
Abstract
Objective
Less attention has been paid to the interaction between voice disorders, stress, and indoor environmental quality for work ability in teachers. Therefore, our aim was to study whether lower work ability associated more strongly when the variables of voice disorders and stress at work were combined as opposed to evaluating these two factors separately.
Methods
We conducted a questionnaire study including validated self-assessment of work ability and a technical assessment of school buildings utilizing a sample of 1198 and a subsample (n = 538) of Finnish teachers.
Results
When combined, voice disorders and stress at work had a stronger association to decreased work ability than when they were evaluated separately. The occurrence of stress was more prevalent in poor and moderate work ability than the occurrence of voice disorders. Nine out of 10 of the teachers who had neither voice disorders nor stress reported good work ability, while four out of 10 of the teachers who suffered from both voice disorders and stress had poor work ability. As regards the background variables, nearly half of the subjects working in the non-problem buildings have neither stress nor voice disorders.
Discussion
We recommend offering support for reducing stress at work to improve teachers’ work performance. The findings also support the maintenance of school buildings and keeping them in good condition. Follow-up studies are needed to investigate the possible effects of voice disorders and the associated variables on work ability.
Introduction
Previous studies have presented valuable findings regarding the multifactorial nature of voice problems in teachers [Citation1–4]. Especially stress and poor indoor environmental quality (e.g. stuffy or dry air, unpleasant odors, changing classroom temperature) are found to be among those with a high risk for voice disorders [Citation1,Citation3,Citation5–7]. However, less attention has been paid to the interaction between voice disorders and the associated variables for work ability.
Our recent findings [Citation8] showed that stress at work (OR 6.5; rather or very much vs. not at all or little stress) and voice disorders (OR 2.4) were significantly associated with decreased work ability in teachers. In addition, other studies have highlighted the associations between voice disorders and decreased work ability [Citation9–11] as well as stress and decreased work ability [Citation12]. We also found that decreased work ability was associated with a perceived poor indoor environment in schools (OR 2.6) [Citation13]. The results indicated a possible association between poor air quality conditions and both voice disorders and stress at work [Citation2]. The findings contribute to previous studies as regards voice symptoms and poor indoor air (IA) [Citation6], stress and poor IA [Citation14], as well as decreased work ability and a poor indoor environment [Citation15,Citation16]. As we suggested in the previous study [Citation13], these three variables may act as a tangle having an impact on work ability.
Decreased work ability is also found to associate with female gender, ageing, and general health [Citation13,Citation17,Citation18]. As regards teachers, asthma and reflux are clear risk factors for voice disorders [Citation8]. Work ability is closely linked to absence due to sickness [Citation13,Citation18]. To compare teachers in different occupations, special education teachers are found to have more sick leaves than class teachers and subject teachers have (9 vs. 11–13 days) [Citation19].
Being that voice disorders clearly associate with stress and other background variables, such as poor IA, there is little information on the interaction between voice disorders, stress, and poor air quality conditions concerning the work ability of teachers. Therefore, our aim was to study whether measuring the combined variables of voice disorders and stress at work would have a stronger association with (1) decreased work ability and (2) background variables, especially poor air quality conditions, than if they were evaluated separately. Based on our recent findings [Citation8,Citation13], we hypothesized that combining voice disorders and stress would have a stronger association with decreased work ability and background variables, especially poor air quality conditions, than if they are evaluated separately. The present paper is a part of an epidemiological study focusing on voice disorders, stress at work, the work environment, and the association with work ability in teachers.
Materials and methods
Study samples
In this study, we utilized two samples; n = 1198 and a subsample of 538 teachers. In March 2017, we sent a questionnaire with two reminders to all primary and secondary school teachers in three cities across Finland (see Supplemental file from questionnaires used for the study). We endeavored to reach altogether 4071 teachers. In total, 1198 subjects completed the questionnaire with a very low amount of missing data. The response rate was 33% (see dataset [Citation20]). The inclusion criteria stipulated that the participants be full-time Finnish-speaking teachers working in comprehensive schools. The exclusion criterion used was to omit teachers working in multiple schools in order to standardize the duration of voice use. Of the participants, 81% were females and 19% males, and the mean age was 44 years (SD 9.1). We have described the design and the descriptive statistics in detail in our previous publications [Citation2,Citation8,Citation13]. The Ethics Committee of the University of Turku gave their ethical approval (statement 26/2016). Permission for the study was also requested from the Education Departments of the Cities in which it was conducted. We sent the questionnaire directly to the work email address of the teachers. The participants gave a written informed consent before taking part, and they were able to answer the questionnaire voluntarily and anonymously.
