OVARIAN FUNCTION
Bidziński Mariusz (Poland)
Abstract not available at the time of going to press.
SM-10: The NAMS 2008 hormone therapy position statement: we seem to be reaching international consensus (organised by the North American Menopause Society)
SM-10-01
THE DEVELOPMENT PROCESS FOR POSITION STATEMENTS
Wulf H. Utian
Executive Director, NAMS; Consultant in Women's Health, the Cleveland Clinic; Professor Emeritus, Reproductive Biology and Obstetrics and Gynecology, Case Western Reserve University Cleveland, Ohio, USA
The concept of developing clinical position statements is recent, initiated in the 1970s by the U.S. National Institutes of Health with the development of consensus reports. The process changed radically through the 1990s with the “evidence-based medicine” movement that mandated a comprehensive and systematic review of the medical and scientific literature and requiring recommendations to be directly linked to supporting evidence. NAMS commenced development of consensus opinions in 1998, emphasizing that they do not represent “practice standards” that could be codified as such by regulatory bodies and insurance agencies. Rather these are prevailing opinion pieces, attempting an honest detailed effort at incorporating current best evidence into practical clinical recommendations.
Presumably, using identical data bases and published evidence, developing position statements should be straightforward. So why then do different organizations, after scrutinizing the same evidence, come out with different interpretations and recommendations?
Obviously, we will always lack a complete database. It is impossible to accomplish evidence-based clinical research in any area of medical science that incorporates all populations, sub-populations, conflicting and confounding factors, co-morbidities and risk factors, and combinations and permutations of medications. The targets such as risk factors, demographics, drug development and usage, and so on, keep moving and a complete contemporary database will therefore always be impossible to achieve. Thus the guideline-development concept would be flawed were it to rely entirely on the base of evidence existing at any one point in time. The process has to allow for clinical and scientific judgment to be taken into account by both the developer and those who ultimately put the recommendations into clinical practice.
Data can be interpreted in different ways, and there are certainly variances between different medical specialties. A strong but neutral chairman and a balanced group should prevent one individual/group biasing the outcome. The extrapolation of evidence based on one select study population to another select population or to the general population must also be considered, and blinded ballots on key points should be utilized. Transparent declaration of conflicts of interest is mandatory and could contribute to unmasking any hidden agendas.
All this was taken into consideration in the development of the latest 2008 NAMS Position Statement on postmenopausal estrogen and progestogen usage. Translating these positions into clinical practice must still necessitate taking into account the complete health profile of the individual woman as well as her personal preferences and beliefs.
SM-10-02
THE NORTH AMERICAN MENOPAUSE SOCIETY (NAMS) POSITION STATEMENT ON HORMONE THERAPY: UPDATE 2008
V. W. Henderson
Stanford University, Stanford, California, United States
In March 2007, the North American Menopause Society (NAMS) published recommendations for use of menopausal hormone therapy (HT) during the menopausal transition and postmenopause (Menopause 2007;14:168–182). New publications have since appeared pertaining to the risks and benefits of HT and to the clinical management of middle-age and older women. The 2007 NAMS recommendations were updated in 2008 by an advisory panel of experts in aspects of women's health, providing revised evidence-based guidelines for HT use. Consensus recommendations by the panel were reviewed and approved by the NAMS Board of Trustees as an official NAMS position statement (Menopause 2008, in press). The 2008 Update contains new sections on sexual function, urinary health, body mass, endometrial cancer, mood, mortality, and timing of HT initiation. Other sections have been revised; these include stroke, coronary heart disease, venous thromboembolism, diabetes mellitus, osteoporosis, depression, cognitive aging, quality of life, breast cancer, and premature menopause. Issues of bioidentical hormones, hormone class effects, routes of administration, and symptom recurrence after HT discontinuation are also considered in the 2008 Update. For many health outcomes, a general conclusion is that the risk-benefit ratio for HT is often more favorable close to menopause and declines with advancing age. Unique features of the 2008 HT Position Statement are an approach to explaining HT risk, areas of non-consensus among advisory panel members, and topics for future HT research.
SM-10-03
PUTTING POSITIONS INTO PRACTICE
R. A. Lobo
Columbia University, New York, New York, USA
Over several years, the Position Statements of the North American Menopause Society (NAMS), which have been derived from discussions among the panelists, have come about with far less debate and with very few areas of disagreement. This is probably because more recent data from the WHI have been much more in line with the conventional thinking of risks and benefits of hormonal therapy (HT) derived from older observational data. Indeed for the 50–59 year old age group in WHI, the data are entirely consistent with older data, and the observational trial of WHI. The major focus of the latest NAMS Position Statement, in addition to reviewing the most recent data, has been to attempt to put the risks and benefits into a clinical perspective.
In broad strokes it is clear that the risk-benefit equation is quite different for the younger symptomatic woman at the onset of menopause, compared to the asymptomatic woman in her 70's. In the younger woman experiencing menopause-related symptoms, it is clear that HT is efficacious and safe, and the benefits outweigh the risks. This includes the consideration of therapy for the prevention of osteoporosis. Most data in this age group point to a potential protection against coronary heart disease as well as osteoporotic fractures, and a reduction in all cause mortality.
Risks for most women into their 60's may be considered as being rare using criteria from the Council for International Organizations of Medical Sciences (CIOMS): ≤10/10,000 woman/years. It is imperative that the provider explain the current evidence of attributable risk in comparison to everyday risks. These data are based on “standard” dose therapy for 5–7 years of use. It is anticipated that lower doses and different regimens may even be safer, without necessarily sacrificing any loss of efficacy. More flexibility is warranted in deciding on the dose and type of therapy for any given woman. In the NAMS Position Statement, it is stated that there is no evidence for a benefit or risk with any particular route of administration or with any particular progestogen, although it should be acknowledged that minimizing the exposure to progestogens in general, may be prudent. It is also quite clear that the use of “bioidentical hormones” as defined and manufactured by compounding pharmacies cannot be recommended.
SM-11: Sexuality and menopause (organised by the Spanish Menopause Society)
SM-11-01
SEXUALITY DURING THE MENOPAUSE. FEMALE SEXUAL RESPONSE
Rosario Castaño (Spain)
Abstract not available at the time of going to press.
SM-11-02
SEXUAL DYSFUNCTION: CLASSIFICATION AND DIAGNOSIS
Carmen Menéndez
Palacios Institute of Woman's Health; http://www.institutopalacios.com; Email: [email protected]
Summary: The concept and classification of sexual dysfunctions and their diagnosis which stem from the studies carried out by Masters and Johnson in 1966, consider that the human sexual response consists of four phases: Arousal, platform, orgasm and resolution for both men and women. Since then research in the field of health and sex has not ceased. Currently the model “Desire-arousal-orgasm”, which has served as a reference for the study of dysfunctions that can appear at any stage is being imposed. Research into erectile dysfunction has opened the doors for the study of hormonal physiology and neurocirculation of the female genital organs and their relation with sexuality.
Definition of Female Sexual Dysfunction: There are two widely recognized definitions of female sexual dysfunction:
DSM-IV (North America): The alterations of sexual desire and the psychophysiological changes which characterize the sexual response cycle and which cause marked distress and interpersonal difficulties.
ICD‐10 (the rest of he world): The diverse modes in which a person is incapable of participating in a sexual relation in the way they would like.
Taking as a reference the concept of “The Circular Model of the Female Sexual Response”, Desire-Arousal-Satisfaction proposed by Basson in 2001, “Female Sexual Disorder” is defined as multicausal, multidimensional problem which combines biological, psychological and interpersonal elements: Related to age, progressive and highly prevalent, it could very much affect quality of life and couple relationships, cause personal distress, that is to say, it fulfills the requisites which deserve clinical attention.
Classification: The current predominating classification highlights is the following: sexual desire disorder (hypoactive sexual desire disorder, sexual aversion disorder), sexual arousal disorder, orgasmic disorder, sexual pain disorder (dispareunia, vaginism).
Diagnosis: The clinical diagnosis should take into account: duration (lifelong or acquired), beginning (rapid or gradual), context (generalized or situational), detailed medical and sexual history, physical examination, laboratory tests, specialized diagnostic tests, validation study instruments: Sexual Activity Log (SAL), Profile of Female Sexual Function (PFSF), Personal Distress Scale (PDS).
Conclusion: It is more and more important to address sexual problems in clinical practice. Self confidence when treating these sexual problems increases with practice, you can learn to determine and assess. By addressing the sexual and medical comorbilities, the quality of care can be improved in general.
The importance of female sexuality has meant that the number of women who raise the question of their problems and difficulties with their gynaecologist is increasing.
SM-11-03
HYPOACTIVE SEXUAL DESIRE DISORDERS (HSDD). TREATMENT
F. Quereda
Miguel Hernández University; Hospital of San Juan; PAA Institute
Introduction: Determinants of sexual libido in women are not completely understood, thus, few treatments have shown efficacy and safety in clinical trials for HSDD. Recently, interest and knowledge about identification and treatment of HSDD have increased and approaches that have proven some efficacy are psychotherapy, hormonal therapy and use of psychopharmacological agents. Yohimbine, apomorphine SL or melatonin receptor agonists (PT–141) have been tried with inconclusive results, but the major evidence exists about the use of hormonal therapy.
Sexual Hormones and HSDD: Androgens have been related for many years to sexual and general well-being. Their levels decline with age and with menopause, but especially with surgical menopause, and more severely with premature menopause. HSDD is prevalent among women at all reproductive stages, but surgically postmenopausal women are at greater risk of less active sex life, decreased sexual satisfaction and sexuality-related distress (which defines HSDD). Bilateral oophorectomy drastically reduces circulating testosterone (more than natural menopause) and often negatively affects sexual drive, sexual arousal and ability to experience orgasm. These findings support the role of hormonal deprivation on HSDD and logically a possible role for treatment, and the most scientific approaches have been done testing hormonal treatments (formulations of estrogens, androgens or nor-derived progestins).
Hormonal treatment of HSDD: Many studies have demonstrated the efficacy of estrogens for dyspareunia and vaginal dryness, improving sexual performance and sexual satisfaction. All these effects can ameliorate HSDD but frequently remains or even worsens (probably because of the estrogen-related increase of SHBG and subsequent decrease of free testosterone level). In these cases, the addition of androgens increases bioavailable testosterone concentration.
Several studies have tried testosterone at pharmacological doses and found positive impact on sexual outcomes (sexual desire, frequency and satisfaction), but androgenic adverse effects are not uncommon and it dissuades most women and doctors to use it.
Nevertheless, recently several randomized clinical trials have shown that testosterone replacement therapy (increasing testosterone levels but in the physiological range) is effective and well tolerated, especially for women after surgical menopause and with HSDD in spite of estrogenic therapy. Testosterone replacement increased frequency of satisfying sexual activity, improved sexual desire, and decreased distress after few months of treatment with a steady effect and with few adverse effects at least during 24 weeks. At the moment, safety data from follow-up studies support the persistence of previous findings at three years.
Conclusions: Prevalence and severity of HSDD are hormone-dependent and women after surgical menopause, especially at young age, constitute the main group at risk.
Estrogens improve sexuality-related factors but many times do not solve the problem. Several androgen treatments can improve the situation but pharmacological doses are limited for adverse effects. Testosterone transdermal replacement at physiological doses can improve sexuality without significant adverse effects, but long-term follow-up studies are needed to better understand the risk-benefits balance for the long-term treatment.
SM-11-04
HUMAN SEXUALITY AT THE BEGINNING OF THE 21ST CENTURY
C. Castelo-Branco
Hospital Clínic, Institut Clínic de Ginecologia, Obstetrícia i Neonatologia, Faculty of Medicine, University of Barcelona, Spain
Regardless of the relationship between aging and sexual dysfunction, most adults continue to be sexually active in their later years. Conditions such erectile dysfunction or hypoactive sexual desire disorder present one of many barriers to maintaining a healthy sex life. We evaluate the links between the social, cultural, political, and economic changes on a worldwide and historical level and the changes observed in sexuality. To give an idea about the interests and trends of modern research on sexuality, a review on the impact of contraception, public advertising, mass media and new technologies on sexuality and introduces the concept of sexual dysfunction are included. This review comprises from medical, biological and behavioural concerns to those of rights and social justice. The evolution of sexuality and human rights as well as social movements concerned with gender inequality and the oppression of sexual minorities is also considered. The influence of all these previous concerns on the field of sexuality notion is particularly apparent in the development of concepts such as sexual health and sexual rights. These new concepts had an effect on researchers allowing them to describe connections between highly limited occurrence and global systems. The international expansion of the metrosexual concept points up this last model. All these items and concepts are used to outline the restricted and open use of civil rights; the firsts as norms to control and the seconds to advance freedoms. Focusing on the relationship between these two approaches is a crucial question for the field of sexuality.
Data suggest that broader cultural beliefs about appropriate sexuality are evident in general practice. Asking about sexual health remains a low priority for many doctors, particularly when it comes to older patients.
Finally, the influence of all these previous concerns on the field of sexuality notion is particularly apparent in the development of concepts such as sexual health and sexual rights. These new concepts had an effect on researchers allowing them to describe connections between highly limited occurrence and global systems. Further education is needed to raise professional awareness about the importance of healthy sexuality in aging.
SM-12: Assessment and management in menopausal Brazilian woman (organised by the Sociedade Brasileira de Climaterio)
SM-12-01
EPIDEMIOLOGY OF THE BRAZILIAN WOMEN AGING
Nilson Roberto de Melo (Brazil)
Abstract not available at the time of going to press.
SM-12-02
THE INFLUENCE OF THE NEW CLINICAL TRIALS (AFTER WHI) ON THE CLINICAL PRACTICE IN BRAZIL
C. E. Fernandes
Gynecology and Obstetrics Department of the Medical Faculty of ABC, São Paulo, Brazil; Scientific Committee President of Brazilian Menopause Society (SOBRAC)
Since the first publication of the Women's Health Initiative (WHI) in 2002, the physicians have received several and conflicting information regarding the efficacy and safety of Hormone Replacement Therapy (HRT). The principal controversy and fear there has been the risk of heart disease in women using estrogen/progesterone combination also called HRT. The outcomes of this study are unknown on the physician's prescriptions in different cultures and in different parts of the world, particularly in Brazil. For this reasons, the objective of this presentation study is to evaluate the effects of the Women's Health Initiative (WHI) study on gynecologists in Brazil, with particular emphasis on knowledge, interpretation of the study and attitude regarding HRT. Therefore, aiming at to know the real impact of the WHI study in our country, We interviewed a total of 806 gynecologists through questionnaires. For the evaluation, questions regarding his/her degree of knowledge and interpretation of the WHI study, number of prescriptions written for HT and opinion regarding the ideal form of HT following the WHI study were analyzed. RESULTS: Physicians were found to have a good knowledge of the study (97.6%). The most common interpretation of the results of the WHI study referred to the single HT regimen used in the trial in patients with specific characteristics, this being the response of 66.3% of physicians. There was a reduction of 21.7% in the intention to prescribe HT, with 32.5% of gynecologists reporting changing to a different therapeutic regimen. After the WHI study, the gynecologists showed a preference for low doses of estrogens and new progestogens. These results permitted to conclude the WHI study had a relevant impact on the attitude of physicians, in particular the gynecologists, in Brazil.
SM-12-03
CHALLENGES IN THE ATTENDANCE TO THE BRAZILIAN CLIMACTERIC WOMAN
Lucas Viana Machado
Abstract not available at the time of going to press.
SM-13: The menopause in Mexico (organised by the Colegio Mexicano para el Estudio del Climaterio y la Posmenopausia)
SM-13-01
THE MENOPAUSE IN MEXICO
Carlos Ruben Salinas Dorantes, M. D. Puebla and Puebla Mexico
President of the Colegio Mexicano para el Estudio del Climaterio y la Posmenopausia (COMEC)
El Colegio Mexicano para el Estudio del Climaterio y la Posmenopausia is the manager of all the menopause associations from across the nation. At the moment 20 Associations are dedicated to the study of the menopause; establishing emphasis in the diffusion, medical upgrade and mainly a commitment with our mexican women to diffuse and to promote health; in order to make of their knowledge all the changes that they suffer as well as their measures of prevention.
The Colegio Mexicano is conscious that the feminine population of our country is growing in a very important way, since at the moment we have an average of 10 million women in the stage of menopause and the posmenopause.
This growth has made that the Colegio Mexicano, committed with the health of the Mexican women, be carrying out a series of tasks in which the base is the medical upgrade. In order to generate important changes, looking for the trust in our doctors for a good handling of the hormonal therapy.
Woman, given the information for means like written press, television and internet, have generated enough fear that has taken it to make important decisions as abandonment of their hormonal therapy, besides increasing their perception in a mistaken form, of which the subjective causes are against those that are really provoking a true increment in the woman's mortality in the menopause and posmenopause stage.
For this reason the Colegio Mexicano, understanding which are the main cause of mortality in the menopause and posmenopause stage, has prosecuted ourselves mainly in the upgrade in pathologies like hypertension, obesity, diabetes, metabolic syndrome and many more.
Likewise, we have looked for to prosecute the woman to take measures of prevention mainly in style and quality of life, informing in being careful with their foods, to take care of their weight, to carry out exercise and mainly in avoiding bad habits like tobacco, alcohol and other drugs. For this mean to take it to a road called quality of life.
SM-13-02
DATOS EPIDEMIOLÓGICOS DE MÉXICO
Raúl Domínguez (Mexico)
Abstract not available at the time of going to press.
SM-13-03
METABOLIC SYNDROME IN MEXICAN WOMEN
G. Cuauhtemoc Celis
Unidad Medica de Alta Especialidad, Hospital de Ginecoobstetricia “Luis Castelazo Ayala” Instituto Mexicano del Seguro Social, Mexico City, Mexico
Metabolic Syndrome (MS) is composed of a series of metabolic alterations caused by the combination of genetic factors and factors associated with life style, especially overfeeding (overeating) and lack (absence ) of physical activity, which causes an excess of body fat (particularly abdominal fat), and physical inactivity favors the development of insulin-resistance. The criteria proposed by the WHO for its diagnosis include: obesity, hypertension, glucose intolerance or type 2 Diabetes Mellitus (DM) and dyslipidemia. At menopause, women gain abdominal fat, which increases the risk of developing type 2 diabetes mellitus and cardiovascular disease.
Some of the variables that were found through the 2006 Mexican National Survey on Health and Nutrition (‘Encuesta Mexicana Nacional de Salud y Nutrición 2006’) were that more than 65% of the adult population (over 20 years) was overweight or obese. Among women, the prevalence was of 71.4% being more frequent among the urban population.
Arterial Hypertension in women was 18.7% in comparison to men at 11.4%; it is worth highlighting that in women over 50 years old the prevalence is 42% and by age 65 it was present in 63%.
Regarding type 2 DM, the number of new cases diagnosed among the population came to 394,208 cases, more frequently affecting women with a 61.2% of the total.
In relation with the prevalence of MS in postmenopausal Mexican women, in 2007, Cruz-Gutiérrez and Hernandez-Marín, from the Hospital Juarez, reported regarding an evaluation of 83 women with average ages of 55 years. The criteria of the National Cholesterol Education Program's Adult Treatment Panel III for the diagnosis of the metabolic syndrome.
The results obtained were: overweight in 56.6% and grade I obesity in 26.5%. Regarding the women, 44.5% presented MS, of which 94.5% had a triglyceride count of >150 mg/dl, 78.3% with waistlines of >88 cm, 72.9% HDL <50 mg/dl, P/B >130/85 mmHg in 64.8% and only 35% with glucose >110 mg/dl. The background of diabetes in the family is associated with an RR of 1.54 to suffer MS.
Conclusions: There is a high prevalence of MS in Mexico according to the results of the National Nutrition Survey and the report carried out at the Hospital Juarez where it was found in 44.57% of the women.
In pre-menopausal women, the characteristics and severity of the MS is related with weight, central obesity and alterations in lipids.
We suggest that patients with these characteristics must be more carefully assessed to make an early diagnosis of MS and avoid its repercussions.
SM-13-04
THE CLIMACTERIC IN MEXICO: QUALITY OF LIFE IN THE MEXICAN WOMAN
M. Eduardo Motta
Colegio Mexicano para el Estudio del Climaterio y la Postmenopausia, México City, México
We understand for quality of life, to live in plenitude by elimination, reduction and control from adverse factors the same fact of living.
Social standings, the social support, economic independence and security are comprehensive aspects that increase the well-being and that include themselves in the traditional concept of status of health.
The increase of the life expectancy followed by the therapeutic advances, places us in front of a new epidemiologic profile of the people of this age group, which is characterized for the bigger prevalence of the chronic processes. In Mexico the life expectancy in 2005 was 79 years for the woman and it is to be expected that for 2010 it will be of 80 years.
According to the US Census Bureau International Data Base for the 2035 in Mexico one of every three women will be in the stage of climacteric or in post-menopause and with a life expectancy of 83.4 years.
Mexico occupies one of the first worldwide places of cases of obesity.
In 1351 women, Hernández Bueno JA, Posadas C, Motta E., et al, found that 30.5% had a bigger Body Mass Index of 27 kg/m2, 36.4% suffered diabetes mellitus, 16.3% presented high blood pressure and the 10.7% had dyslipidemia.
The cardiovascular disease occupies the first place of the 10 more frequent causes of mortality. In 2005, 24,000 bigger women of 50 years died for this cause, while for mammary cancer were 4,221 deaths.
Regarding the symptomatology the result of Murillo's study, he found than of 619 studied women 70.5% presented vasomotor symptoms, decrease of the libido 76.9%, irritability 64% and insomnia 60%.
40% of the Mexican women lack absolute information of the changes that they suffer during pre-menopause and post-menopause, a 27% take a decision in comments from girlfriends or programs of media and only a 33% receive medical adequate information.
The quality of life is a complex situation that it requires of a valid instrument in the diagnosis, information and appropriate treatment so that the Mexican woman achieves a life with plenitude.
SM-13-05
CONCLUSIONS
Julio Morfín (Mexico)
Abstract not available at the time of going to press.
SM-14: Sexual steroids and breasts – endocrinology meets oncology (organised by the German Menopause Society)
SM-14-01
REGULATION OF INTRAMAMMARIAN STEROID METABOLISM
Petra Stute (Germany)
Abstract not available at the time of going to press.
SM-14-02
HORMONAL REGULATION OF BREAST CANCER CELL PROLIFERATION
H. Seeger
University Women's Hospital, Tuebingen, Germany
The proliferation of hormone receptor-positive breast cancer cells is clearly under the control of estrogens and progestogens. Estrogens appear to be the main stimulant of breast cancer cell proliferation. Apart from the parent substance estradiol, also some metabolites seem to be effective. The actions of estrogens can be mediated via two different receptor subtypes, i.e. ER-alpha and ER-beta. Experimental data suggest that these two subtypes may act in a yin-yang manner, whereby ER-beta seems to counteract the proliferative effects of ER-alpha. However, clinical data currently do not clearly support these results. Ligand-bound ERs can work in a classical genomic way and/or a non-genomic way. The classical genomic pathway includes binding to the typical DNA estrogen responsive element and consecutively activation of the transcription machinery. This pathway is usually characterized by a slow reaction time. The non-genomic pathway includes cross-reactions of the ER with intracellular signal molecules such as the tyrosine kinase domain of growth factor receptors or directly with the mitogenic kinase PI3K. In addition the ER-complex can bind to DNA elements such as AP1 or cyclin D1. Some of these effects may occur relatively rapid.
The action of progestogens on breast cancer cell proliferation is less clear. Most in vitro experiments delineated a small antiproliferative effect of progesterone and synthetic progestins in the presence of estrogens. This effect seems to be mediated mainly by activation of the progesterone receptor subtype B. The mechanism seems to be of a genomic manner, although also non-genomic mechanisms are conceivable. The latter, however, are currently only little investigated. The interaction of progestogens with stroma-derived growth factors on the proliferation of breast epithelial cells seems to be of significance, since certain progestins may act in an additive proliferative manner in combination with growth factors. Clinical studies support a proliferative action of synthetic progestins on breast cancer cell proliferation. This might be less prominent for progesterone. The different formation of two progesterone metabolites may be responsible that have been shown in vitro to act proliferative or non-proliferative on breast cancer cells.
SM-14-03
EFFECTS OF ENDOGENOUS AND EXOGENOUS HORMONES ON BREAST EPITHELIUM
I. Wiegratz
University Hospital of Frankfurt am Main, Germany
The influence of various reproductive factors, e.g., age at menarche or menopause, anovulation or lactation, suggests that life-time exposure to endogenous hormones correlates with breast cancer risk. The growth and function of normal human breast tissue is regulated by circulating sex steroids and undergoes cyclic phases of proliferation, differentiation and regression during the menstrual cycle. In the adult non-pregnant breast, epithelial proliferation is low in the follicular phase and maximal during the mid-luteal phase. The correlation between the mitosis rate and the serum levels of progesterone suggests that the endogenous progestogen is an important breast mitogen, probably in synergism with estradiol.
The response to endogenous and exogenous sex hormones differs between normal and malignant breast epithelium. Estrogens and progestogens exert their effects on epithelial cells by binding to the nuclear receptors ERα, ERβ, PRA and PRB. The cells containing sex steroid receptors do not proliferate, but stimulate the growth of adjacent epithelial cells by releasing paracrine growth factors. The malignant transformation of normal epithelial cells to breast cancer cells is associated with a continuous decrease of ERα which inhibits the activity of ERβ, and a shift to autocrine regulation as reflected by an increase in ERβ expression in proliferating cells.
In experimental studies testosterone exerts an anti-proliferative and pro-apoptotic effect mediated by the androgen receptor. In patients with polycystic ovary syndrome who have chronic estrogen exposure and androgen excess, the risk of breast cancer is not increased, but rather decreased. In contrast, postmenopausal women with elevated testosterone levels have a higher breast cancer risk, possibly due to the aromatization of testosterone to estradiol.
Estrogen replacement therapy is associated with a moderately elevated breast cancer risk which is enhanced by the addition of progestogens. A medicolegal autopsy study revealed that at the time of menopause about 40% of the women have already occult breast carcinomas. This suggests that the increase in the breast cancer incidence during hormone replacement therapy is dependent on the proliferative effect of exogenous estrogens and progestogens on pre-existing tumors, rather than on a carcinogenic action. Growth of hormone receptor-positive breast tumors which are more differentiated, may be stimulated by hormone therapy resulting in an earlier diagnosis and a better prognosis. Whether or not progestogens differ in their effect on the development of breast cancer and the influence of additional androgen therapy remain to be elucidated.
SM-15: Progestogens and target tissues (organised by the European Progestin Club)
SM-15-01
GENE POLYMORPHISMS AND BIOLOGICAL ACTIONS OF PROGESTINS
J. H. H. Thijssen
The Netherlands
The biological effects of progesterone and of synthetic progestins in tissues depend on a number of factors: the expression of the Progesterone Receptors (PR), the local metabolism of the ligands, the relative expression of the two PR-isoforms (PRA and PRB), the receptor binding to coregulators and on crosstalk with other signal transduction pathways.
In the DNA coding for the proteins involved in these steps, a large number of polymorphisms has been demonstrated. Polymorphisms have been found in the isoforms of the progesterone receptor, in enzymes involved in steroid biosynthesis and metabolism and in several of the coactivators and corepressors required for the final transcriptional activity in the nuclei of cells. These coregulators control the extent of gene expression from ligand-activated steroid receptors in such a way that changes in their structure and subsequent biological activity can lead to significant differences in responses of target tissues to the hormone ligands.
Already almost 300 of these coregulators have been identified, a number of them play important roles in diverse pathological processes, such as cancer, inherited metabolic diseases, metabolic disorders and inflammation. A number of polymorphisms in these proteins have been studied in relation to specific abnormalities in patients. Some associations have been found but at present it is impossible to positively link specific polymorphisms to specific diseases in the human. In particular no consistent findings have been reported yet in relation to the actions of progesterone and progestins.
SM-15-02
THE DIALECTIC OF BOTH PROGESTERONE RECEPTORS A AND B
J. C. Huber
Department of Obstetrics and Gynecology, Division of Gynecologic Endocrinology and Reproductive Medicine, Vienna General Hospital, Austria
Similar to estrogen-receptors and androgen-receptors, also the progesterone-receptors display two genotypes and two phenotypes. They are transcribed from two alternative promotors and translated into two different zinc-finger proteins, progesterone-receptor A and progesteron-receptor B.
These differ by a 165-amino-aced region presented only in the progesterone-receptor B. Progesterone B is a potent transcriptional activator and contributes to the proliferative effects of estrogen, whereas progesterone-receptor A, the shorter isoform is necessary to oppose the effects of both progesterone-recetor B and the estrogen-receptors. This balance between both receptors modulate angiogenesis and is important for implantation and pregnancy. But in the menopause, the physiological effect of progesterone-receptor A is more desirable.
SM-15-03
PROGESTOGENS AND THE BRAIN
A. R. Genazzani and N. Pluchino
Department of Reproductive Medicine and Child Development, Division of Obstetrics and Gynecology University of Pisa
Progesterone and synthetic progestins play an important role in the modulation of brain activity and responses to environmental stimuli, affecting “reproductive” and “nonreproductive” functions. Progesterone and synthetic progestational agents modulate the synthesis and release of neurotransmitters, neuropeptides and neurotrophic factors in response to specific physiological and pathological stimuli. These effects have been attributed to the direct interaction of progestogens to their receptor in CNS and PNS and to metabolism into neuroactive 3α, 5α metabolites, such as Allopregnanolone. This is a potent endogenous steroid that rapidly affects the excitability of neurons and glia cells through direct modulation of the activity of γ-aminobutyric acid A receptors. Allopregnanolone exerts neuropharmacological actions, with hypnotic/sedative, anxiolytic, anesthetic, analgesic functions and it enhances the myelination/remyelination process.
This last neuroprotective effect of P has first been observed in peripheral nerves, where P synthesized by Schwann cells promotes the formation of new myelin sheaths after lesion, but it has been demonstrated even for CNS. This function is of significance for the aging brain and peripheral nerves, characterized by the loss of myelin. In addition, the profound effects on the serotoninergic and opioidergic systems explain the meaningful influence of progesterone in the modulation of affective behaviour, cognitive function and measures of quality of life.
Synthetic progestins differ widely from natural progesterone in their chemical structure, pharmacokinetics, potency and biological response of target tissues, such as CNS, may results divergent. The full characterization of the biological and pharmacological spectrum of actions of natural progesterone and progestins, will be one of the keys to achieve better and more individualized therapies for postmenopausal women.
SM-15-04
PROGESTOGENS AND TARGET TISSUES: VASCULAR SYSTEMS
Alfred O. Mueck
University Women's Hospital of Tuebingen, Germany
There are more than 1.000 experimental and clinical studies investigating the vascular effects of progestogens. As the addition of a progestogen to estrogen therapy in peri- and postmenopausal women comprises nearly 90% of the total market of progestogens, most of our knowledge is derived from studies with HRT on the effect of progestogens added to estrogens tested for different conditions. Furthermore using progestogens for this indication mostly corresponds to a therapywith treatment durations for more than 1–2 years in contrast to only short-term therapy for other indications like bleeding disorders, endometrial hyperplasia, endometriosis-related symptoms, benign breast disease, premenstrual syndrome etc. Whereas on the molecular level the basic mechanisms of progestogenic action seem to be similar for the different target tissues, the vascular effects of progestogens interfer in a very complex multi-factorial way with nearly all functions in the cardiovascular system, i.e. including not only the direct effects on the target tissue ‘vasculature’ but also interactions with metabolic changes, blood flow functions, nervous regulations etc. The research on this topic mainly includes the following areas:
1) vascular effects on mediators and ‘surrogate markers’ (endothelium- and non-endothelium-derived) and metabolic effects with intravascular impact (lipids, carbohydrates, clotting factors, intermediate metabolism) 2) vascular function studies (blood-flow measurements; reactive flow-mediated dilatation etc.) 3) atherosclerosis staging evaluations (coronary angiography, electron-beam-CT, arterial stiffness; intima media thickness) 4) blood pressure trials (office BP, 24 h ambulatory BP, day/night time differences, correlation with cardiac parameters etc), and, most important 5) clinical endpoint studies. In most of those studies vascular progestogen effects have been shown to be rather unwanted adverse effects reducing or abolishing estrogenic benefits.
For practical recommendations to minimize risk in seems reasonable to consider crucial parameters for different vascular progestational action derived from experimental studies like glucocorticoid or antimineralocorticoid effects, important for initiation of atherosclerosis or blood pressure regulation, resp., or the different impact of progestational vascular effect dependent on pharmacokinetic differences like for peak concentrations during progestogen therapy. In general most negative progestogen effects depend on the stage of the impaired vascular functions. For older patients it is essential to consider the negative results in WHI concerning stroke and coronary heart disease. Clinical endpoint studies on lower evidence level suggest different effects depending on type, dosage and application form of progestogen addition which suggest an individualized choice of progestogen therapy.
SM-16: Cardiovascular risk and hormone therapy: is something changing? (organised by the Asociación Argentina para el Estudio del Climaterio)
SM-16-01
GLOBAL CARDIOVASCULAR RISK IN THE EARLY MENOPAUSE
E. Esteban
AAPEC, Ciudad Autónoma de Buenos Aires, Argentina
CHD is the main killer in women. The epidemiology of cardiovascular disease responds to differences connected with the poblational group studied; its age, ethnic, sociocultural and regional composition.
There's no doubt that currently all the civilization diseases like obesity, diabetes mellitus, hypertension, metabolic syndrome and lipid disorders depend of the interaction between genes and environment.
It's a fact that women during reproductive years are a lot less vulnerable than men to the effect of environment factors and lifestyle.
Estrogens are the unbalancing element as biochemical expression of the sexual difference, markers by excellence, the same as progesterone of the qualities of ‘being a woman’.
SM-16-02
BLOOD PRESSURE DESCENT DURING HORMONE THERAPY
A. Martire
AAPEC, Ciudad Autónoma de Buenos Aires, Argentina
The majority of hormone therapies either don't have an effect on blood pressure or they can increase it due to the estrogenic and/or progestogenic impact over the rennin sustratum and the activation of the rennin-angiotensin-aldosterone system. Since a while ago we have progestogenes available with antimineralcorticoid activity (antialdosteronic), like Drospirenone, which offers advantages over other progestogenes available in the field of CHD. Numerous clinical studies have shown that it achieves a slight decrease of the blood pressure values without increasing the risk of hyperkalemia. That is why it is the ideal progestogen to be indicated to patients with high blood pressure or blood pressure that fluctuates from normal to high.
SM-16-03
HORMONE THERAPY IN RECENT MENOPAUSE AND CARDIOVASCULAR RISK: AVAILABLE EVIDENCE
A. Di Costanzo
AAPEC, Ciudad Autónoma de Buenos Aires, Argentina
The current evidence available that links hormone therapy and coronary heart disease (CHD) is initially based on observational studies on women with and without existing CHD who use hormone therapy. Such use was associated with a reduction of coronary events, but clearly these studies have overestimated the benefits of postmenopausal hormone therapy possibly due to bias on the selection of patients.
In addition to that we are now familiar with the concept ‘window of opportunity’ for the reduction of cardiovascular risk that links the time of initiation of the hormone therapy with the underlying state of the vasculature. The estrogens may delay the onset of the earliest stages of atherosclerosis (present in young women), but they may also trigger events on advanced lesions in older women.
In contrast the clinical randomized controlled studies have shown absence of benefits or increase of cardiovascular risk in some cases; being not less true that they involved older women who began hormone therapy a decade after their menopause.
To conclude, women who start hormone therapy close to menopause tend to reduce the cardiovascular risk in a non-statistically significant way, in comparison with the ones who start it late.
Stroke risk is increased regardless the time elapsed after the onset of menopause though randomized studies indicate a low incidence on the ages between 50 and 59.
Even in younger women prior risk factors for stroke shouldn't be ignored when analysing a patient's clinical history to prescribe hormone therapy.
SM-16-04
CAN HORMONE THERAPY REDUCE CARDIOVASCULAR RISK?
M. Murga
AAPEC, Ciudad Autónoma de Buenos, Argentina
All we know is that CHD is the most frequent cause of morbidity and mortality in women and also that the primary prevention is related to the control of the risk factors.
Hormone therapy is not indicated for primary prevention of CHD at any age, although it probably doesn't increase the risk in healthy young women (50–59 years), with estrogen beneficial actions on endotelial function and blood lipids.
Current data doesn't support the use of hormone therapy in second CHD prevention.
The healthy consequences of hormone therapy are connected with the distance from menopause showing a slightly significant benefit on the reduction CHD risk for women close to menopause.
SM-17: The roles of phytoestrogen in climacteric women (organised by the Indonesian Menopause Society)
SM-17-01
THE BENEFIT OF RED CLOVER IN MEN – QOL & BONE TURN-OVER IN CLIMACTERIC WOMEN
M. S. Darmasetiawan1, G. D. Prayitno1 and A. Hestiantoro2
1Department of Obstetric Gatot Soebroto Central Army Hospital/Pembangunan Nasional “Veteran” University; 2Department Obstetric & Gynaecology, RSCM/Indonesian University
Background:The WHI publication; which represent the latest result of RCT involving a significance large scale of respondents; have created a considerable confusion and concerns among women, care-givers, and the media as well. It seems that the conclusions regarding the possible value of MHT (menopausal hormonal therapy), highly uncertain and devalues the conclusions from the previous publication, from which, so many clinical implication have been drawn. Although IMS has already published an “Updated recommendations” on MHT as a general guidance in clinical decision making, in fact women and even many health providers remained hesitate to receive/prescribe MHT. As a consequence, many postmenopausal women are now using alternative or complementary medicines instead of standard menopausal hormone therapy.
For century, women in Asian and Mediterranean cultures have benefited from the effects of plant phytoestrogens consumes in the form of soybeans and other legumes. They claimed generally breeze through menopause, whereas Western women suffer from hot flush, depression, insomnia, and others unpleasant symptom. Researchers are discovering that the differences may be dietary. Studies show that these important plant compounds such isoflavones, may help bridge the hormonal gap as natural estrogen levels decline with menopause. Standardized red clover extracts as one of the isoflavones derivative are currently being marketed for alleviating of menopausal symptoms and registered as supplement instead of drugs. Although there are many studies on isoflavones including red clover, there is still conflicting data pertaining to the real beneficial effect of this regimen. The aim of this present study was to investigate the role of red clover which easily available and generally accepted in the market on quality of life and bone turnover.
Methodology: This was a prospective randomized, double blind control study. The treatment group was received a regimen contain of red clover 40 mg tablet and was administered 2 times daily and calcium citrate 500 mg as control group. Ethical clearance was obtained from the hospital ethical committee. Menopausal quality of life were assessed using the Hilldinck MENQOL questionnaire which consist of 4 domains. Vasomotor symptoms questionnaire Q1-Q3, psychological symptoms Q4‐Q10, physical symptoms Q11‐Q26, and sexual symptoms Q27-Q29. Subjects were randomly assigned to received red clover 40 mgr twice daily or placebo and assessed for MENQOL, serum C- Telopeptide (CTX), serum N-mid osteocalcin, and densitometry at baseline, 3 month, and after 6 months. Lumbar and hips bone mineral density were measured using dual energy X-ray absorptiomethry (Hologic QDR‐4500). Gathered data were processed through SPSS 12 program and analyzed using Mann-Whithney U and Pearson Chi-Square test.
Result: From September 2005 to July 2006 there were 61 respondents being recruited to this study. They comprises of peri/postmenopausal women age 45–55 years. Women on treatment group showed remarkable improvement (p < 0.05) in 15 out of 29 climacteric symptoms (MENQOL Q‐1, Q‐2, Q‐5, Q‐6, Q‐11, Q‐13, Q‐14, Q‐15, Q‐17, Q‐18, Q‐21, Q‐22, Q‐24, Q‐25, and Q‐28). Bone mineral density was declined in both group which is not statistically significant (rate of change for spine: −2.14% (SD 3.325) VS −0.87% (SD 3.531), p = 0.910 and rate of change for hips: −0.544% (SD 4.902) VS −0.48 (SD 3.050), p = 0.345). Bone turn over was increased in both group. The increment of serum CTX was higher on treatment group compare to that of control group (+ 39.4% VS + 4.74%, p = 0.013). Whilst serum N-mid osteocalcin increased not significantly among two groups (+ 34.4% VS + 16.1%, p = 0.224).
Conclusion: Red clover reduces climacteric symptoms mainly at vasomotor domain, physical, and psychological domain but not at sexual domain. There was no changes on bone mineral density within 6 months of treatment with red clover, but there was an increased of bone turn over in both group. Further investigation should be carried out in a long term study design for investigating the beneficial effect of red clover on bone.
SM-17-02
THE EFFECT OF RED COVER AND BLACK COHOSH COMBINATION IN BONE MINERAL DENSITY
I. A. Rachman, S. Marly, T. Rotikan and A. Tobing
Faculty of Medicine University of Indonesia
Estrogen that derived from plants (Red clover – RC and Black Cohosh – BC) are phytoestrogen consist isoflavon, lignan, and caumestan. The isoflavon from red clover are Genestein, Daidzein, Formonetin, and Biochanin A. The isoflavon formulas are very similar to 17β estradiol and bind beta estradiol receptor seven times sronger from alpha estrogen receptor, but the affinity to alpha estrogen receptor is 35% and the affinity to beta estrogen receptor is 5% compare to estradiol. An active ingredients from black cohosh is cimifuga racemosa extract show as phyto-serm with additional CNS active compound. For these reasons, we were comparing 3 groups consist of perimenopause osteoporosis women in different number with three different therapies for 2 years of observation. First, for Group A, we have been giving Hormon replacement Therapy + Calcium (Cal) + Weight bearing exercise (WBE) to 52 perimenopause osteoporosis women. For Group B consist of 51 perimenopause osteoporosis women, we gave them Phytoestrogen (225 mg RC and 40 mg BC) + Calcium + WBE. For group C consist o 42 perimenopause osteoporosis women, we gave them only Calcium and WBE (Placebo). The results was 98.2% reduction in menopause symptom in Group A after 6 months therapy, and after 1 or 2 years therapy the decrease of menopause symptom is between 95.7% –99.2%. Compared to Group B, there was 49.7% decreased of menopause symptom after 6 months therapy, 78.4% decreased of menopause symptom after 1 year therapy and 80.1% decreased after 2 year therapy. For Group C, after 6 months therapy, there was 9.7% decreased of menopause symptom, 19.1% decreased of menopause symptom after 1 year therapy, and 12.8% decreased of menopause symptom after 2 years of therapy. For bone density in Group A, there was an increase of 5.7% after 1 year therapy, and it increased up to 9.7% after 2 years therapy. For group B, the increase of bone density after 1 year therapy is 3.1%, and 4.6% increased after 2 years therapy. The bone density in group C increase about 1.3% after 1 year therapy, and 2.6% increased after 2 years therapy. We finally found that the power of phytoestrogen in decreasing menopause symptom is about 33% from estrogen conyugation and it was six time better than placebo. The Bone densitometer increase about 60% from estrogen conyugation and it was 2–3 times better than placebo. Further longtime and multi center phytoestrogen study is still necessary to evaluate the safety of using Phytoestrogen therapy.
SM-17-03
THE ESTROGENIC EFFECT OF SOY POWDER RICH-IN-ISOFLAVONE ON THE DENSITY LEVEL OF THE MANDIBULAR BONE (EXPERIMENTAL STUDY ON SPRAGUE DAWLEY HYPOESTROGENIC FEMALE RATS)
W. Anggraini1 and I. A. Rachman2
1University of Trisakti, Indonesia; 2University of Indonesia, Indonesia
Objective: To provide evidence on estrogenic effect of soy powder rich in isoflavone to prevent the decreasing density of the mandibular bone
Subject: Thirty-two female Sprague Dawley (SD) rats at the age of 12 (twelve) months and all have been ovariectomized (ovx).
Design and Method: This study is using the experimental design pre-post condition with control. The in vivo experimental were conducted to the hypo-estrogenic SD female rats. There are four groups, with eight rats in each group as follow: the no ovx group is the normal bone density group used for standard reference, the ovx group is the negative control group, the ovx + 17β-estradiol group is the positive control group and the ovx + soy powder rich in isoflavone as the experimental group. The 17β-estradiol doses is 0.01125 mg/day, which is equivalent to 0.625 mg/day in humans, the soy isoflavones dose is 2.1117 mg/day, which is equivalent to 118.25 mg/day in humans. During experiment, food given to the rats were given portions according to the AOAC (1990) and their blood was taken three times as follows: day‐0, day‐10 and day‐50. The research parameters are as follows: plasma calcium, bone calcium, plasma estradiol, and trabeculation of alveolar mandibular bone value. The statistic evaluation is using 1 way-ANOVA with the contrast test and the post hoc test. Statistical significance was accepted at p < 0.5. The categorylevel of the alveolar mandibular bone density is determinedat the cutting point of 71.67 with a degree of sensitivity at 87.5% and specification at 69.9% area under the ROC curve of 0.815. The statistic evaluation fordata categoryis using the Kruskal-Wallis test.
Results: Plasma calcium analysis indicated the following: no ovx (p:1.000), ovx (p:0.000), ovx + isoflavone (p:0.000), and ovx + estradiol (p:0.012). Plasma estradiol analysis indicated the following: no ovx (p:0.014), ovx (p:0.000), ovx + isoflavone (p:0.007), and ovx + estradiol (p:0.033). Bone calcium analysis between experiment groups indicated p:0.683. A contrast test on the trabeculation of alveolar mandibular bone indicated that the ovx group is lower compared to the trabeculation bone in theovx + isoflavonegroup and the ovx + estradiol group. Result of the Kruskal-Wallis test indicated p:0.002. The post hoc test result between the ovx + isoflavoneand the ovx + estradiol groups, against the plasma calcium delta on day‐10 and day‐50, the estradiol plasma delta on day‐10 and day‐50, the trabeculation of the alveolar mandible, and bone calcium content indicated that there was no significant difference (p>α).
Conclusion: Soy powder rich in isoflavone may decrease the rate or prevent a drop of the alveolar mandible bone density. If compared to the 17β-estradiol, the soy powder rich in isoflavones has the same effect towards the density level of mandibular bone on the hypoestrogenic rats.
SM-17-04
EFFECT OF ISOFLAVON DAIDZEIN (ID) FROM KACANGTUNGGAK (VIGINA UNGUICILATA) ON MENOPAUSAL SYMPTOMS, VAGINAL HEALTH, BONE DENSITY AND DISLIPIDAEMIA IN MENOPAUSAL WOMEN
A. Hidajat, W. Ngartjono, I. W. Arsana, M. D. Pande, Sutrisno, H. Wibisono, M. Tangkas, S. Rahmaniah, T. Sujiati, I. W. A. Indrawan and H. Wiradharma
Objective: To determine effects of Isoflavone Daidzein (ID) derived from Kacangtunggak (Vigina unguicilata) on menopausal symtomps, vaginal health, bone density and dislipidaemia in menopausal women.
Design and Method: RCT in 60 menopausal women, 30 given 67.5 mg/day ID and the other half placebo for control. (By HPLC 100gram dry powder kacangtunggak contain 16.6 mg Daidzein and no Genistein). Evaluation done before and after:
12 weeks for menopausal complaints (Kupperman's Index and Symtoms Severity Score = SSS).
24 weeks for Vaginal Health Index.
24 weeks for Vaginal Cytologic Maturation Index and Maturation Value.
12 and 24 weeks for Bone Density (Quantitative Ultrasound).
12 weeks for Laboratory Lipid Profile (Total Cholesterol, Triglyceride, HDL, LDL).
Symptoms reduced: myalgia (92.3%), fatigue (77%), hot flushes (53.8%). Relative Risk Reduction for myalgia 76.6%, fatique 55.7%, hot flushes 39.2% and SSS 68.7%. Age, postmenopausal interval, occupation and formal graduates have no significant effect on menopausal symptoms (p>0.01).
No significant change of the Vaginal Health Index (p>0.05).
Significant influence on Confounding variable of age (p = 0.014), menopausal length (p = 0.027).
No significant change of vaginal epithel growth after 12 weeks (p = 0.835) or 24 weeks (p = 0.860).
Significant change of densitometry calculation mean (p = 0.006). The T-score meandifference was 0.952 (SE = 0.221) and for control–0.768 (SE = 0.212). Coffee as confounding variable had a significant influence at 12 weeks evaluation (p = 0.43) but not at 24 weeks.
No significant change on lipid fraction (p>0.05). Concomitant variable: age, postmenopausal interval, obesity, high fat diet, physical activity have no significant effect. Respectively, total cholesterol decreased 55.6% (control 55.6% decreased), triglyceride increased 88.9% (control 85.2% increased), HDL decreased 51.9% (control 59.3% decreased) and LDL increased 85.2% (control 74.1% increased).
For 12 weeks reduce menopausal symptoms.
For 24 weeks don't improve menopausal vaginal health.
For 24 weeks don't improve menopausal vaginal epithel growth.
For 12 and 24 weeks give a positif influence on menopausal bone density.
For 12 weeks don't improve menopausal dyslipidaemia.
SM-18: Situación actual del climaterio y menopausia en Ecuador (organised by the SECLIM)
SM-18-01
EVOLUTION OF THE STUDY AND MANAGEMENT OF THE MENOPAUSE IN ECUADOR: THE INFLUENCE OF SCIENTIFIC SOCIETIES
Luis Hidalgo
Enrique C. Sotomayor Gynecology and Obstetrics Hospital, Guayaquil-Ecuador
The Ecuadorian Climacteric and Menopause Society (SECLIM) was established in Quito May 1st 1993 counting with a multidisciplinary medical team among them gynecologists, cardiologists, endocrinologists and internal medicine specialists. A primary initial goal was to recruit physicians interested in the research of the menopause and similar areas. Few months after this aim was fulfilled as more than one hundred specialists had adhered to the cause among them traumatologists, psychiatrists and urologists. Subsequently the promotion and exchange of knowledge and research in morphofunctional, clinical and therapeutical aspects related to the climacteric ensued within Ecuador, followed to several Ibero-American and developed world countries as well. In parallel, the performance and publication of several national and international, and the establishment of 13 society nucleus confirm the positive impact of the initial effort. A positive interaction with other scientific societies has also been established over the years which in general has aided in the spreading of scientific knowledge. Since SECLIM's establishment five national congresses, one international and two national Consensus Workshops have been organized. The latter ending in the editing of two guideline textbooks for the management of the menopause which have definitively had a major impact at the educational level among specialists and non specialists seeking to improve healthcare and specifically quality of life of women during the climacteric.
SM-18-02
QUALITY OF LIFE DURING THE CLIMACTERIC IN ECUADOR
Patricia León-León
Facultad de Ciencias Médicas, Universidad de Guayaquil; Hospital Clínica Kennedy, Guayaquil, Ecuador
Quality of life (QoL) specifically refers to individual's perceived physical and mental health over time. Its assessment during the menopausal transition has become an essential component of clinical practice in providing a comprehensive picture of the effects of the menopause, helping the practitioner decide appropriate management through the valuable information obtained. The useful definition of “Health Related Quality of Life” (HRQoL), as a multidimensional concept that encompasses physical, psychological, social and other domains of functioning specific to a given health condition, requires validated assessing instruments which must be modern, reliable, and capable of giving comparable results when compared to that rendered by other tools. Interest regarding clinical research of aging women has increased in recent years in Ecuador, with focus in measuring their HRQoL and symptoms. HRQoL assessment with sound menopausal-specific tools has been performed worldwide and among the Ecuadorian female population. It has been demonstrated that the severity of climacteric symptoms deeply affects different measures of QoL. An evaluation of a low-socio-economic Ecuadorian climacteric population with the Greene Climacteric Scale determined an overall increasing tendency of climacteric symptoms from the perimenopausal to the postmenopause status. Higher scorings were associated to higher age (47 or more), higher parity and lower educational level. The most prevalent encountered symptoms were those related to the somatic and vasomotor cluster and the psychological subscale. On the other hand, age, ovarian function, hysterectomy, lower schooling and masculine erectile dysfunction caused increased sexual dysfunction, also related to impaired QoL. The frequency and intensity of menopausal symptoms as well as associated risk factors among healthy pre-peri and postmenopausal Ecuadorian women have been also measured with the Menopause Rating Scale, another standardized HRQoL scale, in which higher somatic and psychological scorings were related to lower educational level in peri and postmenopausal women. Higher total, as well as somatic, psychological and urogenital scorings were revealed in sexually inactive women. QoL surveys need to be condition specific. Assessing a specific postmenopausal Ecuadorian population using the Menopause-Specific QoL Questionnaire, revealed impaired QoL among those younger and with <5 years of menopause onset as they presented higher vasomotor domain scores, situation also associated to age, abdominal obesity, hypertension and hyperglycemia. This evidence of impaired QoL found in Ecuador have become a referral for the comparison of other similar female populations. We look forward to encouraging the development of programs seeking QoL improvement among aging women.
SM-18-03
THE METABOLIC SYNDROME DURING THE POSTMENOPAUSE
Peter Chedraui
Institute of Biomedicine, Universidad Católica de Santiago de Guayaquil, Ecuador
The metabolic syndrome is defined as a group of lipid and non-lipid risk factors which increase the risk of developing cardiovascular disease (CVD). According to the Third Adult Treatment Panel (ATP III) three or more of the following risk factors are required to establish the diagnosis: abdominal obesity, decreased high-density lipoprotein cholesterol (HDL-C), and increased serum triglycerides (TG), fasting glucose and/or blood pressure levels. The prevalence of this syndrome increases with age and is higher among women, especially those of Hispanic origin. Moreover, after the menopause there is an emergence of features related to the syndrome, possibly, but not totally related to estrogenic deficiency. In Latin America, Ecuador included, the prevalence of the metabolic syndrome has been reported to be high. Important to mention is that obesity, one of the features of the syndrome, is increasing in Latin America and has been found to be associated to poverty conditions, increased menopausal symptoms, decreased quality of life and high risk for CVD. As sedentarism among postmenopausal women increases the risk of presenting abdominal obesity, educational programs within this population should be encouraged aimed to increase their knowledge regarding the problem, promoting lifestyle and diet modification which in turn will decrease cardiovascular risk. In the developing world, where pharmacologic intervention is shadowed by poverty and lack of public health coverage, these programs constitute an important cost-effective method.
SM-18-04
BONE HEALTH AFTER THE MENOPAUSE
Wéllington Aguirre
Unidad de Salud Postmenopáusica y Endocrinología Femenina, Quito-Ecuador
After the menopause onset and the subsequent ensuing chronic hypoestrogenic state, bone remodeling, necessary for maintaining healthy bone, suffers substantial changes shifting to a state of predominant bone resorption which eventually leads to bone mineral depletion. This situation, three fold in comparison to previous years, may lead, if correlated to inadequate nutrition, sedentary habits and low bone mass, to an increased risk for bone fractures. Osteoporosis is a highly prevalent worldwide problem, affecting both genders (however more frequent in women) and all ethnic backgrounds in varying rates. Bone fracture is the final event and the most severe complication. In Ecuador interest regarding the osteoporosis dates since 1987 year in which the Ecuadorian Mineral Metabolism Society (SECUAMEM) was established. One year after it organizes in Quito the 1st Ecuadorian Osteoporosis and Bone Disorders Congress, also hosting the 1st Congress of Osteoporosis and Mineral Metabolism of the Ibero American Society (SIBOM), scientific society that was established during this event. Simultaneously, in the private and public sector research regarding bone mineral density among the Ecuadorian population commences reporting its incidence among several institutions and fracture prevalences among hospitalized patients. These studies have allowed us to find that the incidence of osteoporosis and its complications are very much similar to that found in the world literature. In the up-coming years, four national and international scientific events have taken place, in some occasions in conjunction with other societies, and two consensus guideline text books have been edited one in 2001 and the other in 2007.
SM-18-05
PRIMARY HEALTH CARE MODEL PROPOSAL FOR THE MANAGEMENT OF THE MENOPAUSE IN ECUADOR AND LATIN AMERICA
Luis Rivadeneira
Facultad de Ciencias Médicas, Universidad de Guayaquil
Female well-being during the menopausal transition depends upon genetic background, and also life styles and therapeutic measures taken in accordance with their physicians, in order to prevent, diagnose or treat the disorders they may confront from the psycho, physical, emotional and social point of view. Management of the menopause must therefore necessarily engage with any primary healthcare model in providing the early identification of chronic illnesses (i.e., diabetes, hypertension, cancer), changes in lifestyle, educational program implementations (i.e., enhancing knowledge regarding the menopause), treatment of symptoms with hormonal and non hormonal methods. One must bear in mind that the female climacteric is a natural phenomena and that all women must transit through it with quality if life. For this we propose a primary health care model for the management of the menopause in Ecuador and other similar Latin American developing countries.
SM-19: Menopause, Asia Pacific perspective and treatment (organised by the Asia Pacific Menopause Federation)
SM-19-01
DIFFERENTIAL PREVALENCE OF QUALITY-OF-LIFE CATEGORIES (DOMAINS) IN ASIAN WOMEN
K. K. Limpaphayom, M. S. Darmasetiawan, R. I. Hussain, S. W. Burriss, C. F. Holinka and M. K. Ausmanas
Chulalongkorn University, Bangkok, Thailand
Objectives: To assess the prevalence of four categories (domains) of menopausal symptoms as markers for quality of life in nine ethnic groups of Asian women. To evaluate changes in quality of life (MENQOL scores) in Asian women following hormone therapy.
Methods: A prospective, randomized, double-blind, multinational clinical trail in 1028 healthy postmenopausal women of nine ethnic groups form 11 Asian countries/regions. Following 2 weeks of baseline observation, the women received one of three conjugated estrogens (CE)/medroxyprogesterone acetate (MPA) doses (in mg) daily for 24 weeks: 0.625/2.5, 0.45/1.5, or 0.3/1.5. At baseline and at the end of weeks 4, 12 and 24 following the start of therapy, the study participants were asked to record, on a menopause-specific quality of life (MENQOL) questionnaire, 29 menopausal symptoms, as experienced during the preceding month. The symptoms were categorized into four domains: vasomotor, psychosocial, physical and sexual.
Results: The baseline (pretreatment) symptom scores in each of the four domains varied substantially among the different ethnic groups, ranging from 2.21 to 5.71 in the vasomotor, 2.37–5.96 in the psychosocial, 2.66–5.39 in the physical, and 2.11–6.55 in the sexual domain. Overall, Vietnamese and Pakistani women had the highest baseline scores, i.e. were most afflicted by each set of symptoms in a given domain, and Indonesian, Malay, Taiwanese and Thai women were least afflicted. In the overall population, intervention resulted in statistically significant decreases in the scores of all four domains within 4 weeks of intervention. The beneficial effects were similar in the three dose groups.
Conclusion: The prevalence of four domains of menopausal symptoms, representative of quality of life as recorded on a MENQOL questionnaire, varies considerably among ethnic groups of Asian women. The MENQOL scores in the overall population were significantly lowered in the course of the study, indicating an improvement in quality of life. In the absence of a placebo group, the relative contribution of hormones and placebo in our intervention is unknown.
SM-19-02
ASIAN WOMEN'S THOUGHTS AND FEELINGS ABOUT MENOPAUSE AND HRT: COMPARISON WITH THAT OF EUROPEAN WOMEN
Ko-En Huang
Chang Gung University/Hospital, Kaohsiung, Taiwan
Objectives: It has been thought that the perspectives of Asian women on menopause could be different from that of Caucasian women. The objective of this study was to survey the Asian women's thoughts and feelings about menopause and HRT and compare the results with that of European women.
Methods: One thousand women ages 45–60 years from five Asian countries/regions, China (300), Hong Kong (100), Malaysia (300), Taiwan (150), and Thailand (150), were interviewed face to face by specifically trained interviewers using the prepared questions on the thoughts and feelings about menopause and HRT. These results were compared with the results of telephone interview done in European.
Results: The results showed that the menopausal symptoms of Asian women were different from those of European women with the most frequently complained symptom being sleeplessness among Asian compared to hot flushes among European. About 85% of both Asian and European women thought menopause should be treated. The awareness of HRT was widely variable among the Asian countries and 43% expressed negative perception. 55% of Asian women mentioned that fear of breast cancer risk prevent them from HRT. 75% of Asian women thought menopause has negative impact to sexuality that may cause poor quality of life. However, majority of them have not intended for treatment and hope that their doctors would bring the sexuality issue for discussion. 85% of Asian and 57% of European women accept that reduced sex after menopause is natural. Although women do not openly discussed about their sexual problems, more than 60% of respondents expect a more enjoyable life if their sexual function improves.
Conclusion: Half of Asian menopausal women are affected by menopause. Sleeplessness and hot flushes are two most common reasons for seeking treatment for Asian women. Although most women have not received any treatment for menopause, they believe menopausal symptoms need to be treated. However, knowledge of HRT is generally quite negative and the main reason of not using HRT was fear of increasing risk of breast cancer. In general, there was lack of doctors' advice for women's using HRT. More than 50% of women would be confident of using HRT if advised by doctors. We conclude that understanding women's thoughts and needs is important for menopause management.
SM-19-03
ASIA-PACIFIC MENOPAUSE FEDERATION (APMF) CONSENSUS STATEMENT ON THE MANAGEMENT OF THE MENOPAUSE
Elizabeth Farrell (Australia)
Abstract not available at the time of going to press.
SM-20: Managing the peri-menopausal women with … (organised by the British Menopause Society)
SM-20-0
MANAGING THE PERI-MENOPAUSAL WOMAN WITH PREMATURE OVARIAN FAILURE
Nick Panay
Queen Charlotte's & Chelsea and Chelsea & Westminster Hospitals, London, Imperial College London UK
Premature ovarian failure (POF) has been estimated to affect about 1% of women younger than 40, 0.1% under 30 and 0.01% of women under the age of 20. However, as the cure rates of cancers in childhood and young women continue to improve, it is likely that the incidence of iatrogenic prematurely menopausal women will rise rapidly.
Management: POF is a difficult diagnosis for women to accept, and a carefully planned and sensitive approach is required when informing the patient of the diagnosis. A dedicated multidisciplinary clinic separate from the routine menopause clinic will provide ample time and the appropriate professionals to meet the needs of these emotionally traumatised patients. At the West London Menopause Centres we have restructured our services and created a dedicated clinic for the POF patients. A database has been developed to collate important information on these patients.
Treatment – General Principles: Specific areas of management include the provision of counselling and emotional support, diet and nutrition supplement advise, hormone replacement therapy, and reproductive health care, including contraception and fertility issues.
Hormone Replacement Therapy: Hormone replacement therapy (HRT) is recommended to control vasomotor symptoms, minimise risks of cardiovascular disease, osteoporosis, and possibly Alzheimers' disease, as well as maintain sexual function. There is no evidence that the results of the Women's Health Initiative study apply to this younger group. HRT in POF patients is simply replacing ovarian hormones that should normally be produced at this age. It is of paramount importance that the patients understand this in view of the recent press on HRT. The aim is to replace hormones as close to physiological levels as possible. Hormone therapy should generally continue at least until the estimated age of natural menopause (on average 51years).
Fertility: Women with POF are not necessarily sterile unless surgically menopausal. There is however only a 5% chance of spontaneous conception. Hence, women for whom fertility is a priority should be counselled to seek assisted conception by IVF using donor oocytes or embryos. Future advances in the technology of in-vitro maturation of eggs derived from stem cells may make it possible for some women with POF to use their own oocytes.
Conclusion: There is an urgent need to precisely quantify the global scale of the problem (ideally through the IMS), to standardised terminology and develop evidence based guidelines from appropriate research, if we are to optimise the management of premature ovarian failure.
SM-20-02
MANAGING THE PERI-MENOPAUSAL WOMAN WITH A FAMILY HISTORY OF CORONARY HEART DISEASE
J. C. Stevenson
National Heart & Lung Institute, Imperial College London, London SW3 6NP, UK
Coronary heart disease (CHD) is the leading cause of death in women as it is in men in Northern Europe and North America. A family history of CHD is important as there are clearly genetic factors involved in the risk for development of CHD. Thus a woman with a family history of CHD occurring below age 70–75 years in close female relatives should be considered to be at increased risk. Consultations regarding menopausal symptoms present an ideal opportunity for risk assessment in such women. A fasting lipid profile to measure total, HDL, LDL cholesterol and triglycerides should be performed to detect any dyslipidaemia. Similarly a fasting glucose should be performed to exclude diabetes, perhaps with an insulin measurement if metabolic syndrome is suspected. An assessment of central obesity is also required, as is measurement of blood pressure. Lifestyle factors are important, with cessation of smoking being essential. Diets low in fat and with sufficient fruit and vegetables should be recommended, as should regular physical exercise. Loss of ovarian function at menopause is a specific risk factor for CHD in women. Thus women with known risk factors for CHD will be at greater risk when they become peri- or postmenopausal, and hormone replacement therapy (HRT) use should be encouraged in such women. The evidence that HRT is beneficial for the prevention of CHD is sound. Observational studies have consistently shown that postmenopausal HRT reduces the incidence of cardiovascular disease by approximately 40%. Women in these studies usually start HRT around the time of their menopause. In agreement with this, the randomised clinical of the Women's Health Initiative showed some evidence of primary prevention of CHD in those women under age 60 years or within 10 years of menopause. Metabolic effects, and hence the cardiovascular effects, of different HRT regimens vary according to the dose and type of estrogen or progestogen used and their route of administration. HRT has major effects on lipids and lipoproteins, on glucose and insulin metabolism, and on body fat distribution. It is thus important to tailor the HRT regimen to correct any underlying metabolic abnormalities. Certain progestogens also have anti-mineralocorticoid effects, and these may be preferred in women with raised blood pressure. HRT started around the time of menopause may have a major preventive effect on CHD. Identifying women at increased risk during this period of life enables prevention strategies, including HRT, to be put in place.
SM-20-03
MANAGING THE PERI-MENOPAUSAL WOMAN WITH DIABETES
Mary Ann Lumsden
Section of Reproductive and Maternal Medicine, University of Glasgow, UK
The incidence of Type 2 diabetes is increasing alongside the rise in obesity and diabetic women with menopausal symptoms are often denied HRT since practitioners are unclear as to the advisability of prescribing it.
The menopause and oestrogen have subtle effects on insulin sensitivity, which is affected by menopausal rather chronological age. Epidemiological studies suggest that women taking HRT are less likely to become diabetic. This maybe related to the beneficial effect of HRT on glycaemic control with reduction in HBA1C levels. The effect of progestogen depends on the type used.
Cardiovascular disease, osteoporosis and cancer are important conditions for diabetics. The incidence of coronary heart disease is greater in diabetics than non-diabetics. Also, women have a higher incidence of cardiovascular disease than age-matched man, for reasons that are still unclear. Recent advice regarding HRT and cardiovascular disease has changed and would suggest that prescription to those of the age of the natural menopause that do not have established cardiovascular disease is not contraindicated.
In regard to cardiovascular risk factors, oral estrogen has a beneficial effect on the lipid profile with the exception of triglyceride levels and it is not thought that diabetes exacerbates hypertension. There is an increase in the incidence of stroke but in women of menopausal age, the actual rate of stroke is extremely low. As with all women, there is a significant increase in the likelihood of having a VTE.
Diabetics are also at risk of osteoporosis. HRT is known to be beneficial in reducing fracture risk although its long term use is no longer recommended
Diabetes is associated with an increase in the risk and breast and endometrial cancer. However, it is unknown if HRT has a greater effect on these individuals than on the non diabetic population. The likelihood of endometrial cancer is significantly increased with unopposed estrogen and also in obese women. The use of intrauterine progestogen is useful to protect the endometrium. It is likely that HRT will have a beneficial effect in regard to colorectal cancer which is increased in those with diabetes but appears to be decreased by administration of CEE and MPA.
Menopausal women who have hot flushing should not be denied HRT. Oral HRT should be avoided in women with hypertriglyceridaemia and appropriate additional treatments for cardiovascular disease prevention should be employed. Any irregular bleeding should be assessed extremely carefully. Both oral and transdermal estradiol can be used and the progestogens with the least impact on metabolism selected.
SM-20-04
MANAGING THE PERI-MENOPAUSAL WOMAN WITH ENDOMETRIAL CANCER
Tim Hillard
Poole Hospital NHS Foundation Trust, Poole, Dorset, UK
Although the incidence of endometrial cancer peaks between 60 and 70 years, around 20–25% occur pre-menopausally. Treatment almost inevitably involves a hysterectomy and bilateral salpingo-oophorectomy, thus rendering the woman menopausal. Women under 45 years tend to have a lower incidence of advanced stage disease, higher degree of tumour differentiation, and better prognosis compared to patients older than 45 years. Although Hormone Replacement Therapy (HRT) is generally contraindicated after endometrial cancer, distressing menopausal symptoms may well be experienced, particularly in the younger age group and HRT in some form is quite frequently prescribed in clinical practice mainly in Stage I or II disease.
The data on the use of HRT after endometrial cancer are limited and are mostly retrospective controlled studies. They have not shown an increased rate of recurrence or mortality either with estrogen alone or in combination with progestogens, indeed some studies found longer disease free intervals and survival times amongst HRT users. One small RCT reported a recurrence rate of around 2% in both ERT and placebo groups over 5 years. Death rates in the two groups were also similar. Progestogen addition is recommended as part of HRT for endometrial protection in non-hysterectomised women. Whilst inherently it would seem appropriate to use combined estrogen and progestogen treatment after endometrial cancer, the data, such as they are, do not indicate any advantage in doing so. With recent high profile publications suggesting that the addition of progestogen may adversely affect cardiovascular disease and breast cancer risk, there is a reasonable argument for the use of estrogen only HRT. Clearly HRT should only be used after careful evaluation of the risks and potential benefits of all the options and should be used at the lowest effective dose.
For many women HRT may not be appropriate or the first choice for symptom control. Progestogens alone may be helpful but may impart other risks. Venlafaxine, Gabapentin and other related drugs may be effective in vasomotor symptom control although long term data are lacking. Various herbal or alternative preparations are used widely, often not under physician guidance. Whilst some may derive symptomatic benefit from these, there are no data on endometrial safety even in the general population let alone with endometrial cancer and they should be used with caution. Osteoporosis and cardiovascular disease risk should be assessed individually and managed as appropriate.
SM-21: Futuras direcciones en el manejo de la mujer en su etapa Posreproductiva (Sociedad Chilena de Climaterio)
SM-21-01
FUTURO EN DISFUNCIÓN SEXUAL
Speaker: René Montaño (Chile)
Abstract not available at the time of going to press.
SM-21-02
SEARCH OF SECONDARY CAUSES OF BONE LOSS IN POSTMENOPAUSAL WOMEN
P. Villaseca, P. Valenzuela, C. Campusano, G. González and E. Arteaga
Facultad de Medicina, Pontificia Universidad Católica de Chile, Santiago de Chile
Objective: To establish the prevalence of secondary causes of bone loss in otherwise healthy women with osteopaenia/osteoporosis in whom there is a high clinical suspicion of secondary bone loss.
Design & Method: A cross-sectional chart review study was done in all consecutive female patients who presented to our outpatient clinic of Gynecological Endocrinology between 2004 and 2007, and had the diagnosis of osteopaenia or osteoporosis made by densitometry, and met the following criteria of secondary bone loss: Z score ≤ –2.0 SD, osteoporosis and/or osteopaenia predominant in hips relative to lumbar spine (Δ ≥ 1.0 SD), and/or failure of antiresortive treatment (≥2% per year). Each medical history was reviewed; all women had normal CBC, and normal hepatic and renal function. Laboratory testing analyzed included serum calcium and phosphorus, 24-h urinary calcium, TSH, PTH, and 25(OH)vitamin D. In patients with clinical history suggesting malabsorption, antiendomysial antibodies were measured. Hypovitaminosis D was defined as 25(OH)vitamin D ≤ 20 ng/ml.
Results: We evaluated 72 patients between 44 and 78 years of age and 1 to 22 years since menopause. Our findings were: hypovitaminosis D (n = 27); hypercalciuria (n = 21); 16 patients had secondary hyperparathyroidism: one due to celiac sprue, three due to hypercalciuria, seven due to hypovitaminosis D, one due to hypovitaminosis D and hypercalciuria, one due to hypercalciuria and exogenous hyperthyroidism and the three others unexplained. Four patients had dual unrelated disorders (hypovitaminosis D and hypercalciuria in three patients; hypovitaminosis D and exogenous hyperthyroidism in one). In 20 women we found no cause for bone loss.
Conclusion: In 72% of the 72 women in whom secondary causes of bone loss were suspected as stated above, we identified previously undiagnosed metabolic or endocrine disorders which can be corrected, and thus optimize osteoporosis treatment. Hypovitaminosis D and other causes for secondary hyperparathyroidism were the most frequent diagnoses.
SM-21-03
FUTURO EN OSTEOPENIA Y OSTEOPOROSIS
Speaker: Sergio Brantes (Chile)
Abstract not available at the time of going to press.
SM-21-04
THE FUTURE OF LOW-DOSE ESTROGEN THERAPY
Jorge Varela Méndez1 and Luis Cuitiño Gaete2
1University of Concepción School of Medicine, Chile; 2University of San Sebastian School of Medicine, Concepción, Chile
The use of estrogen therapy (ET) began soon after 1900. The first experiences were done with isolated ovarian extract with a positive impact on menopausal symptoms. By 1928 inyectable estrogen was commercially available. In 1942 appeared the first orally estrogen, Premarin by Ayesrt Laboratories.
After 1940 a great series of reports on the use of ET can be found in the literature. In the seventies researchers reported the association between prescribed estrogen without progestine opposition and endometrial cancer. Since this observation it was mandatory the use of estrogen with a progestine in women with an intact uterus.
The WHI study in July 2002 led to a rapid change in clinical practice patterns. Since this publication, the assumed cardiovascular protection of ET become controversial (RR 1.29). It was also confirmed a small increase in the incidence of breast cancer (RR 1.26) and a strong increment in stroke (RR.1.44) and deep venous thrombosis.
Since de 80¨s decade, many investigators published recommendations on the use low doses of ET, but even more reports came into the literature after de WHI Study. Some works like the HOPE, and more recently the CHOICE trials, clearly demonstrated the beneficial effects of low-dose ET as compared with regular doses, with several low-dose estrogen and progesterone combinations mimicking what was already known with low-dose oral contraceptives: favorable outcomes with less undesirable effects.
In a recent study of the Nurses Health Study it was shown a reduction of cardiovascular risk with low-dose (0.3 mg/day) conjugated estrogens (CE) (RR 0.74 95% CI 0.52–1.06). The same trial demonstrated a decrease in the risk of stroke with CE 0.3 mg/day, as compared with the regular 0.625 mg/day dose (RR 1.35; (95% CI,1.28–2.26 versus RR 0.54, (95%,CI, 0.28–1.06).
Several observational studies have evaluated the impact of low doses on venous tromboembolism. Jick et al. observed in a case control study, a clear dose-response effect.: CE 0.325 mgr/day (RR 2.1; 95% CI, 0.4–11.1). CE 0.625 mgr/day (RR 3.3; 95% CI 1.4–7.8). CE 1.25 mgr/day (RR 6.9; 95% CI 1.3–33 ).
In a randomized double blind, placebo-controlled study carried out by Borgfeldt et al. they concluded that low doses of E2 (1mgr) in combination with Neta 0.25 mgr or 0.5 mgr resulted in favorable changes of factor VII activity and fibrinogen, compared with placebo. The lower plasma levels of PAI–1 may lead to increased fibrinolytic activity. Also the antithrombin activity was reduced. These findings suggest a decreased risk of developing venous thromboembolism. These facts remains to be clarified.
Favorable outcomes with low-dose ET have been observed with respect to endometrial hyperplasia, mammary density and protection against osteoporosis. With transdermal ET, as low as 14.5 micrograms/day have shown positive changes in markers of cardiovascular risks.
The future of low-dose ET is promising and this form of therapy will become more widely used as we will aware of more reports about this topic in the near future.
SM-22: The French position statement on HT part I (organised by the French Menopause Society)
SM-22-01
WHY A FRENCH POSITION STATEMENT, DOES A FRENCH PARADOX EXIST?
Henri Rozenbaum
President of the French Menopause Society (AFEM)
Treatment of menopausal women by menopausal hormone therapy (HT) has been widely contested in the last 6 years. Publication of the results of several interventional and observational studies involving thousands of women, which have shown an overall harmful effect of HT has led to reconsideration of the indications of this treatment.
It is in this context that the AFEM new position statement on hormonal treatment is published. In particular, this position statement takes into account the publication since 2002, date of the Women's Health Initiative (WHI), of a number of data that are considered relevant in determining the role of HT in postmenopausal women:
Examination of subgroup analyses of the WHI has demonstrated different effects of HT according to timing of initiation of HT relative to the proximity of menopause and the age of the patients.
Publication of the findings from the WHI estrogen therapy (ET) arm (in hysterectomized women) has reported markedly different and more optimistic results than those initially published in women treated with combined estrogen-progestin therapy (EPT) (i.e. conjugated equine estrogens + medroxyprogesterone acetate).
the publication of two French observational studies have emphasized the differences in health outcomes that were associated with various hormones regimens according to specific ET/EPT compouds and routes of administration.
HT is the only treatment which may compensate for all effects resulting from estrogen deficiency. In the absence of its usual contraindications, HT is indicated in the early postmenopausal period:
for the woman who desires such treatment, provided that she has received a clear information on the potential benefits and risks of HT;
for symptomatic women;
for postmenopausal women who are at high risk of osteoporotic fracture.
This treatment is not indicated in asymptomatic older women. In women with climacteric symptoms, HT may be proposed after weighting the benefit/risk ratio.
HT should be prescribed at the lowest effective dose for treatment goals that are either correction of climacteric syndrome and/or prevention of post-menopausal bone loss.
Treatment is warranted for as long as climacteric symptoms persist. Beyond 5 years of treatment and/or in women aged over 60 years, the decision to continue HT should be individualized on the basis of both symptoms persistence and current risk/benefit ratio. A therapeutic window can be thus proposed to assess the recurrence of symptoms after tapering the dose of HT. If HT is stopped the risk of osteoporotic fracture should be evaluated.
SM-22-02
IMPACT OF STEROIDS ON BLOOD VESSELS: ROLE OF MOLECULAR STRUCTURE AND WAY OF ADMINISTRATION
Christian Jamin
169 bd Haussmann F75008 Paris ([email protected])
Vascular risk can be divided into 4 parts: venous thromboembolim, strokes, coronary heart disease, and peripheral arterial disease.
Today, venous thromboembolisms during hormone replacement therapy (HRT) are attributed to its estrogenic component. A strong concentration of estrogens in liver, either because of their structure (artificial estrogens) or of their concentration (pregnancy or oral intake) induces thrombogenic coagulation protein anomalies. Non oral intake of estradiol does not induce coagulation activation and does not increase venous thromboembolim.
It seems that peripheral arterial diseases are not or little modified by HRT.
Coronary heart disease implies different actors such as atheroma, vasomotoricity, inflammation, destabilization of plaque, thrombosis (and its extensive nature), insulin-sensitivity, arterial tension, and many other factors, genetic for instance.
Atherosclerosis: Endogens estrogens (as well as those not orally taken) protect from atherogenesis. Estrogens taken the oral way have less pure metabolic effects, but when given in immediate post menopause they oppose the formation of coronary atheroma. On the contrary, when MPA is associated, estrogens lose part of their beneficial effects on atherogenesis. They seem not to lose their beneficial effects when associated with progesterone. However, when plaque is already constituted, HRT does not slow down plaque progression.
Vasodilation: Estrogens induce an endothelium dependant vasodilatation even if endothelium is injured: this effect is not linked to the molecule structure or to its administration way. When MPA is given at the same time, the vasodilator effect of estradiol disappears, whereas it persists when progesterone is associated with estrogens.
Plaque rupture, thrombosis and its extension.
The association oral estrogens + MPA have been accused to promote plaque rupture. Estrogens taken the oral way increase MMP production and lower its inhibitor TIMP. This effect does not exist when estradiol is given by cutaneous way.
Progestins favour arterial thrombosis. Insulin resistance could have a negative effect in fibrinolytic anomalies. Artificial progestins alter insulin sensitivity, which is not the case of progesterone.
Inflammation: Inflammation plays a part as early as atherogenesis origin and also plays a part in the thrombotic phenomenon. Ultra sensitive CRP is increased by oral estrogenotherapy and not modified when given by cutaneous way.
Blood pressure: Oral estrogens increase angiotensinogène which is not the case of cutaneous administration. Progesterone has a tendency, because of a slight anti mineralocorticoïd activity, to slightly lower arterial tension.
Estrogenotherapy prevents coronary heart disease plaques from appearing as long as it is started soon after menopause. When atheroma exists, negative effects of oral estrogens and of artificial progestins are liable to set off an arterial accident.
SM-22-03
DOSE AND DURATION OF HT
David Elia
2 rue de Phalsbourg 75017, Paris-France ([email protected])
After the summer 2002 WHI publication, AFSSAPS- the French health authorities-recommended in January 2003 that “hormonal therapy must be prescribed for the shortest possible duration with the lowest possible dose and only for managing menopausal symptoms”.
HT dose: Low-dose estrogen treatment refers to half the standard recommended dosage of estrogen, i.e.: the following daily doses of 17 beta estradiol: 1 mg for the oral route, 0.75 mg for percutaneous gels and 0.025 mg for transdermal delivery systems or patches.
The side effects of higher estrogen doses are one of the main reasons for poor compliance, leading patients to abandon their treatment and thus limiting the potential benefits of HT. In order to improve compliance, HT must be personalized and adapted to each individual patient. In the search for personalized treatments, low-dose estrogens play an important role amongst the choices available as they are both effective on vasomotor symptoms and offer an improved clinical tolerance compared to higher dose regimes. Several studies have also shown low-dose estrogens to be beneficial in the prevention of bone loss.
The indications for low-dose estrogens are multiple:
initiation of HT (to judge tolerance and effectiveness).
initiation of HT at an early stage, towards the end of the perimenopause.
HRT initiated or maintained at a late stage of menopause.
in case of intolerance to standard estrogen doses.
in the absence of known long term risk factors, in particular osteoporosis.
in case of estrogen-sensitive gynecological pathology: fibroids, endometriosis, fibro-cystic breast disease, radiologically dense breasts.
HT duration: The French health authorities- recommend that “hormonal therapy duration must be he shortest possible and only for managing menopausal symptoms”.
But, what is the duration of menopause symptoms?
Menopause symptoms are very well known: hot flashes and sweats, vaginal dryness, myalgia and arthralgia, insomnia, depression, eyes dryness, loss of libido, cognitive functions decline.
Few publications are available on this subject since most of them only explore hormonal therapy efficacy on these symptoms.
After the WHI it was often said that the duration of symptoms was not longer than 5 years.
We will review the spontaneous duration of each symptom.
We will confirm indeed that, for example, hot flashes are still present for 20% to 40% of women 10 yeas after menopause. Same, dryness vaginal and arthralgia are very usual symptoms able to impact negatively on quality of life. That is why HT can be useful for a very long time after menopause.
SM-22-04
MIDLIFE CRISIS AND QUALITY OF LIFE
M. Lachowsky
Gynaecologist, consultant for psychosomatic Ob/Gyn, Bichat University Hospital, Paris, France
Definitions: Quality of life is neither a new nor an old concept. Is it simply the way our patients demand it nowadays which is new, or rather different, or maybe simply that we doctors consider it at all. We have always been concerned by our patient's health, but has it something to do with their day-to-day life, and not only as opposed to sickness or death? Our society has little tolerance for age and aging, even less so where women are concerned. Around 50, particular problems may arise, in both man and woman's life what with partner, children, parents, as well as professional and social changes and what about menopause? We wish to underline the necessity and the limits of the gynecologist's role while trying to understand why the menopause, a now well-known feminine milestone marking the time and the way to another period of life, still remains difficult to live through, a bend to negotiate, each woman at her own pace, with her own means, with the cards life has already dealt her.
We do have means to assuage the well-known symptoms affecting body and mood, helping all appetites to revive. But it is essential to take time over those prescriptions, time to explain and reassure, and also to give time to the woman to speak about herself, her present environment, her views about her future, her acceptance and her coping with that normal, biological event. What part has the gynecologist to play in his/her patients lives, what has he to be aware of, and to what extent?
Conclusions: We must sometimes be less discrete, and ask some of those questions women may have trouble voicing aloud. Shame or fear of ridicule are still often part of their representations. Preventing an honest answer, they often modify the learned statistics dealing in fiftyish women. Our respect, our full attention are already therapeutic, showing them there is no age-limit and that we deem their problems as worthy of our medical interest as any somatic complaint.
SM-23: Tissue specific effect of endogenous and exogenous hormones (organised by the German Menopause Society)
SM-23-01
HORMONAL EFFECTS ON THE BONE
Peyman Hadji (Germany)
Abstract not available at the time of going to press.
SM-23-02
EFFECTS OF ENDOGENOUS AND EXOGENOUS HORMONES ON THE CARDIOVASCULAR SYSTEM
Alfred O. Mueck
University Women's Hospital of Tuebingen, Germany
Research on menopause-induced changes in metabolic patterns (lipids, carbohydrates) and cardiovascular functions has been able to demonstrate the importance of endogenous hormones, especially estradiol (E2), on the cardiovascular system. In correlation with those changes also the strong increase of coronary heart disease in women after menopause, particularly after surgical menopause, can only be explained by cardioprotective effects of estradiol although other factors also play a certain role. Likewise the fact that HRT starting in or soon after menopause differs in benefits and risks largely from effects as observed in older women (like in the WHI-trial) is suggestive for different mechanisms.
Cardiovascular target organs express estrogen receptor(ER)-alpha as well as ER–beta, however, the specific role of each receptor in the cardiovascular system remains to be established. E2 can activate both cytosolic protein-bound estrogen receptors that in the nucleus activates gene transcription whereby several cofactors are required. For vascular effects membrane-associated ER are important to stimulate various kinases (SRC, PI3K, GSK3β etc), which leads to activation of NOS and subsequent production of NO. ER-alpha also interacts with MAPK pathway. As shown in own experimental studies E2 can also modulate endothelium-independent calcium influx, and in addition E2 also can exert effects via other ER-independent mechanisms. We also were able to demonstrate that certain E2-metabolites elicit cardiovascular activity, even at very low concentrations.
The main mechanism of a possible cardioprotection by endogenous as well as exogenous estrogens appears to be a direct effect on the vasculature resulting in an improvement of endothelial function and inhibition of atherogenesis. Main cardiovascular risks are venous and arterial thromboembolism, dependent on the age of the women, on dosage and on the application form of HRT, e.g. regarding estrogenic proinflammatory effects. The main difference between oral and transdermal administration may be confined to predictive markers which are mainly or exclusively produced in the liver. Experimental and clinical studies demonstrated that type, dosage and route of progestogen addition can have a negative impact on the beneficial estrogen-induced cardiovascular changes, the most important challenge for the choice of individualized, differentiated HRT, i.e. exogenous hormonal action.
SM-23-03
REGULATION OF ANGIOGENESIS
L. Kiesel, P. Wülfing, M. Smollich, M. Götte and M. P. Stute
Dept. of Gynecology and Obstetrics, University Hospital of Münster, Germany
Endogenous and exogenous sex steroids play a role in the tumorigenesis of malignancies (breast, endometrium). A crucial step for conversion of a tumor from a benign to malignant state is the process of developing a high-density vessel network termed the “angiogenic switch”. This step has been considered an initial and rate-limiting step in malignant conversion. Angiogenesis, the formation of new capillaries, is regulated by various angiogenic and anti-angiogenic factors. Recently, endothelin–1 (ET–1) has been shown to be an important regulator of angiogenesis. This peptide is produced primarily in the endothelial, vascular, smooth muscle and epithelial cells. ET-1 effects are mediated through its two G-protein coupled receptors, endothelial receptor A (ETAR) and B (ETBR), which are expressed in several issues including breast, prostate, ovary, lung and colon. The complex of endothelin and its receptors is referred to as the “ET-axis”. Activation of ETAR promotes various effects important for tumorigenesis and tumor progression, as are proliferation, invasion, angiogenesis and inhibition of apoptosis. In contrast, there is less evidence for ETBR dependend tumor-related functions. In breast cancer predominantly ET-1 via ETAR seems to influence tumour development to progression. Expression of ETAR is associated with clinicopathological parameters characterizing more aggressive types of breast cancer and indicating a poor outcome.
Estrogen receptors up-regulation has been demonstrated to activate angiogenic factors via hormone responsive genes. The presence or absence of estrogen receptors is correlated with the regulation of angiogenesis in the breast and endometrium. Exogenous steroid hormones as well as the production of endogenous sex steroids are potential regulators of benign and malignant tissues in women.
The role of sex steroids in angiogenesis may be of relevance not only in treatment of malignancies but in prevention of certain benign and malignant conditions in the female.
SM-24: Progestogens and the climacteric female (organised by the European Progestin Club)
SM-24-01
PROGESTOGENS IN HRT: SUFFERANCE OR DESIRE?
S. O. Skouby1,2 and J. Jespersen2
1Department of Obstetrics and Gynecology, Herlev Hospital, Faculty of Medical Science, University of Copenhagen, Denmark; 2Department for Thrombosis Research, Institute of Public Health, University of Southern Denmark
Since the publication of the Women's Health Initiative (WHI) study followed by results from the Million Women Study (MWS), the role of hormonal therapy (HRT) in postmenopausal women has been challenged. The risks attributed to hormone therapy from these studies have, however, been overestimated because the epidemiological data have been translated into a general clinical setting for all menopausal women regardless of their age, BMI and co-existing medical conditions. For most gynecologists postmenopausal HRT still occupies a clear clinical position to in order to attenuate degenerative body changes along with prevention of vasomotor symptoms. Despite this, long-term HRT is under continued critical evaluation and a more individualized treatment approach established. Related to this re-evaluation is also a revisory view on the progestogen component. While the benefits of progestogens in HRT are well recognized as far as endometrial protection is concerned the data on breast tissue and the cardiovascular system are contentious. Following the WHI and MWS the question may be raised: When considering optimal HRT is progestogen here on sufferance or is it desired? To answer this, it should be emphasized that the epidemiological data have not only been wrongly extrapolated in relation to the clinical settings, but also to the whole class of therapies. The various progestogens available for HRT exert different partial effects at cellular level according to their biochemical composition. Some have particular antimineralocorticoid effect and some more pronounced antiandrogenic activity while others are close to natural progesterone in clinical effects. Progestogens exert a dual effect on the breast cell. First stimulation in the G-1 phase depending on the type and initiated by estrogen and then followed by apoptosis. Due to the structural differences the progestogens also result in a variety of metabolic and hemostatic changes. Moreover, not only the steroidal formula, but also dose and route of administration translate into differential effects on vascular function when combined with estrogen. Since no single test or algorithm presently can detect the vascular impact the least change or no change may often be desirable. Targeting the lowest possible dose of the progestin to be delivered directly to the uterus is another possibility to avoid unwanted systemic effects. As an exampel we have shown that estradiol combined with intrauterine levonorgestrel can lower LDL oxidation in vivo. Several other delivery systems are either available or in development enabling a sustained desire for an estrogen/progestin combination as optimal future HRT strategy.
SM-24-02
PROGESTOGENS IN THE MENOPAUSE IN HEALTHLY WOMEN AND BREAST CANCER PATIENTS
J. R. Pasqualini
Hormones and Cancer Research Unit, Paris, France
The capital role of progesterone in the development of the normal breast, as well as in the menstrual cycle, pregnancy and lactation, is well documented. The biological response is generally in combination with estrogens. In the breast the principal role of progesterone is promoting lobuloalveolar development and differentiation. At present, more than 200 progestin compounds are synthetized, but their biological effects are different: this is function of their structure, receptor affinity, metabolic transformations, target tissues considered, dose. The action of progestins in breast cancer is controversial; some studies indicated an increase in breast cancer incidence, others showed no differences and yet others a decrease. Many studies agreed that treatment with progestins plus estrogens at low dose and during a limited period (>5 years) can have beneficial effects in peri- and post-menopausal women. It was demonstrated that various progestins (e.g.: nomegestrol acetate, medrogestone, promegestone), as well as tibolone and its metabolites, can block the enzymes involved in estradiol bioformation (sulfatase, 17β-hydroxysteroid dehydrogenase) in breast cancer cells, or in total breast tissue. In various organs progesterone is largely metabolized and these metabolic transformations are important not only in blocking the biological effect of the hormone, but also because the metabolic products can play a major role in its biological responses.
In a series of studies carried out with breast tissues it was demonstrated that progesterone is converted into various metabolic products: in normal breast tissue the transformation is mainly to 4-ene derivatives, whereas in the tumor tissue, 5α-pregane derivatives are predominant. Aromatase activity is the last step in the formation of estrogens by the conversion of androgens. At present anti-aromatases are largely used as first line treatment for breast cancer. The activity of this enzyme is very low in breast cancer tissue; however, a stable cell line, the MCF-aro, with high aromatase activity was obtained by transection with the aromatase gene. In recent studies it was shown that 20α-dihydroprogesterone, a metabolite found mainly in normal breast tissue and with anti-proliferative properties, can act as an anti-aromatase agent. The data suggested the possible utilization of this compound in breast cancer prevention. In conclusion, in order to clarify and better understand the response of progestins in breast cancer (incidence and mortality), as well as in hormone replacement therapy or in endocrine dysfunction, new clinical trials are necessary, using other progestins, in function of the dose and period of treatment.
SM-24-03
PROGESTOGEN DEFICIENCY AND ENDOMETRIAL CANCER RISK
Adolf E. Schindler
Institute for Medical Research and Education, Essen-Germany
There is a close relationship between the amount of estogen and progesterone secreted by the ovary from puberty to menopause and the development of hyperplastic endometrium of all types and finally endometrial cancer. The endogenous endocrine pattern reflects progesterone deficiency (corpus luteum deficiency). Such deficiency can also develope when treatment with exogenous estrogen and progestogen is done and a deficiency of the progestogen in comparison to the used estrogen is induced in pre- and postmenopausal women. This risk is particular accentuated in the climacteric female when the endocrine milieu was unfavorable in the years before (menstrual cycle disorders, PCOS, obesity, no full-term pregnancy, no breast feeding etc).
However, there are the additional factors that modify the biological end result: “Progestogen deficiency”. One main factor is the level of SHBG determined by the amount of free, biologically active estradiol. A low level of SHBG is for instance induced by high body weight. Therefore, the amount of overweight correlates with increased endometrial hyperplasia and finally endometrial cancer. In addition, increasing body weight negatively affects proper ovarian function leading to corpus luteum deficiency and this in addition increases the risk of endometrial cancer. The classical risk increase for endometrial cancer is associated with oligomenorrhea or polymenorrhea combined with corpus luteum deficiency or anovulation. Therefore, women with PCOS are at increased risk for endometrial cancer in the pre- and postmenopausal years. Examples from the therapeutic point of view have been the risk increase found with biphasic estrogen high-dosed oral contraceptives with a long estrogen phase and a short progestogen phase. In climacteric females estrogen-only treatment results in a predictable increase in endometrial cancer risk. Therfore, it is mandatory to use estrogen/progestogen combinations. The lowest risk is achieved when a continuous estrogen/ progestogen regimen is recommended. In addition, the lowest dose of estrogens for the particular woman should be chosen.
SM-25: Premature ovarian “failure” is different from menopause (organised by the American Society for Reproductive Medicine)
SM-25-01
MECHANISMS OF PREMATURE OVARIAN “FAILURE”
L. M. Nelson
National Institutes of Health, Bethesda, Maryland, USA
The term “premature ovarian failure” is problematic. It implies the permanent cessation of ovarian function. In fact, many women with this condition experience intermittent ovarian function that may last for decades after the diagnosis. Pregnancy may occur in some women many years after the diagnosis. Our preferred term for the condition is “primary ovarian insufficiency” (POI) as first introduced by Fuller Albright in 1942. In 90% of cases the mechanism for the primary ovarian insufficiency remains a mystery despite a thorough evaluation. Approximately 2% of cases are due to an abnormal karyotype involving the X chromosome. Approximately 4% are due to autoimmune oophoritis, which can be identified by testing for serum anti-adrenal antibodies. In about 6% of cases the condition is related to a premutation in the in the FMR1 (Fragile X Mental Retardation 1) gene. Complex manifestations that cut across medical specialties may result from expansion of CGG trinucleotide repeats. The major objectives of this presentation with regard to FMR1 are to review the complex genotypic-phenotypic correlations related to this gene, the spectrum of altered ovarian function that can be seen in women who carry the FMR1 premutation, and issues related to genetic testing. Fragile X syndrome, the most common cause of familial mental retardation, is due to a full mutation (>200 CGG repeats) in the FMR1 gene. Initially individuals who carried the premutation (defined as more than 55 but less than 200 CGG repeats) were not considered at risk for any clinical disorders. It is now clear that in reality the premutation is associated with a spectrum of more subtle altered ovarian function. This includes women who have elevated FSH levels despite the presence of regular menstrual cycles and women who respond poorly to gonadotropin stimulation related to attempts at preimplantation genetic diagnosis. Women with premature ovarian “failure” are at increased risk of having an FMR1 premutation and should be informed of the availability of fragile X testing. Pregnancy can occur subsequent to the diagnosis of premature ovarian “failure” and can result in the birth of a child with fragile X syndrome. Testing should also be considered in women with infertility and elevated basal FSH levels and those who have a low response to gonadotropin stimulation. FMR1 testing should be undertaken only after the patient is informed that test results may reveal significant health care issues beyond that involving the reproductive system.
SM-25-02
MANAGEMENT OF PREMATURE OVARIAN “FAILURE”
Robert W. Rebar
American Society for Reproductive Medicine and Department of Obstetrics and Gynecology, University of Alabama, Birmingham, USA
Management of premature ovarian “failure” (POF) is far different from the management of menopause. Approximately 25% of women with POF ovulate and 5–10% conceive following establishment of the diagnosis. Thus, it is important to emphasize that the “failure” may not permanent, even if the likelihood of pregnancy is small. Management begins with careful counseling and an explanation of the disorder; psychological support is often required. Hormone replacement therapy with an estrogen and a progestogen is warranted, and no regimen has been documented to be more appropriate than any other. Still it seems most reasonable to administer estrogen continuously and add a periodic progestogen for at least 12 days at intervals of one to two months to reduce the risk of endometrial hyperplasia. Affected women may require twice as much estrogen as do postmenopausal women to eliminate or reduce significantly signs and symptoms of estrogen deficiency. Despite administration of estrogen and progestogen, even in the form of oral contraceptives, ovulation and pregnancy may occur. Thus, additional counseling, recommending the use of barrier contraception or even an intrauterine device, is indicated for sexually active women who do not desire pregnancy. It is not clear if all women with POF benefit from addition of exogenous androgen, but circulating androgen levels are quite low in affected individuals. Some young women with POF clearly complain of reduced libido. It is reasonable to recommend calcium 1200–1500 mg/day, vitamin D 400 IU/day, and daily weight bearing exercise because so many affected women have low bone density compared to age-matched controls. Affected women also should be tested for associated autoimmune disease, including thyroiditis and Addison disease, at intervals. For those women desiring children, it is clear that the use of donor oocytes is most likely to result in pregnancy; in some series over 70% of women have taken home children following use of donor oocytes. However, donor oocytes should be used with caution in women with gonadal dysgenesis (who have accelerated loss of oocytes) because of the markedly increased risk of development and rupture of aortic aneurysms during pregnancy; a strong case for adoption can be made in such women. In short, appropriate management of POF requires a caring and concerned health care provider willing to individualize treatment based on the needs of each patient.
SM-26: Simposio Colombiano Demografía y Salud en Menopausia (Asociación Colombiana de Menopausia)
SM-26-01
EPIDEMIOLOGY OF MENOPAUSE IN COLOMBIA
W. Onatra
National University of Colombia, University of Applied Sciences and Environmental, Bogotá, Colombia
The people expected worldwide for the year 2000 was 6,056,714,600 inhabitants to Latin America of 518,808,800 for Colombia around 41,468,384 of which 50.9% are female and older than 50 years are estimated at 6,018,785. 71.8% corresponds to urban area mean while 28.2% is for rural area. Life expectancy for Colombia was 69 years for men and 75.3 years for women. It is known that the mortality rate due to cardiovascular disease (CVD) and stroke increases after menopause (44%) and the breast and cervix cancer to occupy the first place. In Colombia the mortality by CDV is similar to the mortality rate in industrialized countries, cardiovascular disease in men is 27.4%, in women is 39.2% and breast and cervix tumours is 21.7%. Age of menopause in different studies showed that varied in the different cities with an average of 48.8 years. This variation is related to Latin American racial factors, height above sea level, socioeconomic status, education level with a significant difference (p < 0.001). Climateric symptoms were evaluated initially with the modified Kuperman scale in a multicenter study (n = 880) showing that the hot flashes occur in 56.1%, sweating 52.2%, headache 50.4%, vaginal dryness 44.0%, insomnia 40.3%, decreased libido 25.6%. In another comparative study with African descent (n = 377) the Green scale showed significant differences in somatic and psychological symptoms but not in the urogenital. In connection with insomnia it was shown that postmenopausal women lose the circadian rhythm of Prolactin. In a multicenter study about Latin American Metabolic Syndrome (SM) was found that the prevalence was 46.3% to 32.6 Bogota, 32.6% Cali, 33.1% in Medellin. Studies on the prevalence of osteoporosis in Bogota (n = 206) and Medellin (n = 363) show that Bone Mineral Density (BMD) is normally 27.3%, osteopenia 50% and osteoporosis 22.3%. By correlating levels of Vitamin D osteopenia women present lower levels (p < 0.05) than the controls. Different studies with hormone replacement therapy by oral or transdermal have shown benefit in the lipid profile and BMD There is another unknown Colombia, the Colombian indigenous, displaced, African descendants, mothers and grandmothers head of the family that we need to study in order to build a better country.
SM-26-02
METABOLIC SYNDROME IN COLOMBIA: DIAGNOSIS AND TREATMENT
Gustavo Gómez Tabares
Universidad del Valle; Cali-Colombia
Metabolic syndrome (METS) is defined as a group of risk factors predisposing subjects to develop diabetes mellitus and cardiovascular disease. The recent National Cholesterol Education Programme Adult Treatment Panel III (NCEP ATP III) guidelines provide a useful basis for the characterization of this condition. Based on those requirements, the diagnosis of METS is common, with 23.7% being the age-adjusted prevalence of this condition among the adult population in the USA.
Recent publication of metabolic syndrome in Latin America include data from two cities of Colombia: Bogotá and Cali
A total of 3965 postmenopausal women, aged 45–64 years, seeking health care at 12 gynecological centers in major Latin American cities was included in this cross-sectional study. The US National Cholesterol Education Programme Adult Treatment Panel III (NCEP ATP III) guidelines were applied to assess METS. This was present if three or more of the following conditions were present: waist circumference 88 cm; blood pressure 130/85 mmHg; fasting plasma triglycerides 150 mg/dl; high density lipoprotein (HDL) cholesterol550 mg/dl; glucose 110 mg/dl or subjects were receiving treatment for their condition.
Gomez et al. in Cali Colombia found in 300 postmenopausal patients aged between 40–70 years (average 53.8 years), 92/300 must be categorized as with a prevalence of 31% of METS.
More frequents combination of parameters of METS founded included: waist >88 cm, HDL <50 mg/dl, TG ≥ 150 mg/dl y waist >88 cm, HDL <50 mg/dl, TA ≥ 130/85 mmHg.
Onatra et al. in Bogotá Colombia in postmenopausal women aged between 45 y 64 years found a prevalence of 35.5% of METS and the best markers were waist and obesity. Loose weight and changes in life style had the best results.
The Colombian Association of Endocrinology in conjunction with nine other scientific societies made in 2006 a consensus about METS in Bogotá Colombia:
The parameter for diagnosis of METS included a waist circumference of 80 cm instead of 88 cm in the classic definition
The consensus determine primary prevention measures as ingestion of vegetables, fruits, diminishing animal fat, salt and sugar and share food in family, and physical exercise and reduce stress.
In secondary prevention treat overweight, obesity, sedentary and atherogenic diet.
Consensus finally recommends physical exercise, changes in life style and pharmacologic treatment if necessary.
SM-27: Postmenopausal therapy across midlife (organised by the Hellenic Society for the Study of Climacterium and Menopause)
SM-27-01
INDICATIONS FOR HORMONE THERAPY
N. Goumalatsos (Greece)
Abstract not available at the time of going to press.
SM-27-02
THE USE OF ANTIRESPORPTIVE AGENTS FOR PREVENTION AND TREATMENT OF OSTEOPOROSIS
Irene Lambrinoudaki
University of Athens, Athens, Greece.
The main pathogenetic mechanism in postmenopausal osteoporosis is the increase in bone resorption due to estrogen deficiency. Antiresorptive agents, therefore, are the mainstay of treatment in postmenopausal osteoporosis. Young postmenopausal women with climacteric symptomatology may receive hormone therapy for the first 4–5 postmenopausal years. The SERM raloxifene is a good option for asymptomatic women with osteopenia or osteoporosis. Raloxifene is effective in reducing vertebral fracture risk and in increasing bone mineral density in the lumbar spine and the hip. Raloxifene, furthermore, reduces the risk for primary ER-postitive breast cancer, so it is specifically indicated in high risk women for breast cancer. Bisphosphonates are potent antiresorptive agents which may be reserved for older women with more advanced bone disease, or for women who do not respond to ER-mediated treatment regimens.
SM-27-03
SERMS: AN INNOVATIVE OPTION FOR DECREASING BREAST CANCER RISK IN POSTMENOPAUSAL WOMEN
George Christodoulakos
University of Athens, Athens, Greece
Breast cancer is predominant among gynecological cancer. The incidence of breast cancer increases with age and although the rate of increase decreases after menopause, 75% of the cases are diagnosed after the age of fifty. The risk is defined by hormonal and life-style factors as well as by the personal and family history. The WHI trial reported an increase in the risk of breast cancer after 5.2 years of EPT administration. As a result alternative therapies are needed for the asymptomatic osteopenic or osteoporotic postmenopausal woman.
Raloxifene is a selective ER modulator which prevents bone loss and maintains bone quality. Furthermore, raloxifene even after prolonged administration does not stimulate the endometrium and the breast. Raloxifene has a minimal effect on breast density and in vitro studies have reported no increase in breast cancer cell proliferation. The clinical trials MORE and CORE have reported a 66% decrease in the incidence of invasive breast cancer while the STAR trial has demonstrated raloxifene to decrease the risk by 50% among high risk postmenopausal women and to have an equal efficacy with tamoxifene. However, in contrast to tamoxifene, raloxifene had a 36% and 29% fewer events of endometrial cancer and thromboembolic events respectively.
SM-27-04
THE ROLE OF ANABOLIC THERAPY IN THE TREATMENT OF POSTMENOPAUSAL OSTEOPOROSIS
Nikos Tsakalakos
Endocrinologist
The treatment of the patients with osteoporosis has progressed dramatically in the last decade. The basis for the drug intervention has been the suppression of bone remodelling, in order to stop the bone loss associated with the disease. Antiresorptive drugs are targeted to this goal since they inhibit the activity of the osteoclast and reverse the high turnover state associated to accelerated bone loss and fracture risk.
After several years of solely having antiresorptive drugs in our armamentarium, a new class of drugs is available with the approval of the bone-forming agent teriparatide. This drug is the recombinant 1–34 fragment of the human parathyroid hormone and induces a rapid formation of bone with dramatic increases in bone volume. New fresh bone is rapidly formed in response to the therapy, with positive balance.
Besides the increases in bone mass, better measurements using 3-D densitometry methods, show that teriparatide improves the microarchitecture by increasing the number and connectivity of the trabeculae as well as the cortical thickness. The result is a strong decrease in the risk of vertebral, non-vertebral fractures and back pain that persists even after stopping the treatment.
SM-28: Temas polémicos en la mitad de la vida (Federación Latinoamericana de Sociedades de Climaterio y Menopausia)
SM-28-01
CONTRACEPTION ADVICE IN THE LATE REPRODUCTIVE YEARS. WHEN TO SWITCH FROM HORMONAL CONTRACEPTION TO HRT
Nestor Siseles
University of Buenos Aires, Argentina
Although it is well known that fertility declines with advancing age, spontaneous conceptions do occur even in the face of elevated gonadotropins. In fact, unintended pregnancies are the major problem in sexually active perimenopausal women, where the use of therapeutic abortion is as high as that found in teen-age women.
When pregnancy occurs in women of advanced reproductive age, the obstetric risks (gestational diabetes, hypertension, spontaneous abortions, Down syndrome) are increased. Thus, effective contraception is vital during this period to minimize anxieties over an unwanted pregnancy.
The methods of contraception in this age group do not differ from those available to younger woman. In fact, declining fertility in perimenopausal women means that many of these methods are relatively more effective. In highly motivated individuals, even barrier contraceptives can reduce the pregnancy rate down to below 4–5 pregnancies per 100 women/year. Moreover, in women with new relationships, condoms should be recommended for personal protection against infection.
The late reproductive years are also associated with irregular menstrual patterns and onset of menopausal symptoms such as hot flushes, which may complicate the choice of contraceptive method. Hormonal contraception has particular advantages that clearly can benefit older women. The combined oral contraceptive pill can be prescribed for healthy, low-risk, non-smoking woman until she reaches the menopause.
For those women with cardiovascular risk factors, progesterone-releasing intrauterine system represents an alternative that also has beneficial effect on menstrual bleeding patterns which may be particulary suitable in perimenopausal women.
Many women, or their partners, will also have opted for sterilization by this age.
The final decision on which contraceptive method to recommend should be based on a knowledge of the women's medical history, physical findings, current frequency of coital activity and prior contraceptive experiences. Risks and benefits of the contraceptives options have to be disscused widely and need to be individualized.
A frequent clinical dilemma for the physician or health care provider is when to switch a patient from hormonal contraception to hormone replacement therapy (HRT). Women are generally adviced to continue contraception for 1 further year after the last spontaneous menstrual period if aged 50 years or over, or for 2 further years if aged under 50. If a women has commenced HRT during the perimenopause or is using a hormonal method of contraception it can be difficult to assess when she becomes menopausal. In the absence of conclusive clinical data, some authors arbitrarily withdrawn hormonal contraception at 51 years (the average age at menopause) for 1–2 months and determine serum follicle-stimulating hormone (FSH) levels, others suggest that measuring FSH levels on the 7th day of pill free interval enables to evaluate ovarian function.
At present there does not exist a simple biochemical test that definitively predicts the onset of menopause. As a measure of reproductive reserve, FSH levels greater than 15 mIU/mL drawn on the third day of the menstrual cycle suggest failing ovarian function and when FSH levels are above 25 mIU/mL pregnancy rarely occurs. Nevertheless, it is important to be aware that there can be substantial fluctuations in FSH levels and requires more then one sample before definitive statement can be made.
SM-28-02
RIESGO CV Y TH: ESTADO ACTUAL
Nilson Roberto de Melo (Brasil)
Abstract not available at the time of going to press.
SM-28-03
TH Y RIESGO ONCOLÓGICO
Italo Campodónico (Chile)
Abstract not available at the time of going to press.
SM-28-04
LAS PROGESTINAS EN LA TERAPIA HORMONAL (TH)
L. Hernández
Past President of Federación Latinoamericana de Climaterio y Menopausia (FLASCYM), Guatemala, Guatemala
Desde mediados de la década de los 70's cuando Smith y Ziel comenzaron a fortalecer el concepto del uso de progestinas complementario al tratamiento con estrógenos para disminuir el riesgo de cáncer de endometrio a la fecha, han surgido un sin número de progestinas con nuevos efectos beneficiosos que se suman a los beneficios del estrógeno en la busqueda de mejorar la calidad de vida de la mujer en el climaterio.
Gambrell Rd publicó en 1987 en el AJOG que en mujeres que conservan su útero, es imprescindible la administración de una progestina por un adecuado número de días para limitar la proliferación endometrial y el riesgo de cáncer que aumenta de 2 a 4 veces y que se asocia con la administración de terapia estrogénica sin oposición. En esa misma época se demostró que dando tratamiento para hiperplasia endometrial simple durante diez días con una progestina había una regresión de 98%, disminuyendo la incidencia de cáncer de 300 por cada 100,000 con estrógeno solo a 49 por cada 100,000 con tratamiento combinado de estrógeno y progestina.
Sin embargo, hay que estar conscientes de que el antagonismo de las progestinas con el estrógeno en el endometrio también lo es en otros órganos en donde lejos de ser un beneficio se convierte en una desventaja, antagonizando el efecto favorable de los estrógenos en el endotelio vascular (1) teniendo efectos desfavorables en el metabolismo lipídico (2), alterando algunos factores de la coagulación (3) y en algunos casos observando efectos adversos en la mama (4), si no, baste citar los resultados del estudio WHI del brazo de EEC más AMP (5)en comparación con el brazo de sólo estrógenos(6) en eventos cardiovasculares y cáncer de mama, en donde el aumento de ambas entidades en el brazo combinado puede atribuirse al AMP (5) y donde surgen algunas interrogantes a estudiar para resolver tales cómo: ¿Son las progestinas responsables de los efectos cardiovasculares negativos de la TH al contraponerse a los efectos beneficiosos de los estrógenos? ¿Del incremento del cáncer de mama asociado a la TH?, o es la MPA, la dosis, la vía de administración o la forma de uso.
De las aseveraciones anteriores, se desprende el concepto de que no todas las progestinas actúan de la misma manera y que vamos a encontrar efectos diferentes según sea el efecto de las mismas. Hay progestinas con efecto androgénico parcial (levonorgestrel, noretisterona, desogestrel, gestodeno, etc), con efecto antiandrogénico (Ciproterona, clormadinona, dienogest), con efecto estrogenico parcial cómo la noretisterona (de aquí el beneficio comprobado de esta en la mejoría del contenido mineral oseo) (7), e incluso progestinas con efecto antimineralcorticoide (Drospirenona), efecto este último que a demostrado su beneficio en la acción sobre el Sistema renina – angiotensina – aldosterona (RAA) y su impacto favorable en la protección cardiovascular complementaria con los estrógenos.
Podemos reconocer entonces, por un lado un efecto directo sobre el endometrio común a todas las progestinas y por el otro, un efecto variable que depende del origen de la estructura, interacción con otros receptores, vías de administración, metabolización, y potencia del fármaco.
Por todas estas razones, se hace necesario considerar para su uso clínico todos los efectos involucrados en la TH, teniendo cómo elementos útiles para su selección, tanto los efectos benéficos adicionales, cómo los efectos adversos y los riesgos, lo que aunado a la solidez de la evidencia nos permita una elección que debe ser individualizada y, por supuesto, con consentimiento informado.
SM-28-05
EL CLIMATERIO EN LATINOAMÉRICA
Rubén Bucheli (Ecuador)
Abstract not available at the time of going to press.
SM-29: Update de la terapeutica de la mujer en menopausia (Sociedad Portuguesa de Menopausia)
SM-29-01
CONTROVERSIES IN MENOPAUSAL OSTEOPOROSIS THERAPY
C. Castelo-Branco
Hospital Clínic, Institut Clínic de Ginecologia, Obstetrícia i Neonatologia, Faculty of Medicine, University of Barcelona, Spain
An exceptional increase in drugs related to osteoporosis therapy has occurred during the last decades. All of these new pharmacological approaches have demonstrated their anti-fracture efficacy. Consequently, the medical approaches to osteoporosis turns into a more refined and multifaceted management.
All bisphosphonates (alendronate, risedronate, ibandronate, zolendronate) have demonstrated their efficacy on the axial and appendicular skeleton preventing both vertebral and non-vertebral fractures including hip fractures. Similarities among the different bisphosphonates difficult to distinguish between them in terms of efficacy and/or safety. A special attention should be focused on obtaining the best patients' adherence, which remains poor with the daily and weekly formulations. New bisphosphonates are in developing process.
Selective estrogen receptor modulators (SERMs), nowadays represented by Raloxifene, have shown anti-fracture efficacy at the level of the lumbar spine and, also, exerts collateral benefits on the breast. New drugs of this group are currently in developing process (Lasofoxifene, Bazedoxifene and Arzaxofine)
Strontium ranelate, a drug that combines inhibition of bone resorption with stimulation of bone formation, is characterized by an extensive distribute of activity, both in terms of skeletal sites positively affected and of patients experiencing benefits of its administration. Recent data suggest a positive action in osteoarthritis. Currently, Strontium is the only drug which has demonstrated anti-fracture efficacy in elderly subjects over 80 years old.
Drugs derived from the parathyroid hormone family are bone formation stimulators. Recombinant PTHs, both 1–34 and 1–84, have demonstrated anti-fracture efficacy in all sites of the skeleton. Because of their excessive cost, their use is restricted to patients at fracture risk with severe osteoporosis.
New pharmacological approaches are being developed in the last years. Drugs as RANKL analogues (denosumab), Osteoprotegerin, Cathepsin K inhibitors (Odanacatib), Integrin receptor inhibitors (L–000845704) and Angels open promising alternatives focusing therapy in different targets.
SM-29-02
STRONTIUM RANELATE: WHAT'S THE VALUE OF INNOVATION?
J. Laíns
Hospitais Universidade Coimbra, Portugal
Strontium ranelate (Sr) acts as an effective antiosteoporotic therapy in postmenopausal women with osteoporosis. Sr has a dual mode of action through antiresorptive and bone forming effects.
Unpaired bone biopsies in postmenopausal osteoporotic patients treated with Sr showed increased bone formation, assessed by both the mineralization rate and osteoblast surface, and decreased osteoclast surface.
Paired iliac crest bone biopsies from 15 postmenopausal osteoporotic patients, previously treated with a bisphosphonate, showed that, one year after Sr therapy, active bone formation sites were increased while osteoclasts were still suppressed.
Micro-computed tomography of bone biopsies showed, in treated patients compared with the placebo group, a higher number of trabeculae, decreased trabecular separation, and an increase in cortical thickness, providing evidence of a better trabecular and cortical bone microarchitecture.
SOTI and TROPOS, two large double-blind, placebo-controlled studies, in postmenopausal osteoporosis, assessed Sr efficacy. Sr decreased the risk of vertebral fractures, by 52% within the first year, and by 38% over 3 years of treatment; the risk of having a first vertebral fracture is decreased by 48% after 3 years. The risk of nonvertebral fractures decreased by 16%, and, in patients at high risk, the risk of hip fracture decreased by 36% over 3 years.
At 3 years, the BMD in the strontium ranelate group increased from baseline by 5.7% at the femoral neck and 7.1% at the total hip, compared with the placebo group. Each percentage point increase in femoral neck BMD was associated with a 3% reduction in risk of a new vertebral fracture. The 3-years changes in femoral neck BMD explained 76% of the reduction in vertebral fractures.
Sr antifracture efficacy is documented across a wide range of patient profiles, independently of the: age, bone mineral density, body mass index, number of prevalent vertebral fractures and family history of osteoporosis.
5-year data from these double-blind, placebo-controlled studies show that the antifracture efficacy is maintained over time.
The most common adverse events consisted of nausea, diarrhoea, headache, and dermatitis and were reported more commonly in the Sr group, but only during the first 3 months.
A slight increase in the incidence of venous thromboembolism was observed, but there is no known interaction between Sr and parameters of haemostasis.
EMEA recommended a warning in the product information due to the risk of hypersensitivity reactions.
Sr induces antiresorbing and bone-forming effects resulting in an improvement in bone microarchitecture and bone strength in vivo, leading to a decrease in vertebral and hip fracture risks.
SM-29-03
PREVENTING BREAST CANCER WITH RALOXIFENE: RESULTS OF THE STAR STUDY
Larry Wickerham (USA)
Abstract not available at the time of going to press.
SM-29-04
MISSION STUDY
Praven Prostuzmick (Croatia)
Abstract not available at the time of going to press.
SM-30: Women's health care during the menopausal transition and beyond (organised by the Dutch Menopause Society)
SM-30-01
CARDIOVASCULAR HEALTH IN PERIMENOPAUSAL WOMEN
Angela H. E. M. Maas
Cardiologist, Isala Klinieken, Zwolle, The Netherlands
During the menopausal transition period the prevalence of risk factors for coronary heart disease (CHD) such as overweight, diabetes, hypertension, hyperlipidemia and the metabolic syndrome rise rapidly. From epidemiologic studies it is known that the risk factor profile in women at the age of 50 years is an important predictor of future CHD events. More than 80% of all cases of cardiac events in women can be prevented through a healthy life-style and treatment of the individual risk factors. Risk factor counseling by gynaecologists is nowadays mandatory to garantee safe presciption of hormone therapy (HT) in the perimenopause.
Hypertension is a key risk factor in aging women and closely related to overweight, insulin resistance and the development of diabetes. High blood pressure often starts in the perimenopausal period and may interfere with vasomotor symptoms. In this presentation current insights in the development of CHD risk factors in women will be shown. Further, easy tools will be given to separate women in low risk and higher risk categories and advise will be provided for women who may need further cardiac screening.
SM-30-02
MENTAL HEALTH AND MENOPAUSE
P. Kölling1 and L. T. W. de Jong-van den Berg2
1Medisch Spectrum Twente, Enschede, Netherlands; 2Groningen University Institute for Drug Exploration (GUIDE), Netherlands
The transition during the menopause is considered to be a period of changes in somatic and psychological functioning. For the mental health aspects the premenopausal phase is the most interesting. Women are more at risk to develop depressive symptoms and sometimes a major depressive disorder in this phase compared to other stages of the perimenopausal period. Women with a history of depression are at greater risk, especially when there is a link with depression and hormonal transition phases (e.g pregnancy, postpartum depression or premenstrual dysphoric disorder). Changes in estrogen levels are linked with mood disturbances. Vasomotor symptoms and altered sleeping patterns are supposed to play a pivotal role in the development of depressive complaints. Hormone therapy (HT) is an effective treatment for vasomotor symptoms and related sleep disturbances, but after the publication in 2002 of the Women Health Initiative trial and the observational Million Women Study in 2003 many women stopped HT. In The Netherlands there was a dramatic decline of HT prescriptions in this period in women aged 40–74 (66% decrease) and in women aged 50–54 (64,4% decrease). We investigated the alternative drug prescriptions in women who stopped their HT and compared this with women who continued their HT. This study was performed with the InterAction database (IADB.nl), which contains prescription drug dispensing data from community pharmacies in The Netherlands. Significantly more women who stopped HT began to use anxiolytics and sedatives (HR 1.41, CI 95% 1.12–1.78).
The duration of HT use plays also a role: women, stopping HT who had been on HT longer than three years were significantly higher incident users of anxiolytics and sedatives (HR 1.61, CI 95% 1.10–2.35). There was no significant increase of the prescriptions of antidepressants.
In the literature some antidepressants have been described to alleviate menopausal symptoms (hot flashes, insomnia). It remains questionable if antidepressants can replace HT. When depressive symptoms are accompanied with vasomotor symptoms HT will still be the first choice treatment. But in case of a major depressive episode antidepressants are the first therapeutic choice.
SM-30-03
SEXUAL HEALTH OF THE OLDER COUPLE
R. H. W. van Lunsen and E. T. M. Laan
Academic Medical Center, University of Amsterdam, The Netherlands
Sexual health by the WHO is defined as “a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled.”
Sexuality for the vast majority of older men and women is an important aspect of quality of life and they deserve not only more attention for their questions and problems regarding sexuality, but also a more comprehensive and less medicalised approach than often seems to be the case.
The incidence of sexual “dysfunctions”(SD) of women and men increases around the age of fifty. This raises the questions to what extent are these complaints related to hormonal and other bodily changes, and what is the contribution of psychological and contextual factors to sexual function in this transitional phase of life. The physiological age related changes in the sexual system are the result of neuro-endocrinological changes and of a loss of vascular elasticity, both resulting in a decrease of arousability or sexual responsiveness. On a motivational level there often is a certain shift from lust to more interactional aspects of sexual functioning.
Changes in arousability and motivation -two aspects of sexual desire- lead to a situation in which both men and women need more time, more relaxation and more direct genital stimulation to make the sexual process work. The best predictors for continuation of a satisfactory sex-life therefore are flexibility, variation in sexual repertoire in the past and present, and most of all: adequate sexual stimulation. Most sexual problems are the result of a process during which partners have been unable to cope with age related changes in wishes and expectations. In these couples the three prerequisites for a successful sexual life are not met: adequate stimuli, context and communication. From our own psychophysiological studies in elder men and women it has become clear that they still are able to have a complete genital sexual response, even though they present themselves with a SD meeting the criteria of so called “objective” rating scales often used in the international literature.
Sexual arousal disorders in the elderly resulting in vaginal dryness, dyspareunia and erectile dysfunction often are the result of a physiological decrease in sexual arousability not compensated by adequate behavioural adjustment and communication. As long as there are no serious neurological, vascular or metabolic diseases and no sexual function influencing drugs are used, only in a minority of cases physical aspects of ageing, such as androgen and estrogen depletion, play a decisive role in the occurrence of SD. Most men and women receiving medication for their SD in fact would not need these often ineffective medications if their prerequisites for a “healthy” sex life were met.
SM-30-04
HIGHER FRACTURE RISK IN NON FRACTURED POSTMENOPAUSAL WOMEN WITH AN INCREASED RISK SCORE FOR OSTEOPOROSIS COMPARED WITH POSTMENOPAUSAL WOMEN WITH A LOW ENERGY FRACTURE
H. R. Franke1 and K. K. M. Sweers2
1Medisch Spectrum Twente Hospital Group, Enschede, Netherlands; 2University of Twente, Enschede, Netherlands
Objective: Postmenopausal women with a low energy fracture are suspected to have a higher chance of having osteoporosis and an increased risk of a subsequent fracture compared with non fractured postmenopausal women with an elevated risk of having osteoporosis.
Design & Method: Patients with a low energy fracture (Group A) and non fractured postmenopausal women from 11 general practices in The Netherlands with a risk score for osteoporosis of 4 or more, see table (Group B) underwent DXA measurements of the lumbar spine and femur. Furthermore we calculated the ten year probabilities of osteoporotic fractures on the basis of age and bone density of the femur of both groups. The Wilcoxon and χ2 tests were performed.
Results: Group A consisted of 224 and Group B of 1002 patients. The only significant difference of the baseline characteristics between both groups was the mean age. In Group A the mean age was 63.6 and in Group B 68.4 years. In Group A 17% of the patients had osteoporosis (T ≤ −2.5) of either the lumbar spine or femur compared with group B with 15% of the patients having osteoporosis. This difference was not statistically significant. The ten year probability of an osteoporotic fracture of higher than 10% of Group A was 48% and of Group B 56%. This difference is statistically significant.
Conclusion: Non fractured postmenopausal women with an increased risk of having osteoporosis do have a higher risk for a fracture than postmenopausal women after a low energy fracture. This is probably due to the higher age of the women in Group B. Nevertheless we suggest that in general practices case finding should be performed to minimise the incidence of future low energy fractures.
SM-31: The french position statement on HT part II (organised by the French Menopause Society)
SM-31-01
HORMONE REPLACEMENT THERAPY AND BREAST CANCER RISK: POSITION STATEMENT OF AFEM
André Gorins
The relationship between hormone replacement therapy (HRT) and breast cancer (BC) risk is controversial. AFEM (Association Française pour l'Etude de la Ménopause) gives its statement for the year 2008. It might be modified according to new french or international studies on the next years.
Results: from the Women Health Initiative Study (WHI) are first reminded. They induced an important change in hormone replacement therapy management. However remarks and critics have followed this publication.
The AFEM statement is as follows:
HRT will be only given to patients whose informed consent is obtained after clear discussion with their physician.
A clinical examination and a recent mammogram, classified ACR1 or ACR2, are mandatory before starting the treatment. A clinical control every 6 months and a mammogram (+ ultra-sound if necessary) every 18–24 months must be carried out, knowing that in 20% cases, mammary density is increased by HRT, making the interpretation more difficult.
Natural hormones : estradiol and progesterone (dydrogesterone also) will be preferentially chosen, according to the E3N study which has found no statistical increased risk of BC with these molecules for a mean follow up of 8 years.
HRT will be administered as long as it will be well tolerated, with no serious side-effect or complication, with the consent of the patient. There is no limit of duration of treatment. Nevertheless, an evaluation is necessary every year and especially after 5 years of treatment.
Although some observational studies reported a smaller risk of BC with sequential treatment regimen as compared to continuous combined therapy, there is currently insufficient evidence regarding BC risk to recommand any specific regimen.
For hysterectomized women, estradiol alone is advised, although there is a desagrement about BC risk between french and american studies.
No studies have demonstrated any increase in mortality associated with breast cancer in women undergoing treatment.
Raloxifen is not a specific treatment of menopause. It is indicated in osteoporosis. It appears that it has a protective effect against BC (See the MORE study).
Tibolone, according to fundamental works, should have a favorable effect on the mammary gland; but epidemiological studies do not confirm the fact.
For special situations:
familial history of BC (including BRCA1 and BRCA2 mutations),
benign breast diseases (proliferation without or with atypia).
There are currently no studies that have demonstrated any additional increase in risk attribuable to HRT. Nevertheless, it is recommanded to explain to the patient the increased basal risk versus the normal feminine population.
It is noteworthy that other factors than HRT, like basal mammary density, parity, obesity, alcohol … , play a not negligible role in BC risk.
At last, no HRT should be given to women with a prior personal history of BC.
SM-31-02
DOES THE DROP OF WOMEN ON HRT EXPLAIN THE DECREASE OF THE INCIDENCE OF BREAST CANCER IN 2005–6 IN FRANCE?
Henri Rozenbaum (France)
Abstract not available at the time of going to press.
SM-31-03
USE OF POSTMENOPAUSAL H.T AND BREAST CANCER RISK: RECENT RESULTS FROM THE FRENCH E3N COHORT
A. Fournier and F. Clavel-Chapelon
Inserm, ERI20, Gustave Roussy Institute, 94805 Villejuif, France
Background. A large number of postmenopausal hormone therapies (PHT) are available. Whether they impact differently the breast cancer risk and whether their impact differs according to histology and hormone receptor status is still unclear.
Objective. To evaluate and compare the impact of various PHT on different subtypes of breast cancer.
Design and Methods. Relative risks (RR) of breast cancer were estimated in 80377 postmenopausal women included in the French E3N cohort. During follow-up (1990–2002; mean 8.1 years), 2354 primary invasive breast cancers occurred; 96% were histologically confirmed.
Results. Compared with PHT never-use, ever-use of estrogens alone was associated with a significant increase in risk of breast cancer, considered as a single entity (RR = 1.29, [95%CI 1.02–1.65]). Estrogen+progesterone use was associated with a RR of 1.00 [0.83–1.22] and estrogen+dydrogesterone with a RR of 1.16 [0.94–1.43]; estrogens combined with other progestagens were associated with a significant increase in risk (RR 1.69 [1.50–1.91]).
Ever-use of estrogen+progesterone was not significantly associated with the risk of any breast cancer subtype. Use of estrogen+dydrogesterone was associated with a significant increase in risk of lobular carcinoma (RR 1.7 [1.1–2.6]). Use of estrogen+other progestagens was associated with significant increases in risk of ductal and lobular carcinomas (RRs 1.6 [1.3–1.8] and 2.0 [1.5–2.7], respectively), of estrogen receptor-positive/progesterone receptor-positive (ER+/PR+) and ER+/PR- carcinomas (RRs 1.8 [1.5–2.1] and 2.6 [1.9–3.5], respectively), but not of ER-/PR+ or ER-/PR- carcinomas (RRs 1.0 [0.5–2.1] and 1.4 [0.9–2.0], respectively).
Conclusion and discussion. The increase in risk of breast cancer observed with the use of PHT other than estrogen + progesterone and estrogen + dydrogesterone seems to apply preferentially to ER+ carcinomas, and to affect both ductal and lobular carcinomas. Further research is needed on estrogen+progesterone and estrogen+dydrogesterone PHT.
SM-32: Lessons from Japan nurses' health study (organised by the JMS)
SM-32-01
DESIGN OF THE JAPAN NURSES' HEALTH STUDY AND MORBIDITY AMONG JAPANESE WOMEN
Kunihiko Hayashi1 and the Japan Nurses' Health Study Group
1Gunma University, Maebashi, Gunma, Japan
Objective: We designed a prospective cohort study of Japanese women based on the design of the Nurses' Health Study that has contributed the most to women's health worldwide. The purpose of this lecture is to clarify the characteristics of design of the Japan Nurses' Health Study (JNHS) and to show the morbidity among Japanese women estimated from the baseline survey of the JNHS.
Subjects & Methods: The study design of the JNHS was compared with other large-scale women cohort studies. The prevalence of an ever-diagnosed, which refers to the proportion who had ever been diagnosed at the baseline survey, was calculated for each disease. The trend of the prevalence of ever-diagnosed among 5-year age groups was examined by the Cochran-Armitage test, and the increasing rate of the prevalence in women aged 45–59 years was calculated.
Results: The JNHS cross-sectional baseline survey was conducted in 2001–2007. A total of 49,925 women responded to the baseline survey. Compared with traditional community-based cohort studies in Japan, the JNHS is characterized by comprising only women aged from 25 to >60 years from a geographic area that encompasses all 47 prefectures of Japan.
The prevalence of an ever-diagnosed of anemia, migraine, uterine myoma, endometriosis, hypercholesterolemia, and hypertension exceed 5%. The increasing rate of prevalence among 45–59 years-old women was higher than 3.0 per 1,000 person-year for hypercholesterolemia, hypertension, osteoporosis, uterine myoma, and diabetes mellitus. The rate for hepatitis, gallstone disease, angina pectoris, transient ischemic attack, thyroid disease, and breast cancer was 1.0<–3.0 per 1,000 person-year. The prevalence of cerebral infarction, subarachnoid hemorrhage, myocardial infarction, endometrial cancer, colorectal cancer, and stomach cancer among 45–59 years-old women increased slightly (less than 1.0 per 1,000 person-year).
Conclusion: The Japan Nurses' Health Study should generate comprehensive current and useful information about the status of women's health in Japan. The so-called ‘lifestyle-related’ diseases increased from the late 40s to 50s in Japanese women.
SM-32-02
ENDOMETRIOSIS AS A RISK FACTOR FOR EARLY MENOPAUSE
Toshiyuki Yasui1, Japan Nurses' Health Study Group
1The University of Tokushima Graduate School, Tokushima, Tokushima, Japan
Objective: Early menopause has been implicated in risk of several factors, including smoking and body mass index (BMI) in women. The purpose of this study is to clarify the status of natural menopause and the factors influencing the onset of natural menopause in Japanese women.
Subjects & Methods: This study is a cross-sectional study between 2001 and 2004. We analyzed the data of 21373 pre- and postmenopausal women who enrolled in the Japan Nurses' Health Study at ages 40–59 years. Women who had surgical menopause were excluded from the analyses. We assessed the proportion of postmenopausal women by age and menstrual status. The relative risk (RR) of menopause was estimated as age-adjusted odds ratio and its 95% confidence interval by using multiple logistic models.
Results: The prevalence of postmenopausal women were 0.9% in subjects aged 40–44 years, 9.0% in subjects aged 45–49 years, 56.6% in subjects aged 50–54 years and 97.1% in subjects aged 55–59 years. The factors influencing the onset of natural menopause were age of menarche, past history of sterility, rate of pregnancy, BMI and smoking. The RR (age-adjusted odds ratio and 95% CI) for late menarche, number of pregnancy and BMI was 0.933 (0.899–0.967), 0.942 (0.910–0.977) and 0.951 (0.934–0.967), respectively. In addition, the RR for smoking and past history of sterility was 1.347 (1.204–1.507) and 1.297 (1.112–1.513), respectively. In the cause of past history of sterility, the RR for sterility due to endometriosis was 3.385 (2.134–5.370). The RR for sterility due to ovulatory disorder and tubal occlusion was 1.055 (0.764–1.456) and 1.488 (1.009–2.193), respectively. The RR was also 0.743 (0.595–0.928) for intake of milk and dairy products (1–5 days per week), but intake of tofu, natto and miso soup have not associated with age at menopause.
Conclusion: Earlier onset of natural menopause among Japanese women is associated with history of reproductive health such as sterility due to endometriosis as well as smoking.
SM-32-03
HORMONE REPLACEMENT THERAPY AND CARDIOVASCULAR DISEASE IN THE USA
Karin B. Michels
Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA
Observational studies have suggested a reduced risk of cardiovascular disease (CVD) associated with the use of hormone replacement therapy (HRT), while results from the Women's Health Initiative raised concern about an increase in the risk of CVD among women using HRT. These apparently discrepant results have lead to concern among prescribing physicians and patients alike. How can the results be reconciled? Recent research has provided clinically relevant insights which may serve to optimize HRT treatment. In the Women's Health Initiative, HRT assignment to participating women did not reflect clinical practice but addressed the question whether women with no or mild menopausal symptoms who started HRT at some point during menopause had a different risk for CVD than women with no or mild menopausal symptoms who did not use HRT. The answer to the question posed was that women who started HRT several years after onset of menopause had an increased risk of CVD and the later they started HRT use the higher the risk. Conversely, women who started using HRT at onset of menopause did not increase their CVD risk, neither in the WHI randomized trial, nor in the observational studies. Using HRT as indicated for the treatment of menopausal symptoms that arise during the transition into menopause and that affect quality of life should not increase the risk for CVD.
SM-32-04
CURRENT STATUS OF HORMONE REPLACEMENT THERAPY IN JAPAN
Toshiro Kubota1 and Japan Nurses' Health Study Group
1Comprehensive Reproductive Medicine, Graduate School, Tokyo Medical and Dental University, Tokyo, Japan
Objective: The results of the Women's Health Initiative (WHI; 2002) study were widely noted and have affected the menopause medicine, especially hormone replacement therapy (HRT) in Japan. The purpose of this study is to clarify the current status of HRT before and after the WHI report in Japan by a large prospective cohort study.
Subjects & Methods: This study is a cross-sectional study between 2001 and 2004. We analyzed the data of 15,441 pre- and postmenopausal women who enrolled in the Japan Nurses' Health Study at ages 45–64 years. The first group is 12,979 women who were HRT users before the WHI report (2001–2002 registered) and the second group is 2,462 women who were HRT users after the WHI report (2003–2004 registered). We assessed the questionnaire concerning about HRT usage during 4 years, and compared the status of HRT between 2 groups by statistical analysis of t-test and Wilcoxon test.
Results: The percentage of HRT user was 12.9% of all 6,157 postmenopausal women and that of current HRT users was 5.8%. The percentages of ever HRT users were 12.3% in the first group and 15.6% in second group. The latter was significantly higher than the former (p < 0.04). The percentages of current users were 5.7% in the first group and 6.1% in the second group. There was no significant difference between these 2 groups. In addition, the percentages of oral administration of only conjugated equine estrogens (CEE) were 13.2% in the first group and 14.2% in the second group. The percentages of oral administration of CEE combined with medroxyprogesterone acetate (MPA) were 23.0% in the first group and 25.7% in the second group. There was no significant difference in these two oral regimens between these 2 groups. On the other hand, the percentages of transdermal administration of the natural estradiol were 8.0% in the first group and 13.3% in the second group. Those of transdermal administration of the natural estradiol combined with MPA were 3.7% in the first group and 6.2% in the second group. The percentages of the second group were significantly higher than those of the first group in transdermal ERT/HRT (p < 0.01).
Conclusion: The Japan Nurses' Health Study showed that the overall percentages of HRT users did not change before and after the WHI report, though there was a change in the routes of hormone administration.
SM-33: The science and sense in managing menopause – the Indian mantra (organised by the Indian Menopause Society)
SM-33-01
EPIDEMIOLOGY
J. Unni
Jehangir Hospital, Pune, Maharashtra, India
India's share of the world population is 16.7%. Due to declining fertility and increase in life expectancy, the population of middle and older aged persons is increasing. India will soon be the second largest country in terms of the absolute number of women above 50 years of age. Elderly women will outnumber elderly men and the health problems of an ageing population will largely be the problems of women.
In India 19% of women aged 40 have already reached menopause and by age 49, two thirds of women have attained menopause. The number of women in the postmenopausal ages of 50–59 years is projected to increase from 36million in 2000 to 63 million in 2020. The onset of menopause occurs later in urban areas than in rural areas. Interstate variations are also observed with respect to age of menopause.
Women from a low socio-economic background reach menopause earlier than their counterparts. The proportion of women who are in menopause decreases considerably with the increase in education. The age standardised proportion of women who are in menopause is highest among illiterate women (19.5 per cent) and this reduces to 11.1 per cent when the education increases to high school or higher.
There are a higher proportion of women who have reached menopause among those with a large number of children than those with fewer children. Women with low body mass index reach menopause early compared with women with higher body mass index.
Working women, especially agricultural labourers have an early onset of menopause compared with those who work in other sections.
Since a large number of Indian women experience menopause in their forties, they have a longer period of estrogen deprivation and its consequences.
Osteoporosis is a major health care problem, associated with substantial morbidity and mortality. There is a high prevalence of osteopenia and osteoporosis and it is almost 100% above the age of 65. The burden of cardiovascular diseases and stroke is also rising in India.
The major cancers in women are of the cervix, breast and mouth/oro-pharynx. The incidence of endometrial carcinoma is low.
As India is still characterised by a large number of illiterate women with a low age at marriage and early childbearing with poor nutritional levels, the problem of early menopause may continue to be an issue in the future also.
SM-33-02
PREMATURE MENOPAUSE & INFERTILITY
Duru Shah
Medical Director: Gynaecworld Assisted Fertility Unit, Kwality House, Kemps Corner, Mumbai 400 026; Consultant, Obs& Gyn, Breach Candy Hospital, Jaslok Hospital, Sir Hurkisondas Hospital (www.gynaecworld.com; Email: [email protected])
Early ovarian ageing affects 10% of the general population. It is completely asymptomatic, has a long latent phase and predictable natural history. There is scope for screening women in their early 30's for “early ovarian ageing” especially in high risk groups. Premenopausal women who have been exposed to gonadotoxic chemotherapy either in childhood or adulthood have specific gynecological concerns. These include the prospect of subfertility and a premature menopause (and its effects), and methods of preserving fertility and ovarian function.
Infertility appears to be most devastating for young women who have not yet started or completed their families. Even for women who do not desire children or do not want any more children, the loss of menstrual function and the lack of choice about having more children is emotionally distressful. These women may benefit greatly from knowledge of their functional ovarian reserve. These women may seek advice and treatment regarding their reproductive status, including ways of preserving their fertility and preventing menopause – factors that have a profound impact on their quality of life. In such women determination of ovarian reserve can help and clarify the decision making process. The recognized limitations of basal markers such as FSH, have led to the evaluation of several other tests of ovarian reserve. Dynamic testing has the potential to unmask “poor responders”. Biophysical markers offer a more ‘direct’ estimate of ovarian reserve, and the widespread use of ultrasound scanning makes it a relatively easy application to integrate into practice. Despite all the options available, the ideal ovarian reserve testing has yet to be identified.
Given the trends for older age at marriage and delayed childbearing, younger women with cancer could miss out on the potential for pregnancy if they do not consider preventive fertility options before undergoing treatment. Fertility options usually don't compromise treatment or survival outcomes.
Advances in reproductive technology have made fertility preservation techniques a real possibility for patients whose gonadal function is threatened by premature menopause, or by treatments such as radiotherapy, chemotherapy or surgical castration. Decision making in this area is particularly difficult because of experimental nature of some of these techniques. Currently, pregnancy is extremely unlikely with cryopreservation of oocytes, although new technologic approaches may improve the viability of this option. Embryo cryopreservation with IVF is a viable option, but a major disadvantage is the delay in cancer treatment because of the time required for ovarian stimulation and the IVF procedure. Ovarian tissue cryopreservation is an experimental alternative that requires further study. A major concern is the possibility of transferring tumor cells, especially in patients with hematologic malignancies. Other parenting options include oocyte donation, surrogate pregnancy and adoption.
In the longer term, advances in molecular reproductive biology and pharmacology may enable us to develop drugs or interventions that will increase the chances of pregnancy for these women and even delay their accelerated decline of ovarian reserve.
SM-33-03
CATEGORISING MENOPAUSE THE INDIAN WAY
Behram S. Anklesaria
President, Indian Menopause Society, 2006–2007; Professor of Ob/Gyn., Nhl Medical College, Ahmedabad, Gujarat, India
CATEGORISATION and STAGING are essential components in the Indian Mantra of modern menopause management, (MMM). India is a vast country with many different regions, languages and ancient cultures. The majority of our women live in rural areas where MMM, is relatively unknown. The good news for Indian women is that modern medicine has increased their life expectancy most dramatically. This means that 40+ women now constitute, for the first time, a significant and ever increasing percentage of the population. We would like to provide INDIVIDUALISED MMM to these women. The crying need for treatment of their symptoms and prevention of their complications has been demonstrated by several recent studies.
Individualized management of Indian 40+ women with their diverse cultural and regional needs is not possible without CLINICAL CATEGORISATION. The full text of this presentation will provide the various categories that have helped Indian physicians deal with this problem effectively. Individualisation of treatment involves another more important aspect. The same ‘patient’ develops different needs at various ‘stages' of menopause. A good physician will encourage the ‘patient’ to report regularly and will alter the management to suit her ever changing needs. A simple scientific ‘staging system’, widely disseminated, has helped us in India, to do just that.
The author presents here, his staging system, first published in India in 1997. Four years later in 2001, the ‘Stages of Reproductive Ageing Workshop (STRAW) and the American Society for Reproductive Medicine published another staging system. This is an excellent system for Reproductive Ageing, useful for managing infertility problems of older women. However, in dealing with symptomatic and preventive aspects of menopause, we feel that our older staging system is superior. It has been widely propagated in text book chapters, journals and through lecturers all over India and even in Pakistan. Recently it has been included as the official menopause staging of the Indian Menopause Society in their latest consensus document, released in 2008.
The detailed text of this presentation will elaborate on the definitions of stages I, II and III of this system. We will also mention the symptoms and complications to be expected at each stage and sub-stage. Medical students, post-graduates and practicing clinicians in the Indian subcontinent have used this simple staging system to understand and manage menopause related problems of women in the Indian subcontinent. Can this system also benefit 40+ women in the World at large?
SM-33-04
WHAT SHOULD WE TELL OUR POSTMENOPAUSAL WOMEN?
Meeta
Tanvir Hospital, Hyderabad, A. P., India
Menopause is a significant Public Health issue as it affects every woman. The post menopausal period can be made as productive as the reproductive phase if the physical and mental well being of the individual is maintained. The Health of the elderly would be a valuable resource rather than a liability for the society. The challenge today is who is to manage this transition phase? To practice menopause and preventive medicine I needed to switch over from the exciting role of an obstetrician and a surgeon to one of a family physician and a counsellor. Basic knowledge and updates in unfamiliar areas like Diabetes, Hypertension, Bone Health, and Nutrition etc needs to be acquired. Menopause is an estrogen deficiency and not a estrogen deplete state. All women experience universal physiological changes, but the biological response of the women vary. The response depends upon the cultural back ground, socioeconomic state, pre-existing health status, emotional and mental attitude of the woman. Hence, the clinical presentation and needs of a menopausal woman is varied. Each woman needs an individualized management plan. Woman present at the clinic with the menstrual problems, symptoms and or for a general health check. Awareness about menopause management options and health related issues need to be communicated by a counsellor, charts, videos or leaflets. Personal risk evaluation and screening for Diabetes, Hypertension, Heart Disease, Osteoporosis, Thyroid, Depression, Obesity, and Cancers would allow women to implement preventive strategies. Scientific evidence supports the role of Lifestyle Management as an important ingredient for maintaining physical and mental health. Role of Nutrition is well stated by Hippocrates. “Thy are what you eat”. There is no debate on the effect the Physical Exercise on the Heart, Bone, Muscle and the overall well being of an individual. Mental Exercise, Social Interaction and a Positive attitude needs to be encouraged. The need of Hormone Therapy- indications, options, pros and cons, duration of therapy, follow up, fears and concerns need to be addressed in detail accurately and patiently. The skill is to translate and communicate the results of various trials in a simple language. Use Absolute Numbers instead of percentages. Adverse reaction are considered rare if they are <10/ 10,000 per year and very rare if <1/10,000 per year. The concept of “Window of Opportunity” in HT in the early postmenopausal period is backed by observational data and recent analysis of the younger women from WHI. The trend is protective effect on the Bone and the Heart. Regarding Breast Cancer, for women currently taking E+P without prior exposure to HT there was no increase for 5 years and a trend to decrease with the use of ET alone. Treatment of symptoms with HT would generally outweigh the risks. God grant me the serenity to accept the things I cannot change, and the courage to change the things I can, and the wisdom to know the difference.
Tabla 1 Staging of Menopause, Dr. Behram. S. Anklesaria, 1997
SM-34: Educating mid-life and aging women about sexuality (organised by the Association of Reproductive Health Professionals [ARHP])
SM-34-01
NURTURE YOUR NATURE: INSPIRING WOMEN'S SEXUAL WELLNESS – A CASE STUDY FOR EDUCATING MID-LIFE AND AGING WOMEN ABOUT SEXUALITY
Lee P. Shulman
Northwestern Memorial Hospital, Chicago, Illinois; Association of Reproductive Health Professionals (ARHP), USA
Although open discussions about sexuality issues have become more common in popular culture in the United States, the subject remains taboo and is rife with contradiction and mixed messages. Governmental policies about sexuality and sexual health, such as the continual funding of abstinence-only education programs and diversion of funds from organizations addressing abortion or sex work, can make accessing evidence-based sexual health information a challenge. While these issues may only seem to affect specific populations such as youth or high-risk women, the impact is felt by all populations, in particular mature women who may be sexually active and/or have questions about their sexuality.
The Association of Reproductive Health Professionals (ARHP) has conducted a review of both the clinical and consumer literature in the United States that showed there is significant concern regarding the “medicalization” of female sexuality, discomfort of health professionals in initiating discussions about sexuality, discomfort of patients in initiating discussions about sexuality, and a lack of health professional training on these issues. A national random-digit-dial telephone survey of women and health care providers revealed women are interested and concerned about sexual health issues, but have genuine concerns about talking to providers and a limited number of resources to which they will turn for information. At the same time, health care providers struggle to balance the high level of interest in libido issues with their lack of time in the examination room and their own training – which often provides incomplete information in how best to talk to women patients about sex and what to offer them to help.
ARHP's Nurture Your Nature curriculum, developed by a consensus of key sexuality experts, will be presented. The presentation will give tools to health care professionals that can help increase the level of meaningful and effective communication about sexuality with their patients.
SM-35: Epidemiología de la Osteoporosis en Iberoamérica (organised by the Sociedad Iberoamericana de Osteología y Metabolismo Mineral)
SM-35-01
FRACTURES IN DIABETIC PATIENTS: EPIDEMIOLOGIC VIEW BY SIBOMM
D. Salica
Healing Argentina Instituto de Osteología y Metabolismo Mineral P. Córdoba Argentina; Cátedra Clínica Médica Facultad Ciencias Médicas Universidad Nacional de Córdoba, Argentina
The complex relationship between diabetes and fractures has been, to the present, a not well recognized instance in clinical practice.
The relationship between osteopenia and diabetes type 1 is recognized in a higher grade than diabetes type 2.
However, the direct effects of diabetes on bone and its metabolism have been analyzed in animals and human beings. In diabetic rats, which have long been treated with insulin, bone alterations and bone metabolism alterations have been observed.
Practices in histomorphometry in human diabetic patients have shown that the higher concentrations of glucemy and HgbA1C, the lower growth and bone formation with lower number of osteoblasts and lower bone formation.
One of the controversial cases constitutes the different results that can be found in bone mineral densitometry (BMD) in diabetic patients. Especially, in diabetes type 2, according to a number of research papers, the bone mass is high, normal, and, less frequently, low. Anyway, there would be a risk of fracture independently of the BMD results. According to epidemiological studies, patients with diabetes type 2 show a higher fracture risk than the general population. Recent studies show a relationship between diabetes treatment and an increase in bone fractures, as it occurs with Thiazolidinediones (TZDs or glitazones), PPAR agonists.
Diabetes affects, in Latin America and the Caribbean, about 20 million people and according to prospects made by the Iniciativa de Diabetes para las Américas (DIA), of the Panamerican Health Organization (PHO), 40 million people are expected to be affected by diabetes in 2025. For this reason, to determine the real fracture risk in this population will be one of the challenges to face.
This challenge motivated our Project FEDI.
(Fracturas en Diabéticos en la Región Iberoamericana, Sociedad Iberoamericana de Osteología y Metabolismo Mineral, 2008) (Fractures in diabetic patients in the Iberoamerican Region; SIBOMM 2008,) which is being carried out at the moment.
Professionals and institutions interested in participating in the Project, please contact www.sibomm.net.
SM-35-02
OSTEOPOROSIS: EPIDEMIOLOGÍA Y REALIDAD SANITARIA EN LA PENÍNSULA IBÉRICA
Javier Ferrer (Spain)
Abstract not available at the time of going to press.
SM-35-03
EPIDEMIOLOGIA DE LA OSTEOPOROSIS EN AMERICA LATINA
Osvaldo Daniel Messina
Buenos Aires, Argentina
La osteoporosis es la mas frecuente enfermedad metabiolica del hueso y se caracteriza por baja masa osea y deterioro de la microarquitectura cuya consecuencia es una mayor fragilidad osea y un aumento del riesgo de fracturas. Es un problema de salud publica a nivel mundial afectando mas de 200 millones de personas y se calcula, entre el 30 y 50% de las mujeres post menopausicas. Estudios realizados en Argentina por densitometría DXA revelan que una de cada cuatro mujeres mayores de 50 años de edad son normales, dos tiene diversos grados de disminución de la densidad mineral y una presenta valores clasificados como osteoporosis. En nuestro pais hay seis estudios epidemiologicos sobre incidencia de fracturas de cadera. En promedio ocurren anualmente alrededor de 320 fracturas cada 100 000 mujeres de mas de 50 años de edad, y 125 fracturas cada 100 000 varones de dicha edad. En cociente mujer/hombre es de 2.56. Extrapolando esta cifra a la población argentina se estima que ocurren alrededor de 18 000 fracturas de cadera/año.
La tabla 1 resume lo hallado en Anerica latina en cuanto a estudios de fractura de cadera.
Re realizo ademas un estudio muy interesante en varios paises de la region sobre osteoporosis vertebral (estudio LAVOS, Latin American Vertebral Osteoporosis Study) cuyos resultados se grafican en la tabla 2.
Tabla 1 Incidencia de fractura de cadera
Tabla 2
SM-35-04
EPIDEMIOLOGIC ASPECTS OF OSTEOPOROSIS IN BRAZIL
B. H. Albergaria
Federal University of Espirito Santo-Vitoria, Espirito Santo-Brazil
Currently, our knowledge of the magnitude of Osteoporosis in most countries from Latin America remains extremely limited except for a few, mainly industrialized nations and it has been stressed the need for considerable research efforts in this area. Particularly in Brazil, declining mortality, along with decreasing fecundity and increasing life expectancy, leads to an aging population and higher rates of chronic diseases, such as osteoporosis.
Therein, we started a burden of illness analysis, as a descriptive tool, with the objective of achieving a better understanding of the impact of this disease in Brazil. We conducted a review of literature and publicly available information as well as a survey of Specialists oriented to the study of osteoporosis to assess the status of research on estimation of burden of osteoporosis in Brazil
The simplest approach to assessing occurrence of osteoporosis is to undertake a cross-sectional survey to ascertain point prevalence. A number of such surveys have been undertaken in Brazil and will be presented. Such surveys have provided important data concerning the age, gender, and geographic influences on osteoporosis and fracture occurrence. However, it has been difficult to compare the prevalence of osteoporosis and osteoporotic fractures in various regions of the country because studies from each region have all used different approaches in selecting samples of the population to study, and each study has used a different method or definition for diagnosing these outcomes.
LAVOS, or the Latin American Vertebral Osteoporosis Study, the first large-scale study designed to estimate the prevalence of vertebral fractures in Latin America, assessed in Brazil 407 women, aged 50 or more, randomly selected using the survey zones defined from the metropolitan area in two cities,Vitoria and Vila Velha, (total population of about 700,000). Hip and lumbar spine bone density, and potential risk factors for and consequences of vertebral fractures were assessed. The study revealed that 33,6% and 33,8% of the Brazilian women surveyed suffer from osteoporosis and osteopenia, respectively. Investigators also found that the risk increases with family history of the disease, yielding a 44% increased risk of vertebral osteoporosis among Brazilian women.
Abstracts of Free Communications
Special Session: Greenblatt Prizes' Presentations
OR1
Hormones and breast cancer
OR2-01
A SURVEY AMONG BREAST CANCER SURVIVORS: TREATMENT OF THE CLIMACTERIUM AFTER BREAST CANCER
Caroline Antoine, Jean Vandromme, Maxime Fastrez, Birgit Carly, Fabienne Liebens and Serge Rozenberg
Department of Obstetrics and Gynaecology, Free Universities of Brussels (VUB-ULB) CHU Saint-Pierre, Rue Haute 322, 1000 Brussels, Belgium
Aim: To evaluate the prevalence and type of menopausal treatments used by breast cancer survivors. To assess factors that impaired the quality of life of these patients.
Material and Methods: Questionnaire assessing Quality of life was sent to 325 breast cancer patients. A 66% valid response rate was obtained: Among them, 169 women were postmenopausal. The following results concern only these patients.
Results: 39 women were using a treatment to alleviate some kind of menopausal symptoms (23,1%). A quarter of the patients (n = 43) did not use anything to alleviate menopausal symptoms either because they had no symptoms or they feared of breast cancer recurrence (n = 24; 14,2%), because they were advised not to do so (n = 27; 16%), because it had shown to be inefficient (n = 5; 3%), or because of contraindication (n = 3; 1,8%).
In this survey, 62,3% of postmenopausal women affected by breast cancer suffered from hot flushes (n = 94), of which half severely (n = 46). Among them, a third used various products to alleviate their symptoms (n = 30). Younger women suffered more often from vasomotor symptoms than did older women (p < 0,000). Current users of aromatase inhibitors suffered more from sexual disorders than non users (p < 0,001).
Conclusion: More than 50% of postmenopausal women suffered from climacteric symptoms such as hot flushes but few were taking a treatment to alleviate these symptoms.
OR2-02
BREAST CANCER INCIDENCE, LONG TIME HRT EXPOSURE AND GYNAECOLOGIST: THE NEW RESULTS OF THE MISSION STUDY
M. Espié1, T. Chevallier2, J.-P. Daurès2, P. Mares3, M.-C. Micheletti4 and P. de Reilhac5
1Hôpital Saint-Louis, Paris, France; 2Laboratoire de Biostatistique, d'Epidémiologie et de Recherche Clinique, Montpellier, France; 3Service de Gynécologie Obstétrique, CHU Hôpital Caremeau, Nîmes, France; 4Laboratoire Théramex, Société de la Division Merck Serono, Monaco; 53 Place Ladmirault, Nantes, France
Objective: The MISSION study is a national historical-prospective study carried out in France by the National Federation of Medical Gynaecology Colleges (F.N.C.G.M.) (1) Its aim is to determine the prevalence (historical phase) and incidence (prospective phase) of the morbidity in postmenopausal women, under a gynaecologist's care, depending on whether or not they are treated with the Hormone Replacement Therapies (HRT) commonly prescribed in France (1). The results of the historical phase and the first follow up of the prospective phase have recently been published (2, 3).Here we present the new results of the prospective phase concerning the breast cancer after a long time HRT exposure.
Design and Method: The prospective phase started on 5 January 2004 and the cut-off date for the 2nd data collection was December 31, 2007 (Follow-up No. 2). Two groups were defined : Exposed Group – postmenopausal women on HRTs commonly prescribed in France or stopped ≤ 5 years previously-; Unexposed Group – never received HRT or stopped >5 years previously-.
Results: 6755 patients were initially included and the MISSION cohort of this prospective phase consisted of more than 5000 randomised patients : about half in the Exposed group and half in the Unexposed group.
The incidence of breast cancer was not significantly different in the Exposed group after an average treatment exposure close to 10 years compared to the Unexposed group.
Conclusion: At the end of the second prospective follow-up of the MISSION cohort, no increased risk of breast cancer was found in the Exposed patients compared to the Unexposed patients.
OR2-03
COMPARATIVE EFFECTS OF ORAL CONJUGATED EQUINE ESTROGENS AND MICRONIZED 17β-ESTRADIOL ON EPITHELIAL CELL PROLIFERATION IN THE POSTMENOPAUSAL BREAST
Charles E. Wood, Thomas B. Clarkson and J. Mark Cline
Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA
Objective: The goal of this study was to evaluate the effects of two widely used estrogen therapies, oral conjugated equine estrogens (CEE) and micronized 17β-estradiol (E2), on breast epithelial proliferation in a postmenopausal primate model.
Design & Method: Data from all available published studies of postmenopausal female cynomolgus macaques were collected and retrospectively analyzed. The primary outcome measure was breast epithelial proliferation determined by immunolabeling for the Ki67/MIB1 antibody. Nine studies were identified (4 CEE and 5 E2). All CEE studies used a woman's equivalent dose of 0.625 mg/d (n = 281), while E2 studies used woman's equivalent doses of 0.5 or 1.0 mg/d (n = 131). Statistical comparisons were limited to estrogen-treated and respective control groups within each study.
Results: Treatment with oral CEE resulted in an overall increase in breast epithelial proliferation of 75% that reached significance at p < 0.05 in 1 of 4 large parallel-arm studies. In contrast, treatment with oral E2 resulted in an increase in breast epithelial proliferation of 259% (all studies) to 330% (parallel-arm studies only) that reached significance at p < 0.05 in all 5 E2 studies evaluated. Increases in breast epithelial expression of progesterone receptor and endometrial thickness were similar following CEE and E2 treatment (p < 0.05 in all available studies). Where available, serum estrogen concentrations were comparable for CEE (0.625 mg/d) and E2 (1.0 mg/d).
Conclusion: This retrospective analysis suggests that standard doses of CEE result in several times less estrogen-induced proliferation in the postmenopausal breast compared to E2. Comparable effects on endometrial thickness and other estrogen-sensitive markers suggest that this difference in proliferation is not due simply to lower systemic estrogen exposure.
OR2-04
CORE NEEDLE BIOPSY IS A SAFE AND EFFICIENT METHOD FOR PROCURING MAMMARY EPITHELIAL TISSUE FROM HEALTHY POSTMENOPAUSAL WOMEN
D. Murkes3, K. Leifland2, L. Skoog1, E. Tani1, A. Beliard4, E. Lundström1 and G. Söderqvist
1Karolinska Hospital; 2St Göran Hospital, Stockholm, Sweden; 3Södertälje Hospital, Södertälje, Sweden; 4University of Liege, Belgium
Objective: The basis of risk for breast cancer associated with hormonal therapies may lie in the regulation of cell turnover.
For many years our group has used fine needle aspiration (FNA) biopsy for the evaluation of proliferation in the normal breast.
The material obtained by FNA biopsy has been sufficient to study proliferation in approximately 80% of women examined, but mostly the cellularity has been to low for simultaneous assessment of apoptosis and other parameters.
The purpose of this study was to enhance cellularity by using core needle biopsy (CNB) for evaluation of cell turnover in the breasts of healthy women.
Design and Methods: Eighty healthy women were recruited for core needle biopsy and randomized to sequential hormone therapy for two 28-day cycles with either 0.625 mg of oral Conjugated Equine Estrogens (CEE) or 2,5g of 0.06% (=1,5 mg) transdermal estradiol gel daily, with the addition of 5 mg of oral medroxyprogesterone acetate (MPA), or 200 mg progesterone daily, for the last 14 days of each cycle, respectively.
Percutaneous core needle biopsy and mammography was performed before treatment and during one of the last three days of the second 28 day treatment cycle. The stereotactic core needle biopsy was performed under local anesthesia, percutaneously, using a 2 mm needle in the upper outer quadrant of the left breast and normal breast tissue was procured for immunohistochemistry for analysis of markers of proliferation, apoptosis and sex steroid hormone receptors. Serum samples were drawn for analysis of hormone levels at baseline and on the day of the last biopsy.
Results: 77 women fulfilled the study according to the protocol. There were no adverse effects from the breast biopsies in any of the women. Data indicate a clearly higher epithelial cellularity in this material compared with FNA-biopsies performed in earlier studies.
Conclusions: The CNB- biopsy is a valuable tool for in vivo studies with immunochemistry in the normal postmenopausal breast. The greater needle diameter gives opportunities for a higher epithelial cellularity compared with FNA-biopsies performed earlier, with no increase in inconvenience or adverse effects.
OR2-05
DIFFERENTIAL EFFECT OF TESTOSTERONE ON SULFATASE ACTIVITY IN NON-MALIGNANT AND CANCEROUS BREAST CELLS IN VITRO
K. Kalkhake, M. Götte, L. Kiesel and P. Stute
University Clinic of Muenster, Muenster, Westfalia, Germany
Objective: Testosterone (T) is a therapeutic option for women with hypoactive sexual desire disorder. T may have an impact on the mammary gland by altering local estrogen synthesis. The aim of the study was to measure the effect of T on estrone-sulfate (E1S)-sulfatase (STS) expression and activity using hormone-dependent breast cancer cells with high and low aggressive potential (BT474, MCF7), and HBL100 as breast cell line of non-malignant origin.
Design & Method: Cells were incubated in RPMI 1640 medium containing 5% steroid-depleted fetal calf serum for 3d and subsequently incubated in absence or presence of T at 10(−8) and 10(−6)M at 37°C for either 24 h or directly in cell extracts (“direct”). STS protein expression was measured by dot blot (immunoblotting) and mRNA levels by rtPCR. STS activity was evaluated by incubating homogenized breast cells with [3H]-E1S. The products E1 and E2 were separated by thin layer chromatography. Analysis of variance (ANOVA) was applied for statistical analysis. A p-value < 0.05 was considered to be significant.
Results: STS mRNA expression did not reveal group differences. Basal and T treated STS protein expression was significantly higher in malignant compared to non-malignant breast cells. However, T did not induce significant intra cell line differences. Similarly, basal and T treated STS activity was significantly higher in malignant compared to non-malignant breast cells. In non-malignant HBL100 T inhibited STS activity significantly at 10(−6) and 10(−8)M after direct and 24 h incubation. In contrast, in BT474 direct incubation induced a significant reduction in local estrogen formation which was counteracted by cellular mechanisms of regulation after 24 h incubation.
Conclusion: The more aggressive the breast cell line the higher the local estrogen formation due to posttranscriptional and posttranslational effects on STS. T exerts a differential effect on STS activity in non-malignant and cancerous breast cells. However, the origin of breast cells has a greater impact on local estrogen formation than hormonal treatment.
OR2-06
THE EVOLUTION OF BREAST CANCER
Barry G Wren
Director, Menopausal Medicine Centre, Edgecliff, NSW Australia
Objective: To present evidence illustrating that the hundreds of genetic alterations involved in converting a normal breast cell into cancer have their origin in the same evolutionary matrix as provides the model for all variations in human life forms and that the majority of these mutations can be identified during the time the breast architecture is being developed in early adolescence.
Design and Method: Biological studies were reviewed to confirm biological evidence that malignant change follows the accumulation of hundreds of putative and can-gene mutations which are known to occur during stem cell division or which are passed as passenger mutations from one cell generation to the next. These genetic alterations in breast cells have now been categorized and involve a minimum of six essential changes to the cell homeostatic mechanism with each cancer accumulating up to 200 aberrant mutations producing a cell which functions in an atypical manner and which may take many years before it finally attains the capacity to invade normal tissue.
Results: A very large reservoir of pre-malignant cells has been detected in autopsy tissue obtained from pre-menopausal females, confirming that the abnormalities leading to invasive cancer originate in young women. Both clinical and biological studies confirm that when they reach the menopause up to 50% of women already have pre-malignant cellular atypia while autopsy studies confirm that between 5% and 20% of women have latent breast cancer.
When the normal homeostatic system of the breast is corrupted, colonies of aberrant breast cells have the potential to grow faster in the presence of sex hormones than the same type of abnormal cell deprived of oestradiol. Epidemiological studies conducted over five years have noted an increase in the diagnosis of breast cancer when combined hormone therapy is used and as a result it is regularly suggested that hormones actually initiate the cancer. However other studies fail to support his hypothesis. It is more plausible to postulate that hormones actively increase growth of those micro-invasive cancers which had been present prior to the menopause.
Conclusion: The mutations responsible for inducing breast cancer are first detected during adolescence when stem cells develop the mature breast architecture. These spontaneous mutations accumulate with inherited passenger mutations to produce an aberrant cell which acquires malignant capabilities as women age.
Breast cancer is an error of evolution.
OR2-07
EXPRESSION OF THE ANDROGEN RECEPTOR AND SYNDECAN-1 IN BREAST TISSUE DURING DIFFERENT HORMONAL TREATMENTS IN CYNOMOLGUS MONKEYS
M. Hofling1, B. von Schoultz1, L. Ma1, L. Sahlin1, C. Haglund2, S. Nordling2 and M. Cline3
1Department Of Obstetrics And Gynecology, Karolinska University Hospital, Stockholm Sweden; 2Department of Surgery and Pathology, University of Helsinki and Central University Hospital, Helsinki, Finland; 3Department of Pathology, Section of Comparative Medicine, Wake Forest University, Winston Salem, NC, USA
Objectives: To analyze the expression of Androgen receptor(AR) and Syndecan-1 in breast tissue during long-term hormonal treatment in cynomolgus monkeys.
Methods: 60 oophorectomized macacaques were randomized to receive either tibolone, conjugated equine estrogens (CEE), CEE + medroxyprogesterone acetate (MPA) or no hormonal treatment. Breast tissue was collected at necropsy after two years and stained for AR and Syndecan-1.
Results: Apparent differences were seen between treatment groups. AR expression was markedly increased by tibolone and supressed by CEE/MPA. Both treatments increased Syndecan-1 in stromal tissue whereas CEE alone had no significant effect.
Conclusions: We found alternative regimens for hormonal therapy to differ in their influence on two markers of importance for the development of breast cancer. The results may be relevant for the ongoing clinical discussion on the long-term safety of different hormonal treatments.
OR2-08
HORMONE THERAPY AND RISK OF BREAST CANCER: A RETROSPECTIVE ANALYSIS OF POSTMENOPAUSAL WOMEN FROM A LATIN AMERICAN CITY
P. R. Figueroa Casas and L. Rinesi
Centro de Ginecología, Rosario, Argentina
Objective: A prospective as well as some other retrospective studies performed in postmenopausal women mostly of Anglo-Saxon origin and living in the Northern Hemisphere showed an increase in the incidence of breast cancer associated with the use of Hormone Therapy (HT). The aim of the present study was to determine whether the same association was found among postmenopausal women living in a Latin American city of one million two hundred thousand inhabitants.
