
ABSTRACT
Introduction: Streptococcus pneumoniae is a leading cause of morbidity and mortality worldwide. Widespread infant vaccination with pneumococcal conjugate vaccines (PCVs) substantially reduced vaccine-serotype pneumococcal disease by direct protection of immunized children and indirect protection of the community via decreased nasopharyngeal carriage and transmission. Essential to grasping the public health implications of pediatric PCV immunization is an understanding of how PCV formulations impact carriage.
Areas covered: Using clinical evidence, this review examines how the immune response to PCVs is associated with subsequent nasopharyngeal carriage reduction in vaccinated infants and toddlers. By combining direct and indirect protection, carriage reduction results in a reduced spread of vaccine serotypes, and eventually, a decrease in vaccine serotype disease incidence in community members of all ages.
Expert opinion: The current review presents some of the aspects that influence the overall impact of PCVs on vaccine-serotype carriage, and thus, spread. The link between reduction of vaccine-serotype carriage and the eventual reduction of vaccine-serotype disease in the wider community is described by comparing data from current PCVs, specifically with respect to their ability to reduce carriage of some cross-reacting serotypes (i.e. 6A versus 6B and 19A versus 19F).
1. Introduction
Streptococcus pneumoniae is a leading cause of morbidity and mortality worldwide with almost two million deaths annually, including up to one million deaths in children <5 years old [Citation1–Citation3]. Vaccination is one of the most effective methods for preventing pneumococcal disease, not only via protecting vaccinated individuals (direct protection) but also by decreasing the circulation of pneumococcal serotypes included in the vaccines (vaccine serotypes [VTs]) in the population as a whole (indirect or herd protection). Though effective in healthy adults, nonconjugated pneumococcal polysaccharide vaccines do not elicit a protective immune response in children younger than 2 years [Citation4]. To overcome this shortfall, vaccines with conjugated polysaccharides were developed. As well as protecting infants and young children against invasive pneumococcal disease (IPD), these vaccines have shown additional benefits, including the reduced nasopharyngeal carriage of vaccine serotypes. Over the past two decades, the first licensed pneumococcal conjugate vaccine (the 7-valent PCV, PCV7) was introduced into national immunization programs (NIPs) in most countries worldwide [Citation5,Citation6]. PCV7 includes purified capsular polysaccharide of serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F. Although PCV7 protects against disease caused by serotypes in the vaccine [Citation7], pneumococcal nonvaccine serotypes (NVTs) began filling the vacant nasopharyngeal niche [Citation8], leading to a gradual increase in disease caused by some NVTs (a phenomenon known as serotype replacement) [Citation9]. The next-generation 10-valent (PCV10) and 13-valent (PCV13) PCVs replaced PCV7 to combat additional serotypes. PCV10 contains PCV7 serotypes plus serotypes 1, 5, and 7F; PCV13 contains PCV10 serotypes plus serotypes 3, 6A, and 19A [Citation10].
Epidemiologic evidence shows that IPD rates are highest in individuals <5 years of age (in particular, those aged <2 years), the primary target group for pneumococcal vaccination [Citation11–Citation15]. However, when all disease outcomes are considered throughout all ages, >80% of morbidity and mortality occurs in individuals aged >5 years—a population not usually targeted for PCV vaccination. Because pneumococcal transmission occurs most often via contact with infants and toddlers, widespread vaccination of this young age group has the potential to substantially reduce disease across all age cohorts [Citation16] by reducing nasopharyngeal carriage and transmission of VTs. Thus, understanding the prevention of carriage by PCVs in healthy young children is key to predicting PCV impact on public health across all ages.
This review focuses on the available clinical evidence regarding antibody responses after PCV vaccination of infants and young children, protection against carriage of vaccine-related serotypes, and vaccination as related to reducing carriage among vaccinated children. A reduction in the carriage may decrease VT transmission and disease incidence in all ages by a combination of direct and indirect protection.
2. Search strategy and selection criteria
References and data were identified by reviewing publicly available country-specific epidemiology databases, congress materials, the author’s personal files, and PubMed searches (limits, English and 1 January 2000, to 1 January 2018; search terms included ‘IPD,’ ‘carriage,’ ‘19A,’ ‘6A,’ ‘6C,’ and ‘PCV’). Additional references cited in identified articles were reviewed.
It should be noted that serotype 3 is not included in this review, as immunogenicity is poor [Citation17,Citation18] and correlation with carriage therefore cannot be demonstrated.
3. Levels of protection elicited by PCVs
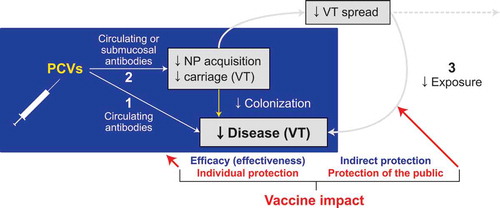
The protection elicited by PCVs against disease caused by VT pneumococci occurs on three levels (). The first is the acquisition of circulating neutralizing antibodies (e.g. serotype-specific immunoglobulin G [IgG]); these antibodies protect against VT pneumococci once they penetrate the infection site. The second level refers to the reduction of nasopharyngeal VT acquisition [Citation19]. Although this is also likely mediated through antipolysaccharide antibodies [Citation19,Citation20], it is not clear whether this protection is afforded by circulating antibodies [Citation21–Citation23] or by locally produced antibodies at the submucosal level [Citation24,Citation25]. Furthermore, it is not clear whether nonantibody-mediated acquired immunity is also involved [Citation26]. However, the serotype specificity of PCV-mediated protection against carriage suggests that mechanisms other than protection by polysaccharide-specific antibodies do not play an important role in PCV-induced protection against carriage, although this may differ for naturally acquired immunity [Citation27]. Nonetheless, reducing nasopharyngeal acquisition in vaccinated subjects affords another level of protection against disease by reducing the risk of pneumococci invading target organs regardless of circulating antibody activity. The third level of protection is afforded by reduction of person-to-person transmission of VT pneumococci, resulting in reduced exposure to these pathogens in vaccinated and unvaccinated individuals. The first two levels of protection are considered individual or direct protection, whereas the third level (reduced exposure) may be termed indirect or societal protection, commonly referred to as ‘herd protection.’ Together, these three protective levels enable PCVs to impact pneumococcal disease in all ages throughout the entire community.
Figure 1. Three levels of protection elicited by PCVs against disease caused by VT pneumococci.
(1) Acquisition of circulating neutralizing antibodies (i.e. serotype-specific immunoglobulin G). (2) Prevention of VT NP acquisition following exposure to the pathogen. (3) Prevention of person-to-person transmission of VT pneumococci. Levels 1 and 2 represent protection of the vaccinated individual, often referred to as direct protection. Level 3 is referred to as indirect or herd protection. NP = nasopharyngeal; PCV = pneumococcal conjugate vaccine; VT = vaccine serotype.
However, immune responses sufficient to afford efficacy against IPD (e.g. septicemia, meningitis, arthritis) alone may not be sufficient to afford acceptable efficacy against all pneumococcal diseases, as most pneumococcal disease is mucosal (e.g. pneumonia, otitis media [OM]). As discussed above, the impact of PCVs on pneumococcal carriage in healthy, asymptomatic children who are responsible for transmitting the bacterium is key to understanding the public health implications of PCV immunization.
The majority of pneumococcal disease is not invasive, but somewhat paradoxically, most knowledge regarding the relationship between immune response and disease relates to IPD. Further complicating this assessment, licensure of new pneumococcal vaccines is based on noninferiority of immune responses, which refers to the relationship between circulating postvaccination IgG antibodies and protection from IPD. The current noninferiority criteria do not account for the relationship between a measurable immune response and protection against carriage and mucosal disease, which is still relatively obscure.
3.1. The current surrogate for noninferiority against IPD does not predict noninferiority against nasopharyngeal carriage
Because effective pneumococcal vaccines have already been licensed, placebo-controlled efficacy studies of subsequent vaccines will meet ethical and practical difficulties; therefore, immunogenicity studies using surrogate markers of efficacy are typically used for licensure of new PCVs [Citation28–Citation30]. Noninferiority of immunogenicity compared with a licensed PCV is determined by comparing the proportion of responders with an IgG concentration equal to or above a surrogate value for protection measured 1 month after three infant doses. The IgG concentration needed for protection against IPD established by the World Health Organization is ≥0.35 µg/mL as measured by serotype-specific pneumococcal polysaccharide enzyme-linked immunosorbent assays (ELISAs) [Citation31–Citation33]. Others use ≥0.2 µg/mL as the surrogate of protection if 22F polysaccharide adsorption is included [Citation34,Citation35].
The protective threshold of ≥0.35 µg/mL was derived from aggregating all seven serotypes in PCV7 from diverse infant populations at three study sites where infants were vaccinated with PCV7 (Northern California, Arizona) or the 9-valent PCV (PCV9), which contains PCV7 serotypes plus serotypes 1 and 5 (South Africa). However, the protective threshold of each serotype and study site varied [Citation20,Citation36,Citation37]. The estimated protective concentrations against the aggregated PCV7 serotypes were 0.20, 1.0, and 0.68 µg/mL for Northern California, Arizona, and South Africa, respectively [Citation33]. Thus, although using a uniform correlate of protection against IPD has enabled licensing of efficacious new PCVs, diversity in a population and serotype-specific correlations should be considered. A postlicensure effectiveness study in the United Kingdom emphasized such serotype diversity [Citation38]. Regardless of the serotype or population examined, the serum antibody concentrations necessary to prevent carriage and mucosal diseases are clearly considerably higher than those needed to protect against IPD, rendering the low threshold of ≥0.35 µg/mL irrelevant for these outcomes.
Limitations of this regulatory approach were highlighted by studies demonstrating an inverse relationship between postvaccination serotype-specific antibody concentrations and the risk of nasopharyngeal pneumococcal acquisition [Citation39–Citation41]. A large double-blind study investigated the relationship between serotype-specific IgG concentration after a three-dose infant PCV7 or PCV13 series (vaccination at 2, 4, and 6 months of age; serum serotype-specific IgG concentrations measured at 7 months of age) and the probability of serotype-specific nasopharyngeal acquisition from age 7 to 24 months [Citation42]. Nasopharyngeal acquisition probability decreased as IgG concentrations increased, reaching statistical significance for serotypes 6A, 6B, 14, and 23F. A nonsignificant but similar pattern was also observed for serotypes 4, 9V, 18C, and 19F. The probability of new acquisitions in children who achieved concentrations of ≥0.35 µg/mL was high, ranging from 65% to 100% for various serotypes, clearly demonstrating that the ≥0.35-µg/mL threshold does not predict protection against carriage. In fact, the predicted acquisition rate was relatively high even when reaching ≥50th percentile of antibody concentrations, and no threshold was demonstrated when reaching concentrations in the 90th percentile [Citation41]. Similar results were observed in a study on the efficacy against acute OM in Finland [Citation43].
