
Abstract
Periaortitis and periarteritis are one of the clinical features of IgG4-related disease. Such vascular manifestations are reported to be present in 10–30% of overall IgG4-related disease, and they may also appear as an isolated lesion of IgG4-related disease. As other types of large vessel vasculitis, IgG4-related vasculitis may cause significant clinical consequences. On the other hand, the diagnosis of IgG4-related periaortitis/periarteritis seems to have been made on the basis of different diagnostic criteria in reported studies; thus far, difficulty seems to be present in assessing the true frequency of the disease as well as determining the optimal therapeutic strategy. In this review, in addition presenting the clinical and pathological features of IgG4-related periaortitis/periarteirtis, we would like to discuss on what kind of points should be resolved for the better understanding of vascular involvement of IgG4-related disease in terms of diagnosis and treatment.
1. IgG4-related periaortitis/periarteritis as a large vessel vasculitis
Immunoglobulin G4 (IgG4)-related disease is a regional or systemic fibro-inflammatory condition [Citation1]. Accumulating evidence suggests that IgG4-related disease may involve various organs including the vascular system. The most frequently involved blood vessel is aorta, but medium-sized arteries, such as the carotid, iliac, and coronary arteries, may also be a potential target. In IgG4-related disease, aortitis is sometimes associated with other arterial inflammatory lesions, supporting the notion that IgG4-related disease may manifest as large vessel vasculitis [Citation2]. Indeed, IgG4-related disease is recognized as a potential cause of large vessel vasculitis in the 2012 revised Chapel Hill Consensus Conference (CHCC) nomenclature on vasculitides [Citation3]. Similar to other types of large vessel vasculitis, IgG4-related disease may sometimes be life-threatening [Citation4].
In terms of histopathology, IgG4-related vascular disease is characterized by infiltration of IgG4-positive plasma cells and lymphocytes into the adventitial layer, which manifests radiologically as markedly thickened perivascular tissue. In contrast to other types of large vessel vasculitis such as giant cell arteritis and Takayasu arteritis, destruction of the intima, and the media layer of the vessel wall is generally minor in IgG4-related disease. As such, vascular involvement of IgG4-related disease is called periaortitis or periarteritis, depending on the vessels involved. If aneurysmal dilatation of the vascular lumen is also present, the disease may be called inflammatory aortic/arterial aneurysm. In practice, it is sometimes difficult to clarify the boundary between IgG4-related abdominal periaortitis and idiopathic retroperitoneal fibrosis, because both conditions may cause nodular hypertrophy around the abdominal aorta [Citation5,Citation6].
IgG4 has unique biological properties that differ from the other three subtypes of human IgG (IgG1, IgG2, and IgG3), including exchange of the Fab-arm, which limits its ability to form immune complexes; minimal capacity to activate the Fc receptor; and interaction with the Fc portion of other IgG subclass antibodies [Citation7]. These features contribute to immune deactivation by IgG4 [Citation8]; as a result, IgG4 is considered to play an anti-inflammatory role in various disorders. It should be noted, however, that IgG4 autoantibodies are pathogenic in some immune-mediated diseases, such as pemphigus vulgaris, pemphigus foliaceus and MuSK-myasthenia gravis [Citation9]. At present, it remains unclear whether IgG4 antibodies accelerate or suppress the structural damage to vessels, or whether they are simply bystanders of ongoing vascular damage in IgG4-related disease [Citation10].
2. Clinical characteristics of patients with IgG4-related periaortitis/periarteritis
In the cases of IgG4-related periaortitis/periarteritis reported so far, diagnosis has often been based on different diagnostic grounds. For example, some studies reported concomitant vascular lesions in patients with known IgG4-related disease in non-vascular organs, while others reported the histopathological diagnosis of vascular involvement in IgG4-related disease. In addition, some studies report only definitive cases of IgG4-relataed periaortitis/periarteritis, while others also describe probable or possible cases. This heterogeneity may hinder our grasp of the complete clinical picture of IgG4-related periaortitis/periarteritis.
In 2016, Perugino et al. assessed 36 patients with IgG4-related who were identified to have large vessel involvement, and reported a male predominance (77%) and a mean age of onset of 54.6 ± 14 years [Citation11]. These characteristics do not seem to differ much from those reported for overall IgG4-related disease (male prevalence, 73%; mean onset age, 61.4 years) [Citation12]. In Perugino et al. series, some patients with IgG4-reated periaortitis/periarteritis presented with pain (chest, back, and groin), dyspnea and edema, but most of the symptoms seemed to be non-specific; in addition, no vascular-related symptoms were noted among 23 (64%) of the 36 patients.
In 2017, a Korean group reported that, among 1245 patients with aortitis or aortic disease, 10 had IgG4-related chronic periaortitis with a male prevalence of 60% and a mean age of 69 years [Citation13]. In their report, only one patient was asymptomatic, while the others had dyspnea, pain (chest, abdominal, back), and claudication of extremities. Smoking history was reported for only 3/10 (30%) of these patients.
More recently, we reported the clinical features of 99 patients in whom IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis were diagnosed by experts in this field [Citation14]. In this series, the mean age was 67.3 years, and male prevalence was 85%. Pain was the most prevalent symptom observed (23.2%), followed by fever (8.1%). Of these 99 patients, 33 (33%) were diagnosed with IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis by histopathological analysis (histologically diagnosed group), and 50 (51%) were diagnosed on the basis of suspected radiologic findings of periaortitis/periarteritis and retroperitoneal fibrosis combined with definitively diagnosed IgG4-related disease in non-vascular organs (radiologically diagnosed group). In the histologically diagnosed group, histologic assessment was performed on tissue samples obtained from surgery (16 cases), autopsy (3 cases), or biopsy (14 cases); thus, the vascular damage might have been more severe as compared with patients in the radiologically diagnosed group. Interestingly, however, the mean age (69.2 and 66.3 years in the histologically diagnosed and radiologically diagnosed groups, respectively) and prevalence of male (85 and 88%, respectively) did not differ significantly differ between the two groups. About two-thirds of the patients in both groups reported a smoking history. On the other hand, In the histologically-diagnosed group, however, the median serum IgG4 level was lower (424 mg/dL versus 877 mg/dL), while aneurysmal dilatation of the aorta/artery was more prevalent (42% versus 12%) as compared with the radiologically diagnosed group.
In general, patients with IgG4-related disease have been frequently observed to have a history of malignancy preceding the clinical onset of IgG4-related disease [Citation15]. In some studies, a history of malignancies has also been among patients with IgG4-related periaortitis/periarteritis [Citation16,Citation17]; however, whether the prevalence of malignancy differs between patients with vascular lesions and those with non-vascular lesions remains unclear.
3. Disease locations and radiologic findings
IgG4-related vascular lesions are most frequently reported in the aorta, most commonly in the infra-renal portion of the abdominal aorta [Citation18,Citation19]. In addition, medium-sized blood vessels, such as the celiac, mesenteric, iliac, coronary, pulmonary, and vertebral arteries have been reported as potential targets of IgG4-related periaortitis/periarteritis [Citation12]. Inoue et al. found that the aorta is the most prevalently affected region (15 [88%]), but the involvement of other medium-sized vessels has also been reported (superior/inferior mesenteric arteries, 4 cases; common iliac artery, 10 cases; splenic arteries, carotid artery, splenic artery, 1 case) [Citation18].
