
Abstract
Acute type A aortic dissection (ATAAD) is still one of the most challenging diseases that cardiac surgeons encounter. This review is based on the current literature and includes the results from the Nordic Consortium for Acute Type-A Aortic Dissection (NORCAAD) database. It covers different aspects of ATAAD and concentrates on the outcome of surgical repair. The diagnosis is occasionally delayed, and ATAAD is usually lethal if prompt repair is not performed. The dynamic nature of the disease, the variation in presentation and clinical course, and the urgency of treatment require significant attentiveness. Many surgical techniques and perfusion strategies of varying complexity have been described, ranging from simple interposition graft to total arch replacement with frozen elephant trunk and valve-sparing root reconstruction. Although more complex techniques may provide long-term benefit in selected patients, they require significant surgical expertise and experience. Short-term survival is first priority so an expedited operation that fits in with the surgeon’s level of expertise is in most cases appropriate.
Introduction
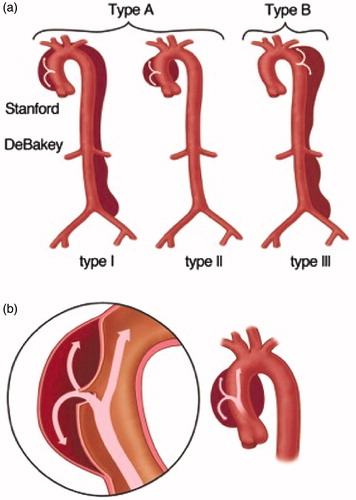
Acute aortic dissection is a rare life-threating condition of the aorta, and is associated with significant morbidity and mortality [Citation1]. The most lethal of dissections involves the ascending aorta and is commonly referred to as acute type A aortic dissection (ATAAD) (). Unless prompt surgical repair is performed, the patients usually die from complications related to the dissection, including rupture of the aorta, pericardial tamponade, aortic regurgitation, end-organ malperfusion, or acute heartfailure [Citation2,Citation3].
Figure 1. (a) Types of aortic dissection according to the Stanford classification system (shown at top) and the DeBakey classification system (shown at bottom). (b) Intimal tear and propagation of the dissection between the media and intima layers of the ascending aorta. Drawings: Hjördís Bjartmarz. Copyright ©Tomas Gudbjartsson.
This review has been written by nine cardiothoracic surgeons who have participated in the Nordic Consortium for Acute Type-A Aortic Dissection (NORCAAD) collaboration, which assembled a cohort of 1159 ATAAD patients who were operated at eight Nordic university hospitals between 2005 and 2014 [Citation4]. For ATAAD, as with most surgical emergencies, there have been few randomized trials providing evidence for optimal management [Citation5]. Thus, contemporary, sizeable, multicenter observational registries, of which NORCAAD is an example, stand out as important sources of information. This review covers different aspects of ATAAD, including epidemiology, pathophysiology, and surgical treatment, and concentrates especially on the NORCAAD studies that have been published so far [Citation6–13]. We searched the PubMed and MEDLINE databases using the search terms “dissection,” “aortic,” “ascending,” and “type A.” In this review, we mainly focus on articles on epidemiology, classification, pathophysiology, risk factors, clinical presentation, diagnostic imaging, biomarkers, treatment, complications, and long-term follow-up of ATAAD that have been published in the past 10 years.
Definitions and classification systems
Dissection of the aorta occurs when the aortic media is separated, usually by pulsatile flow that penetrates the intimal layer of the aortic wall [Citation14] (. This allows blood to flow between the layers of the aortic wall, forcing the layers apart, creating a false lumen parallel to the native (i.e. true) aortic lumen (. Consequently, the false lumen can propagate in both directions from the tear of intima and affect most of its distal branches, including the coronary, cerebral, and mesenteric arteries [Citation15]. Another―but less common―mechanism for aortic dissection is a bleeding into the aortic wall without an intimal tear, often called intramural hematoma [Citation16]. Finally, traumatic dissections occur from tears of the intima secondary to injury, which is most often iatrogenic, such as during percutaneous coronary intervention (PCI), cardiac catheterization, arterial cannulation for cardiopulmonary bypass (CPB), cross-clamping of the aorta during open heart surgery, or during cardiovascular interventions, such as endovascular aneurysm repair (EVAR), transcatheter aortic valve implantation (TAVI), or insertion of an intra-aortic balloon-pump (IABP) [Citation17,Citation18]. Although it is debated, in most instances, the recommended treatment for intramural haematomas and iatrogenic dissections of the thoracic aorta is similar to that for the more common conventional and non-traumatic tear AATADs. Intramural haematoma, ruptured aneurysms and non-traumatic and iatrogenic dissections constitute what is collectively referred to as acute aortic syndrome (AAS) [Citation16,Citation17].
Most dissections of the thoracic aorta present with acute symptoms, although the definition of acute aortic dissection is still debated [Citation19]. ATAAD is usually defined as a dissection that is diagnosed within 14 days after onset of symptoms, but definitions using time frames of 30 or 90 days (subacute dissections) have also been used [Citation20–22]. The much less common chronic type A aortic dissections usually represent a subset of patients who were not diagnosed at the time of onset due to absence of symptoms or atypical symptoms and who remained stable until eventually diagnosed [Citation19]. Chronic dissections are often treated with elective surgical repair and will not be discussed further in this review.
The most commonly used classification for aortic dissections is the Stanford classification system, introduced in 1970 () [Citation23]. Stanford type A dissections involve the ascending aorta proximal to the innominate artery (brachiocephalic trunk), regardless of extension into the aortic arch or the descending aorta. Stanford type-B dissections involve only the thoracic aorta below the left subclavian artery [Citation3,Citation17]. The Stanford classification is not a classification of the tear site. Consequently, an intimal tear distal to the left subclavian artery with retrograde dissection into the ascending aorta will be classified as being type A. By analogy, intimal tear and dissection originating in the aortic arch will be classified as being type A if extending into the ascending aorta, and as type-B if extending into the descending aorta, and as non-A non-B if contained in the arch only [Citation3,Citation17]. According to the modified DeBakey classification from 1982, both DeBakeytype-I and type-II dissections involve the ascending aorta, but type I extends beyond the innominate artery, while type II is located entirely in the ascending aorta () [Citation23]. Thus, Stanford type A dissections include both type-I and type-II DeBakey dissections and Stanford type-B dissections are defined as DeBakey type-III dissections. The Stanford classification is clinically useful, to guide acute management, whereas the DeBakey classification is more informative for long-term follow-up, since it differentiates between proximal and distal aortic involvement.
The Penn classification is a recent method of categorizing type A dissections by their clinical presentation [Citation24–26]. Class Aa is characterized by the absence of branch vessel malperfusion or circulatory collapse, and class Ab by symptoms or signs of localized organ ischaemia. Class Ac is characterized by circulatory collapse, with or without cardiac involvement, and class Abc is characterized by localized and generalized ischaemia combined.
Epidemiology
ATAAD accounts for 58‒62% of all aortic dissections [Citation27,Citation28]. The total case-fatality rate of ATAAD is estimated to be 73% and pre-hospital death up to 49% [Citation29]. Historically, the incidence of ATAAD has been reported to be 2.5‒6 per 100,000 patient years, reaching its peak during the seventh and eighth decades of life [Citation27,Citation29–34]. Howard et al. found that 35% of all aortic dissections occur in patients who are older than 75 years [Citation29], and age has been identified to be an independent predictor of aortic dissection [Citation27]. The increasing age of the population is probably contributing to the higher incidence (8.7 per 100,000 patient years) recently reported by Landenhed et al. (2015) [Citation28], and as a consequence of the increasing life expectancy it has been estimated that the proportion of dissections in patients over 75 years could reach 50% by 2030 and 57% by 2050 [Citation29,Citation32].
Risk factors
The most important risk factors for ATAAD are presented in . Men are over-represented and constitute 62‒68% of all patients with surgically treated ATAAD [Citation3,Citation12,Citation33]. However, women tend to present with their dissection at a higher age and constitute the majority of patients over 75 years [Citation27,Citation35]. Hypertension has been reported in 67‒86% of patients with ATAAD, and is together with smoking and atherosclerosis independent predictors of ATAAD [Citation3,Citation27,Citation28].
