
Abstract
We describe a 67-year-old man with immunoglobulin G4-related disease (IgG4-RD) presenting with optic neuropathy, dacryoadenitis, periaortitis, retroperitoneal fibrosis, and a gastric mass-like lesion. A mass-like lesion measuring 52 × 40 mm in the antrum of the stomach was found incidentally through whole-body screening for other organ involvement of IgG4-RD using contrast-enhanced computed tomography (CT). Histology of the stomach revealed that the lesion was also IgG4-related and was located in the submucosal layer extending to the subserosal region. This case suggests that the stomach can also be a site of involvement of IgG4-RD.
Introduction
IgG4-related disease (IgG4-RD) is a relatively newly established disease entity that involves various organs, such as lacrimal glands, submandibular glands [Citation1], lung [Citation2], pancreas [Citation3], bile duct [Citation4], kidney [Citation5], aorta/artery [Citation6], nervous system [Citation7], and retroperitoneum [Citation8] simultaneously or metachronously [Citation9–11]. IgG4-RD is clinically characterized by a predilection for elderly males, serum IgG4 elevation, and a favorable response to steroid therapy [Citation11]. Pathological features of IgG4-RD include diffuse lymphoplasmacytic infiltration, storiform fibrosis and obliterative phlebitis, and numerous IgG4-positive plasma cells on immunostaining [Citation12].
It is important to diagnose IgG4-RD correctly and promptly because of the good response to early steroid therapy. Diagnosis of IgG4-RD requires a multidisciplinary approach including various clinical, radiological, and pathological examinations. Radiological findings of major manifestations in various organs, including pancreas, lung, kidney, and aorta/artery, have been published, and radiological examinations and determination of serum IgG4 concentrations are the key steps to achieving the correct diagnosis of IgG4-RD [Citation2,Citation7,Citation13–18]. Although IgG4-RD mainly involves glandular tissues or the vascular system, several case reports have shown that IgG4-RD also involves the gastrointestinal tract with ulcer, polypoid lesions, submucosal mass, and wall thickening. However, because of the small number of reports on the gastrointestinal lesions of IgG4-RD, their entire spectrum has not yet been adequately documented, and especially, the radiological aspects of many of these lesions are still obscure [Citation19–28]. Here, we report the detailed imaging findings in a case of IgG4-RD with gastric involvement.
Case
A 67-year-old man with a history of hypertension and cystoscopic surgery for bladder cancer was admitted to our hospital because of decreased right visual acuity. Five years before entry, glaucoma was diagnosed for newly decreased left visual acuity, for which ophthalmic treatment was started. However, the right visual acuity also gradually decreased and visual field disturbance in the bilateral eyes deteriorated. He was referred to the department of ophthalmology in our hospital, and the diagnosis of optic neuropathy was made on the basis of the pattern of visual field disturbance and maintained low-teen intraocular pressure. Brain magnetic resonance imaging (MRI) revealed bilateral enlargement of the lacrimal glands, superior and inferior nerve, alveolar nerve, external ocular muscle, and pituitary gland. In addition, soft tissue was detected around the bilateral orbital nerve. IgG4-related disease was highly suspected from the MRI findings.