Together, these data suggest three important points: (1) the protective threshold for preventing nasopharyngeal acquisition or mucosal disease is considerably higher than that for IPD; (2) variability exists between serotypes in the degree of protection achieved by specific IgG concentrations; and (3) there is an inverse relationship between post-infant series serotype-specific serum IgG concentration and efficacy against nasopharyngeal acquisition rates, with no achievable threshold concentration predicting 90% efficacy. Thus, the post-infant series antibody concentration may approximate the degree of immune stimulation that results in protection against carriage. A recent study reported that the best predictor of protection against nasopharyngeal pneumococcal acquisition is the presence of circulating serotype-specific memory B cells in the blood [Citation44]. Thus, serotype-specific IgG concentrations measured 1 month after vaccination may represent stimulation of memory B cells. It is plausible to speculate that serotype-specific IgG concentrations measured 1 month after vaccination may predict the degree of stimulation to memory B cells.
The studies described above were conducted with a vaccine schedule of 3 + 1 (given at 2, 4, 6, and 12 months of age) and antibody concentrations measured 1 month after completion of the primary series (age 7 months). To date, no published results examining the correlation between postvaccination antibody concentrations and acquisition of carriage have been identified from studies using other vaccine schedules, although it is anticipated that these data are forthcoming [Citation45,Citation46]. However, studies using other schedules have shown an inverse correlation between PCV dose number and carriage acquisition [Citation47–Citation49]. In a study where three doses of PCV7 were given at 2-month intervals starting at age 2 months, efficacy against carriage lasted through the second year for most serotypes. Efficacy was similar in those who did or did not receive a booster dose at 12 months of age, despite a decline in circulating antibody concentrations in children not receiving a booster dose [Citation50].
In contrast to PCVs, nonconjugated polysaccharide pneumococcal vaccines do not afford protection against carriage, despite eliciting high serum IgG concentrations. In one randomized study, a booster with nonconjugated 23-valent pneumococcal polysaccharide vaccine (PPSV23) was compared with placebo in infants previously primed during infancy with one, two, or three PCV7 doses. A brisk increase in antibody concentrations of the PCV7 serotypes was observed after PPSV23 administration, but no effect on carriage was observed [Citation48,Citation51], suggesting that plain polysaccharide booster vaccines do not induce protective antibodies against carriage regardless of the elicited concentrations. Results were consistent with previous studies, suggesting that immunizing vaccine-naive children with PPSV23 or administering a PPSV23 booster does not affect nasopharyngeal carriage in children (in contrast to PCV), despite being immunogenic [Citation52,Citation53]. This difference likely derives from different types of immune response elicited by PCV versus PPSV23 (T-cell dependent vs T-cell independent, respectively) [Citation54].
3.2. Noninferiority, as used for licensure, predicts protection against VT IPD similar to that of a licensed comparator but may mask inferior protection against carriage
Current noninferiority testing required for PCV licensure is not sufficient to predict noninferiority against carriage; thus, the overall potential public health impact of newly licensed vaccines cannot be compared using this method. Considering the data presented above, a PCV eliciting higher serum IgG responses will logically provide better protection against carriage and VT pneumococcal spread, resulting in more effective indirect protection. Alternatively, antibody geometric mean concentrations (GMCs; measured by ELISA) or geometric mean titers (GMTs; measuring functional bactericidal antibody responses by opsonophagocytic activity [OPA]) determined shortly after vaccination are better predictors of efficacy against carriage acquisition than the proportion of vaccine recipients achieving an IgG concentration threshold of ≥0.35 µg/mL [Citation41].
Currently, only two PCVs have been licensed based on the noninferiority principle: PCV13 and PCV10. Although both are noninferior to PCV7 for most serotypes, their effect on carriage is not similar. Studies used for PCV10 licensure that were designed to test noninferiority of PCV10 versus PCV7 [Citation34,Citation35] show the potential limitations of the current assessment method to predict noninferiority for protection against carriage. Specifically, the proportion of children who reached serum IgG concentrations ≥0.20 µg/mL for each serotype was examined to establish noninferiority. Although these proportions were similar for both vaccines for most serotypes (except serotypes 6B and 23F; )) [Citation34,Citation35], the actual serotype-specific IgG concentrations (expressed by their GMCs) showed a large difference for most serotypes, usually in favor of PCV7 () [Citation34,Citation35]. Although these data suggest that direct efficacy of PCV10 and PCV7 against IPD for common serotypes is similar, the data also suggest that PCV7 might better protect against VT carriage.
Figure 2. Differences in inferiority observed when measuring the proportion of children achieving concentrations above threshold vs geometric mean antibody concentrations: A comparison between PCV10 and PCV7.
(a) After the third primary vaccine dose, PCV10 was noninferior to PCV7 for most serotypes using the proportion of subjects achieving a titer of ≥0.20 µg/mL response; the only exceptions were serotypes 6B and 23F. (b) PCV10 was inferior to PCV7 for most serotypes when measuring the geometric mean concentrations of anti-polysaccharide immunoglobulin G; the only exception was serotype 19F. Solid bars, data from Wysocki J, et al. Pediatr Infect Dis J 2009 [Citation34]. Hatched bars, data from Vesikari T, et al. Pediatr Infect Dis J 2009 [Citation35]. ELISA = enzyme-linked immunosorbent assay; PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV.
![Figure 2. Differences in inferiority observed when measuring the proportion of children achieving concentrations above threshold vs geometric mean antibody concentrations: A comparison between PCV10 and PCV7.(a) After the third primary vaccine dose, PCV10 was noninferior to PCV7 for most serotypes using the proportion of subjects achieving a titer of ≥0.20 µg/mL response; the only exceptions were serotypes 6B and 23F. (b) PCV10 was inferior to PCV7 for most serotypes when measuring the geometric mean concentrations of anti-polysaccharide immunoglobulin G; the only exception was serotype 19F. Solid bars, data from Wysocki J, et al. Pediatr Infect Dis J 2009 [Citation34]. Hatched bars, data from Vesikari T, et al. Pediatr Infect Dis J 2009 [Citation35]. ELISA = enzyme-linked immunosorbent assay; PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV.](/cms/asset/d0b72fdd-b319-433d-af81-cd83c84f5409/ierv_a_1627207_f0002_c.jpg)
This suggestion garners support from published information on the efficacy of PCV7 (or its successor, PCV13) and PCV10 (or its precursor, PCV11; ) [Citation42,Citation48,Citation55–Citation61]. When reviewing randomized controlled studies in which efficacy against carriage was examined at 12 months of age in children fully immunized with three infant doses, a pattern toward lower efficacy against VT carriage was observed in PCV10/PCV11 recipients compared with recipients of CRM197-conjugated vaccines (PCV7/PCV13; ). Similar patterns were observed in randomized studies in which children received either two or three doses in infancy and a booster dose toward the second year of life (2 + 1 or 3 + 1 schedule) and for whom efficacy against carriage was tested at various time points during the second year of life (). Although these studies were not designed for direct comparison between vaccines, the findings support the predictions for lower efficacy against VT carriage derived from the immunogenicity studies.
Figure 3. Carriage studies examining the efficacy of CRM197-conjugated vaccines (i.e. PCV7/PCV13) and protein-D conjugated vaccines (i.e. PCV10/PCV11).
(a) All published studies in which PCV was administered as three infant doses, and carriage was measured around 12 months of age, before the toddler dose. (b) All published studies in which PCVs were administered at either two or three doses during infancy, and a booster was administered at around 12 months of age. The age when carriage was measured appears on the y-axis. Several age points were often used for the same study. The circled endpoints are for studies in which children received two doses in infancy. For all others, children received three infant doses. Each circle represents the endpoint efficacy of the vaccine measured against placebo or control vaccine; error bars represent CIs. Adapted from Fleming-Dutra KE, et al. Pediatr Infect Dis J 2014 [Citation55]. Studies on y-axes correspond to: (a) Prymula R, et al. Vaccine 2009 [Citation57]; (b) GlaxoSmithKline COMPAS Study 109563 (10PN-PD-DIT-028) [Citation61]; (c) Vesikari T. European Congress of Clinical Microbiology and Infectious Diseases 2013, Berlin, Germany [Citation56]; (d) Cheung YB, et al. Pediatr Infect Dis J 2009 [Citation58]; (e) Russell FM, et al. Clin Vaccine Immunol 2010 [Citation48]; (f) Dagan R, et al. Clin Infect Dis 2013 [Citation42]; (g) O’Brien KL, et al. J Infect Dis 2007 [Citation59]; (h) Prymula R, et al. Vaccine 2011 [Citation62]; and (i) van Gils EJ, et al. JAMA 2009 [Citation60]. *Data are for the additional six serotypes in PCV13 plus 6C combined. PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV9 = 9-valent PCV; PCV10 = 10-valent PCV; PCV11 = 11-valent PCV; PCV13 = 13-valent PCV; VT = vaccine serotype.
![Figure 3. Carriage studies examining the efficacy of CRM197-conjugated vaccines (i.e. PCV7/PCV13) and protein-D conjugated vaccines (i.e. PCV10/PCV11).(a) All published studies in which PCV was administered as three infant doses, and carriage was measured around 12 months of age, before the toddler dose. (b) All published studies in which PCVs were administered at either two or three doses during infancy, and a booster was administered at around 12 months of age. The age when carriage was measured appears on the y-axis. Several age points were often used for the same study. The circled endpoints are for studies in which children received two doses in infancy. For all others, children received three infant doses. Each circle represents the endpoint efficacy of the vaccine measured against placebo or control vaccine; error bars represent CIs. Adapted from Fleming-Dutra KE, et al. Pediatr Infect Dis J 2014 [Citation55]. Studies on y-axes correspond to: (a) Prymula R, et al. Vaccine 2009 [Citation57]; (b) GlaxoSmithKline COMPAS Study 109563 (10PN-PD-DIT-028) [Citation61]; (c) Vesikari T. European Congress of Clinical Microbiology and Infectious Diseases 2013, Berlin, Germany [Citation56]; (d) Cheung YB, et al. Pediatr Infect Dis J 2009 [Citation58]; (e) Russell FM, et al. Clin Vaccine Immunol 2010 [Citation48]; (f) Dagan R, et al. Clin Infect Dis 2013 [Citation42]; (g) O’Brien KL, et al. J Infect Dis 2007 [Citation59]; (h) Prymula R, et al. Vaccine 2011 [Citation62]; and (i) van Gils EJ, et al. JAMA 2009 [Citation60]. *Data are for the additional six serotypes in PCV13 plus 6C combined. PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV9 = 9-valent PCV; PCV10 = 10-valent PCV; PCV11 = 11-valent PCV; PCV13 = 13-valent PCV; VT = vaccine serotype.](/cms/asset/662b9aa2-2f63-4a2f-a0b9-7c9f85ac7995/ierv_a_1627207_f0003_c.jpg)
4. Serotype-specific efficacy against pneumococcal carriage of a cross-reacting serotype: lessons learned from serotypes 6B versus 6A and 19F versus 19A
4.1. Prelicensure studies
PCV7 and PCV10 were developed with the expectation that the protective anticapsular antibodies induced by serotypes in the vaccine could also protect against related, potentially cross-reacting serotypes. Specifically, antibodies generated against vaccine serotypes 6B and 19F present in PCV7 and PCV10 were anticipated to be sufficient to protect against colonization and disease caused by the related serotypes 6A and 19A. Such cross-protection was shown for serotype 6A in infants fully vaccinated with PCV7 or PCV10 against IPD [Citation63–Citation65]; in addition, some limited data suggested that PCV10 may protect against IPD caused by serotype 19A [Citation65–Citation67]. However, because cross-protection needs higher antibody levels of the parent polysaccharide antigen (i.e., protection against serotype 19A carriage by anti-serotype 19F antibodies) and because an overall higher level of antibodies is needed to protect against carriage than against IPD, the cross-protection afforded against IPD that is needed may not suffice to protect against carriage.