Voice assessments
To assess voice disorders, we utilized a screening questionnaire consisting of questions about the occurrence of different vocal symptoms. The questionnaire is used in several studies with different combinations of the symptoms [Citation7,Citation21,Citation22]. The symptoms surveyed were morning hoarseness – defined from morning hoarseness and voice becomes low or hoarse for analysis purposes –, voice becomes strained or tires, voice becomes low or hoarse, voice breaks, difficulty in being heard, throat clearing or coughing, and pain around larynx, and the options were every day, every week, less often, and never. Teachers with two or more voice symptoms occurring weekly or more often in the previous 12 months were assigned as having voice disorders. We assessed stress at work with a validated single-item question with a five-point Likert scale [Citation23]. We dichotomized the variable in the analysis as follows; subjects with not at all, little, or somewhat stress were assigned as having no stress, and those with rather or very much stress were assigned as having stress. Of the 1198 subjects, 25% reported of stress at work. Further, we combined the information as regards voice disorders and stress at work and categorized it as follows; group A (no voice disorders, no stress)–group B (no voice disorders, stress)–group C (voice disorders, no stress)–group D (voice disorders, stress). The resulting variable is referred to as the combined voice and stress. We measured work ability utilizing a validated single-item question, the Work Ability Score (WAS) [Citation24] that enquired about current work ability compared with a lifetime best. WAS is scored on a scale from 0 (“completely unable to work”) to 10 (“work ability at its best”). We classified WAS as follows [Citation18]: poor (0–5 points), moderate (6–7), good (8–9), and excellent (10), good and excellent were combined as good for the analysis. Of the participants, 71% had good, 23% moderate, and 6% poor work ability.
Background variables
As background variables, we assessed gender, age, and profession category group (class teacher, subject teacher, special education teacher). As regards voice-related diseases, the participants were questioned about asthma and reflux. We assessed sickness absence with two variables, the number of sick leave days during the previous year, and the amount of sick leave over 14 days. We did not assess smoking as it was not associated with voice disorders in the sample [Citation13].
In addition, we utilized a technical assessment of the school buildings to validate the self-reported data according to the recommendations [Citation25]. The assessment was performed with the subsample of 538 subjects who were working in one of the cities where a technical assessment was available for every school building. It was an overall evaluation of the deficiencies that are likely to decrease the IA quality in school buildings and are closely linked to voice problems: challenges with ventilation and impurities [Citation26–29]. The assessment was conducted by two technical experts, who had actively worked with the buildings of interest. The information was based on the recollection of the experts concerning the investigations and measurements that had been carried out in the school buildings during previous years from ventilation and impurities. The experts classified the 67 school buildings as follows: IA non-problems; IA problems, not renovated (including partially renovated problems); IA problems renovated. This classification is used in Finnish benchmarking data from the Finnish Institute for Health and Welfare [Citation30] who assess the health promotion activities in schools every two years. The experts were not aware of the results of the questionnaire.
Statistical analysis
We performed statistical analysis with a Chi-square test or a Fisher’s exact test for categorical variables. For the continuous variables, we performed a one-way ANOVA (age; normally distributed) or Wilcoxon’s rank sum test (the number of sick leave days; not normally distributed). We also created a logistic regression analysis model for the ordinal data, adjusted for gender, age, asthma, reflux, and sick leave over 14 days. All statistical tests were performed as two-tailed, with a significance level set at .05. The analysis was performed using JMP Pro 16.0.0 for MacOS and SAS® System, version 9.4 for Windows (SAS Institute Inc., Cary, NC).
Results
Assessed with a sample of 1198 teachers, the results show that 39% of the subjects were in group A, 36% in group C, 17% in group D, and 7% in group B. When we compared WAS with the combined voice and stress categories, we found a significant association (p<.001). Ninety percent of the subjects in group A reported good work ability whereas 40% of those in group D reported poor work ability (). The association between WAS and the combined voice and stress was significant also when studied by using logistic regression models, adjusted for gender, age, asthma, reflux, and sick leave over 14 days (p<.0001). As shows, the combined voice and stress categories significantly associated with the other background variables except for the professional category (all p values <.05).
Figure 1. The interaction between voice disorders and stress at work for work ability (p<.001; n = 1198).