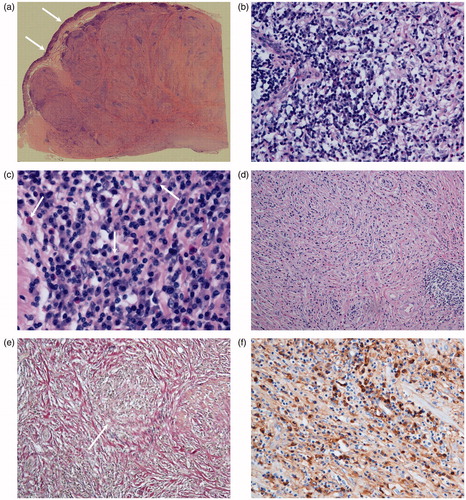
On admission, bilateral exophthalmos and bilateral eyelid swelling were noted. The submandibular and parotid glands were not swollen, and superficial lymph nodes including cervical lymph nodes were not palpable. No abnormalities were detected in the heart, lung, abdomen, or extremities. Laboratory findings included elevated erythrocyte sedimentation rate (74 mm/h), C-reactive protein 0.3 mg/dL, creatinine 1.06 mg/dL, total protein 9.2 g/dL, IgG 4285 mg/dL, IgG4 2090 mg/dL, IgE 4667 IU/mL (normal: <250), soluble IL-2 receptor 1056 U/mL (normal: 220–530), normal serum complement levels (CH50 58 IU/mL, C3 100 mg/dL, C4 37 mg/dL), rheumatoid factor negative, and antinuclear antibody negative. On contrast-enhanced CT, thickening of the bronchovascular bundle of the lung, mediastinal, and hilar lymph node swelling, paravertebral soft tissue, soft tissue around the right portal vein, circumferential wall thickening of the abdominal aortic artery and splenic artery, retroperitoneal fibrosis in the pelvis were detected, and IgG4-RD was strongly suspected. In addition, a mass-like lesion measuring 52 × 40 mm in the antrum of the stomach was revealed. The gastric mass lesion was described as a homogeneously enhanced mass, and the gastric mucosal layer was detected as a strongly enhanced linear structure suggesting the submucosal location of the mass lesion (). Lacrimal gland biopsy revealed diffuse, dense lymphoplasmacytic infiltrates around the ducts with follicle formation and fibrosis. Rearrangement of VH gene sediments in the biopsied specimen in the lacrimal gland was negative suggesting absence of clonal malignant cells. In addition, immunostaining revealed that more than 50% of infiltrating plasma cells were IgG4 positive, and diagnosis of IgG4-related disease was made based on the comprehensive diagnostic criteria proposed by Umehara et al. [Citation29]. After diagnosing IgG4-RD, further imaging examinations including ultrasonography (US), dynamic contrast-enhanced MRI, upper endoscopy, and barium enema were performed. On MRI, the lesion was described as a well-defined mass with low intensity in T1- and T2-weighted images and high intensity in diffusion-weighted images (). On dynamic study, the lesion showed an increasing enhancement pattern, while in arterial phase images, spared gastric mucosa was noted. Perigastric stranding was not found. US showed the lesion to be a homogeneous low echoic mass located in the submucosa, while a normal mucosal layer was noted as a hyper echoic layer (). On endoscopic and barium examination, the mass was seen as a submucosal lesion, and the gastric lumen was compressed. Overlying mucosa was normal and erosion or ulceration was not noted (). As IgG4-related gastric lesion, malignant lymphoma or gastrointestinal stromal tumor (GIST) was considered, endoscopic ultrasonography (EUS) was also performed. On EUS, the lesion was revealed to be a low echoic mass located in the proper muscular or subserosal layer. Biopsy was attempted but sufficient material could not be obtained to make a diagnosis. Thus, subsequently, distal gastrectomy was performed to make the pathological diagnosis. Histopathologically, the mass lesion was located in the submucosal layer and extended to the subserosal region, without involvement of the overlying mucosa (). Microscopically, the mass consisted of diffuse lymphoplasmacytic infiltrates with dense fibrosis. Eosinophils and obliterative phlebitis were easily recognized (). Helicobacter pylori infection was also revealed in the pathological specimen. IgG4-immunostaining revealed that more than 50% of plasma cells were IgG4-positive (). A final diagnosis of IgG4-related stomach lesion was made.
Figure 1. (a) Contrast-enhanced CT (axial image), (b) Contrast-enhanced CT (coronal image), (c) MRI; T2-weighted image (coronal image), and (d) Ultrasonographic image. Contrast-enhanced CT shows well-demarcated mass lesion in the antrum of the stomach (a: arrows). Reflecting the submucosal location of the lesion, gastric mucosa is described as strongly enhanced layer between the gastric lumen and mass lesion (b: arrow). The mass lesion shows homogeneous low intensity in MRI, and spared gastric mucosa is revealed as linear high intensity (c: arrows). In ultrasonography, the mass is described as homogeneous low echoic lesion and normal gastric mucosa is described as high echoic layer (d: arrows).