Table 1. Major risk factors for aortic dissection.
Iatrogenic aortic dissections account for 1‒5% of ATAADs [Citation12,Citation19,Citation27]. ATAAD during pregnancy is uncommon; it usually occurs either during the last trimester or in the puerperium, and is often associated with connective tissue disease [Citation36].
In the NORCAAD registry, 8% of the patients have a family history of aortic dissection [Citation4] and it has been reported that 20% of patients with ATAAD have a first-degree relative with a dilated thoracic aorta [Citation37]. It has been suggested that aneurysms localized in the ascending aorta are more often associated with hereditary conditions, whereas descending aortic aneurysms more often form as a result of atherosclerosis, advanced age, and hypertension [Citation38,Citation39].
Marfan syndrome (MFS) is a monogenic autosomal dominant disorder caused by a mutation in the FBN1 gene, encoding the protein fibrillin-1. MFS patients typically present with a pear-shaped aneurysm of the aortic root. The cardiovascular manifestations of the disease are caused by the loss of the ability of fibrillin-1 protein to form polymeric fibrillins, leading to diffuse medial degeneration with subsequently reduced strength and integrity of the elastin-rich tissue of the aortic wall. All medium-sized and large arteries in MFS patients are at risk of dissection [Citation38]. MFS has been reported in 3.4‒6.7% of ATAAD patients in the large registries [Citation12,Citation19,Citation27], and in the NORCAAD registry the proportion is 4% [Citation4,Citation11]. Fibrillin-1 also appears to have a regulatory role by interaction with tissue growth factor-β (TGF-β), which controls cell differentiation, motility, and proliferation [Citation38]. A mutation of the gene TGFBR1 or TGFBR2, encoding TGF-β, is also the cause of Loeys-Dietz syndrome, which is associated with a disseminated arteriopathy with central and peripheral dissections [Citation38].
Ehlers-Danlos syndrome has been reported in 0.6% of patients with ATAAD in the GERAADA registry [Citation40]. It includes various genetic defects affecting the biosynthesis or structure of collagen type I, II, and V. Among the six major different Ehlers-Danlos subtypes, the vascular subtype—together with the vascular-like subtype—are of special interest in the context of aortic disease as these impact Procollagen type III and Procollagen type I, respectively. The clinical and vascular outcome of these subtypes depends on the genotype and phenotype correlations [Citation41].
Non-syndromic hereditary causes of ATAAD include familial thoracic aneurysms and dissections (FTAAD), resembling the aortic manifestations of Marfan syndrome. These are caused by several different mutations in the gene encoding fibrillin-1, with consequential loss of elastic fibres and cystic medial degeneration [Citation38]. The presence of a bicuspid aortic valve (BAV) was reported in 6% of ATAAD cases in the NORCAAD registry [Citation12,Citation42] which is markedly higher than in the normal population (0.5‒1%) [Citation38].
Inflammatory conditions of the aorta, including aortitis and vasculitis, may be associated with degeneration of the medial and adventitial layers of the aortic wall [Citation43]. Both immunoglobulin G4 and complement 4d have been reported to be involved in the pathogenesis of aortic dissection [Citation44,Citation45], whereas giant-cell and Takayasu arteritis are associated with a T-cell-mediated inflammation of the vasa vasori, potentially leading to aneurysm formation and fibrotic stenosis of the aorta [Citation46].
Clinical presentation
Aortic type A dissection is characterized by a sudden, intense chest pain sometimes described as “ripping” or “tearing”; this occurred in 85% of patients in NORCAAD [Citation17]. The pain is usually located retrosternally or substernally, and may propagate in a distal or proximal direction as the dissection evolves. The aortic adventitia is innervated with autonomic afferent nerve fibres, and the intimal tear and disruption of the media results in intense pain of visceral character () [Citation47]. The severity and presentation of symptoms usually leads to immediate contact with healthcare. In rare cases, the dissection presents with less symptoms and is revealed in a subacute phase, or leads to sudden death [Citation17].
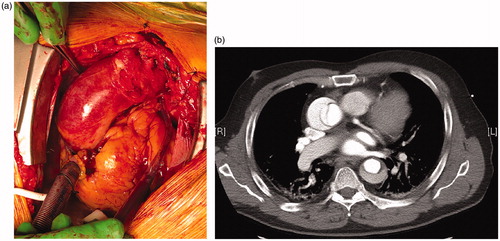
Figure 2. (a) Acute type-A dissection seen intraoperatively with typical appearance where blood can be visualized underneath a thinned out adventitia of the ascending aorta. (b) Preoperative CT scan of the same patient. Photos: Tómas Gudbjartsson.
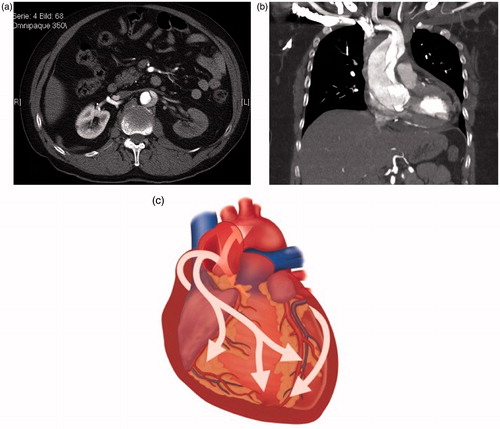
In one-third of the patients, the symptoms are accompanied with malperfusion due to impaired flow in end-organ arteries [Citation48]. Lower-extremity malperfusion and pulse deficit are easily detected clinically, while signs of intestinal and renal ischaemia () may be more difficult to detect in the acute phase. In rare cases, cerebral ischaemia () or paraplegia are the first presenting symptoms of acute aortic dissection [Citation3]. ECG may show signs of cardiac ischaemia or non-specific ST and T-wave alterations, and occasionally coronary flow may be impaired due to coronary ostia dissection [Citation49].
Figure 3. (a) Malperfusion of the kidneys in a patient with ATAAD. The left kidney has delayed enhancement of contrast through the false lumen of the dissection while the right renal artery has normal perfusion from the true lumen. Photo: Tómas Gudbjartsson. (b) Type A dissection stretching from the aortic root and into the brachiocephalic trunk and causing stroke due to carotid malperfusion. The intimal tear is seen with a complex dissection flap which divides the vessels into a true and false lumen. Photo: Arnar Geirsson. (c) The pathology of pericardial tamponade in ATTAD with an intimal tear in the aortic root. Drawing: Hjördís Bjartmarz. Copyright: ©Tomas Gudbjartsson.
Acute chest pain may a lead to the suspicion of acute coronary syndrome, and as the electrocardiogram (ECG) may indicate ischaemia, patients are given anti-thrombotic treatment and transported to coronary intervention units, leading to delay in correct diagnosis and perioperative bleeding complications The characteristic hyperacute onset of chest pain may differentiate aortic dissection from other conditions. In the subacute phase, the symptoms may be related to aortic insufficiency or pericardial effusion in patients with a recent history of chest pain. In more rare instances, aortic dissection may appear as a hemorrhagic pericardial tamponade (), which should lead to the suspicion of aortic dissection (until proven otherwise) [Citation14].
Diagnosis
Prompt diagnosis based on early suspicion of ATAAD is mandatory for successful treatment. Conventional chest X-ray can show a wide mediastinum, which is not specific for diagnosis [Citation27]. The quickest and most accurate method, however, of confirming the diagnosis is CT scanning of the aorta [Citation50]. The aim is to visualize the true and the false lumen of the aorta during dissection, to identify tears of the intima in-between the lumen, and to evaluate the extent of the dissection and the involvement of the branching arteries of the aorta including the arch vessels (). CT also aids in the planning of the surgery and cannulation sites. The sensitivity and specificity of CT are excellent [Citation50], but in patients with poor renal function or allergy to iodinated dye, CT angiography is questionable and other imaging modalities such as magnetic resonance imaging (MRI) or ultrasonography can be considered instead. On the other hand, MRI is seldom used―as it is too time-consuming and still often unavailable, but it may complement CT angiography in follow-up imaging of the aorta [Citation51].