Design & Method: A review and updating of the clinical records of postmenopausal women attending a gynaecological ambulatory Center between 1976 and 2005 were carried out. Incidence of invasive and in situ breast cancer among HT users (estrogens, estrogens plus gestagens or both) and non-users was recorded. In patients with breast cancer, type of hormone received, HT treatment length, age at HT initiation and histological characteristics of the tumour were determined; HT treatment length was also established among those who developed breast cancer and those who did not.
Results: 1148 postmenopausal women were analysed, 611 (53.2%) HT users and 537 (46.8%) non-users. Both groups had similar basal characteristics. Invasive breast cancer was significantly higher in non users (11.4%) when compared with users (4.4%) (p < 0.01).
No significant differences were registered for in situ carcinoma (0.8% users vs. 0.9% non users). There were also no significant differences in the incidence of both cancers when the use of estrogens alone was compared with the use of estrogens plus gestagens.
Age at HT initiation and mean time of follow-up were similar for both groups. No significant histological differences in patients with breast cancer were found between HT users and non-users. HT administration length had no influence among women developing breast cancer and women who did not.
Conclusion: This study showed no increased incidence of invasive breast cancer among postmenopausal HT users when compared with non-users. Further studies of women sharing similar ethnic, environmental and cultural characteristics described in this study are needed to confirm these findings.
OR2-09
MAMMOGRAPHIC BREAST DENSITY ACCORDING TO DIGITIZED ASSESSMENT - EFFECT OF THE ISOPROPANOLIC EXTRACT OF BLACK COHOSH COMPARED TO TIBOLONE, CONTINUOUS COMBINED HT AND PLACEBO TREATMENT
E. Lundström, A. Lindén-Hirschberg and G. Söderqvist
Karolinska University Hospital, Stockholm, Sweden
Objective: The aim of this study is to determine the effects of the isopropanolic extract of black cohosh compared to continuous combined HT, tibolone and placebo treatment on mammographic breast density according to digitized assessment in healthy, naturally postmenopausal women.
Design & Method: From a prospective, open, uncontrolled drug safety study, a total of 64 women were treated with 40 mg black cohosh daily and from a prospective, randomized, double-blind placebo-controlled study a total of 145 postmenopausal women were randomized to receive either tibolone 2.5 mg (n = 49), estradiol 2 mg/norethisterone acetate 1 mg (E2/NETA) (n = 43), or placebo (n = 53). Mammograms were performed at baseline and after 6 month of treatment. All mammograms were digitized and breast density was quantified according to a data-based program.
Results: An increase in mammographic density was much more common among women receiving continuous combined hormone replacement therapy than among those receiving black cohosh, tibolone and placebo treatment. There were no differences at baseline. Mean values for the increase after 6 months for E2/NETA, tibolone, black cohosh and placebo were 14.3%; 2.3%; 1.4% and 0.3% respectively. The difference between E2/NETA, tibolone, black cohosh and placebo treatment was highly significant (p < .0001).
Conclusion: An increase in mammographic density should be regarded as an unwanted side effect of hormone replacement therapy. Since mammographic breast density should be regarded a continuous variable, the digitized method allows a more sensitive measurement. In contrast to estrogen/progestogen treatment, tibolone and black cohosh seem to exert little stimulation of breast tissue.
OR2-10
SPHINGOLIPID METABOLISM DEPENDS ON THE ESTROGEN RECEPTOR STATUS AND HAS PROGNOSTIC IMPACT ON BREAST CANCER
E. Ruckhäberle, A. Rody, U. Holtrich, T. Karn and M. Kaufmann
Department of Gynecology, J. W. Goethe-University, Frankfurt, Germany
Objective: The “sphingolipid rheostat” balances between pro-apoptotic ceramid and anti-apoptotic and growth promoting sphingosine-1-phosphate. Certain enzymes of the sphingolipid metabolism are linked to multidrug resistance. Knowledge of a context between sphingolipid metabolism and Estrogen receptor status as as well as sphingolipid's impact on breast cancer and its prognosis is limited.
Design and Methods: Gene expression of 43 proteins from this pathway was analysed in different subtypes of breast cancer using microarray data of 1269 tumor samples (test set n = 171; validation sets n = 1098). Subgroups were stratified according to ER, Her 2neu- and Top-II- α status and Ki67 level. Additionally survival analyses and immunohistochemistry were done.
Results: Significant differences for several genes of the sphigolipid metabolism were observed between ER positive and ER negative tumors. Glucosylceramidesynthase (GCS), dihydroceramidesynthases (LASS4, LASS 6) and acid ceramidase (ASAH1) were higher expressed in ER positive samples. In contrast, Sphingosine kinase 1 (SPHK1), ceramide galactosyltransferase (UGT8), and Ganglioside GD3-Synthase (ST8SIA1) displayed higher expression among ER negative tumors. Survival analysis revealed a worse outcome of patients with high SPHK1 expression. To avoid a confounding effect of the ER status we also restricted the analysis to 750 patients with ER positive tumors. Again a worse outcome was observed for tumors displaying high SPHK1 expression. While 75.8 ± 1.9% of the patients with tumors low in SPHK1 expression were free of metastasis at 5 years, this was the case for only 64.9 ± 3.6% of patients with tumors displaying high SPHK1 expression (p = 0.008). High LASS 6 expression in ER negative patients implied bad prognosis.
Conclusions: Our results reveal a distinct correlation between Sphingolipid metabolism and hormon receptor status. Alteration in this pathway have impact on the prognosis of breast cancer patients. Targeting the sphingolipid rheostat might open new treatment options.
Quality of life
OR3-01
ASSESSMENT OF QUALITY OF LIFE IN MENOPAUSE AND AGEING
A. Holte1,2 and E. Røysamb1,2
1Division of Mental Health, Norwegian Institute of Public Health, Oslo, Norway; 2Department of Psychology, University of Oslo, Oslo, Norway
Objective: Assessment of quality of life (QoL) has become an integrated part of both menopause research and treatment of menopausal symptoms. The International Menopause Society (IMS) Expert Workshop has therefore published a Position Statement on “Menopause and aging, quality of life, and sexuality” (Climacteric 2007; 10:88-96) suggesting methods of measurement of QoL. Unfortunately, the IMS statement neglects most of what has been learned through the past 25 years of QoL measurement development and research. The purpose of this paper is to inform researchers and practitioners about the state of art in the conceptualisation and measurement of QoL.
Design & Method: The paper defines QoL, reviews the QoL concept as it has been used in QoL research through the past 25 years, differentiates measures of QoL from measures of health outcome - which is frequently and falsely referred to in the menopause literature and by the IMS as measures of QoL.
Results: Ten different standard measures of QoL are listed, including VIA Signature Strengths Questionnaire, Authentic Happiness Inventory Questionnaire, Fordyce Emotions Questionnaire, General Happiness Questionnaire, PANAS Questionnaire, Gratitude Questionnaire, Optimism Test, Meaning in Life Questionnaire and the Satisfaction With Life Scale (SWLS). Psychometric properties of frequently used measures and addresses to relevant Internet sites about QoL and positive psychology are provided (http://www.authentichappiness.sas.upenn.edu/; http://www.psych.uiuc.edu/∼ediener/; http://www.isqols.org/; http://www.ube.com/watch?v=oGCKHX4Lr9o; http://www.youtube.com/watch?v=OtI-FDlrWf8). Well established QoL scales are illustrated with a case: SWLS is a short 5-item instrument designed to measure global judgments of satisfaction with one's life. The scale requires only about one minute of a respondent's time. The scale was developed in 1985 and is in the public domain (not copyrighted). It is therefore free to be used without permission or charge by all professionals (researchers and practitioners), as long as you give credit to the authors of the scale. The SWLS has – like several other scales – well established reliability and validity, is used in more than 40 countries and yields 392 publications in PsycInfo.
Conclusions: Systematic assessment of quality of life in menopause research and clinical practice should be evidence based and follow standard scientific procedures. The concept and methods of measurement suggested by the IMS Position Statement on “Menopause and aging, quality of life, and sexuality” does not hold scientific quality. A new and scientifically accountable International Menopause Society Position Statement on “Menopause and aging and quality of life”, is strongly needed.
OR3-02
CERVANTES SCALE: VALIDATION TO BRAZILIAN PORTUGUESE
J. E. M. Lima1 and M. C. O. Wender1,2
1Pós graduação Medicina: Ciências Médicas UFRGS, Porto Alegre, Brazil; 2Hospital de Clinicas de Porto Alegre, Brazil
Objective: Validate the Cervantes Scale from Spanish to Brazilian Portuguese.
Design & Method: Transversal study. Women between 45 and 64 years-old, from the Gynecology Unit of Faculdade de Medicina da Universidade de Passo Fundo and from 2 private clinics in the same city. We intend to interview 180 women, and here we describe the results of the first 60 women. Exclusion criteria are: impossibility to read the questionnaires and poor health state. The following questionnaires and scales are used: (1) Demography dates (2) The Cervantes Scale (3) Women's Health Questionnaire (WHQ) and (4) Abbreviated for the assessment of the Quality of Life of the World Health Organization) (WHOQOL-breef); notice that 3) and 4) are portuguese validated and are gold-standards. Cervantes Scale was translated as “back translation”. Some corrections were made after application of pilot study to 10 women. After 3 to 4 weeks a number of women are re-tested. After statistical analyses we describe demographic characteristics, internal consistency, Cronbach's alpha, confiability of test-retest, intra class correlation, and Pearson correlation coefficient.
Results: Mean age = 52 years-old (±5.2), 93% self described as white, scholarship as fundamental, high school or superior as 43%, 22% e 35%, respectively. 55% are still workers. Economic status as familiar income under US$ 1.000 (46%), between US$ 1.000 and 2.000 (35%) and more than US$ 2.000 (18%). 52% don't have any chronic disease, and 27% have hypertension. 87% are non smokers. 85% report no alcohol use. 33% of women describe to exercise regularly at least 3 times a week, and 40% are sedentary. 35% are in the premenopausal period without HT, and 6.7% use HT. 65% of the women never used HT, 15% interrupted HT, and 20% are HT users. 3.3% are oral contraception users. Natural menopause = 26.7%, surgical menopause in 21.7%. Menopausal symptoms are present in 80% of the women, hot flushes in 46.7%. Symptomatic women group had a score in Cervantes Scale of 50 (±23.6), and in the non symptomatic group the score was 20.2 (±12.6) CI 95% for both. Global Cronbach coefficient of Cervantes Scale was 0.893 and of the sub scales: menopause and health (0.824), psychological domain (0.825), sexuality (0.721) and couple relation (0.710). Cronbach's alpha for the WHQ and for the WHOQOL breef were 0.812 and 0.914 respectively. The Pearson correlation coefficient for the comparison of Cervantes Scale with WHQ and WHOQOL breef were r = 0.636 and r = −0.633 (p < 0.001).
Cervantes scale is a good questionnaire for women QOL evaluation during perimenopausal period, showing good psychometrics measurements. It is a sensitive scale, as it permits to evaluate other QOL dimensions, not only menopausal symptoms. The Scale also differentiates symptomatic from non symptomatic women.
OR3-04
EVALUATION OF THE EFFECTS ON THE QUALITY OF LIFE IN THE HYSTERECTOMIZED POST-MENOPAUSED WOMAN WITH THE USE OF THE SUBCUTANEOUS BIODEGRADABLE IMPLANT OF 17-BETA-ESTRADIOL BY THE WOMEN HEALTH QUESTIONNAIRE
J. SABINO PINHO and J. C. LIMA
Federal University of Pernambuco, Recife, Brazil
Objectives: The aim of the study was to investigate the effects of the subcutaneous biodegradable implant of 17-beta-estradiol on the quality of life in the post-menopaused hysterectomized women.
Material and Methods: Eighty three patients were included, of the which sixty concluded the study. The quality of life was appraised in a clinical opened and descriptive study along six months using the results of the Women Health Questionnaire.
Results: The quality of life got better significantly with the use of the estradiol implant when compared with the results before the treatment, with obtained them after 3 and 6 months after the insert of the implant, so much in the total score (before treatment = 58,1 – after 3 months = 42,3 * – and after 6 months = 43,1 *), as for its dimensions: anxiety (before treatment = 8,9 – after 3 months = 6,9 * – and after 6 months = 7,0 *), depression (before treatment = 12,1 - after 3 months = 9,0 * – and after 6 months = 9,2 *), somatic symptoms (before treatment = 18,1 – after 3 months = 14,3 * – and after 6 months = 14,3 *), vasomotors symptoms (before treatment = 7,1 – after 3 months = 3,0 * – and after 6 months = 3,2 *), cognitive function (before treatment = 6,6 – after 3 months = 5,2 * – and after 6 months = 5,3 *), sexual problems (before treatment = 6,8 – after 3 months = 5,3 * – and after 6 months = 6,2 **), sympathy (before treatment = 5,2 – after 3 months = 4,3 *** – and after 6 months = 4,5 ***) and sleep (before treatment = 4,6 – after 3 months = 3,4 * – and after 6 months = 3,6 *) with * p < 0,001, ** p < 0,01 and *** p > 0,05 (not significant).
Conclusions: The patients that make use of subcutaneous biodegradable implant of 17-beta-estradiol, for six months, present important relief of the climacteric symptoms and great improvement in the quality of life.
OR3-04
EVALUATION OF POSITIVE PROPERTIES AND SIDE EFFECTS OF ISOFLAVONES AND RALOXIFENE WITH RESPECT TO ITS POTENTIAL USE TO IMPROVE HEALTH OF POST MENOPAUSAL WOMAN
Renuka Sinha and P. Choudhry
Department of ObGy, Safdarjang Hospital, New Delhi, INDIA
Objective: The study was conducted in the department of ObGy at Safdarjang Hospital with the following objectives:
To evaluate the beneficial effects of Isoflavones and Raloxifene on Vasomotor symptoms, Lipid profile, breasts, uterine endometrium and Bones.
To study the side effects and complications of isoflavones and Raloxifene in post menopausal women.
To study the acceptability and compliance of Isoflavones and Raloxifene in post menopausal women.
Results: Analysis was done by Mann Whitney's test of significance or student's t-test or Fisher test were used wherever applicable. Complete abolition of vasomotor symptoms were observed in 40% group (B), 8% in (A) group and 24% in placebo group. Vulvo vaginal symptoms relief occurred in 24% with isoflavones, 28% in Raloxifene and 8% in placebo sexual symptoms relief in 8%(B), 16%(A) and 8% in(C.). There was no relief in musculoskeletal symptoms with placebo, 16% in B and 20% in A group. There was improvement in DEXA Bone densitometry determined T score with both Isoflavones and Raloxifene, but there was no improvement in placebo group. There was no significant increase in endometrial thickness in none of the groups. There was no significant change in mammography. There was a significant fall in total cholesterol and LDL with significant rise in HDL with Raloxifene, significant fall in total cholesterol and triglycerides with rise in HDL in Isoflavones group and no significant change in placebo group.
Conclusion: Isoflavones are more effective in abolishing vasomotor and urinary symptoms. Raloxifene is better in abolishing vulvo-vaginal, sexual, psychological and musculoskeletal symptoms. Both are good for Lipid profile. There was improvement in bone density with both the drugs and there was no change in breasts and endometrium. NO side effects were seen. The drugs were well tolerated.
OR3-05
HEALTH-RELATED QUALITY OF LIFE AFTER COMBINED HORMONE REPLACEMENT THERAPY: RESULTS OF THE WOMEN'S INTERNATIONAL STUDY OF LONG DURATION OESTROGEN AFTER MENOPAUSE (WISDOM) TRIAL
A. Welton1, M. Vickers1, J. Kim3, B. Lawton2, A. MacLennan4, J. Martin1 and T. Meade1
1The MRC General Practice Research Framework, London UK; 2Women's Health Research Centre, University of Otago, Wellington, New Zealand; 3London School of Hygiene and Tropical Medicine, London UK; 4School of Paediatrics and Reproductive Medicine, The University of Adelaide, Australia
The Women's Health Initiative showed that when combined HRT is commenced over 70 years of age the cardiovascular risk is increased and this result is confirmed by the WISDOM trial cardiovascular outcomes. However there are inadequate data about the effect of hormone replacement therapy (HRT) on HRQoL.
Objective: To assess the effect of combined hormone replacement therapy (cHRT) on Health-Related Quality of Life (HRQoL)
Design: Randomised placebo controlled double blind trial.
Setting: General practices in UK (384), Australia (94), and New Zealand (24).
Participants: Postmenopausal women aged 50–69 years at randomisation. 3,721 women with a uterus were randomised to combined oestrogen and progestogen (cHRT) (n = 1862) or placebo (n = 1859). HRQoL data at one year were available from 1,043 and 1,087 respectively.
Interventions: Conjugated equine oestrogens plus medroxyprogesterone acetate 2.5/5.0 mg or matched placebo orally daily for one year.
Main Outcome Measures: HRQoL and psychological well-being as measured by the Women's Health Questionnaire (WHQ), the EuroQol, the Visual Analogue Scale (VAS) and the Centre for Epidemiological Studies Depression Scale (CES-D). Changes in emotional and physical symptoms as measured by a menopause symptoms questionnaire.
Results: After one year of treatment, significantly fewer women reported vasomotor symptoms (P < 0.001), aching joints and muscles (P = 0.001), insomnia (P < 0.001), vaginal dryness (P < 0.001), and bloating (P = 0.005) in the cHRT group compared to the placebo group, but a greater proportion reported breast tenderness and vaginal discharge (P < 0.001). No significant differences in overall QoL were observed at one year using the VAS measure or the depression scale. Small but significant improvements were observed in sexual functioning (P < 0.001), and sleep problems (P < 0.001) for those taking cHRT using the WHQ. Hot flushes were experienced in the cHRT and placebo groups by 30 and 29% at trial entry and 9 and 26% at one year respectively.
Conclusions: cHRT when commenced many years post menopause improves health-related quality of life by improving sleep, sexual functioning and decreasing aching in joints and muscles.
Trial Registration: ISRCTN 63718836.
OR3-06
IS THERE RELATIONSHIP BETWEEN CYP17 POLYMORPHISM AND VASOMOTOR SYMPTOMS IN POSTMENOPAUSAL WOMEN?
A. M. Massad-Costa1, A. C. S. Myiati1, C. C. Gonçalves1, I. D. C. Guerreiro da Silva1, J. M. Soares-Jr1, M. A. Haidar1, K. Moraes1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil
Objective: To determine whether CYP17 polymorphisms in the estrogen synthesis and metabolism pathways are associated with women's vasomotor symptom after menopause.
Design and Methods: Participants were 96 women with a mean age of 52.1 ± 4.4 years, employed, married, and represented a multiethnic population. Genotyping was done for the CYP17 polymorphisms (heterozygote and wild type). Women registered their vasomotor symptom severity in card diaries.
Results: Women with the CYP17 polymorphisms (heterozygote and wild type) reported more severe and frequent hot flashes than women without the polymorphisms. The Relative Risk (RR) was 1.98 (1.08 to 3.61). When compared only Wild type with heterozygote type, there is not a significant difference, RR = 1.13 (0.69 to 1.83). The comparison between the Wild type and the normal patients the RR was 2.16 (1.09 to 4.28).
Conclusions: These findings suggest a possible role for CYP17 polymorphisms in the genesis of vasomotor symptoms after menopause.
OR3-07
QUALITY OF LIFE ASSESSMENT AMONG LATIN AMERICAN MIDDLE AGED WOMEN
Peter Chedraui, Eliana Ojeda, Juan E. Blümel, Monique Royer, Maria T. Espinoza, Desire Mostajo, Edwin Soto, Daniel Flores, German Baron, Gustavo Gomez, Alvaro Monterrosa, William Onatra, Daysi Navarro, Ascanio Bencosme, Andres Calle, Patricia Leon-Leon, Jose A. Hernandez-Bueno, Konstantinos Tserotas, Luis Danckers, Humberto Izaguirre, Eduard Mezones, Selva Lima and Emma Belzares†
†Collaborative Group for Research of the Climacteric in Latin America (REDLINC)
Background: Data provided from several Latin American studies indicate that quality of life (QoL) is impaired by the female climacteric; despite this, up-to-date, assessment of QoL using one validated tool has not been performed at large scale within this population.
Objective: To assess QoL among middle aged Latin American women with the Menopause Rating Scale and determine factors associated to its impairment.
Methods: In this cross-sectional study, 8,373 healthy women aged 40 to 59 years, accompanying patients to healthcare centers in 18 cities of 12 Latin American countries, were asked to fill out the Menopause Rating Scale (MRS) and a general socio-demographic questionnaire.
Results: Mean age of the entire sample was 49.1 ± 5.7 years (median 49), a 62.5% had 12 or less years of schooling, 48.8% were postmenopausal and 14.7% were on hormonal therapy (HT). Mean total MRS score (n = 8,373) was 11.3 ± 8.5 (median 10); for the somatic subscale: 4.1 ± 3.4; the psychological subscale: 4.6 ± 3.8 and the urogenital subscale: 2.5 ± 2.7. After logistic regression it was determined that having 49 years or more (OR: 1.78, 95 CI [1.56–1.94], p = 0.001), being postmenopausal (OR: 1.44, 95 CI [1.29–1.61, p = 0.001]), currently having a partner (OR: 1.30, 95 CI [1.15–1.46], p = 0.001), smoking habit (OR: 1.23, 95 CI [1.09–1.38], p = 0.001), and living in the altitude (OR: 1.29, 95 CI [1.09–1.35, p = 0.001]) were associated to having higher MRS scores ( ≥ 10, median) and thus impaired QoL. Coming from a country with a lower income was related to a lower risk for impaired QoL (OR 0.73 95% CI [0.65–0.81], p = 0.001).
Conclusion: To the best of our knowledge this is the first study to assess QoL in a large Latin American series in which impairment depended upon individual female characteristics and the demography of the studied population.
OR3-08
QUALITY OF LIFE IN SPANISH SPEAKING MEN AND WOMEN AFTER 40. ARE WE REALLY THAT DIFFERENT?
D. Legorreta1, D. Navarro2 and L. Danckers3
1LPA, México D.F., Mexico; 2Instituto Nacional de Endocrinología, La Habana, Cuba; 3Clinica San Pablo, Lima, Peru
Objectives: Women's QOL has been studied in most countries to evaluate possible impacts of the menopausal transition on the perception of wellbeing and other indicators of health-related QOL. However, no comparative study has been conducted to compare QOL perception in men and women aged 40 or more years of age to evaluate whether QOL is perceived differently by both sexes. This preliminary study was conducted to explore QOL psychological perception of: Current QOL (QOL), general wellbeing (WB), achievement (A), self-assurance (SA), emotional equilibrium (E), strength & stamina (SS) and general health (GH) in Spanish-speaking men and women 40 years old or older.
Methods: Comparative study of 343 Spanish-speaking subjects, 153 men and 190 women with mean age in the rank 45-49, range 40-70 from Mexico, Cuba, Peru, other American countries and Spain. Subjects answered the online questionnaire either in own pc or one provided by surveyors in Cuba and rural areas of Mexico. Online questionnaire contained 14 questions about perception of indicators enlisted above and a list of symptoms most related to QOL in aging and climacteric research literature. Subjects were asked to rate in a scale of 1 to 6 with 4 = Same, each indicator in comparison to level had before 40, and to rate current presence and/or degree of each symptom. Descriptives and chi-square tests were run.
Results: No statistical meaningful sex differences were found for any of the QOL indicators which were rated as same or slightly better than before 40 with the exception of SS and GH rated as slightly less than before 40 by both sexes. Sex/age differences were found with women's QOL rated as “slightly less than before 40” from 45-55 and men's decreasing after 59. Men's WB also decreases drastically after 59, while women's increases at same age. Symptoms differences (p > .005) were found for hot flashes, headaches, muscular pains and emotional unstability higher in women and sexual excitation problems in men.
Conclusion: Results show a positive perception of psychological but not health-related QOL after 40 with small but not meaningful differences between men and women's perceptions. Aging stages in both sexes differ in QOL perception with perimenopause in women and retirement in men being critical.
OR3-09
SLEEP AND MENOPAUSE – DO POSTMENOPAUSAL WOMEN SLEEP WORSE THAN PREMENOPAUSAL WOMEN?
Päivi Polo-Kantola1,2, Nea Kalleinen1, Sari-Leena Himanen3, Paula Alhola1,4, Atte Joutsen3, Anna S. Urrila5 and Olli Polo1,6
1Sleep Research Unit, Department of Physiology, University of Turku; 2Department of Obstetrics and Gynaecology, Turku University Central Hospital; 3Department of Clinical Neurophysiology, Tampere University Hospital; 4Department of Psychology, University of Turku; 5Department of Physiology, University of Helsinki; 6Department of Pulmonary Diseases, Tampere University Hospital, Finland
Objective: Questionnaire studies indicate that postmenopausal women suffer more from disturbed sleep than premenopausal women1. However, polysomnographic studies have failed to demonstrate consistent sleep changes behind the symptoms. The objective of this study was to examine the evolution of sleep in three cross-sectional populations: young, premenopausal and postmenopausal women. Further, to study the associations between sleep, menopause, mood and cognitive performance.
Design and Method: 21 premenopausal (45–51 years), 29 postmenopausal (59–71 years) and 11 young (20–26 years) women were recruited through newspaper advertisements. Polysomnography was used to measure objective sleep quality. Subjective sleep quality, sleepiness and mood were assessed using questionnaires. Three attentional test were used to investigate cognitive performance.
Results: Total sleep time in pre- and postmenopausal women was similar, but shorter than in young women (P = .030 and < .003, respectively). Sleep efficiency followed the same pattern, being 84.3% in premenopausal (P = .027), 80.2% in postmenopausal (P < .003) and 93.4% in young women. Pre- and postmenopausal women had less slow wave sleep (duration and activity) and more wake time after sleep onset (duration and frequency). Insomnia complaints were more frequent after menopause (P = 0.023). Sleepiness and mood scores were similar in all groups. Reaction speeds slowed with increasing age. After menopause, better cognitive performance was associated with more rapid eye movement sleep.
Conclusion: The differences in objective sleep measures between postmenopausal and young women are not due to rapid changes across menopause, since similar sleep characteristics are already present in premenopausal women. The increase of sleep complaints after menopause is not associated with sleepiness or disturbances in objective sleep quality, mood or cognitive performance.
Gynecological cancersd
OR4-01
ENDOMETRIAL POLYPS IN POSTMENOPAUSAL WOMEN
A. P. Domingues, H. Lopes, I. Dias and C. Freire de Oliveira
University Hospitals from Coimbra, Portugal
Introduction: Origin and pathogenesis of endometrial polyps are still unknown but they are assumed to be a risk factor for the development of endometrial tumours. If their treatment in symptomatic women is unanimous (surgical removal), in asymptomatic women is arguable.
Objective(s): To evaluate the risk of malignancy within endometrial polyps in post menopausal women.
Design & Methods: A hysteroscopy database was used to select postmenopausal women who underwent between 2004 and 2007 a diagnostic hysteroscopy and were diagnose with endometrial polyps. The medical records of the 482 women selected were reviewed and histological diagnoses of extracted polyps were assessed.
Results: Of the 482 women diagnosed with endometrial polyps in diagnose hysteroscopy, 50.8% were asymptomatic and the others 49.2% had postmenopausal vaginal bleeding. The mean age at diagnose was (asymptomatic vs symptomatic) 62.6 ± 8.5 vs 62.9 ± 9.7 years and menopausal mean age was 49.9 ± 4.3 vs 49.6 ± 4.3 years. The results of transvaginal ultrasound previously performed were endometrial thickness in 60.4 vs 56.9%, polyp in 37.6 vs 33.3%, endometrial tumour in 1.2 vs 0.8% and submucousal myoma in 0.8 vs 2.1%. Around 60 vs 68% of the polyps were removed (in other cases removal was not performed due to the small size of the polyp, being these women in a regular surveillance or in women who are expecting surgical removal) and their histopathologic diagnoses were mucous polyps in 93.2 vs 81.5%, endometrial tumours in 0 vs 8% (p < 0.0001), normal endometrium in 2.1 vs 0.6%, cystic atrophy of the endometrium in 1.4 vs 0.6%, cystic hyperplasia in 1.4 vs 4.9%, atrophic endometrium in 0.7 vs 0.6% and submucousal myoma in 0.7 vs 3.1%.
Conclusions: Risk of malignancy within endometrial polyps in post menopausal women varies with the presence of vaginal bleeding, being null in asymptomatic women. In asymptomatic postmenopausal women with endometrial polyps confirmed by hysteroscopy, transvaginal ultrasound or diagnostic hysteroscopy in a regular surveillance scheme are options to surgery, being a safe procedure and reducing surgical morbidity.
OR4-02
Minihysteroscopic (2,9 mm office hysteroscope) evaluation of endometrial hyperplasia in menopausal women
Krzysiek Józef, Milewicz Tomasz, Zmaczyński Andrzej, Wyroba Jakub, Kacalska Olga, Rajtar-Ciosek Agnieszka, Stachura Jerzy, Szpor Joanna, Bereza Tomasz, Kmita Bożena, Banaś Tomasz, Basta Antoni and Jędrzejczyk Anna
Jagiellonian University Medical Faculty, Cracow, Poland
Objective: Diagnostic minihysteroscopy, recently used 2,9 mm histeroscope, is an accepted as a standard out-patient investigation for diseases involving the uterine cavity.
Design & Method: Diagnostic minihysteroscope 2,9 mm with 30° angle (Storz) and Bettocchi 4,3 operative 4,3 mm, both used without general anesthesia. Eclia Roche kits for serum estradiol, testosteron, DHEAS and Ca125 estimations, microELISA for insulin estimation, immunohistochemistry for estrogen receptor alfa and beta as well as progesterone receptor and protein p53 tissue expression.
Materials: 114 women with abnormal uterine bleedings or ultrasonographically diagnosed endometrial hyperplasia.
Results: Endometrial polyps were found in 48,2% of egzamined women with abnormal uterine bleedings or ultrasonographical suspition of endometrial hyperplasia (mean serum 17β-E2 level in women with polyps was 61,8 pg/ml; being < 50 pg/ml in 16 cases with atrophic endometrium). Mean age of these women did not differ from the whole group (54,1 ± 7,5 yrs) whereas mean age in patients with atypia or adenocarcinoma was 64,9 ± 7,4 yrs (p < 0,01) and mean body weight 74,7 ± 13,0 kg, and mean BMI was 27,4 ± 7,4. Simple endometrial hyperplasia was diagnosed in 31,2% of women; the composed without atypia in 3,2%, cervical polyps in 8,9%, and hyperplasia with atypia or endometrial cancer in 8,6% of women.
In a group of 27 women with endometrial hyperplasia the expression of estrogen receptor alpha and beta as well as progesterone receptor and protein p53 have been estimated by the use of immunohistochemical methods. Only 6 specimens showed estrogen receptor alpha expression (statistically younger, overweighted women – mean age 49,0 ± 1,6 yrs and a 74 yrs old woman with endometrial cancer), two specimens showed estrogen receptor beta expression (endometrial carcinoma in 74 yrs old woman and 48 yrs old woman with polypous endometrial hyperplasia without atypia), and in all cases the expression of progesterone receptors was present. Protein p53 was found in 10 bioptic material from relatively younger women (three of them with endometrial carcinoma).
Conclusion: The relation between serum estrogen level as well as BMI and the presence of endometrial hyperplasia by both minihysteroscopy (2,9 mm office hysteroscopy) egzamination and histological evaluation of bioptic specimens have been confirmed.
The estrogen receptor alpha as well as protein p53 expression was observed mainly in younger women whereas endometrial atypia was found in older women with metabolic syndrome (high BMI, NIDDM, arterial blood hypertension).
OR4-03
POSTOPERATIVE RESULTS OF MODIFIED SURGERY IN VULVAR CANCER AND SURVIVAL ANALYSIS OF SQUAMOUS CELL CARCINOMAS OF THE VULVA IN A USA AND A EUROPEAN INSTITUTIONS
Carmen Bárcena1, Elisa Lopez-Varela2, A. K. Goodman3, Arlan F. Fuller Jr.4, Juan José de la Troca5 and Ricardo Sainz de la Cuesta6
1,6Department of Obstetrics and Gynecology, Hospital Quirón Madrid, Spain; 2,3,4Division of Gynecologic Oncology, Massachusetts General Hospital, Boston, USA; 5Universidad Autónoma de Madrid, Spain
Objectives: 1. To report postoperative complications after modified vulvectomy (MV) ± inguinofemoral lymphadenectomy (LND) in patients with vulvar cancer. 2. To assess survival of patients specifically with squamous cell carcinoma.
Design & Method: From 1996 to 2004, ninety-five patients underwent a MV ± LND at two different University Hospitals in USA and Europe. A retrospective chart review was performed documenting patient and tumor characteristics, associated pathology, postoperative complications, hospital stay, adjuvant therapy and follow-up. Survival information was extracted from the 72 patients with squamous cell histology and tested using Kaplan-Meier and Cox-regression analyses.
Results: The mean age was 69 y.o. Thirty-seven (39%) surgical complications were observed: vulva infection (14%), groin infection (6%), lymphocyst formation (11%), lymphedema (5%) and wound breakdown (4%). The mean hospital stay at the American center was 10 days and at the European hospital 5 days; p = 0.08 (Mann-Whitney test). For the squamous cell carcinoma, the mean overall survival was 68 months, not reaching the median. The 5-year survival by stage was 86% (I), 65% (II), 55% (III) and 49% (IV); p = 0.05. Twenty-six (41%) patients with LND had positive lymph nodes (LN). The mean overall survival of patients with positive LN was 58 months vs. 80 months in patients with negative LN; p = 0.05. In multivariable analyses, positive LN, tumor size (HR = 1.16; p = 0.008), depth of invasion (HR = 1.06; p = 0.025) and radiotherapy (5-year survival was 40% in the radiated group vs. 72% in the non-radiated; p = 0.03) were independent factors for decreased survival. Grade and positive margins were not correlated with reduced survival in this group of patients.
Conclusion: MV ± LND has a low morbidity and reduced hospital stay for patients with vulvar cancer. Poor prognostic factors for patients with squamous cell carcinoma of the vulva were stage, positive LN, tumor size, depth of invasion and postoperative RT. We found no differences between USA and European institutions.
OR4-04
POSITIVE PAP TEST IN POSTMENOPAUSAL WOMEN – RESULTS OF THE NATIONAL CERVICAL CANCER SCREENING PROGRAM IN POLAND IN THE COURSE OF ONE YEAR
M. Spaczynski1,3, E. Nowak-Markwitz1, W. Kedzia1 and P. Seroczynski2
1Universisty of Medical Science Poznan, Poland; 2ABG SPIN, Warszawa, Poland; 3Centre of National Cervical Cancer Screening Program, Poznan, Poland
Objective. In 2007, the Polish Cervical Cancer Screening Program was started. The Polish National Health Found has issued 4.600.000 personal invitations for women between 25–59 years old. 685.760 (14,9%) women have accepted the invitation and undergone the test. 241.629 (35,2%) of them were postmenopausal. The aim was to check whether postmenopausal female population differs from the premenopausal one in PAP test diagnosis.
Design & Method. We have analyzed the results of the positive PAP test in women aged 50-59, who in 2007 took part in the National Cervical Cancer Screening Program.
We have used database SIMP information and performed the statistical analysis.
Results:. 5275 (2,18%) postmenopausal women have been diagnosed with positive PAP test and they accounted for one third of patients who had taken the test. The comparison between postmenopausal women and the whole tested population is shown in the table below. The distribution of PAP test diagnosis differs significantly between women aged 50-59 and 25-49 regarding squamous cell carcinoma, LSIL, HSIL and AGC. In the remaining groups (ASC-US, ASC-H and adenocarcimoma) the differences have not proven to be statistically significant.
Table 1 Positive PAP smear in women in Cervical Cancer Screening Program in 2007
Conclusion: Postmenopausal women constitute a particular, disadvantageous group of patients in PAP test evaluation, especially with regard to squamous cell carcinoma and AGC.
OR4-05
SIGNIFICANCE OF ENDOMETRIAL THICKENING IN ASYMPTOMATIC POSTMENOPAUSAL WOMEN
R. P. Woolas, M. Anderson, D. A. Brinkmann and A. S. Talaat
Department of Gynaecological Oncology, St. Mary's Hospital, Portsmouth, United Kingdom
Background: The measurement of endometrial thickness (ET) by transvaginal sonography (TVS) is a recognised screening tool for further investigation of women presenting with post menopausal bleeding.
Objective: To evaluate the significance of an ET >10 mm amongst asymptomatic women between 50 and 74 years of age participating in the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS).
Design and Methods: 4650 women who accepted an invitation originally generated by the population age sex register, were subsequently randomised to annual TVS. The examination was performed at the Portsmouth UKCTOCS screening centre. Any woman found to have an ET >10 mm was referred for clinical evaluation.
Results: Over 5 years 18201 scans were performed on 4650 women. 169 individual women were found have an ET >10 mm. Subsequent histopathological investigation revealed that 15 (8.8%) of these women had serious progressive pathology. 3 had severe atypical hyperplasia, 11 primary endometrial cancer and 1 a secondary breast tumour.
Conclusion: An incidental finding of an ET >10 mm in a post menopausal women merits a gynaecological consultation and consideration of an invasive test.
The pre-clinical detection of endometrial cancer or precursor lesions may be an additional benefit to screening for ovarian cancer by TVS amongst post menopausal women.
OR4-06
XBAI POLYMORPHISM OF ALPHA ESTROGEN RECEPTOR IN ENDOMETRIAL CANCER
Tomasz Stetkiewicz and Tomasz Pertynski
Clinical Department of Gynaecology and Menopausal Diseases, Polish Mother's Memorial Hospital – Research Institute, Lodz, Poland
Aim of Study: Evaluation of alpha estrogen receptor XbaI polymorphism influence on endometrial cancer risk.
Material and Methods: Endometrial samples from 102 women with endometrial cancer (endometrioid type) and 100 samples from controls. DNA was isolated according to standard methods. Selected DNA fragments were amplified using PCR reaction (MJ Research, INC thermal cycler, model PTC-100 (Waltham, MA, USA)), treated with restricting enzymes and finally electrophoresis was performed.
Results: We found almost three times decreased risk of endometrial cancer in homozygotes XX (C/C) and almost two times increased risk in heterozygotes Xx (C/T).
Conclusion: XbaI polymorphism of alpha estrogen receptor can influence endometrial cancer risk.
Sexuality and ART in female
OR5-01
A NEW ASSESSMENT TOOL TO MEASURE THE EFFICACY OF A TESTOSTERONE PATCH FOR TREATMENT OF HYPOACTIVE SEXUAL DESIRE DISORDER (HSDD) IN SURGICAL MENOPAUSAL WOMEN: THE BRIEF PROFILE OF FEMALE SEXUAL FUNCTION© (B-PFSF©)
A. Schwenkhagen1, S. Palacios2, A. Graziottin3, S. Kingsberg4, L. Derogatis5, S. Schmitt6 and C. Rodenberg6
1Gynecologicum, Hamburg, Germany; 2Instituto Palacios, Madrid, Spain; 3Center of Gynecology and Medical Sexology, H. San Raffaele Resnati, Milan, Italy; 4University Hospitals of Cleveland, Cleveland, USA; 5Center for Sexual Medicine Sheppard Pratt, Baltimore, USA; 6Procter & Gamble Pharmaceuticals, Mason, Ohio, USA
Objective: Quantify the clinical response to testosterone patch treatment and identify what score changes of this new short assessment tool are associated with patients' experience of a meaningful benefit.
Design & Methods: A representative sample of 132 surgically menopausal women with HSDD from two randomized, placebo-controlled trials (INTIMATE SM1 + 2; N = 1094) assessing efficacy and safety of the testosterone patch (300 mcg/day) over 24 weeks was interviewed at study end, prior to unblinding, to determine whether or not a meaningful treatment benefit was experienced. B-PFSF©score values for both baseline and week 24 assessments were compared between the groups that experienced a meaningful benefit or not using a covariance analysis (ANCOVA). ROC analysis was conducted to ascertain what B-PFSF© score changes were associated with experiencing a meaningful treatment benefit and to identify the optimal threshold differentiating between the two groups. The proportion of women on testosterone meeting the threshold criteria were compared to that on placebo in the SM trials.
Results: The score for the earlier published B-PFSF© HSDD screening questionnaire ranges from 0–35 with a score of ≥ 20 corresponding to a non-HSDD state. In this analysis the baseline B-PFSF© scores for patients experiencing a meaningful treatment benefit were similar to those for patients not experiencing a meaningful benefit (mean scores 10.0 and 9.5 respectively) and were consistent with an HSDD state. After 24 weeks of treatment with testosterone or placebo, mean score levels for patients reporting a meaningful treatment benefit were 21.1 (SE 1.0(corresponding to a non-HSDD state, while patients not responding to treatment showed almost no change in mean score value (11.4 (SE 0.8(). ROC analysis showed the B-PFSF© to have excellent discriminatory ability (AUC = 0.84). Sensitivity and specificity analysis suggested a score change of ≥ 5 to best classify patients as experiencing a meaningful treatment benefit. Application of the B-PFSF© to the intent-to-treat population of the SM 1 + 2 trials showed significantly greater score changes in patients randomized to testosterone as compared to placebo patients (p < 0.006), significantly more patients in the testosterone group returned to a non-HSDD state (34% vs. 22%, p < 0.0001) and had a score change of ≥ 5 (55% vs. 36%, p < 0.0001) corresponding to a treatment effect that was meaningful to the patient.
Conclusion: The easy-to-use B-PFSF© questionnaire will enable physicians not only to screen for women that may suffer from HSDD but also to validate HSDD patients' feedback on meaningful treatment response with testosterone.
OR5-02
ASSESSING THE IMPACT OF A SCREENING TOOL IDENTIFYING WOMEN WHO MAY BENEFIT FROM ASSESSMENT FOR HYPOACTIVE SEXUAL DESIRE DISORDER (HSDD) IN A COMPUTER LITERATE POPULATION ACCESSING A MENOPAUSE WEBSITE
H. D. Currie1, G. P. Cumming2 and A. J. Lee3
1NHS Dumfries and Galloway, Dumfries, Scotland, UK; 2NHS Grampian, Elgin, Scotland, UK; 3University of Aberdeen, Aberdeen UK
Objective: To assess the impact of a screening tool identifying women who may benefit from assessment for HSDD using the internet.
Design and Method: A questionnaire including the Brief Profile of Female Sexual Function screening tool (B-PFSF) was offered on the independent UK based, patient-tailored, clinician-led menopause website www.menopausematters.co.uk. The anonymous responses of the website users were then analysed.
Results: 1323 responses were obtained between 29/8/07 and 13/12/07 with 1113 respondents completing the B-PFSF. 13% classified themselves as being premenopausal, 61% perimenopausal and 26% postmenopausal. Overall 71%, (n = 791) screened positive on the B-PFSF (scoring 20 or less). There was no significant difference in scores between women who classified themselves as having had a natural or surgical menopause (p = 0.7). However, there were significant differences in score across menopausal status categories (p < 0.001). Postmenopausal women were more likely to screen positive than both perimenopausal women (79% versus 71% respectively, p = 0.013) and premenopausal women (58%, p < 0.001). The median (interquartile range) B-PFSF score for the 3 groups were 19 (12.7–28), 15 (10–22) and 13 (7–18) for premenopausal, perimenopausal and postmenopausal respectively (p < 0.001).
A previous postal study1 has suggested that European women who have undergone surgical menopause are more like to suffer HSDD than those who have not and that HSDD ranges from 7% in premenopausal women to 16% in younger surgical menopausal women. In this computer literate population, using a validated screening instrument, there was no significant difference in the percentage of women screening positive for HSDD between the natural menopause and surgical menopause groups. However, overall, there was a high prevalence of women screening positive and therefore a higher prevalence of HSDD could be expected. Women who were not postmenopausal have completed the questionnaire and also screen positive thus potentially increasing unnecessary physician consultation.
Conclusion: Websites are being increasingly designed for interactive online assessments. The B-PFSF was designed for use as a screening tool for postmenopausal women to determine whether to seek evaluation for HSDD. Computer literate women accessing menopausal websites utilising the B-PFSF elevate the prevalence of women screening positive. Scores in women who were not postmenopausal suggested a prevalence of pathology justifying validation of a screening tool in these groups to optimise physician consultation and patient quality of life.
OR5-03
BENEFITS AND RISKS OF TESTOSTERONE USE BY POSTMENOPAUSAL WOMEN
W. Somboonporn1, R. J. Bell2 and S. R. Davis2
1Khon Kaen University, Khon Kaen, Thailand; 2Monash University, Melbourne, Australia
Objective: Whether adding testosterone (T) therapy to conventional postmenopausal hormone therapy (HT) is effective or safe is unresolved. Therefore, we aim to determine the efficacy and safety of testosterone therapy for postmenopausal women using HT.
Design & Method: We searched the Cochrane Menstrual Disorders and Subfertility Group register of trials, the Cochrane Library, MEDLINE, EMBASE, Biological Abstracts, PsycINFO and CINAHL through to 1st November 2006. Published information was supplemented by contact with experts in the field. Studies were selected for inclusion if they were randomized controlled trials of T plus HT versus HT alone. Data on study design, characteristics of participants and treatment outcomes were independently abstracted by 2 investigators using a standardized protocol and trials were rated for quality based on established criteria. For dichotomous outcomes, a Peto odds ratio and its 95% confidence interval was calculated. For continuous outcomes, non-skewed data from valid scales were synthesized using a weighted mean difference or standardized mean difference. If statistical heterogeneity was found, a random effects model was used, and reasons for the heterogeneity were explored and discussed.
Results: Twenty-six studies involving 3881 participants were included in the meta-analysis. When compared with HT alone, the T plus HT was associated with significant increases in the frequency of all sexual events, the number of satisfying events and orgasms and increased self-reported desire, arousal pleasure and sexual self-esteem. T therapy was associated with greater reporting of acne and increased facial and body hair growth. Oral T significantly increased LDL cholesterol (weighted mean difference (WMD) 10.39 mg/dL, 95%CI 1.46 to 19.32) and lowered HDL cholesterol (WMD -18.63 mg/dL, 95%CI -22.18 to -15.08) whereas transdermal T only had a modest effect. Treatment with T was not associated with a difference in the overall discontinuation rate.
Conclusion: The addition of T to postmenopausal HT is associated with improved self-reported sexual function with the main adverse effects being increased reporting of acne and hair growth, not manifest as a greater study discontinuation rate. Significant adverse lipid effects were primarily seen with oral T.
OR5-04
CARDIOVASCULAR EFFECTS OF TESTOSTERONE TRANSDERMAL PATCH TREATMENT IN POSTMENOPAUSAL WOMEN EITHER ALONE OR IN COMBINATION WITH HORMONE REPLACEMENT THERAPY
P. Collins1, C. Vitale1,3, J. C. Stevenson1, I. Lodhi2, C. A. Rodenberg2 and G. M. C. Rosano3
1Imperial College London, Royal Brompton Hospital, London, UK; 2Procter & Gamble Pharmaceuticals, Mason, Ohio, USA; 3IRCCS San Raffaele, Rome, Italy
Objective: Testosterone transdermal patch (TTP) has been developed for the treatment of postmenopausal women (PMW) with hypoactive sexual desire disorder (HSDD). Since the cardiovascular (CV) effects of testosterone in women are still unclear we conducted a pooled analysis of the large phase III clinical program to evaluate the efficacy and safety of 300 μg/day TTP, alone or in association with hormone replacement therapy (HRT), versus placebo in surgical or natural PMW.
Design & Methods: A total of 2795 women aged between 26–70 years (mean age 52 (SD = 6.8) years) were included in 5 phase III randomized, double-blind, placebo-controlled clinical trials (treatment duration range 24 - 52 weeks) as part of the TTP Clinical program. Four studies included PMW (natural and surgical, two each respectively) receiving HRT while one study was conducted without HRT in either surgical or natural PMW. Women with known CV disorders were excluded from the studies. Changes from baseline in standard metabolic and cardiovascular risk factors were compared using an analysis of variance (ANOVA) or Van Elteren test adjusted by study. The incidence of stroke, myocardial infarction (MI) and venous thromboembolism (VTE) alone or as a composite CV endpoint was assessed.
Results: The 2795 PMW were randomized to receive either placebo (n = 1297) or TTP (n = 1498). Baseline mean BMI was 27 kg/m2 (SD = 5.3 kg/m2) and 56% were naturally menopausal. The demographic and baseline parameters were similar among the treatment groups. No significant changes in cardiovascular risk factors (total cholesterol, triglycerides, insulin, glucose, systolic and diastolic blood pressure) were detected during the study period apart from a blunting by TTP of the increases in HDL-C at 24 and 52 weeks (placebo 52-week mean change 2.59 mg/dl vs. TTP 52-week mean change 1.20 mg/dl, p < 0.005) and of the decrease by TTP in LDL-C at 24 (p < 0.05) but not at 52 weeks. During the double-blind, placebo-controlled period of the combined studies, 4 major cardiovascular events (2 MIs and 2 strokes) were reported in placebo patients and 3 (2 MIs and 1 stroke) in those receiving TTP. One VTE occurred in a patient receiving TTP and HRT.
Conclusion: TTP therapy in these clinical trials did not adversely affect cardiovascular risk profile and did not change the risk of major cardiovascular events in these surgical and naturally PMW with or without concomitant HRT.
OR5-05
EFFECTS OF ADJUVANT THERAPIES FOR BREAST CANCER ON SEXUAL FUNCTIONING AND RELATED DETERMINANTS
R. E. Nappi1, G. Moggio2, P. Sgandurra2, E. Peano2, D. Marenco2, F. Maggiorotto2 and N. Biglia2
1Research Center for Reproductive Medicine, Gynecological Endocrinology Unit, University of Pavia, Italy; 2Academic Department of Oncologic Gynaecology, University of Turin, Italy
Objective: Breast cancer and its treatment can negatively impact a woman's sexual functioning. Moreover, abrupt estrogen deficiency following chemotherapy and/or hormonal therapy may play a role.
The aim of this study is to evaluate the effects of breast cancer treatment on sexual functioning and related factors, as menopausal symptoms, physcological status and Body Image, in premenopausal or early postmenopausal women.
Design and Methods: The sample is composed of women in premenopause candidate for chemotherapy and/or hormonal therapy with GNRH analogs after primary surgery for breast cancer. Validated questionnaires are used to explore sexual function (MFSQ, CSDS), partner relationship (DAS), menopause symptoms (GCS), depression (BDI) and Body Image (BAT). Questionnaires have been proposed after surgery (T0), after the end of adjuvant chemotherapy or after at least 6 months of hormonal treatment (T1); a further evaluation is planned 1 year after surgery.
Results: Preliminary data of T0 and T1 visits are available for 21 (mean age 45,5 ± 3,2). All of them were forced to iatrogenic menopause using chemotherapy or GnRH analogues. Low levels of sexual function have been registered at baseline; a further decrease in sexual activity and sexual feeling with partner was demonstrated after 6 months of therapy. At T1, explicit erotic cues, typical of male sexuality, were even less effective in exciting libido; on the contrary, romantic cues increased their power in inducing sexual desire. We found a tendency to depression, highly related to loss of desire. Compared to baseline, also anxiety increase significantly (p = 0,04). Not significant deterioration of body image was demonstrated, because 90,4% of women had conservative surgery. Women are more concerned about body size, probably due to weight gain occurring after chemotherapy.
Conclusion: These preliminary data show that adjuvant therapy inducing premature menopause cause an important decline in sexual functioning of young women with breast cancer.
OR5-06
EVALUATION OF TREATMENT SATISFACTION AND IMPROVEMENT OF CLINICAL ENDPOINTS IN WOMEN RECEIVING LONG-TERM TESTOSTERONE IMPLANT TREATMENT
J. Studd1, S. Schmitt2 and K. Worley2
1London PMS and Menopause Centre, London, UK; 2Procter & Gamble Pharmaceuticals, Mason, Ohio, USA
Objective: Testosterone (T) is becoming more widely prescribed for women with sexual desire problems after European approval of an easy-to-administer Transdermal Testosterone Patch for surgically menopausal women with hypoactive sexual desire disorder (HSDD) receiving estrogen. For many years UK physicians have inserted T implants in women complaining of loss of sexual desire. This evaluation summarizes the long-term treatment experiences of women using T implants with respect to general and sexual health, partner relationship and T-related adverse events.
Design & Methods: A total of 306 patients aged 20–83 years (mean 58yrs) from a Menopause-specialists practice who were current or past users of testosterone implants completed a mailed questionnaire on general and sexual health outcomes, relationship and overall treatment satisfaction after written consent. A case series approach was used to summarize the women's reported experiences with T therapy versus prior T usage. Limitations of this survey are response bias, lack of control group and use of non-validated questionnaires.
Results: Mean T implant treatment duration was 103.8 months or 8.7 years among the total of 306 women of whom 7.5% were premenopausal, 57.5% naturally menopausal (NM) and 34% surgically menopausal (SM). 72% were still on treatment at time of evaluation. At least 78% of women used estrogens (E), with most starting before T treatment. Irrespective of age or menopausal status 89% of women reported an overall satisfaction with T treatment, with the highest rate reported by SM women (90%). Regarding change of general and sexual health endpoints since initiating T-therapy, 75% of those afflicted reported improvements in sexual desire, mood, depression and flushes/sweats respectively, 65% reported improved fatigue, 60% better concentration and 67% better self confidence. Among the E + T treated women 75% reported a better general level of health with T compared to the time prior to testosterone intervention. 55% of all women reported a positive impact of T treatment on their personal relationships, with the group of surgically menopausal women presenting the highest impact (59%). Only 35 cases of possible T-related side-effects were reported: hair loss (4), unwanted hair growth (11), acne (3), voice deepening (3), excessive libido (9) and uncharacteristic sexual behaviour (5), 89% of them being mild or moderate.
Conclusion: Women on long-term treatment with testosterone implants report a clear benefit with respect to various symptoms of sexual and general well-being as well as a positive impact on their personal relationships. These positive effects await confirmation from controlled clinical trials.
OR5-07
IMPROVEMENTS IN LIBIDO, PSYCHOLOGICAL AND GENERAL WELLBEING WITH TESTOSTERONE GEL IN OOPHRECTOMISED AND NON-OOPHRECTOMISED POSTMENOPAUSAL WOMEN
S. Taher1,2, C. Rothon1, N. Gupta1, P. Bose1 and N. Panay1,2
1Queen Charlotte's and Chelsea Hospital, London, UK; 2Imperial college, London, UK
Objective: A substantial number of women experience diminished sexual interest in their late reproductive years: we aim to evaluate the efficacy of transdermal testosterone therapy (Testogel) in both oophorectomised and non-oophorectomised postmenopausal women by measuring self-reported perceptions of well-being, mood and sexual function.
Design & Methods: Thirty five women postmenopausal women (mean age 55.2) attending a London menopause centre were appropriately counselled and then supplemented with 10mg topical testosterone (Testogel) for 6 months. A self-reported questionnaire graded changes in energy, libido, mood, hot flushes and improvements in quality of life. Patients were also questioned regarding their preference for topical testosterone versus implants and their willingness to recommend testosterone to a friend.
Results: 66% (23 of 35) patients reported substantial improvements in quality of life but 26% (9 of 35) reported undue side effects (excessive facial hair, feeling ‘grumpy’ etc). 68% would recommend testogel to a friend.
Conclusion: Topical testosterone therapy appears to be well received by postmenopausal women. Counselling should highlight these potential improvements in well-being, mood, and sexual desire but should be appropriately balanced with information regarding possible side effects. 180 words.
OR5-08
THE EFFECT OF TESTOSTERONE TRANSDERMAL PATCH ON MAMMOGRAPHIC DENSITY IN POSTMENOPAUSAL WOMEN NOT RECEIVING SYSTEMIC ESTROGEN THERAPY: FINDINGS FROM THE APHRODITE STUDY
S. R. Davis1, I. Lodhi2, C. A. Rodenberg2 and B. Von Schoultz3
1Monash Medical School, Melbourne, Australia; 2Procter & Gamble Pharmaceuticals, Mason, Ohio, USA; 3Karolinska Institute, Stockholm, Sweden
Objective: To compare the effects of two doses of the testosterone transdermal patch (TTP) with placebo in postmenopausal women not using concomitant estrogen therapy on mammographic density over 52 weeks.
Design & Methods: Participants in the Aphrodite study, a 2- year randomized, double-blind, multinational study, were randomized to treatment with TTP delivering 150 μg/day or 300 μg/day, or placebo twice weekly. Mammograms were performed at screening and at week 52 or study exit to assess eligibility and the effect on breast density after the first year of treatment. 250 women completed 52 weeks of therapy and had paired baseline and week 52 mammograms for assessment. Digitized quantification methods were used and 2 independent radiologists reviewed the films. A sub-sample of 5% of the mammographic images was randomly selected and re-read to assess intra-reader reliability (intra-class correlation coefficient > 0.92). The primary outcome was the change from baseline to week 52 in the percentage of dense tissue in the breast (PD). Each treatment group was compared to placebo using an analysis of covariance (ANCOVA) adjusting for baseline PD, baseline BMI, age, and menopausal type. Additionally, total dense and non dense area was assessed.
Results: The participants in this analysis had a mean age of 54.6 years (range 40–69 years); baseline BMI of 27.5 kg/m2 and 78% were naturally menopausal, with no significant differences between treatment groups. PD at baseline was 28.02% (SD 15.8), 27.26 (16.7) and 27.91 (14.4) for placebo, TTP 150 μg and TTP 300 μg groups respectively. Mean changes from baseline (±SEM) over 52 weeks in PD were small [0.05% (±0.16%), 0.06% (±0.19%), and 0.21% (±0.17%)] respectively. BMI at week 52 was inversely correlated with PD (Spearman −0.48). Changes on neither treatment arm were statistically significantly different from placebo for PD as well as for dense and non-dense area.
Conclusion: TTP therapy over 52 weeks appears to have no significant effect on digitally quantified mammographic density in postmenopausal women not using concurrent estrogen.
OR5-09
THE EFFECT OF MENOPAUSE ON LIBIDO IN A COMPUTER LITERATE POPULATION ACCESSING A MENOPAUSE WEBSITE
H. D. Currie1, G. P. Cumming2 and A. J. Lee3
1NHS Dumfries and Galloway, Dumfries, Scotland, UK; 2NHS Grampian, Elgin, Scotland, UK; 3University of Aberdeen, Aberdeen UK
Objective: To survey women's experience of their libido using the internet.
Design and Method: A questionnaire on the independent UK based, patient-tailored, clinician-led menopause website www.menopausematters.co.uk. The anonymous responses of the website users were then analysed.
Results: 1323 responses were obtained between 28th August and 13th December 2007 with 1208 respondents answering questions on age and menopausal status. 162 (13%) of the women self-classified themselves as premenopausal, 61% (n = 732) as perimenopausal, and 26% (n = 314) as postmenopausal.
Overall 84% (n = 1009/1200) of women felt that an active sex life was important, and 76% (n = 882/1167) felt their libido had been affected by their menopause with 82% (n = 688/837) saying they were distressed by this. Of the premenopausal group who were distressed, 24% (n = 14/59) had discussed their symptoms with a health professional. Of those, 14% (n = 2/14) had been prescribed non-testosterone HRT which one woman had found helpful.
In the perimenopausal and postmenopausal groups, 415 and 213 women were distressed by their symptoms, 24% (n = 97/407) and 39% (n = 81/210) had discussed the problem with a health professional and 20% (n = 19/95) and 28% (n = 23/81) had tried non-testosterone HRT with 37% (n = 7/19) and 36% (n = 8/22) finding it helpful respectively.
One of the two premenopausal women had found testosterone helpful as had 43% (n = 3/7) in the perimenopausal cohort and 58% (n = 11/19) in the postmenopausal group.
Thirty percent (n = 44/147) of perimenopausal, 40% (n = 279/690) of premenopausal and 62% (n = 186/299) of postmenopausal women admitted to dyspareunia secondary to vaginal dryness with 81% (n = 34/42), 81% (n = 220/271) and 86% (n = 154/180) respectively believing it to be a factor in their loss of libido. 19% (n = 6/31) of premenopausal, 25% (n = 52/207) of perimenopausal and 39% (n = 58/147) of postmenopausal women had discussed this with their health professional and 17% (n = 1/6), 23% (n = 12/52) and 40% (n = 23/58) were on treatment respectively. When stratified by age, no woman aged less than 40 years in the perimenopausal group was on treatment despite 89% (n = 16/18) of them believing vaginal dryness to be a factor in their loss of libido.
Conclusion: An active sex life is important to women. Many women suffer from loss of libido sufficient to cause distress yet they are not seeking help from health professionals. In those who sought advice, treatment was commonly not prescribed. Health professionals must address these issues by asking direct questions not only in the postmenopausal and perimenopausal groups, but also in premenopausal women, especially when effective treatments are available.
Urogenital
OR6-01
CLINICAL EFFECTIVENESS OF RETROPUBIC (IVS-02) AND TRANSOBTURATOR (IVS-04) TAPES IN THE TREATMENT OF STRESS URINARY INCONTINENCE AMONG PRE- AND POSTMENOPAUSAL WOMEN
T. Rechberger, K. Jankiewicz, K. Futyma, J. Tomaszewski, P. Skorupski, M. Gogacz, A. Adamiak, A. Wróbel and K. Postawski
University School of Medicine, Lublin, Poland
Objectives: To evaluate clinical effectiveness of the two commonly used surgical procedures (retropubic-IVS-02 and transobturator-IVS-04) for the surgical positioning of the tape at midurethra among pre- and postmenopausal women.
Design & Method: The study group consisted of 537 female patients selected out of 611 incontinent women who underwent full clinical and urodynamic work-up followed by surgical treatment of stress urinary incontinence in II-nd Department of Gynecology, Medical School of Medicine, Lublin from January 2003 to December 2005. All patients signed informed consent and the protocol of the study was accepted by local Ethical Committee.
Results: There was no difference in mean age, menopausal status, BMI and parity between IVS-02 and IVS-04 group. Clinical efficacy of both procedures was evaluated after 18 months in 398 patients. After this follow up period no statistically significant difference in clinical efficacy between these two procedures was found (chi square = 1.88, p = 0.39). The number of pre- and post-menopausal patients among study groups did not differ (p = 0,38, Chi square = 0,76). In IVS-02 group 82 patients (40,8%, mean age 47,1 ± 5,57) were premenopausal and 119 (59,2%, mean age 61,4 ± 8,43) were postmenopausal, whereas in IVS-04 group 72 women (36,5%, mean age 45 ± 6,54) were premenopausal and 125 (63,5%, mean age 61,7 ± 8,9) were postmenopausal. After 18 months follow up period in IVS-02 group there was statistical difference in clinical efficacy between premenopausal and postmenopausal patients (p = 0,01, chi square = 9,06). On the other hand no such observation was found in patients treated by IVS-04 (p = 0,28, chi square = 2,57).
Conclusion: Our results showed that these two slings are equally effective. However, surprisingly IVS-02 is more efficient tool for treatment of urinary incontinence in premenopausal women.
OR6-02
COMPARATIVE TRIAL BETWEEN PROMESTRIENE AND ESTRIOL VAGINAL CREAMS: ANALYSIS OF EFFECTIVENESS AND COLLATERAL EFFECT
R. V. Bruno1,2, F. A. Silveira1,2, K. A. Costa1, M. A. Alvim1, R. C. Freitas1 and D. Postruznik3
Gynecology Institute of Federal University of Rio de Janeiro1, College of Medicine of Valença2, Rio de Janeiro, Brazil and Merck Theramex International Medical, Monaco3
Objective: To compare vaginal creams composed of Promestriene and Estriol for use in symptomatic climacteric women, concerning its effectiveness and collateral effects.
Design and Method: This randomized controlled trial enrolls 40 women divided in two equal groups. The groups were named: group1 (promestriene) and group2 (estriol). The patients will be randomized by order of arrival; patient number one and the following odd numbered patients will take part in group 1, patient number two and the following pair numbered patients will take part in group 2. The patients will receive a 1g/day dosage of the cream for application via vagina, at night, for three consecutive months. A third group (control), composed of fifteen patients, will not receive medications. All the patients will have their plasma analysis of estradiol, FSH, LH and the hormonal vaginal cytology analyzed before the study and after three months of treatment. The hormonal dosages will always be made between 7 and 10 a.m. The direct analysis of the hormonal colpocytology will be carried through in all patients after the study, as a means to prove the effectiveness in the recovery of the vaginal epithelium. The patients will answer a questionnaire on climacteric/menopausal symptoms and on quality of life, having been emphasized mastodynia, dryness, sexual behavior, dyspareunia and general welfare (based on the World Health Organization, WHO). The research was registered in the Committee of Ethics in Research of the College of Medicine of Valença in according to the Declaration of Helsinki. All the patients have volunteered to participate in this research, having signed written informed consent. The patients will be admitted in the ambulatory of Gynecology of the College of Medicine of Valença and in the Institute of Gynecology of the Federal University of Rio de Janeiro(UFRJ). Criteria of inclusion: symptomatic climacteric or menopausal women, mainly with relative complaints about the vaginal atrophy. Criteria of exclusion: Patients using pure or combined estrogenic hormonal therapy for at least three months; patients carrying hormone-dependent neoplasia; pregnant patients; patients with kidney or liver insufficiencies; any other pathologies which contraindicate the hormonal therapy. Statistical analysis: non-parametric tests will be used: X2, Fisher and Wilcoxom. The value of p ≤ 0,05 will be considered significant.
OR6-03
OSPEMIFENE, A NEW SERM, IMPROVES THE SYMPTOMS OF VAGINAL DRYNESS AND DYSPAREUNIA IN POSTMENOPAUSAL WOMEN: RESULTS FROM A PIVOTAL PHASE 3 STUDY
J. A. Simon1 and J. Komi2
1George Washington University, Washington, DC, USA; 2QuatRx Pharmaceuticals Company, Ann Arbor, MI, USA
Objective: In this randomized, double-blind phase 3 study, we assessed the efficacy of ospemifene, a new selective estrogen receptor modulator (SERM), to treat moderate to severe symptoms of vulvovaginal atrophy (VVA).
Design and Methods: A total of 826 postmenopausal women were randomized 1:1:1 to receive ospemifene (30 mg/day or 60 mg/day orally) or placebo. The vulvovaginal atrophy (VVA) symptoms were assessed as a change from baseline in the self-reported moderate to severe symptoms of VVA, using a Likert scale (0 = none, 1 = mild, 2 = moderate, 3 = severe). All subjects were supplied with a non-hormonal lubricant to be applied as needed during the 12 week treatment period.
Results: At baseline, vaginal dryness and dyspareunia were the most common moderate to severe symptoms of VVA, reported by 90% and 66% of the patients, respectively. After 12 weeks treatment, the symptom score for patients reporting moderate to severe vaginal dryness was significantly decreased in both the ospemifene 30 mg and 60 mg groups (−1.08 and −1.25, respectively) compared with placebo (−0.79; p = 0.001 and p < 0.001 for ospemifene 30 mg and 60 mg, respectively). Similarly, the symptom score for patients reporting moderate to severe dyspareunia showed a significant decrease in the 30 mg and 60 mg ospemifene groups (−1.24 and −1.37, respectively) compared with placebo (−1.00; p = 0.03 and p = 0.002 for ospemifene 30 mg and 60 mg, respectively). Ospemifene was well tolerated and demonstrated a favorable safety profile.
Conclusion: Ospemifene is effective in significantly improving vaginal dryness and dyspareunia, the most common symptoms of VVA.
OR6-04
PROLIFERATION ACTIVITY OF CULTURED PUBOCERVICAL FASCIA FIBROBLASTS OBTAINED FROM MENOPAUSAL WOMEN SUFFERED FROM STRESS URINARY INCONTINENCE
J. Tomaszewski1, W. Brzana2, K. Futyma1, P. Miotła1, W. Rzeski2 and T. Rechberger1
1University School of Medicine, Lublin, Poland; 2Institute of Agricultural Medicine, Lublin, Poland
Objectives: The main purpose was to evaluate the proliferation ability of cultured pubocervical fascia fibroblasts after exposure to steroid hormones and drugs often used by menopausal women suffered from stress urinary incontinence.
Design and Method: Specimens of human pubocervical fascia were obtained from 8 menopausal women during midurethral sling procedures. Fibroblasts were isolated and cultured by outgrowth technique. Cells after passage number 3 to 8 were used for assessment. Fibroblasts were cultured on 96-well microplates at density 3 × 104cells/ml. Next day culture medium was changed and cells were exposed to serial dilutions (10–12, 10–9, 10–7, 1, 2.5, 5 and 10 μM/ml) of 17β-estradiol, estriol, daidzein, danazol and tamoxifene in medium supplemented with only with Serum Replacement 2 (Sigma). Cell proliferation was assessed after 96 hrs using MTT method (Cell Proliferation Kit I, Boehringer). Formazan crystals were solubilized overnight in SDS buffer and the product was quantified spectrophotometrically by measuring absorbance at 570 nm weave lenght using E-max Microplate Reader.
Results: Pubocervical fascia fibroblasts showed increased proliferation capacity after 17β-estradiol comparing to estriol and daidzein treatment. Moreover proliferative activity was lower in tamoxifene and danazol groups when compared to 17β-estradiol and estriol.
Conclusions. The results indicate that, at least in vitro, fibroblasts from pubocervical fascia acquired from menopausal women suffering from SUI are more capable to proliferate after estrogen treatment. This is an indirect rationale for local estrogen treatment in case of female SUI.

OR6-05
PRESENTATION OF TWO NON HORMONAL THERAPEUTIC SCHEMES IN CLIMATERIC WOMEN WITH URINARY SYNTOMATOLOGY
S. Torchetti, M. Breccia, P. Micone and N. Del Zoppo
Private practice, buenos aires city, argentina
Objective: To evaluate the combination of a soy isoflvavones plus cranberry orally versus cranberry mono dosis orally in the prophylaxis of urinary infections in climacteric patients.
Design and Methods: Open randomized study. 178 climacteric patients between 55–63 years of age (55.8) who walked in to private practice for urinary infections (no less than three a year) were recruited for the study.
The patients included in the protocol had not received hormonal treatment in the twelve months previous to the study.
All the patients were given a routine gynaecological study.
The patients were divided into two groups
89 patients who received 1 tablet a day of soy isoflavones 48 mg + 7.5 UI of vitamin E + 1 tablet a day of cranberry 500 mg + 50 mg of vitamin C.
87 patients who received 1 tablet a day of cranberry 500 mg + 50 mg of vitamin C.
Results: In the group treated just with cranberry an average of 2.5 infections per patient was observed whereas in the group treated with soy isoflavones plus cranberry the average was 1.2 (p < 0.05).
It was also proved that the patients treated with soy isoflavones were benefited also with a decrease in the vasomotores symptoms.
Conclusions: The combination of soy isoflavones plus cranberry administered orally for the prophylaxis of recurrent urinary infections presented more effectiveness than the use of cranberry as mono therapy.
No side effects were observed during the treatment period.
Thematic Area: 37. Urogenital.
OR6-06
REMEEX DEVICE FOR THE TREATMENT OF URINARY STRESS INCONTINENTE: OUTCOMES ACCORDING TO AGE
A. Cuesta, E. Gómez, M. Bousamra, E. Muñoz, A. Masero, F. Muñoz and J. M. Hernández
Doce de Octubre Hospital, Madrid, Spain
Objective: To assess efficacy and complications of Remeex device for the treatment of urinary stress incontinence (SUI) according to age.
Design and Method: A descriptive, retrospective study of 217 women who underwent Remeex device between 1999 and 2007. Patients had follow-up visits at first, sixth, twelfth and twenty-fourth months after surgery. We performed statistical with SPSS15.0.
Results: The mean age was 57.5 years (SD = 11.28), range: 30–77 years. 72.9% of the patients were older 50 years, 22.4% between 41–50 years and 4.9% between 30–40 years. The majority (87%) had overweight or obesity, of them, 75.7% were older 50 years, 19.3% between 41–50 years and 5% between 30–40. 13% were normal weight or underweight, of them, 42.9% were older 50 years, 52.4% between 41–50 years and 4.8% between 30–40 years.
66.8% of the patients had surgeries in pelvic floor and 82.5% had associated celes. The majority (65.7%) had SUI grade III.
Global cure rate of urinary stress incontinence was 86.2%. According to age, six months after surgery the cure rate between 30–40 years was 57.1%, between 41-50 was 97% and in patients older 50 was 88.9% (p = 0.016). A year after surgery, the cure rate was 42.9% in patients between 30–40 years, 83.3% between 41–50 years and 83.9% in patients older 50 (p = 0.013). Two years after surgery, the cure rate was 50% in patients between 30–40 years, 72.2% between 41–50 and 90.9% in patients older 50 (p = 0.008).
Adjusting by BMI, in overweight or obesity group, two years after surgery, the cure rate between 30–40 years was 60%, between 41–50 years was 69.2% and in patients older 50 years was 89.7% (p = 0.05). Patients older 41 years also had better outcomes than younger six months and a year after surgery (p = 0.015, 0.006, respectively). In normal weight or underweight group, significantly differences were not found in respect to cure rate between groups of age.
Most frequent intraoperative complication was bladder injury (12.7%). Immediate post-operative complications were urinary tract infection (9.3%), fever (7.8%), urinary retention (6.8%), wound infection (1.5%). Most frequent complications during the follow-up were suprapubic fistula (7.4%) and sling erosion (6.9%).
Remeex system had not to be regulated in most of cases (84.2%) and was removed in 5.53% of patients.
Conclusions: The cure rate is high in relation to other techniques of the last decade considering that the majority of the patients had poor prognostic factors. According to our results, the cure rate was higher in patients older 40 years.
OR6-07
THE EXPRESSION OF MATRIX METALLOPROTEINASES 1 AND 2 IN UTEROSACRAL LIGAMENTS OF WOMEN WITH GENITAL PROLAPSE
T. Strinic, M. Vulic, S. Tomic, V. Capkun and B. Leovac
Clinical Hospital Center, Split, Croatia
Objective: Mechanical stability of the genito-urinary tract depends on intact, functional collagen fibers. Collagenous tissue from the uterosacral ligaments is representative. Collagen is a metabolically active structure with constant turnover mediated through proteolysis by a group of enzymes termed matrix metalloproteinases (MMPs). The MMP–1 and – 2 expression in the uterosacral ligaments of women with and without uterine prolapse was evaluated.
Design & Method: After informed consent, uterosacral ligaments biopsies were obtained during surgery from 25 postmenopausal women with uterine prolapse and twenty – five similar controls who underwent gynecologic surgery for benign indications. The experiments were designed to identify the presence of MMP–1 and – 2 in uterosacral ligaments of examinees and controls by immunohistochemical staining in fresh and frozen tissue slides with MMP–1 and – 2 mouse antibodies (Merck Bioscience, UK). The data statistically evaluated with Yates corrected χ2test and Fisher exact test.
Results: The control subjects were anthropometrically and clinically matched to the patients. A significant increase in MMP–1 expression was seen in uterosacral ligaments tissue from women with prolapse compared with controls (P < 0.05). No significant difference in MMP–2 expression was found between examinees with and without prolapse (P = 0.224).
Conclusion: Pelvic organ prolapse in women is associated with a change in collagen metabolism resulting in an increased MMP–1 expression. Our results suggested that imbalance between collagen synthesis and degradation may predispose women to genital prolapse. It was concluded that increased MMP–1 expression and decreased collagen content might be the key factors associated with pelvic support disorders.
Clinical epidemiology
OR7-01
A COMPARATIVE STUDY OF EXPERIENCE OF MENOPAUSAL SYMPTOMS AMONG WOMEN OF DIFFERENT SOCIOECONOMIC CLASSES IN IBADAN, NIGERIA
F. M. OlaOlorun and T. O. Lawoyin
College of Medicine, University of Ibadan, Ibadan, Oyo State, Nigeria
Objective: A woman's experiences during menopause vary from an uneventful transition in some women, with the only symptom being the cessation of menses, to a period characterized by disturbing symptoms which may require significant lifestyle adjustments in others. The goal of this study was to describe and compare the distribution of menopausal symptoms among women of different social classes in Ibadan as well as to determine the predictors of significant menopausal symptoms in the 4 week period preceding the interview.
Design & Method: A cross-sectional comparative study was carried out using the multistage sampling technique. Quantitative data were collected on sociodemographic, obstetric and gynecological variables using a structured questionnaire which included a standardized Menopause Rating Scale (MRS) to assess the reported experience of symptoms in the four week period preceding the interview. Eleven symptom groups were scored for each respondent on a scale of 0-4 with increasing severity for each group, with a maximum possible score of 44. Symptoms were then regrouped as not significant (Scores: 0-8) or significant (Scores: 9-44). Information gathered was compared across the three social classes. Social class was assigned based onoccupation using the 3 class version of the NS-SEC classification. Women's symptomatic experiences in midlife were further explored through 6 focus group discussions.
Results: Joint and muscular discomfort was the commonest reported symptom among all women in this study (58.9%) as well as women in each social class (52.0%, 58.0% and 63.7% respectively), in the four week period preceding the interview. The next most reported symptom in women of the upper, middle and lower social classes were physical and mental exhaustion (42.2%), hot flushes (42.0%), and sexual problems (50.3%) respectively. Following logistic regression, women of the middle social class (OR: 0.56; 95% CI: 0.37–0.84) and premenopausal women (OR: 0.51; 95% CI: 0.36–0.73) were most likely to have reported the experience of significant menopausal symptoms.
Conclusion: Although any woman could face challenges associated with menopausal symptoms, the distribution of significant symptoms varied by social class. All women approaching menopause, especially those who are premenopausal and of the middle social class should receive health information and guidance on possible lifestyle adjustments to ease the disruptions that menopausal symptoms can cause.
OR7-02
BAHRAINI WOMEN'S ATTITUDES TOWARDS THE MENOPAUSE: IMPLICATIONS FOR HEALTH CARE POLICY
G. Jassim and Q. Al-Shboul
Arabian Gulf University, Manama, Kingdom of Bahrain
Objective: To assess the attitudes of Bahraini women aged 30–64 years towards the menopause.
Methods: A cross sectional study of 260 Bahraini women attending primary health care centers was conducted. Multistage stratified and clustered random sampling techniques were used. The first stage was a stratified random sample of the five governorates in the Kingdom of Bahrain, the second stage clustered random sample where one health center from the health centers in each governorate was chosen, the third a stratified random sample on age, where three age groups were identified (30-39, 40-49, and 50-64) and the final stage was a simple random sample from each age group strata of the 5 chosen health centers. The women were interviewed using a questionnaire containing Attitude Towards Menopause checklist and sociodemographics. The collected data was coded, entered and analyzed using the statistical package SPSS version (15.0). Relevant descriptive statistics were computed for all items. The equality of means across the categories of each categorical independent variable was tested using either Analysis of variance (ANOVA) or independent samples t-test. The linear relationship between the Average Attitude Score and each of the quantitative independent variables was assessed by Pearson's linear correlation coefficient. Statistical tests with P-value < 0.05 were considered statistically significant.
Results: The women's mean age ± SD and mean age at menopause ± SD were 45.04 ± 9.43 and 48.67 ± 2.923 years, respectively. Respondents' median age and median age at menopause were 45.5 and 48.0 years, respectively. Almost half of the women (48.5%) had completed high school or diploma, and 41.5% were currently employed outside home. Over half of the women were pre-menopausal, 19.6% peri-menopausal and 26.9% were post-menopausal.
The mean ± SD attitude towards menopause average score (MAAS) was 2.4 ± 0.26 where the minimum score was 1 indicating very negative attitudes and the maximum 4 indicating very positive attitudes. Statistically significant differences in means were noted among categories of educational level, menopausal status, and marital status. Moreover, the mean attitude average score was positively correlated with age of respondents. Premenopausal women had more negative attitude towards menopause than peri- or postmenopausal women.
Conclusion: Bahraini women display a considerable range of attitudes towards menopause, with their general attitudes ranging from neutral to positive. Postmenopausal women had more positive attitudes towards menopause than premenopausal women.
OR7-03
DROSPIRENONE AND THE RISK OF ARRHYTHMIA: RESULTS FROM THE EURAS STUDY
J. Dinger, A. Assmann and S. Moehner
ZEG – Berlin Center for Epidemiology and Health Research, Berlin, Germany
Objective: The progestin drospirenone (DRSP) has antimineralocorticoid properties which besides a number of beneficial cardiovascular effects could potentially increase the risk of hyperkalemia and subsequently arrhythmia of DRSP/estradiol combinations (e.g., OCs or HRT preparations). The study investigated the incidence of new arrhythmias associated with the use of DRSP-containing and established OCs under routine medical conditions.
Design & Method: EURAS was a controlled, prospective, non-intervention cohort study of new users of DRSP-containing and other OCs under routine conditions of medical practice in seven European countries. Baseline survey and semi-annual, active follow-up were based on patient-reported outcomes, with validation of reported events by the women's treating physicians. A multifaceted 4-level follow-up procedure was established to ensure low loss to follow-up rates. Inferential statistics were based on Cox regression analyses.
Results: Overall, 59,510 women were enrolled, and the follow-up yielded 142,475 WY of observation. Loss to follow-up was 2.4%. A total of 336 women had ECG-confirmed arrhythmias after study entry. Of these events, 237 were recurrences of pre-existing conditions and 99 represented new conditions (e.g., hyperthyreoidism with tachycardia, WPW syndrome, tachycardia absoluta, sick sinus syndrome). Arrhythmic events that could be suggestive of an increased serum potassium level (e.g., ECGs with peaked, narrow-based T waves) were not observed. The incidence of new arrhythmias that required medical treatment was similar for current OC users (2.8–3.9 events/10,000 WY) and past OC users (5.0 events/10,000 WY). The hazard ratio for DRSP-containing OCs versus other OCs was 0.7 (95% CI, 0.3–1.4).
Conclusion: Results do not indicate that DRSP/estrogen combinations under routine medical conditions are associated with a higher risk of arrhythmia or hyperkalemia-induced arrhythmia than other progestin/estrogen combinations. Differences between progestins were not found. Study results show that the incidence of arrhythmia in OC users and non-users/past users is similar.
OR7-04
SOCIO-DEMOGRAPHIC, PSYCHOSOMATIC, BEHAVIOURAL CHARACTERSITICS, HORMONAL AND SKELETAL STUDIES OF MENOPAUSAL BLACK SOUTH AFRICAN WOMEN
L. Matsela
Faculty of Health Sciences, University of Limpopo (MEDUNSA CAMPUS), Pretoria, SOUTH AFRICA
Introduction: Very little information is available in the literature about the hormonal as well as the skeletal status of black African women, following menopause. There is a prevailing conjecture that perhaps black African women do not understand the changes that occur at the period of transition from reproductive life to menopause, and that such women may lack the initiative to seek for health care in relation to menopause.
Objective: To evaluate the psychosomatic, socio-demographic and the behavioural features of black African women in relation to menopause. The study also examined the hormonal and the skeletal changes of these women during and after the transition into menopause.
Design & Methods: A structured questionnaire was used to assess the understanding of menopause by peri- and post–menopausal black South African women. Each woman in the study was investigated for hormonal profile and bone mineral density. The hormones evaluated were FSH, LH, oestradiol, progesterone, DHEAS and testosterone. Bone mineral density was performed using the dual energy x-Ray absorptiometry (DEXA) procedure on both hip and lumbar vertebrae.
Results: The age range was 18–32 years for menstruating women and 40–75 years for peri- and post-menopausal women. The study revealed that the women had a good understanding of the concept of menopause. They expressed a strong association between being menopausal and maturity and wisdom. Menopause is understood to be a sign of enhanced status in their respective communities. The hormonal evaluation of these women clearly shows the expected transition from the reproductive period to post-menopausal state. The bone mineral density studies revealed evidence of osteopenic changes in the lumbar spine among the postmenopausal women. Although the women understood and expressed the need for HRT to alleviate the symptoms of menopause, many of them expressed fear for its use.
Conclusion: This study revealed the opposite of what had been expressed as lack of understanding of menopause by black African women, although definite misgivings were expressed by these women, in relation to the use of HRT. There is the need to enhance their understanding of the use HRT if we are to eliminate the long term effects of menopause on their bone mineral density.
OR7-05
THE MENOPAUSE SYMPTOM PROFILE OF MÄORI WOMEN IN NEW ZEALAND
B. A. Lawtona, S. B. Rosea, D. M. Cormackb, J. Stanleyc and A. C. Dowellc
aWomen's Health Research Centre, Department of Primary Health Care and General Practice, Wellington School of Medicine & Health Sciences, University of Otago, Wellington, New Zealand; bTe Ropu Rangahau Hauora a Eru Pomare, Wellington School of Medicine & Health Sciences, University of Otago, Wellington, New Zealand; cDepartment of Primary Health Care and General Practice, Wellington School of Medicine & Health Sciences, University of Otago, Wellington, New Zealan
Objectives: To describe menopause-related symptoms reported by Mäori and non-Mäori Mäori New Zealand women, and to explore relationships between symptoms, socio-demographic profile and usage of hormone replacement therapy (HRT).
Methods: Post-menopausal women were recruited from primary care practices in five regions in New Zealand into a longitudinal observational study and an international trial to investigate the long term benefits and risks of Hormone replacement therapy. Data were collected during face-to-face interviews involving a series of questionnaires relating to general health, reproductive and gynaecological history and menopause symptoms experienced in the past 4-weeks.
Results: 3616 women aged 49–70 years (mean age xxyears) were recruited over a 5 year period. Mäori and non-Mäori participants differed with respect to demographic and clinical characteristics, but few differences were observed in the frequency of menopause-related symptoms reported by these groups. Overall, 28% of women reported vasomotor symptoms (flushes and night sweats) in the last 4-weeks. There was no statistical difference in vasomotor symptoms between Mäori and non-Mäori and this was unchanged when controlling for age, education level, deprivation scores, BMI, HRT use and smoking status. Non-Mäori women reported higher rates of insomnia and vaginal dryness (p < 0.05), whereas Mäori women more frequently reported cramping or swelling in the legs, pain or burning during urination, and abdominal cramps (p < 0.05). Mäori women were less likely than non-Mäori to have ever used HRT (24% versus 54%), and less likely to be current users of HRT with only 5% of participants reporting current use compared to 30% of non-Mäori participants (p < 0.05).
Conclusions: Mäori and non-Mäori have the same rate of self-reported vasomotor symptoms, and similar rates of most other menopause-related symptoms despite marked differences in education level, weight, socio-economic status (SES), smoking, and HRT use. There was a significantly lower use of HRT by non-Mäori compared to Mäori in this study. The reason for this inequality is not clear from this data but may be due to access and clinical pathway inequalities.
OR7-06
THE SIGNIFICANCE OF ACHES AND JOINT PAIN REPORTS ACROSS THE MENOPAUSAL TRANSITION– A LONGITUDINAL STUDY
C. Szoeke1, S. Petrovski1, F. Cicuttini2,3, J. Guthrie1 and L. Dennerstein1
1Office of Gender and Health, University of Melbourne, Australia; 2Monash University, Melbourne, Australia; 3The Alfred Hospital, Melbourne, Australia
Objective: To determine factors associated with reported joint symptoms across the menopausal transition and investigate whether symptom reporting is accounted for by the presence of radiological arthritis in postmenopausal women
Design & Method: Data was analysed from the Melbourne Women's Midlife Health Project a population-based prospective study of 438 Australian born women, aged 45 to 55 years and menstruating at baseline who were interviewed annually over 8 years. We examined interview question about bothersome aches or stiff joints in the previous 2 weeks with physical measures, sociodemographic information, moods scales and menopausal status. A score for the symptom of aches and stiff joints was calculated from the product of the severity and frequency data. This data was analysed using random-effects time-series regression models. X-rays conducted on this cohort in 2004 were scored for evidence of osteoarthritis using a validated scale, by two investigators who were blinded to questionnaire results.
Results: Part I: “Aches and stiff joints” were the most commonly reported symptom and reporting increased over time in the longitudinal study. Variables significantly associated with reporting bothersome aches and stiff joints were high BMI (p < 0.001), high negative mood (p < 0.01), not being employed (p < 0.001), and experiencing the menopausal transition (p < 0.05). A higher severity and frequency of this symptom was associated with BMI (p < 0.01), not being employed (p < 0.05) and high negative mood (p < 0.005). Whilst knee osteoarthritis was significantly associated with symptom reports (p = 0.008) hand osteoarthritis was not (p = 0.2).
Conclusion: Menopausal status, BMI, employment status and depressed mood were all associated with the experience of bothersome aches and stiff joints. Aches and stiff joints, common in postmenopausal women are not necessarily indicative of radiological osteoarthritis. The clinical and research relevance of this is discussed.
OR7-07
THE CULTURAL CONTEXT OF MENOPAUSE: A MULTI-ETHNIC STUDY IN SYDNEY, AUSTRALIA
J. A Eden and J. Liu
School of Women and Children's Health, Royal Hospital for Women, Sydney, Australia; University of NSW, Sydney, Australia
Objective: To investigate the peri-and post-menopausal experience of Chinese, Arabic, Indian and Greek women aged 45–65 years, living in Sydney, Australia. This presentation will focus on the postmenopausal women.
Design & Method: Two research tools were used – focus groups using experienced bilingual health workers and a cross-sectional survey using the MENQOL instrument. The MENQOL was translated into the subject's language and then translated back into English by a different bilingual health worker to ensure accuracy.
Results: The average age of menopause in all the groups was around 50 years. Arabic women had the highest rate of vasomotor symptoms; Indian women had the lowest. There was no correlation with how long they had been in Sydney or educational status. Arabic women also had the highest rate of depression and anxiety; Indian women the lowest. Both Chinese and Arabic women had the highest rate of physical symptoms such as aches and pains, backache and headache. Arabic women had the highest rate of sexual dysfunction; Indian women the lowest. The focus groups revealed significant differences amongst the groups with regard to which health professional they wanted to see. For example, most Chinese women were adamant that they wanted to talk to a doctor about their menopause; whereas Greek women were happy to talk with a nurse or a doctor.
Conclusion: In summary, the Arabic postmenopausal women were the most distressed. The Chinese women had high rates of dry skin, aches and pains and poor memory. Greek women reported the highest rate of feeling bloated as well as high rates of feeling tired, decreased muscle strength and backache. Indian women were the happiest; their most prevalent symptoms were decreased muscle strength, and lack of energy. Interestingly, the length of time that these women had been in Australia did not appear to have a major impact on their menopause experience.
New regimens
OR8-01
BENEFITS AND HARMS OF HORMONE THERAPY IN YOUNGER AND OLDER POSTMENOPAUSAL WOMEN: A RISK-BENEFIT AND COST-EFFECTIVENESS ANALYSIS
S. R. Salpeter1,2, N. S. Buckley3, H. Liu1,2 and E. E. Salpeter4
1Santa Clara Valley Medical Center, San Jose, California, USA; 2Stanford University School of Medicine, Stanford, California, USA; 3Sequoia High School, Redwood City, California, USA; 4Cornell University, Ithaca, New York, USA
Objective: The consensus after the Women's Health Initiative trial was that hormone therapy was harmful for women of all ages and should only be used short-term for menopausal symptoms. Pooled trial data, however, show that hormone therapy reduces coronary heart disease events and total mortality in younger women, but not in older women. The objective of this study is to evaluate the health and economic outcomes of hormone therapy in younger and older postmenopausal women.
Design and Method: We developed a Markov cost-effectiveness model to simulate health effects and costs of hormone therapy or no therapy in postmenopausal women. In the base-case analysis, two cohorts of 50-year-old and 65-year-old postmenopausal women were given hormone therapy or no therapy for 15 years and followed over their lifetime. The health states were: healthy, cardiovascular disease (coronary heart disease event or stroke), breast cancer, fracture (hip or vertebral), combinations of two or three disease states, and dead, due to a disease state or other unrelated causes. Assumptions and ranges were derived from an extensive search of the literature though June 2007. The main outcomes measured were quality-adjusted life-years (QALYs) and incremental cost per QALY gained, for hormone therapy compared to no therapy.
Results: In the base-case analysis, hormone therapy for 15 years in the younger cohort resulted in a gain of 1.45 QALYs, with an incremental cost of $2,655 per QALY gained. The results for younger women were robust to all sensitivity analyses, and treatment remained highly cost-effective (<$10,000 per QALY gained) within the range of individual assumptions used. Treatment durations of 5 years and 30 years were also cost-effective, with costs of < $5,000 per QALY gained. In the older cohort, treatment for 15 years resulted in a net gain of 0.11 QALYS, with a cost of $31,174 per QALY gained. However, a net loss in QALYs was seen for the first 9 years before a gain was realized. The results for older women were sensitive to many of the assumptions used.
Conclusion: Hormone therapy for 5 to 30 years in younger postmenopausal women is cost-effective and results in gains in quality-adjusted life-years. Hormone therapy in older women may result in a small gain in quality-adjusted life, but only after a net loss for several years. The results indicate that hormone therapy is associated with a long-term benefit in younger postmenopausal women.
OR8-02
COMPARATIVE STUDY USING NOMEGESTROL ACETATE NOMAC, LEVONORGESTREL-RELEASING INTRAUTERINE DEVICE, MIRENA AND IMPLANON IN THE MANAGEMENT OF DYSFUNCTIONAL UTERINE BLEEDINGS
G. Grazziotin1 and D. Postruznik2
1Tancredo Neves Medical Center, Mato Grosso, Brazil; 2Theramex, Monte Carlo, Mônaco
Menstrual irregularities are a common gynecologic problem.
Dysfunctional uterine bleeding is defined as a variety of manifestations of uterine bleeding occurring in the absence of pathology or medical illness.
This study discusses treatment of dysfunctional uterine bleeding in fertile women. Selecting the most ‘metabolically friendly’ progestin was another goal of this trial.
Study population:
74 women, divided in 3 groups:
26 women - NOMAC cyclically (10 to 21 days)
23 women - ETO-implant.
25 women - LNG-IUD.
Protocol regulated evaluation - follow up. It was in three months intervals.
History and physical examination.
BMI (body mass index)
Endometrium evaluation by transvaginal ultrasound
(3°/5° day. Endometrial measure until 5mm.)
Mammography
Hysteroscopy
Endometrial biopsy
PAP smear
Lab: Blood (TBC) Coagulation, Glycemia, Triglycerides, Total cholesterol, Urea, Creatinine, TSH, FSH, LH, Prolactin, Testosterone.
Patients that have completed 12 months:
On NOMAC 73%, on LNG-IUD 88%, on ETO-implant 60.8%.
Conclusions:
NOMAC: Effective in DUB treatment, good therapeutic control, tolerance and metabolic neutrality.
Smaller weight gain, smaller spotting incidence:
14% incidence to the 6th month.
10% to the 9th month,
5,2% to the 12th month.
Bigger amenorrhea index:
3th°e 6th month (20% to the 3rd month,. 28,5% 6th month).
Bigger oligomenorrea index:
31,5% to the 3rd month, 38,2% to the 6th, 38% to the 9th, 25% to the 12°mês.
50% classified as treatment success
Smaller incidence at libido and humor disturbances.
LNG – IUD: Effective in DUB treatment, but quite inflexible hormonal control.
High spotting index, during the first 6 months of use
Bigger amenorrhea indexes after the 9 month of use (47, 2% to the 9th mês, 57, 0% to the 12th month).
43% classified as treatment success
2 LNG insertions were performed under general anesthesia.
Bigger incidence of migraine, acne and breast pain.
ETO – IMPLANT: Little effective in DUB treatment; quite inflexible hormonal control.
Bigger incidence:
In spotting, irregular bleeding, weight gain and migraine.
30% classified as treatment success.
The treatment must be individualized according to the patient's age, current need for contraception, side effects, cost of treatment, and easy of compliance in adhering to the treatment modality.
OR8-03
EFFECT OF RALOXIFENE AND LOW-DOSE PERCUTANEOUS 17β ESTRADIOL ON MENOPAUSE SYMPTOMS AND ENDOMETRIUM - A RANDOMIZED AND PLACEBO-CONTROLLED TRIAL
B. Valiati1,2, E. Capp1,2, M. I. Edelweiss1,2 and M. C. O. Wender1,2
1Programa de Pós-Graduação em Medicina: Ciências Médicas, UFRGS, Porto Alegre, Brazil; 2Hospital de Clínicas de Porto Alegre, Brazil
Objective: To investigate the efficacy on climacteric symptoms and endometrial safety of percutaneous low-dose 17β-estradiol associated with raloxifene in postmenopausal women. Design & Methods: In this randomized placebo-controlled study, a total of 52 women (mean age = 53 years), who reported moderate to severe hot flushes, were randomized to receive 60 mg of raloxifene (RLX, n = 20), 0.5 mg of percutaneous 17β-estradiol associated to 60 mg of raloxifene (RLX + E2, n = 16) or placebo (n = 16). Exclusion criteria were: contra-indication for estrogen or use in the 6 previous months of hormone replacement therapy (HRT), a history of cardiovascular, thromboembolic, metabolic, endocrinologic and malignant disease. For 3 months, climacteric symptoms were evaluated using the menopausal Kupperman index. Vaginal bleeding occurrence was also assessed. At baseline and at the end of the study endometrial thickness was measured and endometrial samples were collected for histological study. Hysteroscopy was done at the end of treatments. The t-test, Wilcoxon test and ANOVA were used in the statistical analysis.
Results: At baseline, the mean Kupperman index was 23.7 ± 1.8 in RLX group, 22.9 ± 1.9 in RLX + E2 group and 22.6 ± 1.9 in the placebo group (NS). After 3 months, there was a significant reduction in Kupperman index mean values in both groups, but no statistical difference was observed between groups. However, RLX + E2 and placebo were significantly superior to RLX in reducing hot flush severity (p < 0.05). Endometrial thickness did not change in groups. The association of percutaneous low-dose 17β-estradiol to raloxifene was not associated with proliferation of endometrium neither in hysteroscopies nor in endometrial biopsies at the third month of treatment. No vaginal bleeding was reported during the study. Conclusions: The association of percutaneous low dose of 17β-estradiol with raloxifene exerted favorable effects on hot flushes severity of post menopausal women, providing a safe profile in endometrium at least in short term therapy.
OR8-04
EFFECTS OF SUBDERMAL IMPLANTS ON LIPID PROFILE AND TOLERABILITY, IN POSMENOPAUSAL WOMEN
I. O. Barbosa1, E. Coutinho2, O. Ladipo2, C. Noronha1, R. Mota1, A. C. Lopes1 and R. Lopes1
1Maternidade Climerio De Oliveira, Federal University Of Bahia, Brazil; 2Centro de Pesquisa e Assistência em Reprodução Humana, Salvador-Bahia, Brazil
Objective: To compare the effects of continuous 17-beta estradiol-only silastic implants with those of continuous 17-beta estradiol plus continuous nomegestrol acetate silastic implants on lipid profile and tolerability in postmenopausal women.
Design & Method: This was an open-label, parallel-group study. Women with and without uterus and no contraindications to hormone replacement therapy (HRT) were included in this study, we consider as HRT the replacement of Estrogens-only and Estrogens + Progestogens. Each subject was assigned to receive four 17-beta estradiol-only silastic implants (women without uterus), or four 17-beta estradiol plus one nomegestrol acetate silastic implant (women with intact uterus), for one year. A total of 40 subjects were enrolled and received, the silastic implants of which 40 (100.0%) subjects completed the study (n = 20, estradiol only; n = 20, estradiol plus nomegestrol acetate).
Results: No significant decreases in total cholesterol (1.3%), low-density lipoprotein (LDL) cholesterol (1.1%), in triglycerides (1.2%) and fasting glucose (−1.3%) serum levels were observed in both groups, while HDL cholesterol increased significantly (2.8%), during the study in both groups. The incidences of adverse events were similar in both treatment groups.
Conclusion: Women treated with 17-beta estradiol-only silastic implants or 17-beta estradiol plus nomegestrol acetate silastic implants showed a significant increase in high-density lipoprotein cholesterol and no significant differences in other lipid profiles and tolerability.
OR8-05
RATIONALE FOR THE DEVELOPMENT OF AN “ADAPTED” INTRAUTERINE PROGESTIN-RELEASING INTRAUTERINE SYSTEM IN COMBINATION WITH SYSTEMIC ESTROGEN FOR HORMONE REPLACEMENT THERAPY IN POSTMENOPAUSAL WOMEN AND RESULTS OF A 3-YEAR STUDY
D. Wildemeersch
Contrel Research, Technology Park, Zwijnaarde, Ghent, Belgium
Objective: To investigate the rationale for the development of a new LNG-IUS from a cardiovascular point of view, and to study the clinical aspects of the combined systemic estrogen and intrauterine LNG delivery in postmenopausal women.
Design and Method: Justification analysis and development planning. A 3-year non-comparative prospective clinical trial. Two-hundred-twenty symptomatic postmenopausal women using estrogen replacement therapy (ERT) combined with a novel T-shaped LNG-releasing intrauterine system (Femilis® Slim LNG-IUS), to prevent endometrial proliferation and bleeding. Main outcome measures: insertion-related aspects, acceptability, endometrial histology and ultrasonographic evidence of endometrial suppression, after a period of approximately 3 years of use.
Results: The miniature LNG-IUS is easily inserted, and well accepted. The dominant endometrial histologic picture is that of inactive endometrium characterized by glandular atrophy and stroma decidualization (Kurman classification 5b). No cases of endometrial hyperplasia were found. On transvaginal ultrasound, this corresponds with a thin endometrium (≤5 mm).
Conclusion: The very low absorption of LNG when delivered in the uterine cavity results in an almost “estrogen alone” HRT which has been shown to have clear advantages over combined estrogen-progestin HRT. Due to its high efficacy and absence of systemic effects, this regimen could be a first choice method for the management of menopausal symptoms and for long-term preventive treatment in postmenopausal women.
OR8-06
RESULTS OF 6 MONTH USAGE OF PHYTOESTROGENS AND LOW-DOSE HORMONE REPLACEMENT THERAPY FOR TREATMENT OF CLIMACTERIC SYNDROME
N. Podzolkova1, A. Orekchov2, I. Sobenin2, V. Korennaya1 and V. Myasoedova2
1Russian Medical Academy For Postgraduate Education;2Institute of General Pathology and Pathophisiology, Russia
Objective: To compare the effectiveness and safety of low dose HRT (LD-HRT)and phytoestrogens for treatment of climacteric syndrome in postmenopausal women.
Methods: 159 early postmenopausal, healthy, normotonic, not overweight women aged 45–55 years with moderate climacteric syndrome were randomized in multicenter, placebo-controlled 6 month-study. Patients of first group (n = 19) were given LD-HRT “Angelic”® (1mg of 17-β-estradiol and 2 mg of drospirenon once a day), patients of the second group (n = 76) were given phytoestrogen composition “Karinat”® (procianidins – 27.3 mg, genistein – 2.5 mg, daidzein – 11.8 mg, resveratrol – 3.5 mg daily) Patients of the third group (n = 64) were given placebo.
Examination included ultrasound of uterus and ovaries, mammography, oncocolpocitology, detection of body mss index, arterial pressure and protrombin index (PTI). Severity of climacteric syndrome was evaluated by Kupperman's index and quality of life by Utian Scale (UQOLS).
Results: At the baseline patients didn't differ by original and weighted index of Kuperman and quality of life (р<0,05).
Original index of Kupperman lowered significantly in all three groups (р<0,005). In first group it lowered by −7,8 ± 6,9, in the second by −2,3 ± 4,5 and by −2,7 ± 4,3 in the third group. So, the effectiveness of phytoestrogens was comparable to placebo (р = 0,7), but lower than HRT (р = 0,02). Similar results were obtained for weighted index of Kupperman.
Deeper analysis of complaints, demonstrated that HRT was more effective than phytoestrogens for parastesias, myalgia, arrhythmia and headaches, but didn't show its advantages for insomnia, nervousness, melancholy, dizziness, weakness and palpitation.
Total UQOLS index didn't change in placebo and phytoestrogen group (+ 0,3 ± 1,5, 0,0 ± 2,4 respectively), but increased in the HRT-group by 9,4 ± 3,0.
Social, emotional and sexual components of quality of life increased in three groups, but only in HRT group this change was significant (р < 0,005). Medical component improved significantly in all three groups (р < 0,005).
Compliance rate in LD-HRT group was 93,3%, 93,4%, in phytogroup and 97% for placebo. No serious side effects were detected. Weight, arterial pressure and PTI didn't change significantly, as well as the results of ultrasound, cytological and mammoraphic examination.
Conclusion: LD-HRT can be used in early-postmenopausal women for treatment of moderate climacteric syndrome with prevalence of parastesias, myalgia, arrhythmia and headaches with low quality of life. Phytoestrogens can be administered to women with normal quality of life and prevalence of vasomotor symptoms.
OR8-07
SYSTEMIC ABSORPTION OF TRANSDERMAL TESTOSTERONE FLUCTUATES OVER TIME
S. Taher1,2, C. Bellone3, P. Bose1, A. Cahill1 and N. Panay1,2
1Queen Charlotte's and Chelsea Hospital, London, UK; 2Imperial college, London, UK; 3Chelsea & Westminster Hospital, London, UK
Objective: The aim of this study was to monitor hormone level patterns in women treated with either testosterone gel or testosterone releasing patch.
Design & Methods: Postmenopausal women presenting with symptoms of reduced libido were identified from two teaching hospitals and a private clinic. They each received supplements of either testosterone gel (10 mg/d testogel or 1ml/d testim) or a testosterone patch (300 μg/d intrinsa). Serum levels of free testosterone, SHBG, oestradiol and free androgen index were measured retrospectively.
Results & Conclusion: Serum from patients in the intrinsa patch group showed an initial increase in free testosterone level up to 24 weeks of treatment. Women treated with testosterone gel demonstrated fluctuation in testosterone level. Slight changes in SHBG levels were observed with testosterone gel but free androgen index remained constant within the physiological range. We conclude that various preparations of testosterone are differentially absorbed over time. This observation may explain why there is little direct correlation between symptomatology and serum testosterone.
Table 1 Blood levels at different intervals from commencing testim, testogel or intrinsa
OR8-08
SAFETY AND EFFICACY OF SELECTIVE ESTROGEN RECEPTOR MODULATORS ALONE AND IN COMBINATION WITH ESTROGEN
J. V. Pinkerton and D. W. Stovall
University of Virginia Health System; Charlottesville, Virginia, USA
Objective: Recent reanalysis of the Women's Health Initiative offers reassurance regarding safety of estrogen use for treatment of menopausal symptoms and prevention of bone loss in women under 60 and within 10 years of menopause. However, concerns regarding the stimulatory effects of estrogens on breast and endometrial tissue lead to the development of selective estrogen receptor modulators (SERMs), or estrogen agonists/antagonists. In addition to inhibitory effects on breast tissue proliferation, SERMS may have estrogen agonistic effects on bone and lipids. Concerns of SERM use include increased vasomotor symptoms, endometrial safety and increased venous thromboembolism (VTE). This review evaluates tamoxifen, raloxifene and bazedoxifene and their efficacy on menopausal symptom relief and endometrial safety, both as single agent therapy and in combination with estrogen.
Design: Review of current literature, from pubmed (1990–2008) using published papers and abstracts, on SERMS used either alone or in combination with estrogen for menopausal women.
Results: Tamoxifen is approved for use as adjuvant chemotherapy and chemoprevention of breast cancer, has demonstrated bone and cardioprotective benefits, but increases risk of endometrial hyperplasia and malignancy. Tamoxifen is thus not a good candidate to combine with systemic estrogen. Raloxifene decreases bone loss and vertebral factures and the risk of invasive breast cancer, without evidence of endometrial stimulation. Small clinical trials suggest safety when raloxifene is paired with local vaginal estrogen but higher rates of uterine hyperplasia when combined with systemic estrogen. Bazedoxifene appears to prevent bone loss and mildly increase vasomotor symptoms without stimulating the breast or endometrium. Small RCT suggest that bazedoxifene paired with conjugated estrogens prevents bone loss and relieves hot flashes without stimulating the endometrium or breast.
Conclusion: Current SERMS and those in development have potential benefits and risks and none to date serves as an ideal SERM- to prevent breast cancer, heart disease, osteoporosis and cognitive decline without stimulating the breast or the endometrium, nor increasing hot flashes or VTE. There is a need for newer estrogen antagonists/agonists with improved safety and tolerability profiles or that can be combined safely with estrogen. Early results on short term pairing of bazedoxifene and conjugated estrogens suggest endometrial safety when used for the treatment of menopausal symptoms, without the need for a progestin in women with a uterus. The combination of estrogen with a SERM may prevent bone loss and suppress vasomotor symptoms without stimulation of breast or endometrium.
OR8-09
TISSUE-SELECTIVE ESTROGEN COMPLEXES: THE PAIRING OF BAZEDOXIFENE WITH CONJUGATED ESTROGENS TO TREAT MENOPAUSAL SYMPTOMS AND PREVENT SKELETAL BONE LOSS
B. Komm and Y. Kharode
Wyeth Research, Collegeville, PA, USA
Objective: Hormone therapy (HT, estrogens alone or estrogens + progestin) is commonly used to treat menopausal symptoms (eg, hot flushes, vaginal atrophy) and to provide skeletal protection; however, there are safety concerns associated with HT. We hypothesized that the pairing of conjugated estrogens (CE) with a selective estrogen receptor modulator (SERM) in the form of a tissue-selective estrogen complex (TSEC) would result in a novel treatment paradigm providing the positive benefits of estrogens on menopausal symptoms and bone without uterine or breast stimulation. Here we describe the physiologic profile of a TSEC that pairs the SERM bazedoxifene (BZA) with CE, based on the results of in vivo experiments.
Design & Method: Skeletal, lipid, uterine, and vasomotor responses were assessed using rodent models. Animals were treated with BZA 0.1 to 10.0 mg/kg alone, CE 2.5 mg/kg alone, BZA paired with CE at respective doses, ethinyl estradiol 0.3 mg/kg, or vehicle control. An ovariectomized rat model of osteopenia was used to evaluate the effect of these treatments, after 6 weeks of dosing, on uterine wet weight and endometrial histology, lipid metabolism, and skeletal bone mass as measured by peripheral quantitative computed tomography of the proximal tibia. Effects on vasomotor instability (eg, hot flushes) were assessed using an ovariectomized rat tailskin temperature model.
Results: Over a range of doses (0.1–3.0 mg/kg), BZA paired with CE 2.5 mg/kg maintained skeletal bone mass in ovariectomized rats at a level similar to that of sham-operated rats and of either compound alone. In the same rodent model, total cholesterol levels were reduced by 25% with CE 2.5 mg/kg alone, which was further reduced by 15% to 20% with BZA/CE. Doses of BZA 3.0 mg/kg or greater were required to antagonize the stimulatory effect of CE 2.5 mg/kg on uterine endpoints. In the rat tailskin temperature model, doses of BZA up to 10 mg/kg, including the minimum bone-protective dose (0.3 mg/kg), were not found to antagonize the positive effect of CE 2.5 mg/kg on reduction of vasomotor instability.
Conclusion: Findings indicate that the pairing of BZA with CE effectively prevents loss of skeletal bone mass, reduces total cholesterol levels, and reduces vasomotor instability without uterine stimulation in vivo. This novel TSEC exhibits an optimal blend of tissue-selective activities, suggesting that BZA/CE would be a safe and effective option for the treatment of menopausal symptoms and prevention of postmenopausal osteoporosis.
Women and heart disease
OR9-01
DYDROGESTERONE AND 20-A-DIHYDRODYDROGESTERONE ACTIVITY ON NITRIC OXIDE SYNTHESIS IN HUMAN ENDOTHELIAL CELLS
P. Mannella, A. M. Sanchez, M. S. Giretti, A. Caruso, A. R. Genazzani and T. Simoncini
University of Pisa, Pisa, 56100, Italy
Objective: To investigate the effects of progesterone, medroxyprogesterone acetate, dydrogesterone and 20-α-dihydrodydrogesterone on endothelial synthesis of nitric oxide and characterize the signaling events recruited by these compounds.
Design & Method: Human endothelial cells from umbilical vein treated with Progesterone, medroxyprogesterone acetate, dydrogesterone and 20-α-dihydrodydrogesterone. We measured NO release, endothelial nitric oxide synthase (eNOS) activity and expression, and activation of ERK 1/2 and Akt.
Results: The administration of dydrogesterone alone or in combination with estrogen to endothelial cells results in neutral effects on nitric oxide synthesis and on the activity and expression of eNOS. In parallel, the stable metabolite 20-α-dihydrodydrogesterone acts similarly to natural progesterone, enhancing the expression of eNOS and inducing rapid activation of the enzyme through the regulation of the ERK 1/2 mitogen-activated protein kinase cascade. 20-α-dihydrodydrogesterone and P also potentiate eNOS induction by estrogens. On the contrary, medroxyprogesterone acetate does not trigger eNOS enzymatic activation and decreases the extent of eNOS induction by estrogen.
Conclusions: These findings support the concept that synthetic progestins act differently on vascular cells and that hormonal preparations may differ as to their cardiovascular effects.
OR9-02
ENDOGENOUS ANDROGENS AND ENDOTHELIAL FUNCTION IN EARLY POSTMENOPAUSAL WOMEN: A PILOT STUDY
M. A. Maturana1, M. C. Rubira2, F. M. Consolim-Colombo2, M. C. Irigoyen2,3 and P. M. Spritzer1,3
1Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil; 2Universidade de São Paulo, São Paulo, Brazil; 3Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
Objective: Although much progress has been made in the prevention and treatment of cardiovascular disease, it is still the leading cause of death among postmenopausal women. Changes in endothelial function play an important role in the pathophysiology of atherosclerosis and there is evidence suggesting that interventions to improve endothelial function may impact the progression and the risk of cardiovascular events. In turn, endogenous androgens are thought to be potential mediators of cardiovascular risk in women. Therefore, the aim of this study was to verify whether endogenous androgens are associated with changes on endothelial function in postmenopausal women.
Design & Method: This cross-sectional pilot study included 26 postmenopausal women aged 54 (±4) years. Anthropometric, clinical, and laboratory evaluations were performed. Endothelial function was assessed by dorsal hand vein compliance technique and flow-mediated dilatation was used. Acetylcholine (Ach) and sodium nitroprusside (SNP) dose-response curves were constructed to test the endothelium-dependent and –independent relaxation, respectively. Patients were stratified into 2 groups according to free androgen index (FAI) (higher or lower than the mean FAI of the studied sample).
Results: Median time of menopause was 6 years (interquartile range: 3–9). Waist-to-hip ratio and total testosterone levels were significantly higher in the group with FAI >2.5. Maximum vasodilatation (VD) with Ach and with SNP was similar across the groups stratified by FAI. However, the median dose of Ach for maximum vasodilatation was higher in the FAI group >2.5 (720 (360–3600) ng/mim) than in the group of FAI ≤ 2.5 (36 (0.36–360) ng/mim), p = 0.005. Positive correlations were observed between Ach doses for maximum VD and FAI (r = 0.473, p = 0.015) and waist (r = 0.510, p = 0,011). Sex hormone binding globulin (SHBG) was negatively correlated with Ach doses (r = −0.400 p = 0.043).
Conclusion: The results from this study suggest that androgen levels, even if still in the normal limits, are related to early changes on endothelial function in recently postmenopausal women. Longitudinal studies are needed to evaluate the clinical relevance of these findings.
OR9-03
ESTRADIOL REDUCES F2α-ISOPROSTANE LEVELS BOTH IN POSTMENOPAUSAL WOMEN AND IN ENDOTHELIAL CELLS
A. Laguna1, P. J. Oviedo1, S. Novella1,2, A. Sobrino1, A. Cano3 and C. Hermenegildo1,2
1Research Foundation, Hospital Clinico Universitario, Valencia, Spain; 2Dept. Physiology, University of Valencia, Valencia, Spain; 3Dept. Pediatrics, Obstetrics and Gynaecology, University of Valencia, Valencia, Spain
Objective: F2α-isoprostanes are prostaglandin-like products of nonenzymatic, free radical catalysed peroxidation of arachidonic acid, and are considered a stable, good biomarker for in vivo oxidative stress. F2α-isoprostanes exert different cardiovascular actions and increased F2α-isoprostane levels have been found in human atherosclerotic lesions. Estradiol has been proposed to exert antioxidant effects both in vitro and in vivo in many biological systems. We investigated (1) the effects of hormone therapy on the plasma levels of F2α-isoprostanes, and (2) the effects of estradiol on F2α-isoprostane production by cultured human umbilical vein endothelial cells (HUVEC).
Design & Method: Sixty one healthy postmenopausal women were treated in a randomized trial with estradiol by either oral (2 mg/day, 28 women) or transdermal (50 μg/day, 33 women) route for 4 weeks. Then, women in each group were randomized to oral progestogen, either micronized progesterone (300 mg/day) or medroxyprogesterone acetate (5 mg/day) for 2 additional weeks. Plasma samples were collected before and at the end of each treatment period. HUVEC were exposed to different concentrations (0.1–10 nM) of estradiol for 24 h. In some experiments, progesterone and medroxyprogesterone (1–100 nM) and the estrogen receptor antagonist ICI182780 were added. F2α-isoprostane content was extracted from plasma or culture medium by using specific affinity columns and was assayed by using a F2α-isoprostane commercial enzyme immunoassay.
Results: A significant reduction (21%, p < 0.05 vs. baseline values) in the levels of F2α-isoprostanes was detected only in women receiving transdermal estradiol, alone or in combination with medroxyprogesterone acetate. In HUVEC, estradiol (1 and 10 nM) inhibited F2α-isoprostane production by 36% and 49%, respectively (p < 0.001 vs. control). ICI182780 reversed the estradiol-induced reduction of F2α-isoprostanes. Progestogens alone did not alter F2α-isoprostane production. When used in combination with estradiol, progesterone reversed the estradiol-induced reduction of F2α-isoprostane production while medroxyprogesterone did not.
Conclusion: Estradiol alone or associated with medroxyprogesterone acetate decreased plasma levels and endothelial cell production of F2α-isoprostanes. These data elucidate additional details of the beneficial effect of estradiol on oxidative stress, a relevant mechanism in atherogenesis.
Supported by Spanish Ministerio de Sanidad y Consumo, Instituto de Salud Carlos III (grants FIS 06/0589 and Red HERACLES RD06/0009) and Consellería de Sanidad, Generalitat Valenciana (grants AP 09/2007 and AP 10/2007). PJ Oviedo holds a post-doc position, and A Sobrino is a fellowship recipient from the FPI program (BFPI 06/145), both from Conselleria de Empresa, Universidad y Ciencia, Generalitat Valenciana, Spain.
OR9-04
HORMONE REPLACEMENT THERAPY INITIATED SOON AFTER MENOPAUSE MAY HAVE SIGNIFICANT MORTALITY BENEFITS—A PRECIS DATABASE STUDY
A. Ayyad, D. Brennan, B. Hoar, B. J. Hoogwerf and J. C. Huang
Cleveland Clinic, Cleveland, Ohio, United States
Objective: The HERS Trial (1998) found no mortality benefit to hormone replacement therapy (HRT) in a relatively older population of postmenopausal women (mean age 66.7). Recent subgroup analyses of the Women's Health Initiative (WHI) have indicated possible benefit of HRT in postmenopausal women when therapy is initiated at a younger age and sooner after menopause. We sought to evaluate mortality in association with use of HRT in postmenopausal women at our institution.
Design and Methods: Women presenting for preventive cardiology clinic visits at a large tertiary medical center in the years 2000–2007 were identified from a prospectively collected database and assessed for current or past use of HRT. Mortality data were collected from the Social Security Death Index. The chi square statistic was used to evaluate significance of the results.
Results: A total of 2432 women, 83.5% white, mean age of 55.7 ± 13.8 were evaluated in the study period. Among 1041 women who reported receiving HRT of any form either currently or in the past, the mortality was 5.03% compared with 8.76% of the 1391 women who had never received HRT (p = <0.001). Of 859 patients with a history of cardiovascular disease (CVD), mortality rate was 10.67% among HRT patients compared to 17.92% in non-HRT patients (p = 0.003). Similarly, in 1573 women without history of CVD, death occurred in 1.82% of HRT patients versus 3.88% of non-HRT patients (p = 0.019). Mortality benefit was significant even though patients who received HRT were significantly older than those who never did (52.6 vs. 59.9 years, p = 0.001). Multivariate analysis adjusting for age, smoking, blood pressure, HDL, and CVD history continued to show a benefit of HRT use (hazard ratio 0.606, p = 0.040). Assessed by time from menopause, 5 year mortality was significantly lower in HRT users at < 5 and 5–10 years from menopause (p = 0.003), but was not significantly different at >10 years.
Conclusion: In our study of postmenopausal women younger than those evaluated in the HERS trial, current or past HRT use was associated with significantly lower mortality in both secondary and primary cardiovascular prevention. This effect was most pronounced in women < 10 years from menopause, supporting other trial findings that earlier initiation of HRT after menopause may have beneficial cardiovascular effects.
OR9-05
MENOPAUSAL AGE, ENDOTHELIAL FUNCTION AND CARDIOVASCULAR RISK
S. Mulvagh, T. Behrenbeck, B. Lahr, T. Zais and V. M. Miller
Mayo Clinic, Rochester, MN, USA
Objective: Cardiovascular disease progresses on a continuum throughout life and increases in women at menopause. Therefore, timing of interventions, such as for hormonal therapy, may be critical in order to slow disease progression. Peripheral flow-mediated reactive hyperemia (PRH) is accepted as a marker of endothelial dysfunction and an indicator of early disease processes. This study tested the hypothesis that endothelial dysfunction would increase with time past menopause.
Design andMethod: A subset of asymptomatic women enrolled in KEEPS (Kronos Early Estrogen Prevention Study, a clinical trial of hormone therapy on cardiovascular disease in early (<3 year) menopause, were evaluated prior to randomization to treatment for conventional risk factors as well as CIMT by ultrasound, CAC by electron beam computed tomography, and PRH by ENDOPAT®.
Results: One hundred and three women participated. All were Caucasian and none were diabetic. Four women were current smokers, 26 past smokers and 73 never smokers. Fourteen women had positive CAC scores (range 0.5-133) and two women had CIMT lesions >40%. There was no difference in conventional risk factor profiles between women with positive CAC and CIMT scores compared to those without. Total cholesterol and LDL were positively correlated with time past menopause; these values did not correlate with PHR. PHR did not correlate with time past menopause. However, PHR was inconclusive or abnormal in 40% of the entire cohort and in 45% of women within 12 months of menopause. These women could not be distinguished using conventional risk factors (see Table).
Conclusions: 1) Fifteen percent of women in this fairly low risk group exhibited quantifiable vascular lesions. 2) In a subset of women without lesions and in whom standard assessment algorithms did not detect risk, endothelial dysfunction was present within the first 12 months of menopause. PRH may provide an additional reference point to assess early disease processes in some menopausal women and possibly identify those for whom hormonal therapy may be beneficial.
OR9-06
MENOPAUSAL COMPLAINTS ARE ASSOCIATED WITH CARDIOVASCULAR RISK FACTORS
G. C. M. Gast1,5, D. E. Grobbee1, V. J. M. Pop2, J. J. Keyzer3, C. J. M. Wijnands-van Gent3, G. N. Samsioe4, P. M. Nilsson5 and Y. T. van der Schouw1
1University Medical Center Utrecht, Utrecht, The Netherlands; 2University of Tilburg, Tilburg, The Netherlands; 3Diagnostic Center Eindhoven, Eindhoven, The Netherlands; 4Lund University Hospital, Lund, Sweden; 5University Hospital, University of Lund, Malmö, Sweden
Objective: It has been hypothesized that women with vasomotor symptoms differ from those without with respect to cardiovascular risk factors or responses to exogenous hormone therapy (HT). We studied whether the presence and extent of menopausal complaints is associated with cardiovascular risk profile.
Design & Method: Data were used from a population-based sample of 5,523 women, aged 46 to 57 years, enrolled between 1994 and 1995. Data on menopausal complaints and potential confounders were collected by questionnaires. Total cholesterol, systolic and diastolic blood pressures and BMI were measured. Linear and logistic regression analysis was used to analyse the data.
Results: Night sweats were reported by 38% and flushing by 39% of women. After multivariate adjustment, women with complaints of flushing had a 0.27 mmol/L [95% CI 0.15, 0.39] higher cholesterol level, a 0.60 kg/m2 [95% CI 0.35, 0.84] higher BMI, a 1.59 mm/Hg [95% CI 0.52, 2.67] higher systolic blood pressure, and a 1.09 mm/Hg [95% CI 0.48, 1.69] higher diastolic blood pressure compared to asymptomatic women. Flushing was also associated with hypercholesterolemia (OR 1.52 [95% CI 1.25, 1.84]) and hypertension (OR 1.20 [95% CI 1.07, 1.34]). Results were similar for complaints of night sweating.
Conclusion: The findings support the view that menopausal complaints are associated with a less favourable cardiovascular risk profile. These findings substantiate the view that differences in presence of menopausal symptoms as a reason for using HT could explain discrepant findings between observational research and trials.
OR9-07
PROSTANOIDS PRODUCTION AND REGULATION BY ESTROGENIC COMPOUNDS IN ENDOTHELIAL CELLS
P. J. Oviedo1, S. Novella1,2, A. Sobrino1, A. Laguna1, A. Cano3 and C. Hermenegildo1,2
1Research Foundation, Hospital Clinico Universitario, Valencia, Spain; 2Dept. Physiology, University of Valencia, Valencia, Spain; 3Dept. Pediatrics, Obstetrics and Gynaecology, University of Valencia, Valencia, Spain
Objective: In the cardiovascular system, two main prostanoids play an essential role in vascular physiology: thromboxane A2 (TXA2), which exhibits a proaggregant and vasoconstrictor profile, and prostacyclin (PGI2), a potent vasodilator. Prostanoids production is regulated by the availability of free arachidonic acid and the activity of COX. Release of arachidonate from membrane phospholipids is mainly mediated through phospholipase A2 (PLA2). Arachidonate is converted to prostaglandin H2 by two cyclooxygenases (COX-1 and COX-2). The unstable prostaglandin H2 is then transformed into TXA2 (by thromboxane synthase, TXAS) or PGI2 (by prostacyclin synthase, PGIS). Clinical and experimental data support the consideration of endothelium as a target for estradiol and other estrogenic compounds. Aims of this study were (1) to examine the effects of several estrogenic compounds on prostanoid production by cultured human umbilical vein endothelial cells (HUVEC), (2) to elucidate the role of estrogen receptors (ER) and (3) to study the regulation of PLA2, COX-1, COX-2, TXAS and PGIS.
Design & Method: Cells were exposed to different concentrations of estradiol, genistein, daidzein or raloxifene for 24 hours and PGI2 and TXA2 production was measured in culture medium. At the same time of incubation, PLA2, COX-1, COX-2, PGIS and TXAS protein content and mRNA expression were measured by Western blot and QRT-PCR, respectively. Antagonists were used to study the role of ER on the observed effects: ICI 182780 (ERα and ERβ antagonist), PPT (ERα antagonist) and DPN (ERβ antagonist).
Results: All the tested compounds stimulate prostacyclin production in a dose-dependent manner, although concentrations to achieve the same stimulation were higher for phytoestrogens compared to estradiol or raloxifene. Estradiol did not modify thromboxane production. COX-1, COX-2 and PGIS protein content and mRNA expression were augmented, with differences between the tested compounds. PLA2 and TXAS expression remained unaltered. ICI 182780 prevented the increase of prostacyclin production induced by estradiol and phytoestrogens, but not raloxifene effects. Estradiol effects were mainly mediated through ERα stimulation.
Conclusion: Estrogenic compounds increased endothelial PGI2 production through ER-mediated mechanisms, which involve enhanced COX-1, COX-2 and PGIS expression, without affecting TXA2 production.
Supported by Spanish Ministerio de Sanidad y Consumo, Instituto de Salud Carlos III (grants FIS 06/0589 and Red HERACLES RD06/0009) and Consellería de Sanidad, Generalitat Valenciana (grant AP 09/2007 and AP 10/2007). PJ Oviedo holds a post-doc position, and A Sobrino is a fellowship recipient from the FPI program (BFPI 06/145), both from Conselleria de Empresa, Universidad y Ciencia, Generalitat Valenciana, Spain.
OR9-08
THE ASSOCIATION OF BLOOD LEAD LEVELS AND MORTALITY IN OLDER WOMEN: THE STUDY OF OSTEOPOROTIC FRACTURES
Naila Khalil1, Jane A. Cauley1, John W. Wilson1, Evelyn O. Talbott1, Lisa Morrow1, Marc C. Hochberg2, Teresa Hillier3, Susan B. Muldoon4 and Steven R. Cummings5
1University of Pittsburgh, Pittsburgh, PA, USA; 2University of Maryland, Baltimore, MD, USA; 3Center for Health Research, Kaiser Permanente Northwest/Hawaii, Portland, OR, USA; 4School of Public Health, and Information Sciences, University of Louisville, KY, USA; 5San Francisco Coordinating Center, California Pacific Medical Center Research Institute, San Francisco, CA, USA
Objectives: Higher Blood lead levels are associated with increased all cause and cardiovascular mortality in the general population and in exposed occupational cohorts. To test the hypothesis that community residing elderly women with higher blood lead levels due to environmental exposures experience higher all cause and cause specific mortality.
Design and Methods: Prospective cohort study of 533 women aged 65–87 years enrolled in the Study of Osteoporotic Fractures at 2 US research centers (Baltimore, MD; Monongahela Valley, PA) from 1986–1988. Blood lead levels were determined by atomic absorption spectrometry. Participants were divided into two categories based on distribution of blood lead levels in μg/dl into “low: ≤ 7” and “high: ≥ 8”. Information on mortality was collected over 10 years. Relative hazard of total and cause specific mortality by blood lead levels was calculated using Cox proportional regression analyses.
Results: The mean blood lead level was 5.3 ± 2.3 μg/dl (range 1–21). After 10.0 ± 3 years of >95% complete follow-up, the 123 women who died had slightly higher (±SD) blood lead 5.56 (±3) μg/dl than survivors: 5.17(±2.0) (p = 0.09). High blood lead levels were associated with increased mortality. Women with baseline blood lead level of ≥ 8 μg/dl had a 76% increased risk of dying. (Age and clinic adjusted Hazard Ratio [HR] = 1.76; 95% confidence interval [CI] 1.14, 2.72) (p = 0.010) compared to women in low blood lead level group. Multivariate models included age, clinic, smoking status, hypertension and ability to stand from a chair without using arms; Women in high blood lead group had a 73% higher risk of all cause mortality (HR = 1.73; 1.11, 2.69) (p = 0.015), compared to women in with lower blood lead levels. In cause-specific mortality analysis, increased mortality was predominantly due to cardiovascular disease. The multivariate adjusted hazard ratios (95% CI) for CVD mortality for high versus the low blood lead levels were 1.85(1.00, 3.50), and coronary heart disease 3.44 (1.43, 8.30) (p < 0.006). There was no association of blood lead and mortality from stroke, cancer and other causes.
Conclusions: Women with blood lead levels of ≥ 8 μg/dl experienced increased mortality, in particular from coronary heart disease, as compared to those with lower blood lead levels.
OR9-09
THOMBOPHILIA AND THROMBOEMBOLIC COMPLICATIONS OF HORMONAL REPLACEMENT THERAPY
A. D. Makatsariya, V. O. Bitsadze, S. M. Baimuradova and S. V. Akinshina
Department of obstetrics and gynecology, I. M. Sechenov Moscow Medical academy, Russian Federation
Objectives: Hormonal replacement therapy (HRT) has been shown to be associated with arterial and venous thromboembolic complications. Nevertheless pathogenetic mechanisms of this phenomenon are not completely understood. Our aim was to evaluate the role of multigenic thrombophilia and antiphospholipid syndrome (APS) as pathogenetic factors of HRT-induced thrombosis.
Methods: We examined 41 women with tromboembolic complications of oral HRT (deep vein thrombosis, pulmonary embolism, superficial thrombophlebitis, Budd-Chiary syndrome, retinal thrombosis, and stroke) for genetic thrombophilia and antiphospholipid antibodies (APA). Of note, 75,6% women had obstetric complications in their personal history (placental abruption, preeclampsia, fetal loss syndrome).
Results: Thrombophilia was detected in 100% patients: APA in 43,9%; homozygous and heterozygous FV Leiden in 7,3% and 26,8% respectively; PAI-1 4G/5G polymorphism in 41,4%; prothrombin G20210A in 12,2%; homozygous and heterozygous GPIа 807С/Т in 4,9% and 14,6%, homozygous and heterozygous ACE I/D in 12,1 and 21,9% respectively; combination of genetic thrombophilia and APA-circulation in 36,6%; multigenic thrombophilia in 85,4%.
Сonclusions: Genetic thrombophilia and APS have synergic effect with HRT and may induce prothrombotic state due to the activation of coagulation, inflammation and endothelial dysfunction. Multigenic thrombophilia and combination of genetic and acquired (APS) thrombophilia might be the most unfavorable condition. Screening for thrombophilia seems to be useful before the administration of HRT. Special attention should be paid to the history of obstetrics complications. If thrombophilia is detected, HRT is absolutely contraindicated.
Aging and hormones
OR10-01
EFFICACY OF DIFFERENT ORAL ESTROGENS DOSAGES IN THE SIMPTOMATIC MENOPAUSE TREATMENT
F. Río de la Loza1, A. Alvarado1, A. Murillo2 and A. Arzola3
1Institución Gineco-obstétrica y de Perinatologia, Mexico city, Mexico; 2Hospital Ángeles de Lomas, Mexico city, Mexico; 3Instituto Biosen A.C, Mexico city, Mexico
Objetive: To compare efficacy of a traditional dose hormonal therapy (HT) against low and ultralow dose long cycle HT in symptomatic menopausal women with uterus.
Design & Method: A prospective, longitudinal, open label study was carried out in postmenopausal TH free women, with Kupperman Index ≥ 15, signed informed consent, normal mammogram and cytology, who were assigned randomly to one of following treatment schemes for 6 months: Group A, 0.625mg of esterified estrogens (EE) per day + 14 days of 100mg oral micronized progesterone monthly, group B 0.3mg of EE per day and group C, 0.15mg of EE per day. These two last groups -long cycle therapy- received at the end of the 6thmonth, 14 days of 100mg oral micronized progesterone. The efficacy was evaluated by improvement of menopause symptoms and menopause quality of life scale (MENOQUOL). Safety was monitored by incidence of adverse events, changes in endometrial thickness by ultrasonography and hormonal and lipid profiles. For the statistical analysis the population ITT was used and carried out by means of an ANOVA test.
Results: A total of 71 patients were enrolled, 45 of them completed 6 months of treatment: group A = 14, group B = 15 and group C = 16 patients, with average age of 56 years. Improvement significantly (p < 0.05) showed in all treatment groups in Kupperman's index and MENOQUOL from baseline to the end of the study, however there were not statistical differences among the treatments.
The FSH decreased and estradiol levels increased, with a different statistical p < 0.05 for groups A and B. The lipid profile and the endometrial thickness didn't demonstrate statistically significant changes in any of the groups.
The most relevant adverse events were vaginal bleeding which was showed in the group A: 73%, B: 4% and C: 0% and breast tenderness: group A: 59%, group B: 32%, and group C: 17%. There were not serious adverse events.
Conclusions: Results demonstrate efficacy in all study doses in the improvement of menopause symptoms and quality of life, this supports the use of ultra low dose for symptomatic patients. The advantages of long cycle therapy with ultra low dose are less exposure to hormones studied and lower incidence of adverse events, being this the main reason of non compliance. Endometrial thickness is minimal with low and ultralow doses and similar to the traditional HT.
OR10-02
EFFICACY OF TWO LOW-DOSE REGIMENS OF CONJUGATED ESTROGEN VAGINAL CREAM IN POSTMENOPAUSAL WOMEN WITH ATROPHIC VAGINITIS
G. Bachmann1, C. Bouchard2, D. Hoppe3, R. Ranganath4, C. Altomare4, A. Vieweg4, G. Graepel4 and E. Helzner4
1UMDNJ Robert Wood Johnson Hospital Medical School, New Brunswick, NJ, USA; 2Clinique RSF, Inc., QC, Canada; 3Pacific Coast Women's Health, Encinitas, CA, USA; 4Wyeth Research, Collegeville, PA, USA
Objective: A twice-weekly low-dose regimen of Premarin Vaginal Cream (PVC), commonly used in clinical practice for atrophic vaginitis, has not been studied. This prospective, randomized, placebo-controlled, double-blind study compared the efficacy of twice-weekly and daily PVC to matching placebo regimens for atrophic vaginitis.
Design & Method: This outpatient, multicenter, double-blind, randomized, placebo-controlled phase IIIb trial was conducted in Canada and the United States. Postmenopausal women, aged 45 to 80 years, with moderate-to-severe vaginal atrophy, an intact uterus, and an endometrial double-wall thickness < 5 mm as assessed by transvaginal ultrasound, were randomized to PVC 0.5 g (0.3 mg Premarin) or placebo for 21 days on with 7 days off, or PVC 0.5 g or placebo used twice weekly. After 12 weeks, all subjects received 9 months of PVC open-label at the same respective dosing schedules. Primary endpoints were vaginal maturation index (VMI; % superficial cells), vaginal pH, and severity of most bothersome symptom at Week 12. Secondary endpoints included efficacy data (VMI, vaginal pH) at Week 52. Endometrial safety was also evaluated, but these findings are reported elsewhere.
Results: Of 423 subjects enrolled, 419 (99%) were included in the modified intent-to-treat (MITT) population for VMI, 403 (95%) for vaginal pH, and 317 (75%) for severity of most bothersome symptom. The MITT population included all subjects who received at least 1 dose of study medication and had a baseline and postbaseline value. At Week 12, the change in VMI from baseline was similar with daily and twice-weekly regimens (28% and 26%, respectively) and significantly higher compared with placebo (3%, P < 0.001, and 1%, P < 0.001, respectively). The change in vaginal pH from baseline was similar with both regimens (approximately – 1.6 for both) and significantly higher compared with placebo (−0.4, P < 0.001, and −0.3, P < 0.001, respectively). Most bothersome symptom at 12 weeks was also significantly improved with daily and twice-weekly regimens (P < 0.01 and P < 0.001 vs placebo, respectively). For both daily and twice-weekly regimens, the changes from baseline in VMI (26% and 17%, respectively) and vaginal pH (−1.8 and −1.5, respectively) at Week 52 were similar to those observed at Week 12. Overall, daily and twice-weekly regimens of PVC were well tolerated and no safety concerns were noted.
Conclusion: A twice-weekly low-dose PVC 0.5-g regimen was effective, provided similar relief of vaginal atrophy as a daily regimen, and was safe and well tolerated.
OR10-03
ORAL MELATONIN IMPROVES REPRODUCTIVE HORMONES PATTERN DURING THE COURSE OF MENOPAUSE: FIRST CASE REPORT
B. Díaz1 and P. Llaneza2
1Universidad de Oviedo, Oviedo, Asturias, Spain; 2Hospital Universitario Central de Asturias, Oviedo, Asturias, Spain
Objective: The pineal gland through its hormone melatonin is involved in the mechanisms that regulate the aging process involved in the onset of menopause. Considering the melatonin changes experienced during pre-, peri- and postmenopause, an influence of melatonin on the hormonal changes associated to menopause transition could be expected. We investigated the effects of melatonin administration on the reproductive hormones LH, FSH and 17β-estradiol during that period of the reproductive life.
Design & Method: The study comprised a longitudinal 71/2-yr period form June 1999 up to Janury 2007. Oral melatonin as a tablet, Schiff ®Products, Salt Lake City, UT, USA, was given in two different periods, 1.5 mg, every night, 10 min before bed time (23.30-00.30 h). The melatonin intake began on December 2000 and was maintained up to February 2002. The second period with a melatonin intake extended from January 2003 up to May 2005, and it was followed by new period of melatonin withdrawal up to January 2007. Fasting blood samples were obtained between 09.00 to 10.00 h by venipuncture. Hormone determinations. LH and FSH were determined using radioisotopic kits. Serum estradiol was determined by a double bound antibody RIA.
Results: In the present case report oral melatonin was given in two different periods of the reproductive aging. The first stage, before to start the melatonin intake, showed a status in accordance with a normal reproductive period. At the first oral melatonin intake period, FSH levels were lower and the E2 levels were higher than months before. The third stage, during melatonin withdrawal, resulted in an increase of FSH levels (38.8 U/L) and decreased E2 levels (13 pg/ml). At the second period with oral melatonin intake, FSH concentrations were again within the range of reproductive age standard values for another year and E2 levels remained elevated. The fifth stage of the study at melatonin withdrawal extended from the end of May 2005 up to January 2007. The hormone determinations of this last block showed an important increase of FSH levels (82.7, 84.8 or 94.7 U/L) and a decrease in E2 levels (6.2, 8 or 11 pg/ml).
Conclusión: The present results point out for the first time that melatonin can induce a delay of endocrine parameters associated to the menopause onset in the specific patient under study.
OR10-04
STOPPING HRT—WERE WOMEN ILL ADVISED?
H. Currie1, G. Cumming2 and N. Panay3
1Dumfries and Galloway Royal Infirmary, Dumfries, Scotland UK; 2Dr Gray's Hospital, Elgin, Scotland, UK; 3Queen Charlotte's & Chelsea and Chelsea and Westminster Hospital, London UK, Imperial College London, UK
Introduction: In 2002 publication of the Women's Health Initiative trial, claiming significant health risks from the use of HRT received widespread media attention and led to millions of women worldwide choosing to, or being advised to stop taking HRT. Since then, further analyses have shown that for the majority of women taking HRT, the benefits far outweigh the risks. Although for some women stopping HRT was the right decision, it is feared that many women continue to suffer unnecessarily from menopausal symptoms such as hot flushes, night sweats, poor sleep, mood swings, joint aches and vaginal dryness.
Methods: To assess the extent of the effect of women stopping HRT over the last 5 years, a new survey was developed on the popular website www.menopausematters.co.uk in collaboration with Women's Health Concern, Daisy Network and the British Menopause Society in the UK. Analysis of results so far in 222 respondents has shown that: 49.5% stopped HRT on the advice of their doctor while 50.5% chose to stop themselves. Of those who stopped HRT themselves, 65% were influenced by the media, 28% being strongly influenced. Worryingly, of those who would most benefit from HRT (women under the age of 50), 71% stopped without medical advice.
Results: Of the women who had previously taken HRT for menopausal symptoms, 95% had return of symptoms; flushes, night sweats and poor sleeping being the most common, followed by mood changes, joint aches and vaginal dryness. Return of symptoms affected ability to work in 33%, ability to make decisions in 40%, personal relationships in 51%. Overall, 77% felt that their quality of life was worse since stopping HRT, 18% felt that it was the same and 5% better. HRT was restarted by 41% and the symptoms were relieved in 88% of those that restarted. Alternative therapies were taken by 49% but only 15% of those found them effective. Almost half (49%) of women would not have stopped HRT given the current understanding of risk.
Conclusion: In conclusion, media had a huge influence on women's decision on whether or not to continue HRT. Menopause symptoms often recur on stopping HRT. These symptoms significantly affect quality of life, the ability to work and personal and social relationships. Women and their carers should have access to up to date information so that decisions based on reports from studies can be reviewed as new information becomes available.
OR10-05
SYMPTOMATIC CHANGES IN POSTMENOPAUSE WITH DIFFERENT METHODS OF HORMONAL THERAPY
Marcelino Hernández-Valencia, Arturo Zárate, Lourdes Basurto, Renata Saucedo, Carlos Vargas, Miriam Ruiz, Elizabeth García, Antonio Vargas and Leticia Manuel
Research Endocrine Unit, Specialties Hospital, National Medical Center, Instituto Mexicano del Seguro Social, México, D. F.
Objective: The diversity of opinion in the adverse effects of therapy used to treat the postmenopausal symptoms, has originated the use of diverse ways and mechanisms of action that should be explored, since the biodisponibility of the pharmacological drugs is variable. The actual tendency is to obtain the therapeutic efficacy in base to select the way of administration from hormonal therapy (HT).
Design & Method: As prospective study, in random form 4 groups with postmenopausal women were formed. The group 1 received conjugated estrogens by oral way, the group 2 a synthetic steroid, the group 3 estradiol by nasal aspersion way and the group 4 utilized transdermal estradiol through parch. The evaluation criterion in efficacy of HT was the Greene scale that values six components (vasomotor, sexual, depression, somatic, psychological, anxiety) which applied in each patient before the hormonal intervention and later each month until the 6 months. Also, was investigated association of insulin resistance and changes in biochemical markers of fibrinolysis. LH, FSH and estradiol concentrations were determined by chemiluminiscence and the comparison among groups was done with Student t test before and after processing.
Results: The vasomotor component showed significant descent (p < 0.05) with the use of the four types of HT, the sexual component showed descent with the use of HT nasal, oral estrogens and transdermal way, in depressive component differences with oral synthetic steroid and with conjugated oral use was observed, upon analyzing the somatic component was observed decrease of the symptom with use of nasal and transdermal way, the psychological changes were observed with use of oral synthetic steroid and transdermal, the anxiety had difference with the nasal and with the oral conjugated way, although all the forms of HT in this component had an irregular pattern of changes. When compared coagulation markers and insulin resistance changes, nasal showed a mild increment in PAI-1, trandermal induced a significant decrement in both PAI-1 and HOMA-IR values, with synthetic and conjugated use were unchaged.
Conclusion: The changes in response to each way of pharmacological administration could be due to estrogens have genomic and not genomic effects, moreover can exist absorption variability with repercussion in the control of symptoms, which should be considered when selecting the way in the patient that will initiate HT.
OR10-06
THE EFFECT OF OVARECTOMY ON THE MULTIPLE SCLEROSIS COURSE
P. Koliba1, O. Zapletalová2 and P. Hradílek2
1Dept. of Obstetrics and Gynecology University Hospital, Olomouc, Czech Republic; 2Dept. of Neurology University Hospital, Ostrava, Czech Republic
Objective: Multiple sclerosis (MS) as an autoimmune, inflammatory and neurodegenerative disease is affected by hormonal changes during different life periods. Multiple sclerosis primarily attacks adults, with the age of onset typically between 20 and 50 years, and is more common in women than in men. The ratio is 2-3 : 1. Ovarectomy (OE) in premenopausal women as a strong, important artificial intervention is cause of the acute estrogen deficiency syndrome.
Due to this changes, the levels of gonadotrophins are increased with maximum values 4 months after the surgery following by their decrease. The symptoms of estrogen deficiency syndrome can be similar to MS symptoms.
Material and Methods: a retrospective analysis of 35 patients with MS diagnosis. 25 of the group were diagnosed with secondary progressive (SP) form of the disease and 10 with relapsing-remitting (R/R) form.
Results: In the SP group we observed neurological deterioration in 10 women. 4 patients in the R/R group had relapses with improvement after the treatment. In most patients we observed worsening symptoms of MS as fatigue, depression, urinary symptoms, spasticity and vegetative syndromes.
Conclusion: Hormonal changes resulting from ovarectomy are closely linked to MS relapse and with the change of MS course into secondary progressive.
OR10-07
THE RESTAGE COLLABORATION's REVISED RECOMMENDATIONS FOR STAGING REPRODUCTIVE AGING
S. D. Harlow1, K. Cain2, S. Crawford3, L. Dennerstein4, N. Fugate-Woods2, R. Little1, E. S. Mitchell1, B. Nan1, J. Randolph1, J. Taffe5 and M. Yosef1
1University of Michigan, Ann Arbor Michigan, USA; 2University of Washington, Seattle Washington, USA; 3University of Massachusetts, Worcester Massachusetts, USA; 4University of Melboune, Melbourne Victoria, Austalia; 5Monash University, Clayton Victoria, Australia
Objective: In July 2001, the Stages of Reproductive Aging Workshop (STRAW) proposed bleeding and hormonal criteria for defining onset of the early and late menopausal transition. STRAW's recommendations reflected expert consensus following review of emerging proposals from several cohort studies but were not verified empirically. STRAW recommended a shorter interval of amenorrhea than the current 90-days amenorrhea for late transition and >7-day change in cycle length for early transition. The ReSTAGE Collaboration (ReSTAGE) conducted a quantitative evaluation of the STRAW recommendations with the aim of reaching a consensus regarding optimal bleeding criteria for staging reproductive aging and of providing more precise guidance for use of hormonal criteria.
Design & Method: ReSTAGE used prospective menstrual calendar data from four cohorts (TREMIN (n = 735), Melbourne Women's Midlife Health Project (n = 216), Seattle Midlife Women's Health Study (SMWHS) (n = 279), and Study of Women's Health Across the Nation (SWAN) (n = 2270)) to comparatively assess proposed bleeding criteria for the the early and late menopausal transition. For each proposed bleeding criteria, we assessed frequency of, concordance in age at, time to menopause from and association with serum FSH. For FSH criteria we assessed association with bleeding criteria and FMP.
Results: Supported the STRAW recommendation that 60-days of amenorrhea be used to define onset of the late menopausal transition. An annual serum FSH measure > = 40 IU/L is an independent marker of transition (but less predictive than bleeding criteria) and could be incorporated, in conjunction with bleeding markers, into the STRAW paradigm for markers of the late transition. Experience of hot flashes added no information in the presence of hormonal and bleeding criteria. The early transition may be best described by ovarian activity consistent with bleeding criteria of a persistent 7 or more day difference, as recommended by STRAW. Other proposed bleeding criterion for early transition are consistent with changes associated with the late transition.
Conclusion: This empirical assessment supported the STRAW recommendations that a) > = 60-days of amenorrhea be used to define the late menopausal transition and b) that early transition is consistent with a persistent 7 or more day difference in length of consecutive cycles. Serum FSH criterion could be incorporated into the STRAW paradigm to facilitate prediction of proximity of the FMP.
OR10-08
THE SKIN HYALYRONIC ACID IN POSTMENOPAUSAL WOMEN AFTER TOPIC ISOFLAVONE TREATMENT
A. Moraes1, R. C. Teixeira1, M. A. Haidar1, M. J. Sim[otilde]es1, R. S. Sim[otilde]es1, M. T. Patriarca1, J. M. Soares Jr1, C. Verna1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina de São Paulo, São Paulo, São Paulo, Brazil
Objective: To evaluate in the effects of estradiol and isoflavones on the concentration of hyaluronic acid (ha) in skin of postmenopausal women. Design e methods: a prospective, randomized, and double-blind clinical trial was performed on 30 postmenopausal women (aged 45-55) with topical administration of estradiol and isoflavones on facial skin for 24 weeks. The participants were divided into two groups: GI- 17beta-estradiol 0.01% and GII- isoflavones 40%, skin biopsies were performed in each patient before and after the treatment. The concentration leves of HA in skin samples were determined through a fluorescence-based assay method with hyaluronan-binding protein and europium-labeled streptavidin. Also, we evaluated the histomorphometry of the postmenopausal skin The statistical analysis was performed by the Students t-test.
Results: The table 1 shows the values of hialuronic acid and histomorphometrical parameters. There were significant increase on GI and GIII, GII and GIV the same p = 0,0002. No significant on GI and GII the p = 0,48. The highest values of epidermal thickness was detected in GI after treatment (p = 0.01, compared to baseline and isoflavone). The number of dermal papillae, fibroblasts and blood vessels was superior in estrogen group compared to baseline and isoflavone (p = 0.02). Conclusion: Our data suggest that both treatments positively affect the on the concentration of hyaluronic acid in postmenopausal skin.
OR10-09
WOMEN's VOICE: LONGTERM EFFECTS AFTER HYSTERECTOMY
K. Puangpaka1 and C. Siriporn2
1,2KhonKaen University, KhonKaen, Thailand
Background: Hysterectomy is one of most common surgical procedure that women undergo in Thailand. Very few studies follow up long term effects and care needs of these women. These effects have influence on women's health and their lives.
Objective: The objective of this study is to explore how women with hysterectomy perceive and describe their experiences of long term effects after hysterectomy.
Design and Method: The qualitative study was conducted with Thirty five women who had had hysterectomy more than one year, aged 35–70 years old, and were living in urban and rural communities of Ayuthaya province in Thailand. Participants are both total hysterectomy and total hysterectomy with mono/bisalphingooophorectomy. Data were collected by using in-depth interviews and non-participatory observation until it saturated. Once, the interviews were transcribed. Content analysis and thematic analysis were conducted.
Results: Findings revealed that women expressed both positive and negative feeling toward hysterectomy. Two themes emerged from data analysis included: 1) the positive dimensions emphasized feeling safe lives from severe diseases and convenient conducting one's life, and 2) the negative dimensions included feeling a weakling, decrease of sexual desire, loss of power, and uncontrolled urination.
Conclusions & Suggestions: Women with hysterectomy need long term care to promote good health and quality of life. Nurses, health care providers and families should concern this issue. Cultural sensitive and gender sensitive care are needed to establish appropriate health care services.
Complementary and alternative medicine
OR11-01
ACUPUNCTURE REDUCES HOT FLASHES IN POSTMENOPAUSAL WOMEN. ACUFLASH, A RANDOMISED CONTROLLED TRIAL
S. Grimsgaard1,2, E. K. Borud2 and T. Alræk2
1Clinical Research Centre, University Hospital of North Norway, Tromsø, Norway; 2The National Research Centre in Complementary and Alternative medicine, University of Tromsø, Tromsø, Norway
Objective: To evaluate two low risk strategies for the treatment of vasomotor symptoms. The study compares the effect of traditional Chinese Medicine (TCM) acupuncture and self-care versus self-care alone, on the frequency of hot flashes in postmenopausal women.
Design & Method: The study was a multicentre, pragmatic, randomised controlled trial with two parallel arms. Primary endpoint was change in hot flash frequency from baseline to 12 weeks. Postmenopausal women were recruited by media coverage and newspaper advertisements. Eligible women did not use hormone therapy (HT) or antidepressants, and documented ≥ 7 hot flashes/24 hours during seven consecutive days at baseline. They were randomised to individualized acupuncture treatment (10 sessions) and advice on self-care (acupuncture group), or advice on self-care alone (control group). Hot flash frequency and severity (0-10 unit visual analogue scale) were recorded in weekly diaries at baseline and 12 weeks. The study was conducted in three centres in Norway (Tromsø, Bergen, and Oslo) in 2006–2007. Experienced practitioners provided the acupuncture treatments.
SPSS 14.0 was used for statistical analysis. Change was calculated as hot flash frequency at 12 weeks minus the frequency at baseline. Differences between groups were compared with two-sample t-tests and p < 0.05 was considered statistically significant.
Results: Altogether 535 women were assessed for eligibility, and 267 were randomised to acupuncture (n = 134) or control (n = 133) groups. Overall dropout was 7%, n = 3 in the acupuncture group and n = 16 in the control group. Mean age at inclusion was 53.8 years, and age at menopause was 48.9 years. Mean self reported BMI was 25.2. Previous use of HT and of acupuncture was reported by 50% and by 64% respectively.
Mean baseline hot flash frequency was 12.6/24 hours and intensity was 6.9 units on a 0-10 scale. During the study period, hot flash frequency decreased by 5.8/24 hours in the acupuncture group and 3.7/24 hours in the control group, a difference of 2.1 (95% CI 1.0–3.2, p < 0.001). Hot flash intensity decreased by 3.2 units in the acupuncture group and by 1.8 units in the control group, a difference of 1.4 (95% CI 0.7–2.0, p < 0.001).
Conclusion: Hot flash frequency decreased by 48% in the acupuncture group, and by 28% in the control group, the difference between groups being statistically significant. TCM acupuncture constitutes a low risk and clinically effective treatment strategy for postmenopausal women suffering from hot flashes.
OR11-02
ADVERSE LIVER REACTIONS TO BLACK COHOSH: ARE THEY ACCURATELY REPORTED?
Belal Naser and Eckehard Liske
Schaper & Brümmer GmbH & Co. KG, Bahnhofstraße 35, 38259 Salzgitter, Germany
Objective: Black cohosh (BC) is the most popular herbal treatment for menopausal symptoms. In May 2007, the EMEA expert group (HMPC) has published an assessment report on alleged hepatotoxicity connected to this herb stating that 18 out of the 44 world-wide available cases were considered as sufficiently documented (Fig.). Only in 5 of them a causal relationship could be established with a “probable” or a “possible” connection. The aim of our analysis was not to re-evaluate the causality with BC, but to look on the quality of the reports.
Results: In the table those “probable” (# 1, 2) and “possible” reports (# 3,4,5) are presented. Patients, suspected drugs and reactions are not precisely specified in the reports. Duplicate cases could not easily be identified because e.g. information like duration of intake, dosage, co-medication or medical history were often lacking or even contradictory.
The pharmaceutical quality of the suspected products was hardly assessable. Adulteration can not be excluded. It was not clear whether the suspected BC-products were registered medicinal products or dietary supplements.
Conclusion: In our opinion, even those from the EMEA as “sufficiently” classified reports were found to be inaccurately documented or otherwise inappropriately for analysis.
OR11-03
EFFICACY OF SOY ISOFLAVONES IN THE KUPPERMAN INDEX IN POSTMENOPAUSAL WOMEN: A RANDOMIZED, DOUBLE-BLIND, AND PLACEBO-CONTROLLED STUDY
Hernández Karla, von Helde Sueli, Tobar Cristina, Fragoso Jeniffer, Paredes Adriana and Palacios Santiago
Instituto Palacios, Madrid
Introduction: The use of soy isoflavones in hormone replacement therapy for the climacteric syndrome is an alternative therapy. The results of their efficacy in the management of vasomotor symptoms are controversial.
Objective: To assess 100mg of non genetically modified soy isoflavones (genistein 49 mg, daizen 43 mg, and glicitein 8mg) by means of the Kupperman index in the climacteric symptoms.
Material and Methods: A prospective, randomized, double blind study. 75 women were selected according to the inclusion criteria: healthy postmenopausal women between 45 and 65 years, with a reduced quality of life, and with a uterus. Two groups were formed: Group A with the study drug (38 women) and group B with placebo (37 women). A periodic follow up of the patients was carried out at the first week, at week 14 and week 24. In each of these follow ups, the assessment of the climacteric symptology with the Kupperman index was carried out. The Kupperman index includes the following 11 symptoms: vasomotor, parastesias, insomnia, nervousness, melancholy, vertigo, tiredness, arthralgias and myalgias, headache, palpitations, pins and needles. Each category was assessed on a scale 0–4 points (no symptoms = 0 and severe = 4), each symptom having a factor corresponding to its importance. This way the total score assessed the severity of the symptoms. The categories are the following: slight (0–22 points), moderate (23–33 points), and severe (>34). The statistical treatment of the information was carried out with the ANOVA test by repeated measurements and the interference method.
Results: 68 postmenopausal patients who complied with the inclusion and exclusion criteria were included, of which 35 were in the study drug group (group A) and 33 were in the placebo group (group B). According to the Kupperman index, and taking into consideration the duration of use, between the basal visit and after 24 weeks of treatment with soy, 89.4% of women progressed from a moderate category (22.7 points) to a slight category (16.3 points) (p>0.05).
Conclusions: The use of non genetically modified soy isoflavones at a dose of 100mg (genistein 49 mg, daizein 43 mg, glicitein 8mg) has a positive influence regarding the time in the Kupperman index.
OR11-04
EFFECT OF AQUEOUS GLYCYRRHZA GLOBRA EXTRACT ON MENOPAUSAL SYMPTOMS
F. Abdollahy1, M. Azadbakht2, F. Rezai Abhari2, B. Shabankhani2 and J. lay mun sun1
1University Putra Malaysia, kuallalampur, Selongar, Malaysia; 2Mazandaran University of Medical Sciences, Sari, Mazandaran Iran
Background: Most women considered menopause as natural period in their life, but many of them will experience some problems before and after that. Due to side effects of hormone therapy, various menopausal symptoms in Population with different regime and effects of like – estrogen of Aqueous Glycyrrhza globra, this study has been evaluated for decreasing of some menopausal symptoms for the first.
Material and Methods: After selecting samples and hemogenation for age, menopausal age and BMI, 29 and 24 women divided in case and control groups, respectively. 250 mg Glycyrrhza Globra capsule prescribed to women in case group and control group triple per day. The mean number of hot flash and degree of menopausal symptom (KI, Kupperman Index) calculated every two weeks and then divided to four degree, without, weak, medium and sever symptoms. Data analyzed with SPSS program and t. test and assyssed the effect of drug on hot flash and KI in different weeks. Aqueous Glycrrhaza glabra extract prepared by maceration and alkaline pH and HPLC method. The extract was concentrated and then was powdered. The powder used as capsule 250 mg and standardized by glycrrhizha content.
Results: Results showed that the mean numbers of hot flash, KI and FSH decreased from 6 ± 2.8, 32.2 ± 6.8, 72.29 ± 36 to 1.06 ± 2.8, 9.5 ± 5.2 and 65.12 ± 36, respectively. But decrease in control group at the begin and end of period., was not significant Also estradiol hormone in creased significat in case group (from 63.77 ± 41.2 to 102.29 ± 75.93).
Conclusion: Aqueous Glcyrrhza globra decrease hot flash and KI. Considering aqueous Glycyrrhza globra is a native plant in Iran, So It can be a cheep, simple and without side effect method for menopausal symptoms.
OR11-05
EFFECTS OF ISOFLAVONE GENISTEIN DAIDZEIN (IGD) FROM BITHOK ON ENDOTHELIAL CELLS APOPTOSIS INDEX, OSTEOBLAST AND OSTEOCLAST, ENDOTHELIAL CELLS β ESTROGEN RECEPTOR EXPRESSION, OSTEOPROTEGERIN AND INTERLEUKIN-1 IN HYPOESTROGENIC MICE
A. Hidajat, W. Ngartjono, I. W. Arsana, M. D. Pande, H. Wibisono, Sutrisno
Brawijaya University, Malang, Jawa Timur, Indonesia
Objective: To determine effects of several doses of Isoflavone Genistein Daidzein (IGD) from bithok plant (Pueraria lobata = PL) on endothelial cells apoptosis index level, aorta endotheliums β estrogen receptor (β-ER) expression, number of osteoblast and osteoclast, osteoclast apoptosis index, osteoprotegerin and interleukin-1 in hypoestrogenic ovariectomized mice.
Design & Method: 30 mice (Rattus novergicus) divided into 5 groups. Group I: Positive control (intact) group. 4 groups ovariectomized, waited 2 weeks to be hypoestrogenic, and from these: group II without PL-IGD diet, group III with 15 mg/kgBW/day PL-IGD diet, group IV 30 mg/kgBW/day and group V 60 mg/kgBW/day.
After 21 days, all mice terminated and the aortas taken out to determine apoptotic endothelial cells quantity, β–ER expression per 100 endothelial cells (by immunohistochemistry technique), osteoblast osteoclast quantity, osteoclast apoptosic cells, osteoprotegerin and interleukin-1.
Result: Mean of apoptotic cells per 100 aorta's endothelial cells are for group I:1.33 ± 1.2, II: 10.20 ± 1.9, III: 9 ± 2.4, IV: 6.33 ± 1.7, group V: 2.33 ± 1.5 with one-way anova 26.757 (p < 0.05). Mean of the endothelial cells which expressed β estrogen receptor are for group I: 6.0 ± 1.673, II: 2.4 ± 0.548, III: 2.67 ± 1.211, IV: 5.17 ± 1.835, and for group V: 9.17 ± 1.602 with one-way anova is 20.223 (p < 0.005).
The Pearson correlation between apoptosis and β–ERexpression is –0.694.
The highest number of osteoblast and the lowest of osteoclast were found in ovariectomized + IGD groups of 30mg/kg BW/day.
Osteoclast apoptotic index, group I: 2.33 + 1.63, II: 13.6 + 3.44, III: 9 + 2.53, IV: 9.33 + 2.80, V:4.17 + 1.47.
Osteoprotegerin for group I: 25, II: 9.6, III:12.17, IV: 15.5, V: 22.17
Interleukin-1 for group I: 2, II: 20, III: 18, IV: 13.5, V: 5.83
Conclusion: IGD inhibit aorta endothelial cells apoptosis and stimulate the β-ER estrogen.
IGD dose influenced apoptosis level and β–ERexpression.
IGD decrease bone cell apoptosis index at all doses significantly (p < 0.05).
IGD increase osteoprotegerin and decrease interleukin-1 in bone cells.
OR11-06
IMPROVEMENT OF POSTMENOPAUSAL DEPRESSION AND ANXIETY SYMPTOMS AFTER TREATMENT WITH ISOFLAVONES DERIVED FROM RED CLOVER EXTRACTS
Peter Chedraui1, Anca Gocan2, Franz Reithmayr2, Markus Lipovac3, Claudia Schimitzek3 and Martin Imhof3
1Institute of Biomedicine, Facultad de Ciencias Médicas, Universidad Católica de Santiago de Guayaquil, Ecuador; 2Study Center Med XIX, Vienna, Austria; 3Division of Obstetrics and Gynecology, Landesklinikum Weinviertel Korneuburg, University of Vienna, Austria
Objective: To evaluate the effect of isoflavones derived from red clover extracts (MF11RCE) over anxiety and depression symptoms among postmenopausal women. Methods: One hundred and nine postmenopausal women aged 40 or more were randomly assigned to receive two daily capsules of MF11RCE (80 mg isoflavones, Group A) or placebo of equal appearance (Group B) for a 90 day period. After a washout period of 7 days, medication was crossed over and taken for 90 days more. Anxiety and depression symptoms were measured at baseline, 90 and 187 days with the Hospital Anxiety and Depression Scale (HADS) and Zung's Self Rating Depression Scale (SDS).
Results: After receiving the MF11RCE compound the total HADS (anxiety and depression domain scores) and the total SDS scores decreased significantly. This effect was equivalent to a 76.9% reduction in the HADS total score (76% for anxiety and 78.3% for depression) and an 80.6% reduction in the total SDS score. After placebo, total HADS and SDS scores only decreased in average 20% in relation to basal line.
Conclusion: Red clover derived isoflavones demonstrated to be effective in reducing depression and anxiety symptoms among postmenopausal women.
OR11-07
TRENDS IN HRT AND NON-HRT USE IN POSTMENOPAUSAL WOMEN IN THE UK
A. Gentry-Maharaj1, A. Ryan1, L. Bruscati1, N. Nayak1, M. Burnell1, A. Sharma1, A. Lanceley1, L. Fraser1, I. Jacobs1, M. Hunter2 and U. Menon1 for UKCTOCS
1UCL EGA Institute for Women's Health, University College London, London, UK; 2Institute of Psychiatry, Kings College London, London, UK
Objective: Since the publications of the large HRT trials in 2002, a steady decline in HRT use has been observed. We have previously shown that 29% of postmenopausal women aged 50–74 recruited to the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) in 2001 were using HRT compared to only 10% of those recruited in 2005. The aim of this report is to investigate HRT use at follow up four years later and to assess non-HRT use for relief of menopausal symptoms.
Design & Method: 202,638 postmenopausal women randomised to UKCTOCS between 2001–5 were asked about HRT use at recruitment. At questionnaire follow up, they are asked if they are continuing to use HRT and more recently, also if they have used non-HRT treatments for relief of menopausal symptoms.
Results: Data is currently available on 90,718 women. At recruitment, median age was 59.5 (range 50–74) and 24.1% (21,894) were using HRT. At median follow up 4 (range 1.6–6.4) years later, median age was 63.6 (52–80.5) years and 7.8% (7,096) were using HRT. This included 27.5% (6,023) of those using HRT at recruitment and 1.6% (1,073) of those not using HRT at recruitment. In all age groups there was lower use of HRT but this trend was least in women over 65.
Table 1 HRT use in women by age at recruitment in 2001–5 and follow up 2005–8
In 57,817 women who were asked about non-HRT treatment for menopausal symptom, 19,361 (33.4%) reported use. In these women, highest use was reported for herbal therapies (40.4%), then vitamins (39.5%), lifestyle approaches (28.6%), phytoestrogens (19.6%), aromatherapy, reflexology, acupuncture (13.6%) and homeopathy (11.8%). 25.3% of women reported use of a combination of non HRT therapies.
Conclusion: While there is a fall in HRT use in postmenopausal women in the UK, this is least pronounced in women over 65. One in 3 women are using non-HRT treatments to relieve their menopausal symptoms with herbal therapies being most common.
OR11-08
USE OF HOME REMEDIES FOR MENOPAUSAL SYMPTOMS IN RURAL NORTH INDIA
A. J. Singh
School of Public Health, PGIMER, CHANDIGARH-160012, INDIA
Objective: To ascertain the types of home remedies used by women in rural north India to manage menopausal symptom.
Design & Methods: A female social worker interviewed 75 perimenopausal women aged above 40 years in six villages of field practice area of School of Public Health PGIMER, Chandigarh, India. They were asked about their treatment seeking behaviour pertaining to menopausal symptoms. Detail of home remedies used by them for these symptoms were recorded.
Results: Of the 75 respondents 39 (52%) had consulted various agencies for menopausal symptoms. All the medical practitioners advised them to wait for symptoms to subside on their own. No HRT was recommended. Some prescribed hematinics to the women. Thirty women (40%) reported use of various home remedies for obtaining relief from menopausal symptoms e.g. Drinking lemon water or kachi lassi (heavily diluted milk), application of henna on feet/soles, cucumber massage on sole/feet, mustard oil massage on feet, soaking feet in saline water, drinking a concoction of carrot seeds boiled in water, ajwain + raisins boiled in milk, methi dana + old jaggery + saunf + ajwain + salt = boiled and drink as concoction, (rawturmeric + jaggery) Some practitioners advocated yoga also to get relief from menopausal symptoms.
Conclusions: Use of HRT is very minimal in India. In rural areas it is almost nil. A variety of home remedies are used by women in Indian villages to manage menopausal symptoms.
OR11-09
USE OF STANDARDIZED HOP EXTRACT FOR MENOPAUSAL SYMPTOMS
R. Erkkola1, S. Vervarcke2, S. Vansteenland3, P. Römpötti4, D. De Keukeleire5 and A. Heyerick5
1University Central Hospital of Turku, Finland, 2Metagenics, Ostend, Belgium, 3Department of Applied Mathematics and Computer Science, Ghent University, Belgium, 4Max Medica Halikko, Finland, 5Laboratory of Pharmacognosy and Phytochemistry, Ghent University, Belgium
Objective: To examine the efficacy of a hop extract enriched in 8-prenylnaringenin (8-PN, the phytoestrogen in hops, Humulus lupulus L.) on relief of menopausal discomforts.
Design & Method: A cross-over randomized, double-blind, placebo-controlled study over 4 months with 36 menopausal women, who were administered a hops extract standardized on 8-PN (100 μg) during 2 months after or before a placebo treatment. The responses were determined by means of the Kupperman Index and patients questionnaires Visual Analogue Scale (VAS) and Menopause Rating Scale.
Results: Two administration regimes (placebo vs. hops) were compared after 2 and 4 months. No significant difference after 2 months between the groups was observed, although both groups did better than at the baseline. After 4 months, the group which was given placebo during month 3 and 4 showed a clear worsening of symptoms. Assessment of indicators in the VAS showed that ‘hot flashes’ and ‘sweating’ significantly diminished on hops treatment, while the effect of placebo was not significant.