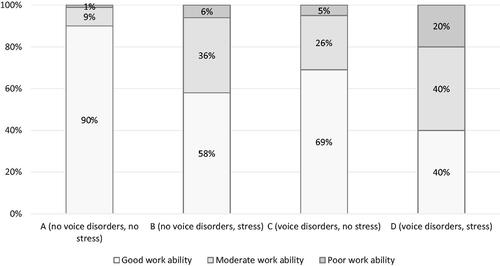
Table 1. The associations between the combined voice and stress categories and background variables in gender, age, profession, asthma, reflux, number of sick leave days, and sick leave >14 days (n = 1198; n = 538 in the technical assessment).
Most of the females were in groups A and C whereas most of the male teachers were only in group A. The participants in group B were significantly younger than the other subjects. Teachers with asthma were mostly in group C compared to the subjects without asthma who were mainly in group A. Parallel results were found for those who suffered from reflux. The number of sick leave days was the lowest among the subjects in group A. Those who had the most amount of sick leave over 14 days, were mainly in group C.
According to the findings with the sample of 583 subjects, group A was the largest group of subjects who worked in the buildings without IA problems. Group C was the largest group in the buildings with both IA problems, not renovated and IA problems renovated. Overall, group B consisted of 8%–10% subjects, depending on the technical assessment whereas group C included 35–39%, respectively.
Discussion
The results demonstrate that combining voice disorders and stress at work has clearly a stronger association to decreased work ability than if they are evaluated separately. Nine out of 10 of the teachers without voice disorders or stress at work reported good work ability, while four out of 10 of the teachers who suffered from both voice disorders and stress had poor work ability. The occurrence of stress was more prevalent as regards poor or moderate work ability than the occurrence of voice disorders. The interaction was not as clearly related to the background variables as it was to voice and stress. Group A was the largest group of subjects who worked in the non-problem buildings while group C was the largest group in the problem- and renovated buildings.
Relation between voice disorders and stress at work, and work ability
Previous studies have found stress to decrease work ability in teachers [Citation12] and the risk of voice disorders to decreased work ability to be high (aOR 12.2), using the same instrument as in our study [Citation9]. Moreover, stress is repeatedly associated with voice symptoms [Citation6,Citation7]. In our study, the number of sick leave days was the lowest in the teachers without voice disorders or stress and this is in line with our findings as regards work ability where the best work ability was in this group. The highest number of sick leave days, in turn, was in those with both voice disorders and stress although the difference was minor. Previous studies reveal that sick leave was more common in teachers with voice symptoms than for those without symptoms [Citation10,Citation11]. The largest group of subjects who had the most sick leave, over 14 days, was the teachers who had only voice disorders without stress. The same trend was also found in other categorical variables (gender, asthma, reflux, and technical assessment) where voice disorders (group C) were clearly more prevalent than stress (group B).
Relation between voice disorders and stress at work, and background variables
The female teachers suffered more often from both voice disorders and stress than males, but there was no elevated interaction association as the prevalence of females was only 19% in group D. Gender differences in teachers are well-known in the areas of both voice disorders [Citation31] and stress [Citation6], and significant gender-related differences related to the association between voice symptoms and stress have been suggested in a sample of the general population [Citation7]. In our study, females reported a lower work ability than males. Parallel results have been suggested in studies in which the female teachers had significantly more sickness absences than the male teachers [Citation11,Citation15].
In our sample, the subjects in group B were significantly younger than the other subjects. Previous findings show contradictory results with young teachers reporting more voice symptoms than older ones [Citation32] whereas a meta-analysis showed inconclusive findings as regards the relation between age and stress [Citation33]. However, young teachers tend to have more sick leave than their older colleagues [Citation15] and there is also a significant association between ageing and decreased work ability [Citation34]. As noted [Citation35], females are also shown to present menopausal voice changes, and this has been even more evident in teachers than in non-teachers. However, our findings did not show a similar trend. The participants in group C had more asthma and reflux than the other subjects. As noted, asthma – and especially asthma medication – as well as reflux are strong risk factors for voice disorders [Citation7,Citation36].