Head-to-head immunogenicity studies comparing immune responses directed against serotypes 6A and 19A elicited by PCV7, PCV10, and PCV13 clearly demonstrated that antibody responses elicited by PCV13 were higher than PCV7 and PCV10 as measured by OPA GMTs () and IgG GMCs [Citation34,Citation35,Citation68–Citation76]. Responses to PCV7 were somewhat better than PCV10 for cross-reactive immunity against serotype 6A; conversely, responses to PCV10 were somewhat better than PCV7 for cross-reactive immunity against serotype 19A () [Citation34,Citation35,Citation68,Citation77]. However, responses elicited by PCV13 were an order of magnitude higher against both serotypes 6A and 19A compared with PCV7 and PCV10 [Citation72]. In addition, a recent study comparing the 2 + 1 schedule of PCV10 and PCV13 showed that postbooster opsonic activity was significantly higher for PCV13 for five of the 10 common serotypes (i.e. 4, 6B, 7F, 9V, and 23F; PCV10/PCV13 ratios 0.22–0.72) and for the additional PCV13 serotypes (0.08, 0.03, and 0.04 for serotypes 3, 6A and 19A, respectively) versus PCV10 [Citation76]. As the effect on mucosal infections and carriage may depend on higher antibody concentrations than for IPD, these differences suggest a higher potential immune response for PCV13 compared with PCV10 for the six common and three additional vaccine serotypes [Citation76]. Moreover, a recent study examining IgG and B-cell responses among humans challenged with S. pneumoniae suggested that serotype-specific circulating memory B-cell responses (but not IgG) are associated with natural protection against carriage [Citation44]. Importantly, serotype 6A and 19A memory B cells were frequently higher in PCV13 recipients than in PCV10 recipients both before and after booster dose administration [Citation78].
Table 1. Immunogenicity of serotypes 19A and 6A using OPA assays from clinical studies comparing PCV7, PCV10, and PCV13.
Nevertheless, it is important to note that studies suggest that PCV7 vaccination does provide some protection against serotype 6A carriage [Citation42,Citation79] and OM [Citation42,Citation80]. However, given markedly higher antibody responses to serotypes 6A and 19A by PCV13 compared with PCV7 and PCV10, it is predicted that PCV13 will provide the best protection against serotype 6A and 19A carriage [Citation42,Citation69,Citation70,Citation81,Citation82].
Still, the question remains: Are the lower immune responses elicited by cross-reacting serotypes in PCV10 sufficient to reduce carriage of serotypes 6A and 19A? A convincing answer to this question derives from randomized studies comparing efficacy against serotype 6A and 19A carriage by PCV13 versus PCV10 (in Papua New Guinea), PCV10 versus PCV7 (in the Netherlands), and PCV13 versus PCV7 (in Israel) (data for serotype 19A shown in ) [Citation42,Citation83,Citation84]. In the Papua New Guinea study [Citation84], PCV10 or PCV13 was given as a three-dose series at 1, 2, and 3 months of age; carriage was examined prior to and at 1 and 6 months following the third vaccine dose. Compared with PCV13 recipients, PCV10 recipients had a higher prevalence of 19A carriage at both post-vaccination time points. However, the number of isolates was too small to determine statistical significance. In the Netherlands and Israel studies, PCVs were given as a three-dose infant series, with a booster toward the second year of life (3 + 1); carriage was examined at multiple age points. Whereas serotype 19A carriage acquisition and prevalence were significantly lower in PCV13 than in PCV7 recipients ()) [Citation42], serotype 19A carriage was not significantly different at any point in PCV10 compared with PCV7 recipients () [Citation83]. Similar findings were found for serotype 6A [Citation42,Citation83]. Studies directly comparing the efficacy of PCV13 versus PCV10 against 6A and 19A carriage with significant carriage outcome to permit statistical significance are lacking. However, since the studies in Israel and the Netherlands compared PCV13 and PCV10, respectively, each to PCV7, this allowed use of PCV7 as the bridging element for comparison. In a double-blind, placebo-controlled study in Finland, PCV10 was more effective than placebo against serotype 19A in one single age point with a 3 + 1 schedule but at no age point with a 2 + 1 schedule. A summary of other studies supports the suggestion that PCV10 may have negligible or even detrimental effects on carriage of serotype 19A [Citation85]. For serotype 6A, no reduction in carriage at any age point was demonstrated with any of these schedules [Citation86]. Importantly, PCV13 reduced serotype 6C carriage due to higher titers of cross-protective antibodies against serotype 6A [Citation42]; this could not be achieved by PCV7 or PCV10, which only contain antigen against serotype 6B and not 6A. These studies strongly suggest that the antibody responses to 6B and 19F in PCV10 and PCV7 may not be sufficient to reduce serotype 6A and 19A nasopharyngeal carriage to a similar level as the actual 6A and 19A antigens in PCV13.
Figure 4. Cross-protection induced by cross-reactive serotype antigens does not provide a similar level of protection to that elicited by the specific serotype antigen against serotype 19A carriage: results of two double-blind studies.
(a) Results of a double-blind study comparing PCV13 and PCV7 for 19A carriage in Israel. Adapted from Dagan R, et al. Clin Infect Dis 2013 [Citation42]. (b) Results of a study comparing the efficacy of PCV10 and PCV7 on 19A carriage in the Netherlands. Adapted from van den Bergh MR, et al. Clin Infect Dis 2013 [Citation83]. PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV; PCV13 = 13-valent PCV.
![Figure 4. Cross-protection induced by cross-reactive serotype antigens does not provide a similar level of protection to that elicited by the specific serotype antigen against serotype 19A carriage: results of two double-blind studies.(a) Results of a double-blind study comparing PCV13 and PCV7 for 19A carriage in Israel. Adapted from Dagan R, et al. Clin Infect Dis 2013 [Citation42]. (b) Results of a study comparing the efficacy of PCV10 and PCV7 on 19A carriage in the Netherlands. Adapted from van den Bergh MR, et al. Clin Infect Dis 2013 [Citation83]. PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV; PCV13 = 13-valent PCV.](/cms/asset/80066f20-042b-41ea-8654-532ddfa99db1/ierv_a_1627207_f0004_c.jpg)
4.2. Postlicensure studies
The results of the studies reviewed above examining immunogenicity and efficacy against carriage are consistent with post-PCV introduction carriage studies () [Citation42,Citation83,Citation86–Citation111]. For example, in Kenya, PCV10 was introduced into the NIP in January 2011 [Citation87]. PCV10 was not only unable to reduce serotype 6A and 19A carriage, but carriage of these two serotypes actually increased after PCV10 introduction, as expected from an NVT serotype [Citation87]. Following the introduction of PCV10 in Fiji in October 2012, annual cross-sectional studies to 2015 showed that carriage of 19A increased in infants aged 5 to 8 weeks and 12 to 23 months but did not change significantly in children aged 2 to 6 years [Citation108]. In contrast, carriage of serotype 6A remained unchanged in the infant and toddler age groups and decreased significantly in 2- to 6-year-old children over the same time period. A surveillance study in the Netherlands examining carriage 7 years after the implementation of PCV7/PCV10 did not support PCV10-induced cross-protection against serotype 19A carriage in children or their parents. At 2 years after PCV10 introduction, serotype 19A was mainly reduced in 24-month-old children vaccinated with PCV7, rather than in younger children who received PCV10 [Citation112]. Three years after PCV10 introduction in Brazil, serotypes 6C, 6A, and 19A were the first, second, and sixth most prevalent carriage serotypes in healthy children aged 12 to 23 months [Citation103]. Similarly, a study in New Zealand evaluating pneumococcal carriage 3 years after PCV10 introduction reported increased carriage of serotypes 19A and 6C compared with the PCV7 period. These two serotypes ranked first and second in carriage prevalence in healthy children <3 years of age [Citation101].
Table 2. Postlicensure PCV10 and PCV13 studies assessing the effect of vaccination on serotype 19A, 6A, and 6C carriage.
In contrast to PCV10, the results of several PCV13 postlicensure studies demonstrated a rapid impact on the carriage of serotypes 19A, 6A, and 6C (). Following PCV13 licensure in the United States in February 2010 and introduction into national recommendations in March 2010 for children aged 6 weeks through 71 months [Citation113], a study showed a substantial decrease in serotype 19A carriage from 26% in 2010 to 3% in 2013 among children aged 6 to 59 months presenting to an emergency department in Atlanta, Georgia [Citation92]. Similarly, in Italy, where PCV13 was introduced in mid-2010, serotype 19A was identified at the end of 2011 in only 9% of nasopharyngeal swab isolates from unvaccinated children, 12% from PCV7 recipients, and none from PCV13 recipients; for serotype 6A, these percentages were 5%, 1%, and 0%, respectively [Citation93].
In the United Kingdom, PCV7 was replaced by PCV13 in April 2010. In 217 households from July 2012 to March 2013, only one unvaccinated adult was found to carry serotype 19A; the respective data for serotype 6A were not reported [Citation99]. Another study comparing carriage 4 years before and 3 years after PCV13 introduction reported a significant decrease in the carriage of serotypes 19A and 6A in children ≤4 years of age by 2013. Serotype 6C carriage fluctuated but returned to 2006 levels by 2013 [Citation106]. In Israel, the proportion of children carrying 6A decreased by 90% from the early PCV7 period to the post-PCV13 period. For the five additional PCV13 serotypes excluding 6A (i.e. 1, 3, 5, 7F, and 19A), carriage declined by 66% [Citation107]. In The Gambia, serotype 6A pneumococcal carriage in infants after PCV13 introduction decreased from 15.3% to 5.7%, although 19A carriage decreases were more modest (8.3% to 6.3%) [Citation98]. In the Aboriginal population in Australia, PCV7 was recommended from 2001 to 2009 (three doses, with a PPSV23 booster). A 3 + 1 PCV10 schedule was used in the Northern Territory only from October 2009 to October 2011, while all other states and territories used PCV7 until they switched to a 3 + 0 PCV13 series beginning in 2011 [Citation114]. In a study comparing carriage in young children across the three periods (all children in the study received the respective vaccines in each period), serotypes 19A, 6A, and 6C were not reduced in the PCV10 period when compared with the PCV7 period, but they were significantly reduced after PCV13 introduction [Citation89,Citation100].
Shortly after the introduction of PCV13 to Lao PDR in late 2013, carriage of serotype 6A decreased both in unvaccinated infants (i.e. aged 5 to 8 weeks) and in toddlers, whereas 6C decreased only in toddlers and 19A carriage did not change significantly in either age group [Citation115].