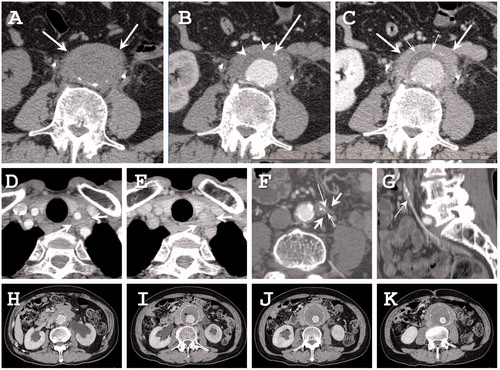
Characteristic computed tomography (CT) findings of IgG4-related periaortitis/periarteritis include a severely thickened aortic/arterial wall, which is involved circumferentially and homogeneously enhanced at the delayed phase of dynamic contrast-enhanced CT () [Citation18]. A high-density thin layer. corresponding to the intima-media complex, is sometimes seen. Characteristic magnetic resonance imaging (MRI) findings have not been evaluated because to date there is no systemic study using MRI.
Figure 1. Radiographic findings. (a–c) Seventy-three-year-old man with IgG4-related periaortitis. (a) Precontrast CT shows the soft tissue density mass around the abdominal aorta (white arrows). (b) The arterial phase of dynamic contrast-enhanced CT shows the inferior mesenteric artery in the soft tissue density mass (thin arrow). The atherosclerotic plaque is not enhanced (arrowheads). (c) The delayed phase of dynamic contrast-enhanced CT shows that the periaortic mass is slightly enhanced (arrows). A high density thin layer is seen between the atherosclerotic plaque and the periaortic mass (small arrows). (d,e) A 68-year-old man with IgG4-related periarteritis. (d) The arterial phase of dynamic contrast-enhanced CT shows a soft tissue density mass around the left common carotid artery (arrows). (e) The delayed phase of dynamic contrast-enhanced CT shows that the mass is slightly enhanced (arrows). Stenosis of the left common carotid artery is not seen in this case. (f,g) A 63-year-old man with IgG4-related periarteritis. (f) The arterial phase of dynamic contrast-enhanced CT shows a soft tissue density mass around the inferior mesenteric artery (arrows) with a luminal stenosis (thin arrow) and calcification (small arrow). (g) In the reconstructed sagittal image, the luminal stenosis can be clearly seen (thin arrow). (h–i) IgG4-related abdominal inflammatory aneurysm treated by stent graft implantation.
In terms of aortic lesions, in addition to cases presenting only perivascular thickening, inflammatory aortic aneurysm accompanied by aneurysmal luminal dilatation can occur [Citation20]. Furthermore, a case of aortic dissection with suspected IgG4-related disease has been reported [Citation11]. It is unknown what effect the IgG4 antibody itself has on the progression of these diseases. The fact that severe stenosis of the aorta, which is sometimes observed in Takayasu’s arteritis [Citation21], has not been reported in patients with IgG4-related aortic lesions may provide diagnostic clues to the different conditions.
Radiologic findings in medium-sized arteries are essentially the same as those in the aorta, i.e. prominent perivascular thickening () [Citation22], aneurysmal luminal dilatation [Citation23], and dissection [Citation24]. On the other hand, luminal stenosis, which may cause ischemia of distal organs [Citation11,Citation25], is seen, albeit not frequently, in medium-sized arteries, such as the coronary artery, internal carotid arteries, or inferior mesenteric artery (). Dong et al reported a case of IgG4-related peripulmonary arteritis with luminal stenosis [Citation26]. The observed stenosis may be due to intramural thrombus or may be secondary to the severe vessel wall injury induced by IgG4-related pathologies. Thickening of the intimal layer might explain the luminal narrowing observed in some cases [Citation11,Citation27]; overall, however, information is limited. One study reported that corticosteroid therapy not only decreased the soft tissue around the coronary artery, but also improved luminal stenosis in patients with IgG4-related coronary periarteritis [Citation28].
4. Histologic findings
Only about half of the cases diagnosed as inflammatory abdominal aortic aneurysm and retroperitoneal fibrosis on the basis of histopathologic findings are IgG4-related [Citation29,Citation30]. Regarding IgG4-related inflammatory abdominal aortic aneurysm and retroperitoneal fibrosis, histopathologic characteristics of IgG4-related disease include IgG4-positive plasmacytic infiltration, storiform fibrosis, and obliterative phlebitis [Citation31], although such characteristics are not always observed [Citation20,Citation29]. Among the reported cases of inflammatory abdominal aortic aneurysm, the degree of inflammatory activity and fibrosis is more severe in IgG4-related disease; in particular, the adventitia is considerably thicker in IgG4-related disease. In addition to the above findings, perineural infiltration, and the emergence of eosinophils and/or regulatory T cells would be a useful marker for distinguishing IgG4-related periaortitis/periarteritis from other vascular diseases including atherosclerotic lesions [Citation32]. Along this line, neutrophilic infiltration, thicker atherosclerotic intima, epithelioid granuloma, and fibrinoid necrosis may be used to rule out the possibility of IgG4-related vascular disease.
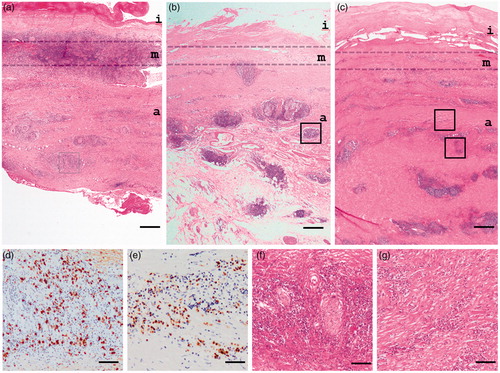
IgG4-related disease has been observed histopathologically in medium-sized arteries, the including carotid, coronary, and iliac arteries [Citation11,Citation33]. In IgG4-related vascular disease, lymphoplasmacytic infiltration and fibrosis predominantly spread from the adventitia to the surrounding adipose tissue. Such findings have sometimes been observed in the medial layer of vessels (), and are generally considered to be secondary changes [Citation29]. In the thoracic aorta, however, aortitis-related changes are reported to occur in all layers of the vessels [Citation34,Citation35]. In this sense, IgG4-related vascular disease might represent another type of large vessel periaortitis/periarteritis.
Figure 2. Histopathological findings of IgG4-related abdominal aortic aneurysm. (a) Inflammation with lymphoplasmacytes is observed predominantly in the medial layer. (b) Diffuse inflammation with lymphoid follicles and fibrosis are detected mainly in the adventitia layer that is in part spreading to adjacent adipose tissue. (c) Fibrosis progresses to adjacent adipose tissue. (d,e) Massive infiltration of IgG4-immunopositive cells in adventitia (d and e correspond to box areas of a and b, respectively). (f) Perineural infiltration. (g) storiform fibrosis. A higher magnification of the box area of (c). Original magnifications and scale bar, respectively, are ×12.5 and 500 μm (a–c), ×200 and 50 μm (d, e), and ×100, and 100 μm (f, g). i, intima; m, media; a; adventitia.
5. Involvement of other organs and isolated cases
How frequently are IgG4-related non-vascular lesions concomitantly present in cases of IgG4-related vascular lesions? In the cases reported so far, the diagnosis of IgG4-related periaortitis/periarteritis seems to have been made mainly via two pathways. In the first, radiologic findings suspicious of periaortitis/periarteritis were present in a patient with a confirmed diagnosis of IgG4-related disease in other organs; and in the second, the diagnosis of IgG4-related vascular lesions was made by direct histopathological assessment of tissue samples acquired from the corresponding vessels.
It should be noted that there is diagnostic bias toward the concomitant involvement of other non-vascular lesions. In the first type of diagnosis, all cases with vascular lesions are theoretically associated with other organ lesions. In the second type of diagnosis, tissues sampling from affected vessels is performed despite the potential risk; for example, this subset may include patients whose tissue samples were obtained by surgery for vascular lesions such as large aortic aneurysm, or by autopsy following fatal rupture of the aneurysm. It is therefore presumed the aortic/arterial lesion may be more severe among patients diagnosed by the second pathway.
