
ABSTRACT
Objectives
To boost COVID-19 vaccine uptake, an innovative ‘vaccinate my village’ (VMV) strategy using door-to-door vaccination by Health Surveillance Assistants (HSA) was adopted. In this study, we assessed the impact of the ‘vaccinate my village’ strategy on COVID-19 vaccine uptake.
Methods
This was a cross-sectional review of the data on COVID-19 vaccination obtained from the Ministry of Health, Malawi, from 11 March 2021 to September 2022.
Results
From March 2021–4 September 2022,091,551 COVID-19 vaccine doses were administered, out of which 2,253,546 were administered over just six months as a part of VMV as compared to 1,838,005 doses were administered over 13 months as a part of other strategies. The proportion of Malawi’s population receiving at least one dose of the COVID-19 vaccine increased substantially from 4.66 to 15.4 with the implementation of the VMV strategy (p = 0.0001). District-wise coverage of the COVID-19 vaccine also increased significantly after its implementation (p = 0.0001).
Conclusions
Door-to-door vaccination involving HSAs benefitted the COVID-19 vaccination program in Malawi by ensuring accessibility, availability, and acceptability.
1. Introduction
Worldwide, COVID-19 vaccination is an ongoing effort to reach many people quickly. In Malawi, like in other countries, the goal of the COVID-19 vaccination exercise is to vaccinate 70% of the population to achieve herd immunity [Citation1]. Through the Ministry of Health, the government of Malawi launched the COVID-19 vaccination programs on 11 March 2021 with vaccine doses it received from the COVID-19 Vaccine Global Access (COVAX Facility) [Citation2].
Malawi experienced health system pressures to deliver multiple vaccine types, some with very short shelf-lives, while ensuring that health workers were trained on each vaccine’s specificities and vaccines were delivered within their lifetime. Despite the practical challenges, Malawi has made great efforts to increase the vaccine uptake through expanding vaccination sites, ensuring effective use of available stocks, pacing delivery of new vaccine stocks, mobilizing communities and addressing doubts and misinformation, training health workers, and providing additional support for low-performing districts to increase vaccine uptake [Citation3]. To increase coverage of COVID-19 vaccine uptake, the Ministry of Health launched a ‘COVID-19 express strategy’ that hinged on the use of community mobilization and mobile vans to reach out to communities with the COVID-19 vaccine [Citation2].
By 31 March 2022, 1,838,005 doses of the COVID-19 vaccine were administered. Despite all efforts, the national proportion of people vaccinated for COVID-19 among all the 29 health districts continued to be overall low at 4.7%, with Mangochi district as the least performing at 0.7%. This is in contrast to the district’s annual performance of other vaccinations under the Expanded Programme on Immunization (EPI) program, which was one of the best-performing districts in the country at 91%.
A preliminary analysis identified a few reasons behind this low vaccination rate. Firstly, EPI vaccinations are delivered to communities using static, outreach, and door-to-door approaches by community health workers called Health Surveillance Assistants (HSA), contrasting the method of COVID-19 vaccinations delivery was nurse/clinician based. Secondly, the targeted population for COVID-19 vaccines was healthy people aged 18 years and above who were mostly busy with socioeconomic activities. In addition, social media was awash with negative information discouraging the uptake of COVID-19 vaccines. Therefore, only some people would have the required motivation to spend their valuable time visiting health facilities for a COVID-19 vaccine.
Therefore, to boost COVID-19 uptake, we employed an innovative ‘vaccinate my village’ strategy adapted from the existing health campaigns such as Child Health Week and Mass Drug Administration to control and prevent various illnesses. In the ‘vaccinate my village’ (VMV) strategy, we hypothesized that community-based delivery of the COVID-19 vaccine using HSA would be easily accessible to communities since HSAs already work in communities and enjoy community trust in health matters. In addition, using HSAs to give COVID-19 messages on vaccine efficacy and safety will be more effective in parrying away community-negative perceptions and fears. In this study, we assessed the impact of the ‘vaccinate my village’ strategy (door-to-door immunization by using HSAs) on covid vaccine uptake.
2. Material and methods
2.1. Setting
Malawi is an African country with 29 health districts having a total population of 21,507,723 [Citation4]. The majority (63.5%) of the population have low-income levels and live with less than one US Dollar ($) per day [Citation2]. 90% of the population stays in hard-to-reach areas [Citation5]. Moreover, poor or non-existent road networks, rugged terrain, long traveling distance, and a lack of public transport facilities limit access and utilization of health facilities, especially during the rainy season [Citation2]. With no public transport infrastructure, most of the population has to spend around 4–6 US Dollars out of their pocket to reach the nearest health facilities, which makes the covid vaccine out of bounds even if it is provided free of cost [Citation2].