Relation between voice disorders and stress at work, and the condition of school buildings
As regards IA quality, the prevalence of stress (alone) was relatively low regardless of the condition of buildings. In contrast, the occurrence of voice disorders was clearly higher in all the buildings. Moreover, the prevalence of the combined voice and stress was nearly three times higher in the renovated buildings compared to the non-problem buildings. This finding is in line with a follow-up study where hoarseness did not decrease after a mold- and moisture renovation [Citation16] whereas other studies show contrary results [Citation37]. In general, respiratory symptoms are suggested to improve to some extent [Citation38]. Findings with a sample of 28,826 employees suggested somewhat parallel findings to ours with the school staff having slightly less stress and more health symptoms than office employees [Citation39]. Previous studies have suggested that psychosocial factors associate significantly with IA problems at workplaces [Citation40]. However, they noted that the employees who had a more negative perception of their psychosocial work environment had more building-related symptoms [Citation40]. This finding is contradictory to our results. A potential cause of stress may be engendered by a situation where the renovation has been prolonged or improperly performed. Open communication is essential in all cases so that employees can be confident that their work environment is safe. In addition to proper management and renovation of the buildings, increasing social support at an organizational level would benefit the impact of symptoms related to IA quality [Citation41]. Our results also indicated that nearly half of the teachers who worked in the non-problem buildings had neither voice disorders nor stress which supports the constant maintenance of the buildings and keeping them in a good condition. It must also be recognized that there are probably other variables associate with work ability that were not included this study.
Strengths and limitations
A strength of our study was that we used a large sample across Finland and well-defined questionnaires that are widely used. Stress at work has been validated in different working groups [Citation23] and it identifies well-being at work better than instruments that are illness-based. WAS refers to current work ability compared with a lifetime best in addition to other work-related issues, e.g. mental resources [Citation18,Citation24,Citation42]. Further, the participants answered almost every question and, thus, the amount of missing data was very low. As a limitation, the questionnaire did not cover the common cold that, however, is associated with voice disorders. A further strength was that we utilized an external evaluation of the school buildings. Multiple individual variables play a key role in occupational voice disorders and teaching work. Voice disorders and stress at work are more present in teaching because of the nature of the work in practice – mentally and vocally loaded with close cooperation with pupils.
There is no possibility of assessing the causality by using a cross-sectional design. The cross-sectional study design is also a potential source of bias because of the tendency to over- or underreport in the questionnaire as well as mistakes in item interpretation [Citation43]. As we named the subject title “Indoor questionnaire for teachers” when sending the questionnaire, the subjects who worked in problem buildings or suffered from health symptoms may have participated more actively. The response rate was 33% despite the limited number of questions and support from the employers. Although we sent the questionnaire to slightly more subjects than was evaluated (4071 vs. 4000), the sample size was smaller than expected (n = 1500). The low response rate has potentially caused a selection bias. However, our results are supported by previous findings as regards significant associations between voice disorders, stress, and decreased work ability [Citation9–12]. In addition, our sample was representative concerning the distributions of gender and age in Finnish teachers [Citation13]. As far as we know, this is the first study to date where the interaction between voice disorders and stress at work for work ability has been evaluated. The results support our previous findings that suggested that voice disorders, stress at work, and a poor indoor environment may act as a tangle that would have an association with work ability that is more than the sum of its parts [Citation13]. Follow-up studies with a large sample size are needed to investigate these possible effects on work ability.
Conclusions
As a conclusion, the findings supported our hypothesis. Voice disorders and stress at work together clearly had a stronger association to decreased work ability than if they had been evaluated separately. The occurrence of stress was more prevalent in poor and moderate work ability than the occurrence of voice disorders. Further, nearly half of the subjects working in the non-problem buildings have neither stress nor voice disorders. The interaction association between voice disorders and stress at work did not have as clear a relation with the other background variables. The results indicate that it is appropriate to offer support to reduce stress at work to improve teachers’ work performance. The findings also support the maintenance of school buildings and keeping them in good condition.
Geolocation information
Finland, Europe.
Supplemental_File._Questionnaire.pdf
Download PDF (64.8 KB)Acknowledgements
We would like to thank Elizabeth Nyman M.A. for providing language help.
Disclosure statement
Tuula Putus has financial interests in Orion Pharma Ltd. without any involvement in the study. The other authors report no conflict of interest.
Additional information
Funding
Notes on contributors
Hanna Vertanen-Greis
Hanna Vertanen-Greis, PhD, is a post-doctoral researcher in the field of voice ergonomics. She has graduated from the medical faculty of the University of Turku. Previously, Ms. Vertanen-Greis was a music instructor and graduated also from the Sibelius Academy (MMus) and the University of Helsinki (MSc). Apart from a strong musical education, she studied logopedics as well as educational sciences and administration.
Eliisa Löyttyniemi
Eliisa Löyttyniemi, MSc, is a biostatistician, who worked for several pharmaceutical companies between 1993 and 2010, and then continued working in a company that developed neonatal and newborn screening technologies. From 2013, she has worked at the University of Turku where she is responsible for analyzing the research data and teaching of medical students.