Kasashima et al. reported that among 13 patients with a histopathological diagnosis of IgG4-related inflammatory aortic aneurysm, none had concomitant non-vascular lesions [Citation29]. However, for the above-mentioned reasons, this does not necessarily indicate that clinically severe vascular lesions, such as those requiring surgical treatment, are not associated with non-vascular lesions.
In a more recent study, Mizushima et al. reported that among 33 patients who had been histopathologically diagnosed to have IgG4-related periaortitis/periarteritis or retroperitoneal fibrosis, 12 (36%) had concomitant involvement of at least one non-vascular organ, most commonly the salivary gland (12%) followed by the pancreas (9%) [Citation14]. In their series, about two-thirds of histopathologically diagnosed cases of IgG4-related periaortitis/periarteritis did not have associated IgG4-related disease in non-vascular organs; therefore, these lesions, at least in part, may fall into the category of clinically isolated aortitis [Citation36]. In the revised CHCC nomenclature on vasculitides, IgG4-related disease is mentioned as one of the potential conditions underlying clinically isolated aortitis [Citation3].
Nevertheless, one should be aware that IgG4-related disease may develop in various organs metachronously. In fact, several case reports have demonstrated the emergence of IgG4-related disease in non-vascular organs subsequent to the development of IgG4-related vascular lesions [Citation16,Citation37]. As advocated by Cinar et al. advocated, systemic examination and careful clinical follow-up are needed before the observed lesions can be declared as isolated aortitis [Citation36].
6. Prevalence of IgG4-related periaortitis/periarteritis
6.1. Geographic prevalence
Several reports have been published from Japanese groups regarding the prevalence of periaortitis/periarteritis among patients diagnosed with IgG4-related disease. In 2010, for example, Zen et al. assessed 114 patients who were diagnosed with IgG4-related disease on basis of pathologic features, reporting that 7 (6%) of them had lesions in the aorta or arteries [Citation38]. More recently, Ozawa et al. analyzed radiologic findings from 179 patients who were diagnosed with IgG4-related disease in non-vascular organs and had not received steroid therapy [Citation19]. Periaortitis and periarteritis were defined to be present when the vessel wall was thickened and contrast-medium enhancement of the wall was observed either partially or circumferentially on CT. The index organ affected with IgG4-related disease included the pancreas, salivary glands, bile ducts, respiratory tract, renal and ureter, lacrimal glands, and prostate. Overall, Ozawa et al. found that 65 (36%) patients had vascular involvement.
In 2014, Mizushima et al. analyzed 333 patients diagnosed with IgG4-related disease in several Japanese hospitals. They diagnosed periaortic/periarterial lesions when there was circumferential or partial thickening of the wall of the affected aortas/arteries with homogeneous enhancement visualized by contrast-enhanced CT [Citation39]. In total, 40 (12%) patients were judged to have periarteritis/periarteritis. Both Ozawa et al. and Mizushima et al. studies indicated that perivascular thickening suspicious of IgG4-related periarteritis/periarteritis is not a rare finding among patients diagnosed with IgG4-related disease in non-vascular organs. Both studies included patients primarily diagnosed with IgG4-related disease in non-vascular organs. More recently, Yamada et al. reported that among 334 patients diagnosed with IgG4-related disease on the basis of either by Comprehensive Diagnostic Criteria (CDC) or organ-specific diagnostic criteria, 83 (25%) were found to have lesions in the retroperitoneum or periaorta [Citation40].
Studies in the United States have also been conducted. In 2016, Perugino et al. reported that vascular involvement was observed in 36 (22.5%) of 160 patients diagnosed with IgG4-related disease via histopathologic findings of the affected tissue [Citation11]. They defined two types of vasculitis, primary IgG4-related vasculitis and secondary IgG4-related vascular involvement. The former was characterized by the presence of one or more of the following features: vessel wall thickening, vessel wall enhancement on contrast study, and increased FDG uptake within the blood vessel wall by FDG-PET. Primary IgG4-related vasculitis seems to refer to lesions with predominant periaortic and concentric involvement, which generally correspond with our term ‘IgG4-related periaortitis/periarteritis’. On the other hand, the latter was characterized by abnormal perivascular soft tissue with minimal vascular wall findings. Secondary IgG4-related vascular involvement seems to refer to retroperitoneal plaque-like or mass-forming lesions extending to periaorta/periartery, which are basically associated with retroperitoneal fibrosis. However, as mentioned above, it may be sometimes difficult to differentiate IgG4-related periaortitis or primary IgG4-related vasculitis from retroperitoneal fibrosis or secondary IgG4-related vascular involvement. In Perugino et al.’s study, primary IgG4-related vasculitis was diagnosed in 13 (8.1%), and secondary IgG4-related vasculitis in 23 (14.3%) of the 160 patients. As expected, patients with primary IgG4-related vasculitis presented with vascular-related signs and symptoms more frequently than those with secondary IgG4-related vasculitis (9/13 [69%] versus 3/23 [13%]). In 2015, Wallace et al. analyzed 125 patients with biopsy-proven IgG4-related disease and reported involvement of the aorta in 14 (11%) of them [Citation41].
In China, Lin et al. reported the results of a prospective study investigating the clinical characteristics of IgG4-related disease, in which they identified 31 (26%) patients with periaortitis/retroperitoneal fibrosis among 118 patients diagnosed with IgG4-related disease [Citation42]. Lin et al. utilized CDC for the diagnosis of IgG4-related disease, but tissue analysis for 68 (58%), and made a definitive diagnosis for 64 (54%). In addition, Chen et al. assessed 28 patients who were diagnosed with definitive IgG4-related disease by CDC; thus, histological assessment was performed for all patients enrolled [Citation43]. They identified 1 (4%) case of aortic involvement and 3 (11%) cases of retroperitoneal fibrosis; however, it was not reported whether tissue sampling of these tissues was carried out.
In a literature review of unselected cases of IgG4-related disease, Brito-Zerón et al. reported that among 375 patients undergoing systemic screening of IgG4-related disease, 33 (9%) had aortic involvement [Citation12]. Although this rate is lower than those in the above-mentioned reports, Brito-Zerón et al. considered the prevalence of retroperitoneal fibrosis (13%) separately.
6.2. Factors affecting prevalence estimation
Regarding the prevalence of overall IgG4-related disease, Umehara et al. estimated that 6,700–26,000 individuals in Japan would have developed IgG4-RD over the past 20 years on the basis of the data from the two university hospitals in Ishikawa Prefecture [Citation44]. However, it may differ by geographic area, and is reported to be ∼8 per 100,000 population in Japan by Uchida et al. based on a nationwide survey [Citation45]. Several ambiguities must be addressed before we can estimate the incidence of IgG4-related periaortitis/periarteritis as 10–30% of this prevalence.
First, under-recognition. It has been less than 20 years since IgG4-related disease was first described in autoimmune pancreatitis [Citation1]; thus, this pathology may not be familiar to cardiovascular physicians. Second, the difficulty of distinguishing IgG4-related periaortitis/periarteritis from other types of vasculitis by radiologic findings. Radiologic images of IgG4-related vasculitis frequently resemble those caused by other disorders of infectious, malignant, and immune-related origin, such as Takayasu arteritis and Bechet’s disease. In addition, IgG4-related periaortitis may not readily be distinguished from its non-IgG4-related counterpart by either the radiologic findings or clinical course [Citation13,Citation29,Citation30].
Third, non-negligible risk of tissue sampling. To make a definitive diagnosis of IgG4-related periaortitis/periarteritis by CDC, tissue sampling of the arterial wall should be carried out [Citation46], which may sometimes not be practical owing to the potential risks [Citation47]. If there is significant difference in clinical course, including therapeutic response, between IgG4-related and non-IgG4-related vasculitis, then the benefits of a definitive diagnosis may not outweigh the risk of tissue sampling. The recent trend of using of stent grafting for the treatment of aortic lesions also makes it more difficult to obtain tissue samples (). These three factors may lead to the underestimation of the prevalence of IgG4-related periaortitis/periarteritis.