Transthoracic echocardiography (TTE) reveals the functional state of the heart, valves and aortic root, and can show dilatation of the aorta and pericardial effusion and tamponade, but it is associated with poor visibility in the obese, in patients with chest deformities, and in patients on mechanical ventilation [Citation52]. More detailed information is obtained with TEE, especially for detection of pericardial effusion and aortic valve regurgitation, and often identification of the primary intimal tear in the aortic root. In expert hands, TEE is a powerful diagnostic tool, and its sensitivity and specificity approach 100% [Citation52,Citation53]. Coronary angiography is not indicated as a primary diagnostic method for ATAAD, but sometimes it is detected at coronary angiography, when acute coronary syndrome (ACS) is initially suspected. In highly specialized centres, coronary angiography is performed as part of a complete work-up done in a hybrid suite, immediately before open surgery, as up to 30% of ATAAD patients have unknown but significant coronary artery disease that may warrant treatment and affect outcomes [Citation54].
Treatment
Medical treatment
Treatment of ATAAD mainly entails open surgery, but medical treatment, anaesthesia, perioperative care, and interventional procedures all have significant roles in management. In each of these areas, there are new approaches of interest, and ongoing controversy and debate. However, aspects of medical treatment, anaesthesia, and novel endovascular approaches are beyond the scope of this overview.
Based on its dismal natural course, with an estimated overall case-fatality rate of 73% [Citation29] and, in the modern era, an in-hospital mortality rate of 58% in patients presented for but not receiving surgical treatment [Citation27], there is a general consensus that emergency open surgical repair is the standard of care in ATAAD [Citation55].
Pre-hospital death actually occurs in 18‒49% of patients with ATAAD [Citation29,Citation30,Citation32,Citation33] and for those patients who decline surgical treatment or are not offered surgery, optimal medical treatment aims to suppress systolic blood pressure to 110 mmHg, thus reducing stress on the aortic wall [Citation18]. However, mortality in medically treated patients increases by 1% to 2% for every hour after onset of symptoms, reaches 30‒68% within two days, and reaches 49‒73% within the first two weeks [Citation1,Citation21,Citation31,Citation34], thus clearly arguing for surgery being the primary treatment of choice.
Surgical treatment
Clinically, the goal of the operation is to improve the prognosis, i.e. to save the life of the patient. In contemporary reports, the overall early mortality from ATAAD (30-day or in-hospital) in operated patients ranges from 5% to 24% [Citation56–59] and has uniformly been around 17% in current multi-centre studies (German Registry of Acute Aortic Dissection type A, (GERAADA), 17%; International Registry of Aortic Dissection (IRAD), 18%; NORCAAD, 16%) [Citation11,Citation48,Citation49]. Patients who are clinically stable with normal perfusion syndrome generally do well after surgery, with low mortality (of around 3%) [Citation59,Citation60]. In contrast, in patients with unstable haemodynamics or preoperative malperfusion, the mortality is substantial (18‒40%) [Citation7,Citation61].
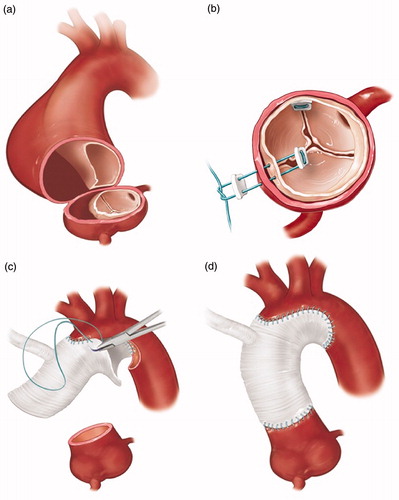
Surgically, the goal of the operation is to resect the primary entry tear of the dissection and re-establish flow in the true lumen of the aorta to avoid or reduce the lethal complications of ATAAD: rupture/tamponade, myocardial ischaemia, cardiac failure related to aortic regurgitation, and life-threatening end-organ malperfusion and ischaemia. This can often be achieved with a supracoronary graft, replacing the dissected ascending aorta ().
Figure 4. Key steps in surgical repair of ATAAD. (a) Resection of the ascending aorta starting proximally at the sinotubular junction. (b) Resuspension of the aortic valve commisures to treat or prevent aortic regurgitation. (c) Open distal anastomosis with hemiarch replacement (with perfusion cannulae omitted for clarity). (d) Completed repair; perfusion through integrated graft side-arm. Drawings: Hjördís Bjartmarz. Copyritght: ©Tomas Gudbjartsson.
Cannulation for cardiopulmonary bypass
Regarding the means of achieving the goal of the surgical management―cannulation for CPB, conduct of cerebral perfusion, proximal and distal extent of the aortic repair―there is no solid evidence and no prevailing strategy, and several opposing concepts are at play. Ideally, arterial cannulation for CPB must bequick, simple, safe, and versatile. For a long time, femoral artery cannulation was the primary choice in ATAAD surgery. Both femoral arteries are accessible and can be cannulated prior to sternotomy, even under local anaesthesia in the haemodynamically deranged patient. On the other hand, the femoral arteries are sometimes arteriosclerotic and frequently dissected. In DeBakey type-I dissections (extending beyond the aortic arch), there is a risk of malperfusion of vital organs including the brain when retrograde flow through the thoraco-abdominal aorta has commenced, depending on the behaviour of the intimal flap [Citation62]. The axillary/subclavian arteries (predominantly on the right) are alternative cannulation sites, are much less prone to arteriosclerosis or dissection, and provide anterograde flow in the aorta―are also suitable to combine with antegrade cerebral perfusion during a period of hypothermic circulatory arrest (HCA) [Citation63,Citation64]. However, these arteries are often less accessible and valuable time can be consumed in this pursuit, especially if the best-documented approach, perfusion through an anastomosed 8 mm graft [Citation65], is used. Alternatively, techniques to directly cannulate the true lumen of the dissected ascending aorta (either epi-aortic ultrasound-guided localization of the true lumen, or by ascending aortic transection) have been proposed and they are associated with acceptable outcomes (0‒15% early mortality, 4‒21% stroke) [Citation66,Citation67], but aortic transection requires temporary exsanguination and cannot be performed before sternotomy. In a recent review and meta-analysis including 715 patients from nine retrospective studies comparing axillary and femoral cannulation, early mortality and neurological dysfunction were lower with axillary cannulation than with femoral cannulation (early mortality: 6.7% vs. 21.6%; neurological dysfunction: 14.3% vs. 26.4%) [Citation68]. Similarly, in a summary of 14 retrospective studies (n = 1829), axillary artery cannulation compared favourably with both central (aortic) and femoral cannulation, with 3‒8.6% early mortality and 1.8‒4% stroke [Citation69]. In larger multi-centre studies, no effect of cannulation sites on early mortality was observed in the GERAADA database (n = 2137): 15.1% vs. 18.8% for axillary vs. femoral cannulation [Citation61]; nor in the NORCAAD (n = 1159): 19.2% vs. 18.9% (unpublished NORCAAD data). Finally, less common approaches to arterial cannulation could be considered as secondary alternatives, if a primary approach fails (due to arterial damage, inadequate vessel dimension, bleeding, malperfusion): innominate or carotid artery, left ventricular apex, or even the right pulmonary vein, as described recently [Citation70].