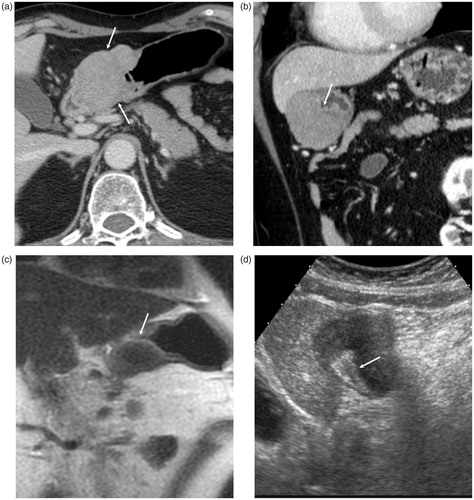
Figure 2. (a) Barium examination, (b) endoscopic image. Gastric lesion is described as compression of the gastric lumen (a: arrows) and submucosal mass projecting into the lumen at the antrum (b). Overlaying mucosa is normal on each examination.
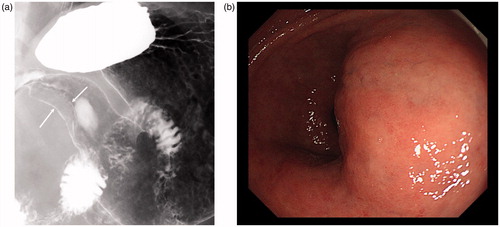
Figure 3. Histopathological specimens of the resected gastric lesion (a–d): H&E staining, (e): Elastica-van Gieson staining, and (f): IgG4 staining. Resected mass is located in the submucosa extending to sub serosal region, and overlaying mucosa is preserved (a: arrows). The mass consists of diffuse lymphoplasmacytic infiltration (b), eosinophils (c: arrows), and dense fibrosis (d). Obliterative phlebitis is also noted (e). In immunostaining of IgG4, abundant IgG4-positive plasma cells are noted.
Two weeks after the operation, prednisolone at 30 mg/day was started, followed by 25 mg/day two weeks later. One month after the start of steroid therapy, he felt improvement of the right eye symptoms. Nine months after initiation of steroid therapy, the bladder cancer recurred and BCG infusion therapy in the bladder was employed. This therapy was successful, and the visual acuity of the right eye also dramatically improved with a maintenance dose (5 mg/day) of prednisolone.
Discussion
We described a definite case of IgG4-RD involving the stomach. It also had extra gastric lesions involving other sites, such as the lacrimal glands, nervous system, lung, aorta, and showed serum IgG4 elevation. In addition, a pathological specimen from the lacrimal gland was also consistent with IgG4-RD. So far, several reports describing cases with gastrointestinal manifestations have been published (). However, more than half of them did not have extra gastrointestinal manifestations or serum IgG4 elevation, and were diagnosed based only on the pathological examinations [Citation19–21,Citation28]. Baez et al. reported a case of autoimmune pancreatitis with wall thickening and nodular lesions in the gastric wall [Citation22]. Kawano et al. also reported gastric lesions in the patients with IgG4-related disease involving the lung [Citation23]. In both cases, the main location of the gastric lesion was submucosal with or without mucosal ulceration. Our present case also showed submucosal involvement of the stomach. When we think about the radiological and pathological features of other organ manifestations, for example, pulmonary lesion mainly involves the interstitial stroma along with the bronchovascular bundle with mucosal sparing, renal pelvic lesion also occurs in submucosal lesion, while the epithelium layer is spared, and in pancreatic lesion, pancreatic duct epithelium is rarely involved, submucosal mass or wall thickening is supposed to be a typical manifestation of IgG4-related gastric lesion [Citation2,Citation30,Citation31]. Mucosal erosion or ulcer could be a secondary change caused by the submucosal lesion having lymphoplasmacytic infiltration or obliterative phlebitis. These secondary changes are sometimes observed in other organs being manifested such as mucosal edema or redness in pulmonary lesion or local arteriosclerosis in aortic lesion [Citation2,Citation16].
Table 1. Summary of reported cases of IgG4-related gastric lesion.