6.3. New diagnostic methods for IgG4-related periaortitis/periarteritis
On the other hand, the emergence of other diagnostic methods may facilitate the diagnosis of IgG4-related vascular lesions. 18F-Fluoro-deoxyglucose positron emission tomography (FDG-PET) is a powerful diagnostic technique in the field of large vessel vasculitis [Citation48,Citation49], and enhanced FDG uptake may be one of the hallmarks of organ involvement in IgG4-related diseases [Citation50,Citation51]. Indeed, a few studies have taken advantage of FDG-PET technology to try and detect vascular lesions among patients with IgG4-related disease.
By using PET-CT and enhanced CT, Ebe et al. identified 7 patients (mean age, 70 years; male prevalence, 86%) with IgG4-related perivascular lesions among 21 patients diagnosed with IgG4-related disease by CDC [Citation52]. In their series, aneurysmal dilatation was not observed in any of the patients with enhanced FDG uptake in the perivascular regions. Similarly, Yabusaki et al. identified 15 (41%) patients (mean age, 69.5 ± 6.0 years; male prevalence, 80%) with perivascular lesions among 37 patients diagnosed with IgG4-related disease in non-vascular organs by using FDG-PET/CT [Citation53]. In their series, the aorta and iliac artery were the most common sites involved, and 10 (27%) patients showed aneurysmal aortic dilatation.
One should be aware, however, that increased uptake of FDG is also observed in other conditions, such as giant cell arteritis, Takayasu arteritis, and infected as well as atherosclerotic aneurysms [Citation54,Citation55]. In addition, persistent enhanced FDG uptake may not necessarily result in a progression of vascular injury [Citation56]. Currently, although FDG-PET/CT enables the acquisition of whole-body images in various inflammatory, malignant, and infectious disorders, its role in the assessment of patients with IgG4-related periaortitis/periarteritis has not been well-established in terms of either clinical impact, specificity for the IgG4-related disease, or cost-effectiveness [Citation57].
7. Diagnosis of IgG4-related periaortitis/periarteritis
7.1. Japan
In Japan, diagnosis of IgG4 related diseases is generally made either by CDC or by organ-specific diagnostic criteria [Citation46]. Although CDC can be used for diagnosis regardless of the organ affected, a definitive diagnosis of IgG4-related disease cannot be made without a histologic investigation of the affected tissues. Organ-specific diagnostic criteria for IgG4-related disease have been established for organs including the ophthalmus, salivary glands, pancreas, bile duct, kidney, and lung. For organs such as the pancreas, IgG4-related disease exhibits relatively specific radiologic findings, which facilitate a definite diagnosis of IgG4-related disease by organ-specific diagnostic criteria even in the absence of histologic findings [Citation58–60]; although these criteria are not approved internationally [Citation61].
For IgG4-related periaortitis/periarteritis, by contrast, radiologic findings cannot readily differentiate among arteriosclerosis, other immune-related disorders, infectious diseases, and malignant diseases. How about the specificity of elevated serum IgG4? Although elevation of serum IgG4 was one of the findings underlying the discovery of IgG4-related diseases, its diagnostic utility in differentiating IgG4-related periaortitis/periarteritis from other diseases, called IgG4-related disease mimickers, remains unclear [Citation62]. In fact, in one study, around 4% of patients admitted to the cardiology department were found to have elevated serum IgG4 levels, indicating that serum IgG4 > 135 mg/dL is far from specific for IgG4-related periaortitis/periarteritis among those with certain cardiovascular problems [Citation63]. When (peri)vascular tissue cannot be obtained, it is not possible to definitively diagnose a case of IgG4-related periaortitis/periarteritis by CDC, which may lead not only to underdiagnosis but also to inappropriate diagnosis.
Taking these situations into account, we have worded with the research group on IgG4-related diseases at the Ministry of Health, Labor and Welfare and the Japanese Circulation Society, leading to the establishment of organ-specific diagnostic criteria for IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis [Citation14] (). A chief feature of these newly proposed organ-specific diagnostic criteria is that periaortitis/periarteritis and retroperitoneal fibrosis can be diagnosed as IgG4-related from histological findings regardless of serum IgG4 levels. This is because serum IgG4 is not always elevated in cases with histopathologically diagnosed IgG4-related periaortitis or retroperitoneal fibrosis [Citation20,Citation64].
Table 1. Diagnostic criteria for IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis.
Another and more clinically useful feature is that the criteria may diagnose periaortitis/periarteritis and retroperitoneal fibrosis as IgG4-related without histological analysis of the corresponding tissues when there is a definitive diagnosis of IgG4-related disease in other organs, coupled with elevated serum IgG4. The introduction of these organ-specific criteria may facilitate the diagnosis of IgG4-related periaortitis/periarteritis; however, their clinical utility awaits verification in future prospective studies.
7.2. Other countries
About three-quarter of all cases of IgG4-related disease have been reported from Japan [Citation12]; however, IgG4-related periaortitis/periarteritis has also been documented in other countries. Based on a search of studies in which IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis were reported as either case reports or cohort studies in countries other than Japan, we identified 103 patients (68 men and 35 women; average age, 58.3 years [range: 12 years–80 years]) [Citation11,Citation23,Citation35,Citation64–97]. Histopathological evaluation was performed in 84 (82%) cases, and tissue infiltration of lymphoplasmacytic cells and gG4-positive plasma cells was positive in all of them. Storiform fibrosis and obliterative phlebitis, the two characteristic histological findings of IgG4-related disease, were reported to be present in 35 and 15 cases, respectively. Of 103 patients, measurement of serum IgG4 level, which is a mandatory for the diagnosis of IgG4-related disease by CDC in Japan [Citation46], was performed for 69 patients, only 34 patients of whom showed elevated serum IgG4 (>135 mg/dL). Only 19 (20%) patients were reported to have concomitant involvement in non-vascular organs, including ophthalmus, salivary glands, pancreas, bile duct, kidney, and lung. Radiologic findings, such as the presence of thickening or mass formation around the vessels, were reported in many cases, although frequently the radiologic images were not presented in the paper.
Taking these findings altogether, the presence or absence of IgG4-positive cell infiltration seems to be the most important factor for diagnosis of IgG4-related periaortitis/periarteritis in countries other than Japan. However, IgG4-positive cell infiltration can occur in various conditions other than IgG4-related disease [Citation98], including non-specific inflammatory conditions [Citation99,Citation100], immune-related pathologies [Citation101–103], and chronic infection [Citation104]. Essentially, therefore, clinicopathological correlation of organ function with IgG4-positive cell infiltration should be comprehensively taken into account for the diagnosis of IgG4-related disease.
Notably, when we applied the organ-specific diagnostic criteria proposed in Japan, 23 (22%) of the 103 patients were diagnosed to have definitive IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis, and 45 (44%), and 17 (17%) patients were diagnosed to have probable and possible disease, respectively.
8. Treatment
Glucocorticoid therapy is recommended as a first-line therapy for the treatment of IgG4-related disease by international consensus [Citation105]; and glucocorticoids, mainly prednisolone and prednisone, are generally effective in ameliorating IgG4-related disease, although recurrence is not rare [Citation106,Citation107]. The effects of glucocorticoids have mainly been reported on the basis of observational data/A few prospective studies have been conducted: however, drug refractoriness, improvement in long-term outcomes, and possible misdiagnosis are problems remaining to be solved [Citation107–109]. In Japan, the recommended starting dose of prednisolone is 0.5–0.6 mg/kg/daily or 0.4–0.6 mg/kg/day, and a slow tapering (<0.4 mg/day) is considered to be important to avoid recurrence [Citation46,Citation106].