2.2. Study design
The study population involved all people aged 12 years and above eligible for the COVID-19 vaccine. This was a cross-sectional review of the data on COVID-19 vaccination obtained from the Ministry of Health, Malawi.
From 11 March–October 2021 and January–March 2022, the Routine covid vaccination (RCV 1 and 2) strategy involving delivery of vaccine at health centers free of cost by health-care personnel (doctor/nurses), and November–December 2021, the COVID-19 vaccine express (CVE) strategy was followed by ensuring availability and utilization of all components of the Covid-19 vaccination program at one platform near to community settlement area, that is, vaccinator (nursing staff), support staff, vaccines and logistics, risk communication and community engagement (RCEE), drama/street play team, reporting, and recording, particularly in the remote and in-accessible locations of Malawi. This VMV strategy was implemented in all catchment areas of health facilities (rural as well as urban areas) in the country from April to September 2022 (11–16 April 2023–27 May 2013–17 June 2027–30 June 2018–22 July 2022–26 August 2012–17 September).
2.3. Patient and public involvement
Being a retrospective evaluation of government data, patients and the public were not involved.
2.4. Vaccinate my village strategy (VMV)
VMV was a performance-based initiative HSAs in their catchment areas. In the VMV strategy, door-to-door COVID-19 vaccination was done by HSA as opposed to doctors/nurses only in RCV-1/2 or CVE strategy. Motivation in the form of lunch allowances was given to a team of HSAs upon accomplishing the task. The implementation was done through three steps as described below:
Identification and training: The head of Health services in their respective district conducted a one-day orientation of the strategy to the environmental health officers (EHO), who in turn drove a series of orientations for HSA in their respective supervision areas.
Community Risk Communication and Engagement: After the training, EHOs and HSAs conducted community engagement meetings at the village levels of their respective catchment areas targeting the community leaders. The sessions were done within the same period in all the health facilities with the participation of all community residents aged 12 and above.
These meetings addressed the following objectives: a) to assess community members’ knowledge of COVID-19 vaccines, b) to increase the level of knowledge on COVID-19 vaccines services and their importance among community members, c) to clear out misconceptions on COVID-19 vaccines, d) to make community members aware of the potential consequences of not having a COVID-19 vaccine and e) to trigger communities towards utilization of COVID-19 vaccines. Concurrent with these meetings, radio panel discussions anchored by traditional leaders and health workers and COVID-19 promotional jingles were aired on the local community radio stations.
Implementation of the COVID-19 vaccination campaign: Before the actual days of implementation, all the HSAs conducted door-to-door mobilization in all the district villages to make prior bookings to get the COVID-19 vaccines. The district health office ensured the availability of COVID-19 logistics and supplies, including vaccines, to all the health facilities so that they were readily available to all HSAs. During the implementation, HSAs used outreach clinics and door-to-door sessions to reach people in their catchment areas to provide COVID-19 vaccines at people’s homes. Concurrently, supervision was conducted by Senior HSAs and EHOs, targeting a minimum of 4 teams per day.
2.5. Data Collection
Quantitative data collected through daily vaccination reports from HSAs were aggregated at the health facility level by the Senior HSAs and then submitted to the district Health office. Data from Mobile vans were submitted daily to the district health office by the HSAs manning the mobile van.
2.6. Statistical analysis
Collected data were compiled and analyzed using Microsoft Excel 2010 (Microsoft Corporation, Redmond, Washington, USA). Descriptive statistics (mean ± standard deviation with 95% confidence interval (CI)) were calculated for quantitative data related to the consumption dose of all vaccines in all 29 districts of Malawi country. The Shapiro-Wilk and Kolmogorov-Smirnov tests were the first normality tests. Depending upon the results from normality tests, a non-parametric test (Kruskal–Wallis) or parametric test (One-way analysis of variance, ANOVA) was done to compare the RCV 1 and 2, CVE, and VMV. The F value in ANOVA is also calculated to determine the p-value for finding the statistical significance in the variance between the means of two populations (within the group and between the group). The p-values ≤ 0.05 were considered statistically significant.
Population proportions were calculated by dividing the number of people who received a single dose of the COVID-19 vaccine by the total population depending upon national or district population proportion. We collected cumulative monthly consumption of COVID-19 vaccine for all doses (first, second, and booster doses) and all types (AstraZeneca, Jhonson and Jhonson, and covaxin) and calculated the monthly average during each strategy (RCV1, CVE, RCV2, and VMV).