Conclusion: Daily intake of a hop extract, standardized on 8-PN as a potent phytoestrogen, exerted favorable effects on vasomotor symptoms and other menopausal discomforts. An improvement of symptoms could be induced by administration of hop extract (amount equivalent to 100 μg 8-PN) which effect disappeared when the hop extract was no longer administered. Hop-derived prenylated flavonoids may provide an estrogen-free alternative in the treatment of hot flushes and other menopausal discomforts.
Metabolic syndrome and Lipids
OR12-01
ASSOCIATION OF ADIPOKINES AND OSTEOPROTEGERIN WITH COMPONENTS OF THE METABOLIC SYNDROME AND PSYCHOSOCIAL COMPLAINTS IN MIDDLE AGED WOMEN: PSYRECA 2005
S. Bergmann, K. Assig, F. Richter and G. Siegert
Universitätsklinikum Dresden IKL, Germany
The menopausal transition is associated with an increasing prevalence of various metabolic disorders summarized as Metabolic syndrome (MetS) and cardiovascular risk score. Corresponding clinical signs include abdominal obesity, osteoporosis, depressive mood and anxiety. Central obesity became the most important clinical criterion for the MetS. Measurement of leptin and adiponectin in middle aged women allows further insights into the metabolic role of the adipose tissue at menopausal transition. High levels of circulating osteoprotegerin (OPG) have been associated with cardiovascular morbidity and mortality in postmenopausal women whereas results about the effect of a postmenopausal HT on OPG were contradictory.
The aim of the present study was to establish factors influencing the serum concentrations of leptin, adiponectin (RIA LINCO) and OPG (ELISA immunodiagnostic Bensheim) in a 40–65 years old subgroup (n = 330) of the PSYRECA_2005 survey. 20,3% showed a MetS according to IDF_2005. Adiponectin in the lowest (<11,59 μg/ml) and/or leptin in the upper quintile (>26,16 ng/ml) may explain 49% of the existence of a MetS: RR 2,29 (95thCI 1,23–4,26), 52% of the insulin resistence (HOMA-IR): RR 3,15 (95thCI 1,69–5,89) and 37% of the cardiovascular risk (PROCAM): RR 2,13 (95thCI 1,06-4,27). Serum concentration of adiponectin tended to lower values among MetS women: 18,97 ± 8,83 vs. 16,59 ± 8,00 ug/ml; p < 0,05) whereas the concentration of leptin (24,82 ± 12,31 vs. 15,65 ± 9,47ng/ml; p < 0,001) and OPG (5,27 ± 1,73 vs. 4,35 ± 1,48 pmol/L, p < 0,01) were sign. higher in MetS women. Abdominal obesity (waist circumference > = 80 cm) and type 2 Diabetes mell. resulted in sign. lower concentration of adiponectin and sign. higher concentration of leptin. Hypertension – the most prominent component of the Mets in the present cohort- was associated with sign. higher concentration of OPG and leptin. Dyslipidemia was accompanied by higher leptin concentration and a tendency to higher OPG levels.
Serum concentration of leptin and OPG were independent of menopausal status or the use of HT, whereas adiponectin was sign. lower among postmenopausal women as compared with premenopausal (15,36 ± 7,52 vs. 19,42 ± 9,56 μg/ml; p < 0,005).
Psychosocial complaints (Greene's menopause inventory) were not very prominent in the cohort: 10% scored in mood M3. Leptin was sign. higher in M3 as compared with M1: 21,93 ± 13,83 vs. 15,75 ± 9,79 ng/ml; p < 0,05. Adiponectin and OPG concentration were not associated with depressive mood or anxiety. On the other hand, among women with cardiovascular risk >10% OPG was sign. higher and adiponectin tended to lower values whereas leptin concentration was not correlated with the PROCAM-score.
OR12-02
HIGH NORMAL THYROID STIMULATING HORMONE LEVELS ARE ASSOCIATED WITH METABOLIC SYNDROME IN EUTHYROID POSTMENOPAUSAL WOMEN
H. T. Park, G. J. Cho, J. H. Shin, T. Kim, J. Y. Hur and S. H. Kim
Korea University Medical Center, Seoul, Korea
Background: It is well established that overt hypothyroidism is associated with an elevated risk of cardiovascular diseases and the components of metabolic syndrome. However, the relationship between metabolic syndrome and thyroid function in euthyroid subjects is still unclear. Most cardiovascular events occur in euthyroid subjects. Thus, the question of whether an association of thyroid function with metabolic syndrome also exists in the euthyroid range is important.
Objective: To investigate the relationship between thyroid function and metabolic syndrome in euthyroid postmenopausal women.
Methods: We conducted a cross-sectional study of 2205 Korean postmenopausal women. Subjects who were not euthyroid were excluded, as were subjects taking thyroid medication. Euthyroidism was defined by thyroid stimulating hormone (TSH) (reference range, 0.3–4.0 mU/liter) and free T4 (FT4) (reference range, 10.19–24.0 pmol/liter). Exclusion criteria included diabetes, chronic liver disease, chronic kidney disease, malignancy or any disease that might affect thyroid metabolism. Also women who had taken lipid lowering drug and oral glucose lowering drug were excluded. Women with history of current or previous use of estrogen replacement, hysterectomy, and who did not know the accurate time period after menopause were also excluded from the study. As the result, 949 Euthyroid postmenopausal women were evaluated and grouped into quartiles of similar size. The metabolic syndrome was defined according to the National Cholesterol Education Program Adult Treatment Panel III.
Results: Multivariate logistic regression analysis determined that TSH levels (OR = 1.55, 95%C.I. = 1.26–1.89) were strong contribution to metabolic syndrome. TSH levels were associated with total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides and diastolic blood pressure. Using a forward stepwise linear regression model, low-density lipoprotein (β = 0.105; p = 0.004) and triglycerides (β = 0.089; p = 0.023) were identified as independently associated with TSH levels. Subjects with high normal TSH levels (2.48–4.0 mU/liter) had significantly higher prevalence of metabolic syndrome than those with low normal TSH levels (0.3–1.44 mU/liter), (34.18% Vs 21.47%, p = 0.007), as well as a 1.95-fold increase risk of metabolic syndrome (95% C.I. = 1.28–3.07).
Results: Within the reference range, increasing TSH levels were associated with increasing the prevalence of metabolic syndrome in postmenopausal women. Therefore, postmenopausal women with high normal TSH levels may belong to the high risk group of metabolic syndrome.
OR12-03
INFLUENCE OF AMENORRHOIC PERIOD, ANTHROPOMETRIC AND HORMONAL PARAMETERS ON METABOLIC SYNDROME
A. Simoncig Netjasov, S. Vujović, M. Ivović, M. Tančić-Gajić and M. Drezgić
Institute of Endocrinology, Diabetes and Metabolic Disorders, Clinical Center of Serbia, Belgrade
Objective: Hypoestrogenic status in the menopausal women shows a shift to a central android fat distribution and metabolic syndrome (MS). Related metabolic changes and hypertension increase risk for cardiovascular diseases. The aim of this study was to investigate the influence of amenorrhoic period, anthropometric and hormonal parameters on metabolic syndrome.
Design & Method: 50 obese women were examined with BMI = 31,92 ± 5,83 kg/m2, 54,40 ± 3,64 y's old, amenorrhoic period 5,90 ± 5,46 y's. Control group was consisted of 37 normal weight women with BMI = 23,50 ± 2,13 kg/m2, 53,92 ± 3,95 y' old, amenorrhoic period 5,96 ± 4,92 y's.
Anthropometric characteristics and blood pressure were measured. Blood was taken at 8 am for: fasting glucose, triglycerides, cholesterol, HDL, LDL, ApoA, ApoB, Lp(a), fibrinogen, FSH, LH, prolactin, estradiol, progesterone, testosterone and SHBG. Hormone analyses: RIA. Statistics: Pirson's test of linear correlation, ANOVA.
Results: In obese women significant negative correlations were found for: BMI and HDL (p < 0,05), waist and HDL (p < 0,05), FSH and systolic blood pressure (p < 0,01), FSH and fasting glucose (p < 0,05), LH and waist (p < 0,05), SHBG and fasting glucose (p < 0,05). Positive correlation was found for time since menopause and waist/hip ratio (p < 0,05). In controls positive correlations were found for: waist/hip ratio and systolic and diastolic blood pressure (p < 0,05), LH and HDL (p < 0,05), estradiol and diastolic blood pressure (p < 0,05). Negative correlations were detected for estradiol and waist (p < 0,05), time since menopause and HDL (p < 0,05).
Conclusion: Hypoestrogenia in the menopause induces gaining weight causing metabolic and hemodynamic imbalances, which contribute to risk for cardiovascular diseases.
OR12-04
METABOLIC SYNDROME IN MENOPAUSAL OBESE WOMEN
P. D. Khandelwal, S. Khandelwal and G. Sharma
Medical College, Rajasthan University of Health Sciences, Jaipur, India
Objective: To study the incidence of metabolic syndrome(as per ATPIII&IDF Criteria)in
Menopausal obese women, as many studies found to have high prevalence of this syndrome in both sexes, which has a very significant contribution in the development of Type II Diabetes & CAD risk.
Design: The study was conducted on 220 subjects (120 obese menopausal women & 100 non obese age matched controls), attending obesity and metabolic clinic in the department of medicine and menopause clinic.
Menopausal women having BMI > 25 were included in the study. Clinical examination, body weight, BMI, WHR, Blood glucose, lipid profile, FSH& BP were measured & recorded on the Performa designed.
Results: The incidence of metabolic syndrome was found to be 30% in obese menopausal women, whereas it was 8% in control group. The obesity was highest in the age group 46–55 yrs (60%), whereas it was insignificant (5%) among normal women. (Age control group). The syndrome was found to have positive correlation with duration (5–7yrs) of menopause. It was also observed that FSH(mean 74 ± 8.6) was found to be statistically significant high among obese menopausal women as compared to their controls (46 ± 6.6). The BMI(27–36),WHR(1.16–1.32)LDLc(136 ± 6.4), TG(210 ± 9.6), HDLc(44 ± 5.2) and SBP (156 ± 7.6) DBP (92 ± 4.2)were found to be in the range of metabolic syndrome. Though the mean blood glucose (108 ± 7.4) was in the range of metabolic syndrome but none of the obese menopausal women was diabetic.
Conclusion: Menopausal women have significant risk of developing metabolic syndrome there by increase chances of type II DM and CAD risks. Overall incidence of metabolic syndrome in the present study was lower as compared to western world. Hypertension and Dyslipidaemia was statistically significant in menopausal obese women, Therefore control of obesity, BP and management of dyslipidaemia along with menopausal care is needed, to give a better quality of life at second adulthood and beyond. The positive life style modification in form of diet and exercise along with control of BP and dyslipidaemia by single or polypill is strongly recommended to this group of population.
OR16‐05
METABOLIC SYNDROME AND CARDIOVASCULAR RISK IN POSTMENOPAUSAL WOMEN
P. Hormaza1,2,3, M. Massaro1, G. Rendón1, J. F. Botero1, J. Montoya1, A. Guevara1, L. C. Prada1 and S. Uribe1
1Universidad Pontificia Bolivariana, Medellín, Colombia; 2Entidad Promotora de Salud, SUSALUD, Medellín, Colombia; 3Caja de Compensación Familiar de Antioquia, COMFAMA, Medellín, Colombia
Objective: To compare metabolic syndrome (METS) prevalence in postmenopausal women, applying the International Diabetes Federation (IDF) and the National Cholesterol Education Program Expert Panel (NCEP/ATPIII) criteria; as well as to assess postmenopausal cardiovascular disease (CVD) risks and related risk factors.
Design & Method: Cross-sectional study of 224 women ≥ 45 years of age, following IDF and NCEP/ATPIII guidelines; age, time since last menstrual period (LMP), previous hysterectomy, body mass index, previous CVD, diabetes mellitus or high blood pressure (HBP), smoking, and serum cholesterol determinations were also recorded. CV risk was estimated using Framingham projections of 10-year absolute CVD risk and the American Heart Association (AHA) CVD risk assessment.
Results: In these women, mean age was 59 ± 8.36 years. Half of them had their LMP ≥ 10 years before. 62.9% were overweight/obese. METS prevalence was 57.1% IDF (95% CI 50.4–63.7) vs. 37.5% NCEP/ATPIII (95% CI 31.1–44.2). HBP was the most prevalent criteria (60.7%) for both indexes, excluding abdominal obesity in IDF (85.7%). 46% of women had a Framingham score ≥ 10%. 76.8% presented AHA at risk or high CVD risk. Otherwise, 69 women at risk, according to the AHA classification, had a Framingham score < 10%; none of these women had METS by NCEP/ATPIII criteria. The multivariate analysis showed the following factors as the strongest, associated to METS/IDF: obesity, (OR 5.05; 95% CI 2.18–11.69) and age ≥ 65 years (OR 2.75; 95% CI 1.34–5.64); for CVD risk: HBP (OR 11.58; 95% CI 4.81–27.86), low HDL-cholesterol (OR 16.63; 95% CI 5.96–46.37) and age ≥ 55 years (OR 4.5; 95% CI 1.90–10.67).
Conclusion: Taking into account the high METS prevalence in these postmenopausal women and the associated CVD risk factors, the best diagnostic tools seem to be IDF for METS and AHA criteria for the CVD risk assessment. Both of them applied together, allow the identification of a greater number of women at risk, to establish adequate primary prevention measures as the main goal.
OR12-06
THE METABOLIC AND INFLAMMATORY PROFILE IN A POPULATION OF ELDERLY WOMEN BEARING OR NOT METABOLIC SYNDROME
M. Karnikowski, S. Silveira, O. Nóbrega and A. Tavares
Catholic University of Brasília, Brasília, DF, Brazil
Objective: In detriment of the demographic and the nutritional transition, nowadays there is a world-wide concern about the knowledge on the aging process, mainly considering the not-transmissible chronic illnesses, specially obesity, arterial hypertension, diabetes mellitus, well-known as risk factor for cardiovascular diseases. All together these disturbances have been described as Metabolic Syndrome (MS) that currently occurs in a relevant number of individuals, specially the aged ones. With the aging process, a phenomenon known as inflammaging ocurrs, which represents an increase of the basal inflammatory activity in reply to the effect of the antigenic chronic stress that can be enhanced by chronic diseases. This study aimed to investigate the relation between metabolic and inflammatory parameters in a population of elderly women with and without MS.
Design & Methods: It is an analytical study in which anthropometrics (BMI, WC, AC and WHR); biochemical (Total lipids, T-COL, VLDL-c, LDL-c, HDL-c and TGL), inflammatory (IL-6, TNFα, INFγ and CRP) metabolic parameters (glycosylated hemoglobin, glycemic index and basal serum insulin level) and arterial tension levels were analyzed in a population of 214 elderly women physically inactive, without nutritional follow-up and with age between 60 to 85 years. The IDF protocol (2005) was used to diagnose MS women and they were classified into individuals with metabolic syndrome, without metabolic syndrome and pre-metabolic syndrome.
Results: Despite of the high prevalence of the MS, 54.2% (n = 116), all the women studied exhibit a close inflammatory profile, independent of being MS bearer. Among the criteria that define MS, the fasting glycemic level was that with better correlation to the inflammatory parameters, particularly with the TNFα, in individuals with metabolic and pre-metabolic syndrome. It was identified that studied population presented a nutritional profile compatible with weight excess, with a prevalence of 43.5% (n = 93). In addition, despite of the reduction of the average values of the BMI associated with aging, the WC, AC and WHR remained with average values above levels considered normal in all the age groups.
Conclusion: This study allows conclude that the inclusion of the fasting glycemic level as a key parameter to define MS is widely justified for the association that this parameter has with the inflammatory process in elderly women bearing MS.
OR12-07
VASOMOTOR SYMPTOMOLOGY AND ADIPOSITY IN POSTMENOPAUSAL WOMEN
M. H. Moreira, A. F. Pereira, J. M. Freitas, J. C. Leitão, J. J. Raposo and E. M. Coelho
University of Trás-Os-Montes And Alto Douro, Vila Real, Portugal
Objective: This study focused on the effect of body mass index (BMI) and waist circumference (WC) on vasomotor symptoms in postmenopausal women.
Design & Method: The sample included 146 postmenopausal women aged 40–75 years, in which 54.1% used HRT and 43.8% were at the time in menopause for 6 to 13 years. Participants completed the Greene Climacteric Scale, which was validated in Portuguese postmenopausal women and it was used anthropometric variables to estimate overall (BMI ≥ 25.5 kg/m2) and central obesity (WC ≥ 80 cm). Basal metabolic rest (BMR) was estimated by bioimpedance tetrapolar and two-way Anova was used to examine group differences.
Results: Seventy-four percent of women exhibited values of BMI ≥ 25.5 kg/m2(18.80–41.70 kg/m2) and the majority (72.6%) revealed WC ≥ 80 cm. The correlation between these two anthropometrics variables was 0.91 (p < 0.01). The BMR prediction was between 1027 and 1517 kcal/day (1253.48 ± 103.15 kcal/day), which justifies the control in the analysis of variance multivariate. Obesity showed in women mainly hot flashes (0.74), night sweatiness (0.69) and final score of vasomotor symptoms (1.44), compared to the medium values identified (0.73, 0.66 e 1.38, respectively), but that effect does not have statistic signification (F = 0.01, F = 0.04 and F = 0.01 respectively, p>0.05).
In the presence of levels of WP ≥ 80 cm, the vasomotor symptoms had also a major (p>0.05) asseveration (0.75, 0.72 e 1.47). We yet concluded that a woman with levels of BMI<25.5 kg/m2and WP<80 cm have tendency to expose a low severity of hot flashes, night sweatiness and final score of vasomotor symptoms. However that effect does not have statistic signification (F = 0.28, F = 0.16 and F = 0.23 respectively, p>0.05).
Conclusion: Our research suggests that total and central obesity in postmenopausal women is not associated with higher prevalence and severity of vasomotor symptoms.
Aging women and male
OR13-01
ADHERANCE WITH HORMONE REPLACEMENT THERAPY IN MENOPAUSE
I. Fistonic1, J. Zekan2, N. Fistonic3 and A. Maletic3
1Menopause Clinic, Zagreb, Croatia; 2University of Zagreb, Ob/Gyn Clinic, Zagreb, Croatia; 3University of Zagreb, Medical School, Zagreb, Croatia
Objective: There are many reasons patients do not adhere to drug treatment. Although the disease itself causes concern, possible side effects may also worry the patient resulting in reluctance to follow the plan. The adherence of patients to HRT was shown to be dependant on a specialisation/position of physician initially recommending it, the adherence rate being highest in private gynaecologists' and university clinics, lowest in general practice and community health centers. This study was conducted to assess the effect of time spent on medical consultation to duration of adherence as well as reasons to adhere or to drop-out from HRT.
Design & Method: The study was conducted using self-filled questionnaire on a sample of patients administered and collected at the Ob/Gyn and GP offices. The patients were interviewed regarding a number of personal and gynaecological history variables, including use of HRT, origination of HRT recommendation, attitudes in favour and against HRT and total duration of HRT. Total of 40 participating offices submitted 1263 patient questionnaires for analysis. The doctor attitudes and time spent on consultation was assessed using telephone interview on the sample of 90 gynaecologists, employed by clinical hospitals, health community centres and private practices. The doctors were interviewed regarding the average time spend with patient, dilemmas in HRT prescribing and counselling in sexuality.
Results: The patients who get recommended HRT by GPs voice most concerns regarding the safety of HRT (especially fear of cancer) and also to “HRT not being natural”, while patients who treated by private GPs fear “getting fat”, “bleeding” and also stress that “their friends do not use HRT” and have the lowest adherence rate of all patient groups. Patients treated by university hospital specialists see most reasons for using HRT (“reducing risk for osteoporosis”, “reducing cardiovascular risk”, “reducing skin dryness”, “reducing vasomotor symptoms”), while patients of private Ob/Gyns have the least concerns and moderate number of supporting arguments. At the same time, gynaecologists based at university hospitals have the highest adherence rates and therapy duration, while private gynaecologists have comparative adherence rate but shorter therapy duration. GPs have lowest adherence rates and lowest average therapy duration. The average per patient time is similar in National insurance community centre based doctors and hospital specialists, but almost double in private practices.
Conclusion: This study shows that extended medical consultation promotes better compliance through lowering patient fears, while trusted authorities seem to be more convincing to patients on the benefits of HRT and therefore more effective, even if not taking more time to talk to patients.
OR13-02
FUNCTIONAL FITNESS, OBESITY AND SARCOPENIA IN POSTMENOPAUSAL WOMEN
M. H. Moreira1, R. V. Castro1, J. M. Freitas1, R. E. Gabriel1, M. A. Monteiro1 and M. L. Machado2
1CIDESD, University of Trás-Os-Montes And Alto Douro, Vila Real, Portugal; 2Faculty of Human Motricity, Lisbon, Portugal
Objective: To investigate the effect of obesity and sarcopenia in functional fitness in postmenopausal women.
Design & Method: Seventy six healthy postmenopausal women (ages, 60 to 77 years; BMI, 20 to 41 kg/m2) participated in the study, among which 36% had HRT. Skeletal muscle mass (SMM), weight and basal metabolic rate (BMR) were evaluated by tetrapolar bioimpedance being the first expressed as skeletal muscle mass index (SMI = skeletal muscle mass/body mass × 100). The subjects were considered to have a normal SMI if their SMI was higher than -one standard deviation above the sex-specific mean for young adults (aged 18–39). The cut-off point to obesity using BMI was 25.5 kg/m2. Based on the combination of sarcopenia and obesity cut point, subjects were further classified into three groups: nonobese/nonsarcopenic (G1), obese nonsarcopenic (G2) and sarcopenic obese (G3). The test to assess physical parameters and functional ability included: 30-Second chair stand, 2-Minute step test, Arm curl, Chair sit-&-reach, Back stratch and 8-Foot Up-&-Go. Data were analyzed with ANOVA followed by Bonferroni correction.
Results: Nine participants (11.84%) were classified as sarcopenic obese, with SMI between 25.66% and 38.67%. The BMR ranged between 1027 and 1517 kcal/day, and its correlation with the factor was −0.42 (p ≤ 0.01). There were no significant trends for a reduction of lower and upper body strength in the sarcopenic obese women compared with the other groups (F = 2.30 and F = 0.09, p>0.05, respectively). The increase of adiposity and a loss of muscle mass were associated with a worse upper and lower body flexibility, aerobic endurance and speed/agility/dynamic balance with significant differences between G3 and G1 (−15.13 cm, −11,93 cm and −20,27 executions, + 0,08 seconds, respectively). Comparing G1 and G2 they were more likely to have a lower result in back stratch (−11.19 cm vs −2.71 cm, p ≤ 0.05).
Conclusion: Our data suggests that postmenopausal women with sarcopenic obesity are more likely to report subsequent functional fitness disability. In the presence of a normal muscular condition, the excess of adiposity tends to affect shoulder range motion.
OR13-03
IN VITRO FERTILISATION WITH DONOR EGGS IN POST-MENOPAUSAL WOMEN: ARE THERE DIFFERENCES IN PREGNANCY OUTCOMES IN WOMEN WITH PREMATURE OVARIAN FAILURE COMPARED WITH WOMEN WITH PHYSIOLOGICAL AGE-RELATED MENOPAUSE
B. Vollenhoven1,2,3, T. Osianlis1, G. Weston1,2,3 and J. Catt1
1Monash IVF, Melbourne, Victoria; Australia; 2Southern Health, Melbourne, Victoria, Australia; 3Monash University, Melbourne, Victoria, Australia
Objective: Donor eggs are used for in vitro fertilisation (IVF) in women with either premature ovarian failure (POF) (<40 years old) or physiological age-related menopause ( ≥ 40 years old) who desire children. This study compared pregnancy rates and pregnancy complication rates in women with POF (group A) with post-menopausal women ≥ 40 years old (group B) after IVF with donor eggs.
Design and Method: We examined patient histories between 2000–2007. Menopause (either premature or normal age-related) was defined as amenorrhoea ≥ 12 months plus 2 FSH measurements >20IU/L. There were 26 women in group A (average age 32.8 years) and 16 women in group B (average age 45 years) who had undergone IVF with donor eggs.
Results: In group A there were 2 women with POF as a result of Turners Syndrome, 2 as a result of chemotherapy and 1 as a result of bilateral oophorectomy. There were 143 initiated cycles (fresh and frozen) in both these groups of patients and there were 110 transfers. The clinical pregnancy rate per embryo transfer was 28% in Group A and 42% in Group B, with no significant differences with varying age of the patient. There were a total of 36 pregnancies in the two groups: 4 ended in miscarriage, 25 delivered, and 7 pregnancies were ongoing (>12 weeks gestation) at the time of writing. In group A there was a 62.5% chance of taking at least one baby home and in group B the chance was 64.3%. Of the delivered pregnancies, 16 were in Group A and 9 in Group B. Complications including IUGR, pre-eclampsia, gestational diabetes, and placenta praevia occurred in 31% of Group A completed pregnancies, and 78% of Group B completed pregnancies (p < 0.01).
Conclusions: Based on this series of patients who were defined into 2 groups by stringent criteria, women with POF have considerably less pregnancy complications than women with age-appropriate menopause. There were no significant differences in pregnancy rates between the two groups. If donor eggs are used for this group of patients irrespective of age, there is a 2 in 3 chance of taking home a baby.
OR13-04
MENOPAUSE - A NATURAL PHENOMENON OR NOT? WHY ARE WE HERE?
L. M. A. Shaw
London Bridge Fertility Gynaecology and Genetics Centre, London SE1 9RY, UK
Objective: The evidence base for why human females have a menopause is explored.
Design and Method: The menopause phenomenon is unique to Homo sapiens amongst the primates. The question of why this should be the case is explored and data is presented from geology, physical chemistry, anthropology and biology to support hypotheses.
Results: Biological data about the life expectancy of primates are presented. Only Homo sapiens has a consistent post-reproductive life phase. Fossil and observational evidence demonstrated a longer expected lifespan and a protracted juvenile phase in humans when compared with other great apes. Palaeo-climate data are shown to be closely related to key moments in human prehistory. Observations of the evolutionary pressures at that time, demonstrates sudden diversification in the hominin line. Skull size changes and the development of stone tool technology seem to coincide with this moment in time. Data from a group of hunter-gatherers in northern Kenya looking at foraging yields in two generations in relation to infant weight is considered and placed in the context of the previous multidisciplinary findings.
Conclusions: It is clear that, when mothers are distracted by the arrival of a new infant, the weaned older child is at risk as the mother has less time to forage just when there are more mouths to feed. The well described benefit of the woman's own mother contributing to the foraging is explored. It is proposed that the adaptation is not in fact the menopause but a decline in reproductive capacity from mid 30s thereby enabling there to be an adequate number of older women in the community with no current dependent children. The relationship of this to 21st century life is explored.
OR13-05
MENOPAUSE: THE BANGLADESH EXPERIENCE
S. Rahman
Combined Military Hospital, Dhaka, Bangladesh
Objective: In Bangladesh, Menopause is a topic hardly talked about. With increase in life expectancy, we are concerned about the consequences of longevity offset by higher rates of illiteracy, poverty and added geriatric problems, putting pressure on the country's socio-economic development. This study was aimed to get a profile of the growing elderly population, the type of problems they face and their attitude towards this change of life.
Design and Method: Population study included women aged 40 years and above from urban and rural areas. The main medical college and a private clinic in Dhaka city served as urban site and a village union of a district as rural study, selected by purposive sampling. Data were collected by a structured questionnaire containing information on age, socio-demographic profile, life-style, symptomatology, choice of therapy and overall attitude.
Results: Among the total of 140 women interviewed, the average age was 54 years. 23.6% had no school education, 19.3%- primary and 12.1% - secondary education; 13.6% had school certificate and 19.3% higher secondary education; 22.1% were graduates and above. 1.4% had no child, 68.6% had more than 3 children. Majority of the women (92%) practiced breast feeding for few months to two years. Regarding personal habits, 27.9% were betel leaf chewers; majority were physically active and 30% of the urban ladies went for jogging and other exercises. Food habit is simple, staple food was rice, vegetable and fish containing plenty of roughage. Different degrees of vasomotor symptoms were noted; hot flushes – 50%, sweating – 45%, palpitation – 22.5%., urogenital problems – 50%, vaginal dryness – 44%, memory and concentration problems - 44% and mood changes – 56.7%.
Common complaints reported among both groups included aches and pains and burning sensation all over the body. Only 32.9% took HT (Hormone Therapy) as tablets among the urban group and 5.7% local medications (cream) in both groups. Most importantly both groups were eager to learn about menopause and solutions to its problems.
Conclusions: Short term hormone therapy for acute symptoms was acceptable. But there was inconvenience of ready availability, cost of therapy and fear of cancer. Educated ladies were more keen to learn about the preventive aspects and natural therapy, although among the common majority it is still a normal change of life, to be accepted naturally. Traditionally the older women are still given due respect and care in the family, which carries a positive impact on the overall situation.
OR13-06
PAST REPRODUCTIVE EVENTS AS RISK MARKERS FOR THE DEVELOPMENT OF DIABETES MELLITUS TYPE-II AMONG ELDERLY WOMEN
D. Gomes, A. Tavares and C. Cárdenas
Catholic University of Brasilia, Brasilia, Federal District, Brazil
Objective: The development of chronic degenerative diseases in the aging process is a common event, including Diabetes Mellitus type-2 (DM-II). DM-II is disease caused by a polygenic base interacting with ambient factors. The major risk factors for its development are age, familial history of DM-II and central obesity. In a relevant number of individuals, the insulin resistance (IR) is the major factor responsible for the development of DM-II. Although the exact mechanisms that cause IR are unknown, this problem plays a central role in the development of many diseases, including DM-II, Polycystic Ovarian Syndrome (PCOS), Metabolic Syndrome and Gestational Diabetes (GD). This study aimed to identify if past reproductive events associated with IR may plau a role as risk markers of DM-II among elderly women.
Design & Method: 200 women aged ≥ 60 years were selected and were divided into two groups: diabetic (75), and elderly non-diabetics ones (125). They were then clinically evaluated, when past obstetric history on parity, miscarriage, frequent miscarriage (3 or more events) and the occurrence of fetal macrosomia were obtained. The Statistical Package for the Social Science for Windows was used for the analysis.
Results: It was observed that past history of fetal macrosomia and spontaneous miscarriage were predictive for the development of DM-II among elderly women (p = 0,001). On the other hand, it was not possible to show that frequent miscarriage (p = 0, 30), nulliparity (p = 0, 13) and parity (p = 0, 25) work as risk factors for it.
Conclusion: This study shows that fetal macrosomia and spontaneous miscarriage work as risk markers for development of DM-II among elderly women. Considering IR an etiopathogenic factor in common for some reproductive diseases, such as, PCOS and GD, and for DM-II, our results suggest that the identification of certain reproductive events in the clinical history of elderly women may help the diagnosis of DM-II.
OR13-07
SEQUENCIAL TREATMENT APPROACH FOR AGEING FEMALES: SINGAPORE EXPERIENCE
V. Dramusic, A. Kale and P. C. Wong
Department of Obstetrics & Gynaecology, National University Hospital, Singapore
Present life expectancy for Singapore females is 82 years, one of the fastest “greying” populations; in a projection for 2050 Singapore will be on 5th place of top 10 “grey” countries. Mean age of natural menopause is 49 years across three ethnic groups (Chinese, Malay, Indian) and predominant symptoms are muscle and joint aches (52,6%), lethargy/loss of energy (50,9%), headaches (41%), urogenital symptoms, but hot flushes far less (16%). Chinese women are less affected/shorter length of symptoms.
From our Menopausal Clinic (established in 1985, clinics 3 × weekly = 50–70 patients) we surveyed 300 patients under treatment and long follow-up (up to 22 years) and 100 who opted for observation/no treatment for symptoms, reproductive history, BMI (for Asians BMI 18,5 to 22,9 being normal range), diet, life habits, impact of various treatment regimes, etc.
Having in mind that our female patients already spend decades being postmenopausal, from 2002 our general treatment approach is to offer HRT/ERT to peri/early menopausal patients for up to 5 years, followed by Tibolone (or start it immediately in older patients) what is usually followed by easier acceptance of life style changes: diet, exercises, partners' involvement (rather new for older patriarchal Asian men). After age of 60–65 yrs stress is more on bone issue with variety of biphosphonates, SERMs and Stroncium Ranelate and “drug holidays” when plausible at any stage of management and very individualized patient dosage. Though big group of patients who had long lasting HRT/ERT (up to 22 yrs) have best preserved bones and feeling of well being, we consider sequential approach to treatment best and safer option for having good quality of life in decades after menopause. However those who opted observation/no treatment, or less than 3 yrs of treatment had fast bone deterioration. Research is started on threshold levels of estrogens needed for preservation of bones in Asian women.
Bone
OR14-01
EFFECT OF PEPTIDE REGULATORS ON STRUCTURAL AND FUNCTIONAL STATUS OF OSSEOUS TISSUE IN AGEING
V. Povoroznyuk1, V. Khavinson2, A. Makogonchuk1, G. Ryzhak2, Y. Kreslov1 and I. Gopkalova3
1Institute Of Gerontology AMS Ukraine, Ukrainian Scientific-Medical Centre For The Problems Of Osteoporosis; 2St, Petersburg Institute of Bioreguiation and Gerontology, Russia; 3V. Ya. Daniievsky Institute of Endorcine Pathology of Ukraine AMS, Ukraine
Post-menopausal osteoporosis is one of the key issues of public healthcare in the developed countries. Medico-social significance of postmenopausal osteoporosis is stipulated by its complications, first of all collum femoris and spinal fractures, which infringe the quality of life and drastically increase the death rate. Hence, the search for new effective means of treatment of system osteopososis is a burning issue of gerontology.
Our study was aimed at evaluating the effect of peptide bioregulators on the structural and functional status of osseous tissue in a post-ovariectomy osteoporosis model in rats. 100 mature female Wistar rats aged 4–6 months with body weight of 200–230 g were randomly subdivided into 8 groups, each consisting of 10 rats, and received the studied substances intramuscularly in different doses, the control being made up of 2 groups of 10 rats—ovariectomized animals not treated with substances, and non-operated animals injected with physiological NaCl solution. The following peptide bioregulators were used in the study: substance extracted from cartilages of young calves, in the dose of 1 mg and 0,03 mg per rat, and peptide medication T-31 (H-Ala-Glu-Asp-OH) in the dose of 10 μg and 0,3 μg per rat. To model the post-menopausal osteoporosis, bilateral ovariectomy was performed. Mineral density of the osseous tissue (MDOT) was evaluated using a two-photon X-ray densitometer “PRODIGY”. Study results pointed out the reliable efficacy of cartilages extract and T-31 peptide in maximum dosages in case of their administration from the 30Ih day since ovariectomy operation. The strongest effect was observed in case of cartilages extract administration in the maximum dosage (1 mg per rat): after a month of observation MDOT was reliably increased, remaining on the same level after 2 months since the beginning of the experiment. The administration of T-31 in the maximum dose beginning immediately after ovariectomy caused a reliable increase in MDOT after 30 days. However, in a month after the completion of the medication course (2 months after the surgery) MDOT was reliably reduced as compared to the initial level.
Thus, peptide bioregulators show good prospects as a means of prevention and treatment of post-menopausal osteoporosis.
OR14-02
EFFICACY AND SAFETY OF BAZEDOXIFENE FOR THE PREVENTION OF POSTMENOPAUSAL OSTEOPOROSIS
J. C. Menegoci1, P. D. Miller2, A. A. Chines3, G. Constantine3 and P. D. Delmas4
1Pontifícia Universidade Católica, São Paulo, Brazil; 2University of Colorado Medical Center, Denver, Colorado, USA; 3Wyeth Research, Collegeville, Pennsylvania, USA; 4University of Lyon and INSERM Research Unit 831, Lyon, France
Objective: Bazedoxifene (BZA) is a novel selective estrogen receptor modulator selected for its agonist activity in bone and antagonist activity in endometrial and breast tissues. This 2-year randomized, double-blind, placebo-controlled phase III trial evaluated the efficacy and safety of BZA for the prevention of postmenopausal osteoporosis.
Design & Method: Healthy postmenopausal women (N = 1,583) with lumbar spine or femoral neck bone mineral density (BMD) T-scores no less than −2.5 (mean, −1.2) were randomized to take BZA 10, 20, or 40 mg; placebo; or raloxifene 60 mg daily, along with supplemental elemental calcium (Caltrate 600 mg). The primary efficacy endpoint was percent change in lumbar spine BMD at 2 years; changes in BMD of the hip and femoral sites and serum bone marker concentrations were also assessed. Safety was evaluated by adverse event (AE) reporting and periodic transvaginal ultrasound and endometrial biopsy.
Results: Whereas all BZA doses and raloxifene 60 mg preserved lumbar spine BMD, a significant reduction in lumbar spine BMD was observed with placebo (P<0.001). The percent change in lumbar spine BMD from baseline to Month 24 relative to placebo was 1.08%, 1.41%, 1.49%, and 1.49% for BZA 10 mg, 20 mg, 40 mg and raloxifene 60 mg, respectively (P<0.001 for all comparisons). Comparable BMD responses at other skeletal sites were noted. Significantly greater reductions in osteocalcin and C-telopeptide levels occurred in all BZA groups compared with placebo as early as Month 3 and were sustained through study end (P<0.001). At Month 24, median serum osteocalcin levels decreased from baseline by 21%, 22%, 22%, and 27% with BZA 10, 20, and 40 mg, and raloxifene 60 mg, respectively, and 6% with placebo (P<0.001 vs baseline for each). Median serum C-telopeptide levels decreased by 25%, 24%, 22%, and 32% with BZA 10, 20, and 40 mg and raloxifene 60 mg, respectively, and by 13% with placebo (P<0.001 vs baseline for each). The overall rates of AEs, serious AEs, and AE-related discontinuations were similar among treatment groups. The incidence of venous thrombotic events was low (<1%) across treatment groups. There were no reports of endometrial hyperplasia or malignancy in the BZA groups. There were no between-group differences in the incidence of breast pain and the number of breast carcinoma cases was low and evenly distributed among treatment groups.
Conclusion: BZA effectively prevented bone loss and demonstrated an acceptable safety and tolerability profile in postmenopausal women with normal or low BMD.
OR14-03
EFFICACY OF BAZEDOXIFENE IN REDUCING NEW VERTEBRAL FRACTURE RISK AND IMPROVING BONE DENSITY IN OSTEOPOROTIC POSTMENOPAUSAL WOMEN: RESULTS FROM A RANDOMIZED, PLACEBO- AND ACTIVE-CONTROLLED 3-YEAR CORE STUDY
T. J. de Villiers1, C. E. Fernandes2, S. Palacios3, A. A. Chines4 and G. Constantine4
1Panorama MediClinic and University of Stellenbosch, Cape Town, South Africa; 2Women's Health and Wellness Institute (ISBEM), São Paulo, Brazil; 3Palacios Institute of Women's Health, Madrid, Spain; 4Wyeth Research, Collegeville, PA, USA
Objective: Bazedoxifene (BZA) is a novel selective estrogen receptor modulator currently under investigation for the prevention and treatment of postmenopausal osteoporosis. We report the 3-year efficacy and safety data from a randomized phase III study that evaluated BZA for the treatment of postmenopausal osteoporosis compared with placebo (primary comparator) or raloxifene (RLX).
Design & Method: The study enrolled healthy postmenopausal women (55–85 years of age) with bone mineral density (BMD) T-scores at the femoral neck or lumbar spine of ≤ –2.5 for women without vertebral fractures, or ≥ –4.0 for women with vertebral fractures. A total of 7,609 subjects were randomly assigned to receive BZA 20 mg, BZA 40 mg, RLX 60 mg, or placebo daily; 7,492 were included in the efficacy analyses. All women were supplemented with 1,200 mg of elemental calcium and 400 to 800 IU of vitamin D. The primary efficacy endpoint was the incidence of new vertebral fractures after 3 years. Secondary endpoints included the incidence of nonvertebral fractures (NVFs) and changes in BMD and bone serum marker concentrations (osteocalcin and C-telopeptide).
Results: Estimated reductions in new vertebral fracture risk were 42% (hazard ratio [HR], 0.58; 95% confidence interval [CI], 0.38–0.89) with BZA 20 mg, 37% (HR, 0.63; 95% CI, 0.42–0.96) with BZA 40 mg, and 42% (HR, 0.58; 95% CI, 0.38–0.89) with RLX 60 mg relative to placebo (P<0.05). Overall, there were no treatment differences in the incidence of NVFs among groups. In a post-hoc analysis of women with femoral neck BMD T-score ≤ (3.0 or ≥ 1 moderate or multiple vertebral fracture at baseline (n = 1,772), the incidence of NVFs was 4.9%, 6.5%, 8.4%, and 9.1% in the BZA 20- mg, BZA 40- mg, RLX 60- mg, and placebo groups, respectively. Relative to placebo, BZA 20 mg reduced NVF incidence by 50% (P = 0.02); a 40% reduction was observed when data for both BZA doses were combined (P = 0.03). BMD was significantly increased relative to placebo in all active treatment groups (P<0.001) at each site analyzed (lumbar spine, hip, femoral neck and trochanter). At all time points, serum marker levels were significantly reduced for all treatment groups compared with placebo (P<0.001). Overall, there were no safety concerns related to the cardiovascular and gynecologic systems, including breast, in any treatment group.
Conclusion: Overall BZA was generally well tolerated, significantly reduced the risk of new vertebral fractures and, in subjects at higher risk for fracture, was associated with a significant reduction in NVFs.
OR14-04
INTERVERTEBRAL DISC HEIGHT IN POSTMENOPAUSAL WOMEN WITH OSTEOPOROTIC VERTEBRAL FRACTURES
Yves Muscat Baron, Mark P. Brincat, Raymond Galea and Neville Calleja
Department of Obstetrics and Gynaecology, St Luke's Hospital, Malta
Objective: To assess Intervertebral Disc Height in postmenopausal women with radiographically confirmed vertebral fractures.
Methods: Two hundred and fifty seven women were collected randomly from a large directory in a data base of a bone density unit. Every fifth woman in the directory was recruited from the DEXA directory.
The image of the vertebral spine on the computer screen was sought for the women recruited. The adjustment mode was then employed allowing the horizontal cursors to be placed at the edges of the vertebral discs between the tenth thoracic vertebra
Results: 257 Women were divided in five groups according to the menopausal/menstrual status. Forty seven (47) menopausal women were on HRT, 77 women were untreated menopausal women, 21 women were on bisphosphonates, 30 women were on calcium supplements, 44 women were premenopausal and 38 women had confirmed vertebral fractures. Age and weight difference were noted across groups and statistical.
The vertebral fracture group was noted to have the lowest disc height (1.57 ± SD 0.1 cm) of the 3 discs D1 - D3. The D1 - D3 disc height in the HRT and premenopausal groups were similar (2.15 ± 01.14 cm) and (2.01 ± 0.19 cm ) respectively. The disc heights in the other three groups (Calcium 1.77 ± 0.08, Untreated menopausal group 1.82 ± 0.12 cm, Bisphosphonates 1.88 ± .012 cm) were significantly lower than the oestrogen replete groups but were significantly higher than the osteoporotic vertebral fractures group.
Conclusion: Postmenopausal women with vertebral fractures have significantly low disc heights. The disc heights are significantly lower then untreated and HRT treated/premenopausal women. These results suggests that the discoid shape and viscoelastic properties of the intervertebral discs may be relevant to the genesis of osteoporotic vertebral fractures.
OR14-05
MENOPAUSAL COMPLAINTS ARE ASSOCIATED WITH A LOWER BONE MINERAL DENSITY
G. C. M. Gast1,5, D. E. Grobbee1, V. J. M. Pop2, J. J. Keyzer3, C. J. M. Wijnands-van Gent3, G. N. Samsioe4, P. M. Nilsson5 and Y. T. van der Schouw1
1University Medical Center Utrecht, Utrecht, The Netherlands; 2University of Tilburg, Tilburg, The Netherlands; 3Diagnostic Center Eindhoven, Eindhoven, The Netherlands; 4Lund University Hospital, Lund, Sweden; 5University Hospital, University of Lund, Malmö, Sweden
Objective: The severity of menopausal complaints has been hypothesized to be linked to a lower bone mineral density (BMD). We examined whether the frequency of menopausal complaints is related to BMD, as a measure that is sensitive for estrogenic effects.
Design & Method: We used data from a population-based sample of 5,600 women, aged 46 to 57 years and free from bone diseases, who were enrolled in the Eindhoven Perimenopausal Osteoporosis Study between 1994 and 1995. Questionnaires were used to collect data on menopausal complaints and potential confounders. BMD of the lumbar spine was measured using DEXA. Linear regression analysis was used to analyse the data.
Results: Flushing was reported by 39% and night sweats by 38% of all women. The average BMD was 1.01 ± 0.14 g/cm2 and decreased with increasing frequency of flushing (P for trend < 0.0001) and night sweats (P for trend 0.0002). After multivariate adjustments, women with the highest frequency of complaints had a 0.022 g/cm2 [95% CI −0.03, −0.01] lower BMD compared to asymptomatic women. Women who reported to have the highest frequency of night sweats had a 0.012 g/cm2 [95% CI −0.02, −0.002] lower BMD compared to women with no complaints of night sweats.
Conclusion: Our findings show that menopausal complaints are associated with a reduced bone density. These results might indicate that women suffering from menopausal complaints differ from those without with respect to susceptibility to estrogens. Further research is needed to extend these findings to other estrogen sensitive end-organs.
OR14-06
RISK OF OSTEOPOROSIS IN PREMATURE OVARIAN FAILURE – APPRAISAL OF DIAGNOSTIC CRITERIA
P. Bose, J. Woodman, H. Grech and N. Panay
Hammersmith/Queen Charlotte's Hospital, London, United Kingdom
Objective: To establish the validity of current diagnostic criteria for osteoporosis/osteopenia in premature ovarian failure.
Design & Method: Bone mineral densities from 42 patients attending the dedicated Premature Ovarian Failure clinic in a London Teaching Hospital were obtained retrospectively from our POF database. The proportion of patients with a dual energy x-ray absorptiometry (DEXA) scan result fulfilling the current WHO criteria for osteoporosis (T2score < −2.5 s.d.) and osteopenia (T score −1 to −2.5 s.d. below mean) were identified.
Results: 48% of patients fulfilled the WHO diagnostic criterion for osteopenia based on reduced lumbar/spine bone mineral density. 4% reached criteria for osteoporosis. 13% of patients were not yet old enough to have reached peak bone density and hence could not be given a formal laboratory diagnosis based on T scores from standard reference charts.
Conclusion: Traditional methods of diagnosis based on T score comparison are inappropriate until maximum bone mass has been attained. The rising incidence of premature ovarian failure in an increasingly younger age group warrants re-evaluation of our diagnostic criteria in order to facilitate management of reduced bone mass in this vulnerable patient group.
Aging brain and hormone protection
OR15-01
A LONGITUDINAL STUDY OF THE ASSOCIATION BETWEEN ENDOGENOUS HORMONE LEVELS AND DEPRESSION IN POSTMENOPAUSAL WOMEN
J. Ryan1,2, H. G. Burger3, P. Lehert4 and L. Dennerstein1
1The University of Melbourne, Parkville, Victoria, Australia; 2Inserm U888, Montpellier, France; 3Prince Henry's Institute of Medical Research, Clayton, Victoria, Australia; 4University of Mons, Belgium
Objective: Across a woman's lifetime, variations in hormonal levels are known to influence well-being and mood. Whether absolute hormone levels or changes in levels over time are associated with depression among postmenopausal women remains unclear.
Design & Method: The Melbourne Women's Midlife Health Project is a longitudinal population based study of women aged 45–55 at baseline, who were followed through the menopause transition. This analysis is based on data collected from 195 postmenopausal women in years 11 and 13 of the study, who were assessed for the presence of depressive symptoms using the Centre for Epidemiological Studies Depression Scale. Multivariate logistic regression models were developed to determine whether absolute hormone levels or change in hormone levels over time influenced depressive symptoms.
Results: Endogenous hormone levels were found to be associated with depressive symptoms in year 11 and with the change in depressive symptoms over the 2-year period. In particular, a large decrease in estradiol levels or increases in follicle-stimulating hormone levels were strong predictors of depression. These associations remained even after adjustment for key confounding factors such as age, the presence of menopausal sympotoms, body mass index and self-rated health.
Conclusion: The risk of depression in postmenopausal women is associated with levels of estradiol and follicle-stimulating hormones. These results further support a role for endogenous hormones in later life depression and suggest the modulation of hormone levels as a potential therapeutic tool.
OR15-02
DEPRESSION AND RELATED RISK FACTORS AMONG CLIMACTERIC WOMEN
P. Chedraui1,2, B. Morales2 and L. Hidalgo1,2
1Academic and Research Department, Hospital Gineco-Obstétrico Enrique C. Sotomayor, Guayaquil-Ecuador; 2Facultad de Ciencias Médicas, Universidad Católica de Guayaquil, Ecuador
Objective: To determine the prevalence of depression and associated risk factors among climacteric women.
Methods: In this cross-sectional study women 40 to 59 years of age were surveyed with the Hamilton Depression Rating Scale (HDRS) and a questionnaire containing general data.
Results: A total of 404 women filled out the HDRS (mean age: 48.2 ± 5.7 years). Mean educational level was 6.9 ± 3.9 years, 85.1% of which had less than 12 years schooling. A 23.8% were premenopausal, 31.4% perimenopausal and 44.8% postmenopausal. At the moment of the survey no participant was on hormonal therapy for the menopause. Mean HDRS total score was 13.7 ± 7 (median 13). A 78.7% had some degree of depression (HDRS total score > 8, mild: 32.1% and 46.6% moderate to very severe). Logistic regression analysis determined that the two main determinant factors involved in presenting depression in this middle aged female group were presenting a more intense menopausal symptoms (OR: 4.47, CI 95%: 2.61–7.64, p < 0.05) and having a partner with low educational level (OR: 1.75, CI 95%: 1.02–3.00, p < 0.05).
Conclusion: In this specific climacteric population, depression was highly prevalent in which symptom intensity and partner educational level were relevant risk factors.
OR15-03
ESTROGEN AND PROGESTINS DIFFERENTLY PREVENT GLUTAMATE TOXICITY IN NEUROBLASTOMA CELLS DEPENDING ON PRIOR HORMONAL EXPOSURE VIA THE INDUCTION OF NEURAL NITRIC OXIDE SYNTHASE
P. Mannella, A. M. Sanchez, A. R. Genazzani and T. Simoncini
University of Pisa, Pisa, 56100, Italy
Background: Sex steroids are important for brain function and neuroprotection. However, growing evidence suggests that these actions might depend on the timing of exposure to steroids.
Objective: We have studied the effects of different protocols of steroid administration on the survival of neuroblastoma cells and partially characterized the mechanisms.
Design & Method: We exposed SK-N-SH neuroblastoma cells to the neurotoxic agent, l-glutamate with or without 24 hours pretreatment with 17β estradiol or 17β estradiol plus progesterone or medroxyprogesterone acetate.
Results: Pre-exposure to any of the steroid combinations turned in enhanced cell survival. However, the addition of the steroids together with l-glutamate, in the absence of a pre-exposure did not protect SK-N-SH cells. Pretreatment with steroid combinations resulted in increased neural nitric oxide synthase (NOS) expression and activity and the pharmacological inhibition of NOS abolished the cytoprotective effects of steroids.
Conclusion: These results suggest NOS induction might be involved in sex steroid induced neuroprotection. Furthermore, these data supports the hypothesis that prolonged and continued exposure to estrogen and progesterone leading to changes in gene expression, could be necessary for sex steroid dependent neuroprotection.
OR15-04
INFLUENCE OF OBESITY ON THE COGNITIVE FUNCTION POSTMENOPAUSAL WOMEN
A. Tavares, H. Romeira and D. Gomes
Catholic University of Brasilia, Brasilia, DF, Brazil
Objective: The study aimed to estimate the influence of obesity on global cognitive function and to identify if there are specific domains of the cognitive function that are affected by obesity, as well as to evaluate if the pattern of obesity, central or peripheral, is associated to impairment of cognitive function.
Design & Method: 301 women aged ≤ 50 years were evaluated, when body mass composition was studied through the following anthropometric measurements: body mass (MC), height (EST), waist circumference (WC), hip circumference (CQ), and average of two abdominal circumferences. From these data, Body Mass Index (BMI), Waist-Hip Ratio (WHR), percentage of body fat (%BF) and Index of Conicity (IC) were obtained. The Mini-mental State Examination (MMSE) test was used to assess the cognitive function.
Results: Evaluating the mmSE performance by these women according to BMI, it was not possible to identify differences between groups regarding to mmSE overall score (p = 0.35). However, it should be noted that taking into account the different sections of the test, it was observed that women classified into the overweight range showed performance on the evocation memory section worse than those with BMI within normal range (p = 0.04). In view of the %BF of these women, once distributed them in quartile groups, those in the highest quartiles of %BF had a significantly worse performance on the evocation memory section when compared to the ones in the lowest quartile group. Considering the IC of these women, it was found that those with body in a more cylindrical shape had better performance on the evocation memory section of mmSE test comparing women whose body shape recalls central obesity.
Conclusion: When the influence of obesity on the cognitive function was evaluated, measured by mmSE, it was identified that obesity, specially, the central one seems to cause impairment to cognitive memory, specifically, to the memory of postmenopausal women. Certainly, future studies will be needed to demonstrate or confirm that way these losses occur.
OR15-05
INFLUENCE OF THE EDUCATION LEVEL ON COGNITIVE FUNCTION IN POSTMENOPAUSAL WOMEN
C. Cárdenas, H. Romeira, A. Tavares and D. Gomes
Catholic University of Brasilia, Brasilia, Brazil
Objective: During the aging process, the emergence of common complaints related to disorders of cognitive function may have multiple causes. This study aimed to identify the degree of influence of the level of education of postmenopausal women on their cognitive function evaluated through mmSE test.
Design & Method: 301 women aged ≤ 50 years ere evaluated. Mini-mental State Examination (MMSE) was taken to assess the cognitive function of postmenopausal women. Overall score for the mmSE of the participants were grouped by age and educational level range. The software Statistical Package for the Social Science version 14.0 was used.
Results: The highest the education level, measured in years of study, the best was the performance of these women in the mmSE test, especially when considering the overall scoring of it (p = 0,001). Considering the different sections of the mmSE test, according to education level, it was possible to identify that postmenopausal women with 0 to 3 years of had significantly lower performance in the overall score (p = 0001), as well as in the sections of the test referring to the language (p = 0001), orientation (p = 0001), attention and calculation (p = 0001). However, it should be noted that, although the level of education has influenced the overall score of mmSE test and some different sections of it, level of education does not seem to influence the performance of postmenopausal women in the section of the mmSE related to memory, especially the evocation memory (p = 0.70).
Conclusion: In this study, an evaluation was made initially to identify the degree of influence of the level of education of postmenopausal women in their performance on the mmSE test. It was not surprised when we found that the education, measured in years of study, plays a major role in the performance of postmenopausal women in the mmSE test. However, we unpredictably observed that low education level was not associated to worse performance in the mmSE test by postmenopausal women despite prior scientific data showing that low education level may determine a higher risk for the development of dementias, and that higher levels of education can set up some form of cognitive reserve.
OR15-06
LIFETIME HORMONAL FACTORS MAY PREDICT LATE-LIFE DEPRESSION IN WOMEN
J. Ryan1,2, I. Carrière1, J. Scali1, K. Ritchie1 and M.-L. Ancelin1
1Inserm U888, Montpellier, France; 2The University of Melbourne, Parkville, Victoria, Australia
Objective: Fluctuating hormone levels are known to influence a woman's mood and well-being. This study aimed to determine whether lifetime hormonal markers are associated with late-life depression symptoms among elderly community-dwelling women.
Design & Method: Detailed reproductive histories of 1013 women aged 65 years and over were obtained using questionnaires and depressive symptoms were assessed using the Centre for Epidemiological Studies Depression Scale. Multivariate logistic regression models were generated to determine whether any lifetime endogenous or exogenous hormonal factors were associated with late-life depression.
Results: The prevalence of depressive symptoms was 17%. Age at menopause was associated with depressive symptoms, but only among women with a lower education level. For these women, an earlier age at menopause increased their risk of late-life depression (linear effect, OR = 0.95, 95%CI: 0.91–0.99). The odds of late-life depression were also increased for women who were past (OR = 1.6, 95%CI: 1.1–2.5), but not current hormonal replacement users. On the other hand, long-term oral contraceptive use ( ≥ 10 years) was protective against depression (OR = 0.3, 95%CI: 0.1–0.9). These associations remained significant even after extensive adjustment for a range of potential confounding factors, including socio-demographic factors, mental and physical incapacities, antidepressant use and past depression. The other factors examined, including age at first menses, parity, age at childbirth and surgical menopause, were not associated with late-life depressive symptoms.
Conclusion: Lifetime hormonal factors that are significantly associated with depression symptoms in later life have been identified. Further work is needed to determine how potential hormonal interventions could be used in the treatment of late-life depression in certain sub-groups of women.
OR15-07
MEDROXYPROGESTERONE ACETATE INCREASES ALLOPREGNOLONE CONTENT IN SELECTED BRAIN AREAS DURING THE REPRODUCTIVE AGING
N. Pluchino, A. Giannini, S. Merlini, A. Cubeddu and A. R. Genazzani
University of Pisa, Pisa, Italy
Objective: The increased use of hormonal therapies has led to the study of the properties of different progestin molecules and their effects on the central nervous system. The aim of the present study was to investigate the effects of a 2-week oral treatment with micronized progesterone or medroxyprogesterone acetate (MPA) alone or in addition to estradiol valerate (E2V) on central and peripheral allopregnanolone content in selected brain areas related to cognition, mood and emotional behavior.
Design and Methods: Thirteen groups of Wistar OVX rats received one of the following treatments: oral progesterone (2, 4 or 8 mg/kg/day); oral MPA (0.05, 0.1 or 0.2 mg/kg/day); E2V (0.05 mg/kg/day); E2V + progesterone (0.05 mg/kg/day + 2, 4 or 8 mg/kg/day), or E2V + MPA (0.05 mg/kg/day + 0.05, 0.1 or 0.2 mg/kg/day) for 14 days. One group of fertile and one group of OVX rats were used as controls. The concentration of allopregnanolone was assessed in the frontal and parietal lobes, hypothalamus, hippocampus, anterior pituitary, adrenals and serum.
Results: Progesterone and MPA increased allopregnanolone levels in all tissues except in the adrenal gland, but some differences between the progestin were evidenced. The combined administration of progesterone or MPA and E2V determined a further increase in allopregnanolone levels with respect to E2V alone except in the adrenal gland and hippocampus only after MPA treatment.
Conclusion: this study demonstrates that progesterone and MPA have a similar but not identical effect on central and peripheral allopregnanolone content. Their association with an estrogenic compound does not interfere with the positive effects produced by estrogen on brain allopregnanolone.
OR15-08
PROGESTERONE TREATMENT IN POSTMENOPAUSAL WOMEN DECREASES TIME OF WAKE IN SLEEP EEG AND HAS NO EFFECT ON COGNITION
P. Schüssler, M. Kluge, M. Dresler, A. Yassouridis, K. Held, J. Zihl and A. Steiger
Max Planck Institute of Psychiatry, Munich, Germany
Objective: In women the cessation of ovarian endocrine function in the menopause is the major turning point in sleep quality. Sleeping problems manifest themselves as difficulty falling asleep, frequent awakenings or awakening in the morning. Fragmented sleep seems to be the main reason for subjectively poor sleep. In animal studies the administration of progesterone into the frontal cortex resulted in an increase of total sleep time. A single oral administration of progesterone in young healthy males prompted benzodiazepine-like effects on sleep-electroencephalogram (EEG). As possible mechanism of progesterone a GABA-agonistic effect and the regulation of gene expression via progesterone receptor are discussed.
Design & Method: We tested whether replacement therapy with progesterone might improve disturbed sleep during menopause. A double blind placebo-controlled cross-over design study with 2 treatment intervals of 21 days duration separated by a 2 weeks washout was performed. A oral dose of 300mg micronized progesterone was given each for 21 days. At the beginning and the end of the two intervals a sleep-EEG was recorded after one night of adaptation and cognitive performance (attention, memory, executive function) was assessed. Subjects consisted of 10 healthy postmenopausal women (age: 54–70 yrs, mean 60.3, SD 5.7), who were free of any medication and of specific sleep disorder (sleep apnoea, restless legs syndrome).
Results: Progesterone treatment led to a decrease of intermittent time spent awake (placebo = 79.7 ± 13.31 min, progesterone = 53.5 ± 7.36 min; p < 0.05) and during the first third of the night to an increase of REM sleep and during the first half of the night to a reduced number of stage shifts. Progesterone produced no consistent effect on cognitive performance.
Conclusion: The decrease of wakefulness is more distinct compared to previous reports in animal studies and males and even more pronounced than effects of estrogens in postmenopausal women. We demonstrated that the oral administration of progesterone partially reverses sleep EEG changes occurring after menopause. The present study opens the possibility that progesterone might be useful in the treatment of sleep disturbances of postmenopausal women.
OR15-09
SLEEP DEPRIVATION IMPAIRS ATTENTION IN YOUNG AND POSTMENOPAUSAL WOMEN: HORMONE THERAPY HAS A MINOR EFFECT
Päivi Polo-Kantola1,2, Paula Alhola2,3, Anna S. Urrila4, Mervi Kylmälä5, Maija Karakorpi2,3 and Outi Huhdankoski4
1Department of Obstetrics and Gynecology, Turku University Central Hospital, Finland; 2Sleep Research Unit, University of Turku, Finland; 3Department of Psychology, University of Turku, Finland; 4Department of Physiology, Institute of Biomedicine, University of Helsinki, Finland; 5Department of Statistics, University of Turku, Finland
Objective: To compare the effect of sleep deprivation on attention in postmenopausal and young women. The modifying effect of hormone therapy (HT) on cognitive performance during sleep deprivation in postmenopausal women was also evaluated.
Design and Method: Twenty-six postmenopausal women (age 58–72 years) participated: 16 HT-users, and 10 non-users. Eleven young women (age 20–26 years) served as controls. All women spent four consecutive nights in the sleep laboratory. Cognitive tests were carried out after the baseline night, the sleep deprivation night and the rebound night. The cognitive measures included tests of several attentional domains.
Results: During sleep deprivation attention was either impaired or the practice effect commonly occurring in repeated cognitive measures was blunted in all groups (p-values<0.05). Generally postmenopausal women performed slower than young controls (p-values<0.05). In Vigilance and 10-choice reaction time (10-CRT) tasks postmenopausal women made less errors and omissions than young controls (p-values<0.05). In simple RT and 10-CRT young and non-users maintained their performance during sleep deprivation, whereas HT-users showed impairment (p-values<0.01). In the Stroop inconguence task performance did not alter in any groups during sleep deprivation. However, in these tasks only the postmenopausal groups showed some recovery after one rebound night (p-values<0.05). In several other measures HT had no effect.
Conclusion: Sleep deprivation impaired attention by hindering the practice effect or causing decline in all groups. Postmenopausal women showed somewhat better recovery and were more likely to maintain accuracy at the expense of reaction speed whereas young women used an opposite strategy. HT had a minor modifying effect.
Supported by the EU grant (QLK6-CT-2000-00499).
HRT and endometrium
OR16-01
GENETIC EXPRESSION OF THE ASSOCIATION OF ESTROGEN AND RALOXIFEN TREATMENT IN THE OVARIECTOMIZED RAT UTERUS
A. V. S. Moraes1, M. J. Sim[otilde]es1, R. S. Sim[otilde]es1, J. M. Soares Jr1, M. A. Haidar1, I. D. C. Guerreiro da Silva1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina Universidade de São Paulo, São Paulo, São Paulo, Brazil
Objective: to evaluate the genetic expression of the association of conjugated equine estrogens (CEE) and Raloxifen (RLX) treatment in the ovariectomized rat uterus. Design and Methods: 90 adult rats, ovariectomized, were divided into seven groups: GI (control); GII (RLX 0.75mg/day); GIII (RLX 0.4mg/day); GIV (ECE 50 μg/day); GV (ECE 25 μg/day); GVI (ECE 50 μg/day + RLX 0.75mg/day) e GVII (ECE 25 μg/day + RLX 0.4mg/day). The length of drug administration was 21 consecutive days. At the end of this period, all animals were sacrificed under anesthesia then the uteri were removed and processed for RT2 Profiler ™ PCR Array Rat Angiogenesis method (Superarray, Cat. No. APR-024A). The expression in each group was compared to control (GI) and the result were identified as u por down-regulated.
Results: In GII, there were seven up-regulated genes and 47 down—regulated genes, In GIII, only 24 genes were down – regulated. In GIV, there were more up-regulated genes than other groups. The GVI and GVII, there were 37 down- regulated genes and 8 up-regulated genes.
Conclusion: The raloxifen partially blocked the angiogenesis effect of estrogen in the ovariectomized rat uterus.
OR16-02
HYSTEROSCOPIC ASSESSMENT OF POSTMENOPAUSAL WOMEN WITH UTERINE BLEEDING ON TIBOLONE THERAPY FOR MENOPAUSAL SYMPTOMS
O. Shawki, M. Aboulghar and W. Sherbini
Cairo university, department of Gynecology, Egypt
Introduction: Tibolone, is currently gaining wide acceptance as safe option for menopausal symptoms relief.
However, up to 20% of women have been reported to have episodes of bleeding whilst on therapy.
Objective: To investigate the prevelance of bleeding episode with Tibolone therapy as well as hysteroscopic and histologic assessment of uterine cavity in those cases.
Patients and Methods:We investigated 38 cases who experienced bleeding episodes whilst on Tibolone (group A) and compared these to 31 cases (group B) who experienced no bleeding whilst on therapy and who underwent similar investigations in the course of a clinical study. All women underwent transvaginal ultrasound, office hysteroscopy and an endometrial biopsy.
Results: Average endometrial thickness in group A was 4.8 ± 1.9 mm and in group B was 4,6 ± 1.3 mm as measured by vaginal sonography.Office hysteroscopy revealed 11 women with intracavitary lesions on (including one in the control group B), 9 with polyps, 2 with fibroids. The high incidence of uterine polyps in the group who bled on Tibolone suggests an etiologic relation.
Conclusion: We conclude that episodes of bleeding in patients receiving Tibolone for hormone replacement therapy, whilst warranting investigation, should not cause undue concern.
Histological assessment in cases with bleeding revealed benign nature of endometrium.
OR16-03
PSYCHOLOGICAL MORBIDITY IN WOMEN INVESTIGATED FOR POSTMENOPAUSAL BLEEDING
A. Gale1, R. Tarling2, P. Martin-Hirsch1 and P. Dey2
1Lancashire Teaching Hospitals NHS Foundation Trust, Preston, England; 2University of Central Lancashire, Preston, England
Background: There is little research into women's concerns about assessment for postmenopausal bleeding.1 We report a pilot study designed to quantify levels of psychological morbidity in these women.
Methods: Women aged over 44 years referred with postmenopausal bleeding were identified prior to any investigation. After informed consent was obtained, women completed the short form state scale of the state trait anxiety index, Impact of Events scale (IES), and Hospital Anxiety and Depression Scale. These questionnaires were postally administered four days (before hysteroscopy) and twelve weeks later. Women diagnosed with cancer were excluded from the twelve week assessment.
Results: Fifty-five women were recruited. The mean age and age at menopause was 63 years and 50 years respectively. Twelve women presented within two weeks of the onset of symptoms which in 17 women was heavy/moderate bleeding. Compared to the women presenting within 3 months of symptom onset, those who delayed presentation tended towards lower levels of anxiety and significantly lower mean scores on the intrusion subscale of the IES (difference = 5.0,95% CI 1.77 to 8.24).
For all women, mean scores of all psychological morbidity measures were high at baseline and 4 days but reduced to population norms within twelve weeks. Women diagnosed with cancer had higher anxiety levels at baseline and 4 days. In women without cancer, those who did not undergo hysteroscopy tended to have lower mean scores on the avoidance scale of the IES at baseline and 4 days compared to women who had a hysteroscopy but, surprisingly, these levels did not decrease by twelve weeks (baseline: 9.2 (sd 7.84) vs 12.3 (9.25); 4 days 9.5 (8.42) vs 13.4 (10.53); 90 days: 9.9 (10.04) vs 6.1 (8.58)).
Conclusion: Psychological morbidity is similar to that observed in women undergoing assessment of breast lumps or cervical abnormalities.2,3 This pilot study suggests some interesting patterns in subgroups of women with postmenopausal bleeding. A larger longitudinal study is warranted.
OR16-04
RECURRENT POSTMENOPAUSAL BLEEDING FOLLOWING PREVIOUS NEGATIVE INVESTIGATIONS WARRANTS RE-INVESTIGATION
R. Ronghe and M. Gaudoin
Southern General Hospital, Glasgow, Scotland, UK
Objective: The SIGN Guidelines recommend re-investigation of women with postmenopausal bleeding (PMB) after 6 months. The aim of this study was to determine the incidence of endometrial carcinoma in patients with recurrent PMB following previous negative investigations and to establish when repeat investigations should be undertaken.
Design & Method: B This was a retrospective analysis of women presenting with recurrent PMB following negative investigations in a dedicated PMB clinic. The study was carried out over a period of 45 consecutive months (January 01, 2003 – August 31, 2007). All women were investigated with transvaginal ultrasound, ± Pipelle endometrial biopsy or hysteroscopy and curettage.
Results: A total of 1106 individual women were seen in the clinic. At first presentation 34 were diagnosed with endometrial carcinoma, 6 with ovarian, 6 with cervical and 1 with fallopian tube carcinoma. 9 had atypical endometrial hyperplasia. 76 patients had initial negative investigations followed by recurrent PMB. Of these 31 had one episode and 45 had >1 episode of PMB at first visit. 20 patients were taking continuous combined hormone replacement therapy (HRT) and 4 were on sequential HRT. The mean body mass index was 28.2 kg/m2 (17.6–51.6). Of the 76 women, 62 had one further episode of PMB, 8 had two and 6 had 3 or more episodes. The mean time from first to second visit was 15.6 ± 9.1 months. The mean endometrial thickness (ET) for all women seen in the clinic was 4.0 ± 5.0 mm. For our study group the mean ET at their first visit was 4.0 ± 3.2 mm (P = NS) and at the subsequent visit was 4.1 ± 4.3 mm (P = NS). On subsequent visits 4 patients had benign endometrial polyps and 2 were diagnosed with endometrial carcinoma (3%). The ET for the first patient was 9 mm at first visit (the second patient underwent hysteroscopy because she was on tamoxifen). Both these patients had negative endometrial biopsy at their first visit. The time between first and second presentation for these patients was 20 and 26 months respectively.
Conclusion: In our study the incidence of endometrial carcinoma in women presenting with recurrent PMB after initial negative investigations was 3% which was the same as women presenting for the first time and none represented with a cancer within 1 year. Our study confirmed the importance of investigating women with recurrent PMB but perhaps the recommendations for re-investigation from the SIGN Guidelines could be altered from 6 to 12 months.
OR16-05
SCREENING OF CERVICAL CANCER IN DEVELOPING COUNTRY BY VISUAL INSPECTION OF CERVIX AFTER APPLYING ACETIC ACID
Latifa Shamsuddin1, M. I. Ullah2, S. Tamanna2, Murshed Jahan Binte Ali3 and R. M. A. Kabir3
1Barnali Nursing Home, Mirpur, Dhaka, Bangladesh; 2Fairmont Medical Center, Mayo Health System, Minnesota, USA; 3Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh
Objective:
The present study is aimed at screening cervical cancer in a defined geographic area by visual inspection of cervix after applying acetic acid (VIA) in liaison with the field level workers.
To develop an easy, simple, low tech and a reliable method to screen cervical cancer which contributes 22–29% of female cancer in the country.
Emphasis is also given to involve the community and to motivate them by creating awareness about this preventive program and educate people about the disease.
Result: A total of 224 respondents were enrolled in this study. They underwent initial clinical evaluation to make sure they meet the study selection criteria. All of them were then subjected to the visual inspection of cervix after applying acetic acid (VIA). Ten of them were identified as having positive test. Four of then were between age 35–40. The other 6 were between age 41–50. Five of the VIA positive cases had regular menstrual period, 3 had irregular menstruation and 2 were postmenopausal. All of them had at least one pregnancy. The screening test was very easy to perform in that remote community where standard screening tests like Paps smear is not available due to lack of resources and infrastructure. The patients with positive findings in VIA were further evaluated by colposcopy and biopsy for definitive diagnosis. All of them were found to have Cervical Intraepithelial Neoplasia (CIN). Six of them had CIN-I, 2 had CIN-II and 1 had CIN-III.
Conclusion: VIA is a cost effective and reliable screening program for primary prevention of cervical cancer in the current infrastructure of Bangladesh. It requires minimal training of existing personnel in the community without expensive equipment or resources. It is possible to integrate cervical cancer screening with this method into the primary health care service throughout the country. This may be the best approach for a developing country for early detection of cervical cancer where standard screening methods like paps smear is not readily available at the grass route level. The patients with positive results could be further referred to larger hospitals or tertiary care centers for definitive diagnosis by colposcopy or biopsy as clinically indicated. This will help in early detection of cervical dysplasia and neoplasm which is critical if we are to reduce the burden of this preventable disease in the country.
OR16‐06
THE ROLE OF AROMATASE EXPRESSION IN REGULATING ENDOMETRIAL POLYP PROLIFERATION DURING MENOPAUSE
H. Maia Jr1,2, K. Pimentel2, J. Casoy1 and T. Cruz2
1Centro de Pesquisas e Assistência em Reprodução Humana (CEPARH), Salvador, Bahia, Brazil; 2Federal University of Bahia, Salvador, Bahia, Brazil
Objective: To determine whether there is a positive correlation between aromatase expression in endometrial polyps during menopause, the proliferation rates of these polyps and Cox-2 expression in the glandular epithelium.
Design & Method: Fifty-two menopausal patients with endometrial polyps were submitted to polypectomy carried out using the Bettocchi hysteroscope. The presence of aromatase, ki-67 and Cox-2 expression was determined by immunohistochemistry in paraffin-embedded blocks of samples of endometrial polyps. The intensity of Cox-2 expression was graded from 0 (negative) to + 3 and percentages of Ki-67-positive cells were counted in the glandular epithelium and correlated with the presence of aromatase expression. Statistical analysis was carried out using the Mann-Whitney or Fisher's Exact tests with significance established at p < 0.05.
Results: Aromatase expression was detected in 44% of endometrial polyps. The staining reaction was detected either in the glandular epithelium, stroma or in both tissues in 60%, 30% and 10% of the cases, respectively. In the endometrial polyps in which aromatase expression was positive, median positive ki-67 values in the glandular epithelium were significantly higher when compared to polyps in which aromatase expression was negative (10 versus 0; p < 0.001). Median Cox-2 expression in the glandular epithelium was also significantly higher (2 versus 0, p < 0.001) in the aromatase-positive polyps. Endometrial hyperplasia was detected in 5 endometrial polyps, all of which were aromatase-positive.
Conclusion: These results suggest that the presence of aromatase expression in endometrial polyps during menopause is associated with higher proliferation rates and a more intense Cox-2 expression in the glandular epithelium. This may indicate a role of local estrogen production in stimulating proliferation and up-regulating prostaglandin production in endometrial polyps, which would be associated with a higher risk of progression to hyperplasia in the polyp.
Miscellaneous
OR17-01
EFFECT OF AGE ON ART OUTCOME IN PATIENTS OF GENITAL TUBERCULOSIS
S. Malik and R. Sharma
Southend Fertility and IVF Center, New Delhi, India
Objective: To assess whether age compounds the effect of genital tuberculosis on already poor ART outcome in these patients
Design & Methods: Retrospective analysis of 200 cases of genital tuberculosis who underwent ART after treatment.
The case records of 200 patients of previously diagnosed and treated genital tuberculosis who had undergone ART were analyzed. All patients had two or more indicators for genital tuberculosis. These were divided into two groups depending on their age. Group A included 122 cases of patients who were less than 35years of age and Group B, 78 cases of patients more than 35yrs of age. The records were then analyzed for the endocrinal profiles, U/S appearance of the ovaries and uterus, type and number of IVF cycles undertaken, response to COH, ART outcome and pregnancy outcome.
Results: The baseline profiles of patients in both groups showed a disturbed anatomy and physiology. Patients in-group A showed tuboovarian mass (T.O. mass) in 20(16.39×) patients, endometrioma in 18(14.75%) & multicystic ovaries in 24(19.67%) patients, while in group B 14(17.94%), 12(15.38%), 16(20.51%) patients showed T.O. mass, endometrioma & multicystic ovaries respectively, 35(28.68%) patients in group A & 32(41.025%) patients in group B showed signs of endometrial damage. 39(31.96%) patients in group A & 30(38.46%) patients in group B showed basal FSH level >10. Group A patients underwent 280 IVF cycles (Average 2.29 cycle/patient) & in-group B total 215 IVF cycles were carried out (Average 2.78 cycles/patient). 39(31.96%) patient in group A & 30(38.46%) patients in group B underwent donor recipient cycle in first attempt. 7(5.7%) patients in group A & 18(23.07%) patients in-group B went through surrogate cycles. 75(26.78%) cycles in group A & 44(20.46%) cycles in group B had clinical pregnancy. Take home baby rate in-group A was 18.57% per cycle & in-group B was 17.94% per cycle.
Conclusion: Our results reveal that tuberculosis probably affects fertility at a much earlier age and even in the younger patients similar functional behavior is observed during ART cycles.
OR17-02
EFFECTIVE DISSEMINATION OF RESEARCH FINDINGS – TAKING IT TO WOMEN AND HEALTH PROFESSIONALS
S. Cook, N. McGrath, S. Foster and J. Michelmore
The Jean Hailes Foundation for Women's Health, Clayton, 3168, Victoria, Australia
Objective: To effectively translate and disseminate key research findings about women's midlife health into evidence based, consistent messages through a variety of mediums.
Design & Method: The Jean Hailes Foundation for Women's Health (the Foundation) has a Research Unit, an Education Unit and a Medical Centre. These three units work closely to ensure that health professionals, women and the community receive up-to-date evidence-based information on health issues relevant to women at midlife. This is achieved through a model of education and health promotion (including media) that ensures consistent information is disseminated through seminars, webcasts, podcasts, videoconferencing, fact sheets and on-line education activities. Seminars are often delivered in rural and remote areas of Australia where health professionals and consumers have limited opportunity to personally receive information. The Foundation's website has information available for health professionals and consumers that can be read on-line, downloaded, listened to via podcast, or viewed via webcast. Health professionals have the opportunity to achieve Continuing Professional Development points by completing Active Learning Modules in areas such as Hormone Therapy, Osteoporosis and Polycystic Ovary Syndrome (PCOS). Education sessions are also delivered to health professionals across Australia via videoconferencing. On-line learning and videoconferencing offers educational opportunities to rural/remote health professionals who may otherwise have difficulty accessing educational programs. Consistent, evidence-based health messages are being provided to health professionals and consumers in Australia through these various mediums to ensure accessibility for all.
Results: In 2007 the Foundation published 20 articles in scientific literature and the medical centre assisted more than 9,000 women. One and a half million people accessed information from the Foundation's website and more than 100,000 fact sheets were downloaded and/or distributed to health professionals and consumers. Fact sheets have also been translated into 16 languages. Three hundred and fifty women and 90 health professionals in rural/remote Australia attended seminars on menopause and midlife women's health, and more than 1400 health professionals accessed the Foundation's on-line educational activities that are rigorously evaluated. Three hundred and sixty-eight national media articles outlined key issues in women's midlife health.
Conclusion: The methods used by the Jean Hailes Foundation for Women's Health demonstrate that key research findings are able to be successfully translated and disseminated to women and health professionals through a variety of mediums. This range of mediums allows women and health professionals to access up-to-date, evidence-based information suited to their individual needs.
OR17-03
HYPERGONADOTROPIC AMENORRHEA AND PREGNANCY
Helena Meden-Vrtovec1, Ksenija Geršak1 and Damir Franić2
1University Medical Center Ljubljana, Department of Obstetrics and Gynecology, 1000 Ljubljana, Slovenia; 2Outpatient clinic Ob&Gyn dr. Franić, 3250 Rogaška Slatina, Slovenia
Background: The diagnosis of premature ovarian failure affects around 10% of patients seeking evaluation of secondary amenorrhea. Beyond oocyte donation there has been no proven effective therapy to achieve pregnancy in these patients. However, some anecdotic cases of successful treatment of special subgroups of hypergonadotropic amenorrhea deserve more attention and evaluation.
Material and Methods: In order to analyze etiologic factors of hypergonadotropic amenorrhea in 70 women aged 32,5 ± 5,71 years precise history of the disease was evaluated together with repeated determination of FSH, E2, PRL and TSH levels and karyotype determination.
Results: Of the 70 patients we registered 17 cases of chromosomal abnormalities, in 18 hypergonadotropic amenorrhea followed extensive gynecologic surgery, 10 were previously using oral contraceptives and 4 had chemo- and radiotherapy for malignant diseases. In 23 patients (32,8%) etiology could not be identified (idiopathic). Three patients of the last group conceived and delivered healthy babies after estrogen-progestin replacement therapy.
Conclusion: Patient with hypergonadotropic amenorrhea and infertility should be precisely investigated on history of the disease, thus identifying the subgroup with possible treatment perspectives. According to our results estrogen and progestin replacement in pharmacological dosage should be offered to those with idiopathic hypergonadotropic amenorrhea and normal karyotype, prolactin levels and thyroid function as soon as diagnosis is confirmed.
OR17-04
INTERNET AND A WEB 2.0 PLATFORM IN SPANISH ABOUT WOMEN'S HEALTH
F. R. Pérez-López1, M. T. López Baena2 and G. R. Pérez Roncero2
1University of Zaragoza Faculty of Medicine, Zaragoza 50009, Spain; 2Instituto Ginecológico de Zaragoza, Zaragoza 50010, Spain
Since 1996 one of the authors (FRPL) has been experiencing with the quality and content of the web 1.0, and has created a specific site for information about women's health in Spanish (http://www.unizar.es/gine/home.htm). Web 2.0 open new opportunities for communication, although it has many different definitions even for web experts. Not all the people, who talk about it, are agree with this term. The Web as a platform means that “if you want to do something with the computer you will do it online by using the browser. You do not need to install nothing or almost nothing at all in order to do that”. Therefore, web 2.0 is more a culture of online expression than a technology platform. These technologies have led to a flurry of new applications and speculation on their potential to revolutionize health care and the entire spectrum of health and medicine. Since 1 May of 2007, we have been developing a blog, in Spanish, considering the previous background with the conventional web. The growth has been very strong, reaching 250.000 visits in nine months. On the other hand, web 2.0 allows new models of e-learning, patient education, medical training and continuing medical education. During the present academic year a new formal educative program has been initiated under the title “Internet and e-learning of Evidence Based Medicine” at the University of Zaragoza Faculty of Medicine, with the main objective to train the future physicians in the use of web 2.0. Women's health information is one of the major topic of this course.
OR17-05
MEDICAL ANTHROPOLIGAL APPROACH TO CLIMACTERIC: PRELIMINARY STUDY IN WOMEN IN LA PLATA AREA, ARGENTINA
O. Forestieri1, L. Fitte1,2, L. Forestieri1, R. Krakover1 and M. Ferreras1
1Universidad Nacional de La Plata, Buenos Aires, Argentina; 1,2CONICET, La Plata, Buenos Aires, Argentina
Objective: To identify the variability of consultation reasons in menopausal women belonging to different sociocultural groups.
To analyse the ways patients who live in La Plata area experience menopause.
Design & Method: Interdisciplinary, transverse and descriptive study carried out from March, 2006 to December, 2007. Two hundred and eleven (211) climacteric women were assessed and assisted at the Chair of Gynecology B surgeries, FCM, UNLP, by a team of gynecologists and an anthropologist. Women included in the study share three characteristics:
They live in La Plata and Gran La Plata.
Age group: 45–65.
More than a year of amenorrhea (spontaneous menopause).
Semi structural interviews and surveys were used in accordance with the research objectives. The information was analysed through basically descriptive statistical methods. The interview items were: age, partnership status, nationality and birth place, period of residence in La Plata, occupation, number of children, educational level, reason for seeking assistance related to menopause, importance given to this stage in life and to gynecological control.
Results: The observed differences among the different subgroups were:
Vasomotor syndrome perceived by Paraguayans (53.4%), Tobas, Peruvians and Bolivians. 28.8% and Japanese: 17,8%.
The relative percentages regarding urogenital atrophy were: Bolivians and Peruvians: 34.6%; Tobas: 32.5%; Paraguayans: 23.6% and Japanese: 12,4%.
The psychoneurobiological syndrome was present at 30.2% of Paraguayan women subgroup and at 8.3% of Japanese women.
As regards the relevance given to the gynecologist consultation during the climacteric, 66.7% of the Japanese population considers it important, followed by 22.2% of Paraguayans and 2.6% of Bolivians, Peruvians and Tobas.
Conclusion: Even though women live in the same geographic area, the expression of menopause and its incidence on health differs in the various sociocultural groups analysed. This leads us to research the sociocultural variables that have influence on the observed diversity in the manifestations of climacteric among each of the studied subgroups. Interdiscipline is the tool that will allow us to analyse and interpret this variability.
OR17-06
MEDICAL CONTINUOUS EDUCATION IN CLIMACTERIC TEN YEARS EXPERIENCE
E. Depiano, O. Forestieri, M. Murga, C. Vassino and D. Pantano
Argentinian Climacteric Study Association, Argentina
Objective: Medical Continuous Education is a group of education experiencies, wich follows the graduate formation. Argentinian Climacteric Study Association objectives are:
– Stimulate and get best formation in postgraduate climacteric.
– Teach doctors in handling menopause woman.
Design and Methods: Argentinian Climacteric Study Association begines activities on 1997 and has developed courses for a year, presential and far, for doctors in Femenine Health. The activities are interdisciplinary. We have done.
Eleven annual presential courses (1997–2007)
Three annual courses on line (2005–2007)
Educative methods:
Presencial : presencial classes, in blocks, whith discussion activities.
On Line: programated classes, in blocks, whith individual key, virtual forums discussions and chats.
The teaching staff is integrated by diferent professionals (gynaecologist, biochemist, psychologist and sociologists). Tests are parcial (in the meddle of year) and another final test, oral and/or write, and also have to do a final monograph about climateric theme. This was analizated whith the dificulty index, which takes note the proportion of student that answer the right question.
Results: In the period 1997–2007 have been teached 14 annual courses, with 531 doctors.
Doctor/year: 48. Discussion activities: 72. Free time between blocks: 7 days (1997–2001), 15 days (2001–2004), 30 days (2005–2007) for the presential course, and for on line course 15 days. Participation percent in the on line forums was 30%. Total percent approvation test 86%. Total percent approvation test and monograph: 83.5%.
Dificulty index: p = 84–50 (relatively easy).
Conclusion: The teaching work realized during 10 years in the AAPEC have shown that the pedagogic innovations (on line courses) and educated model get best for Continues Medical Education Presentail and for Distant in post of beter education quality. The blocks model activity get best results in learning index. The program teching in climateric of AAPEC is the first one in Argentina and Latin America.
OR17-07
MENOPAUSE IN RENAL TRANSPLANT WOMEN
Y. Fan and R. Cubal
Hospital Geral de Santo António, Porto, Portugal
Objective: This study was undertaken to assess menopausal symptoms in renal transplant women and to compare them to the symptoms experienced by healthy women.
Design & Method: One hundred postmenopausal women aged between 50 and 60 participated in this study. They were stratified into 2 groups: group I: 50 renal transplant recipients medicated with immunossupressor drugs; and group II: 50 healthy women. All subjects were asked to complete a questionnaire including age of menopause, a 24-item qualitative evaluation form to assess menopausal symptoms and use of hormone replacement therapy (HRT).
Results: The mean age of the onset of spontaneous menopause was 44.6 (±7.5) years (range: 19–56 years) in group I, having the patients been renal transplanted for an average of 15.5 (±4.5) years (range: 10–24 years); while in group II the mean age of menopause was 50.1 (±3.6) years (range: 37–55 years). Hot flush was the most frequently experienced symptom in moderate or extreme scale in both groups (58% in group I vs 38% in group II). Other common complaints in the same scale were joint pains (58%), depressed moods (52%), night sweats (48%), diminished libid (46%), dry skin (44%), trouble sleeping (42%), memory loss (42%), vaginal dryness (40%) and dispareunia (38%) in group I; and night sweats (38%), joint pains (22%), trouble sleeping (18%) and irritability (14%) in group II. Twenty percent of patients used HRT in group I, when compared to 84% in the group of healthy women. The mean duration of HRT was 3.9 (±1.5) years (range: 0.5–5 years) in the first group, while it was 3.8 (±2.3) years (range: 1–10 years) in the second one.
Conclusion: Renal transplant women are more likely to reach menopause at a younger age. These patients suffer severe menopausal symptoms and a small percentage of them is treated with HRT. Special efforts should be made in the management of menopause and risk-benefit evaluation of HRT in these women in order to improve their quality of life.
OR17-08
IN VITRO FERTILISATION (IVF) WITH DONOR EGGS IN POST-MENOPAUSAL WOMEN: ARE THERE DIFFERENCES IN PREGNANCY OUTCOMES IN WOMEN WITH PREMATURE OVARIAN FAILURE COMPARED WITH WOMEN WITH PHYSIOLOGICAL AGE-RELATED MENOPAUSE
B. Vollenhoven1,2,3, T. Osianlis1, G. Weston1,2,3 and J. Catt1
1Monash IVF, Melbourne, Victoria, Australia; 2Southern Health, Melbourne, Victoria, Australia; 3Monash University, Melbourne, Victoria, Australia
Objective: Donor eggs are used for IVF in women with either premature ovarian failure (POF) (<40 years old) or physiological age-related menopause ( ≥ 40 years old) who desire children. This study compared pregnancy rates and pregnancy complication rates in women with POF (group A) with post-menopausal women ≥ 40 years old (group B) after IVF with donor eggs.
Design and Method: We examined patient histories between 2000–2007. Menopause (either premature or normal age-related) was defined as amenorrhoea ≥ 12 months plus 2 FSH measurements >20IU/L. There were 26 women in group A (average age 32.8 years) and 16 women in group B (average age 45 years) who had undergone IVF with donor eggs.
Results: In group A there were 2 women with POF as a result of Turners Syndrome, 2 as a result of chemotherapy and 1 as a result of bilateral oophorectomy. There were a total of 143 initiated cycles (fresh and frozen) examined and there were 110 resulting transfers. The clinical pregnancy rate per embryo transfer was 28% in Group A and 42% in Group B, with no significant differences between the two groups. There were a total of 36 pregnancies in the two groups: 4 ended in miscarriage, 25 delivered, and 7 pregnancies were ongoing (>12 weeks gestation) at the time of writing. On a per patient basis, in group A there was a 62.5% chance of taking at least one baby home and in group B the chance was 64.3%. Of the delivered pregnancies, 16 were in Group A and 9 in Group B. Complications including IUGR, pre-eclampsia, gestational diabetes, and placenta praevia occurred in 31% of Group A completed pregnancies, and 78% of Group B completed pregnancies (p < 0.01).
Conclusions: Based on this series of patients who were defined into 2 groups by stringent criteria, women with POF have considerably less pregnancy complications than women with age-appropriate menopause. There were however no significant differences in pregnancy rates between the two groups. Menopausal women using donor eggs have a 2 in 3 chance of eventually taking home a baby, irrespective of age.
OR17-09
WHO IS REFERRED TO A DEDICATED PREMATURE MENOPAUSE CLINIC?
D. Yap, A. Vincent, B. Vollenhoven and E. A. Farrell
Monash Medical Centre Menopause Unit., Southern Health Network, Melbourne Australia
Objective: To establish who is referred to a dedicated Premature Menopause Clinic and to compare the differences in management between ad hoc management and standardised management based on Best Practice guidelines practised in a dedicated teaching unit.
Design & Method: A literature review was undertaken examining premature menopause in general and models of care available for the management of Premature Menopause internationally and nationally.
An audit of the first 100 attendees to Premature Menopause Clinic at Monash Medical Centre was undertaken. Standardised data-collection sheets were used to collect both demographic data prospectively and clinical data retrospectively. Patient age at referral, age of diagnosis and age of first symptoms, geographical location and distance travelled to the clinic were collected. The reason for the referral as documented by the referring doctor, type of referring doctor and other specialists seen, prior to attendance were also recorded. Referral investigation and diagnosis, were compared by referrer type, to clinic investigations undertaken and clinic diagnosis. The presence or absence of treatment at time of referral, treatment type where present at referral and clinic treatment changes from this were examined.
Results: In an attempt to provide for the more special-needs of young women suffering from a Premature Menopause, the Monash Medical Centre Menopause Unit started Australia's first dedicated ‘Early Menopause Clinic’ in 2002. The tradition model of care for Premature Menopause sufferers in Australia prior to the establishment of this clinic was non-standardised diagnosis, investigation and treatment from a variety of medical practitioners – General Practitioners, Specialist Gynaecologists, Endocrinologists and Fertility Specialists. A standardized approach to the investigation, diagnosis and management was adopted by the Premature Menopause clinic.
Whilst the majority of women were referred by General Practitioners, other specialists also referred to the clinic. Accuracy of referral diagnosis was variable, as was rigorousness of pre-referral investigation. Comprehensive management including psychological care could be provided through a dedicated multidisciplinary specialist service.
Many women who had experienced their menopause prematurely but who were no longer under 40 utilised the clinic for the purposes of review and explanation. The clinic did not service just their local community, but women who had travelled significant distances. Treatment regimens at referral were quite variable in both type and suitability.
Results: Women with Premature Ovarian managed ad hoc in their community are subjected to a fluctuating accuracy of diagnoses, types of investigations undertaken and a varying standard of and management. Women will travel long distances if they perceive that a dedicated clinic will better service their needs. Women will present to a Premature Menopause Clinic at a variety of ages seeking an explanation or review of their Early Menopause status. Standardised guidelines facilitate a comprehensive management approach.
Premature menopause audit.
Abstracts of Poster Sessions
Hormones and breast cancer
PS-01
AGE AT DIAGNOSIS IN BREAST CANCER: PROGNOSTIC FACTOR FOR DISEASE FREE SURVIVAL
Claudia Arce-Salinas, P. Santaella-Morales and Jorge L. Martínez-Tlahuel
Women diagnosed with breast cancer, which are younger than 35 years-old, and older than 65 years-old seem to have a poorer prognosis. Young women with breast cancer are more likely to have affected lymph nodes, be negative for oestrogen receptors, and have larger and anaplastic tumours. Women older than 65 years-old, usually are considered as a fragile patients, with co-morbidities (obesity, renal failure and diabetes), and could not receive chemotherapy at full doses.
Objective: To investigate whether young and old age at diagnosis is a negative prognostic factor in primary breast cancer and how stage of disease at diagnosis and treatment influences such an association.
Design: Retrospective cohort study based on a population based database of patients with breast cancer containing detailed information on tumour characteristics, treatment regimens, and relapse.
Results: We evaluate 286 patients with diagnosis of breast cancer confirmed by core-needle biopsy, in stage I-III, treated from January 1998 to December 1999, with adjuvant or neoadjuvant chemotherapy based in doxorubicin, for at least 4 cycles. We defined younger woman, those who had less than 35 years-old, middle age those who were between 35 to 64 years-old and older woman those who were older than 65 years-old. The median follow-up was 91 months interpercentilar interval was 46 to 102 months. The distribution of the groups according stage, tumor grade, presence of lymphatic permeation and treatment were not different. We estimated disease free survival with Kaplan-Meier method; at 91 months, the median disease free survival for age group was 68, 93 and 91 months respectively with log-rank 0.047. We performed a multivariate cox analysis, stage at diagnosis was an independent prognostic factor for disease free survival p = 0.001. There were not differences in overall survival.
Conclusion: Age and stage at diagnosis were independent prognostic factor for disease free survival. Younger women have poor prognosis in comparison with middle age and older women. This data suggested than older women should be treated as same as middle age women.
PS-02
AUTOIMMUNE THYROID DISEASE, A RISK FACTOR FOR BREAST CANCER
P. Carpintero1, M. Franchina1,2, D. Della Latta2 and B. Campostrini2
1Centro de Medicina Preventiva Lanús, Buenos Aires, Argentina; 2Hospital Narciso López de Lanús, Buenos Aires, Argentina
Objective: To describe the behaviour and establish the statistical significance of diabetes, obesity, smoking, nulliparity and autoimmune thyroid disease on the possibility of having breast cancer in post menopausal women (PMW) in our study population.
Design & Method: Retrospective, case-control model, consecutive review of 600 medical records of PMW that attended Centro de Medicina Preventiva and Hospital Narciso López de Lanús between 1/1/2006 and 8/31/2007. 534 cases were selected.
Exclusion criteria: Patients that had not completed the requested laboratory.
Variables: Age-Menopause-TSH- TPOAb- Breast Cancer- Diabetes – Obesity- Nulliparity. Statistics: Descriptive and comparative statistics were used according to the variable scale and comparative model. χ2 and odds ratio tests were used for the comparative bivariate model and confidence intervals (CI) of 95% were calculated. Logistic regression method was used for the multivariate analysis. It was considered an α error = 0, 05.
Results: n = 534 PMW. Menopause: Mean 47,7, SD ± 8,6. Range: 43–85. Autoimmune thyroid disease: 165 (30,9%). Hypothyroidism: 25 (4,7%). Nulliparity: 71 (13,3%). Breast Cancer: 63 (11,8%). Diabetes: 100 (18,7%). Smoking: 94 (17,6%). Obesity: 258 (48,3%).
The following estimated risk factors of having Breast Cancer for each independent variable were obtained from the bivariate analysis.
The following results were obtained from the logistic multivariate regression analysis.
Conclusion: From 534 patients reviewed, 165 had autoimmune thyroid disease (30,9%) and 63 had Breast Cancer (11,8%). There was a significant relation between autoimmune thyroid disease, diabetes, nulliparity, smoking and the possibility of having breast cancer in post menopausal women.
The logistic regression analysis showed that these variables could act independently from each other.
PS-03
ACUTE TRYPTOPHAN DEPLETION, CENTRAL SEROTONIN, AND HOT FLASHES AFTER BREAST CANCER
J. S Carpenter, T. Skaar, A. M. Storniolo, J. Milata, J. Wu and M. Yu
Indiana University, Indianapolis, IN, USA
Objective: Among women with breast cancer, hot flashes are frequent, severe and bothersome symptoms that can negatively impact quality of life and compromise compliance with life-saving medications (e.g., tamoxifen). Clinicians' abilities to treat hot flashes are limited due to inadequate understanding of physiological mechanisms involved in hot flashes. Using an acute tryptophan depletion paradigm, we tested whether alterations in central serotonin levels were involved in the induction of hot flashes in women with breast cancer.
Design and Method: This was a within subjects, double blind, placebo controlled, balanced, crossover study. 27 women completed two 9-hour test days. On one test day, women ingested a concentrated amino acid drink and encapsulated amino acids (no tryptophan) according to published procedures that have been shown to have specific effects on serotonin within 4.5 to 7 hours. On the other test day, women ingested a control drink. Serial venous blood sampling and objective hot flash monitoring were used to monitor response to each condition.
Results: Response to acute tryptophan depletion was variable and unexplained by use of selective serotonin receptor inhibitors, anti-estrogens, or breast cancer disease and treatment variables. Contrary to our hypothesis, hot flashes were not uniformly worsened by reduction of central serotonin levels (p = ns).
Conclusion: Direct manipulation of the serotonin system may not affect physiologically documented hot flashes. Future research is needed to understand these findings which contradict the reported efficacy of serotonin reuptake inhibitors for treatment of hot flashes. Additional analyses are underway on genetic polymorphisms in serotonin receptor and transporter genes that may help explain the variable response.
PS-04
BREAST CANCER AND HRT. INCIDENCE IN THE MENOPAUSE UNIT AT THE UNIVERSITY HOSPITAL SAN CECILIO
E. Carmona Sánchez, J. L. Cuadros López, A. Cuadros Celorrio, O. R. González Vanegas and A. Fernández
Hospital Clínico San Cecilio, Almuñecar, Granada, Spain
Aim: The aim of this study is to describe the incidence of breast cancer in women treated with HRT in the menopause unit at the University Hospital of San Cecilio over a follow-up period of 10 years.
Material: The study included menopausal patients who started their treatment with HRT between 1989 and 1998; thus, by 2007, they had undergone a minimum follow-up of 10 years (N:877). Before starting treatment all patients underwent screening (breast screening and mammogram) to eliminate breast malignancies. Three women in whom breast cancer was detected during the previous screening did not receive treatment and thus were not included in the study.
Method: During the treatment period all patients had annual check-ups which included comprehensive laboratory tests (blood and urine), breast screening and mammograms.
Results:
Further to these six cases, we had anothers four cases of breast cancer in this population which was detected 6 months after starting the treatment, after 11 years of treatment, after 14 years of treatment and after 17 years of treatment. The patients who dropped out were contacted by phone to check whether they had developed breast cancer.
All cancers were infiltrating ductal carcinoma. The disease was detected in the early stages and all the patients are currently alive and disease-free.
The incidence in our study is significantly lower than in the general population.
If we bear in mind the biology of breast cancer from the moment of the first malign cell to the presence of a 0.5 cm tumor, the incidence in our study would have been even lower because we only had one case of breast cancer in the first 5 years.
PS-05
BREAST CANCER RISK FACTORS AND URINARY LEVELS OF ESTROGEN HYDROXYMETABOLITES IN RUSSIAN POSTMENOPAUSAL WOMEN
V. N. Konovalova and V. P. Smetnik
Research Center for Obstetrics, Gynecology and Perinatology, Moscow, Russia
Objective: It has been suggested that women, who metabolize endogenous estrogens predominantly via 16α-hydroxylation rather than via 2-hydroxylation with low 2/16α ratio are at an increased risk of breast cancer. But ethnic differences of breast cancer incidence and prevalence of estrogen metabolic pathways are discussed. The majority of studies were held in USA, there are no accessible results from Russian population. Data of relationship with breast cancer risk factors are also lacking. That's why we examined the mentioned above correlation in healthy postmenopausal Russian women.
Design and Method: Estrogen metabolites were measured by ESTRAMET 2/16α in urine samples obtained from 60 white postmenopausal women aged 45–64 (mean 52,6 ± 4,6 years) with no history of breast cancer and not using hormone replacement therapy at least for 3 months. We gathered information about breast cancer risk factors and also calculated Gail index: women in our trial were representatives of low risk group – mean Gail index was 1,2.
Results: The mean value of 2-hydroxyestrone (2-OHE1) in urine was 10,6 ± 6,1 ng/ mg, 16α-hydroxyestrone (16α-OHE1) – 5,9 ± 6,6, 2/16α ratio – 2,4 ± 1,5. In 7 (11,7%) women 2/16α ratio was below 1, in 20 (33,3%) – from 1 to 2, in 33 (55,0%) – above 2.
Evaluating association between levels of estrogen metabolites and breast cancer risk factors we found no relationship with age, family history of breast cancer, body mass index, age at menarche and menopause. But we found correlation with pregnancy (for 2-ОНЕ1 r = 0.257, p < 0,05), age at first birth (for 2-ОНЕ1 r = −0.413, p < 0,01, for 16α-ОНЕ1 r = −0.367, p < 0,05), especially after 30 years (r = −0.303, p < 0,05 and r = −0.277, p < 0,05, respectively), and sterility (r = −0.439, p < 0,01 and r = −0.268, p < 0,05, respectively). No association with 2/16α ratio was observed.
No relationship with mammographic density was observed, excluding negative correlation of 2/16α ratio and P2 Wolfe mammographic pattern (r = −0.276, p < 0,05).
Conclusion: Estrogen metabolites levels and their ratio can be used in complex assessment of breast cancer risk, including risk factors evaluation and mammographic density.
PS-06
BREAST CELL PROLIFERATION DURING MIFEPRISTONE TREATMENT EVALUATED BY FINE NEEDLE ASPIRATION CYTOLOGY
M. Engman, L. Skoog, G. Söderqvist and K. Gemzell-Danielsson
Karolinska University Hospital, Stockholm, Sweden
Background: Progestins are used during hormone therapy to block estrogen dependent endometrial proliferation. Progestins as well as estrogen have a role in the development of breast cancer. Here the effect of mifepristone on cell proliferation in human breast tissue in vivo was studied.
Methods: Thirty menstruating women, scheduled for surgical treatment of leiomyomas, were randomized to either 50 mg mifepristone or placebo every other day, for 12 weeks. Fine needle aspiration biopsies were obtained at baseline and after 12 weeks. Immunocytochemical analysis of Ki-67 was performed to assess breast epithelial cell proliferation.
Results: The proportion of Ki-67, MIB-1 positive cells was significantly reduced during mifepristone treatment. Breast symptoms like soreness and swelling was reduced in the treatment group.
Conclusion: Mifepristone seems to reduce breast epithelial cell proliferation. This may be beneficial when used for HT. Our results implicate a possible protective effect of mifepristone on the normal breast epithelium.
PS-07
BREAST CONSERVING SURGERY IN POSTMENOPAUSAL BREAST CARCINOMAS
B. Sancho Perez, M. Gallego Guerrero, M. R. Noguero Meseguer, M. Gallego Alvarez, M. C. Sanz Ferrandez, L. Yago Lisbona, I. Herraiz Garcia and J. M. Hernandez Garcia
Hospital 12 de Octubre, Madrid, Spain
Background: Breast conserving surgery (BCS) has become a common surgical approach and many times, when given a choice, the elderly are likely to choose this option.
Material and Methods: We retrospectively analysed surgery of breast carcinomas (years 2003–2006) in 191 premenopausal women (29%) and compared them with those of 468 postmenopausal patients, dividing postmenopausal women into 4 groups: 13,5% early (≤5 years from menopause), 20,1% medium (6–15 years), 25,8% late (16–25 years) and 11,7% elderly group (>25 years) post menopause.
Results: Mammographic wire-guided biopsy (MWGB) was more frequent (p = 0,03) in postmenopausal women (42,1%) than in premenopausal ones (33%), and in the group of early postmenopause this proceeding was (p < 0,0001) the most frequent (56,2%), and in the elderly group was the least (16,9%). In ductal carcinoma in situ BCS rate was similar (p = 0,3) in the group of premenopausal women (69%) and in postmenopausal ones (60,1%) as a unique group, although in the latest all of the elderly (3 patients) had BCS. In invasive carcinomas, BCS rate was smaller (p = 0,003) in the group of premenopausal women (49,7%) than in postmenopausal ones (60,1%), and in the latest, is was in the elderly in which BCS was greater (78,9%) than in the others (p = 0,004). One unique surgery (84,5%) was more frequent (no re-excision) in the elderly group than in the other 4 groups (p = 0,001). In invasive carcinomas 94,9% of premenopausal women underwent axillary lymph node dissection (ALND) but only 71,8% of postmenopausal group (p < 0,0001). In postmenopausal women it was in the group of between16 and 25 years (73,8%) and in the elderly (18,3%) in whom ALND was less common (p < 0.0001).
Discussion: MWGB was more frequent in postmenopausal women until 15 years postmenopause, because of mamographic screening range of age between 50 and 69 years. 80% of women with >25 years from menopause underwent BCS, with no differences between the other groups. No single approach for management of postmenopausal women fits all, specially the elderly group. Candidates for BCS include most patients with smaller tumors or those which despite having greater lumps have severe co-morbities or functional deficits. In these, lumpectomy alone can offer a less aggressive option of surgery. When axillary evaluation is necessary (with a clinically negative node status) a good choice in the groups of late postmenopausal patients or elderly group, could be sentinel node biopsy (much lesser arm dysfunction especially in this groups of age).
PS-08
COMPARATIVE ACTIONS OF PROGESTERONE, MEDROXYPROGESTERONE ACETATE, DROSPIRENONE AND NESTORONE ON BREAST CANCER CELL MIGRATION AND INVASION
Maria Silvia Giretti, Xiao-Dong Fu, Lorenzo Goglia, Marina Flamini, Angel Matias Sanchez, Chiara Baldacci, Silvia Garibaldi, Regine Sitruk-Ware1, Andrea R. Genazzani and Tommaso Simoncini
Molecular and Cellular Gynecological Endocrinology Laboratory (MCGEL); Department of Reproductive Medicine and Child Development, University of Pisa, Italy; 1Population Council and Rockefeller University, New York, USA
Background: The role of progestins used in hormone replacement therapy on breast cancer development is controversial. Little is known on the effects of progestins on breast cancer progression and metastasis and on possible differences between progestins.
Objective: We investigated the effects of progesterone (P), medroxyprogesterone acetate (MPA), drospirenone (DRSP) and nestorone (NES) alone or with 17β-estradiol (E2) on T47-D breast cancer cell migration and invasion and we characterized the signaling steps recruited by these progestins.
Results: Breast cancer cell horizontal migration and invasion of three-dimensional matrices are enhanced by all the investigated progestins, but differences are found in terms of potency, with MPA being most active and DRSP being markedly less active. This is related to the differential ability of the progestins to activate the actin-binding protein moesin, leading to distinct effects on actin cytoskeleton remodeling and on the formation of cell membrane structures that mediate cell movement. The addition of E2 to any of these progestins enhances moesin activation, actin cytoskeleton remodeling, cell migration and invasion of breast cancer cells over that achieved by each progestin alone.
Conclusions: These results imply that P, MPA, DRSP and NES alone or in combination with E2 enhance the tendency of breast cancer cells to move in the surrounding environment. However, these progestins show different potencies and to some extent use distinct intracellular intermediates to drive moesin activation and actin remodeling. These findings support the concept that each progestin acts differently on breast cancer cells, which may have relevant clinical implications.
PS-09
CLINICAL AND ANATOMO-PATHOLOGIC CHARACTERISTICS OF BREAST CANCER IN PRE AND POSTMENOPAUSAL WOMEN
M. R. Noguero Meseguer, L. Yago Lisbona, M. Blanco Guerrero, M. Gallego Alvarez, M. C. Sanz Ferrandez, B. Sancho Perez, M. L. Arroyo Vozmediano and S. Aragon Sanchez
Hospital “12 de Octubre” Madrid, Spain
Background: The aim of this study was to determine the differences between two groups of premenopausal and postmenopausal patients with breast cancer. The variables analysed were: Methods of breast cancer detection and diagnosis, type of surgery, mean tumour size, stage, histological type, histological grade, axillary lymph affection, post-surgery complications and adjuvant treatment.
Methods: A retrospective study was carried out at the “12 de Octubre” Hospital on 281 patients diagnosed and treated for breast cancer, from 2005 to 2006. Statistical analysis was performed using the SPSS statistical programming software (13.0.)
Results: Thirty-five percent of patients were premenopausal and 64,9% postmenopausal. A palpable mass was the first symptom in both groups (65,9% vs 58,6% in pre and postmenopausal) (ns). The core needle biopsy was the most common method of diagnosis in premenopausal (31,9%) whereas the Rx-guided biopsy was used in the postmenopausal (p < 0,03). We performed a mastectomy in 44,1% of premenopausal and 33,9% of postmenopausal (ns). The mean tumoral size was similar in both groups (2,11 cms in the postmenopausal and 2,07 for the premenopausal) (ns). The Invasive Ductal carcinoma was the most frequent type of tumour in the two groups. The proportion of ductal in situ carcinoma was higher among premenopausal patients: 36,4% vs 15% in postmenopausal (p < 0,03). No statistical differences were found in the number of lymp nodes affected. The frequency of complication postsurgery was low and similar in the two groups. Premenopausal women were more likely to receive adjuvant chemotherapy (p < 0,004).
Conclusions: The Rx-guided biopsy was the most common method of diagnosis in postmenopausal, whereas in premenopausal the core biopsy was used.
More mastectomies were practised in the premenopausal group.
Ductal carcinoma in situ was most frequently diagnosed in the premenopausal group.
Premenopausal women were more likely to receive adjuvant chemotherapy.
PS-10
CLINICAL PRESENTATION OF BREAST CARCINOMAS IN POSTMENOPAUSAL WOMEN
B. Sancho Perez, I. Herraiz García, M. R. Noguero Meseguer, M. C. Sanz Ferrandez, M. Gallego Alvarez, L. Yago Lisbona, M. L. Arroyo Vozmediano and S. Aragón Sánchez
Hospital 12 de Octubre, Madrid, Spain
Background: A breast lump is the most often clinical breast problem that causes women to seek treatment and remains the more common presentation of breast carcinomas. Nevertheless, nowadays screening mammography allows preclinical carcinomas be diagnosed before becoming palpable. We analyzed clinical presentation (whether palpable lump or only mammographic detection) of breast carcinomas in postmenopausal women, in order to know the difference regarding this issue with premenopausal ones.
Design and Method: We retrospectively analysed clinical presentation of breast carcinomas (years 2003–2006) in 191 premenopausal women (29%) and compared it with that of 468 postmenopausal patients, subdividing postmenopausal women into 3 groups: 33,5% early postmenopause (≤15 years from menopause), 25.8% medium (16–25 years) and 11,7% late (>25 years from menopause).
Results: Mammographically detected carcinomas were more frequent (p = 0,03) in postmenopausal patients (42,1%) as a whole group than in premenopausal ones (33%). Within postmenopausal women, it was in the group of early post menopause in which more mammographically detected (p < 0,0001) carcinomas (50,2%) were found, followed by the group of medium postmenopause (42,9%) and only 16,9% of late postmenopausal group were mammographically detected. In situ carcinomas were more frequent (p = 0,002) in the group of early postmenopausal women (19,5%) than in premenopausal or the 2 other groups of postmenopausal ones. There was no difference regarding mean histological size in ductal carcinomas in situ between any of the 4 groups. In invasive carcinomas mean histological size in premenopausal women (19,2 mm ± 10,6) was smaller than mean size (p = 0,008) of the late postmenopausal group, with no difference between none of the other groups. Locally advanced carcinomas were more frequent (p = 0,04) in the latest postmenopausal group (6,9%) than in the other 3 groups.
Conclusion: Because of mammographic screening, mammographically detected carcinomas were more frequent in postmenopausal women, so in this group in situ carcinomas were more frequent (early diagnosis) and this confers a relative better prognosis to these patients.
We found more locally advanced carcinomas in late postmenopausal group.
Older postmenopausal women are likely to benefit from breast cancer screening because their risk of breast carcinoma is higher than that of younger postmenopausal women. But the optimal upper age limit for mammographic screening is still a matter of debate. Because survival for mammographic screening are evident after 5 years of follow-up, cut off should be based on life expectancy individually, because the magnitude of benefit of breast cancer screening decreases with age and morbidity.
PS-11
DUCTAL CARCINOMA IN-SITU: CLINICAL AND HISTOLOGICAL DIFFERENCES ACCORDING TO HORMONAL STATE
M. Carvalho, M. Dias, S. Custódio and C. de Oliveira
Coimbra University Hospitals, Coimbra, Portugal
Objective: Comparison of clinical and histological parameters concerning ductal carcinoma in-situ (DCIS) in pre-menopausal vs. post-menopausal patients, diagnosed and treated in our department.
Design & Method: Analysis of 89 patients with DCIS of the breast.
Results: Patients were pre-menopausal in 42,7% (N = 38) and post-menopausal in 57,3% (N = 51). Mean age in pre-menopausal group was 47 (33–56) and in post-menopausal was 66 (50–92), with mean menopausal age 49 (37–55). In this last group, 23,5% of patients mentioned hormonal replacement therapy. Comparing pre-menopausal vs. post-menopausal patients, 63,2% vs. 90,2% (p = 0,002) had one or more gestations and 75% vs. 69,6% (p = n.s.) were nursing women. Clinical presentation was palpable lesion in 10,5% vs. 15,7% (p = n.s.), radiological alteration in 84,2% vs. 78,4% (p = n.s.), nipple discharge in 2,6% vs. 3,9% (p = n.s.) and Paget disease in 2,6% vs. 1,9% (p = n.s.). Histology revealed, concerning tumor size, 55,3% vs. 47,1% (p = n.s.) measuring 0,1–2 cm, 26,3% vs. 47,1% (p = 0,044) 2,1–5 cm and 15,8% vs. 5,9% (p = n.s.) more than 5 cm. Cytonuclear grade was G1 in 28,9% vs. 29,4% (p = n.s.), G2 in 44,7% vs. 39,2 (p = n.s.) and G3 in 26,3% vs. 31,4% (p = n.s.). Necrosis was present in 44,7% vs. 19,6% (p = 0,011). Multifocal lesions were described in 5,3% vs. 43% (p < 0,001).
Conclusion: Clinical presentation did not reveal significant differences between both groups on what concerns the majority of parameters studied. Concerning histological parameters, tumors measuring 2,1–5 cm were statistically more relevant in post-menopausal women, cytonuclear grade had a similar distribution between both groups. Necrosis was statistically more associated with pre-menopausal DCIS but multifocal lesions more representative in post-menopausal DCIS, reaching statistic significance.
PS-12
EFFECTS OF RALOXIFENE AND ESTROGEN ON BREAST CANCER CELL MIGRATION AND INVASION
Marina Flamini, Angel Matias Sanchez, Silvia Garibaldi, Chiara Baldacci, Maria Silvia Giretti, Xiao-Dong Fu, Lorenzo Goglia, Andrea R. Genazzani and Tommaso Simoncini
Molecular and Cellular Gynecological Endocrinology Laboratory (MCGEL), Department of Reproductive Medicine and Child Development University of Pisa, Italy
Estrogens and SERMs have differential effects on breast cancer cell division and cancer growth, but little is known on the effects on breast cancer cell migration, invasion and metastasis. We used ER-positive human breast cancer cells to study the effects of estrogens or SERMs on cell movement and we characterized the molecular events that mediate these actions. In T47D cells, estradiol (E2) induces a rapid remodeling of cortical actin associated with migration and invasion. These effects are mediated by the activation of the actin-binding protein, moesin. Moesin activation by E2 relies on the recruitment of a cell-membrane estrogen receptor-α (ERα). Activated ERα interacts with Gα13 at the cell membrane, and activates the signaling to RhoA and Rho-associated Kinase 2, that phosphorylates moesin. Raloxifene (RAL) administration to T47D cells is also associated with a weak and transient activation of this pathway. When RAL is used in co-treatment with E2, a strong inhibition of the activation of moesin and of cytoskeletal remodelling are seen, suggesting that this SERM may antagonize breast cancer cell migration induced by E2. Estrogen directs the interaction with the extracellular environment and the movement of T47D cells through the regulation of the assembly of the actin cytoskeleton. RAL alter this signaling of estradiol, which may translate in reduced migration of breast cancer cells in the presence of estrogens. These findings increase our understanding of breast cancer cell biology and may have clinical relevance for the development of new therapeutic strategies for the prevention or control of breast cancer.
PS-13
EFFECT OF LOW-DOSE HORMONE THERAPY WITH NORGESTIMATE IN MAMMOGRAMS FROM POSTMENOPAUSAL WOMEN OF A NORTHEASTERN MUNICIPALITY FROM BRAZIL
L. M. Brito1, A. M. Silva1, M. B. Chein1, L. G. Brito2 and P. A. Navarro2
1Federal University of Maranhão, São Luís, Brazil; 2Faculty of Medicine of Ribeirão Preto, São Paulo University, Ribeirão Preto, Brazil
Objetives: To assess the effects between non-treatment (placebo group) and a low dosage estrogen-progestin regimen with norgestimate on changes in mammographic density in postmenopausal women after 12 months of hormone therapy.
Design & Method: A prospective study was performed with 40 postmenopausal patients from Materno-Infantil University Hospital (São Luís, Maranhão, Brazil), divided into two groups: A (n = 20) using 1 mg of beta-estradiol (E2) and 1mg of E2 + 90mcg norgestimate (NMG); and B (placebo). Mammographic examinations were done before and after a 12-month period of hormone therapy and breast density between the two exams in each group was compared. Mammographic density was measured by Wolfe classification (1976), subdivided in: N1 – normal; P1 – proeminent ducts occupying <25% breast volume; P2 – proeminent ducts occupying >25% breast volume; DY – dysplasia/high density. BI-RADS classification (2006) was evaluated by two different observers. Data were analysed using Epi-Info program, with statistical significance of 5%. Interobserver variability from mammograms was considered low (kappa = 0.811). T-student test was used for means and chi-square test for binomial variables.
Results: Both groups were considered homogeneous regarding age, body mass index (BMI), parity, menacme and menopause duration, race. BMI did not change during the study period in both groups. The classification of breast density according to Wolfe was, respectively in Groups A and B, N1 = 12, P1 = 5, P2 = 3, DY = 0; and N1 = 11, P1 = 6, P2 = 3, DY = 0 before and after low dose hormone therapy, with no significant differences. A similar pattern was observed at placebo group using Wolfe classification. There were no changes in mammographic density according to BI-RADS category in both groups.
Conclusion: Low dosage hormone therapy with norgestimate was not associated with increased mammographic density after 12 months of treatment, supporting current literature. Larger prospective studies should be performed to confirm this finding. Further studies using devices with better technology in analyzing mammary density are needed to confirm a stability of breast epithelium with different types of low dosage hormone therapy.
PS-14
EFFECT OF TAMOXIFEN ON ENDOMETRIUM IN PRE AND POST MENOPAUSAL WOMAN
N. Kiriakopoulos, C. Gavala, I. Aggos and A. Papadopoulou
Ippocratio General Hospital, Kos, Greece
Objective: Tamoxifen is effective in treating breast cancer, reduces breast cancer incidence among high-risk women, and seems to be associated with increased endometrial cancer risk.
Design & Methods: A retrospective study, from 1995 to 2007, in pre and postmenopausal woman with a history of breast carcinoma was held to determine the effects of treatment with tamoxifen. 26 patients who subsequently developed endometrial cancer were included in our study.
Result: 15 patients received tamoxifen for breast carcinoma and 11 did not. The mean interval between detection of breast and endometrial cancers was 5 years in the tamoxifen group and 11 years in the non treated group. There was no significant difference in the age of the tamoxifen treated and non treated group.
Conclusions: Long-term tamoxifen users have a worse prognosis of endometrial cancers, which seems to be due to less favorable histology and higher stage. However, the benefit of tamoxifen on breast-cancer survival far outweighs the increased mortality from endometrial cancer. The increased risk of endometrial cancer associated with tamoxifen treatment should be considered clinically, for both premenopausal and postmenopausal women during treatment, for at least 5 years after the last treatment.
PS-15
HISTOLOGY AND IMMUNOHISTOCHEMISTRY AS PROGNOSTIC FACTORS IN EARLY, MEDIUM OR LATE POSTMENOPAUSAL PATIENTS WITH BREAST CANCER
B. Sancho Perez, M. Blanco Guerrero, R. Noguero Mesegur, L. Yago Lisbona, M. Gallego Alvarez, C. Sanz Ferrandez, S. Aragon Sanchez and J. M. Hernandez García
Hospital Universitario “12 de Octubre” Madrid, Spain
Background: Breast cancer age-specific incidence profile rises exponentially until menopause and increases more slowly thereafter, reflecting the superimposition of early-onset (mainly inherited or early transforming effects on immature epithelium) and late-onset (mainly exposures to promoting stimuli). We analysed histological and immunohistochemical (IHC) characteristics of breast carcinomas, in order to know if menopausal status, or number of years from menopause, could correlate with any kind of difference between them.
Design and Method: We retrospectively analysed tumoral characteristics (histology and IHC) of breast carcinomas (years 2003–2006) in 191 premenopausal women and compared them with those of 468 postmenopausal patients, dividing postmenopausal women into 3 groups: 13,5% early (5 years or less from menopause), 20% medium (6 to 15 years) and 36,7% late (>15 years) post menopause.
Results: In situ carcinomas were most frequent (p = 0,002) in the group of early postmenopausal women (27%) than in premenopausal or 2 other groups of postmenopausal ones. Mucinous invasive carcinomas were more frequent in the group of late postmenopausal (4.5%) than in premenopausal (1%), early (1,1%) or medium (2.3%) postmenopausal patients (p = 0,002). In early postmenopausal patients, ductal carcinoma in situ (DCIS) (18%) and lobular carcinoma in situ (9%) were more frequent (p = 0,002) than in the 3 groups of pre or postmenopausal women. No other differences were observed regarding histological type. Premenopausal patients had (p = 0,005) a smaller mean size (19,2 ± 10,6 mm) than late postmenopausal ones (21,6 ± 14,1 mm). Locally advanced carcinomas were more frequent (p = 0,04) in the latest postmenopausal group. Bloom-Richardson histological grade I was more frequent (p = 0,01) in early postmenopausal (41,9%) than in premenopausal (19,3%), medium (18,1%) or late (23,4%) postmenopausal women. No differences were observed in histological grades of DCIS. We found no differences between premenopausal or the 3 groups of postmenopausal regarding IHC characteristics (positive hormonal receptor status, positive p53, cerbB2 overexpression or rates of proliferative index (MIB-1) of <20%, 20–30% or >30%).
Conclusion: Our results support that early postmenopausal status confers a relative good prognosis to patients (more DCIS, probably because of mammographic screening in this range of age, and higher rates of histological grades I in invasive ductal carcinomas). Except for this, and that we found more locally advanced carcinomas in late postmenopausal group, we couldn't find any more differences in histology or IHC. According to our results, postmenopausal patients with breast cancer do not have better prognosis than premenopausal ones, as both had similar tumoral biological characteristics.
PS-16
HORMONAL THERAPY: MAMMOGRAPHIC FINDINGS AND RISK OF BREAST CANCER IN ASYMPTOMATIC WOMEN
J. Lamas1, H. Koch2 and S. Paixão3
1Clinica Janice lamas, Brasília, Brazil; 2Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil; 3Senado Federal da República, Brasília, Brazil
Summary-Objective: To evaluate the dependence relationship between hormonal therapy (HT), breast density and time of use according to women's age and to estimate the frequency of breast cancer.
Material and Method: A cross – sectional and prospective study was carried out from December 1993 to July 1996 at a mammography facility in Brazil where 3209 asymptomatic women were scheduled for screening. 543 were in current use of hormone (oestrogens/progestogens) and 2666 were never – users. The mammograghic findings and breast composition were described according the ACR- BI-RADS. The dependence relationship established between density breast and hormone was investigated according to women's age using the qui- square test, 5% of significance and SAS. The logistics regression technique were used in the point analysis of 10 risk factors, including age and HT.
Results: Breast tissue heterogeneously or extremely dense women over 50 years of age and duration of use were associated with HT. P (x2 = 384,42 = 0,00). The categories 4 and 5 BI-RADS, confirmed to the biopsy as cancer, had not relation with hormone (P = 0,20, odds ratio = 1,6; CI 95%: 0,8- 3,3).Breast cancer rate was 8,7 per thousand, most of them, at an early stage.
Conclusion: Considering the evidence of relationship between mammary density and hormonal therapy, the perception of low – density malignant lesions could became decreased in old women, in use of hormonal therapy.
PS-17
IS QUALITY OF LIFE THE GOAL OF TREATMENT IN BREAST CANCER PATIENTS OVER 75 YEARS?
M. C. Sanz Ferrandez, M. R. Noguero Meseguer, M. Gallego Alvarez, M. Blanco Alvarez, L. Yago Balbona, M. L. Arroyo Vozmediano, S. Aragon Sanchez, B. Sancho Perez and J. M. Hernandez Garcia
Hospital 12 Octubre, Madrid, Spain
Background: The incidence of breast cancer increases with age and up to 50% occur in women over 65. The aim of this study was to analyze our existing protocol in two groups of elderly patients, one group made up of patients between 65–75 and the other group over 75. We wanted to see if there were differences in pathology characteristics and treatment options in the two groups.
Methods: This retrospective study was carried on 203 patients over 65 diagnosed with breast cancer and treated at our public teaching hospital between 2003–2006. Chi-square was used to assess the differences between patients between 65–75 and a group of patients over 75. p value 0.05.
Results: The median age was 72.2. Patients aged 65–75 made up 59.6% of the population studied and 37,5% older than 75.
The mean size of the tumor in both groups was 2.2 cm. The reason for consultation was due to microcalifications and non-palpable nodule seen by mammogram in 88% of all cases. The most common method of diagnosis was X-ray guided biopsy (36.6%). Most patients (84.9%) were diagnosed in Stage I-II. Infiltrating ductal carcinoma was the most frequent pathology found. The mean of positives nodes was 3.09 (ns).
Conservative surgery was performed in 60.6% of all cases. The frequency of complication postsurgery was low and similar in the two groups. The 59% underwent radiotherapy (Patients aged 65–75). None of them chemotherapy
Hormone therapy was administered in 81.3%.
Chi square showed that patients over 75 had bigger tumors (p 0.05) with a higher axillary involvement (p 0.007). In the younger group the number of reexcision was more frequent as was lymphadenectomy (p 0.001) and radiotherapy administration (p 0.035). There were no differences in NSs involvement, ER/EP, HER-2 status or percentages of hormone therapy.
Conclusion: In patients over 75 our unit has become more conservative in the past years and since 2005 offer lumpectomies ± sentinel node and hormone therapy and sometimes only hormone therapy in older patients or those with deteriorated health.
Despite the histological an clinical characteristics in the group over 75 were less favourable.
PS-18
LOSS OF LH/HCG RECEPTOR EXPRESSION IN INVASIVE BREAST CANCER TISSUE COMPARED TO PREINVASIVE COMPONENT
G. Pfeiler1, P. Wülfing2, G. Hudelist1, C. F. Singer1 and E. Kubista1
1Medical University of Vienna, Austria; 2University of Münster, Germany
Objective: LH/human chorionic gonadotropin (hCG) receptors are present in a variety of nongonadal tissues including normal breast as well as breast cancer tissue. In vitro studies and animal studies, respectively, have demonstrated that hCG inhibits the initiation and progression of experimental breast carcinoma. According to these observations it seems that LH/hCG recptor could be a target for prevention and therapy of breast carcinoma. We therefore investigated the LH/hCG receptor expression of preinvasive and invasive breast cancer as well as phylloides tumor specimen on tissue microarrays.
Design and Method: Immunocytochemistry was used to analyze 206 preinvasive, 188 invasive breast cancer samples as well as 251 preinvasive specimen with adjacent invasive component. 62 phylloides tumor samples were investigated. A Chi Square test was used to identify differences of LH/hCG protein expression levels.
Results: LH/hCG receptor expression was significantly higher in preinvasive DCIS samples compared to invasive breast carcinomas. No difference of LH/hCG receptor expression could be identified between DCIS and adjacent invasive component, when both components derived from one solid tumor. Phylloides tumors showed significant higher LH/hCG receptor expression compared to invasive breast cancers. Though there was a trend of higher LH/hCG receptor expression in phylloides tumors compared to preinvasive DCIS, this did not reach statistical significance.
Conclusion: Based on our observation that LH/hCG receptor was selectively downregulated in invasive tumor components, we suggest that the loss of LH/hCG receptor favours mammary carcinogenesis.
PS-19
LONG TERM FOLLOW UP OF ACUPUNCTURE AND HORMONE THERAPY ON HOT FLUSHES AND WELL-BEING IN WOMEN WITH BREAST CANCER – A PROSPECTIVE, RANDOMIZED CONTROLLED MULTI CENTRE TRIAL
J. Frisk1,2, S. Carlhäll1, A.-C. Källström2, L. Lindh-Åstrand1, A. Malmström3 and M. Hammar1
1Division of Obstetrics and Gynaecology, Department of Molecular and Clinical Medicine, Faculty of Health Sciences; 2Department of Surgery, County Council Östergötland; 3Department of Oncology, University Hospital of Linköping, Sweden
Objective: Evaluate effects of electro-acupuncture (EA) and hormone therapy (HT) on vasomotor symptoms and wellbeing in women with a history of breast cancer.
Design and Methods: 45 women were randomized to EA (n = 27) for 12 weeks or HT (n = 18) for 24 months. The number of and distress caused by hot flushes were daily registered before, during and up to 24 months after start of treatment. Kupperman's Index (KI) and Psychological and General Wellbeing Index (PGWB) was recorded before, after 3 months of treatment, and at 6, 9, 12, 18 and 24 months after start of treatment. PGWB includes 22 questions, with scores 0–5; total score 110. Wilcoxon signed rank test was used for changes over time within groups, and ANOVA between groups and within groups over time.
Results: 19 women completed 12 weeks of EA, and the median number of hot flushes/24h decreased from 9.6 (interquartile range (IQR) 6.6–9.9) at baseline to 4.3 (IQR 1.0–7.1) at 12 weeks of treatment (p < 0.001). At 12 months after start of treatment, 14 women with only the initial 12 weeks of EA had a median number of flushes/24 h of 4.9 (IQR 1.8–7.3), and at 24 months seven women with no other treatment than EA had 2.1 (IQR 1.6–2.8) flushes/24h. Another five women had decreased flushes by having additional EA. KI went from a median score of 24(IQR19–29; n = 26) to 12(IQR 9–17; n = 19) after 12 weeks of treatment (p < 0.001), and was 13(IQR 10–17; n = 14) at 12 months after start of treatment (p = 0.002). Median PGWB changed from 78(IQR 53–89; n = 26) at baseline to 79(IQR 68–93; n = 19) after 12 weeks of treatment (p = 0.002), and to 85(IQR 74–95; n = 14; p = 0.028) 12 months after start of treatment. Eighteen women with HT had a baseline median number of flushes/24 h of 6.6(IQR:4.0–8.9), and 0.0(IQR:0.0–1.6; p = 0.001) at 12 weeks. KI went from a median score of 23(IQR 15–28; n = 18) to 6(IQR 3–9; n = 18) after 12 weeks of treatment (p < 0.001), and to 6(IQR 2–8; n = 17) at 12 months after start of treatment (p = 0.001). Their median PGWB changed from 75(IQR 59–88; n = 18) at baseline to 90(IQR 62–97; n = 18) after 12 weeks of treatment (p = 0.102), and to 93(IQR 86–97; n = 17; p = 0.008) 12 months after start of treatment.
Conclusion: Electro-acupuncture is a possible treatment of vasomotor symptoms for women with breast cancer. Although the reduction of hot flushes is stronger with HT than EA, the increase in wellbeing is similar after EA as during HT. Acupuncture should be further studied for this group of women.
PS-20
MAMMOGRAPHIC BREAST DENSITY EVALUATION AFTER ONE YEAR SOY EXTRACT TREATMENT
B. Pornel1, Gh. Lemaur1, S. Rovenne2, V. Pellichero1, S. Palacios3, F. Vazquez4, P. Chantre5, L. Aubert5 and P. Mares6
1Brussels Menopause Center, Brussels, Belgium; 2EPIsearch, Brussels, Belgium; 3Instituto Palacios, Madrid, Spain; 4Clinica de Ginecologia, Lugo, Spain; 5Arkopharma, Carros, France; 6Hôpital Caremeau, Nîmes, France
Objective: To analyse the breast density evolution of patients treated with an isoflavone extract during 12 months.
Design & Method: Post menopausal women 45–65 years old were included in an international open study whose secondary objective was to assess breast safety after an one-year daily treatment of 70 mg soy extract (35 mg daidzin, 21 mg glycitin and 14 mg genistin).
Breast density of patients was first estimated with the four BI-RADS density categories.
We developed a computer-aided mammographic density estimation software allowing to calculate precisely the percentage of dense tissue. Breast density analysis was performed on digitized mammograms using the same film scanner. All the breast images were blinded and randomly displayed to the operator. The total breast area was delimited by the radiologist whereas the dense area were determined using an assisted computerized method based in grey scale threshold.
Results: 175 bilateral mammographies have been collected from the 3 largest centres of the study. They have been classified according to BI-RADS density categories. An increase between T0 and T12 months was observed in only 6 breast whereas a classification decrease was noticed in 13 breasts. No increase from Type 2 to 3, nor type 3 to 4 has been recorded.
Using our computer-assisted method, we didn't observe any significant modification in density percentage after 12 months of treatment.
Conclusion: No significant change in breast density has been observed after 1 year of treatment, suggesting that intake of our specific and standardized soy extract doesn't increase the risk to develop breast cancer. However, these results are to be confirmed with patients who have accepted to be treated for 3 years.
PS-21
MEMBRANE-INITIATED EFFECTS OF PROGESTERONE ON PROLIFERATION AND ACTIVATION OF VEGF GENE EXPRESSION IN HUMAN BREAST CANCER CELLS
Gordian Adam, Tanja Fehm, Harald Seeger, Hans Neubauer and Alfred O. Mueck
Department of Obstetrics and Gynecology, University of Tuebingen, Germany
Objective: Progesterone influences mammary gland development and probably breast cancer tumorigenesis and functions by regulating a broad spectrum of physiological processes. We investigated receptor membrane-initiated actions of progesterone in MCF-7 breast cancer cells via progesterone receptor membrane component 1 (PGRMC1).
Design & Method: For verification of PGRMC1 expression in breast cancer paraffin sections were labelled with PGRMC1-specific antiserum. For functional analysis MCF-7 cells were transfected with PGRMC1 (MCF-7-PGRMC1) cloned into pCDNA3 expression vector and stimulated with a membrane-impermeable progesterone: BSA:fluorescein-isothiocyanate conjugate (P4:BSA-FITC) or unconjugated progesterone (P4) in the presence or absence of RU486. Effects on cell proliferation were determined by measuring the intracellular ATP content and by employing the MTT assay over a time period of seven days. Additionally, a dose-dependent action of P4:BSA-FITC was analyzed on day 4. Expression of vascular endothelial growth factor A (VEGF-A) was determined with qRT-PCR.
Results: Immune fluorescent analysis indicated a perinuclear distribution of PGRMC1 in breast cancer cells. MCF-7-PGRMC1 cells show an increased proliferation of approximately 35% after seven days of incubation with P4:BSA-FITC (10–6 M) compared to MCF-7 control cells. This effect can be observed in both ATP and MTT assay and cannot be blocked by co-inbubation with the progesterone receptor blocker RU486 (10–6 M). Incubation with P4 (10–6 M) reduced proliferation of MCF-7-PGRMC1 cells by approximately 10% compared to untreated controls. The proliferative effect of P4:BSA-FITC on MCF-7-PGRMC1 cells peaks at a concentration of 10-6 M, higher concentrations act antiproliferative. In MCF-7 cells transfected with a PGRMC1-mutant the proliferative action of P4:BSA-FITC is abolished. Induction by P4:BSA-FITC led to a roughly 3-fold activation of VEGF-A gene expression compared to MCF-7 cells. Incubation with BSA alone did not have any effect.
Conclusion: Our data indicate that PGRMC1 is expressed in breast cancer cells and is mediating an RU486-independent proliferative signal. It might also contribute to VEGF induced neovascularization in tumor tissue. Thus screening might be of interest to identify women who show a higher expression of PGRMC1 than normal women and who might thus be susceptible for breast cancer development under HRT. The data presented are very important in terms of the positive results of progesterone and breast cancer risk in clinical studies so far. Of further interest is if synthetic progestins that are used for HRT are different in their stimulation of PGRMC1.
PS-22
NEW TECHNOLOGIES FOR BREAST CANCER PREVENTION AT THE LEVEL OF PRIMARY HEALTH CARE: PRIMARY AND SECONDARY PREVENTION APPROACHES IN OUTPATIENT WAITING ROOMS
R. L. Oliveira1, E. F. Tambellini2, D. D. Kim3, L. F. Otsuka Junior3, J. S. Takashima3, R. A. Gamboa3 and R. Kimura3
1Depto.Medicina Social Faculdade De Ciências Médicas Irmandade Santa Casa Miseric, Brazil; 2Centro de Saúde Escola Barra Funda “Alexandre Vranjac” Irmandade Santa Casa Misericórdia de São Paulo, Brazil; 3Faculdade de Ciências Médicas Irmandade Santa Casa de São Paulo, Brazil
Introduction: Breast cancer prevention is one of the main objectives of public health programs in view of the growing incidence and high mortality rates related to the disease. Despite the progress made in the diagnosis and treatment 70% of breast cancer related deaths occur in poor or developing countries such as Brazil. Secondary prevention through self examination, clinical examination and mammography is publicized and made available in public health services. However, this has not contributed satisfactorily to a decrease in the incidence of the disease since it does not affect the factors that contribute to the onset of the disease. Primary prevention has not been taken into account.
Objectives: Devising a strategy for primary breast cancer prevention at the level of primary health care in public units and disseminating secondary prevention.
Methodology: A primary breast cancer prevention educational campaign was organized for the outpatients in the waiting rooms of a Health Centre located in the central metropolitan region of the City of São Paulo, Brazil. The intervention consisted of an interactive questionnaire, an informational talk and an open discussion about the theme, followed by a qualitative and quantative data analysis.
Results: The approach proposed resulted in a qualitative and quantitative improvement of the outpatients understanding about the themes discussed, a good interaction and the creation of knowledge multiplying agents.
Conclusion: There is a niche for primary breast cancer prevention on primary health care units, and the waiting rooms technology is compatible and conducive to the objectives proposed.
PS-23
SEVERITY OF SLEEP DISTURBANCES IN LONG-TERM BREAST CANCER SURVIVORS
J. L. Elam, J. S. Carpenter, K. M. Russell, and V. C. Champion
Indiana University, Indianapolis, Indiana USA
Objective: Breast cancer accounts for 22% of female cancers worldwide. Of those diagnosed with Stages I-III, 85–100% of those women survive at least 5 years. The number of breast cancer survivors (BCS) is projected to increase each year. Current evidence suggests that a significant proportion of BCS suffer from poor sleep quality. Researchers have found that 48–90% of BCS report poor sleep based on cut-off scores from the Pittsburgh Sleep Quality Index (PSQI) questionnaire. However, it is unclear what factors contribute to the severity of poor sleep in long-term survivors. It is also unclear if these factors are similar or different compared to women without cancer. Therefore, this research examined factors that contribute to the severity of poor sleep in American BCS compared to age-matched women without breast cancer (WWBC).
Design & Method: Analysis of cross-sectional data included descriptive and frequency statistics to describe sample characteristics and global sleep scores on the Pittsburgh Sleep Quality Index (PSQI). Multiple regression was used to determine factors contributing to poor sleep.
Results: The sample consisted of 246 BCS and 246 age-matched WWBC who were a mean age of 48 years old (SD = 8.50), Caucasian (70%), employed (69%), married or partnered (76%), postmenopausal (59%), with a college education (56%), and with at least one concurrent medical problem (95%). BCS women were not taking endocrine therapy (67%) and were a mean of 5.62 years post-treatment (SD = 2.03). Results showed that BCS had poorer sleep quality (M = 7.31, SD 3.80) compared to WWBC (M = 5.80, SD = 3.45). Those with poorest sleep quality were BCS, with a high number of co-morbid conditions, hot flashes, presence of symptoms related to cancer, and high levels of depressive symptoms. Interestingly, menopausal status, age, socioeconomic factors, level of physical functioning, disease and treatment factors, side effects of cancer, worry about recurrence, impact of a breast cancer, having a bed partner, and having children in the home did not predict severity of sleep disturbances in BCS.
Conclusion: Poor sleep quality is more prevalent in long-term BCS compared to age-matched WWBC. Knowledge of contributing factors provides useful information during clinical evaluations and treatment of BCS reporting poor sleep. Additional research is needed to determine the impact of poor sleep on quality of life and develop/test effective interventions for long-term BCS.
PS-24
STUDY ON THE DEVELOPMENT OF BREAST CANCER DURING POSTMENOPAUSAL HORMONE THERAPY IN KOREA
Jae-Yen Song1, Jeong-Min Moon1, Jae-Eun Jung2, Yong-Taik Lim1, Jin-Hong Kim1 and Mee-Ran Kim1
1Catholic university of Korea, Seoul, Korea; 2Wonkwang university, Korea
Objective: The objective of this study was to investigate clinocopathologic characteristics of postmenopausal patients with breast cancer arising during postmenopausal hormone therapy.
Design & Method: The study included 29 patients diagnosed with breast cancer during postmenopausal hormone therapy (HT group) and 285 patients diagnosed with breast cancer during menopause who did not receive hormone therapy (non-HT group). The data were reviewed for the size of tumor, the presence of metastasis in lymph nodes, the presence of estrogen receptor, the stage at the time of diagnosis, the method of treatment, the means of operation, the recurrence rate, and the mortality rate. The unpaired T test, chi-square and log rank test were done by using SAS (version 8.02). The 5 – year survival analysis and additive survival rate were measured by Kaplan-Meier method. All P values that are less than 0.05 (P<0.05) are considered statistically significant.
Results: HT group had a smaller size of tumor than non-HT group (P = 0.0032). T1 in TNM staging was 55% in HT group and 28% in non-HT group. The rate of well differentiation was 53% in HT group and 13% in non-HT group (P = 0.0026). There were no differences in the rate of estrogen receptor expression, lymph node metastasis and recurrence among HT regimens. 5-year survival rate was 100% in HT group and 87% in non-HT group (P < 0.001).
Conclusion: Breast cancer developed during a hormone therapy had a higher rate of well differentiation, smaller tumor and a higher 5-year survival rate than that developed without therapy.
PS-25
IMMUNOHISTOCHEMICAL AND MORPHOMETRIC ANALYSIS OF THE TGF-B AND P27 PROTEINS IN POLYPS AND ADJACENT ENDOMETRIUM ON POSTMENOPAUSAL WOMEN USERS OF TAMOXIFEN
S. M. R. R. Lima, S. R. Botogoski, M. A. L. Galvão, B. F. Reis, P. A. A. G. Ribeiro and T. Aoki
School of Medical Sciences of the Santa Casa de São Paulo, São Paulo, Brazil
Objective: Tamoxifen (TMX) spread freely in the cell and connecting to the hydroxilate metabolic estrogen in endometrial tissue while increasing the occurrence of polyp proliferation. The beginning phase of the cellular cycle is undergoes a higher influence of extra-cellular factors and related to proteins. To verify and compare the role of the TGF-β and p27 proteins in the endometrial polyps and adjacent endometrium in postmenopausal users of tamoxifen.
Design & Method: A prospective study was carried out with 30 postmenopausal women treated for breast cancer, users of tamoxifen, with a suspect diagnostic of endometrial polyp in transvaginal ultrasonography and hysteroscopy surgery and hystopathological study, from April 2005 to May 2007. A comparative immunohistochemical and morphometric study on the immunoreactivity of the TGF-β and p27 proteins in polyps and in the adjacent endometrium was also carried out. The study was approved by the Ethics Committee on Research.
Results: The average age was 61.7 ± 9.2 years, age of the menopause 49.5 ± 4.5 years. The average endometrium thickness was 15.6 ± 8.1 mm and the endometrial ecotexture 30 (100%) were heterogeneous. The polyps were removed by diagnostic hysteroscopy and surgery: 9 (30%) was in uterine bottom; 9 (30%) posterior wall; 6 (20%) anterior wall and 6 (20%) on the right side wall. The adjacent endometrium: 26 (86.6%) was low risk hyperplasia and 4 (13.4%) was high risk hyperplasia. The average concentration of TGF-β protein immunocolored in the glandular epithelium polyp and stroma was 62.63 ± 4.57 cells/mm2 and in glandular adjacent endometrium and stroma was 62.10 ± 12.01 cell/mm2. For the p27 protein in the glandular epithelium polyp the range was 24.27 ± 18.67 cell/mm2 and stroma 19.23 ± 15.22 cell/mm2. In the adjacent endometrium the glandular epithelium range was 17.73 ± 18.46 cell/mm2 and stroma 13.60 ± 14.34 cell/mm2.
Conclusion: We have verified that there was no significant statistical difference of the TGF-β and p27 proteins in the polyp glandular epithelium and in the adjacent endometrium. We also verified and there was no significant difference when we compared the stroma of the polyp and of the adjacent endometrium. When comparing the glandular epithelium and the stroma in the polyp and the glandular epithelium and the stroma in the adjacent endometrium, we found that there was a significant higher occurrence of the p27 protein in the glandular epithelium.
PS-26
TRANSVAGINAL SONOGRAPHY IN POSTMENOPAUSAL BREAST CANCER PATIENTS RECEIVING TAMOXIFEN
M. Onofriescu, D. Nemescu, M. Tirnoveanu and A. Luca
University of Medicine IASI, Romania
Objective: This retrospective study was conducted in university-affiliated hospital to examine the histopathologic changes in asymptomatic tamoxifen-treated postmenopausal breast cancer patients with transvaginal ultrasonography.
Methods: The endometrium of 200 gynecological asymptomatic postmenopausal patients was examined. 100 had been treated with tamoxifen (20 mg of tamoxifen daily) for twelve up to sixthy months and 100 had not received any hormonal treatment. All the patients underwent transvaginal ultrasonography (Voluson 530 Kretz Technik – Austria), followed by histeroscopy and dilation and curettage if endometrium is more 5 mm. Endometrial histopathologic findings were examined. The two groups were similar in age, parity, age at menopause, and body mass index.
Results: Compared with the control subjects, the tamoxifen patients had a thicker endometrium (11.4 ± 4.5 mm versus 4.5 ± 3.1 mm) and larger uterine volume (65 ± 32 versus 37 ± 12 cm3), and more uterine fluid (12% versus 2%; P = 0.005). Furthermore, an ultrasonographic suspect ‘Swiss-cheese’ endometrial pattern was noted in almost a quarter of the patients treated with tamoxifen, but this was clearly not associated with intracavitary pathology. Endometrial polyps were more frequent in the tamoxifen group (36 versus 10%; P = .004), which included two patient with atypical hyperplasia, two with adenomatous hyperplasia, and two with endometrial adenocarcinoma with myometrial invasion, one of which was poorly-differentiated. One case control had endometrial adenocarcinoma.
Conclusion: The results provide evidence for an estrogenic effect of long-term tamoxifen treatment on the postmenopausal uterus and show it to be associated with an increased occurrence of polyps. The isolated use of transvaginal ultrasonography is insufficient for screening the endometrium of these women. Women receiving tamoxifen, especially those who are asymptomatic, should be closely monitored by transvaginal sonography and hysteroscopy to detect endometrial pathologies. In asymptomatic postmenopausal women receiving tamoxifen, 5 mm is the optimal endometrial thickness cutoff for diagnosing endometrial abnormalities with transvaginal ultrasonography. Tamoxifen promotes endometrial growth and endometrial polyps may be an important intermediate step in endometrial carcinogenesis.
PS-27
COMPARISON OF SERUM 17β-ESTERADIOL LEVELS AND THE RELATIONSHIP WITH SOME BREAST CANCER RISK FACTORS IN ATHLETIC AND NON ATHLETIC POSTMENOPAUSAL WOMEN
B. Tartibian1 and A. Zarneshan2
1Urmia University, Urmieh, Iran; 2Tarbiatmoalemazarbiajan university, Tabriz, Iran
Objective: The aim of this study was to investigate the comparison of serum 17β-estradiol (breast cancer biomarker) levels and that relationship with some breast cancer risk factors in athletic and non athletic postmenopausal women.
Design & Method: nineteen athletes (body building) aged 53/57 ± 7/87 yr and twenty two non-athletes aged 56/61 ± 5/17 years postmenopausal women in uremia participated in this study. 17βestradiol concentrations were measured by electrochemiluminescence. All participants completed a questionnaire witch included details of age, menarche age, menopause age, pregnant age, null parity, family history, alcohol consumption and smoking. Body fat percent and body mass index measured by body logic/body fat and lyzer (Omron model). Variations in means were compared using independent t test and relationship between variables using Pierson correlation coefficient.
Results: Athletic women had lower serum estradiol concentration, BMI and waist to hip ratio than non-athletic women. But this difference was not significant (p < 0/05) and only body fat percent difference was significant (p = 0/044). There was no relationship between weight, age, body fat percent, waist to hip ratio, BMI and serum concentration of estradiol in subjects. Average age, early menses, late onset of menopause, pregnancy, alcohol consumption and smoking risk factors in athletic women were lower than non athletic womens.
Conclusion: This study showed that low body fat percent and estradiol exposure, late menarche and early menopause in athletic women can indicate low breast cancer risk, but non significant difference in serum estradiol between athletic and non athletic women can be result of irregular intensity and duration of athletic women's exercises.
PS-28
THE EFFECT OF SELECTIVE AEROBIC EXERCISE ON 17β-ESTERADIOL (BREAST CANCER BIOMARKER) AND OBESITY IN POSTMENOPAUSAL WOMEN
B. Tartibian1 and A. Zarneshan1,2
1,2Urmia University, Urmieh, Iran
Objective: Elevated circulating estrogens, especially estradiol and a sedentary lifestyle increase the risk of breast cancer. The purpose of the present research is to examine the effect of selective aerobic exercise with moderate intensity on serum 17β-estradiol and changes of obesity measures in postmenopausal women.
Design & Method: Thirty two sedentary, postmenopausal women with the age of 54 ± 7 years, height 158 ± 7 (cm) and weight 73 ± 8 (kg) participated in this study as subjects and then they were divided randomly in to experimental (n = 17) and control (n = 15) groups.
Serum 17β-estradiol with Electrochemiluminescence, body mass index (BMI), percent body fat (PBF) and waist to hip ratio (w: h) were once measured at baseline and then they were measured after ten weeks of selective aerobic exercise (60–70%max heart rate). Variations of characteristics in each group were done by t-test (dependent) after 10 weeks and variation between dm (differences means) of characteristics exercise and control group were compared by t-test (independent) and the effect of body mass index, percent body fat and waist to hip ratio at 17β-estradiol concentration changes were examined by two recreations.
Results: There was significant decrease of selective exercise on 17β-estradiol concentration (p = 0/038) and BMI (p = 0/004). There were statistically significant differences between exercise and control differences meant in BMI and 17β-estradiol changes from base line to 10 weeks of selective exercise(p < 0/05). There were no significant effect of BMI and %BF and W: h changes on 17β-estradiol changes from baseline in 10 weeks.
Conclusion: Selective aerobic exercise with moderate intensity, independent of obesity, decreases 17β- estradiol concentration in the serum of postmenopausal women. That it can be considered as a factor in preventing the occurrence of breast cancer in women.
PS-29
WHAT IS OUR EXPERIENCE IN POST-MENOPAUSAL PATIENTS WITH BREAST CANCER UNDERGOING SENTINEL NODE BIOPSY IN OUR HOSPITAL?
M. Blanco Guerrero, M. R. Noguero Meseguer, M. C. Sanz Ferrandez, M. Gallego Alvarez, E. Gomez Montes, P. Manosalvas Martinez, A. Izquierdo Rodriguez and J. M. Hernandez Garcia
12 Octubre Hospital, Madrid, Spain
Background: The incidence of breast cancer increases with age and up to 50% occur in women over 65. They show associated morbidity, shorter life expectancy and more favourable biological characteristics. The optimal choice is a less aggressive surgery. The aim of this study was to evaluate the age and menopausal state in the two cohorts of patients.
Material and Methods: A prospective study was carried out on two cohorts of patients diagnosed with breast cancer in the “12 de Octubre” hospital from april 2006 to may 2007. The first group of 62 patients underwent a sentinel node biopsy (SNB), and in the second one of 57 patients a complete axillary dissection (AD) was performed. Statistical analysis was carried out with SPSS 13.0.
Results: Mean age at diagnosis was 61.8 years (Range 30.7–81) in the SNB group and 54 (Range 33–82.3) in the AD group (p < 0.006).
Stratified analysis showed that elderly patients were more likely to undergo a SNB (55.4% above 65 years old) while the age of the AD group was lower (44.1% between 35–50 years old, 28.6% between 50–65 years old.
Menopause was more frequently present in the SNB patients (72.4% vs 47.4%). (p = 0.006).
Hormone therapy was administrated to all patients with oestrogen receptor positive. Pre-Menopausal women were treated with tamoxifen and the first choice for post-menopausal ones was aromatase inhibitors.
Conservative surgery was performed on 83.9% of patients in the SNB group. Radical surgery was carried out on 42.1% of patients of the AD group. (p < 0.002)
Axillary disease present in 12.1% of SNB patients vs 38.6% of AD patients. (p < 0.0001).
Post-surgery chemotherapy was more frequently applied to AD patients (66.1% vs 45.7%). (p = 0.038) In contrast, post-surgery radiotherapy was more common in the SNB group (93.5% vs 77.4%). (p = 0.026).
Cerb-2 was more frequently present in the AD group (75.9% vs 48.1%). (p = 0.037).
Histological type, grade and immunohistochemical study were independent from the axillary surgery.
Conclusion: In our hospital the profile of patients undergoing sentinel node biopsy is characterised by elderly patients, post-menopausal and asymptomatic. The disease is usually a casual diagnosis from mammographic screening confirmed by Rx-guide biopsy. Conservative surgery with additional radiotherapy has been the most common treatment with less axillary disease. This treatment is less aggressive and provides them with more quality of life.
Quality of life
PS-30
AEROBIC EXERCISES CAN IMPROVE QUALITY OF LIFE IN POSTMENOPAUSAL WOMEN REGARDLESS OF ESTROGEN THERAPY: A RANDOMIZED PLACEBO CONTROLLED TRIAL
C. Moriyama, A. Fonseca, B. Oneda, F. Bernardo Cardoso Jr Forjaz, S. Abrahao, D. Mion Jr and T. Tinucci
University of São Paulo. Brazil
Objective: This study was designed to evaluate the isolated and associated effects of moderate aerobic exercises (3h/week) and estrogen therapy (estradiol valerate 1 mg orally/day) on quality of life among previously sedentary postmenopausal women who had undergone hysterectomy.
Design and Methods: It was a six-months, randomized, double-blind, placebo-controlled clinical trial with 44 postmenopausal women (52.0 + 4.0 years) who had undergone hysterectomy. The controlled interventions were: physical exercise and hormone therapy (PEHT, n = 9); sedentary and hormone therapy (SEDHT, n = 14); physical exercise and placebo (PEPLA; n = 11), sedentary and placebo (SEDPLA, n = 10). Quality of life (QOL) was assessed at baseline and after six months by a Brazilian version of World Health Organization Quality of Life -WHOQOL-BREF. The WHOQOL-BREF is a twenty-six items questionnaire that measures four different domains: physical, psychological, social relationship and environment. Menopausal symptoms were recorded during an interview using a Kupperman index.
Results: After six months there was a decrease of symptoms in all groups, but only groups which performed physical exercises showed increases in QOL. ANOVA showed that changes in physical domain (P = 0,013), psychological domain (P < 0,001), and social relationship (P = 0,028) scores over the six months period differed significantly between exercisers and sedentaries, regardless of hormone therapy. There were no effects of hormone therapy, and no significant association between physical exercise and hormone therapy in QOL.
Conclusions: Physical exercises can reduce menopausal symptoms and enhance QOL, independently of taking or not hormone therapy.
PS-31
ASSESSING HEALTH RELATED QUALITY OF LIFE WITH TIBOLONE IN SURGICALLY MENOPAUSAL WOMEN WITH MENOPAUSE RATING SCALE
Gulshan Ara
Dept of obstetrics and gynaecology, Shaheed Ziaur Rahman Medical College, Bogra, Bangladesh
Objectives: To assess the change in HRQL with Tibolone in surgically menopausal women.
Design & Method: One hundred and two women had surgical menopause with known preoperative psychological status were advised to take Tibolone 2.5 mg daily to control menopausal symptoms. MRS was used to assess the change three month,six month and twelve month. At first visit scoring was done by woman herself and then accordingly.
Results: Eighty women were returned for followup after three months with significant improvment of somatovegetative and psychological and urogenital component change was not significant. At six month psychological component improved significantly than urogenital component. At twelve month 10 women were not returned and somatovegetative and psychological component were in significant improved status than urogenital component in returned 70 cases.
Conclusion: Tibolone only is effective for rapid improvement of somatovegetative component but slow for psychological and urogenital component.
PS-32
ASSESSMENT OF KUPPERMAN AND YESAVAGE INDEXES IN CLIMATERIC WOMEN AFTER THE USE OF CONJUGATED EQUINE STROGEN, ISOFLAVONE AND PLACEBO
A. C. Accorsio1, S. C. Cury2, R. M. Mirandola2, G. Y. Ishisaki2, G. A. Barbosa2, M. M. Takagi2 and G. S. Accorsi3
1Prof. Doctor at Padre Albino Foundation, Medicine Faculty, Catanduva/São Paulo-Brazil; 2Students at Padre Albino Foundation, Medicine Faculty, Catanduva/São Paulo-Brazil; 3Student at Medicine Faculty, Fernandópolis/São Paulo, Brazil
Objective: Evaluate the impact of the use of conjugated equine estrogen, isoflavone and placebo in Kupperman and Yesavage indexes.
Design and Methods: A prospective and randomized double-blind study was developed with 30 post menopausal patients attended at the climateric clinic of Medicine Faculty of Catanduva during a period of 120 days. Patients were divided into three groups of 10: GI (placebo) - were administrated with an oral capsule per day, GII (conjugated equine estrogen) - were medicated, orally, with 0.625 mg/day, GIII (phytoestrogen) - were medicated, orally, with 80 mg/day of isoflavone. All patients were evaluated before and after treatment through the Kupperman and Yesavage indexes regarding to symptoms and depression stage during climacteric period.
Results: Sign Test for Median: YdifFITESTR; YdifPLACEB; YdifESTcnj; KdifFITESTR; KdifPLAC; KdifESTcnj - The test analyzes if the Yesavage and Kupperman value decrease, stays the same or increase with the remedy used. The test used was the “signal test-a non parametric test”. Sign test of median = 0,00000 versus not = 0,00000.
Conclusion: Conjugated equine estrogen and isoflavone administrated in post menopausal patients promoted significant improvement of the Yesavage and Kupperman indexes when they are analyzed by the signal test, however there is no significant difference when the placebo is used.
PS-33
COMPARISON OF GLOBAL QUALITY OF LIFE IN THE MENOPAUSE USING DE CERVANTES® SCALE BETWEEN A SPANISH AND A MEXICAN POPULATION
S. P. Gonzáz Rodríguez1, A. Horna-López2, E. Pérez-Luque2, G. Romero-Gutiérrez2, J. M. Malacara2, A. E. Henríquez Linares3, M. H. García Sánchez4, Lanchares Pérez J. L.4 and R. Sainz de la Cuesta3
1Gabinete Médico Velázquez, Madrid, Spain; 2Hospital General de León, Guanajuato, Mexico; 3Hospital Quirón, Madrid, Spain; 4Hospital Universitario de Salamanca, Spain
Objective: To evaluate differences in the global quality of life in the menopause in two different populations, one from Spain and the other from Mexico.
Design and Methods: A total of 425 patients were recruited from the general population of Salamanca (Spain) and 500 patients from León (Guanajuato, México). All patients were given an explanation of the reason of the study and all signed a consent form approving their participation in the investigation. A Gynecologic-obstetrical history and physical were performed and then patients were invited to fill the Cervantes® Scale for quality of life in the menopause. Previously a permission for its use was obtained from the Spanish Association for the Study of the Menopause and validation of the scale was obtained for the Mexican population. A descriptive analysis of the data of the sample was performed using variables and cases for its study applying SPSS v. 13.
Results: We found statistically significant differences in some of the basic characteristics of both populations, such as median age, median age at menarchy, menopause, parity and schooling (p < 0.001), but not in the total body mass index (p = 0.55). Mexican population presented global scores statistically superior of the Spanish population, without breaking them down by items or dominions (gross scores 72 vs 62, p < 0.001), even after correcting for age or years from menopause.
Conclusion: Mexican population from León (Guanajuato) demonstrate a worse quality of life during menopause compared to Spanish population from Salamanca, in accordance with gross scores obtained by the Cervantes® Scale.
PS-34
CHARACTERISTICS OF THE FAMILY ENVIRONMENT AND THE ATTITUDE TO MENOPAUSE AND ITS INFLUENCE ON THE CLIMATERIC SYNDROME
G. Vega-Malagón, T. Ortiz-Ortiz, L. H. Hernández-Montiel and P. García-Solis
Faculty of Medicine, Universidad Autonomous of Querétaro, México
Introduction: The climateric is a sep in the life of women, in which important physical, psychological, social and cultural changes occur, these changes test women's of their psychic capacity to carry out the psychological and social adjustments in order to maintain emotional balance.
Objective: To determine the characteristics of the family environment and the attitude to menopause and its influence on the climateric syndrome.
Material and Methods: It was a comparative study on menopausal women who were attended to the Family Medicine Units in Querétaro, México from July 2004 to february 2005. Two groups were formed: one with and one without climateric symptoms. The results were analyzed with Chi Square and Odds Ratio with an alpha value 0.05.
Results: Of 140 women interview, 94 (67%) mentioned some climateric-related symptom. The factors associated with climateric with a significant statistical difference (p: < 0.05) were: dysfunctional couple (O.R. 4.69); low self-esteem (O.R. 4.52); negative attitude to climateric (O.R. 3.4); history of oral contraceptive use (O.R. 2.69); dysfunctional family (O.R. 2.48). Residence, education, occupation, history of childbirth, being in an active sexual relationship, body mass, exercise, nicotine addiction, alcoholism, family typology and family cohesion had no significant association. The most common symptoms were fatigue (69%); hot rashes (67%); dry skin (47%); headache (46%); irritability (43%); insomnia (39%); anxiety (39%); reduction in libido (36%); depression (34%); loss of concentration and/or memory (30%); arthralgia (29%); vaginal dryness (24%).
Conclusions: The family and conjugal enviroment and a negative predisposition to menopause are more likely to cause climateric symptoms, for which reason an integral and interdisciplinary handling of the climateric period is very important.
PS-35
CLINICAL PROFILE OF MENOPAUSAL WOMEN IN RURAL SETTING
Rowshan Ara Begum
Department of Obstetrics & Gynaecology, Holy Family Red Crescent Medical College & Hospital, Dhaka, Bangladesh
This study aimed at assessing incidence of menopausal syndrome among women age 45 years and above, and their clinical variations by age, and socio-economic conditions. A cross-sectional study was carried out between August 2000 and August 2003. All women above 45 years of age were asked to participate in the clinic. In total about 2000 women attended in the out patient department. Physicians examined them clinically when attending the clinic. Age, household income was collected by using standard questionnaire. Majority (56% and 89%) of participating belongs to younger age group and lowest house income group. The distribution of backache, hot flush, insomnia, irritability, dementia, and uterine prolapsed, anorexia and weight loss among the population ≥45–55 compared to 55- 60 age group and 61–80 age group. The association is significant in both groups (p < 0.001). However, the main complain including vaginal problem (vaginitis, discharge, bleeding) were significant comparing 45–60 and 61–80 age group (p < 0.001). The result demonstrated age and socio-economic differentials in both clinical complains and symptoms. Findings clearly showed the urgency of enhancing attention for menopausal women.
PS-36
CLINICAL, LABORATORIAL AND EPIDEMIOLOGICAL PROFILE FROM ELDERLY JAPANESE DESCENDENT AND WHITE WOMEN
A. M. Fonseca, J. O. P Massabki, C. Del Giorno, V. R. Bagnoli, J. S. Assis, W. M. Y. Arie and E. C. Baracat
Department of Obstetrics and Gynecology, Medical School, University of São Paulo, Brazil
Introduction: The significative increase of mean age of female people during the last decades, justify the works with this people considering different aspects very frequent in post menopausal women.
Objective: To evaluate clinical, laboratorial and epidemiological aspects in elderly descendent from Japanese and white people.
Casuistry and Methods: Were included 80 women, 40 Japanese descendents (mean age 62,3years) and 40 white descendents (mean age 63,2 years). Were considered the parameters: tobacco users; number of pregnancies; normal deliveries, cesarean sections; miscarriages (%); age of menopause; relevant diseases in close relatives; Kupperman's Menopausa Index (KMI light: 0–19; moderate: 20–35; severe more than 35), fast glucose (mg/dl), body mass index (BMI kg/m2); lipids profile (mg/dl).
Results: The results observed in the Japanese and white people were respectively: tobacco users: 20% and 30%; mean pregnancies: 3 ± 1 and 4 ± 1; normal delivery: 60% e 40%; cesarean section: 30% and 40%; miscarriages: 10% and 20%; mean age of menopause: 50 ± 3 and 49 ± 2. The family diseases were: gastric cancer 40%, diabetes 30%, coronary heart disease 20%, others 10%, in Japanese people; and, coronary heart disease: 50%; diabetes: 30%; ischemic stroke: 20%, others: 10%, in white people. KMI = 11 ± 7 and 16 ± 5; BMI = 25 ± 4 and 27 ± 3; total cholesterol 218 ± 4,0 and 225 ± 6,0; HDL: 54,3 ± 3 and 47 ± 4; LDL: 136 ± 6 and 143 ± 2; triglicerides 118 ± 15 and 140 ± 2 were observed in the groups of Japanese and white women, respectively.
Conclusions: We concluded that white women in relation yellow women were much more frequent tobacco users; higher number of pregnancies; high frequency of cesarean sections; use to have early menopause; use to refer more symptoms, higher BMI and higher cholesterol level.
PS-37
COMPARATIVE STUDY OF QUALITY OF LIFE BETWEEN SPANISH AND IMMIGRANT MENOPAUSAL WOMEN
I. Santillán and T. Gallardo
Isabel Santillán Palencia: Hospital Universitario la Paz. Madrid, Spain; Teresa Gallardo Doménech: Hospital Universitario la Paz, Madrid, Spain
Objective: The aim of this study was the assessment of climacteric symptoms and the quality of life between Spanish and immigrant menopausal women.
Design and Method: In this cross-sectional study Spanish and immigrant menopausal women were asked to fill out the quality of life questionnaire from the Cervantes Scale in order to compare the two groups. The statistical analysis was performed by the SPSS program.
Results: A total of a 100 women were surveyed. There were no differences among the studied groups in terms of age, parity or Hormone Replacement Therapy. Intensity of menopausal symptoms was found to be higher among immigrant women which was due to higher somatic and psychological subscale scores.
Conclusion: Despite the limitations of this study, as determined by the Cervantes Scale, immigrant women exhibited more impaired quality of life when compare to Spanish ones due to higher rate and severity of menopausal somatic and psychological symptoms.
PS-38
COMPARATIVE STUDY IT APPROACHES OF THE QUALITY OF LIFE IN POSTMENOPAUSAL WOMEN IN THE CITIES OF LIMA AND CUZCO IN PERU WITH CERVANTES SCALE
L. Danckers1, E. Ojeda2 and E. Rojas1
1San Pablo Clinic, Lima, Peru; 2South East National Hospital ESSALUD, Cusco, Peru
Objective: The objective of the present study was to compare the obtained results to evaluate the Quality of Life in postmenopausal women according to the Cervantes scale in the cities of Lima at level from the sea and Cuzco to 3400 meters on the level of the sea, in Peru.
Design & Method: Women included themselves in the study between 40 and 67 years of age that go to medical consultation and in the last do not present/display menstruation previous year to the interview. To all of them it was evaluated to them using the Cervantes scale. The study was of descriptive and comparative type and was taken between January 02 and June 30 of the 2007.