Hypothermic cardiac arrest and brain protection
Related to the choice of arterial cannulation site is the approach to CPB and management during HCA. Historically, deep HCA (<18 °C to 20 °C) was used for cerebral and organ protection, with an attending high prevalence of neurological dysfunction and stroke, especially when the time period of HCA increased. Retrograde cerebral perfusion (RCP) by means of perfusion through a superior caval vein cannula was introduced as an adjunct to give cerebral protection [Citation71], and favourable outcomes have been reported, from Houston for example: 10% stroke and 30-day mortality of 14% in 489 ATAAD repairs [Citation72,Citation73]. Even so, RCP has largely been displaced by selective antegrade cerebral perfusion (SACP), delivered through direct or in direct cannulation of one, two, or three cervical vessels. Especially when combined with moderate HCA (25‒30 °C), the perceived benefits include physiological (i.e. antegrade) perfusion, reduced pump-time, and reduced coagulopathy. The disadvantages of SACP include increased complexity of perfusion, catheters obscuring the operative field, and―perhaps more importantly―uncertainties regarding optimal perfusate temperature, perfusion flow and pressure, a plethora of techniques and, above all, ambiguous neurological outcomes, with some series reporting very low prevalence of stroke and neurological dysfunction (0‒6%) [Citation74–76] and others, again including GERAADA and NORCAAD, somewhat worse prevalence (12.6‒13.9%) (unpublished NORCAAD data).
Technical aspects of surgical repair
In terms of extent of the surgical repair, the supracoronary graft with aortic valve resuspension is the most prevalent and also the most conservative alternative. When the intimal tear extends into the root, if the aortic root is aneurysmatic, or if there is uncertainty regarding the aortic valve integrity and competence of the aortic valve, the root should be replaced. This can be done as a composite graft (biological or mechanical) or as a valve-sparing aortic root repair (VSARR). Patients with known or suspected connective tissue disease will probably benefit from primary aortic root replacement [Citation74]. Distally, the surgical alternatives are numerous. A simple end-to-end anastomosis to the distal ascending aorta, with or without an aortic cross-clamp in place, is at the conservative extreme. A hemiarch replacement, including the lesser curvature of the arch, would be advocated by most; it is more radical but still comparatively comfortable and safe to perform (. Arch replacement entails reimplantation of one or more cervical vessels. Reimplantation can be performed as a Carrell patch or by individual grafts, or a combination. Arch replacement can be supplemented by an elephant trunk, a 10–15 cm long vascular prosthesis to direct flow preferentially into the true lumen. If the true lumen is compressed, a stent-graft (so called frozen elephant trunk) is preferable. Dedicated combined, hybrid, stent-graft and vascular prostheses are available. In effect, arch replacement of any kind is certainly more challenging and time-consuming.
Indications would include, by analogy with the root, pre-existing aneurysm/dilatation (uncommon), a severely compressed true lumen inducing distal malperfusion, and a primary tear traversing the arch, rendering it prone to rupture and significantly increasing the risk of cervical vessel malperfusion. In practice, arch replacement is only contemplated if deemed absolutely necessary. Use of a frozen elephant trunk may be of particular interest in retrograde ATAAD, with a primary entry downstream of the arch, or when the true lumen is severely compressed with risk of―or manifest―malperfusion to subsequent end-arteries (mesenteric, renal, iliac, etc.). Use of hybrid frozen elephant trunk techniques are recently discussed in detail [Citation77,Citation78], noting an increased prevalence of spinal cord ischemic injury, but also with documented excellent outcomes in dedicated units [Citation79].
An important component of aortic arch operation, even hemiarch replacement, is a period of HCA where the distal anastomosis is performed in so-called “open” fashion, and it is considered by many to be an axiomatic part of ATAAD surgery. HCA and open distal anastomosis allow arch inspection, identification of primary or secondary tears, resection of a clamped aortic wall, accurate suture placement in a more controlled fashion, and also the ability to perform subsequent procedures if necessary. However, it also adds CPB and procedural time with subsequently more disturbed coagulation, and possible cervical vessel manipulation (if ACP is used). A possible exception for the use of HCA would be DeBakey type-II dissections, where the intimal flap does not extend beyond the ascending aorta, and there are no distal re-entries; an aortic cross-clamp can be placed quite distally on the ascending aorta. There is very little evidence that HCA actually improves outcomes in ATAAD repair; as early mortality tends to be similar to that of the strategy of cross-clamped aorta and normothermia [Citation5,Citation11,Citation80–82]. However, in NORCAAD, 153 of 1134 patients (14%) had ATAAD repair without HCA and open distal anastomosis (of which 29% had DeBakey type-II dissection): the early mortality in these patients being worse than with HCA and open distal anastomosis (24% vs. 15%, p = .004), as was their medium-term (5-year) survival (62% vs. 73%, p = .002) [Citation11].
Conservative approaches are being increasingly challenged, and more extensive primary aortic repairs suggested, addressing associated and potential future problems of aortic dilatation (in the root, arch, proximal descending aorta, or entire thoracoabdominal aorta) that may both affect long-term survival and necessitate reinterventions. Reoperations after primary ATAAD repair are not uncommon in long-term survivors, or up to 25‒30% [Citation83,Citation84], and mortality is at a respectable 10‒20% for elective reoperations on the proximal aorta (25‒31% on the distal aorta),but as high as 67% in acute settings [Citation8,Citation83–85].
Surgical treatment of ATAAD cannot be truly evidence-based. The advantages and disadvantages of each permutation of cannulation, perfusion, and surgical repair remain. Often, a conservative approach, using femoral artery cannulation, HCA with any form of cerebral perfusion, and a supracoronary graft replacing the dissected ascending aorta will suffice and provide the safest alternative. Even repair under aortic cross-clamp cannot be rejected outright, based on the data available. Still, unique patient and dissection characteristics must be recognized and, if necessary, influence strategy. If a risk of malperfusion through the femoral artery is envisioned or detected, an alternative arterial cannulation site should be chosen. Younger patients, or patients with connective tissue disease, may benefit most from valve-sparing aortic root repair (which, notably, can be undertaken during rewarming and may not necessarily prolong CPB time or procedural time). Arch inspection during HCA may reveal a longitudinal tear motivating arch replacement, in turn an impetus for meticulous cerebral perfusion and protection, allowing ample time for repair. Thus, optimal management of a wide spectrum of ATAAD patients requires surgical adaptation and versatility, which is provided more and more often in dedicated aortic centres and is often associated with documented improvement in outcomes [Citation86].
Demographical and geographical conditions to some extent dictate ATAAD management in the Nordic area. Surgical treatment is offered at tertial centers exclusively, making time-consuming transportation necessary in a proportion of cases. Patient selection will entail: some patients die during this interval, creating a positive selection bias. On the other hand, and likely more commonly, patients may arrive at the operating center in a more deranged condition due to relatively prolonged periods of malperfusion, ischemia, tamponade, or suboptimal hemodynamic control. While catchment areas are large, catchment populations are often limited in the Nordic countries. In effect, relatively few advanced root and arch repairs are performed electively, which will, and should, influence surgical strategy in ATAAD as well and forms the background for a generally conservative approach.
Complications
The most common complications following ATTAD repair are shown in . The disturbances of the coagulation system in combination with the poor quality of the dissected aorta contribute to 25% of patients having massive bleeding associated with ATAAD surgery [Citation10,Citation87]. In several studies, bleeding has been identified as an independent predictor of early and late mortality after surgery for ATAAD and accounts for 20% of in-hospital deaths [Citation6,Citation10,Citation88]. The bleeding can also extend into the pericardium and cause tamponade that can aggrevate cardiac and hypovolemic shock (. When blood surges through the intimal tear, it is exposed to the subendothelial tissue of the false lumen. The contact between blood and tissue factor causes a coagulopathy resembling disseminated intravascular coagulation, with consumption of coagulation factors and increased fibrinolysis [Citation89]. Furthermore, there is an activation and consumption of platelets, the latter of which has been shown to be associated with increased mortality [Citation73,Citation90]. In addition, the use of CPB has deleterious effects on the coagulation system and platelet function. This is further enhanced by routine use of hypothermia during surgery, which causes alterations in the coagulation system and results in splenic sequestration of platelets and increased platelet activation and aggregation [Citation91–95].
Table 2. Postoperative complications following ATAAD repair as reported from the NORCAAD registry.