5. Reduced efficacy against VT carriage predicts lower impact on VT disease across ages
Given the studies reviewed above, a reduced immune response to a PCV may logically result in reduced efficacy against VT carriage, which in turn may lead to a lower ability to afford indirect protection. To date, no head-to-head comparative studies have been conducted between PCVs to validate this hypothesis. However, insights can be garnered by comparing post-PCV implementation data on IPD in all ages. If the above hypothesis is correct, in the presence of similar vaccination rates in infants and toddlers, the more immunogenic vaccine should have a greater impact on VT IPD through indirect protection in all ages.
Widespread PCV7 introduction was associated with a substantial reduction in diseases caused by VT serotypes, but a more complex picture was observed for the cross-protecting serotypes 6A and 19A. For example, PCV7 rapidly reduced serotype 6A disease in the vaccinated population, but disease reduction in the nonvaccinated population was incomplete, demonstrating a reduced impact on serotype 6A carriage [Citation116,Citation117]. In most countries using PCV7, a clear increase in serotype 19A carriage and disease was observed; serotype 19A was actually the most successful replacing serotype in all age groups [Citation63,Citation116–Citation118]. Furthermore, shortly after PCV7 introduction, it was discovered that what was thought to be a pure serotype 6A actually consisted of two cross-reacting serotypes, 6A and 6C [Citation119,Citation120]. Although antibodies to serotype 6B were protective against serotype 6A IPD, and to a lesser extent carriage [Citation116,Citation117], antibodies to serotype 6B were not of sufficient concentration to protect against disease or carriage of serotype 6C [Citation120]. This resulted in significant post-PCV7 increases in 6C carriage and disease in all ages [Citation121–Citation124].
For the cross-reacting serotype 19A, some cross-protection was described against IPD caused by this serotype in children fully vaccinated with PCV10 [Citation118,Citation125,Citation126]; however, this was not shown for mucosal disease or carriage. In fact, while early post-PCV10 introduction studies in the Netherlands [Citation127] and Finland [Citation65] suggested a reduction of serotype 19A diseases in young children, longer follow-up showed that for both children and adults, serotype 19A IPD rates were higher after PCV10 introduction [Citation126,Citation128]. In contrast to PCV7 and PCV10, after implementation of PCV13, a rapid and marked reduction in disease from and carriage of serotypes 6A and 19A was observed, as well as a reduction in cross-reactive serotype 6C [Citation38,Citation90,Citation97,Citation129–Citation139].
When attempting to compare PCV13 and PCV10 for the differences in the impact on serotypes 19A and 6A in all ages, one must include only countries for which data on IPD are thoroughly collected and vaccine uptake is high. Examining such studies clearly demonstrated the dichotomy between the two vaccines regarding their impact on serotypes 19A, 6A, and 6C IPD in all ages () [Citation104,Citation118,Citation126,Citation127,Citation134,Citation136,Citation140–Citation151]. In Australia and Finland, for example, IPD caused by serotypes 19A and 6C increased after PCV10 introduction; however, PCV13 was associated with a rapid and marked decrease in IPD caused by these serotypes in multiple countries among all ages [Citation104,Citation134,Citation136,Citation142,Citation143]. An exception is Ireland, where serotype 19A IPD remained unchanged in children <5 years of age and increased slightly in those ≥5 years of age after PCV13 implementation, the reason for which is unknown [Citation144]. For serotype 6A, IPD was generally reduced with both vaccines in young children, but the impact on disease in the elderly was less apparent for PCV10 than for PCV13 [Citation104,Citation118,Citation126,Citation134,Citation136,Citation140–Citation144].
Table 3. Impact of PCV10 and PCV13 against IPD caused by serotypes 19A, 6A, and 6C across all ages in countries with robust surveillance.
The differential impact of PCV10 and PCV13 on serotype 19A IPD in six countries is illustrated in [Citation118,Citation125,Citation126,Citation134]. The figure clearly shows a sharp decline in IPD caused by serotype 19A both in children <5 years of age (mainly by direct protection through vaccination) and in those >5 years of age (primarily elderly individuals ≥65 years of age by indirect protection) in the three countries using PCV13 (Israel, United Kingdom, and United States). In contrast, in the three countries using PCV10, IPD caused by serotype 19A increased in both children and the elderly, with a sharper and more dynamic increase in the elderly resulting from the increase in carriage of serotype 19A in vaccinated children. A similar, although less dramatic, pattern was observed with serotype 6A (Supplementary Figure 1) [Citation125,Citation126,Citation134], which was reduced in young children but less clearly in those >5 years of age (primarily adults).
Figure 5. Differential impact on serotype 19A IPD post-PCV10 vs post-PCV13 implementation in six countries: three countries post-PCV13 introduction (Israel, United States, United Kingdom) and three countries post-PCV10 introduction (Chile, New Zealand, Finland).
(a) Number of cases of serotype 19A IPD in children <5 years of age between 2004 and 2016. (b) Number of cases of serotype 19A IPD in individuals ≥5 years of age between 2004 and 2016. Vertical dashed lines denote the implementation year of PCV7, PCV10, or PCV13. Vaccination with PCV10 was conducted in Chile and Finland per 3 + 1 and 2 + 1 schedules, respectively. Data are adapted from (a) Israel National Surveillance. Personal communication to Ron Dagan; (b) Moore MR, et al. Lancet Infect Dis 2015 [Citation134]; (c) S. Ladhani, Pediatric Infectious Disease, Public Health England, London, UK, personal communication, 12/30/2017; (d) Pan American Health Organization. SIREVA II (Sistema de Redes de Vigilancia de los Agentes Responsables do Neumonias y Meningitis Bacterianas) [Citation125]; (e) Public Health Surveillance. Information for New Zealand Public Health Action. Invasive Pneumococcal Disease Reports [Citation118]; and (f) National Institute for Health and Welfare. Incidence of Invasive Pneumococcal Disease in Finland [Citation126]. *Number of cases (scale) per country differs. †Threshold for Chile is <2 years and ≥2 years of age. §Surveillance years may span January–December or July–June. IPD = invasive pneumococcal disease; PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV; PCV13 = 13-valent PCV.
![Figure 5. Differential impact on serotype 19A IPD post-PCV10 vs post-PCV13 implementation in six countries: three countries post-PCV13 introduction (Israel, United States, United Kingdom) and three countries post-PCV10 introduction (Chile, New Zealand, Finland).(a) Number of cases of serotype 19A IPD in children <5 years of age between 2004 and 2016. (b) Number of cases of serotype 19A IPD in individuals ≥5 years of age between 2004 and 2016. Vertical dashed lines denote the implementation year of PCV7, PCV10, or PCV13. Vaccination with PCV10 was conducted in Chile and Finland per 3 + 1 and 2 + 1 schedules, respectively. Data are adapted from (a) Israel National Surveillance. Personal communication to Ron Dagan; (b) Moore MR, et al. Lancet Infect Dis 2015 [Citation134]; (c) S. Ladhani, Pediatric Infectious Disease, Public Health England, London, UK, personal communication, 12/30/2017; (d) Pan American Health Organization. SIREVA II (Sistema de Redes de Vigilancia de los Agentes Responsables do Neumonias y Meningitis Bacterianas) [Citation125]; (e) Public Health Surveillance. Information for New Zealand Public Health Action. Invasive Pneumococcal Disease Reports [Citation118]; and (f) National Institute for Health and Welfare. Incidence of Invasive Pneumococcal Disease in Finland [Citation126]. *Number of cases (scale) per country differs. †Threshold for Chile is <2 years and ≥2 years of age. §Surveillance years may span January–December or July–June. IPD = invasive pneumococcal disease; PCV = pneumococcal conjugate vaccine; PCV7 = 7-valent PCV; PCV10 = 10-valent PCV; PCV13 = 13-valent PCV.](/cms/asset/ca58eef4-f45e-4989-883f-d2580a9b10fb/ierv_a_1627207_f0005_c.jpg)
As noted above, there are substantial differences between PCV10 and PCV13 in their impact on the carriage of serotypes 19A, 6A, and 6C in vaccinated children, and thus on indirect protection. These observations can be used as the proof-of-concept for the direct link between PCV-induced antibody concentration, carriage, and overall community protection against pneumococcal diseases. The overall disease caused by these three serotypes is sizeable, especially in countries using PCV10, but much of the IPD in all ages is still caused mainly by NVTs that increase after PCV introduction [Citation126,Citation131]. In a phenomenon known as serotype replacement, VT serotype carriage decreases and NVT carriage increases after PCV implementation [Citation8,Citation9]. Indeed, IPD caused by NVT increased post-PCV implementation, especially in the elderly [Citation126,Citation134]. Currently, more than 6 years after PCV13 and PCV10 implementation, the disease and carriage replacement by NVT has not yet reached steady-state [Citation102,Citation141,Citation145]. Therefore, it is possible that overall IPD rates in the frailest elderly and those at highest risk for IPD may not reflect the benefits derived from the infant vaccination programs until a steady-state is achieved.
6. Conclusion
This review provides links between the degree of immune responses to PCVs, acquisition of carriage, and resulting reductions in vaccine serotype carriage and circulation in the community. The differential impact of PCV10 versus PCV13 on serotype 19A, 6A, and 6C carriage can serve as the proof-of-concept for the relationship between immune response to PCVs and impact on public health. Considering the overall dynamics of pneumococcal serotypes with other microbiota, antibiotics in the community, and environmental conditions, judging the net effect of PCVs on serotype dynamics is difficult. Vigilant and long-term follow-up is needed before firm conclusions can be made regarding the overall impact of PCVs in the community, especially for the frailest individuals.
7. Expert opinion
S. pneumoniae causes substantial morbidity and mortality globally, leading to nearly two million deaths annually and up to one million deaths among those aged <5 years [Citation1–Citation3]. Nasopharyngeal carriage is thought to be a prerequisite for clinically symptomatic pneumococcal infections but is also responsible for the circulation of the pathogens in the community [Citation153]. Young children are the main carrier of vaccine-serotype pneumococci (the serotypes that are most commonly responsible for pneumococcal disease), and thus, are the main source of dissemination of these serotypes in the community [Citation154]. Although the highest incidence of pneumococcal disease is in children <5 years (mainly <2 years of age) [Citation16,Citation153], this age group constitutes only a small cohort; however, by spreading S. pneumoniae in the community, this age group is responsible for high rates of pneumococcal disease in other age cohorts [Citation155] and in the immunocompromised [Citation156].
The introduction of PCV7 (the first licensed PCV) was received with great enthusiasm since it not only protected against IPD caused by the 7 serotypes in the vaccine but also against mucosal disease [Citation79]. Most importantly, PCV7 reduced carriage and spread of the VT7 serotypes, leading to increased protection of all ages [Citation16]. However, at the same time, it rapidly became clear that two main limitations were associated with PCV7 that reduced long-term expectations for the vaccine. The first was the limited number of serotypes in the vaccine (only 7 of the existing >90). The second was the serotype replacement phenomenon, where non-PCV7 serotypes rapidly occupied the nasopharyngeal niche after the seven vaccine serotypes were reduced [Citation8]; this was also associated with an increase in diseases caused by the non-VT serotypes, especially among the immunocompromised [Citation9,Citation156]. These phenomena resulted in extensive investment in research in an attempt to expand the valency of PCVs. However, to date, close to 20 years past implementation of PCV7, the two currently licensed vaccines are still limited to 10 and 13 serotypes (PCV10 and PCV13, respectively).