Jukka Uitti
Jukka Uitti, MD, PhD, is a professor emeritus of Occupational Health Care and Occupational Medicine at the University of Tampere. He also worked as the chief physician at the Finnish Institute of Occupational Health. He is qualified as a specialist in Occupational Health Care and in occupational medicine. He was awarded the title of docent at the University of Tampere in 2004. His research areas are, inter alia, epidemiology, occupational medicine, and asthma.
Tuula Putus
Tuula Putus, MD, PhD, is a professor of Occupational Health and Environmental Medicine at the University of Turku. She is qualified as a specialist in occupational medicine. She was awarded the title of docent at the University of Kuopio in 2010. Her research areas are, inter alia, occupational health and medicine, environmental medicine.
References
- Rantala LM, Hakala S, Holmqvist S, et al. Associations between voice ergonomic risk factors and acoustic features of the voice. Logoped Phoniatr Vocol. 2015;40(3):99–105.
- Vertanen-Greis H, Löyttyniemi E, Uitti J, Putus T. Self-reported voice disorders of teachers and indoor air quality in schools: a cross-sectional study in Finland. Logop Phoniatr Vocology [Internet]. 2021;0(0):1–11. Available from: https://doi.org/10.1080/14015439.2021.1953132.
- Houtte E v, Claeys S, Wuyts F, et al. Voice disorders in teachers: occupational risk factors and psycho-emotional factors. Logop Phoniatr Vocol. 2012;37(3):107–116.
- Lyberg-Åhlander V, Rydell R, Löfqvist A, et al. Teachers’ voice use in teaching environment. Aspects on speakers’ comfort. Energy Procedia. 2015;78:3090–3095.
- Trinite B. Investigating voice differences in teachers with and without self-reported voice disorders, and healthcare workers without self-reported voice disorders. Logoped Phoniatr Vocol. 2021;46(2):47–54.
- Kooijman PGC, de Jong F, Thomas G, et al. Risk factors for voice problems in teachers. Folia Phoniatr Logop. 2006;58(3):159–174.
- Holmqvist S, Santtila P, Lindström E, et al. The association between possible stress markers and vocal symptoms. J Voice. 2013;27(6):787.e1–787.e10.
- Vertanen-Greis H, Löyttyniemi E, Uitti J. Voice Disorders are Associated With Stress Among Teachers: A Cross-Sectional Study in Finland. J Voice. 2020 May;34(3):488.e1-488.e8.
- Giannini SPP, Latorre M, Fischer FM, et al. Teachers’ voice disorders and loss of work ability: a case-control study. J Voice. 2015;29(2):209–217.
- Lyberg Åhlander V, Rydell R, Löfqvist A. Speaker's comfort in teaching environments: voice problems in Swedish teaching staff. J Voice. 2011;25(4):430–440.
- van Houtte E, Claeys S, Wuyts F, et al. The impact of voice disorders among teachers: vocal complaints, treatment-seeking behavior, knowledge of vocal care, and voice-related absenteeism. J Voice. 2011;25(5):570–575.
- Kyriakou C. Teacher stress: from prevalence to resilience. In: Langan-Fox J, Cooper CL, editors. Handbook of stress in the occupations. Edward Elgar Publishing Limited; 2011. p. 161–173.
- Vertanen-Greis H, Löyttyniemi E, Uitti J, Putus T. Work ability of teachers associated with voice disorders, stress, and the indoor environment: A questionnaire study in Finland. J Voice. 2020;Oct 8;S089(Online ahead of print).
- Finell E, Haverinen-Shaughnessy U, Tolvanen A, et al. The associations of indoor environment and psychosocial factors on the subjective evaluation of indoor air quality among lower secondary school students: a multilevel analysis. Indoor Air. 2017;27(2):329–329.
- Ervasti J, Kivimäki M, Kawachi I, et al. School environment as predictor of teacher sick leave: data-linked prospective cohort study. BMC Public Health. 2012;12(1):770.
- Patovirta RL, Husman T, Haverinen U, et al. The remediation of mold damaged school – a three-year follow-up study on teachers’ health. Cent Eur J Public Health. 2004;12(1):36–42.
- van den Berg TIJ, Elders LAM, de Zwart BCH, et al. The effects of work-related and individual factors on the work ability index: a systematic review. Occup Environ Med. 2009;66(4):211–220.
- Ahlstrom L, Grimby-Ekman A, Hagberg M, et al. The work ability index and single-item question: associations with sick leave, symptoms, and health—a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;36(5):404–412.