In a recent report from the NORCAAD registry, preoperative cardiac malperfusion was found to be associated with the highest rates of 30-day mortality (33%) [Citation7]. This was primarily driven by intraoperative deaths, possibly due to myocardial infarction and the inability to wean the patients off CPB. However, of the patients who survived surgery, only 7% suffered a perioperative myocardial infarction (MI) [Citation7]. Di Eusanio et al. reported that preoperative mesenteric malperfusion was associated with a mortality rate of 63.2% [Citation96], while data from the NORCAAD registry showed a mortality rate of 31% in patients with gastrointestinal malperfusion [Citation7]. Di Eusanio et al. also reported 95% hospital mortality in medically treated patients with mesenteric malperfusion [Citation91], so the recent data from NORCAAD strongly suggest that patients with gastrointestinal malperfusion should not be denied surgery.
In the large multi-centre registries such as IRAD, GERAADA, and NORCAAD, postoperative stroke and coma occurred in 10‒15% and 3‒9% of the patients, respectively [Citation7,Citation96–98]. Stroke is one of the leading causes of death after ATAAD surgery [Citation25,Citation88], where the mechanism of brain injury is heterogeneous. Data from the NORCAAD registry show that preoperative cerebral malperfusion () is associated with a threefold increase in stroke rates when compared to patients with other sites of malperfusion. However, rates of coma do not follow a similar pattern, suggesting different injury mechanisms [Citation7]. Several intraoperative risk factors for perioperative stroke have been identified, including prolonged duration of CPB and HCA [Citation97,Citation98]. It has also been hypothesized that femoral cannulation would cause retrograde embolization but to date, no evidence has been presented that cannulation strategy has any effect on postoperative stroke rates [Citation97–99].
Acute kidney injury (AKI) is a common complication following ATAAD, and previous studies have found that AKI ranges between 40% and 55% [Citation100]. shows how ATAAD causes impaired flow to the kidneys and renal malperfusion. In the NORCAAD registry, 5.5% of patients presented with renal malperfusion and postoperatively 11% of all the patients required renal replacement therapy (RRT) [Citation7]. Also in the NORCAAD registry, a rate of postoperative AKI of 41% was found using the RIFLE criteria (unpublished NORCAAD data). Age, BMI >30 kg/m2, hypertension, DeBakey type-I dissections, prolonged CPB time, and red blood cell transfusions were all found to be independent risk factors for AKI and it was associated with poorer 30-day and long-term survival (unpublished NORCAAD data).
A NORCAAD report from Pan et al. recently showed freedom from reoperation rates of 98% at one year and 95% at five years [Citation8]. Other studies have shown freedom from reoperation of 82‒94% at five years [Citation85,Citation101,Citation102]. However, Wang et al. found that patients with connective tissue disease had a 45% risk of reoperation at a median follow-up time of 2.5 years and Pan et al. found that patients with connective tissue disease had a five times higher risk of proximal reoperation [Citation8,Citation103]. This possibly indicates that a more aggressive primary approach may be feasible in patients with hereditary conditions.
Outcome and long-term follow-up
In ATAAD patients, aortic rupture with massive bleeding leading to cardiac tamponade and/or exsanguination is the most common cause of mortality before the patient reaches hospital [Citation104,Citation105]. For those who reach hospital alive, important prognostic factors for 30-day and late mortality are shown in . These include advanced age [Citation49], cerebrovascular injury [Citation24,Citation86], malperfusion [Citation6,Citation24,Citation94], acute kidney injury (AKI) [Citation106–108], preoperative tamponade or shock [Citation109] (unpublished NORCAAD data), and also surgical factors such as cannulation site, duration of the operation, CPB time, and extent of surgery. The existing literature often implicates the aforementioned non-surgical characteristics as prognostic factors for late mortality, but on the other hand age and the comorbidity burden of the patients (mainly atherosclerosis) is also important for long-term survival in contemporary single-centre and multi-centre series. Long-term postoperative survival after ATAAD repair is satisfactory and has improved in recent years: 84‒85% at 5 years [Citation9,Citation62,Citation109,Citation110], 64‒68% at 10 years [Citation31,Citation109,Citation111,Citation8], and up to 38% at 30 years [Citation110].
Table 3. Major predictors of 30-day and long-term mortality in ATAAD patients.
Postoperative health-related quality of life (HRQoL) in operated ATAAD patients has been reported to be significantly lower than in the general population [Citation112–114]. Furthermore, HRQoL has been shown to decline over time [Citation112] and there is a 32% incidence of ATAAD patients suffering from episodes of depression; up to 32% are at risk of post-traumatic stress disorder and ATAAD patients have reported that they have reduced sexual activity [Citation115]. Clearly, patients who have undergone surgery for ATAAD have an increased risk of psychiatric morbidity, and screening for psychiatric disease and factors related to poor HRQoL may therefore be considered.
Postoperative follow-up by means of CT and TTE is essential and is aimed at detecting rapid or persistent aortic enlargement or, when the native valve has not been replaced, increased aortic regurgitation. Over 50% of operated ATAAD patients have resistant hypertension on follow-up [Citation116], so clinical follow-up is necessary in order to maintain adequate control of blood pressure.
Intervals for scheduled imaging after ATAAD have been described both in the EACTS/ESC 2014 guidelines and in the AHA/ACC 2010 guidelines [Citation56,Citation117]. In the case of a treated ATAAD, with or without persistent residual dissection, a follow-up CT of the aorta is recommended at 1 month (additionally at 3 months in the American guideliness), 6, and 12 months and annually thereafter [Citation56,Citation117]. The European guidelines state that with stable disease, imaging every two years after the first control after one year should suffice. However, it should be noted that the recommendations for ATAAD are extrapolated from data on the natural course of type-B dissections, and arguably the residual dissection after a type A dissection should be considered to be a different entity. This is reflected by the guidelines stating that data on optimal surveillance schedules for ATAAD specifically are not available [Citation56,Citation117].
After valve-sparing surgery for acute dissection, aortic regurgitation at follow-up is almost exclusively associated with root dilatation, but the 5-year rates of moderate or greater aortic valve regurgitation or regurgitation as indication for reoperation have been reported to be below 5% in most series, including the NORCAAD registry [Citation8,Citation118–120]. To date, there are no recommendations specific for aortic insufficiency following ATAAD, but it seems reasonable to conform to general guidelines on aortic regurgitation with echocardiographic follow-up every 1‒2 years for mild regurgitation and every year for moderate and asymptomatic severe regurgitation [Citation121].
Conclusion
Type-A aortic dissection (ATAAD) is a highly deadly cardiovascular emergency. Acute surgical treatment is indicated for all patients, except for those who are moribund or severely comorbid. Surgical and perioperative procedures vary depending on the presentation and aortic pathology. Despite the considerable morbidity and mortality, both early and medium-term outcomes are improving. Current multi-centre data from NORCAAD demonstrate that ATAAD-related short- and medium-term survival, the highest surgical priority, is improving and that late re-interventions are uncommon. Conservative yet contemporary surgical approaches (conserving the native root and aortic valve, and performing the distal anastomosis as a hemiarch replacement under a period of HCA with cerebral perfusion) are applicable in the majority of cases and may reduce morbidity, which, however, remains substantial. In selected patients, individualized approaches to perfusion and surgical repair are necessary to treat or avoid severe complications. Future efforts will focus on patient selection, improved perioperative management, and reduction of complications, but also on true long-term follow-up and identification of patients who are at particular risk of ATAAD, such as patients with aortic aneurysms due to connective tissue diseases—to treat them with prophylactic elective operation with considerably lower risks.
Disclosure statement
No potential conflict of interest was reported by the authors.
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
References
- Jassar AS, Sundt TM, III. How should we manage type A aortic dissection? Gen Thorac Cardiovasc Surg. 2019:67(1):137–145.
- Goldfinger JZ, Halperin JL, Marin ML, et al. Thoracic aortic aneurysm and dissection. J Am Coll Cardiol. 2014;64(16):1725–1739.
- Nienaber CA, Clough RE. Management of acute aortic dissection. Lancet 2015;385(9970):800–811.
- Geirsson A, Ahlsson A, Franco-Cereceda A. The Nordic Consortium for Acute type A Aortic Dissection (NORCAAD): objectives and design. Scand Cardiovasc J. 2016;50:1–7.