Results: 152 patients in the city of Lima were polled and 130 in the city of Cuzco, the average of age in the first group was of 49,3 years and in the second 49,9 years respectively. One was that in Lima the 5,2% did not present/display any kind of problems related to quality of life unlike the 14,6% found in the Cuzco population; nevertheless the 94,1% of the first group and the 85,4% of the second they presented/displayed some kind of problems, or are of slight, moderate or severe degree corresponding 11,1% and the 13,1% to the severe type. In addition was minor incidence of problems of menopause and health in the population of Cuzco.
As far as problems in the sexuality it is comparatively similar 90,2% of the first and 93,9% of the second.
The pair relation also was affected the 96,7% of the population of Lima and the 100% of the population of Cuzco had some kind of problems with their pair.
Conclusion: If it is certain well they compare two groups of idiosyncratically different populations the found results are similar in both groups nevertheless they did not present/display annoyances in 5.2% in the women of Lima versus 14,6% in the city of Cuzco.
PS-39
EFFECTS OF AEROBIC TRAINING ON CLIMACTERIC SYMPTOMS OF HEALTHY AND HYSTERECTOMIZED POST-MENOPAUSAL WOMEN WITHOUT HORMONE THERAPY
C. G. Cardoso Jr., E. Labes, C. K. Moriyama, B. Oneda, L. G. Pinto, F. L. Medina, J. L. Gusmão, S. B. Abrahão, T. Tinucci, C. L. M. Forjaz, D. Mion Jr. and A. M. Fonseca
University of São Paulo, São Paulo, Brazil
Background: The onset of climacteric symptoms appears to involve a several conditions, especially in reduced estrogen. At present, hormone therapy is considered the most effective treatment for climacteric symptoms, but due to adverse reactions such as risk of onset breast an endometrial cancer others therapy such as lifestyle habit modification has been emphasized.
Objective: This abstract report a study examining the effects of aerobic training on climacterics symptoms of healthy and hysterectomized post-menopausal women without hormone therapy.
Design & Method: Twenty-three healthy and hysterectomized post-menopausal women were recruited to participate as voluntary in a quasi-experimental study. They were randomly assigned to one of two groups: control (n = 11) and experimental (n = 12). The experimental group engaged in a 12-month programme of cycle ergometer of three fully supervised exercise sessions per week in moderate intensity. Climacteric symptoms were assessed by Kupperman index of menopausal symptomatology at the begun and after the 12-month in both groups. To statistical analysis was employed ANOVA to non-parametric data (Friedman test) following to Wilcoxon's Post-hoc test and considered p < 0.05 to identify the statistical difference.
Results: The intervention group had improved on the Kupperman index (p = 0.02), especially in paresthesia (p = 0.04) and formication (p = 0.04) after 12-month. No change was observed in other parameters (vasomotor, insomnia, nervousness, melancholia, vertigo, fatigue, arthralgia and myalgia, headaches and palpitations (p>0.05). Furthermore, no difference was observed in a control group.
Conclusion: Based on the results it is suggesting that aerobic training influences the climacteric symptoms. Therefore, a physical programme designed for therapeutic purposes is valuable to treatment of climacteric complaints.
PS-40
EVALUATION OF THE EFFECTS ON THE QUALITY OF LIFE IN THE HYSTERECTOMIZED POST-MENOPAUSED WOMAN WITH THE USE OF THE SUBCUTANEOUS BIODEGRADABLE IMPLANT OF 17-BETA-ESTRADIOL BY THE PSYCHOLOGICAL GENERAL WELL-BEING ÍNDEX
J. C. Lima and J. Sabino Pinho
Federal University of Pernambuco, Recife, Brazil
Objectives: The aim of the study was to investigate the effects of the subcutaneous biodegradable implant of 17-beta-estradiol on the quality of life in the post-menopaused hysterectomized women.
Material and Methods: Eighty three patients were included, of the which sixty concluded the study. The quality of life was appraised in a clinical opened and descriptive study along six months using the results of the Psychological General Well-Being Index.
Results: The quality of life got better significantly with the use of the estradiol implant when compared with the results before the treatment, with obtained them after 3 and 6 months after the insert of the implant, so much in the the total score (before treatment = 92,0 – after 3 months = 105,5* – and after 6 months = 102,2*), as for its dimensions: well-being (before treatment = 14,6 – after 3 months = 16,9* – and after 6 months = 16,7*), anxiety (before treatment = 20,8 – after 3 months = 24,2* – and after 6 months = 25,6*), vitality (before treatment = 14,7 – after 3 months = 17,7* – and after 6 months = 18,8*), self-control (before treatment = 13,2 – after 3 months = 15,1* – and after 6 months = 16,1*), depression (before treatment = 14,1 – after 3 months = 16,1* – and after 6 months = 18,1*) and health (before treatment = 14,6 – after 3 months = 15,6* – and after 6 months = 17,2*) with * p < 0,001.
Conclusions: The patients that make use of subcutaneous biodegradable implant of 17-beta-estradiol, for six months, present important relief of the climacteric symptoms and great improvement in the quality of life.
PS-41
EVALUATION OF THE EFFECTS ON THE QUALITY OF LIFE OF THE POST-MENOPAUSED HYSTERECTOMIZED WOMAN WITH THE USE OF THE SUBCUTANEOUS BIODEGRADABLE IMPLANT OF 17-BETA-ESTRADIOL BY THE NOTTINGHAM HEALTH PROFILE
J. Sabino Pinho and J. C. Lima
Federal University of Pernambuco, Recife, Brazil
Objectives: The aim of the study was to investigate the effects of the subcutaneous biodegradable implant of 17-beta-estradiol on the quality of life in the post-menopaused hysterectomized women.
Material and Methods: Eighty three patients were included, of the which 60 concluded the study. The quality of life was appraised in a clinical opened and descriptive study along six months using the results of the Nottingham Health Profile.
Results: The quality of life got better significantly with the use of the estradiol implant when compared with the results before the treatment, with obtained them after 3 and 6 months after the insert of the implant, so much in the total score (before the treatment = 98,3 – after 3 months = 40,1* – and after 6 months = 45,2*), as for its dimensions: sleep (before the treatment = 33,1 – after 3 months = 14,5* – and after 6 months = 16,2*), social isolation (before the treatment = 14,1 – after 3 months = 6,5* – and after 6 months = 7,5*), emotions (before the treatment = 23,4 - after 3 months = 8,8* – and after 6 months = 9,2*) and energy (before treatment = 30,5 – after 3 months = 14,2* – and after 6 months = 15,2*) with * p < 0,001. Improvements were also observed in the complaints of symptoms related to the health evaluated in the part 2 of the Nottingham Health Profile (sexual life, family life, paid employment, domestic work, social life, hobby and holidays).
Conclusions: Patients that make use of the subcutaneous biodegradable implant of 17-beta-estradiol, for six months, present important relief of the climacteric symptoms and great improvement in the quality of life.
PS-42
IMPACT OF HORMONAL TRANSDERMAL THERAPY IN WOMEN WITH CHRONIC LIVER DISEASE
M. A. F. Pádua, A. M. Fonseca, V. R. Bagnoli, M. D. Mitiko, F. J. Carrrilho and E. C. Baracat
Departments of Obstetrics and Gynecology and Gastroenterology, Medical School, University of São Paulo, Brazil
Introduction: There are more than 175 million individuals infected with the hepatitis C virus (HCV), making this disease a significant public health issue worldwide (Barth H et al; 2006). The majority of patients with HCV report tiredness, cognitive abnormalities and a decrease in their quality of life (Weissenborn K et al; 2006).
Objective: To analize climacteric symptoms, liver function, cholesterol, glycemia, blood and hemostatic parameters in patients with chronic viral hepatitis C, during hormone therapy.
Design: Patients were divided in 2 groups: Case Group - 25 patients on transdermal hormone therapy (50mcg of estradiol and 170 mcg of norethisterone/day) for 9 months and Control Group–25 hormone-untreated patients, both with climacteric symptoms.Menopause was confirmed by measuring FSH and estradiol, and hepatitis C was diagnosed by serology, PCR (Polymerase Chain Reaction) and liver biopsy (histological type stages I to IV). Both groups were evaluated in the months 0, 1,4,7 and 9; and the climacteric symptoms measured by Kupperman's menopausal index (KMI), liver function by laboratory tests: alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma glutamyl transferase, alkaline phosphatase, bilirubin, albumin, cholesterol, glycemia, blood and hemostatic parameters.
Statistical Analysis: Mann-Whitney test and two-factor analysis of variance with repeated measures were applied. After analysis of variance, multi-factor analysis of variance was applied for the statistically significant effects using contrasts or Dunnett's test.
Results: The mean age of patients was 53.72 and the mean age of menopause was 47.3 years. The total mean scores for vasomotor symptoms, fatigue, palpitations and the sum of the values attributed to Kupperman menopausal index do change throughout time, (p < 0.05). Levels of alkaline phosphatase show alteration throughout time (p < 0.05), however, other measures for liver function, blood, choresterol, glycemia, hemostatic parameters did not show mean difference between the groups.
Conclusion: Short-term transdermal hormone therapy might be an effective and safe option to improve postmenopausal symptoms in women with chronic hepatitis C and to improve the quality of life of these women.
PS-43
INSULIN RESITANCE AND QUALITY OF LIFE IN MENOPAUSE
P. Llaneza1, J. Fernández-Iñarrea2, I. Arnott1, A. Alonso3, C. González3, Maria Diaz-Fernandez4 and Y. J. Ferrer1
1Central University Hospital of Asturias, Oviedo, Spain; 2Cabueñes Hospital, Gijon, Spain 3Department of Functional Biology, Oviedo University, Oviedo, Spain; 4Valle del Nalon Hospital, Langreo, Spain
Objective: The present work evaluates whether insulin resistance influences the Health Related Quality of Life (HR-QoL) in a sample of post-menopausal Spanish women.
Design & Method: Insulin sensitivity was assessed in 496 healthy post-menopausal women, aged 50–65 years, by Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) and 110 of them were elected to participate in the study as they had values of HOMA-IR ≥ 2.25 (IR group). Another 110 women with normal HOMA-IR values and similar BMI, age, smoking habits, physical activity, chronic treatments or educational level were selected as a control group (C Group) in order to study their HR-QoL with the Cervantes Scale.
Results: HR-QoL domains were similar between the IR and C Groups. BMI, waist circumference, fat or lean mass had not influences on HR-QoL. Fifty six women (50.9%) in the IR Group and twenty five women (22.7%) in the C Group were considered women with Metabolic Syndrome (MS). When IR women with MS were considered, more women with a high level of problems on the Cervantes Scale Global Score were found and the difference was mainly due to Health and Sexuality domains.
Conclusions: IR was not related with changes in HR-QoL, but when MS is associated, higher level of problems in HR-QoL was found due to sexuality and menopause and health domains.
Financial Support: The present study was backed by a Health Investigation Grant funded by the Spanish Government (PI-O51616).
PS-44
INVESTIGATION OF FOOD INTAKE AND BODY COMPOSITION IN POSTMENOPAUSAL WOMEN
A. P. Tardivo1, J. Nahas-Neto1, N. Maesta1, E. A. P. Nahas1, A. Delmanto1, C. E. Fernandes2, G. Uemura1 and P. Traiman1
1Botucatu Medical School, UNESP-São Paulo State University; 2ABC Medical School; São Paulo, Brazil
Objective: To investigate the food intake and indicators of body composition in post-menopausal women.
Design & Methods: This cross-sectional, clinical study was undertaken in a convenience sample consisting of 173 Brazilian postmenopausal women, aged 45–65 years, registered, as well as followed up, at the a public outpatient clinic. All women without menstruation for at least 12 months, users and non-users of hormone therapy (HT), were included in the study. The food consumption was assessed by the 24h-record food inquiry and the healthy eating index (HEI). The anthropometric indicators included: weight, height, body mass index (BMI = weight/height2), abdominal circumference (AC), waist/hip ratio (WHR), body fat (%BF) and lean mass (%LM). Data on total cholesterol, HDL, LDL, triglycerides and glycemia were also collected. The nonparametric t test of Student and Pearson's correlation were used in the statistical analysis.
Results: Mean age was 54 years ± 7.6. Overweight and obesity were observed in 76% of the patients. Based on the HEI values obtained, diet quality was poor in 91% of the cases. Protein and carbohydrate intakes were adequate, but the quality of the lipids consumed was inadequate in relation to saturated fat >7% and polyunsaturated fat > 10%. Calcium and iron intakes were adequate in only 9% and 7% of the cases, respectively. The risk of cardiovascular disease, as determined by the waist/hip ratio, was considered high in 39% and very high in 36% of the women. Abdominal circumference was elevated (>80 cm) in 89% of the patients, which contributed for the occurrence of metabolic complications. On average, total cholesterol, LDL, and triglycerides levels were higher than recommended in 79%, 55% and 79% of the women, respectively and HDL was low in 55%. HEI correlated negatively with abdominal circumference (r = −0.164) and%BF (r = −0.156), and positively with %LM (r = 0.157) (p < 0.05). No significant differences were found between users and non-users of HT regarding food consumption, indicators of body composition and biochemical.
Conclusion: In the postmenopausal women seen at a public outpatient clinic, food intake was considered to be of poor quality, characterized by high intake of the lipids and low intake of calcium and iron, with unfavorable anthropometric indicators for the cardiovascular disease.
PS-45
LIFESTYLE - CHANGE - MINIMISE MENOPAUSAL SYMPTOMS
Devindraben S. Shah and Umaben V. Shah
Gulabbai Hospital and Kachhi Jain Medical Center, Ahmedabad, Gujarat, India
Objective: Menopause is a phase which comes in all women but how do the patients view it? Is it the end of a women's life because fertility ends? Proper concrete counseling, change of lifestyle including diet, habit, hobby, exercise and creativity definitely reduces/controls menopausal symptoms. At last she herself becomes useful to her family members, society and professionally to her colleagues and thus leads a cheerful, enjoyable life.
Design & Method: 87 cases were randomly collected between the age group from 35 to 60 and only 2 patients were above 75. All patients were divided into perimenopausal, menopausal and postmenopausal groups. The patients of perimenopausal age were counseled gradually for menopausal and postmenopausal life. Menopausal patients were counseled for their lifestyle, to develop some good hobby and creativity and positive attitude towards menopausal phase. Postmenopausal patients were counseled for their associated diseases like High Blood Pressure, Diabetes, and Osteoporosis etc.
All the patients were clinically examined thoroughly for their height, weight, BMI calculation,routine P/S,P/V examinations, appropriate evaluations according to their complaints and if required, physicians and orthopedic surgeons were consulted.
Results: Between the age of 35 to 40 there were 24 patients; from 41 to 45, 14 patients. Out of 87 patients, 67 were from the hospital and 20 were taken from a yoga class – age was between 38 to 48. 67 patients who had come to the hospital – preliminary record of name, age, address, birth date, education, professionally working or not working etc were taken and chief complaints were taken in detail. Also they were allowed to convey whatever they wanted in their words e.g. scary menses and fear of obesity, delayed period and fear of pregnancy. When taking the complaints – some of the patients had no complaints so far and suddenly the complaints had stated. Related to their complaints, positive answers encouraged that she will be okay through proper advice about diet, exercise, and how to keep herself busy for the whole day. Twenty patients from the yoga class were counseled.
At the end, some investigation required for Diabetes, USG, BMD etc were done with prescription related to their complaints – menstrual irregularity,for UTI antibiotics and alkalisers were prescribed, Flavoxate, Soya, analgesics etc were prescribed for 7 to 10 days. They were called for follow up and necessary modifications in management were tried.
Conclusion: Proper counseling, changing of lifestyle, exercise, yoga,positive attitude definitely minimizes and reduces the severity of menopausal symptoms and ultimately minimizes the drug therapy.
PS-46
MENOPAUSE QUALITY OF LIFE EXPERIENCE AMONG CHILEAN WOMEN AND THEIR HUSBANDS
A. Salazar and T. Paravic
University of Concepción, Concepción, Chile
Objective: To relate menopause quality of life in Chilean women with menopause quality of life experience perceived by their husbands.
Design & Method: Cross-sectional and correlative desing. Participants were 49 women aged from 40 to 60 years old, and their husbands from Concepción, Chile. Both, women and their husbands were assessed using the Menopause-Specific Quality of life Questionnaire (Hilditch y cols., 1996). Statistic descriptive and Pearson's correlation coefficient were used. Significant differences were determinated with p value <0,05.
Results: Mean age was 50,7 years for women and 53,2 for men. Most women under study showed a moderate alteration of the quality of life. The menopause quality of life of women in vasomotor, phisical and sexual domains had correlation with menopause quality of life perceived experience by their husbands (p < 0,01), but psychosocial domain had no correlation.
Conclusion: Association between menopause quality of life of Chilean women in vasomotor, phisical and sexual domains with menopause quality of life perceived experience by their husbands was observed. Notably, the finding of no correlation between women experience in psychosocial domain and perceived experience by their husbands suggests the inclusion of women and their husbands in menopause quality of life studies.
PS-47
PSYCHOSOCIAL ASPECTS CONCEARNING SURGICALLY INDUCED MENOPAUSE
P. Chitulea, Ioana Popa and L. Popa
Obstetrics and Gynaecology University Clinic, Oradea
This study was conducted in the Oradea - Obstetrics and Gynaecology University Clinic,between 1999–2007, during this period being investigated a number of 575 patients with surgically induced menopause, main study issue being the psychosomatic impact of this particular kind of surgery.
A specially elaborated questionnaire was applied to this group, regarding their psychological state and the expectancy regarding some psychosomatic functions as early mobilisation, resuming domestic and professional activity, as well as sexual activity.
Contrary to expectations, total histerectomy with bilateral anexectomy, wasn't perceived as a major mutilation, due to the conditions wich consisted in the surgical indication, as well as haemorrhage and pain, those being a stress-factor by themselves. Studying the psychosocial functions listed above, approximately 70% of our patients had a positive expectancy of those and after surgery 80% confirmed this positive expectancy. Our H.R.T., applied in the first five to ten days after surgery, probably added to this positive impact, too.
PS-48
QUALITY OF LIFE AND RELATED FACTORS IN MENOPAUSAL WOMEN IN KASHAN CITY
M. Abedzadeh, M. Taebi, F. Saberi and Z. Sadat
Kashan University of Medical Sciences, Kashan, Iran
Objective: Menopause is a physiological event that occurs in women's life and result in physical, emotional and social changes which affects their quality of life. Considering to controversial finding in previous researches and lack of such study in kashan city, this study investigated the quality of life in menopausal women and its related factors.
Design and Methods: A cross - sectional study was performed on 700 menopausal women aged 40–60 in Kashan city with cluster sampling. Menopausal Specific Quality of life questionnaire (MENQOL) was used for estimation of QOL and related factor such as age, job, educational level, marital status, duration of menopause, child at home, income satisfaction, marital satisfaction, exercise, smoking and family smoking were examined with statistical tests.
Results: The quality of life was high in 17.9%, medium in 68.9% and low in 13.3% of women. Most of women had medium quality of life at vasomotor domain (67.3%), psychosomatic domain (67.4%), physical domain(46.3%) and sexual domain (51.6%). Also there was a significant difference between quality of life and educational level (P = 0.004), income satisfaction (P = 0.01) and exercise (P = 0.0001).
Conclusions: Considering our findings, we emphasis on teaching about menopause, its symptom and adverse effects. Also emphasizes the necessity use of non pharmacological methods such as exercise and change in life style and diet to improve quality of life in menopausal women.
PS-49
QUALITY OF LIFE IN A VALENCIAN WOMEN'S COHORT DURING CLIMATERIUM
R. M. Marín1, J. Quiles2, M. D. Juliá3, E. Pastor2, J. Redón4, J. Chaves4 and A. Romeu3 Research Group about influence of life styles, genetic and biological factors on women's health in Valencian Region(+)
1Valencian School for Health Studies, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 2Public Health Department Directorate, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 3University La Fe Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 4University Clinic Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain
Objective: to assess quality of life and factors related to climacteric women in the Valencian Region.
Subjects and method: Population cross-sectional study of a sample of 675 women from 45 to 65 years old in four different geographical areas of Valencian Region. Personal interview for variables and performance of Quality of Life Questionary (CCV), validated in the Valencian Region (Sánchez-Cánovas et al.) which explores: information and attitudes to menopause, anxiety-depression, partner relationship and sexuality, social and family help. Statistical analysis: descriptive and non condicionated logistic regression model to measure associative strength. Statistical Packs: SPSS-v12.0 y STATA/SE v8.
Results: Total CCV scale results showed that 19% had any problem and need to be asses by Primary Attention staff, and could be improved upon with educational and promoting health activities. Also, 17% of the women showed scores of bad quality of life and it was indicated specialized professionals intervention.
There was significant differences (p < 0,05) for total score of CCV with the presence of disable people at home, visits to doctor, number or drugs taken, tobacco, alcohol consumption, sleeping hours, presence of genital pain and pruritus, sexuality variables, Kupperman Index, and presence of intestinal and urologic inconveniences.
Factors related to bad quality of life in regression model: climacteric syndrome severity (Kupperman), sleeping hours, and the presence of pruritus. For climacteric syndrome intensity, they were estimated Odds ratio (OR) of 4.8 [CI95%: 3.0–7.6] for light; de 5.7 [CI95%: 3.2–10.3] for moderate and 18.6 [CI95%: 6.4–53.9] for severe. Women who slept less than 7 hours showed OR of 3.3 [CI95%: 1.9–4.5]. Women with pruritus showed 1.9 [IC95%: 1.1–3.3] times more risk of worst quality of life.
Conclusions: Women's quality of life was deteriorated specially due to intensity of climacteric symptoms. Quality of life is affected by multiple aspects needing more studies for a deep analysis.(++)
(+)Research Group: Marín RM, Quiles J, Redón J, Chaves J, Romeu A, Juliá D, Pastor E, Mejia MJ, Marín P, Pírez AF, Bertolín A; Alonso C, Rozada R; Sánchez M; Rico MJ.
(++)The data of this study are included in: “Epidemiological Study on Cardiovascular Disease risk during the climacteric period of four different areas of the Valencian Region”. This project was partially financed by Women's Institute of the Department of Job and Social Matters of Spanish Government, Exp. number 65/01.
PS-50
RELATIONSHIP BETWEEN PAIN AND INTERPERSONAL ACTIVITY AMONG THE ELDERLY OVER 5O YEARS OLD AT DISTRICT OF PURWOREJO, CENTRAL JAVA, INDONESIA
D. Dasuki1, Kartini2 and N. G. Nawi3
1Magister, Mother and Child Health – Reproductive Health, Gadjah Mada University, Yogyakarta, Indonesia; 2Midwife Department, Health Polytechnic, Kendari, Indonesia; 3Magister, Field Epidemiology and Training Program, Gadjah Mada University, Yogyakarta, Indoensia
Objective: Increasing life expectancy every year followed by increasing number of the elderly from 1990–2025 (41.4%) requires particular attention in order that the elderly can spend their lives in optimum ways. Purworejo District has higher rate of the elderly numbers (11%) than that in Central Java (6%). Changes that occur during ageing have caused some health problems such as pain. This brings about negative impacts to quality of life of the elderly, one of which is interpersonal activity consisting of relationship with others and social participation. The study was conducted to identify the relationship between pain and interpersonal activity disorder among the elderly over 50 years old.
Design & Method: This was an observational study with cross sectional design. There were as many as 13,890 elderly people over 50 years old as the subjects of the study. Data were obtained using questionnaire from Study of Global Ageing and Adult Health (SAGE), WHO, and International Network for INDEPTH. Data analysis used multinomial logistic regression test and the significance level (p) was <0.05 and 95%CI.
Results: The prevalence of pain was 70% and activity interpersonal disorder was 63%. The result showed that there was a significant relationship between pain and interpersonal activity disorder whereby the greater the pain was the greater interpersonal activity disorder became, OR 3.4 (95% CI = 2.67–4.44) p = 0.000. Other independent variables such as age, education, status of job and marital status had significant relationship with interpersonal activity disorder.
Conclusion: There was relationship between pain and interpersonal activity disorder.
PS-51
THE HEALTH IMPACT OF PHYSICAL AND PSYCHO-SOCIAL STRESSORS ON WOMEN REFERRING TO THE SHIRAZ HEALTH CLINICS
Iran Jahanbin1, Zohreh and Makiabadi2
1Faculty of nursing & midwifery Shiraz University of Medical Sciences, IRAN, Farhang shahr, Istgah12, rajaee29, Shaghayigh1, No. 56, [email protected]; 2Faculty of nursing & midwifery, Shiraz University of Medical Sciences IRAN
Purpose of the Study: To investigate the health impact of physical and psychosocial stressors on women referring to the Shiraz health clinics.
Although many studies have focused on the relationship between stress and health, few have examined the impact of multiple types of stressors.
Methods: The sample included 1120 female clients from referral-based health clinics. Stressors described by women in the in-depth interviews, included financial strains, work, family safety, experiences of discrimination.
Results: We found that the above stressors were related to poor health. Although women live longer than men, they are more likely to use health services and report greater rates of disability. Women are more likely than men to make visits to physician's offices. Family structure and social support problems were the two most commonly addressed psycho-social stressors. Social support appears to be related to better health and feeling of well-being. Lack of recreation and relaxation activities can cause stress, overwork, anxiety and in some instances depression.
Conclusion: The findings suggest the need for health education interventions and policy strategies that strengthen social support and aim at macro level changes necessary to reduce chronic stressful conditions.
PS-52
STRESSORS PERCEIVED BY CARDIAC SURGICAL ELDERLY PATIENTS IN THE INTENSIVE CARE UNIT
E. Parreira Da Veiga, L. Gomes and C. J. de Cárdenas
Catholic University of Brasília, Brazil
Objective: One of the main reasons for hospitalizing elderly patients in Intensive Care Units (ICU) are the heart diseases. Due to the need of remaining there after heart surgeries, it is important to identify the stress generator factors in this group, so that better assistance can be provided. The aim of this study was to identify and to stratify the stress grade in elderly patients submitted to heart surgery.
Design & Method: A cross-sectional descriptive study was carried out between August and November 2007 in a heart diseases ICU. The sample was composed by 20 elderly patients of both genders. In order to identify and to stratify stressful factors, it was used the Intensive Care Unit Environmental Stressor Scale (ICUESS). A total stress score (TSS) was calculated, from the sum of all the answers of the scale.
Results: The mean age was 67,80 ± 6,46 years (60–81), being 50% males. The mean TSS was 76,45 ± 20,65. The following more stressful factors were identificated: having tubes in your nose or mouth, not being able to sleep, have pain, have thirsty, being tied down by tubes.
Conclusion: This study identified the stressful factors for elderly patients in ICU's. The elderly have ranked the stressful factors in ICU as no stressful or little stressful.
PS-53
SELENIUM AND QUALITY OF LIFE IN MENOPAUSE
P. Llaneza1, J. Fernández-Iñarrea2, I. Arnott1, A. Alonso3, C. González3 and Y. J. Ferrer1
1Central University Hospital of Asturias, Oviedo, Spain; 2Cabueñes Hospital, Gijon, Spain; 3Department of Functional Biology, Oviedo University, Oviedo, Spain
Objective: Ageing and obesity are associated to plasma selenium fall. Selenium is an essential trace element involved in the complex system of defence against oxidative stress and may be particularly important for the maintenance of brain functions. The prevalence of the obesity and overweight are rising in Western Countries and are associated with increased oxidative stress due to insulin resistance (IR) and cognitive function can be altered in women with hiperinsulinemia.
The objective of the present study is to evaluate if there is some relation between serum selenium levels and HRQoL in a sample de menopausal women with IR.
Design & Method: One hundred and sixteen postmenopausal women with values of HOMA-IR ≥ 2.25 were evaluated with Cervantes Scale, a validated tool to evaluate HRQoL in Spanish women between the ages of 45 and 64. These women had intact uterus and ovaries and were sexually active and non-hormone therapy users. In two cases were not possible to evaluate the Scale because women did not fill all the scale items.
Blood samples were taken between 9 and 10 a.m. after an overnight fast and we measured fasting glucose, insulin, the lipids profile and selenium. The general characteristic of the sample were expressed as mean ± standard deviation and percentages. Analysis were adjusted for age, BMI, waist circumference, fat and lean mass, smoking habits, physical activity, chronic treatment and educational levels.
Results: Women in the lowest Serum Selenium tertile had higher triglycerides levels than the medium tertile (p = 0.002) and the highest tertile (p = 0.011). Homocysteine mean values in the lowest tertile were lower than the medium tertile (p = 0.039).
According with Cervantes Scale, women sorted out as a Good level HR-QoL showed higher mean values levels of serum selenium (mean 113.3 ng/ml SD 5.131) than women with High Level of Problems or Severe Symptoms (mean 101.0 ng/ml SD 18,7136) p = 0.048. Not differences were observed among the rest of the groups.
Conclusion: Serum selenium levels could have some influence in HR-QoL in menopausal women with IR. Some specifics domains like climatic symptoms and sexuality were worse in women with lower levels of serum selenium.
PS-54
SOCIAL AND BIOLOGICAL FACTORS RELATED TO SLEEP QUALITY IN MIDDLE-AGED WOMEN IN HAVANA
Navarro Daysi1, Manzano Blanca Rosa2, Artiles Leticia3, Diaz Dayami2, Garcia Tatiana4, Fontaine Yadiria4 and Figuera Adahli2
National Institute of Endocrinology1, Ramon Gonzalez Coro Gynecologic Hospital2, Havana Medical School; 3Heroes del Moncada Primary Health Center; 4Cuba
Objective: To assess the frequency of changes in sleep quality and the influences of biological and social factors on it.
Subjects and Methods: Cross section study. Includes; 1) 1920 women interviewed at home between 1996 and 2006 and 2) 212 patients who asked for medical care at the Climacteric and Osteoporosis Clinic between 1997 and 2004. Their age span was between 40 and 59, all of them having high education level and full accesses to health care services. We considered as “bad sleep quality” any of the following circumstances: early wakening, insomnia, restless sleeping and morning tiredness. Evaluated variables: current age, climacteric stage (peri and post menopausal), intensity of the climacteric syndrome (according to their own perception and to the Cuban Scale of Perez), gender overload. In women interviewed at home we also looked for the reasons they considered unnecessary to ask for help. To assess the differences between groups the Chi-square test and the Odd Ratios were used.
Results: Among the women interviewed at home 2–3 of 10 complained of “bad sleep quality”, increasing to 5–6 of 10 during the first 5 post-menopausal years; the frequency was even higher among women attending clinics. There was no association with the intensity of the climacteric syndrome in any group. After the first 5 post-menopausal years the frequency decreased to 3–4 of 10. Working out of home, not having a regular sexual partner, being over 45 years old together with gender overload (OR 0.5) were factors having a negative impact on sleep quality. Lack of time and being unable to identify the relationship between bad sleep quality and the climacteric period were given as reasons for not seeking help.80% of the women receiving HRT referred an improvement in sleep quality(n = 112).
Our results suggest: the need to perform studies on the influence of hypoestrogenism in sleep quality and to incorporate gender overload and lack of information to the established factors contributing to a bad sleep quality.
PS-55
STATUS OF PERCEIVED HEALTH AND ASSOCIATED FACTORS IN A CLIMACTERIC WOMEN'S COHORT IN VALENCIAN REGION
J. Quiles1, M. D. Juliá2, R. M. Marín3, E. Pastor1, J. Redón4, J. Chaves4 and A. Romeu2 and Research Group about influence of life styles, genetic and biological factors on women's health in Valencian Region(+)
1Public Health Department Directorate Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 2University La Fe Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 3Valencian School for Health Studies, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 4University Clinic Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain
Objective: To study factors related to status of perceived health in climacteric women of the Valencian Region.
Subjects and method: Population cross-sectional study of a sample of 675 women from 45 to 65 years from four different geographical areas of the Valencian Region. Variables were obtained through personal interview. Statistical analysis: descriptive and unconditioned logistic regression model to measure associative strength. Statistical Pack: SPSS-v12.0 y STATA/SE v8.
Result: 597% of women showed to have excellent-good health; 34′2% perceived it as regular and 6% as bad-very bad.
Significant differences (p < 0.05) were observed in perceived health status and resident area, age, body mass index (BMI), frequentation to doctor, number of doctors consulted, number of drugs taken, tobbaco, alcohol consumption, external job or housewife; hours a day of external work, intensity of exercise a day, sleeping hours and passive leisure time, and sexuality aspects (sexual desire, satisfaction and frequency), Kupperman Index, presence of genital pain, digestive pain, pruritus and dislipemia.
Factors related to bad perceived health status in regression model were: BMI, drugs consumption, frequentation to doctor, Kupperman Index and quality of life. Obesity women had 2.1 times [CI95%: 1.1–3.8] more risk of perceiving as bad their health status. As much drugs they consumed the OR increased till reach a maximum of three drugs, OR = 4.2 [CI95%: 2.1–8.3]. Visit to doctor more than once weekly: OR = 3 [CI95%: 1.6–5.5]. Climacteric syndrome intensity: were estimated OR = 1.9 [CI95%: 1.0–3.6] for moderate syndrome. Quality of life: women showing worst score showed 7.2 [CI95%: 3.8–13.7] times more risk of perceiving worst their health status.
Conclusions: Interpretation of health status was objective if obesity, more frequentation to health system, worst quality of life and more drugs consumption were considered.(++)
(+)Research Group: Marín RM, Quiles J, Redón J, Chaves J, Romeu A, Juliá MD, Pastor E, Mejía MJ, Marín P, Pérez AF, Bertolín A; Alonso C, Rozada R; Sánchez M; Rico MJ.
(++)The data of this study are included in: “Epidemiological Study on Cardiovascular Disease risk during the climacteric period of four different areas of the Valencian Region”. This project was partially financed by Women's Institute of the Department of Job and Social Matters of Spanish Government, Exp. number 65/01.
PS-56
STUDY OF MENOPAUSAL SYMPTOMS AMONG MIDDLE AGED WORKING WOMEN: FREQUENCY, INTENSITY AND RELATED FACTORS
Gulshan Ara
Shaheed Ziaur Rahman Medical college, Bogra, Bangladesh
Objectives: To determine frequency, intensity and associated factors among healthy middle aged working women.
Design & Methods: Cross sectional study of women aged 40–59 yrs working in Bank, High schools and hospitals. Assessed by using MRS. 400 hundred women were included. Demographic data was correlated.
Results: Mean age was 46.2 ± 2.1 yrs. 20% was post menopausal, 50% was perimenopausal stage. Muscle and joint pain was most frequent symptoms with overlaping of other symptoms. MRS scores significantly increased with age. Logistic regression confirmed association.
Conclusion: Age, menopause, sexual problems and level of education was independent risk factors for severe menopausal symptoms.
PS-57
SURVEY ON THE PROFILE OF THE MENOPAUSIC VENEZUELAN WOMAN
J. Moreno-Isturiz and D. Martin
Clinica El Avila, and Caracas Venezuela
Introduction: In order to evaluate the quality of life in the menopause women world-wide there are diverse surveys and instruments, but all are Anglo-Saxon except the Cervantes scale created in Spain.
We decided to make a typical survey for the Venezuelan woman and this is the preliminary results.
Design and Method: 200 surveys were made, to evaluate the profile of the Venezuelan menopause woman, age 50 and older in Maracaibo (30) and Caracas (170), distributed of the following form: 129 surveys in women between the 50–60 years: 50 surveys in women between the 60–75 years and 21 surveys in greater of 75 years.
Parameters of Quality of life were measure such Sexual activity, general menopause sintomatology, Psychological sphere, Social sphere and Holistic Sphere.
Results: Between the preliminary results was a series of coincidences in all the ages such as that all the women believe in herself, they trust in her intelligence to solve problems, they likes to learn new things, think that the menopause is not a punishment, feel little seductive and wise people and, but their life HAVE sense.
To the questions: if there is lost of the patience (65%), easy irritability (68%), menopause is a punishment (82.6%), God left to me (95%), Insomnia (68%); the percentage were of negative answer in all the ages.
My life has sense (68%), I am supported myself (89.3%), I have confidence in my (68%), I have confidence in my intelligence (68%), muscular pains (68%), I learn new things every day and with facility (68%); the percentage were of affirmative answer for all the ages.
To the question if God left her, the 100% of the survey over the 75 years said NO.
Conclusions: First survey made in Venezuela that explores several aspects on the menopause Venezuelan woman.
With these and other questions we think that we can have an idea of the profile of our women in this stage of the life.
It can be source for the creation of our own scale of life in this stage of the woman.
We hoped to be able to extend but the data and to obtain a greater universe of women with the purpose of with this data comparing us to the world-wide works.
PS-58
THE CERVANTES SCALE®: MEASURING A WOMAN'S QUALITY OF LIFE DURING THE CLIMACTERIC PHASE IN SANTA CRUZ, BOLIVIA
M. Pommier1, D. Mostajo2, J. Villarroel3, S. Carvajal4, J. Mendoza5, C. Rodriguez6 and P. Davalos7
1Clinica Urbarí Santa Cruz-Bolivia; 2Centro Medico Udime Santa Cruz-Bolivia; 3Clinica Urbarí Santa Cruz, Bolivia; 4Caja Nacional Seguro Social Santa Cruz, Bolivia; 5Corporación Social de Seguro Militar Santa Cruz, Bolivia; 6Clínica Siraní Santa Cruz, Bolivia; 7MSc, Univ, Gabriel René Moreno Santa Cruz, Bolivia
Objective: To measure the quality of life of women during the climacteric phase by applying the questionnaire of the Cervantes Scale® to a sample of 600 women between 45 and 64 years old in Santa Cruz, Bolivia.
Methodology: Using the single-stage conglomerate sampling method, 600 women between 45 to 64 years old, were selected from several Santa Cruz neighborhoods presenting similar characteristics. The women were mentally and physically capable to answer the questionnaire and accepted to take part in the investigation. They were interviewed over a 4-month period. The internal consistency was validated through Cronbach's α coefficient. For test-retest marking stability, Spearman's non-parametric correlation coefficient was calculated. This objective was achieved by using the statistical processor SPSS 11.5.
Results: Socio-demographic characteristics of the participants:
Women's age: 45–49 = 31%; 60–64 = 22.5%
Instruction level: high school or more 45.7%; illiterate 6.0%
Number of children: none: 6.7%; 3–4 children: 44.5% 5; more than 4 children: 25.4%
Occupation: works outside the house 73.8%; does not work outside the house 26.2%
The personality scale consists of three domains: introversion, emotional instability, and honesty, and 20 questions were used. The Cronbach α index was between 0.80 and 0.83, with a global Cronbach α index of 0.9282.
The Cronbach α index over the total of 51 questions was 0.9392.
Conclusions: The Cervantes Scale allows measuring and acknowledging the deterioration of the quality of life in climacteric women as a function of their age.
PS-59
THE MEANING OF THE PLAYFUL FOR THE AGING WOMEN
N. Moreira De Matos, M. A. Germano Bouzada, C. Jansen de Cárdenas and L. Gomes
Catholic University Of Brasília, Brazil
Objective: The playful activities generate please and emotional equilibrium, contributing for the social development and leading to the individual autonomy about acts and thoughts. The playful is associated to the joke and the play acts. The objective of this work was to know the playful meaning for the elderly women of the “Samambaia's Elders Association Group of the New Hope”, Brasilia, Brazil, when they experienced ten games and jokes offices, selected and adapted for the aging group.
Design & Method: It was designed a social research of qualitative base, according the research-action. The used instruments were: interview outlines, collective evaluation of the workshops and a diary with all the procedures and photographs carried out. The criteria utilized were: female sex, 60 years or more, no physical or psychological problems that commit the answers, and participation in 70% of the offices.
Results: 20 elders participated of the ten offices, 61% of them been young elders (60–79 years); 65% were married; 50% were retired; and 50% of them had studied up to the primary school first grade. The elder group understand the benefits of playful during the games and jokes as: joy, learning, laughter, fun, feel light, please, do exercise, be creative, beauty, socializing and integration. The given initial answers for the playful meaning were shorter and simpler. In the second answer, the women spoke about the experiences lived and well succeeded during the offices, as well as make addition of positive adjectives in all the speeches. Elder women have a better understanding of the playful when they have the opportunity to experience it.
Conclusion: The playful meaning was modified positively after the experience of games and jokes offices. The elderly women understand better the playful when they have the opportunity of experience it once again in the senility. The playful activity offers multiple benefits for the aged group, needing adaptations for better use in the senility.
PS-60
THE SPECIFICS OF THE CLIMACTERIC SYNDROME AT A WOMEN WITH HYSTEROMYOMA
S. I. Kim and N. N. Mezinova
Kazakh National Medical University, Almaty, Kazakhstan
The hysteromyoma, hormone-dependent tumor, often accompanied by complex symptomatology. The symptomatology is caused by oncoma and climacteric syndrome.
The demonstration of climacteric syndrome was observed at a 130 woman patients with oligosymptomatic hysteromyoma and 50 woman patients without gynecologic pathology.
The average age of two researched groups was not different essentially (47,5 ± 1,2 and 45,5 ± 1,6).
The severity and individual demonstration (neuro vegetal, psychoemotional, endocrine metabolic) of the climacteric syndrome were measured by modified menopausal index
(“ MMI”, E.V.Uvarova, 1982).In the basic group (with hysteromyoma and climacteric syndrome)
The MMI was 50,9 ± 1,5 in opposition to 63,2 ± 2,7 units in the compared group, that demonstrates the average severity of the climacteric syndrome at a women with hysteromyoma and serious severity in the compared group.
The serious demonstration of climacteric syndrome in compared group was caused by neuro vegetal disorders (38,8 ± 1,6 in opposition to 30,1 ± 1,8 units). Psychoemotional, endocrine metabolic disorders had the mean severity demonstration in both groups.
Conclusion: The climacteric syndrome at a women with hysteromyoma proceeds in average level of severity while the women without hysteromyoma has got bad run caused by expressed neuro vegetal disorders. Probably, this fact is caused by the character of the hormonal level that will be the subject for next researches.
PS-61
UROGENITAL ATROPHY IN CURRENT USERS OF POSTMENOPAUSAL HORMONE THERAPY AT SIRIRAJ MENOPAUSE CLINIC
S. Indhavivadhana, P. Leerasiri, M. Rattanachaiyanont, S. Laiwejpithaya, P. Tanmahasamut, K. Techatraisak and S. Angsuwathana
Department of Obstetrics and Gynecology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Objective: To determine the prevalence of urogenital atrophy and their relationship to types of hormone therapy (HT) in current users of postmenopausal HT.
Design & Methods: A cross-sectional study was conducted in 97 current users of postmenopausal HT at Siriraj Menopause Clinic from 2005 to 2007. Symptoms and signs of urogenital atrophy were assessed by interviewing using a questionnaire and pelvic examination, respectively. The objective signs of vaginal atrophy were assessed using vaginal pH and maturation value (MV).
Results: The prevalence of urogenital atrophy in current users of HT were 44.3%, 41.2% and 10.0% determining from patient's symptoms, vaginal pH, and MV, respectively. The symptom of vaginal dryness was not significantly associated with MV <50 or vaginal pH >4.5 but there was high association between MV and vaginal pH (kappa = 0.78, P = 0.000). Stress and urge urinary incontinence presented in 53.6% and 21.6% of all participants, respectively. The prevalence of incontinence, either stress or urge, had no association with causes of menopause (i.e. natural or surgical), or the presence of symptoms or signs of urogenital atrophy. Among various types of HT (estrogen-only, estrogen-progestogen, tibolone, and raloxifene), tibolone had the lowest prevalence of subjective atrophic symptoms (28.6%), whereas estrogen-only HT had the lowest prevalence of objective atrophic signs (high pH of 23.8% and low MV of 6.5%). There was statistically significant association between types of HT and atrophic signs (P = 0.003 for pH, and 0.000 for MV).
Conclusion: The prevalence of urogenital atrophy varies depending on the assessment methods. The subjective method gave higher prevalence than the objective one did. There was statistically significant association between types of HT and urogenital atrophy assessed by objective methods but the present study had not enough power to detect the association when the urogenital atrophy was assessed by a subjective method. Since the subjective symptoms of urogenital atrophy would have more adverse effect on quality of life than the objective signs do, further research is required to assess factors affecting urogenital atrophy determining from patients' complaints.
Gynecological cancers
PS-62
A HISTOLOGICAL FINDING IN PROCESSES WITH DISTINCT ETIOLOGY: GRANULOMATOUS ENDOMETRITIS
Jesus S. Jimenez1, Jose L. Muñoz1, S. Concha Perez1, C. Carmen Alvarez1, G. Carmen Guillen1, M. Cristina Gonzalez1, G. Gregorio Lopez1 and V. Victoria Bravo1
1Dept. Obst./Gyn. Hospital 12 Octubre, Madrid, Spain
Objective: A finding of granulomatous endometritis in the biopsy or endometrial specimen should lead to suspicion of genital tuberculosis. Granulomatous endometritis is a chronic inflammation histologically characterized by the presence of granulomas in an endometrium with lymphoplasmacytic infiltrate.
Design & Method: We present seven cases of genital tuberculosis in postmenopausal women, diagnosed between June 2002 and April 2005. In this period were made 6.235 hysteroscopies diagnostics in our unit of endometrial pathology, which 54% corresponded to menopauses patients. I am applied the scheme diagnose associate.
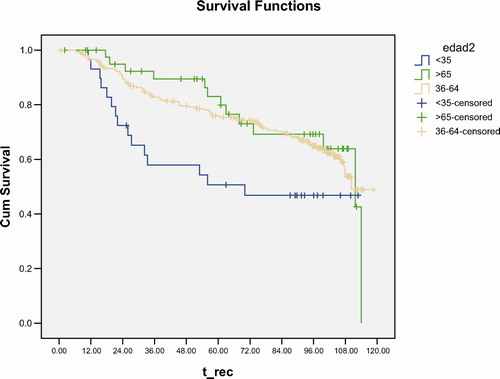
Results: The incidence of granulomatous endometritis in our population, of postmenopausal patients was of 0,28%. The evolution of the patients was satisfactory in cases of fulfilment of the guideline of tuberculostatic treatment (66,6%). The case of xantogranulomatose endometritis, the patient continues asintomatic, and the 2 cases of cancer endometrial of high degree, the patients have died.
This infection is not usual in women. Tubal, endometrial and ovarian localizations are almost always secondary to a focus in another location. This entity is less frequent in postmenopausal women, probably because the atrophic endometrium provides a poor environment for growth of the tuberculosis bacillus.
Conclusion: Definitive diagnosis of genital tuberculosis is culture of the Koch bacillus. A presumptive diagnosis can be made on the basis of granulomas in biopsy and a positive Mantoux test. Treatment is medical and the prognosis is good.
PS-63
ATIPICAL POLIPOID ADENOMYOMA OF ENDOMTRIUM (APA): DIAGNOSTIC AND THERAPEUTIC CONDUCT
Jesús S. Jiménez1, Concha Pérez S1, Carmen Álvarez C1, Cristina González M1, Carmen Guillen G1, Jose L. Muñoz1, Gregorio Lopez G1 and Victoria Bravo V1
1Dept. Obst./Gyn. Hospital 12 Octubre, Madrid, Spain
Objective: Atypical polypoid adenomyoma (APA) is rare benign lesion of the uterus. APA is difficult to distinguish from endometroide adenocarcinoma. In the case presented the diagnosis and therapeutic conduct.
Design & Method: Case report: patient a 45 year old. Menarche 12 years of age. Presented irregular vaginal bleeding. TMM:5-6/30. Gesta 2 Para 2. Physical examination was normal. An ultrasound demonstrated a endometrial polyp (21 × 14 mm) and subserosous myoma (35 mm).
Diagnostic histeroscopy: endometrial polyp was 2,5 cm. and proliferative endometrium.
Diagnostic Biopsy: endometrial polyp.
Results: Surgical hysteroscopy with resectoscope, the result of the pathological anatomy was APA. Follow-up hysteroscopicaly and biopsy every six months without pathological findings.
The differential diagnosis of APA includes : endometrial well differentiated adenocarcinoma; complex hyperplasia; adenofibroma; adenosarcoma and carcinosarcoma.
Atypical polypoid adenomyoma (APA) is rare benign lesion of the uterus, The lesions usually have an exophytic and endophytic component., the epithelial component consists of complex branching endometrial glands with cytological atypia, non epithelial component consist varying proportions of smooth muscle and fibroblasts, which may be mitotically active. Squamous differentiation component is a frequent feature. Clinically APA affects younger women, whereas adenocarcinoma is more often seen in postmenopausal women. The authors concluded that have two classes: *APA with architectural index and *APA of low malignant potential (APA/LMP)
Conclusion: The treatment in patients with APA supports:
1. Conservative treatment of APA with polypectomy hysteroscopic and flow-up for premenopausal.
2. Simple hysterectomy is an option for postmenopausal women or APA-LMP.
PS-64
ADNEXAL MASSES TREATED SURGICALLY IN POSTMENOPAUSAL WOMEN: THE EXPERIENCE OF A TERTIARY CARE CENTRE
R. Ribeiro, S. Figueiredo, P. Manso, R. Passarinho, H. Leite, F. Geraldes, F. Ventura, I. Botto and F. Águas
Bissaya-Barreto Maternity Hospital, Coimbra, Portugal
Introdution and objective: More adnexal masses are being detected in postmenopausal patients, because the increased use of transvaginal ultrasound. Screening studies indicate that 3% to 5% of asymptomatic postmenopausal women will have an adnexal mass confirmed sonographically. Malignant neoplasms are uncommon in younger women, but become more frequent with increasing age (>80% of ovarian cancers occur in women over 50 yr). The aim of this study was to review our experience regarding clinical presentation, management and surgical treatment of adnexal masses at postmenopausal age.
Design & Method: A retrospective review of the records of postmenopausal patients with adnexal mass, treated surgically in a tertiary Hospital, during a 6 year period, from January, 2001 to December, 2006. Postmenopausal status was defined as women older than 45 yr, with at least 12 months of amenorrhea and compatible laboratory studies. We performed data analysis with the programme Statistical Package for the Social Sciences (SPSS) version 15. The chi-square and T student tests were used, when appropriate. A value of p < 0.05 was considered significant.
Results: 75 women were identified. The mean age was 62,29 ± 10,89 years. The majority of patients was asymptomatic (54,7%) and the adnexal masses were detected more often during a routine ultrasound scan (45,3%). Histologic examination revealed benign tumours in 30 cases (40%), borderline tumours in 7 cases (9,3%) and malignant tumours in 38 cases (50,7%). The most frequent benign tumour was serous cystadenoma, whereas the most frequent malignant was cystadecarcinoma. Comparison between benign tumours and malignant tumours showed, respectively: mean size of 6,04 ± 2,16 vs 10,73 ± 5,56cm (p = 0,000); mean serum CA-125 of 13,81 ± 7,36 vs 2777,18 ± 7547,11 (pNS); mean operating time of 82,62 ± 63,12 vs 140,92 ± 55,61 min (p = 0,005) and mean time of hospitalization of 3,62 ± 2,33 vs 7,37 ± 3,63 days (p = 0,002). 11 (36,7%) benign tumours were managed laparoscopically and 19 (18,2%) by laparotomy. All malignant and borderline tumours were managed by laparotomy.
Conclusion: Adnexal masses, in postmenopausal patients, are frequently found in both symptomatic and asymptomatic women. In our experience, the majority of patients (54,7%) was asymptomatic and 45,3% were detected during a routine ultrasound scan, emphasizing the importance of this exam in the screening of this pathology. Benign tumours (40%) were smaller and needed less operating and hospitalization times. 36,7% were managed laparoscopically confirming that, using transvaginal ultrasound and serum CA-125, this treatment is technically feasible and can be performed safetly in non-suspicious postmenopausal adnexal cysts.
PS-65
ATIPICAL DIAGNOSIS OF A MESENQUIMAL UTERINE TUMOR
E. Carballo Alvarez, D. Guedea Murillo, M. J. Cancelo Hidalgo, B. Pérez Mies and J. I. Álvarez de los Heros
Hospital General Y Universitario De Guadalajara, Spain
This is a case of a 54 years old woman without interesting background.
She asked about amenorrhea periods alternated with hipermenorrhea periods. We made her a transvaginal ultrasound where we found a uterus with a giant miomata sized 102 × 88 × 104 mm. She had two small miomatas (14 and 20 mm) in a two years previous ultrasound.
Because of the growth of the miomata we decided to operate on her. Previous of the surgery we realized a hysteroscopy where we watched a 2 cm polyp with anomalous blood vessels. One month later, we made her a surgery hysteroscopy. There we watched a uterine cavity with brain like tissue, necrotic areas and anomalous blood vessels.
We took a biopsy and the result was a high grade messenquimal tumor with muscular differentiated compatible with leiomiosarcoma.
In Computerized Tomography and Magnetic Resonance we watched a big uterine cavity occupied by a neoformative tissue which brought up the serose in the funds. There wasn't extra uterine affectation.
She was realized an abdominal hysterectomy with double anexectomy.
The sarcomas are strange uterine tumors. Leiomiosarcomas are only 30% of uterine sarcomas.
Usually we can't get a diagnosis before surgery. This case is interesting because the diagnosis was made previous to surgery.
PS-66
CLINICAL CHARACTERISTIC AND ULTRASONOGRAPHY, HYSTEROSCOPY AND HYSTOPATHOLOGICAL DATA ON POSTMENOPAUSAL TAMOXIFEN USERS AND ENDOMETRIAL POLYPS
S. R. Botogoski, S. M. R. R. Lima, M. A. L. Galvão, B. F. Reis, P. A. A. G. Ribeiro and T. Aoki
School of Medical Sciences of the Santa Casa of São Paulo, São Paulo, Brazil
Objective: The Selective Estrogen Receptive Modulators (SERMs) are a heterogeneous group of compounds that connect to estrogen receptors and have a specific tissue effect; an agonistic function in some tissues and an anti-agonistic in others. The tamoxifen (TMX) is a SERM used in the adjuvant treatment of women with positive estrogen receptor breast cancer with an anti-agonistic function and might causes an increase in the incidence of endometrium polyps. To analyze the clinical characteristic, ultrasonography, hysteroscopy and hystopathological data in tamoxifen's users and endometrial polyps.
Design & Method: A prospective study with 30 postmenopausal women treated for breast cancer, users of tamoxifen and diagnostic of endometrial polyp by transvaginal ultrasound, surgery hysteroscopy and a hystopathological study, (April 2005 - May 2007). The study was approved by the Ethics Committee on Research.
Results: The average age was 61.7 ± 9.2 years, age of menopause 49.5 ± 4.5 years and time after menopause 12.2 ± 8 years. The time they used the TMX was 25.3 ± 13.6 months. The average endometrial thickness was 15.6 ± 8.1 mm; the uterus volume 104.2 ± 68.6 cm3; the right ovary volume 2.7 ± 2.1 cm3 and the left ovary volume was 2.4 ± 1.6 cm3. As to the endometrial ecotexture, 30 (100%) were heterogeneous. The polyps were found in the diagnostic hysteroscopy and surgery: 9 (30%) in the uterus bottom; 9 (30%) in the posterior wall; 6(20%) in the anterior wall and 6 (20%) in the right side wall and adjacent endometrium: 26(86.6%) low risk hyperplasia endometrial and 4(13.4%) high risk hyperplasia endometrial. The polyps histopathology was: 16 (53.3%) atrophic; 8 (26.7%) atrophic with a TMX related lesion; 4 (13.3%) hyperplasic and 2(6.7%) functional. The adjacent endometrium was: 11 (36, 7%) atrophic epithelium; 8(26.7%) epithelium with a TMX related lesion; 5(16.7%) cystic atrophy epithelium; 2(6.7%) proliferating; 1(3.3%) secretor; 1(3.3%) flaking and 2(6.6%) simple hyperplasia.
Conclusion: The average age was 61 years, the age of menopause was 49.5 years and time of the tamoxifen use was 25 months. The average of the endometrial thickness was 15 mm, and there was an increase uterine volume and ovaries were atrophic. Most of the polyps removed through surgical hysteroscopy were in the uterine bottom and in the posterior wall. The hystopathological analysis showed that most of the polyps were atrophic and the adjacent endometrium was atrophic too.
PS-67
DEMOGRAPHIC CHARACTERISTICS AND FREQUENCY OF CERVICAL LESIONS IN ROUTINE PAPANICOLAU-SMEARS IN PRE- AND POSTMENOPAUSAL WOMEN
A. Augoulea1, I. Lambrinoudaki1, F. Lazaraki3, E. Kada3 and P. Skolarikos2
1Menopause Clinic, 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital, Athens, Greece; 21stDepartment of Obstetrics and Gynecology, “Elena Venizelou” Hospital, Athens, Greece; 3Hormonal and Biochemical Laboratory, “Elena Venizelou” Hospital, Athens, Greece
Introduction: Sociodemographic characteristics, reproductive and sexual history are risk factors for genital dysplasia and cancer.
Objective: Retrospective study of 150 women underwent routine Papanicolau-smear in our clinic during the year 2005. Parity, gravity, number of partners, invasive past cervical treatments and cigarette smoking with grade of cervical lesion, HPV infection, endocervicitis, endocervical hyperplasia and squamous metaplasia.
Results: Cervical lesion was diagnosed in 58,7%, L.G.SIL was diagnosed in 46,7%, H.G.SIL was diagnosed in 10,7% and endocervicitis in 1,3%. HPV positive women were 81,3%, 40% were nulliparus, 97,5% were sexually active, 21,3% had invasive past cervical treatments, 15,3% had one or more abortions, 34,7% were cigarette smokers. Squamous metaplasia was found in 50,7%. There was no correlation in our study between grade of cervical lesion, HPV infection, endocervicitis, endocervical hyperplasia and parity, number of partners, invasive past cervical treatments, number of abortions, number of children and cigarette smoking. Squamous metaplasia exhibited a statistically significant correlation with parity as well with gravity (p < 0,001).
Conclusions: Pregnancy may increase the risk for squamous metaplasia, possibly by leading to a looser cervix.
PS-68
DIAGNOSTIC ACCURACY OF TRANSVAGINAL SONOGRAPHY TO EXCLUDE ENDOMETRIAL PATHOLOGY IN POSTMENOPAUSAL WOMEN
C. Díaz-García, S. Fortuño, N. Roig, D. Oltra, D. Juliá and A. Romeu
University Hospital La Fe, Valencia, Spain
Objective: An introductory To describe prevalence of sonographic findings in a population of postmenopausal women and to determine the accuracy of endometrial thickness measurement with transvaginal ultrasonography (TVUS) to diagnose endometrial characteristics and alterations.
Design & Method: We performed a search in our service records from January 2001 to January 2008. Patients undergoing a hysteroscopy procedure were identified. Sonographic scans, hysteroscopic findings and pathological findings were reviewed. Hysteroscopy examinations were performed using a Betocchi hysteroscope (2,8mm) under cervical anesthesia (Mepivacaïne 3%). Siemens Sonoline Versa Pro ultrasound machine, 6.5 EV13 endo-vaginal probe were used to perform ultrasound examination. Statistical study was performed using SPSS™ 13.0 software.
Results: 3611 postmenopausal women were identified. Mean age was 59,65 ± 9,17 years [26–94y]. Mean age at onset of menopause was 49,34 ± 5,21 years [26–62y]. 448(12,4%) were nullipari. 90(2,5%) had an iatrogenic menopause (bilateral ooforectomy and post-chemotherapy) and less than 1% had early menopause. 96(2,6%) women were treated with tamoxifen and 6(11,7%) estroprogestatives. 168(4,6%) presented abnormal bleeding. 1787 women (49,48%) underwent a TVUS examination performed by a senior sonographist. Main sonography findings were: Endometrial thickness >5 mm: 746(41,7%); myoma 116(6,5%); polyp 241(13,5%); hydrometra 66(3,7%) and adnexal masses 15(0,8%). Sensibility (S), Specificity (E), Positive predictive value (PPV) and Negative predictive value (NPV) were as follow: If endometrial thickness was thicker than 5mm we found S: 45% E: 62% PPV: 61% NPV: 46% for polyps; S: 55% E: 58% PPV: 4,7% NPV: 97,3% for endometrial hyperplasia; S: 50% E: 58% PPV: 3,3% NPV: 97,6% for submucous myoma S: 51,4% E: 58,7% PPV: 5,1% NPV: 96,5% for endometrial carcinoma. This values changes when applied to a genital bleeding population: For endometrial carcinoma we founded S: 100% E: 60% PPV: 6,6% NPV: 100%.
Conclusion: Although TVUS is usefull to obtain information about endometrial processes its accuracy is poor, specially to diagnose benign pathology. It has a very strong NPV to predict absence of malignant endometrial pathology in women with postmenopausal bleeding.
PS-69
E-CADHERIN EXPRESSION IN CERVICAL EPITHELIAL CELLS OF POSTMENOPAUSAL WOMEN: ASSOCIATION WITH HORMONE THERAPY, TIBOLONE AND RALOXIFENE
Vassilios Sioulas1, Sophia Vlachou1, George Christodoulakos1, Irene Lambrinoudaki1, Ekaterini Politi2, Emmanuel Economou3, Theodoros Sergentanis1, Constantinos Panoulis1, Areti Augoulea1, Andreas Alexandrou4 and George Creatsas1
1Menopause Clinic, 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital, Athens, Greece; 2Cytology Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 3Hormonal Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 41st Department of Surgery, University of Athens, Laiko Hospital, Athens, Greece
Objective: To evaluate possible associations between hormonal factors and epithelial cadherin (E-cadherin) expression in cervical epithelial cells from postmenopausal women.
Design: 105 healthy postmenopausal women aged 45–68 years old were investigated in a cross-sectional study. Women were recruited from the Menopause Clinic of the 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieion Hospital. Serum FSH, LH, estradiol, Δ4-androstendione, total testosterone, DHEA-SO4 and SHBG levels were measured. Pap smears derived from current users of 17β-estradiol 1 mg + norethistrone acetate 0.5mg; (E2/NETA, n = 28), tibolone (2.5 mg, n = 23), raloxifene HCL (60 mg, n = 21) or from women not receiving treatment (n = 33). The main outcome measure was E-cadherin immunostaining in squamous, glandular and squamous metaplastic cells, using a semi-quantitative method (rating scale: 0–3).
Results: In glandular cells, there was a marginally positive association of E-cadherin with serum estradiol (p = 0.057) and a negative one with serum FSH (p = 0.033). In metaplastic cells, E-cadherin immunoreactivity was lower in tibolone users (p = 0.037 vs. controls), while HT or raloxifene users did not exhibit differences in E-cadherin expression compared to controls.
Conclusions: Tibolone associated with lower E-cadherin expression in cervical metaplastic cells, while HT did not induce alterations in E-cadherin levels in any type of the examined cells. This finding may be related to the molecular background responsible for the reported lack of association between HT and the incidence of high grade SIL and cervical cancer.
PS-70
ENDOMETRIAL DIAGNOSIS OF PRESURGICAL ATYPICAL HYPERPLASIA VERSUS ENDOMETRIAL CANCER IN THE HYSTERECTOMY PIECE
Jesus S. Jimenez, Carmen Alvarez C, Carmen Guillen G, Cristina Gonzalez M, Gregorio Lopez G, Leticia Muñoz, Laura Marqueta and Alvaro Tejerizo
Dept. Obst./Gyn. Hospital 12 Octubre, Madrid, Spain
Objective: Analyze the correlation between the atypical diagnose pre-surgical of endometrial hyperplasia and endometrium adenocarcinoma in the hysterectomy piece.
Design & Method: Retrospective study of the obtained endometrial biopsies after hysteroscopy, with atypical diagnosis of hyperplasia complex (HCA) of endometrium and its later study piece of hysterectomy in the Unit of “Endometrial Pathology” between 2001 and of 2003. A total of 15 patients. The surgical pieces were sent to the Service of Pathological Anatomy, for their habitual processing.
Results: In 8 cases (53%) that it maintained the diagnosis presurgical, in 7 (47%) showed to the existence of adenocarcinoma endometroide degree I of differentiation. In 3/7 with adenocarcinoma (20%) the miometrial infiltration was verified:
The incidence of endometrial carcinoma in the piece of hysterectomy after the atypical diagnosis of hyperplasia oscillates 15–43% King and Trimble. Our results (47% of endometrial carcinoma after hysterectomy by HCA and 20% of smaller miometrial invasion of 50%).
Conclusion: We raised an active conduct of diagnosis-therapeutic boarding:
Make previous study of extension to the treatment of hyperplasia atypical, with search of miometrial invasion – ecographic transvaginal - abdominopelvic magnetic resonance if there were and the tumorlike marker, Ca-125.
Make a vaginal hysterectomy, attended laparoscopy and peritoneal washing, intraoperating study of the piece and continue treatment in necessary case.
PS-71
ENDOMETRIAL THICKNESS EVALUATED BY HYSTEROSCOPY IN POSTMENOPAUSAL WOMEN
A. P. Domingues, H. Lopes, I. Dias and C. Freire de Oliveira
University Hospitals from Coimbra, Portugal
Introduction: The endometrium progressively atrophies following menopause so that ultrasound measurements of 5 mm or greater in postmenopausal patients not on hormone replacement therapy (HRT) are considered abnormal. Thickening of the endometrium may indicate the presence of pathology.
Objective(s): To evaluate the significance of endometrial thickness in post menopausal women who performed a diagnose hysteroscopy.
Design & Methods: A hysteroscopy database was used to select postmenopausal women who underwent diagnostic hysteroscopy between 2004 and 2007 because transvaginal ultrasound revealed endometrial thickness. Their medical records were reviewed.
Results: Of the 491 cases selected, 45.6% were asymptomatic and 54.4% had postmenopausal vaginal bleeding. The mean age at diagnose was (asymptomatic vs symptomatic) 62.9 ± 8.4 vs 63.3 ± 10.8 years and menopausal mean age was 49.7 ± 4.5 vs 49.2 ± 4.6 years. Hysteroscopy revealed endometrial polyps in 77.1 vs 58.9% of the women, endometrial tumour in 0 vs 16.2%, atrophic endometrium in 8.9 vs 10%, adhesions in 6.3 vs 3.1%, fundic salience in 5.2 vs 3.5%, thickened proliferative endometrium in 0.5 vs 5.7% and submucousal myomas in 0.5 vs 0%. Around 45.3 vs 68.6% of the lesions found were removed with histopathologic diagnosis of mucous polyps in 89.7 vs 60.5% (p < 0.0001), endometrial tumors in 0 vs 22.2% (p < 0.0001), simple hyperplasia in 2.3 vs 3.8%, complex hyperplasia in 0 vs 2.5%, cystic atrophy in 2.3 vs 1.3% and submucousal myoma in 0 vs 1.3%.
Conclusions: Endometrial thickness in post menopausal women should be studied and any lesion found in symptomatic women should be removed. In asymptomatic women regular assessment may be performed.
PS-72
ENDOMETRIAL POLYPS AND RISK OF PREMALIGNANT AND MALIGNANT LESIONS
N. Kiriakopoulos, C. Gavala, I. Aggos and A. Papadopoulou
Ippocratio General Hospital, Kos, Greece
Objective: Endometrial polyps is the most frequent pathology diagnosed during ambulatory hysteroscopies. The purpose of our study is to evaluate the prevalence of premalignant and malignant polyps and their association with peri and postmenopausal status.
Design & Methods: 122 women from 44 to 57 yrs with abnormal uterine bleeding were submitted to diagnostic and operative hysteroscopy in our ambulatory. Histological specimens were sent for biopsy. Arterial hypertensions, diabetes mellitus, obesity, use of hormone therapy or tamoxifen were reported.
Results: 96,75% were endometrial polyps and polyps with simple or complex endometrial hyperplasia without atypia. Polyps with endometrial hyperplasia with atypia were the 2,45% of cases, while 0,8% were carcinomatous polyps. No significant association was found between arterial hypertension, diabetes mellitus, obesity, use of hormone therapy or tamoxifen and premalignancy or malignancy.
Conclusion: The malignat potential of endometrial polyps seems to be low and age- related. Hysteroscopic investigation in postmenopausal women with uterine bleeding can reduce the risk of false negative histopathological results. Hysteroscopy is the most appropriate, effective and safe, method for diagnosis and treatment.
PS-73
ENDOMETRIOID ADENOCARCINOMA OF THE OVARY CO-EXISTING WITH ENDOSALPINGIOSIS IN A PERI-MENOPAUSAL WOMAN
A. Augoulea1, I. Constandinidou2, I. Lambrinoudaki1, A. Stilianidou3, E. Kouri3 and P. Skolarikos2
1Menopause Clinic, 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital, Athens, Greece; 21st Department of Obstetrics and Gynecology, “Elena Venizelou” Hospital, Athens, Greece; 3Pathology Department, “Elena Venizelou” Hospital, Athens, Greece
Background: Endometriosis, endosalpingiosis, and endocervicosis represent non-neoplastic glandular proliferations showing müllerian differentiation and occurring predominantly in pelvic and abdominal tissues. The term “mullerianosis” is used when two type co-exist. These lesions are usually identified at laparotomy. Endosalpingiosis is characterized by the presence of benign glands lined by tubal-type epithelium outside the tubal cavity. The development of malignant tumors is a well-known complication of endometriosis and endosalpingiosis.
Case: The 47-year-old nulliparus woman with a 25 year history of endometriosis underwent laparotomy to investigate symptoms and signs of acute abdomen. A left ovarian 23 cm solid mass with cystic components was found. Blueberry spots in vesicouterine pouch and posterior cul-de-sac obliteration were observed as well during surgery. Histological examination revealed left ovarian endometrioid adenocarcinoma co-existing with endosalpingiosis. The histologic type was endometrioid adenocarcinoma with a clear cell pattern. The uterus, right tube and ovary were disease free. The omentum, para-aortic lymph nodes and appendix were also negative. The relationship between endometriosis, endosalpigiosis and cancer suggest careful assessment of the peri-menopausal woman.
PS-74
ENDOMETRIUM EVALUATION FOR IRREGULAR BLEEDING IN POSTMENOPAUSE
Iuliana Ceausu1,2, Al. Ciulcu2, H. Rahimian2 and D. Hudita1,2
1“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; 2“Dr. I. Cantacuzino” Hospital, Bucharest, Romania
Objective: The aim of this study was to compare the efficacy of blind endometrial biopsy by Pipelle with that of histeroscopic biopsy with biopsy forceps under direct view.
Design & Methods: The study included 46 postmenopausal women in the gynecology department of the “Dr. I. Cantacuzino” Hospital selected for endometrial biopsy because of irregular bleedings in menopause or for endometrial thickness 4–6 mm on transvaginal ultrasound. All women were between 45 and 70 years, at least after one year without any menstrual bleedings and without hormonal therapy.
Results: All women undergo biopsy with Pipelle and in 24 cases the results indicated endometrial hyperplasia, 18 with atrophy, 2 polyps and 2 case with insufficient tissue sample. The hysteroscopy was performed after 4 weeks from the first biopsy, and enabled a selective biopsy of the areas of visualized endometrium. The results were 28 hyperplasia, 8 polyps and 10 atrophic endometrium. The rate of confirmation rate for polyps by Pipelle was 1 to 4, the rest of 3 polyps were initially considered atrophy (4 cases) or hyperplasia without atypia (2 cases). Also, 6 cases of initially considered atrophy were discovered with simple hyperplasia without athypia, and in 6 cases of simple hyperplasia it was discovered a complex hyperplasia without athypia. The conformity rate calculated by analysis between blind and under direct visual control biopsy for hyperplasic endometrium was 84,61%.
Conclusion: Histeroscopic biopsy under visual control is necessary at least for the patients with any hyperplasic changes at the blind biopsy.
PS-75
EXPRESSION OF ANGIOGENESIS MARKERS AND MODULATORS IN PRE-, PERI- AND POSTMENOPAUSAL WOMEN WITH OVARIAN CANCER
W. Bednarek, B. Barczyński, J. C. Kotarski, I. Wertel and J. Kotarski
Medical University of Lublin, Lublin, Poland
Objective: One of the most commonly investigated angiogenesis markers in ovarian cancer is microvessel density (MVD). It is usually assessed immunohistochemically according to Weidner et al. (1991) on the basis of specific endothelial antigen expression (CD31, CD34, CD105, LM609) in the areas of the greatest concentration of blood vessels (hotspots). Additionally several other angiogenesis modulators are investigated, including growth factors, different proteases and their inhibitors, oncogenes and suppressor genes. The aim of the study was to assess if there are any differences in ovarian cancer angiogenesis markers and modulators expression in patients with different menopausal status.
Design & Method: 100 women aged 30–70 years old (median 52 years), treated due to ovarian cancer (FIGO I–IV) were included in the study; 22 of them were premenopausal (group I), 31 were perimenopausal (group II) and 47 were postmenopausal (group III). MVD was assessed on the basis of CD34 (MVDCD34) and CD105 (MVDCD105) expression. In addition, tumor tissue expression of P53 protein and EGF receptor (EGFR) was investigated. Active EGF receptor form and soluble VEGF receptor form (sVEGF-R1) was assessed with the use of ELISA assay procedure in blood serum of patients before debulking surgery.
Results: In the study group, the median value of MVDCD34 was 48.0/HPF and ranged from 10.3/HPF to 163.4/HPF. The results were comparable in groups I–III (p>0.05). The median value of MVDCD105 was 31.4/HPF (range from 10.3/HPF to over 100/HPF). Similarly, the results did not show any differences in groups I–III (p>0.05). P53 protein nuclear expression was found in 41 cases (59 cases showed lack of P53 protein expression). The frequency of P53 expression was similar in groups I–III (p>0.05). Lack of EGFR expression was found in 56 cases (44 women showed moderate or strong EGFR expression) and the results did not differ in the study groups (p>0.05). Finally, neither EGFR nor sVEGF-R1 serum concentration showed significant changes in the study groups (p>0.05).
Conclusion: The expression of angiogenesis markers and modulators is similar in pre-, peri- and postmenopausal patients with ovarian cancer. Our data indicate that ovarian cancer angiogenesis is not dependent on the menopausal status of patients.
PS-76
HORMONAL FUNCTION AFTER OVARIAN TRANSPOSITION IN CERVICAL CANCER PATIENTS
Y. Machado, A. Lubrano, O. Arencibia, N. Medina, V. Benito, J. M. Falcón Santana and O. Falcón
Objetive: Ovarian tranposition, out of the minor pelvis, was described for the first time by Mc Call et al in 1958 for patients treated with cervical cancer that procedure to preserve the ovarian function in young premenopausic women and avoid castration for radiotherapy.
The aims was to assess the functional outcome after ovarian transposition followed by radiation therapy.
Design and Methods: From January 1996 to December 2007, 15 patients in our institution underwent ovarian transposition during surgical treatment of cervical cancer (radical hysterectomy with lymphadenectomy). Ovarian transposition was performed when the ovaries looked macroscopically normal, they were transposed bilaterally to the paracolic gutters at the level of the aortic bifurcation. Three metallic clips were applied to each transposed ovary to be identified by subsequent x-ray localization. Postoperative treatment was administered in the patients with metastatic lymph nodes, invasion of the surgical margins or with parametrial lymphovascular space involvement, who received external irradiation, brachytherapy and cisplatin. Ovarian function was assessed by measurement of gonadotropin and E2 levels 6 months after the transposition considering normally preserved when the FSH level was <10 mIU/mL, E2 was >50 pg/mL.
Results: The median age of the patients was 37 years (range, 30–47 years). 14 patients in stage IB1 and one patient in stage IA1.Nine patients were treated for adenocarcinoma and six patients were treated for squamous cell carcinoma. Only one case received radiation therapy. Ovarian function was preserved in 86.6% of the patients (13/15). One case of menopausal patient, wich was the oldest patient (47 years old). No complications of ovarian transposition were observed. None patient presented ovarian metastasis nor ovarian cysts.
Conclusion: Ovarian transposition is a safe and effective procedure for preserving ovarian function in patients treated by radical hysterectomy in cervical cancer.
PS-77
HORMONAL REPLACEMENT THERAPY AND GYNECOLOGICAL CANCER
R. Passarinho, M. G. Castro, R. Ribeiro, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Maternidade Bissaya-Barreto, Coimbra, Portugal
Objective: Many women are already in menopause when treated for a gynecological cancer, while other younger patients will go into an early menopause due to ovarian function ablation through surgery (oophorectomy), radiotherapy or chemotherapy, worsening their quality of life by menopause symptoms and increasing the long-term risk of osteoporosis and cardiovascular disease.
The main purpose of this work was to review the clinical evidence in favour and against hormonal replacement therapy (HRT) use in gynecological cancer survivors.
Design & Method: Retrospective study of 10 women with a history of cervical, endometrial, tubal and ovarian cancer diagnosed between 1991 and 2006 and checked-up annually, at our department, until the end of 2007. The following parameters were analysed: age, menarche, menopause, gynaecological cancer type, disease stage, and their treatment, menopause symptoms, HRT use and tumour recurrence.
Results: The mean age of the patients was 51,6 years, with a median menopause at 43 years (20% spontaneous, 50% surgical and 30% iatrogenic). The types of gynecological cancer found was: squamous cervical cancer (40%), cervical adenocarcinoma (10%), endometrial carcinoma (20%), tubal adenocarcinoma (10%), ovarian adenocarcinoma (20%), endometrioid ovarian cancer (10%) and breast angiosarcoma (10%). The HRT was used in every case after a mean time of 50 months after cancer treatment, during a mean time of 67 months, with a global improvement of vasomotor symptoms. There was not tumour recurrence after a mean follow-up of 8,5 years.
Conclusion: It is still controversial whether patients with a history of gynecological cancer can be prescribed HRT, but appears that there is no clinical evidence that HRT use increases their recurrence risk. Yet it should be provided to these women, since estrogen deficiency can be responsible for severe menopause symptoms and long-term consequences on the incidence of osteoporosis and cardiovascular disease. Breast angiosarcoma, cervical, tubal and ovarian cancers are not estrogen dependent conditions and estrogen replacement is not contraindicated. However there is some doubt related to endometrioid ovarian cancer and endometrial carcinoma. Most of the authors suggest that HRT may be used in symptomatic women after adequate information about risks and benefits.
PS-78
HYSTEROSCOPIC EVALUATION OF POSTMENOPAUSAL ENDOMETRIAL PATHOLOGY
C. Braña Pelayo, M. Cañamares Martín, M. Uriel Calvo and J. Calleja
Hospital Fundación Jiménez Díaz, Madrid, Spain
Objective: To estimate the occurrence of malignancy, typical and atypical hyperplasia and endometrial polyps in postmenopausal women who underwent diagnostic hysteroscopy and curettage.
Design & Method: Retrospective study and descriptive analysis was done. Gynaecology Department database was used to identify all patients who were treated by hysteroscopy and resection of endometrial tissue in our department from January 1, 2007 to January 1, 2008.
Parameters like age, menopausal status, postmenopausal bleeding, ultrasound evaluation of endometrium as well as histologic diagnosis were documented.
A hundred fifty eight hysteroscopies were done among this period, only postmenopausal women (58.86%) were included in the analysis
Results: Ninety-three (58.86%) were postmenopausal women, forty one (44.08%) of them had no symptoms, and fifty-two (55.91%) had postmenopausal bleeding.
Prevalence of benign polyps was 50% in symptomatic women and 65.85% in those without symptoms. The prevalence of malignancy histology was 9.61% in women with symptoms and there isn't any case in asymptomatic women.
Conclusion: The most frequent histologic diagnosis in postmenopausal women, with or without symptoms, who underwent histeroscopy and curettage, was benign polyps. No carcinoma, typical or atypical hyperplasia was founded in asymptomatic women in our database.
All asymptomatic women who underwent histeroscopy because of the ultrasound inclusion criteria were diagnosed of benign processes.
PS-79
HIGH PARITY IS ASSOCIATED WITH FAINT E-CADHERIN EXPRESSION IN SQUAMOUS CERVICAL EPITHELIAL CELLS IN POSTMENOPAUSAL WOMEN
Vasileios Sioulas1, Fotini Galapi1, Irene Lambrinoudaki1, George Christodoulakos1, Ekaterini Politi2, Theodoros Sergentanis1, Constantinos Panoulis1, Andreas Alexandrou3, George Kaparos4, Areti Augoulea1, Maria Creatsa1 and Constantinos Papadias1
1Menopause Clinic, 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital, Athens, Greece; 2Cytology Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 31st Department of Surgery, University of Athens, Laiko Hospital, Athens, Greece; 4Biochemical Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece
Objective: Epithelial cadherin (E-cadherin), a transmembrane glycoprotein, is involved in calcium-dependent homophilic cell-cell adhesion and is considered to be a critical molecule in cervical carcinogenesis. However, E-cadherin expression and putatively implicated predictors in healthy women are still under further investigation. The aim of this study is to evaluate the possible associations between E-cadherin expression and reproductive/lifestyle factors in cervical epithelial cells from postmenopausal women.
Methods: 105 healthy postmenopausal women (aged 45–68 years old) were recruited in this cross-sectional study from the Menopause Clinic of the 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieion Hospital. Pap smears were derived and E-cadherin immunostaining was evaluated in squamous, glandular and squamous metaplastic cells, using a semi-quantitative method (rating scale: 0–3). Reproductive and lifestyle and factors were obtained from patient's chart review. Information about lifestyle parameters and gynecological-obstetric history was obtained from patient's chart review.
Results: In squamous cells, women with history of 0–1 deliveries presented with higher score vs. women with 2–4 deliveries (p = 0.003). E-cadherin immunostaining score in squamous cells was higher among social drinkers and women drinking alcohol daily vs. non-drinkers (0.96 ± 0.72 vs. 0.56 ± 0.65, p = 0.004). Higher dietary calcium intake was marginally associated with lower staining score in squamous cells (0.94 ± 0.78 for low, 0.71 ± 0.70 for average, 0.45 ± 0.52 for high consumption, p = 0.073).
Conclusions: Association is observed between E-cadherin and reproductive history and lifestyle habits in squamous cervical cells from healthy postmenopausal women. Parity is a well-established risk factor for cervical cancer and E-cadherin might play a part in the molecular mechanisms of carcinogenesis.
PS-80
HYSTEROSCOPIC DIAGNOSE IN MENOPAUSE WOMEN
A. Candela, J. A. López Fernández, L. Vaquer, F. Dieguez, J. Marcos, N. Esteve, A. Saco and J. C. Martinez
Hospital General Universitario Alicante, Spain
Objectives: To evaluate both the indications and diagnoses made by hysteroscopy and the probability of each diagnosis depending on the indication.
Material Methods: Retrospective analysis of 4416 patients who experienced a hysteroscopy from January 2000 to November 2007 at the outpatient service of the Hospital General Universitario de Alicante (Spain). Data from a base in Access 2003 were analysed with SPSS 12th Spanish version. We evaluated diagnose frequency, reasons for consultation and its sensitivity (S), specificity (E), positive predictive value (PPV) and negative (NPV) for endometrial hyperplasia and endometrial cancer.
Results: The average age of patients was 48 years (range: 15–90). Methrorragia (43 percent) and Suspected ultrasound disease in asymptomatic patients (27 percent), were both the most usual reasons for consultation. Endometrial polyp (35 percent) was the most frequent diagnosis, followed by normal finding (27 percent). One hundred and twenty two endometrial cancers were diagnosed (2.8 percent) and ninety nine hyperplasia (2.2 percent). In menopause women with methrorragia, 44 percent showed endometrial polyps, 2.8 percent demonstrated endometrial cancer and 8.8 percent presented endometrial hyperplasia. In asymptomatic patients with suspected ultrasound disease (endometrial thickness bigger than 4 milimeters) we found 59 percent polyps, 1 percent hyperplasia and 1.4 percent cancer. In menopause women metrorrhagia introduced S: 86 percent, E: 48.8 percent, PPV: 12.6 percent and VPN: 97.6 percent for the diagnosis of endometrial cancer or hyperplasia.
Conclusions: Endometrial polyps represented the most frequent pathology as Hysteroscopic finding in patients before and after menopause. Endometrial hyperplasia and cancer were very unlikely in asyntomatic patients. In the present study, the ultrasonic finding alone, leaded to endometrial benign diagnoses.
PS-81
HYSTEROSCOPY AND MENOPAUSE: STUDY OF ENDOMETRIAL PATHOLOGY
M. Brik, A. Pérez-Calvo, N. Roig Casabán, D. Oltra, L. Ortega and M. D. Juliá
University La Fe Hospital. Valencian Regional Government Ministries of Health, Valencia, Valencia, Spain
Objective: To study endometrial findings in peri- and postmenopausal women, and to analyze the role of hysteroscopy in diagnosis of related conditions.
Design and Method: Retrospective study from January 2004 until January 2005, including 342 women, older than 45 years. They were under a diagnostic hysteroscopy procedure at the Day Surgery Unit of Hospital La Fe (Valencia). Patients mean age was 57.72 ± 9.67 (45–90) years; 47.52% (163/343) were menopausal women; menopause beginning mean age was 49.67 ± 3.84 years. Mean BMI was 28.96 ± 6.67. The indication of performing a hysteroscopy was established in 79.3% of the cases due to previous transvaginal scan, in 18.6% of the cases due to uterine bleeding and in 2.1% of the cases due to malignancy suspicion (previous endometrial biopsy).
Betocchi hysteroscope 2.8 mm optic, for oblique vision 30° was used and previous paracervical anesthesia (lidocain and mepivacain) was injected. Different variables were studied: previous scan, indication, hysteroscopic diagnosis of polyps, myomas, and malignancy suspicion findings and the correlation with pathology results. Scissors were used in 59.8% of the cases, Versapoint bipolar current in 31.2% of the cases and both method in 9%. Statistical study was performed using SPSS 13.0 program.
Results: In hysteroscopic endometrial study, 6.6% (22/342) showed malignancy suspicion finding, 24.6% (82/342) secretor endometrium, 10.8% (36/342) proliferative endometrium and 6.3%(21/342) glandulocystic atrophy. 90.1% (308/342) presented an image of polyp and 12.6% (43/342) of myoma. In 94.5% of the cases histological material was obtained, being diagnose of: 75.1% (257/342) polyp, 9.1% (31/342) myoma, 5.6% (19/342) hyperplasia y 0.6% (2/342) adenocarcinoma of endometrium. For polyp diagnose, hysteroscopy showed a sensibility (S): 96.53% and specifity (E): 33.33%; and for malignancy suspicion diagnose: S: 30% and E: 95%.
Conclusions: The main endometrial finding during peri and postmenopause is the endometrial polyp. There is a correlation between hysteroscopic findings and pathology results, even in malignancy suspicion pathology.
PS-82
HYSTEROSCOPY IN THE DIAGNOSIS OF POSTMENOPAUSAL BLEEDING
A. Figueiredo, G. Gomes, T. Paula, A. Fatela, D. Rosa and A. Martins
Maternidade Dr. Alfredo da Costa, Lisboa, Portugal
Background: Postmenopausal bleeding (PMB) accounts for 5% of gynaecology referrals. In 15% of women it represents the first symptom of endometrial cancer. Therefore any abnormal PMB should be carefully investigated.
Objective: To evaluate the diagnostic accuracy of hysteroscopy in the detection of endometrial cancer in women with PMB.
Design & Methods: Retrospective study of 31 women referred to Maternidade Dr. Alfredo da Costa in the first trimester of 2007 for PMB. All women included in the study underwent hysteroscopy and were submitted to directed biopsy during the procedure. Hysteroscopy findings were classified as normal endometrium, atrophic endometrium, focal abnormality (benign or suspicious) and diffuse thickening (benign or suspicious). Data was compared with the histological diagnosis.
Results: Among the 31 women enrolled in the study, 2 were excluded because hysteroscopy was impossible. Polyps were the most frequent hysteroscopic finding (n = 21, 72,4%), being suspicious in 3 cases (10,3%), followed by diffuse thickening (n = 5, 17,2%); being suspicious in 3 cases (10,3%), atrophic endometrium (n = 2, 6,9%) and normal endometrium (n = 1, 3,5%). The histological diagnosis were normal endometrium in one (3,5%), atrophy in two (6,9%), polyps in seventeen (58,6%), endometrial hyperplasia in one (3,5%), endometrial adenocarcinoma in seven (24%) and endometrial sarcoma in one (3,5%). For the assessment of endometrial carcinoma, hysteroscopy revealed sensitivity of 62,5%, specificity of 95,2%, positive predictive value of 83,3% and negative predictive value of 86,9%.
Conclusion: This study revealed that hysteroscopy is a technique with high accuracy for the diagnosis of endometrial cancer. Hysteroscopy with biopsy is currently the gold standard for evaluation of women with PMB as it is a safe and simple procedure and allows simultaneously the diagnosis and treatment of endometrial pathology.
PS-83
LEVONORGESTREL INTRAUTERINE DEVICE IN THE TREATMENT OF SIMPLE ENDOMETRIAL HYPERPLASIA COMPARED TO MEDROXIPROGESTERONE ACETATE: A MULTICENTER DOUBLE BLIND RANDOMIZED STUDY
A. Arango1, J. Garcia2, G. Hernandez1, N. Posada2, C. Henao3 and J. Gómez1
1CES University, Medellín, Antioquia, Colombia; 2Antioquia's Institute of Reproductive Medicine, INSER, Medellín, Antioquia, Colombia; 3Medellín General Hospital, Medellín, Antioquia, Colombia
Objective: To evaluate the effectiveness and side effects of the levonorgestrel intrauterine device (IUD-LNG) compared to medroxiprogesterone acetate given orally (MPA-O) or intramuscularly (MPA-M) in the treatment of endometrial hyperplasia (EH) without atypias.
Design and Method: Comparative, randomized, evaluator-blinded study.
Setting: Gynecologic clinic.
Patient(s): 97 women with histological diagnosis of EH without atypias aged 35 to 50 years recruited during 2003–2006.
Intervention (s): Group I (n = 32 women) received IUD-LNG; group II (n = 33) received MPA-M 150 mg monthly for three consecutive months; group III (n = 33) received MPA-O, 10 mg/day for ten days during three consecutive months. All patients were followed during one year and evaluated at 4, 8 and 12 months after study entry with endometrial biopsy and transvaginal pelvic ultrasound.
Main Outcome Measures: Endometrial histological evaluation, endometrial thickness, patient treatment acceptance, treatment side effects and need for hysterectomy.
Continuous variables were described as the mean ± standard deviation (SD) and categorical variables as proportions with confidence intervals (CI).
Statistical evaluation was done with the Krusskall-Wallis, Wilcoxon and Mc Nemar tests to compare the different treatment modalities. P < 0.05 was considered statistically significant. Data was processed with SPSS 15® software.
Result(s): There was no statistical difference between study group characteristics. During follow up, Group I did not present any cases of endometrial hyperplasia compared with Groups II and III (P < 0.05).
There was an 85.7% reduction in the absolute risk of persistent or recurrent endometrial hyperplasia in Group I compared to Group III (95% CI: 72.7–98.68), and 36% compared to Group II (MPA-M, 95% CI: 17.18–54.82) with a NNT = 1 and 3 at 12 months, respectively.
The endometrial thickness was significantly greater in Groups II and III, compared to Group I, at 4 and 8 months (P < 0.05), but not at 12 months after study entry.
Side effects consistent of abnormal uterine bleeding and weight gain were more frequent in groups II and III compared to the Group I (P < 0.05) and patient treatment acceptance was greater in Group I (P < 0.05). Finally, the percentage of women requiring hysterectomy was significantly greater in Groups II and III (20% and 14%, respectively), compared to Group I (3%, P < 0.05).
Conclusion(s): IUD-LNG is an effective treatment alternative for endometrial hyperplasia without atypias, with less frequent side effects and better patient acceptance then conventional treatment regimens with MPA.
PS-84
OCCURRENCE OF ENDOMETRIAL CANCER 6 YEARS AFTER TREATMENT WITH THERMACHOICE®
A. Le Marrec, H. Duval, K. Morcel, M.-L. Novello and J. Levêque
CHU Anne de Bretagne-16 Boulevard de Bulgarie, BP 90 347 F-35 203 Rennes Cedex, France
Objective: First case described of endometrial cancer occurring six years after treatment with Thermachoice®.
Design and Method: A patient of 48 years of age presented with metrorrhagia diagnosed as functional after normal hysterosonography examination. She had a personal history of bilateral breast cancer treated with mastectomy and axillary lymph node dissection, and breast-conserving surgery without adjuvant hormone therapy. A hysteroscopy (revealing a normal uterine cavity) was performed with biopsy-curettage (endometrium in proliferative phase without atypia) and she underwent Thermachoice® therapy (controlled 83°C intracavitary heating of the uterus for 8 minutes using a balloon technique). Metrorrhagia recurred 6 years later during the perimenopausal period. A hysterosonography examination revealed an endometrial/uterine polyp, a submucous myoma and an irregular thickening of the uterine fundus confirmed by hysteroscopy. The biopsy-curettage revealed atypical endometrial hyperplasia with a few clusters of grade 2 endometrioid endometrial adenocarcinoma cells. Treatment consisted of Piver type I hysterectomy with pelvic lymph node dissection. The final histological examination revealed a FIGO stage IA, grade 2 endometrioid adenocarcinoma without lymph node involvement and with negative peritoneal cytology associated with atypical endometrial epithelial hyperplasia lesions.
Results: This is the first case of endometrial adenocarcinoma to have occurred de novo after Thermachoice®, as witnessed by the negative curettage 6 years earlier and the existence of associated atypical hyperplasia lesions. The occurrence of cancer cells in the uterine fundus, which is particularly accessible to the Thermachoice® system, shows that complete endometrial thermoablation was not achieved. Furthermore, the occurrence of endometrial cancer in young women led to a search on the specimen for an RER phenotype suggestive of Lynch II syndrome.
Conclusion: Thermachoice® is an effective treatment for functional metrorrhagia but it should not be considered to prevent endometrial cancer.
PS-85
OXIDATIVE STRESS IN ENDOMETRIAL HYPERPLASIAS
J. Arbués, M. A. Gomez-Zubeldia, A. Perez, A. García and J. C. Millan
“12 De Octubre” Hospital, Madrid, Spain
Reactive oxygen species (ROS) seem to be involved in the onset and promotion of carcinogenesis. In 80% of cases of endometrial adenocarcinoma type I, a clear association exists with endometrial hyperplasias, which are considered key factors in the endometrial oncological spectrum. The presence or not of atypical cells determines oncological potential.
Objetive: This study explores the behavior of oxidative stress (catalase and malondialdehyde) in endometrial hyperplasias (with or without atypical cells), by comparing it to the oxidative stress existent in both the proliferative and secretory phases.
Desing: Endometrial specimens from 55 women were used, 32 of which were histologically diagnosed as physiological (17 proliferative and 15 secretory endometria), and 23 as endometrial hyperplasias (18 non-atypical and 5 atypical endometrial hyperplasias).
Results: Significant differences were found in the malondialdehyde variable between the proliferative endometria and the endometria with atypical hyperplasia (p = 0.0208), and between both types of endometrial hyperplasias (p = 0.0441). The other comparisons were not stastically significant. No changes in catalase activity were observed.
Conclusion: Our findings seem to suggest that the presence of atypical cells in endometrial hyperplasias induces a reduction in lipid peroxidation, which could permit survival and growth of these cells. This possible diminishing of lipid peroxidation does not seem to be mediated by an increase in endometrial catalase activity.
PS-86
IMMUNOHISTOCHEMICAL AND MORPHOMETRIC ANALYSIS OF THE P53 AND P21 PROTEINS IN POLYPS AND ADJACENT ENDOMETRIUM ON POSTMENOPAUSAL USERS OF TAMOXIFEN
S. R. Botogoski, S. M. R. R. Lima, M. A. L. Galvão, B. F. Reis, P. A. A. G. Ribeiro and T. Aoki
School of Medical Sciences of the Santa Casa de São Paulo, São Paulo, Brazil
Objective: Tamoxifen (TMX) is used as adjuvant treatment of breast cancer with positive estrogen receptor and might causes an increase occurrence of polyps and endometrial neoplasia. The p53 and p21 proteins, whenever increased, inhibit the complex cyclin D and E, thus interfering in the activity and stop the cell in the beginning phase (G1) of the cellular cycle. To verify and compare the effects of the p53 and p21 proteins in endometrial polyps and adjacent endometrium of postmenopausal women by immunohistochemical and morphometric study.
Design & Method: A prospective study was carried out with 30 postmenopausal women treated for breast cancer, tamoxifen's users, with a diagnostic of endometrial polyp suspect by transvaginal ultrasonography and proven by diagnostic hysteroscopy, surgery and hystopathological study (April 2005- May 2007). A comparative immunohistochemical and morphometric study of the p53 and p21 proteins in polyps and adjacent endometrium was also carried out. The study was approved by the Ethics Committee on Research.
Results: The average age was 61.7 ± 9.2 years, age of menopause 49.5 ± 4.5 years. The average of the endometrium thickness was 15.6 ± 8.1 mm; the uterine volume was 104.2 ± 68.6 cm3; the volume of the right ovary was 2.7 ± 2.1 cm3 and the volume of the left ovary was 2.4 ± 1.6 cm3. As to the endometrial ecotexture, 30 (100%) were heterogeneous. The polyps were removed by diagnostic hysteroscopy and surgery: 9 (30%) was in uterine bottom; 9 (30%) posterior wall; 6 (20%) anterior wall and 6 (20%) on the right side wall. The average concentration of immunocolored cells of the p53 protein in the glandular epithelium polyp was 3.23 ± 3.39 cell/mm2 and the stroma were no immunocolored cells. The average concentration of immunocolored cells of the p53 protein and in the glandular epithelium adjacent endometrium was 1.90 ± 1.80 cel/mm2 and stroma and there were no immunocolored cells. For p21 in the glandular epithelium polyp was 23.53 ± 20.99 and stroma 15.93 ± 14.81 cell/mm2. In the adjacent endometrium the glandular epithelium was 11.93 ± 16.86 and stroma 7.47 ± 11.15 cell/mm2.
Conclusion: We have verified that there was significant statistical difference of the p53 protein in the polyp glandular epithelium, while there was none in the p21 protein when compared to the endometrium. We have not verified a significant difference when we compared the stroma of the polyp and of the adjacent endometrium.
PS-87
P53 CODON 72 POLYMORPHISMS AND SUSCEPTIBILITY TO ENDOMETRIAL CANCER
Arianna Adorati Menegato
Department Of Obstetrics And Gynecology; University Of Udine, Italy
Objective: Endometrial cancer (EC) is the most common gynaecological malignancy, especially in the postmenopausal status. Recent studies revealed that several genetic changes including alterations to the p53 gene have occurred in endometrial carcinomas. p53 is an oncosoppressor gene (cr. 17) encoding for a multifunctional protein which plays a critical role in the regulation of cellular proliferation and in the maintenance of DNA integrity.
The purpose of this study was to investigate whether p53 codon 72 polymorphism is associated with an increased risk for EC in a caucasical postmenopausal population.
Design & Methods: This is a case-control study that analyses the allelic frequenty of codon 72 of P53, using polymerase chain reaction and restriction fragment length polymorphism techniques (PCR-RFLP).
The study population consists of 113 postmenopausal women: 62 endometrial cancer and 51 healthy patients.
Results: The genetic analysis showed in the healthy population a higher incidence of the homozygous genotype Pro/Pro of p53 codon 72 (p = 0,0402), when compared with genotype Arg/Arg + Arg/Pro.
Conclusions: Homozygous Pro at codon 72 of the p53 gene may be a genetically trasmitted protective factor for EC in postmenopausal women.
PS-88:Abstract not available at time of going to press.
PS-89
POSTMENOPAUSAL HIRSUTISM AND LEYDIG CELL TUMORS
C. Díaz-García, S. Fortuño, M. Telenti, A. Martín, D. Juliá, L. Ortega and A. Romeu
University Hospital La Fe, Valencia, Spain
Objective: Leydig cells from ovarian struma can be the origin of virilizing tumors in postmenopausal women although they are extraordinary. They produce high testosterone serum levels and classical clinical features described are hirsutism, virilization and metrorrhagia. Endometrial carcinoma has been associated to these kinds of tumors. Differential diagnosis has to be made: ovarian hyperthecosis and androgen non-producing tumors which cause stimulation of ovarian struma can cause a similar clinical picture. The aim of this study is to describe clinical and hormonal pattern of this kind of tumors in postmenopausal women.
Design & Method: We performed a search in our service records from 1975 to 2007. Hirsutism was identified as a clinical diagnose. Every pathology record was revised and 4 women with histological confirmation of Leydig cell tumors were found.
Results: The mean age of our patients was 60,75 ± 3,7 years (all menopausal). Clinical features were as follow: Two of them presented hirsutism, one hirsutism and alopecia and the last one postmenopausal metrorrhagia. First symptoms appeared between 7 and 28 years after instauration of menopause, and the time between onset of symptoms and diagnosis was 5,7 ± 3,4 months [3–10]. Physical examination showed hirsutism (Ferriman = 30) and alopecia in 2 patients; hirsutism, alopecia and metrorrhagia in other patient and the last one had just facial hair growth. No other virilization signs were found. Total testosterone levels were high in every woman. 3 of them had values up to 2ng/ml. Androstendione, free testosterone, and androgen-free index were also high; in the other hand SHBG was always low. S-DHEA was high in just one patient and 17-hydroxyprogesterone in three of them. Cortisol levels were normal and functional tests were inconclusive. Pelvic sonography and suprarenal TC were performed: An ovarian tumor was identified in two patients, and endometrial hyperplasia in other. No suprarenal mass was found. Hysterectomy and bilateral salpingooforectomy was performed in all the patients. Androgen levels became normal after surgery and clinical features were no longer present after 1 year. Pathology findings confirmed diagnosis.
Conclusion: Moderate hirsutism can be found in postmenopausal women, usually associated to hyperthecosis and hyperinsulinemia. However progressive clinical hirsutism should make us suspect a neoplasic origin especially with testosterone plasma levels up to 2ng/ml. Echography and TC play an important role in diagnosis and functional tests seem useless.
PS-90
POSTMENOPAUSAL STATUS, HYPERTENSION AND OBESITY AS RISK FACTORS FOR MALIGNANT TRANSFORMATION IN ENDOMETRIAL POLYPS
A. Gomes1, G. Carvalho1, C. Frutuoso1, C. Marinho2 and C. F. de Oliveira1
1Ginecology Department, Coimbra University Hospital; 2Pathology Department of Coimbra University Hospital
Objective: To review risk factors, clinical presentation, diagnostic methods, and histopathologic findings in cases of endometrial cancer arising in polyps.
Methods: The surgical pathology files of the Pathology Department of Coimbra University Hospital were searched for cases of endometrial polyps with nests of endometrial carcinomas, from the years 2000–2007 and a descriptive, retrospective study was made. Endometrial cancer arising in polyps occurred in 16 patients during this period.
Results: Patients had a mean age of 69 years. All except one woman were postmenopausal. The majority of our patients with malignant endometrial polyps had risk factors for the development of endometrial carcinoma such as hypertension and obesity (mean BMI: 30). Three breast cancer patients were currently given tamoxifen. Methrorrhagia was the presenting symptom in 88% of cases, although 22% of patients were asymptomatic at the time of diagnosis. Ultrasonography performed in 13 patients showed images compatible with an endometrial polyp in 25% of cases. The median endometrial thickness was 11 mm (range 4–33 mm). In 14 patients, diagnostic hysteroscopy was performed. Diagnosis was made by hysteroscopic endometrial sampling in 10 patients and by hysteroscopic surgical ressection in 3 patients. Endometrial carcinoma was incidentally found in the surgical specimen in 3 patients. Endometrioid carcinoma was found in 81% of cases and serous papillary in 19%. FIGO Stage IA was found in 63% of patients, and Stage IB was found in 31%.
Conclusions: Postmenopausal status, hypertension and obesity could all be considered as risk factors for carcinomatous transformation within endometrial polyps in women without a history of breast carcinoma and Tamoxifen treatment. Endometrial carcinoma arising in endometrial polyps is an early endometrial carcinoma with good prognosis, except for papillary serous carcinoma, which can be associated with multiple omental involvement, despite low stage of development in the uterus. Postmenopausal women with endometrial polyps diagnosed by ultrasonography should undergo directed biopsies under hysteroscopic vision. The present series confirms the good prognosis of endometrial cancer arising in polyps.
PS-91
RELATIONSHIP BETWEEN HPV-ONCOTEC® RESULTS AND VIRAL SEROTYPES DETERMINED BY PCR IN PERI AND POSTMENOPAUSAL WOMEN
S. P. González Rodríguez1, A. E. Henríquez Linares2, R. Sainz de la Cuesta2, M. D. Ojeda Jabardo1 and M. Cantarero Bandrés1
1Gabinete Médico Velázquez, Madrid, Spain; 2Hospital Quirón, Madrid, Spain
Objetive: To establish the correlation between the over-expression of viral oncoproteins E6/E7 and high grade viral serotypes using the HPV-ONCOTECT® method.
Design and Method: A sample of 98 peri/postmenopausal patients over 40 years old was selected among women referred to our Center for the realization of Oncotect Test. The selection was independent of the reasons for the referral (positive HPV test, colposcopic findings, risk factors for cervical premalignant lesions, patients choice, abnormal cytology or biopsy). HPV Oncotect® was used to detect the over-expression of E6/E7 oncoproteins, after granting informed consent. A total of 110 tests were performed. Data was analysed using SPSS version 13.
Results: 35,5% of the sample was PCR positive to a specific HPV serotype, predominantly a high-risk oncogenic subtype. 34,5% had a positive Oncotect® result (>2.00% overexpression), predominantly in smokers and high-parity women, and in patients with premalignant lesion in the cytology. We found a statistically significant difference of a positive Oncotect® test between high risk and low risk oncogenic subtypes, but not in cases with co-infection with more than 2 serotypes. In several cases we found a positive Oncotect® result with a negative viral PCR. This lack of association could be explained by a viral genomic deletions at de the integration phase making the virus undetectable by PCR.
Conclusion: We found significant correlation between different HPV serotypes, clustered as low risk or high risk oncogenic types and positive results in Oncotect®, even considering high serotypes dispersion and small sample size.
PS-92
REPRESENTATION OF VAGINAL SYMPTOMS IN CERVICAL CANCER PATIENTS
Jennifer M. Tornatta1, Janet S. Carpenter1, R. N. Higinia Cardenes2 and Jeanne M. Schilder2
1Indiana University, School of Nursing, Indianapolis, IN; 2Indiana University, School of Medicine, Indianapolis, IN
Introduction: Cervical cancer is the second most common cancer worldwide for women and the third most frequent cause of cancer death, accounting for nearly 300,000 deaths annually. Typically, advanced stages of cervical cancer are not found during annual screening and occur in women over the age of 55. Treatment involves radiation and chemotherapy, resulting in multiple side effects such as vaginal dryness, vaginal stenosis, chemically induced menopause, dyspareunia, and sexual disinterest. Results from one study showed that 74% of women treated for cervical cancer complained of vaginal dryness, 79% complained of painful intercourse, and 79% complained of feeling a shortened or narrowed vagina. These symptoms can contribute to lower ratings of sexuality. The purpose of this study was to explore the dimensions of vaginal symptom representation (identity, timeline, consequence, cause, control and cure) among women treated for cervical cancer and how these relationships impacted quality of life.
Methods: The study was a cross-sectional, convenience sample of women who had completed treatment. Eligible women completed a questionnaire assessing the severity of symptoms such as vaginal dryness, loss of libido, and intercourse. Women ranked symptoms in order from most bothersome to least bothersome. Participants used the three most bothersome symptoms to answer questions about the representation of each symptom in their life. Items from the FACT-G were also used to assess quality of life.
Results: The sample consisted of cervical cancer survivors who were a mean age of 52.5 years old (SD = 12.2) with 11.3 years of education (SD = 2.2). Most were Caucasian (67%), partnered or married (42%), and sexually active (58%). Length of current relationship was 14.45 years (SD = 18.78). Most were diagnosed with stage I or II disease (75%), were post menopausal at diagnosis (75%), and had received both chemotherapy and radiation (83%). The three most bothersome symptoms were decrease in sexual desire, vaginal dryness, and vaginal odor. Mean severity ratings for all symptoms were mild (mean between 0 and 3.25) but standard deviations indicated high variability in symptom severity. Representations of symptom identity and consequences were highly correlated with FACT-G quality of life subscores and total scores (r = .65 to. 90, p < .05).
Conclusions: These findings confirm that assessing symptom representations is important for understanding the impact of side effects women experience after treatment for cervical cancer. Findings support the need for future research on prevention and treatment strategies for these side effects that will lead to improved quality of life.
PS-93
THE EFFECT OF TIBOLONE ON BONE DENSITY IN WOMEN WITH EARLY MENOPAUSE RESULTING FROM CANCER TREATMENT
D. O. Lee, Y. K. Chung and S. Park
Center for Uterine Cancer, National Cancer Center, Goyang, Korea
Objective: To evaluate the effect of tibolone on bone density in women with early menopause (<45 years old) resulting from treatment of cervical cancer.
Design & Method: Through retrospective chart review, 13 women with early menopause resulting from bilateral oophorectomy or pelvic radiation therapy were compared with age-matched healthy women. All the women had taken tibolone continuously. Two normal women were matched per one woman with early menopause, so 26 of healthy women with regular menstruation were selected. Initial bone density data of lumbar spine, femur neck, and total hip were compared with those of two years later.
Results: For 2 years, there were no significant changes in bone density of women treated with tibolone for early menopause. In normal control, bone density of total hip was significantly decreased after 2 years. (p = 0.02) In inter-group analysis, there were no significant differences in changes of bone density between two groups.
Conclusion: Women treated with tibolone for early menopause kept normal age-related change in bone density. Tibolone may be effective for prevention of bone loss in women with early menopause after bilateral oophorectomy or pelvic radiation therapy.
PS-94
THE EFFECT OF HYSTEROSCOPY IN POSTMENOPAUSAL BLEEDING
Jung Hyuk
Department of Ob & Gy., College of Medicine, Chosun University, Korea Rep
Objective: To compare the diagnostic accuracy of ultrasonographic endometrial thickness and hysteroscopy, to establish the most appropriate exam for the diagnosis of endometrial cancer and other endometrial diseases in postmenopausal women with abnormal uterine bleeding (AUB).
Methods: This prospective study was conducted on 105 consecutive postmenopausal patients with AUB, who underwent ultrasonographic evaluation of endometrial thickness, hysteroscopy and endometrial biopsy. Evaluation of sensitivity and specificity was performed.
Results: Histological findings for <4 mm level revealed that atrophy was present in 30 (71.4%) and in 1 cases (2.4%) endometrial cancer was found; for ≥ 4 mm values polyps and myomas were present in 31 (49.2%) and there were 3 (4.8%) endometrial cancer. Sensitibity and specificity for trans-vaginal ultrasound, with a cut-off value ≥ 4 mm, was 75% and 40.6%.
Conclusions: In conclusion, endometrial thickness <4 mm can miss malignancies but trans-vaginal ultrasound remains the first line diagnostic procedure in postmenopausal women without AUB, because it is not invasive and has high sensitivity for detecting endometrial cancer and other endometrial disease; according to our experience, hysteroscopy with biopsy is mandatory in all postmenopausal women with AUB.
PS-95
THE PREDICTIVE VALUE OF ENDOMETRIAL THICKNESS MEASUREMENTS IN DETECTION OF ENDOMETRIAL CARCINOMA IN SCOTTISH WOMEN WITH POST-MENOPAUSAL BLEEDING
S. Mathew1, J. Crawford1, M. S. Allam1, A. Paterson1, J. C. R. Hardwick2, A. J. Thomson1 and W. M. Hair1
Departments of Obstetrics & Gynaecology, the Royal Alexandra Hospital, Paisley1 and the Southern General Hospital, Glasgow2, Scotland
Introduction: National clinical guidelines (Scottish Intercollegiate Guideline Network, SIGN Guideline 61), indicate that transvaginal ultrasound scanning (TVS) is the primary investigation in women with post-menopausal bleeding (PMB). Endometrial sampling is reserved for an endometrial thickness (ET) measurement of >3 mm in non-HRT users. This contrasts with other commonly-used guidelines where sampling is recommended only when the ET is ≥ 5 mm.
Objective: The purpose of this study was to determine the rate of histologically confirmed endometrial cancer in women presenting to our unit with a first episode of PMB who also had an ET measurement between 3 and 4.9 mm.
Design and Methods: Clinical, ultrasound and histological data for consecutive women attending our PMB clinic from September 2001 until October 2007 were retrieved from a computerised database. All women were managed according to SIGN recommendations. (endometrial sampling was performed when the ET was > 3mm in non-HRT users).
Results: 1833 women underwent TVS. 231 women had ET measurements between 3 and 4.9 mm. 154 of these were not taking HRT and all underwent endometrial sampling. There were no cases of endometrial cancer where the ET was between 3 and 4.9 mm. 40 cases of endometrial carcinoma were diagnosed in this series; these cases had ET range 6–34 mm.
Conclusion: We describe a large consecutive series of women with PMB. Our data indicate that endometrial sampling at an ET threshold of 3 mm may subject women to over-investigation with no improvement in the detection rate of endometrial cancer.
Sexuality and ART in female
PS-96
A POPULATION-BASED STUDY OF DYSPAREUNIA IN MIDDLE-AGED BRAZILIAN WOMEN
A. Valadares1, A. Mendes Pinto-Neto1, M. H. Sousa1, M. J. Osis1, D. M. Conde2 and L. Costa-Pavia1
1Unicamp, Belo Horizonte, Brazil; 2UFG
Objective: To evaluate the prevalence of dyspareunia in middle-aged women and the factors associated with this complaint.
Design: A cross-sectional, population-based study was carried out using an anonymous, self-report questionnaire completed by 200 Brazilian-born women, 40–65 years of age, with 11 years or more of formal education. The evaluation instrument was based on the Short Personal Experiences Questionnaire. Sociodemographic, clinical, behavioral, reproductive and partner-related factors were assessed. Poisson multiple regression analysis was performed and prevalence ratios (PR) with their 95% confidence intervals (95%CI) were calculated.
Results: The prevalence of dyspareunia was 39.5%. Multiple analysis showed that dyspareunia was more common in women who reported nervousness (PR = 1.94; 95%CI = 1.22–3.09) and depression (PR = 1.69; 95%CI = 1.09–2.61). A score >3 for frequency of sexual activities (PR = 0.20; 95% CI = 0.05–0.84) and having had more than two pregnancies (PR = 0.62; 95%CI = 0.48–0.80) were factors indicative of a protective effect against dyspareunia.
Factors associated with dyspareunia (score ≥2) in middle-aged women. Multiple analysisa
Conclusions: Dyspareunia was common in this cohort of middle-aged women. Nervousness and depression increased the likelihood of suffering dyspareunia. These findings suggest that psychological symptoms should be taken into consideration in the management of the middle-aged woman with dyspareunia, and measures should be adopted to minimize the repercussions of these factors on sexuality.
PS-97
ANALISIS OF THE ASSOCIATION BETWEEN THE HORMONAL LEVELS IN NATURAL POSTMENOPAUSE AND SEXUAL DISORDER
M. Guinot1, B. Roca2, R. Sust1, R. Homs1, J. Rodriguez1 and J. Calaf1
1Hospital de la Santa Creu i Sant Pau. Barcelona; 2Hospital de Terrassa, Barcelona
Objective: To analyse the existence of an association between hormonal levels and the Hypoactive Sexual Desire (HSD) in natural menopausal women.
Design and Method: Transversal study of 193 non selected, consecutive, natural menopausal women without hormonal replacement therapy (HRT) between 45 and 65 years old which were sexually active, attending our menopause outpatient clinic. They answered a questionnaire validated at a multinational level and known as “Brief Profile of Female Sexual Function” (B-PFSF).
It is established that a woman presents a HSD when punctuation is lower than 20. Group A was composed by ten women randomly selected among those scoring under 10 and group B 14 women among those with a score higher than 20.Women with a score between 10–20 have not been evaluated
The following variables were analysed: body mass index (BMI), time of menopause, hot flashes, vaginal dryness, associated diseases, and concomitant treatments. The following hormonal parameters were analysed: androstendione (A2), testosterone, sex hormone binding globulin (SHBG) and free testosterone index (FTI).
Analytical hormonal methods have been performed with chemiluminiscent immunoassays.
Categorical data were compared by use of Fisher's exact test. Continuous variables were assessed with the Student t-test for normally distributed data or the Mann–Whitney U tests otherwise.
Results: The mean age of patients was of 56,4 years in group A (range: 50–64) and of 58,7 years (range: 51–65) in group B. An average time of menopause of 9,4 years in group A, and 11 years of menopause in group B without statistically significant differences between both groups. Mean BMI was 25in both groups. Twenty per cent of women from group A presented hot flashes, being daily in a 50% and 43% of group B, being daily in an 83%. Vaginal dryness was present in 80% of women with HSD and in 50% of group B (p = 0. 2). Sixty per cent of the patients in group A and 64% in group B suffered from any associated disease and received a concomitant treatment.
The mean testosterone values were 0.61 and 0.48 nmol/L, the mean SHBG was of 77.5 and 69.5 nmol/L and the mean A2 was 4.04 and 3.68 nmol/L in group A and B, respectively, without significant differences between both groups. The values of FTI were 1.61 in group A and 0.776 in group B (p < 0,02).
Conclusion: Based on these results we can conclude that the occurrence of HSD is multifactorial. Other factors, related or unrelated to menopause, are more relevant than circulating levels of sex hormones in determining sexual function of midlife”.
PS-98
ASSESSMENT OF SEXUAL HEALTH IN PRIMARY CARE CENTRES IN SPAIN. THE EFFECT OF AGING ON THE PREVALENCE OF FEMALE SEXUAL DISORDERS
L. García-Giralda1, L. Guirao2, J. Delgadillo3 and F. Torres4
1Centro de Salud Murcia-Centro, Murcia, Spain; 2Centro de Salud Alguazas, Murcia, Spain; 3Procter & Gamble Pharmaceuticals Iberia, Barcelona, Spain; 4Universitat Autònoma de Barcelona, Barcelona, Spain
Objective: Epidemiological study to assess the prevalence of sexual dysfunctions in subjects attending primary healthcare centres in Spain.
Design & Method: Cross-sectional, observational study. Men and women older than 18 years attending primary healthcare centres in Spain were enrolled into the study using a systematic consecutive sampling procedure. Demographic, medical background and sexual activity information were collected. Sexual dysfunction was assessed using a specific questionnaire based on DSM-IV/TR diagnostic criteria. The chi-square exact test was used to compare categorical data, the t-test or ANOVA for continuous variables and non-parametric tests (Mann–Whitney or Kruskal-Wallis) for ordinal and non-normally distributed variables.
Results: Between March and December 2006, 6.199 subjects (3.600 men and 2.599 women) were enrolled into the study by 301 participating physicians in Spain. The results described here refer only to the female population. Mean age (SD) was 44.5 (14.3) years. To assess the effect of aging on sexual disorders, women were grouped into 6 age groups (n; %): ≥ 18–24 years (178; 7.9%); 25–39 years (714; 31.8%); 40–49 years (555; 24.7%); 50–59 years (430; 19.1%); 60–69 years (249; 11.1%) and ≥ 70 years (121; 5.4%). In the whole population, the prevalence of the different sexual disorders ranged between 2.8% and 6.6%. The prevalence each individual disorder was hypoactive sexual desire disorder, 6.6%; arousal disorder, 6.4%; orgasmic disorder, 6.3%; dyspareunia, 4.1%; aversion disorder, 3.4%; and vaginismus, 2.8%.
The prevalence of sexual disorders was significantly higher as women age. The lowest prevalence of sexual disorders was seen in younger women (≥18–24 years and 25–39 years), with prevalences ranging between 1% and 3%, respectively and without predominance of any individual disorder. The prevalence of different sexual disorders peaked at the age intervals between 40 and 69 years, ranging between 3% and 11%. At those age intervals, the most prevalent disorders were hypoactive sexual desire disorder (between 9% and 11%), orgasmic disorder (around 9%) and arousal disorder (between 7 ad 10%). Vaginismus was the less prevalent disorder (between 3% and 5%). In the oldest women (≥70 years), arousal disorder was the most prevalent one (10%) while hypoactive sexual desire disorder was the less prevalent disorder (5%).
Conclusion: In a representative sample of women attending primary healthcare centres in Spain, the prevalence of sexual dysfunctions increased as women aged, with a peak in prevalence at ages between 40 and 69 years. Hypoactive desire, arousal and orgasmic disorders were the more prevalent sexual dysfunctions reported.
PS-99
ASSESSMENT OF SEXUAL HEALTH IN PRIMARY CARE CENTRES IN SPAIN. THE IMPACT OF HYSTERECTOMY ON FEMALE SEXUAL DYSFUNCTIONS
L. García-Giralda1, L. Guirao2, J. Delgadillo3 and F. Torres4
1Centro de Salud Murcia-Centro, Murcia, Spain; 2Centro de Salud Alguazas, Murcia, Spain; 3Procter & Gamble Pharmaceuticals Iberia, Barcelona, Spain; 4Universitat Autònoma de Barcelona, Barcelona, Spain
Objective: Epidemiological study to assess the prevalence of sexual dysfunctions in subjects attending primary healthcare centres in Spain. The impact of sexual dysfunctions on subject's quality and satisfaction with life was also assessed.
Design & Method: Cross-sectional, observational study. Men and women older than 18 years attending primary healthcare centres in Spain were enrolled into the study using a systematic consecutive sampling procedure. Demographic, medical background and sexual activity information were collected. Sexual dysfunction was assessed using a specific questionnaire based on DSM-IV/TR diagnostic criteria. Women were grouped in 3 menopausal status according to her age (pre-menopause, age 18 to 44 years; peri-menopause, age 45 to 54 years; post-menopause, age older than 55 years). The chi-square exact test was used to compare categorical data, the t-test or ANOVA for continuous variables and non-parametric tests (Mann–Whitney or Kruskal-Wallis) for ordinal and non-normally distributed variables.
Results: Between March and December 2006, 6.199 subjects (3.600 men and 2.599 women) were enrolled into the study by 301 participating physicians in Spain. The results described here refer only to the female population and the comparison between hysterectomized and non hysterectomized women. Mean age (SD) of the whole population was 45.6 (14.5) years. In 176 out of 2.599 women (6.8%) a history of previous hysterectomy was reported. Overall, the prevalence of the different sexual disorders was significantly higher among hysterectomized women as compared to non hysterectomized women. The most prevalent sexual disorders were arousal disorder (15.3% vs 6.4%), hypoactive sexual desire disorder (HSDD; 13.1% vs 6.6%) and orgasmic disorder (11.9% vs 6.3%). When stratified by menopausal status, hysterectomized women as compared to non hysterectomized women showed a significantly higher prevalence of aversion disorder (13.3% vs 1.5%), arousal disorder (20.0% vs 3.3%) and dyspareunia (13.3% vs 1.8%) in the pre-menopause, dyspareunia in the peri-menopause (14.3% vs 5.0%) and, arousal disorder (17.3% vs 10.4%) and HSDD (15.3% vs 7.8%) in the post-menopause. Regarding the impact of hysterectomy on sexual activity, hysterectomized peri- and post-menopausal women reported having significantly lest interest in engaging in sexual activity than non-hysterectomized peri- and postmenopausal women (interest 62.3% vs 77.3% and 31.3% vs 44.1%, respectively).
Conclusion: In a representative sample of women attending primary healthcare centres in Spain, the prevalence of sexual dysfunctions increased in hysterectomized women as compared to non hysterectomized women. Hysterectomy also decreased the interest in engaging in sexual activity of peri- and post-menopausal women.
PS-100
CONTRACEPTION AND SEXUALITY IN THEIR 40s
T. Orte Sanz, R. Sánchez Borrego*, P. Prieto Martínez, E. Laso Pérez and R. Carreras Collado
Primary Attention (Ramón Turró, Villa Olímpica Barcelona) Woman Attention Clinic (*Diatros Barcelona)
Context: When women are in their forties, fertility gradually decreases and the risk of pregnancy still remains. The use of contraceptive methods after the age of 40s has associated some risks and benefits. The balance between them is very important in order to choose the best contraceptive option.
Purpose: To know the birth-control methods (BCM) and aspects of the sexuality of the women that you/they go to gynecological consultation.
Setting: Women clinic in a metropolitan Barcelona setting.
Methods: Descriptive, longitudinal, retrospective study of the users assisted from January ‘05 to June ‘05, evaluating the use of BCM, age to the first coitus, number of even sexual, children's n°, origin country.
Patient(s): Three hundred seventy three women (n = 373). 90.1% is autochthonous; 6.7% South America; 2.2% CCEE; 1% (Countries of the East, Africa, and Asia).
Result(s): The age of the 1er coitus <of 15 years old = 24 (6.4%); between 16–20 years old = 250 (67.0%); >21 years old = 98 (26.3%). The Spanish woman uses the surgical methods in 29.5% of the cases; barrier methods in 29.2%; hormonal methods only in 5%; DIU in 12,1%; they don't maintain sexual relationships in 13,9%; other 10,3%.
The South American woman 27.8% doesn't have sexual intercourse; 22.2% barrier; 11.1 hormonal%; 16,7% of various types of intrauterine devices (IUD); surgical 11,1%; other 11,1%. The women with 0 children (nulliparous) represent 40% it uses barrier; 1–2 children 28.6% barrier and surgical 27.8%; >2 children 48.8% surgical. Number of partners: 1 couple at 47.3%; 2–5 couples at 43.2%; >5 couples at 9.5%.
Conclusion(s): In our study 90% of women is autochthonous, they begin the 1er coitus among the 16–20 years, and 47.3% has a single couple. The use rate of Spanish woman is similar between the barrier methods and the surgical methods.
The rate of South American women that they came to our centre consult and they didn't maintain sexual relationships it was of 27.8%.
In the general group when the no of children > of 2, the contraceptive choice is the surgical method.
PS-101
DOES MENOPAUSAL STATUS OR HEALTH FACTORS DETERMINE SEXUAL DISFUNCTION?
B. Roca2, M. Guinot1, M. I. Cayuela2, F. Torres3 and J. Calaf1
1Hospital de la Santa Creu i Sant Pau. Barcelona; 2Hospital de Terrassa, Barcelona; 3Laboratory of Biostatistics & Epidemiology (Universitat Autonoma de Barcelona)
Objective: To analyze if there is an association between different factors related to estrogen decrease after menopause and others related to women's health and the hypoactive sexual disorder (HSD).
Design & Method: Transversal epidemiological and descriptive study of 193 natural or surgical menopausal women aged between 45 and 65 years old which were sexually active, attending our menopause outpatient clinic. They answered a questionnaire validated at a multinational level and known as “Brief Profile of Female Sexual Function” (B-PFSF).
It is established that a woman presents a HSD when punctuation is lower than 20. Three groups were differentiated: group I, with a score between 0 to 10; group II scoring from 11 to 20 and group III punctuation over 20. The following variables were analysed: Body mass index (BMI), time of menopause, hot flashes, vaginal dryness, local therapy with estrogens, present use or previous use of hormonal replacement therapy (HRT), bone mineral density (BMD) when available, associated diseases, and concomitant treatments.
The Fisher's exact test was used to compare categorical data, t-test or ANOVA for continuous variables or the Kruskal-Wallis test for non-normally distributed variables. The analysis was performed using SAS and the level of significance was 0.05 (two-sided).
Results: Of 193 women, 38 (19.68%) corresponded to group I, 74 (38.3%) to group II and 81 (42%) to group III. No significant statistic differences were found between the age groups (mean: 57 years; range 45–65), BMI (average:26), hot flashes, HRT and BMD variables. Significant statistic differences were found when grouping women according to the type of menopause: a 10% of group I had a premature ovarian failure (POF) (p < 0,013). Also, significant differences were found in the time since menopause (12.5 years in group I, 8 in group II and 10 in group III,; p < 0.01), vaginal dryness (79% in group I, 63% in group II and 39% in group III; p < 0.0003) and the presence of associated diseases (79% in group I, 61% in group II and 78% in group III).
Conclusion: Based on these results, we can conclude that some factors related to both low estrogen levels and the health status of women can have an impact on sexual function.
PS-102
DOES TRANSDERMAL TESTOSTERONE IMPROVE ALL AREAS OF SEXUAL FUNCTION
C. Bellone1, C. Domoney1 and N. Panay2
1Chelsea & Westminster Hospital Foundation Trust, London, UK; 2Chelsea & Westminster Hospital & Queen Charlotte's and Chelsea Hospital, London, UK
To determine the effect of transdermal testosterone on female sexual function: desire, arousal, lubrication, satisfaction, orgasm and pain.
40 women were identified from pharmacy records who were prescribed transdermal testosterone (gel or patch) in the last 12 months. All were sent questionnaires to determine the response on sexual function. The initial questionnaire included a 10 point visual analogue scale (VAS) to measure the effect of testosterone treatment on libido and energy. Secondly, the Female Sexual Function Index (FSFI) questionnaire objectively assessed the benefits of the current testosterone intervention.
39 women were identified and 11 questionnaires returned to date with 36% (4) of women using testosterone gel, 46% (5) on implants and 18% (2) using a patch: all were prescribed concurrent estrogen. 82% of the women had been on previous testosterone treatment but 3 women did not commencing the prescribed transdermal testosterone and 2 continued on implants.
Libido was seen to improve in all routes of administration with an average increase in VAS from 3.3 to 5.3. Similarly average energy levels improved from 3.6 to 5.8 along with an overall improvement in reported quality of life (4.9). The FSFI demonstrated a consistent correlation to the VAS scores observing an improvement in sexual function for all five of the domains. Scored from 1–6, where 6 indicated improved sexual function, the results were: desire 3.0, arousal 3.7, lubrication 3.5, satisfaction 3.7, orgasm 3.8 and (less) pain 5.0. The most significant overall improvement was reduced pain.
Based on the average results for both VAS and FSFI, Testosterone replacement does appear to improve overall sexual function. However, due to the current small sample size and disproportionate distribution between gel, patch and implant no statistically significant conclusions could be drawn with regard to the benefits of specific routes. Further ongoing evaluation is required to determine overall patient satisfaction with transdermal testosterone replacement on sexual function.
PS-103
EFFECT OF POST. COLPOPERIONEORRHAPY TO PELVIC FLOOR DYSFUNCTION SYMPTOMS
EunJung Kim, HyunHee Cho, JangHeub Kim, JinHong Kim, GunYong Chun and SuYoeun Kim
Catholic University Medical College, Seoul, Korea
Post: perineoplasty improves sexual life satisfaction.
Introduction & Objectives: Posterior colpoperineorrhapy is a curative surgery for a rectocele. However, in the Republic of Korea, some women request this type of surgery to reconstruct the perineum, which has become flaccid as a result of aging and child bearing. They refer this type of surgery to ‘A BEAUTY SURGERY’, and believe it can also improve the sexual satisfaction of their partner. Moreover, some regional gynecologic hospitals perform this type of surgery on women who do not have a rectocele only for cosmetic reasons and as a type of sexual therapy. Due to Confucian ideas, many Koreans still do not talk about sexual disorders even with their physician. Moreover, there is limited information about the sexual function after a colpoperineorrhapy performed only for cosmetic reasons. As a result, many people even gynecologists misunderstand the results of colpoperineorrhapy. The aim of this study was to evaluate sexual function in women before and after post. colpoperinoeplasty performed only for cosmetic reasons.
Material & Methods: 60 patients who took post. colpoperioneoplasty for improvement of flassid vaginal outlet were involved this study.
They filled symptoms questionnaries about stress incontinence, constipation and satisfaction of sexual life before and after 6 months of surgery.
Surgery was carried out as follows: The patient was placed in the lithotomy position. The pubic area and perineal area were prepared with povidone balls and sterile draperies in a routine performance. Under the local anesthesia using lidocaine, the posterior wall was designed in a square shape and the mucosa was dissected. The removed area was limited from the introitus to 5cm below the Os of cervix. With 3–0 delayed absorbable suture, the edges of the vaginal wall and the underlying rectovaginal fascia were closed with a single layer of interrupted suture. The caliber of the introitus was designed two ∼ three fingers in breadth. After surgery, the patients were prescribed antibiotics with analgesics. No medication was used to increase the level of sexual desire.
Results: After post. perineoplasty, 83% of the patients reported improvement of sexual satisfaction, 85% reported improvement of stress incontinence symptoms, and 62% of the patients reported improvement of constipation.
Conclusions: post.colpoperineoplasty has effect for improvement of sexual satisfaction.
PS-104
FEMALE HYPOACTIVE SEXUAL DESIRE DISORDER: EVALUATION IN A GENERAL GYNECOLOGIC OFFICE
A. B. Martin Escobedo, J. I. Alvarez de los Heros, C. Zorzo Ferrer, M. J. Cancelo Hidalgo, M. D. Perez-Jaraiz Lopez-Zabala, R. Rodrigez Puente, M. C. Gutierrez Velez, S. Tapiador Albertos, D. Guedea Murillo, E. Carballo Alvarez, C. R. Macarie and G. O. Salazar
Hospital General de Guadalajara, Spain
Introduction: Female sexual dysfunction refers to persistent or recurring reduction in sex drive, aversion to sexual activity, difficulty becoming aroused, inability to achieve orgasm, or dyspareunia that causes distress. Is more prevalent among women than men.
Dysfunctions of the desire phase (as defined in the DSM-IV) include hypoactive sexual desire, and sexual aversion disorder. Dysfunctions of the arousal phase include female sexual arousal disorder as well as dyspareunia and vaginismus. Orgasm phase disorders include female orgasmic disorder. In addition, there are the dysfunctions due to general medical conditions and substance-induced dysfunctions.
There are two common reasons that difficult the diagnosis: first, the clinician may feel uncomfortable with the questions about sexual topics and second the amount of time needed for discussion maybe is very long.
Low sexual desire is the most prevalent sexual dysfunction. Is defined that a recurrent or persistent deficiency or absence of sexual thoughts, fantasies, and/or receptivity to sexual activity that causes personal distress.
No specific tests are universally recommended in all women and this is guided by history and physical examination. Brief test are necessary to diagnostic in a general gynecologic office.
Design: Transversal, descriptive study.
Setting: General gynecologic office.
Participants: 250 women from 20 to 65 years old and who wanted to take part in the study.
Main measurements: The sexual function was measured by anonymous, self-questionnaire (Brief Questionnaire Low Sexual Desire). The questionnaire comprised 7 questions. Punctuation between 0–20 indicates low sexual desire.
The analysis was performed by using the chi2-test and multivariate regression analysis.
Objective: To determine the prevalence of low sexual desire among women who are provided in a general gynecologic office and to describe the influence of related factors especially menopause.
Results: The women with a higher level of education, reported better performance in the desire. Age and the non existence of sexual partner influenced in a negative way on the desire. In sexual active women the orgasm was negatively influenced by low satisfaction scores, and low educational level. Menoapause was associated negatively by sexual desire. The hormone therapy (HT) was associated with better scores in orgasm.
Conclusion: Sexual dysfunctions in women have strong positive associations with low feelings of physical and emotional satisfaction and low feelings of happiness. In our study, age, level of education, menopause and use of HT, influence the desire and orgasm domains in a significant way.
PS-105
IS POSTMENOPAUSAL OSTEOPOROSIS A RISK FACTOR FOR HYPOACTIVE SEXUAL DESIRE DISORDER?
J. Fragoso, R. Castaño, K. Hernández, S. Von Helde and S. Palacios
Instituto Palacios de Salud y Medicina de la Mujer, Madrid, Spain
Objective: Not only osteoporosis but also female sexual dysfunction are frequent pathologies which alter the quality of life in postmenopausal women. These two diseases have not been related until now. The objective of this study is to determine if bone mineral density is associated with hypoactive sexual desire disorder (HSDD).
Design & Method: This was a descriptive, transversal study. The Palacios Institute carried out a free bone densitometry campaign which was promoted by the mass media. This was how women with at least 3 years of menopause, and who were interested in having a bone densitometry measurement taken, were given an appointment in the period from October 15, 2007 to December 15, 2007. Before the results were given, a voluntary anonymous self-questionnaire was facilitated by the health care staff of the Palacios Institute. The questionnaire consisted of general health questions, a brief profile of Female Sexual Function (PFSF) and a questionnaire on Personal Distress Scale (PDS). The results of the questionnaires on sexuality were compared with the results of the bone mineral density, carried out with a Hologic densitometer (Delphi model W S/N 70757). The data were analyzed using a statistical programme SPSS 13 with a measure of central tendency and a parametric dispersion by means of an analysis of logistic regression and Pearson's Chi-square test.
Results: Of the 226 women (average age 59.4 years), 159 (70.3%) had a sex life during the previous 2–3 months before the study was carried out. 146 women completed both questionnaires (PFSF and PDS). Of these, 49% showed low sexual desire and 17.1% were diagnosed with hypoactive sexual desire disorder (HSDD). No significant statistical relation was found between bone mineral density and HSDD.
Conclusion: 17.1% of the women with more than 3 years of menopause who were interviewed showed a diagnosis of hypoactive sexual desire disorder (HSDD). No significant statistical relation was found between bone mineral density and hypoactive sexual desire.
PS-106
IMPACT OF SOCIAL PRECONCEPTION ON SEX DURING MENOPAUSE OF HANOI'S WOMEN
Nguyen The Luong
Committee of Population, Family and Children, Hanoi Vietnam
Preamble:In recent years many researches on sex have been approached gradually in Vietnam. Almost these researches covered juvenile, youth and other objects of child-bearing age. Sex of menopause women is a new theme, which nearly has not been studied in Vietnam.
Objective
Study demands relating to sex of menopause women
Consider impact of social preconception on sex
Object: Women with natural menopause are living in Hanoi.
Study method: Cross-section. Data were processed by EPI-INFO2002 and AnSWR5
Findings:
Some general information on the object:
The are 1385 ladies participated in the research. The average age is 52.16 ± 4, average menopause age is 48.88 ± 3.5.
Some demands relating to sex of menopause women.
The women still having sex are 26.3% and this number reduced in correspondence with menopause time. This differentiation has statistic meaning (p < 0.01). However, the number of objects still have feeling of sex desire when reading a paragraph or watching film clip relating to sex still is quite high (46.64%). Among the women having sex, number of women with sexless made up 95.8%
Impact of social preconception on sex.
Recommendation: There should be an effective intervention strategy to change the social preconception on sex so that menopause women can improve their life quality.
PS-107
LOCAL TREATMENT OF THE UROGYNAECOLOGICAL AGEING
N. Del Zoppo, M. Breccia and S. Torchetti
Private practice, buenos aires city, argentina
Objective: To evaluate the effectiveness of the treatment with estriol administered vaginally in the treatment of urogenital symptoms in climacteric patients.
Design and Methods: Descriptive multi centric study.
147 sexually active climacteric patients that came to our practice with symptoms of dyspareunia, burn and vaginal dryness in the period from March to September 2007.
All patients had a physical check up, SMEAR Test, colposcopy, transvaginal scan, and mammography.
Each of the patients was prescribed with an estriol 0.5mg ovule three times a week for six consecutive months.
A visual analogue scale was used (1–10) to evaluate the vaginal burn, dyspareunia and vaginal dryness in basal conditions at three and six months.
The media and SD of the values obtained was reported in relation to the symptoms in the analogue visual scale, in basal conditions at three and six months of treatment.
Wilconxon rank test was used for analysing the difference between the before and after values.
The patients signed an agreement before entering the study.
Results: 147 patients agreed to participate in the study and were evaluated in basal conditions.
At three months 139 patients came back for the evaluation and at six months the total of patients who attended evaluation was 128.
The average age was 53 years of age (49–57)
For the vaginal burn symptom the average in the analogue visual scale was 7.26 ± 1.2 points pre treatment at three months and 3.46 ± 0.9 at six months (p < 0.05)
Significant statistical differences were also observed for dyspareunia and vaginal dryness.
No side effects were reported.
Conclusions: Due to its common embryological origin, the symptoms for the lack of oestrogen in the gynaecological sphere as much as the urological one. The vaginal mucosa, urethra, trigonovesical, peri urinal muscles as well as the connective tissue have estrogenic receptors acting as effectors of the ovary hormones.
The uro gynaecological ageing symptom with its three items, atrophic mucosa (vaginal dryness, dysuria, dyspareunia and frigidity), recurrent urinary infection and urethra vesical dysfunction is favoured by the use of estrogens.
In our case, we observed a significant statistical reduction in the local symptoms related to the lack of oestrogen at vaginal level, evaluated at three and six months of treatment.
The use of 0.5 mg ovules of estriol constituted an effective therapeutical option with good response to the treatment and no side effects associated.
PS-108
PREVALENCE AND FACTORS ASSOCIATED TO SEXUAL BEHAVIOUR IN BRAZILIAN POSTMENOPAUSAL WOMEN OUTPATIENTS IN A SEXUAL CLINIC – THE APHRODITE PROJECT
I. Silva, N. P. Faleiros, M. C. M. Pusch, C. C. Ambrogini, M. C. Waitman and M. A. Haidar
Department of Gynecology, University Federal de São Paulo, UNIFESP, São Paulo, Brazil
Introduction: The female sexuality is a reflex of many factors such as age, partner relationship (quality), and hormonal level among others.
Objective: Characterize the prevalence and factors associated with sexual problems in postmenopausal women treated during Jan 2005 until in August 2007 in “The Aphrodite Project” – the multidisciplinary clinic specialized in women with sexual symptoms.
Design & Method: We analysed data of 172 postmenopausal women from 40–79 years old. Demographic, familiar, sexual data, religious, disease, job, education level, depression and the others information that may affect the sexual behaviour for that we collected these information from individual interviews. We performed structured interviews using the female sexual questionnaire validated in Brazil.
Results: The mean age of the group was 59 years old. The major problem was the decrease of desire (47%). We could observe problems such as: difficulty to reach orgasm (18%), dyspareunia (7%). High blood pressure was the most common disease (34%) followed by diabetes (9%).
Conclusion: Post menopausal women are more likely to engage in sexual problems and partner relationships emerged as a highly relevant predictor of sexual problems. The high correspondence between high pressure and diabetes may have important clinical implications.
PS-109
PROFILE OF POSTMENOPAUSAL WOMEN WITH SEXUAL DISORDER
B. Roca2, M. Guinot1, A. Francesch1, F. Torres3 and J. Calaf 1
1Hospital de la Santa Creu i Sant Pau. Barcelona; 2Hospital de Terrassa, Barcelona; 3Laboratory of Biostatistics & Epidemiology (Universitat Autonoma de Barcelona)
Objective: Postmenopausal women have a high probability of loosing their sexual desire. This is commonly known as Hypoactive Sexual Desire (HSD). Our objective is to evaluate HSD through a questionnaire validated at a multinational level and known as “Brief Profile of Female Sexual Function” (BP-FSF).
Design & Method: Transversal epidemiological and descriptive study of 193 natural or surgical menopausal women aged between 45 and 65 years, which were sexually active and attended consecutively the menopause outpatient clinic. They were asked to answer the BP-FSF questionnaire. It is established that a woman presents a HSD when the score is lower than 20. The following variables were analysed: Body mass index (BMI), time of menopause, presence of hot flashes and its frequency, vaginal dryness, local therapy with estrogens, present or previous use of hormone replacement therapy (HRT), bone mineral density (BMD) when measured, associated diseases, and concomitant treatments.
Categorical data were compared by use of Fisher's exact test. Continuous variables were assessed with the Student t-test for normally distributed data or the Mann–Whitney U test otherwise.
Results: 112 (58%) patients presented HSD. Of them, 84% (n = 94) were natural menopause, 12% (n = 25) surgical menopause and 4.5% (n = 6) presented premature ovarian failure (POF). Of the surgical menopause a 52% (n = 94) presented HSD, of the natural menopause 58% (n = 13) and an 83% (n = 5) of premature ovarian failure presented HSD. The patients mean age was 57.5 (range 45–67), with an average of 9.7 years of menopause (range 1–34) and a BMI of 26. A 42% presented hot flashes, and, among them 87% presented them daily. Vaginal dryness was detected in 69% of patients with HSD with changes statistically different (p < 0.0001) from women with normal sexuality. In this sexually normal group 20% used local estrogens and a 52% HRT.
BMD evaluation had been performed in 35 women. Of them 40% presented osteopenia and 60% osteoporosis. A 67% had one or more diseases associated and 59% received a concomitant treatment.
Conclusion: Based on the results we have concluded that the prevalence of the HSD is high in menopausal women. Vaginal dryness is closely associated to sexual disorder in these women. The low oestrogen levels is responsible of a decrease in vaginal blood flow, a loss vaginal secretions and alkaline vaginal Ph.
PS-110
SEXUAL DYSFUNCTION IN LATIN AMERICA: PREVALENCE AND RISK FACTORS
Juan Enrique Blümel, Patricia Leon-Leon, Peter Chedraui, German Baron, Emma Belzares, Ascanio Bencosme, Andres Calle, Daniel Flores, María Teresa Espinoza, Humberto Izaguirre, Eliana Ojeda, Selva Lima, Edwards Mezones, Alvaro Monterrosa, Desire Mostajo, Daysi Navarro, William Onatra, Monique Royer, Edwin Soto and Konstantinos Tserotas*
*Collaborative Group for Research of the Climacteric in Latin America (REDLINC)
Background: Although it has been reported that the female climacteric imposes the presentation of sexual disorders, which significantly impair quality of life (QoL), the diversity of questionnaires used to assess sexuality have limited the comparison of results.
Objective: To assess the prevalence of sexual dysfunction (SD) and associated risk factors among middle aged Latin American women using one validated instrument.
Methods: The female sexual function index (FSFI) was applied to 7,243 healthy women aged 40 o 59, users of 19 healthcare systems of 11 Latin American Countries. A itemized questionnaire containing personal and partner's socio-demographic data was also filled out.
Results: Mean age of surveyed women was 49 ± 5.7 years, 46.8% were postmenopausal, 14.1% used hormonal therapy (HT), 55.1% were married and had 11.6 years of schooling in average. A 25.6% of these women were sexually inactive. Among those who were active mean FSFI score was 25.2 ± 5.9 and a 56.8% of them presented SD (FSFI score <26.5), with a prevalence varying from 98.5% in some centers to 21.0% in others. After grouping centers in terciles according to the prevalence of SD, it was observed that the tercile with higher SD (86.4%) in comparison to the tercile with less SD (32.2%), significantly had women wit: increased age (49.5 ± 5.3 vs. 47.9 ± 5.6), higher schooling (12.6 ± 3.9 vs. 11.6 ± 4.0), partner with increased age (53.0 ± 6.9 vs. 50.2 ± 7.5). Equally there was a significantly higher rate of married women (68.5% vs. 63.1%), postmenopausal (49.7% vs. 39.3%) and HT users (23% vs. 9.2%). There were no differences in regard to the perception of their health, history of oophorectomy, rape neither in the rate of SD of their partner (27% vs. 26.2%). The FSFI score was significantly lower in the tercil with higher SD (22.0 ± 5.0 vs. 27.5 ± 5.4). During the analysis of the domains of the FSFI it was observed that those centers with higher SD rates had women with less vaginal lubrication (3.7 ± 1.0 vs. 4.9 ± 1.1, p < 0.0001) and more dyspareunia (3.2 ± 1.5 vs. 5.0 ± 1.1, p < 0.0001). Logistic regression analysis determined that main factors associated to SD were: bad lubrication (OR:31.19, CI 95%: 31.27–46.64), dyspareunia (OR:8.74, CI 95%: 7.28–10.48); partner sexual failure (erectile dysfunction and/or precocious ejaculation) (OR:2.43, CI 95%: 1.97–2.99), history of rape (OR:1.67, IC 95%: 1.10–2.54), older female age, > 48 years (OR:1.57, CI 95%: 1.31–1.89), oophorectomy (OR:1.45, CI 95%: 1.03–2.03) and being married (OR:1.29, CI 95%: 1.07–1.55).
Conclusion: The prevalence of SD in Latin America was found to be is high, varying widely in different populations. La decrease in vaginal lubrication and dyspareunia were important associated risk factors; these disorders had different prevalence among studied groups and could explain the variation of the prevalence of SD observed in this study.
PS-111
SEXUAL FUNCTION AND QUALITY OF LIFE IN A COHORT OF MIDDLE AGED WOMEN
Glenda San Miguel1, Carlos Avila1,2 and Peter Chedraui2
1Unidad Materno-Infantil del Hospital Dr. Teodoro Maldonado Carbo; 2Facultad de Ciencias Médicas, Universidad Católica de Santiago de Guayaquil, Ecuador
Objective: To correlate sexual function and quality of life (QoL) in a cohort of middle aged women.
Method: In a cross sectional designed study women aged 40 to 59 simultaneously filled out the Female Sexual Functioning Index (FSFI) and the Menopause Rating Scale (MRS) as well as a data sheet containing general demographic information.
Results: During the study period a total of 409 women filled out the surveys. Mean age was 47 ± 5.3 years. A 42.1% were premenopausal, 24.4% perimenopausal and 33.5% postmenopausal. At the moment of the survey 10.5% were hysterectomized, 1.5% were using antidepressants and 9.8% hormonal therapy for the menopause. An 80.4% of women indicated having only one sexual partner. Of these, 5.9% consumed alcohol, 8.3% had erectile dysfunction, and 9% had premature ejaculation and 51.3% were not faithful to their female partner. Mean total MRS and FSFI scorings were 9.1 ± 6.4 (median 9) and 20.1 ± 12.4 (median 24.7) respectively. The FSFI total score significantly and inversely correlated to the total MRS scoring (r2 = 0.39, p < 0.05).
Conclusions: In this specific climacteric population the severity of menopausal symptoms correlated to lower female sexual function.
PS-112
SEXUALITY IN MIDDLE-AGED WOMEN. Clinical Experience, Havana, 1996–2007
Navarro, Daysi1, Seuc Armando1, Artiles Leticia2, Diaz Dayami3 and Manzano Blanca Rosa3
1National Institute of Endocrinology; 2Havana Medical School, Ramon Gonzalez Coro Gynecologic Hospital 3Havana, Cuba
Objective: To identify the factors having an influence on climacteric women's sexuality in Havana.
Subjects and Methods: Women with a regular sexual partner, residing in Havana, between 40 and 59 years old, with high education level and full access to health services. 1331 women were evaluated at THEIR HOMES by means of ad hoc questionnaires aimed at identifying changes in sexuality related to their current age, school level, climacteric stage and intensity of climacteric symptoms. Other variables were analyzed by subgroups: i) in 300 healthy women, mood changes, gender conditioning and characteristics of the sexual partner were assessed; ii) in 180 women, the presence of a Diabetes Mellitus condition and its influence on sexuality was evaluated, and iii) in 400 healthy women, sexual satisfaction was assessed by the Sexual Function Index (self-administered). In CLIMACTERIC CLINIC two groups of women were studied: i) in 100 climacteric women attending the clinic, the frequency and changes in sexual intercourse were evaluated compared with a similar group of women not attending the clinic (n = 100), and ii) in 112 healthy women the sexual response to hormonal replacement therapy during twelve months was assessed. Statistic analysis used logistic regression Chi-square test, and odd ratios method test.
Results: In the group studied, as a whole, the change most frequently referred to was a decrease in sexual appetite (36–59%), but in many cases having a post-coital satisfaction. The change, not associated with the intensity of the climacteric syndrome, was linked to bad relations between couple members, sexual dysfunction of the partner and gender overload. Dispareunia (30%) and vaginal dryness (34%) were linked to the post-menopausal period, showing both of them a good response to HRT, although no response was observed in 1 of 4 women. Anorgasmia was related to school level, age and post-menopausal period. Many women (44%) felt unsatisfied with their current sexual life. Twenty percent of the women did not seek help due to the following reasons: they thought those changes were “normal and expected”; they did not have time to go to a physician; they lacked information about the clinics they could go to for help.
Diabetic women referred a decrease in sexual appetite with similar frequency to not diabetic women, but having more frequent orgasms.
We identified the factors having a negative impact on the sexuality of Cuban middle-aged women, particularly those related to gender condition.
PS-113
SEXUAL DESIRE HIPOACTIVE IN THE MENOPAUSE RELATED TO NATIONALITY AND PROFESSION
M. J. Cornellana, E. Khartchenko, M. Honrado, S. Lopez-Lacal, C. Trens and R. Carreras
PASSIR, Hospital del Mar, Barcelona
Objectives: To value if the Sexual Desire Hipoactive in menopausal woman changes depending on the nationality or the profession.
Design & Method: Prospective, random study. This includes all the women who makes consult for gynecological periodic controls in a public Center during a month. It's studied the influence of the different nationalities and the professions in Sexual Desire Hipoactive (DSH) of the menopausal woman. One classifies the women in different age groups, analizing nationality and profession in next categories: housewife, non university student and university ones. All of them fill questionnaire B-PFSF to define Sexual Desire Hipoactive before entering consultation and without personal identification.
Results: N = 231women; Rank: 40–75 years. DSH%. Spanish 91% South American woman 7%, East countries 2%. Housewife 58%, non university degree 7% university degree 15%. Of all the housewives 48% DSH, non university degree DSH 60%, university degree 67%. Spanish Menopausals DSH 46%, South American women 75%, East countries 0%.
Conclusions: In our casuistry only 10% it is immigrant population, mainly from South America. A small percentage of Chinese and also Arab women are not included because of an idiomatic difficulty. South American women presented the greater incidence of DSH followed by the Spanish ones. Not menopausal of the East referred DSH. About Profession, university degree women presented greater index of DSH, followed by the non university degree ones. Those of less incidence of DSH are the housewives. Filling the questionnaire was pronounced as a good tool to facilitate consultations on sexuality.
PS-114
SEXUAL BEHAVIOR OF POST-MENOPAUSE WOMEN
A. L. Cavalcanti, J. S. Paixao, A. M. Fonseca, V. R. Bagnoli, M. A. F. Padua, P. F. R. Margarido and P. A. A. Junqueira
Department of Obstetrics and Gynecology, Medical School, São Paulo University, São Paulo, Brazil
Introuduction: The sexuality is considered an important topic for the life quality. The menopause is associated with physiological and psychological changes that can have important influences in sexual function. That is why many aspects connected with sexual health during this period of women's life have been studied with much more interest. The sexuality is something complex and dynamics; expressed by all dimensions of the life and built individually and socially; and not restrict at sexual intercourse. Sexual behavior usually considered only with the several kinds of sexual practices that a person is engaged.
Objective: to analyze behavior and sexual satisfaction in post-menopause women.
Casuistry and Methods: Were applied Griss' Inventory (Golombok Rust Inventory of Sexual Satisfaction) in 114 post-menopause women, aged from 40 to 61 years (mean age 49,7years), with 1 to 20 years (mean 7 years) in menopause.
Results: Considering the frequency of sexual intercourses 40(35,1%) referred one to two intercourses a week; 14(12,3%) three or more times a week; 25(21,9%) once each 15 days, and 35(30,7%) once a month. One stable sexual partner were referred by 109(95,6%) of the women, with mean time of 25,1 years. Only 11(9,6%) referred self masturbation. Among women studies, 65(57,0%) related indifference for sex, 53(46,5%) that they miss love and affection and 61(53,5%) difficulties to speak with her partner about sexual preferences, this lack of communication is associated with sexual unsatisfaction and during preliminary sexual stimulus in 41,8% of the women. Difficulty to sexual stimulation referred by 68,3% of women and absence of orgasm during sexual intercourses with the partner 53,2%.
Conclusions: The post-menopause period was associated with reduction of sexual performance, showed by the low sexual interest and also by deficient sexual response and orgasm, during sexual intercourse with the partner. Lack of communication about sexuality is another unfavorable factor.
PS-115
SEXUAL DYSFUNCTION IN A POPULATION-BASED STUDY WITH BRAZILIAN WOMEN BETWEEN 40–65 YEARS OLD
A. Valadares1, A. Mendes Pinto-Neto1, M. J. Osis1, M. H. Sousa1, D. M. Conde2 and L. Costa-Pavia1
1Unicamp, Belo Horizonte, Brazil; 2UFG, Brazil
Objective: To evaluate the prevalence and factors associated with sexual dysfunction of middle-aged women.
Design: Cross-sectional, population-based survey using an anonymous self-response questionnaire. A total of 315 Brazilian-born women, 40–65 years old with 11 years or more of formal education participated in the study. The evaluation instrument was based on the Short Personal Experiences Questionnaire (SPEQ). Sexual dysfunction was calculated from the average sum score of sexual responsivity (sexual enjoyment, arousal, and orgasm), sexual frequency and libido. Sociodemographic, clinical, behavioral and reproductive factors were evaluated. Poisson multiple regression analysis was performed and prevalence ratios (PR) with their 95% confidence intervals (95%CI) were estimated.
Variables associated with sexual dysfunction (scores ≤ 7) in middle-aged women. Multiple analysisa
Results: The prevalence of sexual dysfunction was 35.9%. The multiple analysis showed that sexual dysfunction was higher in older women (PR = 1.04; 95% CI = 1.01–1.07) and in women who presented hot flushes (PR = 1.37; 95% CI = 1.04–1.80) whereas women who had a sexual partner (PR = 0.47; 95% CI = 0.34–0.65) and those who felt good/ excellent (PR = 0.68; 95% CI = 0.52–0.88) were less likely to have sexual dysfunction.
Conclusions: Hot flushes and aging in women in midlife adversely affected sexual function. Having a sexual partner and felling well were found to be protective against sexual dysfunction. Therefore, greater attention should be paid to identifying these factors, and measures should be adopted to minimize their repercussions on the sexuality of middle-aged women.
PS-116
SEXUAL DYSFUNCTION: COMPARATIVE STUDY IN LNG-UID AND ETO-IMPLANT USERS
G. Grazziotin
Tancredo Neves Medical Center, Mato Grosso, Brazil
Sexual desire depends on mood and motivation to sexual intimacy as well as on hormonal factors. Previous studies indicate that 20% to 30% of Hormonal contraception users experience a reduction in sexual desire.
The goal of the study is to compare the frequency of sexual complaints among the users of: LNG-UID AND ETO-IMPLANT.
31 women, divide in 2 groups:
17 women LNG-DIU.
14 women ETO-implant.
Protocol follows up. It was in three months intervals. Protocol regulated evaluation - follow up. It was in three months intervals.
Participants received 3 questionnaires, applied of 3 in three months during one year.
Sexual McCoy Scale.
Psychological General Well-Being Índex (PGWB).
Short Sexual Functioning Scale (SSFS).
History and physical examination.
BMI (body mass index).
Endometrium evaluation by transvaginal ultrasound.
(3°/5° day. Endometrial measure until 5mm.).
Lab: Blood (TBC) Coagulation, Glycemia, Triglycerides, Total cholesterol, Urea, Creatinine, TSH, FSH, LH, Prolactin, Testosterone.
Patients that have completed 12 months:
Inclusion criteria:
Women in use of Eto Implant or LNG – DIU there is at least 3 months.
At least 18 years old.
Stable heterosexual relation during at least 3 months.
Non smokers.
Did not have any other psychiatric pathology.
In a heterosexual relationship, the method there is at.
Normal levels of FSH, LH, DHEA, TSH, Prolactina.
Physiologic levels of Testosterona.
Also analyzed demographic characteristics: - age, civil status, education, occupation.
LNG 88% had completed 12 months.
ETO 60.8% completed 12 months. The most common reason causing the retreat need was bleeding irregularity.
McCoy Sexual Scale.
LNG: Had no significant ALTERATIONS.
ETO: Decreased an average of 2.5 points during the study time.
LNG - IUD:
High spotting index, during the first 6 months of use.
Bigger amenorrhea indexes after the 9 month of use (47, 2% to the 9th mês, 57, 0% to the 12th month).
43% classified as treatment success.
2 LNG insertions were performed under general anesthesia.
Bigger incidence of migraine, acne and breast pain.
ETO_IMPLANT:
Bigger incidence: In spotting, irregular bleeding, weight gain and migraine.
30% classified as treatment success.
23% of the patients presented sexual dysfunction in the group LNG-DIU.
35% of the patients presented sexual dysfunction in the group it ETO-implants.
This study shows that women that use DIU and Implant HIUS they don't differ with regard to psychological variables as depression, well-being or relationship quality with the partner.
PS-117
HYPERTENSION AND SEXUAL FUNCTION IN POSTMENOPAUSAL WOMEN
P. De Franciscis, K. Esposito, C. Bisogni, E. Trabucco, L. Cobellis and N. Colacurci
Outpatient Menopausal Clinic, Second University of Naples, Naples, Italy
Objective: Female sexual dysfunction (FSD) is a critical issue at menopause for many women. Recent data show that women with metabolic syndrome have an increased prevalence of sexual dysfunctions as compared with matched control women, but data in postmenopausal women are lacking. We evaluated the prevalence of sexual dysfunction in postmenopausal women affected by hypertension compared with normotensive women according to antihypertensive treatment.
Design & Method: The Female Sexual Function Index (FSFI questionnaire) was used to evaluate sexual function in 540 postmenopausal health sexually active women divided in three groups: 240 normotensive patients, 220 hypertensive patients undergoing an antihypertensive treatment, 80 hypertensive untreated patients. Female sexual dysfunction was defined by a FSFI score lower than 26.
Results: FSD was found in 48/240 (20%) normotensive women, in 84/220 (38%) of hypertensive treated women, 22/80 (27%) of hypertensive untreated women. Systolic blood pressure levels were significantly negatively related to FSFI score (figure 1), while medical treatment in hypertensive women was correlated with higher prevalence of FSD.
Conclusion: FSD is more prevalent in women with essential hypertension compared with women with normal blood pressure, but its prevalence does not decline with blood pressure control.
PS-118
HORMONAL AND PSYCHO-RELATIONAL ASPECTS OF SEXUAL FUNCTION AT MENOPAUSAL TRANSITION
F. Albani1,2, C. Pisani1,2, A. Ornati1,2, V. Santamaria1,2, S. Tonani1,2, P. Vaccaro1, F. Polatti1 and R. E. Nappi1,2
1Research Center for Reproductive Medicine, Dept of Morphological, Eidological and Clinical Sciences, 2Unit of Gynecological Endocrinology and Menopause, Dept of Internal Medicine and Endocrinology, IRCCS “S Maugeri Foundation”, University of Pavia, Italy
Objective: The aim of the present observational, cross-sectional study was to describe hormonal and psycho-relational variables related to sexual function according to the stage of menopausal transition in a clinical sample of symptomatic women. Predictors of sexual function were also investigated.
Study design: A sample of women with hot-flushes (n° = 656) were studied according to STRAW staging criteria. Sexual function was measured by using the Female Sexual Function Index (FSFI), while anxiety (state and trait), depression, binge-eating and marital relationship were evaluated by validated self-report questionnaires. Hormonal determinations for FreeTestosterone, DHEAS and estradiol were also performed.
Results: Sexual function measured by the FSFI full score was significantly different according to the stage of menopausal transition with a significant reduction in women after 1 year of amenorrhea in comparison with women during the early perimenopausal stage (p = .009). Sexual desire (p = .02), arousal (p = .01), orgasm (p = .01) and pain (p = .02) showed a similar pattern with a significantly reduction in amenorrheic women in comparison with those with a variable cycle length (>7 days different from normal), while lubrication and satisfaction did not show any significant differences according to the stage of menopausal transition. Interestingly, anxiety, depression, and eating scores were superimposable in different stages of the menopausal transition with median scores rather normal. No significant differences were found in marital adjustment. Non parametric comparisons reveled that FreeT is slightly reduced in different stages of menopausal transition with significantly lower value after 1 year from last menstrual bleeding in comparison with women at early perimenopausal transition (p = .01). A similar trend was evident for DHEAS which was significantly elevated (p = .03) during the early perimenopausal transition in comparison with the late perimenopause/early postmenopause stage. Circulating levels of Free Testosterone was the more important factor to predict higher FSFI full score (β = .48; p = 0.004) in women at early perimenopausal transition (menstrual cycle > 7 days different from normal), while depression score was the more important factor to predict lower FSFI full score (β = −.62; p = 0.0001) in late perimenopausal transition (≥60 days interval of amenorrhea). The best model predicting FSFI full score in late perimenopausal transition/early postmenopause included DHEAS, estradiol circulating levels and state anxiety score.
Conclusions: Hormonal and psychological variables are extremely relevant to women's sexuality during menopausal transition but their role is different according to the stage of reproductive aging.
PS-119
SEXUAL REPERCUCION ON THE CLIMATERIC SYNDROM IN WOMEN OF MEDIUM AGE
Misael González González, Roberto Rodríguez Pargas and Yamila Soto Silva
Facultad de ciencias Medicas. Provincia de Las Tunas, Cuba
He was carried out an observational, descriptive and traverse study on the repercussion of the sexuality on the syndrom climateric in women of medium age in the municipality of The Tunas of the county. They take all of the women from 40 to 59 years of age of the area of health Policlínica Manuel Piti Fajardo of the mentioned municipality (4848 women).
The universe was constituted by 401 women with ages among 40 and 59 years that they live before in the area mentioned. According to sampling simple aleatory probabilístico 381 are selected in this age range. The technique of Interview was used, for that which was elaborated like instrument for the gathering of data a questionnaire or schedule semiestructure.
The data were tabulated in contingency squares and of distribution of frequencies. The package statistical epi-info 7.0 was used, it was calculated the square Chi of independence and homogeneity and the test of difference of proportions with 95% of dependability and a significant value for an inferior probability at 0.05. Main conclusions that the woman of medium age of the area of health of the Policlínico Pity Fajardo sociodemografic is characterized to have a level half educacional, these women play a list of the hogar. The women's of medium age of the urban area bosses they have a level of severity of the Síndrome Climateric: it forms moderate prevailing the circulatory symptoms and those of the rural area have a level of severity of the Syndrom Climateric: it forms light prevailing the psychological symptoms and genitourinary. to conclude the test related with the sexuality verifies that the woman of medium age of this area of health has big affectations of this sphere.
PS-120
SEXUALITY IN VALENCIAN WOMEN'S COHORT DURING CLIMACTERIUM
M. D. Juliá1, J. Quiles2, R. M. Marín3, A. Romeu1, E. Pastor2, J. Chaves4 and J. Redón4 and Research Group about influence of life styles, genetic and biological factors on women's health in Valencian Region( + )
1University La Fe Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 2Public Health Department Directorate, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 3Valencian School for Health Studies, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 4University Clinic Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain
Objective: To determinate sexuality features in a climacteric women sample from Valencian Region and to assess the association with presence and type of menopause.
Subjects and Method: Population Cross-sectional study of a sample of 675 women from 45 to 65 years old from four different geographical areas of the Valencian Region through personal interview and assessing a Sexuality Subscale included in Life Quality Questionnaire (CCV), validated in Valencian Region (Sánchez-Cánovas et al.). Statistical analysis packs: SPSS-v12 and STATA/SE v8.
Results: 50% of women began their sexual relationship from 21 to 24 years, and 23%, later on. At the beginning of the study 40% did not have sexual relationship. 43% showed a decrease of the libido since menopause and 25% libido absence. Among those with relationship, 38% had occasional satisfaction and 10% none. 48% had discomfort (dry, dyspareunia).
Sexuality Subscale: from items collected, 49.6% did not present important problems; 25.8% had any problem which could be solved with information, health education and social help, and 24.5% needed referral to sexologist or psychologist.
Sexuality features depending on presence and type of menopause: it was estimated a higher degree of sexual discomfort, less degree of desire, satisfaction and less frequency, as well as lack of vaginal discharge among menopause women (p < 0,05). For these variables, there was no difference according to type of menopause (natural o surgical), except for sexual relationship frequency: 56,6% surgical menopause women did not have them versus 43,3% natural menopause women.
Conclusions: Valencian Region climacteric women sexuality is modified by presence of menopause, being this factor an aspect that must be incorporated to future research for a better understanding and management.(+ + )
(+ )Research Group: Marín RM, Quiles J, Redón J, Chaves J, Romeu A, Juliá MD, Pastor E, Mejía MJ, Marín P, Pérez AF, Bertolín A; Alonso C, Rozada R; Sánchez M; Rico MJ.
(+ + )The data of this study are included in: “Epidemiological Study on Cardiovascular Disease risk during the climacteric period of four different areas of the Valencian Region”. This project was partially financed by Women's Institute of the Department of Job and Social Matters of Spanish Government, Exp. number 65/01.
PS-121
TESTOSTERONE REPLACEMENT THERAPHY IN HIPOACTIVE SEXUAL DESIRE DISORDER
M. Cañamares Martín, M. Uriel Calvo, C. Braña Pelayo and J. M. Fernández Moya
Objective: To review if transdermal testosterone patch is an effective treatment for hipoactive sexual desire disorder (HSDD) in surgically postmenopausal women receiving concomitant estrogen theraphy, and if it has a favorable safety profile.
Design & Method: The data from five recent, parallel, double blind placebo-controlled Phase III trials in surgically postmenopausal women with hipoactive sexual desire disorder were reviewed.
Results: After 24 weeks of treatment, 300 ug testosterone-treated women experienced significantly greater increases in satisfying sexual activity and sexual desire, and greater decreases in distress than placebo-treated women with a favorable safety profile.
Conclusion: Reduced levels of testosterone in postmenopausal women are associated with loss of libido, decreased sexual activity, diminished feelings of physical well-being and fatigue. Bilateral oophorectomy can lead to decreases in sexual desire in 50% of cases by removing ovarian contribution to the circulating levels of testosterone. Testosterone replacement therapy may thus be useful in treating hipoactive sexual desire disorder (HSDD), offering advantages over other routes.
PS-122
THE IMPAIRMENT OF SEXUAL FUNCTION STRESSES MENOPAUSE LESS THAN PREMENOPAUSAL WOMEN
Marta Berra, Francesca De Musso, Francesca Armillotta, Antonietta Costantino, Silvia Cerpolini, Giuseppe Pelusi and Maria Cristina Meriggiola
Centro per la Tutela della Salute Sessuale, Clinica Ostetrica e Ginecologica, Università di Bologna, Policlinico S. Orsola Bologna
Objective: Menopause requires psychological and physical adjustments, due to the occurring dramatic hormonal changes. Sexuality is one of the aspects that undergoes the most profound modifications. Preliminary data suggest that sometimes women do not regard sexual changes as being problematic often readjusting their life and relationship according to their new physical status.
The aim of our study was to evaluate sexual function and the way women feel comparing postmenopausal and premenopausal women.
Design and Method: The Female Sexual Index Function (FSIF) and the Female Sexual Distress Scale (FSDS) were completed by 100 menopausal and 100 premenopausal women (Rosen RC et al., J Sex Marital Ther, 26:191 2000; Derogatis et al., J Sex Marital Ther, 28:317 2002).
Results: are reported in postmenopausal versus premenopausal women as median ± SD:
–age: 54.42 ± 5.5 versus 27.82 ± 4.2 years;
–sexually inactive: 10% versus 9% p = n.s.;
–FSFI score: 20.5 ± 9.6 versus 26.4 ± 7.7 (p < 0.0005);
–FSFI score <26.5: 69.3% versus 31% (p < 0.0005);
–FSDS score >15: 31.7% versus 28.0% (p = ns);
–sexual dysfunction 24.8% versus 20.0% (p = ns).