As yet, there is no therapeutic regimen specific for vascular lesions of IgG4-related disease; thus, treatment usually follows the protocol for patients with IgG4-related disease and organ failure [Citation110]. According to the therapeutic guidance, all patients with symptomatic active IgG4-related disease require treatment [Citation105].
When assessing the indication of glucocorticoid therapy for a patient with IgG4-related vascular lesions, in addition to potential adverse effects of glucocorticoids, such as metabolism dysregulation of lipids and glucose, and susceptibility to infection, the possibility of unfavorable aortic/arterial remodeling should be taken into consideration because aortic/arterial luminal dilatation may occur during the steroid-based therapy, especially if luminal dilatation is present before the treatment [Citation19,Citation39]. Although such changes are usually subclinical, cases in which aortic or arterial dilatation leads to a fatal rupture or requires surgical correction have been reported [Citation4,Citation25,Citation111]. Although the link between glucocorticoid therapy and vascular fragilization is not definitive, one should be aware of the correct indications for the treatment of IgG4-related vascular disease. According to the therapeutic guidance, urgent treatment is recommended for inflammatory aortic aneurysms that are continuing to enlarge and at risk for dissection; however, mechanical intervention or surgery might be an option to be considered [Citation39,Citation105]. Glucocorticoid therapy for asymptomatic IgG4-related periaortitis/periarteritis without impending organ failure should be done with caution.
Alternative strategies for the medical treatment of IgG4-related disease include immunosuppressants (methotrexate, azathioprine, mizoribine, mycophenolate mofetil, cyclosporine A, etc.) and targeted immunomodulators (rituximab, abatacept, etc.) [Citation2,Citation106,Citation112], but in Japan, the use of targeted immunomodulators including the monoclonal anti-CD20 antibody rituximab is not covered by health insurance at this time. The effect of immunosuppressants and targeted immunomodulators in terms of suppressing on-going vascular remodeling in patients with IgG4-related periaortitis/periarteritis needs further investigation.
9. The value of a diagnosis of IgG4-related periaortitis/periarteritis
Establishing a diagnosis of IgG4-related periaortitis/periarteritis may have several merits. First, considering that IgG4-related disease affects various organs not only simultaneously but also metachronously, the emergence of IgG4-related disease in non-vascular organs may be anticipated in patients with IgG4-related periaortitis/periarteritis [Citation113,Citation114]. Second, if vascular lesions are associated with IgG4-related disease in non-vascular organs, careful follow-up of vascular morphology may be performed after glucocorticoid therapy is started. Third, the post-therapeutic clinical course might differ between IgG4-related and non-IgG4-related vascular lesions. Fourth, it may be anticipated that the post-operative clinical course may differ from that of the non-IgG4-related cases, in terms of progression of fibrosis, dilation of vessels, and persistence of symptoms [Citation115]. Last, we might be able to alleviate organ hypoperfusion with less invasive medical therapy [Citation11,Citation28], although this possibility should be examined in further analysis.
10. Future directions
IgG4-related vascular lesions are by no means a rare condition; they may occur in about 10–30% of patients with IgG4-related non-vascular disease, although this prevalence depends on how vascular involvement is diagnosed. Our newly proposed organ-specific diagnostic criteria may facilitate the diagnosis of IgG4-related periaortitis/periarteritis, especially among patients at high risk for tissue sampling. Future studies should clarify the optimal medical therapeutic strategy for IgG4-related periaortitis/periarteritis [Citation32,Citation116]. We hope that the pathogenic mechanisms of vascular remodeling will be understood in more detail by clarifying the pathogenesis of IgG4-related vascular lesions, through which we can develop an improved approach for the diagnosis and treatment of various vascular disorders.
Conflict of interest
None.
Acknowledgements
We are highly appreciative of Megumi Hashimoto for her technical assistance.
Additional information
Funding
References
- Hamano H, Kawa S, Horiuchi A, Unno H, Furuya N, Akamatsu T, et al. High serum IgG4 concentrations in patients with sclerosing pancreatitis. N Engl J Med. 2001;344(10):732–8.
- Ebbo M, Daniel L, Pavic M, Seve P, Hamidou M, Andres E, et al. IgG4-related systemic disease: features and treatment response in a French cohort: results of a multicenter registry. Medicine (Baltimore). 2012;91(1):49–56.
- Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill consensus conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1–11.
- Tajima M, Hiroi Y, Takazawa Y, Muraoka H, Iwata H, Yamashita H, et al. Immunoglobulin G4-related multiple systemic aneurysms and splenic aneurysm rupture during steroid therapy. Hum Pathol. 2014;45(1):175–9.
- Vaglio A, Salvarani C, Buzio C. Retroperitoneal fibrosis. Lancet 2006;367(9506):241–51.
- Rossi GM, Rocco R, Accorsi Buttini E, Marvisi C, Vaglio A. Idiopathic retroperitoneal fibrosis and its overlap with IgG4-related disease. Intern Emerg Med. 2017;12(3):287–99.
- Yamamoto M, Takahashi H, Shinomura Y. Mechanisms and assessment of IgG4-related disease: lessons for the rheumatologist. Nat Rev Rheumatol. 2014;10(3):148–59.
- Davies AM, Sutton BJ. Human IgG4: a structural perspective. Immunol Rev. 2015;268(1):139–59.
- Trampert DC, Hubers LM, van de Graaf SFJ, Beuers U. On the role of IgG4 in inflammatory conditions: lessons for IgG4-related disease. Biochim Biophys Acta Mol Basis Dis. 2018;1864(4 Pt B):1401–9.
- Shiokawa M, Kodama Y, Kuriyama K, Yoshimura K, Tomono T, Morita T, et al. Pathogenicity of IgG in patients with IgG4-related disease. Gut 2016;65(8):1322–32.
- Perugino CA, Wallace ZS, Meyersohn N, Oliveira G, Stone JR, Stone JH. Large vessel involvement by IgG4-related disease. Medicine (Baltimore). 2016;95(28):e3344.
- Brito-Zeron P, Ramos-Casals M, Bosch X, Stone JH. The clinical spectrum of IgG4-related disease. Autoimmun Rev. 2014;13(12):1203–10.
- Kim IY, Eun YH, Jeong H, Park TK, Kim H, Lee J, et al. Clinical characteristics and outcomes of 61 patients with chronic periaortitis including IgG4-related and non-IgG4-related cases. Int J Rheum Dis. 2017;20(11):1751–62.
- Mizushima I, Kasashima S, Notohara K, Fujinaga Y, Saeki T, Zen Y, et al. Clinical and pathological characteristics of IgG4-related periaortitis/periarteritis and retroperitoneal fibrosis diagnosed based on experts’ diagnosis. J Jpn Coll Angiol. 2018;58: 117–29.
- Wallace ZS, Wallace CJ, Lu N, Choi HK, Stone JH. Association of IgG4-related disease with history of malignancy. Arthritis Rheumatol. 2016;68(9):2283–9.
- Sakamoto A, Nagai R, Saito K, Imai Y, Takahashi M, Hosoya Y, et al. Idiopathic retroperitoneal fibrosis, inflammatory aortic aneurysm, and inflammatory pericarditis–retrospective analysis of 11 case histories. J Cardiol. 2012;59(2):139–46.
- Hourai R, Kasashima S, Fujita SI, Sohmiya K, Daimon M, Hirose Y, et al. A case of aortic stenosis with serum IgG4 elevation, and IgG4-positive plasmacytic infiltration in the aortic valve, epicardium, and aortic adventitia. Int Heart J. 2018;59(5):1149–54.