In this regard, the potential effect of these vaccines on serotypes closely resembling but not identical to those in the vaccines (the so-called ‘cross-reacting serotypes’) generated great interest. By far, the two most common vaccine-related serotypes both in carriage and disease were serotypes 6A and 19A [Citation157,Citation158]. It was clear that cross-protection against serotypes 6A and 19A (which are not constituents of PCV7) can be stimulated by serotypes 6B and 19F (which are included in PCV7), respectively. However, it was not clear whether this cross-protection was sufficient to result in the reduction of carriage and disease caused by serotypes 6A and 19A.
The data discussed in the current review clearly demonstrate that the lack of serotype 19A as an integral antigen in PCV formulations resulted in an insufficient impact on the carriage of 19A, leading to serotype 19A replacement in community-wide carriage and disease. The lack of serotype 6A in PCV formulations led to ambiguous results after PCV7 or PCV10 use because 6A carriage was often but not universally reduced [Citation42,Citation79,Citation83,Citation87]. A recent discovery revealed the emergence of serotype 6C [Citation119], a new serotype that could be cross-protected by serotype 6A but not serotype 6B. Such cross-protection by serotype 6A is possible only if serotype 6A is included in the vaccine [Citation42,Citation120]. Thus, an inherent difference became clear between PCV10, which does not contain serotype 6A, and PCV13, which does contain serotype 6A. Specifically, PCV13 implementation reduced carriage and disease caused by serotypes 19A and 6C in the community in all ages, while PCV10 implementation resulted in an increase in the prevalence of these serotypes. For serotype 6A, the differences are more subtle.
To date, the factors responsible for reduced carriage acquisition of vaccine serotypes afforded by PCVs are not fully understood, but it is clear that the intensity of the immune response (as measured by serotype-specific IgG and memory B cell responses) plays a major role [Citation42,Citation44,Citation69,Citation70,Citation81,Citation82]. Thus, a vaccine that contains more serotype antigens represents one side of the equation for success in reducing diseases in the entire community; on the other side is vaccine immunogenicity as related to serotype-specific memory B cells and antibody stimulation.
Efforts to expand the serotype range in the vaccine are ongoing, as currently extended serotype PCVs are being developing (from PCV15 [Citation159] to PCV20 [Citation160]). Inclusion of additional serotypes will aid further reduction of disease in the community, if the additional serotypes behave similarly to those in the current PCVs. However, the vaccines under development include additional serotypes that are all conjugated to a single carrier (mainly CRM197) [Citation159]. Carrier protein overload with CRM197, which is antigenically related to diphtheria toxoid, presents the risk of interference, especially through the mechanism of carrier-induced epitope suppression [Citation161]. Thus, in theory, the inclusion of more serotypes in a conjugate vaccine may result in lower antibody responses for some serotypes, resulting in reduced protection against carriage. Therefore, studies of vaccines under development must specifically investigate serotype-specific immune responses and their effect on the acquisition of vaccine serotypes. Such analyses will ensure continued community-wide reduction in disease.
Continued surveillance after the implementation of current and future vaccines is crucial to ensure the best protection of the community from pneumococcal diseases.
8. Five-year view
Infant pneumococcal vaccination programs directly protect vaccinated subjects against IPD caused by VTs and confer indirect protection to others through the decreased likelihood of transmission of VT pneumococci. Increased prevalence of IPD caused by NVTs after vaccine introduction places vulnerable populations, such as the elderly, at risk for IPD caused by NVTs due to serotype replacement in younger individuals who are carriers. As higher-valency PCVs are developed and introduced, carriage of all serotypes must be monitored. Similar to the observations regarding PCV13, the greatest protection against carriage for a given serotype is likely to be afforded by a vaccine containing a higher number of the most important serotypes globally. Such a vaccine must also contain the common serotypes included in any older vaccine formulation to maintain protection against the broadest number of serotypes.
Article highlights
Pneumococcal conjugate vaccines (PCVs) protect against invasive pneumococcal disease (IPD), both directly through the acquisition of antibodies and decreased nasopharyngeal carriage and indirectly through decreased person-to-person transmission.
The efficacy of PCVs in reducing acquisition of vaccine-serotype carriage depends on the innate response to PCVs, namely the serotype-specific immunoglobulin G (IgG) response and the serotype-specific memory B-cell response.
The immune responses elicited by cross-reacting serotypes may be insufficient to decrease carriage of vaccine-related serotypes (i.e. serotypes 6A and 6C by serotype 6B in the vaccine, and serotype 19A by serotype 19F in the vaccine).
Considerable differences between PCV10 and PCV13 in the carriage of serotypes 19A and 6C, and to a lesser extent serotype 6A, have been seen in vaccinated children, resulting in differences in indirect protection.
Incidence of IPD caused by nonvaccine serotypes has increased after PCV implementation, particularly in the elderly, necessitating extended-spectrum PCVs—especially those that maintain robust immune response to each serotype in these vaccines.
Assessing the impact of infant PCV programs on nasopharyngeal carriage requires further long-term follow-up.
Declaration of interest
R Dagan has received research grants and consulting and speaker fees from Pfizer; grant and consulting fees from MSD; and consulting fees from MeMed. The author has no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose
Supplemental Material
Download Zip (51.4 KB)Acknowledgments
This work was supported by Pfizer Inc. The sponsor had no involvement in the study design; collection, analysis, and interpretation of the data; or the writing of the report. R Dagan confirms he had full access to all data and has the final responsibility for the decision to submit the manuscript for publication. Editorial/medical writing support was provided by Nicole Gudleski O’Regan, PhD, and Jill E. Kolesar, PhD, at Complete Healthcare Communications, LLC (North Wales, PA), a CHC Group company, and was funded by Pfizer Inc.
Supplemental material
Supplemental data for this article can be accessed here.
Additional information
Funding
References
- World Health Organization. Pneumococcal conjugate vaccine for childhood immunization–WHO position paper. Wkly Epidemiol Rec. 2007;82:93–104.
- World Health Organization. Estimated Hib and pneumococcal deaths for children under 5 years of age, 2008. [ cited 2018 August 27]. Available from: http://www.who.int/immunization/monitoring_surveillance/burden/estimates/Pneumo_hib/en/
- O’Brien KL, Wolfson LJ, Watt JP, et al. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet. 2009;374:893–902.
- Centers for Disease Control and Prevention. Pneumococcal disease. CDC Pink Book. 2015;13:279–296.
- GAVI Alliance. Countries approved for support: 51 countries approved for pneumococcal vaccine support (PCV). [ cited 2014 June 30]. Available from: http://www.gavialliance.org/results/countries-approved-for-support/
- Snape MD, Philip J, John TM, et al. Bactericidal antibody persistence 2 years after immunization with 2 investigational serogroup B meningococcal vaccines at 6, 8 and 12 months and immunogenicity of preschool booster doses: a follow-on study to a randomized clinical trial. Pediatr Infect Dis J. 2013;32:1116–1121.
- Oosterhuis-Kafeja F, Beutels P, Van Damme P. Immunogenicity, efficacy, safety and effectiveness of pneumococcal conjugate vaccines (1998-2006). Vaccine. 2007;25:2194–2212.
- Spijkerman J, van Gils EJ, Veenhoven RH, et al. Carriage of Streptococcus pneumoniae 3 years after start of vaccination program, the Netherlands. Emerg Infect Dis. 2011;17:584–591.
- Weinberger DM, Malley R, Lipsitch M. Serotype replacement in disease after pneumococcal vaccination. Lancet. 2011;378:1962–1973.
- Choi EH, Kim KH, Kim YJ, et al. Recommendation for use of the newly introduced pneumococcal protein conjugate vaccines in Korea. Korean J Pediatr. 2011;54:146–151.
- Health Protection Agency. Invasive pneumococcal disease incidence rate per 100,000 population by age grouping England and Wales. 1996-2005. [cited 2018 Aug 27]. Available from: http://webarchive.nationalarchives.gov.uk/20140714084352/http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1195733823380?p=1203409671876
- Ho PL, Chiu SS, Cheung CH, et al. Invasive pneumococcal disease burden in Hong Kong children. Pediatr Infect Dis J. 2006;25:454–455.
- McIntyre P, Gilmour R, Watson M. Differences in the epidemiology of invasive pneumococcal disease, metropolitan NSW, 1997-2001. N S W Public Health Bull. 2003;14:85–89.
- Jokinen C, Heiskanen L, Juvonen H, et al. Incidence of community-acquired pneumonia in the population of four municipalities in eastern Finland. Am J Epidemiol. 1993;137:977–988.
- Centers for Disease Control and Prevention. Chapter 11: pneumococcal - manual for the surveillance of vaccine-preventable diseases. [ cited 2018 August 27]. Available from: http://www.cdc.gov/vaccines/pubs/surv-manual/chpt11-pneumo.html
- Klugman KP. Herd protection induced by pneumococcal conjugate vaccine. Lancet Glob Health. 2014;2:e365–366.
- Silva-Costa C, Brito MJ, Pinho MD, et al. Pediatric complicated pneumonia caused by Streptococcus pneumoniae serotype 3 in 13-valent pneumococcal conjugate vaccinees, Portugal, 2010-2015. Emerg Infect Dis. 2018;24:1307–1314.
- Cohen O, Knoll M, O’Brien K, et al. Pneumococcal Conjugate Vaccine (PCV) product assessment. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health; 2017.
- Dagan R, Givon-Lavi N, Zamir O, et al. Reduction of nasopharyngeal carriage of Streptococcus pneumoniae after administration of a 9-valent pneumococcal conjugate vaccine to toddlers attending day care centers. J Infect Dis. 2002;185:927–936.
- Black S, Shinefield H, Fireman B, et al. Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser Permanente Vaccine Study Center Group. Pediatr Infect Dis J. 2000;19:187–195.
- Nurkka A, Ahman H, Korkeila M, et al. Serum and salivary anti-capsular antibodies in infants and children immunized with the heptavalent pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2001;20:25–33.
- Korkeila M, Lehtonen H, Ahman H, et al. Salivary anti-capsular antibodies in infants and children immunised with Streptococcus pneumoniae capsular polysaccharides conjugated to diphtheria or tetanus toxoid. Vaccine. 2000;18:1218–1226.
- Kauppi M, Eskola J, Kayhty H. Anti-capsular polysaccharide antibody concentrations in saliva after immunization with Haemophilus influenzae type b conjugate vaccines. Pediatr Infect Dis J. 1995;14:286–294.
- Ada G. Vaccines and vaccination. N Engl J Med. 2001;345:1042–1053.
- Clutterbuck EA, Lazarus R, Yu LM, et al. Pneumococcal conjugate and plain polysaccharide vaccines have divergent effects on antigen-specific B cells. J Infect Dis. 2012;205:1408–1416.
- Malley R, Trzcinski K, Srivastava A, et al. CD4+ T cells mediate antibody-independent acquired immunity to pneumococcal colonization. Proc Natl Acad Sci U S A. 2005;102:4848–4853.
- Lipsitch M, Whitney CG, Zell E, et al. Are anticapsular antibodies the primary mechanism of protection against invasive pneumococcal disease? PLoS Med. 2005;2:e15.