- Myrmel T, Lai DT, Miller DC. Can the principles of evidence-based medicine be applied to the treatment of aortic dissections? Eur J Cardiothorac Surg. 2004;25(2):236–242.
- Zindovic I, Sjogren J, Ahlsson A, et al. Recombinant factor VIIa use in acute type A aortic dissection repair: a multicenter propensity-score-matched report from the Nordic Consortium for Acute Type A Aortic Dissection. J Thorac Cardiovasc Surg. 2017;154(6):1852e2–1859e2.
- Zindovic I, Gudbjartsson T, Ahlsson A, et al. Malperfusion in acute type A aortic dissection: an update from the Nordic Consortium for Acute Type A Aortic Dissection. J Thorac Cardiovasc Surg. 2019;157:1324.e6–1336.e6.
- Pan E, Gudbjartsson T, Ahlsson A, et al. Low rate of reoperations after acute type A aortic dissection repair from The Nordic Consortium Registry. J Thorac Cardiovasc Surg. 2018;156(3):939–948.
- Olsson C, Ahlsson A, Fuglsang S, et al. Medium-term survival after surgery for acute Type A aortic dissection is improving. Eur J Cardiothorac Surg. 2017;52(5):852–857.
- Hansson EC, Geirsson A, Hjortdal V, et al. Preoperative dual antiplatelet therapy increases bleeding and transfusions but not mortality in acute aortic dissection type A repair. Eur J Cardiothorac Surg. 2019;56(1):182–188.
- Geirsson A, Shioda K, Olsson C, et al. Differential outcomes of open and clamp-on distal anastomosis techniques in acute type A aortic dissection. J Thorac Cardiovasc Surg. 2019;157:1750–1750.
- Geirsson A, Ahlsson A, Franco-Cereceda A, et al. The Nordic Consortium for Acute type A Aortic Dissection (NORCAAD): objectives and design. Scand Cardiovasc J. 2016;50(5–6):334–340.
- Geirsson A, Ahlsson A, Franco-Cereceda A, et al. Hospital volumes and later year of operation correlates with better outcomes in acute Type A aortic dissection. Eur J Cardiothorac Surg. 2018;53(1):276–281.
- Gawinecka J, Schonrath F, von Eckardstein A. Acute aortic dissection: pathogenesis, risk factors and diagnosis. Swiss Med Wkly. 2017;147:w14489.
- Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management: Part II: therapeutic management and follow-up. Circulation 2003;108(6):772–778.
- Mussa FF, Horton JD, Moridzadeh R, et al. Acute aortic dissection and intramural haematoma: a systematic review. JAMA 2016;316(7):754–763.
- Elsayed RS, Cohen RG, Fleischman F, et al. Acute type A aortic dissection. Cardiol Clin. 2017;35(3):331–345.
- Nienaber CA, Eagle KA. Aortic dissection: new frontiers in diagnosis and management: Part I: from etiology to diagnostic strategies. Circulation 2003;108(5):628–635.
- Rylski B, Beyersdorf F, Kari FA, et al. Acute type A aortic dissection extending beyond ascending aorta: limited or extensive distal repair. J Thorac Cardiovasc Surg. 2014;148(3):949–954.
- Erbel R, Alfonso F, Boileau C, et al. Diagnosis and management of aortic dissection. Eur Heart J. 2001;22(18):1642–1681.
- Hirst AE, Jr., Johns VJ, Jr., Kime SW, Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine (Baltimore) 1958;37(3):217–279.
- Rylski B, Milewski RK, Bavaria JE, et al. Outcomes of surgery for chronic type A aortic dissection. Ann Thorac Surg. 2015;99(1):88–93.
- DeBakey ME, McCollum CH, Crawford ES, et al. Dissection and dissecting aneurysms of the aorta: twenty-year follow-up of five hundred twenty-seven patients treated surgically. Surgery. 1982;92(6):1118–1134.
- Augoustides JG, Szeto WY, Desai ND, et al. Classification of acute type A dissection: focus on clinical presentation and extent. Eur J Cardiothorac Surg. 2011;39(4):519–522.
- Olsson C, Hillebrant CG, Liska J, et al. Mortality in acute type A aortic dissection: validation of the Penn classification. Ann Thorac Surg. 2011;92(4):1376–1382.
- Pisano C, Balistreri CR, Torretta F, et al. Penn classification in acute aortic dissection patients. Acta Cardiol. 2016;71(2):235–240.
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283(7):897–903.
- Landenhed M, Engstrom G, Gottsater A, et al. Risk profiles for aortic dissection and ruptured or surgically treated aneurysms: a prospective cohort study. J Am Heart Assoc. 2015;4(1):e001513.
- Howard DP, Banerjee A, Fairhead JF, et al. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation 2013;127(20):2031–2037.
- Melvinsdottir IH, Lund SH, Agnarsson BA, et al. The incidence and mortality of acute thoracic aortic dissection: results from a whole nation study. Eur J Cardiothorac Surg. 2016;50(6):1111–1117.
- Meszaros I, Morocz J, Szlavi J, et al. Epidemiology and clinicopathology of aortic dissection. Chest. 2000;117:1271–1278.
- Olsson C, Thelin S, StåHle E, et al. Thoracic aortic aneurysm and dissection: increasing prevalence and improved outcomes reported in a nationwide population-based study of more than 14,000 cases from 1987 to 2002. Circulation. 2006;114(24):2611–2618.
- Rylski B, Hoffmann I, Beyersdorf F, et al. Acute aortic dissection type A: age-related management and outcomes reported in the German Registry for Acute Aortic Dissection Type A (GERAADA) of over 2000 patients. Ann Surg. 2014;259(3):598–604.
- Trimarchi S, Eagle KA, Nienaber CA, et al. Role of age in acute type A aortic dissection outcome: Report from the International Registry of Acute Aortic Dissection (IRAD). J Thorac Cardiovasc Surg. 2010;140(4):784–789.
- Boening A, Karck M, Conzelmann LO, et al. German Registry for Acute Aortic Dissection Type A: structure, results, and future perspectives. Thorac Cardiovasc Surg. 2017;65(2):77–84.
- Kinney-Ham L, Nguyen HB, Steele R, et al. Acute aortic dissection in third trimester pregnancy without risk factors. WestJEM 2011;12(4):571–574.
- Albornoz G, Coady MA, Roberts M, et al. Familial thoracic aortic aneurysms and dissections-incidence, modes of inheritance, and phenotypic patterns. Ann Thorac Surg. 2006;82(4):1400–1405.
- Isselbacher EM, Lino Cardenas CL, Lindsay ME. Hereditary influence in thoracic aortic aneurysm and dissection. Circulation. 2016;133(24):2516–2528.
- Vapnik JS, Kim JB, Isselbacher EM, et al. Characteristics and outcomes of ascending versus descending thoracic aortic aneurysms. Am J Cardiol. 2016;117(10):1683–1690.
- Zindovic I, Sjögren J, Bjursten H, et al. The coagulopathy of acute type A aortic dissection: A prospective, Observational Study. J Cardiothorac Vasc Anesth. 2019;33(10):2746–2754.
- Malfait F, Paepe A. 2014. The Ehlers-Danlos syndrome. In: Halper J, editor. Progress in heritable soft connective tissue diseases advances in experimental medicine and biology. Dordrecht: Springer.
- Mennander A, Olsson C, Jeppsson A, et al. The significance of bicuspid aortic valve after surgery for acute type A aortic dissection. J Thorac Cardiovasc Surg. 2019:pii: S0022-5223(19)30680-4.
- Stone JR, Bruneval P, Angelini A, et al. Consensus statement on surgical pathology of the aorta from the Society for Cardiovascular Pathology and the Association for European Cardiovascular Pathology: I. Inflammatory diseases. Cardiovasc Pathol. 2015;24(5):267–278.
- Kajander H, Paavonen T, Valo T, et al. Immunoglobulin G4-positive ascending thoracic aortitis may be prone to dissection. J Thorac Cardiovasc Surg. 2013;146(6):1449–1455.