In our case, all of the imaging modalities well documented the submucosal location of the gastric lesion, with especially coronal images of dynamic contrast-enhanced CT and ultrasonography being useful. The gastric lesion showed homogeneous echogenicity and enhancement in US and contrast-enhanced CT, reflecting the inflammatory cells and fibrosis without degenerative changes or calcifications. EUS was also useful to presume the exact layer of the lesion location. The differential diagnosis of our case included GIST and malignant lymphoma. GIST can often present intra-tumor hemorrhage or degenerative change in contrast to IgG4-related disease, and thus, evaluation of intra-tumor homogeneity using US or contrast-enhanced CT might provide a clue to its differentiation [Citation32]. Another possible differential approach is to seek the presence of any extra gastric lesions suggestive of IgG4-RD; however, when we consider the current status in which the total spectrum of IgG4-related gastrointestinal lesions has not been elucidated, it is important to also pay full attention to other possible diseases, which in some cases might require surgical intervention.
Compared with other organ manifestations of IgG4-related disease, the gastric lesion still has some uncertainties and controversies. For example, the exact prevalence of IgG4-related gastrointestinal lesions is not known. One possible explanation for this is that small gastrointestinal lesions may be overlooked in imaging examinations. Inoue et al. reported a case of IgG4-related gastric lesion involving the submucosal layer coexisting with gastric cancer and IgG4-related kidney lesion; however, the gastric lesion had not been described in the preoperative contrast-enhanced CT, and the gastric lesion was found only in the postoperative pathological examination [Citation26]. Gastrointestinal lesions are sometimes difficult to detect in CT or US, and determination of wall thickening of the gastrointestinal tract can also be challenging. To avoid overlooking these small lesions, we should perform CT examinations with thin slice thickness. EUS also has the possibility to improve the detectability of small submucosal gastric lesions. Shinji et al. reported frequent gastric ulcers and abundant IgG4 positive plasma cell infiltration in biopsied specimens seen in patients with autoimmune pancreatitis [Citation24]. If EUS had been performed for these patients, small submucosal lesions might have been detected in some cases.
In conclusion, numerous issues regarding IgG4-related gastrointestinal lesions remain to be resolved, including their prevalence, adequate diagnostic process, and clinical significance. To tackle these issues, more research based on large case cohorts of IgG4-related gastrointestinal lesions is necessary.
Conflict of interest
None.
References
- Kitagawa S, Zen Y, Harada K, Sasaki M, Sato Y, Minato H, et al. Abundant IgG4-positive plasma cell infiltration characterizes chronic sclerosing sialadenitis (Küttner's tumor). Am J Surg Pathol. 2005;29(6):783–91.
- Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Kobayashi T, et al. Immunoglobulin G4-related lung disease: CT findings with pathologic correlations. Radiology. 2009;251(1):260–70.
- Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732–8.
- Zen Y, Harada K, Sasaki M, Sato Y, Tsuneyama K, Haratake J, et al. IgG4-related sclerosing cholangitis with and without hepatic inflammatory pseudotumor, and sclerosing pancreatitis-associated sclerosing cholangitis: do they belong to a spectrum of sclerosing pancreatitis? Am J Surg Pathol. 2004;28(9):1193–203.
- Cornell LD, Chicano SL, Deshpande V, Collins AB, Selig MK, Lauwers GY, et al. Pseudotumors due to IgG4 immune-complex tubulointerstitial nephritis associated with autoimmune pancreatocentric disease. Am J Surg Pathol. 2007;31(10):1586–97.
- Kasashima S, Zen Y, Kawashima A, Konishi K, Sasaki H, Endo M, et al. Inflammatory abdominal aortic aneurysm: close relationship to IgG4-related periaortitis. Am J Surg Pathol. 2008;32(2):197–204.
- Inoue D, Zen Y, Sato Y, Abo H, Demachi H, Uchiyama A, et al. IgG4-related perineural disease. Int J Rheumatol. 2012;2012:401890.
- Zen Y, Onodera M, Inoue D, Kitao A, Matsui O, Nohara T, et al. Retroperitoneal fibrosis: a clinicopathologic study with respect to immunoglobulin G4. Am J Surg Pathol. 2009;33(12):1833–9.
- Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366(6):539–51.
- Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385(9976):1460–71.
- Inoue D, Yoshida K, Yoneda N, Ozaki K, Matsubara T, Nagai K, et al. IgG4-related disease: dataset of 235 consecutive patients. Medicine (Baltimore). 2015;94(15):e680.
- Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012;25(9):1181–92.
- Irie H, Honda H, Baba S, Kuroiwa T, Yoshimitsu K, Tajima T, et al. Autoimmune pancreatitis: CT and MR characteristics. AJR Am J Roentgenol. 1998;170(5):1323–7.