- Gardner SE, Anderson DC, Webb BJ, et al. Evaluation of Streptococcus pneumoniae type XIV opsonins by phagocytosis-associated chemiluminescence and a bactericidal assay. Infect Immun. 1982;35:800–808.
- Brown EJ, Hosea SW, Frank MM. The role of antibody and complement in the reticuloendothelial clearance of pneumococci from the bloodstream. Rev Infect Dis. 1983;5:S797–805.
- Janoff EN, Fasching C, Orenstein JM, et al. Killing of Streptococcus pneumoniae by capsular polysaccharide-specific polymeric IgA, complement, and phagocytes. J Clin Invest. 1999;104:1139–1147.
- Jodar L, Butler J, Carlone G, et al. Serological criteria for evaluation and licensure of new pneumococcal conjugate vaccine formulations for use in infants. Vaccine. 2003;21:3265–3272.
- World Health Organization. WHO Expert Committee on Biological Standardization. World Health Organ Tech Rep Ser. 2005;927:1–154.
- Siber GR, Chang I, Baker S, et al. Estimating the protective concentration of anti-pneumococcal capsular polysaccharide antibodies. Vaccine. 2007;25:3816–3826.
- Wysocki J, Tejedor JC, Grunert D, et al. Immunogenicity of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) when coadministered with different Neisseria meningitidis serogroup C conjugate vaccines. Pediatr Infect Dis J. 2009;28:S77–88.
- Vesikari T, Wysocki J, Chevallier B, et al. Immunogenicity of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) compared to the licensed 7vCRM vaccine. Pediatr Infect Dis J. 2009;28:S66–76.
- O’Brien KL, Moulton LH, Reid R, et al. Efficacy and safety of seven-valent conjugate pneumococcal vaccine in American Indian children: group randomised trial. Lancet. 2003;362:355–361.
- Klugman KP, Madhi SA, Huebner RE, et al. A trial of a 9-valent pneumococcal conjugate vaccine in children with and those without HIV infection. N Engl J Med. 2003;349:1341–1348.
- Andrews NJ, Waight PA, Burbidge P, et al. Serotype-specific effectiveness and correlates of protection for the 13-valent pneumococcal conjugate vaccine: a postlicensure indirect cohort study. Lancet Infect Dis. 2014;14:839–846.
- Dagan R, Givon-Lavi N, Fraser D, et al. Serum serotype-specific pneumococcal anticapsular immunoglobulin G concentrations after immunization with a 9-valent conjugate pneumococcal vaccine correlate with nasopharyngeal acquisition of pneumococcus. J Infect Dis. 2005;192:367–376.
- Millar EV, O’Brien KL, Bronsdon MA, et al. Anticapsular serum antibody concentration and protection against pneumococcal colonization among children vaccinated with 7-valent pneumococcal conjugate vaccine. Clin Infect Dis. 2007;44:1173–1179.
- Dagan R, Juergens C, Trammel J, et al. Modeling pneumococcal nasopharyngeal acquisition as a function of anticapsular serum antibody concentrations after pneumococcal conjugate vaccine administration. Vaccine. 2016;34:4313–4320.
- Dagan R, Patterson S, Juergens C, et al. Comparative immunogenicity and efficacy of 13-valent and 7-valent pneumococcal conjugate vaccines in reducing nasopharyngeal colonization: a randomized double-blind trial. Clin Infect Dis. 2013;57:952–962.
- Jokinen JT, Ahman H, Kilpi TM, et al. Concentration of antipneumococcal antibodies as a serological correlate of protection: an application to acute otitis media. J Infect Dis. 2004;190:545–550.
- Pennington SH, Pojar S, Mitsi E, et al. Polysaccharide-specific memory B cells predict protection against experimental human pneumococcal carriage. Am J Respir Crit Care Med. 2016;194:1523–1531.
- ClinicalTrials.gov. Trial of pneumococcal vaccine schedules in Ho Chi Minh City, Vietnam (NCT01953510). [ cited 2019 April 22]. Available from: https://clinicaltrials.gov/ct2/show/NCT01953510
- Temple B, Toan NT, Uyen DY, et al. Evaluation of different infant vaccination schedules incorporating pneumococcal vaccination (the Vietnam Pneumococcal Project): protocol of a randomised controlled trial. BMJ Open. 2018;8:e019795.
- Dagan R, Givon-Lavi N, Porat N, et al. The effect of an alternative reduced-dose infant schedule and a second year catch-up schedule with 7-valent pneumococcal conjugate vaccine on pneumococcal carriage: a randomized controlled trial. Vaccine. 2012;30:5132–5140.
- Russell FM, Carapetis JR, Satzke C, et al. Pneumococcal nasopharyngeal carriage following reduced doses of a 7-valent pneumococcal conjugate vaccine and a 23-valent pneumococcal polysaccharide vaccine booster. Clin Vaccine Immunol. 2010;17:1970–1976.
- Ota MO, Akinsola A, Townend J, et al. The immunogenicity and impact on nasopharyngeal carriage of fewer doses of conjugate pneumococcal vaccine immunization schedule. Vaccine. 2011;29:2999–3007.
- Dagan R, Givon-Lavi N, Greenberg D. A prospective study to evaluate Streptococcus pneumoniae nasopharyngeal acquisition (SPNA) in the first 30 months of life following a 3-dose primary pneumococcal conjugate vaccine (PCV7) regimen: effect of a booster dose at 12 months of age. Presented at: Interscience Conference on Antimicrobial Agents and Chemotherapy; 2009 September 12-15; San Francisco, CA, USA.
- Russell FM, Licciardi PV, Balloch A, et al. Safety and immunogenicity of the 23-valent pneumococcal polysaccharide vaccine at 12 months of age, following one, two, or three doses of the 7-valent pneumococcal conjugate vaccine in infancy. Vaccine. 2010;28:3086–3094.
- Veenhoven RH, Bogaert D, Schilder AG, et al. Nasopharyngeal pneumococcal carriage after combined pneumococcal conjugate and polysaccharide vaccination in children with a history of recurrent acute otitis media. Clin Infect Dis. 2004;39:911–919.
- Dagan R, Melamed R, Muallem M, et al. Reduction of nasopharyngeal carriage of pneumococci during the second year of life by a heptavalent conjugate pneumococcal vaccine. J Infect Dis. 1996;174:1271–1278.
- Daniels CC, Rogers PD, Shelton CM. A review of pneumococcal vaccines: current polysaccharide vaccine recommendations and future protein antigens. J Pediatr Pharmacol Ther. 2016;21:27–35.
- Fleming-Dutra KE, Conklin L, Loo JD, et al. Systematic review of the effect of pneumococcal conjugate vaccine dosing schedules on vaccine-type nasopharyngeal carriage. Pediatr Infect Dis J. 2014;33:S152–160.
- Vesikari T. Impact of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) on bacterial nasopharyngeal carriage in Finnish children: a cluster-randomized controlled trial. Presented at: ECCMID; 2013 April 27–30; Berlin, Germany.
- Prymula R, Kriz P, Kaliskova E, et al. Effect of vaccination with pneumococcal capsular polysaccharides conjugated to Haemophilus influenzae-derived protein D on nasopharyngeal carriage of Streptococcus pneumoniae and H. influenzae in children under 2 years of age. Vaccine. 2009;28:71–78.
- Cheung YB, Zaman SM, Nsekpong ED, et al. Nasopharyngeal carriage of Streptococcus pneumoniae in Gambian children who participated in a 9-valent pneumococcal conjugate vaccine trial and in their younger siblings. Pediatr Infect Dis J. 2009;28:990–995.
- O’Brien KL, Millar EV, Zell ER, et al. Effect of pneumococcal conjugate vaccine on nasopharyngeal colonization among immunized and unimmunized children in a community-randomized trial. J Infect Dis. 2007;196:1211–1220.
- van Gils EJ, Veenhoven RH, Hak E, et al. Effect of reduced-dose schedules with 7-valent pneumococcal conjugate vaccine on nasopharyngeal pneumococcal carriage in children: a randomized controlled trial. JAMA. 2009;302:159–167.
- GlaxoSmithKline. Clinical study result summary for study no. 109563. COMPAS: a phase III study to demonstrate efficacy of GlaxoSmithKline Biologicals’ 10-valent pneumococcal vaccine (GSK1024850A) against community acquired pneumonia and acute otitis media. [ cited 2018 August 27]. Available from: http://www.gsk-clinicalstudyregister.com/files2/22814666-baca-4916-ae7c-dd54f30ae5ba&rct=j&frm=1&q=&esrc=s&sa=U&ved=0CBQQFjAAahUKEwi6oI_C1vvHAhVDrD4KHemvASw&sig2=BvisfYzQchbtNK1ufwvdwA&usg=AFQjCNFZvacPCdwgoww53KJ2perdONAQOQ
- Prymula R, Hanovcova I, Splino M, et al. Impact of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) on bacterial nasopharyngeal carriage. Vaccine. 2011;29:1959–1967.
- Whitney CG, Pilishvili T, Farley MM, et al. Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: a matched case-control study. Lancet. 2006;368:1495–1502.
- Kyaw MH, Lynfield R, Schaffner W, et al. Effect of introduction of the pneumococcal conjugate vaccine on drug-resistant Streptococcus pneumoniae. N Engl J Med. 2006;354:1455–1463.
- Jokinen J, Rinta-Kokko H, Siira L, et al. Impact of ten-valent pneumococcal conjugate vaccination on invasive pneumococcal disease in Finnish children – a population-based study. PLoS One. 2015;10:e0120290.
- Deceuninck G, De Serres G, Boulianne N, et al. Effectiveness of three pneumococcal conjugate vaccines to prevent invasive pneumococcal disease in Quebec, Canada. Vaccine. 2015;33:2684–2689.
- Domingues CM, Verani JR, Montenegro Renoiner EI, et al. Effectiveness of ten-valent pneumococcal conjugate vaccine against invasive pneumococcal disease in Brazil: a matched case-control study. Lancet Respir Med. 2014;2:464–471.
- Kim CH, Kim JS, Cha SH, et al. Response to primary and booster vaccination with 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine in Korean infants. Pediatr Infect Dis J. 2011;30:e235–243.
- Yeh SH, Gurtman A, Hurley DC, et al. Immunogenicity and safety of 13-valent pneumococcal conjugate vaccine in infants and toddlers. Pediatrics. 2010;126:e493–505.
- Kieninger DM, Kueper K, Steul K, et al. Safety, tolerability, and immunologic noninferiority of a 13-valent pneumococcal conjugate vaccine compared to a 7-valent pneumococcal conjugate vaccine given with routine pediatric vaccinations in Germany. Vaccine. 2010;28:4192–4203.
- Togashi T, Okada K, Yamaji M, et al. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine given with DTap vaccine in healthy infants in Japan. Pediatr Infect Dis J. 2015;34:1096–1104.
- GlaxoSmithKline. Clinical study result summary for study 116485. Immunogenicity and safety study of two formulations of GlaxoSmithKline (GSK) Biologicals’ pneumococcal vaccine (2830929A and 2830930A) when administered in healthy infants. [ cited 2018 August 27]. Available from: https://www.gsk-clinicalstudyregister.com/files2/116485%20-%20Clinical-Study-Result-Summary.pdf
- Wijmenga-Monsuur AJ, van Westen E, Knol MJ, et al. Direct comparison of immunogenicity induced by 10- or 13-valent pneumococcal conjugate vaccine around the 11-month booster in Dutch infants. PLoS One. 2015;10:e0144739.