- Niinimaki E, Paavonen T, Valo T, et al. Lack of C4d deposition may reveal susceptibility for ascending aortic dissection. Scand Cardiovasc J. 2012;46(3):177–182.
- Kermani TA. Takayasu arteritis and giant cell arteritis: are they a spectrum of the same disease? Int J Rheum Dis. 2019;Suppl 1: 41–48.
- Berthoud HR, Neuhuber WL. Functional and chemical anatomy of the afferent vagal system. Auton Neurosci. 2000;85(1–3):1–17.
- Czerny M, Schoenhoff F, Etz C, et al. The impact of pre-operative malperfusion on outcome in acute type A aortic dissection: results from the GERAADA Registry. J Am Coll Cardiol. 2015;65(24):2628–2635.
- Evangelista A, Isselbacher EM, Bossone E, et al. Insights from the International Registry of Acute Aortic Dissection: a 20-year experience of collaborative clinical research. Circulation. 2018;137(17):1846–1860.
- Rogers IS, Banerji D, Siegel EL, et al. Usefulness of comprehensive cardiothoracic computed tomography in the evaluation of acute undifferentiated chest discomfort in the emergency department (CAPTURE). Am J Cardiol. 2011;107(5):643–650.
- Wang GX, Hedgire SS, Le TQ, et al. MR angiography can guide ED management of suspected acute aortic dissection. Am J Emerg Med. 2017;35(4):527–530.
- Meredith EL, Masani ND. Echocardiography in the emergency assessment of acute aortic syndromes. Eur J Echocardiogr. 2009;10(1):i31–i39.
- Shiga T, Wajima Z, Inoue T, et al. Survey of observer variation in transesophageal echocardiography: comparison of anesthesiology and cardiology literature. J Cardiothorac Vasc Anesth. 2003;17(4):430–442.
- Tsagakis K, Konorza T, Dohle DS, et al. Hybrid operating room concept for combined diagnostics, intervention and surgery in acute type A dissection. Eur J Cardiothorac Surg. 2013;43(2):397–404.
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(41):2873–2926.
- Arsalan M, Squiers JJ, Herbert MA, et al. Comparison of outcomes of operative therapy for acute type A aortic dissections provided at high-volume versus low-volume medical centers in North Texas. Am J Cardiol. 2017;119(2):323–327.
- Hawkins RB, Mehaffey JH, Downs EA, et al. Regional practice patterns and outcomes of surgery for acute type A aortic dissection. Ann Thorac Surg. 2017;104(4):1275–1281.
- Nishida H, Tabata M, Fukui T, et al. A systematic approach to improve the outcomes of type A aortic dissection. J Thorac Cardiovasc Surg. 2017;154(1):89e1–96e1.
- Uchida K, Karube N, Kasama K, et al. Early reperfusion strategy improves the outcomes of surgery for type A acute aortic dissection with malperfusion. J Thorac Cardiovasc Surg. 2018;156(2):483–489.
- Augoustides JG, Geirsson A, Szeto WY, et al. Observational study of mortality risk stratification by ischemic presentation in patients with acute type A aortic dissection: the Penn classification. Nat Rev Cardiol. 2009;6(2):140–146.
- Conzelmann LO, Weigang E, Mehlhorn U, et al. Mortality in patients with acute aortic dissection type A: analysis of pre- and intraoperative risk factors from the German Registry for Acute Aortic Dissection Type A (GERAADA). Eur J Cardiothorac Surg. 2016;49(2):e44–e52.
- Van Arsdell GS, David TE, Butany J. Autopsies in acute type A aortic dissection. Surgical implications. Circulation 1998;98(19 Suppl):II299–II302.
- Leshnower BG, Thourani VH, Halkos ME, et al. Moderate versus deep hypothermia with unilateral selective antegrade cerebral perfusion for acute type A dissection. Ann Thorac Surg. 2015;100(5):1563–1568.
- Strauch JT, Spielvogel D, Lauten A, et al. Axillary artery cannulation: routine use in ascending aorta and aortic arch replacement. Ann Thorac Surg. 2004;78(1):103–108
- Sabik JF, Nemeh H, Lytle BW, et al. Cannulation of the axillary artery with a side graft reduces morbidity. Ann Thorac Surg. 2004;77(4):1315–1320.
- Conzelmann LO, Kayhan N, Mehlhorn U, et al. Reevaluation of direct true lumen cannulation in surgery for acute type A aortic dissection. Ann Thorac Surg. 2009;87(4):1182–1186.
- Khaladj N, Shrestha M, Peterss S, et al. Ascending aortic cannulation in acute aortic dissection type A: the Hannover experience. Eur J Cardiothorac Surg 2008;34(4):792–796; disussion 6.
- Ren Z, Wang Z, Hu R, et al. Which cannulation (axillary cannulation or femoral cannulation) is better for acute type A aortic dissection repair? A meta-analysis of nine clinical studies. Eur J Cardiothorac Surg. 2015;47(3):408–415.
- Tiwari KK, Murzi M, Bevilacqua S, et al. Which cannulation (ascending aortic cannulation or peripheral arterial cannulation) is better for acute type A aortic dissection surgery? Interact Cardiovasc Thorac Surg. 2010;10(5):797–802.
- Schoeneich F, Rahimi-Barfeh A, Grothusen C, et al. Transatrial left-ventricular cannulation in acute aortic dissection type A: a novel cannulation technique. Eur J Cardiothorac Surg. 2015;48(3):e51–e52.
- Ueda Y, Miki S, Kusuhara K, et al. Surgical treatment of aneurysm or dissection involving the ascending aorta and aortic arch, utilizing circulatory arrest and retrograde cerebral perfusion. J Cardiovasc Surg (Torino). 1990;31(5):553–558.
- Rice RD, Sandhu HK, Leake SS, et al. Is total arch replacement associated with worse outcomes during repair of acute type A aortic dissection? Ann Thorac Surg. 2015;100(6):2159–2165.
- Tian DH, Weller J, Hasmat S, et al. Adjunct retrograde cerebral perfusion provides superior outcomes compared with hypothermic circulatory arrest alone: a meta-analysis. J Thorac Cardiovasc Surg. 2018;156(4):1339e7–1348e7.
- Burgstaller JM, Held U, Mosbahi S, et al. A systemic review and meta-analysis: long-term results of the Bentall versus the David procedure in patients with Marfan syndrome. Eur J Cardiothorac Surg. 2018;54(3):411–419.
- Panos A, Murith N, Bednarkiewicz M, et al. Axillary cerebral perfusion for arch surgery in acute type A dissection under moderate hypothermia. Eur J Cardiothorac Surg. 2006;29(6):1036–1039.
- Zierer A, El-Sayed Ahmad A, Papadopoulos N, et al. Fifteen years of surgery for acute type A aortic dissection in moderate-to-mild systemic hypothermia. Eur J Cardiothorac Surg. 2017;51(1):97–103.
- Czerny M, Schmidli J, Adler S, et al. Current options and recommendations for the treatment of thoracic aortic pathologies involving the aortic arch: an expert consensus document of the European Association for Cardio-Thoracic surgery (EACTS) and the European Society for Vascular Surgery (ESVS). Eur J Cardiothorac Surg. 2019;55(1):133–162.
- Shrestha M, Bachet J, Bavaria J, et al. Current status and recommendations for use of the frozen elephant trunk technique: a position paper by the Vascular Domain of EACTS. Eur J Cardiothorac Surg. 2015;47(5):759–769.
- Shrestha M, Haverich A, Martens A. Total aortic arch replacement with the frozen elephant trunk procedure in acute DeBakey type I aortic dissections. Eur J Cardiothorac Surg. 2017;51(Suppl 1):i29–i34.
- Danner BC, Natour E, Horst M, et al. Comparison of operative techniques in acute type A aortic dissection performing the distal anastomosis. J Cardiac Surgery 2007;22(2):105–110.
- Kruger T, Weigang E, Hoffmann I, et al. Cerebral protection during surgery for acute aortic dissection type A: results of the German Registry for Acute Aortic Dissection Type A (GERAADA). Circulation. 2011;124:434–443.