Conclusion: Our data confirm that menopause is associated with changes in sexual function that may be compatible with sexual dysfunction.
However, personal distress caused by these changes in sexual life appears to be lower among menopausal women as compared to premenopausal women.
According to our study, during menopause, the number of women who feel their sexual problems with distress and that therefore should be treated does not increase.
PS-123
TREATMENT OF ORGASTIC DYSFUNCTION IN POST-MENOPAUSE WOMEN WITH SILDENIFIL CITRATE
A. L. Cavalcanti, V. R Bagnoli, A. M. Fonseca, A. R. Pastore, C. E. Blanco, F. Saadi, J. S. Paixão and E. Baracat
Department of Obstetrics and Gynecology, Medical School, University of São Paulo, Brazil
Objective: to evaluate the effects of Sildenafil Citrate in the clitoris circulation in post-menopause women with orgastic dysfunction.
Casuistry and Methods: were selected 22 post-menopause women with orgastic dysfunction. All the women were submitted to the interview “Sexuality Questionnaire Hospital das Clínicas” and to the “Sexual Griss Scale”. The group A with 11 women received Sildenafil Citrate 50 mg, once a day, and group B with another 11 women received placebo once a day. The circulation of the clitoris was evaluated through color pulse Doppler in different moments: 0 (T0), 1 (T1) one hour after the ingestion of the tablet and 15 days (T15) of treatment in both the groups, considering resistance and speed index.
Results: the circulation of the clitoris through Doppler showed differences statistically significant, when evaluating the measures of the different moments (T0,T1,T15) and comparing the two groups (A and B), by resistence and speed indexes, were observed that the improvement presented by group A is superior to the improvement by the group B.
Conclusions: the Sildenafil Citrate is a safe and useful drug for the treatment of orgastic dysfunction in post-menopause women.
PS-124
WHAT TYPE OF MESSAGES MEXICAN WOMEN PREFER FOR PREDICTING THEIR HEALTH AND SEXUALITY DURING MENOPAUSE
López-Sosa C. Universidad de Salamanca, España
Sánchez-Ramírez G. El Colegio de la Frontera Sur, San Cristóbal de Las Casas, Chiapas Mexico; Álvarez-Gordillo M. El Colegio de la Frontera Sur, San Cristóbal de Las Casas, Chipas Mexico
Objective: To undertake investigations into womens preferences for receiving messages (whether in a positive or negative way) with information, which would lead to contingency plans for, self cure of, their health and sexuality by means of a programme about quality of life during menopause by means of a focus on the gender and health (through workshops) of women from three regions of Mexico with the aim of proposing contents of messages to promote well being during female maturity and ageing.
Materials and Methods: The methodology employed to evaluate preferences about messages to promote care of self consisted of the distribution of letters with pictures and texts, which had written opinions (compiled positively in some cards and negatively in others, so that each participant could choose the type of message they preferred). They were read in part by the person applying the evaluation test, therefore recopying the womens' preferences after finishing their partcipation. The study took place in 2005 with 138 women from two social groups (middle and lower class), from three Mexican provinces (Veracruz, the state of Mexico and Chiapas) whose ages ranged between forty and sixty. The results were statistically analysed separating the replies of the participants according to the social class they belonged to, applying a “Chi squared” test to establish independance between classes, comparing the percentage of replies according to the preferences for messages for self help.
Results: The results of the investigation gave rise to the knowledge that almost all women prefer to receive positive messages about self help because 86% of the women interviewed from lower class and 94% (with a “p” of 0.000) of those interviewed from the middle class chose these, as a recompense for the effort of achieving personal well being, understanding as well that the use of pictures accompanied by written phrases facilitates the evaluation of content in this type of investigation in contexts where the majority of women have limited resources (illiteracy, low level of education, little experience of participation in courses and health workshops, etc).
Conclusions: The preference for positive messages to prevent feminine health is linked to the necesity of women to change the pessimistic view which prevails in Mexico respecting female menopause, maturity and ageing because alarm bells are all ready ringing reguarding the development of osteoporosis, cancer, heart problems, etc leaving aside all that relates to prevention.
PS-125
WOMEN'S PERCEPCION ON THE EFFICACY OF A SOY EXTRACT WITH PROBIOTIC ON SEXUALITY: THE M3 STUDY
M. J. Cancelo1, S. Palacios2, R. Castaño3, J. L. Neyro4, I. Alvarez5 and C. Castelo Branco6
1Hospital Universitario de Guadalajara, Universidad de Alcalá de Henares, España; 2Instituto Palacios de Salud y Medicina de la mujer, Madrid, España; 3Instituto Palacios de Salud y Medicina de la mujer, Madrid, España; 4Servicio de Ginecología y Obstetricia, Hospital de Cruces, Universidad del País Vasco, España; 5Medical Department of Rottapharm; 6Hospital Clínic, Universidad de Barcelona, España
Objective: To determine women's perception of a soy extract with probiotic on sexuality.
Design & Method: A prospective multicentric survey was carried out. A total of 2044 women 40–65 years of age, who were recruited by a group of 198 random Spanish gynaecologists. The women completed a self report survey in the beginning and after 6 months of use of a soy extract(30mg of genistein and 30 mg of daidzein), with probiotic (500 million sporos of lactobacillus sporagenes), calcium (141mg) and vitamin D(5mcg). The questionnaire included 15 items of menopause and health, and 4 about sexuality from the Cervantes scale. Patients and gynaecologists completed an assessment about the clinical state.
Results: The score of the sexuality domain in the beginning of the survey show that women consider that sex is fairly important in their lives, and to the same degree about being happy with their sexual lives, and also interest in sexual intercourse (mean score 2.36; 2.32; 2.15;1.98 respectively).
After 6 months, the studied soy extract improved the women's perecption on sexuality. Women's perceptions were clearly significant in relation with their sexual lives and interest in sex (p < 0.01), significant about sexual intercourse (p < 0.05), and non significant about the importance of their sexual lives (Table 1).
Table 1 Mean scores (initial and after 6 months) of the answers to the 4 questions of the “Sexuality” block of the Cervantes Scale
Conclusion: The peri and postmenopausal patients usually experience common menopausal symptoms and many believe that soy extract improve sexuality. Physician providers should be aware of patient's positive attitude.
Urogenital
PS-126
ASSESSMENT VAGINAL TROPISM IN CLIMACTERIC WOMEN WITH AND WITHOUT HORMONAL THERAPY
M. Dinardi1, S. Lima2, A. Causade3 and A. Bozzolo4
Women Clinic, Asociación Española de Mutuo Socorro, Montevideo, Uruguay; 1Asistent Anatomopathology Department, Pereira RosselHospital; 2Prof. Adj. Gynacologic clinicPereira Rossel Hospital; 3Gynaecologist Asistent Low genital tract Dept; 4Prof Gynecologic Clinic, Pereira Rossel Hospital, and director of women clinic
The changes of vaginal tropism during the climacteric age, are a common reason for sexual discomfort, and increase of infections in the low genital urinary tract.
The objective of this research was to assess the characteristics of vaginal tropism in women older than 40 years old, who are comprised in the perimenopause and postmenopausal period.
We compared the vaginal tropism in postmenopausal patients with less than 5 years or more of post menopause, non users and users of hormonal therapy (kind and way).
We studied 1003 women between 40 and 80 years old, with vaginal cytology, through Papanicolaou test, colposcopy, and histology when this was necessary.
We registered the oncologycal pathologies in the genital and breast area in these patients.
The group of perimenopausic women (40 to 50 years old) represented the 4,7% of the patients. The 95,3% of the researched patients corresponded to postmenopausal women.
From the group of postmenopausal women non users of hormonal therapy, with less than 5 years of post menopause: 66% showed good vaginal tropism, 33,7% slight vaginal atrophy.
In the group of women with more than 5 years of post menopause without hormonal therapy: good tropism 0%, vaginal atrophy 98%, without data 2%.
In the group of women with less than 5 years of post menopause users of hormonal therapy : 60% showed good tropism, (91% users of TH orally, 9% users of TH locally), 40% showed slight atrophy (66% users of TH orally, 17% users of transdermic TH, and 17,5% users of local TH).
The women with more than 5 years of post menopause and users of hormonal therapy: good tropism 30% (with oral TH 70,5%, transdermic 20,5%, local and orally 9%), hypotrophic : 16% (62% oral TH, transdermic 19%, local 19%), atrophic vaginal: 10% (47,5% oral TH, transdermic 16,5%, local TH 34% and oral and local TH 1,5%).
We found 1,99% breast cancers: 85% in non users of hormonal therapy, 15% in users of TH.
Conclusions: the improvement of the vaginal tropism and the discomfort correction that this change causes is one of the objectives of the climacteric women assistance.
According to the obtained data, we can conclude the systemic hormonal treatment is not always effective, in patients with more than 5 years of post menopause for the correction of the vaginal tropism. We might consider the addition of local hormonal therapy.
PS-127
CHANGES OF FIBRONECTIN IN WOMEN WITH PELVIC ORGAN PROLAPSE
J. Li, P. Bachkangi and F. Al-Azzawi
University Hospitals of Leicester, Leicester, United Kingdom
Background: Pelvic organ prolapse (POP) is common- in up to 50% of parous women, and the incidences of POP and urinary stress incontinence (USI) increase significantly in postmenopausal women. The underlying mechanism for ligamentous failure in POP has not been elucidated. The purpose of this study is to determine Fibronectin (FN) expression in the cardinal ligaments from women with severe prolapse compared to controls with normal pelvic support.
Methods: Tissue specimens of the cardinal ligament were obtained at hysterectomy regardless of route from women with Grade III POP: 19 postmenopausal women (9 women on Hormone Replacement Therapy (HRT) and 10 women not taking HRT) and 8 pre-menopausal women. Control samples included 10 postmenopausal women and 10 pre-menopausal with normal pelvic support. FN expression was detected by immunohistochemistry. The area of positive staining was calculated in 15 randomly selected fields per specimen (×400) and analysed by using Carl Zeiss Imaging System (AxioVision 4.5).
Results: The mean FN expression in the cardinal ligaments of postmenopausal women with prolapse was 17.50 ± 7.73% compared to controls 31.48 ± 13.77% (p < 0.05). HRT (n = 9) dramatically increased FN expression by 3.3 fold-changes (p < 0.001). Fn level in pre-menopausal women with POP was low 26.22 ± 13.74 compared to 47.18 + 12.75 in women without POP (p < 0.01). In addition, FN expression in pre-menopausal women was higher than postmenopausal women (p < 0.05).
Conclusions: Significantly decreased FN expression was documented in the cardinal ligament from women with POP regardless of the menopausal status and as such this reduction may contribute to pelvic ligament failure in this condition. Significantly, HRT is associated with partial reversal in the expression of FN in postmenopausal women with POP.
PS-128
EFFECTIVENESS EVALUATION OF TENSION-FREE VAGINAL TAPE SECUR DEVICE IN THE TREATMENT OF URINARY INCONTINENCE AND SATISFACTION OF THE PATIENTS. MIDDLE-TERM FOLLOW-UP
I. Zapardiel, J. DelaFuente-Valero, A. Martín-Arias, J. Botija, L. San Frutos and J. M. Bajo
Santa Cristina University Hospital, Madrid, Spain
Objective: Urinary incontinence is an extended problem between middle-aged women. There are several options for its correction with different effectiveness and complication rates. Our objective is to evaluate the effectiveness of tension-free vaginal tape secur system (TVT-S) in the repair of this incontinence. Also to evaluate the patients satisfaction rate with this kind of surgery.
Design & Method: Retrospective study in 47 women with a surgical repair of their urinary incontinence with TVT-S without associated surgeries. We did a descriptive statistical analysis of the rates of effectiveness and satisfaction of the patients with the surgical repair after 2 and 6 months. The complication rate was also analyzed.
Results: The 68,1% of the women were postmenopausal, the age average was 54,94 ± 10,53 years old and the parity average was 2,40 ± 1,64. The media surgical time was 15,11 ± 4,12 minutes. Urinary continence rate 2 months after surgery was 72,3% and the satisfaction rate was 68,1%. After 6 months the rates were 40,4% and 51,1% respectively. The immediate complication rate was 2,1% and the late one was 8,4% (excluding incontinence as a complication).
Conclusion: The use of TVT-S for the repair of urinary incontinence is an effective and safe option with a very low complication rate. Moreover the rate of patients' satisfaction is high mainly in short-term follow-up. More studies are needed to asses the real middle and long-term efectiveness and satisfaction.
PS-129
EVALUATION OF KELLY KENNEDY S SURGERY IN THE TREATMENT OF URINARY INCONTINENCE OF EFFORT: ANALYSIS OF 391 CASES
A. C. Accorsi Neto1, S. C. Cury2, R. M. Mirandola2 and L. S. Accorsi3
1Prof. Doctor at Padre Albino Foundation, Medicine Faculty – Catanduva/São Paulo, Brazil; 2Students at Padre Albino Foundation, Medicine Faculty – Catanduva/São Paulo-Brazil; 3Nurse at Accorsi Institute – Catanduva/São Paulo-Brazil
Objective: To evaluate the result of Kelly Kennedy s surgery in women in the powder-menopause users or not of terapy of hormonal replacement, with uretrocistocele and urinary incontinence of effort.
Material and Methods: They were studied 391 women multíparas in the powder-menopause in use or not of therapy of hormonal replacement, that they presented uretrocistocele, urinary incontinence of effort and that you/they had been submitted to the surgery of Kelly Kennedy in the service of Gynecology of University of Medice of Catanduva in the last five years. All women were submitted to a questionnaire where you/they answered the following questions; she had been cured (without urine loss), if gotten better (decrease of the number of episodes of losses), without alteration, they got worse and if they were satisfied with the surgery. It was still verified the relation ship of the time of powder-surgery and the obtained result.
Results: They obtained cure 232 (59,3%) patient, 99 (25,1%), they referred improvement of the incontinence, 52 (13,3%) not they presented alteration with the surgery and 8 (2,1%) they told increase of the urinary loss after the surgery. Of the patients users of the therapy of hormonal replacement 129 (65,2%) they came cured, in other words, without urinary loss and of the patients with five years of postoperative 44,4% were not losing urine, with four years 50,1%, three years 52,6% and with two years 71,4% they didn't present episodes of urinary loss.
Conclusion: Technically easy surgery, with low morbidity.
Most of the patients have been pleased with the surgery.
Users of hormone replacement therapy have got better results.
Postoperative timing proved to be important in the incontinence maintenance.
PS-130
INFRACOCCYGEAL SACROPEXY IMPROVES THE QUALITY OF LIFE OF WOMEN WITH UTERINE PROLAPSE
JangHeub Kim, HyunHee Cho, EnJung Kim, JinhJong Kim and InChul Jung
Catholic University Medical College, Korea
Aims: This study evaluated the quality of life following infracoccygeal sacropexy in patients with pelvic organ prolapse by using the short versions of the Pelvic Floor Distress Inventory (PFDI-20) and the Pelvic Floor Impact Questionnaire (PFIQ-7).
Methods: We prospectively studied 35 women who underwent infracoccygeal sacropexy for the management of uterine or stump prolapse. The recurrence of pelvic organ prolapse was assessed 6 months after surgery. The prolapse, urinary, and colorectal scales of PFDI-20 and PFIQ-7 were assessed at baseline and 6 months after surgery.
Results: The preoperative grade of prolapse was 2.7 ± 0.7; six months after the surgery, it decreased to 0.4 ± 0.6. PFDI-20 and its 3 respective scales demonstrated statistically significant improvements following the surgery (P < 0.05). (POPDI-6 score, 57.7 ± 12.3 VS 41.6 ± 8.3; CRADI-8 score, 36.6 ± 7.2 VS 28.5 ± 3.2; and UDI-6 score, 57.1 ± 14.8 VS 33.9 ± 7.6; preoperatively VS postoperatively) The three scales of PFIQ-7, namely, UIQ-7, CRAIQ-7, and POPIQ-7, exhibited statistically significant improvements after the surgery (UIQ-7 score, 22.3 ± 5.6 VS 9.8 ± 3.8; CRAIQ-7 score, 11.1 ± 4.2 VS 28.8 ± 7.1; and POPIQ-7 score, 38.7 ± 12.5 VS 16.9 ± 7.8; preoperatively VS postoperatively).
Conclusions: Infracoccygeal sacropexy was an effective method for the management of uterine/stump prolapse; further, it improved the quality of life of women with pelvic organ prolapse.
PS-131
LACTOBACILLUS COLONIZATION AMONG A POSTMENOPAUSAL WOMEN POPULATION
L. Galluzzo, D. Yankelevich, B. Perazzi, M. Bigozzi, M. S. Moggia, A. Famiglietti, C. Vay and S. Provenzano
Hospital de Clínicas José de San Martín, Buenos Aires, Argentina
Objective: The aim of the present study was to evaluate the prevalence of lactobacillus colonization in postmenopausal women related to years of menopause. We also considered it relationship with pH and body mass index. (BMI).
Material and Methods: A total of 91 women, mean age 56.8 years old (45–75) were studied. None of the subjects received local or systemic hormone therapy. Women were stratified as follows: less than 5 years menopause (n = 25 [27.5%]), 5–10 years menopause (n = 26 [28.6%]), and more than 10 years menopause (n = 40 [43.9%]).
The microbiologic samples of vaginal content were taken from the vaginal fornix in order to perform: pH determination, Gram stain and culture of the sample in blood agar plates with 48-hour incubation period at 37°C in an atmosphere of 5% CO2. The sample was preserved with Stuart transport medium.
BMI measurements were obtained in our patients.
Relationship between age, years of menopause and presence of lactobacillus were evaluated with T Test. BMI and pH with Wilcoxon Matched Pairs Test.
Patient were sorted in groups with four criteria and analyzed with Fisher exact one tailed test: Obesity (patients with BMI ≥ 30 kg/m2), pH (≤4.5), presence or absence of lactobacillus and presence of lactobacillus equal or higher than 30/field 1000X.
Results: Vaginal lactobacillus were present in 35 women (38.5%) and more than 30/field 1000X in 10 patients (11.0%). Obesity was detected in 23 women (25.3%) and vaginal pH ≤ 4.5 in 7 women (7.7%). Lactobacilli presence had no relation with years of menopause and age. Presence of Lactobacillus was higher in patients with BMI ≥ 30 kgm2 (p = 0.0027) and pH ≤ 4.5 (p = 0.0121).
Large amount of lactobacillus only correlates with pH ≤ 4.5 (p = 0.0270).
We find a significant negative correlation between BMI and pH (p = 0.05).
Conclusion: little is known about the vaginal microflora of postmenopausal women. In our study the prevalence of lactobacillus was not related to years of menopause, as we can expect. Nonetheless, variations in the vaginal pH, do not exhaustively explain the balance of the vaginal flora. We can elucidate that BMI, in terms of hormonal status, better predicts the presence of Lactobacillus in our population.
PS-132
OUTCOMES OF MANCHESTER PROCEDURE FOR THE CORRECTION OF UTERINE PROLAPSE
Paulina Manosalvas; María De Matías, Ana R. Masero, Marta Blanco, Belén Fraile, Francisco Muñoz, Eloy Muñoz, Maroun Bousamra and Jose Manuel Hernandez
Division of Pelvic Floor Surgery, Department of Obstetrics and Gynaecology, Hospital Doce de Octubre, Madrid (Spain)
Objectives: The technique of choice for the uterine prolapse (UP) is the vaginal hysterectomy excluding the patients that wished to preserve their uterus or patients suffering from multiple diseases. Our aim is to expose the results obtained in our hospital with the intervention of Manchester technique.
Study Design: This retrospective observational study evaluated data from 85 women who underwent the Manchester operation at the Department of Obstetrics and Gynecology of Hospital Doce de Octubre,Madrid, Spain, from January 1999 to June 2007.
Follow-up was done at 1 month, 6 months and yearly (1 and 2 years) thereafter.
It was carried out statistical analysis of frequencies of valid cases.
Results: The mean age was 54.44 ± 14.04 years.
61 women (71.7%) complained of vaginal bulging, 20 (23.5%) of urinary incontinence (UI), 2 (2.35%) of urinary retention and 1 case of UI plus PU.
27 patientes (21.7%) suffered from Grade I UP, 43 (50 per cent) grade II UP and 7 (8.2%) grade III UP. 76 women (89%) had cystocele associated, 68 (80 per cent) rectocele, and 37 (43%) UI.
The Manchester procedure by itself, was practised in 11 cases (12.9%),it had a cystocele correction technique added in 5 cases (5.8%), rectocele correction added in 6 cases (7.05%), and both techniques added in 49 cases (57.6%). 56 cases included also an urinary-incontinence surgery.
Pathological anatomy: cervix length average 3.59 cm.
In 76 women (89.4%) there were no intraoperative complications.
Postoperative complications: 10 cases of urinary tract infection (11.7%), 3 mild fever (3.52%), 2 postoperative anemias (2.35%), 2 urinary retention, 1 bleeding from time later, 1 suprapubic haematoma and 1 wound infection. Not all due to the technique.
The recurrence rates observed were
1 month follow-up: 84 patients (98.8%) no relapse, 1 case (1.2%) with asymptomatic grade II cystocele.
6 months follow up: 80 cases (98.8%) no relapse, 1 kept with asymptomatic grade II cystocele.
1 year follow-up: 63 women (98.4%) no relapse1 kept with asymptomatic grade II cystocele (1.6%).
2 years follow-up: 44 patients (97.8%)no relapse, 1 (2.2%) progressed to grade III.
Conclusions: The technique of Manchester appears to be a safe and effective treatment option for UP in patients who desire uterine preservation. We remark a low percentage recurrence rate of prolapse and complications.
PS-133
PATIENTS WITH VULVAR PATHOLOGY ON THE MENOPAUSE
J. Marcos Sanmartín, J. A. López Fernández, F. Diéguez de Benito, A. Candela Hidalgo, A. Saco López, N. Esteve Fuster and J. C. Martínez Escoriza
Hospital General Universitario de Alicante, Spain
Objective: Study the pathology of the vulva found on menopausical patients that are sent to a unit of Lower Genital Tract (ULGT).
Design & Method: An observational and descriptive study of patients with vulvar pathology on the menopause sent to the ULGT of Hospital General Universitario de Alicante (Spain), between January 2000 and December 2007. We assessed the more frequent diseases, lesion type, location, diagnosis and treatment. Patients with lichen sclerosus and atrophic (LEA) were undergone a questionnaire to establish the current status and personal satisfaction. The database management and statistical program was carried out with SPSS version 12.
Results: The total number of patients evaluated in that period was 1501, of whom 189 were older than 55 years. Of these, 98 had cervical pathology, 23 vaginal and 68 vulvar. The disease that was most frequently found was vulvar lichen sclerosus and atrophic (38.5%), followed by seborreica keratosis and squamous cell carcinoma of the vulva (4.6%), and liquen planus and vulvar Paget (3.1%). The main symptom of these patients were itching (53.8), followed by feeling tumour (9.2%), and pain (4.6%). The average age of onset of vulvar symptoms was 69 years. As for the lichen sclerosus and atrophic, the average age of onset was 70 years, the main symptom was itching (64%), followed by pain (4%). The most common location was in labia majora (28%), clitoris and labia minora (12%). 84% of the injuries were biopsied. The treatment most often established were high-powered steroids (64%), and was also the most effective. 98% of the patients understood the nature of the problem and felt satisfied with the prescribed treatment and results.
Conclusion: The most common vulvar pathology on postmenopausical patients of our ULGT is the lichen sclerosus and atrophicus. Itching was the main symptom. High-powered steroids were the most effective treatment for these patients.
PS-134
PILOT STUDY OF EFFECTIVENESS OF AGLYCONE ISOFLAVONES VERSUS GLYCONE ISOFLAVONES OF SOY IN THE VAGINAL TOPICAL USE
J. Haya1, A. Sacristán2 and P. Bermejo3, In representation of “Consensus Group” of the Spanish Society of Gynecologist Phytotherapy
1Universidad Autonoma of Madrid, Madrid, Spain; 2Primary Care Unit, Madrid, Spain; 3Universidad Complutense of Madrid, Madrid, Spain
Objective: To evaluate the effectiveness of a gel for topical vaginal use with soy isoflavones aglycones and hyaluronic acid versus another with glycone soy isoflavones and other excipients different of hyaluronic acid.
Design & Method: We selected 32 menopausal women, attending gynecological consultation referring main symptom as vaginal dryness and discomfort. Mean age was 62 years old, with a minimum of 58 and a maximum of 72. These women were selected at random in two groups 16 women to receive a vaginal topical gel with aglycone isoflavones with hyaluronic acid (group A), or another product with glycone isoflavones (group B) and other excipients different of hyaluronic acid. The treatment regimen was an application nightly every 24 hours, on an ongoing basis, for 4 weeks. Prior to the initiation of treatment was conducted an autofilled survey in which the patient rated on a visual scale for intensity (from 0 to 10) of dryness, itching, burning, dyspareunia, and discomfort. In group A the average of symptoms was 34 points, and in group B was 33.7 points (no statistical difference).
Results: After 4 weeks of treatment, patients in both groups returned to respond to the autofilled survey. In group A there was a reduction of symptoms to an average of 7 points (p < 0.01, compared to initial). In group B was reduced to an average of 19 points (p < 0.05, compared to baseline). The decrease in symptoms was significantly higher in group A than in group B (p < 0.05). There were no dropouts in treatment, nor were reported side effects during the study period.
Conclusion: Our results suggest that the use of topical vaginal isoflavones can improve symptoms related to vaginal atrophy in menopausal women. But in this study aglycone isoflavones are more effective than glycone isoflavones (possibly due to better local absorption) and hyaluronic acid as an excipient (perhaps for its moisturizing effect locally). Larger studies are needed to confirm these preliminary results.
PS-135
POLYMORPHISM OF THE GENE ENCODING α−1 CHAIN OF COLLAGEN TYPE I AND A RISK OF PELVIC ORGAN PROLAPSE - A PRELIMINARY STUDY
Paweł Skorupski, Paweł Miotła, Katarzyna Jankiewicz and Tomasz Rechberger
2nd Department of Gynecology, University School of Medicine, Lublin, Poland
Objective: It has been postulated that the changes in the quantity and the quality of collagen may be involved in the pathogenesis of pelvic organ prolapse. Polymorphism of the gene encoding α−1 chain of collagen type I (COLIA1) gene can affect rate of its expression. This polymorphism is caused by a substitution of guanidine for the thymidine residue (G → T) at position 1240 in the first intron of COLIA1 gene. As a result three different genotypes exist: homozygotes G/G, heterozygotes G/T and homozygotes T/T. The clinical effect of Sp1 COLIA1 polymorphism is reduced mechanical strength of connective tissue in G/T and especially in T/T individuals in comparison to G/G subjects.
Design and Method: We checked hypothesis that the polymorphism in the transcription factor Sp1 binding site of COLIA1 gene predisposes for the development of pelvic organ prolapse in women. Study group: 37 patients with significant defects of the pelvic floor static (grades II, III and IV in POPQ scale). The control group consisted of 40 women without significant prolapse (more then grade I). Genomic DNA was extracted from whole blood leukocytes. Determination of COLIA1 polymorphism was done by RFLP. The patterns of DNA fragments obtained in the electrophoresis enable to identify type of polymorphism. Single band 598 bp corresponds to homozygote TT, two bands 598 and 430 bp to heterozygote GT and single band 430 bp to homozygote GG.
Results: The compared groups were well matched with regard to demographic and clinical characteristics. In the study group the GG polymorphism in COL1A1 gene was identified in 26 (70,3%), GT sequence in 10 (27%) and TT in 1 (27%) patient. The distribution of the investigated polymorphisms in the control group were: 27 (67,5%), 9 (22,5%) and 4 (10%), respectively. The statistical analysis (chi2 test) did not show any significant differences between compared groups.
Conclusion: We did not found the association between COL1A1 gene transcription factor Sp1 binding site polymorphism and a risk of development of pelvic floor prolapse. This is in contrast to the previous study which established link between GT and especially TT sequence in the polymorphic site and increased risk of SUI. The explanation for this finding is possible difference of pathogenesis of pelvic floor defects and SUI. Also, it is necessary to remember that both pelvic floor defects and SUI are complex disturbances in which genetics plays minor role compared to environmental factors.
The study was supported by the KBN grant no N407 093 32/3453.
PS-136
PREDICTORS OF SUCCESS OR FAILURE TWO YEARS AFTER TRANS-OBTURATOR TAPE PROCEDURE
I. Herraiz, R. Carpintero, E. Muñoz, E. Lorenzo, F. Muñoz, A. Masero, M. Bousamra and J. M. Hernández García
Division of Pelvic Floor Surgery, Department of Obstetrics and Gynaecology, Hospital Doce de Octubre, Madrid (Spain)
Objective: to assess efficacy, complications and success or failure factors of TOT along two years of follow-up.
Design and Method: a descriptive, retrospective study of 229 women who underwent TOT between 2003 and 2005. Obtape™, TVT-O Gynecare™ and Monarc™ were used. Patients had their follow-up visits at first, sixth, twelfth and twenty-fourth month after surgery. We performed statistical univariate analysis (Student's t-test or χ2-test as needed) and multivariate analysis (logistic regression) to assess efficacy factors of TOT, both with SPSS13.0 for Windows (SPSS inc., Chicago, Illinois, USA).
Results: stress urinary incontinence was cured in 91.3% (209/229), 87.6% (198/226), 91.2% (186/204) and 91.9%(158/172) of cases at first, sixth, twelfth and twenty-fourth month after procedure, respectively. Most frequent intraoperative complication was bladder injury (0.87%). Most common immediate post-operative complications were fever (2.2%), urinary tract infection (4.8%), urinary retention (0.9%), vault haematoma (2.2%), abscess (0.9%) and blood transfusion (0.4%). Complications during the follow-up were symptomatic mesh rejection (2,2%), onset of urge urinary incontinence (4.8%), chronic pelvic pain (1.3%). No significant association was found between recurrence after two years and age (P = .76) or body mass index (P = .81), or cystocele stage (P = .15), nor the degree of stress urinary incontinence (P = .79) or prior history of hysterectomy (P = .25). Multivariate analysis showed that the only predictors associated to technique's failure were higher stages of cystocele (P = .08) and, although it was not statistically significant, prior hysterectomy (P = .12). Neither age (P = .64), nor body mass index (P = .88) or previous degree of stress urinary incontinence (P = .99) were statistically significant risk factors for technique's failure at two years of follow-up, based on multivariate analysis.
Conclusions: trans-obturator tape is a very simple and safe means to treat urinary stress incontinence with excellent results even two years after surgery. It seems that the only risk factors for incontinence recurrence are previous hysterectomy and higher stages of cystocele before procedure.
PS-137
TRANSOBTURATOR AND POSTERIOR TENSION-FREE VAGINAL MESH (PROLIFT*) IN THE MENOPAUSE WOMEN WITH PELVIC ORGAN PROLAPSE
Yoon Soon Lee1, Jung M Lee1, Ji H Bae1, Mi J Kim1, Yoon J Kim1 and Kyung D Park2
1Kyungpook National University, Daegu, Korea; 2Hyosung hospital, Daegu, Korea
Objective: We evaluated the efficacy and the complications of ProLIFT*, new procedure for pelvic organ prolapse in patients of menopause.
Design & Methods: We performed ProLIFT* procedures in 15 cases of pelvic organ prolapse from Feb. 2006 to May. 2006. Total TVM procedure was performed in seven cases. Anterior TVM(Transvaginal mesh) procedure was performed in seven cases and posterior TVM was performed in one case. We didn't perform hysterectomy but 4 cases had vaginal rectocele repair and one case had laparoscopic uterosacral ligament suspension.
Results: The mean age was 62 years(range 49years–82 years). And mean parity was 3.6 (range 1–10). The mean operation time was 72.3 min (range 30 min–110 min). The mean blood loss was 35.2□ (range 10□–100□). The mean postoperative hospital stay was 4.9 days (range 4 days–6 days). The mean postoperative POP-Q stage was 3.3. And the mean postoperative POP-Q stage was 0. The mean preoperative C length was 1.7 cm but postoperative C length was −7.2 cm. The mean preoperative and postoperative Aa was 1.6 cm and −3 cm. The mean preoperative and postoperative Ap was 0.85 cm and −2.9 cm. And the mean postoperative follow-up period was 7.6 weeks (range 2.7 weeks −17.4 weeks). And there were no injuries to bladder, rectum and no mesh erosions. But two patients were aggravated stress urinary incontinence.
Conclusions: In spite of our limited cases and short follow-up period, our experience of ProLIFT* procedures was safe and anatomically good results in patients of menopause. But long term follow-up studies were needed.
PS-138
TENSION-FREE VAGINAL TAPE SECUR DEVICE VERSUS TRANSOBTURATOR TAPE IN THE TREATMENT OF URINARY INCONTINENCE
I. Zapardiel, J. DelaFuente-Valero, E. Pérez-Carbajo, J. Botija, T. Pérez-Medina and J. M. Bajo
Santa Cristina University Hospital, Madrid, Spain
Objective: The main objective is to compare the effectiveness of tension-free vaginal tape secur system (TVT-S) with transobturator tape (TOT) in the repair of urinary incontinence. Also to evaluate the patients' satisfaction rate between both techniques.
Design and Method: A retrospective study was carried out including a total of 141 women, 47 of them were treated with TVT-S, and 94 women with TOT. We did a descriptive statistical analysis of the rates of effectiveness and satisfaction of the patients with the surgical repair after 2 and 6 months comparing the results between the different procedures. The complication rate in both techniques was also analyzed.
Results: In the group treated with TVT-S, the age average was 54,94 ± 10,53 years old and the parity average was 2,40 ± 1,64. Urinary continence rate 2 months after surgery was 72,30% and the satisfaction rate was 68,10%. After 6 months the rates were 40,40% and 51,10% respectively. The immediate complication rate was 2,10% and the late one was 8,40% (excluding incontinence as a complication). In the other group (TOT), the age average was 55,28 ± 9,79 years old and the parity average was 2,56 ± 1,31. Urinary continence rate 2 months after surgery was 76,80% and the satisfaction rate was 72,46%. After 6 months the rates were 72,20% and 69,69% respectively. The immediate complication rate was 4,25% and the late one was 27,65% (excluding incontinence as a complication).
Conclusion: The use of TVT-S for the repair of urinary incontinence is less effective than the use of transobturator tape, but is a safer option due to the higher complication rate with the TOT. Moreover the rate of patients' satisfaction is higher with TOT mainly in middle-term follow-up.
PS-139
THE LEVLES OF SERUM ESTRADIOL, URINE DEOXYPYRIDINOLINE AND MATURATION INDEX IN KOREAN POSTMENOPAUSAL WOMEN TREATED WITH ESTRADIOL VAGINAL TABLET
H. Choi1, M. H. Kim1, W. Y. Paik2, H. Jung3 and S. T. Oh4
1Department of Obstetrics & Gynecology, Inje University Sanggyepaik Hospital, Seoul, South Korea; 2Department of Obstetrics & Gynecology, Gyeongsang National University Hospital, Jinju, Kyungsangnamdo, South Korea; 3Department of Obstetrics & Gynecology, Chosun University Hospital, Kwangju, South Korea; 4Department of Obstetrics & Gynecology, Cheonnam University Hospital, Kwangju, South Korea
Objective: Our purpose was to assess systemic effects and local effects on the vaginal mucosa of estriol vaginal tablet for treatment of vaginal atrophy.
Design & Method: In this placebo-controlled trial, fifty postmenopausal women with vaginal atrophy were assigned to receive with 500□ estriol vaginal tablet (n = 21) or placebo (n = 14) twice per week for 12 weeks. We compared the levels of serum estradiol and urine deoxypyridinoline in both groups before treatment with those after treatment for 12 weeks. In study group, we also compared maturation index before treatment with that after treatment for 12 weeks. Values were compared using Wilcoxon signed rank test.
Results: In study group, serum estradiol(E2) concentration decreased from 15.1 ± 3.7(SD) pg/ml to 12.9 ± 2.7(SD) pg/ml and urine deoxypyridinoline(uDPD) concentrations decreased from 8.5 ± 3.8(SD) nM DPD/mM cr to 6.6 ± 2.9(SD) nM DPD/mM cr after estriol vaginal tablet treatment for 12 week (E2 p = 0.074, uDPD p = 0.003, respectively). In placebo group, urine deoxypyridinoline(uDPD) concentrations also decreased from 9.9 ± 8.3(SD) nM DPD/mM cr to 5.2 ± 1.8(SD) nM DPD/mM cr after 12 weeks(p = 0.028). E2 level decreased from 14.2 ± 3.1(SD) pg/ml to 12,3 ± 2.2(SD) pg/ml without statistically significance(p = 0.84). The mean maturation index has significantly shifted from 82: 15.5: 2.5 to 3: 86.5: 10.5 (% parabasal cell: intermediate cell: superficial cell)(p = 0.005: 0.007: 0.032, respectively) in study group.
Conclusion: Twice weekly 500□ estriol vaginal tablet treatment for 12 weeks has local effects on vaginal mucosa without systemic effects in postmenopausal women. It can be used safely in postmenopausal women with vaginal atrophy for 12 weeks.
PS-140
ULTRASOUND EXAMINATION OF THE FEMALE LOWER URINARY TRACT STRUCTURES AFTER SHORT-TERM INTRAVAGINAL ESTROGEN TREATMENT IN WOMEN WITH THE URGE URINARY INCONTINENCE
P. Milart, E. Wozniakowska and T. Paszkowski
University of Medicine, Lublin, Poland
Objective: The depletion of estrogens during the menopause period seems to be the cause of the improper metabolism of collagen thus influencing the morphological structures of the lower urinary tract (LUT). Transvaginal ultrasound examination allows the detailed assessment of the female LUT structures.
The aim of the study was to evaluate the influence of the vaginally administered estrogens on ultrasonographic features of the selected LUT structures in women suffering from the urge urinary incontinence.
Design & Method: The studied group consisted of 16 women suffering from urinary urge incontinence. The bladder wall thickness was measured before, after 1, and after 3 months of treatment with vaginal estrogens. The selected variable was measured 3 times as a single dimension using a 7.5 MHz transvaginal probe (Medison SONOACE 9900 Prime). Transvaginal power Doppler ultrasonography was used to study the pulsatility index (PI) and resistence index (RI) of arterial vessels in the examined structure.
Results: The median values of bladder wall thickness before, after 1 month and after 3 months of local administration of estrogens were 0.62, 0.65 and 0.66 cm respectively (Friedman ANOVA, χ2 = 7.05, p = 0.029). No significant changes in the PI and RI in the bladder wall arterial vessels were found.
Conclusion: Short-term estrogen therapy results in the significant thickening of bladder wall although it does not affect the vascularization of the assessed tissues.
PS-141
VAGINAL HYSTERECTOMY IN ELDERLY WOMEN. PROGNOSIS AND RECURRENCE OF PELVIC ORGAN PROLAPSE AT LONG TERM FOLLOW-UP
E. Muñoz, E. Lorenzo, F. Muñoz, A. Carrascal, A. Masero, M. Bousamra and J. M. Hernández García
Division of Pelvic Floor Surgery, Department of Obstetrics and Gynaecology, Hospital Doce de Octubre, Madrid (Spain)
Objective: To assess prognosis, complications and incidence of recurrence of pelvis organs prolapse (POP) after vaginal hysterectomy (VH) in a cohort of elderly women.
Design and Method: retrospective cohort study of prognosis of vaginal hysterectomy (complications, hospitalization and recurrence of POP) in women aged 75 or over (study group), in whom that surgical procedure was carried out between January 1998- June 2005. Comparison of the results in the study group with figures obtained in younger patients (control group). Follow-up visits in both groups were performed at one month, six months, one year and two years after surgery. Statistical tests included Student's t-test, Fisher's exact test, χ2-test and Mann-Whitney test as needed. P values lower than 0.05 were considered statistically significant. Analyses were carried out using SPSS 11.0.
Results: Study population was composed by 129 women aged 75 or over (mean age 77.6 ± 2.5 years, range 75–86) and control group by 875 women (mean age 62.9 ± 8.2 years, range 35–74). We have not found diferences between groups regarding to percentage of urinary antiincontinence surgical tecniques performed at the same time of VH (67.4% study group vs 68.7% control group). Also, there were no differences in POP recurrence rates after two years of follow-up (9/102, 8.8% vs 75/784, 9.8%, p = 0.7) and nor in the other time periods (one month, six months and one year). We have found differences in mean hospitalization time (7.4 ± 5.0 days vs 6.1 ± 3.1, p < 0.001) and between the postoperative complications percentages (including fever, haematomas, abscesses): 34/196, 26.4% vs 162/875, 18.5%, p = 0.03, OR for postoperative complications in elderly women: 1.47 (CI95% 1.03–2.11). There were no differences in intraoperative complications (7.0 vs 7.4%).
Conclusions: VH is a surgical procedure with good results in elderly population, being recurrence rates similar to rates found in younger women, taking into account that surgical complexity is equal in both populations (no differences between proportions of procedures with antiincontinence techniques associated). Moreover, intraoperative complications rates are similar. On the other hand, there is an increased risk of postoperative complications, and a longer stay in elderly group, both probably related with basal characteristics of these women.
Clinical epidemiology
PS-142
ATTITUDES TO AGING OF PERIMENOPAUSAL WOMEN IN MEXICO AND PANAMA. A COMPARATIVE STUDY
D. Legorreta1 and K. Tserotas2
1LPA, México D.F., México; 2Complejo Hospitalario “Dr. Arnulfo Arias Madrid”, Panamá, Panamá
Objective: To explore and compare attitudes to aging of perimenopausal women in two Latinamerican countries: Mexico and Panama.
Design & Method: Comparative study of two population-based samples of women aged 40–55 recruited in Panama (n = 147) and Mexico (n = 146). Subjects were asked to answer a questionnaire in Spanish based on the Australian Reactions to Aging Questionnaire to assess positive and negative attitudes to aging. An additional medical questionnaire to determine current menopausal stage, use of HT and other medical or psychiatric conditions was also included. Descriptive frequencies, crosstabs, independent samples comparison of means as well as path analysis to determine weight of sociodemographic variables, menopausal stage and use of HT in different positive and negative attitudes to aging were conducted.
Results: Using a scale from 0 = Total disagreement to 5 = Total agreement, a more postive than negative attitude to aging was found in both samples (Mexico: 4.6 mean positive vs. 3.36 mean negative; Panama: 4.74 mean positive vs. 3.36 mean negative) Meaningful differences among both countries (p < .001)were found in “capacity to preserve a good attitude”, “concern about preserving self-care capacity”, “fear of loneliness” with Panamanian women scoring higher in these attitudes. Possible differences due to menopausal stage were not meaningful with a slight increase in mean postive attitudes in general and slight decrease in all negative attitudes with the exception of “concern about preserving self-care capacity” and “may become rigid and less open to change” in post-menopause. In path analysis, “fear of loosing independence” and “loosing strength and stamina” were partially explained by use of HT and work type which was also correlated to “fear of becoming irritable and difficult” and “fear of loneliness” being more present in house-wives and positive attitudes of “postmenopause stage will be more enjoyable than previous stages” more present in women with a payed job.
PS-143
ATTITUDES, SYMPTOMS AND PERCEPTIONS TO MENOPAUSE IN ARGENTINIAN POSTMENOPAUSAL WOMEN
D. Yankelevich1, M. Bigozzi1, L. Galluzzo1, M. Pérez Sainz2, M. S. Moggia1 and S. Provenzano1
1Climacteric Unit, Hospital de Clínicas José de San Martin; Universidad de Buenos Aires, Argentina; 2Centro TIEMPO, Buenos Aires, Argentina
Objective: To investigate signs, symptoms, perceptions and health controls, related to menopause, in women that attend a climacteric unit.
Design and Methods: descriptive study in 416 women, mean age 58.9 years (36–80) that attend to the climacteric unit at Hospital de Clínicas, from April to November 2007. Patients filled a self administered survey with 17 items. Height and weight were measured; and these values were correlated with their own perception. We established the prevalence of different symptoms.
Results: 416 surveys were analyzed from a total of 443; mean age of menopause was 47.6 ± 5.2 years; surgical menopause: 23.56%. There was a significant difference (p < 0.001) in the mean age of surgical menopause (46.12 ± 6.3) and natural menopause (48.08 ± 4.7). Women in hormone therapy 37%; moderate to severe hot flashes, 59.37%; night sweats, 50.24%; sexual dysfunction, 40.62%; sleep disorders, 45.91; 19.47% women were asymptomatic, 21.87% had one symptom; 19.23% two symptoms; 21.88% three symptoms, and 17.55% four symptoms.
In the last 3 years, the majority of the women performed the following controls: mammography (88.2%), Pap smear (89.18%), bone densitometry (68.27%), blood sample for: cholesterol (93.51%), glucose levels (93.99%), and control of arterial pressure (92.79%). 52.16% of women exercised at least twice a week. 45.67% perceived themselves as overweight or obese, but our data showed BMI <20 (n = 8) 1.92%; BMI between 20–25 (n = 164); 39.42% and BMI > 25 (n = 244) 58.66%. 31.2% perceived themselves much taller than they really are (2 to 15 cm more). 97.8% of the studied women considered that menopause is a natural step in life. 71.05% considered the climacterium as a positive stage of life and 74.73% the periodic controls should be more frequent.
Conclusion: the majority of our population performed periodical control, however a high percent of patients were overweight and obese and this issue was not perceived by them. Half of the patients did not perceive a height decrease. Although 80% of women have symptoms, only 37%, were in hormone therapy.
PS-144
AGE AT NATURAL MENOPAUSE AND MENOPAUSAL SYMPTOMS AMONG SAUDI ARABIAN WOMEN IN AL-KHOBAR
M. Al-Sejari
Kuwait University, Kuwait
Menopause is physiological event, experienced as a long process of climacteric change (transition phase that is immediately prior to and after menopause, when clinical, biological, and endocrinological symptoms of menstrual cession commence), occurring universally in all women who reach midlife. The timing of menopause as well as women's experience of menopausal symptoms varies between populations and within populations. Climacteric symptoms have been extensively studied in the developed world as well as in developing countries; but there have been few systematic studies of menopause in Arab countries.
The current study was conducted in 2003 among Saudi Arabian women in the city of Al-Khobar in the East of Saudi Arabia. Biocultural and lifespan perspective were used to assess age at natural menopause and the prevalence of menopausal symptoms. The objectives of the study are (1) to assess the mean and the median age at natural menopause;(2) to detect the factors that might contribute significantly to a more rapid decline in ovarian function experienced among Saudi Arabian women;(3) to determine the factors that significantly affect the prevalence of menopausal symptoms that Saudi Women's experience; and (4) to assess the relationship between women's perceptions and attitudes toward the menopausal event. This study also examines the differences in women's attitudes toward menopause, depending in whether these women were experiencing, or had already experienced natural menopause.
In this cross-sectional study, a face-to-face questionnaire was administrated to 200 Bedouin and Hadar Saudi Arabian women. The mean age of the sample ranged from 40 to 55 years. The finding of this study indicated that while age at natural menopause varied within and among the menopausal factors(anthropometric measures, sociodemographic status, reproductive history, and lifestyle); the only factors that were significantly associated with age at natural menopause were women's weight, marital status, and employment status. The finding also indicated that the respondent's martial status and number of children were significantly associated with the prevalence of menopausal symptoms. Women's attitudes toward menopause varied based on their menstrual status and ethnicity. And there was a significant association between the respondents' total menopausal symptoms reported and their attitudes toward the menopausal event and the women's educational level.
PS-145
BAHRAINI WOMEN'S KNOWLEDGE ABOUT THE MENOPAUSE AND HORMONE REPLACEMENT THERAPY (HRT): IMPLICATIONS FOR HEALTH CARE POLICY
G. Jassim and Q. Al-Shboul
Arabian Gulf University, Manama, Kingdom of Bahrain
Objective: To evaluate knowledge of Bahraini women aged 30–64 years about the menopause and HRT.
Methods: A cross sectional study of 260 Bahraini women attending primary health care centers was conducted. Multistage stratified and clustered random sampling techniques were used. The women were interviewed using a questionnaire containing Menopause and HRT Knowledge scale and sociodemographics. The collected data was coded, entered and analyzed using the statistical package SPSS version (15.0). Relevant descriptive statistics were computed for all items. The equality of means across the categories of each categorical independent variable was tested using either ANOVA or independent samples t-test. The linear relationship between Knowledge Percentage and each of the quantitative independent variables was assessed by Pearson's linear correlation coefficient. Statistical tests with P-value <0.05 were considered statistically significant.
Results: The women's mean age ± SD and mean age at menopause ± SD were 45.04 ± 9.43 and 48.67 ± 2.923 years, respectively. Respondents' median age and median age at menopause were 45.5 and 48.0 years, respectively. Almost half of the women (48.5%) had completed high school or diploma, and 41.5% were currently employed outside home. Over half of the women were pre-menopausal, 19.6% peri-menopausal and 26.9% were post-menopausal.
The Knowledge Percentage mean of all participants was 59.86 with a standard deviation of 25.77. There were significant differences in the knowledge percentage means among categories of education (P = 0.025), and employment (P = 0.005) respectively. No significant differences in the Knowledge percentage means were found among categories of menopausal status. The statement with the highest percentage of correct answers was “Pregnancy cannot occur after menopause” (75.8%). Statements regarding risk of cardiovascular risk had the lowest percentage of correct answers, “HRT increases risk of cardiovascular diseases” (33.8%) and “risk of cardiovascular diseases increases with menopause” (40.0%).
Conclusion: Bahraini women display an average knowledge of menopause and HRT. Health information regarding menopause and HRT to the public and culturally relevant patient education should be improved as they are critical perquisites to any preventive behavioral strategies. Better education needs to be accomplished regarding the long term risk associated with menopause and the pros and cons of HRT.
PS-146
CHARACTERISTICS OF THE GYNECOLOGICAL HISTORY OF A COHORT OF VALENCIAN WOMEN DURING CLIMATERIUM
M. D. Juliá2, J. Quiles1, R. M. Marín3, A. Romeu2, E. Pastor1, F. J. Cháves4, J. Redon4, E. Ruíz1 and M. Escolano1
1Public Health Department Directorate, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 2University La Fe Hospital, Valencian Regional Government Ministries Of Health; 3Valencian School for Health Studies, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain; 4University Clinic Hospital, Valencian Regional Government ministries of Health, Valencia, Valencia, Spain
Objective: To assess the gynecological conditions in a sample of climacteric women in the Valencian Region.
Subjects and Method: Cross-sectional population study in a sample of 675 women from 45 to 65 years old from four different geographic areas in the Valencian Region by personal interview. Statistical analysis SPSS-v12 and STATA/SE v8.
Results: 78.2% of the sample had confirmed menopause. Of them: 85.6% had natural menopause, 1.7% early one, surgical 11% and 1.7% iatrogenic menopause. The average age of menopause was 48.6 years old (DE ± 4,57) and the age of menarche 12.3 years old (DE ± 1,64).
Related to menstrual cycle, 90.5% of the women had normal menstrual cycles, 4.7% oligomenorrhoea, 3.9% proiomenorrhoea and 0.3% other (amenorrhoea, polimenorrhoea, anovulation).
The considered average of gestations by woman was of 2,6 (DE ± 1,28), with a range between 0 and 8. 5.2% of women had not had any gestation. Among the ones who had gestated (640), the average was of 2.05 childbirths (DE ± 1,15). 25.6% of the women had miscarriage and 1.1% ectopic pregnancies. The caesarean section percentage was 11,8%.
84% of the women breastfed. Of them, 89% during less than three months, 10% from three to six months and just 1% more than 6 months.
About the contraceptive methods: 54′6% used just one method, 32% two, and 12% more than two. The methods mostly used were hormonal (32%) and barrier (28%), specially the masculine one and smaller proportion from the feminine one. Other methods used were break coitus (20%), periodic abstinence (2%), the intra uterine device (13%), the tubaric blockade (4%) and the vasectomy of the partner (2%).
Conclusions: The collected data from the gynecological variables of the studied Valencian Region women define the characteristics of a representative group of the climacterical valencian population(+ + ).
(+ )Research Group: Marín RM, Quiles J, Redón J, Chaves J, Romeu A, Juliá MD, Pastor E, Mejía MJ, Marín P, Pérez AF, Bertolín A; Alonso C, Rozada R; Sánchez M; Rico MJ.
(+ + )The data of this study are included in: “Epidemiological Study on Cardiovascular Disease risk during the climacteric period of four different areas of the Valencian Region”. This project was partially financed by Women's Institute of the Department of Job and Social Matters of Spanish Government, Exp. number 65/01.
PS-147
CLINICAL ANALYSIS OF THE PATIENTS WITH PREMATURE OVARIAN FAILURE : COMPLIANCE OF THE TREATMENT
Mi La Kim, Joo Myung Kim, Won Sik Lee, Kwan Young Joo, Hyo Jung Kim and Hyun Chul Lee
Cheil General Hospital and Women's Healthcare Center, Kwandong University, Seoul, Republic of Korea
Objective: We analyse the clinical feature of the premature ovarian failure (POF) and the patients' compliance with hormonal treatment.
Design & Method: Retrospective analysis of 126 patients diagnosed POF were selected between January 2003 and December 2007. The clinical, etiologic features and treatment compliance were evaluated.
Results: The mean age of diagnosis was 33.2 ± 5.2 years. Mean value of FSH was 78.8 ± 28.8IU/L. Most common symptom was amenorrhea or oligomenorrhea (54%). 88 patients were married and 22 of them visited our clinical because of infertility. The etiology of POF was classified to chromosomal, autoimmune related, iatrogenic such as surgery or chemotherapy, environmental and unknown. Most common etiology was unknown (54%) and the second was iatrogenic (30.2%). It showed that only 61 patients were taken hormonal treatment (48.4%). Other 11 patients were not taken HRT because of other medical condition such as breat cancer or liver disease, but followed up regularly (8.7%). Among the treatment group, only 46 patients were followed up over 12 months (36.5%).
Conclusion: About half of women diagnosed POF was not accepted their own problem and delayed the essential treatment. Clinician should educate the importance of early treatment for preventing degenerative changes.
PS-148
CROSS-SECTIONAL COMMUNITY SYRVEY OF MENOPAUSAL SYMPTOMS AMONG JAPANESE WOMEN
A. Taniuchi1, B. Ishizuka1, N. Shimbashi1, S. Igsarashi1, M. Ino1, Y. Watanabe1, T. Shirota1 and Y. Kudo1,2
1St. Marianna University, School of Medicine, Kawasaki, Japan; 2Okayama University of Science, Okayama, Japan
Objective: To determine the characteristics of climacteric symptoms and related factors among 50-year-old Japanese women.
Design & Method: A self-administered questionnaire was mailed to all women aged 50 years (n = 3,166) in 3 northern wards of Kawasaki City regarding 10 menopausal symptoms (hot flushes, sweats, insomnia, depression, palpitations, chills, irritation, headache, fatigue, and stiff shoulders) as well as lifestyle, psychological, demographic, socio-economic and physical factors. The questionnaire included closed-end questions about symptoms over a 1-year recall time frame. The response rate was 55% and women with a history of gynecological or endocrinological disorders and those on HRT were eliminated. We finally analyzed data from 1,169 (35.4%) women.
Results: The prevalence of hot flushes was 36.9%. These, together with sweats, insomnia and depression were associated with menstrual status. All 4 symptoms were also associated with lifestyle and socio-psychological factors. Psychological stress (unease or anxiety) was associated with all 10 symptoms investigated. The two most prevalent symptoms, namely, fatigue (64.7%) and stiff shoulders (75.4%) were associated with psychological and lifestyle factors.
Conclusion: Hot flushes were experienced by more women in the present community-based study than in previous Japanese studies. We found that hot flashes (hoteri in Japanese) are related to menstrual status and thus to vasomotor disturbances. Symptoms both related and unrelated to menstrual status were associated with lifestyle, psychological factors and BMI.
PS-149
CHANGES IN THE PRESCRIPTION RATE FOR HORMONE REPLACEMENT THERAPY ACCORDING TO INDICATION FOLLOWING THE WOMEN'S HEALTH INITIATIVE REPORT IN TAIWAN
T. F. Chan, H. S. Chen, Y. C. Chen, C. J. Shen, C. H. Wu, S. C. Hsu, J. N. Lee and E. M. Tsai
Kaohsiung Medical University Hospital, Kaohsiung 807, Taiwan (R.O.C.)
Objectives: This study aims to investigate whether the prescription rate (PR) for hormone replacement therapy (HRT) in Taiwan varied according to indication between the years 2000 and 2004, following the release of the Women Health Initiative (WHI) report on risks and benefits of HRT.
Methods and Designs: The researchers analyzed out-patient data collected by the Taiwan Health Insurance Bureau for the period 2000–2004. Data on possible confounding factors was examined, including the doctors' gender and age and the age and residence of patients.
Results: The results revealed that, following the release of the WHI report, the PR for postmenopausal syndrome fell from 58.1% to 39.7% (a reduction rate of 31.7%), while for osteoporosis the PR fell from 9.2% to 1.1% (88.1%). For combined postmenopausal syndrome and osteoporosis the figures were 73.3% and 58.3% (20.5%) respectively. After adjustment for hospital type, doctors' gender and age, and patients' age and residence, the researchers found that there were some variations between different specialists. For postmenopausal syndrome, the odd ratios (OR) for gynecologists rose from 1.41 (1.35–1.46, 95%CI) to 2.21 (1.35–1.46, 95%CI) when compared with general physicians. Among orthopedics, the equivalent figures were 0.6 (0.41–0.87) to 1.4 (0.88–2.22). For osteoporosis, the gynecologists' OR fell from 6.1 (5.14–7.22) to 5.38 (3.94–7.35), while among orthopedics the figures were 0.52 (0.46–0.59) to 0.67 (0.53–0.85). For combined postmenopausal syndrome and osteoporosis, the OR among gynecologists dropped from 2.18 (1.99–2.39) to 1.98 (1.75–2.24), while for orthopedics the OR increased from 1.78 (1.28–2.47) to 3.21 (1.72–5.99).
Conclusion: The largest decrease in PR occurred where osteoporosis alone was indicated, while the smallest decrease occurred where combined menopausal syndrome and osteoporosis was indicated. The attitudes towards prescription for HRT vary among the different specialists and indications. Gynecologists' prescription rates are higher than either orthopedics or general physicians. However, following the release of the WHI report on HRT, gynecologists appeared to withdraw such prescription less than general physicians where postmenopausal syndrome alone is indicated, but higher than general physicians where osteoporosis alone or combined postmenopausal syndrome and osteoporosis is indicated. Orthopedics' prescription rates are lower than either gynecologists or general physicians where postmenopausal syndrome or osteoporosis alone is indicated, but higher than general physicians where combined postmenopausal syndrome and osteoporosis is indicated. Although there was a reduction in the PR for all specialists following the release of the WHI report on HRT, orthopedics appeared to withdraw such prescription less than general physicians.
PS-150
CHANGES IN THE PRESCRIPTION RATE FOR HORMONE REPLACEMENT THERAPY FOLLOWING THE RELEASE OF THE WOMEN HEALTH INITIAITVE REPORT IN TAIWAN
E. M. Tsai, T. F. Chan, H. S. Chen, Y. C. Chen, C. J. Shen, C. H. Wu, S. C. Hsu and J. N. Lee
Kaohsiung Medical University Hospital, Kaohsiung 807, Taiwan (R.O.C.)
Objectives: This study aims to investigate the changes in the prescription rate (PR) for hormone replacement therapy (HRT) following the release of the Women Health Initiative (WHI) report on risks and benefits of HRT in Taiwan from 2000 to 2004.
Design and Method: The researchers analyzed out-patient data collected by the Taiwan Health Insurance Bureau for the period 2000–2004. Data on possible confounding factors was examined, including the doctors' gender and age and the age and residence of patients.
Results: The results revealed that, following the release of the WHI report, the PR for HRT decreased from 49.2% in 2000 to 26.6% in 2004. Analysis of possible confounding factors revealed that the PR of gynecologists fell from 63.9% to 49.2% (a reduction rate of 23%), while for orthopedic surgeons the PR fell from 6.2% to 1.4% (77.4%) and for general physicians the figure declined from 37% to 14.6% (60.6%). The results also showed that PR to patients over 60 dropped from 37.3% to 17.6% (a reduction rate of 52.8%) while the equivalent figures for patients under 60 were 56.4% and 35.1% (37.8%). For urban/rural patients the figures were 48.6%–26.9% (44.7%) and 51.5%–25.6% (50.3%) respectively. The PR reduction rate for doctors over 45 years old was 42.6% (50.2% to 28.8%) while for those under 45 it was 49.7% (48.5% to 24.4%). Figures for male doctors showed a reduction rate of 46.3% (49% to 26.3%) while the equivalent figure for female doctors was 42.8% (50.9% to 29.1%).
Conclusion: The release of the WHI report on HRT has significantly reduced the prescription rate for HRT in Taiwan. The attitude of specialists and the age of patients are the two major influencing factors. The decrease in the PR among gynecologists is lower than that of orthopedic surgeons and general physicians. The PR to patients under 60 declined less than that to patients over 60. Other factors, the gender and age of doctors and the residence of patients, have only a minor influence.
PS-151
DESCRIPTIVE ANALYSIS OF THE MENOPAUSE UNIT ACTIVITY AT A UNIVERSITY HOSPITAL
F. Quereda, M. I. Conca, M. Abad and P. Acién
University Hospital of San Juan/Miguel Hernández University/PAA Institute, Alicante, Spain
Objective: to describe the epidemiological profile of patients who were attended at a University Hospital Menopause Unit.
Methods and Design: Descriptive analysis of 729 women who were attended between 1999 and 2007 in our Menopause Unit. Age at the first visit, origin, consultation reason, age at menopause, gynaecological history, prevalence of some important diseases, proportion of deliveries from the Unit and mean time of follow up were considered study outcomes.
Results: Mean age of patients at first visit was 49.9 ± 7.1 years and average age at menopause had been 46.4 ± 5.9 years. 34.0% were derived from other gynaecological offices, 26.0% from general practicioners, 18.9% were hospital workers, 13.5% had an appointment at delivery from the hospital after oophorectomy, and 7.9% were referred from other specialists.
61% of women had had natural menopause, 27.4% surgical menopause, 4.7% menopause secondary to chemotherapy for malignant disease, and 6.9% were at perimenopause at the first visit. 36.6% had been hysterectomized most of them with bilateral oophorectomy, and main reasons for intervention had been large or symptomatic myomas and no reproductive desire (46.6%), endometriosis (14.9%), genital cancer (12.7%), and ovarian tumour (12.3%).
Women came to the Unit or were referred principally to be advocated about possible use of HT (about beginning (40.1%) or to continuing therapy (21.2%)), and for follow up of menopause after cancer (12.8%).
Only 21.8% were asymptomatic, and 56.3% were suffering moderate-severe vasomotor symptoms, 17.2% mild ones, 2.5% only significant psychological symptoms and the rest others.
Prevalence of some important or chronic diseases among our patients were: personal antecedent of depression (14.1%), osteoporosis (11.2%), prior endometriosis (9.9%), prior breast cancer (6.6%), other cancers (6.4%), fibromyalgia (5.8%), other rheumatologic disease (3.3%), increased breast cancer risk (hyperplasia) (2.9%), and 24.3% suffer urinary incontinence.
Finally, the mean follow-up in the Unit was 3.1 ± 2.7 years and the percentage of patients who were delivered during follow-up was 16.5%.
Conclusions: Actually, the patients attended in a Hospital Menopause Unit are high-risk menopausal women, high-affected menopausal women, or women with chronic diseases. Considered altogether, it seems that, effectively, our patients can be more affected in their quality of life and have more difficulties in their management than general population. So, it seems that the existence of a specialized unit is justified.
PS-152
EFFECTS OF AGING ON CLIMACTERIC SYMPTOMS OF JAPANESE POSTMENOPAUSAL WOMEN
K. Takamatsu1, M. Ogawa1 and K. Makita2
1Tokyo Dental College Ichikawa General Hospital, Ichikawa, Chiba, Japan; 2Makita Clinic, Niiza, Saitama, Japan
Objective: Climacteric symptoms are influenced by many factors, including hormonal status, aging, and psychosocial conditions. These factors are complex and interrelated. To investigate the effects of aging, we reevaluated climacteric symptoms of Japanese women.
Design & Methods: Subjects were 388 postmenopausal Japanese women who visited our menopause clinic. All of the subjects had natural menopause. Data from 52 women in their forties (Group–40: mean age ± SD; 47.3 ± 1.7 years, periods after menopause ± SD; 2.4 ± 2.1 years), 138 women in the first half of their fifties, which age range was from 50 to 54 years old (Group-50F: 52.3 ± 1.3 years, 2.9 ± 2.4 years), 137 women in the second half of their fifties (Group-50S: 56.8 ± 1.5 years, 6.0 ± 4.1 years), and 61 in their sixties (Group-60: 64.3 ± 4.1 years, 14.3 ± 7.0 years) were recorded. There was no significant difference in the period after menopause between Group-40 and Group-50F. Climacteric symptoms were assessed at their first visit by use of the Keio Climacteric Questionnaire, which classifies symptoms under 40 headings: 29 physical symptoms and 11 psychological ones.
Results: In general, the prevalence of symptoms increased through Group-50S, but decreased in Group-60. Among the forty symptoms assessed by the Keio Climacteric Questionnaire, general fatigue was the most common symptom in Group-40, -50F, and -50S, but not in Group-60. On the other hand, forgetfulness increased with age, and was the most frequent symptom in Group-60. Shoulder stiffness maintained a high prevalence rate in all age groups.
The prevalence of seven symptoms (hot flashes, sweating, joint pain, irritability, numbness, vaginal dryness, and dysphagia) was significantly higher in Group-50F than Group-40. In Group-60, the prevalence of three of these symptoms (hot flashes, sweating, and irritability) decreased significantly, but that of other symptoms showed no significant change.
Compared to Group-50F, the prevalence of lumbago, loss of hair, and wrinkled skin significantly increased in Group-60, while that of other symptoms was stable or decreased.
Conclusion: Among climacteric symptoms of Japanese postmenopausal women, it is thought that aging more strongly influences joint pain, numbness, vaginal dryness, and dysphagia. As lumbago, loss of hair, and wrinkled skin seemed to be more prevalent in older age groups, it is necessary to manage these symptoms in the early stages of menopause to help maintain patients' quality of life.
PS-153
INVESTIGATING THE SEVIRITY OF MENOPAUSAL SYMPTOMS IN MIDDLE-AGED WOMEN IN KASHAN CITY
M. Abedzadeh, M. Taebi, F. Saberi and Z. Sadat
Kashan University of Medical Sciences, Kashan, Iran
Objective: Menopause is a physiological event that occurs in women's life and result in physical, emotional and social changes. The aim of this study was investigated the severity of menopausal symptoms in middle-aged women in Kashan city.
Design and Methods: In this cross - sectional study we assessed the severity of menopausal symptoms on 700 menopausal women aged 40–60 in Kashan city with cluster sampling. Menopausal Specific Quality of life questionnaire was used for evaluation of menopausal symptoms and other information such as age, job, educational level, marital status, menopausal age, menarche age, duration of menopause and physical activity were collected and analyzed with statistical tests.
Results: Mean and SD of women age was 53.8 ± 4.25 years. 89.9% of women were married and 96% were housewife. Educational level in 51% was under diploma. Mean and SD of menopausal age was 47.6 ± 4.08 years. 24.7% of women had physical activity that in 63.6% of women was 3 time or more in a week.
The most sever symptom in vasomotor domain was sweating (34.1%), in psychosocial domain was feeling anxious or nervous (28.6%), in physical domain was aching in muscles and joints (40.3%) and in sexual domain was change in sexual desire (30%). Also there was a significant relationship between severity of symptoms in vasomotor domain with duration of menopause and menarche age; in psychosocial domain with educational level, job, duration of menopause and physical activity; in physical domain with educational level and physical activity; in sexual domain with educational level.
Conclusions: Considering our findings, we emphasis on teaching about menopause, its symptom and adverse effects. Also emphasizes the necessity use of non pharmacological methods such as exercise and change in life style to improve quality of life in menopausal women.
PS-154
LOWERING THE AGE OF MENARCHE AND INCREASED THE FERTILE PERIOD IN SPANISH POSTMENOPAUSAL WOMEN OVER THE LAST FEW DECADES
N. Mendoza Ladrón De Guevara1, A. González2, A. Salamanca1, F. J. Morón2, D. Galliano1, F. Vázquez3, T. Martínez-Astorquiza 4 and A. Ruíz2
1Hospital Universitario “Virgen de las NIeves”; 2Neocodex; 3Clínica GEOGA; 4Sanatorio Bilbaino
Objetive: Several risk factors for breast cancer and osteoporosis have been identified, including age at menarche and adult height. Studies have consistently shown that women having their menarche at an earlier age have an increased risk for breast cancer compared with women who had their menarche at a later age. On the other hand, delayed menarche has been associated with lower BMD gain and increased risk of Osteoporosis.
The aim of this work is to describe secular trends in age at menarche, height and fertility window in the past decades. For this purpose, we used data on 1779 postmenopausal women who participated in a multicenter study of genetic risk in osteoporosis.
Matherial and Methods: We are conducting a multicenter population-based study of postmenopausal women in Spain. We are collecting clinical and epidemiological data from each of the women using a consensus protocol developed by the clinical researchers involved in this study.
Results: The age of menarche of women in the study was 12.8 years. There was a trend was statistically significant (p < 0.001) towards a decrease in age at menarche associated with the year of birth. The average age of menarche fell 0.2 years (73 days) per decade. With a trend to statistical significance in the fertile period.
The average size of women in the study was 157.1 cm. When we stratify by age birth see a positive trend in this parameter. This increase was 1.5 cm per decade average and was statistically significant (p < 0.001).
Conclusions: It confirms a trend towards a decrease in age at menarche and an increased height and fertile period in Spanish women, with their implications for the processes that occur after menopause.
PS-155
MEMOPAUSE: SOCIAL ASPECTS, POINT OF VIEW OF MEN
M. Ghazli, F. Ouadirga, A. Kazouini, F. Mikou, M. El Karroumi and N. Matar
University Hassan II, CHU Ibh Rochd Casablanca, Morocco
Objective: Appreciate the non explored faced of the social aspect of the menopause, to know the conception of men about it, the factors that influence their perceptions and the consequences that ensue.
Patients and method: A transversal prospective study has been done concerning 400 men of more than 20 years old, choose in a randomized way.
Results: 0.5% of men don't know that women have a menstrual cycle, and 17.6% don't know that a definitive stop of this cycle exists at a certain age.
The term of menopause is only known of 25.3% of the men, the rest uses pejorative expressions of dialectal Arabic to name this period.
The main signs of the menopause are barrenness 33.5%, amenorrhoea 25,4%, and the trouble of the mood 13,1%.
The most known demonstrations of the men are the nérvosity (53.2%), insomnia (36.8%), fatigue (34.3%) and the falls of hair (32.3%).
According to our investigation, 32.9% of men estimated that the menopause represented a danger for the woman's health. 57.6% estimate that it can disrupt the conjugal relation. The repercussion of the menopause on domestic and professional relations is evident for 32.9% of the men.
But 54.4% think that there is no need to treat to menopause because it is a natural evolution of the woman's body, and 33.9% agree with the treatment, 70% know the substitutive hormonal treatment without knowing its characteristics.
Finally, 85% of the men think to need more informations concerning the menopause.
Conclusion: Two main ideas: The ignorance of the menopause phenomenon by most of men and a very important need of information to which it will be necessary to answer.
PS-156
MENOPAUSAL SYMPTOMS IN RURAL WOMEN IN BANGLADESH AND THEIR HEALTH SEEKING BEHAVIOUR
Abdul Halim1, Sameena Chowdhury2, Akteruzzaman3, Ahmed Syed2 and Fazlur Rahman4
1OGSB Hospital and Institute of Reproductive & Child Health, Mirpur, Dhaka, 2Institute of Child & Mother Health, Matuail, Dhaka, Bangladesh, 3Faridpur Medical College, Bangladesh, and 4Centre for Injury Prevention & Research, Bangladesh
Introduction: Menopause is the permanent cessation of menstruation and diagnosed after twelve months of amenorrhoea which may significantly affect the women's health.
Objective: This cross sectional study was aimed to determine the prevalence of menopausal symptoms, health seeking behaviour and quality of life in rural women of Bangladesh.
Methodology: 3814 women of age 40–60 years recruited from randomly selected rural villages of Bangladesh were interviewed to assess the prevalence of menopausal symptoms, their health-seeking behaviour and quality of life.
Results: The mean menopausal age (±SD) was 47.8 ± 5.4 years (range 39–55). 38.2% of the rural women (n = 3814, 40–60 years) were menopausal. Menopausal symptoms namely Hot Flush, Night Sweat, Insomnia, Joint Pain, Bone Pain, Headache, Nocturia, Incontinence, Vertigo and Palpitation were found in high proportion in peri-menopausal women. 65.4% and 26.3% of the menopausal women had experienced hot flush and night sweat while 64.8%, 50.2%, have had it at a level beyond tolerance limit. They also reported joint/bone pain in 45.1%, headache in 33.5%, vertigo in 40.4% and palpitation in 50.2% which were beyond their tolerance limit. 54.3% of the menopausal women reported to have an overall good health while 19.8% had bad or worse. 52.6% had sought health care/counseling from doctor (61%), homeopathic (7.8%), quack (12%) etc.
Conclusion: This study reflects the magnitude of the menopausal symptoms on women health in rural Bangladesh which constitute about 90% of the country population and it demands more attention in respect to awareness building and provision of support and care for their problems.
PS-157
PERCEPTION OF THE MENOPAUSE BY THE WOMAN IN FARMING ENVIRONMENT (INVESTIGATION NEARBY OF 1500 WOMEN)
G. Mahjoub, Z. Hanane, M. Faouzi, E. Mohamed and M. Nourredine
CHU Ibn Rochd, Casablanca, Morocco
The objective of this work is to assess the knowledge and attitudes of Moroccan women face to the phenomenon, its social and psychological impact, and whether there may be regional differences in the approach and experience of menopause.
Patients and Methods: We achieved a transversal survey, on a sample of 1,500 women from different rural areas of morocco, from July 14 of 2005 to April 30 of 2007, inclusion criteria: age superior to 45 years, and spontaneous menopause, and woman of rural areas.
Result: The average age of menopause was 50.27 years, 22.6% of women have a positive view of menopause, but 87.4% have a pejorative view of menopause. They associate it either to the beginning of old age (68.1%), has a break in fertility (71.3%) or a break in sex (17%). 97.9% of female respondents said they had experienced changes during menopause. The impact on the marriage was revealed to be significant (29%), the consultation rate was 60.5%, and hormonal replacement therapy was taken in 2.1% of cases and 63.9% of women unaware of the existence of ‘treatment of menopause.
Conclusion: The impact on married life is more obvious among women in urban areas and consultation at a physician and taking hormonal replacement therapy is more marked among this last group. The ignorance of the majority of women about the phenomenon of menopause, and the low rate of women treated leads us to stress the need for public information on menopause, its challenges, its dangers and its treatment.
PS-158
PREVENTIVE HEALTH- PROMOTING BEHAVIORS OF MENOPAUSAL WOMEN IN CUKUROVA DISTRICT OF TURKEY
Y. Incecik, E. Akpinar, L. Toksoz, E. Saatci, N. Bozdemir, S. Ozcan and H. Kurdak
University of Cukurova, Adana, Turkey
Objective: Menopause is a natural phase in a woman's life cycle, heralded by disturbances in both the flow and time interval of menstrual periods. Menopausal women present health care providers with unique and challenging health issues. The aim of our study was to explore preventive health promoting behaviors of menopausal women living in Cukurova region of Turkey.
Design & Method: Data were gathered through semistructured interviews with 44 women all aged 43 years at baseline who did not have a menstruation at least for one year. During interviews a questionnaire was used including items about demographic characteristics of participants, receiving preventive health care, such as annual pelvic examinations, Pap smear, Dual energy X-ray Absorptiometry (DEXA) scan or mammography screening were investigated and analyzed using the Statistical Package for the Social Sciences.
Results: A total of 44 women aged 53.61 ± 5.8 (min.43, max.66) years old and did not have a menstruation at least for one year (88,6% had more than one year) enrolled in our study. Twenty five percent of the women lived in rural areas and 75% lived in urban areas. The average age at menopause of the women in the present study was 46.54 years. 18.2% of women were illiterate, 4.5% can read and write and 36.4% had elementary school education. 70.5% of women had never menopausal consultation. Although the most (54.5%) afraidable symptom of menopausal is osteoporosis, for the the bone health assessment standard 29.5% women had the DEXA scan, mammography and Pap smear screening regularly (Table 1).
Table 1 Preventive health behavior of menopausal women (n:44)
Conclusion: Health care professionals must consider the menopausal population in the context of their helath care behaviors. Our findings underscore that nonadherence to follow-up of cervical smears, bone density and breast malignancy was uncommon. The gender-specific preventive health care may be in mind of physician in order to follow the clinical guidelines. Along with routine health care, including Pap smears and mammograms, these practices may lessen the incidence of life-threatening, life-disrupting diseases and malignancies.
PS-159
PRESCRIPTIONS ATTITUDES AMONG GP'S, CARDIOLOGISTS AND GYNAECOLOGISTS: A BELGIAN SURVEY
B. Pornel1, M. Dumoulin2 and S. Moyens3
1Brussels Menopause Center, Brussels, Belgium; 2Dedicated Research, Brussels, Belgium; 3Solvay Pharma, Brussels, Belgium
Objective: After some negative data regarding HRT use, followed by reassuring ones about osteoporosis and cardiovascular diseases, it was time to update the hormones prescriptions attitudes by the most concerned Belgian GP's and specialists.
Design & Method: 219 telephonic interviews were conducted for this survey in October 2007: 102 GP's, 52 gynaecologists and 65 cardiologists; Dutch (46%) and French (54%) speaking.
Results: A similar rate of Dutch and French speaking GP's initiated (83%), changed (62%) or interrupted (71%) HRT versus cardiologist who doesn't touch anything (93%). The most frequent reasons to interrupt hormone replacement fo GP's are women with or risking breast cancer (26%), length of the treatment (28%) or a certain age (12%, average age 63 yrs).
The ideal treatment duration is between 4 and 10 years for GP's (62%) and for the Gyn (69%). Respectively 14% of GP and 6% of Gyn are considering HRT for more than 10 years.
GP's more than Gyn (95% vs 86%) have no precise ideas regarding the factors on which the treatment duration depends.
When we ask in practice for how long will patients in average follow their HRT treatment? The GP's answered 56% between 4 to 10 years and the Gyn 61%; more thans 10 years: 10% vs 8%. If 42% of GP's and 33% Gyn prescribe a treatment to prevent osteoporosis during the first 10 years of asymptomatic postmenopausal women, only 34% and 41% will give HRT for this purpose. All of them are giving also calcium or vitamin D.
For the osteopenia prevention confirmed by BMD test and during the first ten years after menopause, 21% of GP's and 37% of Gyn prescribed hormones when no symptoms. When they refuse to give HRT, 99% give calcium or vitamine D.
When light, moderate or severe symptoms appeared, the prescriptions follow a crescendo (51, 62 and 82%). But cardiovascular prevention for women between 50 and 59 years doesn't really represent an indication (13% for GP's, 23% for Gyn).
All physicians from the North and the South of Belgium stated the contra-indications to start HRT (GP's 84%, Gyn 89%).
The mains contra-indications remain breast cancer risk (GP's 70% and Gyn 83%), past or presenting risks of thrombosis (55 and 40% vs 56 and 36%).
Conclusion: Gynaecologists are the most active physicians to manipulate Hormonal Replacement Treatments followed by GP's. Cardiologists don't interfere. Gynaecologists and GP's remained reluctant mainly because of the breast cancer risk. More than 60% of the GP's and Gyn think that the optimal treatment duration is between 4 to 10 years.
Relatively few physicians are prescribing HRT to prevent osteopenia and osteoporosis, but all are considering calcium or vitamine D as an active solution.
Cardiovascular prevention by hormonal substitution is accepted by only one-fifth of the GP's and Gyn.
PS-160
PREVALENCE OF CONTRA-INDICATIONS TO TRADITIONAL HORMONAL THERAPY IN THE CLIMACTERIC PHYTOTHERAPY OUTPATIENT CLINIC IN THE SANTA CASA DE SÃO PAULO, BRAZIL
S. M. R. R. Lima1, B. F. Reis1,2, S. Saito1, A. Ruggero1 and T. Aoki1
1School of Medical Sciences of Santa Casa de São Paulo, São Paulo, Brazil; 2Vale do Sapucai University, Pouso Alegre, Minas Gerais, Brazil
Objective: To evaluate the profile of post-menopausal women with symptoms, who sought the service of an alternative therapy rather than traditional hormonal therapy.
Methods: We included 230 women with ages ranging from 40 to 65 years, with time of menopause greater than a year with symptoms identified by the Kupperman Menopausal Index, attended in the Climacteric Phytotherapy Outpatient Clinic in the Santa Casa de São Paulo, Brazil, in the period from January to April 2007. The patients had a diagnosis of climacteric based on the clinical data, and had not had prior treatment with hormones for menopause, or had the use of antimicrobial activity or other nutritional supplements for this indication for at least six months before the start of the study. The reason why they sought the service was questioned at the beginning of treatment and the other risk factors that were mentioned the traditional hormonal therapy.
Results: The average age of women was 53.7 years, with the menopausal age of 47.3 years and post-menopausal ranging from 1 to 20 years, with an average of 6.7 years. The reasons that contra-indicate the traditional hormonal therapy were: 70% preference for non-synthetic drugs, 11.6% of contra-indications for hormone-dependent diseases; 11.6% without preference for any of the treatments and 5.8% non adherence to traditional hormonal therapy. The fear of increased incidence of cancers has been reported as one of the possible side effects and the main reason for the choice of phytomedications.
Conclusion: Currently there is great demand for medical services that offer a range of therapeutic possibilities, because the public knows instinctively that the complementary approaches play an important role in the remission of symptoms. The World Health Organization (WHO) in the year of 1978, recognized phytotherapy as a valid form of treatment and should be prescribed after advising of its risks and benefits. There is still the need for more knowledge and information about these medications.
PS-161
PREVALENCE OF MENOPAUSAL SYMPTOMS IN DIFFERENT MENOPAUSAL STATUS: A COMPARATIVE ANALYSIS
M. Prasit1, C. Sakondhavat2, K. Lao-unka1, S. Soontrapa2, S. Kaewrudee2, W. Somboonporn2 and P. Tharnprisan1
1Srinagarind Hospital, Khon Kaen, Thailand; 2Khon Kaen University, Khon Kaen, Thailand
Objective: To determine and compare prevalence of menopausal symptoms of women in different menopausal status at the Menopausal Clinic, Srinagarind Hospital, Khon Kaen, Thailand.
Design & Method: This descriptive analytical study was conducted at Srinagarind Hospital, Khon Kaen, Thailand. We retrospectively reviewed the questionnaires of one thousand and two hundred twenty-one women who attended the Menopause Clinic at Srinagarind Hospital during January 1997 to December 2006. The questionnaire comprised of 23 menopausal symptoms. The menopausal status was divided into 2 groups that were surgical induced menopause and natural menopause. For the latter group, we divided into 2 subgroups, perimenopausal group and postmenopausal group. The results were expressed as mean value ± standard deviation. Chi-Square test was used for statistical comparison. The level of statistical significance was chosen as p < 0.05.
Results: Mean age of the subjects was 51.53 ± 6.05 year-old. 52.82% were postmenopausal group. Mean age of natural menopause was 48.76 ± 4.33 years. The three most common menopausal symptoms were forgetfulness (90.90%), muscle/joint pains (87.05%) and tiredness (83.12%). For the comparative analysis, the prevalence of hot flushes was significantly higher in women with surgical induced menopause (70.7%) than those in women with natural menopause. Mood disorders and a decrease in sexual desire were most commonly found in perimenopausal group (87.6% and 75.5%, respectively) while the prevalence of vaginal dryness was highest in postmenopausal group (62.8%).
Conclusion: Menopausal symptoms differ among three menopausal statuses. Biologically, an abrupt decline in estrogen levels induced the occurrence of hot flushes and this may explain the highest prevalence of hot flushes found in the group of women with surgical induced menopause. The hormonal fluctuation in perimenopausal period may affect mood and sexual desire while sustained low estrogen levels found in postmenopausal women associates with atrophy of urogenital organs.
PS-162
PREVALENCE OF OVERWEIGHT AND OBESITY IN ARGENTINE POSTMENOPAUSAL WOMEN; RELATIONSHIP WITH CLINICAL PARAMETERS AND SELF-PERCEPTION OF CORPORAL IMAGE
M. Martino, L. Rinesi and P. Figueroa Casas
SOMUPO Cooperative Group, Argentina
Objective: The principal objective was to establish, in a group of Argentine postmenopausal (PM) women, the prevalence of overweight (OW), obesity (OB) and increased waist perimeter (WP), factors which raise both cardiovascular disease (CVD) and metabolic syndrome (MS) risk. The secondary objective was to correlate the body mass index (BMI) and WP to several clinical parameters and self-perception of corporal image.
Design and Methods: Descriptive, observational study, based on an anonymous questionnaire and measurement of physical parameters (weight, height and WP) among PM women, aged 46–60 years (y), selected at random in Gynaecology offices during 2007. They should have uterus and at least one ovary, no cancer history and absence of hospitalisation during the previous six months.
Results: 1221 women were included. Prevalence of OB and OW was 21,9% and 33,1%, respectively, and WP increase was (≥88 cm), 49,5%. Median age of: participants 54.2 y, menopause 48.0 y and PM length 6,3 y were not significantly related to either BMI or WP. Among hypertensive (26.3%) and diabetic women (6.2%) a significant relationship with higher BMI and WP values was found. Users of hormonal therapy (20.2%) showed significant lower BMI and WP rates when compared to non-users. There was no significant association among those who were on some type of diet (31.4%) or current smokers (20.9%) concerning BMI or WP increase. 55.5% of participants performed physical activity; they had significantly lower BMI and WP values when compared to sedentary women. According to BMI, 0.6% had low weight, 44.4% normal, 33.1% OW and 21.9% OB. Only the first group showed a significantly different self-perception: 10.3% of women considered themselves to be thin. In the other three groups, self-perception showed no significant differences related to BMI: 41.2%, 43.2% and 5.2%, respectively.
Conclusion: This study showed one negative result related to health issues as around half of PM women of our area showed OW, OB and WP above normal values implying a CVD high risk and giving support to the need for immediate counselling and/or interventions. Positive results as low prevalence of smoking, dieting in one third of women, physical activity in half and a proper self-perception of body image in most participants may facilitate the task to be undertaken.
PS-163
THE PERCEPTION OF THE MENOPAUSE: POINT OF VIEW OF THE PARAMEDICAL STAFF
M. Ghazli, A. Kazouini, F. Ouadirga, F. Mikou, M. El Karroumi and N. Matar
University Hassan II, CHU Ibh Rochd Casablanca, Morocco
Objective: Evaluate the knowledge of the paramedical staff about the menopause, its treatment and to appreciate their attitude towards the HRT (Hormonal Replacement Therapy).
Patient and method: Prospective study about 500 women of the paramedical staff, exercising in the three sectors of health and in five cities of Morocco during 6 months, from August 1st, 2005 to February 1st, 2006.
Results: The average was 48 years old, 87% were nurses, 36, 4% menopausal.
For 71,8%, the menopause is the definitive stopping of the menses or its equivalents, the age it occurs is 45 to 55 years for 88% of the women, it is influenced by the genetic factors for 57,6% and by the age of the puberty for 74,4% of the involved women.
According 89,4%, the menopause may occur after the perimenopause. For 3% only, it may occur suddenly or after a perimenopause.
The symptoms consist in hot flushes (94,8%), amenorrhoea (90,8%), nervosity (83,2%), nocturnal sweats (80,4%), tiredness and headaches (74,8%), osteoarticular pains 67,8%, sexual disorders (55,8%), depression (48%), memory disorders (40,6%), and cutaneomucous signs (35,8%).
50,8% agree with medical treatment of the menopause. But only 11, 53% of the menopausal participating women are under treatment, 77% refuse it and 11% stopped it because of various reasons that the main one is the fear of cancers.
54% think that the treatment contains risks generally in relation with the development or the provocation of the cancers.
73,4% don't know the controversy caused by the use of the HRT.
Conclusion: The necessity of information and a formation of the paramedical staff on the menopause remain very important. It incites to elaborate a strategy to make all actors of health to participate to palliate the insufficiency of information noticed at this staff and to demystify really the topic of the menopause in all layers of the society.
As the paramedical staff succeeded in the domain of the contraception, it is able to succeed also in the menopause.
PS-164
THE INFLUENCES OF BENIGN GYNECOLOGICAL DISEASES ON MENOPAUSE - THE TRANSITION OF AGE OF MENOPAUSE AND LIPID PROFILES -
K. Hosokawa, H. Iwasaki, K. Mitsuya, H. Satomi, N. Fukuno, M. Kaneshima and N. Kamitani
Fukuiken Saiseikai Hospital, Fukui, Japan
Objective: To evaluate the influences of benign gynecological diseases on the age of menopause and lipid profiles around it.
Design & Methods: The study group consisted of 367 women ranging from 35 to 60 years of age at the start of investigation who have taken annual medical check-ups in our hospital from April 2000 through March 2007, with no past medical history of any operation of the uterus or ovary, and who have not received any hormone therapy. Every time, history taking, body measurements, pelvic examination, transvaginal ultrasound, laboratory studies were performed, and based on these data, the time of menopause was medically predicted. The study group was divided into two groups, the disease group (93 who was clinically diagnosed for one of the following: uterine myoma, adenomyosis, endometriosis, benign ovarian tumors), and the control group (the remaining 274), where menopausal age was compared. Next, 127 who were diagnosed for menopause during this study period (menopause group during study period) was extracted, this was divided into two groups, as the whole study group, and serum lipid levels for different ages starting from menopause age as zero, were measured.
Results: The 50%-menopausal age of the study group in the last investigated year was 50.79 for control, 51.98 for the disease group, and the rate of not entering menopause was significantly higher (Odds ratio = 1.77) for the disease group. During the period of investigation, changes in total cholesterol and LDL-cholesterol levels between ages menopause −5 to + 5, was 180.4 → 223.9 (mg/dl), 110.6 → 140.0 (mg/dl) respectively for control. In comparison, for the disease group, it was 237.4 → 177.0 (mg/dl), 164.3 → 108.5 (mg/dl) respectively, which showed remarkable decrease. The triglycerides levels varied in a manner similar to the above lipids, but there was no significant change in HDL-cholesterol levels for both groups.
Conclusion: When untreated benign uterine or ovarian diseases existed, menopause was delayed, and lipid profiles seemed to be improved through the menopause transition.
New regimens
PS-165
ADVANCES OF NEW HORMONE REPLACEMENT THERAPY IN WOMEN WITH SURGICAL MENOPAUSE” VERSUS ON WOMEN WITH “NATURAL MENOPAUSE”
P. Tsikouras, G. Galazios, C. Zografos, E. Skyfta, C. Panagiotidou, N. Koutlaki, V. Liberis and A. T. Teichmann
Obstetrics And Gynecology, Greece
Introduction: Postmenopausal hormone replacement therapy HRT has been seen as a specific treatment for symptoms in the short term and preventative therapy in the long term. In this retrospective study we aimed to compare the effects of a new HRT regime on symptoms and complains of women with natural menopause versus those with surgical one.
Material and Methods: During the period from 1 January 2006 to 30 November 2007 in seventy six women was administrated HRT, 1 mg 17β-estradiol (E2) combined with 2 mg drospirenone (DRSP) in a continuous-combined regimen), for daily intake. The study participants had climacteric symptoms after naturally or surgical menopause and were examined in the Menopause centre in the Department of Gynecology of the Democritus University Hospital in Alexandroupolis (twenty six women ) and Department of Gynecology of the Teaching Hospital in Aschaffenburg (fifty women). 76 women totally were enrolled in 2 groups: N (natural menopause), and S (Surgical menopause) to answer to a questionnaire regarding climacteric symptoms after menopause. Only 70 women, 40 women in group N and 30 women in group S completed the questionnaire correctly and answered a wide range of questions concerning their psychological profile. The efficacy and side effects of the HRT were studied after 3,6,12,18 months of treatment.
Results: In both groups the patients-characterics were similar. The mean age was 49,5 years old. The study women have not been treated with any HRT for estrogen deficiency symptoms prior to start of the observational period, had never any gynecological malignancy or other serious disease in the past. In the group S the participants had abdominal or vaginal hysterectomy with bilateral oophorectomy for benign conditions and were recruited into study one month after the operation.
Only 6 patients in S group presented transitional postoperative depression.
During the 23-months follow up HRT therapy effectively reduced menopausal complaints especially hot flushes and night sweats after three months of the therapy. No serious side effects were observed. Only 9% of the women reported adverse effects (headache, nausea), which turned out to be transitional. N group of women reported less problems compared to S group, but there were no significant differences in their total climacteric profile.
Conclusion: HRT with 17β-estradiol and drospirenone is a valuable treatment option for women with climacteric complaints. Additional studies will determine whether the promise of increased safety with this therapy will be realized.
PS-166
DROSPIRENONE INCREASES ENDOTHELIAL NITRIC OXIDE SYNTHESIS VIA A COMBINED ACTION ON PROGESTERONE AND MINERALOCORTICOID RECEPTORS
A. M. Sanchez, M. I. Flamini, M. S. Giretti, X.-D. Fu, L. Goglia, S. Garibaldi, C. Baldacci, P. Mannella, A. R. Genazzani and T. Simoncini
Molecular and Cellular Gynecological Endocrinology Laboratory (MCGEL); Department of Reproductive Medicine and Child Development, University of Pisa, Italy
Background: Progestins have actions on the cardiovascular system, which depend on the structure as well as on receptor binding characteristics. Drospirenone (DRSP) is a progestin that uniquely interferes with the signaling of the mineralocorticoid receptor (MR). Hormone therapy containing DRSP results in blood pressure reduction in hypertensive post-menopausal women.
Objectives: We describe the effects of DRSP on endothelial nitric oxide (NO) synthesis and compare them with those of progesterone (P) and of medroxyprogesterone acetate (MPA) highlighting the differences in the signal transduction induced by these compounds through P and MRs. In addition, we herein tested the relevance of the anti-mineralocorticoid activity of DRSP for NO synthesis.
Results: DRSP results in rapid activation of the endothelial NO synthase (eNOS) through mitogen-activated protein kinases and phosphatidylinositol 3-kinase as well as in enhanced eNOS expression. These actions depend on P receptor. When the cells are exposed to aldosterone, a reduction of eNOS expression is found that is antagonized by DRSP. This action is not shared by P or MPA. In addition, DRSP does not interfere with the induction or activation of eNOS induced by estradiol, as opposed to MPA.
Conclusions: In conclusion, we show that DRSP exerts a complex array of actions on human endothelial cells. Some of these effects are mediated by PRs but others depend on the interference with the MR. This unique mix of molecular actions on human endothelial cells sheds light on some of the actions of this compound on vascular function and help to interpret the anti-hypertensive effects of hormonal therapies containing DRSP.
PS-167
TRANSCRIPTIONAL RESPONSES TO PULSED VERSUS CONTINUOUS ESTRADIOL EXPOSURE IN HUMAN UMBILICAL VEIN ENDOTHELIAL CELLS
J. Li1, H. Wang1, S. Johnson2, E. Horner-Glister2, J. Thompson2, I. White2 and F. Al-Azzawi1
1University Hospitals of Leicester, Leicester, United Kingdom; 2University of Leicester, Leicester, United Kingdom
Objective: Comparable doses of Estradiol−17β (E2) administered orally, transdermally or by nasal spray are equi-potent in controlling vasomotor symptoms. However, the frequency of mastalgia and the amount of uterine bleeding are significantly lower with pulsed treatment compared with other routes of administration. To help address the exact roles of pulsed versus continuous estrogen-mediated gene regulation in the human endothelial cell model, we hypothesized that the identification of a set of hormone responsive genes could provide evidence for a differential effect specific to mode of administration.
Design & Method: We treated human umbilical vein endothelial cells (HUVECs) with E2 for 5 days as 1 h pulse or 24 h continuous treatment at concentrations such that the 24 h exposure (concentration × time) was identical in both conditions. Transcriptional profiling was performed using the Affymetrix GeneChip microarray analysis. Cell proliferation was studied and changes in morphology and apoptosis in HUVECs were examined with flow cytometry and electron microscopy.
Results: Cell proliferation was significantly decreased over days 3–5 with pulsed E2 treatment relative to constant exposure (P<0.05). Microarray results showed that after 5 days, 801 genes differed (P<0.05) between continuous versus pulsed E2 treatment. In addition, relative to controls, a total of 640 genes were up- or down-regulated by E2 either in the continuous or pulsed treatment. Of these, only 231 (36%) were down-regulated by E2, whereas the majority; 409 (64%) were up-regulated. Functional analysis showed a significant number of genes to be associated with apoptosis and cell cycle pathways. Flow cytometry and electron microscopy examination showed no evidence of apoptosis.
Conclusion: Our study presents the first microarray data on normal human endothelial cells after 5 days in culture rather than the short-term effects reported on tumor cells. These data highlight a large number of significantly different molecular responses to E2 dependent upon the mode of administration of E2, particularly in genes involved in apoptosis and proliferation including VEGF, IGF receptors, and thrombospondin-1.
Women and heart disease
PS-168
AGE, RISK FACTORS AND HOSPITAL MORTALITY IN ACUTE MYOCARDIAL INFARCTION THROUGHOUT THE CLIMACTERIC PERIOD
P. Nogueira, L. Ribeiro, R. Berber, E. Alexandre, E. Santos, A. Timerman, C. Gun, R. Ramos and L. Piegas
Dante Pazzanese Institute of Cardiology, São Paulo, Brazil
Objective: The aim of this study was to analyze if there was any correlation between age, classical risk factors, hospital mortality and type of Acute Myocardial Infarction (AMI) throughout the climacteric period.
Design: 349 consecutive patients (pts) were hospitalized in our Institution, with Acute Myocardial Infarction (AMI), over the period of 2000/01 to 2004/07. 46 pts were women and the patients' ages range from 40 to 65 years (mean 55,5y ± 6,86). All of them had AMI diagnosed by World Health Organization (WHO) criteria (typical pain, ECG, enzymes – at least two from these three). They were divided in two groups according to the ST segment analysis: one group with ST elevation (STEMI) and the other with non-ST elevation (NSTEMI). The risk factors (RF) analyzed were defined as high blood pressure (HBP), diabetes mellitus (DM), hyperlipidemia (Hyperlip) and cigarette smoking (Smoking). Hospital Mortality was defined as cardiovascular mortality during the hospitalization period.
Results: See the table below:
Conclusion: Despite of the different hormonal profile throughout the climacteric period there was no significant age difference between the two AMI groups (p = 0,35) neither between hospital mortality (p = 0,58). The most prevalent RF was HBP followed by Smoking, Hyperlip and DM, however there was no statistical significance between the two AMI groups.
Table 1 Age, Risk Factors and Hospital Mortality
PS-169
ANTIOXIDANT EFFECT OF ESTROGEN ON BOVINE AORTIC ENDOTHELIAL CELLS
Gun-Young Chun, Sue-Yeon Kim, Jin-Hong Kim and Mee-Ran Kim
Catholic University Of Korea, School Of Medicine
Objective: To examine the role of estrogen as an antioxidant in the damage of vascular endothelial cells by oxidative stress.
Design: 17β-estradiol (E2) treated bovine vascular endothelial cell line bovine Aortic Endothelial Cell (bAEC) was incubated with 1 mM H2O2 for 15, 30, or 60 minutes. The cell survival was evaluated by 3-(4,5-dimethylthiazol-2-yl)- 2,5-diphenyl-tetrazolium bromide (MTT) assay and fluorescence activated cell sorter (FACS), and the Hoechst 33342 staining was used for morphologic characteristics of cellular apoptosis. Oxidative stress was evaluated by measurement of intracellular reactive oxygen species (ROS) and Western blotting for phospho-p38, p38, and Bcl-2 was performed to examine the expression of proteins involved in apoptosis after oxidative stress.
Results: MTT assay showed that bAEC viability was reduced to 55.7 ± 3.0%, 39.1 ± 3.7% after 30 and 60 minutes of H2O2 treatment, respectively. E2 and H2O2 treated cells did not show significant decrease in the cell survival. Similarly in the FACS analysis, the treatment with H2O2 increased the apoptosis of bAEC by 48.8 ± 2.4%, and by the pretreatment with E2, it decreased by 3.5 ± 2.4%. Intracellular ROS increased by 181.6 ± 68.9% in H2O2 treated cells and by 37.0 ± 3.9% in E2 and H2O2 treated cells (P<0.05). Hoechst 33342 stain showed the morphological evidence that the pretreatment with E2 decreased cellular apoptosis induced by H2O2. The expression of phospho-p38 MAPK was higher in E2 and H2O2 treated group than H2O2 treated group and decreased after the pretreatment with the phospho-p38 MAPK inhibitor SB203580.
Conclusions: E2 mediates antioxidant effects on the oxidative stress induced by H2O2. This antioxidant effect on bAEC may elucidate the scientific basis of hormone replacement therapy for maintaining cardiovascular integrity in postmenopausal women.
PS-170
ARTERIAL STIFFNESS AND ENDOTHELIAL FUNCTION IN POSTMENOPAUSAL WOMEN WITH AND WITHOUT HOT FLUSHES
P. Tuomikoski1, P. Ebert1, P.-H. Groop1,2, P. Haapalahti1, H. Hautamäki1, M. Rönnback1,2, O. Ylikorkala1 and T. S. Mikkola1
1Helsinki University Central Hospital, Helsinki, Finland; 2Folkhälsan Research Center, Helsinki, Finland
Objective: Menopausal vasomotor symptoms may indicate the sensitivity of the heart and blood vessels to menopause-induced hypoestrogenism. Since no data exists on the impact of menopausal hot flushes on arterial stiffness and endothelial function, we assessed these factors between healthy, recently postmenopausal women with different severities in symptoms status.
Design & Method: Over 400 women recorded their vasomotor hot flush symptoms on structured questionnaire for two weeks. Hundred and forty-three healthy women between the age of 48–55 years were included; 22 were asymptomatic, 33 had mild symptoms, 29 had moderate symptoms and 59 suffered from severe vasomotor symptoms. Arterial stiffness expressed as aortic augmentation index (AIx) was assessed by pulse wave analysis (PWA). Endothelial function was assessed by using nitroglycerin (maximal endothelium-independent vasodilatation) and salbutamol (maximal endothelium-dependent vasodilatation). Endothelial function index (EFI), defined as the maximum change in AIx induced by salbutamol divided by the maximum change in AIx induced by nitroglycerin, expressed as a percentage was calculated.
Results: AIx and EFI were in asymptomatic women 23.7 ± 1.7% and 21.3 ± 11.2%, in women with mild symptoms 22.6 ± 1.4% and 37.7 ± 16.1%, in women with moderate symptoms 22.0 ± 1.3% and 24.7 ± 6.2%, and in women with severe symptoms 22.1 ± 1.1% and 26.7 ± 5.2%, respectively. Arterial stiffness or EFI were not dependent on the severity of symptoms.
During treatment with nitroglycerin T1 (time [in milliseconds] for the waveform to reach 1st systolic peak) was 115.5 ± 3.5 in asymptomatic women and 131.5 ± 3.4 in women with severe symptoms. TR (time [in milliseconds] to the return of the reflection of the aortic waveform) was in asymptomatic women 149.8 ± 2.2 and 164.0 ± 2.6 in women with severe symptoms. There was a significant difference in T1 (p = 0.024) and TR (p = 0.012) between women with severe symptoms when compared to asymptomatic women. All data expressed as mean ± SEM.
Conclusion: We did not detect major difference in arterial stiffness or endothelial dysfunction in postmenopausal women with frequent vasomotor symptoms compared to asymptomatic women. However, we show that in women with severe symptoms T1 and TR during nitroglycerin were longer compared to asymptomatic women implying differences in the central adjustment of vessel tone, and suggesting a more profound autonomous nervous system regulation in symptomatic women.
PS-171
ASSESSMENT OF ASYMPTOMATIC CORONARY ARTERY ATHEROSCLEROSIS IN POSTMENOPAUSAL WOMEN
Ki-Hyun Park1, Byung–Seok Lee1, Hwa-Sook Moon2, Dong-Han Bae3, Hyuk Jung4, Won-Young Pak5, Heung-Yeol Kim6, Jin-Hong Kim7 and Kyu-Seop Lee8
1Yonsei University School of Medicine, Seoul, Korea; 2Good Moonwha Hospital, Busan, Korea ± ; 3Soonchunhyang Medical school, Chunan, Korea; 4Chosun University College of Medicine, gwangju, Korea; 5Kyung Sang University College of medicine; 6Kosin medical school, Busan, Korea; 7The catholic university, Seoul, Korea; 8Pusan University College of Medicine, Busan, Korea
Objective: It is important to assess the asymptomatic atherosclerosis status in postmenopausal women for effective management of postmenopausal symptoms. Multidetector computed tomography (MDCT) assesses the coronary calcium plaque burden by way of assessing the vessel wall calcium deposition, and at the same time non-calcified plaque can also be detected. We conducted a cross-sectional study on asymptomatic postmenopausal women using MDCT and small dense LDL which is currently considered important as a cardiovascular risk factor on entering menopause.
Design & Method: The atherosclerotic status was assessed in 287 healthy asymptomatic postmenopausal women from March 2003 until December, 2007 with either 16 or 64 channel multi - slice CT (Sensation 16, Siemens, Germany). LDL subfraction was analysed by polyacrylamide tube gel electrophoresis (Quantimetrix TM LDL system,Redondo Beach, CA, USA). Statistical analysis was done using SPSS version 12.0.
Results: The mean age of the patients was 57.5 ± 7.43 years, and the mean BMI 23.21 ± 3.2 Kg · m2. By linear regression, the age (r = 0.33; p < 0.036) and LDL subfraction (r = 0.34; p < 0.033) showed statistically significant correlation with CACs (Coronary Artery Calcification Scoring). The change of % CAC positivity (CACs>0) according to the age start to accelerate from around the late age 50 s. We found out noncalcified plaque in 6 out of total 101 patients by 64 channel multi - slice CT.
When analysing the patients according to the mean LDL particles size, type A patients showed statistically lower CAC than type B patients (small dense LDL)(1.7 vs 52.82 ± 108.46; p < 0.0001).
Conclusion: Evaluation of coronary athelosclerosis using direct noninvasive Multidetector computed tomography(MDCT) in postmenopausal women is encouraging tools for detection of asymptomatic coronary atherosclerosis to prevent cardiovascular events, especially when considering of HT. And assessment of LDL subclass is also helpful tool for estimation of CAD risks in postmenopausal women.
PS-172
CARDIOMETABOLIC SYNDROME RISK FACTORS AND LOW BONE MINERAL DENSITY
B. Meneses, A. Esparza, A. Sao, J. Bello, Ll. Cabero and F. Baró
Vall d' Hebron University Hospital, UAB, Barcelona, Spain
Objective: To show association between several components of the cardio metabolic syndrome such as hypertension, increased triglycerides, and reduced high-density lipoprotein cholesterol (HDL-c) and the presence of low bone mineral density (BMD).
Design & Methods: Retrospective study in 275 postmenopausal women aged from 40–60 years. We determined the frequency of cardiovascular risk factors and obtained systolic and diastolic arterial pressure and blood levels of low-density lipoproteins (LDL-c), high-density lipoproteins (HDL-c), triglycerides and glycaemia levels that were determined by routine test in patients stratified with low BMD [osteoporosis (values under 2,5 SD) and osteopenic (values between -1 and -2,5 SD)]. Determinations were made with densitometry in lumbar spine and femur. Statistic analysis between categories of BMD and mean cardiovascular risk factors was performed by analysis of variance.
Results: The 88,3% of patients showed low BMD (73% in lumbar spine and 75% in femur). The 22,3% was obese, 26,6% had high arterial pressure, 49% serum lipids alteration, 7,4% diabetes and 15% vascular disease: coronary, cerebral and peripheral.
The negative correlation between lumbar BMD and diastolic arterial pressure (p-value 0,004), triglycerides level (p-value 0,002), low-density lipoproteins (LDL-c) (p-value 0,039) and PCR (p-value 0,01). The correlation analysing low femur BMD did not show these correlations.
Conclusion: In conclusion, accumulating evidence indicates that low bone mineral density might be part of the risk factors for cardio metabolic syndrome. Nonetheless further studies are necessary to establish the correlation between elements of cardio metabolic syndrome and the patho-physiological mechanisms for low lumbar and femur BMD.
PS-173
CARDIORESPIRATORY FITNESS IS ASSOCIATED WITH INSULIN SENSITIVITY, ANTHROPOMETRIC AND METABOLIC PROFILE IN PREMENOPAUSAL WOMEN: A MONET STUDY
J. Abdulnour1,2, E. Doucet1,2, P. Boulay2, M. Brochu3, R. Rabasa-Lhoret4, S. Yasari1,2 and D. Prud'homme1,2
1University of Ottawa, Ottawa, ON, Canada; 2Behavioral and Metabolic Research Unit, Montfort Hospital, Ottawa, ON, Canada; 3Université de Sherbrooke, Sherbrooke, PQ, Canada; 4Université de Montréal, Montréal, PQ, Canada
Many studies have shown that cardiovascular disease (CVD) is the first cause of mortality in women. Cardiorespiratory fitness (CRF) has been demonstrated to be an independent predictor of the risk of mortality and cardiac events among asymptomatic women. Interestingly, it has been reported that women with an % predicted CRF (%CRF) of less than 85% of the age-predicted value are at a higher risk (hazard ratio of 2.44) of death from cardiac causes than those with at least 85% of the age-predicted value. In addition, women with less than 100% of the age-predicted value show some functional impairment.
Objective: To investigate the anthropometric and metabolic determinants of %CRF for a given age in asymptomatic premenopausal women.
Design & Method: The sample consisted of 97 healthy premenopausal women (age: 49.9 ± 1.9 yrs; BMI: 23.3 ± 2.2 kg/m2) participating in a longitudinal study on the effect of menopause on body composition and cardiovascular risk factors. All women underwent a stress-test on treadmill to measure VO2 peak. A nomogram was used to determine the % of predicted CRF achieved (%CRF) according to their age and the measured VO2 peak. Body composition was measured by dual-energy x-ray absorptiometry (DEXA) and abdominal fat by axial computed tomography. Other measurements included blood pressure and fasting lipid samples. Insulin sensitivity index (SIisOGTT, HOMA-IR), insulin and glucose areas under the curve (AUC) were calculated during OGTT.
Results: Body mass index, fat mass, fat-free mass, %fat, waist circumference, triglycerides, triglyceride/HDL-C, total cholesterol/HDL-C, insulin, HOMA-IR score, mean AUC of plasma insulin and the SIisOGTT score were all significantly related to %CRF (−0.47>r<0.35; P<0.05). Areas of abdominal adipose tissue (AT) were also significantly (P<0.01) correlated with %CRF: total AT (r = −0.36), subcutaneous AT (r = −0.30) and visceral AT (r = −0.39). A stepwise multiple regression analysis showed that % fat, plasma triglycerides and total abdominal AT were significantly related to the inter-individual variation observed in %CRF (R2 = 0.463, P<0.01). In addition the women were divided in two groups (high>100%; low<100%) of the %CRF. Fasting plasma insulin, HOMA-IR score and insulin AUC during OGTT were found to be significantly different between groups (P<0.05).
Conclusion: This study underlines the importance of % predicted cardiorespiratory fitness in healthy women and suggests that a high %CRF is associated with better anthropometric and metabolic profile and particularly insulin sensitivity, reducing the risk of CVD.
PS-174
COMPARISON BETWEEN CARDIOVASCULAR RISK FACTORS IN POSTMENOPAUSAL CHINESE AND AUSTRALIAN WOMEN
C. J. Haines
The Prince of Wales Hospital, The Chinese University of Hong Kong, Shatin, NT, Hong Kong
Objective: As of 2002, the standardized death rate from ischaemic heart disease became higher in Chinese than in Australian women (63 vs 56 deaths per 10,000 women). The aim of this study was to compare various cardiovascular risk factors in the two populations as well as in Hong Kong Chinese women.
Design & Method: We compared the prevalence of various cardiovascular risk factors using data provided by WHO as well as local data.
Results: There was a clear disparity in the prevalence of cardiovascular risk factors between Chinese and Australian women. While Australian women had a higher prevalence of overweight and obesity as well as hypercholesterolaemia, Chinese women had a higher prevalence of hypertension and diabetes. In our own “healthy” population of postmenopausal Hong Kong Chinese women, 46% were either overweight or obese and 62.4% had either borderline or elevated concentrations of total cholesterol. 30.5% and 13.1% respectively had systolic or diastolic blood pressures in the range of high normal or Grade 1 hypertension.
Conclusion: Compared with recent years, these data suggest that the prevalence of all cardiovascular risk factors is rising in postmenopausal Chinese women. It can be anticipated that cardiovascular disease will soon be a far greater problem in this region than it is at present. We are uncertain why such an imbalance in the distribution in cardiovascular risk factors exists between Chinese and Australian women, but we assume that in the Chinese population it has resulted from the failure of the body to adjust to a relatively rapid change in both diet and lifestyle.
PS-175
COMBINED EFFECT OF GENISTEIN, MEDITERRANEAN DIET AND PHYSICAL EXERCISE ON INSULIN SENSITIVITY ON GLUCOSE HOMEOSTASIS IN MENOPAUSAL WOMEN
A. Alonso1, P. Llaneza2, J. Fernández Iñarrea3, M. J. Díaz4, C. González1 and Y. J. Ferrer2
1Department of Functional Biology, Oviedo University, Oviedo, Spain; 2Central University Hospital of Asturias, Oviedo, Spain; 3Cabueñes Hospital, Gijón, Spain; 4Valle del Nalón Hospital, Oviedo, Spain
Objective: Present work was designed in order to evaluate if the practice of aerobic, moderate and regular exercise and Mediterranean diet (Control group, CG), or the same therapeutic recommendations including the administration of a single oral daily dose of genistein (40 mg), (Genistein Group, GG), were able to improve glucose homeostasis in insulin resistant menopausal women.
Design & Methods: One year, double blind, multicentral, observational, longitudinal and prospective study was undertaken on 110 menopausal women with an initial HOMA-IR > 2.25. Plasma insulin and glucose levels were determined and HOMA and BMI were calculated after 6 and 12 months of study.
Results: HOMA results were analyzed using a Wilcoxon Signed Ranks test. A p ≤ 0.05 was considered as significant. In GG we have found a significant decrease in HOMA values at 6 and 12 months while in control group we have only detected a decrease at the end of the study.
Conclusions: Present study shows that the practise of physical exercise and Mediterranean diet were able of improving the homeostasis of the glucose in patients with insulin resistance. The inclusion of genistein favours the benefits of the exercise and Mediterranean diet on HOMA results. In summary, physical exercise and Mediterranean diet are suitable tools for improve glucose homeostasis in postmenopausal women with insulin resistance. Moreover, according to present results, it also should be recommended to these patients the inclusion of an oral single daily dose of 40 mg of genistein in order to increase the combined effects of diet and physical exercise on insulin sensitivity. However, more studies are needed to be conducted in order to elucidate the mechanism responsible for these effects.
PS-176
COMPARISION OF THE EFFECTS OF TIBOLONE AND CONTINUOUS COMBINED HORMONE REPLACEMENT THERAPY ON SOME HEMOSTASIS PARAMETERS IN POSTMENOPAUSAL WOMEN
L. Tasic, R. Dunic, M. Vasiljevic, M. Dzinic, M. Djuric and D. Tasic
Gynecology/Obstetric Clinic Narodni front, Beograd, Serbia; Institute for Orthopedic diseases, Belgrade, Serbia
Introduction: Postmenopausal hormone replacement therapy alleviate the unpleasant symptoms associated with the menopause such as hot flushes, night sweats, vaginal dryness, depressed mood and also prevent postmenopausal osteoporosis. However, there are some potential hazards of HRT. One of them is the potential thrombogenic effect of estrogen in the venous and arterial vasculature. Estrogen has many different effects on the coagulation system such as increasing of procoagulation factors VII, X, XII and XIII and reducting the anticoagulant factor protein C (PC), protein S (PS) and antithrombin.
Objective: To investigate the effects of tibolone and continuous combined Hormone Replacement Therapy on various parameters of coagulation and fibrinolysis that may contribute to increased risk for venous thromboembolic events.
Material and Methods: A total of 87 healthy, early postmenopausal women aged 44–56 were randomized to receive treatment with either tibolone, ccHRT, or placebo, as control. To 29 women were prescribed tibolone 2,5 mg/day, to 36 women ccHRT containing 2 mg of estradiol plus 1 mg of norethisteron acetate(E2/NETA) and 22 women received placebo. Effects of this 2 medicaments on some hemostasis parameters were measured after 3 and 6 months of treatment.
Results: Short-term use (3 months) of both tibolone and ccHRT had a detrimental effect on the prothrombin time and activated partial thromboplastin time (shorted) and on antithrombin, protein C and protein S levels (decreased), but more so in the group treated with ccHRT.
Plasminogen-activator inhibitor type 1 levels were decreased by both tibolone and ccHRT, but more so by ccHRT. There were no changes in hemostatic parameters between 3 months and 6 months of treatment in all groups.
Conclusion: Both estrogen-progestin and tibolone are associated with an activation of thrombogenic and fibrinolytic markers within 3 months of use. Tibolone appears to produce a better balance between thrombogenesis and fibrinolysis than estrogen-progestin therapy. Whether this results in a lower incidence of thrombotic events requires further study.
PS-177
PROFILE OF CORONARY RISK IN MENOPAUSICAS PATIENTS IN PRIVATE CONSULTATION
J. Moreno-Isturiz and D. Martin
Clinica El Avila, Caracas, Venezuela
Introduction: As we know well, a protective hormonal effect exists on a series of organs and in Menopause, this effect diminishes, and one of the affected systems is the cardiovascular sphere. Let us remember that the cardiovascular disease cause 50–60% of the deaths in women over 50% and morbidity of 70% in this stage of the life.
In order to avoid this, Avila Clinics designed a laboratory profile denominated first Menopausic Profile and later Coronary Risk Profile.
A series of variables like Complete Hematology, blood sugar, Cholesterol, High Density Lipoprotein (HDL), Low DensityLipoprotein (LDL), Trigliceric, Apolipoprotein A, Apolipoprotein B, Homocistein, Protein C reactive ultrasensible and Fibrinógeno.
Parallelly N-telopeptid, TSH, T3, T4 is included.
Design and Methods: We were made evaluation of Coronary Risk to 200 patients in the lapse February-November 2007 in the private consultation. The age average of the sample was of 55.9 years (49–80).
Results: It was obtained value average of the total cholesterol of 196,7 mg/dl (Vn 120–200). HDL: 60,6 mg/dl (Vn 40–60). LDL: 128,6 (Vn 0,0–130,0). Blood sugar: 90 mg/dl (Vn 70–110). Reactive protein C: 2,08 (smaller Vn of 3.0). Homocisteina: 9,85 (Vn 5–15–20). Fibrinógeno: 326,36 (Vn 200–400). Apolipoprotein A: 151,05 (Vn 97–150). Apolipoprotein B: 109,3 (Vn 79–123).
Conclusions: It is observed that in our sample there is a tendency to have values of total cholesterol in the superior limit like its fractions and of apolipopotrein A.
The rest of the profile is within the parameters established by AVILAB as referential normal and it allows us to conclude that we must campaign suitable of changes in the feeding and the style of life of our women over the 50 years.
In any case future studies with a greater universe and in smaller women of 50 years (that already in execution) will help us to know our panorama better Cardiovascular Risk.
PS-178
DROSPIRENONE DOES NOT DECRESE NITRIC OXIDE PRODUCTION IN POSTMENOPAUSAL WOMEN
G. Ayala1, M. Semanate1 and J. Galarraga2
1Hospital Metropolitano de Quito, Ecuador; 2Hospital Eugenio Espejo, Ecuador
The objetive of the study was to demostrate that drospirenone does not decrese the effects of estradiol on the nitric oxid production. This open study included fourty two non obese, 40 to 55 years old, postmenopausal women without any hormonal treatment, within the recomendations of the international menopause society for the use of hormone therapy. Every patient had serum determinations of high density lipoprotein (HDL), low density lipoprotein (LDL), total colesterol (TC), triglicerids. The patients was aleatory asigned to one of the following three groups: Group A: Drospirenone 2 mg + Estradiol 1 mg; group B: Estradiol 1 mg; group C: Placebo. They took the treatment during 3 months. Before begining and after finishing treatment each patient had blood nitric oxide (NO) determination. The statistical analysis include ANOVA, Euclidian differences and contrasts, with a p value <0.05 for every variables. Thirty patient finished per protocol: 11 for group A, 11 for group B and 8 for group C, there were not differences between the groups in the basal variables. After fisnishing the study there were non signiticative increses in NO in any group. In group A 5.12 μmols/l (24.67 to 29.68), group B: 6.27 μmols/l (24.34 to 30.61) and group C 1.29 μmols/l (24.26 to 25.55). We conclude that this study confirms in vivo the in vitro previous observations in which drospirenone did not impair NO production.
PS-179
EFFECT OF ORAL HORMONE THERAPY IN BLOOD PRESSURE IN HYPERTENSIVE WOMEN: COHORT STUDY
K. Oppermann1,2, V. Possamai1, V. W. Dallagasperina1 and R. Schneider1
1Medicine College of University of Passo Fundo, Passo Fundo, RS, Brazil; 2Hospital São Vicente de Paulo, Passo Fundo, RS, Brazil
Objectives: Hypertension disease is frequent in climacteric women. The use of oral hormone therapy could be unfavorable to pressure levels. The aim of this study was to verify the changing on the blood pressure and lipids levels in hypertensive women throughout 24 months of oral hormone therapy.
Design & method: Retrospective cohort evaluated medical records of 64 hypertensive menopausal transition and post-menopausal women who were in use of hormone therapy (HT) and a group of 110 hypertensive patients who were not in use of oral hormone therapy, from January 1998 to December 2004. The regimes employed were oral estrogens or oral estrogen plus progestin if the patient had intact uterus. Besides blood pressure, BMI, cholesterol, triglycerides and glucose levels, the number of different anti-hypertensive medications also was evaluated each 6 months during the 24 months of follow-up. Differences between HT and non-HT groups were examined for statistical significance using Chi-Square, Mann-Whitney U or Student's T tests. It was used the pair sample T Test and Wilcoxon test to compare variables within the same group. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 11.0.
Results: The mean of the age of HT and non-HT group was 51.5 ± 7.3 and 57.5 ± 9.5 years old respectively (p < 0.001). The weight could be evaluated in 26 patients in the HT group, and the BMI was 29.3 ± 4.8 and 29.3 ± 4.9 at basal and 24 months (p = 0.90). During 24 months of follow-up there was not statistically significant changing in the systolic or diastolic blood pressure in the HT women group. In the non-HT hypertensive women, the systolic blood pressure decreased significantly at 12 (p = 0.001) and 24 months (p = 0.007) of follow-up. Both groups increased similarly the number of the anti-hypertensive medication. It occurred a decreasing in total cholesterol in the non-HT hypertensive women between baseline and 24 months of follow-up (p = 0,014). The triglycerides levels were not modified in both groups.
Conclusion: The use of oral hormone therapy in hypertensive women did not modify significantly the levels of blood pressure during 24 months of follow-up. On the other hand, the oral hormone therapy could be an adverse factor to decrease the blood pressure in hypertensive women in those on treatment.
PS-180
EFFECT OF POSTMENOPAUSAL THERAPY WITH ESTRADIOL/DROSPIRENONE OR TIBOLONE ON VASCULAR FUNCTIONS IN EARLY POSTMENOPAUSAL WOMEN
C. Vitale, M. Miceli, C. Mammi, M. Caprio, S. Lello and G. M. C. Rosano
IRCCS San Raffaele Roma, ITALY
Objective: Ovarian hormone deficiency reduces endothelial function in post-menopausal women (PMW). This effect is reversed by hormone and estrogen replacement therapy. Different progestins however may have different vascular effects thereby influencing the cardiovascular effects of estrogen replacement. Estradiol (E) combined with Drospirenone (DRSP) has been recently introduced in HRT schemes for the treatment of menopausal symptoms in postmenopausal women. Besides its progestogenic actions, DRSP has anti-mineralocorticoid properties with positive effects on the cardiovascular system, e.g. blood pressure reduction in hypertensive women. Other agents like tibolone (T) have been suggested to modulate estrogen receptor and have been proposed for the treatment of PMW. The effect of T on endothelial function of PMW is controversial while the effect of EDRSP are at the present unknown.
Design & Method: The aim of the present randomized double-blinded study was to evaluate the effect of Tand HRT with EDRSP on endothelial function by assessing flow-mediated vasodilatation of brachial artery and by Reactive Hyperemia as assessed by the endo-path system, augmentation Index and pulse wave velocity in 30 non-hypertensive early (<5 years since menopause) PMW before and after 3 months of therapy.
Results: A significant reduction in Augmentation Index (28%) and Pulse Wave Velocity (9%) were found with EDRSP while no changes were detected with T. Reactive Hyperaemia was significantly improved with EDRSP from 2.1 to 2.5 while no changes were observed with T (from 2.1 to 2.15). A significant reduction in total cholesterol was observed with EDRSP but not with T (214 vs. 193 p < 0.05 and 207 vs. 201, respectively). EDRSP reduced fasting plasma glucose from 96.8 to 87.7 mg/dl while no change was detected with T. No significant changes in plasma triglycerides were detected with either treatments.
Conclusion: In conclusion EDRSP significantly improves vascular physiology in non-hypertensive early PMW while T has no effect. These effects of EDRSP on vascular physiology may have important clinical implications long term.
PS-181
ENDOGENOUS ANDROGENS AND VASCULAR MARKERS OF ATHEROSCLEROSIS IN HEALTHY POSTMENOPAUSAL WOMEN
G. Georgiopoulos1, V. Velissaris2, I. Lambrinoudaki2, K. Stamatelopoulos1, S. Vlachou2, F. Galapi2, D. Papadimitriou2, I. Kalligerou2, D. Rizos2, A. Alexandrou3, G. Creatsas2 and C. Papamichael1
1Alexandra University Hospital, Clinical Therapeutics, Athens, Greece; 2University of Athens Aretaieio Hospital, 2nd Department of Obstetrics and Gynecology, Athens, Greece; 3University of Athens, Laiko Hospital, Athens, 1st Department of Surgery, Athens, Greece
Objective: Women after menopause exhibit a significant increase in cardiovascular morbidity and mortality. There are only few and controversial data regarding the role of serum androgen levels in this phenomenon although several studies have underlined the significance of postmenopausal estrogen decline as a probable cause. The present study aims to examine the relationship between the levels of endogenous androgens with functional and structural vascular markers of early atherosclerosis in postmenopausal women not on hormone therapy.
Methods/Design: Thirty seven healthy postmenopausal (age 56.7 ± 4.8 years, years in menopause 8.3 ± 5.4 years) women, without receiving exogenous hormone administration, were recruited from the Menopause Clinic of the 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieion Hospital. Glucose level, blood lipid profile, estradiol (E2), total testosterone (T) levels and sex-hormone binding protein (SHBG) were measured in all participants and (FAI) was calculated. Flow-mediated dilatation (FMD) was used as a marker of endothelial function, mean carotid and femoral intima-media thickness (IMT) used as a marker of generalized atherosclerosis, and carotid-femoral pulse wave velocity (PWV) used as a marker of aortic stiffness were measured in all individuals in one session. Abdominal preperitoneal (PPT) and subcutaneous (SCFT) fat thickness were also measured ultrasonographically. E2, SHBG and FAI were divided into tertiles and differences between groups were assessed by ANOVA.
Results: Age and the duration of menopause were not significantly different across tertiles of all 3 examined parameters. BMI (p = 0.009), SCFT (p = 0.035) and mean carotid IMT (p = 0.05) progressively increased across tertiles of SHBG. PPFT (p = 0.014) and LDL cholesterol (p = 0.013) progressively increased and HDL cholesterol (p = 0.004) progressively decreased across E2 tertiles. Systolic blood pressure (p = 0.047), diastolic blood pressure (p = 0.065) and mean carotid IMT (p = 0.1) progressively increased across tertiles of FAI although DBP and IMT did not reach statistical significance. No differences were observed among groups in FMD, PWV and femoral IMT.
Conclusions: Increased androgenicity, indicated by low SHBG and increased FAI, may be associated with increased arterial blood pressure and accelerated atherosclerosis while expressed by the increase of IMT in healthy postmenopausal women. The proatherogenic profile observed in women with high endogenous estrogens could indicate an indirect androgen effect, as the serum levels of estradiol in postmenopausal women are mainly determined by circulating androgens, which serve as precursor steroids.
PS-182
ESTROGEN/PROGESTERONE COMBINATION ELICITS FAVOURABLE EFFECTS ON THE PRODUCTION OF ENDOTHELIUM-DERIVED MARKERS IMPORTANT FOR MACROPHAGE RECRUITMENT
H. Seeger, F. U. Deuringer and A. O. Mueck
University Women's Hospital of Tuebingen, Germany
Objective: Macrophages are abundant in ruptured atherosclerotic plaques. Their recruitment by abnormal endothelium over a developing atherosclerotic plaque is aided by endothelial expression of adhesion molecules, chemokines and probably vasoconstrictory substances. In the present study we have compared three estrogen/progestogen combinations commonly used in replacement therapy on markers which may be involved in macrophage recruitment.
Design & Method: The experiments were conducted for 24 h with a fixed estradiol concentration of 0.1 μM and progestogen concentration in the range of 0.01, 0.1 and 1 μM in the presence of 1 μg/mlTNF-a. The progestogens evaluated were progesterone (P), medroxyprogesterone acetate (MPA and norethisterone (NET). The effect on the production of the following markers in endothelial cells from human female coronary arteries was evaluated: endothelin, E-Selectin, intercellular adhesion molecule (ICAM-1) and monocyte attracting protein-1 (MCP-1). The markers were determined by enzyme immunoassays in the cell supernatant.
Results: Estradiol alone elicits a decrease of endothelin-1 concentrations. This decrease was not attenuated by the addition of progesterone but antagonized by NET and MPA at 1 μM. Additionally estradiol alone was able to decrease MCP-1 concentrations. This effect was not attenuated by the addition of progesterone or synthetic progestins. Regarding E-selectin and ICAM-1 concentrations a significant decrease was observed after addition of estradiol. This effect was not antagonised by progestogens considering E-selectin. However, ICAM-1 concentrations increased significantly after addition of higher concentrations of NET and MPA, respectively. For progesterone no such effect was found.
Conclusion: Macrophage recruitment appears not to be stimulated by estrogen alone. However, the addition of progestogens may be detrimental, although progesterone acts neutral. Thus the progestogen choice for hormone replacement therapy may have some importance.
PS-183
EVALUATION OF HEMOSTASIS IN MENOPAUSAL WOMEN WITH RISK FACTORS FOR CORONARY HEART DISEASE QUALIFIED FOR HORMONE THERAPY
G. Stachowiak, A. Zając and T. Pertyński
From Department of Gynecology and Menopausal Diseases in Polish Mother's Memorial Hospital, Research Institute, Lodz, Poland; Head: Prof. Tomasz Pertyński
Aim of study: To determine some hemostatic parameters in menopausal women with coronary heart disease (CHD) risk factors qualified for hormone therapy (HT).
Methods: The study group consisted of 30 postmenopausal females (mean age: 54.3 ± 5.58 years) being qualified for HT because of severe climacteric symptoms. All the subjects from the study group exhibited two or more CHD risk factors e.g. arterial hypertension, obesity, hypertriglyceridemia, hypercholesterolemia, smoking, without the presence of CHD itself. Controls: 31 generally healthy premenopausal women (mean age: 49.6 ± 4.00 years) with one or without CHD risk factor(s). The following parameters were measured in blood before introducing HT to the women: platelet count, fibrinogen concentration, AT III activity, protein C activity, protein S activity, factor VII activity, t-PA concentration, PAI-1 concentration, GP IIb/IIIa (mean fluorescence of fibrinogen receptor on platelets).
Results: The study group as compared with the controls was characterized by higher levels of t-PA (10,79 ± 5,44 ng/ml and 4,64 ± 3,41 ng/ml respectively, p < 0,001) and GP IIb/IIIa (5,18 ± 5,59* and 1,41 ± 0,79* respectively). *mean fluorescence.
Conclusions: The presence of two or more CHD risk factors in menopausal women qualified for HT is connected with some changes in fibrinolysis and platelet hemostasis.
PS-184
GENDER DIFEFERENCE IN THE ALDOSTERONE LEVEL AND RENIN ACTIVITY IN ESSENTIAL HYPERTENSION
N. Podzolkova1, V. Podzolkov2 and A. Bragina2
1Russian Medical Academy of Postgraduate Education, Moscow, Russian Federation; 2Moscow Medical Academy, Moscow, Russian Federation
Objective: to assess aldosterone level, renin activity and their correlations with sex hormones in male and female hypertensives.
Design & Method: blood samples were taken from 57 patients (mean age 57 ± 6 years) with essential hypertension composing two comparable groups (19 males and 38 females). Aldosterone, estradiol, 17 α-hydroxyprogesterone and angiotensin I levels were determined in vitro in serum or plasma by radioimmunoassay. None of the subjects underwent the examination have been taken any steroids, angiotensin-converting enzyme inhibitors and/or spironolactone. Statistical methods included descriptive statistics, nonparametric statistics for comparisons (Mann-Whitney) and Spirman correlation analysis.
Results: all women were postmenopausal with the duration of postmenopause 5 ± 2 years. Female hypertensives demonstrated significantly higher aldosterone level 212.5 ± 123.9 pg/ml vs 148.9 ± 82.5 in males (p < 0.05). The levels of angiotensin I differed non-significantly: 3.3 ± 2.6 ng/ml/h vs 2.6 ± 1.7, respectively. Analysis of both aldosterone and angiotensin I levels revealed significant correlation with estradiol level (rs = −0.42, p < 0.05 and rs = −0,53, p < 0.05, respectively) in women. Moreover, aldosterone level in women was in significant correlation with 17 α-hydroxyprogesterone level (rs = −0.44, p < 0.05).
Conclusion: evaluation of hormonal status in hypertenives reveals gender differences of aldosterone level and renin activity assessed via determination of angiotensin I level. Higher renin-angiotensin-aldosterone system activity in women is apparently related to the decline of sex steroid production. The key headings are as follows.
PS-185
HYPERTENSION PROGRESS IN WOMEN WITH SURGICAL MENOPAUSE
S. Yureneva, V. P. Smetnik, E. Y. Maychuk, I. V. Pechenkina and I. Voevodina
Research center of obstetrics and gynecology and perinatology; Moscow, Russia. Moscow Medical Stomatological University, Moscow, Russia
Objective: to assess the role estrogen replacement therapy (ERT) in the development o of arterial hypertension (AH) in patients with surgical induced menopause.
Methods: Clinical, BP monitoring, echo-Doppler cardiography, Doppler sonography of the carotid arteries, test of reactive hyperaemia.
Results: We examined 81 women, surgically menopaused in reproductive age. The follow up period after surgery was 8,6 ± 3,1 years. The patients were divided in two groups : 1 group – 39 women on long term ERT, 2 group 42 patients - control. AH was diagnosed in 52% patients of the 1 group and 80,9% in the control group. An increased variability of systolic BP was noted in both groups of patients with the prevalence of hypertension of the first and second stages. The analysis of daily BP profile showed a lower decrease in blood pressure at night in over 40% of patients. In the 1 group were revealed significantly lower indexes of brachial artery pulsation compared with the control. The echo study of the parameters of intracardiac haemodynamics revealed disorders of diastolic function ot he left ventricle in 72% in women with hypertension. Signs of vascular complications were detected among patients of the 2 group. Conclusions: Hypertension is often found in surgically menopaused women. Hypertension runs a more favourable course in women taking oestrogen replacement.
PS-186
IMPORTANCE OF THE HEALTH EDUCATION IN THE CARDIOVASCULAR RISK IN THE CLIMACTERIC WOMEN
A. Fdez Pareja, E. Hdez Blanco and V. J. Riera Rubio
Centros Madrid Salud. Ayuntamiento De Madrid
Objectives: To test out the evolution of the cardiovascular risk in the climacteric period after receiving a specific health education about it.
Material and Methods: 125 climacteric women aged between 45 and 55 treated in the menopause municipal program. They have attended three lectures about Education for Health in the Climacteric (symptoms, signs, treatments and cardiovascular and osteoporosis risks).
All the patients were treated in the center where the medical history was recorded after a physical and gynecological exam and complementary tests (analytic, cytology, bone densitometry, etc).
To assess the cardiovascular risk the following parameters have been valuated in a four year period: Quetelet index, cholesterol, LDL-cholesterol, HDL-cholesterol, tryglicerics, Arterial Tension and the practice of any physical exercise (more than three weekly sessions of half an hour each).
Results:
✓ Quetelet Index greater than 30: 60% in the first visit, decreasing successively to 39,9%; 37%; 32% and 29,5% in the next years.
✓ Physical exercise: Performed in the first visit by the 15% of the women, increasing up to 50%; 60%; 65% and 67% in the next revisions.
✓ Cholesterol total: The average value decreases in the period of study (229,68; 220; 219,8; 218 and 215,4).
✓ HDL-cholesterol: The average value increases during the period of study (58,8; 62,2; 63,4; 64,4 and 65).
✓ LDL-cholesterol: The average value decreases progressively in the period of study (155,68; 138,9; 138; 135,7 and 133,9).
✓ Tryglicerics: In this case the average value oscillates (85; 83; 87; 86 and 91).
Conclusions: With these parameters assessed throughout the four year period, we can see that if the women use the information received, the cardiovascular risk decreases (Quetelet index, total cholesterol and LDL are reduced whereas HDL is increased). That would prove the effectiveness of the Health Education Programs and Prevention Programmes, although the efficiency is higher during the first year after the lectures.
PS-187
INFLUENCE OF HORMONAL REPLACEMENT THERAPY IN LIPID PEROXIDATION LEVELS OF POSTMENOPAUSAL WOMEN WITH DIFFERENT CARDIOVASCULAR CAPACITY
M. P. Mota1, J. Soares1, M. H. Moreira1, J. C. Leitão1, J. Freitas2, M. Monteiro3, P. Figueiredo4 and J. A. Duarte4
1Universidade de Trás-os-Montes e Alto Douro, Vila Real, Portugal; 2Hospital de São João, Porto, Portugal; 3Instituto Politécnico de Bragança, Bragança, Portugal; 4Universidade do Porto, Vila Real, Portugal
Objective: It has been suggested that exercise has a positive impact on the prevention and progression of cardiovascular disease (CVD). One of the main mechanisms is through the modification of lipoprotein levels and the risk of its oxidation, especially LDL lipoproteins. After menopause, women experience an increased incidence of cardiovascular disease. In contrast, women receiving hormonal replacement therapy (HRT) seem to be protected. The aim of this study was to infer how HRT affect lipid peroxidation levels in postmenopausal women with different levels of aerobic fitness.
Design & Method: Sixty four women participate in this study, 32 of them receive HRT (group with HRT – GWHRT) (average age = 55.9 years, average weight = 66.9 kg and average high = 156.0 cm) and the remained 32 women didn't receive HRT (group without HRT – GWOHRT) (average age = 61.0 years, average weight = 67.6 kg and average high = 154.3 cm). Total cholesterol (mg · dL−1), HDL-cholesterol (mg · dL−1), LDL-cholesterol (mg · dL−1) and triglycerides levels (mg · dL−1) have been analyzed in serum obtained from a blood sample collected after 8 hours of fasting, and measured in Dr. Lange LP20 according to the specific manufacturer instructions. Serum MDA concentration (ng · L−1) was determined by spectrophotometric method. Aerobic capacity (VO2max · ml · kg−1 · min−1) was assessed according to an adaptation of Bruce protocol. Differences between groups were tested through Student t-test. A Spearman correlation was performed in order to test variables associations. Significance level was established at 5%.
Results: Our results have found differences between groups in age (t = 3.018; p < 0.01), in VO2max (t = −3.774; p < 0.01) and in serum MDA concentration (t = 6.750; p < 0.01). The GWHRT were younger, had a higher VO2max (31.38 for GWHRT and 26.19 for GWOHRT), and had lower levels of serum MDA concentration (0.29 for GWHRT and 0.73 for GWOHRT) comparatively with those women from the GWOHRT. However, our results failed to find any differences between groups regarding serum triglycerides, total cholesterol, HDL-cholesterol, LDL-cholesterol or BMI. In this study, serum MDA concentration didn't correlate with higher levels of lipid profile, as we might have expected, but correlate inversely with HRT (r = −.726, p = .00) and with VO2max (r = −.287, p = .02).
Conclusion: Our results suggest that HRT should exert an antioxidant protective effect against lipid peroxidation, as well as exercise perhaps through the stimulation of antioxidant capacity.
PS-188
INFLUENCE OF HORMONAL REPLACEMENT THERAPY IN LIPID PEROXIDATION LEVELS OF POSTMENOPAUSAL WOMEN WITH DIFFERENT CARDIOVASCULAR CAPACITY
M. P. Mota1, J. Soares1, M. H. Moreira1, J. C. Leitão1, J. Freitas2, M. Monteiro3, P. Figueiredo4 and J. A. Duarte4
1Universidade de Trás-os-Montes e Alto Douro, Vila Real, Portugal; 2Hospital de São João, Porto, Portugal; 3Instituto Politécnico de Bragança, Bragança, Portugal; 4Universidade do Porto, Vila Real, Portugal
Objective: It has been suggested that exercise has a positive impact on the prevention and progression of cardiovascular disease (CVD). One of the main mechanisms is through the modification of lipoprotein levels and the risk of its oxidation, especially LDL lipoproteins. After menopause, women experience an increased incidence of cardiovascular disease. In contrast, women receiving hormonal replacement therapy (HRT) seem to be protected. The aim of this study was to infer how HRT affect lipid peroxidation levels in postmenopausal women with different levels of aerobic fitness.
Design & Method: Sixty four women participate in this study, 32 of them receive HRT (group with HRT – GWHRT) (average age = 55.9 years, average weight = 66.9 kg and average high = 156.0 cm) and the remained 32 women didn't receive HRT (group without HRT – GWOHRT) (average age = 61.0 years, average weight = 67.6 kg and average high = 154.3 cm). Total cholesterol (mg · dL−1), HDL-cholesterol (mg · dL−1), LDL-cholesterol (mg · dL−1) and triglycerides levels (mg · dL−1) have been analyzed in serum obtained from a blood sample collected after 8 hours of fasting, and measured in Dr. Lange LP20 according to the specific manufacturer instructions. Serum MDA concentration (ng · L−1) was determined by spectrophotometric method. Aerobic capacity (VO2max · ml · kg−1 · min−1) was assessed according to an adaptation of Bruce protocol. Differences between groups were tested through Student t-test. A Spearman correlation was performed in order to test variables associations. Significance level was established at 5%.
Results: Our results have found differences between groups in age (t = 3.018; p < 0.01), in VO2max (t = −3.774; p < 0.01) and in serum MDA concentration (t = 6.750; p < 0.01). The GWHRT were younger, had a higher VO2max (31.38 for GWHRT and 26.19 for GWOHRT), and had lower levels of serum MDA concentration (0.29 for GWHRT and 0.73 for GWOHRT) comparatively with those women from the GWOHRT. However, our results failed to find any differences between groups regarding serum triglycerides, total cholesterol, HDL-cholesterol, LDL-cholesterol or BMI. In this study, serum MDA concentration didn't correlate with higher levels of lipid profile, as we might have expected, but correlate inversely with HRT (r = −.726, p = .00) and with VO2max (r = −.287, p = .02).
Conclusion: Our results suggest that HRT should exert an antioxidant protective effect against lipid peroxidation, as well as exercise perhaps through the stimulation of antioxidant capacity.
PS-189
INSULIN-RESISTANCE AND ABDOMINAL OBESITY IN RELATION TO ANDROGENIC PROFILE IN MENOPAUSAL TRANSITION
V. Mesch1, N. Siseles2, L. Boero1, H. Benencia1, M. Royer2, M. Prada2, F. Sayegh2 and G. Berg1
1Faculty of Pharmacy and Biochemistry. University of Buenos Aires, Buenos Aires, Argentina; 2University Hospital. Buenos Aires, Argentina
Objective: In postmenopausal women (PostM) an increment in the androgenic milieu has been described, this can be associated with insulin-resistance states and higher risk of type 2 diabetes. Androgens also contribute to abdominal obesity, which in turn is related to insulin-resistance in PostM. Our aim was to evaluate androgenic status in relation to abdominal adiposity and insulin-resistance markers in menopausal transition (MT) women.
Design & Method: 83 women were divided into four groups: 1-premenopausal women with regular menstrual cycles (PreM, n = 19, age: 25–38); 2-MT women with menstrual bleeding with oligomenorrhea (MTM, n = 21, age: 42–53); 3-MT women with 3–6 months of amenorrhea (MTA, n = 28, age: 44–55) and 4-PostM women (n = 15, age: 49–68). None of them was under hormone replacement therapy. SHBG, total Testosterone (To), Estradiol (E2), insulin (Ins), glucose (Glu) and triglycerides were determined. The indexes E2/To, FAI (Free androgen index), HOMA, Quicki and McAuley were calculated and waist circumference (WC) was measured. Results were analyzed through one way or Kruskal-Wallis ANOVA and Tukey or Dunn post-tests. Correlations between variables were calculated through Pearson test.
Results:
Table 1 Androgenic profile, E2/To ratio and insulin-resistance markers
Table 2 Correlations between SHBG and FAI vs abdominal obesity and insulin-resistance markers
When WC was considered, neither FAI (p = 0.440), nor SHBG (p = 0.474), showed differences between groups; WC correlated only with SHBG (p = 0.022). After adjusting by WC, correlations between SHBG and insulin-resistance markers continued being significant (p < 0.05) but relationships with FAI were lost.
Conclusions: The gradual increase in the androgenic status could be related to the development of insulin-resistance from the earlier stages of MT; abdominal obesity may condition this situation.
PS-190
MENOPAUSE AS A RISK FACTOR FOR VENOUS THROMBOEMBOLISM
J. Payer, M. Borovsky, Z. Killinger, T. Koller and T. Petrovic
Comenius University in Bratislava, Slovak Republic
Introduction: Venous thromboembolism (VTE) is a frequent serious medical complication. It is well known that age is considered as a risk factor for VTE. There is a lack of information about correlation of VTE with gender and age.
Aim: The aim of the study was to evaluate the age and sex differences as risk factors for VTE.
Methods: Retrospective analysis of data of 680 patients, including 407 women and 273 men. In 124 patients VTE was diagnosed (using CT pulmoangiography, CT venography, Dupplex ultrasound), including 69 women and 65 men. 49 women with VTE were postmenopausal – above the age of 55 years (72,2%). From 65 male patients with VTE 48 (68,9%) were comparable age to the postmenopausal female group. Using regression analysis we compared the incidence of VTE in the male and female group and found that there are significant differences in progression of incidence of VTE between both groups (men: T value 0,3683, p = 0,713, women: T value 3,644, p = 0,0003). Also see Table 1,2.
Conclusions: In both sex age represents higher risk for venous thromboembolism (p < 0,001). The incidence of VTE was higher and progressively increased in the group of postmenopausal women compared to the same aged group of men.
PS-191
RALOXIFENE INDUCES ENDOTHELIAL CELLS PROLIFERATION BY INCREASED GENE EXPRESSION OF CYCLINS A AND B1
P. J. Oviedo1, S. Novella1,2, A. Sobrino1, A. Laguna1, A. Cano3 and C. Hermenegildo1,2
1Research Foundation, Hospital Clinico Universitario, Valencia, Spain; 2Dept. Physiology, University of Valencia, Valencia, Spain; 3Dept. Pediatrics, Obstetrics and Gynaecology, University of Valencia, Valencia, Spain
Objective: To evaluate whether raloxifene may exert a proliferative effect on cultured human umbilical vein endothelial cells (HUVEC), investigating if there is an associated modification in the gene expression of some key regulators of the cell cycle such as cyclin A, B1 (cell cycle progression) and p27 (cell cycle inhibitor).
Design & Method: HUVEC were stimulated either with 1 or 10 nM raloxifene or estradiol (as comparison parameter). ICI182780 was added in some experiments to investigate the implication of estrogen receptors. Measurement of cell proliferation was performed by XTT, MTT and BrdU assays. Protein levels of cyclin A, cyclin B1, cyclin D1, cyclin dependent protein kinase (CDK) 2, CDK4, and p27Kip1 were measured by immunoblotting. QRT-PCR was used to evaluate mRNA expression of cyclin A, cyclin B1 and p27Kip1.
Results: Both 1 and 10 nM of either estradiol or raloxifene achieved a similar increase in cell proliferation. ICI182780 blocked only the estradiol-induced proliferative effect. Immunoblotting detected an increased expression of cyclins A and B1, as well as a decreasing trend for p27Kip1. Cyclin A and cyclin B1 gene expressions were enhanced in response to estradiol and raloxifene, without changes for p27Kip1 mRNA levels. ICI182780 effectively abrogated the increased gene expression associated with estradiol for cyclin B1, but not for cyclin A. In contrast, ICI 182780 was ineffective in the case of raloxifene.
Conclusion: Therapeutical doses of raloxifene increased proliferation of HUVEC in a magnitude similar to estradiol. This effect was associated with enhanced gene expression of cyclins A and B1.
Supported by Spanish Ministerio de Sanidad y Consumo, Instituto de Salud Carlos III (grants FIS 06/0589 and Red HERACLES RD06/0009) and Consellería de Sanidad, Generalitat Valenciana (grants AP 09/2007 and AP 10/2007). PJ Oviedo holds a post-doc position, and A Sobrino is a fellowship recipient from the FPI program (BFPI 06/145), both from Conselleria de Empresa, Universidad y Ciencia, Generalitat Valenciana, Spain.
PS-192
STRATEGIES FOR THE EARLY DETECTION OF THE CARDIOVASCULAR RISK IN PREMENOPAUSAL AND POSTMENOPAUSAL WOMEN
A. Belardo, M. Tutzer, F. Salort and L. Bozza
Climateric section, Hospital Italiano. Buenos Aires, Argentina
Objective: To evaluate the cardiovascular risk of the women that attended to the climateric section of a comunity hospital, identifying cardiovascular risk factors as part of Framingham's score.
Design and Methods: The study has a transversal design. Data was registered into an electronic medical record. We assessed total cholesterol, HDL-cholesterol, plasma insulin concentration, fasting plasma glucose and calculated HOMA index.
We registered antropometric parameters (waist circumference, weight, height) and BMI was calculated.
Blood pressure was measured in twice opportunities by mercury sphygmomanometer.
We recorded The Framingham Heart Study parameters (gender, cigarette smoking, diabetes, plasma cholesterol levels and systolic blood pressure) to calculate cardiovascular risk (CVR) (<1%–20%).
A hundred patients were included between May and October 2007. They were divided in two groups: premenopausal (GA) and postmenopausal women(GB). Postmenopausal women had no menses for at least 1 year before enrollment.
Results: The mean age was 52 ± 6 years (41–65). Total cholesterol values range were 148 a 294 mg%. The mean CVR (10 years) was 2.97% (<1–22%). 16.6% were smokers, CVR 5.5%,(1–11%) and non smokers CVR 2.37%.
We found an age related CVR increase as an independent variable.
Physical inactivity rate (120 minutes/week) was 61.2%.
According to BMI: women were stratified as: G1 (BMI <25) 49.8%, G2: (BMI ≥ 25 and <30) 32.5%; G3: (BMI ≥ 30 and <35) 11.6%; G4: (BMI ≥ 35 and <40) 4.65%; and G5: (BMI ≥ 40) 2.32%.
50% had a waist circumference over 88 cm and 62.5% had a HOMA index ≥ 3, 25% between 2.5–3 and 12.5% had a normal HOMA index (<2.5).
Conclusions: According to The Framingham Score, a low risk for cardiovascular disease was observed in the women who attended to the climateric office. As the high prevalence of abdominal obesity, insulin resistance and physical inactivity, the Framingham Score alone may be not enough to evaluate the cardiovascular risk in this population.
PS-193
TRANSDERMAL ESTROGEN THERAPY EFFECT ON HAEMOSTATIC FUNCTION IN WOMEN WITH HISTORY OF VENOUS THROMBOEMBOLISM
Paulo Francisco Ramos Margarido1, Vicente Renato Bagnoli1, Ângela Maggio da Fonseca1, Tânia Rubia Flores da Rocha2, Gustavo A. R. Maciel1, Élbio Antônio D'Amico2 and Edmund Chada Baracat1
1Departments of Obstetrics and Gynecology; 2Hematology, São Paulo University Medical School, São Paulo, Brazil
Objective: To evaluate coagulation markers in women previously diagnosed with venous thromboembolism submitted to transdermal hormonal therapy using 17β estradiol.
Casuistry and Methods: Twenty-nine menopausal women with history of venous thromboembolic (VTE) disease, aged from 40 to 65 years, were prospectively assigned to begin transdermal hormonal therapy for 6 months to treat menopausal symptoms. Nine (9) patients were included in the treatment group (estradiol) and twenty (20) in the control group. Coagulation parameters prothrombin time (PT) presented as percentage of activity and International Normalized Ratio (INR), thrombin time (TT) and activated partial thromboplastin time (APTT) accessed before the therapy, 3 and 6 months later.
Results: We found a significant increase in INR (p = 0.007) and a decrease in thrombin time (P = 0.002). The other parameters studied did not change significantly.
Conclusions: Our data suggest that transdermal hormonal therapy did not alter coagulation parameters in women with a previous diagnostic of venous thromboembolism and might be considered for use in menopausal women with intense symptoms.
PS-194
VARIOUS MENOPAUSAL HORMONE THERAPIES AND MARKERS OF INFLAMMATION, COAGULATION, FIBRINOLYSIS, LIPIDS AND LIPOPROTEINS IN HEALTHY POSTMENOPAUSAL WOMEN
B. Žegura1, B. Gužič Salobir2, M. Šebeštjen2 and I. Keber2
1University Clinical Centre Maribor, Clinic for Gynaecology and Obstetrics, Maribor, Slovenia; 2University Clinical Centre, Hospital of Internal Medicine, Department of Angiology, Ljubljana, Slovenia
Objective: Androgenic progestins such as norethisterone acetate (NETA) may influence the effect of estradiol (E2) therapy. We compared the influence of oral E2, with and without NETA, and transdermal E2 on markers of coagulation, fibrinolysis, inflammation and on lipids and lipoproteins in healthy postmenopausal women.
Design & Method: 112 healthy postmenopausal women were randomized to receive treatment with either oral E2, with or without NETA, transdermal E2, or placebo. At baseline and after 28 weeks, levels of serum lipids and lipoproteins and markers of coagulation, fibrinolysis and inflammation were determined.
Results: Of the fibrinolytic parameters, oral E2 (p < 0.05) and E2 with NETA (p < 0.01) shortened euglobulin clot lysis time. Oral E2 decreased plasminogen activator inhibitor (PAI-1) activity (p < 0.05). Oral E2 with NETA reduced PAI-1 antigen levels (p < 0.01) and increased D-dimer antigen levels (p < 0.001). All three modes of menopausal hormone therapy (MHT) reduced tissue type plasminogen activator antigen. Of the coagulation parameters, both routes of E2 therapy decreased fibrinogen levels (p = 0.002 for oral and p = 0,007 for transdermal E2), while E2 with NETA showed no effect. The decrease of fibrinogen was larger after oral E2 (p = 0.02). Oral E2 with NETA reduced AT III (p < 0.001) and protein C (p < 0.001) activity. Oral E2 (p = 0.04) and E2 with NETA (p < 0.01) increased CRP. Transdermal E2 showed no influence on CRP. The addition of NETA influenced the change in CRP, as the increase in CRP was more pronounced after E2 without NETA (p = 0.005). The levels of SAA, Il-6 and TNF-α did not change significantly after any of the modes of HRT. Of the lipids and lipoproteins, oral E2 decreased LDL-C (p < 0.01), Lp(a) (p < 0.05) and increased HDL-C (p < 0.05). Transdermal E2 decreased triglycerides (p < 0.02) and increased HDL-C (p < 0.03). Oral E2 with NETA decreased total cholesterol (p < 0.01) and HDL-C (p < 0.005).
Conclusion: Oral E2, with or without NETA, produced no net activation of coagulation but improved fibrinolysis. Both modes of oral MHT have a greater impact on markers of inflammation, coagulation, fibrinolysis, lipids and lipoproteins than transdermal E2. NETA attenuates some E2 effects. Further studies are needed to elucidate the impact of these effects on clinical end-points.
Aging and hormones
PS-195
APPLICATION OF A SPECIFIC HYDRATING CREAM FOR VULVAR DRYNESS ACHIEVES A SIGNIFICANTLY GREATER REDUCTION IN PRURITUS WITHOUT THE ADDITION OF ANTIPRURITIC AGENTS. A COMPARATIVE, RANDOMIZED, DOUBLE BLIND STUDY
M. Guinot1, M. D. Julia2, A. Mirada3 and A. Martí4
1Hospital de Sant Pau, Barcelona, Spain; 2Hospital Universitario La Fe, Valencia, Spain; 3ISDIN, Barcelona, Spain; 4Clever Instruments, Barcelona, Spain
Objective: Since pruritus is one of the most frequent complaint in women who consult their physician for vulvar dryness, this study aimed to determine whether increasing the antipruritic agent content improves the result of using a specific hydrating cream for vulvar dryness.
Design & Method: Comparative, randomized, double blind study of the effects of a hydrating cream alone (A) compared with the same cream with increased antipruritic agent content (B). Forty-eight patients with vulvar dryness and/or pruritus were included. Seventeen received treatment A, and 31 treatment B. Patients were followed up for 30 days. The physician assessed clinical symptoms (dryness, pruritus, stinging sensation, burning sensation, pain, erythema, desquamation, excoriations and fluid deficit) at the beginning and at the end of the study on a 5-point scale (0 = zero, 4 = very high). The clinical evolution was rated according to the change between initial versus final scores (Wilcoxon's signed-rank test). The antipruritic effect of the two presentations was compared on the basis of the percentage reduction of pruritus scores between the first and last visits (Mann-Whitney U test).
Results: At baseline, there were no significant differences between the groups in terms of intensity of dryness, stinging sensation, burning sensation, pain, erythema, desquamation, excoriations or fluid deficit. The mean initial intensity of pruritus was greater in group A (2.31 vs 1.43; p < 0.05). After 30 days of use, patients presented a significant clinical improvement in most symptoms (dryness, pruritus, erythema, desquamation, fluid deficit and pain; p < 0.05) with both presentations and group A presented a significant clinical improvement in burning sensation and excoriations (p < 0.05). The reduction in pruritus was significantly higher (80% vs 41%; p < 0.05) in patients in group A than in group B.
Conclusion: Though both presentations achieved significant improvements in most symptoms in patients with vulvar dryness, the addition of antipruritic substances did not improve the reduction in pruritus obtained with the hydrating cream. This suggests that improving dryness alone should be sufficient for controlling the pruritus that accompanies vulvar dryness, and avoids adding substances that may prove to be irritants.
PS-196
EFFECTS OF ORAL AND TRANSDERMAL ESTROGEN ON IGF-1, IGFBP-3, IGFBP-1 AND METABOLISM OF LIPIDS AND GLUCOSE IN PATIENTS WITH HYPOPITUITARISM DURING GROWTH HORMONE TREATMENT: A RANDOMIZED STUDY
A. L. Isotton1,2, M. C. O. Wender1,2, A. Casagrande1,2, G. Rollin1,2, C. Oliveira1,2 and M. A. Czepielewski1,2
1Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil; 2Medical Sciences Postgraduate Program: Endocrinology, School of Medicine, Universidade Federal do Rio Grande do Sul (UFRGS), Porto Alegre, Brazil
Objective: Previous studies in postmenopausal women have shown a differential effect between the route of estrogen administration on GH and IGF-1 concentrations. The oral estrogen route reduce IGF-1 and increase IGFBP-1 levels. No effects, however, are detected by the transdermal route. The aim of these study is to detect the effects of administration of oral estradiol and 17β estradiol transdermal on IGF-1 and IGF binding proteins in hypopituitary women.
Design & Method: We studied 11 hypopituitary patients who were randomly allocated to receive 2 mg of estradiol orally (n = 6) or 50 μg of 17 β estradiol transdermally (n = 5) by a 3-month period.
Results: In the oral group, we observed a significant decrease of IGF-1 level by 42.7% ± 41.4, p = 0.046. No significant difference was detected in the transdermal group. IGFBP-1 value increased by 170.2% ± 230.9 (p = 0.028), in the oral group but don't in the transdermal group.
Conclusion: Our data indicate that the route of estrogen administration can influence IGF-1 and IGFBP-1 levels. The clinical relevance of these effects in hypopituitary patients can influence the response of GH treatment, whereas these patients on oral estrogen therapy need more GH dosage. However, the clinical significance of the decrease in IGF-1 levels mediated by oral estrogen still needs to be clarified regard to the risk of cardiovascular disease.
PS-197
EFFICACY AND SAFETY OF 1 MG ESTRADIOL AND 2 MG DROSPIRENONE IN POSTMENOPAUSAL WOMEN
C. Galesanu
Endocrinology, University of Medicine and Pharmacy, Iasi, Romania
The decreased production of estrogens hormons during peri and postmenopausal period induced physical and psychological symptoms that impact the owerall quality of life. Hormone replacement therapy is considered to be effective for climacteric symptoms such as hot flashes, sweating, sleep disturbances etc.
Objective: The aim of this study was to demonstrate the efficacy, safety and tolerability of a new treatment: 1 mg estradiol + 2 mg drospirenone (Angeliq®) in menopause symptoms.
Design & Methods: Twenty-seven postmenopausal women were randomized into two treatment groups: A. ten women treated with 1 mg estradiol + 2 mg drospirenone (E2/DRSP); B. seven women treated with 1 mg estradiol + 5 mg dydrogesterone (E2/DGS). The period of treatment was six months. The efficacy parameters were the individual relative change of hot flashes, sweating episodes and sleep problems, nervousness, brest tenderness, sexual activity, memory. At the beginning and end of the study were performed clinical and gynecological examinations and laboratory analysis.
Mean age of women was 49.9 ± 6.4 years for E2/DRSP vs 53.8 ± 0.5 years for E2/DGS. Time since menopause was 3.9 ± 3.5 years for the first group and 5.2 ± 3.0 years for the second. The weight mean was 66.5 ± 1.6 kg vs 72.1 ± 1.6 kg.
Results: The mean number of hot flashes per day decreased by 100% under E2/DRSP vs 80% under E2/DGS. The sweating episodes decreased by 80% in the both groups. The sleep disturbances decreased by 100% under E2/DRSP vs 83% under E2/DGS. Brest tenderness decreased by 66% only the first group. The mean weight loss was at 9.3 kg in the first group and 2.6 kg in the second.
Conclusions: The E2/DRSP (1 mg + 2 mg combination) was efficacious in the treatment of hot flashes, sweating episodes and other climacteric symptoms in postmenopausal women. Good results were obtained in brest tenderness and loss weight during E2/DRSP treatment. This results can be explained by drospirenone, a new generation progestin who has potent anti-mineralocorticoid activity. This preparation (E2/DRSP) is both safe and tolerable.
PS-198
EFFECTS OF HORMONE THERAPY ON SERUM HS-CRP LEVELS IN SURGICALLY MENOPAUSED WOMEN
Kyu Sup Lee1, Sung Tack Oh2, Young Min Choi3, Hwi Gon Kim1 and Jung Wan Jung4
1Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602–739; 2Obstetrics and Gynecology, Chonnam National University, Kwangju, Republic of Korea, 501‐757; 3Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602-739; and 4Obstetrics and Gynecology, Miraero Hospital, Busan, Republic of Korea, 616‐820
Objectives: To investigate the effects of hormone therapy (HT) on high-sensitivity C-reactive protein (hs-CRP) in surgically menopaused women.
Methods: In this study, 156 healthy women were enrolled. After surgical menopause, 28 women were receiving HT and 32 women were not for 3 months, 28 women were receiving and 32 women were not for 1 year. Control group included 36 healthy premenopausal women not receiving HT. The effect of HT on plasma levels of hs-CRP and lipids were investigated.
Results: Mean hs-CRP concentrations were significantly higher in surgically menopaused women receiving HT thanpremenopausal women (premenopausal: 0.069 ± 0.080 mg/dl, HT for 3 months: 0.095 ± 0.079 mg/dl, HT for 1 year: 0.159 ± 0.313 mg/dl, p < 0.05). Mean hs-CRP concentrations were also higher in surgically menopaused women not receiving HT than premenopausal women (premenopausal: 0.069 ± 0.080 mg/dl, 3 months after surgical menopause: 0.108 ± 0.215 mg/dl, 1 year after surgical menopause: 0.081 ± 0.146 mg/dl, p>0.05). There was no statistically significant difference between receiving HT group and not receiving HT group in 3 months and 1 year after surgical menopause.
Conclusion: hs-CRP was increased in surgically menopaused women than premenopausal women, however, there was no significant changes in hs-CRP between HT group and no HT group for 3 months and 1 year.
PS-199
EPIDEMIOLOGICAL PROFILE FROM ELDERLY WOMEN TAKING LOW DOSES HORMONAL TREATMENT
V. R. Bagnoli, J. O. P. Massabki, A. M. Fonseca, E. G. Labes, P. Y. A. Cezarino, J. S. Paixao and E. C. Baracat
Department of Obstetrics and Gynecology, Medical School, University of São Paulo, Brazil
Introduction: Low doses hormonal treatment is justified to improve the life quality and to be in health of young and elderly post-menopause women.
Objective: To verify the epidemiological profile from elderly women taking low doses hormonal treatment.
Casuistry and Methods: Were included 60 post-menopause women, aged from 60 to 63 years (mean age 61,3years) taking equino conjugated estrogens 0,3mg/day, in continual use (women without uterus 40%), or in association with medroxiprogesterone acetate 2,5mg/day also in continual use (women with uterus 60%). All they were symptomatic and without contra-indications for hormonal treatment. All the women had light arterial hypertension and taking some diuretics and /or some specific drug to treat hypertension.
Results: We observed mean age of menopause 50,8 ± 3,5 years; 50% were married, 30% widow, 15% divorced and 5% single; the mean age of the first delivery was 20 ± 3 years, with 4 ± 3 delivery (66% vaginal delivery, 34% cesarean section, and 50% had at last one miscarriage). The parameters considered for the evaluation of low doses hormonal treatment were: hot flushes and insomnia 90% and 70%, before and 20% and 30% during treatment respectively; body mass index (weight/height – kg/m2) 26,8 ± 3,3 before and 26,3 ± 2,8 during treatment; mean time on treatment 3 years, during from 1 to 5 years. The treatment was stopped due to breast pain – 60%, genital bleeding – 20%, headache – 10% and others.
Conclusions: We concluded that for elderly women low doses hormonal treatment is safe and effective for treatment of climacteric symptoms, did not change body mass as well blood pressure during the mean time of 3 years of treatment. The most important reason to stop the treatment was breast pain and fear of breast cancer.
PS-200
FLOWCHARTS FOR HEALTH PROFESSIONALS DEALING WITH INTEGRAL PRIMARY HEALTH CARE FOR CLIMACTERIC WOMEN
R. Oliveira1, J. B. Albuquerque2, R. B. Ramos2, L. C. Pazero2, L. C. Vega2, J. A. Oliveira Neto3 and S. M. Pachoal3
1Depto, Medicina Social Faculdade De Ciências Médicas Da Santa Casa De São Paulo, Brazil; 2Prefeitura do Município de São Paulo/Secretaria Municipal da Saúde, Brazil; 3Irmandade da Santa Casa de Misericórdia de São Paulo, Brazil
Introduction: In Brazil, like in other countries around the world, two things can be noticed: an increase in life expectancy and the feminization of ageing. Consequently, the higher the age range, the higher the proportion of women in the population. According to SUS (the Brazilian Unified Health Care Services ) activities related to ageing women's health promotion and prevention should be at the level of primary health care and be started in the climacteric period.
Objective: Devising and organizing flowcharts to help in a practical manner in routine diagnosis and protocols for integral health care of climacteric women.
Methodology: Drawing on the practical experience of the Centro de Saúde Escola Barra Funda “Alexandre Vranjac” (a primary health care center for climacteric women) and on the scientific evidence of current literature, a team of professionals and technicians of the Health Department of the Municipality of São Paulo, including gynaecologists, geriatricians, GPs, clinical doctors, acupuncturists, homeopaths, pharmacists, and psychologists) reflected upon, studied and devised a series of flowcharts encompassing diagnosis possibilities, protocols, referral needs, allopathic and alternative treatments and follow-up strategies. The flowcharts were implemented through the publication of a Handbook for health professionals, containing information about key themes related to climacterium. The Handbook was distributed in the Basic Health Units of the Municipality of São Paulo.
Results: Six flowcharts were devised, having as a model the following flowchart:
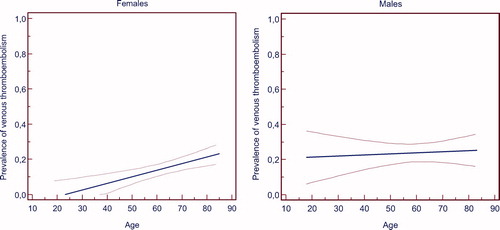
Discussion: Counting exclusively on an initial approach by a single Specialist (a gynaecologist, for that matter) would be impossible in the Brazilian Public Health Care Services. The standardization of flowcharts and protocols according to scientific evidence and directives from the Health Ministry becomes increasingly important to guarantee good quality health care and the action of general practitioners that integrate the Federal Family Health Program, as well as of nurses, resident and GP doctors. The flowcharts are the necessary instruments for the materialization of such proposal. CONCLUSION: In developing countries with a feminization of ageing, the devising of flowcharts to guide integral health care of climacteric women provide a greater diversity in terms of professionals dealing with primary health care, leading to a larger number of people attended to and to the optimization of referrals concerning patients who require specialized attention.
PS-201
HORMONAL REPLACEMENT THERAPY IMPROVES POSTMENOPAUSAL SYMPTOMS
A. Manaj1,2, A. Musta1,2 and O. Janushaj2
1Obsetric Gynecological Hospital “Mbreteresha Xheraldine”, Tirana, Albania; 2Private Clinic “Manaj”, Tirana, Albania
Objective: The effect of angeliq in postmenopausal women as first treatment of that kind in our country.