- Bermal N, Szenborn L, Chrobot A, et al. The 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) coadministered with DTPw-HBV/Hib and poliovirus vaccines: assessment of immunogenicity. Pediatr Infect Dis J. 2009;28:S89–96.
- van Den Bergh MR, Spijkerman J, Francois N, et al. Immunogenicity, safety, and reactogenicity of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine and DTPa-IPV-Hib when coadministered as a 3-dose primary vaccination schedule in The Netherlands: a randomized controlled trial. Pediatr Infect Dis J. 2011;30:e170–178.
- Temple B, Toan NT, Dai VTT, et al. Immunogenicity and reactogenicity of ten-valent versus 13-valent pneumococcal conjugate vaccines among infants in Ho Chi Minh City, Vietnam: a randomised controlled trial. Lancet Infect Dis. 2019;19:497–509.
- Poolman J, Frasch C, Nurkka A, et al. Impact of the conjugation method on the immunogenicity of Streptococcus pneumoniae serotype 19F polysaccharide in conjugate vaccines. Clin Vaccine Immunol. 2011;18:327–336.
- van Westen E, Wijmenga-Monsuur AJ, van Dijken HH, et al. Differential B-cell memory around the 11-month booster in children vaccinated with a 10- or 13-valent pneumococcal conjugate vaccine. Clin Infect Dis. 2015;61:342–349.
- Cohen R, Varon E, Doit C, et al. A 13-year survey of pneumococcal nasopharyngeal carriage in children with acute otitis media following PCV7 and PCV13 implementation. Vaccine. 2015;33:5118–5126.
- Park SY, Moore MR, Bruden DL, et al. Impact of conjugate vaccine on transmission of antimicrobial-resistant Streptococcus pneumoniae among Alaskan children. Pediatr Infect Dis J. 2008;27:335–340.
- Song JY, Moseley MA, Burton RL, et al. Pneumococcal vaccine and opsonic pneumococcal antibody. J Infect Chemother. 2013;19:412–425.
- Juergens C, Patterson S, Trammel J, et al. Post hoc analysis of a randomized double-blind trial of the correlation of functional and binding antibody responses elicited by 13-valent and 7-valent pneumococcal conjugate vaccines and association with nasopharyngeal colonization. Clin Vaccine Immunol. 2014;21:1277–1281.
- van Den Bergh MR, Spijkerman J, Swinnen KM, et al. Effects of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D-conjugate vaccine on nasopharyngeal bacterial colonization in young children: a randomized controlled trial. Clin Infect Dis. 2013;56:e30–39.
- Pomat WS, van Den Biggelaar AHJ, Wana S, et al. Safety and immunogenicity of pneumococcal conjugate vaccines in a high-risk population: a randomised controlled trial of 10-valent and 13-valent PCV in Papua New Guinean infants. Clin Infect Dis. 2018. [Epub ahead of print]
- Isturiz R, Sings HL, Hilton B, et al. Streptococcus pneumoniae serotype 19A: worldwide epidemiology. Expert Rev Vaccines. 2017;16:1007–1027.
- Vesikari T, Forsten A, Seppa I, et al. Effectiveness of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D-conjugated vaccine (PHiD-CV) against carriage and acute otitis media-a double-blind randomized clinical trial in Finland. J Pediatric Infect Dis Soc. 2016;5:237–248.
- Hammitt LL, Akech DO, Morpeth SC, et al. Population effect of 10-valent pneumococcal conjugate vaccine on nasopharyngeal carriage of Streptococcus pneumoniae and non-typeable Haemophilus influenzae in Kilifi, Kenya: findings from cross-sectional carriage studies. Lancet Glob Health. 2014;2:e397–405.
- Andrade AL, Ternes YM, Vieira MA, et al. Direct effect of 10-valent conjugate pneumococcal vaccination on pneumococcal carriage in children Brazil. PLoS One. 2014;9:e98128.
- Leach AJ, Wigger C, Hare K, et al. Reduced middle ear infection with non-typeable Haemophilus influenzae, but not Streptococcus pneumoniae, after transition to 10-valent pneumococcal non-typeable H. influenzae protein D conjugate vaccine. BMC Pediatr. 2015;15:162.
- Lee GM, Kleinman K, Pelton SI, et al. Impact of 13-valent pneumococcal conjugate vaccination on carriage in young children in Massachusetts. J Pediatric Infect Dis Soc. 2014; 3:23–32.
- Loughlin AM, Hsu K, Silverio AL, et al. Direct and indirect effects of PCV13 on nasopharyngeal carriage of PCV13 unique pneumococcal serotypes in Massachusetts’ children. Pediatr Infect Dis J. 2014;33:504–510.
- Desai AP, Sharma D, Crispell EK, et al. Decline in pneumococcal nasopharyngeal carriage of vaccine serotypes after the introduction of the 13-valent pneumococcal conjugate vaccine in children in Atlanta, Georgia. Pediatr Infect Dis J. 2015;34:1168–1174.
- Zuccotti G, Mameli C, Daprai L, et al. Serotype distribution and antimicrobial susceptibilities of nasopharyngeal isolates of Streptococcus pneumoniae from healthy children in the 13-valent pneumococcal conjugate vaccine era. Vaccine. 2014;32:527–534.
- Cohen R, Levy C, Bingen E, et al. Impact of 13-valent pneumococcal conjugate vaccine on pneumococcal nasopharyngeal carriage in children with acute otitis media. Pediatr Infect Dis J. 2012;31:297–301.
- Dunais B, Bruno P, Touboul P, et al. Impact of the 13-valent pneumococcal conjugate vaccine on nasopharyngeal carriage of Streptococcus pneumoniae among children attending group daycare in southeastern France. Pediatr Infect Dis J. 2015;34:286–288.
- Felix S, Valente C, Tavares D, et al. Temporal trends of serotypes included in the novel 13-valent pneumococcal conjugate vaccine (PCV13) among young children from Portugal. Presented at: ISPPD; 2012 March 11-15; Iguaçu Falls, Brazil.
- Ben-Shimol S, Greenberg D, Givon-Lavi N, et al. Early impact of sequential introduction of 7-valent and 13-valent pneumococcal conjugate vaccine on IPD in Israeli children <5 years: an active prospective nationwide surveillance. Vaccine. 2014;32:3452–3459.
- Roca A, Bojang A, Bottomley C, et al. Effect on nasopharyngeal pneumococcal carriage of replacing PCV7 with PCV13 in the Expanded Programme of Immunization in The Gambia. Vaccine. 2015;33:7144–7151.
- Van Hoek AJ, Sheppard CL, Andrews NJ, et al. Pneumococcal carriage in children and adults two years after introduction of the thirteen valent pneumococcal conjugate vaccine in England. Vaccine. 2014;32:4349–4355.
- Leach AJ, Wigger C, Beissbarth J, et al. General health, otitis media, nasopharyngeal carriage and middle ear microbiology in Northern Territory Aboriginal children vaccinated during consecutive periods of 10-valent or 13-valent pneumococcal conjugate vaccines. Int J Pediatr Otorhinolaryngol. 2016;86:224–232.
- Best EJ, Walls T, Souter M, et al. Pneumococcal vaccine impact on otitis media microbiology: a New Zealand cohort study before and after the introduction of PHiD-CV10 vaccine. Vaccine. 2016;34:3840–3847.
- Wyllie AL, Wijmenga-Monsuur AJ, van Houten MA, et al. Molecular surveillance of nasopharyngeal carriage of Streptococcus pneumoniae in children vaccinated with conjugated polysaccharide pneumococcal vaccines. Sci Rep. 2016;6:23809.
- Brandileone MC, Zanella RC, Almeida SC, et al. Effect of 10-valent pneumococcal conjugate vaccine on nasopharyngeal carriage of Streptococcus pneumoniae and Haemophilus influenzae among children in Sao Paulo, Brazil. Vaccine. 2016;34:5604–5611.
- Galanis I, Lindstrand A, Darenberg J, et al. Effects of PCV7 and PCV13 on invasive pneumococcal disease and carriage in Stockholm, Sweden. Eur Respir J. 2016;47:1208–1218.
- Collins DA, Hoskins A, Snelling T, et al. Predictors of pneumococcal carriage and the effect of the 13-valent pneumococcal conjugate vaccination in the Western Australian Aboriginal population. Pneumonia (Nathan). 2017;9:14.
- Devine VT, Cleary DW, Jefferies JM, et al. The rise and fall of pneumococcal serotypes carried in the PCV era. Vaccine. 2017;35:1293–1298.
- Ben-Shimol S, Givon-Lavi N, Greenberg D, et al. Pneumococcal nasopharyngeal carriage in children <5 years of age visiting the pediatric emergency room in relation to PCV7 and PCV13 introduction in southern Israel. Hum Vaccin Immunother. 2016;12:268–276.
- Dunne EM, Satzke C, Ratu FT, et al. Effect of ten-valent pneumococcal conjugate vaccine introduction on pneumococcal carriage in Fiji: results from four annual cross-sectional carriage surveys. Lancet Glob Health. 2018;6:e1375–e1385.
- Sigurdsson S, Erlendsdóttir H, Quirk SJ, et al. Pneumococcal vaccination: direct and herd effect on carriage of vaccine types and antibiotic resistance in Icelandic children. Vaccine. 2017;35:5242–5248.
- Brandileone M-C, Zanella RC, Almeida SCG, et al. Effect of 10-valent pneumococcal conjugate vaccine on nasopharyngeal carriage of Streptococcus pneumoniae and Haemophilus influenzae among children in São Paulo, Brazil. Vaccine. 2016;34:5604–5611.
- Hammitt LL, Akech DO, Morpeth SC, et al. Population impact of 10-valent pneumococcal conjugate vaccine (PCV10) on nasopharyngeal carriage of Streptococcus pneumoniae in Kilifi, Kenya. Presented at: 11th International Symposium on Pneumococci & Pneumococcal Diseases (ISPPD-11); 2018 April 15-18; Melbourne, Australia.
- Bosch AA, van Houten MA, Bruin JP, et al. Nasopharyngeal carriage of Streptococcus pneumoniae and other bacteria in the 7th year after implementation of the pneumococcal conjugate vaccine in the Netherlands. Vaccine. 2016;34:531–539.
- Centers for Disease Control and Prevention. Licensure of a 13-valent pneumococcal conjugate vaccine (PCV13) and recommendations for use among children - Advisory Committee on Immunization Practices (ACIP), 2010. MMWR Recomm Rep. 2010;59:258–261.
- National Centre for Immunisation Research & Surveillance (NCIRS). Significant events in pneumococcal vaccination practice in Australia. [cited 2019 June 7]. Available from: http://www.ncirs.org.au/sites/default/files/2018-11/Pneumococcal-history-August-2018.pdf
- Satzke C, Dunne EM, Choummanivong M, et al. Pneumococcal carriage in vaccine-eligible children and unvaccinated infants in Lao PDR two years following the introduction of the 13-valent pneumococcal conjugate vaccine. Vaccine. 2019;37:296–305.