- Lai DT, Robbins RC, Mitchell RS, et al. Does profound hypothermic circulatory arrest improve survival in patients with acute type A aortic dissection? Circulation. 2002;106(12 Suppl 1):I218–I228.
- Bachet JE, Termignon JL, Dreyfus G, et al. Aortic dissection. Prevalence, cause, and results of late reoperations. J Thorac Cardiovasc Surg. 1994;108(2):199–205.
- Geirsson A, Bavaria JE, Swarr D, et al. Fate of the residual distal and proximal aorta after acute type a dissection repair using a contemporary surgical reconstruction algorithm. Ann Thorac Surg. 2007;84(6):1955–1964.
- Dell'Aquila AM, Pollari F, Fattouch K, et al. Early outcomes in re-do operation after acute type A aortic dissection: results from the multicenter REAAD database. Heart Vessels 2017;32:566–573.
- Andersen ND, Ganapathi AM, Hanna JM, et al. Outcomes of acute type a dissection repair before and after implementation of a multidisciplinary thoracic aortic surgery program. J Am Coll Cardiol. 2014;63(17):1796–1803.
- Zindovic I, Sjogren J, Bjursten H, et al. Predictors and impact of massive bleeding in acute type A aortic dissection. Interact Cardiovasc Thorac Surg. 2017;24(4):498–505.
- Zindovic I, Sjogren J, Bjursten H, et al. Impact of hemodynamic instability and organ malperfusion in elderly surgical patients treated for acute type A aortic dissection. J Card Surg. 2015;30(11):822.
- Cate JW, Timmers H, Becker AE. Coagulopathy in ruptured or dissecting aortic aneurysms. Am J Med. 1975;59(2):171–176.
- Huang B, Tian L, Fan X, et al. Low admission platelet counts predicts increased risk of in-hospital mortality in patients with type A acute aortic dissection. Int J Cardiol. 2014;172(3):e484–e486.
- Gelb AB, Roth RI, Levin J, et al. Changes in blood coagulation during and following cardiopulmonary bypass: lack of correlation with clinical bleeding. Am J Clin Pathol. 1996;106(1):87–99.
- Linden MD. The hemostatic defect of cardiopulmonary bypass. J Thromb Thrombolysis. . 2003;16(3):129–147.
- Martini WZ. The effects of hypothermia on fibrinogen metabolism and coagulation function in swine. Metab Clin Exp. 2007;56(2):214–221.
- Martini WZ. Coagulopathy by hypothermia and acidosis: mechanisms of thrombin generation and fibrinogen availability. J Trauma 2009;67(1):202–208.
- Van Poucke S, Stevens K, Marcus AE, et al. Hypothermia: effects on platelet function and hemostasis. Thromb J. 2014;12(1):31.
- Di Eusanio M, Patel HJ, Nienaber CA, et al. Patients with type A acute aortic dissection presenting with major brain injury: should we operate on them? J Thorac Cardiovasc Surg. 2013;145(3):S213e1–S221e1.
- Buonocore M, Amarelli C, Scardone M, et al. Cerebral perfusion issues in acute type A aortic dissection without preoperative malperfusion: how do surgical factors affect outcomes? Eur J Cardiothorac Surg. 2016;50(4):652–659.
- Conzelmann LO, Hoffmann I, Blettner M, et al. Analysis of risk factors for neurological dysfunction in patients with acute aortic dissection type A: data from the German Registry for Acute Aortic Dissection type A (GERAADA). Eur J Cardiothorac Surg. 2012;42(3):557–565.
- Geirsson A, Szeto WY, Pochettino A, et al. Significance of malperfusion syndromes prior to contemporary surgical repair for acute type A dissection: outcomes and need for additional revascularizations. Eur J Cardiothorac Surg. 2007;32(2):255–262.
- Wang J, Yu W, Zhai G, et al. Independent risk factors for postoperative AKI and the impact of the AKI on 30-day postoperative outcomes in patients with type A acute aortic dissection: an updated meta-analysis and meta-regression. J Thorac Dis. 2018;10(5):2590–2598.
- Concistre G, Casali G, Santaniello E, et al. Reoperation after surgical correction of acute type A aortic dissection: risk factor analysis. Ann Thorac Surg. 2012;93(2):450–455.
- Pugliese P, Pessotto R, Santini F, et al. Risk of late reoperations in patients with acute type A aortic dissection: impact of a more radical surgical approach. Eur J Cardiothorac Surg. 1998;13(5):576–580.
- Wang H, Wagner M, Benrashid E, et al. Outcomes of reoperation after acute type A aortic dissection: implications for index repair strategy. J Am Heart Assoc. 2017;6:pii:e006376.
- Li Y, Li L, Mu HS, et al. Aortic dissection and sudden unexpected deaths: a retrospective study of 31 forensic autopsy cases. J Forensic Sci. 2015;60(5):1206–1211.
- Pierce LC, Courtney DM. Clinical characteristics of aortic aneurysm and dissection as a cause of sudden death in outpatients. Am J Emerg Med. 2008;26(9):1042–1046.
- Ko T, Higashitani M, Sato A, et al. Impact of acute kidney injury on early to long-term outcomes in patients who underwent surgery for type A acute aortic dissection. Am J Cardiol. 2015;116(3):463–468.
- Mehta RH, O'Gara PT, Bossone E, et al. Acute type A aortic dissection in the elderly: clinical characteristics, management, and outcomes in the current era. J Am Coll Cardiol. 2002;40(4):685–692.
- Tsai TT, Trimarchi S, Nienaber CA. Acute aortic dissection: perspectives from the International Registry of Acute Aortic Dissection (IRAD). Eur J Vasc Endovasc Surg. 2009;37(2):149–159.
- Bekkers JA, Raap GB, Takkenberg JJ, et al. Acute type A aortic dissection: long-term results and reoperations. Eur J Cardiothorac Surg. 2013;43(2):389–396.
- Pan E, Kyto V, Savunen T, et al. Early and late outcomes after open ascending aortic surgery: 47-year experience in a single centre. Heart Vessels 2018;33(4):427–433.
- Ehrlich MP, Ergin MA, McCullough JN, et al. Results of immediate surgical treatment of all acute type A dissections. Circulation 2000;102(19 Suppl 3):III248–III252.
- Endlich M, Hamiko M, Gestrich C, et al. Long-term outcome and quality of life in aortic type A dissection survivors. Thorac Cardiovasc Surg. 2016;64:91–99.
- Ghazy T, Eraqi M, Mahlmann A, et al. Quality of life after surgery for Stanford type A aortic dissection: influences of different operative strategies. Heart Surg Forum. 2017;20(3):102E6–1E6.
- Jussli-Melchers J, Panholzer B, Friedrich C, et al. Mid- and long-term outcomes of total arterial myocardial revascularization in patients aged 70 years and older: a single-center experience. Thorac Cardiovasc Surg. 2018.
- Chaddha A, Kline-Rogers E, Braverman AC, et al. Survivors of aortic dissection: activity, mental health, and sexual function. Clin Cardiol. 2015;38(11):652–659.
- Eggebrecht H, Schmermund A, von Birgelen C, et al. Resistant hypertension in patients with chronic aortic dissection. J Hum Hypertens. 2005;19(3):227–231.
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27–e129.
- Rosenblum JM, Leshnower BG, Moon RC, et al. Durability and safety of David V valve-sparing root replacement in acute type A aortic dissection. J Thorac Cardiovasc Surg. 2019;157(1):14.e1–23.e1.
- Rylski B, Hahn N, Beyersdorf F, et al. Fate of the dissected aortic arch after ascending replacement in type A aortic dissection. Eur J Cardiothorac Surg. 2017;51(6):1127–1134.
- Tanaka H, Ikeno Y, Abe N, et al. Outcomes of valve-sparing root replacement in acute Type A aortic dissection. Eur J Cardiothorac Surg. 2018;53(5):1021–1026.
- Baumgartner H, Falk V, Bax JJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739–2791.