Design & Method: This study is a randomized clinical trial. 50 patients treated with angeliq (experiment group) and 52 patients under placebo (control group) for one year. Fisher's exact test for comparison of two independent proportions was used. Postmenopausal symptoms were observed during the treatment period of one year. From a total of 275 subjects we carefully selected a trial group of 50/52 healthy postmenopausal women to treat respecively with angeliq/ placebo.
Results: From data analyses resulted that patients treated with angeliq have a much lower rate of psychiatric P = 0.676, of cardiac P = 0.054 and of gastro intestinal disorders P = 0,062, of musculoskeletal disorders P = 0.113 and a higher rate of vascular disorders, P = 0.054.
Patients treated with angeliq have a similar rate of nervous system disorders P = 0.676 and skin and subcutaneous tissue disorders compared with the control group. There is no statistically significant difference in the rates of reproductive system disorders and the difference in the rates of general disorders.
Conclusion: Angeliq quicky treats the occurrence of moderate to severe vasomotor symptoms. Patients treated had a much lower rate of psychiatric, cardiac disorders and a higher rate of vascular disorders.
Usage of angeliq was associated with good rates of compliance and acceptability, only a low number of subjects were oblidged to discontinue the therapy because of the adverse effects.
PS-202
HOW TO CHOOSE THERAPY IN MENOPAUSE – HORMONAL VERSUS TRADITIONAL MEDICINE IN ROMANIA
Corina Grigoriu1, Iuliana Ceausu2, Corina Parau1, Mirela Grigoras1, Al. Ciulcu2, Cristina Cezar1, Adina Lungu1, A. L. F. Anca1 and V. Horhoianu1
1University Emergency Hospital Bucharest Romania; 2Cantacuzino Hospital Bucharest Romania
Objective: Beginning with the WHI study and the non-answered questions which followed, physicians all over the world became allert in informing themselves and the patients about new frames in prescribing therapy in menopause. We tried to verify which criteria apply best for patients, respectively for physicians in choosing therapy in menopause.
Design and Methods: We studied prospectively 128 patients from four ambulatory settings, who presented for regulary check-up at menopause. After clinical examination and basic lab analysis, the patients completed a detailed questionnaire regarding their knowledge about therapy in menopause (hormonal substitutive or traditional medicine), side effects of each, results of clinical trials, information through mass/media, friends or other medical persons; personal believings and feelings about what therapy the doctor will prescribe. Afterwards, patients had a thorough discussion with their doctor and have been encouraged to ask open questions regarding the possibilities of therapy. Finally, doctors and patients answered each another questionnaire regarding the choosen treatment. Follow-up visits were scheduled every three months for the next two years.
Results: The study revealed that few patients (26%) have a solid baseline knowledge about therapy in menopause. Missunderstading of reason of therapy was rather common (68%). Most of patients declared that they would be content if results of clinical trials would be presented by their doctor (75%) and 82% that they prefer to be quickly informed about new data that appear during their treatment period. 68% of patients declared they would be happier with a traditional therapy (herbs, roots etc), mainly because mothers or other relatives used them before.
Conclusion: Cultural background in traditonal societies can seriously interfere in choosing and maintaining therapy in menopause.
PS-203
IS THERE ANY DIFFERENCE IN SERUM ESTRADIOL LEVEL BETWEEN MORNING AND EVENING ORAL ESTROGEN ADMINISTRATION IN POSTMENOPAUSAL WOMEN
B. Kang, S. Kim, H. Chae and C. Kim
Ulsan University, Asan Medical Center, Seoul, Korea
Objective: To compare the serum estradiol (E2) level of hormone therapy (HT) taken in the morning or evening in Korean menopausal women.
Design and Methods: A prospective randomized clinical trial was conducted on 51 postmenopausal women without contraindication for HT use. Patients were divided into 2 treatment groups. Morning group patients (n = 23) received the pill at 8 a.m. and evening group patients (n = 22) received the pill at 8 p.m. for 3months.
Results: Groups were homogenous for age and basal parameters. Serum E2 levels increased significantly (p < 0.05) after 3 months HT in both groups. However, there was no difference in the baseline serum E2. And there were no differences in the serum E2 levels after 3mo HT between two groups.
Table 1. Patients Characteristics
Table 2. Serum estradiol levels of baseline and after 3 months oral
Conclusion: Morning or evening administration of oral HT did not show any difference in the serum E2 levels after 3mo HT.
PS-204
MÜLLERIAN INHIBITING SUBSTANCE AS A PROMISIING PREDICTOR OF THE MENOPAUSAL TRANSITION
J. H. Kim, G. Y. Chun, S. Y. Kim, H. H. Jo, M. R. Kim, D. J. Kwon, Y. O. Lew and E. J. Kim
Catholic University of Korea, Seoul, Korea
Objective: To measure Müllerian inhibiting substance (MIS) levels during menstrual cycle and to evaluate whether MIS may be used as a predictive marker for the occurrence of menopausal transition.
Design & Method: Serum MIS was checked by ELISA twice per each sample in 87 reproductive, 58 menopausal transition, and 5 menopausal women. Immunohistochemical staining of MIS was performed in ovarian tissues from 15 reproductive, 15 menopausal transition, and 5 menopausal women.
Results: Serum MIS levels in reproductive women was lower during secretory phase (1.34 ± 0.94 ng/ml) than proliferative (2.11 ± 1.06 ng/ml) and ovulatory phases (2.05 ± 1.21 ng/ml). MIS showed only a fluctuation during menstrual cycle, consistent with continuous noncyclic growth of small follicles. MIS level in menopausal transition was significantly lower than that of reproductive women (0.18 ± 0.11 vs. 1.73 ± 1.07 ng/ml, P<0.001). The cutoff value of MIS for menopausal transition was 0.5 ng/ml. MIS was not detected in menopause. Overall, MIS was significantly decreased as patient age was increased. In reproductive women, MIS did not show any significant correlation with E2, FSH, and LH. In menopausal transition, MIS was correlated with only FSH. In reproductive group, MIS was strongly expressed in granulosa cells of primary and growing follicles, but not in preovulatory follicle, atretic follicle, and corpus luteum. In menopausal transition, MIS was expressed in nearly same pattern as reproductive women, but with weaker expression, and was not expressed in large antral follicle. MIS was not expressed in menopause.
Conclusion: Serum MIS levels decreased with increasing female age and was not detected in menopause. It suggests that MIS is a predictive marker for ovarian aging and menopausal transition.
PS-205
PROSPECTIVE OPEN LABEL STUDY TO EVALUATE THE VASOMOTOR SYMPTOMS CONTROL and BLEEDING PATTERNS WITH A CONTINUOUS REGIMEN OF A NEW PROGESTINE TRIMEGESTONE 0.125 mg. AND 17 B ESTRADIOL 1 mg. (TOTELLE®), AS HT IN GENERALLY HEALTHY POSTMENOPAUSAL WOMEN
J. Vázquez1, L. M. Bravo2, A. Basavilvazo3, S. Carranza Lira4, H. Bierschwale5, G. LaVilla5, F. Sordo and G. Tamariz5
1Hospital Universitario Eleuterio González, Monterrey, NL, Mexico; 2Hospital López Mateos; ISSSTE; 3Centro Médico La Raza; IMSS; 4Hospital de Gineco Obstetricia No. 4, IMSS; 5Wyeth Pharmaceuticals Mexico
Objectives: It is established that low doses of HT are as effective as the standard doses for symptoms control in postmenopausal women.1 Therefore, it is predicted that a combination of estradiol 1 mg with trimegestone 0.125 mg (TMG) will be effective and safe for postmenopausal women taking HT.
Primary objective: to evaluate the control of vasomotor symptoms with a continuous regime of 17-(Estradiol 1 mg. and Trimegestone 0.125 mg. Secondary objectives: evaluation of bleeding patterns and Quality of Life.
Methods:
Study Design: Prospective, open label, multicentric, non comparative phase IV study, in Mexican generally healthy postmenopausal women.
Medication: a continuous regime of 17-(estradiol 1 mg. and Trimegestone 0.125 mg. once/day, 6 28-day cycles. Physical exam, basic blood chemistry and Menopause Quality of life Specific Questionnaire (MENQoL) were applied at all visits.
Statistical Method: descriptive statistics for the demographic data, comparison among the initial and final visit of the variables of effectiveness. Sign ranges Wilcoxon Test for related samples.
Results: Out of 130 recruited patients, 107 completed all visits.
Demographic data: The average age was 50,6 years (SD: 3.3), mean weight 65,6 kg. (SD; 9.3),mean Body mass index 27,1 (SD: 3.3).
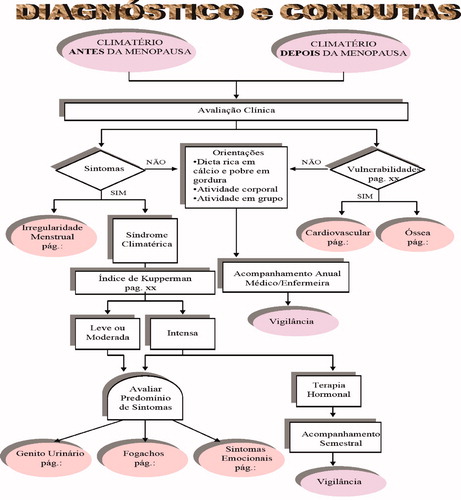
No significant variations in weight or Body mass index were detected between baseline and final visit.
Efficacy:
General Health Condition: There was statistically significant improvement from baseline (p = 0.001) after the administration of 6 cycles of the study drug.
Vasomotor Symptoms: Hot flushes, night sweats and sweating, significantly decreased (p < 0.0001) from baseline.
Quality of Life:
Domains included in the MENQoL like dissatisfaction, anxiety/nervousness and lack of memory, also showed a statistically significant decrease (p < 0.0001).
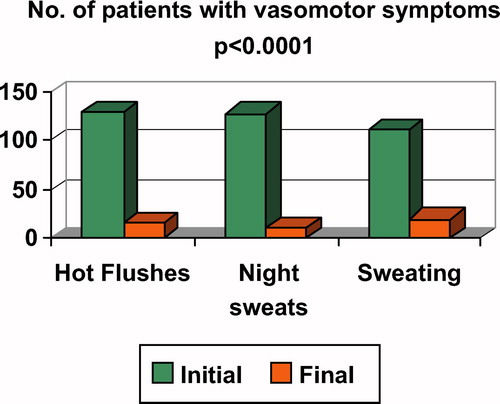
Bleeding: Occurred as expected with low dose, being spotting the most frequent. There was no clinical significance in bleeding events.
Safety: Adverse Events: 69 patients reported at least one adverse event, 334 events in total. The most frequent AE was bleeding with 162 events, 107 were spotting, followed with breast tenderness in 49 and mild abdominal pain in 18.
Conclusions: The use of this low dose combination with estradriol and trimegestone as HT in generally healthy postmenopausal women demonstrated a significant improvement in vasomotor symptoms and in all domains of Menopause Quality of life Specific Questionnaire. Adverse events were mild and expected. Totelle (, is an efficacious and well tolerated low dose regime for Hormone therapy.
PS-206
QUALITY OF LIFE ASSESSMENT OF POST MENOPAUSAL WOMEN AT HIGH RISK FOR BREAST CANCER USING THE ASSOCIATION OF RALOXIFENE AND CONJUGATED EQUINE ESTROGEN
A. L. Carneiro, F. A. Souza, M. G. Nunes, M. A. Haidar and R. C. Dardes
Department of Gynecology, Federal University of São Paulo, Brazil
Background: Kupperman Index of women at high risk for breast cancer using isolated oestrogen and raloxifen is well described. However, the association of these two therapeutic drugs have been demonstrated briefly. Such associations are being used to provide those women the effects of what should be the perfect treatment for menopause: symptoms relief and low collateral effects on uterus and breast. High risk women, estimated by Gail's algorithm model, would have even more benefits from this association.
Objective: The objective of this study was to evaluate the Kupperman Index on women with high risk for breast cancer using the association of low dose oestrogen and raloxifen.
Methods: Sixty nine patients were randomly allocated into 3 groups: conjugated equine oestrogen (GI), raloxifene 60 mg (GII) and conjugated equine oestrogen and raloxifene 60 mg (GIII) on a single dose daily for 6 months. Kupperman Index was evaluated at basal and 6 months visits.
Results: The 3 groups had no statistic differences regarding age or Gail risk. At the beginig of the study the mean age was 56,4 years and mean Gail Index was 2. Kupperman Index at inicial visit was 13,9; 13,8 and 14,8 for groups I, II and III, respectively. At 6 months, it was 3,8; 9,2 e 4,1, respectively. Women receiving the associaton of raloxifen and oestrogen and those taking oestrogen alone had improvement on Both Kupperman Indez and hot flushes by the end of 6 months. Mean hot flushes on groups I, II and III were, respectively, 4,5; 5,4 e 6,5 e 1,2; 4,4 e 1,1 on basal and 6 months visits.
Conclusions: This study demonstrated that the concomitant use of low dose of conjugated equine oestrogen and raloxifene for 6 months improves the Kupperman Index and hot flushes on post menopause women at high risk for breast cancer.
PS-207
REEMPLACEMENT HERMENAL THERAPHY ACCEPTANCY SOME MEDICAL RESULTS IN CLIMATERIA WOMEN
Rafael Abreu Naranjo1 and Ovial Reyes Amat2
1Policlínico Universitario Dr. Rudesindo Antonio García de Río, Email: [email protected] Telefono: 0141336000 ext – 160, Sancti Spiritus, Cuba; 2Hospital General Docente Guillermo Domínguez López, Servicio de Ginecobstetricia, Email: [email protected], Teléfono: 512011 ext – 246
Expentancy of living in human beings has increased up to a 50%. A woman lives longos than a third of hes life in post menopapesal period in the was that ovaric hormones dicrease up to advanced age. A descriptine, transversal study was carried out with a sample of 110 women who went to the climateric integral women service belonging to Dr. Rudesindo Antonio García del Río, Sancti Spiritus University Policlinic, in the years 2007. All these women where given standardized questionaries to know what they knew and how they could accept re-emplacement hormonal therapy almost all of then were from 40 to 65 years old, representing the 96%. Two thirds considered tha menopause was a natural change that needed medical attention and treatment. The mjority of then were using RHT, representing the 67% or used it in the past, representing the 21%. Among the reasons they gave to be using RHT these was hot flashes, representing the 73%, vaginal dryness, representing the 41%, and psyquical symptoms, representing the 35%. A third of the present's consumers informed to suffer from secondary side efffects from moderate to wild. Among there, they were breast pain, headaches and vaginal bleeding. From the present users, the 78% expresesed their wishes to continue treatment and their satisfaction with the results in terms of betterment quality of life with the use of RHT. The uses who discontinued treatment mentioned not to have any others symptoms, representing the 42% and its secondary effects, representing the 17%.
PS-208
SHBG AND ESTRADIOL: EVALUATION AFTER TEN YEARS OF THR
J. L. Cuadros1, A. M. Fernández1, A. M. Cuadros, F. J. González2, R. M Sabatel1, O. R. González1 and I. M. Fernández
1HU San Cecilio, Granada, Spain; 2H Costa del Sol, granada, Spain
Objective: SHBG is a glycoprotein synthesized by the liver. The main steroids (estradiol and testosterone) circulate in blood bound to SHBG (69%) and albumin (30%), while the remaining 1% circulates as a free hormone. In this paper we analyze the response of SHBG to different standards of THS.
Material and Methods: We studied 474 patients who began and continued THS for ten years (167 patients). We evaluated the mean of SHBG and estradiol at the beginning of the treatment and after 1, 5 and 10 years. According to the standard of THR, we created four groups: A tibolone; B estradiol daily(TTS 50) and medroxyprogesterone (10mg)/ progesterone (200mg) (12–25 per month); C estradiol daily (TTS 50) and medroxyprogesterone (2,5mg)/progesterone (100mg) daily; D estradiol daily (TTS 50).
Results: We observed an increase of SHBG in proportion to the increase of estradiol with the use of THS. In all cases the increase is significant with (p < 0,005), reaching its maximum after 5 years of treatment, irrespective of the gestagen that we used (Table 1) Tibolone didn't affect the nevels of SHBG, does the decrease leave?
Conclusions: The use of THS in this study produced an increase of estradiol with is relatied to greater production of SHBG by the liver. The addition of medroxyprogesterone and natural progesterone don't change this effect. This effect doesn't exist with tibolone.
PS-209
STUDY TO COMPARE ELDERLY YELLOW AND WHITE WOMEN IN LOW DOSE HORMONAL TREATMENT
V. R. Bagnoli, J. O. P. Massabki, A. M. Fonseca, P. A. A. Junqueira, M. H. A. Arie, D. G. Curi and E. C. Baracat
Department of Obstetrics and Gynecology, Medical School, University of São Paulo, Brazil
Introuduction: during last years increased the prescription of low dose hormonal treatment, specially for old women, to reduce the risks of hormonal treatment in regular doses, justifying this comparative evaluation.
Objective: to evaluate the effect of low dose hormonal treatment in Japanese and white women descendents.
Casuistry and Methods: for this study were included 80 women, 40 yellow (mean age 62,3 years) and 40 white women (mean age 63,2 years). Before treatment and with one year with hormonal treatment (equine conjugated estrogens 0,3 mg/day and medroxi progesterone acetate 2,5 mg/day) orally, for continual use. All the women with intact uterus and without contra-indication for hormonal treatment, and were evaluated by Kupperman's menopausal Index (KMI - light: 0–19; moderate: 20–35; severe more than 35), fast glucose (mg/dl); body mass index (BMI kg/m2); bone mass densitometry (DO L2-L4 and femur – Hollogic: g/cm3).
Results: we observed before treatment and at the end of the hormonal treatment the results, respectively: Yellow women – KMI = 11 ± 7 and 8 ± 4; BMI = 25 ± 4 and 27 ± 2,8; fast glucose 89 ± 8,7 and 93 ± 10,2; DO-L2-L4 = 0,943 ± 0,16 and 0,947 ± 0,13; DO-Femur = 0,754 ± 0,15 and 0,770 ± 0,12. White women KMI = 16 ± 5 and 14 ± 6; BMI = 27 ± 3 and 29 ± 2; fast glucose 92 ± 7 and 95 ± 10; DO-L2-L4 = 0,985 ± 0,17 and 0,990 ± 0,18; DO-Femur = 0,764 ± 0,16 and 0,780 ± 0,16.
Conclusions: the results showed significative improvement of climacteric symptoms and bone mass densitometry; not significative increased fast glucose levels and body mass index in both the groups of women.
PS-210
STUDY TO COMPARE THE EFFECTS OF HORMONAL AND PHYTOTHERAPIC TREATMENT IN CLIMACTERIC WOMEN
A. M. Fonseca, V. R. Bagnoli, C. R. Shigaki, J. S. Assis, M. H. A. Arie and E. C. Baracat
Department of Obstetrics and Gynecology, Medical School, São Paulo University, São Paulo, Brazil
Introuduction: hormonal treatment has been the first choice for the treatment of climacteric symptoms. However the high number of risk factors and also many contra-indications for hormonal treatment, have increased the options for alternatives treatments.
Objective: to compare three kinds of treatment for relief of climacteric symptoms.
Casuistry and Methods: a double blind study, that included 90 women, aging from 45 to 60 years (mean age 52,6years). They were separated in three groups: 30 treated with an association of micronized estradiol 2mg and noretisterona acetate 1mg (TH); 30 with “Trifolium pratense” (FT), extract with 40mg of isoflavonas, and 30 placebo (PT). The patients were evaluated by the parameters: Kupperman's Menopausal Index (KMI), Depression by Beck's Questionnaire and Griss Female Scale to evaluate the sexuality. All the parameters were evaluated before and one year of treatment, by techniques called Generalized Estimation Equations in three different moments to compare the results during the evolution of the study.
Results: the three parameters evaluated showed statistically significative improvement with the hormonal treatment. The phytoterapic and placebo treatment were similar.
Conclusions: although the patients treated with phytoterapic and placebo referred some improvement, this was not similar and effective to hormone treatment.
PS-211
THE EFFECT OF MODERATE INTENSITY EXCERCISES ON HOT FLASHES
B. Tartibian, S. sharabiany and A. Abbasi
Urmia University, Urmieh, Iran
Objective: Hormone therapy (HT) has been associated with an increased risk of chronic diseases. Therefore, attention is increasingly focused on managing vasomotor symptoms via behavioral approaches, including physical activity. The purpose of this study was to investigate the effects of aerobic exercises with moderate intensity on hot flashes.
Design & Method: Twenty healthy postmenopausal women participated randomly within 2 groups (control and experimental) in this investigation. The subjects had an average age of 53.6 ± 4.3 years, height of 156 ± 6.02 cm, body weight of 74.3 ± 14.6 kg, and BMI of 30.4 ± 5.31 kg/m2. They experienced at least five hot flashes per 24 h. The experimental group followed exercise training program including walking (60%–70% of MHR) over 30–40 min, three times a week for 10 successive weeks. Blood samples were taken before and after the exercise program to measure FSH concentration by method of RIELE. The results were analyzed by ANCOVA and paired t-test.
Results: A significant decrease was observed in FSH levels in the experimental group in comparison to the control group (P = 0.001).
Conclusion: The results of this study demonstrated that FSH level of postmenopausal women was decreased significantly following 10 weeks walking exercises training. This was probably associated with decreased vasomotor symptoms.
PS-212
THE IMPACT OF THE MULTIPLE SCLEROSIS ON THE ONSET OF MENOPAUSE
P. Koliba1, O. Zapletalová2 and P. Hradílek2
1Dept. of Obstetrics and Gynecology University Hospital, Olomouc, Czech Republic; 2Dept. of Neurology University Hospital, Ostrava, Czech Republic
Objective: Multiple sclerosis (MS) is a neurodegenerative, demyelinating and inflammatory disorder with an autoimmune etiology. It is thought to be a multifactorial disease with a complex mode of inheritance. Disease activity is supposed to vary during different hormonal periods and the relationship of sex hormones patterns to the MS c1inical course is evident. The impact of hormonal changes on the clinical disease process is well known especially in pregnancy, but not in perimenopause and menopause period even if the menopause in these patients starts earlier compared to healthy women. It is not yet known, if it is result of the neurodegenerative and inflammatory process according hypothalamo-pituitary-ovarian axis or the influence of the immunosuppressive, anti-inflammatory and symptomatic treatment, which could also evocate a precocious menopause.
Material and Methods: a retrospective analysis of 63 postmenopausal women with multiple sclerosis. The history, physical findings, stage of MS and also the potential etiology considering used drug treatment were analyzed.
Results: 33 patients (52.4%) of the analyzed group were diagnosed with the precocious menopause.
Conclusion: No clear evidence of direct influence of MS on the onset of menopause was found.
PS-213
THE INFLUENCE OF HORMONE REPLACEMENT THERAPY AND THE NATURE OF MENOPAUSE IN THE CLIMACTERIC SYMPTOMS
M. H. Moreira1, C. B. Rodrigues1, J. J. Raposo1, E. M. Coelho1 and J. L. Mocho2
1University of Trás-Os-Montes And Alto Douro, Vila Real, Portugal; 2North Health Administration/Health Sub-region of Vila Real, Vila Real, Portugal
Objective: The present study aims to assess the influence of both the HRT and the nature of menopause in the climacteric symptoms in postmenopausal women.
Design & Method: The sample included 401 Caucasian women (47–91 years old), 78.8% without HRT and 80.8% with natural menopause. Menopausal symptoms were evaluated by the Greene climacteric scale, validated in the postmenopausal Portuguese women. Standard t test for independent samples was used to compare means between groups (non-HRT and HRT users; natural and surgical menopause).
Results: The psychological symptoms (PS) showed a higher percentage (98.8%), followed by the somatic (SS, 97.5%) and a loss of interest in sex (84.5%). Moreover, the PS that showed higher manifestation were feeling tense or nervous (1.42 ± 0.87), sudden will of crying (1.40 ± 1.49), feeling tired or lacking in energy (1.39 ± 0.36) and irritability (1.33 ± 0.93). The mean value for SS varied between 0.68 (±0.85) for breathing difficulties and 1.85 (±0.92) for muscle and joint pains, having the sample revealed a higher frequency for the last one (88.3%) and parts of body feel numb or tingling (83%). As for the VS, more than half of the sample (55.4%) referred hot flushes, with an average of 0.90 (±0.98). Women with HRT had the highest score in the scale (+2.95. p ≤ 0.05) and total of SS (+1.94, p ≤ 0.01), and more heart beating quickly or strongly (+0.24, p ≤ 0.05). In relation to SS, we didn't differentiate feeling dizzy or faint and breathing difficulties.
Women with surgical menopause showed a higher score (p ≤ 0.05) in the total Greene climacteric scale (+2.71) and hot flushes (+0.39), demonstrated also high values (p ≤ 0.01) of feeling unhappy or depressed (+0.32) and muscle and joint pains (+0.30).
Conclusion: Our research suggests that nature of menopause has less influence in the climacteric symptoms than HRT. Surgical menopause was damaging for hot flushes, feeling unhappy or depressed (+0.32) and muscle and joint pains. The HRT is harmful to the majority of the SS and heart beating quickly or strongly, suggested less adequate medical prescription or inadequate use of them.
PS-214
TYPOLOGIES OF MIDDLE-AGED WOMEN ACCORDING TO SOCIAL LIVING CONDITIONS
Manzano Ovies Blanca Rosa1, Artiles Leticia2 and Navarro Daysi3
1Ramon Gonzalez Coro Gynecologic Hospital; 2Havana Medical School; 3National Institute of Endocrinology
Objective: To characterize middle-age women, structuring integral typologies according to: environmental context, morphological particularities, social living conditions and gender relations.
Subjects and Methods: The results of several studies on middle-aged women carried out in Cuba during the last decade were analyzed. These studies included different geographical places; municipalities of Plaza (n = 240), Playa (n = 412) and Centro Habana (n = 100) located in Havana urban areas, and in the municipality of Jobabo (n = 188) rural area located in the province of Las Tunas in the eastern part of the country. In addition, 250 women attending the Climacteric Clinic of the Ramon Gonzalez Coro Hospital in Havana were included.
The questionnaire used allowed us to obtain information on living conditions, social and demographic characteristics, family and couple dynamics, and about the different spaces where the productive (work links and satisfaction) and reproductive women roles are performed, personal satisfaction and perception of climacteric symptoms.
The qualitative techniques used (in depth interviews) as well as the quantitative ones allowed us to define a structural typology integrated by social and morphologic characteristics establishing a particular behavior.
Results: The following typologies were identified: TYPE I, ACCORDING TO RACIAL MORPHOTYPE, HOUSING CONDITIONS AND DIETARY PATTERN. Women with negroid morphotype, low cultural level, second-rate or bad housing conditions, low rate of labor links and a great household overload show a higher frequency of intense climacteric symptoms. Women with mongoloid morphotype, high cultural level, with no household overload and having intellectual jobs, show a lower frequency and intensity of climacteric symptoms, while women with europoid morphotype show climacteric symptoms of intermediate frequency and intensity. TYPE II ACCORDING TO SOCIAL LIVING CONDITIONS AND GENDER RELATIONS, include women living in urban areas, bad living conditions and gender overload showing a high perception of climacteric symptoms and TYPE III ACCORDING TO PERSONAL CONDITIONS AND THE PERCEPTION OF CLIMACTERIC SYMPTOMS, include women with low self-esteem, low personal satisfaction and low satisfaction with their work showing more intense climacteric symptoms.
Conclusion: The above-mentioned proposed typologies facilitate the creation of a basis to favor the decision-making process on these matters and the proper way the specialist should follow in each particular case.
PS-215
THE ROLE OF THE MENOPAUSE NURSE IN THE UK, A MULTIFACETED APPROACH
K. Abernethy1, A. Hillard2, D. Holloway3, E. Hughes4, P. Mc Fall5 and C. Amin1
1The Menopause Clinical and Research Unit, Northwest London NHS Trust, UK; 2Poole Menopause Centre, Poole Hospital NHS Foundation Trust UK; 3Guys and St Thomas NHS Foundation Trust, London, UK; 4City Hospital, Birmingham, UK; 5Menopause Clinic, Belfast Health and Social Care Trust, UK; 6Margaret Pyke Centre for sexual and reproductive health, London, UK
Objective: To show how in the UK the role of the Menopause Nurse varies between primary and secondary care and the independent nature of practice within these roles. To demonstrate this the profile of each of the members of the RCN Menopause Group steering group are used. The role that this group has in the education and updating and developing nurses in the UK is also shown.
Design: To outline a brief example of the roles and the responsibilities within the group. The main theme for this is to show the diversity of nursing roles. Each of the steering members as detailed above as authors will have a section outlining their role within menopause and/or gynaecology with an over action role for the RCN Menopause Group and how the group has been integral in organising courses for nurse education for menopause standards, such as competencies, and advice and support and dissemination of research to its members.
Conclusion: The role of the nurse within menopause in the UK is not a single flat one dimensional role. The role varies from primary care where the women see nurses for advice and consultation, through to advance practice nurses where they have their own menopause clinics and prescribe HRT independently. In secondary care for more specialised menopause services, nurses can be assistant or chaperone, can see simple cases, insert HRT implants, and following on from this some nurses take on the total care of the menopausal woman, including examination, prescription, hysteroscopy and endometrial biopsy. Underpinning all of this is the nursing background and the philosophy of nursing that the nurses take when entering consultation, which looks at the whole patient rather than the one area relating to hormone deficiency.
PS-216
TRADITIONAL CHINESE MEDICINE – ACUPUNCTURE AND CLIMATERIC SYNDROME TREATMENT
A. C. B. Luca, A. M. Fonseca, C. M. C. Lopes and E. C. Baracat
University of São Paulo, Clinic Hospital of São Paulo, São Paulo, Brazil
Objective: The use of complementary and alternative medicine such as Traditional Chinese Medicine – Acupuncture has been the result of treatment of vasomotor symptoms and the general of symptom of climacteric syndrome.
The goal of this research is evaluate the symptoms (Kupperman Index and hot flashes) using different treatment such as acupuncture and placebo.
Methods: There were selected 122 symptomatic climacteric women aged 45–60 years in two groups: Group 1: Traditional Chinese Medicine – Acupuncture and Group 2: Placebo. At the beginning the symptoms were called Moment 0. Group 1: Treatment was given for once a week per 10 weeks (Moment 1) and then twice a month (Moment 2) per a year with acupuncture. After a year the treatment changed to placebo for once a week per 10 weeks (Moment 3) and then twice a month per sixth months (Moment 4). Group 2: Treatment was given for once a week per 10 weeks (Moment 1) and then twice a month per sixth months (Moment 2) with placebo. After sixth months the treatment changed to acupuncture for once a week per 10 weeks (Moment 3) and then twice a month per a year (Moment 4).
Results: The frequency of flushes decreased significantly by more than 85% in both groups at the beginning when the treatment was given for once a week per 10 weeks. When placebo started twice a month the frequency of flushes increase, and acupuncture remained decreased. Value for the Kupperman Index decreased significantly by more than 93% in acupuncture treatment, instead of placebo that decrease only 15%.
Conclusions: The use of alternative therapy such as acupuncture for menopause symptoms is beneficial and relief almost all symptoms without any side effects.
PS-217
ULTRA LOW LEVELS OF 17BETA-ESTRADIOL NOT PREDISPOSE TO THE DEVELOPMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN WHO ATTENDED A CAMPAIGN OF POPULATION SCREENING
J. Presa, A. Santalla, F. Morón, C. Moreno, T. Aguilar, B. Romero, J. L. Gallo, J. Mozas, A. Salamanca, D. Galliano, A. Salinas and N. Mendoza
Hospital Virgen De Las Nieves, Granada, Spain
We know the relationship of hypoestrogenism with the development of postmenopausal osteoporosis and other diseases. Usually, by technical difficulties, in the laboratory not show us estradiol levels below what 20 pg/ml, and are considered a level below that value can be related to lower bone mineral density and increased risk of osteoporosis.
Materials and Methods: In a campaign detection of osteoporosis was enabled a bus with a peripheral densitometer (PIXI-calcaneus) and qualified personnel for information and sampling. The diagnosis of osteoporosis was confirmed by measuring hospital BMD of lumbar spine and hip (HOLOGIC). 94 postmenopausal women from attending gave their written consent to perform a measurement of the level of estradiol with ELISA technique.
Results: The average age of the patients was 59.03 ± 10.8 years and the body mass index 26.02 ± 1.12. Time since menopause until the study was 11.3 ± 8.42 years. 52 women had osteopenia and 20 osteoporosis values after central densitometry study. Although we noted a correlation between age and BMD (p < 0.05), we found no relationship between the levels of estradiol with either of these three variables.
Moreover, 23 women had estradiol levels below 10 pg/ml, and 7 under 5 pg/ml. None of the two groups there was a higher proportion of women with osteopenia or osteoporosis.
Conclusion: Statistical analysis shows that bone mineral density and postmenopausal period were significantly correlated; nevertheless, no correlation between serum 17beta-estradiol and age, bone mineral density or body mass index was found.
PS-218
VASOMOTOR SYMPTOMS REAPPEAR AFTER DISCONTINUATION OF POSTMENOPAUSAL HORMONE THERAPY – A SWEDISH POPULATION-BASED STUDY
L. Lindh-Åstrand1, J. Brynhildsen1, M. Hoffmann2, K. Magnusson3 and M. Hammar 1
1Department of Clinical and Experimental Medicine, Faculty of Health Sciences, Linköping University, Linköping, Sweden; 2Department of Medical and Health Sciences, Faculty of Health Sciences, Linköping University, Linköping, Sweden
Objective: To investigate to what extent vasomotor symptoms (hot flushes and sweating) reappeared after discontinuation of postmenopausal hormone therapy (HT) and possible background factors that contributed to women's decision to abandon HT.
Design & Method: In the second quarter of 2003 we performed a cross-sectional postal survey of all women (n = 1733), 53- and 54 years old, living in Linköping, Sweden. A validated questionnaire containing questions about menopause, HT, and vasomotor symptoms was used. Response rate was 77.3% and after omitting answers that were not complete 72.9% remained for analysis. Pearson chi-square test and logistic regression were used for statistical analysis.
Results: In our study 319 (25.3%) women were current users of HT, 242 (19.2%) previous users and 702 (55.6%) were never users. Of the 242 previous users 142 (59%) had discontinued HT within the last 2 years. Of those 242 women who were previous users 165 (69%) women clearly stated that they had vasomotor symptoms before starting HT. Out of these 165 women 143 (87%) reported that vasomotor symptoms recurred after they had abandoned HT. In those 143 women where vasomotor symptoms recurred (64%) reported that the symptoms were less frequent than before they started HT while only 9 (6%) thought that the symptoms were more frequent than before HT. There was no statistically significant difference in symptom recurrence between women who had used HT for 0–1, 2–4 or 5 years or more. Half of the women who were previous users had used HT between 0–3 years (50.4%).
In the logistic regression model background factors such as education, native language, smoking habits, area of residence, marital status, and occupation were included. Only residency was associated with a proneness to abandon HT. Women who were rural residents abandoned HT to a greater extent than urban women (p = 0.002).
Conclusion: The majority of women with vasomotor symptoms when they initiated HT (87%) reported recurrence of symptoms after discontinuation of HT. Effective and safe treatment approaches for women with recurrence are needed.
Complementary and alternative medicinet
P219
A RANDOMIZED DOUBLE BLIND TRIAL COMPARING SERTERALINE, GABAPENTIN, PLACEBO FOR TREATMENT OF MENOPAUSAL HOT FLUSH
Moghtadaei Parisa, Obstetrition and Gynecologist
Iran Medical Sciences University, Shohadaye Yaftabad Hospital
Objective: To estimate the effect of serteraline, gabapentin on hot flush frequency and severity in perimenopausal and menopausal women.
Method: We performed a randomized, double-blind, placebo-controlled trial in women aged 42–54 years with >20 hot flush per week or >3 per day (N = 90). Women were randomly assigned initially serteraline (50 mg), gabapentin (300 mg), placebo for two weeks. If no improvment were noted, the dose was increased to serteraline 100 mg, gabapentin 600 mg and placebo for six weeks.Hot flush frequency and severity were recordedon a daily dairy. Participants also completed questionaires addressing quality of life, menopausal symptoms, sleep quality, sexual function, mood, side effects.
Results: After eight weeks, hot flush frequency decreased in gabapentin group (40%), placebo (38%), serteraline (60%). Mean hot flush scores also decreased similarly in placebo and gabapentin groups (41%) but 56% in serteraline group. Campared with placebo, women in serteraline group were more likely to report dry mouth, dizziness and in gabapentin group to report more gasterointestinal complains, malaise. Sexual satisfication were similar in all groups.
Conclusion: Treatment with gabapentin did not improve hot flush frequency but serteraline improve hot flush frequency and severity compared placebo with bothersome effect.
PS-220
ACUPUNCTURE INCREASES DURATION OF SLEEP IN POSTMENOPAUSAL WOMEN WITH VASOMOTOR SYMPTOMS. ACUFLASH, A RANDOMISED CONTROLLED TRIAL
E. K. Borud1, T. Alræk1 and S. Grimsgaard1,2
1The National Research Centre in Complementary and Alternative medicine, University of Tromsø, Tromsø, Norway; 2Clinical Research Centre, University Hospital of North Norway, Tromsø, Norway
Objective: The study compared the effect of acupuncture and self-care versus self-care alone on vasomotor symptoms in postmenopausal women. We here report on the effects on sleep at night.
Design & Method: The study was a multicentre, pragmatic, randomised controlled trial with two parallel arms. Primary endpoint was change in hot flash frequency from baseline to 12 weeks. Postmenopausal women were recruited by media coverage and newspaper advertisements. Eligible women did not use hormone therapy or antidepressants, and documented ≥ 7 hot flashes/24 hours during seven consecutive days at baseline. They were randomised to individualized acupuncture treatment (10 sessions) and advice on self-care (acupuncture group) or advice on self-care alone (control group). The study was conducted in three centres in Norway (Tromsø, Bergen, and Oslo) in 2006–2007. Ten experienced practitioners provided the acupuncture treatments. The participants recorded hours of sleep each night in one-week diaries at baseline and at week 12. At week 12 they answered global questions addressing changes in menopausal symptoms.
SPSS 14.0 was used for statistical analysis. Change in sleep was calculated as hours of sleep/24 hours at 12 weeks minus hours of sleep/24 hours at baseline. Differences in change between groups were evaluated with two-sample t-tests, and Chi-square tests were used for categorical variables. Two-sided p < 0.05 was considered statistically significant.
Results: Altogether 535 women were assessed for eligibility, and 267 were randomised to acupuncture (n = 134) or control (n = 133) groups. Overall dropout rate was 7%. Mean age at inclusion was 53.8 years.
Baseline mean hours of sleep per night were 6.1, (range 2.9 to 8.3) among all participants. At 12 weeks, mean hours of sleep increased by 0.42 hours in the acupuncture group and 0.14 hours in the control group, a difference of 0.28 hours (95% CI 0.05–0.50), p = 0.015.
In the acupuncture group, 121 (90%) of the participants reported that their climacteric complaints had changed during the study period, compared to 52 (39%) in the control group, p < 0.001. Eighty-eight participants (66%) in the acupuncture group reported increased sleep quality and 96 (72%) reported increased well-being, respectively, compared to 21 (16%) and 31 (23%) in the control group (p < 0.001 and p < 0.001).
Conclusion: Hours of sleep at night increased significantly, and a significantly higher proportion of women in the acupuncture group reported increased wellbeing at 12 weeks.
PS-221
ASSOCIATION BETWEEN DAILY ISOFLAVONES INTAKE AND THE EXISTENCE OF HOT FLUSHES IN INDONESIAN POST MENOPAUSAL WOMEN
A. Hestiantoro1, A. Pertamawan1, S. Sayogo2 and S. Sudarsono3
1Reproductive Immunoendocrinology Division, Department of Obstetrics and Gynecology; 2Department of Nutrition; 3Department of Public Health, Faculty of Medicine, University of Indonesia, Cipto Mangunkusumo Hospital, Jakarta
Objective: Due to low estrogen circulating levels, post menopausal women may have Climacteric syndrome. A hot flushes is one of the climacteric symptoms which are quite often observed in Caucasian and African post menopausal women population. On the contrary, such condition is observed less in Asian post menopausal population particularly in Indonesian postmenopausal women. High amount intakes of isoflavones containing food are hypothesized to be associated with low incidence of hot flushes in Indonesian post menopausal women. Our study is to determine whether such amount of isoflavones intakes may contribute in reducing the hot flushes complaining in post menopausal women in Jakarta, Indonesia.
Design and Methods: This study is cross sectional study. 192 Indonesian postmenopausal women ranging between 40–59 years old were recruited into this study. They were interviewed for 3 × 24 hours' food recalls and food frequency amount (FFA) in order quantifying the amount of isoflavones daily intake. In addition, we quantified the daily urine isoflavones excretion, and determined the hot flushes prevalence.
Results: 16.7% participants revealed low daily isoflavones intake (<30 mg/day) and 69.4% participants revealed good daily isoflavones intake (>30 mg/day). 95.4% participants showed low excretion of isoflavones daily (<5.36 μM/l) and 4.6% participants showed good excretion of isoflavones daily. 2.8% participants is suffering from hot flushes, and they tend to have lower amount of daily isoflavones intake compared to whom did not suffer from hot flushes symptom.
Conclusion: Isoflavones intake is only subset from other factors involved in the hot flushes symptoms observed in Indonesian post menopausal women.
PS-222
CHANGES OF ANGIOPOIETIN-1, -2 CONCENTRATIONS BY PHYTO ESTROGENS IN HUMAN ENDOMETRIUM
SeRyun Kim1, JeeHyun Park2, YoungJoon Park1, JongWook Kim1, BuyngIck Lee2, Kiyoung Ryu1 and JaeWook Kim1
1Myongji Hospital, Kwandong University, Koyang, Kyunggi, Republic of Korea; 2Inha University Hospital, Incheon, Incheon, Republic of Korea
Objective: Angiogenesis is a process how new blood vessels are created from preexisting vasculature. It is related with gynecologic disease such as endometrial hyperplasia, endometrial cancer, and dysfunctional uterine bleeding. Angiopoietins are important angiogenic factors. This study was designed to assess the changes of concentrations of angiopoietins in cultured human endometrial cells by phytoestrogens.
Design & Method: This study included premenopausal women who were undergone hysterectomy for benign disease excluding endometrial pathology. Endometrial epithelial cells and stromal cells were isolated and cultured separately. We treated 17β-estradiol, daidzein, and equol whose concentrations were 10–6M, 10–5M, 5×10–5M on the cultured cells and incubated the cells for 12, 24, 48 hours. Then cultured media were extracted, centrifuged, and stored at -70? until ELISA for engiopoietin-1, -2.
Results: Concentrations of aniopoietin-1 and angiopoietin-2 were highest at 12hour in stromal and glandular cells which were treated by 17β-estradiol and then decreased. However, it is not statistically significant. Same trends were observed in epithelial cells and stromal cells which were treated by daidzein. In equol treated groups, angiopoietin-1 was highest at 12 hour in both stromal and glanduar cells. Angiopoietin-2 in glandular cells was highest at 12hour, but angiopoietin-2 in stromal cells was not changed in time. There were no differences in concentrations of angiopoietin-1, -2 according to increasing concentration of 17β-estradiol, daidzein, and equol.
Conclusion: Secretions of angiopoietin-1, -2 in cultured normal human endometrium which was treated by daidzein and equol were highest at 12hour and not increased in time although it was not statistically significant.
PS-223
EFFECT OF SOY ISOFLAVONES ON SEXUAL FUNCTION IN POSTMENOPAUSAL WOMEN: A RANDOMIZED, DOUBLE-BLIND, AND PLACEBO-CONTROLLED STUDY
Hernández Karla, von Helde Sueli, Tobar Cristina, Castaño Rosario, Paredes Adriana and Palacios Santiago
Instituto Palacios de Salud y Medicina de la Mujer, Madrid
Introduction: 43% of women between 18 and 19 years have some sexual dysfunction problem. The relation between the use of soy isoflavones as an alternative treatment of climacteric symptoms and female sexual function has not yet been studied.
Objective: To analyze whether the treatment with 100mg non genetically modified soy isoflavones (genistein 49 mg, daizen 43 mg, and glycitein 8mg) modified sexuality in climacteric women.
Material and Methods: A prospective, randomized, double blind, placebo control study was carried out with a 24 week follow up. The following inclusion criteria was applied: healthy, postmenopausal women between 45 and 65 years, with a subjective reduced quality of life, and with a uterus. Two groups were randomly formed by the block technique, the study drug was disguised in the form of a capsule which was identical in both groups. The statistical treatment of the information was carried out with the ANOVA test by repeated measurements and the interference method. For 24 weeks, 3 interviews took place: at the beginning, at week 14 and week 24 in which the sexual pathology of the participants was assessed according to The Female Sexual Index (FSFI) and The Personal Distress Scale (PDS).
Results: 75 patients who complied with the inclusion and exclusion criteria were included, of which 38 were in the active drug group (group A), and 37 were in the placebo group (group B). The Female Sexual Function Index (FSFI) has 6 dimensions, desire, lubrication, orgasm, satisfaction and pain, with no statistically significant results at 14 weeks of treatment (>0.5) but a significant difference in the desire dimensions was found (p = 0.0305), and pain (p = 0.0119), with respect to the time at 24 weeks of treatment. In the assessment of The Personal Distress Scale (PDS), there was no significant statistical difference neither at 14 nor at 24 weeks of treatment.
Conclusions: The use of non genetically modified soy isoflavones at a dose of 100mg (genistein 49 mg, daizein 43 mg, glicitein 8 mg, gelatine, titane dioxide E171 2%) seems to have a positive influence in terms of the time of use in the dimensions of desire and pain of the (FSFI). More follow up studies are necessary to confirm this result.
PS-224
EFFECT OF SOY ISOFLAVONES ON PROSTAGLANDIN SYNTHESIS IN HUMAN ENDOTHELIAL CELL CULTURES
M. Paulo, M. M. Salvador, M. M. B. Montes and M. R. T. Toloi
Faculty of Pharmaceutical Sciences of Ribeirão Preto- University of São Paulo, Brazil
Objective: It is now well recognized that natural estrogen, 17β-estradiol, has beneficial effects on the vasculature of postmenopausal women, providing a reduced mortality of cardiovascular diseases. This protective effect is partly caused by direct estradiol actions on the vascular cells, one of the mechanisms being stimulation of endothelial synthesis of prostaglandins (a potent vasodilatador and strong inhibitor of platelet aggregation). However, conventional hormone replacement therapy (HRT), that use estrogen is suspected to increase the risk of breast cancer and to cause other undesirable side effects (breast tenderness, uterine bleeding, etc). So many women seek for a more natural alternative to HRT and prefer the so-called phytoestrogens, which are a group of natural compounds that exert estrogenic activity and are used for the treatment of menopausal disorders. The three main categories of phytoestrogens are isoflavones, lignans and coumestans. The present investigation was conduct to determine if the soy isoflavones (biochanin A, daidzein, formononetin and genistein) stimulate prostaglandin E2 (PGE2) synthesis in human endothelial cell ECV-304.
Design & Methodology: EVC-304 cells were incubed with soy isoflavones (biochanin A, formononetin, daidzein and genistein) at 6 μM/mL for 60, 80 and 120 minutes and with 17β-estradiol (1 μM/mL) for 60, 80 and 120 minutes. The prostaciclin production was measured by ELISA- Enzyme Linked Immuno Sorbent Assay (Prostaciclin E2 Biotrak TM ELISA System - Amersham Biosciences, 2004). Statistical analysis was performed by ANOVA and Student's test was performed. P < 0,05 was considered significant.
Results:
Table 1 Effect of soy isoflavones daidzein and genistein on PGE2 prodcution
Conclusion: Soy isoflavones daidzein and genistein enhance PGE2 production in endothelial cell. Biochanin A and formononetin did not change significantly PGE2 production.
PS-225
EFFECTS OF SELECTIVE ESTROGEN RECEPTOR MODULATOR CIMICIFUGA RACIMOSA ON BONE METABOLISM AND SERUM LIPIDS IN POSTMENOPAUSAL WOMEN ON CHRONIC HEMODIALYSIS
Martynyuk Liliya1, O. I. Dyachan2 and Martynyuk Larysa3
1Department of Nephrology Ternopol State Medical University; 2Department of Psychiatry Ternopol State Medical University; 3Department of Endocriniligy Ternopol State Medical University, Ternopil, 46002 Ukraine [email protected].
Uremic hypogonadism with premature amenorrhea and hypoestrogenism and lack of hormone replacement therapy after menopause have been frequently found in end stage chronic renal disease (ESRD) women on dialysis. In addition to renal osteodystrophy, postmenopausal women on dialysis are at risk of osteoporosis, hyperlipidemia, arteriosclerosis and depression. Оbjective. The aim of this study was to evaluate the effects of a combined low-dose therapy of alphacalcidol, calcium carbonate and phytoselective estrogen receptor modulator (phytoSERM), particularly, Cimicifuga racimosa extract BNO 1055 in postmenopausal ESRD women. Material and methods. The study included 50 postmenopausal women with ESRD (glomelular filtration rate less than 15 ml/min). In all patients, we evaluated biochemical parameters (serum concentration of calcium, phosphorus and alkaline phosphatase (AP), serum lipids (total low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol and triglycerides), and HADS scale parametres. BMD was measured at 2 sites- lumbar spine (L1-L4) and femoral neck using dual energy X ray absorptiometry at baseline and after 12 months of treatment. Patients were randomized into two groups: is first group (26 women) were administered 1000 mg of calcium, alfacalcidol at a daily dose of 0,25 microg and Cimicifuga racimosa extract 1 casp twice a day. In second group (24 women) calcium carbonate at daily dose 1,0 gram of elemental calcium was administered. Results. In phytoSERM's group the mean serum calcium, increased significantly and alkaline phosphatase (AP) declined significantly, LDL-cholesterol decreased and HDL cholesterol increased significantly in the phytoSERM's group with no changes in serum triglycerides, total cholesterol. In the control group the levels of calcium, phosphorus and AP and lipid spectrum were not significantly different at baseline and after 12 months. The indeces of HADS scale showed significant reduce of depressive and anxiety symptoms in phytoSERM's group in comparison with no changes in control group. In the control group, the mean BMD at lumbar spine decreased in ((5,41 ± 0,01) %, from at baseline. In comparison in phyto SERM's group it increased in (+ 1,33 ± 0,82) % from baseline (p < 0,01). No significant side effects were observed in the phytoSERM's group. Conclusions. The study demonstrates that after one year phytoSERM Cimicifuga racimosa extract and alphacalcidol treatment, postmenopausal women on hemodialysis have a significant increase in trabecular BMD, HDL cholesterol, decrease in bone resorption markers and LDL-cholesterol values, reduction of depressive and anxiety symptoms suggesting that phytoSERM's can be used safely for prevention of postmenopausal osteoporosis, lipid disorders, depression and anxiety in ESRD women on hemodialysis.
PS-226
EFFECTS OF SOY PROTEIN SUPPLEMENTATION ON MENOPAUSAL SYMPTOMS IN MENOPAUSAL ORUMIEH WOMEN
M. Ebrahimi, Z. Yecta, M. Taghizadeh and H. Vatandoost
Orumieh medical university, Iran
Introduction and Objective: According to statistics from the world Health Organization, the average life span of a women living in most countries is approximately 80 years. Therefore the vast majority of women will reach menopause. Between 55% and 75% of these women will experience vasomotor symptoms (hot flash) or other symptoms, such as depression, mood swing, sleep disorders, vaginal dryness, and joint pain. The goals of this study were designed to evaluate changes in menopausal symptoms in responds to soy protein supplementation on menopausal symptoms in postmenopausal women who leave in Orumieh city in Iran.
Methods: This study was a randomized, double- blind, Placebo- controlled trial designed to investigate the effect of 20-grams daily soy protein supplements. In 80 healthy postmenopausal women reporting vasomotor symptoms at base line. They were randomized into two groups; In case group (n = 40) and in control group (n = 40). The control group consumed a daily 20-g of placebo. The menopausal Kupperman index was used to assess changes in menopausal symptoms at base line and after 4, 8 and 12 weeks of intervention.
Result: The epidemiologic and clinical characteristics of age education, and social status, use of nicotine, BMI, Blood pressure and Diabetes were similar in both groups. In the first visit symptoms were similar between placebo and soy protein groups (P = 0.385). The data showed a decrease in menopausal symptoms (P = 0.000 paired t test, two paired, between base line and soy protein group. Also ANOVA test showed a decrease in menopausal symptoms. Between case and placebo groups (F = 8/69 P = 0.004).
Conclusion: This study suggests that soy protein 20- grams daily supplement may be a safe and effective alternative therapy for menopausal symptoms.
PS-227
ENDOMETRIAL SAFETY ASSESSMENT OF A SPECIFIC AND STANDARDIZED SOY EXTRACT
S. Palacios1, F. Vazquez2, B. Pornel3, J. Eden4, P. Chantre5, L. Aubert5, E. Buendia6 and P. Mares7
1Instituto Palacios, Madrid, Spain; 2Clinica de Ginecologia, Lugo, Spain; 3Brussels Menopause Center, Brussels, Belgium; 4Sydney Menopause Centre, Sydney, Australia; 5Arkopharma, Carros, France; 6Arkochim, Madrid, Spain; 7Hôpital Caremeau, Nîmes, France
Objective: To assess the endometrial safety of an oral soy isoflavones extract according to the EMEA Guidelines which specified that 300 patients treated for 1 year are necessary to estimate the incidence rate of hyperplasia with the required precision.
Design & Method: 395 post menopausal women 45–65 years old were included in this international open study. Patients received daily 70 mg of a soy isoflavones extract (35 mg daidzin, 21 mg glycitin and 14 mg genistin) for 52 weeks. Patients had the possibility to continue the treatment 2 additional years.
Endometrial biopsy and transvaginal ultrasounds were performed at inclusion and after 12 months and 36 months of treatment according to the European guidelines.
Results: No case of hyperplasia or cancer was diagnosed for the 305 biopsies of women who completed the 1 year of treatment. For all results “no endometrial tissue” or “tissue insufficient for diagnosis”, the endometrial thickness was ≤ 4 mm. At 1 year, the calculated incidence rate of hyperplasia outcome was 0% with an upper limit of 95% Confidence Interval of 0.012.
Among the 235 patients who wished to continue the study, 87 have already completed their 3 years of treatment (biopsy results below).
Endometrial thickness did not show any increase after 12 months of treatment (2.2 ± 0.98 mm at inclusion and 2.12 ± 1.1 mm at the end of the study).
The vaginal bleeding were monitored daily by using an electronic patient diary. We collected a total of more than 89000 days with answer during treatment period. The percentage of days without any bleeding represented 99.2% of days with answers during the treatment period whereas they were 95% during selection period.
Conclusion: On the basis of our results, we can conclude that this specific and standardized soy extract doesn't exert a mitogenic effect on the endometrium. It can represent a safe alternative among the various treatments proposed to post menopausal women.
PS-228
NUTRITIONAL SUPPLEMENTS AMONG HEALTH-CONSCIOUS PRE-/POST-MENOPAUSAL THAI WOMEN AT SIRIRAJ MENOPAUSE CLINIC
P. Leerasiri, C. Chayachinda, M. Rattanachaiyanont, S. Indhavivadhana, P. Tanmahasamut, K. Techatraisak and S. Angsuwathana
Department of Obstetrics and Gynecology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Objective: To study the use of nutritional supplements among health-conscious, pre-/post-menopause Thai women at Siriraj Menopause Clinic.
Design & Methods: A cross-sectional study was conducted in pre-/post-menopause Thai women who registered to our health promotion program from January to December 2006. Before attending a health education class in the program, all participants completed a self-administered questionnaire enquiring about their demographic data, use of nutritional supplements, attitude and knowledge regarding the nutritional supplements commonly used in Thailand.
Results: Of 172 participants, 45.3% were non-users, 37.3% were current users, and 17.4% were past users. All groups were similar in age (range 40–67 years), education level (the majority had education for >12 years), reading habit (the majority was frequent readers), economic status (the majority had adequate income for living), and medical history (30–40% had medical diseases). The prevalence of inappropriate attitude and inadequate knowledge of each nutritional supplement varied from 8.7% to 65.9%. Relatives and friends were the main source of their information. Most of the users obtained the supplements from drugstores. The non-user group was different from the user group in the following attitudes: they believed that only the supplements suggested by medical doctors were beneficial, the proper food consumption could replace any supplements, and the supplements could cause adverse effects.
Conclusions: More than 50% of health-conscious pre-/post-menopausal Thai women use or had used nutritional supplements. Although the majority of this population has high education, the prevalence of misconception about nutritional supplements is high. The correct information regarding the nutritional supplements should be more publicized in order to improve the proper consumption of these products.
PS-229
PATIENTS POSITIVE ATTITUDE ABOUT A SOY EXTRACT WITH PROBIOTIC: THE M3 STUDY
S. Palacios1, M. J. Cancelo2, C. Castelo Branco3, J. L. Neyro4 and I. Alvarez5
1Instituto Palacios de Salud y Medicina de la mujer, Madrid, España; 2Hospital Universitario de Guadalajara, Universidad de Alcalá de Henares, España; 3Hospital Clínic, Universidad de Barcelona, España; 4Servicio de Ginecología y Obstetricia, Hospital de Cruces, Universidad del País Vasco, España; 5Medical Department of Rottapharm
Objective: To determine women's perception of a soy extract with probiotic on climacteric-related symptoms.
Design & Method: A prospective multicentric survey was carried out. A total of 2044 women 40–65 years of age, who were recruited by a group of 198 random Spanish gynaecologists. The women completed a self report survey in the beginning and after 6 months of use of a soy extract(30mg of genistein and 30 mg of daidzein), with probiotic (500 million sporos of lactobacillus sporagenes), calcium (141mg) and vitamin D(5mcg). The questionnaire included 15 items of menopause and health, and 4 about sexuality from the Cervantes scale. Patients and gynaecologists completed an assessment about the clinical state.
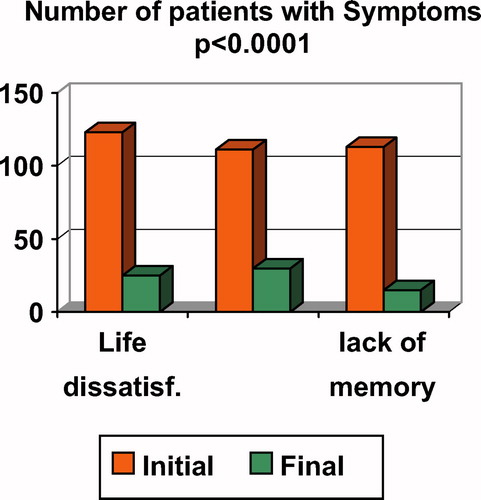
Results: The most frequent and important symptoms were hot flushes, sleeping disorders and sweats (Fig 1).
Table 1 Mean scores (initial and after 6 months) of the answers to the 15 questions of the “Menopause and Health” block of the Cervantes Scale
After 6 months, the studied soy extract improved the climacteric symptoms (Table 1).
Fig 1 The most important climacteric symptoms (n = 1820)
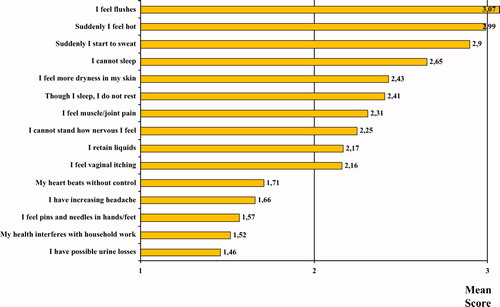
Conclusion: The peri and postmenopausal patients usually experience common menopausal symptoms and many believe that soy extract improve their menopause symptoms. Physician providers should be aware of patient's positive attitude.
PS-230
QUALITY OF LIFE OF POST MENOPAUSAL WOMEN TREATED FOR 1 YEAR WITH A SOY EXTRACT
P. Mares1, L. Aubert2, S. Palacios3, F. Vazquez4, J. Eden5, P. Chantre2, E. Buendia6 and B. Pornel7
1Hôpital Caremeau, Nîmes, France; 2Arkopharma, Carros, France; 3Instituto Palacios, Madrid, Spain; 4Clinica de Ginecologia, Lugo, Spain; 5Sydney Menopause Centre, Sydney, Australia; 6Arkochim, Madrid, Spain; 7Brussels Menopause Center, Brussels, Belgium
Objective: To evaluate the quality of life of patients treated with an isoflavone extract during the course of a study assessing the endometrial and breast safety lasting 12 months.
Design & Method: 395 post menopausal women 45–65 years old were included in this international open study whose primary outcome was endometrial safety assessment. Patients were included if they suffered from hot flushes (but no incapacitating ones) and/or climacteric troubles and if they had no breast nor endometrial abnormality.
Patients received daily 70 mg of a soy isoflavones extract (35 mg daidzin, 21 mg glycitin and 14 mg genistin) for 52 weeks.
Patients were questioned by the investigator to complete the Kupperman questionnaire at each visit. To monitor precisely the number hot flushes and their intensity, the patients were requested to answer daily to a Symfo Electronic Diary (SED).
Results: The total Kupperman score at inclusion was 17.04 ± 7.81 and it decreased by 40.8% to 10.11 ± 7.84 after one year of treatment. The largest mean decreases from baseline were in hot flushes, nocturnal sweating and nervousness.
The positive effects of Phytosoya on hot flushes have been analyzed in details with Symfo data. More than 6900 cumulative days were analyzed for selection period (period duration = 24.8 ± 14.5 days) and more than 80 000 cumulative days of answers were available for treatment period (period duration = 276.6 ± 72.3 days). The number of days without hot flushes represented 27.5% during selection period and it increased to 50% of days during treatment period. This analysis clearly demonstrated an improvement on hot flushes symptoms during treatment period.
A subsequent analysis of SED data has been performed on a sub group of patients who suffered from important hot flushes. This stringent population was defined as patients who reported at least 5 hot flushes/day during ¾ days of selection period. 71 patients met these criteria. During screening period, the answers with at least 5 hot flushes per day represented 72.6% of answers, whereas it decreased to 36% during the treatment period. For 21.8% of days in selection period the intensity of hot flushes were rated as severe whereas it decreased to 8% of days during treatment period.
Conclusion: Reductions from baseline in the frequency and severity of hot flushes as well as decrease in Kupperman score demonstrated that Phytosoya improved quality of life of post menopausal women.
PS-231
REASONS OF DEMAND FOR PHYTOTHERAPY DRUGS IN THE CLIMACTERIC
S. M. R. R. Lima1, B. F. Reis1,2, S. Saito1, A. Ruggero1 and T. Aoki 1
1School of Medical Sciences of Santa Casa de São Paulo, São Paulo, Brazil; 2Vale do Sapucai University, Pouso Alegre, Minas Gerais, Brazil
Objective: To assess the reasons why symptomatic women at the time of the climacteric, spontaneously sought attention at the Climacteric Phytotherapy Outpatient Clinic.
Methods: We included 230 women aged from 40 to 65 years, with time after menopause greater than a year, with symptoms quantified by the Kupperman Menopausal index, in the Climacteric Phytotherapy Outpatient Clinic of the Santa Casa de São Paulo, Brazil, in the period from January to April 2007. The diagnosis of climacteric was given based on clinical history and dosage of FSH ≥ 30 mIU/mL. All women had not had hormonal treatment, or the use of antimicrobial activity or other nutritional supplements for this indication at least six months before the start of the study. The reason why they sought the Service was asked at the start of treatment and the other risk factors that contra-indicate the traditional hormonal therapy.
Results: The average age of women assessed was 54.1 ± 5.59 years, with the menopausal age of 45.7 ± 6.03 years and after menopause period of 1 to 20 years, with an average of 6.9 ± 6.9 years. The reasons for the preferred phytoterapy were: 70% preference for phytomedications, 11.8% contra-indications for hormone-dependent diseases; 11.6% without preference for any kind of the treatments and 5.8% noncompliance of hormonal therapy. The fear of the increased incidence of cancers reported as one of the side effects of hormonal therapy was the main reason for the choice of phytomedications.
Conclusion: Currently there is a great demand for medical services that offer a range of therapeutic possibilities for the remission of symptoms among them includes therapy with phytomedications. The World Health Organization (WHO) in the year of 1978, recognized phytotherapy as a valid form of treatment and should be prescribed after mentioning its risks and benefits. Most of the women (70%) who sought phytomedications instead of traditional hormone therapy, did so with main reason being the fear of developing cancer.
PS-232
SOJA ISOFLAVONES WITH LACTOBASCILLUS SPOROGENES IN RECENT MENOPAUSE WOMEN: EFFECTS ON CLINICAL SYMPTOMS AND BONE DENSITY: A COMPARATIVE PROSPECTIVE STUDY OF 62 PATIENTS
S. Zervoudis1,2, G. Iatrakis1, I. Navrozoglou2, C. Tsionis1, D. Chaniotis1 and I. Diakakis1
1Technol, University TEI, & Lito Maternity Hospital, Athens, Greece; 2Gynaecological Clinic Ioannina University Hospital, Ioannina University, Greece
Objective: The aim of this prospective study was to assess the efficiency on climacteric symptoms and bone density of a phytoestrogen product (soja isoflavones plus lactobascillus sporogenes plus calcium: SLC) in a group of menopausal patients, compared with a control group.
Methods: In a multicentric 52 weeks trial, 68 women (42–53 years mean 50.9) with recent menopause were randomized to be treated with either SLC (n = 33,Group1) or with Vitamin E 500 ui per day : control group (n = 33 Group 2). A QUOL questionnaire assessed the presence of hot flushes > 5/day, sweating eρisodes >5 day, libido's disturbance and insomnia. Bone density was measured with DEXA technique both on spine and hip. The patients were assessed in the beginning of the study and after 1 year of treatment. Six patients: three in each group were excluded for abandonment or incomplete datas, finally, 62 patients (31 in each group were studied.
Results: Percents of complete responders (total absence of complaints) after 52 weeks were 41,9% Group 1 (n = 13) and 16,1% Group 2 (n = 5) regarding hot flushes. (p < 0.05). For sweating episodes the percentages were 38,7% (n = 12) versus 9,6% (n = 3) (p < 0.05). Libido improved in 71% (n = 22) versus 29%(n = 9), (p < 0.05), insomnia decreased in 35,4% (n = 11) versus 16,1% (n = 5),(no significant). Bone density was slightly increased after 1 year in group 1: mean + 1,2% (hip) and + 0.6% (spine). In contrast, DEXA measurements in group 2 after I year showed: mean: −0.4% (hip) and −0.8% (spine). The difference between the 2 groups was not significant.
Conclusion: SLC contains not only phytoestrogens and calcium but also lactobacillus that increase their absorption in the bowel. This potential effect of lactobascillus is probably responsible for the good results on most climacteric symptoms. Moreover calcium with isoflavones could have a slight positive effect on bone density. This product could be an effective alternative treatment to classical HRT in menopause patients with climacteric symptoms.
PS-233
THE EFFECT OF SOY DIETARY SUPPLEMENT AND ESTROGEN ON MAIN CARDIOVASCULAR HEALTH BIOMARKERS: A RANDOMIZED CONTROLLED TRIAL
L. O. Carmignani, A. O. Pedro, A. M. Pinto-Neto and L. H. S. Costa-Paiva
Faculty of Medicine of State University of Campinas, São Paulo, Brazil
Objective: To assess the effects of a soy dietary supplement on the main biomarkers of cardiovascular health in postmenopausal women compared with the effects of the hormone replacement therapy (HRT) and placebo.
Design & Method: Sixty healthy postmenopausal women, aged 45–60, were recruited and randomized into three double-blind controlled groups: a soy dietary supplement group (isoflavone 90mg), a HRT group (estradiol 1mg plus noretisterone 0,5mg) and a placebo group. Lipid profile, glucose level, body mass index, blood pressure and abdominal/hip ratio were evaluated in all the participants at the baseline and after 16 weeks. Statistical analyses were performed using chi-squared and Fisher's exact test and repeated-measures analysis of co-variance.
Results: after a 16 weeks intervention period, total cholesterol decreased 12% in HRT group, but in the soy dietary supplement and placebo groups, it did not change. The LDL-cholesterol decreased 18% in the HRT group and it did not change in the other groups. HDL-cholesterol, triglycerides, glucose level, body mass index, blood pressure, and abdominal/hip ratio did not change over the time in all three groups. As expected, FSH decreased and 17β-estradiol increased only in the HRT group.
Conclusion: The dietary soy supplement did not show a significant favorable effect on cardiovascular health biomarkers comparing with HRT use.
PS-234
THE EFFECT OF SOY DIETARY SUPPLEMENT AND ESTROGEN ON MENOPAUSAL SYMPTOMS: A RANDOMIZED CONTROLLED TRIAL
L. O. Carmignani, A. O. Pedro, A. M. Pinto-Neto and L. H. S Costa-Paiva
Faculty of Medicine of State University of Campinas, São Paulo, Brazil
Objective: To compare the effects of daily ingestion of soy dietary supplement, hormone replacement therapy (HRT) and placebo on menopausal psychological, somatic and urogenital symptoms in postmenopausal women.
Design & Method: This was a double-blind, randomized, controlled, intention-to-treat trial. Sixty healthy postmenopausal women, 1 to 13 years after menopause were recruited and randomized into three groups: a soy dietary supplement group (isoflavone 90mg), a HRT group (estradiol 1mg plus noretisterone 0,5mg) and a placebo group. The Menopause Rating Scale (MRS) was used to assess change in menopausal symptoms at baseline and after 16 weeks of treatment. To examine the effects of this regime on endogenous hormone levels, follicle-stimulating hormone (FSH) and 17β-estradiol were measured. Statistical analyses were performed using chi-squared and Fisher's exact test and repeated-measures analysis of co-variance.
Results: The data showed a decrease on total MRS score comparing the baseline and after 16 weeks in all groups. There were significant improvements on somatic and urogenital symptoms comparing baseline and after 16 weeks in HRT and isoflavone group. Psychological symptoms did not change over the treatment period in all the studied groups. As expected, FSH decreased and 17β-estradiol increased only in the HRT group.
Conclusion: This study suggests that a soy dietary supplement regime treatment may be an effective alternative therapy for somatovegetative and urogenital menopausal symptoms.
PS-235
THE CHAGE OF BONE MINERAL DENSITY, BONE TURNOVER MARKER,FIBRINOGEN LEVEL BY ADMINISTRATION OF FERAMIN-Q¢Ç FOR 1 YEAR IN KOREAN POSTMENOPAUSAL WOMEN
H. Suh and S. Noo
Gachon Medical School, Gil Medical Center, Korea
Background: Feramin-Q® is a compositeness of ‘Black Cohosh’ and ‘St. John's Wort’. There have not been studies about the influence of Feramin-Q® on bone mineral density, bone turn over markers, and plasma fibrinogen in Korea. For this study, the influence of Feramin-Q® on each factors were examined.
Method: 100 participants who visited the clinique in a hospital were involved. The criteria were as follows: a woman who menopaused for at least one year and had not been treated with HRT for more than 3 months, All participants took 2–4 tablets of Feramin-Q® which contains black cohosh 0.0364 ml and hypericium 84 mg per one tablet, for one year. Pre and post numerical values on each factors were compared.
Result: Statistically, a significant increase was shown in the urine deoxypyridinoline (P = 0.000), the serum FSH (P = 0.000) and the total cholesterol (P = 0.025) after taking Feramin-Q® for one year. Significantly, there were statiscal decreases in the serum estradiol (P = 0.000) and plasma fibrinogen (P = 0.021) after taking Feramin-Q® for one year. And there were no statiscal changes in BMD and other factors.
Conclusion: In this study, after taking Feramin-Q® for one year, there were increments of urine deoxypyridinoline, and no change in BMD. What we would like to carefully suggest is that Feramin-Q® dose not affectively control the suppression of the born absorption in menopaused women. Moreover, there is a significant decrease of the plasma fibrinogen. Many large-scale prospective studies would be needed.
PS-236
THE INFLUENCE OF RED CLOVER DERIVED ISOFLAVONES ON METABOLIC CARDIOVASCULAR RISK FACTORS IN POSTMENOPAUSAL WOMEN
M. Terzic1, J. Dotlic1, S. Maricic2, T. Mihailovic3 and I. Pavlovic1
1School of Medicine University of Belgrade Institute of Gynecology and Obstetrics, Belgrade, Serbia; 2General Health Center “Savski Venac”, Belgrade, Serbia; 3Ultramedica Clinic, Belgrade, Serbia
Objective: The goal of this study was to estimate the effects of red clover derived isoflavones on serum lipid levels in postmenopausal women.
Design & Method: The study involved 40 healthy postmenopausal women, divided in two groups. The first group of 22 women received red clover derived isoflavones while the second group of 18 women was without medications. We investigated total cholesterol, cholesterol fractions and triglycerides in blood of patients in both groups, before treatment and in three months periods throughout 12 months. Statistical tests for assessing differences were used for data analysis.
Results: Both total serum cholesterol and LDL cholesterol as well as the level of triglycerides were decreased significantly in the group receiving phytoestrogens. On the other hand HDL cholesterol level showed a significant increase.
Conclusion: Phytoestrogen supplementation in postmenopausal women showed favorable metabolic effects on serum lipids. These effects could have the potential to reduce the risks of postmenopausal cardiovascular diseases in such women.
PS-237
TREATING HOT FLUSHES IN MENOPAUSE WOMEN WITH VITA GNUS (HERBAL MEDICINE)
F. Yari, S. Vahabi, A. Khadish and A. Yari
Lores tan university of medical sciences, Khoramabad, IRAN
Objective: To compare effect of vita gnus with placebo for the treatment of hot flush in menopause women.
Design & Method: In this study, double-blind, placebo-controlled trial enrolled 100 healthy, postmenopausal women with hot flush signs. Participants randomly received vita gnus (oral drop) or placebo daily. Primary outcomes were change from baseline in average daily number of moderate-to-severe hot flushes and in daily hot flush severity score at weeks 4 and 12.
Results: In this study results showed vita gnus have a significantly greater reduction compared with placebo in average daily number of hot flushes at weeks 4 and 12 (P = .005). Average daily severity of hot flushes was significantly lower in the vita gnus group compared with placebo at week 12 (P = .005).
Conclusion: Vita gnus are an effective herbal treatment for Hot flush signs in postmenopausal women.
Metabolic syndrome and lipids
PS-238
ASSOCIATIONS BETWEEN THE METABOLIC SYNDROME AND BONE MINERAL DENSITY IN UKRAINIAN WOMEN IN POSTMENOPAUSAL PERIOD
V. Povoroznyuk1, L. Martynyuk2, N. Shved2, N. Dzerovych1, V. Vayda1 and L. Martyntyuk2
1Institute Of Gerontology AMS Of Ukraine, Kiev, Ukraine; 2I. Hobachevsky Ternopil state medical university, Ternopil, Ukraine
Objective: The metabolic syndrome (MS), which includes obesity, dyslipidemia, impaired glucose tolerance, and hypertension, is a major public health problem. The prevalence of MS among women in postmenopausal period is nearly 24%. In postmenopausal period the accelerated bone loss, contributing to the development of osteoporosis begins. Obesity or increased body mass index (BMI) is known to have a protective effect against osteoporosis. However, recent studies demonstrated that the MS can raise the risk of osteoporotic fractures. The purpose of our study was to reveal associations between components o f the MS and BMD in postmenopausal women.
Design & Method: The sample consisted of 47 postmenopausal women (age: mean = 62,1; S.D. = 1,2; duration of menopause: mean = 12,7; S.D. = 1,2). Women were considered to have the MS (according to IDF (2005 yr) criteria) if they had waist circumference >80 cm and two or more of the following abnormalities: hypertriglyceridemia ≥ 1,7 mmol/l; low high-density lipoprotein (HDL) cholesterol <1,29 mmol/l; high blood pressure ≥ 130/85 mm Hg or use of antihypertensive medication; high fasting glucose ≥ 5,6 mmol/l or use of antidiabetic medication (insulin or oral agents). Total body, lumbar spine, femoral neck, radius bone mineral density (BMD) measured by dual-energy X-ray absortiometry were compared for the cohorts with and without the MS. Other parameters including age, weight, height, waist circumference, the level of glucose, lipids were taken into account. Data were analyzed using Statistical Package 6.0 (Statsoft).
Results: Findings revealed that 28 (59,6%) of these postmenopausal women had MS. 18 (64,3%) of them had 3 components of MS, 8 (28,6%) had 4 components and 2 (7,1%) had all of them. In patients with and without MS compared, BMD was lower in the former group at lumber spine (1,01 ± 0,03 and 1,17 ± 0,04, respectively; F = 10,2; p = 0,002), femoral neck (0,83 ± 0,02; 0,97 ± 0,03, respectively; F = 14,6; p = 0,0004), radius (0,59 ± 0,02; 0,69 ± 0,02, respectively; F = 13,1; p = 0,0008), total body (1,03 ± 0,02; 1,16 ± 0,02, respectively; F = 20,5; p = 0,00005). Increasing quantity of the MS components in women during the postmenopausal period had a negative correlation with BMD at every site. Frequency of osteoporosis (according to WHO (2004 yr) recommendations).was higher at all sites except femoral neck in patients with MS.
Conclusion: Development of MS in postmenopausal women increases the risk for the negative changes in BMD (such as osteopenia and osteoporosis). Furthermore, postmenopausal women need observation to prevent the development osteoporotic fractures.
PS-239
ANDROGEN LEVELS ARE ASSOCIATED WITH CENTRAL ADIPOSITY AND INSULIN RESISTANCE IN POST-MENOPAUSAL WOMEN: A MENOPAUSAL STATUS POPULATION-BASED STUDY
K. Oppermann1,2, S. C. Fuchs3 and P. M. Spritzer3,4
1School of Medicine, University of Passo Fundo, Passo Fundo, RS, Brazil; 2Hospital São Vicente de Paulo, Passo Fundo, RS, Brazil; 3Institute of Health Basic Sciences and School of Medicine, Universidade Federal do Rio Grande do Sul, Porto Alegre, RS, Brazil; 4Hospital de Clínicas de Porto Alegre, RS, Brazil
Objectives: There is evidence that androgens play a role in the metabolism of glucose and insulin resistance, and they might mediate some of the cardiovascular consequences of insulin resistance. The aim of this study was to determine whether androgen levels and menopausal status are associated with central adiposity and insulin resistance in pre-, menopausal transition and post-menopausal women.
Design & Method: This study is part of a longitudinal population-based study of menopausal status, including a representative sample of 358 women and conducted in the city of Passo Fundo, in Southern Brazil. The cross-sectional data for this analysis were collected in 2001–2002. Sixty-six women, aged 39 to 58 years old and not receiving drugs known to interfere with hormonal levels were included in the present analyses. Menopausal status was categorized as pre for those with no change in menstrual frequency or flow; menopausal transition for those who had these changes, and post-menopausal was diagnosed after 12 months of amenorrhea or bilateral oophorectomy. Body mass index and waist circumference were determined and waist circumference ≥ 80 cm was adopted to indicate central adiposity. Blood pressure was measured in mm Hg. Total testosterone, SHBG, fasting glucose and insulin, triglycerides, total and HDL-cholesterol were determined. LDL-cholesterol, homeostasis model assessment (HOMA) index and free androgen index were calculated. Statistical analysis was performed considering menopausal status and stratifying waist circumference according to the cutoff of 80 cm.
Results: Waist circumference, total cholesterol, triglycerides, HOMA and total testosterone were significantly higher in menopausal transition and post–menopausal women in comparison to pre-menopausal women (p < 0.05). Women with waist circumference >80 cm showed higher age, body mass index, glucose, HOMA and free androgen index than those with waist circumference ≤ 80 cm. In a model of linear regression, waist circumference was independently and significantly associated to body mass index, free androgen index and post-menopause status, but not menopause transition.
Conclusion: Endogenous androgen levels are associated with central adiposity, insulin resistance and postmenopausal status.
PS-240
BODY COMPOSITION, BODY WEIGHT, ABDOMINAL CIRCUNFERENCE AND HORMONAL THERAPY IN POSTMENOPAUSAL WOMEN
J. R. Sakon, Z. S. Alves, C. S. S. Oliveira, L. C. Stella and D. P. Pardini
Federal University of São Paulo, Brazil
Objective: This study was conducted to determine the association between hormonal replacement therapy in postmenopausal women and body composition, body weigth and insulin resistance.
Design & Method: Participants were 18 postmenopausal women aged 48 to 53 years old. Body mass index (BMI), abdominal circunference (AC), age at menopause and years since menopause were recorded. Body fat distribuition and the ratio of trunk fat (TF) to leg fat (LF) mass was determined by dual energy x-ray absorptiometry (DEXA) using a Lunar DPX in basal conditions and after six mouths of hormonal therapy (HT) with a combination of estradiol (1mg/day) with trimegestrone (0,125mg/day) in 10 women, 8 women taking placebo. Lean and adipose tissue weight and abdominal fat weigth were determined from the DEXA total body scans. Estradiol, insulin levels,cholesterol total and fractions, triglycerides and glicose tolerance test (GTT) also were performed before and after HT.Insulin resistance was performed before HT by Homeostasis Model Assessment (HOMA). There were no diferrences in basal body weigth or body fat distribuition in the two groups before the study. All results are reported as the mean ± SE. Statistical analysis of the results was performed by paired Student's t test to compare the variables in the two groups before and after treatment.
Results: There was a reduction measures in AC and the BMI, decreased serum levels of total cholesterol, insulin and glucose in the treated group compared to baseline but no statistical significance. LDL colesterol fraction decrease from 126 ± 9,1 to 108.8 ± 12 (p < 0,001) after HT. Trunk fat decreased after HT (10640 ± 1400 to 10150 ± 1500) (p < 0.05). Although the total fat has not declined as well total lean increased in the group taking HT, both parameters, did not reach statistical significance. In the placebo group results were opposed to treated group but when compared with each other also did not reach statistical significance. The test of tolerance to glucose and the calculation of HOMA showed 2% of the insulin resistance without diabetes at baseline conditions and 1.8% after reposition treatment Similar results was found in the placebo group.
Conclusion: Our results show a tendency to weigth loss, decrease in total and trunk fat mass and AC after hormone therapy. This tendency did not attain statistic difference, except in trunk fat and LDL colesterol, probaly in decorrency of the small number of patientes studied. The results suggest that HT can counteract at least in part the postmenopausal increase in body weight and body fat and prevent central body fat distribution after menopause.
PS-241
DISTURBANCES IN GLYCEMIC AND LIPID METABOLISM IN DIABETIC WOMEN ON MENOPAUSE WITH OR WITHOUT HORMONAL THERAPY
Iuliana Ceausu1,2, Al. Ciulcu2 and D. Hudita1,2
1“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania; 2“Dr. I. Cantacuzino” Hospital, Bucharest, Romania
Objective: The aim of this study was to assess the effects of oral and transdermal hormonal treatment (HT) in a group of women with diabetes mellitus type II (DM) on menopause compared with nondiabetic patients.
Design and Methods: In the period 2000–2005, 225 cases were divided, in 3 groups: 97 women without HT (11 DM), 70 women on menopause with oral HT (12 DM) and 68 women with transdermal HT (8 DM). The follow-up was realized for two years. The descriptive data were socio-demographic, BMI, dietary habits, alcohol consumption, smoking, menopause symptoms before and after HT, with or without HT. Laboratory tests were assessed every 6 months combined with a physical exam. HT was represented by estradiol, orally or transdermal with dydrogesteron - 12 days per month. Mammography and Pipelle endometrial biopsy were performed yearly in the groups with HT. Statistical data were obtained by SPSS 15. Hysterectomized women and DM type I was excluded.
Results: Menopause symptoms were similar for DM and nonDM patients, but in DM patients the urogenital problems were significant higher. The age at menopause was statistically lower, 43.2 in DM vs 54.7 years nonDM. In TH groups the BMI decreased, significantly for transdermal HT in the DM vs control group. Trigliceridemia was also decreased significantly in DM group treated with transdermal therapy, and the results were present at 6 month of therapy and were maintained till the end of the 2 years follow up. HDL-Cholesterol increased at 6 month of treatment in the transdermal group, mostly for the DM patients, significantly different from the oral and control group. LDL Cholesterol and total-Cholesterol levels were lower in HT patients, for both types of HT, without any differences between DM and non DM. Glycemia levels decreased under HT in DM patients, and during the follow-up no patient with DM under HT changed on insulin therapy. In nonDM patients transdermal therapy increased glycemia and oral HT decreased it, both no statistical significantly. QoL questionnaire revealed significant improvement under HT for DM and nonDM, achieved in 6 month, and maintained during follow-up.
Conclusions: HT has positive effects on lipid and glycemic metabolism, more on DM patients then in nonDM. Transdermal HT had more beneficial effects in DM. The key point of the good results of HT in DM and nonDM in menopause are strict controlled indications, a good follow-up and individualization of the dose in HT.
PS-242
EFFECT OF CONTINUOUS COMBINED HRT ON LIPID LEVELS IN POSTMENOPAUSAL WOMEN WITH DIABETES TYPE 2 AND HYPERLIPIDEMIA
T. Beljic Zivkovic1, M. Vuksanovic1 and S. Popovic2
1Zvezdara University Medical Center, Belgrade, Serbia; 2Clinical Center of Serbia
Objective: Hormone replacement therapy (HRT) is known to decrease lipid levels in healthy postmenopausal women. Women with diabetes type 2 frequently have lipid abnormalites. However, they rarely accept HRT, except when climacteric symptoms are present, in fear of cardiovascular events. The aim of this study was to assess the effect of oral HRT on lipid levels and glucose metabolism in postmenopausal women with type 2 diabetes and hyperlipidemia.
Design & Method: Continuously combined, estradiol (E2) 2mg + norethisterone acetate (NETA) 1mg was given to 90 postmenopausal women with vasomotor symptoms: 30 women with diabetes type 2 and hyperlipidemia, 30 women with hyperlipidemia and 30 healthy women over a 6 month period. Total holesterol (t-HOL), triglycerides (TG), LDL-cholesterol, HDL-cholesterol, fasting insulin and glycated haemoglobin A1c were evaluated in 3 months intervals. Fasting and postprandial (2 hours after breakfast) glucose were evaluated monthly.
Results: HRT significantly decreased levels of t-HOL (χ2Friedman = 11,712; p < 0,01) and LDL-c (χ2Friedman = 10,403; p < 0,01) in postmenopausal women with type 2 diabetes. The effect was more pronaunced in women with hyperlipidemia and healthy women without lipid abnormalitis. TG and HDL-c did not change in postmenopausal women with type 2 diabetes (χ2Friedman TG = 5,400; p≥0,05)(χ2Friedman HDL-c = 1,113; p>0,05). Six months of oral HRT significantly decreased HbA1c (F = 44,693; p < 0,01). There was no differences in the fastng insulin (χ2 Friedman = 1,267; p>0,05) and fasting and postprandial glucose levels (χ2Friedman = 6,527; p>0,05).
Conclusion: Besides being effective in treating vasomotor symptoms, six months of HRT can significantly lower lipid levels and HbA1c in postmenopausal women with type 2 diabetes.
PS-243
EFFECT OF OBESITY AND AGE ON SERUM ANDROGEN LEVELS IN ESTROGEN-TREATED AND UNTREATED POSTMENOPAUSAL WOMEN
F. Z. Stanczyk, R. Karim, P. Sánchez, W. Mack and H. Hodis
University of Southern California Keck School of Medicine, Los Angeles, California, USA
Objective: We have previously shown that obesity, but not age, had a significant impact on serum estrogen and SHBG concentrations in postmenopausal women using and not using estrogen therapy (ET). Although androgens have an important physiologic effect in postmenopausal women, there is a paucity of data on the effect of obesity and age on circulating androgen levels in this population. The aim of the present study was to determine the effect of obesity, both central and overall, on serum levels of relevant androgens in estradiol-treated and untreated postmenopausal women.
Design and Method: A total of 180 postmenopausal women participating in the Estrogen in the Prevention of Atherosclerosis Trial (EPAT) were studied. Ninety-one of the women ingested micronized 17β-estradiol and 89 ingested a placebo daily for 2 years. Obesity was measured by BMI and waist-hip ratio (WHR). Blood samples were obtained at baseline and every 6 months thereafter, which were subsequently used to measure serum levels of total testosterone, androstenedione and DHEA by validated extraction/chromatographic RIAs; free testosterone was calculated.
Results: Among ET users, there was no significant difference in androgen levels with respect to age, BMI or WHR. Only a borderline significant reduction in DHEA levels with increasing age was observed among ET users. Among non-ET users (placebo group), there was a significant reduction in DHEA and androstenedione levels with increasing age. Also, free testosterone levels were significantly higher in the women with higher BMI or WHR.
Conclusions: (1) ET reverses the age-related decline in circulating androstenedione levels in postmenopausal women. (2) ET also decreases FT levels, particularly in women with higher BMI and WHR, which may help reduce adverse cardiovascular effects related to higher FT levels.
PS-244
EFFECT ON SERUM LIPID PROFILES OF ESTROGEN REPLACEMENT THERAPY IN KOREAN MENOPAUSAL WOMEN
Y. Cho and C. Kim
National Health Insurance Corporation Ilsan Hospital, Kyonggido, Korea
Object: To evaluate the effect of estrogen replacement therapy on serum lipid profile in healthy Korean menopausal women during the first one year.
Design: Retrospective study, review the medical records.
Setting: Out patient clinic of NHIC Ilsan hospital.
Patient(s): 36 women were selected among the 364 women. Who has no experience of estrogen replacement therapy and healthy menopausal women aged 38 to 59 years.
Intervention(s): Sequential combination of 2mg estradiol valerate from day 1 to 28 and 1mg cyroterone acetate from day 15 to 28 (Climen).
Main outcome measure(s): Serum total cholesterol, triglyceride, high-density and low density lipoprotein (HDL and LDL) cholesterol at baseline and I years of treatment.
Result(s): The serum level of total cholesterol showed significant decrease between baseline and 12 months treatment (209.14 ± 44.54 mg/dl(mean ± S.D.), 180.89 ± 37.79 mg/dl, P<.001). Triglyceride was not changed significantly (123.31 ± 94.67 mg/dl, 127.27 ± 60.06 mg/dl, P = .785), HDL was not changed significantly (60.76 ± 18.61 mg/dl, 60.10 ± 16.53 mg/dl, P = .815). LDL was statistically significant decreased after treatment (138.43 ± 38.48 mg/dl, 108.19 ± 36.85 mg/dl, p = .001).
Conclusion(s): The serum level of total cholesterol and LDL cholesterol were statistically significant decrease after 12 months estrogen replacement therapy in Korean menopausal women.
PS-245
EFFECTS OF LONG TERM HORMONE REPLACEMENT THERAPY CESSATION ON THE METABOLIC RISK FACTORS: PREMATURE OVARIAN FAILURE VS. NATURAL MENOPAUSE
S. Vujovic, M. Stojanovic, M. Ivovic, M. Tancic-Gajic, L. J. Marina, M. Barac and M. Drezgic
Institute of Endocrinology, Clinical center of Serbia, Beograd, SERBIA
When and why do we have to stop hormone replacement therapy (HRT)? Are there any differences in HRT duration between women with premature ovarian failure (POF) and natural menopause? Powerful statistics can prove anything. Huge numbers are impressive but very often false. Only clinical follow up studies with individualization of HRT can answer many questions.
Objectives: to find out changes of metabolic risk factors after three months cessation of 10 years HRT.
Design & Methods: Group I natural menopause, 40 women, 52.7 ± 0.9 years, BMI = 23.4 ± 2.4 kg/m2. Group II POF, 40 women, 45.3 ± 2.3 years, BMI = 24.4 ± 3.5 kg/m2, both groups on HRT 10 years. Group III controls: 40 hormone non-users, 54.1 ± 4.2 years, BMI = 25.6 ± 2.1 kg/m2, last menstruation 9.2 ± 2.2 years before. All women were otherwise healthy, not using statins. Blood samples for metabolic risk factors (glycaemia, cholesterol, HDL,LDL,tryglycerides, ApoA,ApoB,Lp(a), fibrinogen, insulin were taken at 8am once a year for 10 years. year of HRT and after 3 months cessation. Waist/hip ratio was measured and ambulatory blood pressure monitoring (24h) was done at the same time. Statistics: Friedman ANOVA and Kendall coefficient of concordance.
Results: BMI, cholesterol, LDL, fibrinogen, HOMA index, blood pressure (p = 0.03) were higher in controls than in HRT users. After only three months of HRT cessation, all parameters showed increment tendencies, especially LDL in the group I (p = 0.01). No difference was found between group I & II. Nobody from HRT users had metabolic syndrome, myocardial infarction, sudden death, hypertension or hyperlipidaemia.
Conclusion: Potent anabolic effects of HRT protect against metabolic syndrome (inflammatory disease), atherosclerosis and cardiovascular diseases. Only 3 months cessation deteriorates these effects. Women's age is not crucial for HRT cessation. Continuation of appropriate individual dosage of HRT (according to receptor sensitivity) has a key role in achieving better quality of long healthy life.
PS-246
EFFECTS OF REPRODUCTIVE CHARACTERISTICS AND HORMONE THERAPY ON METABOLIC RISK FACTORS IN KOREAN WOMEN
S. M. Kim1,3, J. R. Lee1, B. C. Jee1, C. S. Suh1,2, Y. M. Choi1, J. G. Kim1, S. Y. Moon1,2 and S. H. Kim1,2
1Seoul National University College of Medicine, Seoul, Korea; 2Institute of Reproductive Medicine and Population, Medical Research Center, Seoul National University, Seoul, Korea; 3Seoul National University Hospital Health Care System Kangnam Center, Seoul, Korea
Objective: To assess the prevalence of metabolic syndrome (METS) in Korean pre- and postmenopausal women and to investigate the effect of reproductive characteristics such as age at menarche, reproductive years, years since menopause and hormonal treatment (HT) status on body composition and METS risk factors in Korean women.
Design & Method: A cross sectional study was performed on a cohort of 771 premenopausal (mean age 44.4 ± 2.7), and 569 postmenopausal (mean age 58.4 ± 6.4) Korean women who visited Seoul National University Kangnam Center for routine health check-up from July to December 2007. Surgically menopaused women were excluded. All postmenopausal women had experienced a natural menopause more than a year. The use of medication including HT, antidiabetic and antihypertensive agents, age of menarche, age of menopause, and last period were recorded using a structured questionnaire.
Serum levels of lipids: total cholesterol (t-chol), triglyceride (TG), HDL-cholesterol, insulin and glucose were measured after at least 10-hour fasting. Body weights, heights and waist circumferences (WC) were measured and body mass indexes (BMI) were calculated. One-way ANOVA, linear logistic regression analysis using SPSS version 12.0 were used for the statistical analysis, as appropriate. METS was defined using the NCEP APT III guidelines.
Results: The prevalence of METS was 5.4% and 19.3% in pre- and post-menopausal women respectively. Subjects were divided into three subgroups: early menarche (EM: age 10–12), intermediate menarche (IM: age 13–16) and late menarche (LM: age 17–19), according to the lower and higher 10th percentile of the age at menarche in the study population. In premenopausal women, WC, BMI, t-chol, and fasting insulin levels were higher in EM group. In postmenopausal women t-chol was lower in LM group than the other groups (200 vs. 207.5 and 216.7 mg/dL, p = 0.36 and 0.22). Postmenopausal women were divided into never user (n = 397, 69.8%), prior user (n = 126, 22.1%, mean duration of treatment 3.68 years) and current user group (n = 46, 8.1%, mean duration of treatment 5.2 years) according to HT status. Fasting glucose was significantly higher in never user than current user group even after correction of the aging effect (97.5 vs. 90.9 mg/dL, p = 0.01). There was no difference in body composition or METS risk factors according to HT status.
Conclusion: This study indicates that early menarche is associated with higher body fat composition and possibly insulin resistance in premenopausal women. And late menarche is associated with lower t-chol level in both pre- and postmenopausal women. HT seems to be beneficial in glucose metabolism. However the association of those with METS is not evident in this study.
PS-247
INCIDENCE OF METABOLIC SYNDROME AFTER TEN YEARS OF TREATMENT
A. M. Fernández1, J. L. Cuadros1, A. M. Cuadros, F. J. González2, R. M. Sabatel1, O. R. González1, I. M. Fernández and J. D. Luna3
1HU San Cecilio, Granada, Spain; 2H Costa del Sol, granada, Spain; 3Universidad de Granada, Spain
Objective: The menopause is associated with greater cardiovascular risk due to an increase in atheronal factors. The prevalence of metabolic syndrome increases in the menopause and triplicates the risk of cardiovascular diseases. For this reason, it's very important to value the prevalence of metabolic syndrome with different standards of THS after ten years of treatment. We will evaluate the influence of age in this behaviour.
Material and Methods: We studied 641 patients who began and continued THS for ten years (252 patients). We evaluated the prevalence of metabolic syndrome at the beginning of the treatment and after 1, 5 and 10 years. We took the definition of metabolic syndrome as being NEP-ATP III, but we changed abdominal fat for BMI > 30 kg2/m. According to the standard of THR, we created four groups: A tibolone; B estradiol daily (TTS 50) and medroxyprogesterone (10mg)/progesterone (200mg) (12–25 per month); C estradiol daily (TTS 50 and medroxyprogesterone (2,5mg)/progesterone (100mg) daily; D estradiol daily (TTS 50).
Results: The prevalence of metabolic syndrome is shown in Table 1. We didn't find any difference between standards of treatment. If we evaluated the treatment time, only the tenth visit was clinically significant, with an increase of 1.58 times more risk, CI (1.19–2.08).
If we controlled the age, the risk decreased every year. These results are shown in Table 2.
Conclusion. The probability of metabolic syndrome with all standards of treatment is the same. Besides, the prevalence of metabolic syndrome increases every year; if we vary by age, this prevalence decreases.
Table 1 Prevalence of metabolic syndrome
Table 2 Probability of metabolic syndrome varied by age
PS-248
METABOLIC SYNDROME IN PRE-/POST-MENOPAUSAL THAI WOMEN AT SIRIRAJ MENOPAUSE CLINIC
M. Rattanachaiyanont, S. Indhavivadhana, P. Leerasiri, P. Tanmahasamut, K. Techatraisak, S. Angsuwathana and T. Wongwananurak
Department of Obstetrics and Gynecology, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand
Objective: To determine prevalence of metabolic syndrome (MS) and its associating factors in pre-/post-menopause Thai women at Siriraj Menopause Clinic.
Design & Methods: A retrospective study was conducted in pre-/post-menopause Thai women who attended Siriraj Menopause Clinic from January 1999 to January 2008. Medical records were reviewed and the patients who had adequate data to evaluate MS according to the International Diabetes Federation (IDF) 2005 criteria were included.
Results: During the 10 years of study period, 488 eligible women, 43–73 years old, were identified. MS was found in 59 women rendering a prevalence (95% confidence interval, CI) of 12.1% (9.3 to 15.3%). Patients with or without MS were comparable in socioeconomic status, physical activities, and family history of cardiovascular disease. In premenopausal women, the prevalence of MS did not significantly vary with menstrual pattern (regular cycle, irregular cycle, or amenorrhea). In postmenopausal women, the prevalence of MS was higher in the surgical menopause group than in the natural menopause group (OR, 95% CI = 1.9, 1.0 to 3.5). The prevalence of MS tended to increase with age, especially after 60 years old, however, the number did not reach statistical significance. Comparing to the patients without MS, those with MS had higher body mass index (27.3 ± 3.2 vs. 23.3 ± 3.0 kg/m2, P = 0.000), more abnormal uterine bleeding (OR, 95% CI = 7.6, 1.5 to 38.6), and less exposure to hormonal contraception (OR, 95% CI = 0.3, 0.1 to 0.8).
Conclusions: According to the IDF 2005 criteria, approximately 12% of pre-/post-menopausal Thai women have MS. The associating factors of MS include surgical menopause, high body mass index, abnormal uterine bleeding, and non-exposure to hormonal contraception.
PS-249
METABOLIC SYNDROME IN WOMEN AFTER MENOPAUSE IN A CLOSED BRAZILIAN POPULATION
S. M. R. R. Lima1, B. F. Reis1,2, S. Saito1, S. Botogoski1 and T. Aoki1
1School of Medical Sciences of Santa Casa de São Paulo, São Paulo, Brazil; 2Vale do Sapucai University, Pouso Alegre, Minas Gerais, Brazil
Introduction: The metabolic syndrome (MS) is a complex disorder with a high prevalence, represented by a set of cardiovascular risk factors responsible for the increase in mortality. With the advent of menopause, the risk of cardiovascular events and death are higher for women compared to men.
Objective: To assess the prevalence of MS in women after menopause living in a small rural Brazilian municipality, with a fixed population of women and compare with the data in the literature.
Method: It is an observational, cross-sectional study in the small town of Congonhal in the state of Minas Gerais, whose economic activity is based on agriculture, 9,747 inhabitants (IBGE Census - 2005), of whom 4,716 are female, 654 of these women are in the period of the climacteric, and 117 after menopause. They were accompanied at the Gynaecology clinic in the Basic Health Unit for the period of March 2006 to March 2007. The MS was defined by the National Cholesterol Education Program - Adult Treatment Panel III.
Results: The average age of women was 56.5 ± 5.5 years. The age of menopause was 48 ± 4.4 years and the time elapsed after menopause was 8.5 ± 6.8 years. The cardiovascular risk factors were: Total cholesterol 217.7 ± 39 mg/dL, HDL-c 51.8 ± 12 mg/dL, LDL-c 33.4 ± 28.7 mg/dL, VLDL-c 159.7 ± 68.1 mg/dL, fasting blood glucose of 103.4 + 38.7 mg/dL, abdominal circumference 94.3 ± 10.1 cm, systolic blood pressure 136 ± 19.4 mmHg and diastolic blood pressure 82.1 ± 12.3 mmHg. 27.4% of the participants were classified as carriers of MS. When we compared our results with those of the international literature and the findings were consistent: 10.7 to 40.5% are affected by the MS (Gami AS, 2007). In this period were 17 deaths: 6 by cardiovascular disease (35.3%), 3 by pneumonia (17.6%), 3 by neoplasms (17.6%), 2 of Chronic obstructive pulmonary disease (11.7%), 2 by malnutrition (11.7%) and 1 by hepatic failure (5.9%).
Conclusion: The municipality of Congonhal, despite being composed of rural people with high levels of activity, showed a prevalence of metabolic syndrome similar to the world population and mortality by cardiovascular disease. This fact makes us question the behavior, eating habits and genetic inheritance of these women. This small town of a stable population without migration can be a representative sample for future studies.
PS-250
ORAL AND TRANSDERMAL ESTROGEN REPLACEMENT THERAPY SIGNIFICANTLY DECREASES CONCENTRATION OF RLP-CHOLESTEROL
Tomas Fait1 and Michal Vrablik2
1General Faculty Hospital Prague; 21st Faculty of Medicine Charles University Prague
Objective: Remnant lipoprotein particles (RLP) in plasma play an important role in atherogenesis. Estrogen replacement therapy (ERT) influences levels of RLPs. The impact of different routes of ERT administration (oral vs. transdermal) on RLP concentrations has yet not been studied. Therefore we performed a randomized, cross-over study comparing 2mg of 17-beta estradiol administered orally and 50ug of estradiol in a transdermal route.
Material and Methods: 45 hysterectomized women (age 49 ± 6 years) were randomly assigned to one of the treatments. After 3 months there was a week wash-out period and then the second type of ERT was administered for another 3 months. 41 participants completed the study.
Concentration of RLP-cholesterol (RLP-C) was assessed by immunoseparation at the baseline and at the end of each treatment period. Paired t-test was used for statistical analysis.
Results: Compared to the baseline the concentration of RLP-C decreased significantly after both the oral and transdermal ERT (0.38 ± 0.24 mmol/l, p = 0.003, 0.48 ± 0.35 mmo/l, p = 0.01; baseline 0.6 ± 0.43 mmol/l). There was no difference between the two ways of ERT administration.
Conclusions: Both oral and transdermal ERT significantly decrease concentrations of RLP-C with similar magnitude. This effect is another potentially antiatherogenic property of estrogens in case of early start of ERT.
PS-251
“PREVALENCE OF METABOLIC SYNDROME IN POSTMENOPAUSAL WOMEN USER AND NONUSER OF HORMONE REPLACEMENT THERAPY”
C. G. Arruda, L. M. Pompei, R. Strufaldi; E. P. Cunha, S. Peixoto and C. E. Fernandes
ABC School of Medicine – SP, Department of Gynecologic, Brazil
Objective: This study was conduced to assess the prevalence of metabolic syndrome (MS) in women user and nonuser of hormone replacement therapy (HRT).
Design & Method: In this cross sectional study, 317 subjects in post-menopausal women (182 users of HRT and 135 nonusers of HRT) were analyzed from October to December 2007, in the academic medical center. We evaluated the effect of HRT on components of the MS, following to the ATP III (Adult Treatment Panel III) criteria.
Results: The mean ages, menopause age and menopause time, of users and nonusers HRT, were 52.9 ± 5.4, 46.9 ± 5.4 and 5.9 ± 5.2 years respectively.
The relative frequencies of metabolic syndrome in the two groups were: nonusers HRT = 29,6% and users HRT = 19,2% (p = 0,031).
The most frequent marker of the MS was increased waist circumference (p = 0,042).
Among the groups, no significant changes in these parameters occurred: HDL-cholesterol, glucose, triglycerides, systolic blood pressure, diastolic blood pressure and body mass index.
Conclusion: It is concluded that the frequency of MS is significantly higher in post-menopausal women that nonuser HRT as compared to post-menopausal women that user HRT and abdominal obesity was the most frequent feature observed. The components of metabolic syndrome are risk factors to cardiovascular disease and need to be controlled.
PS-252
RELATION OF HIGH SENSITIVITY C-REACTIVE PROTEIN WITH METABOLIC SYNDROME IN HEALTHY MENOPAUSAL WOMEN
Un Suk Jung, Min Sun Kyung, Joong Sub Choi, Kye Hyun Kim, Kyo Won Lee and Jong Sul Han
Department of Obstetrics and Gynecology, Kangbuk Samsung Hospital; Sungkyunkwan University School of Medicine, Seoul, Korea
Objective: In recent years, some studies have shown that metabolic syndrome (MetS) is associated with inflammation, indicated by high-sensitivity C-reactive protein (hs-CRP). But most cross-sectional studies of hs-CRP and the MetS have undertaken sex-adjusted analysis or have been performed in single-sex cohorts. Otherwise, considering the fact that hs-CRP levels area increased after menopause, it remains unclear whether hs-CRP is associated with MetS in menopausal women, especially in Korea. In this study, we investigated the association between hs-CRP and MetS in Korean menopausal women.
Design & Method: We conducted a cross-sectional study of 2729 patients (age ≥ 60) who participated in annual health examiniations at Kangbuk Samsumg Hospital between Januray 1st 2005 and December 31st 2006. Exclusion criteria included hypertension, diabetes, obesity secondary to hypothyrodism or Cushing's disease, severe debilitating diseases, and cancer. Women with a history of current or previous use of estrogen replacement were also excluded from this study.
Result: Women with MetS and abnormalities in its individual components showed higher hs-CRP level than those without such abnormalities. All components of MetS had a correlation with hs-CRP after adjustment for age, smoking status, alcohol status and exercise status. After adjusting various known risk factors, the odds ratios (95% CI) of quartiles of hs-CRP for MetS were 1.0, 1.92 (1.38–2.67), 2.68 (1.92–3.75), and 3.65 (2.62–5.09). A linear relationship between the increase in number of components of Mets and hs-CRP levels was observed (p value for linear trend<0.05).
Conclusion: The level of hs-CRP is strongly associated with MetS and its components in healthy postmenopausal women.
PS-253
SHBG AND LIPOPROTEIN: EVALUATION AFTER TEN YEARS OF HRT
J. L. Cuadros1, A. M. Fernández1, A. M. Cuadros, F. J. González2, R. M Sabatel1, O. R. González1 and I. M. Fernández
1HU San Cecilio, Granada, Spain; 2H Costa del Sol, Granada, Spain
Objective: We evaluated the relationship between SHBG and lipoprotein (Cholesterol and HDL) with different standards of HRT after ten years of treatment.
Material and Methods: We studied 474 patients who began and continued HRT for ten years (167 patients). We evaluated the mean of SHBG and lipoprotein (cholesterol and HDL) at the begining of the treatment and after 1,5 and 10 years. According to the standard of HRT, we created four groups: A Tibolone; B estradiol daily (TTS 50) and medroxyprogesterone (10mg)/ progesterone (200mg)(12–25 per month); C estradiol daily (TTS 50) and medroxyprogesterone (2,5mg)/ progesterone (100mg) daily; D estradiol daily (TTS 50).
Results: We evaluated HDL, LDL, TG, VLDL and cholesterol and only we found a relationship between SHBG and estradiol in the patients that used estradiol or/and medroxyprogesterone/progesterone. This effect was not found with the tibolone. SHBG increased with the use of HRT except with tibolone, which decreased (Table 1). This SHBG increment correlated significantly (p < 0.005) with the increase of HDL, except for tibolone. Tibolone had a significant decrease.
Table 1
Conclusions: The use of HRT in this study produced an increase of SHBG which correlated with an increase of HDL. This event was not produced with Tibolone.
PS-254
THE EFFECTS OF ESTROGEN REPLACEMENT THERAPY ON SERUM LIPID PROFILE IN SURGICALLY MENOPAUSED WOMEN
Kyu Sup Lee1, Sung Tack Oh2, Young Min Choi3, Hwi Gon Kim1 and Jung Wan Jung4
1Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602-739; 2Obstetrics and Gynecology, Chonnam National University, Kwangju, Republic of Korea, 501-757; 3Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602–739 and 4Obstetrics and Gynecology, Miraero Hospital, Busan, Republic of Korea, 616-820
Objectives: To evaluate short-term and long-term effects of estrogen replacement therapy (ERT) on lipid profile in surgically menopaused women.
Methods: In this cross-sectional study, 120 surgically menopaused women after total hysterectomy and bilateral oophorectomy and 107 natural postmenopausal women were enrolled. After surgical menopause, 28 women received 0.625 mg conjugated equine estrogen (CEE) and 32 women did not for 3 months, 28 women received and 32 women were did not for 1 year. Natural postmenopausal women received 0.625 mg conjugated equine estrogen (CEE) and 5 mg medroxyprogesterone acetate (MPA). The effects of Hormone therapy on plasma levels of lipids were investigated. Wilcoxon signed rank was performed on the results obtained before and after administration of drugs between each group. The differences were considered statistically significant at P < 0.05.
Results: During hormone therapy, total cholesterol and LDL cholesterol level decreased significantly for 3 months and 1 year in surgically menopaused women (p < 0.05). HDL cholesterol level raised at 3 months but there was not significant statistical difference (p>0.05). Triglyceride level decreased in surgically menopaused women not received ERT but there was no significant statistical difference (p>0.05).
Conclusion: The results of our study results suggest that ERT had more beneficial effects on lipid profile in surgically menopaused women.
PS-255
THE PRODUCTION OF LEPTIN IS ASSOCIATED WITH THE RATIO OF ESTROGEN RECEPTOR SUBTYPTES ALPHA AND BETA IN 3T3-L1 ADIPOCYTES
K. W. Yi1, J.-H. Shin1, T. Kim1, Y. T. Lim2, S. H. Kim1 and J.-Y. Hur1
1Korea University School of Medicine, Seoul, Korea; 2Catholic University School of Medicine, Seoul, Korea
Objective: To evaluate the role of estrogen receptor subtypes alpha (ERα) and beta (ERβ) in the regulation of leptin expression in 3T3-L1 adipocytes.
Design & Method: In vitro, mouse 3T3-L1 fibroblasts were grown and fully differentiated into mature adipocytes. We treated each 3T3-L1 adipocyte with estradiol (E2), ERα agonist (PPT), ERβ agonist (DPN), E2 with ERα antagonist (MPP), and E2 with ERβ antagonist (R,R-THC) at different concentrations. To clarify the expression and regulation of adipokines by ER subtypes (ERα and ERβ), the total RNA was extracted from cells and measured using quantitative real-time reverse transcription-polymerase chain reaction (real-time RT-PCR). Western blot analysis was performed to evaluate the protein expression of leptin, ERα and ERβ.
Results: Treatment with only E2 at several concentrations did not affect leptin mRNA expression in 3T3-L1 adipocytes. In the PPT treated cells, the leptin mRNA levels increased significantly in accordance with the PPT dose (P < 0.05). By contrast, the leptin mRNA levels decreased in a dose dependent manner in the MPP treated group (P < 0.05). Treatment with high concentration (10–5M) of R,R-THC with E2 (10–7M), caused a significant increase in the leptin mRNA levels (P < 0.01). The leptin mRNA levels showed a positive correlation with the expressed ERα mRNA level (r = 0.584, P < 0.01) and a negative correlation with the expressed ERβ mRNA level (r = −0.236, P = 0.03) in the adipocytes. The ratio of the ERα and ERβ levels (ERα/ERβ) in adipocytes showed a significant correlation with leptin mRNA levels (r = 0.454, P < 0.01).
Conclusion: The results of this study showed that ERα induces in leptin expression, and ERβ inhibits its expression in 3T3-L1adipocytes. The ratio of ERα and ERβ expression, in adipocytes is strongly associated with leptin expression.
PS-256
TWO YEARS OF LIPID PROFILE MONITORING ON TRANSDERMAL ESTROGENS AND VAGINAL MICRONISED PROGESTERONE COMPARED TO ORAL ROUTE OF HORMONE THERAPY IN HEALTHY POSTMENOPAUSAL WOMEN
Manuela Russu, Ş. Nastasia, N. Mubarak, J. A. Marin and D. Hudiţă
“Carol Davila” University of Medicine & Pharmacy, Bucharest; “Dr. I. Cantacuzino” Department of Obstetrics, Gynecology
Objective: Lipid profile assessment and clinical registration of cardiovascular events after transdermal estrogens and vaginal micronized progesterone administration vs oral hormone therapy (HT), and control in the first 5 years of menopause in healthy women.
Material and Methods: From January 1, 2002- December 31, 2003, total -, LDL-, HDL-cholesterol, and triglycerides of 50 postmenopausal women were analyzed after 6, 12, 24 months on 5 types of sequential HT [different routes for estrogens- oral/transdermal, and progestogen/progesterone - oral/vaginal, duration of progestogen/progesterone - 12/14 days/month and 14 days cycle at 3 months] and 10 postmenopausal controls, who refused HT. Total cholesterol <200 mg/dl, LDL-c <130 mg/dl, HDL-c >65 mg/dl, triglycerides <150 mg/dl appreciated as protective for atherosclerosis.
Statistical analysis: each non-oral(NO) group compared to oral(O) and control groups, by pair Student's test (ANOVA). Differences between treatments and control were considered significant at P values <0.05.
Results: After 6 months: increased total cholesterol: 7 (3NO + 4O) (14%) treated, 4 (40%) controls; reduced total cholesterol: 18(11NO + 7O) (36%) treated, 1(10%)control; HDL-c in normal range: 12 (8NO + 4O) (2.4%) treated, no control; HDL-c of 50–64 mg/dl: 34 (20NO + 14O) (68%) studied, 8(80%) controls; HDL-c <50 mg/dl: 4(2NO + 2O) (8%) studied, 2(20%) controls; triglycerides >150 mg/dl: 10(2NO + 8O)(20%) treated, 6(60%) controls. After 12 months of HT: total cholesterol >200 mg/dl: 5(3NO + 2O)(10%) treated, 4(40%) controls; increased LDL-cholesterol: 4(3NO + 1O) (8%) treated, 8(80%) controls; high triglycerides: 10(2NO + 8O)(20%) studied, 6(60%) controls. There was a registered reduction of: total cholesterol (with 12%, 15–18%, and 18% at 6, 12, 24 months), LDL-c (with 20%, 25% at 6, 12 months, unchanged values at 24 months) in all treated groups, triglycerides (only with transdermal estrogens: with 14%, 15% at 6, 12 months, unchanged values at 24 months), an increase of HDL-c (by 8–10%, 14–18% at 6, 12, 24 months, best values after 24 months being on micronized progesterone vaginal route monthly vs control, and cycle administered at 3 months vs oral progestogen/dydrogesteron). There was no cardiovascular event registration during all the examined period.
Conclusions. Lipid profile was most positively influenced after the first 12 months, with less change after 24 months; oral estrogens induced a slight rise of triglycerides; vaginally administered estrogens monthly and cycle at 3 months associated micronized progesterone induced the most antiatherogenic levels (P<0.05). Medroxyprogesterone acetate had the worst effect ever associated to transdermal estrogen.
The estrogen production decrease in menopause induces:
the increase of lipoprotein (a) and LDL-cholesterol, triglyderides
an accentuate the increase of the risk of morbidity and mortality
from cardiovascular diseases (Kramarow E et al, 1989, PEPI trial, 1995; Peterson L, 1998).
It is very well known that the effects on lipoprotein metabolism depend on the type of molecule, dose, route of administration of estrogen and as well on type, time, route of administration of progestin/progesterone used for endometrium protection.
Estrogen oral administration reduces most significant LDL-c, increases HDL-c (Nachtigall LE, et al, 1979) and tryglicerides, influences endothelial function, increases C reactive protein (Cushman M, et al, 1999).
Transdermal estrogens increase HDL-c, reduce LDL-c in a less degree, have no effect on triglycerides (Crook D, et al 1992), but their effects appear after longer duration of use (Jamin C, 1990), do not influence hemostatic factors (Oger E, Scarabin PY, 2003).
progestins used in combined HRT regimens may diminish the cardioprotective effect of estrogen replacemen.
Progestins tend to increase LDL-c and lower HDL-c concentrations.
Opposite to the situation of inducing cardiovascular complications sometimes vital when atherosclerosis is present even if lipid profile is favorable changed (Hodis NH, et al, 2003, for WELL-HART.
Aging women and male
PS-257
AGE, AEROBIC FITNESS AND DIET INFLUENCE ON OXIDATIVE STRESS DAMAGE IN POST MENOPAUSAL WOMEN
M. P. Mota1, J. Soares1, J. C. Leitão1, S. Fonseca1, T. Bento3, P. A. Figueiredo2, J. A. Duarte2 and M. H. Moreira1
1Universidade de Trás-os-Montes e Alto Douro, Vila Real, Portugal; 2Faculdade de Desporto da Universidade do Porto, Vila Real, Portugal; 3Escola Superior de Rio Maior, Portugal
Objective: Aging process is associated with an increase in oxidative stress that contributes to the pathology of atherosclerosis and other cardiovascular diseases. It has also been pointed out that hypercaloric diets may also increase these damage levels. On the other hand, physical exercise and a high-antioxidant diet consumption seem to exert a protective effect on cardiovascular system improving the scavenge of free radical species. This might became particularly important when considering post-menopausal women, which have their estrogen levels decreased, and so their potent antioxidant effect. Bearing this in mind, the main aim of this study was to analyze the relative contribution of age, aerobic fitness and diet to serum lipid peroxidation levels in post-menopausal women.
Design & Method: The sample included 61 post-menopausal women Caucasian (age, 58,94 ± 7,34 years old) without hormonal replacement therapy. Aerobic fitness (VO2max · ml · kg-1.min-1) was assessed by spirometry according to an adaptation of Bruce protocol. Calories, protein, carbohydrates, fat and antioxidants intake in diet (vitamin E, vitamin, C, vitamin B and selenium) was assessed through food frequency questionnaire, validated in adult Portuguese population. Serum lipid peroxidation levels (MDA concentration, ng · L−1) were determined by spectrophotometric method. Linear regression analysis, method steptwise, was used to assess the relative contribution of age, aerobic fitness and antioxidant intake in diet to MDA concentration. P-value less than 0.05 was considered significant.
Results: The mean values to VO2máx was 28.24 (±6.23) ml · kg-1.min-1, 2063.99 calories (±499.75), 91,93 (±23.83) mg protein, 272.49 (±82.88) mg carbohydrates, 70,23 (±20.83) mg fat, 208.65 (±71.39) antioxidants vitamin intake and 102.80 (±35.05) μg selenium. Stepwise analysis revealed that age is the only predictor variable (R = .259, F = 4.538, p < .05), explaining 6.7% of MDA variance.
Conclusion: Our data suggests that aging process explains in part the increase in serum lipid peroxidation levels in post menopausal women. Although literature advocate that exercise and diet may reduce oxidative stress damage, in what concerns to lipid peroxidation our data couldn't confirm these statements.
PS-258
EVALUATION OF BLOOD PRESSURE CONTROLLED BY AGE AND MENOPAUSE TIME AFTER TEN YEARS OF THS
A. M. Fernández1, J. L. Cuadros1, A. M. Cuadros, F. J. González2, R. M. Sabatel1, O. R. González1, I. M. Fernández and J. D. Luna3
1HU San Cecilio, Granada, Spain; 2H Costa del Sol, granada, Spain; 3Universidad de Granada, Spain
Objective: We compared blood pressure with different standards of THS after ten years of treatment. We evaluated if age and menopause time influenced our results.
Material and Methods: We studied 641 patients who began and continued THS for ten years(252 patients). We evaluated the mean at the beginning of the treatment and after 1,5 and 10 years. According to the standard of THR, we created four groups: A tibololne; B estradiol daily (TTS 50) and medroxyprogesterone (10mg)/progesterone (200 mg) (12-25 per month); C estradiol daily (TTS 50 and medroxyprogesterone (2,5mg)/progesterone (100 mg) daily; D estradiol daily (TTS 50).
Results: If we evaluated systolic blood pressure, the values of A standard are less than C standard (p = 0.014). Besides, systolic blood pressure decreased with all standards until the fifth year (p = 0.07) and it increased thereafter until the tenth year, but these results aren't significant. If we evaluated the influence of age and menopause time, the results were the same.
On the other hand, diastolic blood pressure decreased until the sixth month (p = 0.005), the fifth year (p = 0.1608) and the tenth year (p = 0.1455). If we evaluated the influence of age, the results were the same. However, if we evaluated the influence of menopause time, the decrease after ten years was significant (p = 00.0376).
Conclusion: The use of THS in this study produced a decrease in blood pressure until the fifth year of treatment. Therefore we found a insignificant increase in systolic blood pressure and a significant decrease in diastolic blood pressure. Besides, Tibolone had less value than the other standards. The menopause time at the beginning of THS influenced this behaviour.
PS-259
EVALUATION OF FALL RISKS IN THE AGED POPULATION OF A PUBLIC HOSPITAL IN BRASILIA, BRAZIL
M. P. S. Campos, L. Gomes, A. Bueno Tavares, M. V. S. Campos and A. R. Campos
Catholic University Of Brasilia, Brazil
Objective: The life expectancy increase and consequence aged population growth have generated changes in the morbility and mortality profiles, implying prevalence increased of chronic-degenerative illnesses and the appearance of events that can have ominous consequences as the falls. The objective of this study was to evaluate the risk of falls in the aged population, identifying the possible involved factors.
Design & Method: Transversal study with 155 patients, 60 years or more, 131 women and 24 men, was carried out from April to November 2007 in the fisiotherapic and geriatric ambulatories of a public hospital in Brasilia, Federal District. It was applied a questionnaire for identification of the risk factors and two tests to evaluate the balance (1. Functional Reach; 2. To raise and to walk chronometered). In the statistical analysis, for evaluation of the categorical variable had been used the Qui-square and Fisher tests. Models of Logistic Regression had been used to calculate odds ratio and value of corresponding p. The Curve Receiver Operating Characteristic (ROC) was used to evaluate the balance tests as falls predictors. The Correlation of Pearson verified the correlation between the number of falls, the age and the balance tests.
Results: Significantly higher incidence of falls was identified in: 1. the aged woman; 2. in that they had told to fear falls; 3. in that using polipharmacy (4 or more medicines). The balance tests had not shown to be good predictors of falls.
Conclusion: The identification of the three factors significantly related with falls is of great importance, making possible educational and preventive strategies for independence and health maintenance of the aging individuals.
PS-260
FALLS PREVALENCY AND INTRINSIC RISK FACTORS IN AGED WOMEN LIVING IN THE COMMUNITY, BRASILIA, BRAZIL
J. Gai, L. Gomes and O. T. Nóbrega
Catholic University Of Brasília, Brazil
Objective: The objective of the present research was to determine the falls prevalence and the intrinsic risk factors related in aged women living in the community.
Design & Method: 112 aged women had been analyzed, from 61 to 81 years, consulted in the Catholic University of Brasilia Hospital (UCB) in the Project “Health Promotion of the Aging”. The enclosed intrinsic risk factors criteria had been: illness or neurological sequel, osteo-muscle-articulation illness difficulting the daily life activities, dementia, blindness or serious visual deficiency, ramble difficulty and cardiac insufficiency. The patients were asked about the number of falls suffered during the last year. The present project received the approval of the Ethics Committee in Research of the HUCB. It was applied statistical study.
Results: 28 individuals present falls risk factors. The risk factors had been: osteoarthritis (8); breaking sequel (5); diabetic neuropathy (4), fibromialgic disease (3) cerebral vascular accident sequel (2); unspecific ocular illnesses (2); unspecific deambulation difficulty (2); medullar traumatic injury (1); skull-encephalic trauma sequel (1); heel “esporão” (1); mental confusion (1); orthopedic surgery sequel (1); blindness (1); varicosis ulcers (1); etilic encephalopathy (1); unspecific tremors in the members (1); painfull halux valgus (1); infectious mielitis (1) and cardiac insufficiency (1). 8 aged individuals presented two or more associated illnesses. 13 (46,54%) of the risk factors carriers had fallen in the last year, with one to five falls. Between the individuals not carrying risk factors, 46 (54,76%) had fallen, with one to four falls. There was no significant statistical difference between this results in the two groups.
Conclusion: The number of falls through a year was great in all the population studied, independent of the presence of fall risk factors. This points to the necessity of preventive falls intervention for the aging women.
PS-261
OPEN PLACEBO-CONTROLLED STUDY THE EFFICACY OF PHENIBUTUM (NOOPHEN) IN COMPLEX TREATMENT CHRONIC NECK PAIN AND MENOPAUSAL SYMPTOMS IN THE WOMEN IN EARLY POSTMENOPAUSAL PERIOD
V. Povoroznyuk, T. Orlik and E. Dudko
Institute Of Gerontology AMS Ukraine
The aim of this research was to study the efficiency of phenibutum (Noophen®) in complex treatment of chronic neck pain and menopausal symptoms in the women in early postmenopausal period. Object. It was examined 30 postmenopausal women with chronic neck pain, which took Noophen on 1 tablet (250 mg) 2 times per day during 30 days (I group). Second (II) group (n = 20) accepted Noophen-placebo on the same circuit. Both groups were similar as regards age, duration of menopause and age at menopause (p>0.05). Methods. We used X-ray method, questionnaires and studied the evaluation of pronouncement of the pain syndrome, psycho-emotional displacements, distinctness of climacteric syndrome, definition of jet and individual alarm, state of vegetative nervous system, biological age. The inspections were carried out in the beginning of treatment, on 15 and 30 days from a beginning of treatment. Results. It was shown the reduction the intensity of the headache and decreases the neck pain and menopausal symptoms, parameters of jet uneasiness in Noophen group (Table 1). In placebo group of significant changes not got, but only the tendency to reduction of jet and individual alarm, intensity of pain syndrome and climacteric symptoms.
Table 1
Conclusion: Noophen® is effective in complex treatment chronic neck pain in early postmenopausal women. It decreases the intensity of pain syndrome, improves the physical condition of the patients, and promotes the increasing the quality of life, delay of processes of the accelerated ageing.
PS-262
PERIMENOPAUSAL AMENORRHEA – A RARE CASE
Raquel Robalo, Filipa Ribeiro and Luís F. Vicente
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Background: Gestational trophoblastic disease (GTD) comprises a heterogeneous group of interrelated lesions arising from the trophoblastic epithelium of the placenta. The two main risk factors for GTD are extremes of maternal age and a history of previous GTD.
Case: We describe a 52 year's old woman with three months of amenorrhea after two years of irregular vaginal bleeding and a recent history of hyperthyroidism and hypertension. Clinical evaluation detected an enlarged uterus, ultrasound evaluation reported an enlarged endometrial thickness and histological results revealed a complete hydatiform mole.
Discussion: The authors remark that irregular vaginal bleeding characteristic of the perimenopause period may mask important pathologies and reinforce the importance of contraception in the perimenopause.
PS-263
PREVALENCE OF GIDDINESS AND ITS RELATION WITH FALLS IN AGED WOMEN LIVING IN THE BRASILIA COMMUNITY, BRAZIL
Juliana Gai, Lucy Germano Bouzada and Otavio Toledo Nóbrega
Catholic University Of Brasília, Brazil
Objective: The objective of this research was to determine the prevalence of giddiness and its correlation with occurrence of falls in independent aged women living in the community.
Design & Method: 84 aged women living in the community had been evaluated. They were consulted in the Catholic University of Brasilia Hospital (HUCB) in the Project “Health Promotion of the Aging”. They had been interrogated about giddiness symptoms and number of falls occurred through the last year. Falls occurring inside mobile vehicles and caused for landslide in smooth surface had not been considered. This work had approval of the “Ethics Committee in Research” of the HUCB.
Results: 44 women (52,38%) presented giddiness. 21 (47,72%) women had unspecific sensation of giddiness following corporal disequilibrium, sensation of empty head and space disorientation. 23 (52,27%) presented rotatory character typical of the vertigo. Between these, 23,8 (34,78%) presented this symptom when moving in places as street, supermarket and shopping, preventing since them these places; 12 (52,17%) presented this symptom during changes of body position; 2 (8,69%) related not to get bending down to catch objects in the soil, dress pants and stockings, and to roll in the bed, without presenting this symptom, them also preventing these tasks; and 1 (4,34%) women told buzzed associated. In the group with giddiness, 27 (61,36%) had falls in the last year, been the number of episodes varied from 1 to 4. In the group without giddiness, 16 (40%) had fallen, been the number of falls varied from 1 to 3.
Conclusion: The giddiness symptom was frequent in the studied population, being related to difficulties in the accomplishment of the day-by-day tasks as to sleep, to dress and to move in the community, as well as with auto-restriction. The number of falls was high and the women who presented giddiness had suffered greater number of falls.
PS-264
WOMEN'S PERSPECTIVE AND THE SOCIOCULTURAL CONTEXT OF MENOPAUSE IN CUKUROVA
Y. Incecik, E. Akpinar, L. Toksoz, E. Saatci, N. Bozdemir, S. Ozcan and H. Kurdak
University of Cukurova, Adana, Turkey
Objective: Menopause represents the end of a woman's reproductive life and is commonly associated with midlife and aging, both of which have cultural implications in all societies. The aim of the our study was to explore the menopausal sociocultural experiences of women and perception of menopause, living in Cukurova region of Turkey.
Design & Method: Data were gathered through semistructured interviews with 44 women all aged 43 years at baseline who did not have a menstruation at least for one year. During interviews a questionnaire was used including items about demographic characteristics of participants, perception of menopause, partners attitudes toward menopause and social aspects of menopause were investigated and analyzed using the Statistical Package for the Social Sciences.
Results: A total of 44 women aged 53.61 ± 5.8 (min.43, max.66) years old and did not have a menstruation at least for one year (88,6% had more than one year) enrolled in our study. All of the women were married and have active sexual life, 65,9% had more than three children and most of them had core family type (77.3%). Twenty five percent of the women lived in rural areas and 75% lived in urban areas. The average age at menopause of the women in the present study was 46.54 years. 63.6% of them never had any menopause consultation before. 18.2% of women were illiterate, 4.5% can read and write and 36.4% had elementary school education. Most of the women (72.7%) who participated in our study mentioned that at this stage of their lives, sociocultural response of others does not change. They said, ‘whatever I did I still do it’ and ‘life continues as usual’. Most of the women mentioned that even though their social status does not change, their health status changes and they feel worst (29.5%) and fair (52.3%). However, most of the partners feel that this period is worst ever (76%).
Conclusion: The results suggest that cultural factors, partners attitudes toward menopause may influence the experience of menopausal women. Uncomfortable feelings and some symptoms that accompany the end of the menstrual period might have a different meaning due to changes on women's lives in a transitional culture. These findings may improve health professionals' understanding of cultural beliefs relating to menopause so that culturally appropriate care can be provided.
Bone
PS-265
A COMPARISON OF EFFECTS TO THE BONE BY ORAL RISEDRONATE FOR POSTMENOPAUSAL OSTEOPOROSIS VARIED THE TIME TAKING MEDICINE
T. Higuchi, A. Tarakida, K. Abe, R. Taniguchi and H. Mizunuma
Hirosaki University School of Medicine, Hirosaki City, Japan
Objective: The aim of this study is to compare the effects to the bone for one year between taking daily resedronate orally at morning fasting time and other time feeling hungry in postmenopausal osteoporosis.
Design & Method: The 27 postmenopausal women diagnosed primary osteoporosis were randomly divided into two groups with their informed consent described as below, one is taking oral resedronate (2.5 mg/day) at morning fasting time (group A, n = 14) and another at any time feeling hungry (group B, n = 13). For one year treatment, we assessed lumbar bone mineral density (L-BMD) using dual X-ray absorptiometry (DXA) at base line and one year after. We also examined bone metabolic parametes described as below, bone type alkaliphosphatase (BAP), serum N-terminal telopeptide of bone collagen (S-NTx) and urine N-terminal telopeptide (U-NTx) at base line, 1, 3, 6, 9, 12 months later. All data were compared between both groups.
Results: At the baseline profiles, there was no significance between both group. L-BMD was increased in both group for one year treatment. Comparing bone parameters chronologically, BAP was decreased from 3 months and S-NTx and U-NTx also decreased from one month later significantly in the group A. In the group B, BAP was decreased from 6 months and U-NTx from 3 months later significantly.
Conclusion: The similar effects to bone metabolism by oral risedronate were observed at sixth month from baseline and L-BMD also increased at one year later in both groups. It was suggested that varying the time of taking risedronate may be one of the choice for long term treatment of osteoporosis.
PS-266
A OPEN-LABEL, RANDOMIZED, MUTICENTER STUDY TO EVALUATE THE EFFICACY AND TOLERABILITY BETWEEN THE COMBINATION THERAPY GROUP OF ALENDRONATE SODIUM AND HORMONE AND HORMONE REPLACEMENT THERAPY GROUP IN THE TREATMENT OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN: KOREAN FOSAMAX ESTROGEN COMBINAITON TRIAL
B. K. Yoon1, H. M. Park2, S. H. Cho3, M. C. Park4 and Y. M. Choi5
1Sungkyunkwan University, Seoul, Korea; 2Chung-Ang University, Seoul, Korea; 3Hanyang University, Seoul, Korea; 4Hallym University, Seoul, Korea; 5Seoul National University, Seoul, Korea
Objective: To evaluate the clinical efficacy and tolerability between the combination therapy of alendronate and hormone replacement therapy (HRT) vs. HRT alone in Korean postmenopausal women with low bone mineral density (BMD).
Design & Method: An open-label, randomized, multicenter study was conducted in postmenopausal women with T- score<−2.0 at lumbar spine or femur neck measured by dual-energy X-ray absorptiometry. Patients with secondary osteoporosis or a history of HRT or any other osteoporososis treatment one yr prior to study were excluded. HRT (conjugated equine estrogen, 0.625 mg/d plus medroxyprogesterone acetate, 2.5 mg/d) alone or in combination with alendronate (10 mg/d) was administered for one yr. Calcium (ironic calcium 400–500 mg/d) was also supplemented if tolerable. BMD and bone turnover markers such as osteocalcin and deoxypyridinoline were checked periodically. Data were analysed using t-test, chi-square test, repeated-measure analysis of variance, etc., and two-tailed p < 0.05 was considered statistically significant.
Results: Among 344 subjects recruited, 203 completed the study (combined therapy: 104, HRT alone: 99). Age (mean ± SD) and body mass index at baseline were comparable between two groups (61.8 ± 7.2 vs. 60.5 ± 6.2 yr, 23.2 ± 3.1 vs. 23.7 ± 2.9 Kg/m2). Baseline measurements of BMDs and turnover markers were also not different. BMDs at spine and hip were significantly increased in both groups. However, percent change in lumbar BMD with combination therapy (7.90 ± 6.21) was not significantly different from that with HRT (6.92 ± 7.24). BMD changes at femur neck or total hip were comparable between groups. With respect to bone turnover, both markers were significantly declined with each treatment and reduction was greater in combination group than in HRT group. Rates of drop-out and adverse experiences were alike between groups.
Conclusion: Combination therapy of alendronate and HRT in postmenopausal women with low BMD was similar to HRT in BMD increase and tolerability, but superior to HRT in reduction of bone turnover markers. Further study is warranted to test fracture prevention effect.
PS-267
ASSESSMENT OF SERUM CARTILAGE MARKERS IN POSTMENOPAUSAL WOMEN WITH HORMONE THERAPY OR BISPHOSPHONATE
ByungSeok Lee1, SiHyun Cho1, KiHyun Park1, ChanHo Song1, HyoungMoo Park2, JinYong Lee3, Hoon Choi4 and HongKyoon Lee5
1Yonsei University College of Medicine1, Seoul, Korea; 2Chung-Ang University College of Medicine, Seoul, Korea; 3Eulji University College of Medicine, Daejun, Korea; 4Inje University College of Medicine, Seoul, Korea; 5H Cube Clinic, Seoul, Korea
Objectives: To evaluate whether treatment with hormone therapy or bisphosphonate affects the levels of cartilage turnover marker (serum cartilage oligomeric matrix protein, COMP).
Design & Methods: Blood samples were taken from 83 postmenopausal women after informed consents for assessment of serum cartilage oligomeric matrix protein (COMP). All were within 1 year from the diagnosis of menopause. These patients were divided into hormone therapy, bisphosphonate, or control groups according to the treatment they received. Samples were taken before the initiation of medication, after 3 and 6 months. Known bone markers such as serum osteocalcin and urine deoxypyridinoline were evaluated at the same time. COMP levels were assessed using a commercial ELISA kit (COMP Elisa, Human, Kamiya Biochemical Company, USA). Paired t-test, independent t-test and Pearson correlation were used for statistical analysis and p value less than 0.05 was considered statistically significant.
Results: 33 with typical postmenopausal symptoms received hormone therapy (HT group), either standard or low dose continuous combined regimen and 28 without severe hot flushes, but with osteoporosis or osteopenia received alendronate sodium 70mg weekly regimen (BPN group). 22 patients received no medication (control group). The mean age, BMI, initial COMP levels and initial urine deoxypyridinoline levels were not significantly different between 3 groups. The mean COMP levels at 0, 3, and 6 months in the control group increased. (32.91 ± 14.3 ug/mL, 37.01 ± 17.95 ug/mL, 37.55 ± 17.39 ug/mL, p < 0.05) In BPN group, mean COMP levels at 0, 3 and 6 months were 25.57 ± 12.82,25.64 ± 12.8, and 23.22 ± 10.01. Marginal decrease between 3 and 6 months (p = 0.051). In HT group, COMP levels tended to increase at 3 months and decrease at 6 months (mean values 26.82 ± 12.67, 29.58 ± 9.93, 25.83 ± 11.62), but with no statistical significance. Bone markers were all suppressed significantly at 3 and 6 months in HT and BPN groups, but not in control group. There existed weak correlations between COMP and bone markers. (r = 0.221 between COMP and UDP, r = 0.216 between COMP and osteocalcin) Between BPN and HT, the degree of COMP suppression didn't differ significantly.
Conclusions: Bisphophosnate marginally suppressed the excretion of cartilage marker in the treated patients and hormone therapy tends to increase the cartilage marker initially, but might lower in a long run according to this study. These results indicate that either treatment with bisphosphonate or hormone decrease cartilage turnover.
PS-268
ASSOCIATION BETWEEN BODY MASS INDEX, ABDOMINAL PERIMETER AND OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN
A. Esparza, G. Soro, B. García, B. Meneses and F. Baró
Vall d'Hebrón University Hospital, Barcelona, Spain
Objective: To show the association between body mass index, abdominal perimeter and bone mineral density in postmenopausal women.
Design & Method: We performed an analytic and retrospective study in 224 postmenopausal women aged from 43 to 82 years (mean 63 ± 6). We obtained weight, height and abdominal perimeter during physical examination in outpatient clinic in our hospital. Blood levels of total cholesterol, low and high-density lipoproteins, homocysteine, lipoprotein (a) and C-reactive protein were determined by routine blood tests. Bone mineral density in lumbar spine and proximal femur was measured by dual-energy x-ray absorptiometry (DEXA) using LUNAR. Patients were categorized in three groups according to the WHO classification, values under 2.5 standard deviations were considered osteoporosis, between −1 and −2.5 standard deviations were considered osteopenia, and superior to −1 standard were considered normal. Statistic analysis between categories of bone density and means in abdominal perimeter and body mass index was performed by analysis of variances, using the software SPSS 13.0.
Results: In lumbar spine, distribution was 25%, 49.1% and 25.9% for normal, osteopenic and osteoporotic women, respectively. In femur the frequencies were 25.4%, 60.3% and 14.3%. Means of abdominal perimeter were 96.1 cm, 91.0 cm and 89.2 cm respectively in the previously mentioned groups. Means of the body mass index were 30.0 kg/m2, 27.4 kg/m2 and 26.5 kg/m2 in the same groups. Analysis of variances showed a correlation between bone mineral density in lumbar spine and body mass index (p-value 0.0002) and also between lumbar bone mineral density and abdominal perimeter (p-value 0.0003). The same results were obtained when analysing data from bone mineral density in femur for body mass index (p-value 0.0002) and abdominal perimeter (p-value 0.0008). In this series, there was no statistically significant association between bone mineral density with other known factors associated to both osteoporosis and obesity (cholesterol, low-density lipoproteins, high-density lipoproteins, homocysteine, lipoprotein (a), C-reactive protein).
Conclusion: Body mass index is in tight relation with bone mineral density. Secondary hyperestrogenism has been suggested as the responsible mechanism. Obviously, overweight is not advisable way of improving bone density, as it can lead to other comorbidities. On the other hand, women with low body mass index are at increased risk of osteoporosis, and a normal weight is a goal in postmenopausal women management. Anyway, as the percentage of osteoporosis is high in the general postmenopausal women, we recommend that even obese patients should be screened for osteoporosis.
PS-269
ASSOSIATION BETWEEN ARTHRITIS AND PHYSICAL ACTIVITY LIMITATION IN INDIVIDUALS OVER 50 YEARS OLD IN PURWOREJO DISTRICT, CENTRAL JAVA, INDONESIA
D. Dasuki1, J. L. Simbolon2 and M. Hakimi1
1Magister, Mother and Child Health, Reproductive Health, Gadjah Mada University, Yogyakarta, Indonesia; 2Midwifery Academy of Tarutung, North Sumatera
Objective: Arthritis, a condition dealing with pain or inflammation at joints, is a chronic disease in elderly life suffered by people over 60 years of age. It has more than 100 varieties and the commonest one is osteoarthritis. Age is one of the arthritis factors since the older someone is, the higher the possibility she is affected by arthritis. In Indonesia as the life expectancy rate is longer (67.8 in 2000–2005 becoming 73.6 in 2020–2025), the incidence of arthritis cases is higher as well. The increase of the elderly over 50 years of age in Indonesia especially in Purworejo District that was as many as 186.671 people (24.11%) in 2005 needs to get a special treatment and attention in order that they live happily at the old age. This study was undertaken to analyze the association between arthritis and the physical activity limitation for people over 50 years old in Purworejo District.
Design & Method: It was an observational study using cross-sectional design. The 13890 subjects were people over 50 years old. The data were collected by conducting interview with questionnaire from Study of Global Ageing and Adult Health (SAGE),WHO and INDEPTH by 63 interviewers and 7 field coordinators. The analyses used were univariable, bivariable with chi-square and multivariable with logistic regression test and the significance level (p) was <0.05 and confidence interval (Cl) was 95%.
Results: There was a significant correlation between individuals with arthritis and physical activity limitation OR 1.7 (95%CI = 1.51–1.87), p = 0.00. Individuals with arthritis would have a higher risk of physical activity limitation than those without arthritis history.
Conclusion: There was a significant correlation between individuals over 50 years of age with arthritis and physical activity limitation.
PS-270
ASSOCIATION BETWEEN LIPID PROFILE AND BONE MINERAL DENSITY IN POST-MENOPAUSAL WOMEN
J. Almeida, M. Rodrigues, P. Manso, S. Sousa, R. Passarinho, C. Silva, N. Pereira, R. Ribeiro; G. Castro, F. Geraldes, F. Aguas and F. Ventura
Maternidade Bissaya Barreto, Centro Hospitalar de Coimbra, Coimbra, Portugal
Objective: A number of recent findings seem to indicate that fat and bone metabolism are connected.
The purpose of the study is to investigate the potential association between serum lipid profile and bone mineral density (BMD) in post-menopausal women.
Design & Method: This was a retrospective study of 760 post-menopausal women that did Dual energy X-ray absorptiometry during the year 2002 in Maternidade Bissaya Barreto.
Exclusion Criteria: Post menopausal patients presenting risk factors for cardiovascular disease, with pathology that could interfere in the bone metabolism, or taking hormonal therapy hormone replacement therapy, in the present or in the past.
We evaluated total serum cholesterol and triglycerides levels and for each variable, the patients were divided in two groups: normal and anormal lipid profile and we compared bone mass by densitometry of the lumbar spine and femur in each group.
Data were analysed with the programme Statistical Package for the Social Sciences (SPSS). The chi-square and T student tests were used, when appropriate. A value of p < 0,05 was considered significant.
Results: One hundred and forty three women were included in the study.
There were no statistical differences between groups in what concerns demographic characteristics.
The comparation of groups according bone mineral density showed that there was no association between lipid profile variables and BMD values.
Conclusion: According to our study, lipid profile variables did not show a significant association with bone mass and could not be used as indicators for bone mineral density.
PS-271
ASSOCIATION BETWEEN POLYMORPHISMS IN TUMOR NECROSIS FACTOR (TNF) GENES AND CIRCULATING TNF LEVELS, AND BONE MINERAL DENSITY IN POSTMENOPAUSAL KOREAN WOMEN
Jung Gu Kim1, Hoon Kim1, Chang Suk Suh1, Seok Hyun Kim1, Young Min Choi1 and Jin Yong Lee2
1Seoul National University Hospital, Seoul, Korea; 2Eulji University Hospital, Seoul, Korea
Objective: To investigate the association between polymorphisms in tumor necrosis factor (TNF)-α, and TNF β genes and circulating TNF levels, and bone mineral density (BMD) in postmenopausal Korean women.
Design & Method: The TNF-α G(−308)A, C(−857)T, C(−863)A, T(−1031)C, and TNF-β A252G polymorphisms were analyzed by polymerase chain reaction-restriction fragment length polymorphism or Taqman assay in 377 postmenopausal Korean women. Levels of serum TNF- α, TNF-β, osteocalcin, bone alkaline phosphatase, and C-telopeptide of type I collagen were measured. BMD at the lumbar spine and femoral neck was examined by dual energy X-ray absorptiometry.
Results: No significant associations were found between single genotypes of TNF-α, or TNF-β polymorphism and BMD of proximal femur. The prevalence of osteoporosis is higher in TT genotype of TNF-α T (−1031) C polymorphism compared to other genotypes but lower in AA genotype of TNF-β A252G polymorphism. Haplotype analysis of 4 TNF-α polymorphisms did not show any significant association with BMD and the distributions of haplotype genotypes were not different among normal, osteopenic, and osteoporotic women. No significant differences in the levels of any biochemical marker among single and haplotype genotypes of these polymorphisms were found.
Conclusion: The TNF-α T(−1031)C, and TNF-β A252G polymorphisms are genetic factors which may evaluate Korean postmenopausal women at risk of osteoporosis.
PS-272
ASSOCIATION OF LRP5 GENE POLYMORPHISMS WITH BONE MINERAL DENSITY AND BONE RESPONSIVENESS TO HORMONE REPLACEMENT THERAPY IN POSTMENOPAUSAL KOREAN WOMEN
Kwon Dong Jin
St. Vincent's Hospital, Department of Obstetrics and Gynecology, College of Medicine, The Catholic University of Korea, Suwon, Korea
Objective: To evaluate the association of LRP5 gene polymorphisms with bone mineral density (BMD) and bone responsiveness to hormone replacement therapy (HRT) in postmenopausal Korean women.
Methods: The LRP5 gene polymorphisms were analyzed by restriction fragment length polymorphism (RFLP) in 229 postmenopausal Korean women receiving HRT for 1 year. The BMD before HRT was check using dual-energy x-ray absorptiometer (DEXA) at lumar spine, femur neck, Ward's triangle, and greater trochanter of femur, and women in the study were classificed into 3 gorup, normal, osteopenia and osteroporosis according to their BMD.
Results: The frequency of genotype C/C of C1677A was significanty high in osteoporosis group, and that of C/A was much low in osteoporosis group. The frequency of genotype T/C of T2268C was high in osteoporosis group, while that of C/C was low in the same group.
There was no significant relationship between LRP5 polymorphisms and BMD before HRT. In patients whose genotype was A/A of C3405G, C/C of T2268C, or C/C of T4037C had meaningful responsiveness to HRT at the lumbar spine, regardless of their initial BMD. The Genotype C/A of C1677A also had great responsiveness to HRT at the greater trochanter of femur in both osteopenia and osteoporis group.
Conclusions: The LRP5 gene polymorphisms were not associated with the BMD before HRT, but there were some reponsiveness to HRT at specific site according to genotypes of the gene.
PS-273
BONE MASS EVOLUTION IN MENOPAUSAL PATIENTS OVER 40 YEARS OLD TREATED WITH DIFFERENT HORMONAL REGIMES ALONG 8 YEARS
M. Lamarca Ballestero, J. Martinez Medel, O. Gil Lafuente, A. Miñano Navarro, A. Lanzón Laga and R. Lanzón Lacruz
Hospital Universitario Miguel Servet. Zaragoza, Spain
Objective: To evaluate the efficacy of 4 different hormonal treatment regimes in the bone mass evolution of menopausal women over 40 years old.
Design & Method: We performed a descriptive retrospective study of the bone mass evolution in 4 different treatment groups: tibolona, estradiol and hormone therapy replacement (HTR) in 2 different regimes (low and medium dose).
We studied the densitometric bone mass evolution tested biannually with a Lunar® dual photon absorptiometry (DEXA).
Results: 371 patients were included in the study: 183 in the tibolona group, 39 in the estradiol group and 149 in the HRT group (82 in the medium dosis group and 67 in the low dosis group).
The mean age at the end of the study for each group was 57,71 ± 6,68 years, 64,48 ± 1,83 years, and 53,85 (52 ± 6,41 years in the medium-dose group and 55,7 ± 7,43 in the low-dose group) respectively. The mean age of menopause was 48,40, 51,56, 44,93 and 46,52 years old respectively.
The bone mass increase after 8 years of treatment was 20,32%, 14,4% 9,92% (medium-dose) and 7,87% (low-dose group) respectively.
In all the cases the bone mass starts under the reference values for its age and persists below them at the end of the study. In all the cases the bone mass increase is stadistically significative.
Conclusion: The treatment of menopausal women over 40 years old with tibolona is associated with a higher bone mass increase than with other hormonal treatments.
In all the cases the bone mass was under the normal rate for its age.
PS-274
BONE MASS EVOLUTION IN MENOPAUSAL WOMEN UNDER 40 YEARS OLD TREATED WITH DIFFERENT HORMONAL REGIMES FOR 8 YEARS
O. Gil Lafuente, M. Lamarca Ballestero, J. Martinez Medel, A. Miñano Navarro, A. Lanzón Laga and R. Lanzón Lacruz
Hospital Universitario Miguel Servet, Zaragoza, Spain
Objective: To evaluate the efficacy of 3 different hormonal treatment regimens in the bone mass evolution of menopausal women under 40 years old.
Design & Method: We performed a descriptive retrospective study of the bone mass evolution in 3 different treatment groups: contraception, estradiol and hormone replacement therapy (HRT).
We focused our attention on the densitometric bone mass evolution tested biannually with a Lunar® dual photon absorptiometry (DEXA).
Results: 125 patients were included in the study: 97 in the A group (HRT), 10 in the B group (estradiol), and 18 in the C group (contraception). All the patients in the B group had no uterus and had surgical menopause. The remaining patients did have a uterus and had menopause caused by an early ovarian failure.
The mean age at the end of the study for each group was 34,8, 38,6 and 37,7 respectively. The mean age of menopause was 26,5, 31,9 and 28,9 respectively.
The bone mass which increased after 8 years of treatment was 23,96% (estradiol) and 12,63% (HRT) respectively.
In all cases, the bone mass started below the reference values for its age and persisted below these values at the end of the study. In all cases the bone mass increase was statistically significant.
Conclusion: The treatment of menopausal women under 40 years old with estradiol is associated with a higher bone mass increase than with other hormonal treatments.
In patients with uterus, HRT offers a better result than contraception.
In all cases the bone mass was under the normal rate for its age.
PS-275
BONE MINERAL DENSITY AND FRACTURE RISK
R. Passarinho, S. Sousa, P. Manso, J. Almeida, C. Silva, M. Rodrigues, M. G. Castro, R. Ribeiro, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Maternidade Bissaya-Barreto, Coimbra, Portugal
Objective: Fractures are the most important consequence of osteoporosis, accounting for the majority of cases of morbidity, mortality and costs associated with this disease. Bone mineral density (BMD) measurement is a widely available non-invasive mean of predicting fracture risk.
The main purpose of this work was to determine the relationship between BMD and fracture risk.
Design & Method: Retrospective study of 240 postmenopausal women, submitted to a lumbar spine and hip BMD measurement by dual X-ray absorptiometry (DXA) who never did hormonal replacement therapy or drug treatment known to affect bone metabolism. The following parameters were analysed: age, BMI, menarche, menopause, fertility years, personal and family history of fracture, type and age of fracture. WHO diagnostic criteria was used for osteoporosis based on t-score <−2,5, and SPSS 15,0 (Statistical Package for Scientific Science) for statistical calculations. Categorical variables were analysed using a chi-square test and the significance level was set at p < 0,05.
Results: In a subset of 240 women, a total of 42 had a personal history of fracture. The mean age of our universe was 57,3 years and for the fracture group were 60,6 years. The mean menopause age of the fracture group was 50,1 years and there were 19% of cases of family history of fracture. The fractures reported were vertebral (4,8%), hip fracture (11,9%), Colles fracture (14,3%) and other fractures (69%). A greater percentage of osteoporosis was found in women with fracture (p < 0,05), with a positive correlation for the typical types of osteoporotic fractures (vertebral, hip and Colles fractures) in the osteoporosis group (p < 0,05 at lumbar spine). Postmenopausal fractures were correlated with a lower t-score and a greater percentage of osteoporosis than fractures occurring in premenopause (p < 0,05).
Conclusion: These results suggest that BMD is an important risk factor for fractures. Treatment of osteoporosis and prevention of future osteoporotic fractures should be recommended.
PS-276
BONE MINERAL DENSITY IN HEALTHY POSTMENOPAUSAL WOMEN – EFFECTS OF HORMONAL AND NON-HORMONAL THERAPIES
C. Silva, M. Rodrigues, J. Almeida, P. Manso, R. Passarinho, S. Sousa, G. Castro, R. Ribeiro, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Maternidade Bissaya, Barreto, Coimbra, Portugal
Objectives: to compare the effects of hormonal and non-hormonal therapies in the Bone Mineral Density (BMD) of healthy postmenopausal women.
Design and Methods: Bone density was measured by dual energy X-ray absorptiometry (DXA) at lumbar spine and femoral neck. We selected all women that did DXA at our institution during one year. Of the universe of 772 women that was found the authors did a retrospective analysis of the files of the 151 postmenopausal women with abnormal BMD and without pathology that could interfere with bone metabolism (intestinal resection, thyroid disease, breast cancer, etc).
The women were sorted into two groups, those who have osteopenia and those who have osteoporosis; osteopenia was defined as BMD between 1,0–2,5 Standard Deviations (SD) below the mean of a young adult, and osteoporosis as BMD 2,5 SD below the mean of a young adult. For each group the demographic characteristics and therapies in use were summarized. We compared the value of BMD in two consecutive densitometries with a two year interval, considering the different therapies in use (hormone replacement therapy, bisphosphonates, selective estrogen receptors modulators, combination schemes, etc.). Statistical analysis was performed with the program Statistical Package for the Social Sciences (SPSS) 15.0; the chi-square and T student tests were used, when appropriate. A value of p < 0,05 was considered significant.
Results: We found significant statistical differences between the two groups in the following items: age at menarche, age at menopause and years since menopause (YSM).
The majority of women did hormone replacement therapy (HRT), bisphosphonates or a combination of these two (other combinations were used less frequently). In the group of women with osteopenia, there was a slight improvement in BMD in women doing some kind of therapy, but there was no significant statistical difference when we compared the therapies in use. In the group of women with osteoporosis, there was a greater improvement in BMD when bisphosphonates or bisphosphonates plus HRT were used, with statistical significance.
Conclusion: The results of the present analysis confirm the important role of YSM and years of fertility on the risk of osteoporosis. Estrogen deficiency is responsible for one-third to one-half of the bone loss during a woman's lifetime, which is consistent with the fact that HRT increases BMD. Evidence supports the bisphosphonates as first-line therapy for the treatment of osteoporosis and in our study this was the most effective therapy.
PS-277
BONE MINERAL DENSITY IN PATIENTS WITH OVARIAN CANCER
Chan Yong Park, Seung Ho Lee and Hong Ki Park
Gachon University Gil Medical Center, Incheon, South Korea
Objective: Ovarian cancer represents therapeutic challenge, and requires intensive & often complex surgery and chemotherapy which can reduce bone mass. Our purpose was to evaluate the bone mineral density (BMD) in patient with ovarian cancer before treatment.
Design & Method: We retrospectively analyzed the BMD of spine and femur measured by dual-energy X-ray absorptiometry (DEXA) in 46 patients with ovarian cancer and 70 control women. All patients with ovarian cancer and the control women experienced menopause. There were no bone metastases in patients with ovarian cancer. The control group was treated with surgery for benign disease. We compared age, height, body weight, body mass index (BMI) and BMD of spine and femur between the ovarian cancer and control, and compared BMD between early and advanced ovarian cancer.
Results: There were no differences in the BMD of spine and femur in patients with ovarian cancer and control group (Table 1). In patient with early and advanced ovarian cancer, we could not find differences in the BMD of spine and femur (Table 2).
Table 1 Comparison of BMD in patients with ovarian cancer and control group
Table 2 Comparison of BMD between early and advanced stage
Conclusion: Ovarian cancer appeared to have no effects on BMD before treatment. But, to define its detailed effect on BMD, prospective study with large sample size is needed.
PS-278
BONE MINERAL DENSITY IN UKRAINIAN WOMEN
V. Povoroznyuk, N. Dzerovych and T. Karasevskaya
Institute Of Gerontology AMS Ukraine, Ukrainian Scientific-Medical Centre For The Problems Of Osteoporosis
Objective: The aim of this study were: to determine spine, femoral and radial BMD for a representative sample of healthy women of Ukrainian female descent, to determine the effect of age, height and weight on BMD, and to compare these results with those from US/European reference sample.
Materials and Methods: The research was conducted at the Ukrainian Scientific-Medical Centre for the Problems of Osteoporosis, and included 353 women aged 20–79 years. Conventional BMD measurements of the spine (L1-L4 in the anterior-posterior position), proximal femur (neck, Ward's triangle and trochanter regions) and radial shaft (33% site) were determined by DXA using a densitometer Prodigy (GE Medical systems).
Results: Age-related changes in BMD were similar in form to those of US/European reference data. However, BMD of spine for subjects of 50–59 years in our sample were lower than published values. Regression analyses showed that weight was a significant predictor of female spine and femur BMD for both the premenopausal and postmenopausal decades. Age was a significant predictor of female spine BMD in the 50–79 year age. The prevalence of osteoporosis and osteopenia for female subjects was 11% at the femur neck, and 20% and 24% at the spine and radial shaft respectively. Substantially lower prevalence of osteoporosis of lumbar spine in Ukrainian population, based on the WHO criteria, was established in comparison with US/European reference values.
Conclusion: Thus, standardizing of BMD measurements by DXA through the appropriate use of population-specific reference values is recommended to improve the quality of medical care provided in relation to the prevention and treatment of female subjects who are at risk as for osteoporosis or are already osteoporosis.
PS-279
BONE MINERAL DENSITY IN WOMEN WITH AND WITHOUT HYSTERECTOMY AND OOPHORECTOMY – IS THERE ANY EFFECT?
M. Rodrigues, C. Silva, P. Manso, J. Almeida, S. Sousa, R. Passarinho, R. Ribeiro, G. Castro, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Maternidade Bissaya Barreto, Coimbra, Portugal
Objectives: Evaluate the bone mineral density (BMD) of postmenopausal women with previous hysterectomy with bilateral oophorectomy, compared to a group of naturally menopausal women. Analyse the effects of estrogen replacement therapy (ERT) on BMD in the group of women with hysterectomy and bilateral oophorectomy.
Materials and Methods: Retrospective analysis of the files of 614 postmenopausal patients with follow-up at Maternidade Bissaya Barreto (MBB). Those patients were divided in two groups: women who had hysterectomy and bilateral oophorectomy(n = 123), and those who didn't (n = 491). We excluded from our study women with pathology that could interfere in the bone metabolism (intestinal resection, thyroid disease, breast cancer, etc). Bone density was measured by dual energy X-ray absorptiometry (DXA) at lumbar spine and femoral neck; osteopenia was defined as BMD between 1,0–2,5 Standard Deviations (SD) below the mean of a young adult, and osteoporosis as BMD 2,5 SD below the mean of a young adult.
We performed data analysis with the programme Statistical Package for the Social Sciences (SPSS) version 15. The chi-square and T student tests were used, when appropriate. A value of p < 0, 05 was considered significant.
Results: There were no statistical differences between groups concerning to demographic characteristics, and the BMD and T-Score at the lumbar spine and femoral neck had no differences too. When we evaluated the effect of therapy with estrogen in the group of women who underwent hysterectomy with oophorectomy, we verified that T-score value and BMD were higher then in women who didn't do the therapy, with statistical significance.
Conclusions: There are no long term effects of hysterectomy and bilateral oophorectomy on bone mineral density. Women who use ERT have better BMD than nonusers.
PS-280
BLOOD VITAMIN D LEVELS IN MEXICAN OSTEOPOROTIC POSTMENOPAUSAL WOMEN WITH OR WITHOUT SUPPLEMENT ADMINISTRATION
José A. Hernández-Bueno1, Alejandro Vázquez-Alanís1, Esther Sánchez-Méndez1 and Sergio Sobrino-Cossío2
1Atención Médica Integral para la Mujer, SC, Naucalpan de Juárez, Estado de México, México; 2Instituto Nacional de Cancerología, México, D. F. México
Vitamin D is essential either for an adequate intestinal absorption of calcium and to prevent bone loss (due in part to a relative secondary hyperparathyroidism). In postmenopausal women there are predisposing factors to present inadequate levels of vitamin D, such as age, skin ageing and lack of vitamin D supplements. Blood levels of 25(OH) D below 30 ng/ml (75 nmol/l) sem. To correlate with deficient intestinal calcium absorption anda n increase (compensatory perhaps) of PTH.
Objective: To evaluate if blood 25(OH) D vitamin levels correlate with age in urban mexican osteoporotic postmenopausal women.
Material & Methods: From january to september, 2005 we performed a transverse, cross-sectional study (private practice) of consecutive cases of urban, middle-class postmenopausal women diagnosed with osteoporosis by central densitometry, according with the WHO criteria (metropolitan area, Mexico City). Informed conset was obtained before applying a validated questionaire for osteoporosis symptoms, as well for assesing the usual daily ingestión of calcium & vitamin D. Blood samples were drawn to meassure 25 (OH) Vitamin D levels, calcium, phosphorusand PTH. We excluded patients with hypothyiroidism, diabetes mellitus, chronic liver disease and known hyperparathyroidism.
We applied descriptive Statístics with means and SD, X2 for nominal variables, Students's t test, ANOVA and correlation coefficients.
Results: We included 46 osteoporotic postmenopausal women with mean age of 65.8 years (SD 7.7). 12 out of 13 (92.3%) younger than 60 years and 25/33 (75.7%) older than 60 years were taking Calcium & Vitamin D supplements. Mean blood 25(OH) Vitamin D levels was 31.2 (SD 12.6 ), Phosphorus 3.55 (SD 0.49 ), PTH 29.0 (SD 9.8) and calcium 9.41 (SD 0.85) ng/ml. In women older than 60 years, 25 (OH) Viamin levels were 33.65 (SD 14.9) taking supplements and 25.7 (SD 11.8) without it (ANOVA independent samples p = 0.0001).
There was no correlation between age and 25(OH)Vitamin D leves (X2 0.378, 1 GL, p = 0.53) (ANOVA 0.56, NS) (2 ways non-paired t test p = 0.56 95% CI −10.83–5.96).(R 0.038, p = −0.7, t = 0.25,DF 44, Y = 0.06).
Conclussion: We found no linear relationship between age and blood vitamin D levels. In patients older than 60 years, blood levels of vitamin D are different with statistical significance between those taking or not supplements.
PS-281
BODY COMPOSITION AND BONE MINERAL DENSITY IN MIDDLE AGED WOMEN
E. J. Kim1, I. S. Lee2, H. K. Lee3, J. E. Chung4 and M. R. Kim
1The Catholic University of Korea, Seoul, Korea; 2Soonchunhyang University, Seoul, Korea; 3H-Cube Hospital, Seoul, Korea; 4Wongkwang University Sanbon Medical Center, Sanbon, Korea
Objective: The aim of this study was to investigate the relationship between body composition and bone mineral density in middle aged women.
Design & Method: Bone mineral density (BMD) of lumbar spine and both femur neck was measured with dual-energy X-ray absorptiometry (DXA) in 89 middle aged women aged between 38 and 77 years old. Lean and fat mass of the arms, trunk, legs, total body, were measured same time with DXA.
Results: Android fat mass was increased with aging (P < 0.05). Body weight has positive correlation with BMD of lumbar and femoral neck, especially right side of femur. However, regional fat mass did not show any significant correlation with lumbar or both femur neck BMD. Lean body mass of left leg, left trunk, left total, right leg, right trunk, right total, arms, legs, trunks was positively correlated with BMD of the lumbar and both femur neck, respectively.
Conclusion: BMD was decreased and android fat mass was increased by aging of middle aged women. However, Lean body mass rather than fat mass is more important determinant of axial bone mineral density.
PS-282
BONE MINERAL DENSITY AT THE LUMBAR SPINE IN INDIAN WOMEN
J. Unni1, N. Kadam2, S. Chiplonkar2 and A. Khadilkar3
1Jehangir Hospital, Pune, Maharashtra, India; 2Agharkar Research Institute, Pune, Maharashtra, India; 3HCJMRI, Jehangir Hospital, Pune, Maharashtra, India
Objective: According to the World Health Organization (WHO), Osteoporosis is second only to cardiovascular disease as a global healthcare problem. Studies suggest that Indians have lower bone density than their North American and European counterparts and that osteoporotic fractures occur 10–20 years earlier in Indians. Thus the aim of our study was to assess bone mineral density (BMD) and the decline in bone mineral density in Indian women above 40 years of age.
Design & Methods: Retrospective data (from February 2006 to December 2007) on bone mineral density and anthropometry was collected on 983 women in the age group of 40–70 years coming to Jehangir Hospital, Pune, India, for routine health check. The subjects mostly came from middle class and upper middleclass families. Anthropometric parameters included height, weight and body mass index (BMI). The bone parameters studied were bone mineral density (BMD), bone mineral content (BMC) and bone area (BA) at the lumbar spine using a Lunar DPX-PRO total body Densitometer.
Data was divided into three groups, Group 1: 40–50 years, Group 2: 50–60 years and Group 3: 60–70 years.
Results: Data on BMD was available for 339 women in Group 1, 428 women in Group 2 and 216 women in Group 3.
For the whole group the mean BMC was 48.4gm (1.7), BMA was 47.6cm2(5.7) and BMD was 1.01gm/cm2 (0.17). BMC was significantly correlated with age, height and weight (p = 0.000 for all). As per the WHO classification for Osteoporosis 23.2% women had Osteoporosis, 40% had Osteopenia and the 36.8% subjects were normal.
The mean BMC observed in the three Groups was 52.2 (11.7) g, 47.2(11.6) g and 44.7(12.2) g respectively. One hundred and sixteen (9%) women in Group 1 had osteoporosis while 116(27%) and 82(38%) women of Group 2 and Group 3 respectively were Osteoporotic. The reduction in BMC from the 5th decade to the 6th decade was 10% and from the 6th to the 7th decade was 5% and the differences were statistically significant.
Conclusions: As per the WHO classification 23.2% of our study subjects had Osteoporosis and 40% had Osteopenia. The percentage of women with T score less than –2.5 was highest in the 7th decade. There was a rapid fall in BMC from the 5th to 6th decade and the bone loss reduced in the 7th decade. Thus osteoporosis and osteopenia are a major concern even in middle and upper-middle class Indian women.
PS-283
THE EPIDEMIC FEATURES OF OSTEOPOROSIS AND THE TREATMENT COMPLIANCE IN POPULATION OF TAIWAN
Y. K. Soong, H. Y. Huang and K. E. Huang
Chang Gung Memorial Hospital, Chang Gung University, Tauyan, Taiwan
Objective: To understand the epidemiology of osteoporosis in postmenopausal women. To answer the compliance of treatments for menopause and/or osteoporosis in population of Taiwan.
Design and Method: Post menopausal women or seniors have been provided with a mobile bone-care unit and network. The mobile unit is a multi-disciplinary approach with QUS devices and well-trained technologist, pharmacist, dietician and physiotherapist. They were chosen to different public stations for screening osteoporosis, health education and recommendations for improving patient's functional performances in last one year.
Results: A total 650 postmenopausal women were studied. The prevalence of osteoporosis was 17%, 50% in age group of 51–60 yrs and 70–80 yrs. Low bone mass was 45%.High risk for fall and bone fracture, severe osteoporosis was 13% without any interventions. The hormone therapy user rate was dropped from 26.6% in year 2001 to 16.8% in year 2003 then slowly increases up to now. Patients of osteoporosis only 57% accepted different drugs treatments. The patients' compliance after 6 months was dropped to 50%.Patients had many misconcepts such as calcium can treat the osteoporosis, etc.
Conclusion: The mobile bone-care unit is a cost-effective way to improve patients' knowledge, compliance reduce osteoporosis risk and fall prevention. Furthermore, it will improve access to osteoporosis, hypertension hyperglycemia and hyperlipidemia.