- Sahani DV, Kalva SP, Farrell J, Maher MM, Saini S, Mueller PR, et al. Autoimmune pancreatitis: imaging features. Radiology. 2004;233(2):345–52.
- Takahashi N, Kawashima A, Fletcher JG, Chari ST. Renal involvement in patients with autoimmune pancreatitis: CT and MR imaging findings. Radiology. 2007;242(3):791–801.
- Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Yoshikawa J, et al. Immunoglobulin G4-related periaortitis and periarteritis: CT findings in 17 patients. Radiology. 2011;261(2):625–33.
- Fujinaga Y, Kadoya M, Kawa S, Hamano H, Ueda K, Momose M, et al. Characteristic findings in images of extra-pancreatic lesions associated with autoimmune pancreatitis. Eur J Radiol. 2009;76(2):228–38.
- Fujita A, Sakai O, Chapman MN, Sugimoto H. IgG4-related disease of the head and neck: CT and MR imaging manifestations. Radiographics. 2012;32(7):1945–58.
- Cheong HR, Lee BE, Song GA, Kim GH, An SG, Lim W. Immunoglobulin G4-related inflammatory pseudotumor presenting as a solitary mass in the stomach. Clin Endosc. 2016;49(2):197–201.
- Rollins KE, Mehta SP, O'Donovan M, Safranek PM. Gastric IgG4-related autoimmune fibrosclerosing pseudotumour: a novel location. ISRN Gastroenterol. 2011;2011:873087.
- Kim do H, Kim J, Park do H, Lee JH, Choi KD, Lee GH, et al. Immunoglobulin G4-related inflammatory pseudotumor of the stomach. Gastrointest Endosc. 2012;76(2):451–2.
- Baez JC, Hamilton MJ, Bellizzi A, Mortelé KJ. Gastric involvement in autoimmune pancreatitis: MDCT and histopathologic features. JOP. 2010;11(6):610–3.
- Kawano H, Ishii A, Kimura T, Takahashi T, Hironaka H, Kawano M, et al. IgG4-related disease manifesting the gastric wall thickening. Pathol Int. 2016;66(1):23–8.
- Shinji A, Sano K, Hamano H, Unno H, Fukushima M, Nakamura N, et al. Autoimmune pancreatitis is closely associated with gastric ulcer presenting with abundant IgG4-bearing plasma cell infiltration. Gastrointest Endosc. 2004;59(4):506–11.
- Kaji R, Okabe Y, Ishida Y, Takedatsu H, Kawahara A, Aino H, et al. Autoimmune pancreatitis presenting with IgG4-positive multiple gastric polyps. Gastrointest Endosc. 2010;71(2):420–2.
- Inoue K, Okubo T, Kato T, Shimamura K, Sugita T, Kubota M, et al. IgG4-related stomach muscle lesion with a renal pseudotumor and multiple renal rim-like lesions: a rare manifestation of IgG4-related disease. Mod Rheumatol. 2015. [Epub ahead of print]. doi: 10.3109/14397595.2015.1081743.
- Koizumi S, Kamisawa T, Kuruma S, Tabata T, Chiba K, Iwasaki S, et al. Immunoglobulin G4-related gastrointestinal diseases, are they immunoglobulin G4-related diseases? World J Gastroenterol. 2013;19(35):5769–74.
- Woo CG, Yook JH, Kim AY, Kim J. IgG4-related disease presented as a mural mass in the stomach. J Pathol Transl Med. 2016;50(1):67–70.
- Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012;22(1):21–30.
- Kawano M, Saeki T, Nakashima H, Nishi S, Yamaguchi Y, Hisano S, et al. Proposal for diagnostic criteria for IgG4-related kidney disease. Clin Exp Nephrol. 2011;15(5):615–26.
- Notohara K, Burgart LJ, Yadav D, Chari S, Smyrk TC. Idiopathic chronic pancreatitis with periductal lymphoplasmacytic infiltration: clinicopathologic features of 35 cases. Am J Surg Pathol. 2003;27(8):1119–27.
- Horton KM, Juluru K, Montogomery E, Fishman EK. Computed tomography imaging of gastrointestinal stromal tumors with pathology correlation. J Comput Assist Tomogr. 2004;28(6):811–17.