- Sick leave absences in Finnish municipalities [Internet]; 2020; [cited 2020 Sep 8]. Available from: https://tyoelamatieto.fi/#/fi/dashboards/kunta10-sick-leave
- Vertanen-Greis H, Löyttyniemi E, Uitti J, Putus T. “Dataset of the participants.”, Mendeley Data, V1. 2021.
- Simberg S, Sala E, Vehmas K, et al. Changes in the prevalence of vocal symptoms among teachers during a twelve-year period. J Voice. 2005;19(1):95–102.
- Sala E, Laine A, Simberg S, et al. The prevalence of voice disorders among day care center teachers compared with nurses: a questionnaire and clinical study. J Voice. 2001;15(3):413–423.
- Elo AL, Leppänen A, Jahkola A. Validity of a single-item measure of stress symptoms. Scand J Work Environ Health. 2003;29(6):444–451.
- Tuomi K, Ilmarinen J, Jahkola M, et al. Työkykyindeksi [work ability index] (Työterveyshuolto 19). Helsinki, Finland: Finnish Institute of Occupational Health; 1997.
- Occurrence of moisture problems in schools in three countries from different climatic regions of Europe based on questionnaires and building inspections – the HITEA study. Indoor Air. 2012;22:457.
- Corgnati SP, da Silva MG, editors. Indoor climate quality assessment. REHVA guidebook. Forssa (Finland): REHVA, Federation of European Heating, Ventilation and Air-conditioning Associations; 2011.
- Vilkman E. Occupational safety and health aspects of voice and speech professions. Folia Phoniatr Logop. 2004;56(4):220–253.
- Bayer CW, Crow SA, Fischer J. Causes of indoor air quality problems in schools. Summary of scientific research. Revised edition. Oak Ridge (TN): U.S. Department of Energy; 2000.
- ASHRAE. Ventilation for acceptable indoor air quality. Atlanta: American Society of Heating and Air-Conditioning Engineers Inc.; 2010.
- THL (The Finnish National Institute of Health and Welfare). Benchmarking system of health promotion capacity building. The Finnish National Institute of Health and Welfare (THL); 2022.
- Dejonckere PH. Gender differences in the prevalence of occupational voice disorders. In: Dejonckere PH, editor. Occupational voice: care and cure. The Hague, The Netherlands: Kugler Publications; 2001.
- Leão SHDS, Oates JM, Purdy SC, et al. Voice problems in New Zealand teachers: a national survey. J Voice. 2015;29(5):645.e1–645.e13.
- Brewer EW, Shapard L. Employee burnout: a meta-analysis of the relationship between age and years of experience. Hum Resour Dev Rev. 2004;3(2):102–123.
- El Fassi M, Bocquet V, Majery N, et al. Work ability assessment in a worker population: comparison and determinants of work ability index and work ability score. BMC Public Health. 2013;13(1):305.
- Sovani P, Mukundan G. Comparison of postmenopausal voice changes across professional and non-professional users of the voice. S Afr J Commun Disord. 2010;57(57):76–81.
- Roy N, Merrill R, Thibeault S, et al. Prevalence of voice disorders in teachers and the general population. J Speech Lang Hear Res. 2004;47(2):281–293.
- Putus T, Vilén L, Atosuo J. The association between work-related stress, indoor air quality and voice problems among teachers – is there a trend? J Voice. 2021.
- Sauni R, Uitti J, Jauhiainen M, et al. Remediating buildings damaged by dampness and mould for preventing or reducing respiratory tract symptoms, infections and asthma. Cochrane Database Syst Rev. 2015;(9):CD007897.
- Tähtinen K, Remes J, Karvala K, et al. Perceived indoor air quality and psychosocial work environment in office, school and health care environments in Finland. Int J Occup Med Environ Health. 2020;33(4):479–495.
- Lahtinen M, Sundman-Digert C, Reijula K. Psychosocial work environment and indoor air problems: a questionnaire as a means of problem diagnosis. Occup Environ Med. 2004;61(2):143–149.
- Mendelson MB, Catano VM, Kelloway K. The role of stress and social support in sick building syndrome. Work Stress. 2000;14(2):137–155.
- Ilmarinen J. Work ability—a comprehensive concept for occupational health research and prevention. Scand J Work Environ Health. 2009;35(1):1–5.
- Hardy B, Ford LR. It’s not me, it’s you: miscomprehension in surveys. Organ Res Methods. 2014;17(2):138–162.