- Pilishvili T, Lexau C, Farley MM, et al. Sustained reductions in invasive pneumococcal disease in the era of conjugate vaccine. J Infect Dis. 2010;201:32–41.
- Hicks LA, Harrison LH, Flannery B, et al. Incidence of pneumococcal disease due to non-pneumococcal conjugate vaccine (PCV7) serotypes in the United States during the era of widespread PCV7 vaccination, 1998-2004. J Infect Dis. 2007;196:1346–1354.
- Public Health Surveillance. Information for New Zealand Public Health Action. Invasive pneumococcal disease reports. [ cited 2018 August 27]. Available from: https://surv.esr.cri.nz/surveillance/IPD.php
- Park IH, Pritchard DG, Cartee R, et al. Discovery of a new capsular serotype (6C) within serogroup 6 of Streptococcus pneumoniae. J Clin Microbiol. 2007;45:1225–1233.
- Cooper D, Yu X, Sidhu M, et al. The 13-valent pneumococcal conjugate vaccine (PCV13) elicits cross-functional opsonophagocytic killing responses in humans to Streptococcus pneumoniae serotypes 6C and 7A. Vaccine. 2011;29:7207–7211.
- Jacobs MR, Bajaksouzian S, Bonomo RA, et al. Occurrence, distribution, and origins of Streptococcus pneumoniae serotype 6C, a recently recognized serotype. J Clin Microbiol. 2009;47:64–72.
- Nahm MH, Lin J, Finkelstein JA, et al. Increase in the prevalence of the newly discovered pneumococcal serotype 6C in the nasopharynx after introduction of pneumococcal conjugate vaccine. J Infect Dis. 2009;199:320–325.
- Nunes S, Valente C, Sa-Leao R, et al. Temporal trends and molecular epidemiology of recently described serotype 6C of Streptococcus pneumoniae. J Clin Microbiol. 2009;47:472–474.
- Park IH, Moore MR, Treanor JJ, et al. Differential effects of pneumococcal vaccines against serotypes 6A and 6C. J Infect Dis. 2008;198:1818–1822.
- Pan American Health Organization. SIREVA II (Sistema de Redes de Vigilancia de los Agentes Responsables do Neumonias y Meningitis Bacterianas). [ cited 2018 August 27]. Available from: https://www.paho.org/hq/index.php?option=com_content&view=article&id=5536:2011-sireva-ii&Itemid=3966&lang=en
- National Institute for Health and Welfare. Incidence of invasive pneumococcal disease in Finland. [ cited 2018 August 27]. Available from: https://www.thl.fi/en/web/thlfi-en/research-and-expertwork/projects-and-programmes/monitoring-the-population-effectiveness-of-pneumococcal-conjugate-vaccination-in-the-finnish-national-vaccination-programme/incidence-of-invasive-pneumococcal-disease-in-finland
- Knol MJ, Wagenvoort GH, Sanders EA, et al. Invasive pneumococcal disease 3 years after introduction of 10-valent pneumococcal conjugate vaccine, the Netherlands. Emerg Infect Dis. 2015;21:2040–2044.
- National Institute for Public Health and the Environment. The national immunisation programme in the Netherlands. Surveillance and developments in 2015-2016. [ cited 2018 August 27]. Available from: http://www.rivm.nl/dsresource?objectid=a5cbbe78-1d6e-4263-a214-7fee39b5e287&type=pdf&disposition=inline
- Demczuk WH, Martin I, Griffith A, et al. Serotype distribution of invasive Streptococcus pneumoniae in Canada after the introduction of the 13-valent pneumococcal conjugate vaccine, 2010-2012. Can J Microbiol. 2013;59:778–788.
- Wei SH, Chiang CS, Chiu CH, et al. Pediatric invasive pneumococcal disease in Taiwan following a national catch-up program with the 13-valent pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2015;34:e71–77.
- Waight PA, Andrews NJ, Ladhani SN, et al. Effect of the 13-valent pneumococcal conjugate vaccine on invasive pneumococcal disease in England and Wales 4 years after its introduction: an observational cohort study. Lancet Infect Dis. 2015;15:535–543.
- Harboe ZB, Dalby T, Weinberger DM, et al. Impact of 13-valent pneumococcal conjugate vaccination in invasive pneumococcal disease incidence and mortality. Clin Infect Dis. 2014;59:1066–1073.
- Kaplan SL, Barson WJ, Lin PL, et al. Early trends for invasive pneumococcal infections in children after the introduction of the 13-valent pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2013;32:203–207.
- Moore MR, Link-Gelles R, Schaffner W, et al. Effect of use of 13-valent pneumococcal conjugate vaccine in children on invasive pneumococcal disease in children and adults in the USA: analysis of multisite, population-based surveillance. Lancet Infect Dis. 2015;15:301–309.
- Iroh Tam PY, Madoff LC, Coombes B, et al. Invasive pneumococcal disease after implementation of 13-valent conjugate vaccine. Pediatrics. 2014;134:210–217.
- Steens A, Bergsaker MA, Aaberge IS, et al. Prompt effect of replacing the 7-valent pneumococcal conjugate vaccine with the 13-valent vaccine on the epidemiology of invasive pneumococcal disease in Norway. Vaccine. 2013;31:6232–6238.
- Olarte L, Barson WJ, Barson RM, et al. Impact of the 13-valent pneumococcal conjugate vaccine on pneumococcal meningitis in US children. Clin Infect Dis. 2015;61:767–775.
- Fenoll A, Granizo JJ, Gimenez MJ, et al. Secular trends (1990-2013) in serotypes and associated non-susceptibility of S. pneumoniae isolates causing invasive disease in the pre-/post-era of pneumococcal conjugate vaccines in Spanish regions without universal paediatric pneumococcal vaccination. Vaccine. 2015;33:5691–5699.
- Lefebvre B Programme de surveillance du pneumocoque: rapport 2013. [ cited 2018 August 27]. Available from: https://www.inspq.qc.ca/pdf/publications/1946_Programme_Surveillance_Pneumocoque.pdf
- Instituto de Salud Publica de Chile. Boletin Instituto de Salud Publica de Chile. Julio 2015. Vigilancia de laboratorio de Streptococcus pneumoniae procedente de enfermedad invasora. Chile, 2007–2015. [cited 2018 Aug 27]. Available from: http://www.ispch.cl/sites/default/files/Boletín%20de%20Vigilancia%20de%20Laboratorio%20de%20Streptococcus%20pneumoniae.pdf
- Instituto de Salud Publica de Chile. Boletin Instituto de Salud Publica de Chile. Junio 2016. Vigilancia de laboratorio de Streptococcus pneumoniae procedente enfermedad invasora. Chile, 2010–2016. [cited 2018 Aug 27]. Available from: http://www.ispch.cl/sites/default/files/BoletinPneumo-27092016C_0.pdf
- Australian Government Department of Health. Invasive pneumococcal disease surveillance 2016. [ cited 2016 October 10]. Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/cda-surveil-nndss-ipd-reports.htm
- Australian Government Department of Health. Pneumococcal disease (invasive) public dataset. [ cited 2016 October 10]. Available from: http://www9.health.gov.au/cda/source/pub_pneum.cfm
- Health Protection Surveillance Centre. Annual epidemiological report (Ireland). [ cited 2018 August 27]. Available from: http://www.hpsc.ie/AboutHPSC/AnnualReports/
- Regev-Yochay G, Katzir M, Strahilevitz J, et al. The herd effects of infant PCV7/PCV13 sequential implementation on adult invasive pneumococcal disease, six years post implementation; a nationwide study in Israel. Vaccine. 2017;35:2449–2456.
- Knol MJ, De Melker HE, Sanders EAM, et al. Incidence of IPD in the Netherlands up to five years after introduction of PCV10. Presented at: 10th International Symposium on Pneumococci and Pneumococcal Diseases; Glasgow, Scotland, United Kingdom; 2016.
- von Gottberg A, de Gouveia L, Tempia S, et al. Effects of vaccination on invasive pneumococcal disease in South Africa. N Engl J Med. 2014;371:1889–1899.
- Richter L, Schmid D, Kanitz EE, et al. Invasive pneumococcal diseases in children and adults before and after introduction of the 10-valent pneumococcal conjugate vaccine into the Austrian national immunization program. PLoS One. 2019;14:e0210081.
- Cassiolato AP, Almeida SCG, Andrade AL, et al. Expansion of the multidrug-resistant clonal complex 320 among invasive Streptococcus pneumoniae serotype 19A after the introduction of a ten-valent pneumococcal conjugate vaccine in Brazil. PLoS One. 2018;13:e0208211.
- Lu CY, Chiang CS, Chiu CH, et al. Successful control of Streptococcus pneumoniae 19A replacement with a catch-up primary vaccination program in Taiwan. Clin Infect Dis. 2019. [Epub ahead of print]
- Pan American Health Organization. SIREVA II regional reports. [ cited 2019 May 15]. Available from: https://www.paho.org/hq/index.php?option=com_content&view=article&id=5536:2011-sireva-ii&Itemid=3966&lang=en
- Leal AL, Montañez AM, Buitrago G, et al. Impact of ten-valent pneumococcal conjugate vaccine introduction on serotype distribution trends in Colombia: an interrupted time-series analysis. Open Forum Infect Dis. 2017;4:S463–S463.
- Simell B, Auranen K, Kayhty H, et al. The fundamental link between pneumococcal carriage and disease. Expert Rev Vaccines. 2012;11:841–855.
- Bogaert D, De Groot R, Hermans PW. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis. 2004;4:144–154.
- Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease study 2010. Lancet. 2012;380:2095–2128.
- Flannery B, Heffernan RT, Harrison LH, et al. Changes in invasive pneumococcal disease among HIV-infected adults living in the era of childhood pneumococcal immunization. Ann Intern Med. 2006;144:1–9.
- Hausdorff WP, Bryant J, Kloek C, et al. The contribution of specific pneumococcal serogroups to different disease manifestations: implications for conjugate vaccine formulation and use, part II. Clin Infect Dis. 2000;30:122–140.
- Hausdorff WP, Yothers G, Dagan R, et al. Multinational study of pneumococcal serotypes causing acute otitis media in children. Pediatr Infect Dis J. 2002;21:1008–1016.
- Sobanjo-Ter Meulen A, Vesikari T, Malacaman EA, et al. Safety, tolerability and immunogenicity of 15-valent pneumococcal conjugate vaccine in toddlers previously vaccinated with 7-valent pneumococcal conjugate vaccine. Pediatr Infect Dis J. 2015;34:186–194.
- Pfizer Inc. Pfizer granted FDA breakthrough therapy designation for 20-valent pneumococcal conjugate vaccine for the prevention of invasive disease and pneumonia in adults aged 18 years and older. [ cited 2019 January 7]. Available from: https://www.pfizer.com/news/press-release/press-release-detail/pfizer_granted_fda_breakthrough_therapy_designation_for_20_valent_pneumococcal_conjugate_vaccine_for_the_prevention_of_invasive_disease_and_pneumonia_in_adults_aged_18_years_and_older
- Dagan R, Poolman J, Siegrist CA. Glycogonjugate vaccines and immune interference: a review. Vaccine. 2010;28:5513–5523.