- Inoue D, Zen Y, Abo H, Gabata T, Demachi H, Yoshikawa J, et al. Immunoglobulin G4-related periaortitis and periarteritis: CT findings in 17 patients. Radiology 2011;261(2):625–33.
- Ozawa M, Fujinaga Y, Asano J, Nakamura A, Watanabe T, Ito T, et al. Clinical features of IgG4-related periaortitis/periarteritis based on the analysis of 179 patients with IgG4-related disease: a case-control study. Arthritis Res Ther. 2017;19(1):223.
- Kasashima S, Zen Y. IgG4-related inflammatory abdominal aortic aneurysm, spectrum of IgG4-related chronic periaortitis. Ann Vasc Dis. 2010;3(3):182–9.
- Kim YW, Sung K, Park YJ, Kim DK. Surgical treatment of middle aortic syndrome due to Takayasu arteritis. J Vasc Surg. 2015;62(3):750–1.
- Urabe Y, Fujii T, Kurushima S, Tsujiyama S, Kihara Y. Pigs-in-a-blanket coronary arteries: a case of immunoglobulin G4-related coronary periarteritis assessed by computed tomography coronary angiography, intravascular ultrasound, and positron emission tomography. Circ Cardiovasc Imaging. 2012;5(5):685–7.
- Ruggio A, Iaconelli A, Panaioli E, Bernardini F, Tinelli G, Savino G, et al. Coronary artery aneurysms presenting as acute coronary syndrome: an unusual case of IgG4-related disease vascular involvement. Can J Cardiol. 2018;34:1088. e1087–e1010.
- Barp A, Fedrigo M, Farina FM, Lepidi S, Causin F, Castellani C, et al. Carotid aneurism with acute dissection: an unusual case of IgG4-related diseases. Cardiovasc Pathol. 2016;25(1):59–62.
- Ikutomi M, Matsumura T, Iwata H, Nishimura G, Ishizaka N, Hirata Y, et al. Giant tumorous lesions (correction of legions) surrounding the right coronary artery associated with immunoglobulin-G4-related systemic disease. Cardiology 2011;120(1):22–6.
- Dong A, Wang Y, Zuo C. FDG PET/CT in IgG4-Related Peripulmonary Arteritis. Clin Nucl Med. 2016;41(10):e439–40.
- Deng H, Zhao S, Yue Y, Liu Y, Xu Y, Qian J, et al. IgG4-related disease of pulmonary artery causing pulmonary hypertension. Medicine (Baltimore). 2018;97(20):e10698.
- Sakamoto A, Tanaka T, Hirano K, Koike K, Komuro I. Immunoglobulin G4-related coronary periarteritis and luminal stenosis in a patient with a history of autoimmune pancreatitis. Intern Med. 2017;56(18):2445–50.
- Kasashima S, Zen Y, Kawashima A, Endo M, Matsumoto Y, Kasashima F. A new clinicopathological entity of IgG4-related inflammatory abdominal aortic aneurysm. J Vasc Surg. 2009;49(5):1264–71; discussion 1271.
- Zen Y, Onodera M, Inoue D, Kitao A, Matsui O, Nohara T, et al. Retroperitoneal fibrosis: a clinicopathologic study with respect to immunoglobulin G4. Am J Surg Pathol. 2009;33(12):1833–9.
- Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet. 2015;385(9976):1460–71.
- Kasashima S, Kawashima A, Zen Y, Ozaki S, Kasashima F, Endo M, et al. Upregulated interleukins (IL-6, IL-10, and IL-13) in immunoglobulin G4-related aortic aneurysm patients. J Vasc Surg. 2018;67(4):1248–62.
- Ishizaka N. IgG4-related disease underlying the pathogenesis of coronary artery disease. Clin Chim Acta. 2013;415:220–5.
- Kasashima S, Zen Y, Kawashima A, Endo M, Matsumoto Y, Kasashima F, et al. A clinicopathologic study of immunoglobulin G4-related sclerosing disease of the thoracic aorta. J Vasc Surg. 2010;52(6):1587–95.
- Stone JH, Khosroshahi A, Deshpande V, Stone JR. IgG4-related systemic disease accounts for a significant proportion of thoracic lymphoplasmacytic aortitis cases. Arthritis Care Res. 2010;62(3):316–22.
- Cinar I, Wang H, Stone JR. Clinically isolated aortitis: pitfalls, progress, and possibilities. Cardiovasc Pathol. 2017;29:23–32.
- Hamano H, Kawa S, Ochi Y, Unno H, Shiba N, Wajiki M, et al. Hydronephrosis associated with retroperitoneal fibrosis and sclerosing pancreatitis. Lancet. 2002;359(9315):1403–4.
- Zen Y, Nakanuma Y. IgG4-related disease: a cross-sectional study of 114 cases. Am J Surg Pathol. 2010;34(12):1812–9.
- Mizushima I, Inoue D, Yamamoto M, Yamada K, Saeki T, Ubara Y, et al. Clinical course after corticosteroid therapy in IgG4-related aortitis/periaortitis and periarteritis: a retrospective multicenter study. Arthritis Res Ther. 2014;16(4):R156.
- Yamada K, Yamamoto M, Saeki T, Mizushima I, Matsui S, Fujisawa Y, et al. New clues to the nature of immunoglobulin G4-related disease: a retrospective Japanese multicenter study of baseline clinical features of 334 cases. Arthritis Res Ther 2017;19(1):262.
- Wallace ZS, Deshpande V, Mattoo H, Mahajan VS, Kulikova M, Pillai S, et al. IgG4-related disease: clinical and laboratory features in one hundred twenty-five patients. Arthritis Rheumatol. 2015;67(9):2466–75.
- Lin W, Lu S, Chen H, Wu Q, Fei Y, Li M, et al. Clinical characteristics of immunoglobulin G4-related disease: a prospective study of 118 Chinese patients. Rheumatology (Oxford). 2015;54(11):1982–90.
- Chen H, Lin W, Wang Q, Wu Q, Wang L, Fei Y, et al. IgG4-related disease in a Chinese cohort: a prospective study. Scand J Rheumatol. 2014;43(1):70–4.
- Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. A novel clinical entity, IgG4-related disease (IgG4RD): general concept and details. Mod Rheumatol. 2012;22(1):1–14.
- Uchida K, Masamune A, Shimosegawa T, Okazaki K. Prevalence of IgG4-related disease in Japan based on nationwide survey in 2009. Int J Rheumatol. 2012;2012:358371.
- Umehara H, Okazaki K, Masaki Y, Kawano M, Yamamoto M, Saeki T, et al. Comprehensive diagnostic criteria for IgG4-related disease (IgG4-RD), 2011. Mod Rheumatol. 2012;22(1):21–30.
- Topel I. Noninfectious aortitis: what the cardiologist needs to know. Curr Opin Cardiol. 2017;32:692–8.
- Loffler C, Hoffend J, Benck U, Kramer BK, Bergner R. The value of ultrasound in diagnosing extracranial large-vessel vasculitis compared to FDG-PET/CT: a retrospective study. Clin Rheumatol. 2017;36:2079–86.
- Tajima M, Nagai R, Hiroi Y. IgG4-related cardiovascular disorders. Int Heart J. 2014;55(4):287–95.
- Abe A, Takano K, Seki N, Jitsukawa S, Yamamoto M, Takahashi H, et al. The clinical characteristics of patients with IgG4-related disease with infiltration of the labial salivary gland by IgG4-positive cells. Mod Rheumatol. 2014;24(6):949–52.
- Takahashi H, Yamashita H, Morooka M, Kubota K, Takahashi Y, Kaneko H, et al. The utility of FDG-PET/CT and other imaging techniques in the evaluation of IgG4-related disease. Joint Bone Spine. 2014;81(4):331–6.