PS-284
BONE MASS IN PATIENTS WITH BREAST CANCER
R. Serrano, A. Estévez, M. Sanchez-Sevilla, I. Gasca, M. De la Peña, E. Iglesias and R. Garrido
University Hospital, Valme, Seville, Spain
Introduction: Women with breast cancer have a greater risk of fractures in comparison with women of equal age without this history. These patients have more risk factors for osteoporosis and fractures due to the different treatments that they receive: Chemotherapy, GnRH analogues, aromatase inhibitors (AIs). In women with receptor-positive breast cancer, AIs have demonstrated a significant improvement in disease-free survival in comparison with Tamoxifen, they have also been related to greater loss of bone mass and fractures.
Objetive: To investigate the relationship of bone mineral density (BMD) in women with breast cancer with: age, characteristics of the tumour, treatment received and possible protective treatment.
Design and Method: 167 women with breast cancer in which a bone study was made in the breast unit of the U.H. Valme, Seville, Spain, during 2007. The age at diagnosis, hormonal and chemotherapy treatment received, BMD value, menopausal state of the woman and the bone protective treatment established were analysed.
Results: The average age at which breast cancer was diagnosed was 59.09 (standard deviation of 9.94).Of these 167 women, 82.3% were menopausal at the time of diagnosis, with 50 being the average age of menopause. Positive oestrogen receptors were present in 76.2% of the cases, and progestagen receptors in 60.1%. Of these 167 women, 61.1% received some form of chemotherapy, 85.5% received hormone therapy, 14.7% with an SERM and 85.3% with an AI. The average age at which a BMD study was made in the follow up of the tumour process was 63.54. Of these studies 26.5% had a result in the range of osteoporosis and 37.7% in the range of osteopenia. Of the patients who presented osteoporosis, 90.7% were menopausal when the breast cancer was diagnosed. Of the cases with osteoporosis 72.1% had received chemotherapy, as opposed to 27.9% that had not. Of the cases with osteoporosis that had hormone therapy, 91.9% received an AI, and 8.1% a SERM.
Conclusions: Chemotherapy and hormone therapy based on AIs increase the risk of osteoporosis, which is why we must consider accompanying these treatments with vitamin D, calcium and anti-reabsorptive agents.
PS-285
BREAST CANCER, BONE DENSITY AND HORMONE THERAPY
P. Manso, R. Ribeiro, M. G. Castro, M. Rodrigues, J. Almeida, S. Sousa, R. Passarinho, C. Silva, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Bissaya-Barreto Maternity, Coimbra, Portugal
Objective: Recent studies have suggested a direct relation between bone mass and invasive estrogen-receptor positive breast cancer. On the other hand, women with breast cancer have a higher risk for osteoporosis: osteoclastic activity increases due to cancer, early menopause is more probable (chemotherapy-induced ovarian failure or oopherectomy) and chemotherapy can lead to hostile effects on bone mineral density (BMD). Loss of bone mineral is a complication of estrogen suppression associated with aromatase inhibitors.
The purpose of this study was to evaluate the relationship between bone mass and breast cancer and to determine the effect of hormone therapy in bone density.
Design & Method: Data were analysed in all postmenopausal women who did dual-energy x-ray absorptiometry scans (DEXA) during the year of 2002 and from that year on. A universe of 760 women was found and a descriptive statistic analysis was performed for age, body mass index (BMI), menarche, age at menopause and years of fertility.
Independent samples t-test was performed to evaluate baseline bone mass in women with and without breast cancer. Crosstab with chi-square and Fisher's exact test were done to determine the relationship between nulliparity and breast cancer.
In breast cancer subgroup, descriptive statistic analysis was performed, frequencies of histological type and hormonal receptors were evaluated and chi-square determination was calculated to evaluate hormonotherapy effects on vertebral and femoral t-scores.
Results: In our universe of 760 women, 45 had breast cancer (75.6% being estrogen-receptor positive). There was a statistical significance for high BMI and breast cancer (p < 0.05). We found no statistical significance between fertility years or nulliparity and breast cancer (p>0.05). There was no statistical difference between breast cancer and baseline vertebral or femoral t-scores (p>0.05). Crosstabs procedure revealed, with statistical significance (p < 0.05), that the risk of osteoporosis with hormonotherapy was higher with aromatase inhibitors, lower with the switch therapy and even lower with tamoxifen as unique therapy.
Conclusion: We found no evidence of relationship between bone mass and breast cancer. High BMI was related with breast cancer. Use of aromatase inhibitors rather than tamoxifen for breast cancer will likely lead to more osteoporosis. Tamoxifen may give potential benefits for bone health during switching therapy with aromatase inhibitors. Nevertheless, healthy life style, adequate calcium and vitamin D intake and biphosphonate therapy should be considered.
PS-286
CLINICAL AND DEMOGRAPHIC FEATURES IN POSTMENOPAUSAL WOMEN WITH LOW BONE MASS
J. Neves, A. P. Candeias, J. Pauleta, A. M. Coelho and L. M. Graca
Obstetrics, Gynecology and Reprodution Medicine Department, Santa Maria Hospital, Lisbon, Portugal
Objective: Osteoporosis is related with higher risk for fractures, despite finding in majority of postmenopausal women, normal value for bone mineral densitometry (BMD) or just low bone mass (LBMD). In postmenopausal women, half cases of fragility fractures, are related with LBMD, a signifcant number of fractures could be related with LBMD, so it is necessary to integrated differents features for risk facture calculation. Nowdays, is very important for a proprely risk facture evaluation, to recognize appropriated clinical and demographic features of postmenopausal women with osteoporosis and also with LBMD.
Design & Method: We evaluated 95 postmenopausal women with at least one risk factor for osteoporosis. Data are presented as mean ± sd and distributed in absolute and relative values.
Results: We find the following clinical and demographic data: age 59.5 ± 7.57 years; menarche 13.2 ± 1.77 years; menopause 48.8 ± 4.80 years; years from menopause – 10.7 ± 7.4; body mass index (BMI) 28.3 ± 11.14 Kg/m2 and waist-hip-circunpherence 88.9 ± 11.99cm; 62 women (65%) had been submited on HT. Present or past smoking habits were found in 16 cases (16.8%); no smoking in 72 cases (75.7%); missing data from smoking in 7 cases (7%). Glucocorticoids therapy was found in 3 cases (3.1%) and not refered in 77 cases (81%); in the remain population there were no data regarding this therapy. Osteoporosis family history was present in 28 cases (29%) and absent in 62 cases (65.2%); no data were available in 5 cases. Dyslipidemia as, a co-morbidity, was found in 54 cases (56%).
Conclusions: In this sample of postmenopausal women, LBMD was found in average at 59.5 years; more than a half had taken HT in the past, and even that, LBMD had been a diagnosis. We did not find any dominant clinical or demographic risk factor for osteoporosis, as smoking or family history or glucocorticoids therapy, and it can be explained because menopause with lack of estrogen and aging are the leading cause of LBMD and osteoporosis. BMI values are in average above the normal range; normaly, references in the literature, relate low BMI with osteoporosis. A point for futher evaluation, the percentage of postmenopausal women with LBMD and dyslipidemia.
PS-287
CLINICAL RISK FACTORS FOR FRACTURE IN POSTMENOPAUSAL OSTEOPOROTIC WOMEN: A PROSPECTIVE SPANISH COHORT STUDY
M. J. Cancelo1, C. Castelo-Branco2, J. L. Neyro3, S. Palacios4, R. Sánchez Borrego5 and J. Ferrer6
1Hospital Universitario de Guadalajara, Universidad de Alcalá de Henares; 2Hospital Clinic Barcelona, Universidad de Barcelona; 3Hospital de Cruces, Universidad de Bilbao; 4Instituto Palacios, Madrid; 5Clinica Diatros, Barcelona; 6Hospital Central de Asturias, Oviedo
Introduction: The osteoporotic fractures that annually occur in Spain are associated with high morbidity, mortality, and cost. Identification of those at high risk is a step toward prevention.
Objective: To asses epidemiological differences between two groups of osteoporotic woman: affected with fracture and non-fracture.
Material and Methods: An epidemiological, multicentric, transversal study was conducted to determine the current situation in Spain regarding epidemiological factors of patients with osteoporosis in primary care and different specialist settings.
A total of 18.680 patients who had undergone dual-energy x-ray absorptiometry (DXA) scans for bone mass density assessment with osteoporosis diagnosis was included in the study. A questionnaire covered demographics and personal characteristics of the patients, risk factors, diagnosis and treatment of the disease.
Results: The overall response includes 15.836 patients (84.8%). The percentage of patients with fracture was 37.2% vs. 62.7% non-fracture. Age and body mass index (BMI) were associated with fractures (69.1 ± 9.2 yrs vs 61.8 ± 8.5 yrs for non-fracture), (age more than 66 yrs, 64.2% vs.31.6% non fracture P<0.0001) and obesity greater than grade I of SEEDO criteria (44.4% vs 37.3% P<0.0001). Information on social and demographic data was obtained: 24.1% patients with fracture living alone vs.17.2% in non-fracture (p < 0.0001). With regard to habits in patients, there is significance in the following habits in patients with fracture vs non fracture: Physical exercise (23.7% vs. 33.5%) p < 0.0001; High calcium food (56.9% vs. 66.9%) p < 0.0001; Sun exposure (36.4% vs.43.1% p < 0.0001); Family history of fractures/osteoporosis (51.6%vs.43%) p < 0.0001; Background of fractures due to inestability (51.3% vs. 10.9%); Height loss (68.6% vs. 48%) p < 0.0001; Recent falls (63.8% vs. 20.6%) p < 0.0001; Inestability (32.9% vs. 16.5%) p < 0.0001; Visual dysfunction (41.7% vs. 27.1%) p < 0.0001. In contrast, pin back, smoking, use of alcohol were not significant differences between patients with fracture and non fracture.
Conclusions: These results suggest that women who have risk factors should receive the highest priority for prevention of osteoporotic fractures.
PS-288
COMPARİNG EFEFCTS of RİSEDRONATE, ATORVASTATİN, RALOXİFENE and CLOMİPHENE CİTRATE on POSTMENOPAUSAL OSTEOPOROSİS in OVARİECTOMİZED RATS
Y. Uyar, Y. Baytur, U. Inceboz, G. Gumuser and K. Ozbilgin
Faculty of Medicine, Celal Bayar University, Manisa, Turkey
Objective: Aim of this study was to investigate bone protective effects of risedronate, atorvastatin, raloxifene and clomiphene citrate in ovariectomized rats by forming an animal experiment model for postmenapousal osteoporosis and evaluating bone by densitometric, mechanical and hystomorphometric methods.
Design and Method: Our study was conducted on 50 rats at Experimental Research Center of Celal Bayar University. 6 months old rats were divided into 7 groups. 6 of the rat groups were overiectomized. There were 5 drug administered ovariectomized groups, 1 ovariectomized control group without drug administration (OVX, n = 5) and 1 non-ovariectomized control group without drug administration (NOVX, n = 5). Following OVX, 6 weeks were allowed for rats to heal and enter menopause. And then, rats were gavaged daily for 8 weeks with Risedronate sodium (2.5 mg/kg) (OVX + RSN, n = 9), Atorvastatin (50 mg/kg,) (OVX + AV, n = 5), 17β-Estradiol (0.1 mg/kg) (OVX + E2, n = 9), Raloxifene hydrochloride (3 mg/kg) (OVX + RL, n = 8), Clomiphene Citrate (1 mg/kg) (OVX + CC, n = 9). OVX and NOVX control groups were gavaged orally with 1 ml sterile saline solution on a daily basis. At the end of the study, rats were killed under anesthesia. For densitometric evaluation, left femurs and tibiae were removed. Left femurs were also used to measure bone volume. Right femurs were used for three-point bending test. Statistical evaluation was conducted using Mann-Whitney U test, Kruskal Vallis variance analysis and correlation analysis.
Results: Compared to OVX group, femur cortex volume increased significantly in NOVX group (p = 0.016). Compared to NOVX group, distal femoral metaphyseal and femur midshift bone mineral density (BMD) values were significantly lower in OVX group (p = 0.047). In OVX + AV group, distal femoral metaphyseal BMD and three-point bending test maximal load values were significantly higher than OVX group (p = 0.023, 0.018). In OVX + RSN group, all femur and distal femoral metaphyseal BMD values were significantly higher than the values in OVX group (p = 0.049, 0.05). A significant positive correlation was found between distal femoral metaphyseal BMD values and maximal load values (p = 0.003, r = 0.481).
Conclusion: While risedronate sodium prevented the decrease in postmenopausal bone mineral density in ovariectomized rats, atorvastatin both maintained mechanical characteristics of bone after ovariectomy and also prevented the decrease in bone mineral density as risedronate sodium. In the literature, positive effects of atorvastatin, which is an.
Anti-hypercholesterolemia, and similar statins are frequently reported. Similar studies with bigger groups may reveal that statins may be much more useful than present drugs protecting bone.
PS-289
CALCIDIOL AND IPTH SERUM LEVEL IN POSTMENOPAUSICAL WOMEN TREATED WITH ERGOCALCIFEROL
D. Salica1,2 and C. Salica1
1Healing Argentina Instituto de Osteología y Metabolismo Mineral P. Córdoba Argentina; 2Cátedra Clínica Médica Facultad de Ciencias Médicas Universidad Nacional Córdoba Argentina
Introduction: The therapeutic administration of Vitamin D is usually determined by empirical bases ruled by clinical criterion and not by seric dosage. The PTH response, in cases of low seric levels of calcidiol, can have a negative effect on bone health.
Objetives: Evaluation, before winter, of calcidiol levels in postmenopausical women (PMW) patients treated with ergocalciferol (800 UI/d average).
Material and Method: 28 PMW of 72 years old (±9.2 years old) have been studied, who were receiving doses of ergocalciferol 800 UI/d in average. The ergocalciferol was suspended a few days before the practice. The determinations made before winter, in 2007, included measurements of 25(OH) D with RIA (DIASORIN) and iPTH intact molecule with IRMA (DSL).
Results: values of mean 25(OH) D were 44 ng/ml (±18.4); from which the 50% of PMW showed values <40 ng/ml (<10 ng/ml 0% PMW; 10–20 ng/ml en 14% PMW; 20–30 ng/ml 17% PMG: 30–40 ng/ml 17% PMW. Levels of iPTH = 42.9 ng/ml (±21.7). Among the serum levels of iPTH and 25(OH) D, a negative correlation of a very significant difference was found (r = −0.643; p = <0.000).
Discussion: In the study group of patients treated with ergocalciferol 800 UI/d, the presence of low concentrations of 25(OH) D was important (<20 ng/ml 32% y <40 ng/ml 50%) and significant in relationship with iPTH. For this reason, it is requestioned the dose usually provided to these patients with ergocalciferol in 800UI/d can be insufficient.
Conclusions: It has been proved low serum levels of 25(OH) D with iPTH response tested in patients treated with 800 UI/d of ergocalciferol.
Bibliography: Fradinger E, Medicina 1999, Salica D, JBMR 1991.
PS-290
CLINICAL REALITY OF PREVENTION AND TREATMENT OF OSTEOPOROSIS IN LONG-TERM CORTICOSTEROID USERS – A TAIWANESE PERSPECTIVE
C. Y. Tsai, H. Y. Chang and Y. K. Soong
Chang Gung Memorial Hospital, Taoyuan, Taiwan
Objective: Corticosteroids are used in a wide variety of allergic and inflammatory conditions. Osteoporosis is a well-recognized side effect of long-term corticosteroid therapy and is associated with significant morbidity and mortality. Although there are many effective drugs in the management of osteoporosis, the majority of patients who require them do not receive them. Our aim was to review data of long-term steroid users and the management of osteoporosis at a medical centre in northern Taiwan.
Design and Methods: We reviewed patients on long-term corticosteroids in a cross-sectional study. Demographic and clinical details of 1432 patients were available from Rheumatology and Immunology departmental records in a medical centre for the 8-month study period of April to November 2002.
Results: Over half of the patients in this study used corticosteroids for the treatment of rheumatoid arthritis (RA). Among the 1432 patients, 430 (30%) received medication for osteoporosis including 10 patients on bisphophonate, 216 on calcium combined with vitamin D, 166 on calcium alone, 28 on hormone replacement therapy, 8 on calcitonin and 2 on Raloxifene. Three hundred patients (20.9%) had pre-existing osteoporosis, of which just 68% were treated. Female and elderly patients were more likely to have osteoporosis and female patients were more likely to be treated for it. Paradoxically, we found significantly more low-dose steroid users on osteoporosis therapy than high-dose steroid users.
Conclusions: This study elucidated in long-term steroid users the relationships between osteoporosis management and various patient factors and highlighted the inadequacies in osteoporosis management for long-term steroid users. Improved efforts in the management of osteoporosis are recommended for this vulnerable group of patients.
PS-291
COMPARISION AND STANDARDIZATION OF DUAL ENERGY X-RAY DENSITOMETRY SYSTEMS
In-Cheul Jeung, Hyun Jung Kim, Hyun Hee Jo, Sung Jin Hwang, Jae Yeun Song, Jang Heub Kim, Jin Hong Kim and Mee Ran Kim
Medical Collage Of The Catholic University Of Korea
Objectives: The Dual energy X-ray absorptiometry (DXA) has different results in reported bone mineral density (BMD) among manufactures, system and measurement site, so called T-score discrepancy. In this study, the comparision and standardization between DXA systems was obtained. Consequently evaluation of the cross calibration formaula and Korean reference database was also obtained.
Methods: A total of 100 Korean women were recruited and studied between September 2006 and February 2007 in Kangnam St. Mary's Hospital, the Catholic University of Korea. The BMD was measured in the lumbar vertebrae (L1−4) and the both femoral neck one the same day using a GE Lunar Prodigy and Hologic QDR-4500. We compared the BMD values, T-scores, Z-scores and patients' diagnoses based on WHO criteria between two systems. We calculated standardized BMD(sBMD) and compared Lunar to Hologic. This study evaluated and calculated new conversion formula between Lunar and Hologic DXA for Korean women.
Results: Both the L-spine and the femur neck, the Lunar yielded consistently higher results than the Hologic (P<0.001). The BMD values measured by the two instruments were highly correlated (lumbar spine r = 0.97, femur neck r = 0.95, P<0.01). The sBMD values by the conversion formula which were compared with BMD measured, had significant differnces in lumbar spine (P<0.01, paired t-test). New conversion formulas between two systems for Korean women are calculated. For the lumbar spine: Hologic = (0.844 × Lunar) + 0.006, For the femur neck: Hologic = (0.886 × Lunar) −0.05.
Conclusion: For correcting the discrepancy of different DXA systems, we can use sBMD, cross calibration, and furthermore calculate new conversion formula for the reference population.
PS-292
COMPARISON OF BONE DENSITY CHANGES FOLLOWING ADDBACK THERAPY WITH DIFFERENT GNRH AGONISTS IN ENDOMETRIOSIS PATIENTS
Yong-Taik Lim1, Je-Yeon Song1, Kyu-Sup Lee2, Taek-Hoo Lee2, Sung-Tack Oh2, Young-Min Choi2, Byung-Seok Lee2, Jun-Yong Hur2 and Jung-Ho Shin2
1Kang Nam St. Mary's Hospital, The Catholic University of Korea, Seoul 137-040, South Korea; 2Korean Endometriosis Society
Objectives: GnRH agonist was one of most useful medical therapy of endometriosis, but proven to lower bone mass density by inhibit secretion of estrogen. This study was designed to compare the clinical characteristics, changes of bone mass density among gonadotropin-releasing hormones (leuprolide (Leuprin), triptorelin (Decapeptyl) and goserelin (Zoladex)) for postoperative hormonal therapy of endometriosis.
Design & Method: For each group, thirty women were subjected to use 6 times GnRH agonists for postoperative treatment of endometriosis from January 1998 through December 2006 in Kangnam St Mary's hospital, Korea. All patients had add-back therapy by using estrogen plus progesterone, tibolone, alendronate. The patients who had history of smoking, alcohol, steroid therapy, previous fracture were excluded.
Results: Three kinds of GnRH agonist were applied for postoperative therapy of endometriosis, which were leuprolide, triptorelin and goserelin. Each of groups had similar age (38.3 vs 36.5 vs 36.1 years), parities (1.2 vs 1.4 vs 1.2), BMI (21.3 vs 21.6 vs 21.5 kg/m2), presence of dysmenorrhea (80% vs 73% vs 70%) and stage of endometriosis at diagnosis (3 vs 2.87 vs 2.5). When comparing GnRH agonist by BMD, the mean changes of T score of lumbar vertebra 2–4 (−0.33 ± 0.47), lower part of lumbar vertebra (−0.31 ± 0.51), Rt femur neck (−0.35 ± 0.77), lower part of Rt femur (−0.25 ± 0.44), Lt femur neck (−0.19 ± 0.36), lower part of lumbar vertebra (−0.19 ± 0.31) of leuprolide were similar with those of triptorelin, which were (−0.43 ± 0.56), (−0.33 ± 0.95), (−0.37 ± 0.73), (−0.39 ± 0.84), (−0.42 ± 0.72), (−0.38 ± 0.61) and those of goserelin, which were (0.53 ± 6.25), (−1.59 ± 6.95), (−0.11 ± 0.77), (−0.21 ± 0.76), (−0.19 ± 0.70), (−0.16 ± 0.73), respectively. The differences were statistically insignificant (all p > 0.05).
The FSH measured after 6 times of goserelin use was lower (3.3 ± 3.6 mIU/ml) than those of leuprolide (9.7 ± 8.3 mIU/ml) and triptorelin (6.9 ± 6.9 mIU/ml) (p < 0.01). The estradiol measured after 6 times of leuprolide use was higher (83.3 ± 123.0 pg/ml) than those of triptorelin (42.9 ± 63.1 pg/ml) and goserelin (21.6 ± 33.4 pg/ml) (p = 0.04). The proportion of patients whose value of estradiol were checked less than 30pg/ml were 40% from leuprolide, 56% from triptorelin and 91% from goserelin.
Conclusion: Among GnRH agonist (leuprolide, triptorelin, goserelin) for postoperative hormone therapy of endometriosis, no statistically significant change on BMD were appeared. But, when we compared the potential bone protective effect by estradiol level, leuprolide could be considered the most effective and conservative choice.
PS-293
CONTROL OF THE EFFECT OF OSSEIN-HYDROXIAPATITE COMPLEX AND RALOXIFENE ON THE POSTMENOPAUSAL BONE MEASURED BY ULTRASOUND DENSITOMETRY
I. Pelayo1, J. Haya2, J. J. De la Cruz3, C. Seco4, Diaz Jose Luis5, M. J. Pablos1, J. Lazaro1 and M. Repolles1
1Hospital Ramón y Cajal, Madrid, Spain; 2Hospital Universitario Santa Cristina, Madrid, Spain; 3Universidad Autónoma de Madrid, Madrid, Spain; 4Hospital Universitario de Getafe, Madrid, Spain; 5Fundación Jimenez Diaz, Madrid, Spain
Objective: We evaluated the efficacy and safety of raloxifene (RLX) plus ossein-hydroxyapatite compound (OHC) for controlling bone loss in postmenopausal women. The primary endpoint was mean change in Amplitude Dependent Speed of Sound (ADSoS) score from baseline. The evolution of bone pain was recorded.
Design and Method: We selected 48 postmenopausal women who referred bone general pain not attributed to an osteoarticular precise patohology, and assigned them to treatment with RLX plus OHC for up to 3 years. Bone mineral density was measured using ultrasound techniques on the proximal phalanx of the non dominant hand. The mean change in ADSoS score was calculated substracting the ADSoS value of the 3 year's visit to the basal data.
Bone pain was evaluated in an analogical scale, where 0 means no pain and 10, the most horrible pain. We also recorded adverse effects.
Results: ADSoS values were mantained throughout the 3 years of treatment. At baseline visit ADSoS were 1956.11 (124.99) m/s; 1969.13 (118.67) m/s in first year of follow up; 1963.94 (113.07) m/s in the second year; and 1955.68 (100.65) m/s in year 3. The mean change in ADSoS score was 23.77 (62.65) m/s from baseline to year 3, which meant a 1.21% of reduction in respect to basal value. Similar results were seen on T and Z scores.
In relation to the bone pain, a 90% of the patients referred improvement. The pain values were 7.47 (1.34) at the basal visit and 4.33 (1.78) at the 3 years visit (p < 0.001).
Adverse effects were infrequent and mild, such as hot flushes (8.3%).
Conclusion: RLX + OHC appears to be effective in controlling bone loss and reducing bone pain in postmenopausal women.
Bone mineral density measured using ultrasound techniques could be useful in controlling postmenopausal women.
PS-294
CORRELATION BETWEEN BONE DENSITY AND TOOTH LOSS
E. Correa1, M. N. Rancel2, M. Correa3, B. C. Ceballos4, P. Beltri1 and M. Segura4
1Faculty of Odontology, European University of Madrid, Madrid, Spain; 2Faculty of Medicine, University of La Laguna, Tenerife, Spain; 3Hospital Universitario de Canarias, La Laguna, Tenerife, Spain; 4Hospital U Nuestra Señora de Candelaria, Santa Cruz de Tenerife, Spain
Objective: To assess the effect of bone density on tooth loss.
Material and Methods: A group of postmenopausal women (30 cases) were tested for bone density in the spine and femur. Average values were calculated in both cases and were correlated with the number of missing teeth.
Results:
The average age of the patients was 58.8, ranging from 47 to 71.
The menopause started at 49.6, with ages ranging from 38 to 55.
Average time from the menopause to the bone density test was 9.2 years (minimum 1 year and maximum 33).
Missing teeth. The most frequent number was 8 (46%) and in 20% of the cases more then 24 teeth were lost.
Bone density. 23% had osteoporosis, 44% osteopenia and 33% normal bone density.
Bone density and missing teeth. We found many cases in which bone density was low and yet teeth had been conserved and also cases with high bone density and loss of numerous teeth. If we group together all the cases with the highest number of teeth lost and all those with the lowest number of teeth lost, we find a 0.042 g/cm2 of difference in favour of those who have kept their teeth more successfully.
PS-295
DIAGNOSIS AND ASSESSMENT IN POSTMENOPAUSAL OSTEOPOROTIC WOMEN: A PROSPECTIVE SPANISH COHORT STUDY
J. L. Neyro1, S. Palacios2, M. J. Cancelo3, J. Ferrer4, R. Sánchez-Borrego5 and C. Castelo-Branco6
1Servicio de Ginecologia y Obstetrícia, Hospital de Cruces, Baracaldo, Spain; 2Instituto Palácios de Ginecologia e Investigación, Madrid, Spain; 3Servicio de Ginecologia y Obstetrícia, Hospital Universitário de Guadalajara, Guadalajara, Spain; 4Hospital Central de Asturias, Oviedo, Spain; 5Clinica Diatros, Barcelona.Spain; 6Institut Clínic de Ginecologia, Obstetrícia i Neonatologia, Hospital Clinic, Universitat de Barcelona, Barcelona, Spain
Introduction: In the last years a great increase in the knowledge of the underlying changes in bone and the mechanisms that lead to the disease has been done. Osteoporosis has been defined as a skeletal disorder characterized by a compromised bone strength that predispose to an increased risk of fracture1. White and Asian women are at greater risk for osteoporosis and associated fracture than black women. Smoking and lack of exercise also may contribute to the development of osteoporosis, but they are not major risk factors. The more risk factors a women has the higher the likelihood that she has or she will develop osteoporosis.
Objective: To assess epidemiological and diagnostic characteristics of 18680 women in Spain, diagnosed with Postmenopausal Osteoporosis and to evaluate the principle risk factors to develop such a disease.
Material and Methods: An open, epidemiological, multicentric, transversal study was conducted to determine the current situation in Spain regarding diagnosis and care of patients with osteoporosis in the primary care and different specialist settings. A total of 2.332 researches of different specialties (gynecology, rheumatology, endocrinology, primary care…) with a total of 18680 patients were grouped in autonomous communities throughout our country. The questionnaire covered demographics and personal characteristics of the patients, risk factors, diagnosis and treatment of the disease. The principle risk factors were included in a logistic model in order to asses positive and negative association and find risk and protection factors (Stepwise method).
Results: The overall response includes 15.836 patients (84.8%). We study the principle risk factors to osteoporosis (family history (bloodline) of fractures/osteoporosis, smoker, age more than 66, body mass index (BMI), age more than 66 yrs, obesity greater than grade I of SEEDO criteria, living alone, physical exercise, high calcium food intake, habitual sun exposure, visual dysfunction etc).
Protection factors were in order of appearance: physical exercise (OR = 1.35), high calcium food (OR = 1.33) and hygiene-dietetic advice (OR = 1.72). On the contrary, risk factors were, patient status (living alone) (OR = 1.32), background of fractures due to instability (OR = 5.56), height loss (OR = 1.27), recent falls (OR = 4.45) and visual dysfunction (OR = 1.15).
1NIH Consensus Development Panel. JAMA 2001; 285:785–95.
PS-296
EFFECTIVENESS OF COMPLEX MEDICATION (GLUCOSAMIN SULPHATE, CHONDROITIN SULPHATE AND IBUPROFEN) FOR TREATMENT OF PAIN SYNDROME UNDER KNEE OSTEOARTHRITIS
V. Povoroznyuk and N. Dzerovych
Institute Of Gerontology AMS Of Ukraine
The research was aimed at evaluating the effectiveness of Theraflex-Advance (TA), (250 mg glucosamin sulphate, 200 mg chondroitin sulphate and 100 mg ibuprofen). The first group included 16 patients (aged 64,2 ± 1,9 years) with knee osteoarthritis of II-III stages, according to Кеllgren-Lourenz. The control group included 16 patients with the same diagnosis (aged 63,9 ± 1,7 years), who took Theraflex (Т) (500 mg glucosamin hydrochloride and 400 mg chondroitin sulphate). The following methods of study were used: Mc-Gill questionnaire, VAS, Leken index, Womac scales, determination of life quality by EuroQol 5D scale.
After two weeks of treatmen, patients taking TA observed a reliable decrease of pain syndrome by Womac scale (before treatment 58,5 ± 5,5; after two weeks 40,7 ± 5,9; t = 2,38; р = 0,037), decrease of constraint in movements (index before treatment 57,8 ± 6,5; after two weeks 36,7 ± 6,3; t = 2,65; р = 0,022), improvement of index of everyday activity (before treatment 64,6 ± 4,1; after a fortnight - 44,0 ± 6,1; t = 2,82; р = 0,017). Over a month intensity of pain in the knee lowered in the group taking TA, according to VAS scale (before treatment 55,0 ± 3,1; over a month 44,2 ± 4,9; t = 2,32; р = 0,041), according to Womac scale (before treatment 58,5 ± 5,5; over a month 38,7 ± 5,7; t = 2,45; р = 0,032). Constraint of movement also decreased, according to Womac scale (before treatment 57,8 ± 6,5; over a month 37,5 ± 7,2; t = 2,96; р = 0,013) and index of everyday activity improved (before treatment 64,6 ± 4,1; over a month 42,1 ± 5,4; t = 3,51; р = 0,005). A month after patients ceased taking the drug, intensity of pain remained lower in comparison with indexes before treatment: by VAS scale (before treatment 55,0 ± 3,1; over a month - 39,0 ± 4,1; t = 2,26; р = 0,049), by Womac scale (before treatment 58,5 ± 5,5; over a month −41,1 ± 5,5; t = 1,40; р = 0,20). By contrast, the constraint of movements increased (indexes after a month of treatment −37,5 ± 7,2; after two months - 47,0 ± 6,6), and index of everyday activity decreased according to Womac scale (after a month - 42,1 ± 5,4; after two months - 49,4 ± 5,3). However, the given indexes were lower than before treatment (57,8 ± 6,5 and 64,6 ± 4,1, respectively). In the group taking T, intensity of pain syndrome certainly decreased after two months of treatment, according to VAS scale (before treatment - 50,9 ± 3,9; after two months- 42,7 ± 4,6; t = 3,1; р = 0,011), Womac pain scale (before treatment - 47,0 ± 5,3; after two months- 30,4 ± 6,5; t = 2,89; р = 0,016). The constraint of movements decreased (before treatment 47,4 ± 5,1; after two months- 35,9 ± 6,6; t = 2,67; р = 0,023), and index of everyday activity improved (before treatment 50,0 ± 6,1; after two months- 38,3 ± 6,3; t = 2,25; р = 0,048).
Hence, Theraflex-Advance is instrumental in rapid decrease of intensity of the pain syndrome (after two weeks) in patients with knee osteoarthritis. Over a month after cessation of preparation taking, positive effect remains: knee pain is significantly lower in comparison with indexes before treatment; constraint index increases and index of everyday activity aggravates. Herewith, the given indexes remain lower than before treatment. The analgesic effect after taking Тeraflex becomes noticeable after two months when it is followed by the essential decrease of constraint index, improvement of index of everyday activity. Quality of life significantly improved in patients of both groups.
PS-297
EFFECTS OF ESTROGEN ON THE ACTIVITY AND GROWTH OF HUMAN OSTEOBLAST AND OSTEOCLAST CELLS IN VITRO
Fang-Ping Chen1, Chin-Hwa Hu2, Kun-Chuang Wang1, Yung-Kui Soong1 and Ko-En Huang1
1Chang Gung Memorial Hospital, Keelung, Taiwan; 2National Taiwan Ocean University, Keelung, Taiwan
Objecitve: Bone metabolism is regulated by a balance between bone resorption by osteoclasts and bone formation by osteoblasts. Estrogen deficiency during menopause is associated with an increased rate of bone loss. The mechanism related to the effects of estrogen on osteoblasts and osteoclasts is still unresolved.
Design & Methods: Osteoblast cultures were prepared from the upper femur of postmenopausal patients or MG 63. To investigate that whether in co-culture with human osteoblasts, mononuclear macrophages from cord blood or bone marrow can differentiate into mature osteoclasts. Further to examine the effect of estrogen on the activity and growth of osteoblasts and osteoclasts.
Results: In the human primary osteoblast-like cells culture, 17β-E2 caused a significant reduction of interleukin−6 and osteocalcin secretion to a maximum of 34% and 60% the control value (un-treated cells) respectively. 17β-E2 significantly induced alkaline phosphatase activity and cell proliferation to 183% and 150% of control value. We have characterized the differentiation potential of mononuclear cells from cord blood or bone marrow into mature osteoclast when co-culture with human osteoblast cells. During 28-day co-culture, macrophage markers CD 11b and CD 14 were down-regulated and vitronectin receptor (VNR) was up-regulated. After incubation for 28 days, the addition of 17β-E2 caused a significant decrease of the expression of VNR and TRAP-positive multinucleated cells both in the culture from bone marrow or cord blood. A significant decrease in the extent of bone resorption on bone slices was also noted in the presence of 17β-E2.
Conclusions: This study demonstrates that 17β-E2 has effects on osteoblasts, as well as osteoclasts. These results confirm and explain part of the mechanism that appears in clinical studies of postmenopausal osteoporosis, in which 17β-E2 play an important role in the prevention of osteoporosis. The prevention of osteoporosis by estrogen may be related not only to direct effects on osteoblastic activity and proliferation but also to direct and indirect effects on osteoclastogenesis and osteoclastic activity.
PS-298
ESTROGENS AND OSTEOPROTEGERIN – BONE MARKER REMODELING IN POSTMENOPAUSAL OSTEOPOROSIS
Camelia Vidita Gurban1, Camelia Ciacli2, Maria Puschita3 and Doina Drugarin4
1,4„Victor Babes” University of Medicine and Pharmacy, Timisoara; 2,3„Vasile Goldis” West University, Arad
Introduction: Estradiol (E2) and Osteoprotegerin (OPG) play an important role in the regulation of bone turnover, including bone formation by osteoblasts.
Objectives: The aim of this study was the determination of serum levels of two markers: E2 and OPG implicated in bone remodeling of postmenopausal women with osteoporosis.
Material & Methods: The study was made on two cohorts of patients with postmenopausal osteoporosis (depending on estrogenic deprivation) comparing them with the control group (menopausal women without osteoporosis). Serum levels of E2 and OPG were measured by enzyme-linked immunoasorbent assay (ELISA) and evaluation BMD (Bone Mineral Density) were analysed using DEXA methods assessment T scores.
Results: Cohort 1 (<15yr of estrogenic deprivation): OPG serum 42,15 ± 0,55 pg/ml, E2 serum 28,32 ± 1,81 pg/ml, iar sT spine −3,63 ± 0,65 DS. Cohort 2 (>15yr of estrogenic deprivation): OPG serum 27,78 ± 1,04 pg/ml, E2 serum 19,66 ± 1,23 pg/ml, iar sT spine −3,71 ± 0,36 DS. Control group: OPG serum 38,05 ± 4,89 pg/ml, E2 serum 43,07 ± 10,04 pg/ml, iar sT spine −1,77 ± 0,11 DS.
Conclusions: The serum levels increase of OPG demonstrate osteoblasts activation. The decreased serum levels of OPG demonstrate osteoblasts apoptosis stimulation, associated with estrogen deficiency in a postmenopausal women, which will increase significantly bone turnover, producing a decrease of bone formation and increasing bone resorption, and the imbanlance favorising the appearance of osteoporosis.
PS-299
EVALUATION OF VALIDITY OF IOF'S ONE-MINUTE OSTEOPOROSIS RISK TEST FOR POSTMENOPAUSAL WOMEN
V. Povoroznyuk and N. Dzerovych
Institute Of Gerontology AMS Of Ukraine
Background: This research was aimed at proving validity of IOF's One-Minute Osteoporosis Risk Test and evaluating the relation between structural-functional state of bone according to the ultrasound densitometry and results of IOF's One-Minute Osteoporosis Risk Test for postmenopausal women.
Materials and Methods: We've examined 147 postmenopausal women aged 50–69 years (mean age 59,8 ± 0,7). Structural-functional state of bone was evaluated by means of an ultrasound bone densitometer (“Achilles + ”). The speed of sound (SOS, m/s), broadband ultrasound attenuation (BUA, dB/MHz) and a calculated “Stiffness” index (SI, %), T and Z-range were measured. IOF's One-Minute Osteoporosis Risk Test was translated into Ukrainian.
Results: Significant correlation was found between positive answer to question 2 (“Have you broken a bone after a minor bump or fall?”) and SOS (r = −0.17; р = 0,042), BUA (r = −0.28; р = 0,0005), SI (r = −0.25; р = 0,002), Z- range (r = −0.26; р = 0,015); between positive answer to question 3 (“Have you taken corticosteroid tablets for more than 3 month”) and SOS (r = −0.16; р = 0,047), BUA (r = −0.29; р = 0,0003), SI (r = −0.21; р <0,000001), and between positive answer to question 4 (“Have you lost more than 3 cm (just over 1 inch) in height?”) and the following indexes of structural-functional state of bone: SOS (r = −0.32; р <0,00001), BUA (r = −0.27; р = 0,00096), SI (r = −0.36; р <0,000001), Z- range (r = −0.27; р = 0,0015).
Conclusion: Application of IOF's One-Minute Osteoporosis Risk Test gives an opportunity to determine structural-functional changes of bone. Among the test questions, the most reliable and informative as for postmenopausal women proved to be questions 2 (“Have you broken a bone after a minor bump or fall “), 3 (“Have you taken corticosteroid tablets for more than 3 month “) and 4 (“Have you lost more than 3 cm (just over 1 inch) in height?).
PS-300
EFFECTS OF SOY ISOFLAVONE AND RESISTANCE TRAINING ON BONE MINERAL DENSITY AND BODY COMPOSITION IN POSTMENOPAUSAL WOMEN
F. L. Orsatti1, E. A. P. Nahas1, J. Nahas-Neto1, C. E. Fernandes2, C. L. Orsatti1, A. Delmanto1, N. Maesta1 and P. Traiman1
1Botucatu Medical School, UNESP-São Paulo State University; 2ABC Medical School; São Paulo, Brazil
Objective: To investigate the independent and additive effects of soy isoflavone (SI) and resistance training (RT) on bone mineral density (BMD) and body composition in postmenopausal women.
Design & Method: This study used a placebo-controlled, double-blind (soy), randomized two (SI vs placebo) × two (RT vs no-RT) design. A total of 80 sedentary Brazilian postmenopausal women (>12 months amenorrhea and FSH>40mIU/ml), aged 45–70 years, was randomized one of four groups (64 completed 9-months intervention): SI + RT (n = 14); placebo + RT (n = 15); SI (n = 17); placebo (n = 18). Participants randomized to SI received 250mg of standardized soy extract, total of 100 mg/day of isoflavone. Subjects randomized to RT attended supervised resistance exercise sessions, three days/week for 9-months and included 2–3 exercises for the larger muscle groups, and 1 exercise for smaller groups in 3 series of 8–12 repetitions. At baseline and 9-months, body composition (fat and muscle mass) and BMD were estimated by dual-energy x-ray absorptiometry. Serum levels of C-terminal cross-linked telopeptides of type I collagen (CTX) and osteocalcin were measured as markers of bone resorption and formation, respectively. The plasma levels of isoflavones were measured to assess compliance. The ANOVA with time as the repeated measure, Fisher test, and Pearson's correlation were used in the statistical analysis.
Results: There were no significant differences in all baseline parameters between groups. Subjects were classified as overweight and showed central fat distribution. After 9-months of intervention, RT increased significantly strength (35.2%) and muscle mass (3.1%). A significant decreases muscle mass (2,8%) and increases fat mass in the whole-body (1.8%) and trunk (10.1%) was found in no-RT groups (p < 0.05). In SI groups, there were no differences in body composition. Neither SI nor RT affected independently BMD at any site and levels of osteocalcin. However, RT attenuated the bone resorption; the CTX increased 2,6% in the RT groups versus 15,3% in the no-RT groups (p < 0.05). No additive effects of SI and RT were found on body composition and BMD. There was positive correlation among values of BMD and muscle mass (r = 0.30); and waist circumference and %trunk fat (r = 0.96) (p < 0.05). The subjects given SI showed significantly higher detectable levels of isoflavones than those in the placebo group.
Conclusion: In postmenopausal women: (1) soy isoflavone did not alter BMD and body composition; (2) the resistance training exerted favorable effects on muscle mass and bone resorption; (3) There were no additive effects of soy and exercise on BMD or body composition.
PS-301
EFFECTS OF VITAMIN E ON CELL PROLIFERATION IN DIFFERENTIATION OF HUMAN MESENCHYMAL STEM CELLS INTO OSTEOBLASTS
Tak Kim1, Jung Ho Shin2, Jun Yong Hur2, Heung Yeol Kim3, Hyoung Moo Park, Kyu Wan Lee and Sun Haeng Kim
1Korea University Ansan Hospital, Korea; 2Korea University Guro Hospital, Korea; 3Kosin University Hospital, Korea
Objectives: Our objective was to examine cell proliferation in differentiation of human mesenchymal stem cells into osteoblast treated with vitamin E (α-tocopherol) in vitro.
Materials and Methods: Human bone marrow stem cells were cultured in 96-well culture plates. Cells were cultured for 0∼3 days in osteogenic differentiation medium and added α-tocopherol to the wells at the final concentrations of 10 μM and 100 μM. Cell Proliferation ELISA, colorimetric immunoassay for the quantification of cell proliferation, based on the measurement of BrdU incorporation during DNA synthesis was used as a measure of osteoblast differentiation. One or three days after, we measured the absorbance of the samples in an ELISA reader at 370 nm.
Results: We found that vitamin E had better enhancing effect on cell proliferation as compared to those cultured in media without vitamin E. Alpha-tocopherol, 10 μM, enhanced cell proliferation in the culture by 2.3-fold (P<0.05) on day 1 and 2.2-fold (P<0.05) on day 3. Alpha-tocopherol, 100 μM, enhanced cell proliferation in the culture by 1.5-fold (P<0.05) on day 1 and 1.2-fold (P<0.05) on day 3.
Conclusions: Our results showed that α-tocopherol is a potent stimulator for inducing mesenchymal stem cells to differentiate into osteoblasts with further enhancement on bone formation.
PS-302
EFFICACY OF OSSEIN-HYDROXYAPATITE COMPLEX COMPARED WITH CALCIUM CARBONATE TO PREVENT BONE LOSS: A META-ANALYSIS
C. Castelo-Branco1, M. Ciria-Recasens2, M. J. Cancelo-Hidalgo3, S. Palacios4, J. Haya-Palazuelos5, J. Carbonell-Abello2, J. Blanch-Rubio2, M. J. Martinez-Zapata6, J. Manasanch7 and L. Perez-Edo2
1Hospital Clínic i Provincial, Barcelona, Spain; 2Hospitales Universitarios del Mar y de la Esperança, Barcelona, Spain; 3Hospital Universitario de Guadalajara, Univ, de Alcalá de Henares, Guadalajara, Spain; 4Palacios Women's Health and Medicine Institute, Madrid, Spain; 5Hosp. Univ. Sta. Cristina, Univ, Autónoma de Madrid, Madrid, Spain; 6Hospital de la Santa Creu i Sant Pau, Barcelona, Spain; 7Pierre Fabre Iberica S. A., Barcelona, Spain
Objective: There is increasing evidence to suggest that ossein-hydroxyapatite complex (OHC) is more effective than calcium supplements in maintaining bone mass. The aim of this meta-analysis was to determine whether OHC has a different clinical effect on bone mineral density (BMD) compared to calcium carbonate (CC).
Design & Method: A meta-analysis of randomized controlled clinical trials was carried out to evaluate the efficacy of OHC versus CC on BMD. Publications on clinical trials were identified by a search of electronic databases, including MEDLINE (1966 - March 2007) and the Cochrane Controlled Clinical Trials Register.
The primary endpoint was percent change in BMD from baseline. Data were pooled in a random-effects model and the weighted BMD mean difference was calculated. A sensitivity analysis was performed excluding trials without full data.
Results: Of the 14 controlled trials initially identified, 6 were included in the meta-analysis. There was no significant heterogeneity among the included trials (p = 0.29). The percent change in BMD significantly favoured the OHC group (1.34% [95% CI: 0.61 - 2.08] p = 0.0003). These results were confirmed in the sensitivity analysis.
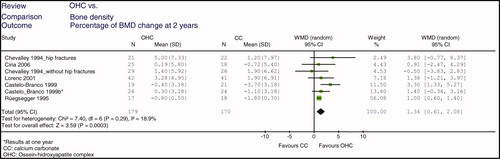
Conclusion: Ossein-hydroxyapatite complex is significantly more effective in preventing bone loss than calcium carbonate.
PS-303
EVALUATION OF RISK FACTORS FOR DEXA REFERAL IN INDIAN WOMEN
Meeta Singh
Tanvir – Tanvir Hospital, Hyderabad, Andra Pradesh, India
Objective: To evaluate the performance of Risk Factors for DEXA referral.
Material and Methods: 376 postmenopausal women participated in the study.
Risk Assessment Questionnaire with eighteen variables was used and Bone Mineral Density at hip and spine measured.
Results: The mean age was 53.82 years (SD 9.21, median age 53.00 years, range 27.00 to 84.00 years). The mean BMI in the study was 26.69 (SD 4.34, Median 26.40, range 14.45 to 40.25). The mean age at menopause was 44.06 years (SD 6.04, Median 45.00 years, range 22.00 to 55.00 years). 92 (24.80%) reported premature menopause, 232 (61.87%) were on calcium supplements, 46 (12.33%) reported fragility fractures, 194 (51.73%) reported exposure to sunlight, Family history of fragility fractures was reported by 63 (16.80%), 25 (6.67%) were reportedly on steroids, 9 (2.40%) of them reported alcohol intake, 41 (10.93%) were on eltroxin, 132 (35.20%) reported high caffeine intake, 8 (2.13%) were on anticonvulsants, 115 (30.75%) had multiple pregnancies, 49 (13.07%) had Rheumatoid Arthritis, 109 (19.07%) had prolonged lactation, 28 (7.49%) had Hyperparathyroidism, 29 (7.73%) had Malabsorption, 36 (9.63%) had Diabetes, and 286 (77.09%) of patients were obese. The mean BMD hip was 0.89 (SD 0.18, Median 0.88, range 0.246 to 1.605), the mean BMD Spine was 0.94 (SD 0.20, Median 0.95, range 0.084 to 1.91).
The prevalence of osteoporosis was 4.26% (95% CI 2.2, 6.3) based on the hip and 22.07% (95% CI: 17.86, 26.28) based on the spine. The prevalence of osteopenia was 17.82% (95% CI: 13.91, 21.70) based on the hip and 35.11% (95% CI: 30.26, 39.95) based on the spine.
On univariate analysis, premature menopause was significantly associated with osteopenia of the spine (p = 0.001), family history of fragility fractures was significantly associated with osteopenia of the hip (p = 0.048), Eltroxin was associated with osteoporosis of the spine and hip (p = 0.02 and 0.01 respectively).
DEXA testing is indicated if a person has premature menopause, history of fragility fracture, steroid intake, alcohol consumption, eltroxin intake, anticonvulsants, rheumatoid arthritis, hyperparathyroidism, malabsorption or diabetes. The clinical challenge is to identify at Risk Population based on the best evidence available. With the plethora of management options, it's a service to women's health in early diagnosis and treatment for low BMD. Acknowledgement- Dr. Praveen Nirmalan Biostatistician, Mrs. Wajahat and Women participants.
PS-304
FACTORS OF RISK ASSOCIATED TO OSTEOPENIA AND OSTEOPOROSIS IN SPANISH POSTMENOPAUSAL WOMEN
F. Baró1, E. Rodríguez Bueno2, L. Esteban3, I. Ibars4, M. Guinot6, B. Roca7 and E. Ruiz8
1Hospital Materno-Infantil Vall d'Hebron, Barcelona Spain; 2PASSIR Sant Andreu, Barcelona; 3PASSIR Casgemes, Badalona; 4PASSIR Manso Barcelona; 6Hospital Sant Pau, Barcelona; 7Hospital Terrassa, Barcelona; 8PASSIR Antoni Creus, Terrassa, Barcelona Spain Group Study Menopause and Osteoporosis in Cataluña (GEMOC), Barcelona, Spain
Objective: To analyse the prevalence factors of risk, in greater women of 45 years and menopauses, and to correlate it with BMD diagnostic of osteopenia or osteoporosis (according to the WHO), with the purpose of improving the possible suitable medical intervention.
Material and Methods: 5476 women have studied who have gone to consultations of menopause of sanitary centres public who reunited the requirements. She has been put under a questionnaire that contains, among other parameters, questions on the existence or not of risk factors (18 possible factors of risk) and to which them densitometries DXA has practiced.
Results: The patients have an average of age of 63.0 years (rank of age of 45–86) and OF 6.9; We were with 2714 (50%) osteopenia and 2614 (48%) osteoporosis's ones. Between the osteopenia were 3 or more factors of risk (medium) and equal number between the osteoporosis. The prevalence's factors were: BMI <20 in 18,68%; fractures previous in a 18,26%; sedentarisme in a 30,05%, familiar previous osteoporosis in 12.4% and steroid consumption and inmunosupresors in 9.7%; but also in 20.84% of them without risks factors.
Conclusions: It is important to value data of factors of risk at the time of taking determinations on the intervention to follow in these patients with these bony pathologies, but in a number of patients they had a loss of bone mineral density without these risks factors.
PS-305
FSH LEVELS IN POSTMENOPAUSAL OSTEOPOROTIC WOMEN
M. S. Moggia, M. S. Larroudé, J. C. Morgenstern, M. Perez Sainz, R. Díaz, M. G. Torres Cerino, M. P. Yantorno and Z. Man
Centro TIEMPO – Buenos Aires – Argentina [email protected]
Postmenopausal osteoporosis is a leading cause of morbidity and mortality.
Traditionally, this bone loss has been attributed solely to declining estrogen levels. However follicle-stimulating hormone (FSH) directly enhances osteoclasts formation and function and suggest that elevated FSH contributes to the genesis of postmenopausal osteoporosis.
Objective: To correlate bone mineral density (BMD) and body mass index (BMI) with FSH levels in osteoporotic postmenopausal women.
Materials and Methods: Population: 69 women, mean age 60 years old (51–75), with ≥ 5 years of menopause.
Anteroposterior (AP) lumbar spine BMD was measured by DXA in a Lunar Prodigy densitometer. FSH was meassured by RIA. BMI was determined and women were classified as follows: low weight, <20; normal, 20–25; overweight, 25–30; obese >30.
Variables were correlated with Student test.
Results:A clinically significant negative correlation between BMI and FSH values (p = 0.034) was observed, and also between years of menopause and BMD (p = 0.05). BMD and BMI relation was positive (p = 0.27) and was also positive between BMD and FSH (p = 0.55), but these relations were not clinically significant.
Conclusion: Although FSH levels are proposed as a factor involved in the physiopathology of postmenopausal bone loss, in our population this relation was not confirmed, possibly due to the fact that the number of patients studied was low. BMD major determinant was years of menopause.
PS-306
GYNECOLOGICAL AND ANTHROPOMETRIC FACTORS AS DETERMINANTS OF BONE MASS IN HEALTHY POSTMENOPAUSAL WOMEN
S. Sousa, J. Almeida, R. Passarinho, P. Manso, M. Rodrigues, C. Silva, R. Ribeiro, G. Castro, C. Rodrigues, F. Geraldes, F. Ventura and F. Águas
Maternidade Bissaya Barreto, Coimbra, Portugal
Objective: Many factors have been identified as determinants of bone mineral density and risk factors for osteoporosis. This paper studied the influence of several gynaecological factors (years since menopause – YSM –, age at menarche, parity, breastfeeding, etc) simultaneously with anthropometric (Body mass index – BMI) and lifestyle factors (smoking, calcium intake, physical exercise) as determinants of bone mass in healthy postmenopausal women.
Design & Method: Bone mineral density (BMD) was determined by dual energy X-ray absorptiometry (DXA) at the lumbar spine and hips in postmenopausal women. We selected all women that did DXA in our institution during one year. Subjects were interviewed using a structured questionnaire on age, reproductive history and gynaecological status, height, weight, consumption of tobacco, medication and previous diseases. An initial universe of 772 women was found. Women with diseases and taking drugs that are known to severely affect bone metabolism were excluded (personal history of breast cancer, bowel resection, hypothyroidism and women taking corticosteroids, bone reabsortion inhibitors or on hormone replacement therapy). Data were analyzed with Statistical Package for the Social Sciences (SPSS) version 15 applying chi-square test for categorical variables and T student for numeric variables. A value of p < 0, 05 was considered significant.
Results: Two hundred and thirty six women were included in the study. Mean age was 57 years (±6,85). Osteoporosis according to the classification of WHO (T-score ≤ −2,5 SD) was observed in 40 women (16,9%) in lumbar spine and in 18 (7,6%) in hips. BMD at the lumbar spine and the hips was correlated negatively with age and YSM and in lumbar spine correlated positively with BMI (p < 0,05). Comparing osteoporotic patients with nonosteoporotic according to the age at menarche, the age at menopause, the period of fertility, use of hormonal contraception and lifestyle factors did not highlight an association.
Conclusions: Our data stress the importance of age, YSM and IMC as factors that mainly determines BMD. Other gynaecological and lifestyle factors might have some influence, but statistical significance was not demonstrated.
PS-307
HYDROXYAPATITE IN CALCIUM URINARY LOSS: NEW MODEL?
A. Bazarra Fernández
Juan Canalejo University Hospital Trust. Culleredo, La Coruña, Spain
Consumption of animal protein, grain, and high amounts of milk increases the acidity of the body. Life is a struggle against hydrogen ions. Long-term acid loading in humans causes an increase in renal acid excretion. Proton-pump inhibitors (PPIs), suppress acid production through a different biological mechanism. People taking high doses of PPIs are more likely to break a hip. PPIs interfere with the continuous breakdown and rebuilding of bone. Acid dissolves old or damaged bone, and PPIs limit the acid production.
Dietary protein has a magnitude-dependent anabolic effect on bone, because protein supplies the amino acid substrates for building bone matrix. Contemporary Western diets contain acid precursors in excess of base precursors. Acidosis influences the homeostasis of calcium, partly due to the influence on renal mechanisms.
Scant evidence supports nutrition guidelines focused specifically on increasing milk or other dairy product intake for promoting child and adolescent bone mineralization.
In humans, essential amino acid supplementation increases circulating concentrations of insulin-like growth hormone. The catabolic effect on bone related to the magnitude of the diet's net acid load can offset the anabolic effect of higher dietary protein intakes. Sodium chloride, elevates urinary calcium excretion.
Higher long-term protein intakes are associated with the bone variables as an anabolic factor, whereas higher long-term diet-dependent net acid loads are associated with those variables as a catabolic factor. The net effect proved anabolic but is apparently short of protein's anabolic potential because of the catabolic effect of the positive net acid load that causes calcium urinary loss induced by acidity.
Ca from Ca-rich mineral waters is equivalent to that of milk Ca but the acidogenic action of SO4 is responsible for the increased calciuria.
Consumption of fruits and vegetables has been implicated in lowering net acid excretion. The association between fruit and vegetable consumption and indexes of bone health was first identified within the older population by the alkalizing effect of fruit and vegetable consumption.
Acid/base balance diet is meant along with hydroxyapatite Ca10(PO4)6(OH)2 and oseine as a new παραδείγμα versus calcium carbonate for osteoporosis in calcium urinary loss.
PS-308
INCIDENCE OF OSTEOPOROSIS IN POST-MENOPAUSAL WOMEN WITH LOW BACK PAIN
G. Soro, A. Esparza, M. T. Avilés and F. Baró
Vall d'Hebron Hospital, Barcelona, Spain
Objective: The principal aim of the study was to know the incidence of lumbar osteoporosis in postmenopausal women with low back pain who were attended at the unit of menopause in our hospital. As secondary aims we analyse the incidence of femoral osteoporosis and the radiological alterations in the lumbar column.
Design & Method: We made an observational study. We included all the postmenopausal women we attended between September and December of 2006 who referred low back pain. The demographic characteristics of the sample were analyzed. All the women were sent to make a densitometry study and an X ray examination of the dorsolumbar column.
Results: The sample had a mean age of 65 (±7) years. The mean menopause age was 48 (±5), the mean menarquia age was 13 (±2) and the mean parity of 2,1 (±1,4). We classified women in three groups depending on their densitometry results. The bone mass density (BMD) was measured in proximal femur and lumbar spine by dual-energy X-ray absorptiometry (DEXA) using a Lunar model and we follow the OMS classification to do the different groups. 96 women were studied, 40 had lumbar osteoporosis (41.7%), 44 of them osteopenia (45,8%) and 12 (12,5%) of them a normal lumbar examination. We observed 28 women with femoral osteoporosis (29,2%), 57 (59,4%) with femoral osteopenia and 11 patients (11,5%) with a normal examination. 60 women had a dorsolumbar X ray examination, in 19 (31.7%) it was normal and in 41 (68,3%) radiological alterations were found: 2 (4.8%) vertebral fractures, 4 (9.7%) vertebral crushing, 2 (4.8%) loss of vertebral height, 2 (4.8%) espondilosis and in 31 (75,6) degenerative signs of osteoarthritis.
Conclusion: The low back pain is an important symptom. We saw that women with low back pain had a high percentage of lumbar and femoral osteoporosis and radiological damages.
PS-309
INFLUENCE OF PRIOR PREGNANCIES AND LACTATIONS ON PERIMENOPAUSAL BONE MINERAL DENSITY
F. Quereda, T. Santoyo, S. Fernández-Ibáñez and P. Acién
University Hospital of San Juan/Miguel Hernández University/PAA Institute, Alicante, Spain
Objective: to investigate the possible relationship between number of pregnancies or duration of breastfeeding and bone mineral density (BMD) at the moment of perimenopause.
Methods and Design: Case control study from a database prospectively collected in our Hospital Menopause Unit since 2002. Women who met the following inclusion criteria were included: age 45–55 and BMD determined by DEXA at this time. Patients with any of the following criteria were excluded: prior history of cancer, arthritis, severe chronic disease or bone metabolism related disease, more than two years of difference between densitometry and real date of menopause, prior corticoids use or ignorance about possible HRT use. 237 women were included in this study. Statistical analysis was performed using SPSS 15.0 software.
Results: Some characteristics of included women were: age 49.8 ± 2.7 years, 86.9% had been pregnant with a mean number of pregnancies (>20 weeks) of 2.3 ± 0.9 (1–7). 70% of women had lactated a mean of 2.1 ± 0.9 (1–7) times and for a mean duration of breastfeeding in their life of 8.1 ± 0.9 months (1–60).
We did not find differences in perimenopausal BMD between number of prior pregnancies. However, there were significant differences in Lumbar BMD between duration of lactation. Women who had lactated during less than 12 months had a mean spine BMD of 1130.3 ± 145.5 gr/cm2 (t-score: −0.05 ± 0.12) and those who had lactated longer than one year of their life 1073.4 ± 140.4 (t-score −0.10 ± 0.11) (p < 0.01).
Prevalence of osteoporosis was higher with longer duration of breastfeeding, but differences were not statistically significant (2.8% of women who did not lactated, 4.7% of those who did it for less than one year, and 13.6% if longer than 12 months).
Correction for time with estrogenic deprivation (HRT use or not before densitometry if it was done after menopause) did not change these results, but main differences were not found in perimenopausal women without time of estrogenic deprivation but in women with more than one year with estrogenic deprivation, suggesting that prior breastfeeding longer than one year acts as a risk factor for greater and faster loss of BMD along the first postmenopausal or estrogen-deprivated year.
Conclusions: Our data suggest that prior breastfeeding longer than one year of woman life can reduce the level of spine BMD with which women affront perimenopausal transition. The small difference that we have found suggest a low clinical significance of this influence, but differences in prevalence of osteoporosis, although non-statistically significant, clearly suggest that it could be important for some women, perhaps for those at special risk or more sensible to bone loss with breastfeeding.
PS-310
INGESTION OF CALCIUM IN CLIMATERIC WOMEN
A. Fdez Pareja, E. Hdez Blanco, M. C. Magro Domingo and A. Correas Garcia
Centros Madrid Salud (Cms). Ayuntamiento De Madrid
Objetives: To check out the average amount of calcium ingested by a set of women treated in the menopause municipal program developed in the Municipal Health Center (MHC) in Tetuan and Hortaleza (Madrid).
Material and Methodology: 421 Postmenopausal women aged between 43 and 58, and averaged 50,56 years old, with different education levels and employment areas.
All the patients were provided with a questionnaire about alimentary habits (CFCA) based on the table of aliments composition designed by the Spanish Ministry of Health.
The questionnaire was intended to value the weekly frequency of calcium consumption and was designed as an exhaustive list of products codified in portions where the amount of calcium was well known (i.e. a glass of full-fat milk contains 250 mg of calcium).
The participants filled in the number of portions consumed in a week and from this data the diary calcium ingestion was calculated as the Σ (number of weekly portions X calcium mg per portion)/7.
Results: The average alimentary calcium ingestion obtained was 965,6 mg per day (standard deviation: ± 462,4 and data range: 226–3534) This data is very similar to the 991 mg/day obtained in the INDICAD 2001 study about the calcium ingestion in the adult population.
The results of grouping the population of the study by means of their consumption level follows the distribution:
0–500 mg/day—24(5,8%).
501–800 mg/day—134(31,9%).
801–1000 mg/day—113(26,8%).
1001–1200 mg/day—66(15,7%).
1201–1500 mg/day—58 (13,7%).
>1501 mg/day—26(6,1%).
Conclusions: A high percentage of the women interviewed ingests less calcium than the 1200–1500 mg/day minimum recommended by the Asociación Española para el Estudio de la Menopausia (AEEM) and by the North American Menopause Society (NAMS).
As the calcium is one of the basic nutrients for the prevention and treatment of osteoporosis, this fact stresses the importance of the CFCAs and therefore how important is to recommend good alimentary habits and suggest the ingestion of calcium supplements by the doctors to people who present an insufficient consumption.
PS-311
LEVEL OF THYROID HORMONES IN POSTMENOPAUSAL WOMEN WITH OSTEOPOROSIS
M. Milivojevic1 and L. Nikolic2
1Institute of Medical Biochemistry, Clinicl Centre of Serbia, Belgrade; 2Institute for Gynecology and Obstetrics, Clinicl Centre of Serbia, Belgrade
Introduction: Osteoporosis (OP) is generalized disorder of bone tissue structure. It is a systemic disease characterized by reduced bone mass and changes microarchitecture of bone tissue. In menopausal women, the reduction of ovarian functions leads to loss of bone tissue, and, therefore, the majority of women meet the criterion of OP before 70 years of age.
Objective: The aim of the study was to measure the level of thyroid hormones and standard biochemical parameters in postmenopausal women with osteoporosis.
Method and Material: In 38 patients, who were verified for osteoporosis by bone mineral density (BMD) measurement, the level of biochemical blood components was determined, as follows: TSH, FT, T, PTH, alkaline phosphatase (ALP), Ca ionized, and cholesterol. Statistical data processing of the results obtained included χ2 test and ANOVA.
Results: Out of 38 patients, 23 (60.5%) had TSH over 2.5 mIU/L. FT4 and T4 were within reference limits in all patients: 16.5 ± 3.17 μmol/L and 89.7 ± 29.5 μmol/L, respectively. PTH level was normal in 30 women (79%) (p < 0.01), elevated in 7 (18%) and decreased in 1 woman (3%). ALP was within limits (89.3 ± 40.82 μmol/L), but the respective value was closer to lower limit in the majority of subjects, suggesting the lower activity of osteoblasts. Ionized Ca value was within limits in 21 females (55%), lower in 16 (42%) and higher in 1 (3%) patient. Elevated cholesterol level was noted in 26/38 (68%) patients (p < 0.01).
Conclusion: A considerable number of individuals with osteoporosis had higher values of cholesterol and TSH.
PS-312
MONTHLY 150 mg ORAL IBANDRONATE THERAPY IN POSTMENOPAUSAL OSTEOPOROSIS: 18-MONTH RESULTS
P. V. Petropoulos, D. Rousso, G. Mavromatidis, J. Tsibanakos, S. Masouridou and V. Karayannis
3rd Dep. of Obstet. Gynecol. Aristotl University of Thessaloniki, Thessaloniki, Greece
Introduction: Postmenopausal osteoporosis is a skeletal disorder characterized by compromised bone strength leading to an increased risk of fracture, which imposes a considerable and growing socioeconomic burden. Ibandronate is a potent nitrogen-containing bisphosphonate, with proven antifracture efficacy for monthly oral administration. Bone turnover markers (BTM) and bone mineral density (BMD) are often used as surrogate markers for fracture. This report presents data on the effects of monthly oral ibandronate therapy on BMD and C-telopeptide serum levels (sCTX).
Design and Methods: A total of 97 women (55–67y) with postmenopausal osteoporosis (lumbar spine L2-L4 BMD T-score ≤ −2.5 and ≥ −3.6) were assigned for the first time to oral ibandronate, 150mg monthly. All participants received daily oral calcium 500mg and vitamin D 400IU. Twenty two patients with postmenopausal osteoporosis, who did not agree to the treatment constituted the control group. Lumbar spine BMD were measured by DXA, at the beginning, after 12 and 18 months. Serum levels of CTX, a biochemical marker of bone resorpsion, were measured at baseline and after 6, 12 and 18 months.
Results: Three women (3,9%) discontinued therapy, due to side-effects (myalgia nausea, vomiting, pyrexia). The mean percent increase from baseline (beginning of treatment) in lumbar spine (L2–L4) BMD was 5.01% after 12 months and 6.31% after 18 months therapy. The mean percent increase from baseline in total hip BMD, at the same time was 3.21% and 3,96% respectively, in comparison to pre-treatment levels. The mean percent serum levels of CTX decrease was −72.2%, −74.8% and −69.9% at 6, 12 and 18 months respectively, in comparison to pre-treatment values. Among the women in the control group, 16 of them presented a small increase in the sCTX levels and degrease in the LS T-score, 2 presented vertebral fractures, while 4 did not present changes in their condition.
Conclusion: This data confirm that the majority of patients achieve clinically meaningful responses to once-monthly oral ibandronate in postmenopausal osteoporosis, with well-tolerated therapy.
Once-monthly oral ibandronate 150mg rapidly normalizes the elevated rate of bone turnover and achieves substantial decreases in sCTX. Also most patients achieved substantial gains in BMD.
PS-313
NEW TIMES NEW RESEARCH ΠAP'AΔEIΓMA: OSTEOPOROSIS RESEARCH
Antonio Bazarra Fernández
Juan Canalejo University Hospital Trust, La Coruña, Spain
Bones are composed of tissues being not a uniformly solid material, has some spaces between its hard elements. Embedded in a mineralized matrix to give bone strength, and collagenous fibers and ground substance to give bone flexibility, with spaces and canals, symmetry and asymmetry, with microsystems, isotropy and anisotropy and variety of cross-section. Osteoporosis is a big problem. So, to measure strength bone involve a great deal to cope with. Dual energy X-ray absorptiometry (DXA) has served as a fit surrogate for the measurement of bone strength. By reason of the two-dimensional nature of DXA, assumptions must be made regarding the tridimensional nature of the bones involving a great deal to cope with. Therefore it is deduced, that this method seems to be very sensitive to error, and it is necessary to know how to deal with these errors, especially with the systematic errors introduced by using a parameterized model. Even though a high concordance between the densitometers was observed on a single measurement occasion, a significant discordance in longitudinal changes in BMD was observed. So, a mathematical, physical and physiological 5-dimensional model must be developed in order to gauge bone properties including geometry(2-dimensional DXA), space, time, motion and stress with some portable-computer-devices in base of mouse models for quantitative trait loci (QTL) analyses. In the field of skeletal micro-structure, μCT has proven to be an invaluable imaging tool and the use of high resolution peripheral quantitative computed tomography (HR-pQCT), in vivo nanotomography and nanofractography, must be considered for studies of bone disease and its treatment, and here new research παραδείγματα for new times and new pathologies must stay in.
PS-314
OBSERVACIONAL STUDY IN POSTMENOPAUSAL WOMEN WITH LOW BONE DENSITY: THE SPREAD OF BONE SPECIFIC MEDICATION
J. Neves, A. P. Candeias, J. Pauleta, A. M. Coelho and L. M. Graca
Obstetrics, Gynecology and Reprodution Medicine Department, Santa Maria Hospital Lisbon Portugal
Objective: Diagnosis and risk for fracture have limitations in postmenopausal women with low bone mass (LBMD). Relation between risk fracture and bone mineral density (BMD) is not very well established in women less than 65 years old. So, the managment for fracture risk reduction in those population is not yet defined, but there was a suprising finding reporting that the risk for fracture is similar in postmenopausal women less or above 65 yeasr old. This finding is an interesting challenge for BMD screening and in presence of BMD abnormalities, preventing measures should be taken. The purpose of this study was the reporting of bone specific medication in postmenopausal women with LBMD.
Design & Method: We studied 95 postmenopausal women with universal criteria for LBMD. Data are represented as mean ± sd and distributed in absolute and relative values.
Results: Clinical and demographic data are the following: age 59.5 ± 7.57 years; menarche 13.2 ± 1.77 years; menopause 48.8 ± 4.80 years; years from menopause – 10.7 ± 7.4; body mass index 28.3 ± 11.14 Kg/m2 and waist-circunpherence 88.9 ± 11.99cm. The spread of medication was: raloxifen (n = 47; 49.4%); hormone therapy (HT) (n = 12; 12.6%); calcium and vitamine D (n = 13 13.6%); bisphosphonates (n = 10; 10.5%). Calcium and vitamine D supplementation was refered on 57 cases (60%). No medication was reported on 8 women (8.4%). No calcium and vitamine D supplementation was apointed in 15 cases (15.7%), with the following distribution - raloxifen 13 cases (13.6%) and residronate, 2 cases (2.1%). In women whith present or past use HT, the therapy duration was 48.6 ± 30.75 months.
Conclusions: In this sample of postmenopausal women with LBMD, the bone specific medication most used was raloxifen and supplementation of calcium and vitamine D.
PS-315
OBSERVACIONAL STUDY IN POSTMENOPAUSAL WOMEN WITH LOW BONE MASS: BONE MINERAL DENSITY VARIATION 24 MONTHS AFTER THE ONSET OF MEDICATION
J. Neves, A. P. Candeias, J. Pauleta, A. M. Coelho and L. M. Graca
Obstetrics, Gynecology and Reprodution Medicine Department, Santa Maria Hospital Lisbon Portugal
Objective: Bone mineral density (BMD) values are the universal standard parameters for osteoporosis or low bone mass (LBMD) definition. Age, prior fracture and higher bone mineral makers are the most important factors for fracture risk calculation. In postmenopausal women with osteoporosis or LBMD, age is crucial for risk of fracture and can act independently.
Design & Method: We studied 81 postmenopausal women with one risk factor for osteoporosis and with universial criteria for LBMD; variation on BMD was evaluated, basal and 24 months after medication and the population was divided in two groups based on age – Group A, less than 60 yeasr and Group B, 60 years or more. Data are represented as mean ± sd; Student t test and test for frequence variation were used for statiscal comparasion.
Results: Clinical and demographic data are the following:
Conclusions: In this sample of postmenopausal women with LBMD, there was a positive variation for the BMD, 24 months after the onset of medication, namely on FN; after this period of time, mean BMD values for FN are in the normal range. The variation is more pronunced in women less than 60 years.
PS-316
OSTEOCALCIN AND ESTRADIOL – BONE MARKERS REMODELING IN POSTMENOPAUSAL OSTEOPOROSIS
Maria Puschita1, Camelia Vidita Gurban2, Camelia Ciacli1 and Doina Drugarin2
1Vasile Goldis West University, Arad; 2Victor Babes University of Medicine and Pharmacy, Timisoara
Introduction: Estradiol (E2) and Osteocalcin (OC) play an important role in the regulation of bone turnover, stimulating the bone formation by the osteoblasts.
Objectives: The aim of this study was to determine serum levels of Estradiol and Osteocalcine which are elevated in postmenopausal women with osteoporosis.
Material & Method: The study was carried out on two cohorts of patients with postmenopausal osteoporosis (depending on estrogenic deprivation) by comparing them with the control group (menopausal women without osteoporosis). Serum levels of the markers were measured by ELISA technique and evaluation Bone Mineral Density (BMD) were analysed using DEXA method assessment T scores (sT spines).
Results and discussion: Cohort 1 (under 15yr of the estrogenic deprivation): OC serum levels were 20.12 ± 0.87 ng/ml, E2 serum levels were 28.32 ± 1.78 pg/ml, and sT spines were 3.63 ± 0.65 DS. Cohort 2 (over 15yr of the estrogenic deprivation): OC serum levels were 15.12 ± 1.55 ng/ml, E2 serum levels were 19.66 ± 1.23 pg/ml, and sT spines were −3.71 ± 0.36 DS. Control group: OC serum levels were 16.22 ± 1.62 ng/ml, E2 serum levels were 43.07 ± 4.04 pg/ml, and sT spines were −1.78 ± 0.11 DS.
Conclusion: The serum levels increased Osteocalcin which demonstrated osteoblasts activation. The decreased serum levels of Osteocalcin demonstrated osteoblasts apoptosis stimulation, associated with estrogen deficiency in postmenopausal women. Bone turnover will be significantly increased, thus producing a decrease of bone formation and increasing bone resorting. This imbalance favors the appearance of osteoporosis.
PS-317
OSTEOPENIA AND FRACTURES
F. Baró1, E. Rodríguez Bueno2, M. Guinot3, L. Esteban, I. Ibars4, E. Ruiz6 and B. Roca7
1Hospital Materno-Infantil Vall d'Hebron, Barcelona Spain; 2PASSIR Sant Andreu, Barcelona; 3Hospital Sant Pau, Barcelona 4PASSIR Casgemes, Badalona; 6PASSIR Antoni Creus, Terrassa, Barcelona; 7Hospital Terrassa, Barcelona, Spain, Group Study Menopause and Osteoporosis in Cataluña (GEMOC), Barcelona, Spain
Objective: To assess the relation between osteopenic women, prevalence of fractures and its treatment.
Material and Methods: A prospective study with a sample of 2714 women between 40 and 73 years has been carried out, with an average age of 60 years (6,9 SD), in which their bone situation was quantified (DEXA). The inclusion criteria were a BMD between equal or inferior T-score to −1,5 SD and −2,5 SD or previous fractures to their BMD.
Results: After analysing the results it was observed that 2714 patients presented osteopenia, 30% did not have any factor risk and 16% had suffered a fracture. 60% of which had been treated, whereas 40% had not been previously treated. After the visit 100% of the women with previous fracture were treated.
Commentary: The existing correlation between osteoporosis and fractures has been known and established for a long time in scientific studies. Nevertheless, the results obtained in our study, reflect that 16% of women's fractures are osteopenic.
Conclusions: The BMD does not indicate bone resistance, which is demonstrated in our sample in which 16% of the population with osteopenia, fractures took place. It should be remembered that a previous fracture is a powerful indicator of a new fracture. Our group highly recommends initiating early pharmacologic treatment in this group of patients with prevalent o clinical fractures together with an exhaustive study of these patients.
PS-318
PARTICULARITIES OF NUTRITION AND BONE TISSUE FUNCTIONAL STATE IN POSTMENOPAUSAL WOMEN
V. Povoroznyuk and N. Grygoryeva
Institute Of Gerontology AMS Of Ukraine
Objectives: There has been increasing evidence that balanced diet and maintained optimal status significantly reduce morbidity and mortality. High calcium intake prevents bone loss and osteoporotic fractures in postmenopausal women although the association is less obvious in the first years after menopause.
Design and Methods: We've investigated the influence of diet on bone tissue functional state and anthropometric data in 247 postmenopausal women. Bone tissue functional state was determined by ultrasound densitometry (I-osteoporosis, II-osteopenia, III-normal bone tissue).
Results: The diet of Ukrainian postmenopausal women is characterised by a reduced intake of proteins, especially animal; fats, especially vegetable; vitamins, main mineral macro- and microelements. The intake of main mineral element, necessary for bone turnover - calcium - is lower than recommended. Results for main nutrients are presented in the table 1. It is evident that all elements essential for the bone are below the recommended values. It is advised that the diet must be rich in proteins, calcium and vitamin D.
PS-319
PANORAMIC RADIOGRAPHS IN ASSESSMENT OF THE BONE MINERAL DENSITY
E. Balcikonyte1 and V. Alekna2
1Institute Odontology, Faculty of Medicine, Vilnius University, Lithuania; 2Faculty of Medicine, Vilnius University, Lithuania.
Objective: The aim of the study was to evaluate the diagnostic efficacy of the panoramic based mandibular indices and to determine whether they correlate with bone mineral density of the lumbar area.
Design & Method: 130 women participated in the study. None of the participants were known to have endocrine, metabolic, skeletal disorders. The values for bone mineral density of the lumbar area L2-L4 were determined by a dual-energy x-ray absorptiometry. Each woman was classified into one of three groups according to T-score. The mandibles were examined on panoramic images. Two measurements of mandible were recorded: the height of the mandibular inferior cortex (CI) and Mandibular Cortical Index (MCI). MCI was assessed according to the following criteria (Klemetti et all.): C1) the endosteal margin of the cortex was even sharp on both sides; C2) the endosteal margin showed semilunar defects or seemed to form endosteal cortical residues; C3) the cortical layer formed heavy endosteal cortical residues and was clearly porous. The results of the study of panoramic images were compared with bone mineral density (BMD). Statistical analysis was performed using STATISTICA for Windows. Analysis of variance (ANOVA) was performed to determine group differences in BMD. Person correlation coefficients were used to identify relationship between variables.
Results: 130 women aged 30.1–79.2 yr (mean 60.4) were examined. Of all participants 22.3% (n = 29) women were defined as osteoporotic, 49.2% (n = 64) as osteopenic and 28.5% (n = 37) as normal. The endosteal margin of the cortex even sharp on both sides was in 13.9% (n = 18) women, in 61.5% (n = 80) the endosteal margin showed semilunar defects or seemed to form endosteal cortical residues and in 24.5% (n = 32) the cortical layer was clearly porous. MCI correlated positively with CI and with the BMD (p < 0.01). Correlation between CI and BMD is high significant (p < 0.01).
Conclusion: MCI is a simple three-graded classification of changes in the bone cortex, which is enable to distinguish normal and osteopenic or osteoporotic women. Correlation between mandibular cortex groups also between the height of cortical bone of mandible and the bone mineral density were significant. The efficacy of the panoramic based mandibular indices in diagnosing osteopenia/osteoporosis is high.
PS-320
PHALANGEAL RADIOGRAPHIC ABSORPTOPMETRY AS A SCREENING TOOL FOR OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN
H. Sarkawi1, H. Suharjono1, N. Adeeb2, T. Suzet3, R. Annuar4, S. Mohd Aris5 and M. M. N. Haizal5
1Department of Obstetrics & Gynaecology, Sarawak General Hospital, Sarawak, Malaysia; 2Department of Obstetrics & Gynaecology, Hospital Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia; 3Department of Radiology, Sarawak General Hospital, Sarawak, Malaysia; 4Department of Medicine, Universiti Malaysia Sarawak, Sarawak, Malaysia; 5Department of Obstetrics & Gynaecology, Universiti Malaysia Sarawak, Sarawak, Malaysia
Objective: The aim of this study was to evaluate the role of phalangeal radiographic absorptiometry (RA) as a screening tool for osteoporosis in postmenopausal women compared to the gold standard, Central Dual Energy X-ray (DEXA). The secondary aim was to assess the risk factors for osteoporosis among women attended to the gynaecological clinic of Sarawak General Hospital.
Design & Method: A prospective study was conducted at Sarawak General Hospital, Sarawak. Subjects where all postmenopausal women, aged 45 and above, attended our Gynaecology Specialist Clinic. All subjects were given a questionnaire which listed their demographic details, risk factors and protective factors for osteoporosis. All patients were sent for bone mineral density (BMD) assessment for the non-dominant hand by phalangeal RA; and BMD of the hip, spine and whole body by central DEXA. Pearson correlation coefficient and Bland Alman Test were used for analysis with the level of significant set at p < 0.05. Valadity and predictivity values of phalangeal RA were compared with central DEXA.
Results: A hundred subjects participated in the study. Out of this hundred, nine subjects were diagnosed osteoporosis based on the BMD of the hip by central DEXA. There was a significant correlation between T-score of non-dominant hand by phalangeal RA and T-score of hip, spine and whole body by central DEXA, with strongest correlation found with the T-score of the whole body (r = 0.682, p = 0.000). Bland Alman plots showed that T-score by phalangeal RA agreed best with T-score of whole body. In comparison to central DEXA, phalangeal RA had a good specificity (88–91%), good negative predictive value (94–99%), moderate sensitivity (44–71%) but poor positive predictive value (8–38%). Hormone replacement therapy (HRT) was protective against osteoporosis (r = −0.285, p = 0.004). However, Low Body mass index (BMI).
Conclusion: Based on the results, Phalangeal RA was shown to be comparable to central DEXA, in particular the whole body measurement by the central DEXA. Despite a good specificity and negative predictive value, it has poor positive predictive value. Thus, this showed that phalangeal RA has a role as a screening tool for osteoporosis in postmenopausal women. Confirmation, however, of the diagnosis should be done by central DEXA. Future interest includes population based study and long-term follow-up of abnormal subjects screened by phalangeal RA in order to evaluate its role as a predictor of future fracture risk.
PS-321
PLACEBO CONTROLLED, RANDOMISED, DOUBLE BLINDED CLINICAL TRIAL TO ASSESS THE EFFECTS OF A CONTINUOUS COMBINED LOW DOSE TRANSDERMAL HORMONE REPLACEMENT THERAPY COMPARED TO A COMBINATION WITH MONOFLUOROPHOSPHATE OR PLACEBO ON BONE MINERAL DENSITY AND QUANTITATIVE ULTRASONOMETRY
M. Ziller, A. Kauka, D. Cassebaum, V. Ziller and P. Hajdi
Phillips-University Marburg, Dep. Of Gyn. Endocrinology, Reproductive Medicine And Osteology, Hessen, Germany
Introduction: The effectiveness of hormone replacement therapy (HRT) and fluoride therapy on bone turnover and BMD is well documented. Both therapeutic options have been proven to be cost effective with a well established side effect profile. In 1995, a study of Christiansen et al. showed significantly higher increase of BMD in the combination of HRT and fluorides compared to HRT or fluorides alone. Since then this approach was not further investigated. The aim of this study was to investigate the effects of HRT with and without fluorides on BMD and QUS compared to placebo in a randomised controlled, double blinded clinical trial.
Material and Methods: 113 postmenopausal women with a mean age of 60,0 (±5,3 Years) participated in the trial. After randomisation, patients were treated with a continuous, combined transdermal HRT (50 μg E2 and 140 μg Norethisteronacetat) or with HRT in combination with Monofluorophosphate (76mg) or with placebo (600mg Calcium and 800 IE Vitamin D) alone. At baseline patient history including all relevant risk factors for osteoporosis, physical examination including gynaecological examination, transvaginal ultrasound and a mammography were performed. All women with a history of Osteoporosis or with treatments or diseases known to affect bone metabolism were excluded. BMD was assessed by DXA with a Prodigy device (GE/Lunar). QUS was assessed with an Achilles + device (GE/Lunar) as well as with a Bone Profiler (IGEA).
Results: Data are analysed at the moment and results will be available at the meeting.
Discussion: The therapeutic regimens used in the trial have proven to be cost effective with a well established side effect profile. Or results will evaluate if a combination therapy reveals superior result compared to mono therapy. If so, prospective trials should be performed to investigate fracture risk reduction efficacy.
PS-322
PREVALENCE OF OSTEOPOROSIS AND VITAMIN D DEFICIENCY IN A SEMIURBAN SOUTHERN INDIAN POPULATION
T. V. Paul, N. Thomas, M. S. Seshadri, R. Oommen, A. Jose and Mahendri
Christian Medical College & Hospital, Vellore, India 632004
Objective: To determine the prevalence of osteoporosis and vitamin D insufficiency in a semiurban population in Southern India.
Design and Methods: Ambulatory post menopausal women were studied from a semi-urban location in Vellore Town,Tamil Nadu, India. Out of 7082 women in this area, 1040 were postmenopausal. The number of subjects to be studied to detect a prevalence of 20–40% with 95% confidence was 145. One hundred and fifty subjects [ 30 clusters of 5 each ] were randomly selected for the study and informed consent obtained. Bone mineral density was measured using QDR 4500 Hologic DEXA. 25 (OH) Vitamin D was measured by radioimmunoassay using Dia Sorin kit [Stillwater, Minnesota]. Serum calcium, phosphorus, albumin, creatinine and alkaline phosphatase were measured by Hitachi model 911 autoanalyzer.Vitamin D status was classified as per Lipp's criteria. Chi square was used as test of proportions and multiple logistic regression to determine risk factors for osteoporosis.
Results: Prevalence of osteoporosis was 48% at the lumbar spine, 16.7% at the femoral neck and 50.4% at either site. Dietary calcium intake (399 ± 190 mg/24 h) was much lower than the recommended intake. In multiple logistic regression analysis BMI> 30 was found to have a protective effect (odds ratio 0.89, 95% CI 0.81–0.97) at the lumbar spine and at the femoral neck (odds ratio 0.86, 95% CI 0.76–0.96). BMI showed a significant positive correlation with BMD at lumbar spine and at femoral neck (r = 0.4, P<0.0001 at both sites). Parity showed a significant negative correlation with BMD at the lumbar spine (r = −0.25, P<0.05 ) and at the femoral neck (r = −0.227, P < 0.01). BMD at the femoral neck was significantly lower (mean 0.657 vs 0.694 gm/cm2, P < 0.05) in vitamin D insufficient subjects as compared to vitamin D sufficient subjects.
Conclusions: In this community based study, a high prevalence of osteoporosis and vitamin D deficiency was observed in ambulatory post-menopausal women and the average dietary calcium intake was found to be only 40% of the recommended intake. Calcium and vitamin D supplementation on a mass scale is probably a beneficial intervention and should certainly be undertaken before initiating bisphosphonate therapy.
PS-323
PROFILE OF PATIENTS WITH FIBROMYALGIA ATTENDED AT A UNIVERSITY HOSPITAL MENOPAUSE UNIT
F. Quereda, T. Santoyo, M. I. Conca, S. Fernández-Ibáñez, M. Abad and P. Acién
University Hospital of San Juan/Miguel Hernández University/PAA Institute. Alicante. Spain
Objective: To describe clinical profile of patients with fibromyalgia attended at a Hospital Menopause Unit, and to investigate if some differences exist among patients with or without fibromyalgia in the context of perimenopausal management.
Methods and Design: Descriptive analysis and case-control study from a database prospectively collected in our Hospital Menopause Unit since 2002. Only were accepted as patients with fibromyalgia those that had been diagnosed out of the Unit and by a trained specialist (usually rheumatologist). 729 women were included in this study (cases (n = 42) and controls (n = 687)). Statistical analysis was performed using SPSS 15.0 software.
Results: Prevalence of fibromyalgia at our Menopause Unit was 5.8%. Mean age of these patients was 51.2 ± 5.1 (41–63) years versus 49.8 ± 7.2 (27–77) for the control group (not significant). Age at menopause was 49.1 ± 3.8 years versus 46.2 ± 6.0 (p < 0.05) what means that women with fibromyalgia did not come to the Unit for early menopause. We found higher prevalence of severe symptoms and lower of being asymptomatic in fibromyalgia, but these differences were not statistically significant (64.7% versus 55.7% moderate-severe symptoms, 11.8 versus 22.5% asymptomatic women). There were not differences in surgical menopause rate or reason of consultation, but women with fibromyalgia were more likely referred from rheumatologist than controls (11.8% versus 1.0%, p < 0.01). Finally, analysis of co-morbidity showed that women with fibromyalgia had higher prevalence of depression (33.3 versus 13.0%, p < 0.01), higher (but not significant) of other rheumatologic disease (7.1 versus 3.1%), osteoporosis (16.7 versus 10.9%) and similar rate of prior breast cancer, other cancer, prior endometriosis (11.9 versus 9.8%), or for example urinary incontinence.
Conclusions: Fibromyalgia is a relatively common syndrome in clinical practice at a Menopause Unit. Women suffering fibromyalgia seemed to have natural menopause at usual age, do not have higher rate of surgical menopause, and were more derived from rheumatologist probably looking for help to improve the already affected quality of life of these women in perimenopausal period. Association of this syndrome with depression is clear but it is unknown whether this is secondary to fibromyalgia or independent. In any case, our data suggest that perimenopausal transition in women with fibromyalgia require equal, or perhaps higher, attention than other patients usually attended in a Menopause Unit.
PS-324
PROJECT: BONE HEALTH PREVENTION
S. Lima1, V. Chijani2, J. Hernandez3, A. Aleman4 and A. Vaglio5 and cols, Study group of osteopaties of the Uruguayan Society of Rheumatology (GEOSUR) Montevideo. Uruguay
1Prof. Adj. Gynecologyc.Clinic of School of Medicine of Republic, Member study group of investigation in osteopaties of the Uruguayan Society of Rheumatology, Prof. Private School of Medicine Claeh; 2,3Rheumatologists, Members study group of investigation in osteopaties of the Uruguayan Society of Rheumatology; 4Gynecologist, Epidemiologist Member study group of investigation in osteopaties of the Uruguayan Society of Rheumatology; 5Genetist, Pediatrics, Member study group of investigation in osteopaties of the Uruguayan Society of Rheumatology
Objectives: Osteoporosis is a well-know morbimortality with a high incidence world wide. In our country about 70% of the population older than 50 years old suffers from osteopenia or osteoporosis.
Due to the importance of the period of higher acquisition of bone mass, during childhood and adolescence we carried out research at primary and secondary schools, to know the nutritional habits, physical activities, toxic habits among children and adolescents, which are factors of high impact in the bone mass.
Design and Method: We made a survey of the factors to be studied in public and private schools in the capital city and in the country.
The surveyed children, with average age of 9, were 573, with similar percentages in both genders. The surveyed adolescents were: 1050, average age 15,7years old: 58% female, 42% males.
From the children's group: 16% do not have milk, 57% have milk below the minimum requirements, 45% do not do any physical activity.
From surveyed children group: 17% do not have breakfast, 4% do not have lunch, 13% do not have afternoon snack, and 8% do not have dinner.
We registered a high consumption of soda cola.
The group of adolescents, 25% do not have milk, 48% have milk below the minimum requirements. Only 70% have daily breakfast, 80% have soda cola, alcohol consumption in more than 50%. More than 50% do rare or no weekly physical exercise.
Results: Considering the results where we registered a low consumption of milk in the young population, little physical activity, high consumption of non adequate or toxic nutrients (alcohol, tobacco), we made an educational project in the primary schools. We organized educational centers and control centers. In the educational centers we gave three-month courses about bone health to teachers and parents. After that we evaluated the eating and the physical activities habits of the children in those institutes. The difference in the consumption of milk and the physical activities was significant.
In the control centers there were no significant changes in both habits.
Conclusions: the results obtained in this project let us state the importance of education in the younger population regarding nutritional habits, physical activities, as well as the quitting of toxic habits, with the purpose of optimizing the peak of bone mass, and decreasing the future risk of osteoporosis fractures. The extension of this education to there homes also reassures the policy of preventive actions for the adult population.
PS-325
RISK FACTORS ASSOCIATED WITH OSTEOPOROSIS IN SPANISH POSTMENOPAUSAL WOMEN: THE BENEFIT OF MEDITERRANEAN AND ATLANTIC DIETS
A. Santalla1, N. Mendoza1, F. Vázquez2, T. Martínez-Astorquiza3, F. Quereda4, R. Sánchez-Borrego5, F. Morón6, A. González6 and J. Presa1
1Hospital Virgen De Las Nieves, Granada, Spain; 2Clínica GEOGA: Lugo, Spain; 3Sanatorio Bilbaino, BIlbao, Spain; 4Hospital San Juan, Alicante, Spain; 5Clinica DIATROS, Barcelona, Spain; 6Genética estructural, Neocodex, Sevilla, Spain
Different studies have demonstrated the importance of the Mediterranean diet for the prevention of osteoporosis. In Spain there are other remote regions of the Mediterranean area, but have a lifestyle and diet similar. The aim of this study is to analyze whether these protective factors for osteoporosis found in the Mediterranean diet also appear in the Atlantic diet (Cantabrian cornice).
Patients and Methods: A observational multi-centric study was carried out with 1692 postmenopausal women from 5 spanish hospitals, two in the north (Lugo and Bilbao) and three in the Mediterranean area (Alicante, Barcelona and Granada). Complete clinical data and femoral and lumbar densitometry was obtained from participants.
Women were separated into two groups according to their origin: 345 from the cornice Cantabrian and the remaining 1347 from the Mediterranean area. In turn, they were separated in another 3 subgroups depending on densitometry results: osteoporosis, osteopenia or normal.
Results: Known risk factors (lower weight, size, early menopause and shorter fertile interval) were associated with lower BMD in both populations. Moreover, there is an inverse relation between eating fish, milk, fruit, cereals and vegetables and developing osteoporosis in both populations(p < 0.05). In the same way, smoking cigarretes and eating red meat are risk factors for osteoporosis in all postmenopausal women (p < 0.05). However, moderate alcohol consumption was a protective factor for osteoporosis in women in the Mediterranean area but not in the Atlantic area.
In addition, Mediterranean women had more weight (67.75 vs 60.9 Kg, p < 0.05) and BMI (27.5 vs 24.4, p < 0.05) than Atlantic.
Conclusions: Our study confirms the importance of already known risk factors for osteoporosis. Moreover, we chose the beneficial effects of eating food included both in the Mediterranean and Atlantic diets, especially the consumption of fish, fruit and milk. Some protective factors for osteoporosis, such as moderate alcohol consumption, are not in women's Atlantic area, perhaps because of the smaller sample.
PS-326
SURVEY OF AWARENESS OF ROLE OF CALCIUM SUPPLEMENTATION IN COMMON WOMEN OF NAGPUR, A CITY IN INDIA
Seema Kanetkar
Shrushti Menopause Clinic, Nagpur, Maharshtra, India
Objectives: To study the awareness of role of calcium supplementation in common women of Nagpur, a city in India.
Design and Method - One hundred women attending a women's meet organized by a local women's organization on world women's day were asked to fill up a questionnaire containing various aspects regarding Calcium Supplementation in menopause. A scoring system was adopted. An informative lecture on “Importance of Calcium in woman's Health” was later on delivered to the audience. In the lecture stress was laid on the importance of Calcium in various stages of a woman's life including puberty, pregnancy and menopause. The other important functions of calcium apart from bony health like blood coagulation and muscle contractility were also highlighted. At the end importance of exercises was also stressed upon. Myths about Vitamin D as adjuvant with Calcium were also cleared.
Results: 60% of the audience were between 35 to 45years of age and only 28% were of more than 45 years of age.96% of them were married and rest were unmarried.28%of them had their hysterectomy done.
About 88% of the women knew what menopause is, but were not aware of the changing scenario about quality of life after menopause. 86% of them were aware about functions of Calcium but only 68% women were aware of Osteoporosis.78% of them were aware of dietary sources of Calcium. 24% had the knowledge of HRT and 62% were well informed about Calcium Supplementation. 64% were aware of Soya and other isoflavones. Amongst the audience 88% were aware about the importance of exercises.
Conclusions: The common women of India are not fully aware of the key measures to be adopted for a healthy menopausal achievement. Their attitude towards Calcium Supplementation and fitness is very casual and they are ignorant about the latest medicinal advances available even today.
PS-327
THE DECLINE OF NON-SHBG BOUND SEX STEROIDS IS ASSOCIATED WITH INCREASED BONE TURNOVER AND DECREASED BONE DENSITY IN BRAZILIAN AGING MEN
Maria Lucia Farias, Renata Lopes and Claudia Coeli
Federal University Of Rio De Janeiro, Brazil
Objective: The aim of this study was to evaluate the variations of sex steroids along aging and their influence on bone turnover and bone loss in a sample of Brazilian men. Methods: Serum testosterone (T), estradiol (E2), sex hormone binding globulin (SHBG) and the biochemical marker of bone turnover carboxyterminal cross-linked telopeptide of type I collagen (ICTP) were measured in 104 men aged 50–93 yr. Free and bioavailable sex steroids (FTI, FEI, BioT and BioE2) were calculated. Bone mineral density was measured by DXA at the lumbar spine (LS BMD) and femoral neck (FN BMD). Non-parametric analysis and Poisson regression models were used.
Results: Significant increases in SHBG and ICTP and decreases in body mass index (BMI), FN BMD, FTI, FEI, BioT and BioE2 were observed with decades (p < 0.003 for all analyses). ICTP was inversely correlated with FN BMD, and both were significantly associated with SHBG, FTI, BioT, FEI and BioE. The highest values of ICTP and the lowest values of FN BMD were found in the lowest quartiles of FTI and FEI. Men with BioE2 < 40 pmol/L had higher values of ICTP and lower femoral neck BMD than men with BioE2 ≥ 40 pmol/L. Thirty men (28.85%) were osteoporotic at the FN. There was a direct and graded association between age and osteoporosis prevalence rate (p = 0.028). Compared to participants less than 70 years old, the crude prevalence ratio (PR) for osteoporosis of those 80 years old or more was 3.2 (95% CI 1.4–7.3). Osteoporosis prevalence rate was also higher in those men with BMI < 25 kg/m2, BioT < 2.7 nmol/L, BioE2 < 40 pmol/L and ICTP > 4.3 μg/L. Adjusting sequentially for BMI, bioavailable sex hormones levels and ICTP levels attenuated the age effect in osteoporosis prevalence, respectively, by 55%, 77% and 86%. In conclusion, our data support the view that low body mass index, declining free and bioavailable forms of both testosterone and estradiol serum levels and increased bone turnover explain most of the negative effects of aging on the male skeleton.
PS-328
THE EFFECTS OF ESTRADIOL AND VARIOUS PHYTOESTROGENS IN COMBINATION WITH VIBRATION THERAPY ON BONE MINERAL DENSITY AND STRENGTH IN OVARIECTOMIZED RATS
D. Seidlová-Wuttke, M. Wuttke, A. Loeffler and W. Wuttke
Georg-August-University of Goettingen, Robert-Koch-Str, 40, D-37075 Goettingen, Germany
Objective: It is known that various phytoestrogens have mild osteoprotective effects and that physical activity performed either actively or in form of high frequency vibration stimuli has also positive effect on bone mineral density. Whether these two treatments have additive effects on bone mineral density and stability is unknown. Therefore, we compared the effects of vibration therapy alone or in combination with oral application of the phytoestrogens genistein, daidzein, equol, estradiol 17ß (E2) on several bone parameters in ovariectomized (ovx) rats treated over a period of 3 months.
Design and Method: The bone of ovx rats demineralises similar to bones of postmenopausal women. Bone mineral density (BMD) of the upper metaphysis of left tibia was measured utilizing computer tomography. Following necropsy body and uterine weights and the lengths of the tibiae were determined; bone stability (strength strain index per 100g BW) was also calculated. Vibration was daily performed with a SwingVibe at 30 Hz with 1 g acceleration while the animals remained in their home cages.
Results: Uterine weights were largely stimulated by the E2 treatment and less, though still statistically significant by genistein and daidzein but not by equol. Body weights in the E2 treated animals increased only slightly following ovx whereas the ovx-controls and the genistein, daidzein and equol treated animals developed obesity which was not significantly affected by the vibration therapy. BMD was largely reduced in the ovx animals and this loss was slightly prevented by the vibration therapy. E2 prevented bone demineralization; puerarin and equol were significantly less and genistein totally ineffective to prevent the development of osteoporosis. In the E2 a slight but in the phytoestrogen treated and additionally vibrated animals no additive effect was seen. The SSI/100g BW was highest in the E2 treated animals and lowest in the ovx rats and slightly improved in the equol and puerarin treated animals. No additional effects on body weight related SSIs were seen in the vibrated animals.
Conclusion: It is concluded that the phytoestrogen genistein had no bone sparing effect at a dose which was slight stimulatory to the uterus. Daidzein had a mild antiosteoporotic effect even though it stimulated uterine weights. Equol at the dose used was devoid of uterotrophic effects but had significant bone sparing effects. A slight effect was seen in the E2 but no additive effect occurred in the phytoestrogen-treated animals which were subjected to a daily vibration therapy.
PS-329
THE NEGATIVE CONSEQUENCES OF MATERNAL STRESS AT EARLY PREGNANCY FOR THEIR FEMALE OFFSPRING REPRODUCTIVE AND BONE SYSTEMS
L. Sergienko, O. Kartavtseva, O. Perets, T. Bondarenko and G. Cherevko
Kharkiv, Ukraine, Institute of Endocrine Pathology Problems
Objective: It's known that elevation of glucocorticoids level induced by stress situation or hormonal treatment of pregnant females before the parturition has long-term effects on functional state of hypothalamo-pituitary-adrenal system (HPAS) and neuroendocrine regulation of offspring. Recently we confirmed the presence of the elevation plasma corticosterone and retardation of sexual maturation accompanied by the low level of testosterone in male offspring of the rats stressed at the first term of pregnancy. The aim of this study was to determinate the consequences of stress during early pregnancy for fertility, placental and fetal weights in pregnant dams, thedynamic of the maturation and the aging of reproductive system in comparison with the processes of the osteogenesis and remodeling of bone tissue of the their female offspring.
Design and Methods: Pregnant Wistar rats were daily exposed to social stress starting from 2nd to 8th day of pregnancy (group SPR). The control pregnant rats remained intact (group - CPR). The research objects were placentas and fetuses of SPR and CPR which were killed at 20nd day of pregnancy and the reproductive organs, blood and bone of the limbs of the female offspring of different age old. The hormonal concentrations were measured by the IFA methods. We performed the cellular analyses of vaginal smears to fix the features of ovarial cycles of stressed and intact offspring (groups – SO, IO) and used microscope “Olimpus” with the compute analyzer of microstructures and statistical assessment of data of histological examinations of pups bones in the base state and after the short immobilization.
Results: It has been established that that fertility rate of SPR decreased by 17%. The placenta weights in 63% of SPR was increased (P<0.05 v.s. CPR) and 37% of fetuses from SPR were decreased weight (P<0.05 v.s. CPR). At 3 months age old only 21% of SO had the normal ovarial cycles; 27% from them were acyclic and 52% had disorders of ovarial cycles. The estrogen concentration in blood of SO at all studied periods of postnatal life was in 1,5–2 times lower then in IO of corresponding ages. At the same time the testosterone level in SO was always increased (P<0.05 v.s. IO).
The histologic examination shown the strongly pronounced evolutional changes in ovaries of SO starting from 8–10 months age old, when the processes of bone resorption (in particular of spongy substance) accelerated and short immobilization induced numerous osteoporosis loci in SO hips.
Conclusion: Our finding suggest that maternal stress in early pregnancy has negative consequences for reproductive system of their female offspring and creates conditions for development of osteopathies else in reproductive period of life.
PS-330
THE SUPPLEMENTATION OF ALFACALCIDOL SHOWS MORE BONE SPARING EFFECT IN RALOXIFENE THERAPY THAN WHEN RALOXIFENE IS USED ALONE IN POSTMENOPAUSAL JAPANESE WOMEN WITH OSTEOPOROSIS AND OSTEOPENIA
I. Gorai1, Y. Tanaka1, S. Hattsutori1 and Y. Iwaoki2
1International University Of Health And Welfare Atami Hospital, Japan; 2Obstetrics and Gynecology, JA Yoshida General Hospital, Yoshida-cho, Hiroshima, Japan
Objective: It has been reported that vitamin D insufficiency is prevalent in osteopenic and osteoporotic postmenopausal women. Secondary hyperparathyroidism decreases the beneficial effects of antiresorptive therapy on bone mineral density (BMD) in osteoporotic women.We aimed to see the effects of raloxifene, 1α(OH)vitamin D3 and a combination of both on bone density and turnover in postmenopausal Japanese women with osteoporosis or osteopenia (<−2.0SD).
Design & Method: A total of 153 subjects aged 49 to 81 years [64.8 ± 6.9 years, 16.2 ± 8.5 years since menopause (YSM)] were randomly assigned to 60mg raloxifene (R), 1 μg 1α(OH)vitamin D3 (D) or a combination of both (R + D) daily for 1 year. Lumbar spine (L-) BMD, biochemical indices, and intact (i-)PTH were monitored over 1 year. Baseline 25(OH)D levels were measured at the start of the study.
Results: There were no significant differences in the background characteristics among the three groups. Baseline 25(OH)D levels were 24.3ng/ml in D-group, 22.9ng/ml in R-group and 24.2 ng/ml in D + R-group (P = 0.3980). PPS analysis was used for statistical analysis. In the combination-treated group there was a significant increase in L-BMD (+ 3.6% in 6 mo. and + 4.4% in 1 yr, P<0.001) and the increases were significant as compared with those in D-treated group (vs. + 0.7% and 0.9%, P<0.05). At 6 mo. i-PTH showed significant decrease in D-group (−17.7%, P<0.01), significant increase in R-group (+ 19.2%, P<0.05) and non-significant change in combination-group (−4.8%) and the change in D-group was significantly different from that in R-group (P<0.05). We found significant decreases in corrected serum calcium in R-group (−4.5% and−3.8%, P<0.01) at 6 mo. and 1 yr. Bone-specific alkaline phosphatase (BAP), urinary cross-linked N-telopeptides of type I collagen (u-NTX) and urinary type I collagen C-telopeptide breakdown products (u-CTX) in combination-group showed significant decreases at 1 mo., 3 mo., 6 mo. and 1 yr (−17.1%–−36.7%, −13.5%–34.0% and −28.3%–−47.4%, respectively) except for BAP at 1 mo., whereas BAP and u-NTX after 6 mo. (−13.4%–−16.7% and –22.3%–−28.0%) and u-CTX after 1 mo. (−14.8%–−32.3%) significantly decreased in R-group.
Conclusion: The combination of calcitriol shows more bone sparing effect by suppressing secondary increment of parathyroid hormone and lowering bone turnover more greatly in raloxifene therapy than when raloxifene was used alone in postmenopausal Japanese women with osteoporosis and osteopenia.
PS-331
THE sRANKL/OPG SYSTEM – MARKER OF BONE REMODELING IN POSTMENOPAUSAL WOMEN WITH OSTEOPOROSIS
Camelia Vidita Gurban1, M. Cojocaru2 and Doina Drugarin3
1„Victor Babes” University of Medicine and Pharmacy, Biochemistry Department, Timisoara, Romania; 2„Colentina” Clinical Laboratory, Immunology Department, Bucharest, Romania; 3„Victor Babes” University of Medicine and Pharmacy, Imunology Department, Timisoara, Romania
Receptor activator of nuclear factor- kB ligand soluble (sRANKL) is expressed on osteoblastic cells together osteoprotegerin (OPG) regulate bone metabolism.
Objective: To analyze if serum levels of sRANKL, OPG and Estradiol (E2) are elevated in postmenopausal women with osteoporosis.
Design & Method: We determined serum levels of sRANKL, OPG and E2 in postmenopausal women with osteoporosis (two cohorts of patients, depending on estrogenic deprivation) as compared to controls (menopausal women without osteoporosis). Serum levels of the markers were measured by ELISA technique and evaluations Bone Mineral Density (BMD) were analyzed using DEXA method with the assessment of T scores (sT spines).
Results: cohort 1: serum levels sRANKL were 67.63 ± 3.55 pg/ml, serum levels OPG were 42.15 ± 0.55 pg/ml, serum levels E2 were 28.32 ± 1.78 pg/ml, and T score spines were −3.63 ± 0.65DS; cohort 2: serum levels sRANKL were 49.26 ± 2.85 pg/ml, serum levels OPG were 27.78 ± 1.04 pg/ml, serum levels E2 were 19.66 ± 1.23 pg/ml, and T score spines were −3.78 ± 0.36DS; control groups: serum levels sRANKL were 32.48 ± 3.03 pg/ml, serum levels OPG 38.05 ± 4.89 pg/ml, serum levels E2 were 43.07 ± 4.04 pg/ml, and T score spines were −1.78 ± 0.11DS.
Conclusion: sRANKL and OPG constitute a complex mediator system involved in the regulation of the bone resorption process in postmenopausal women with osteoporosis. Therefore sRANKL mediates osteoclastogenesis and the bone resorption. The OPG functions are as a soluble „decoy” receptor for the sRANKL. The serum levels sRANKL are semnificantly higher in postmenopausal women with osteoporosis (p < 0.002- cohort 1; p < 0.003- cohort 2) as compared to control group. The serum levels OPG in postmenopausal women with osteoporosis were increased (p < 0.002- cohort 1), demonstrating osteoblast activation, and were decreased (p < 0.003- cohort 2) demonstrating osteoblasts apoptosis stimulation, associated with estrogens deficiency, as compared to control group. The bone remodelling inbalance in postmenopausal women produces a decrease in bone formation and increases bone resorption, and the inbanlance favorising the osteoporosis appearance.
PS-332
TNFSF11 AND ESR1 POLYMORPHISMS AND HAPLOTYPES MAY BE ASSOCIATED WITH BONE MINERAL DENSITY OF TAIWANESE EARLY POSTMENOPAUSAL WOMEN
Bi-Hua Cheng1,2, Hong-Yu Kong1, Tzu-Hua Wang3, Chun-Chen Huang2, Ying-Chu Lin4 and Ko-En Huang2
1Chang-Gung University, Lin-kou, Taiwan; 2Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 3Chang Gung Memorial Hospital, Lin-kou, Taiwan; 4Kaohsiung Medical University, Kaohsiung, Taiwan
Objective: Genetic studies of osteoporosis have focused on analyzing single polymorphisms (SNPs) in individual genes with inconclusive results. An alternative approach may be involved haplotypes and gene-gene interactions. The aim of this study was to test the association between the TNFSF11 and ESR1 polymorphisms or haplotypes and bone mineral density (BMD) in Taiwanese early postmenopausal women.
Design & Method: We analyzed 6 ESR1 tag SNPs and 5 TNFSF11 tag SNPs in 325 early postmenopausal women without major disease who were not recent hormonal users. ANOVA and Chi-square tests were used to perform the statistical analysis.
Results: ESR1 rs18*4054 tag SNP was significantly (p = 0.019) associated with low lumbar spine BMD adjusted with age, years after menopause, BMI and calcium intake by ANOVA test. TNFSF11 rs952*641 tag SNP and rs 374*257 were significantly (p = 0.03, and p = 0.026, respectively) associated with adjusted LS BMD by ANOVA test. In addition to the association with BMD, we found that ERS1 rs18*4054 tag SNP was associated with low T score at LS. TNFSF11 haplotype CGCTG was associated with low risk for poor T score at lumbar spine (OR = 0.45, C.I. = 0.22−0.92). Mean while, significant association between the interactions of ERS1 rs 188*054 to TNFSF11 rs3742*557 (P = 0.009) and TNFSF11 rs952*641 (p = 0.017) was noticed.
Conclusions: We suggest that polymorphisms and haplotype at TNFSF11 and ESR1 may be associated with BMD in early postmenopausal Taiwanese women.
PS-333
THE CORRELATION OF SERUM HOMOCYSTEINE AND BONE MINERAL DENSITY IN THE PERIMENOPAUSAL AND POSTMENOPAUSAL KOREAN WOMEN
H. Suh and K. Yang
Gachon Medical School, Gil Medical Center, Korea
Background: Interests in serum homocysteine concentration and BMD(Bone Mineral Density) are currently on the increase. Hence the objective of this research was to find out the relevance of serum homocysteine concentration and BMD using perimenopausal and postmenopausal women.
Method: In total of 109 perimenopausal and postmenopausal female participants were recruited who visited the department of family medicine at certain University Hospital from August 2006 to January 2007. The blood sampling, lumbar and femur neck BMD, smoking, drinking, caffeine and milk consumption of the participants were investigated. The participants were divided into three groups according to their state of BMD(osteoporosis, osteopenia, normal), and their differences between three groups through ANOVA or Fisher's exact test were analyzed. The multiple regression analysis was used to analyze factors affecting to serum homocysteine. And the correlation analysis was performed to find out the relationship between the serum homocysteine concentration and BMD adjusted by factors affecting to homocysteine in the multiple regression analysis result.
Result: In BMD, the three groups exhibited some differences (P<0.05) in terms of age and milk consumption but serum homocysteine was no difference between three groups. Serum homocysteine is associated (P<0.05) with serum glucose, serum creatinine, HDL cholesterol, femur neck BMD each independently. Although a correlation relationship was established (β = −0.25, P = 0.01) between the femur neck BMD and homocysteine adjusted by serum glucose, serum creatinine and HDL cholesterol, there was no such relationship present (β = 0.027, P = 0.786) between the lumber BMD and homocysteine.
Conclusion: Increasing serum homocysteine in perimenopausal and postmenopausal women is associated with the reduction of the femur neck BMD. Hence the increase in the serum homocysteine can be considered to be one of the risk factors of osteoporosis.
PS-334
THE EFFECTS OF RED CLOVER DERIVED ISOFLAVONES ON BIOCHEMICAL MARKERS OF BONE TURNOVER AND BONE MINERAL DENSITY IN POSTMENOPAUSAL WOMEN
J. Dotlic1, M. Terzic1, S. Maricic2 and T. Mihailovic3
1School of Medicine University of Belgrade Institute of Gynecology and Obstetrics, Belgrade, Serbia; 2General Health Center “Savski Venac”, Belgrade, Serbia; 3Ultramedica Clinic, Belgrade, Serbia
Objective: The aim of the study was to investigate the effects of red clover derived isoflavones on biochemical markers of bone turnover and bone mineral density.
Design & Method: The case-control study was carried out during the period of twelve months on forty healthy postmenopausal women divided in two groups. The first group of twenty-two women received red clover isoflavones while the second group of eighteen women was without medications. The effects on bone structure were assessed by the level of markers of bone composing (osteocalcine, alkaline phosphatase) which were measured prior to therapy initiation and in six months periods throughout one year and by osteodensitometry, which was performed before isoflavone commencement and after twelve months. Statistical tests for assessing differences were used for data analysis.
Results: During phytoestrogen intake, a significant increase of both bone composition markers and osteodensity was observed.
Conclusion: Our findings suggest that phytoestrogen intake in postmenopausal women can have potentially positive effects on bone structure and bone tissue turnover, thus preventing the progression of osteoporosis.
PS-335
THE EVALUATION OF THE RISK ASSESSMENT TOOL (OSTEORISK) APPLICATION IN POST-MENOPAUSAL WOMEN WITH OSTEOPOROSIS
M. L. Steiner, C. E. Fernandes, L. M. Pompei, R. Stufraldi, E. P. Cunha and S. Peixoto
Faculdade de Medicina do ABC, São Bernardo do Campo, Brazil
Objective: The aim of this study was to evaluate the sensitiveness of the Osteorisk in identifying osteoporosis in menopausal women.
Design & Method: Eight hundred and twelve postmenopausal osteoporotic women were retrospectively evaluated from medical registries of two clinical centers. All the 812 women were more than 50 years old, had bone-densitometry T-score less than −2.5 in spinal lumbar or hip and there was information about their weight. A woman was considered at ‘high risk for osteoporosis’ when the Osteorisk calculation resulted ‘high’ or ‘medium’. The women were divided into 50–59, 60–69, 70–79 and more than 80 age groups and the results of the Osteorisk clinical tool were compared to the bone-densitometry T-score and were statistic evaluated.
Results: The correlations between the results of the Osteorisk clinical tool and the results of the bone-densitometry were evaluated through Fisher's Test and showed significance when compared to the lumbar spine (P = 0.027) and to the hip (P<0.001), not revealing an arbitrary relationship. The global sensitiveness of Osteorisk in identifying women with ‘high risk for osteoporosis’ was 86.5% (table 1). When considering only lumbar spine osteoporosis, sensitiveness was a little lower, reaching 85.8%, but when considering only hip osteoporosis, sensitiveness of Osteorisk was higher, 97.2% (table 1). The older the population, the better the Osteorisk sensitiveness, being of 46%, 82%, 98% and 98.5% for women of 50–59, 60–69, 70–79 and over 80 years, respectively.
Conclusion: Finally, it could be concluded that the sensitiveness of the Osteorisk was good in identifying over−60-year-old women under risk for osteoporosis and should be used in regions were the bone-densitometry is not easily available or used as a way to select who should be referred to bone-densitometry. Its sensitiveness is greater toward osteoporosis of the hip.
Table 1 Results from Osteorisk for women with bone-densitometry osteoporosis in lumbar spine (L1-L4), hip and lumbar spine or hip
PS-336
THE FREQUENCY OF OSTEOPOROSIS IN POSTMENOPAUSAL WOMEN ACCORDING TO THE WHO DIAGNOSTIC CRITERIA, AND THE 2007 INTERNATIONAL SOCIETY FOR CLINICAL DENSITOMETRY (ISCD) OFFICIAL POSITIONS IN A CERTAIN UNIVERSITY HOSPITAL
H. H. Lee1, A. L. Ryu1, I. S. Lee2, S. D. Choi3, D. H. Bae3, W. S. Moon4, T. H. Kim1, K. H. Nam1 and S. H. Chung1
1Soonchunhyang University Bucheon Hospital, Bucheon-si, Gyeunggi-do, Republic of Korea; 2Soonchunhyang University Seoul Hospital Seoul, Republic of Korea; 3Soonchunhyang Univerisity Cheonan Hospital, Cheonan-si, Chungnam, Republic of Korea; 4Dr. Moon Wonsil Woman's Clinic, Seoul, Republic of Korea
Objective: We evaluated the frequency of osteoporosis in Korean postmenopausal women who have visited our hospital according to the WHO diagnostic criteria and the 2007 International Society for Clinical Densitometry (ISCD) Official Positions Statement.
Design & Method: From the database of our department, we assessed about 250 postmenopausal women aged 45∼69 (mean average age: 56.9 years) from January 2005 to December 2007. We divided them into 5 groups according to age, with each group consisting of 50 postmenopausal women. The bone mineral density (BMD) was measured using dual X-ray absorptiometry (DXA), Prodigy, HR-76-P, Lunar, GE Healthcare systems. Osteoporosis was defined according to the criteria of the WHO which was implemented for postmenopausal Caucasian women on a T score ≤ 2.5 standard deviations (SD). The ISCD also indicates this same diagnostic threshold.
Results: When the WHO threshold for postmenopausal women was applied, the frequencies of osteoporosis were 22.8% at lumbar spine, 30.4% at the femoral neck, and 38.0% in at least one of the designed evaluation sites. However, when the ISCD criteria were applied, the frequencies of osteoporosis were 14.0%, 2.8%, and 14.8%, respectively. The frequencies of osteopenia according to both the ISCD criteria and the WHO threshold were 31.6%, and 40.4% each.
Conclusion: The frequency of osteoporosis according to the WHO in postmenopausal women is much lower than the frequency of osteoporosis according to the 2007 ISCD Official Positions Statement. As indicated, a wide differential was demonstrated when the criteria of the WHO was compared to the ISCD Official Positions Statement; the WHO criteria are much broader and more generalized diverse symptoms. As such, the diagnosis of osteoporosis with the ISCD is so strict that prevention and treatment may be overlooked by healthcare providers. On the other hand, the WHO's criteria are so tough that there is a high probability of prescribing some needless prevention and treatment for postmenopausal women. Therefore, we wish to propose that there be a new criteria that co-joins these systems of evaluation.
PS-337
THE RELATIONSHIP BETWEEN BONE QUALITY AND GLYCOSAMINOGLYCANS CHANGES IN AN OVARIECTOMIZED RAT MODEL OF POSTMENOPAUSAL OSTEOPOROSIS
R. Taniguchi, A. Tarakida, K. Abe, T. Higuchi and H. Mizunuma
Department Of Obstetrics And Gynecology, Hirosaki University School Of Medicine, Japan
Objective: Proteoglycan (PG), a glycoprotein consisting of a core protein linked to glycosaminoglycan (GAG) chains, is the main component of bone extracellular matrix, and participates in various physiological and pathological processes such as maintenance of structural integrity and bone aging. Postmenopausal osteoporosis is a pathological condition where bone loses its quantity and quality during the course of aging, in particular after menopause. The present study investigated changes in CAGs in the bone of postmenopausal osteoporosis model rats and aimed to clarify roles of GAGs in conjunction with the pathological conditions.
Design and Methods: PGs extracted from femora of postmenopausal osteoporosis model rats with low bone density were digested with endo-ß-xylosidase to liberate intact GAG chains from the core protein as previously described. Each GAG chain was fluorescence-labeled with pyridylamination reactions and performed by HPLC analysis using anion-exchange chromatography.
Results: The amount of chondroitin sulfate (ChS) and hyaluronic acid (HA) specifically decreased in osteoporosis model rats by 75% and 50%, respectively, compared with control rats, whereas no differences were observed in amount of heparan sulfate. Furthermore, no significant reduction of collagen amount, a specific indicator of bone quality, was detected in any group.
Conclusion: The present study demonstrated for the first time that postmenopausal osteoporosis appeared to involve qualitative and quantitative changes in both ChS and HA. These results suggest that measurement of bone GAGs in combination with conventional bone densitometory may be a more useful approach for evaluating bone quality.
PS-338
THE RELATIONSHIP BETWEEN OSTEO SONO-ASSESSMENT INDEX AND LIPID PROFILES OF FEMALE RESIDENTS IN A RURAL JAPANESE COMMUNITY
A. Tarakida, K. Abe, R. Taniguchi, T. Higuchi, H. Mizunuma and S. Nakaji
Hirosaki University School of Medicine, Hirosaki City, Japan
Objective: The morbidity rates of lifestyle-related illnesses and osteoporosis in female people increase rapidly after menopause. Recently it is emphasized that the fat/sugar metabolism interrelates bone metabolism in some reports. However it is speculated that adipocytokines play important roles in both metabolism, this mechanism was yet unknown in detail. The aim of this study is to assess the relationship between lipid profiles, adipocytokines and osteo sono-assessment indices (OSI).
Design & Method: From a list of inhabitants, 184 women aged 23–81 years were selected. They are residents in a rural Japanese community and participated in the health-promote project, named IWAKI project, that is intended for the general residents and people receive guidance in a diet and exercises as well as physical examinations. All of them have no history of hypertension, diabetes, hyperlipidemia, osteoporosis, breast cancer and a hysterectomy. We measured their serum lipid profiles, and calculated OSI with the speed of sound and transmission indexs measured at the calcaneus at baseline and one year after. Furthermore we measured adiponectin and leptin of post-menopausal women in a same manner. We classified the post-menopause women into four groups by years since menopause, processed data statistically and assessed the relationship between lipid, adipocytokines and OSI.
Results: In pre-menopausal group and post-menopausal group, total cholesterol was 191.9 ± 32.1 mg/dl and 217.1 ± 29.0 mg/dl, HDL-cholesterol was 68.4 ± 13.9 mg/dl and 65.8 ± 15.4 mg/dl, LDL-cholesterol was 109.7 ± 28.9 mg/dl and 134.8 ± 26.8 mg/dl, triglyceride was 68.8 ± 33.1 mg/dl and 82.6 ± 45.0 mg/dl, BMI was 21.8 ± 2.9 and 22.5 ± 2.5, OSI was 2.69 ± 0.29×106 and 2.36 ± 0.26×106 respectively. In post-menopausal group, adiponectin was 14.4 ± 8.3 μg/ml and leptin was 6.4 ± 5.1ng/ml (each number indicates the mean and the standard deviation). Only LDL-cholesterol level significantly correlated with OSI in the above-mentioned items concerning lipid. We assessed the relationship between rate of change of OSI and lipid profile, and the results showed that the higher total cholesterol level was, the more OSI tended to decrease after one year in women who were less than five years since menopause. Moreover OSI in women with high total/LDL-cholesterol levels tended to decrease one year later in the pre-menopausal and all post-menopausal groups.
Conclusion: It is generally said that obesity acts on bones protectively. However, bone mineral density in women with abnormal cholesterol levels tends to decrease. And so a proper lipid control is required to prevent not only arteriosclerosis but osteoporosis.
PS-339
VITAMIN D DEFFICIENCY IN SPANISH POSTMENOPAUSAL WOMEN
A. Esparza, G. Soro, B. García and F. Baró
Vall d'Hebron University Hospital, Barcelona, Spain
Objective: To study the prevalence of lack of vitamin D in postmenopausal women and its relation with hyperparathyroidism.
Design & Method: We conducted a descriptive and retrospective study among 150 postmenopausal women aged 63 ± 6 years (range 43 to 82) that were studied in our Institution for vitamin D lacking. Blood concentration of vitamin D was obtained in routine blood tests. We considered deficit of vitamin D values inferior to 10 mg/dL, insufficiency of vitamin D values between 10 mg/dL and 30 mg/dL, and normal values those equal or superior to 30 mg/dL. From these, 126 women were also examined for secondary hyperparathyroidism according to their blood parathormone levels. A chi-square test was used to assess the association between insuficiency or deficit of vitamin D and parathormene levels.
Results: Results obtained from 150 patients showed than 7.3% (11 patients) presented with deficit of vitamin D, 72.0% (108 patients) presented with insufficiency of vitamin D, and 20.7% (31 patients) presented with normal values of Vitamin D. That is, more than three quarters of postmenopausal women had abnormal values of vitamin D blood concentration. No association was observed between insufficiency or deficit of vitamin D and secondary hyperparathyroidism (p = 0.55).
Conclusion: Vitamin D deficiency has been proved in postmenopausal women with osteoporosis. Many studies have shown the need to administer vitamin D in the treatment of osteoporosis. Vitamin D supplements have resulted in lower risk of fractures and falls in these women. This study shows, first, unexpectedly low vitamin D values in our population, in spite of being Spain a sunny country, and second, the need for supplementation with vitamin D and calcium of our postmenopausal women treatment. Our data have failed to show an association between lack of vitamin D and secondary hyperparathyroidism.
PS-340
VALUE OF PERIPHERAL DENSITOMETRY FOR DIAGNOSIS OF OSTEOPOROSIS
J. Presa, T. Aguilar, A. Santalla, B. Romero, M. S. López Criado, A. Salamanca, J. Mozas, J. L. Gallo, D. Galliano and N. Mendoza
Hospital Virgen De Las Nieves, Granada, Spain
The bone densitometry is a range of non-invasive techniques that measure bone mass in different areas of the skeleton. At present there is a broad consensus that the central densitometry is the best technique for assessing the state of BMD. His big problem lies in the high cost and the need for a comprehensive physical space. For that reason, peripheral densitometries pose an alternative, as they are relatively inexpensive and can be transported easily.
Material and Methods: Our study compares the results of the peripheral DXA (PIXI-calcaneus) with the central DXA of the lumbar spine and hip. It has been studied a group of 97 postmenopausal women who had attended a campaign population about osteoporosis and who had a measurement of BMD through a PIXI. They were classified into three groups according to the value of the T-score: normal (N) with T-score greater than −0.6; osteopenia (OPN) with T-score between −0.6 and −1.6 and osteoporosis (OP) when the T-score was lower than −1.6.
The women who gave a value of the T-score less than 0.6 had undergone bone densitometry hip and spine to confirm the diagnosis of osteopenia or5 osteoporosis.
Subjects were divided into two comparisons: on the one hand those women with osteoporosis versus osteopenia and normal BMD, on the other hand normal versus women who presenting osteopenia or osteoporosis.
Results: In the first comparison (women with osteoporosis compared to the rest), the PIXI calcaneous showed sensitivity of 77.8% and 83.3% specific, with a positive predictive value of 77.8% and a negative predictive value of 83.3%.
In the second comparison (women with osteopenia or osteoporosis compared to normal), the PIXI calcaneous showed sensitivity of 100% and 50% specific, with a positive predictive value of 95% and a negative predictive value of 100%.
Conclusion: With these results we can consider that the densitometry calcaneous presents a great benefit for the screening of osteoporosis in the general population of postmenopausal women.
PS-341
VITAMIN D DEFICIENCY
E. Rodríguez Bueno, E. Ruiz Domingo** and F. Baro Marine***
P. A. S. S. I. R. “Sant Andreu"* and “Antoni Creus” **Menopause Dispensary. (I.C.S). Barcelona And Tarrasa, And “Vall D'hebron” Hospital***
AIM: Vitamin D level valuation in menopausal women.
Materials and Methods: Vitamin D (25-OH colecalciferol) level was measured by RIA in 400 menopausal women aged 27 to 79 years old (mean = 55,96, mode = 50 and median = 55. As McKenna and Freaney proposed, we consider levels < 10 ng/ml as “vitamin D deficiency”, levels >10 and < 20 ng/ml as “vitamin D insufficiency”, levels >20 and < 40 ng/ml as “hypovitaminosis D”; and levels >40 ng/ml as “desirable”. Moreover, in agreement with experts on this subject, we also classify as “suitable” levels between 30 and 40 ng/ml; as “inadequate” levels between 10 and 30 ng/ml; and as “grave deficiency” levels <10 ng/ml.
Results:
a) McKenna and Freaney classification:
– deficiency (<10 ng/ml): 42 patients (10,5%)
– insufficiency (between 10 and 20 ng/ml): 216 patients (54%)
– hypovitaminosis (between 20 and 40 ng/ml): 132 patients (33%)
– desirable (>40 ng/ml): 10 patients (2,5%)
b) Experts classification:
– grave deficiency (<10 ng/ml) : 42 patients (10,5%)
– inadequate level (between 10 and 30 ng/ml): 315 patients (78,75%)
– suitable level (between 30 and 40 ng/ml o more): 43 patients (10,75%)
Discussion: These results show that menopausal women visited by us and resident of a town with a supposed correct sunlight throughout the year, have no serum 25-OH-vitamin D correct levels. To afford by a desirable level of 28–32 ng/ml, as Dawson-Hughes says, it would be necessary an average daily intake of 800–1600 U. of vitamin D associated to calcium.
Aging brain and hormone protection
PS-342
BRAIN VOLUME CHANGES IN RECENTLY MENOPAUSAL WOMEN IN A HORMONE REPLACEMENT TRIAL
K. Kantarci, V. M. Miller, T. G. Zais, J. L. Gunter and C. R. Jack Jr
Mayo Clinic, Rochester, Minnesota, USA
Objective: Estrogens are thought to enhance neurological function and exert neuroprotective effects. We hypothesized that brain volumetric magnetic resonance imaging (MRI) measurements can track hemispheric atrophy in menopausal women and the neuroprotective effects of estrogens in the Kronos Early Estrogen Prevention Study (KEEPS). Our objective in this study was to quantify the rates of brain volume and ventricular volume change in newly menopausal women in the KEEPS trial.
Design & Method: 106 women (40–55 years of age), who were enrolled to the KEEPS trial at the Mayo Clinic, underwent brain MRI at baseline and were randomly assigned to one of the three treatment arms (oral conjugated estrogen with active progesterone, transdermal 17-β estradiol skin patch with active progesterone, and placebo). 30 of these women (mean ± SD age at baseline = 54.5 ± 2.8) underwent a follow-up MRI exam at 18 months. The investigators were blinded to the treatment groups. All MRI studies were performed on a single 1.5T system using 3D Magnetization Prepared Rapid Acquisition Gradient-Echo acquisition. Rates of change in whole brain and ventricle volumes were calculated using a home-built software algorithm which computes change in brain and ventricular volume from baseline to follow-up MRI exam (Gunter et al. 2003).
Results: On average, the brain volumes decreased and the ventricular volumes increased at 18 months. The mean ± SD annual percent decline in the brain volume was 0.3% ± 0.35% and the mean ± SD annual percent expansion in ventricular volume was 3.59% ± 3.72%. There was a significant correlation between the annual percent decline in the whole brain volume and the expansion in the ventricular volume (R2 = 0.35, p < 0.001). The rate of decrease in brain volume in KEEPS subjects was comparable to the brain volume decrease we previously observed in cognitively normal elderly with a median (range) age of 79 (56,93) (Jack et al. 2004) (0.4% in elderly subjects vs. 0.35% in KEEPS subjects). However, the ventricular volume increase was more than twice as high in KEEPS subjects (1.7% in elderly subjects vs. 3.7% in KEEPS subjects).
Conclusion: The changes in brain structure in KEEPS subjects, were as much as the changes observed in individuals two decades older than KEEPS subjects. Because we are blinded to the treatment information at this time, it is unknown to us whether there is accelerated atrophy of the brain during menopausal transition, or if estrogens modify the change in brain structure.
P343
EFFECTS OF ESTRADIOL ON THE COGNITIVE FUNCTION OF POSTMENOPAUSAL WOMEN
R. Marinho1, J. M. Soares Jr1, M. A. Haidar1, R. S. Simoes1, M. C. P. Baracat2 and E. C. Baracat3
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Universidade de Santo Amaro, São Paulo, São Paulo, Brazil; 3Faculdade de Medicina de São Paulo
Objective: To analyze the effect of estrogen on cognitive function of postmenopausal women through psychometric tests.and compare to placebo. Methods: Seventy-four postmenopausal women were selected and divided into two groups: a) estradiol group (n = 34): patients who received treatment, that is, tablets containing 2 mg 17 beta-estradiol; placebo group (n = 31): patients who received tablets with an inactive substance. After inclusion, they were submitted to a series of psychometric tests, in addition to Greene's Scale of Climacteric Symptoms and Hamilton Scale por depression. Analysis of the clinical characteristics of the study patients and comparison between the groups was performed by Mann-Whitney and Student's t tests. In order to evaluate if the effect of treatment on the tests is related to improvement of symptoms or depression, Spearman's correlation coefficient was calculated.
Results: Estrogen did not determine a significant improvement in the used psychometric tests as compared to placebo, despite the fact that improvement occurred in evocation of story (immediate and late recall) in the estradiol group. Climacteric symptoms (improved in the treated group, when compared to placebo. Depressive symptoms improved a fact which did not occur in the placebo group. On comparing the groups, there was no significant difference between them. Reduction in climacteric symptoms was associated with improvement in executive function performance as evaluated by the Stroop test. Conclusion: Our results suggest that estrogen improves the cognitive function and this action would be related to decrease in vasomotor symptoms.
PS-344
EVALUATION OF SYMPTOMS AND EFFECTS OF THERAPIES AMONG DEPRESSIVE, ANXIETY, AND MENOPAUSAL DISORDERS IN POSTMENOPAUSAL JAPANESE WOMEN
Y. Somekawa, A. Furusawa, D. Satoh and H. Umeki
Toride Kyodo General Hospital, Hongo 2-1-1 Toride, Ibaraki 3020022, Japan
Objective: The purpose of this study was to analyze the relationships among insomnia, depressive, and menopausal symptoms in postmenopausal women, and to evaluate the effects of SSRI, Hormone replacement therapy (HRT), and Chinese herbal medicines (CHMs).
Design and Method: The subjects were 276 postmenopausal Japanese women aged 44 to 76 years (mean age 53.8 ± 6.5 yr.) who visited our menopause clinic. They were classified into menopausal disorder (MD), depressive disorder (DD), anxiety disorder (AD), adjustment disorder, somatoform disorder, and other mood disorder. Their insomnia, menopausal symptoms, and depressive tendencies were examined with the insomnia self-assessment inventory, Climacteric Symptom Evaluation Form Checklist (CSC) for Japanese women, and Zung self-rating depression scale (SDS) respectively. Effects of SSRI, HRT, and CHMs were evaluated by comparing the scores before and after 6 months of treatment.
Results: The numbers of patients of MD, DD, AD, adjustment disorder, somatoform disorder and other mood disorder were 127, 67, 26, 10, 4 and 4 respectively. SDS sores were significantly higher in DD than in AD or MD. These differences were mainly found in the scores related to “restless, lack of satisfaction, and loss of enjoyment or pleasure”. Insomnia scores were significantly higher in DD than MD. These differences were found in the scores related to “feeling difficulty in falling asleep and arising in the morning, woke up feeling tired, and unrefreshing sleep”. Differences of CSC scores were weak among MD, AD, and DD. The scores of “lacking of energy” were higher in DD than in MD. SSRI and HRT were effective to alleviate SDS scores or CSC scores at the same level. CHMs were effective though the effects were a little weak.
Conclusion: There are considerable numbers of DD and AD who complains of menopausal symptoms. A careful diagnosis and appropriate treatments are necessary. Sleep disturbance is related to DD, AD, and MD. SSRI, HRT and CHMs were effective to alleviate these symptoms.
PS-345
HORMONES WITHDRAWAL IS CONNECTED WITH A DECREASE IN BRAIN DERIVED NEUROTROPIC FACTOR IN MENOPAUSE. EFFECTS OF THE HORMONAL REPLACEMENT THERAPY
S. Begliuomini, E. Lenzi, N. Pluchino, E. Casarosa, S. Merlini, A. Giannini, A. Cubeddu, M. Luisi and A. R. Genazzani
University of Pisa, Pisa, Italy
Objective: Brain-derived neurotropic factor (BDNF) is a member of the neurotrophin family, abundantly expressed in the nervous system. It works as a mediator of neuronal plasticity and influences learning, memory and cognitive behaviour. We aim to test the hypothesis of an influence exerted by endogenous and/or exogenous sex hormones on BDNF levels. Consequently, the purposes of the present study are: 1) to compare plasma BDNF levels between non-treated postmenopausal women and fertile subjects in the follicular phase; 2) to evaluate if/how a six months hormonal replacement therapy influences peripheral BDNF levels.
Design & Method: A total of 45 women were included. They were divided into the followings two groups: 1) 20 fertile women aged 20–40 years (BMI 20–23 Kg/m2), with a regular menstrual cycle. 2) 25 postmenopausal women aged 48–70 years (BMI 21–25 Kg/m2). A blood sample was drawn from each subject in EDTA-coated tubes. After the first blood sampling, postmenopausal women started receiving a combined sequential oral hormonal replacement therapy (HRT: estradiol valerate (E2V) 2 mg/day for 16 days, followed by E2V 2 mg/day + levonorgestrel (LNG) 0.075 mg/day for 12 days) and they underwent a second sampling after 6 months of treatment. Plasma BDNF was measured by ELISA and expressed in pg/ml. Data obtained were analyzed by one-way analysis of variance (ANOVA). Differences between single pairs of groups were compared by means of the Bonferroni test.
Results: Postmenopausal women showed significantly lower plasma BDNF levels compared to fertile subjects (p < 0.001). There was an age-related decrease in BDNF plasma levels: in fact, aged women showed the lowest concentrations (r = −0.87, p < 0.001). Moreover, BDNF circulating levels showed a negative correlation (r = −0.86, p < 0.001) with menopausal age. In this view, women who experience an earlier menopause may have detrimental effects from the longer deficiency of BDNF with respect to the women who enter postmenopause later on in life. Finally, after 6 months of HRT treatment, BDNF plasma levels increased significantly (p < 0.01) to values present in fertile women during the follicular phase.
Conclusion: Plasma BDNF levels are influenced by hormonal status, suggesting a role for sex gonadal hormones in regulating neurotrophin production and activity. Menopause is associated with a decrease in peripheral BDNF levels, feasibly connected with the hormonal withdrawal. A 6-month oral HRT efficiently restores BDNF levels to those present in fertile women. This last phenomen could be responsible of an improvement in cognitive performances in postmenopausal women taking HRT.
PS-346
IMPACT OF THE CATECHOL-O-METHYLTRANSFERASE VAL158MET GENOTYPE ON PREFRONTAL FUNCTION IN HEALTHY MENOPAUSAL WOMEN
M. Gutiérrez-Muñoz, S. Solís-Ortiz, E. Pérez-Luque and L. Morado
Instituto de Investigaciones Médicas, Universidad de Guanajuato. León Guanajuato, México
In the prefrontal cortex, catechol-O-methyltransferase (COMT) enzyme is critical in the metabolic degradation of dopamine, a neurotransmitter involved in human cognitive function. The COMT gene contains the val158met functional polymorphism, which has been associated with cognitive impairment in healthy volunteers and schizophrenia patients. Menopausal period is characterized by impairment in some aspects of memory.
Objective: To investigate whether prefrontal cognition and attention varies with COMT genotypes in healthy women at menopausal period.
Design & Method: We genotyped to 74 middle age healthy women (48 to 60 years) at menopausal time for the COMT val158met polymorphism using PCR-RFLP. We evaluated prefrontal functions using Wisconsin Card Sorting Test (WCST). Kruskal-Wallis?s test was using for examine the effects of this polymorphism on prefrontal functions.
Results: We found 27 women with the val/val COMT genotype, 15 with met/met genotype, and 32 with val/met genotype. In the WCST, the number of categories completed for the group of women with the val/val genotype was high (p < 0.04), the number of errors made was low (p < 0.02), and this group tended to commit fewer perseverative errors (p = 0.07) than the met/met group or the val/met group. The number of trial to reach each category for the group of women with the met/met genotype was significantly low (p < 0.002).
Conclusion: These findings suggest that this functional genetic polymorphism may influence the executive functions in menopausal healthy women, besides of the hormonal changes.
This work was supported by CONACYT Grant 060645 and Grant 52365 and CONCYTEG Grant 06–16-K117–142, Universidad of Guanajuato.
PS-347
NOMEGESTROL ACETATE ADMINISTRATION EFFECTS ON THE CENTRAL AND PERIPHERAL LEVELS OF BETA-ENDORPHIN AND ALLOPREGNANOLONE IN OVARIECTOMIZED RATS
E. Lenzi, S. Begliuomini, N. Pluchino, S. Merlini, A. Giannini, A. Cubeddu, E. Casarosa, M. Luisi and A. R. Genazzani
University of Pisa, Pisa, Italy
Objective: The aim of the present study was to investigate the effects of nomegestrol acetate (NOMAc), a synthetic progestin largely used in hormone therapy, on the central nervous system by studying two markers of the neuroendocrine function: the neurosteroid allopregnanolone and the opioid beta-endorphin.
Design & method: 104 Wistar female rats 5 months old were used in this study. One group of fertile and one of ovariectomized rats (receiving placebo) were used as control. Once ovariectomized, the rats underwent a 2-week oral treatment of NOMAc (0.05, 0.1, 0.2, 0.5, 1 mg/kg/day), alone or with estradiol valerate (E2V 0.05 mg/kg/day). Allopregnanolone and beta-endorphin were then assessed in different brain areas and in circulation.
Results: Ovariectomy decreased allopregnanolone anywhere except in the adrenal gland and E2V reversed the effects of ovariectomy. 0.5 and 1 mg/kg/day of NOMAc increased allopregnanolone levels in hippocampus. The combined administration of 1 mg/kg/day of NOMAc plus E2V induced a further increase of allopregnanolone levels in the hippocampus, the hypothalamus, and in the anterior pituitary. 1 mg/kg/day of NOMAc decreased the adrenal content of allopregnanolone, both by itself and associated with E2V. NOMAc increased the hippocampal and the hypothalamic content of beta-endorphin at the highest doses, and it increased positively E2V action, at 1 mg/kg/day, also in anterior pituitary and plasma. Comparison among different treatment groups was performed by means of one-way ANOVA. Differences between single pairs of groups were analysed by Bonferroni test.
Conclusion: These findings reinforce the clinical data regarding the capability of NOMAc to modulate the pathways involved in mood and behaviour. In fact, due to the NOMAc action on hippocampus, hypothalamus, and anterior pituitary our results highlight the selectivity of NOMAc on part of the limbic system and the anterior pituitary, regarding both allopregnanolone and beta-endorphin, thus suggesting its involvement in mood and behaviour.
PS-348
NEUROLOGICAL AND NEURODEGENERATIVE PATHOLOGY IN A VALENCIAN WOMEN'S COHORT DURING CLIMATERIUM
A. Pérez-Calvo1, M. D. Juliá1, J. Burguera1, N. Roig Casabán1, M. Brik1, J. Quiles2, R. M. Marín3 and A. Romeu1
1University La Fe Hospital, Valencian Regional Government Ministries of Health, Valencia, Valencia, Spain; 2Public Health Department Directorate, Valencian Regional Government Ministries of Health, Valencia, Valencia, Spain; 3Valencian School for Health Studies, Valencian Regional Government Ministries of Health, Valencia, Valencia, Spain
Objective: screening neurological and neurodegenerative pathologies in climacteric women of the Valencian Region.
Design and Methods: Cross -sectional population study of a sample of 427 women from 43 to 65 years in four different geographical areas of Valencian Region by personal interview and evaluation of screening tests with the aim of detection neurological and neurodegenerative pathologies in healthy population, validated in Spanish population: Mini-Mental State Examination (MMSE) of Folstein to evaluate cognitive deficit, Screening Parkinson disease Questionnaire of Duarte to evaluate mobility disorders, Migraine Disability Assessment Score (MIDAS) to evaluate headache intensity, Screening Epilectic Crisis Questionnaire of Plasencia, Functional Activity Test of Pffefer. Statistical analysis: descriptive. Statistical Pack: SPSS-v12.0.
Results: The evaluation of qualification level showed 3 analphabetic women (0,7%), 51 patients could read and write (12%), 248 had school studies (58%), 61 women had secondary studies (14,3%) and 64 patients, university studies (15%).189 women (44%) had normal results in their questionnaires and 238 (56%) had at least, one positive questionnaire. A total of 294 questionnaires were positive tests Duarte 199 (68%), MMSE 12 (4%), MIDAS 36 (12,5%), Plasencia 36 (12,5%), Pfeffer 11 (3%). 189 women (79,5%) had only one positive test; 43 patients (18%) had two positive tests; 5 (2%) had three positive tests and only one patient had four positive tests (0,5%). None of them had five positive tests.
The most frequent associations were Duarte-MIDAS with 24 patients (10%) and Duarte-Plasencia with 12 patients (5%). We observed the association between Duarte-MMSE and Duarte-Pfeffer in 8 patients (3,5%).
In 43 to 49 subgroup, 25 patients (75%) proved positive in the Duarte test increasing this number to 94% in the older women subgroup.
Conclusions: Screening neurological and neurodegenerative pathologies can lead to the reduction of the frecuency of these diseases, with better therapeutic management. These discoverments can change the natural history of the disorder, with less number of complications and minor sociosanitary cost. These findings allow the introduction in the Menopause surveillance activity a screening programme for possible diseases in climacteric women.
(+ + ) The data of this study are included in: “Epidemiological Study on Cardiovascular Disease risk and Neurological and Neurodegenerative Disease during the climacteric period of four different areas of the Valencian Region”. This project was partially financed by EVES, Reference PS-051/2002.
PS-349
NEUROPROTECTIVE EFFECT OF 17 β-ESTRADIOL AGAINST FOCAL CEREBRAL ISCHEMIC DAMAGE VIA ANTIAPOPTOTIC ACTION IN RATS
Kyu Sup Lee1, Sung Tack Oh2, Young Min Choi3, Hwi Gon Kim1 and Jung Wan Jung4
1Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602-739; 2Obstetrics and Gynecology, Chonnam National University, Kwangju, Republic of Korea, 501-757; 3Obstetrics and Gynecology, Pusan National University, Busan, Republic of Korea, 602-739 and 4Obstetrics and Gynecology, Miraero Hospital, Busan, Republic of Korea, 616-820
Objective: Overall incidence of stroke is uniformly higher in men than in women, and rare especially in women during the reproductive stage. Although clinical uses of hormone replacement therapy for stroke remains controversial, the protective effect of estrogen has received much attention in ischemic stoke. A number of studies are demonstrated the reduced infarct size upon administration of estrogen to ovariectomized females in ischemic brain injury models.
Design: We aimed to examine the potential neuroprotective effects of 17 beta-estradiol on the cerebral infarct size and then on the apoptotic mechanism after the completion of 2-hour occlusion of middle cerebral artery and 24-hour reperfusion. Rats received 17 beta-estradiol (1.4 and 10 mg/kg, intraperitoneal) 24-hour before and 5 minute after the completion of 2-hour middle cerebral artery occlusion. Differences between data of infracted area and volume in each section between groups were analyzed by repeated-measures analysis of variance (ANOVA), followed by Tukey's multiple comparison test as a post hoc comparison. Student's t-test was performed on the results obtained before and after administration of drugs between each group. The differences were considered statistically significant at P < 0.05.
Results: Mean arterial blood pressure in the rats subjected to 2-hour occlusion of middle cerebral artery and 24-hour reperfusion (108.9 ± 4.7 mmHg, n = 25) did not significantly differ from the sham-operated rats (112.5 ± 5.8 mmHg, n = 6). Blood gas and pH were not significantly different from those in normal control. Intraperitoneal injection of 4 and 10 mg/kg 17 beta-estradiol caused little change in mean arterial blood pressure. The ischemic zone with cerebral infarct was consistently observed in the cortex and striatum of the left hemisphere at 24 hours of reperfusion after the completion of 2-hour occlusion of left middle cerebral artery. The infarct area and volume were significantly reduced, when rats received 4 and 10 mg/kg 17 beta-estradiol intraperitoneally 24 hours before and 5 mininute after 2-hour ischemia. Samples from the regions corresponding to the penumbra showed markedly reduced Bcl-2 protein level and, in contrast, high levels of Bax protein and cytochrome c release. Both increased Bax and cytochrome c were significantly reduced, and decreased Bcl-2 protein was markedly restored by 17 beta-estradiol. 17 beta-estradiol potently scavenged hydroxyl radicals and inhibited intracellular hydrogen peroxide production.
Conclusion: 17 beta-estradiol treatment decrease ischemic brain infarction in association with inhibition of apoptotic cell death in rats model.
PS-350
RELATIONSHIP BETWEEN SLEEP DISORDER AND AFFECT DISORDER AMONG THE ELDERLY OF OVER 50 YEARS OLD AT DISTRICT OF PURWOREJO, CENTRAL JAVA, INDONESIA
D. Dasuki1, N. Wayan1 and N. G. Nawi1,2
1Magister, Mother and Child Health – Reproductive Health, Gadjah Mada University, Yogyakarta, Indonesia; 2Midwife Department, Health Polytechnic, Malang, Indonesia; 3Magister, Field Epidemiology and Training Program, Gadjah Mada University, Yogyakarta, Indoensia
Objective: Advancement of knowledge especially in health sciences has brought the increase of life expectancy. The process of ageing causes hormonal, physical and mental changes. Some problems occur due to the process of ageing. Insomnia is one of sleep disorders which often happen among the elderly. If it is ignored for a long time, it will cause affect disorder such as depression, anxiety, anger and ultimately, and it can lead to suicide. Factors of education, sex, marital status, location, disability and farmer diseases are related to the prevalence of sleep disorder and affect disorder of the elderly over 50 years old. The study aimed to identify relationship between sleep disorder and affect disorder of the elderly over 50 years old.
Design & Method: The study was observational with cross sectional design. Subjects of the study were all the elderly over 50 years old from data of the household of Community Nutrition and Health Research Laboratory of The Faculty of Medicine, Gadjah Mada University. Univariable analysis used frequency distribution, bivariable analysis used chi square and multivariable analysis used logistic regression.
Results: The result of the study showed that serious affect disorder was 8.91%, serious sleep disorder was 23.59%. There was significant relationship between sleep disorder and affect disorder which occurred was light affect disorder, as much as 59.63% in female and 40.37% in male. Meanwhile, variable of sleep disorder showed that no disorder was the greatest proportion, as much as 38.47% in female and 45.70% in male with Ratio Prevalence = 9.38 and 95%CI is 7.82–11.24.
Conclusion: There was relationship between affect disorder and serious sleep disorder and greatest risk factor was serious sleep disorder.
PS-351
WE INVESTIGATED THE EFFECT TO THE SYMPTOM OF PSYCHONEUROSIS OF THE MENOPAUSE COMPARED THE HRT WITH KAMPO MEDICINE KAMI-SHOYO-SAN DOSAGE
Kazuhiro Abe, Ayako Tarakida, Ryousuke Taniguchi, Tsuyoshi Higuchi and Hideki Mizunuma
Department Of Obstetrics And Gynecology, Hirosaki University School Of Medicine, Japan
Objectives: Effects of hormone replacement therapy (HRT) and KAMPO medicine Kami-Shoyo-San (KSS) for climacteric symptom are widely accepted, but there aren't the evident consensus of the choice of therapy. The present study investigated the difference of effects for menopausal women with climacteric symptom between HRT and KSS.
Design & Method: Thirteen one Japanese women aged 44–58, with climacteric symptom were categorized into three group at random assignment : HRT group (n = 10), the KAMPO medicine (KSS) group (n = 12), and combination of two medication group (combination ) group (n = 9). We evaluated treatment effects of the climacteric symptoms by Self-rating Depression Scale (SDS), Hamilton Anxiety Scale (HAS), and Pittsburgh Sleep Quality Index (PSQI), and compared with each group at 0, 4, 8 weeks.
Results: There are no significant differences in the background among three groups at 0 week. KSS group and combination group significantly improved effects in SDS score (p values < 0.05). While, HRT group did not. On the other hand, all groups significantly improved HAS score and PSQI score (p values < 0.05).
Conclusion: Both KSS and HRT are acceptable as an effective treatment of climacteric symptoms. However, it is disclosed that KSS is suitable for subject with depression.
HRT and endometrium
PS-352
A COMPARATIVE STUDY OF INTRAUTERINE PATHOLOGY IN POSTMENOPAUSAL WOMEN USING HORMONAL REPLACEMENT THERAPY
G. Alexandris, K. Liargovas, S. Dritsas and P. Skolarikos
Helena Venizelou Hospital, 1st Department of Ob/Gyn, Hysteroscopy Unit, Athens, Greece
Aim: The aim of this study was to evaluate the role of hormonal replacement therapy, in intrauterine pathology for postmenopausal women.
Patients and Methods: 387 postmenopausal women were found with intrauterine pathology with TVS and office hysteroscopy.18%of the patients were taking HRT. Selected biopsies were taken and histological examination was performed for all patients.
Results: An increase in the endometrial thickness occurred significantly more often in women on HRT (p < 0,04). Abnormal uterine bleeding was found with similar results. The presence of endometrial polyps was 3 times higher in women on HRT. No difference in the incidence of endometrial adenocarcinoma was reported between the HRT and the non HRT group.
Conclusion: In postmenopausal women taking HRT we can confirm a higher incidence of benign intrauterine pathology which does not coincide with a higher incidence of malignant pathology.
PS-353
EFFECTS OF GLYCINE MAX IN ENDOMETRIUM OF CASTRATED FEMALE WISTAR RATS
C. R. Silva1,2, S. M. R. R. Lima1, D. L. Alves1,2, M. A. L. Galvão1 and T. Aoki1
1Santa Casa of São Paulo Medical School, São Paulo, Brazil; 2Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Objective: The aim of this study was to analyze the effects of Glycine max in endometrium of castrated female Wistar rats, comparing these results with placebo and estradiol valerate.
Methods: Twenty-four castrated adult female Wistar rats were divided into three groups (eight animals for each group) that received daily: tap water, estradiol valerate, isoflavones from Glycine max. The doses were equivalent to the usual doses applied for humans. After 21 days, animals were sacrificed and fragments of the uterus were submitted to routine histological techniques for morphometric study. The results were analyzed through endometrial histology, the expression of the estrogen receptor α and protein Ki67. The expression of α-receptors and Ki67 was assembled through immunohistochemical and morphometric analysis. Data from morphometric results were analyzed using Kruskal-Wallis non-parametrical ANOVA.
Results: The endometrium histology remained atrofic in herbal extract but the Glycine max supplementation enhanced the expression of α-estrogen receptors compared to placebo, without enhancement of protein Ki67 expression. The herbal extract presented a lower Ki67 expression compared to placebo.
Conclusion:Glycine max showed α-estrogen receptor stimulation in endometrium compared to placebo. The herbal extract reduced endometrial proliferation compared to placebo. This herbal extract may exert estrogenic stimulation without affecting endometrium in usual doses. Also, they might protect endometrial cells from abnormal proliferation.
PS-354
ENDOMETRIAL EFFECTS OF SUBDERMAL IMPLANTS OF ESTRADIOL AND TESTOSTERONE IN POSTMENOPAUSAL WOMEN
Adelmo Mauricio Botto de Barros Filho, Salvador Bahia (Brazil)
Introduction: Due to the protective effect of progestins on estrogen-stimulated endometrial proliferation, combined estrogen-progestin hormone replacement therapy is recommended for patients in the menopause who have not undergone hysterectomy. If the hypothesis is confirmed that testosterone may exert a protective effect similar to that of progestins on endometrial proliferation, combined estrogen/testosterone hormone therapy may avoid the side effects attributed to progestins.
Objectives: To analyze the effects of hormone therapy with subdermal implants of estradiol and testosterone on the endometrium and to compare them with the effects of hormone therapy already known to confer effective endometrial protection.
Study design: An open retrospective essay based on a review of the medical records of menopausal patients in use of combined hormone therapy consisting of implants containing estrogen and testosterone. The effects of this androgen on endometrial proliferation were analyzed.
Material & Methods: The incidence of endometrial thickening was evaluated by the ultrasonographic measurement of the endometrium of 258 menopausal patients in continuous use of combined hormone therapy with subdermal implants containing estradiol and testosterone for a continuous period of two years. Histology evaluation had been carried out on samples of thickened endometrium obtained during hysteroscopy with endometrial biopsy.
Results: At the end of the second year of implant use, ultrasonography detected endometrial thickening 44 of the 258 patients. The results revealed polyps as being the most common endometrial pathology, detected in 61,3% of patients with endometrial thickening, followed by normal endometrium in 31,8% of cases and myoma in 6,81% of cases. Histology confirmed diagnosis of endometrial polyp in 38,6% of cases, followed by normal endometrium in 31,8% of cases, simple hyperplasia in 20,45% of cases and, both, myoma e atrophic endometrium in 4,54% of cases.
Conclusions: In this study, the endometrial polyps were the most common pathology histologically confirmed. Our findings are similar to those observed in menopausal women using combined estrogen-progestogen therapy in which the progestogen protects the endometrium from the proliferative changes conferred by the estrogens on the endometrium, but does not protect against the development of polyps. Likewise, it is possible that testosterone exerts its antiproliferative effects on the endometrium but not on polyps. This study revealed a major incidence of simple endometrial hyperplasia, a low degree lesion, when compared with the continuous regimens with estrogens and progestogens. Therefore, the use of progestogens as the ideal endometrium protector must be reviewed.
PS-355
ENDOMETRIAL THICKNESS IN POSTMENOPAUSAL HORMONAL THERAPY : A CLINICAL RANDOMIZED TRIAL COMPARING ESTRADIOL IN ASSOCIATION WITH LEVONORGESTREL INTRAUTERINE SYSTEM OR WITH DROSPIRENONE
L. Schvartzman1,2, J. A. Magalhães1,2,3, F. M. Freitas1,2, F. Vigo1, V. Philipsen1, C. C. Pereira1, J. Azevedo1 and M. C. O. Wender1,2,3
1Faculdade de Medicina Universidade Federal do Rio Grande do Sul - Porto Alegre, Rio Grande do Sul, Brasil; 2Programa de Pós-graduação em Ciências Médicas- Faculdade de Medicina Universidade Federal do Rio Grande do Sul - Porto Alegre, Rio Grande do Sul, Brasil; 3Hospital de Clínicas de Porto Alegre, Rio Grande do Sul, Brasil
Objective: Menopause results from the cessation of ovarian function, which causes not only the end of woman's reproductive life but also several associated symptoms. Although Hormonal Therapy has its efficacy on relieving those symptoms, there are some remaining questions as the best dose and the ideal progestin administration route to protect endometrium, without other tissues significative effects. This protection should be achieved in a low dose basis or/and local hormone release. The main objective of this study is to compare endometrial effects and uterine bleeding patterns of two different types of hormonal therapy: levonorgestrel intrauterine system (LNG-IUS) and estradiol (1mg/d, p.o.) and oral association of drospirenone (2mg/d) and estradiol (1mg/d).
Design & Method: During a 1-year trial, investigators assessed the efficacy and effects of the LNG-IUS compared to drospirenone (2mg/d), both in association with estradiol (1mg/d). Patients (n = 36) were randomized to each group and the initial screening included transvaginal ultrasound and hysteroscopy with endometrial biopsy. Women kept menstrual calendars and reported any adverse effects; they were evaluated for several aspects (body weight, blood pressure, Kupperman menopausal index) every three months and their endometrium were reassessed by the end of the twelfth month (transvaginal ultrasound and hysteroscopy).
Results: Of 36 women eligible for the study, 15 in the LNG-IUS/estradiol group and 9 in the drospirenone/estradiol group have already completed the 12-month assessment. None of them reported any major adverse effect. Slight vaginal bleeding was reported in the first month of treatment by 9 patients of the LNG-IUS/estradiol group and none in the drospirenone/estradiol group; by the end of the treatment, only one patient, from the first group, reported that effect. Patients of the LNG-IUS/estradiol group have mean (±SD) endometrial thickness (pre-treatment) 4.57mm (±1.82) and final measures mean in this group was 5.07mm (±1.83). The drospirenone/estradiol group presented initial mean endometrial thickness of 4.42mm (±2.67) and final measures mean of 5.11mm (±1.83). There were no significative differences between groups (p = 0.857) nor by the time of measurement (p = 0.265).
Conclusion: The endometrial thickness assessed on transvaginal ultrasound of both groups remained in appropriate limits for postmenopausal women ongoing hormonal therapy. Our results suggest good endometrial protection in both HT regimens.
PS-356
ENDOMETRIAL ULTRASOUND ASPECTS OF POST MENOPAUSAL WOMEN USING RALOXIFEN ASSOCIATED WITH OESTROGEN
A. L. Carneiro, F. A. Sousa, M. G. Nunes, M. A. Haidar and R. C. Dardes
Department of Gynecology, Federal University of São Paulo, Brazil
Endometrial assessment of post menopausal women on oestrogen or raloxifen treatment is well described on literature. However, their association has been described briefly. The concomitant administration of oestrogen and raloxifen has been proposed by animal models experiments as it showed benefits on hot flushes along with endometrial and breast security. As women at righ risk for breast cancer, assessed by Gail's algorithm, seem to have also an increased risk for endometrial proliferation, they could benefit from this therapeutic.
Objective: To evaluate the endometrial thickness of post menopausal women at high risk for breast cancer after 6 months of administration of raloxifene and low dose oestrogen.
Methods: Sixty nine women were randomly allocated into 3 groups: conjugated equine oestrogen 0,3mg (GI), raloxifen 60 mg (GII) and conjugated equine oestrogen 0,3mg and raloxifen 60 mg (GIII) once daily. Ultrasound evaluation took place on initial visit and every 3 months. Histological endometrial evaluation was required if endometrial thickness were more than 4 mm.
Results: The mean age at randomization was 56,4 years and mean gail algorythm value was 2. The groups had no statistical differences at baseline. Endometrial thickness on baseline was 2,3; 2,0 e 2,0 mm for groups I, II and III respectively. After 3 months of treatment, no differences between the groups were noticed (2,6; 2,2 e 1,9 mm, respectively). On 6 months however, mean endometrial thickness were 3,4; 2,1 e 2,6 mm respectively. Groups II and III didn't have any differences on mean endometrial thickness throughout the study. On the other hand, group I showed a raise on endometrial thickness after 6 months of treatment (p < 0,05). Ten women had measures higher than 4 mm after 6 months (6 women from group I and 4 from group II) and they all underwent hystologic analysis of endometrial tissue. Both groups had 3 women each diagnosed as polipoid formation and the others had proliferative endometrium with no atipic cells.
Conclusion: This study evaluated endometrial thickness of post menopause women at high risk for breast cancer receiving the association of raloxifene 60 mg and conjugated equine oestrogen 0,3 mg for 6 months. No increase on ultrassonography parameters were seen during this study.
PS-357
EFFECT OF LOW DOSE HORMONE REPLACEMENT THERAPY ON ENDOMETRIAL AND UTERINE BLOOD FLOW IN POSTMENOPAUSAL WOMEN
Y. Zaydieva, A. Gus, G. Kurbanbekova, L. Ejova and L. Minosyan
Research Center for Obstetrics, Gynecology and Perinatology, Moscow, Russia
Objective: To study influence of various types of combined low dose hormone therapy on endometrium in early postmenopausal women.
Material and Methods: 86 women in early postmenopause with climacteric complaints 51,6 ± 4,2 years, duration of postmenopause 2,3 ± 3,2 years. All patients were randomized in 3 groups: 26 women (gr.1) were treated 1 mg Е2V + 2,5 mg MPA; 25 women (gr.2) -1 mg Е2V + 5 mg MPA and 35 patients (gr.3) - 1mg 17ßЕ2 + 5 mg DYD. Basely and at the end of the study we performed ultrasound evaluation of endometrium with Doppler and Pipelle biopsy to all participants. Results after 6 and 12 months of hormone therapy were compared with initial data.
Results: and discussion: Clinical efficacy treatment of climacteric syndrome was 93–96% (p < 0,001). After one year treatment in 1 gr. 98,3%, 2 gr. 98,3% and 3 gr. 98,5% women had amenorrhea. During screening period endometrial thickness did not differ between groups (p>0,05) and was 4–6 mm. At the end of the study M-echo did not significantly differ between groups (3,1–2,8–2,9 mm depending on HRT group). Blood flow was evaluated in 45(15 in each) patients. Basically, in all women vascular RI in uterine arteries were high: the relation S/D 11,6 ± 0,8 uterine (UA), 4,5 ± 0,3 in radial (RA) (p < 0,05) and the tendency to augmentation in arcuate arteries (AA) 5,8 ± 0,74. Uterine perfusion disturbances also influenced IR and PI. In all vessels IR were risen: UA 0,96 ± 0,08, AA 0,87 ± 0,03; RA 0,85 ± 0,02 (p < 0,05), as well as PI (UA 3,1 ± 0,1; RA 1,49 ± 0,07 and AA 1,93 ± 0,12) (p < 0.05), comparing with normal indexes in young women and did not significantly change during HRT. In all 3 groups initially endometrium was typical for postmenopausal atrophy: in 1 gr.- 90,79% women, in 2 gr. - 88,89%, in 3 gr. - 87%. At the end of the study atrophic endometrium was diagnosed in 1 group in 92,81% women (3% progestin type, 2% is not enough material), in 2 group in 94,66% (2% progestin type, 3% is not enough material), in 3 group in 94% (2% progestin type, 2% is not enough material).
Conclusion: Thus, there were shown high efficacy of low dose hormone replacement treatment in early postmenopausal women. Low dose hormone therapy does not change uterine blood flow, maintains atrophic endometrium and renders protective effect on it. According to histological data after 1 year of hormone therapy there were no cases of endometrial hyperplasia or cancer.
PS-358
EFFECTS OF TRIFOLIUM PRATENSE AND CIMICIFUGA RACEMOSA IN ENDOMETRIUM OF CASTRATED FEMALE WISTAR RATS
D. L. Alves1,2, S. M. R. R. Lima1, C. R. Silva1,2, M. A. L. Galvão1, A. Shanaider2 and T. Aoki1
1Santa Casa of São Paulo Medical School, São Paulo, Brazil; 2Federal University of Rio de Janeiro, Rio de Janeiro, Brazil
Objective: The aim of this study was to analyze the effects of Trifolium pratense and Cimicifuga racemosa in endometrium of castrated female Wistar rats, comparing these results with placebo and estradiol valerate.
Methods: Thirty-two castrated adult female Wistar rats were divided into four groups (eight animals for each group) that received daily: tap water, estradiol valerate, isoflavones from Trifolium pratense and deoxiactein from Cimicifuga racemosa. The doses were equivalent to the usual doses applied for humans. After 21 days, animals were sacrificed and fragments of the uterus were submitted to routine histological techniques for morphometric study. The results were analyzed through endometrial histology, the expression of the estrogen receptor α and protein Ki67. The expression of α-receptors and Ki67 was assembled through immunohistochemical and morphometric analysis. Data from morphometric results were analyzed using Kruskal-Wallis non-parametrical ANOVA.
Results: The endometrium histology remained atrofic in both herbal extracts but the Trifolium pratense supplementation enhanced the expression of α-estrogen receptors compared to placebo, without enhancement of protein Ki67 expression. Both herbal extracts presented a lower Ki67 expression compared to placebo.
Conclusion:Trifolium pratense showed α-estrogen receptor stimulation in endometrium compared to placebo. Both herbal extracts reduced endometrial proliferation compared to placebo. These herbal extracts may exert estrogenic stimulation without affecting endometrium in usual doses. Also, they might protect endometrial cells from abnormal proliferation.
PS-359
EFFECT OF THREE MONTHS OF LOW DOSE CONJUGATED ESTROGENS AND MEDROXYPOGESTERONE ACETATE (0.3/1.5 MG PREMELLE® Lite) ON BREAST, ENDOMETRIUM & CLIMACTERIC SYMPTOMS IN EARLY POSTMENOPAUSAL TAIWANESE WOMEN – A PRELIMINARY REPORT
Yu-Jean Chen1, Bi-Hua Cheng1,2, Ying-Chu Lin3, Fu-Tsai Kung1 and Ko-En Huang1
1Chang Gung Memorial Hospital, Kaohsiung, Taiwan; 2Chang-Gung University, Lin-kou, Taiwan; 3Kaohsiung Medical University, Kaohsiung, Taiwan
Objective: Low dose conjugated estrogens and medroxyprogesterone acetate (0.3/1.5 mg Premelle® Lite) was approved into Taiwan since mid 2007, based on that epidemiological studies indicate less risk of cardiovascular disease and venous thromboembolism in women who use low dose estrogens compared to standard dose. It has been shown to reduce hot flashes an average of 65% and relived climacterics as standard dose also. This report wants to share our experience about the effects of three months of Premelle® Lite on breast, endometrium when those early postmenopausal Taiwanese women tried to use it to relive climacteric symptoms in our hospital.
Design & Method: Healthy early postmenopausal Taiwanese women who suffered from her own climacteric symptoms and would like taking Premelle® Lite were enrolled from our menopausal consulting out patient clinic which routinely run those healthy evaluations for menopausal women, such as self-reported climacteric symptoms questionnaire, transvaginal sonography and breast echo and biochemical examination.
Results: There were 168 participants who took Premelle® Lite since during the period since mid 2007 to Jan. 2008 and had filled at least twice questions and been checked her own endometrial thickness twice. The mean age and SD was 53.6 ± 4.35 years old and mean months from menopause were 29.7 ± 22.8 months. Mean serum level of FHS and estradiol were 64.6 ± 40.37, 14.1 ± 24.27 separately. The climacteric symptoms for them to used hormonal therapy (HT) were mainly due to sleeping problems, dyspareunia, chest tightness and feeling dyspnea, fatigue. After three months of HT, the s/s as easily excited and agitated, feeling dyspnea, chest tightness, hot flush, no will to do sex with husband, dyspareunia with were significant, no will to go out were significantly relived a lot. The mean thickness of endometrium were 0.6 ± 0.03 cm before and 0.57 ± 0.03 cm after HT. The characteristics of breast echo were kept same was 60% after HT in those cohort cases. Others were shown cystic or fibroadenoma change. Conclusions We agreed that short term and low dose can relieve most of the climacteric symptoms without significantly effects on endometrium and breast. But, longer experience is still wanted. Key words: climacteric symptom, dyspareunia, endometrium, breast echo, conjugated estrogens and medroxyprogesterone acetate.
PS-360
ENDOMETRIAL HISTOLOGY AND SAFETY IN HEALTHY POSTMENOPAUSAL WOMEN AFTER A NOVEL REGIMEN OF TRANSDERMAL ESTROGEN AND VAGINAL MICRONIZED PROGESTERONE COMPARATIVE TO ORAL ROUTE OF HORMONE THERAPY. RESULTS AFTER 2 YEARS MONITORING
Manuela Russu, Dana Terzea* and D. Hudiţă
“Dr. I. Cantacuzino” Department of Obstetrics and Gynecology; *“V. Babeş” National Institute for Research, Development in Pathology and Bio-Medical Sciences; “Carol Davila” University of Medicine and Pharmacy, Bucharest, ROMANIA; e-Mail: [email protected].
Objective: endometrial histology and safety on non-oral (NO) comparative to oral (O) sequential hormone therapy (HT) in healthy postmenopausal women.
Materials and Methods: Assessment of 2 patients groups by microscopy at pre-study, after 12 and 24 months of HT: (days 9–11 of progestogen/progesterone phase of HT, after WHO classification: insufficient tissue, inactive/atrophy, proliferative, secretory, hyperplasia, carcinoma): 1) registered completely oral drugs (2mg/d estradiol valerate (E2 V) 21 days, E2V plus cyproterone 10 days; 2mg/d 17β micronized estradiol (E2 micronized) 14 days, E2 micronized plus dydrogesterone: 14 days); 2) 17 (estradiol patch (25 (g/d 21 days) plus oral MPA (10mg/ 5mg/day) last 12 days; 1g/day 17 (estradiol gel 28 days plus 200mg/day vaginal micronized progesterone last 12 days. All patients are comparable according to age, time since menopause, weight, height, smoking.
Safety was assessed in terms of prevention of estrogen- induced endometrial hyperplasia.
Statistic Analysis: Paired-sample t test was performed. Differences between O and NO patients were considered significant at P < 0.01.
Results: Microscopy registered after 12 months: inactive/atrophic endometrium in the groups completely oral (4:18%) vs NO (3:14%) and secretory changes in NO groups (25: 80.6%) vs O (14: 64%), with accentuation of this status after 2 years (atrophy: Oral 9: 47.3% vs NO 6:26%- and secretory: NO 16: 66.6% vs Oral 8: 42.1%); special mention for secretory changes when vaginal micronised progesterone (8: 80%); one case with simple hyperplasia without atypia after 24 months, on transdermal estrogen and 5mg MPA. No carcinoma registration.
Conclusions: Non-oral HT is endometrial safe for 2 years. Proliferative endometrium is rare after NO vs O: P<.01 (3.2% vs 9% at 12 months, 4.5% vs 10.8% at 24 months); secretory changes are more frequent after NO: P<.01 (80.6% vs 63.6% at 12 months, 51.6% vs 36.7% at 24 months), and atrophy is predominant after oral HT vs NO: P<.01 (9.81% vs 9.35% at 12 months, 40.5% vs 16.4% at 24 months). The case with hyperplasia after transdermal estrogen and 5 mg MPA (incidence 1/43 cases) is inside the oncological safety (2 cases/100 women year). The highest percentages of secretory changes are after vaginal micronized progesterone, decreasing rates with 10mg MPA, dydrogesterone and cyproterone.
PS-361
LEVONORGESTREL-RELEASING INTRAUTERINE SYSTEM FOR TREATMENT OF ENDOMETRIAL HYPERPLASIA: LONG-TERM FOLLOW-UP
O. Shawki, Mona Aboulghar and Waleed Sherbini
Department of Gynecology, Cairo university, Egypt
Objectives: Levonorgestrel (LNG), intrauterine delivery system has a prominent and profound effect on the histopathology of endometrium. The aim of the study was to use a LNG intrauterine system to treat non-atypical and atypical endometrial hyperplasia in women and to evaluate the long-term cure rate.
Methods: Each of the 12 women in the study, of whom five were diagnosed with atypical hyperplasia, received a LNG-IUS, releasing 20 microg LNG/day. The study is a non-comparative study with long-term follow-up (range 12–36 months).
Intervention: ultrasound, endometrial biopsy and hysteroscopy for follow up.
Results: All women developed a non pathological proliferative pattern of endometrium, except one asymptomatic woman with atypical hyperplasia who still had persistent bleeding and proved to be adenomatous hyperplasia at 16 monthes follow-up.
Conclusion: Continuous intrauterine delivery of LNG appears to be a promising alternative to hysterectomy for the treatment of endometrial hyperplasia and could enhance the success rate when compared with other routes of progestagen administration as well as intrauterine progesterone delivery.
PS-362
OUTPATIENT HYSTEROSCOPY FOR EVALUATION OF POST-MENOPAUSAL BLEEDING
Anupriya Agarwal1 and Yoke-Fai Fong2
1National University Hospital, Singapore; 2National University of Singapore
Post-menopausal bleeding is not uncommon and accounts for 5–7% of all gynecology referrals. Hysteroscopic evaluation of the endometrium followed by directed biopsy of suspicious lesions is the gold-standard for the evaluation of this symptom.
Objective: To evaluate the feasibility of outpatient hysteroscopy and endometrial sampling for evaluation of postmenopausal bleeding.
Design & Method: A retrospective analysis of 31 postmenopausal patients seen at the clinic between May 2005 and Dec 2007 was carried out. All patients were referred for post-menopausal bleeding and had oral or vaginal misoprostol (400 micrograms), 2 hours prior to the procedure. Outpatient hysteroscopy was done using the 5 mm flexible hysteroscope using normal saline as the distention medium. Pipelle sampling of the endometrium was done if required for endometrial assessment. Biopsy for any evident focal lesions was done under direct vision, using the rigid hysteroscope and biopsy forceps. A five-point visual analogue score was used to determine the pain score on four occasions during the procedure – at entry in to the external and internal cervical os, while inside the uterus and during the Pipelle sampling.
Results: Outpatient hysteroscopy was successfully performed in all except 3 (9.6%) cases. Thirteen (41.9%) patients had atrophic endometrium and were discharged. Endometrial polyps were found and successfully removed at the same setting in 7 (22.6%) patients. Two patients (6.4%) had submucous fibroids. Thickened suspicious looking endometrium was found in 2 (6.4%) patients; histological examination confirmed endometrial carcinoma in these patients. All except 4 (12.9%) patients tolerated the procedure well, with an average visual analogue pain score of 2.8/5. Pipelle sampling was reported to be the most painful part of the entire procedure, with an average pain score of 3.3/5 compared to 2.5 during negotiation of the internal os. Overall, hospital admission was avoided in 28 (90.3%) cases.
Conclusion: The outpatient hysteroscopy can be easily performed following by adequately trained gynecologists. It is a well tolerate procedure and is effective in reducing the number of hospital visits per patient as well as hospital admissions for inpatient hysteroscopy.
Miscellaneous
PS-363
A SURVEY ON THE CURRENT MANAGEMENT OF PREMATURE OVARIAN FAILURE IN PRIMARY CARE
H. Gauci Grech, E. Kalu and N. Panay
West London Menopause and PMS Centre, London, United Kingdom
Objective: Premature ovarian failure (POF) is defined as the triad of amenorrhoea, oestrogen deficiency and elevated levels of gonadotrophins in women less than 40 years of age. The incidence of POF is estimated to be 1–3% of the general population. Although POF is a distressing condition that negatively affects the life of a significant number of young women, many aspects of this condition remain an enigma. Issues regarding the diagnostic criteria and management still need to be clarified.
The aim of the survey was to assess the current management of POF in the primary care and to outline the need for a consensus on the diagnosis and treatment of this important condition.
Design & Method: Questionnaires were sent to 100 Primary Care Practioners in West London. 32 doctors replied. The following questions were asked:
At what age do you consider menopause to be premature?
After how many months of amenorrhea would you start investigating for premature ovarian failure?
What levels of FSH indicate premature ovarian failure?
Would you repeat FSH levels to make a diagnosis?
Do you think women with premature ovarian failure should be managed in primary, secondary care or both?
What treatment would you give for oestrogen replacement?
What dose of oestrogen would you prescribe?
For how long would you prescribe HRT?
Do you think that women with spontaneous premature menopause require?
contraception if they don't want anymore children?
Most doctors (84%) considered menopause to occur prematurely at an age younger than 40 years.
63% wait for 6 months of amenorrhea before investigating for POF. 9% wait for 8 months.
63% consider FSH levels above 20U/l to indicate premature menopause. 37% consider FSH to be in the range of menopause if above 30IU/l.
Most of the doctors would repeat FSH level once. 9% would not repeat it.
75% think that POF should be managed in both primary and secondary care.
75% prescribe HRT for oestrogen replacement. 22% would consider the oral contraceptive pill as an alternative. 3% won't prescribe any hormonal treatment.
56% prescribe 2mg oestradiol whilst 44% would prescribe 1mg oestradiol.
Most doctors would prescribe HRT up to the average age of menopause but 25% think that use of HRT should be limited to 5–15 years.
60% think that women with spontaneous POF don't require contraception.
PS-364
BCL-2 ANTIGEN AND TNF-ALPHA EXPRESSİON İN MYOMAS AT PERİMENOPAUSAL PERİOD
Uyar Yildiz, Nese Nalan, Baytur Yesim, Yildiz Hasan, Inceboz Umit and Kandiloglu Ali Riza
Faculty of Medicine, Celal Bayar University, Manisa, Turkey
Objective: Myomas which are the most frequently observed benign smooth muscle tumors of the uterus during reproductive age are also shown as the most important cause of menstrual bleeding complaints experienced during this period; however, their etiopathogenesis has not been fully clarified yet. In the present study, our aim was to examine Bcl-2 antigen, which is a physiological inhibitor of apoptosis, and TNF-α expression, which is thought to have a role in cell growth and differentiation, in myomas and explore their possible roles in the development and pathogenesis of myoma.
Design and Method: 30 cases (ages 41–50) applying to Celal Bayar University, Medical Faculty Hospital, Obstetrics and Gynecology outpatient clinic were included in the study. None of the cases were given hormone treatment and all were histopathologically diagnosed with “myoma uteri” after surgery. Our groups were myoma tissue (group 1), normal myometrium tissue (group 2) and myometrium tissue adjacent to myoma (group 3). In group 1, 2 and 3, the levels of TNF-α and Bcl-2 antigens were evaluated by calculating the immunohistochemical staining ratios. Statistical analyses were carried out using Mann-Whitney test and Kruskal Wallis test. p < 0.05 was considered statistically significant.
Results: The age interval of the 30 patients was 41–50 while the average age was (±SD): 45.83 (±2.97). The mean myoma diameter of the patients was 4.86 cm. It was found that, regarding TNF-α and Bcl-2 expression, myomas showed a higher positive histochemical staining rate compared to myometrium and myometrium tissue adjacent to myoma. Such a difference was not found between myometrium and myometrium tissue adjacent to myoma. In myomas, the mean staining rate for TNF- α was 60.75 while the average staining rate for Bcl-2 was 68.25. These figures were, respectively, 37.5 and 45 in myometrium and 38.25 and 37.5 in myometrium tissue adjacent to myoma.
Conclusion: The data obtained shows that TNF-α, whose regulatory mechanism in uterus has not been clearly understood yet, may have a role in the development of myoma. Likewise, showing Bcl-2 expression supports that inhibition of apoptosis may have a role in the pathogenesis. However, it is thought that examining presence of different cytokine and growth factors and their effect mechanisms may clarify the pathogenesis of myoma.
PS-365
COMPARATIVE ANALYSIS OF SURGICAL EXPECTATIONS AMONG PERI AND POSTMENOPAUSAL GYNECOLOGIC PATIENTS
S. P. González Rodríguez1, A. E. Henríquez Linares2, M. Belloso Martín-Mateos3, J. L. Lanchares Pérez3, M. H. García Sánchez3 and R. Sainz de la Cuesta2
1Gabinete Médico Velázquez, Madrid, Spain; 2Hospital Universitario de Salamanca, Spain; 3Hospital Quirón, Madrid, Spain
Objective: To describe pre-surgical expectations among peri and postmenopausal patients and to analyze differences between both groups.
Design and Methods: We recruited a total of 110 spanish patients among those subsidiary of gynaecological surgery at Salamanca's Hospital (Spain). All patients were given an explanation of the reasons of the study and all signed a consent form approving their participation in the investigation. A Gynecologic-obstetrical history and physical were performed and then patients were invited to fill a questionnaire designed to appreciate the pre-surgical expectations codified as “cured, improvement, no improvement but no worse, decreased worry associated to the problem” based on the socio-demographic and clinical characteristics of the patients, the preoperative diagnosis, the surgeon and the procedure itself. Data was analyzed based on the pre, peri or postmenopausal status of the patient, and finally, if it was a natural or surgical menopause. A descriptive analysis of the data of the sample was performed using variables and cases for its study applying SPSS v. 13.
Results: Data from 45 premenopausal patients, 47 with natural menopause, 10 with surgical menopause and 8 perimenopausal were collected. 37,7% expected a cure, 24,5% expected to stop worrying about this specific health problem, and 14,5 and 14,4% expected to stop developing the disease and improvement, respectively. There were no statistically significant differences regarding pre-surgical expectations based on the hormonal status of the patients. In addition we found no differences based on socio-demographic and clinical characteristics of the patients, nor in the pre-surgical diagnosis, surgeon or type of procedure.
Conclusion: Considering our small sample size, we found no significant differences between pre-surgical expectations in pre, peri or postmenopausal women.
PS-366
CAUSES THAT EXPLAIN THE LACK OF EFFECTIVENESS OF ISOFLAVONES OF SOYBEAN IN SOME WOMEN
J. Haya1, J. Allué2 and F. Perez-Lopez3, In representation of “Consensus Group” of the Spanish Society of Gynecologist Phytotherapy
1Universidad Autónoma de Madrid, Madrid, Spain; 2Universidad Autónoma de Barcelona, Barcelona, Spain; 3Universidad de Zaragoza, Zaragoza, Spain
Objective: There are metaanalysis that show level I of evidence in alleviating of hot flushes in the climacteric syndrome. Clinical experience shows many women who show marked improvement with this treatment. However, we also find others with lack of effectiveness. The aim of the authors was to investigate the possible causes that justify the lack of effectiveness in some patients.
Design & Method: We conducted a deep review of all the scientific literature published to explain the causes of the lack of effectiveness of isoflavones in some patients. Of all of these, we selected those that really showed biological or biochemical basis.
Results: We found that the main reasons that explain the lack of effect on some patients would be as follows:
Do not expect latency in the beginning of the therapeutic actions, which is estimated at between 4 to 10 weeks.
Little activity of the intestinal flora in the transformation of inactive isoflavones, together with side chains of sugars (natural form) to their active forms, without these sugar chains.
Patients with low processing capacity of daidzeine in equol.
Activity increased hepatic: smoking, alcohol, inducing liver … .
Dosage inadequate. The lowest effective dose is 40 mg/day of isoflavones. Dose minors will not produce any effect. The optimal dose, effective for the majority of women are 80 mg/day of isoflavones.
Using inadequate preparations; preparations not really provide the dose that indicate (some dietary supplements).
Using tamoxifen or raloxifene, which block the beta estrogen receptor in the hypothalamus.
We have waited latency time (until ten weeks).
The taking of isoflavones was with the main meal of the day, at which time there is an increased activity of intestinal bacteria.
Product that woman takes is not a nutritional supplement (not security in the dose that leads), but a specialty pharmaceuticals, with 80 mg/day of isoflavones.
Woman is no using tamoxifene or raloxifene.
PS-367
CHANGES OF ESTROGEN, PROGESTERONE RECEPTOR AFTER TRANSVAGINAL RADIOFREQUENCY MYOLYSIS
JinHong Kim, HyunHee Cho, EnJung Kim, YoungOk Rhew, GunYoung Chun, SeuYeoun Kim, InChul Jung and MeeRan Kim
Catholic University Medical College, Korea
Objective: The aim of this study was to investigate the changes in hormone receptors of myoma cells, clinical effectiveness, and volume decrement of myoma after high-frequency myolysis.
Design and Methods: From 2005 January to 2006 January, thirty patients who have had high-frequency myolysis were included in this study. They were all premenopausal women who d wanted to avoid other surgical interventions despite the need for them.
Needle aspiration biopsy was done at three sites that included the central portion of myoma before the operation and in six months after operation. Under guidance of ultrasonogram, high frequency myolysis was finished when the discoloration of myoma was accomplished to 80%.
To estimate its effectiveness in volume decrement of myoma, three-dimensional ultrasonography was used in 1st, 3rd, 6th, 12th and 18th month after radiofrequency myolysis. The stain intensity of estrogen receptor(ER) and progesterone receptor(PR) was classified into “negative”, “trace”, “weak”, “moderate” and “strong”.
Results: The volume decrement was 96.4% in the group that showed trace to week stain intensity (under 50% stain intensity), but it decreased to 66.6% in the group that showed strong stain intensity (over 50%, moderate to strong) (P<0.05). ER showed moderate to strong positive response in 79% of patients before operation, but it showed negative to week response in 83% of patients after the operation. Also, PR showed moderate to strong positive response in 80% of patients before operation, but it showed negative to week response in 86% of patients after the operation.
The degree of tissue necrosis in the group that had moderate to strong positive response of ER/PR was 0%/ 3% respectively, and that in the group that had trace to week positive response of ER/PR was 53%/ 50%. So, this result showed that the change of hormone receptor after the operation was proportional to the degree of the tissue necrosis (Pierson correlation coefficient: ER vs necrosis 0.65(P<0.05), PR vs necrosis 0.74(P<0.05)).
Conclusion: These results showed that the effect of high-frequency myolysis resulted from direct damage to myoma cells regardless of ER and PR and that decrease of hormone receptor was accompanied with damage of myoma cell. Also, to coagulate entire myoma, we suggested that controlling the intensity of operation by lengthening the time or expanding the extent of operation was more effective in treatment, because the volume decrement of myoma was larger in case that PR was under 50% before the operation.
PS-368
COMPARATIVE ANALYSIS OF MAXIMUM PHONATION TIME (MPT) BETWEEN WOMEN SINGERS IN MENACME AND POSTMENOPAUSAL WOMEN SINGERS TAKING OR NOT HORMONAL THERAPY (HT)
J. Mendes-Laureano, G. Salata Romao, R. Alberto Ferriani and M. F. Silva de Sá
Faculdade De Medicina De Ribeirao Preto Da Universidade De São Paulo, Brazil
Objective: Maximum phonation time (MPT) is one of the parameters of respiratory measurements. The sustained vowel test evaluates the ability of a patient to control the aerodynamic forces of the pulmonary current and the myoelastic forces of the larynx and represents a test of glottic efficiency. Thus the objective of the present study was to analyze comparatively the MPT of the sustained vowels /a/, /i/ and /u/ between soprano and contralto singers in menacme and menopausal and taking or not hormonal therapy (HT).
Design & Method: Of the 46 singers selected, 23 were contraltos, 3 of them belonging to the menacme group (women aged 20 to 40 years with regular menstrual cycles and taking no hormonal contraceptives), 5 to the HT group (women aged 45 to 60 years, in menopause for at least 2 years, taking no HT for at least 6 months), 8 belonging to the group taking no HT, in menopause for at least 2 years, taking no HT for at least 6 months), and 10 to the group taking no HT (women aged 45 to 60 years, in menopause for at least 2 years and taking no HT for at least 6 months). Of the 23 sopranos, 3 belonged t the menacme group, 8 to the HT group and 12 to the group taking no HT. The mean age of the contralto singers was 32, 58, and 57 years for the control, HT and no HT groups, respectively. The mean age of the sopranos was 30, 56 and 56 years for the control, HT and no HT groups, respectively. For each vocal type, the groups were analyzed comparatively regarding the MPT for the sustained vowels /a/, /i/ and /u/ by One-Way using the GraphPad Prism® software, with the level of significance set at 5%.
Results: The mean MPT (in seconds) for the sustained vowels /a/, /i/ and /u/ of contralto singers was 14 s, 15 s and 15 s for the menacme group, 12 s, 14 s and 14 s for the HT group, and 11 s, 14 s and 14 s for the group taking no HT, with no significant difference for the vowels between the groups analyzed. The means for soprano singers were 13 s, 14 s and 15 s for the menacme group, 12 s, 14 s and 14 s for the group taking HT, and 11s, 13s and 13s for the group taking no HT, with no significant difference for the vowels between the groups analyzed.
Conclusion: There were no relevant differences in MPT values between menopausal singers, singers taking HT and singers in menacme. Other parameters of vocal quality should be analyzed to better qualify the role of sex steroids in the female voice.
PS-369
EFFECT OF THE MENOPAUSE IN THE VOCAL EXTENSION OF WOMEN CHORAL SINGERS
J. Mendes-Laureano, G. S. Romão, R. Alberto Ferriani and M. F. Silva de Sá
Faculdade De Medicina De Ribeirao Preto Da Universidade De São Paulo, Brazil
Objective: The complaints between the women are frequent of whom alterations in the voice occur after the menopause, particularly the women singers emphasize problems affecting the high registers and control of the voice. In literature it has stories that the voice of the woman if modifies the menopause after. The objective of the present study was to evaluate comparatively the vocal extension measuring the frequencies minimum and maximum of the sung voice of women singers of choral of the menacme and after-menopause without hormonal therapy (TH).
Design & Method: Of the 30 singers selected, 15 were contraltos, 5 of them belonging to the menacme group (women aged 20 to 40 years with regular menstrual cycles and taking no hormonal contraceptives) and 10 to the HT group (women aged 45 to 60 years, in menopause for at least 2 years, taking no HT for at least 6 months). Of the 15 sopranos, 3 belonged t the menacme group and 12 to the HT group. The mean of age of the singers contralto had been 32 and 57 years and of soprano had been 30 and 56 years, for the groups it has respectively controlled and without TH. The groups had been analyzed comparatively how much the vocal extension measuring the frequency most acute (F2) and the frequency most serious (F1). The used statistical test was the One-Way for the o software GraphPad Prism®, considering the level of significance of 5%.
Results: The averages in hertz (Hz) of the value of F2-F1 in contralto had been 300Hz and 227Hz and in soprano 290Hz and 214Hz for group menacme and TH respectively not having significant differences between the analyzed groups.
Conclusion: Significant differences between the vocal extensions of women had not been found related singers of choral to the menopause.
PS-370
EFFECTS OF HEXESTROL IN MOUSE OVARIAN MORPHOLOGY
J. M. Soares Jr1, J. M. Oliveira1, E. C. Baracat2, M. C. P. Baracat3, R. S. Sim[otilde]es, A. G. Z. Rossi1, R. S. Sim[otilde]es1, T. C. Moraes1, M. G. Ribeiro1, J. Iavelberg1, C. C. Maganhin1 and M. J. Sim[otilde]es1
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil; 3Universidade de Santo Amaro, São Paulo, São Paulo, Brazil
Objective: To analyze histological aspects of the stroma and follicles of the ovaries of adult mouse treated anabolic agent hexestrol. Methods: Fifteen adult mice were divided into 3 groups: GI: Animals received a dose of 3mg/kg of hexestrol; GII: Animals received a dose of 6 mg/kg of hexestrol; GIII: animals received injections of distilled water (vehicle). Hexestrol was administered via intra-peritoneal once a day and the treatment lasted 30 days. Animals were sacrificed then ovaries were removed and submitted to histological routine for histological analysis with light microscopy.
Results: In mice treated with hexestrol (6mg/kg) (Group II), ovaries were smaller than controls but highly vascularized. A great number of follicles in several stages of development were found, however, with no corpora lutea. Also, it was possible to identify a great number of interstitial cells scattered in the stroma compared to GI and GIII. Conclusion: our data suggested that the hexestrol (6mg/mL) in high dose may decrease the ovulation in mice.
PS-371
EVALUATION OF AN ACCREDITED NURSE EDUCATION PROGRAMME FOR UK NURSES WORKING IN THE FIELD OF MENOPAUSE
K. Abernethy
North West London NHS Trust, Harrow, Middlesex, UK
Objective: To evaluate the first cohort to complete an accredited advanced course for UK nurses working in the field of menopausal health.
Design and Method: Nurses in the UK see and advise menopausal women independently from a physician and make treatment recommendations, often prescribing HRT and monitoring its safety and efficacy. However there is no requirement for nurses to complete an accredited education programme in menopause and nurses' knowledge can vary widely. This course was established to enable nurses to achieve and demonstrate a level of competence in this field of nursing expertise. Content of the course was as follows:
Physiology and psychology of menopause.
Menopause Symptomatology and long term biological effects.
Osteoporosis.
HRT Pharmacology and prescribing.
Complementary therapies used in menopause.
Evaluation, assessment and monitoring.
Multidisciplinary working and team skills.
Cultural, social and psychological aspects.
General menopause knowledge.
Physiology understanding.
Specific HRT prescribing knowledge.
Confidence in prescribing HRT.
Knowledge of therapies other than HRT.
Understanding of risks and benefits of various therapies.
Confidence in teaching others about menopause.
Conclusion: Based on these nurse evaluations, it would appear that some nurses are seeing and advising women with knowledge that they consider to be ‘poor’ and with little confidence. This course offers nurses the opportunity to improve their knowledge base and increase their confidence in menopause practice.
PS-372
HORMONAL REPLACEMENT THERAPY (HRT) HAS GONE THROUGH SEVERAL PHASES IN RECENT YEARS. ONE OF THE MAIN REASONS OF DRAWBACK IN HRT USERS IS THE HIGH COST OF THE TREATMENT. WHAT WOULD BE THE SITUATION IN A POPULATION WHERE THE PRICE OF THE TREATMENT IS NOT AN ISSUE?
Maria Cristina Portianko
Argentina
Objectives: Our group decided to evaluate compliance with HRT in a private population group with secondary and tertiary education.
Materials and Methods: 963 patients between 42 and 58 years old were evaluated from may 2006, to may 2007. 100% of this population had gone through primary and high school studies, and 46.3% had completed an university education. The main reason for consultation was,
68% seeked treatment for their symptoms, 51.8% accepted HRT and 48.2% non hormonal treatments. There was a 32.8% drawback rate in the first year. Main reasons of drawback,
The compliance rate concerning different options of HRT within a year was.
Conclusions: The main reason for drawback in the first year of use, in HRT users, without economic problems, and in properly informed patients, is fear and lack of confidence in the treatment.
PS-373
HORMONE REPLACEMENT THERAPY (HRT) IN POST MENOPAUSAL WOMEN AND MACULAR DEGENERATION RISK
C. Gavala, N. Kiriakopoulos, I. Aggos and A. Papadopoulou
Ippocratio General Hospital, Kos, Greece
Objective: In Western countries, age-related macular degeneration (AMD) is the one of the major causes of legal blindness in the population over 60 years of age. The purpose of our study is to assess the effect of post-menopausal hormone replacement therapy (HRT) on the presence and the severity of age related macular degeneration.
Design & Methods: A group of 72 women from 60 to 70 yrs under HRT at the time of the study or that had interrupted therapy recently after at least 3 years of treatment, as well as a control group of 54 women, of the same age group, were submitted to detailed clinical funduscopic evaluation and fundus photographs to determ AMD grading.
Results: The HRT and the non-HRT group did not differ in terms of early AMD prevalence. However women with AMD, who had used postmenopausal estrogen therapy in the past, had lower odds of advanced AMD than non-users.
Conclusion: Postmenopausal HRT may not affect the risk for early AMD but seem to have a beneficial effect of reducing the risk of advanced types of AMD in postmenopausal women.
PS-374
IMPORTANCE OF HORMONE REPLACEMENT THERAPY IN TURNER SYNDROME
Youn-Jee Chung, Hyun-Mi Shin, Jae-Yeon Song, Yong-Taik Lim and Mee-Ran Kim
The Catholic University of Korea, Kangnam St. Mary's Hospital, Seoul, Korea
Objective: Puberty is important in secondary sexual development and acquisition of bone densitometry. Adequate replacement of hormone replacement therapy is important to maintain secondary sexual development and maintain of bone mass in Turner syndrome. This study is about our hospital Turner syndrome patient's characteristics and their bone densitometry. The difference of BMD, before and after HRT means HRT is important in bone mass in Turner syndrome.
Design & Method: A retrospective study, Setting: a tertiary university hospital. Thirty Turner patients were examined by chart review from January 1998 to April 2007. Measurements The age, chromosome, complication, secondary sexual characteristics, hormone replacement therapy type and other growth hormone therapy, bone densitometry difference in HRT.
Results: Motive to first visit of Turner patient was prenatal diagnosis, undergrowth, low height in Pediatrics and they were treated with growth hormone and estrogen replacement therapy after this. Motive to first visit of Turner patient was primary and secondary amenorrhea in Gynecology and they were treated with estrogen replacement therapy after this. In 30 patients, 15 patients were treated with estrogen replacement therapy and 7 patients were follow-up loss and 8 patients were too young to treat with estrogen replacement therapy. The BMD and Z-score before and after estrogen replacement therapy shows meaningful improvement.
Conclusion: Estrogen replacement therapy is important to bone in Turner syndrome in their puberty.
PS-375
IN VITRO EFFECTS OF TIBOLONE AND ITS METABOLITES ON HUMAN VASCULAR CORONARY CELLS
F. U. Deuringer, A. O. Mueck, H. L. Kloosterboer and H. Seeger
University Women's Hospital of Tuebingen, Germany
Objective: Tibolone is a tissue selective compound with estrogenic, androgenic and progestogenic properties in classical bioassays. It is used for alleviation of menopausal symptoms and for osteoporosis prophylaxis in postmenopausal women. Only few data are available regarding the effects of tibolone on the cardiovascular system. We investigated therefore the in vitro effects of tibolone and its metabolites on the vasculature under special controlled conditions, using human female coronary endothelial and smooth muscle cells.
Design & Method: The effect on the production of the following markers in endothelial cells from human female coronary arteries was evaluated: nitric oxide synthase, prostacyclin, endothelin, plasminogen-activator-inhibitor-1 (PAI-1), E-Selectin, Intercellular adhesion molecule (ICAM-1), monocyte attracting protein-1 (MCP-1) and the precursor of matrix metalloproteinase-1 (pro-MMP-1). Tibolone, its metabolites, estradiol (E2), E2/norethisterone (NET) and E2/(medroxyprogesterone acetate (MPA) were tested at 0.1 μM and 1 μM. The markers were determined by enzyme immunoassays in the cell supernatant. Cell proliferation of smooth muscle cells from female coronary artery was measured by an adenosine triphosphate-assay.
Results: Tibolone, its 3-hydroxy metabolites, E2/NET, E2/MPA and estradiol alone had significant effects on the synthesis of all markers tested. The magnitude of the tibolone effects, however, was mostly smaller than that of E2/NET and E2/MPA. Concerning smooth muscle cells tibolone and its 3-hydroxy metabolites also elicited an inhibition of the proliferation compared to control values. The strongest effect here was found for E2/NET and E2 alone, whereas E2/MPA had no effect.
Conclusion: The results of this in vitro study conducted with cells of the most important vascular bed with respect to the problem of cardiovascular risk suggest that tibolone can positively influence the vasculature. However, these tibolone effects may depend on intact vascular cells and may vary due to the different atherosclerotic stages of the vessels. Thus, experimental studies are useful to explore mechanisms, but clearly cannot replace clinical studies.
PS-376
MEDICAL ATTITUDES CONCERNING PRESCRIPTION OF HORMONE REPLACEMENT THERAPY
A. C. Rodrigues, A. P. Domingues, C. Frutuoso, I. Torgal and C. F. de Oliveira
Coimbra University Hospital, Portugal
Objective: To analyse the attitude regarding hormone replacement therapy (HTR) of a sample of Gynaecologists/Obstetricians (GOs) and General Practitioners (GPs) and to investigate the differences between specialist and general practice.
Design & Method: To achieve our objective, we used an anonymous questionnaire, which included questions about time of onset, duration of treatment, therapeutic regimes, indications and contraindications to HRT, benefits and risks of HRT, and alternative treatments.
Results: Complete replies were received from 76 GOs and from 42 GPs. In both groups, the majority was female and significantly more menopausal female GOs were using or had used HRT (54%vs.15%, p = 0.028). More GOs than GPs offered HRT to all menopausal women assuming no contraindications (86%vs.41%, p < 0.0001). The main reason for not prescribing HRT was the risk of breast cancer. Significantly more GOs compared to GPs initiated HRT in the climateric period and were in favour of a longer treatment. Most of the GPs (50%) had no preferential regime for women with an intact uterus, while most of the GOs (53.9%) preferred to use a continuous combined regime. Use of tibolone was greater in the group of specialists (79%vs.57%, p = 0.012). Ninety-five percent of both groups regarded vasomotor symptoms as indications for HRT, but less GPs than GOs established premature (55%vs.87%, p < 0.0001) and surgical menopause (48%vs.75%, p = 0.003) as indications. Only a minority (20%) of both groups believed in cardiovascular benefit. Substantially more GOs felt that HRT prevents colorectal cancer (34%vs.7%, p = 0.001) and improves cognitive function (71%vs.36%, p>0.0001) compared to GPs. Recent breast cancer represented an absolute contraindication to treatment for all the doctors. For more GPs than GOs, family history of breast cancer (48%vs.28%, p = 0.024)) and diabetes (31%vs.11%, p = 0.007) was considered as an absolute contraindication. Alendronate was the most commonly used alternative to HRT.
Conclusions: The majority of doctors submitted to this questionnaire agreed that HRT is an effective treatment for women experiencing hot flushes and that it increases the risk of breast cancer. However, they expressed doubts about the place of HRT in cardiovascular disease.
PS-377
MULTIPROFESSIONAL EVALUATION OF CLIMACTERIC WOMEN HEALTH: IS THERE A DIFFERENCE BETWEEN MENOPAUSAL TRANSITION AND POSTMENOPAUSE?
I. C. Esposito1, L. H. L. Vieira1, M. A. Haidar1, I. Silva1, C. E. Bonduki1, R. Dardes1, M. C. P. Baracat2, M. G. Nunes1, E. C. Baracat3 and J. M. Soares Jr1
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Universidade de Santo Amaro, São Paulo, São Paulo, Brazil, 3Faculdade de Medicina de São Paulo
The aim of this study was to evaluate the health of women during the menopause transition and postmenopause through mutiprofessional analysis that includes ginecologist, physiotherapeutic, nutricionist and psicologist. Methods. The age of participants were from 38 up to 70 years-old. The volunteers were recruited through verbal convocation from June to August, 2005. After the study explanation, 115 women were submitted to medical history with questions on queries, personnal and familiar antecedents as well as the gynecology-obstetric data. We applied the following questionnaries: Kupperman-Blatt Menopausal Index, Women Health, Nutrition Health evaluation, simplified MHAQ – BRASIL. The patients were divided into two groups: a) Menopausal transition (n = 18) and b) postmenopause (n-94).
Results: There is not a difference in Kuppermann-Blatt Menopausal Index and Functional Capacity between both groups. The consumption of carboidrates, mainly sugars, in the postmenopausal women (65.6%) was higher than the menopausal transition ones (71.4%). We did not find significant differences in both groups on the MHAQ-Brazil questionnaire. Conclusion: Although we did not register significant differences between menopausal transitional and postmenopause in the analyzed parameters, the women presented a reduction in the life quality and functional capacity. In addition, the postmenopausal women had bad nutritional behavior that may contribute for increasing the weight and diabetes risk due to the consumption of sugars.
PS-378
ORIGIN, TREATMENT AND FINAL DESTINATION OF POSTMENOPAUSAL PATIENTS ATTENDING INTERCONSULTATIONS
M. Correa1, M. N. Rancel2, J. A. Cortell3, B. C. Ceballos3, J. F. De Luis3 and J. C. Alberto1
1Hospital Universitario de Canarias, La Laguna, Tenerife, Spain; 2Faculty of Medicine, University of La Laguna, Tenerife, Spain; 3Hospital U, Nuestra Señora de Candelaria, Santa Cruz Tenerife, Spain
Objetive: To analyse the specialities that requested interconsultations for postmenopausal women, the treatment these patients received and their final destination.
Material and Methods: Of the 3360 gynaecological consultations over a period of two years, 247 were interconsultations (7.35%) and 71 of these were postmenopausal (28.7%).
Results:
Origin: Specialities that requested interconsultations: 6 departments requested 66% of the interconsultations: 1. Surgery 17%; 2. Neurology 14%; 3. Oncology 10%; 4. Digestive 10%; 5. Urology 10%; 6. Cardiology 5%. The remaining 34% of the interconsultations were requested by another 13 specialists. 3 cases each: nephrology, internal medicine and rheumatology. 2 cases each: haematology, neurology, traumatology, preventive medicine and neurosurgery. 1 case each: geriatrics, rehabilitation, endocrinology, maxillofacial surgery and dermatology.
Final destination. 1. 4% of the patients did not attend the consultation; 2. Transfer to gynaecology for immediate surgical treatment 7%; 3. Referred back to department of origin 89%.
Outcome of patients referred back to department of origin (89%). 1. 24% did not receive treatment for anything genital; 2. Problems resolved during the consultation 5%; 3. Topical antiseptic treatment 11%; 4. Recommended for HRT 14%; 5. Evaluation completed for planned gynaecological surgery 27%; 6. Continuation of evaluation with a view to non-gynaecological pathological surgery.
PS-379
PREMENOPAUSE AND PREGNANCY WITH PRE-ECLAMPSIA AND OR ECLAMPSIA. FAST RECUPERATION, 0/1000 PUERPERAL ECLAMPSIA
Manuel Zuniga
Hospital Gineco-Ostetrico “Enrique C. Sotomayor” Guayaquil, Ecuador
Introduction: The dysfunctions of pre-eclampsia hypertension during the pregnancy constitute a complication of the gestation period and they are one of the big responsible affections, even today, of most of the maternal deaths; they are an important cause of morbid perinatal mortality. The form in the one that the pregnancy for itself stimulates and or increases the vascular hypertensive illness and their complications, is a question that continues without an answer, despite of the intense investigation that has been developed during decades. These dysfunctions still constitute one of the most important pending problems in obstetrics, as much in the pregnancy as in the puerperio.
Objectives: To know the reality of the incidence of complicated arterial hypertension with pre-eclampsia and of eclampsia in the premenopausic woman. To obtain a fast recuperation without puerperal eclampsia. To mainly correct the hemodynamic changes such as the hypervolemia and the systematic vascular resistance.
Methods: We show a sampling from January to December of 2003, among 430 hypertense patients with pre-eclampsia and or eclampsia, a group of 35 premenopausic patients were studied and treated in the surgical puerperio of the Gyneco Obstetric Hospital “Enrique C. Sotomayor” at Guayaquil-Ecuador. The patients had and age fm 40 to 49 years old, the same ones that suffered complicated arterial hypertension during pregnancy, with systolic blood pressure of 180 mmHg over 110 mmHg of the diastolic one with serious pre-eclampsia in 23%, with neurological symptoms. The eclamptic patients were in number of 3 (9%) during pregnancy. The group of 35 pregnant premenopausic patients and complicated arterial hypertension, whose age varies between 40 and 49 years old, received appropriate antihypertensive treatment with hidralazine, nifeditine, betablocking and metildopa in individualized form at the surgical puerperio. The relevant for the treatment was to correct the hemodynamic changes that exist in the puerperio like the hypervolemia, with the rigorous restriction of the liquids ingest. The patients were evaluated clinic and obstetrically and the following controls included clinic and laboratory exams.
In our continued studies, the sample covers 141 premenopausic patients, of a universe of 2303 premenopausic patients, analysed from January of 2003 until December of 2007.
Results: We confirm the absence to 0/1000 of puerperal eclampsia. The premenopause and pregnancy incidence was 8.13% with pre-eclampsia and or eclampsia. It was highly satisfactory, in the sampling of 35 puerperal premenopausic patients, to obtain a fast recuperation of the arterial hypertension between 48 up to 72 hours. In the 430 patients total group, which includes premenopausic and non premenopausic (young women) there was not any puerperal eclampsia, therefore this 0% incidence is highly satisfactory.
Conclutions: The correction of the hemodynamic dysfunctions such as hypervolemia with the rigorous restriction of liquids ingest together with the employment of the anyhypertensive ones constituted an appropriate treatment for these premenopausic hypertense puerperal patients that normalized its serious pressure between 48 up to 72 hours, decreasing the hospitalization time. Foregoing is confirmed during our continuos five years study.
PS-380
PERCEPTIONS OF MENOPAUSE AMONG MENOPAUSAL WOMEN LIVING WITH DISABILITY IN THE NORTHEAST OF THAILAND
P. Rukwong1, S. Chirawatkul2, M. Markovic3 and N. Nualnetr4
1Maharach Hospital, Nakonrachaseema, Thailand; 2Faculty of Nursing, Khon Kaen University, Thailand; 3Monash University, Melbourne, Australia; 4Faculty of Medical Technology, Khon Kaen University, Thailand
Objective: This study aims to explore how disabled women in northeastern part of Thailand or Isaan perceive menopause and manage the menopausal symptoms.
Design & Method: A mixed method including qualitative and quantitative study was employed at the Merng district of Khon Kaen city of the northeast of Thailand in 2006. Fifty one women living with disability participated in this study. In qualitative part, in-depth interviews and observations were used to generate qualitative data. The data were analysed using content analysis and thematic analysis. Triangulation was used to determine data rigor. Stratified random sampling was exercised in the quantitative part. Estrogens hormone deficit syndrome questionnaire was applied. Data was analysed by using descriptive statistical analysis.
Results: It is found that complaints of menopausal symptoms were very mild. Menopause is regarded as a natural event and it released them from a difficulty of dealing with menstruation. There are no any special health practices for menopause. Even though they concerned of osteoporosis but they did nothing. They heard about HRT and it is perceived as a pill for sexually active women.
Conclusion: Women living with disability welcome menopause. However, the ignorance of health practice and the inaccessible to health services during and after menopause may cause their lives more difficult later on.
PS-381
PERIMENOPAUSE AND THE USE OF MIRENA: A SEVEN YEARS ANALYSIS
M. Pommier1 and M. Pommier2
1Clínica Urbarí Santa Cruz Bolivia; 2Rochester Institute of Technology, USA Std
Objective: To determine the efficacy of Mirena® during premenopause as a contraceptive method, in association with myomas and metrorrhagia, and as hormone replacement therapy associated with estrogens, by establishing and evaluating the indication for its use, the symptoms that resulted, and the impact of these symptoms on the cause of premature extraction.
Methodology: The report examines the medical records of 72 patients presenting 167 indications (in some cases there are multiple indications for a single patient), who had Mirena inserted between December 2000 and December 2007. The report presents and analyzes data gathered during patient clinical controls, in which the physician identified the indications, recorded any resulting symptoms caused by the use of Mirena, and determined whether a premature extraction was necessary.
Results: During premenopause, the average age for insertion was 43.59 years old and for extraction it was 47.86 years old. During menopause the average age for insertion was 50.13 years old and for extraction it was 55.25 years old.
Indications: There were 64 indications with a premenopausal diagnosis; 16 associated to myomas and 25 to metrorrhagia. 54 patients used Mirena as a contraceptive method. 6 presented tubal ligation. 8 patients used Mirena during menopause.
Continuation rate or duration: In the premenopausal group, 36.11% reached five years of use. Among patients associated with myomas, 68.75% reached the first year of use, 18.75% reached five years of use. Among patients with metrorrhagia, 12.50% of patients reached five years of use. During menopause 62.50% reached five years use.
Symptoms and reasons for extraction: The most frequent symptoms associated with the use of Mirena were amenorrhea, vaginal infection, depression, spotting, weight gain, and loss of libido. The most common reason for extraction presented itself when a patient had more than one symptom related to a hormonal reaction to Mirena, including the association of any of the following: depression, hair loss, and libido reduction. Other symptoms included bleeding and persistent spotting, suspicious finding in the breast, weight gain (when exceeding 2kg/yr), and hysterectomy.
Discussion: The results of this study indicate that Mirena, despite symptoms and complications associated with its use, is an effective contraceptive method whose best application is during the premenopause phase and menopause, and as an alternative to hysterectomy in cases of menorrhagia and fibroids.
PS-382
PREMATURE OVARIAN FAILURE
R. Lermann, C. Julio, F. Ribeiro, T. Paula, A. Fatela and A. Martins
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: Premature menopause is a relatively rare disease. It is associated with amenorrhea, symptoms of estrogen deficiency, and gonadotrophin levels in the menopausal range before age 40 years. Most often, etiologic investigation is disappointing. The aim of this paper is to analyse all cases of premature menopause attending to our hospital.
Design & Method: We evaluated retrospectively all cases of premature menopause that were referenced to our hospital between 1999 and 2007. We analysed age at menopause, etiologic factors, associated diseases and comorbidities, diagnostic tools, the fertility prognostic and the therapeutic possibilities (hormonal replacement and treament of associated diseases).
Results: We reviewed 83 cases of early menopause. The mean age at menopause was 34,6 years old (min.- 18; max.- 39). Spontaneous menopause occurred in 65% (54 cases) and surgical menopause in 35% (29 cases), 3 of this cases were associated to cancer. 48,2% (40 cases) had anovulatory pill at least one year. Diabetes mellitus, hypotirodism and auto-imune disorders were found in 6%, 7,2% and 7,2% respectively. Hormonal replacement therapy was used in 93,8% of women. The mean duration of hormonal therapy was 8 years. Osteoporosis was present in 7,5%, hypertension in 7,5% and dyslipidemia in 25,6%.
Conclusion: Premature menopause diagnosis is important in order to explain the patient the variable natural history of the condition, to look for associated diseases, and, most importantly, to treat the hypogonadism preventing premature menopausal complications.
PS-383
RESEARCHES IN STROMAL FIBROSIS OF THE BREAST
M. J. Aldea, A. Cărăuleanu, D. M. Dumitru, G. Costăchescu and A. Pangal
University of Medicine and Pharmacy „Gr. T. Popa” Iaşi Romania
Objective: Stromal fibrosis of the breast is a histopathologic entity characterized by the obliteration of mammary acini and ducts by hypocellular fibrous tissue in peromenopause. The result is a localized or diffused area of fibrous tissue associated with hypoplastic mammary ducts and lobules. The purpose of this study was to evaluate the imaging features of stromal fibrosis of the breast (mammographic and ultrasonographic). The results were compared with histological findings at surgery.
Design & Method: We are presenting a prospective study of 41 cases of stromal fibrosis of the breast diagnosed and investigated in The Second Clinic of Obstetrics and Gynecology in Iasi. We analyzed the sonographic and mammographic findings according to the Breast Imaging Reporting and Data System. The results were compared with histologic findings after surgery.
Results: The patterns of fibrosis we described was categorized into the following two groups: masslike fibrosis (a discrete area of fibrosis containing few epithelial elements) and septal fibrosis (narrow bands of fibrosis). 60% of the women in our study had a personal history of benign breast disease. In all these cases we discovered chronic inflammation at the histopathologic examination. 7 lesions were palpable and 34 were impalpable. All of them were biopsied under sonographic guidance. Obtained images had variable appearances, not characteristic for stromal fibrosis. More than that, 25% of the images were suspected of breast cancer. All the patients underwent mammography. For 21 patients the lesion was mammographically occult, and for 5 of 41 patients the mammogram was concordant with the sonographic findings. The mammographic features of stromal fibrosis are more characteristic than the sonographic ones.
Conclusions: Our first concern, when establishing the diagnosis of stromal breast fibrosis is to eliminate the suspicion of breast cancer. This is mainly realized by the triple test of the breast examination: the clinical and the imagistic exams and the core guided biopsy. Both core guided biopsy and fine needle aspiration may extract breast tissue from an area located near an early malignant site which simulates a benign breast disease. In this situation, false-negative findings for cancer are obtained, with the possibility of discovering the malignant disease later. The main problem, in conclusion, is the early detection of a breast cancer which can simulate initially a benign process.
PS-384
REVIEW OF PREMATURE OVARIAN FAILURE
M. Guinot, J. Garcia, C. Medina, L. Santos, M. Amenedo, J. J. Espinós and J. Calaf
Hospital de la Santa Creu i Sant Pau, Barcelona, Spain
Objective: To review the most relevant elements related to premature ovarian failure (POF) observed in our Department. POF was considered to occur in secondary amenorrehea when high gonadotropin levels failed to induce an adequate ovarian response in the absence of bilateral surgical excision or oncologic treatments.
Design & Method: A retrospective observational study of patients (n = 87) fulfilling our criteria for POF who consulted to our Department from January 1992 to December 2007. Basal evaluation began with: hormone determinations (FSH, LH, E2, PRL and TSH). In all patients with high gonadotropins and low estrogens a complete inmunological study was performed including: antithyroid, antiphospholipid (lupic anticoagulant, anticardiolipin) and antinuclear (ANA) antibodies. Karyotype was complemented, up from December 1998, with a determination of FMRI permutations to detect molecular changes related to Fragile X Syndrome. Bone mineral density (BMD) was measured by dual X-ray energy and lipid profile was also performed.
Results: Mean age at the moment of diagnosis was 35,3 years (range 19 to 39 years). Hormonal mean values were; FSH 71,4 UI/L, LH 36,5 UI/l, E2 < 0,07 pg/ml. Hypertension was diagnosed in 7 patients (18,4%), dyslipemia in 15 (22,72%) and hyperprolactinaemia in 8 (4 of them were macroprolactinaemias). 20 (22.98%) patients had familiar history of POF.
In 11 patients thyroidal work up was abnormal. In two cases ooforitis was diagnosed after an incidental ovarian biopsy.
In 29 cases (39,72%) positive antibodies were detected: 13 patients with ANA, 13 patients with antithyroid antibodies (6 of them were previously diagnosed of thyroideal pathologies),12 patients with antiphospholipid antibodies, and none of them presented antimitochondrial antibodies.
We found minor previous ovarian surgery (biopsy/cyst exeresis) in 4 patients, major surgery in 4 patients (unilateral anexectomy).
Six patients presented abnormal karyotyp: 2 mosaicisms (45X/isochromosome X, 46XX/47XXX), and 1 inversion of cromosome 9, one Turner Syndrome(45XO) one multiple alteration and one XY. 9 patients had FMRI permutations, 6 of them with abnormalities pending of final evaluation.
In 31 of these women, we identificated BMD alterations, 21 presented osteopenia (11 lumbar, 2 femoral, and 8 both), and 10 osteoporosis (5 lumbar,1 femoral and 4 lumbar and femoral).
In 66 cases women hormonal therapy was prescribed, in 55 with natural estrogens and in 11 with oral contraceptives.
Conclusion: A diagnosis of POF deserves a complete work up including karyotype and fragile X study. The incidence of early BMD decreases justifies the prescription of adequate hormonal therapy.
PS-385
ROLE OF JNK1 AND JNK2 IN MURINE OVARIAN GERM CELL APOPTOSIS
M. R. Kim1, I. S. Lee2, H. K. Lee3, J. E. Chung4, J. H. Kim1 and J. H. Kim1
1The Catholic University of Korea, Seoul, Korea; 2Soonchunhyang University, Seoul, Korea; 3H-Cube Hospital, Seoul, Korea; 4Wongkwang University Sanbon Medical Center, Sanbon, Korea
Objective: Each female is endowed with a finite numbers of oocytes, which when depleted leads to ovarian senescence, the menopause. The objective of this study was to investigate the role of JNK1 and JNK2 in murine ovarian germ cell apoptosis.
Design & Method: Murine oocytes were retrieved by superovulation of female C57BL/6 mice at the age of 21–24 days. At 10 minutes after UV irradiation, immunocytochemistry was performed. Ovarian granulosa cells were cultured from antral follicles. At the 24 hours of the culture period, UV was irradiated on culture dishes. After 30 minutes, protein was extracted and western blotting done. Serial ovarian sections were stained with modified Lee's picric methyl blue, and we estimated the numbers of oocyte−containing primordial, primary and small preantral follicles of female mice at day 4 and day 42 postpartum. Ovarian granulosa cells were cultured from female wild-type and JNK1-/- or JNK2 -/- mice. The granulosa cells were fixed at 2, 4, 6 hours after UV irradiation and stained with Hoescht 33342, and then evaluated for characteristics of apoptosis under fluorescence microscopy.
Results: After UV irradiation, oocytes showed intense signal of phospho-JNK. In ovarian granulosa cells, JNK was activated to phospho-JNK after UV irradiation. There was no difference in oocyte counts between wild type and JNK1 -/- or JNK2 -/- at day 4 and day 42 postpartum. The incidence of apoptosis of ovarian granulosa cells from wild type were 13.0 ± 3.3%, 22.2 ± 12.8%, 32.0 ± 10.4%, 42.9 ± 11.3% after 0, 2, 4, 6 hour of UV irradiation, respectively. The incidences were 10.5 ± 4.1%, 18.3 ± 9.1%, 24.8 ± 9.1%, 29.5 ± 12.4%, respectively in granulosa cells from JNK1 -/- mice. These results showed only a partial suppression of apoptosis in granulosa cells from JNK1 -/- mice, however, it was not statistically significant. There was no significant difference in the rate of apoptosis of granulosa cells after UV irradiation between wild type and JNK2 -/- mice.
Conclusion: JNK1 and JNK2 are recognized as critical regulators of various aspects of mammalian physiology, including cell proliferation, cell survival and cell death. This study showed that UV irradiation caused activation of JNK in murine oocytes and granulosa cells of ovary. In murine ovary, JNK1 and JNK2 may be redundant or have compensatory role to each other in apoptosis.
PS-386
SURGERY IN POSTMENOPAUSAL WOMEN WITH ADNEXAL BENIGN TUMOURS
M. A. Nieto Naya, M. Padilla Castillo, R. García Rodríguez, P. López Gutiérrez, M. Sosa Marrero and D. Madera
Hospital Universitario Materno Infantil de Canarias, Póster
Objective: To analyze the outcomes and complications of menopausal women with adnexal masses without clinical or ultrasonographic findings of malignancy, who undergo a surgery procedure.
Material and Methods: We reviewed the medical records of 13 postmenopausal patients who underwent surgery in our hospital between January and December 2007, due to adnexal tumour finding, without clinical or ultrasonographic findings of malignancy. The following items were analyzed: demographic data, age, complications, tumour markers, laparoscopic findings and anatomopathological study.
Results: The median age of these patients was 61.4 years (range 53–82). Tumor markers (CA 19.9, CEA, AFP, Ca 125, β-hcG, CA 15.3) were negative in all cases. As well, all patients underwent laparoscopic surgery. In 1 case (7.7%), the laparoscopy had to be reconverted to a laparotomy because of uncontrollable bleeding. In 2 cases (15.4%), the surgeon decided to do a laparotomy due to the laparoscopic examination (1 case due to technical problems, 1 case due to macroscopic appearance of malignancy). None of the patients presented postoperative complications.
The anapathological studies reported: 33% mature teratomas, 41.7% serous cystoadenomas, 8.3% endometriomas, 8.3% symple cysts, 8.3% borderline tumours (1 case, which was referred to the Gynaecologyc Oncology Unit to carry out a complete study and treatment).
Conclusion: Laparoscopic surgery in menopausal women with adnexal tumours assumed to be benign, is a satisfactory procedure, with a lower rate of postoperative complications, morbidity, mortality and length of hospital stay, compared to laparotomic procedures.
PS-387
TIBOLONE USE FOR DRY EYE SYNDROME TREATMENT
F. L. Moggia1, M. S. Moggia2, A. M. Todone1, R. D. Diaz1, R. Peruyera1, C. Lampropulus1, D. Dominguez1 and M. S. Larroude
1Hospital Gral. de Agudos Parmenio Piñero, Buenos Aires, Argentina; 2Centro TIEMPO, Buenos Aires, Argentina [email protected]
Dry eye syndrome is a disorder of the tear film that affects the interpalpebral ocular surface determining specific sings and symptoms. Androgens modulate Meibomian glands –which produce the lipid secretion of the film- through de androgenic receptor and the 5-alfareductase enzyme. It was suggested that the androgenic deficit may be the cause of dry eye syndrome. The androgenic action of tibolone may be of therapeutic use.
Objective: to evaluate the ophthalmologic response to tibolone, in postmenopausal women with dry eye syndrome.
Design and Method: 5 postmenopausal women, mean age 52.2 (50–54) with dry eye syndrome symptoms and altered tear production evaluation tests (Break-up time -BUT- and Schirmer test).
Dry eye syndrome symptoms questionnaire and tear production evaluation tests were performed at baseline and after six months tibolone therapy (1.25/2.5 mg/day). Primary indication for tibolone was climacteric syndrome treatment.
Results: all the patients referred improvement of their specific symptoms after six months therapy. Three patients showed normalization of functional tests. One exhibited BUT normalization and Schirmer tests results near the normal limit. The last one remained with both function tests results altered.
Conclusion: tibolone was objectively useful in 80% of the cases. Correlation of these results with larger study populations is warranted. In order to assess tibolone secondary benefit for dry eye syndrome within the context of climacteric syndrome, further research is necessary.
PS-388
THE CONGRUENCE BETWEEN THE REASONS FOR CONSULTATIONS AND THE DIAGNOSES GIVEN IN POSTMENOPAUSAL PATIENTS
M. Correa1, M. N. Rancel2, B. C. Ceballos3, A. Gimeno3, S. Iglesias3 and F. R. Martín3
1Hospital Universitario de Canarias, La Laguna, Tenerife, Spain; 2Faculty of Medicine, University of La Laguna, Tenerife, Spain; 3Hospital U, Nuestra Señora de Candelaria, Santa Cruz Tenerife, Spain
Objective: To analyse the reasons for the requested consultation and the diagnosis given by gynaecologists and how much agreement there was between them.
Material and Methods: 71 patients who presented with problems related to the menopause were referred for gynaecological assessment. They constituted 28.7% of 247 interconsultations in a total of 3360 gynaecological consultations carried out over a two-year period.
Results:
Reasons for consultations. They are summarized here in ten diagnoses: 1. leukorrhea 22%, 2. metrorrhagia 16%, 3. abdominal pain 14%, 4. tumour still to be diagnosed 11%, 5. urinary incontinence 10%, 6. pelvic mass 8%, 7. prolapse 7%, 8. climacteric symptoms 6%, 9. fistula 4%, 10. swelling in the bladder 2%.
Diagnoses given. Also divided into ten groups: 1. no genital pathology 23%, 2. vulvovaginitis 14%, 3. menopausal symptoms 13%, 4. metrorrhagia 12%, 5. genital tumour 10%, 6. cystorectocele 9%, 7. prolapse 7%, 8. cervical pathology 4%, 9. fistula 3%, 10. others 5%. 3 patients did not attend the consultations.
Congruence. There was agreement in 58% of the consultations, and no agreement in 18%. The consultation was justified in 24% of the cases even though no agreement was reached.
PS-389
THE POLY-MEDICATION OF THE MENOPAUSE. THE USE OF MULTIPLE DRUGS IN ADDITION TO HORMONE THERAPY, A REPORT FROM A SINGLE RESEARCH CENTRE IN ARGENTINA
A. Mirkin1 and R. Diaz2
1Hospital E. Perón. School of Medicine. National University of Rosario-Argentina; 2ECLA (Estudios Clínicos Latinoamericanos)
Objective: The objective of this study is to asses and critically analyse the use of the various drug in a cohort of 119 postmenopausal women that were evaluated at a single research in Rosario, Argentina.
Design & Method: prospective cohort study. Subjects were evaluated and it was recorded the type of HT that they were on,as well as any medication that they might be taking. The indication for this additional medication was also recorded.
Results: From the 119 women evaluated,100% were taken additional medication for different complaints:
Sexual Disfunction: 40 women (34%) use vaginal cream for painful intercourse.
Cardiovascular Disease: 49 women (41%) had hypertension and in 15 cases(14%) they ignored the problem. The vast majority take antihipertensive medication and low salt intake.
Sixty per cent of the women had BMI > 30.
High level of lipids (49 women) take statins or ezetimibe.
Sleep disturbance: 82% (97 women) take sedatives or psycotropic medication mainly for insomnia given for other physician.
Hormonal Therapy: For treat moderate or severe hot flushes the medication was Premarin 0,3,Tibolone or Estradiol + Drosperinone.
Miscellaneous: other medication: levotiroxine, orlistat, metformine, aspirine, folic acid, alendronate.
Conclusion: as it well know HT is effective to treat VMS,VVA and prevent osteoporosis.
However, in our preliminary study it was determine that 100% of the subjects evaluated were taken additional medication for various reason.
Our study indicates that the HT is only one of the many medication prescribe for menopausal women. In addition, menopausal care is a unique opportunity to provide primary and preventive medicine.
PS-390
TOLERABILITY OF DIFFERENT ORAL IRON FORMULATIONS: A SYSTEMATIC REVIEW
C. Castelo-Branco1, M. J. Cancelo-Hidalgo2, S. Palacios3, J. Haya-Palazuelos4, M. Ciria-Recasens5, L. Perez-Edo5 and J. Manasanch6
1Hospital Clínic i Provincial, Barcelona, Spain; 2Hospital Universitario de Guadalajara, Univ. de Alcalá de Henares, Guadalajara, Spain; 3Palacios Women's Health and Medicine Institute, Madrid, Spain; 4Hosp. Univ. Sta. Cristina, Univ. Autónoma de Madrid, Madrid, Spain; 5Hospitales Universitarios del Mar y de la Esperança, Barcelona, Spain; 6Pierre Fabre Iberica S. A., Barcelona, Spain
Objective: Gastrointestinal intolerance is one of the most common adverse effects associated with oral treatment for iron deficiency. Several formulations have been marketed in an attempt to reduce it. The aim of this systematic review was to compare the incidence of adverse drug reactions (ADR) and gastrointestinal adverse drug reactions (GADR) associated with several oral iron salts.
Design & Method: A systematic review of clinical trials published from 1966 until January 2007 was performed in biomedical (EMBASE, PubMed y Cochrane Library Plus) and manufacturers' data-bases to identify clinical studies reporting safety data. The endpoints evaluated for each iron salt included were incidence of ADR and GADR.
Due to the difference in dosage reported in the clinical trials, for the GADR analysis the incidence was compared among the iron salts taking into account the most widely used daily dose (80–120 mg of elemental iron).
Results: A total of 49 publications informed about ADR including data from more than 5,400 patients (table 1). The lowest incidence of ADR was observed for ferrous sulphate plus mucoproteose and iron protein succinylate. Related to GADR, 24 publications reported data (table 2).
Table 1 Incidence of ADR
Table 1 Incidence of GADR
Conclusion: Ferrous sulphate with mucoproteose and iron protein succinylate had the lowest incidence of ADR and GADR among the iron salts analysed.
PS-391
TRANSVAGINAL RADIOFREQUENCY THERMAL ABLATION: A DAY-CARE APPROACH TO SYMPTOMATIC UTERINE MYOMAS
HyunHee Cho, MeeRan Kim, JinHong Kim, JangHeub Kim, SueYoun Kim and InChul Jung
Catholic University Medical College, Seoul, Korea
Objective: In myoma patients, the traditional surgical treatment of choice is myomectomy for women who wish to retain their uterus. However, myomectomy must be performed under general anesthesia, and the patient requires a long time to recover. In the present study, we report our experience with a group of patients who underwent transvaginal radiofrequency (RF) thermal ablation of uterine myomas, with emphasis on the safety and efficacy of this procedure.
Design and Methods: Premenopausal women with symptomatic uterine myoma or recently growing myoma were included in this study. The pre- and postoperative myoma volumes were measured by 3D ultrasonography. The impact of the symptoms on health-related quality of life (HRQL) was assessed using the Uterine Fibroids Symptom and Quality of Life (UFS-QOL) questionnaire.
Results: The mean initial size of the dominant myoma was 5.3 cm (SD, ± 1.58). The reoperation rate was 4.3%. The final reduction rate of the volume of the dominant fibroid was 73%. The symptom scores and HRQL scores showed great improvement after 18 months of myolysis.
Conclusions: The results of this study suggest that RF ablation may represent a safe, well-tolerated, and effective day-care alternative to conventional surgery for the treatment of uterine myomas.
PS-392
TREATMENT COMPLIANCE WITH A CALCIUM AND VITAMIN D COMBINATION AMONG SPANISH PATIENTS: ADHERENT PATIENT'S PROFILE VS. NON PERSISTENT PATIENT (THE UNICAD STUDY)
C. Castelo Branco1 and X. Cortés2
1Hospital Clínic i Provincial de Barcelona. C/ Rosselló 163, 3a planta, 08036 Barcelona. E.mail: [email protected]; 2Procter & Gamble Pharmaceuticals Iberia, S.L., WTC Almeda Park, Edificio 1, 2a planta, Plaça de la Pau s/n, 08940 Cornellà de Llobregat, Barcelona. E.mail: [email protected].
Objectives: In spite of the proved efficacy of calcium and vitamin D supplementation (CaVD) on the bone mass loss and fracture prevention, it is known that a considerable number of patients abandon treatment or show poor compliance. Adherence to CaVD for Spanish patients is unknown. The UNICAD study was designed to determine current figures, in order to study patient profile in terms of adherence.
Design and Methods: 1,342 primary care physicians, traumatologists, rheumatologists and gynaecologists, recruited both gender patients aged 45 or over, who were prescribed with CaVD at least 1 year prior. Bio-demographic, relevant clinical history data, reason for prescription and fracture risk factors were collected in a single visit. Non persistent patients (NPP) were assessed, and compliance determined by Morisky-Green test (MG). Persistent patients showing good compliance were considered adherents (AP). AP and NPP profiles were described.
Results: Of the 7,624 patients studied, mean age 65.7 years and mean BMI was 26.0 Kg/m2, 94.2% were women, the majority postmenopausal, being CaVD generally prescribed 2–5 years prior due to osteoporosis (56.3%). More frequent conditions were osteoporosis family history (41.4%) and previous fractures (40.7%). 1 year or more after prescription, 27.7% were NPP, reasons being: tiredness for long term treatment and the inconvenience of the regimen conditions. Among patients continuing with treatment (72.3%), MG answers indicated that the 31.2% were APs. These patients showed lower mean age, higher studies degree, frequent osteoporosis family history and were living alone less frequently. Among NPPs, smoking, alcohol consumption, long immobilization history, malabsorption syndrome and previous bone fractures were more likely.
Conclusions: 1 out of 4 patients had discontinued the CaVD treatment 1 year or more after its prescription, and those continuing, only 3 out of every 10 patients showed good compliance. For NPPs, the highest accumulation of risk factors for suffering bone fractures has been detected.
PS-393
TREATMENT OF MINOR BENIGN GENITAL ALTERATIONS IN THE PREMENOPAUSAL YEARS WITH ETHYNIL-ESTRADIOL AND DROSPIRENONE
F. R. Pérez-López1 and J. Haya2
1Zaragoza Clínico Hospital, Zaragoza, Spain; 2Universidad Autónoma de Madrid, Madrid, Spain
Premenopausal women with menstrual disorders represent a major public health problem. The purpose of the study was to determine the clinical response to the combined treatment with ethynil-estradiol (EE) and drospirenone (DROS) in premenopausal patients (age > 45 years) with benign menstrual disorders like menorrhagia, endometrial hyperplasia, premenstrual syndrome, fluid ovarian cysts, endometriosis-related dysmenorrhea. One hundred twenty seven premenopausal women were submitted to systematic evaluation including hematologic analysis, ultrasound scan, pap smear, and biopsy when needed to discard cancer or any other specific severe condition. 74 of these patients were previously seen at the emergency facilities, and 11 cases had endometrial hyperplasia in the biopsy. After informed consent was signed, all patients completed a 6-month hormone treatment consisting in combined administration of EE + DROS. The clinical results included: improvement of premenstrual symptoms in 35/64 patients, reduction in the amount of bleeding in 112/127, reduction in dysmenorrhea intensity or duration in 32/54. All patients with anemia at the beginning of the study (n = 23) presented normalization of hematocrit and hemoglobin levels after 6 months of treatment (p = 0.05). Besides menorrhagia, important consequences of bleeding disorders in premenopausal women include iron deficiency anemia, miscarriage, postpartum bleeding, uterine bleeding and hysterectomy. The use of the combined EE + DROS can be effective in controlling uterine bleeding secondary and other symptoms even in the absence of reduction of uterine volume.
Genetics of menopausal complications
PS-394
A DIGENIC COMBINATION OF POLYMORPHISMS WITHIN NRIP1 AND BMP15 GENES IS ASSOCIATED WITH AGE AT MENOPAUSE IN THE SPANISH POPULATION
N. Mendoza Ladrón De Guevara1, F. Morón2, T. Martínez-Astorquiza3, A. Ruíz2, F. Quereda4, M. E. Sáez2, R. Ramírez-Lorca2, F. Vázquez5, A. González2, R. Sánchez-Borrego6, E. Molero2 and A. Salinas2
1Hospital “Virgen de las NIeves”, Granada, Spain; 2Genomica estructural Neocodex, Sevilla, Spain; 3Sanatorio Bilbaino, Bilbao, Spain; 4Hospital San Juan, Alicante, Spain; 5Clinica GEOGA, Lugo, Spain; 6Clinica DIATROS, Barcelona, Spain
Objective: The BMP15 gene is a di-exonic gene that encodes a preproprotein activated by proteolytic processing. Direct evidence of the role of BMP15 gene in a high follicles production in mammals, strongly suggest that this oocyte factor might play a key role in an early age at menopause and consequently in premature ovarian failure (POF) phenotype. Recently, three new studies have reported different variants located within BMP15 gene in patients with POF.
Methods: To analyze four single nucleotide polymorphisms (−673C>T, −9C>G, IVS1+905A>G and N103S) located in BMP15 gene in 1,190 postmenopausal women (901 natural menopause), in order to find the role of this gene in relation to age at menopause. We performed a quantitative trait locus (QTL) study of these markers individually or in digenic combinations with other markers located at different candidate genes related to the oestrogen signaling pathway: FSHR (S680N), ESR1 (PvuII), ESR2 (*39A>G), NRIP1 (G75G), CYP19A1 (*19C>T) in relation to age at menopause.
Results: None of studied markers in BMP15 gene was significantly associated with age at menopause or praecox menopause (before 45 years of age). In contrast, linear regression analysis suggests epistatic interactions including, BMP15 and NRIP1 loci in relation to onset of praecox menopause in our series (p = 0.046). Specifically, we have observed that BMP15 IVS1 + 905A>G AG/NRIP1 G75G AA combined genotype appears to be associated with a lower mean (SD) age at menopause [46.1 (5.9) vs 48.6 (4.8); p = 0.002], and a shorter reproductive period [33.6 (5.9) vs 35.6 (4.9); p = 0.017] in the Spanish population.
Conclusions: Our results suggest that BMP15 gene may contribute to variance in age at menopause and reproductive period in a complex manner.
PS-395
A DIGENIC COMBINATION OF POLYMORPHISMS WITHIN ESR1 AND ESR2 GENES ARE ASSOCIATED WITH AGE AT MENARCHE IN THE SPANISH POPULATION
R. Sánchez-Borrego1, F. Quereda2, F. Morón3, A. Ruíz3, M. E. Sáez3, F. Vazquez4, T. Martínez-Astorquiza5, R. Ramírez-Lorca3, A. González3, E. Molero3, C. Moreno3 and N. Mendoza6
1Clinica DIATROS, Barcelona, Spain; 2Hospital San Juan, Alicante, Spain; 3Genómica Estructural Neocodex, Sevilla, Spain; 4Clinica GEOGA, Lugo, Spain; 5Sanatorio Bilbaino. Bilbao, Spain; 6Hospital Virgen de las NIeves, Granada, Spain
Objective: The age at menarche (AAM) can be considered a pure complex parameter that depends on the interaction of a myriad of factors including environmental, genetic and socio-economic elements In the present study we will look at the role of genetic variants within oestrogen synthesis and signalling pathways in the AAM in Spanish women.
Methods: We analysed nine polymorphisms in six different genes named N103S, rs3810682 and rs3897937 (BMP15), rs10046 and rs11575899 (CYP19), rs2234693 (ESR1), rs4986938 (ESR2), rs6166 (FSHR) and rs2229741 (NRIP1) in 714 well-characterized postmenopausal women from Spain. We performed a quantitative trait locus (QTL) study of these markers individually or in digenic combinations in relation to AAM.
Results: None of studied markers, with the exception of FSHR (p = 0.013) was significantly associated with AAM in the Spanish population and, no marker resisted after multiple testing corrections (p > 0.0055). Our result does not support the individual involvement of these loci as genetic determinants of AAM in our series. In contrast, linear regression analysis suggests epistatic interactions including, ESR1 and ESR2 loci in relation to AAM in our series (p = 0.003). Specifically, ESR1 rs2234693 TT/ESR2 rs4986938 AA combined genotype appears to be associated with a later menarche in the Spanish population (p = 0.008).
Conclusions: Our results suggest that epistatic interactions of ESR1 and ESR2 alleles could be associated with a delayed menarche amongst European women.
PS-396
ANALYSIS OF PROGINS IN POSTMENOPAUSAL WOMEN
K. F. Q. Moura1, A. M. Massad-Costa1, A. C. S. Myiati1, C. C. Gonçalves1, I. D. C. Guerreiro da Silva1, J. M. Soares-Jr1, M. A. Haidar1, M. C. P. Baracat1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil
Objective: The authors evaluated if the presence of the progesterone receptor polymorphism (PROGINS) is associated with the decrease in bone density in postmenopausal women.
Design and Methods: One hundred and ten women (all within the first five years after menopause) were included. None received any hormone replacement therapy before their inclusion in this protocol. Genomic DNA were extracted from oral cells collected with a cotton swab and processed for gene analysis. Bone mineral density was measured and results were compared with PROGINS polymorphism.
Results: 58.2% of patients were PROGINS negative homozygous (P1/P1) and 41.8% were positive heterozygous (P1/P2). Statistical significance was not found in the correlation between the presence of PROGINS positive and the measure lumbar Tscore.
Conclusion: The PROGINS polymorphism does not appear to correlate to bone density in postmenopausal women.
PS-397
ANALYSIS OF OESTROGEN-RELATED GENES IN THE ONSET OF PRAECOX MENOPAUSE LESS THAN 45 YEARS
T. Martínez-Astorquiza1, N. Mendoza Ladrón de Guevara2, F. Morón3, F. Quereda4, A. Ruíz3, R. Ramírez-Lorca3, F. Vazquez5, M. E. Sáez3, A. González3, E. Molero3, M. C. Rivero3 and R. Sánchez-Borrego6
1Sanatorio Bilbaino, Bilbao, Spain; 2Hospital Virgen de las Nieves, Granada, Spain; 3Genómica estructural Neocodex, Sevilla, Spain; 4Hospital San Juan, Alicante, Spain; 5Clínica GEOGA, Lugo, Spain; 6Clínica DIATROS, Barcelona, Spain
Objective: In the present study we will look at the role of genetic variants within oestrogen synthesis and signalling pathways in the age at menopause in Spanish women.
Methods: We analysed six polymorphisms in five different genes (FSHR, CYP19A1, ESR1, ESR2 and NRIP1) in 901 well-characterized postmenopausal women (with a natural menopause) from Spain. We performed a quantitative trait locus (QTL) study of these markers individually or in digenic combinations in relation to age at menopause and, a praecox menopause (less than 45 years old).
Results: None of studied markers, with the exception of NRIP1 (p = 0.001) was significantly associated with a praecox menopause in the Spanish population. In contrast, linear regression analysis suggests two epistatic interactions including, CYP19A1 with ESR2 and NRIP1 loci in relation to praecox menopause in our series (p = 0.003 and p = 0.007 for CYP19A1-ESR2 and CYP19A1-NRIP1, respectively). Furthermore, it seems that women carrying both digenic interactions have a lower mean of age at menopause and they have a shorter reproductive period of life.
Conclusions: Our results suggest that epistatic interactions of oestrogen-related alleles may contribute to variance in age at menopause in a complex manner. Moreover, NRIP1 appears also as an attractive candidate gene for praecox menopause but requires an independent replication to confirm our results.
PS-398
APOLIPOPROTEIN E AND PARAOXONASE 1 POLYMORPHISMS ARE ASSOCIATED WITH LOWER SERUM THYROID HORMONES IN POSTMENOPAUSAL WOMEN
Fotini Galapi1, Irene Lambrinoudaki1, George Kaparos2, Demetrios Rizos2, Andreas Alexandrou3, Theodoros Sergentanis1, Maria Creatsa1, George Christodoulakos1, Evangelia Kouskouni2 and Dimitrios Botsis1
12nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital; 2Hormonal and biochemical Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 31st Department of Surgery, University of Athens Medical School, Laiko Hospital, Athens, Greece
Objective: Subclinical and overt hypothyroidism as well as autoimmune thyroiditis often co-exists with cardiovascular disease (CVD). This study was conducted in order to investigate the association between gene polymorphisms related to CVD with thyroid function and autoimmunity.
Methods: FT3, FT4, anti-TPO and anti-TG were assessed in 84 healthy postmenopausal women aged between 49–69 years recruited from the Menopause Clinic of the 2nd Department of Obstetrics and Gynecology, University of Athens, Aretaieion Hospital. The following polymorphisms were genotyped: Apolipoprotein E E2/E3/E4 and Glycoprotein IIIa leu33pro.
Results: A statistically significant correlation was found between Apolipoprotein E and serum thyroid hormones: carriers of the E2 or E4 allele of the ApoE gene had lower levels of FT4 (p: 0.0005). A statistically significant positive association (p: 0.049) was also observed between anti-TG antibodies and the presence of the E2 allele of the Apolipoprotein E gene. No association was found between Glycoprotein IIIa leu33pro and serum FT3, FT4, anti-TPO and anti-TG.
Conclusions: Polymorphisms of the antioxidant enzyme Apolipoprotein E relate with thyroid dysfunction and autoimmunity. However, further research is needed to clarify the mechanism underlying this association.
PS-399
ASSOCIATION OF GENETIC MARKERS WITHIN THE BMP15 GENE IN WOMEN WITH PRAECOX MENOPAUSE
N. Mendoza Ladrón De Guevara1, F. J. Morón2, F. Quereda3, R. Ramírez-Lorca2, A. Santalla1, J. L. Gallo1, R. Sanchez-Borrego4 and A. Ruíz2
1 Hospital Universitario “Virgen de las Nieves”, Granada; 2Genómica estructural Neocodex, Sevilla; 3Hospital Universitario “San Juan”, Alicante; 4Clínica DIATROS, Barcelona
Objetive: The BMP15 gene is a di-exonic gene that encodes a preproprotein activated by proteolytic processing. The BMP15 protein is expressed in the oocyte and is a potent stimulator of granulosa cells proliferation, largely involved in the progression of folliculogenesis from the primary stage till the FSH-dependent stage.
In humans, the important role of BMP15 in fertility has recently been shown. A study of a family affected by hypergonadotropic ovarian failure, with primary amenorrhea, identified the first mutation (Y235C) in the pro-region of the BMP15 gene in two sisters affected by this Mendelian phenotype. Furthermore, our group has sufficient evidence to associate three linked markers within the BMP15 gene with high follicle production in women undergoing recombinant FSH stimulation.
Material and Methods: Automated DNA sequencing methods were employed to scan the entire coding region of the BMP15 gene in 45 women with menopause before 40 years of age. Overlapping PCRs covering the coding sequence (including 5’ and 3’ UTR regions) of gene were designed. PCR products were purified and bi-directionally sequenced using the corresponding primers. Sequencing reactions were performed according to the manufacturer's instructions, and analysed using CEQ™ 8000 Genetic Analysis System (Beckman Coulter, Inc., Fullerton, CA). To confirm the different variants observed by automated sequencing, we employed a different protocol (pyrosequencing) in a new DNA re-extraction.
Results: We observed six heterozygous variants in patients with secondary amenorrhea. Two variants with the same allelic frequencies and in complete linkage disequilibrium between them in thirteen women within the 5′UTR region (−673C>T and −9C>G). Two missense alterations located in exon 1 (N103S) and exon 2 (A180T) in three and one women respectively. Moreover, in exon 2, we observed one insertion (263InsL) and one silent variant (S284S) in the same patient. Subsequently, we observed all these variants in a control population.
Conclusion: There are different variations in BMP15 gene in women with menopause before 40 years of age, although the observed mutations are not a major cause of ovarian insufficiency in women. An exhaustive analysis of this gene in independent large population would be required.
PS-400
GENETIC BACKGROUND OF SUBCLINICAL ATHEROSCLEROSIS IN HEALTHY POSTMENOPAUSAL WOMEN
S. Vlachou1, I. Lambrinoudaki1, G. Kaparos2, K. Stamatelopoulos3, G. Georgiopoulos3, A. Alexandrou4, M. Creatsa1 and C. Papamichael3
12nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital; 2Hormonal and biochemical Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 3Vascular Laboratory, Department of Clinical Therapeutics, Alexandra Hospital, Athens, Greece; 41st Department of Surgery, University of Athens Medical School, Laiko Hospital, Athens, Greece
Objective: To evaluate the relation of common genetic polymorphisms, involved in lipoprotein oxidation, platelet activation and cholesterol and homocysteine metabolism, to indices of endothelial function and arterial elasticity in healthy postmenopausal women.
Methods: The following polymorphisms were genotyped in 84 healthy postmenopausal women: apolipoprotein B 3500, apolipoprotein E (E2/E3/E4), cholesterol 7alpha hydroxylase A-204C (CYP A-204C), cholesterol ester transfer protein B1/B2, glycoprotein IIIa leu33pro, integrin beta 3 PLA1/PLA2, plasminogen activator inhibitor 1 4G/5G, paraoxonase 1 gln192 arg, methylenetetrahydrofolate reductase ala222val. Ultrasound examination aimed to assess the presence of atherosclerotic plaques and to measure intima - media thickness in the carotid and femoral artery, as well as to estimate the augmentation index, brachial flow-mediated dilatation and radial and femoral pulse wave velocity.
Results: Cholesterol 7alpha hydroxylase A-204C polymorphism was positively associated with the presence of atherosclerotic plaques (p = 0.004) and carotid and femoral intima-media thickness (p = 0.047 and p = 0.025, respectively). Women bearing the C allele had significantly increased mean carotid and femoral IMT and increased presence of atherosclerotic plaques compared to women bearing the A allele. No other associations emerged between polymorphism status and the ultrasound markers.
Conclusions: Cholesterol 7alpha hydroxylase catalyses the rate-limiting step of bile acid synthesis in the liver, having a key role in the regulation of cholesterol excretion. CYP A-204C polymorphism was found to be positively associated with subclinical atherosclerosis in healthy postmenopausal women. The significance of this finding with regard to cardiovascular disease risk in postmenopausal women requires further clarification.
PS-401
GENETIC POLYMORPHISMS AND LIPID PROFILE IN HEALTHY POSTMENOPAUSAL WOMEN
Dimitra Papadimitriou1, Irene Lambrinoudaki1, George Kaparos2, Theodoros Sergentanis1, Maria Creatsa1, Andreas Alexandrou3, Irene Kalligerou1, George Christodoulakos1 and Evangelia Kouskouni2
12nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital; 2Hormonal and biochemical Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 31st Department of Surgery, University of Athens Medical School, Laiko Hospital, Athens, Greece
Objective: The aim of this study was to assess the impact of certain genetic polymorphisms on serum lipid profile in postmenopausal women.
Methods: Participants were 84 postmenopausal women aged 49–69 years old. The genetic polymorphisms examined at this study were: Glycoprotein IIIa leu33pro, Apolipoprotein E2/E3/E4, Methylenotetrahydrofolate reductase ala222val, Apolipoprotein B arg3500gln, Paraoxonase 1 gln192arg, Plasminogen activator inhibitor 1 4G/5G, Cholesterol 7 alpha hydroxylase A-204C and Cholesterol ester transfer protein (TaqIB) B1/B2 polymorphism. Biochemical assays included Total Cholesterol (TC), triglycerides (TGL), Low-density Lipoprotein (LDL), High-density Lipoprotein (HDL), Apolipoprotein A (ApoA), Apolipoprotein B (ApoB) and Lipoprotein (a) (Lp(a)).
Results: Cholesterol ester transfer protein (TaqIB) B1/B2 polymorphism is associated with decreased mean levels of HDL and ApoA(p = 0.001, p = 0.0001, respectively). Glycoprotein IIIa leu33pro polymorphism is associated with low levels of ApoB(0.019), while Apolipoprotein B arg3500gln polymorphism bears a statistically significant positive association with total cholesterol (p = 0.032) and HDL cholesterol (p = 0,048). Finally, plasminogen activator inhibitor 1 4G/5G polymorphism was marginally associated with increased mean levels of triglycerides (p = 0.058).
Conclusions: Cholesterol ester transfer protein (TaqIB) B1/B2 polymorphism is associated with an unfavourable lipidaimic profile in postmenopausal women, while other polymorphisms, such as Glycoprotein IIIa leu33pro polymorphism may act protectively. The significance of these genetic polymorphisms with respect to serum lipids in postmenopausal women remains to be clarified in future studies.
PS-402
MTHFR C677T POLYMORPHISM AND SERUM ANDROGENS IN HEALTHY POSTMENOPAUSAL WOMEN
Dimitra Papadimitriou1, Irene Lambrinoudaki1, George Kaparos1, Theodoros N. Sergentanis1, Maria Creatsa1, Andreas Alexandrou3, Irene Kalligerou1, George Christodoulakos1 and Evangelia Kouskouni2
12nd Department of Obstetrics and Gynecology, University of Athens, Aretaieio Hospital; 2Hormonal and biochemical Laboratory, University of Athens, Aretaieio Hospital, Athens, Greece; 31st Department of Surgery, University of Athens Medical School, Laiko Hospital, Athens, Greece
Objective: To assess the association of genetic polymorphisms related to CVD risk with serum androgens in healthy postmenopausal women.
Design: Cross-sectional study in a University Menopause Clinic.
Methods: The following polymorphisms were assessed in 84 healthy postmenopausal women: Glycoprotein IIIa leu33pro, Apolipoprotein E2/E3/E4, Methylenetetrahydrofolate reductase ala222val, Apolipoprotein B arg3500gln, Paraoxonase 1 gln192arg, Plasminogen activator inhibitor 1 4G/5G, Cholesterol 7 alpha hydroxylase A-204C and Cholesterol ester transfer protein (TaqIB) B1/B2. Hormonal assays included FSH, LH, 17-β-estradiol (E2), Testosterone, Sex Hormone Binding Globulin (SHBG), Dehydroepiandrosterone sulphate (DHEAS), Delta-4-androstendione (Δ4A), Free Androgen Index (FAI), Free Estrogen Index (FEI) and Homocysteine (Hcy). Results: MTHFR ala222val polymorphism was positively associated with testosterone, FAI and FEI (p = 0.001, p = 0.0004, p = 0.014, respectively) and negatively with SHBG (p = 0.047).
Conclusions: MTHFR ala222val polymorphism is associated with increased androgenicity in healthy postmenopausal women. The significance of this association with respect to the CVD risk of postmenopausal women remains to be elucidated in future studies.
PS-403
POLYMORPHISMS OF TRANSFORMING GROWTH FACTOR β GENE AND BONE MINERAL DENSITY IN POSTMENOPAUSAL KOREAN WOMEN
H. Chung, W. Lee and H. Moon
Ewha Womans University School of Medicine, Seoul, Korea
Objective: Osteoporosis is a common systemic skeletal disease, defined as both a decrease in bone mass and strength, which increases the fracture risk. Recent studies have shown that osteoporosis is strongly associated with genetic components and genetic factors, which play major roles in the development of peak bone mass, with hereditability accounting for about 50–85% of the variance in bone mass. TGF-β is a growth factor in human bone, which is produced by osteoblasts, and which has various effects on osteoclasts and osteoblasts. TGF-β has been implicated as an important regulator of both bone formation and resorption. Several polymorphisms of the TGF-β gene have recently been suggested to be associated with BMD and susceptibility to osteoporotic spine fractures. The possible associations of genetic variants in TGF-β with spinal and femoral BMD were investigated in Korean postmenopausal women.
Design & Method: The Lumbar (L2-L4) and femoral BMD were measured by dual energy X-ray absorptiometry using a Lunar DEXA in 855 postmenopausal women. Allele specific PCR was performed by genotyping. The logistic regression was performed by SPSS11.0.
Results: The TGF-b C -509T genotypic frequency in the Korean population were 27.0% for CC, 42.5% for CT, 27.0% for TT. Average spinal BMD in women with the CC genotype was 1.024 ± 0.177 mg/cm2, CT genotyope was 1.043 ± 0.182 mg/cm2, TT genotype was 1.059 ± 0.181 mg/cm2. Average total femoral BMD in women with the CC genotype was 0.831 ± 0.138 mg/cm2, CT genotyope was 0.843 ± 0.182 mg/cm2, TT genotype was 0.876 ± 0.254 mg/cm2. There was no significant relation with TGF-b genotype and BMD at lumbar and femoral BMD. The result of this study showed no association TGF-b C -509T genotypic single nucleotide polymorphism and osteoporosis.
Conclusions: These data indicate that TGF-β gene polymorphsm are not predictive of BMD.
PS-404
THE CYP1A1 POLYMORPHISM IN WOMEN WITH VASOMOTOR SYMPTOMS AFTER MENOPAUSE
A. M. Massad-Costa1, A. C. S. Myiati1, C. C. Gonçalves1, I. D. C. Guerreiro da Silva1, J. M. Soares Jr1, M. A. Haidar1, K. Moraes1, M. C. P. Baracat1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil
Objective: To determine whether CYP1A1-Hinc polymorphisms is associated with women s vasomotor symptom after menopause.
Design and Methods: articipants were 96 women with a mean age of 52.1 4.4 years, employed, married, and presented a multiethnic population. Genotyping was done for the CYP1A1-Hinc poymorphisms heterozygote and wild type) Women rated their vasomotor symptom severity in card diaries.
Results: We did not find the wild type for CYP1A1-Hinc in our patients. Women with the heterozygote CYP1A1-Hinc polymorphisms reported similar number of hot flashes to women without the polymorphisms. The number of patients with CYP1A1-Hinc heterozigote was 49. The Relative Risk (RR) for vasomotor symptoms was 0.8606 (0.5009 to 1.479).
Conclusion: Our data suggest CYP1A1-Hinc polymorphisms may be not associated to vasomotor symptoms in postmenopausal women.
PS-405
THE EVALUATION OF CYP-17, COMT AND ESTROGEN RECEPTOR GENE POLYMORPHISM IN POSTMENOPAUSAL WOMEN WITH LOW BONE MINERAL DENSITY
K. F. Q. Moura1, A. M. Massad-Costa1, A. C. S. Myiati1, C. C. Gonçalves1, I. D. C. Guerreiro da Silva1, J. M. Soares Jr1, M. A. Haidar1, M. C. P. Baracat1 and E. C. Baracat2
1Federal University of São Paulo, São Paulo, São Paulo, Brazil; 2Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil
Objective: To evaluate the polymorphism of CYP-17, COMT and estrogen receptor genes in postmenopausal women with bone mineral density.
Design and Methods: 110 women after five years of menopause without any hormonal therapy were included. The epidemiological and clinical data were registered through medical history. The bone densitometry was applied in lumbar vertebral column in all patients. The Genomic DNA was extracted from oral cells collected with a cotton swab and processed for gene analysis through PCR. The statistical analysis was performed using Kruskal-Wallis and Bonferroni test.
Results: The mean age of participants was 51.96 years. The CYP-17 wild type (homozygous CC), heterozygous (Cc) and mutated homozygous (cc) were detected in approximately 19%, 66% and 15% of participants, respectively The COMT wild type (GG), heterozygous (Gg) and mutated homozygous (gg) were found in 59%, 41% and 10% of patients, respectively. The estrogen receptor gene wild type (EE), heterozygous (Ee) and mutated homozygous (ee) were 59%, 45% and 6%, respectively. No significant differences were detected in all gene analyzed.
Conclusion: The CYP-17, COMT and estrogen receptor gene polymorphism did not present significant correlation with low bone mineral density of postmenopausal in lumbar vertebral column.
PS-406
UNILOCUS ANALYSIS OF ESTROGEN-RELATED GENES (FSHR, ESR1, ESR2, NRIP, CYP19 Y BMP15) IN THE PATHOGENESIS OF POSTMENOPAUSAL OSTEOPOROSIS
A. Santalla1, F. J. Morón2, M. S. López-Criado1, F. Quereda3, E. Molero2, R. Sánchez-Borrego4, A. Ruíz2 and N. Mendoza1
1Hospital Virgen De Las Nieves, Granada, Spain; 2Genómica Estructural Neocodex, Sevilla, Spain; 3Hospital San Juan, Alicante, Spain; 4Clínica Diatros, Barcelona, Spain
Osteoporosis is a common disease with multiple environmental and genetic risk factors involved. Looking for markers related to osteoporosis, we have analyzed single nucleotide polymorphisms located in genes related to the estrogen pathway.
Matherial and Methods: A multicentric study with 1089 unrelated postmenopausal women was carried out. Complete clinical data, femoral and lumbar densitometry and peripheral blood were obtained from participants in order to determinate candidate genes polymorphism. To perform the genotyping of the markers we employed pyrosequencing technology. We have analyzed single nucleotide polymorphisms located at different candidate genes related to the oestrogen signalling pathway: Follicle Stimulating Hormone Receptor, the CYP19 aromatase, the Estrogen Receptor alpha, the Estrogen Receptor beta, the Nuclear Receptor Interacting Protein 1, and the Bone Mineral Protein 15 genes.
Results: Of the 1089 patients in the study, 281 were considered with osteoporosis, 502 with osteopenia, and the remaining 306 had normal BMD. We analyzed 30 different polymorphisms of genes identified, some of them unknown to date. From unilocus pathway, none of them was associated with osteopenia/osteoporosis in our patients.
Conclussion: Our population presents an important variety of estrogen-related genes polymorphism. No association was found between any polymorphism of these of estrogen-related genes and osteoporosis/osteopenia. These results may suggest that the development of osteoporosis does not depend only in one gene but in the self-relation of multiples genes, and in the interaction of these genes with environmental factors.
Imaging
PS-407
AMBULATORY HYSTEROSCOPY AS A TECHNIQUE FOR DETECTION OF ENDOMETRIOID ADENOCARCINOMA IN POSTMENOPAUSAL PATIENTS
P. Rubio, M. Hernández, B. Galve, M. Lamarca, I. Morollón and R. Lanzón Lacruz
Hospital Universitario Miguel Servet, Zaragoza, Spain
Objective: To evaluate the usefulness of the images obtained by hysteroscopy and biopsy led to the detection of endometrioid carcinoma in postmenopausal women in our hospital.
Design & Method: We carried out a descriptive retrospective study of the ambulatory hysteroscopies performed on a consultation for gynecologic cancer prevention in our hospital, in the period from June 2002 to December 2007.
When the hysteroscopic image suggested an adenocarcinoma and the biopsy was not diagnostic, subsequent surgical interventions were investigated (curettages, hysterectomies…) to reach the diagnosis positive or negative for endometrioid adenocarcinoma.
Results: During the study period were carried out 3775 ambulatory hysteroscopies, 2632 in postmenopausal patients. In 161 (6.11%) of the postmenopausal patients the hysteroscopic image suggested an endometrioid adenocarcinoma, while the total number of patients undergoing an initial hysteroscopic suspected adenocarcinoma was the 4.39% of the overall group.
Patients were symptomatic at a 92.54% (n = 149). The asymptomatic women were referred to an hysteroscopic evaluation for endometrial thickness over 4 mm. The ultrasound imaging showed an endometrial thickness greater than 4 mm in a 89.28% of all the cases.
In 126 of the cases (78.26%) the diagnosis was confirmed by the hysteroscopic biopsy. Of the 35 cases in which the biopsy was not diagnostic, subsequent surgery confirmed the existence of an endometrioid adenocarcinoma in 13 of them. Of the remaining 21, 5 of them had a malignant tumour of another histological type.
In 9 cases the hysteroscopic imaging diagnostic was benign and was later confirmed as an endometrioid adenocarcinoma.
Conclusion: The direct hysteroscopic visualization of the endometrial cavity and the endometrial biopsy has led a sensitivity of 86.33% in the detection of endometrioid adenocarcinoma in postmenopausal patients in our hospital.
PS-408
AMBULATORY SURGERY RESECTOSCOPY IN MENOPAUSAL WOMEN – 2 YEARS REVIEW
R. Ribeiro, R. Robalo, R. Lermann, A. Martins and A. Fatela
Maternidade Dr. Alfredo da Costa, Lisbon, Portugal
Objective: To evaluate the therapeutic efficacy and safety of ambulatory surgery resectoscopy performed in menopausal women.
Design & Method: Retrospective, descriptive study of 42 case series ranging from 2005 to 2006 in a hospital center. Epidemiological characteristics, risk factors, diagnostic aproach, resectoscopy data, complications and follow-up were evaluated.
Results: 133 resectoscopies procedures were performed during the study period: frequency of menopausal women is 31,6%. The mean (±SD) age of the patients was 59 (±4,5) years. 26,2% did hormone therapy replacement. Obesity was diagnosed in 23,8% of the women and 47,6% were overweight. Hypertension was the main associated pathology (21,4%). Polyps were the first indication for surgery (95,2%) and histologic findings confirmed the diagnosis in 85%. We found 1 case of adenocarcinoma. We only report two cases with complications: cervical laceration, that impaired the procedure.
Conclusion: Our data supports the role of ambulatory surgery resectoscopy in the assessment of uterine cavity pathology, without significant damage. It is associated to less morbidity and less costs.
PS-409
DIAGNOSTIC HYSTEROSCOPY IN POSTMENOPAUSAL PATIENTS. EXPERIENCE AT THE UNIVERSITY HOSPITAL MIGUEL SERVET (ZARAGOZA)
M. Hernández, B. Galve, P. Rubio, I. Morollón, D. De Pablo and R. Lanzón Lacruz
Hospital Universitario Miguel Servet, Zaragoza, Spain
Objective: To analyse the role of diagnostic hysteroscopy as a detecting method for the pathology of endometrial cavity, as well as the population characteristics and the indications for its realization.
Design & Method: We performed a descriptive retrospective study of the diagnostic hysteroscopies made in postmenopausal patients at the University Hospital Miguel Servet between June 2002 and December 2007, both included.
Results: During the period of study 3775 diagnostic hysteroscopies have been made performed in our hospital, 2632 of them (69.72%) in postmenopausal patients. The mean age of patients in this study was 61.54 years, with mean age of 49.05 years of menopause age.
1828 patients (69.45%) were symptomatic, 78 of them (4.26%) with tamoxifen therapy for breast cancer, 57 with hormone replacement therapy (3.11%). These patients had an endometrial thickness measured by ultrasound over 4 mm in a 66.12% of the cases. The hysteroscopic findings were: 672 (36.76%) cases of atrophic endometrium, 106 (5.79%) endocervical polyps, 708 (38.73%), endometrial polyps, 1 cervical mass, 62 (3.39%) submucous myoma, 108 (5.9%) endometrial hyperplasia, 149 (8.15%) endometrioid adenocarcinoma, 23 (1.25%) tamoxifen pattern.
804 patients (30.55%) were asymptomatic. The indication for diagnostic hysteroscopy was an increase of endometrial thickness in 98.63% of cases, the other indications were cytological abnormalities. 209 (25.99%) patients were treated with tamoxifen. The hysteroscopic findings were: 166 (20.64%) cases of atrophic endometrium, 40 (0.49%) endocervical polyps, 461 (57.33%), endometrial polyps, 18 (2.23%) submucous myomas, 28 (3, 48%) endometrial hyperplasia, 12 (1.49%) endometrioid adenocarcinoma, 79 (9.82%) tamoxifen pattern.
Conclusion: Diagnostic hysteroscopy in postmenopausal patients allows to diagnose bening pathology in 73,35% and adenocarcinoma in 1,49% of the asymptomatic women with an abnormal endometrium thickness measured by echography.
PS-410
HYSTEROSCOPIC IN POSTMENOPAUSAL WOMEN
M. Prieto Martínez, M. A. Nieto Naya, M. Padilla Castillo, R. García Rodríguez, P. López Gutiérrez, C. Blanco Soler, M. Sosa Hernández, L. Ocón Padrón, D. Madera, M. Sosa Marrero and S. Seara Fernández
Hospital Universitario Materno-Infantil de Canarias
Objective: This study examined the endometrial pathology in postmenopausal women who underwent to hysteroscopy in our hospital.
Material and Methods: A retrospective observational study. From January 1997 to December 2006 we have done 4666 hysteroscopy's studies in postmenopausal woman. We analyzed the indications of the study, the prior treatment, hysteroscopy's findings and its complications. We used an Access database to collect the patient's dates. The hysteroscopy's studies were made with a Gynecare hysterocope of 3,5mm with a Store camera and Gynecare surgical instruments.
Results: The indications for the Hysterospy were: postmenopausal bleeding 3399 patients (72, 8%), pathological ecography endometrial findings 929 patients (19, 9%), and endometrial carcinoma staging 152 patients (3.2%), other indications 90 patients (2.1%). 835 patients (17.8%) have had prior hormonal replacement treatment and 275 of this had combinated hormone replacement treatment.
The hysteroscopics findings were: no pathological findings 1535 cases (33.6%), endometrial polyp 1917 cases (41.9%), submucosal myoma 194 (4.2%), endometrial hyperplasia without atypia 58 cases (1.2%), endometrial hyperplasia with atypia 61 cases (1.3%), endometrial carcinoma 355 patients (7.8%), endometritis 19 cases (0.4%), cervix carcinoma 9 cases (0.2%), cervical polyp 40 cases (0.8%), and insufficient for the diagnosis in 380 cases (8.3%).
In 98 patients (2.1%) were impossible to study the endometrial cavity due to profuse bleeding. We have complications in 67 patients (1.4%).
Conclusions: The patients who had prior hormonal prior hormonal treatment replacement that need hysteroscopy study were 17.8%. The percentage of malignant endometrial findings was 9.1% agreed with the literature.
PS-411
HYSTEROSCOPIC AND HISTOPATHOLOGICAL FINDINGS IN ASYMPTOMATIC POSTMENOPAUSAL WOMEN WITH ENDOMETRIAL THICKENING
G. Gomes, A. Figueiredo, T. Paula, A. Fatela, D. Rosa and A. Martins
Maternidade Dr. Alfredo da Costa, Lisboa, Portugal
Background: Endometrial thicknening measured by transvaginal ultrasonography (TVU) is considered to be an indicator of risk for endometrial carcinoma. About 90% of women with endometrial malignancy will present with abnormal vaginal bleeding or discharge. Only less than 5% of women diagnosed with endometrial cancer are asymptomatic.
Objective: To analyse the hysteroscopic and histopathological findings in asymptomatic postmenopausal women with endometrial thickening measured by TVU, in order to evaluate the clinical usefulness of an invasive diagnostic procedure in this population.
Design & Methods: Retrospective chart review of 35 postmenopausal women referred to Maternidade Dr. Alfredo da Costa in the first trimester of 2007 for suspected endometrial abnormality based on the ultrasonographic finding of a thickened endometrium (endometrial-thickness threshold value of 5mm). Women included in the study were asymptomatic and all of them underwent hysteroscopy with directed biopsy. Data from ultrasonography, hysteroscopy and histopathological analysis was compared.
Results: Of the 35 women initially enrolled in this study, two were excluded because hysteroscopy was not possible. The mean endometrial thickeness measured by TVU in this population was 15,03 ± 7,09 mm (range, 5,8–32 mm). Polyps were the most frequent hysteroscopic finding (n = 27, 81,8%), followed by atrophic endometrium (n = 5, 15,2%) and uterine septum (n = 1, 3%). The histological diagnosis were consistent with the results from hysteroscopy in most cases: polyps in twenty five cases (75,8%), atrophic endometrium in six (18,2%), submucosal leyomioma in one (3%) and endometritis in another (3%). There were no cases of endometrial carcinoma.
Conclusion: The results of this study are in consonance with the generally accepted fact in current medical literature that only a minority of women with endometrial cancer are asymptomatic. This raises the question whether asymptomatic postmenopausal women with endometrial thickening detected on TVU, should undergo a more invasive diagnostic procedure, such as hysteroscopy, solely on the basis of the TVU indication.
PS-412
HYSTEROSCOPIC MANAGEMENT OF ENDOMETRIAL PATHOLOGY IN POSTMENOPAUSAL WOMEN
Guillermo Campuzano1,2, Gabriel Leon-Letamendi1,2, Patricia Leon-Leon2 and Johana G. Alcivar1
1Enrique C. Sotomayor Gynecology and Obstetrics Hospital, Guayaquil, Ecuador; 2Facultad de Ciencias Médicas, Universidad de Guayaquil, Ecuador
Background: Hysteroscopy has proven it usefulness for the assessment and management of endometrial pathology among postmenopausal women whether or not on hormonal therapy.
Objective: To determine the effectiveness of the hysteroscopic procedure for the management of endometrial pathology among postmenopausal women.
Design: A retrospective analysis of 483 hysteroscopic procedures performed among postmenopausal women, with clinical, sonographic or hydrosonographic indication, at the Laparoscopic Service of the Enrique C. Sotomayor Gynecology and Obstetrics Hospital, Guayaquil Ecuador between 1994 and 2007. Analyzed data included: subjects clinical and surgical history, complications encountered during procedures and the correlation to initial sonographic assessment.
Results: Mean age was 55 years (range 40 to 79 years). Abnormal bleeding was the main referral reason for hysteroscopy (37.6%). Forty two subjects were on hormone therapy for the menopause. Hysteroscopic procedure was ambulatory in 81.3% and successfully completed in 96% of cases. In 16 cases no anesthesia was necessary whereas cervical stenosis and uterine perforation caused the non completion of the procedure. Endometrial polyps were found in 12% and hyperplasia in 10%. Biopsies were performed in 67% of cases of which 17 cases resulted abnormal and 8 cases reported endometrial adenocarcinoma. Polyp resection, endometrial ablation, intrauterine adhesiolysis and IUD extraction were the main additional procedures.
Conclusions: In the present series hysteroscopy was an effective diagnostic and managing tool for endometrial pathology of postmenopausal.
PS-413
MOLECULAR BREAST IMAGING: EVALUATION OF AN ADDITIONAL DIAGNOSTIC TOOL FOR WOMEN PRESENTING WITH A HISTORY OF BLOODY NIPPLE DISCHARGE AND NEGATIVE ROUTINE IMAGING STUDIES – A PILOT STUDY
D. L. Wahner-Roedler, M. K. O'Connor, S. W. Phillips, D. H. Whaley, P. J. Peller, C. B. Hruska, R. E. Johnson, A. C. Degnim, L. L. Loehrer and D. J. Rhodes
Mayo Clinic, Rochester, Minnesota, USA
Background: Evaluation of BND focuses on excluding a malignant cause. When BND is clinically reproducible management involves surgical duct excision. When BND is not reproducible and mammogram and ultrasound are negative, the management relies on “watchful waiting” - serial breast imaging and continued observation for recurrent BND. This provokes anxiety among patients not having a clear explanation for the BND. MRI has not been studied in this context and is costly. The availability of a less costly method of excluding breast cancer would be of great value in this population.
Objective: To evaluate Molecular Breast Imaging (MBI) in the workup of patients with a history of bloody nipple discharge (BND), not reproducible in the office and with negative routine imaging studies.
Design & Method: A dual-detector cadmium-zinc-telluride gamma camera system mounted on a modified mammography gantry was used. The injection dose was 20 mCi of 99m Tc sestamibi. Depending on uptake in the breast the following MBI scoring system was used: negative, benign, probably benign, suspicious for malignancy, highly suggestive of malignancy. Thirteen women presenting to a multidisciplinary breast clinic between October 2006 and December 2007 with a history of BND not reproducible in the office and with a negative mammogram and ultrasound were enrolled in the study.
Results: Median age: 46 years (range 26–75). BND left-8; right-4; bilateral-1 patient. BND spontaneous-7; non-spontaneous-4; spontaneous left, non-spontaneous right-1; not recorded-1 patient. All women had negative clinical breast exam, mammogram, and ultrasound of the symptomatic breast. MBI interpretations: negative-7; benign-5; probably benign-1 patient. Two patients with spontaneous non-reproducible BND underwent subareolar duct excision due to patients' concern about a family history of breast cancer. Pathology: small radial scar and papilloma (0.3x0.2x0.2cm), respectively (missed by mammogram, US, MBI). The patient with a “probably benign” MBI interpretation and spontaneous BND underwent post MBI special mammographic views and targeted repeat US examinations, which were negative. As per protocol, the patient will return for a repeat MBI in 6 months. All patients were advised to return if they should notice any recurrent BND.
Conclusion: This pilot study evaluated MBI, an imaging procedure which has been demonstrated to detect mammographically occult lesions, as an additional diagnostic procedure in patients presenting with a history of non-reproducible BND. The concordance between MBI, mammogram, and US in regard to the absence of suspicious findings is reassuring. Larger studies with careful patient follow-up are needed to confirm these preliminary findings.
PS-414
OFFICE HYSTEROSCOPY AFTER MENOPAUSE – A 2 YEARS STUDY
C. Júlio, A. Cordeiro, N. Amaral, R. Condeço, S. Coutinho, M. C. Silva and R. Mira
Hospital Dona Estefânia, Lisbon, Portugal
Objective: Endometrial carcinoma is the most common malignancy of the female genital tract and occurs primarily in postmenopausal women. Frequently, it is symptomatic, being the most feared cause for vaginal bleeding after menopause. In the present, hysteroscopy can be done in an office setting, provides information that can not be obtained by blind sampling and it is accurate for differential diagnosis of uterine cavity pathology. The aim of this study is to evaluate two years of office hysteroscopy performed in postmenopausal women.
Design & Method: A total of 458 postmenopausal women were submitted to office hysteroscopy during 2 years in our department. Clinical data was evaluated for age, hormonal therapy, presence of symptoms, abnormal sonographic findings, use of pre-procedure medication, hysteroscopic findings, associated pain and complications, and pathological diagnosis. Pearson χ2 test and T-student were used for statistical analysis (SPSS 10.0, Inc.).
Results: Mean-age was 65,9 years old (42–100). Hormonal replacement therapy was used by 8,1% of women (37/458) and 7,9% were medicated with tamoxifen. Misoprostol was use for cervical dilation in 410 patients. Pain was subjectively assessed in a numeric scale from 0–10 and no differences were found between women who received anesthesia (local/paracervical, 385 cases) and those who did not. Vaginal bleeding was present in 22,5% (n = 103) of the cases, 90,3% of which had abnormal sonographic evaluation. In this group, the most frequent hysteroscopic finding was endometrial polyp and there were 17/103 exams suggestive of neoplasia. Pathologic diagnosis revealed 14 endometrial carcinomas (11 with histeroscopy suggestive of neoplasia, 1 suggestive of endometrial hyperplasia and 2 endometrial polyps). In asymptomatic patients (77,1%) 218 endometrial polyps were identified, 9 exams were suspicious for neoplasia and 2 for endometrial hyperplasia. Pathologic diagnosis was endometrial carcinoma in 9 cases (8 with suggestive hysteroscopic and 1 in polyp). Overall, neooplasia was more frequent in symptomatic women 13,6% (14/103) vs. 2,55% (9/353) in the asymptomatic group (p < 0,05). One uterine perforation was reported.
Conclusion: Endometrial pathology after menopause, either symptomatic or not, always starts a diagnostic cascade to exclude malignancy. Office hysteroscopy is a rapid, well tolerated, safe and efficacious ambulatory technique for the diagnosis and treatment of this condition.
PS-415
PROCENTUAL MAMMOGRAPHIC DENSITY – A BETTER MARKER FOR MAMMOGRAPHIC CHANGES ON HORMONE THERAPY?
S. Nastasia, M. C. Russu and D. Hudita
“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
Objective: To asses the sensitivity of the procentual mammographic density (PMD) in detection of mammographic changes for patients on hormone therapy (HT), as opposed to Wolfe scale. PMD is the percent of mammary tissue density from the total surface of breast in digital mammography.
Design & Method: Digital mammograms in 51 healthy patients, treated for menopausal symptoms with sequential transdermal 25 mcg estradiol and 5 mg medroxiprogesteron acetate, were evaluated for Wolfe scale and PMD before and after 1 year of HT. Mammograms were done after the progesteronic phase. PMD was manually calculated using free ImageJ software. Wolfe index changed after one year HT, respectively a 66% increase of PMD, were considered significant.
Ten healthy symptomatic patients, who refused HT, served as controls.
Statistical analysis was performed with JMP software, under licence.
Results: Mean age was 53,68y in treated group and 52,87y in controls.
Before HT, Wolfe scale showed nine N1 patients, eighteen P1, nineteen P2 and five DY in the treated group and four N1, four P2 and two P2 in control group.
No change in Wolfe index and PMD was observed after one year HT in control group.
After one year HT, three patients (5,88%) had modified Wolfe index (one N1 (11,11%) and two P1 (11,11%)).
After one year HT, ten patients (19,60%) had a 66% increase of PMD(five N1 (55,55%) and five P1 (27,77%)); this doesn't include one P1 patient, who had a modified Wolfe index, but not a 66% increase of PMD.
Considering changes both in PMD and Wolfe index, 21,56% of the patients (11 patients) demonstrated mammographic changes, as opposed to Wolfe scale only, which showed an increase in mammographic density in 5,88% patients (3 patients).
Conclusions: PMD is able to detect more subtle mammographic changes in HT patients. However, the prognostic significance of these changes on current HT users is to be established.
PS-416
RETROSPECTIVE ANALYSIS OF ENDOMETRIAL FLUID IN POSTMENOPAUSAL WOMEN
U. Inceboz, S. Bugday, Y. Uyar, Y. Bulbul and A. R. Kandiloglu
Celal Bayar University, Faculty of Medicine, Manisa, Turkey
Objective: To investigate the importance of the presence of endometrial fluid in postmenopausal women without any bleeding.
Design & Methods: Retrospective analysis of postmenopausal women attending university hospital during the last 10 years revealed thirty-one women with endometrial fluid on transvaginal sonography. All women underwent endometrial biopsy for histologic evaluation.
Results: The mean age of women was 57 (range: 46–74). The mean time since menopause was 11 years (range: 2–29 years). Histologic results were benign in 30 women. The diagnose was endometrial adenocarcinoma in one case. Hypertension, diabetes and both were found in 8, 3, and 6 cases, respectively. The woman with endometrial carcinoma had hypertension only. The only notable difference was the endometrial thickness in that case. The endometrial thickness (one leaf) in all cases with benign histologic result was less than 2.5 mm whereas it was 7.5 mm in case with endometrial cancer.
Conclusion: Although endometrial fluid collection is important finding in postmenopausal years, endometrial thickness would give more powerful prediction about the pathology.
Inmunology
PS-417
ASSOCIATION OF HOT FLASHES WITH CIRCULATING CYTOKINE LEVELS IN PRE-, PERI- AND POSTMENOPAUSAL WOMEN AND BILATERAL OOPHORECTOMIZED WOMEN
Toshiyuki Yasui1, Hirokazu Uemura1, Yuka Miyatani1, Masayo Yamada1, Naoko Tsuchiya2, Mitsutoshi Yuzurihara2, Yoshio Kase2 and Minoru Irahara1
1Institute of Health Biosciences, The University of Tokushima Graduate School, Tokushima, Japan; 2Tsumura Central Research Institute, Inashiki-gun Ibaraki, Japan
Objective: Vasodilation was observed in midlife women with hot flashes and night sweating. Cytokines such as IL-6 and TNF-a have been reported to be potent vasodilators. The purpose of this study is to clarify serum cytokine concentrations in pre-, peri- and postmenopausal women and bilateral oophorectomized women with hot flashes.
Subjects & Methods: One hundred twenty-nine midlife women and 50 bilateral oophorectomized women were enrolled in this study. The 129 midlife women enrolled in this study included 16 pre-, 56 peri- and 57 postmenopausal women. We assessed severity of hot flashes using the FDA published draft guidance for clinical evaluation of vasomotor symptoms. Severity is defined as mild, moderate and severe. A Bio-Plex human cytokine 17-Plex assay kit was used to test samples for the presence of 17 cytokines: IL-1b, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12, IL-13, IL-17, TNF-a, granulocyte colony-stimulating factor (G-CSF), granulocyte/macrophage CSF (GM-CSF), interferon (IFN)-g, macrophage inflammatory protein (MIP)- 1b and monocyte chemotactic protein (MCP)-1.
Results: Serum IL-8 concentration in pre-, peri, and postmenopausal women with severe hot flashes was significantly (p < 0.0001, p < 0.0001 and p < 0.01, respectively) higher than the concentrations in women without hot flashes and women with mild and moderate hot flashes. Serum IL-8 concentration in bilateral oophorectomized women with severe hot flashes was significantly (p < 0.0001, p = 0.0002 and p = 0.0004, respectively) higher than the concentrations in women without hot flashes and women with mild and moderate hot flashes. Serum MIP-1b concentrations in pre-, peri- and postmenopausal women and bilateral oophorectomized women with severe hot flashes were significantly higher than the concentrations in women without hot flashes and women with mild and moderate hot flashes. In addition, serum IL-6 concentrations in midlife women with moderate and severe hot flashes were significantly higher than the concentration in women without hot flashes. Serum IL-6 concentration in bilateral oophorectomized women with severe hot flashes was also significantly higher than the concentrations in women without hot flashes and women with mild hot flashes.
Conclusion: Serum concentrations of IL-8, MIP-1b and IL-6 in pre-, peri- and postmenopausal women and bilateral oophorectomized women with hot flashes were significantly higher than those in women without hot flashes. IL-8, MIP-1b and IL-6 may be associated with peripheral vasodilation in women with hot flashes.
PS-418
EFFECTS OF 17 BETA ESTRADIOL BOTH ISOLATED AND ASSOCIATED TO TRIMEGESTONE OVER THE ACUTE INFLAMMATORY PROCESS IN RATS
S. M. R. R. Lima, G. P. Ciabotti, C. C. Carvalho, L. O. Medeiros, G. T. G. Pereira and M. N. C. Abel
Santa Casa of São Paulo Medical School FCMSCSP-São Paulo-São Paulo-Brazil
Objective: To check the influence of 17β-estradiol both isolated and associated to trimegestone over the acute inflammatory process in rats, reproducing the therapeutic use employed in female hormone replacement therapy.
Desing and Methods: Thirty female Wistar rats, with weights between 150-250g, kept in the animal facility of FCMSCSP, with a 12-hour light/dark cycle and free access to food and water, were ovariectomized. The several experimental groups were treated orally, for 28 consecutive days, with 25 μg/kg/day of 17β-estradiol both isolated or associated to 6.25 μg/kg/day of trimegestone. The control group has received vegetal oil. After that period, the inflammatory process was induced through the subcutaneous injection of carrageenan 1% (0.1mL) in the footpad and evaluated by the digital pletismography method 1h (T1), 2h(T2), 4h(T4) and 6h (T6) afterwards.
Results: For the control group, the inflammatory edema has increased quickly up to 4 hours after injecting the irritant substance, being reduced in T6 experimental time. The group of animals treated with 17b-estradiol isolated presented a significant reduction of the edema in T4 (p = 0.029), if compared to control group. 17β-estradiol group presented an increase of 15% of the volume of the foot in 4hs in relation to the initial volume. Meanwhile, for the control group, there was an increase of 27% in the same period. On the other hand, in the treatment combined with trimegestone, a significant increase of the edema was identified when compared to control in T2, T4, and T6 (during these times, p = 0.000). The increase was respectively, 44%, 65%, and 71% against 21%, 27%, and 20% for control group. The comparison of the effects of isolated 17β-estradiol and combined to trimegestone, has shown that trimegestone was capable of increasing the inflammatory edema in T2, T4, and T6 (also, during these times, p = 0.000). 17β -estradiol has respectively presented in those times an increase of 19%, 15%, and 13% in relation to the initial footpad volume. The results were evaluated through the analysis of the variance of repeated measurements and T test for both samples independently.
Conclusions: The results obtained have shown that 17b-estradiol induces the anti-inflammatory effect over the experimental edema and, when associated to trimegestone, there is an increase of the edema, thus characterizing a pro-inflammatory action.
PS-419
EFFECT OF ESTRADIOL TREATMENT ON MONOCYTE FUNCTION IN POSTMENAUPOSAL WOMEN
V. Douin-Echinard1,2,4, F. Tremollières1,2,4, C. Seillet1,3, H. Berges1, F. Lenfant1,2, C. Ribot1,2,4, J. F. Arnal1,2,4, J. C. Guéry1,3 and P. Gourdy1,2,4
1Université Paul Sabatier; 2Inserm U858 I2MR; 3Inserm U563 CPTP; 4Centre Hospitalier Universitaire, Toulouse, France
Objective: 17β-œstradiol (E2) treatment is atheroprotective in LDLR deficient mice, but increases production of inflammatory cytokines by macrophages, dendritic cells, CD4 T helper type 1 cells and Natural killer T cells in C57BL/6 mice which production could be deleterious in atheromatous plaques. A 2-years clinical trial is ongoing to characterize the effect of œstradiol treatment on monocyte function in post-menopausal women.
Design & Method: This clinical trial will include 34 post-menopausal women treated for 30 days with transdermal (n = 17) or oral (n = 17) E2. Monocyte function is characterized by three visits, twice before and 30 days after treatment.
Results: During the first year, 19 women have been recruited. We confirmed increased seric CRP levels in the oral E2 group compared to the transdermic one. The two visits before initiation of the treatment showed a good intra-individual reproductibility for expression of activation markers by monocytes and IL-6 production in vitro after TLR-stimulation. These preliminary data confirmed the necessity for a longitudinal study in the same patient to characterize E2 effect on monocyte activation status.
Conclusion: The follow-up of monocyte reactivity under E2 treatment should help to dissect the ambiguous role of estrogen on disease progression involving inflammatory players like in cardiovascular diseases.
PS-420
EFFECT OF THE SOY ISOFLAVONE ON THE HEMOLYTIC ACTIVITY OF THE COMPLEMENT SYSTEM OF HEALTHY POSTMENOPAUSAL WOMEN
C. M. Marzocchi-Machado1, S. P. S. Migueleti1, A. E. C. S. Azzolini1, Y. M. Lucisano-Valim1, D. R. A. Rios1, E. T. Rodrigues1, M. B. A. Montes1, S. A. Franceschini2 and M. R. T. Toloi1
1Faculdade de Ciências Farmacêuticas de Ribeirão Preto-USP, Ribeirão Preto-SP, Brasil; 2Universidade de Ribeirão Preto-UNAERP- Ribeirão Preto-SP, Brasil
Objective: The use of estrogen, as oral contraceptives or hormonal replacement therapy (HRT), is associated with the thromboembolic and chronic inflammatory diseases. It has been described the increase of the serum levels of factor XII, decrease of the S protein and a clinical manifestation similar that due to the deficiency of C1 inhibitor (angioedema). C1 inhibitor regulates of factor XII and its decrease can result in the increase of factor XII and subsequently generation of the bradykinin and C2 proteolysis by the classical pathway activation, leading to angioedema. Since the complement and the coagulation are related physiological systems, there is an important interest in the investigation of the estrogen effects on these systems and their involvement in the physiopathology of the inflammatory processes. Given the structural similar of the isoflavones to estrogen and the potential importance of the prothrombotic effects of estrogen, this phytoestrogen has been used as an alternative therapy. Epidemiologic studies indicate that high consumption of soy (rich in isoflavones) is associated with a lower risk of coronary heart disease. In addition, the activation of complement is known to be involved in many forms of cardiovascular disease. Then the effect of isoflavone on the complement system is also clearly of interest. The aim of this study was investigate the influence of the isoflavone on the hemolytic activity of the complement system of postmenopausal women. METHODS: In this double placebo-controlled study, 25 postmenopausal women, 47 to 66-year-old healthy volunteers, were randomly assigned to one of two groups: G1 (n = 13), oral soy isoflavone, 40mg/day, or G2 (n = 12), oral placebo, 40mg casein/day, for 6 months. The hemolytic activity of the classical (CP) and alternative (AP) pathways of the complement was analysed by using a kinetic assay. The hemolytic assay, plasma and sheep erythrocytes/antibody (CP) or rabbit erythrocytes (AP), was monitored at 700nm and the time required for absorbance to drop by half (50% lysis = T1/2) was calculated. Statistical analyses: paired t test for matched pair and unpaired t test (G1 vs. G2), considering P<0.05. RESULTS: The hemolytic activity of the complement, for both CP and AP, was not different between isoflavone and placebo groups. In addition, no differences were observed within the same group before vs. after treatment. CONCLUSION: The hemolytic activity of the complement was not influenced by soy isoflavone. Although these results constitute a preliminary study, they can contribute for supporting the epidemiologic studies, which associate the favorable and beneficial use of the isoflavone to HRT with a lower risk of cardiovascular diseases. Furthermore, the mechanisms involved in the regulation of the complement, hemostasis and hormonal therapy should be investigated.
PS-421
LYMPHOCYTE T SUBSETS, 25-HYDROXYVITAMIN D, LEPTIN, INSULIN GROWTH FACTOR 1 AND INSULIN GROWTH FACTOR-BINDING PROTEIN 3 BLOOD LEVELS IN WOMEN
F. R. Pérez-López, G. R. Pérez Roncero, M. T. López Baena, L. Larrad and I. Orden
Clinico Hospital and University of Zaragoza Faculty of Medicine, Zaragoza, Spain
The formation of lymphocytes and other blood cells is a carefully regulated process that is essential for maintenance of a normal immune system. The lymphocytes are responsible for both the humoral and the cell mediated immune responses. Sex hormones influence the immune system activity, and vitamin D levels have been related with gynecologic cancer (Pérez-López FR, Maturitas, in press). However, the links between these hormones, leptin, insulin growth factor (IGF) 1 and IGF-binding protein (IGFBP-3) with the lymphocyte T subsets are unknown. In a group of healthy unselected pre- and postmenopausal women attending the general gynecologic consultation, the cited hormones and lymphocyte T subset counts were determined. Immunofluorescene cell surface staining was performed with monoclonal antibody Cyto-Stat Coulter Clone from Beckman Coulter. Optimal staining is achieved with blood cell counts in the range of 3–10 × 103 cells/mm3. White blood cell counts exceeding 10 × 103 cells/mm3 were diluted, and white blood cell counts below 3 × 103 cells/mm3 were submitted to centrifugation and resuspension, to achieve counts in the range of 3–10 × 103 cells/mm3. The monoclonal antibodies allow to identify and enumerate peripheral blood T and B lymphocytes on a flow cytometer capable of dual fluorescence analysis. Two-color flow cytometry was used to determine lymphocyte subsets in the peripheral blood of 21 women with regular menstrual cycles (RMC), 22 women aged 46 to 54 years, and 27 women aged more than 54 years (table: mean ± SEM).
The data gathered in this preliminary study indicate that the vitamin D levels were normal and there was an inverse relation between IGF-1 with age and years since menopause. Furthermore, T and/or B lymphocyte percentages and absolute values may be used as aids to evaluate competency underlying are-related and body composition-related changes and to monitor lymphocyte levels.
PS-422
PREMATURE OVARIAN FAILURE IN A PATIENT WITH SYSTEMIC LUPUS ERYTHEMATOSUS
I. Vaz1, M. Brandão2, S. Sousa1 and L. Sousa1
1Centro Hospitalar do Porto/Maternidade de Júlio Dinis, Porto, Portugal; 2Centro Hospitalar do Porto/Hospital de Santo António, Porto, Portugal
Autoimmune diseases may involve any organ and are among the most important known causes of premature ovarian failure.
Patients with Systemic Lupus Erythematosus (SLE) have a higher risk of premature ovarian failure, mainly after treatment with cyclophosphamide, as it reduces follicular reserve. It is important to know this risk, draw strategies to avoid it and, when installed, it is essential to define a plan to our patient reproductive life.
We report a case of a 36-year-old patient with Systemic Lupus Erythematosus, diagnosed when she was 27.
Tubal obstruction was shown after a surgery for endometriotic ovarian cysts and an episode of bilateral pelvic abcesses, in 1999, when she was 28.
After two years, acute nephritis occurred and the patient needed treatment with cyclophosphamide. Premature ovarian failure was diagnosed in 2005, when she completed 34 years old.
In the last years, the disease has been stabilized and the patient was offered an assisted reproductive cycle with donor oocytes. Embryo transfer was performed in February of 2008. Pregnancy results will be known soon.
Prevention
PS-423
DEVELOPMENT OF A NEUROENDOCRINE CONVERTER FOR PREVENTING CHRONIC MENOPAUSAL DISORDERS
H. Ishigami and S. Tomita
Kyushu Kyoritsu University Graduate School, Kitakyushu, Japan
Objective: Although stress is said to be the major cause of menopausal disorders, stress involves the manifestation of physiological changes from excitation of the sympathetic nervous system, and a theory has previously been elucidated for inhibiting those physiological changes. In actuality, however, stress is currently treated without eliminating this excitation. We have worked to develop a medical device for applying this neglected theory to medical treatment. We have thus developed a neuroendocrine conversion device on the basis of this theory, a description of which is reported here. This device is believed to prevent the onset of chronic menopausal disorders by silencing excitation of the sympathetic nervous system in advance.
Methods: Methods for blocking adrenalin are described in the medical literature. This device was developed on the basis of those descriptions using human subjects. In order to determine the allowable limit of the intensity of the applied pressure, the stimulation device was worn by 30 patients receiving treatment each day. As a result, more than 20,000 persons were asked about the level of pressure they could tolerate and any changes in how they felt over the course of 3 years. This method was used to perfect this stimulation device. Blood tests, urinalyses and functional tests were also respectively performed by volunteers on 6 to 12 persons each.
Results: Decreased adrenalin levels and increased noradrenalin levels were observed in all subjects. Increased lymphocyte counts, decreased lactic acid, decreased 8-isoprotane, increased prostaglandin E, decreased adrenocortical hormones, increased vital capacity, unchanged myoglobulin and increased rapid recovery from fatigue were also observed.
Conclusion: Increased production of prostaglandin E2 and increased lymphocyte counts are considered to verify the elimination of stress as indicated by the theory that insufficient production of prostaglandin E2 is attributable to gastric ulcers, bronchial asthma and decreased lymphocyte counts observed in stress patients. Even though stress has been depicted in the manner of waves that seem to roll through the body, stress can be prevented by returning cells to their normal healthy state. Thus, this method is believed to be able to contribute to the elimination of stress as a preventive and therapeutic method that does allow menopausal disorders to become chronic or exacerbate.
PS-424
LOW LIVER FAT CONTENT IS ASSOCIATED WITH HIGH CARDIORESPIRATORY FITNESS IN HEALTHY PERIMENOPAUSAL WOMEN. A MONET STUDY
S. Yasari1,2, J. Abdulnour1, P. Imbeault1, R. Rabasa-Lhoret3, J. M. Lavoie3 and D. Prud'homme1
1Behavioral and Metabolic Research Unit, Montfort Hospital, Ottawa, ON, Canada; 2Laboratory of Genetics of Cardiac Diseases, University of Ottawa Heart Institute, Ottawa, ON, Canada; 3University of Montreal, Montreal, QC, Canada
Objective: A high liver fat content (LFC) is now recognised as the hepatic manifestation of the metabolic syndrome. This deterioration occurs during the menopausal transition as a result of oestrogen fluctuation and seems to worsen in the postmenopausal stage. Menopause seems to induce liver fat accumulation and metabolic disturbances independently of obesity. Studies on animal model demonstrated that regular physical activity decreases liver lipid infiltration. The purpose of the present study was to examine the association between cardiorespiratory fitness (CRF) and LFC in healthy premenopausal women.
Design & Method: The sample consisted of 92 healthy premenopausal women (age: 49.9 ± 1.9 yrs; BMI: 23.3 ± 2.3kg/m2) participating in a longitudinal study on the effect of menopause on body composition and cardiovascular risk factors. Subjects reported regular menstrual cycles and were not taking oral contraceptives or hormone replacement therapy, FSH<30IU/L; no surgically-induced menopause; non-smoking. Body composition was measured by dual-energy x-ray absorptiometry (DEXA). Subjects underwent a stress-test on treadmill to measure VO2 peak. LFC was assessed by computed tomography (CT) scan at the T11-T12 level and was presented as a ratio of mean liver to spleen attenuation values (1.14–1.55). Other measurements included fasting plasma lipid profile. Results (Preliminary data): A significant association was found between LFC and VO2 peak (r = −0.22) and total chol/HDL-chol ratio (r = 0.23), (p < 0.05). LFC was not correlated to adiposity level or body composition. When the sample was subdivided into tertiles of LFC, VO2 peak was significantly different (p < 0.05) between subjects characterized by a high and low values of LFC. Regression analyses indicated that 5.6% and 4.6% (0.046 < R2 < 0.056) of the inter-individual variation of LFC was explained by total chol/HDL-chol ratio and VO2 peak respectively. Conclusion: The present finding of an inverse relationship between LFC and CRF independently of adiposity in premenopausal women suggests that a high level of CRF may be an asset to prevent liver lipid accumulation known to occur during the menopausal transition. These results support the notion that physical activity is an effective intervention to prevent liver lipid infiltration.
PS-425
LIPID PROFILE OF MENOPAUSAL INDIAN WOMEN: GENDER AND BODY WEIGHT CONCERNS
P. C. Mittal and R. Kant
University of Allahabad, Allahabad, Uttar Pradesh, India
Objective: Dyslipidemia has been linked to aging, gender and obesity. Since menopause is a landmark in the process of aging, reported to be associated with weight gain, lipid profile of disease-free males and females needs to be compared and assessed in relation to reproductive stage and weight gain.
Design and Methods: Blood lipid profile, comprising of total cholesterol (TC), triglycerides (TG), high density lipoprotein (HDL-C), low density lipoprotein (LDL-C) and very low density lipoprotein (VLDL-C) was studied in relation to age, body weight and gender in a cross-section of 180 Indian disease-free females(F) and males(M) aged 25 to 65 years. Female respondents were divided into three groups: ‘Control’ 25–35 years, ‘premenopausal’ 35–45 years and ‘postmenopausal’ >45 years, and compared with age-matched males. Statistical analysis included Student's t-test, Odds Ratios (OR) and 95% Confidence Intervals (CI) for bivariate analysis and Pearson's correlation coefficients (r).
Results: Body weight and blood cholesterol, LDL-C and VLDL-C were initially lower for females than males but rose rapidly and difference did not remain statistically significant between postmenopausal women and age-matched males. HDL declined after 45 years, but no gender difference was visible. Weight and age were more highly correlated for females (r = 0.79) than for males (r = 0.51). Significant correlation of cholesterol (F: 0.80, M: 0.62) and LDL-C (F: 0.77, M: 0.59) was found with weight but, with increase in age, cholesterol correlated significantly for females (0.54) but not males (0.16), and rise in LDL was less highly correlated (F: 0.49, M: 0.27 for males). In females, for hypercholesterolemia, weight gain (OR 17.94, 95% CI 6.20-51.94 for weight ≥ 65 kg) was a bigger risk factor than age (OR 4.57, 95%CI 1.59-13.11 for age ≥ 44 years) as well as for high LDL-C (OR 20.31, 95% CI 7.46–55.24 for weight ≥ 65 kg and OR 3.50, 95%CI 1.29–9.44 for age ≥ 44 years). For males, neither age nor weight reached statistical significance as risk factors for hypercholesterolemia while the effects on LDL-C were also less pronounced (OR 3.02, 95% CI 1.13–8.07 for weight ≥ 68 kg and OR 2.35, 95% CI 0.88–6.28for age ≥ 42 years).
Conclusion: Weight gain is found to be a greater risk factor than age for dyslipidemia in postmenopausal females, and to a lesser extent for older males raising the possibility that the risk of dyslipidemia can be reduced if weight is not allowed to increase with age.
PS-426
THE INFLUENCE OF HORMONE REPLACEMENT THERAPY ON INTRACRANIAL VESSELS
P. Tsikouras1, G. Galazios1, J. Heliopoulos2, K. Vadikolias2, S. Bouchlariotou1, A. Savidis1, C. Piperidou2 and V. Liberis1
1Obstetrics And Gynecology, Greece; 2Department of Neurology, Neurovascular ultrasound laboratory, Greece
Introduction: Hormonal replacement therapy (HRT) has been suggested to be a risk for stroke, although the data are not consistent. There is the hypothesis that HRT may be related with arterial wall thickening and atherogenesis. Intracranial atherosclerosis leads to stroke that accounts for 8% to 10% of ischemic strokes and are associated with a risk of recurrent stroke approaching 15% per year. With emphasis to identify high-risk patients, recent clinical trials evaluated ways to prevent stroke due to intracranial disease. Transcranial Doppler (TCD) ultrasound noninvasively evaluates cerebral hemodynamics and may be valuable as a screening method to detect >50% stenosis in major intracranial arteries. We assessed women with HT using the TCD in order to detect any abnormal finding and in particular any focal intracranial stenosis.
Patients and Methods: Twenty patients aged from 44 to 53 years were treated with HRT(1 mg 17β-estradiol (E2) combined with 2 mg drospirenone (DRSP) daily in a continuous-combined regimen) for 2 years. All the study women presented with climacteric symptoms, had intact uterus and not any contraindication for therapy.
We evaluated these women from 01.04.07 to 31.10.07 in the neurovascular ultrasound laboratory for complete TCD examination. The study included only postmenopausal women, who have not previously received any regiment for estrogen –progesterone deficiency related symptoms. TCD study was performed using previously described standard insonation protocol using the EME COMPANION (Nicolet Biomedical, Madison, WI, USA) with a 2MHz probe. We assessed women with HRT with TCD for abnormal findings and detection of focal intracranial stenosis. Maximum mean flow velocities (MFV) were obtained from major arteries of the circle of Willis. MFV was classified as normal (30 to 99 cm/s), high (>100 cm/s), and low (<30 cm/s) for the MCA, anterior cerebral artery, and terminal internal carotid artery. MFV in the posterior cerebral, basilar, and vertebral arteries were considered normal (20 to 49 cm/s), high (>50 cm/s), and low (<20 cm/s). We also calculated Pulsatility Index (PI) as (PSV-EDV)/MFV, where PSV is the peak systolic velocity and EDV is the end diastolic velocity.
Results: Normal values of PI are in the range of 0.6 to 1.1 All TCD measurements were between the normal levels We did not also detect any suspicious finding for focal stenosis in the examined intracranial vessels.
Conclusions: The findings of the present study could not demonstrated any association of HRT with stenotic lesions or any other pathology on intracranial vessels.
PS-427
THE USE OF LEVONORGESTREL INTRAUTERINE DEVICE IN THE TREATMENT OF ENDOMETRIAL SIMPLE HYPERPLASIA WITHOUT ATYPIA IN PERI AND POSTMENOPAUSAL WOMEN
S. Haimovich, M. A. Checa, G. Mancebo, F. Larrazabal, and R. Carreras
Del Mar University Hospital, IMAS, Barcelona, Spain
Objective: To assess the effectiveness of the levonorgestrel releasing intrauterine system (LNG-IUS) as a treatment option for peri and postmenopausal women with non atypical simple endometrial hyperplasia.
Design: All consecutive women with the histological diagnosis of non atypical simple endometrial hyperplasia recruited over 1 year period were included in an open, prospective, single-center study. Follow up for at least 2 years after the insertion of LNG-IUS insertion. We evaluated the pattern of uterine bleeding on a 4 point qualitative scale (1 = amenorrea, 2 = scarce, 3 = normal, 4 = abundant).
Results: 15 women were included with a mean age of 49 (2.7) years. Compared with baseline, bleeding decreased quantitatively from a mean score of 3 at baseline (normal bleeding) to 2 (scarce) at 3 and 6 month, and 1 (amenorrhea) at 24 months. We performed endometrial biopsies at 12 months that revealed an atrophic endometrium in 14 women (93,3%) and secretory endometrium in 1(6,7%) (P<0.001). At 24 months, endometrium atrophy was documented in 100% of women.
Conclusion: The LNG-IUS seems to be an effective and save alternative in the treatment of non atypical (simple) endometrial hyperplasia of peri and postmenopausal patients.
PS-428
WHAT TYPE OF MESSAGES MEXICAN WOMEN PREFER FOR PREDICTING THEIR HEALTH AND SEXUALITY DURING MENOPAUSE
G. Sánchez-Ramírez1, C. López-Sosa2 and M. Álvarez-Gordillo1
1El Colegio de la Frontera Sur, San Cristóbal de Las Casas, Chiapas Mexico; 2Universidad de Salamanca, Spain
Objective: To undertake research into women's preferences for receiving messages (whether in a positive or negative way) with information, which would lead to contingency plans for self care of their health and sexuality. This was done by means of a programme about quality of life during menopause, together with a focus on the gender and health (through workshops) of women from three regions of Mexico, with the aim of proposing contents of messages to promote well being during female maturity and ageing.
Materials and Methods: The methodology employed to evaluate preferences for messages to promote self care consisted of the distribution of letters with pictures and texts, which had written opinions (compiled positively in some cards and negatively in others, so that each participant could choose the type of message they preferred). They were read in part by the person applying the evaluation test, therefore recopying the women's preferences after finishing their participation. The study took place in 2005 with 138 women from two social groups (middle and lower class), from three Mexican provinces (Veracruz, the state of Mexico and Chiapas) whose ages ranged between forty and sixty. The results were statistically analysed by separating the replies of the participants according to the social class they belonged to, applying a “Chi squared” test to establish independence between classes and by comparing the percentage of replies according to the preferences for messages for self help.
Results: The results of the investigation gave rise to the knowledge that almost all women prefer to receive positive messages about self help because 86% of the women interviewed were from lower class and 94% (with a “p” of 0.000) of those interviewed were from the middle class chose these, as a reward for the effort of achieving personal well being. The use of pictures accompanied by written phrases facilitates the evaluation of content in this type of investigation in contexts where the majority of women have limited resources (illiteracy, low level of education, little experience of participation in courses and health workshops, etc).
Conclusions: The preference for positive messages women's health prevention is linked to the necessity of women to change the pessimistic view which prevails in Mexico respecting female menopause, maturity and ageing. This is due to the fact that alarm bells are already ringing regarding the development of osteoporosis, cancer, heart problems, etc thus leaving aside all that relates to prevention.
PS-429
WOMEN'S HEALTH AND HYGIENE HABITS IN SPAIN
J. M. Lailla Vicens1 and J. Ferrer Barriendos2
1Hospital Sant Joan de Déu, Barcelona, Barcelona, Spain; 2Hospital Universitario Central de Asturias (HUCA), Oviedo, Asturias, Spain
Objective: To describe women's health and hygiene habits in Spain self-reported by women themselves and to identify potential educational needs.
Design & Method: A cross-sectional survey via post was conducted with a population-based sample of Spanish women from 12 to 74 years old, using age and geographic area of residence to stratify the sample. A structured questionnaire was used to collect information related to:
nutritional habits, exercise and rest
health and gynaecological visits
skin, general and intimate hygiene
menstruation
pregnancy, childbirth and postpartum
menopause
17.3% of women had never gone to visit a gynaecologist. 48.8% had not visited their gynaecologist over the past 12 months (age group 12–19: 82.8%), the main reason being that they did not have any problems (63.3%), and 12.9% did not like to visit the gynaecologist. The most commonly raised doubts related to age and recommended frequency of gynaecologist visits, breast and cervical cancer, sexually transmitted diseases, menstruation, pregnancy and menopause. The most prevalent concerns for women >45 years old were menopause and related diseases and treatments.
59.7% of women reported following a healthy and balanced diet regularly. The intake of vegetables and fruit increased with age. Compliance with nutritional recommendations of the Spanish Communitarian Nutritional Society (SENC) 2004 was greater as age increased from 30 years old, while women in the 20–29 year old group were the least compliant. 13.7% of women reported following a diet. 21.6% were overweight (BMI among 25–30 kg/m2) while 62% of women aged between 12–19 were below normal weight BMI<20 kg/m2. 28.6% of women reported not doing any exercise at all and 17.8% reported sleeping less than 7 hours nightly during the week. 20.7% were current smokers.
98% of the cases took a daily shower. 42% of women reported following a specific hygiene routine of the vulvovaginal area once daily, mainly with common soap and water (63.5%).
Conclusion: The results of this study suggest the need to improve several health habits related to nutrition, exercise and tobacco consumption among women in Spain as well as raising awareness of the importance of regular gynaecologist visits. The gynaecologist must play an important role in training and reporting on women's health and hygiene habits.
PS-430
WORKSHOP ON STRATEGIES FOR POSTMENOPAUSAL WOMEN WELL-BEING: EMPHASIS ON A PREVENTION PATH EXPERIENCED WITH A MULTIPROFESSIONAL TEAM OF HEALTH CARE PROVIDERS
S. Leda
Private Practice Office, Campinas, São Paulo, Brazil
Objectives: To inform women and their husbands about Menopause, and all the changings it brings to the women's life, emphasizing the possibility of experiencing a period of good health, new challenges and personal growing at this stage of life.
To use information as a means of prevention for postmenopausal women.
Design and Method: A multiprofessional team of health care providers create experiences that add good choices for lifestyle changes for postmenopausal women and their families. Nutritionist, physiotherapist, dermatologist, dentist, gynecologist, psychologist and a yoga teacher have each their one-hour session in the program. Health food dishes are prepared “in loco”; body-moving exercises are practiced with music; lectures and question and answer sessions are provided by the physicians and dentist; dynamic activities give everyone an outgoing feeling through the psychologist participation; a moment of relaxation is prepared by the yoga teacher. Lunch time is a real social event that gives the opportunity of sharing experiences and making friends.
Results: Feedback given by the husbands and wives are good, and show their impressions of how information help as real remedy. Although we run these workshops every other month, many couples come back several times. They evaluate the event as being an experience of learning, having fun, and proposing good changes for daily life well-being.
Conclusion: Menopause is just one more step in life and these workshops facilitate to embody this idea. The Workshop on strategies prepared by a multiprofessional team gives to the postmenopausal women and their husbands a means of lifestyle change procedures tha lead to prevention and wellness. It has been a real promotion of life and health.
PS-431:Abstract not available at time of going to press.
Abstracts of Sponsored Symposia
Note to readers:only symposia with abstracts available at the time of publication are listed below.
SS-02: SERMS: tailored treatment for postmenopausal women (organised by Lilly)
SS-02-01
OVERVIEW OF SERMS IN THE MANAGEMENT OF POSTMENOPAUSAL RELATED CHANGES
Joaquim Calaf i Alsina
Prof. Obstetrics and Gynecology; Hospital de la Santa Creu i Sant Pau, Barcelona, Spain.
SERMs are substances that can act as estrogens agonists or antagonists depending on estrogen circulating levels and structure of the complex generated after binding to estrogen receptors. Such structures can bind to alternative response elements and induce different responses throughout the body. Consequently each molecule can have a different profile and has to be tested specifically in the clinical setting. Clomiphene, tamoxifen (TAM) and raloxifene (RLX) are the SERMs currently available for clinical use. TAM is the first SERM to show different effects at level of breast, uterus, bone. As a consequence of positive effects shown by TAM on bone, RLX was developed as a bone protector substance. The clinical trials showed its ability to significantly reduce risk of presenting ER + invasive breast cancer (BrCa). Post hoc analysis of a subgroup of osteoporotic patients with high cardiovascular (CV) risk and observation of positive changes in surrogate markers suggested a potential preventive effect on CV disease.
Results of two big studies exploring these positive additional effects of RLX have been published. RUTH was designed to determine whether treatment with RLX compared with placebo reduces incidence of coronary events and invasive BrCa among postmenopausal women (PMW) with established coronary heart disease (CHD) or multiple CHD risk factors. Study conclusions are that administration of RLX does not increase or decrease risk of coronary events and did not cause early harm. Also it reduced risk of invasive BrCa and of clinical vert fractures. Patients treated with RLX had an increased risk of VTE, and even if there is no difference in overall incidence of stroke, an increased risk of fatal stroke was observed. Treatment with RLX had no effect on overall mortality.
STAR evaluates in 19747 PMW age 35+ years and at increased risk for BrCa, the effect of RLX vs. TAM on the incidence of invasive BrCa. Secondary outcomes are endometrial cancer, ischemic heart disease, and hip, spine, wrist (Colles) fractures. The study shows RLX is as effective as TAM in prevention of primary invasive BrCa. Compared to TAM, RLX use results in fewer thromboembolic events and fewer cataracts. With RLX therapy compared with TAM, there was a nonsignificant higher incidence of noninvasive BrCa (LCIS and DCIS) and decrease in incidence of uterine cancers.
New SERMs are in advanced stages of development. Bazedoxifene co-administered with conjugated estrogens can alleviate hot flushes and protect bone. Ability to antagonize estrogen effects at endometrial level observed in experimental studies has allowed to avoid progestagens in this combination. Arzoxifene is developed for osteoporosis (OP) prevention and treatment and BrCa risk reduction in PMW. Lasofoxifene is under development for OP prevention and treatment and for treatment of vaginal atrophy.
SS-02-02
THE ROLE OF SERMS IN REDUCING BREAST CANCER RISK
Steven R. Cummings
Professor, San Francisco Coordinating Center, USA.
In North America, Europe and Spain, breast cancer is the most common cancer in women and the leading cause of cancer death in nonsmoking women. Breast cancer is preventable. Lifestyle changes, such as reducing weight or increasing exercise, can reduce this risk a little. Unfortunately, studies have shown that dietary changes, including high intake of fruits and vegetables, have little or no effect on breast cancer risk.
Selective estrogen receptor modulators (SERMs) – tamoxifen and raloxifene – reduce the risk of breast cancer by about 50% by reducing the risk of estrogen receptor breast cancer by a greater degree. The STAR trial of nearly 20,000 women at high risk of breast cancer showed that raloxifene and tamoxifen had identical effects on the risk of invasive breast cancer. However, raloxifene is safer than tamoxifen. Compared with women taking tamoxifen, those who received raloxifene had a lower risk of endometrial problems, including hyperplasia, hysterectomy and, probably, endometrial cancer. Those taking raloxifene were less likely to develop cataracts. Raloxifene was also less likely to cause venous thromboembolic disease.
The benefits of chemoprevention appear to last long after treatment is stopped. After 5 years of treatment with raloxifene, the risk of invasive cancer continues to be reduced by about 50% for at least 10 more years.
Doctors should routinely check postmenopausal women for their risk of breast cancer. Women ≥ age 60 who have a family history of breast cancer, or postmenopausal women with high breast density, have a high risk of breast cancer. They should make lifestyle changes to prevent breast cancer and consider taking raloxifene or tamoxifen to further reduce their risk.
SS-02-03
UTERINE SAFETY OF SERMS
Steven R. Goldstein
Professor of Obstetrics and Gynecology, New York University School of Medicine, USA
Tamoxifen has been the most widely prescribed antineoplastic drug worldwide. In the mid to late 1980's a link between tamoxifen and endometrial neoplasia was first reported and since then reports consistently show an increase in endometrial carcinoma in postmenopausal patients treated with tamoxifen. In the mid 1990's an unusual ultrasound appearance in the uterus of patients treated with tamoxifen was first described. In addition tamoxifen treated patients have been shown to have an increased incidence of endometrial hyperplasias and polyps.
The breast cancer prevention trial (NSABP P-1 trial) was the first time that tamoxifen was utilized in women who did not already have breast cancer. Overall relative risk of endometrial carcinoma was 2.53 (CI 1.25–4.97). However there was no statistically significant increase in the women under 50 whereas in women over 50 the relative risk was 4.01 (CI 1.70–10.90). Updated data from the P-1 Trial revealed 53 cases of endometrial carcinoma associated with tamoxifen versus 17 cases in the placebo group. Furthermore there were 4 cases of uterine sarcoma associated with tamoxifen versus none in the placebo group. As a result the FDA required a boxed warning be added to the label of tamoxifen directed at its use for breast cancer prevention not for treatment.
Raloxifene is benzothiophene SERM whereas tamoxifen is a triphenylethylene. A 12 month prospective uterine safety study utilizing transvaginal ultrasound every 3 months as well endometrial biopsy and sonohysterography at 6 and 12 months showed that raloxifene therapy was no different than placebo in terms of endometrial thickness or histology. In a “real world” setting through 4 years of treatment in the MORE trial the relative risk of developing endometrial carcinoma compared to placebo was 0.91 (CI, 0.31–2.71).
Most recently in the STAR trial there was a 39% reduction in uterine cancer in raloxifene treated patients relative to tamoxifen, although this did not achieve statistical significance. Raloxifene treated patients had a statistically significant 63% reduction in hysterectomy, an 83% reduction in hyperplasia, and an 87% reduction in hyperplasia with atypia compared to tamoxifen.
Other SERMs, idoxifene and levormeloxifene, which never received governmental approval, produced unusual ultrasound changes centrally located in the uterus similar in appearance to that of tamoxifen. However neither of these substances reported an increase in endometrial hyperplasias or cancers. Basedoxifene, in the highest doses, showed a diminution in endometrial thickness relative to placebo.
SS-02-04
SERMS – AN INNOVATIVE OPTION TO PREVENT FRACTURES AND INVASIVE BREAST CANCER IN POSTMENOPAUSAL WOMEN
Andrea R. Genazzani
Professor of Obstetrics and Gynecology, Director, Institute of Obstetrics and Gynecology, University of Pisa, Italy
Breast cancer (BrCa) and osteoporosis (OP) have a major impact on life expectancy and QOL of postmenopausal women (PMW). Several risk factors for BrCa include family history, obesity, null parity, early menarche, late menopause. Some of these factors are related to prolonged cumulative exposure to estrogen. Estrogen may be the link between bone and BrCa risk because of its potent effects on mitotic activity of breast epithelium and bone turnover. Bone mineral density (BMD) can be considered a marker of lifetime estrogen exposure because bone contains estrogen receptors and is sensitive to levels of circulating estrogens. Several prospective studies report that women with higher BMD have increased incidence of BrCa. This inverse association between BMD and BrCa however has not been confirmed in other studies. The two most common risk factors for both conditions are age and family history.
SERMs such as tamoxifen (TAM) and raloxifene (RLX) are available for clinical use to reduce the risk of BrCa in PMW. Although RLX did not appear to reduce risk of non-invasive BrCa as well as TAM, it has a lower risk of VTE and does not stimulate the endometrium. Thus RLX has potential for broader application to BrCa risk reduction based upon its better benefit-risk profile in PMW.
The effects of RLX on prevention of osteoporotic fractures and invasive BrCa have been evaluated in multiple trials assessing three different populations of PMW. MORE and CORE evaluated PMW with OP and showed that RLX reduced risk of invasive BrCa. RUTH evaluated PMW with known or at increased risk for coronary disease and demonstrated RLX significantly reduced invasive BrCa risk in PMW. STAR involved 19747 PMW at increased risk for invasive BrCa. Observed incidence rates of invasive BrCa showed that RLX was as effective as TAM in reducing the risk of invasive BrCa.
Based on these study results RLX should be considered the standard of care for reducing invasive BrCa risk in PMW at high risk of the disease. RLX has demonstrated similar efficacy to TAM and has a more favorable safety profile than TAM. It is important for PMW taking RLX for the approved indications of OP prevention and treatment to be informed about potential treatment benefit to lower their risk of invasive BrCa. As women age and enter the postmenopausal phase, incidence of certain diseases such as invasive BrCa and OP increases dramatically and it's important for them to be aware of these serious risks and have treatment choices. To this end, SERMs, and particularly RLX, represent an innovative treatment choice for PMW who are concerned about their skeletal and breast tissue health.
SS-03: Efficacy and safety of soy isoflavones in menopause management. Are they all the same? update and latest news (organised by Arkochim)
SS-03-01
ENDOMETRIAL SAFETY OF PHYTOSOYA
Santiago Palacios1, Francisco Vazquez2, Bruno Pornel3, John Eden4, Philippe Chantre5, Laurence Aubert5, Esmeralda Buendia6 and Pierre Mares7
1Instituto Palacios, Madrid, Spain; 2Clinica de Ginecologia, Lugo, Spain; 3Brussels Menopause Center, Brussels, Belgium; 4Sydney Menopause Centre, Sydney, Australia; 5Arkopharma, Carros, France; 6Arkochim, Madrid, Spain; 7Hôpital Caremeau, Nîmes, France
Many women have chosen to no take Hormonal Treatment either because they have contra indication or because they prefer taking a natural treatment. Considering soy extract as substitute for Hormonal Treatment in the treatment of post menopausal women, the question of the endometrium response to these phytoestrogen is raised. Some clinical studies on the effects of soy isoflavones on the endometrium have been carried out during the last few years, but their results are discordant. The differences observed could be explained mainly by the differences in the type and concentration of isoflavones as well as by the assessment method.
Therefore, the objective of the present study was to assess the endometrial safety of our specific and standardized soy extract (Phytosoya®) according to the EMEA Guidelines.
395 post menopausal women 45–65 years old were included in this international open study. Patients received daily 70 mg of a soy isoflavones extract (35 mg daidzin, 21 mg glycitin and 14 mg genistin) for 52 weeks. Patients had the possibility to continue the treatment 2 additional years. Endometrial biopsy and transvaginal ultrasounds were performed at inclusion and after 12 months and 36 months.
No increase in endometrial thickness has been observed during the course of the study (2.2 ± 0.98 mm at inclusion and 2.12 ± 1.1 mm at 12 months).
The biopsy results were the following after 1 year of treatment : 2 no tissue, 47 insufficient tissue, 255 inactive and 1 proliferative. At 1 year, the calculated incidence rate of hyperplasia outcome was 0% with an upper limit of 95% Confidence Interval of 0.012.
Among the 235 patients who wished to continue the study, 105 have already completed their 3 years of treatment. The repartition of the histologic classifications is the following: 1 no tissue, 15 tissue insufficient for diagnosis (atrophic) and 89 inactive.
The vaginal bleeding were monitored daily by using an electronic patient diary. We collected a total of more than 89000 days with answer during treatment period. The percentage of days without any bleeding represented 99.2% of days with answers during the treatment period whereas they were 95% during selection period.
Conclusion: The endometrial safety of Phytosoya® has been demonstrated with the precision required by European guidelines. Considering the constantly growing population of post menopausal women with their different symptoms and the potential adverse effects of long-term HT, Phytosoya® may be a safe alternative.
SS-03-02
BREAST DENSITY AND CANCER RISK: LATEST NEWS IN BREAST SAFETY OF SOY ISOFLAVONES
B. Pornel1, Gh. Lemaur1, S. Rovenne2, V. Pellichero1, S. Palacios3, F. Vazquez4, P. Chantre5, L. Aubert5 and P. Mares6
1Brussels Menopause Center, Brussels, Belgium; 2EPIsearch, Brussels, Belgium; 3Instituto Palacios, Madrid, Spain; 4Clinica de Ginecologia, Lugo, Spain; 5Arkopharma, Carros, France; 6Hôpital Caremeau, Nîmes, France
Mammographic density is a strong predictor of breast cancer risk and women with high densities are more likely to develop the disease. Estrogeno-progestative therapy has been associated with an higher breast cancer risk and with an increase in breast density. Whereas soy extracts are taken as post menopausal treatment, only few studies have examined the relation between soy intake and mammographic density.
Post menopausal women 45–65 years old were included in an international open study whose secondary objective was to assess breast safety after an one-year daily treatment of 70 mg soy extract (35 mg daidzin, 21 mg glycitin and 14 mg genistin).
Breast density of patients was first estimated with the four BI-RADS density categories (Fourth edition). Breast density was also assessed with a precise mammographic density estimation software.
A total of 166 bilateral mammographies have been classified according to BI-RADS density categories. An increase between T0 and T12 months was observed in only 6 breast whereas a classification decrease was noticed in 13 breasts. No increase from Type 2 to 3, nor type 3 to 4 has been recorded.
We developed a computer-aided mammographic density estimation software allowing to calculate precisely the percentage of dense tissue. Breast density analysis was performed on digitized mammograms using the same film scanner. All the breast images were blinded and randomly displayed to the operator. The total breast area was delimited by the radiologist whereas the dense area were determined using an assisted computerized method based in grey scale threshold. In contrast to Birads classification, even a slight density modification can be recorded for each patient, leading a better precision. After one-year treatment, we didn't observe any significant modification in density percentage.
Conclusion: No significant change in breast density has been observed after 1 year of treatment, suggesting that intake of our specific and standardized soy extract doesn't increase the risk to develop breast cancer. However, these results are to be confirmed with patients who have accepted to be treated for 3 years.
SS-03-03
IMPROVEMENT OF QUALITY OF LIFE WITH PHYTOSOYA: PLACE OF PHYTO ESTROGENS IN MENOPAUSE MANAGEMENT
P. Mares1, L. Aubert2, S. Palacios3, F. Vazquez4, J. Eden5, P. Chantre2, E. Buendia6 and B. Pornel7
1Hôpital Caremeau, Nîmes, France; 2Arkopharma, Carros, France; 3Instituto Palacios, Madrid, Spain; 4Clinica de Ginecologia, Lugo, Spain; 5Sydney Menopause Centre, Sydney, Australia; 6Arkochim, Madrid, Spain; 7Brussels Menopause Center, Brussels, Belgium
A randomized placebo-controlled study* has been conducted to assess the efficacy of Phytosoya®. Hot flushes decreased by 60% after 4 months of treatment, that was significant compared to placebo group (p=0.0095).
During the course of a tolerance study whose main objective was to assess the endometrial safety of Phytosoya®, the quality of life of 305 patients treated for 1 year was monitored. The included patients were not suffering from incapacitating hot flushes and their mean of hot flushes was 3.2 (±3). The total score of Kupperman index at inclusion was 17 (±7.8) and it decreased to 10.1 (±7.8), this represents a significant reduction of 40%. The main improved symptoms were: hot flushes, nocturnal sweating and nervousness.
Hot flushes were recorded very precisely by using an electronic patient diary. The results (expressed in number of answered days on ediary) were analyzed for global population by comparing data obtained during selection period versus during treatment period. During selection period the days without any hot flushes represented 27.5%, this percentage increased to 50% during treatment period, this represents a real improvement for women.
The incidence and intensity of hot flushes were then analyzed in a sub population suffering from more hot flushes. This population was defined as patients having reported more than 3 hot flushes at least ¾ days during selection period (71 patients met these criteria). During the selection phase the answers with at least 5 hot flushes per day represented 72.8% of answers whereas it decreased to 33.7% during treatment. In the same manner, the number of days with hot flushes with severe intensity represented 22% of answers and it decreased to 8% during the treatment phase.
From all these results we can assess that this specific and standardized extract improved the quality of life of post menopausal women.
Conclusion: As the breast and endometrial safety of Phytosoya® have been demonstrated (see presentation N°1 and N°2), this specific and standardized soy extract represents a safe and efficient treatment to alleviate climacteric symptoms.
*Drapier-Faure et al, Effects of a standardized soy extract on hot flushes: a multicenter double-blind, randomized, placebo-controlled study; Menopause 2002 Vol 9; p329–34.
SS-4: Estetrol: a fetal SERM From soy (organised by Pantarhei Bioscience)
SS-4-01
ESTETROL: A NATURAL SERM FOR HRT AND PREVENTION OF OSTEOPOROSIS
Jean-Michel Foidart1, Monique Visser2 and Herjan J. T. Coelingh Bennink2
1Department of ObGyn, University Liège, Belgium; 2Pantarhei Bioscience, Zeist, The Netherlands
Estetrol is effective in alleviating hot flushes in an experimental model considered representative for studying menopausal hot flushes (vasomotor symptoms). The effect of E4 on vaginal cornification and uterine wet weight was studied in the ovariectomised (OVX) rat, demonstrating that E4 has estrogenic effects on the vagina and on the uterus. Oral administration of E4 conveys dose-dependent bone-sparing effects of high quality bone in estrogen depleted OVX rats. The potency of E4 is approximately 20-fold lower compared to EE in all three models. However in breast cell and tumour models E4 appeared to act as an estrogen antagonist (in the presence of estradiol) with a potency comparable to tamoxifen and ovariectomy. Based on this profile E4 is classified as a natural SERM (Selective Estrogen Receptor Modulator).
In the human E4 is orally bioavailable with an elimination half life of 28 hrs and steady-state blood levels are achieved by single daily dose administration. Multiple dose studies were performed with E4 in early postmenopausal volunteers for 28-day treatment periods and with doses of up to 40 mg/day. The effect of a single daily dose of 2 mg E4 on vaginal cytology is comparable to 2 mg E2. A daily dose of 10 mg E4 in 10 women with frequent hot flushes showed possible efficacy. Biochemical bone formation and resorption parameters demonstrated a significant and dose-dependent decrease of bone turn-over, even during short treatment periods of 4 weeks.
Estetrol may become an alternative for the symptomatic treatment of menopausal complaints such as hot flushes and vaginal dryness in early postmenopausal women. Estetrol may also be suitable for the prevention of osteoporosis in the same population. Potential advantages of E4 over E2 and other estrogens include fewer subjective side effects, less interaction with liver function, less venous thromboembolism, a lower incidence of gallbladder disease and possibly also protection of the breast against breast cancer.
SS-4-02
ESTETROL AS THE ESTROGENIC COMPONENT IN THE CONTRACEPTIVE PILL
Philippe Bouchard1, Monique Visser2, Christine Klipping3 and Herjan J. T. Coelingh Bennink2
1Service d“Endocrinologie, Hopital Saint-Antoine, Paris, France; 2Pantarhei Bioscience, Zeist, The Netherlands; 3Dinox, Groningen, The Netherlands
Combined oral contraceptives (COC's) contain an estrogen (E) and a progestin (P). Since the introduction of the pill, efforts have been made to improve the P component. However the E component has been unchanged for decades and today all COC's contain ethinylestradiol (EE).
Estetrol (E4) is a steroid produced by the human fetal liver during pregnancy only. It was discovered in 1965 by Egon Diczfalusy and co-workers at the Karolinska Institute in Stockholm. In the human E4 is orally bioavailable with an elimination half life of 28 hrs. Pharmacological and clinical data have shown that E4 acts as an estrogen on the vagina, the uterus including the endometrium, bone and brain (effect on hot flushes). Surprisingly E4 appeared to act pharmacologically in several in vitro and in vivo breast cell and tumour models as an estrogen antagonist (in the presence of estradiol) with comparable potency to tamoxifen and ovariectomy. Based on this profile E4 is classified as a natural SERM (Selective Estrogen Receptor Modulator).
Oral administration of E4 inhibits ovulation in cycling rats dose-dependently. The relative potency of E4 is about 18 times less compared to that of EE.
The inhibitory effect on ovarian function of daily oral administration of E4 alone or combined with either progesterone or desogestel is being investigated in human volunteers with a proven ovulatory menstrual cycle. Follicular development and endometrial thickness were measured 2–3 times per week and hormone levels were assessed concomitantly during one 28-day cycle. Data will be presented during the meeting.
Potential advantages of E4 over EE include fewer subjective side effects, less interaction with liver function, less venous thromboembolism, a lower incidence of cardiovascular and gallbladder disease and possibly also protection of the breast against breast cancer. When significant clinical advantages are proven indeed and safety and efficacy are comparable to available COC's, the human fetal SERM estetrol could be used as the estrogen in COC's and might replace EE.
SS-4-03
THE POSSIBLE ROLE OF THE FETAL SERM ESTETROL IN THE TREATMENT OF BREAST CANCER
Christian F. Singer1, Monique Visser2, Herjan J. T. Coelingh Bennink2 and Ernst Kubista1
1Division of Special Gynecology, AKH Wien, Vienna, Austria; 2Pantarhei Bioscience, Zeist, The Netherlands
The anti-estrogenic effects of Estetrol (E4) on breast cancer have been evaluated in both in vitro and animal experiments. Studies performed in the estrogen-responsive human breast cancer cell line MCF–7 have demonstrated that E4 acts as a weak estrogen in the absence of estradiol (E2). In the presence of E2, however, E4 acts as estrogen antagonist in a dose-dependent fashion. The effect of E4 on the development of estrogen-responsive breast tumors was confirmed by data obtained from animal experiments. Rats treated with DMBA develop estrogen-responsive breast tumors. This model has become the standard pharmacological model to investigate the effect of new compounds on breast tumors. When DMBA induced rats were co-treated with E4 for 8 weeks, this resulted in a dose-dependent reduction in the number and size of tumors, an effect that was comparable to tamoxifen treatment or ovarectomy. When E4 was administered to rats in which tumors had already developed, a decrease in the number and size of tumors was similarly seen after 4 weeks. This decrease was dose-dependent, comparable to tamoxifen-treated animals, and at high dose levels as effective as ovariectomy.
In summary, available data indicate that E4 has weak estrogen-agonistic effects in vitro, but acts as an estrogen-antagonist in the presence of estradiol in vitro and in vivo. This feature is particularly remarkable, since in pre-menopausal women the ovaries are a physiological source of estrogens, and in post-menopausal women the tumor itself provides for a growth-stimulatory pro-estrogenic environment through local conversion from estrogen precursors.
In view of the beneficial agonistic effects of E4 on other tissues such as bone, brain (suppression of hot flushes) and vagina, E4 might be a promising candidate for the treatment of estrogen-responsive breast cancer, not only in post-menopausal, but also in pre-menopausal women, since E4 inhibits gonadotrophins.
Currently a prospective, two-week treatment, double-blind, placebo-controlled pre-operative phase II trial is ongoing in women with early breast cancer, focusing on markers of proliferation and apoptosis.