- Ebe H, Tsuboi H, Hagiya C, Takahashi H, Yokosawa M, Hagiwara S, et al. Clinical features of patients with IgG4-related disease complicated with perivascular lesions. Mod Rheumatol. 2015;25(1):105–9.
- Yabusaki S, Oyama-Manabe N, Manabe O, Hirata K, Kato F, Miyamoto N, et al. Characteristics of immunoglobulin G4-related aortitis/periaortitis and periarteritis on fluorodeoxyglucose positron emission tomography/computed tomography co-registered with contrast-enhanced computed tomography. EJNMMI Res 2017;7(1):20.
- Menezes LJ, Kotze CW, Hutton BF, Endozo R, Dickson JC, Cullum I, et al. Vascular inflammation imaging with 18F-FDG PET/CT: when to image? J Nucl Med. 2009;50(6):854–7.
- Tezuka D, Haraguchi G, Ishihara T, Ohigashi H, Inagaki H, Suzuki J, et al. Role of FDG PET-CT in Takayasu arteritis: sensitive detection of recurrences. JACC Cardiovasc Imaging. 2012;5(4):422–9.
- Kanzaki Y, Morita H, Ishizaka N. Increased (18)F-FDG uptake in IgG4-related coronary periarterial pseudotumor. Intern Med. 2017;56(12):1603–4.
- Nakatani K, Nakamoto Y, Togashi K. Utility of FDG PET/CT in IgG4-related systemic disease. Clin Radiol. 2012;67(4):297–305.
- Shimosegawa T, Kanno A. Autoimmune pancreatitis in Japan: overview and perspective. J Gastroenterol. 2009;44(6):503–17.
- Masaki Y, Sugai S, Umehara H. IgG4-related diseases including Mikulicz’s disease and sclerosing pancreatitis: diagnostic insights. J Rheumatol. 2010;37(7):1380–5.
- Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 2011;40(3):352–8.
- Umehara H, Okazaki K, Kawano M, Mimori T, Chiba T. How to diagnose IgG4-related disease. Ann Rheum Dis. 2017;76(11):e46.
- Umehara H, Okazaki K, Nakamura T, Satoh-Nakamura T, Nakajima A, Kawano M, et al. Current approach to the diagnosis of IgG4-related disease - Combination of comprehensive diagnostic and organ-specific criteria. Mod Rheumatol. 2017;27(3):381–91.
- Ishizaka N, Fujinaga Y, Hourai R, Fujisaka T, Sohmiya K. Prevalence of elevated serum IgG4 level among patients diagnosed or suspected with cardiovascular disorders. J Jpn Coll Angiol. 2017;57(6):91–8.
- Koo BS, Koh YW, Hong S, Kim YJ, Kim YG, Lee CK, et al. Frequency of immunoglobulin G4-related aortitis in cases with aortic resection and their clinical characteristics compared to other aortitises. Int J Rheum Dis. 2014;17(4):420–4.
- Qian Q, Kashani KB, Miller DV. Ruptured abdominal aortic aneurysm related to IgG4 periaortitis. N Engl J Med. 2009;361(11):1121–3.
- Palmisano A, Corradi D, Carnevali ML, Alberici F, Silini EM, Gatti R, et al. Chronic periaortitis associated with membranous nephropathy: clues to common pathogenetic mechanisms. Clin Nephrol. 2010;74(6):485–90.
- Byeon K, Han J, Kim JS, Kim WS, Choe YH, Lee EJ, et al. Immunoglobulin G4-related periaortitis mimicking an intramural hematoma. Ann Thorac Surg. 2011;92(4):1506–8.
- Trinidad-Hernandez M, Duncan AA. Contained ruptured paravisceral aortic aneurysm related to immunoglobulin G4 aortitis. Ann Vasc Surg. 2012;26(108):e101–4.
- Shu HJ, Tan B, Xue HD, Yang AM, Qian JM. IgG4-related sclerosing cholangitis with autoimmune pancreatitis and periaortitis: case report and review of the literature. J Dig Dis. 2012;13(5):280–6.
- Sarac M, Marjanovic I, Bezmarevic M, Zoranovic U, Petrovic S, Mihajlovic M. An aortoduodenal fistula as a complication of immunoglobulin G4-related disease. World J Gastroenterol. 2012;18(42):6164–7.
- Lipton S, Warren G, Pollock J, Schwab P. IgG4-related disease manifesting as pachymeningitis and aortitis. J Rheumatol. 2013;40(7):1236–8.
- Agaimy A, Weyand M, Strecker T. Inflammatory thoracic aortic aneurysm (lymphoplasmacytic thoracic aortitis): a 13-year-experience at a German Heart Center with emphasis on possible role of IgG4. Int J Clin Exp Pathol. 2013;6:1713–22.
- Laco J, Podhola M, Kamarádová K, Novák I, Dobeš D, Broďák M, et al. Idiopathic vs. secondary retroperitoneal fibrosis: a clinicopathological study of 12 cases, with emphasis to possible relationship to IgG4-related disease. Virchows Arch. 2013;463(5):721–30.
- Monti S, Crepaldi G, Peri A, Pietrabissa A, Morbini P, Bobbio-Pallavicini F, et al. Perivascular fibrosis and IgG4-related disease: a case report. Reumatismo 2014;66(3):245–8.
- Colombier S, Ruchat P, Gronchi F, Pretre R, Niclauss L. Surgical procedure in immunoglobulin G4-related ascending aortitis?. Ann Thorac Surg. 2014;97(4):e111–3.
- Rossi M, Virgilio E, Laurino F, Orgera G, Mene P, Pirozzi N, et al. Giant hepatic artery aneurysm associated with immunoglobulin G4-related disease successfully treated using a liquid embolic agent. Korean J Radiol. 2015;16(4):953–4.
- Maleszewski JJ, Tazelaar HD, Horcher HM, Hinkamp TJ, Conte JV, Porterfield JK, et al. IgG4-related disease of the aortic valve: a report of two cases and review of the literature. Cardiovasc Pathol. 2015;24(1):56–9.
- Tran MN, Langguth D, Hart G, Heiner M, Rafter A, Fleming SJ, et al. IgG4-related systemic disease with coronary arteritis and aortitis, causing recurring critical coronary ischemia. Int J Cardiol. 2015;201:33–4.
- Anandh U, Virarkar M, Shah A, Hastak M. Immunoglobin G4-related disease: two case reports and review of the recent literature. Saudi J Kidney Dis Transpl. 2015;26(6):1282–8.
- Tay DZ, Goh PY, Teo TK, Boey ML, Chachlani N, Wong PS. Immunoglobulin G4-related aortitis mimicking an intramural hematoma. Asian Cardiovasc Thorac Ann. 2015;23(9):1083–6.
- Koo BS, Koh YW, Hong S, Kim YJ, Kim YG, Lee CK, et al. Clinicopathologic characteristics of IgG4-related retroperitoneal fibrosis among patients initially diagnosed as having idiopathic retroperitoneal fibrosis. Mod Rheumatol. 2015;25(2):194–8.
- Loffler C, Hoffend J, Rebel M, Waldherr R, Uppenkamp M, Bergner R. A rare cause for lower back pain: a case of an IgG4-related periaortitis. Clin Rheumatol. 2016;35(1):265–70.
- Niaz A, Ahmad AH, Saeed MA, Sabir O, Tarif N. IgG4-related retroperitoneal fibrosis: a case report and review of literature. J Pak Med Assoc. 2016;66(2):220–2.
- Jun H, Jung CW. Immunoglobulin G4-related inflammatory abdominal aortic aneurysm associated with myasthenia gravis, with contained rupture. Vasc Endovascular Surg. 2016;50(8):571–4.
- Lalueza A, Ruiz S, Villacampa F, Lopez R, Zabia E, Sarandeses P, et al. Recurrent aortitis associated with IgG4-related disease. Circ J. 2016;80(4):1044–6.
- Lindsay D, Ismajli M, Bucknall R, Lipscomb G, Boyle JJ, Mason JC, et al. Simultaneous presentation of IgG4-related chronic peri-aortitis and coeliac disease in a patient with Marfan’s Syndrome. Rheumatology (Oxford). 2016;55(6):1141–3.
- Moore DW, Hansen NJ, DiMaio DJ, Harrison WL. The great imitator: IgG4 periaortitis masquerading as an acute aortic syndrome on computed tomographic angiography. Radiol Case Rep. 2016;11(4):287–91.
- Fernandes B, Anacleto R, Carvalho L. IGG4 disease and slerosing aortitis. Rev Port Cir Cardiotorac Vasc. 2017;24(3–4):162.
- Sanchez-Alvarez C, Bowman AW, Menke DM, Wang B. IgG4 isolated retroperitoneal fibrosis and aneurysmal periaortitis. Am J Med. 2017;130(12):e521–4.
- Aguirre V, Connolly C, Stuklis R. IgG4-aortopathy: an underappreciated cause of non-infectious thoracic aortitis. Heart Lung Circ. 2017;26(11):e79–81.
- Marlin ES, Dornbos D III, Ikeda DS, Lehman NL, Powers CJ. IgG4-related disease: a new etiology underlying diffuse intracranial dilating vasculopathy. World Neurosurg. 2017;107:1048 e1015–e1020.
- Unlu O, Schulman E, Wolff SD, Narula N, Stone JH, Bass A, et al. Immunoglobulin G4-related aortitis: a clinical pathology conference held by the division of rheumatology at the hospital for special surgery. HSS J. 2017;13(3):307–12.
- Cha MJ, Chong S, Kim YS, Park B, Seo JH, Lee ES. Immunoglobulin G4-related periaortitis involving the aortic arch mimicking a mediastinal tumor. Ann Thorac Surg. 2017;103(3):e267–70.
- Terzic B, Spasic M, Djuric P, Vasiljevic V, Radjen S, Mijuskovic M. Retroperitoneal fibrosis and constrictive pericarditis-IgG4 related diseases: a case report. Exp Ther Med. 2017;13(6):3603–6.
- Barbu M, Lindstrom U, Nordborg C, Martinsson A, Dworeck C, Jeppsson A. Sclerosing aortic and coronary arteritis due to IgG4-related disease. Ann Thorac Surg. 2017;103(6):e487–9.
- Almeqdadi M, Al-Dulaimi M, Perepletchikov A, Tomera K, Jaber BL. Rituximab for retroperitoneal fibrosis due to IgG4-related disease: a case report and literature review. Clin Nephrol Case Stud. 2018;6(01):4–10.
- Luis M, Brites L, Fernandes B, Jesus D, Santiago T, Serra S, et al. The many faces of IgG4-related disease: report of a case with inaugural recurrent aortic aneurism ruptures and literature review. Rheumatol Int. 2018;38:1565–1570.
- Houghton DC, Troxell ML. An abundance of IgG4+ plasma cells is not specific for IgG4-related tubulointerstitial nephritis. Mod Pathol. 2011;24(11):1480–7.
- Strehl JD, Hartmann A, Agaimy A. Numerous IgG4-positive plasma cells are ubiquitous in diverse localised non-specific chronic inflammatory conditions and need to be distinguished from IgG4-related systemic disorders. J Clin Pathol. 2011;64(3):237–43.
- Virk R, Shinagare S, Lauwers GY, Yajnik V, Stone JH, Deshpande V. Tissue IgG4-positive plasma cells in inflammatory bowel disease: a study of 88 treatment-naive biopsies of inflammatory bowel disease. Mod Pathol. 2014;27(3):454–9.
- Chang SY, Keogh K, Lewis JE, Ryu JH, Yi ES. Increased IgG4-positive plasma cells in granulomatosis with polyangiitis: a diagnostic pitfall of IgG4-related disease. Int J Rheumatol. 2012;2012:1.
- Chang SY, Keogh KA, Lewis JE, Ryu JH, Cornell LD, Garrity JA, et al. IgG4-positive plasma cells in granulomatosis with polyangiitis (Wegener’s): a clinicopathologic and immunohistochemical study on 43 granulomatosis with polyangiitis and 20 control cases. Hum Pathol. 2013;44(11):2432–7.
- Zoshima T, Yamada K, Hara S, Mizushima I, Yamagishi M, Harada K, et al. Multicentric castleman disease with tubulointerstitial nephritis mimicking IgG4-related disease: two case reports. Am J Surg Pathol. 2016;40(4):495–501.
- Siddiquee Z, Zane NA, Smith RN, Stone JR. Dense IgG4 plasma cell infiltrates associated with chronic infectious aortitis: implications for the diagnosis of IgG4-related disease. Cardiovasc Pathol. 2012;21(6):470–5.
- Khosroshahi A, Wallace ZS, Crowe JL, Akamizu T, Azumi A, Carruthers MN, et al. International consensus guidance statement on the management and treatment of IgG4-related disease. Arthritis Rheumatol. 2015;67(7):1688–99.
- Shirakashi M, Yoshifuji H, Kodama Y, Chiba T, Yamamoto M, Takahashi H, et al. Factors in glucocorticoid regimens associated with treatment response and relapses of IgG4-related disease: a multicentre study. Sci Rep. 2018;8:10262.
- Masamune A, Nishimori I, Kikuta K, Tsuji I, Mizuno N, Iiyama T, et al. Randomised controlled trial of long-term maintenance corticosteroid therapy in patients with autoimmune pancreatitis. Gut 2017;66(3):487–94.
- Yamamoto M, Yajima H, Takahashi H, Yokoyama Y, Ishigami K, Shimizu Y, et al. Everyday clinical practice in IgG4-related dacryoadenitis and/or sialadenitis: results from the SMART database. Mod Rheumatol. 2015;25(2):199–204.
- Masaki Y, Matsui S, Saeki T, Tsuboi H, Hirata S, Izumi Y, et al. A multicenter phase II prospective clinical trial of glucocorticoid for patients with untreated IgG4-related disease. Mod Rheumatol. 2017;27(5):849–54.
- Kamisawa T, Shimosegawa T, Okazaki K, Nishino T, Watanabe H, Kanno A, et al. Standard steroid treatment for autoimmune pancreatitis. Gut 2009;58(11):1504–7.
- Kasashima S, Kawashima A, Kasashima F, Endo M, Matsumoto Y, Kawakami K, et al. Immunoglobulin G4-related periaortitis complicated by aortic rupture and aortoduodenal fistula after endovascular AAA repair. J Endovasc Ther. 2014;21(4):589–97.
- Fernandez-Codina A, Martinez-Valle F, Pinilla B, Lopez C, DeTorres I, Solans LR, et al. IgG4-related disease: results from a multicenter Spanish registry. Medicine (Baltimore) 2015;94:e1275.
- Ito H, Kaizaki Y, Noda Y, Fujii S, Yamamoto S. IgG4-related inflammatory abdominal aortic aneurysm associated with autoimmune pancreatitis. Pathol Int. 2008;58(7):421–6.
- Khosroshahi A, Stone JR, Pratt DS, Deshpande V, Stone JH. Painless jaundice with serial multi-organ dysfunction. Lancet. 2009;373(9673):1494.
- Kasashima S, Kasashima F, Kawashima A, Endo M, Matsumoto Y, Kawakami K. Clinical outcomes after endovascular repair and open surgery to treat immunoglobulin G4-related and nonrelated inflammatory abdominal aortic aneurysms. J Endovasc Ther. 2017;24(6):833–45.
- Stone JH, Klearman M, Collinson N. Trial of tocilizumab in giant-cell arteritis. N Engl J Med. 2017;377(15):1494–5.