3. Results
From March 2021-September 2022, a total of 4,091,551 COVID-19 vaccine doses were administered, out of which 2,253,546 doses were administered over just six months (April–September 2022) as a part of VMV as compared to 1,838,005 doses were administered over 13 months (11 March 2021–31March 2022) as a part of other strategies (RCV 1, CVE, and RCV 2 combined).
The proportion of Malawi’s population receiving at least one dose of the COVID-19 vaccine increased substantially from 4.66 before the implementation of the VMV strategy to 15.4 after its implementation ().
Table 1. Effect of VMV strategy on national COVID-19 vaccine coverage.
Mann-Whitney U test was used to establish a statistical difference, showed a highly significant difference (p = 0.0001). District-wise coverage of the COVID-19 vaccine was also very low before the implementation of the VMV strategy, which had also increased significantly after its implementation (p = 0.0001) ().
Figure 1. Proportion of population before and after VMV strategy who received a single dose of COVID-19 vaccine.

Comparing the district-wise mean doses of the COVID-19 vaccine administered in the VMV, RCV-1, CVE, and RCV-2 showed that the mean monthly doses administered were higher in VMV than in RCV-1, CVE, and RCV-2 in all the 29 districts ().
Table 2. Comparison of mean doses of COVID-19 vaccine across all 29 districts in four different phases.
Depending upon the results from normality tests, a non-parametric test (Kruskal-Wallis) or parametric test (one-way analysis of variance; ANOVA) was used to establish a statistical difference, which showed a significant difference (p < 0.05) between mean doses administered during VMV strategy as compared to mean doses administered during RCV-1, CVE, and RCV-2 strategy in most of the districts as well as the overall country (). Few districts whose results, although not statistically significant, had higher mean doses administered than other strategies ().
Out of the total doses of the COVID-19 vaccine administered over a period of March 2021-September 2022, the monthly proportion of the COVID-19 vaccine was statistically significant in VMV strategy as compared to RCV 1 and 2 (post-hoc Bonferroni test; p = 0.0001) whereas although high as compared to CVE, but not statistically significant (p = 0.74) (). A comparison of the overall mean monthly doses of the COVID-19 vaccine between VMV with RCV-1, CVE, and RCV-2 also showed a statistically significant difference (p-value = 0.001) ().
Figure 2. Monthly proportion of the COVID-19 vaccine, out of the total consumed doses.
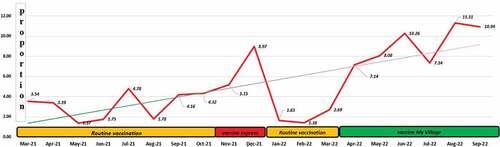
Table 3. A comparison of mean doses of the COVID-19 vaccine between VMV versus RCV-1, CVE, and RCV-2.
4. Discussion
VMV’s strategy ensured the delivery of the vaccine to all parts of the country, including hard-to-reach areas, through outreach clinics and door-to-door sessions by HSAs. This study established the impact of door-to-door vaccination and community-based health workers’ involvement in COVID-19 vaccine uptake. The proportion of Malawi’s population receiving at least one dose of the COVID-19 vaccine increased substantially from 4.66 to 15.4 after implementing the VMV strategy. We also found a steady increase in district-wise population coverage and mean COVID-19 vaccine uptake with VMV. This finding is consistent with studies from India, Bangladesh, Nigeria, and Kenya, where similar interventions were implemented to improve child immunization coverage, especially in rural and hard-to-reach areas [Citation6–9].
Significant variations (over 10% before and after VMV implementation) in vaccine coverage indicate a considerable population unreached with vaccination strategies like RCV-1, CVE, and RCV-2. The effectiveness of the vaccination program depends on the community type to be served and its catchment population for mobilization, planning, and monitoring. Identifying pockets in the community with an unvaccinated population can inform where to invest the constrained resources to improve vaccination coverage and maximize its impact [Citation10,Citation11]. Inequalities in accessing such people can have severe implications for the control and prevention of COVID-19 [Citation12]. ‘One size does not fit all,’ So interventions that are not as per the area’s specific needs may not be adequate [Citation12].
Vaccination in community-based settings near a place of their dwellings, like a place of worship, school, community-based organizations, and door-to-door efforts (like our strategy) can be helpful, particularly for economic disadvantage populations and those residing in hard-to-reach areas to avoid financial loss like loss of earnings due to travel or waiting time to obtain vaccines and transportation costs [Citation8,Citation9,Citation13–15]. In Malawi also, most of the population lives below the poverty line, surviving on less than one US Dollar per day and staying in hard-to-reach areas. Moreover, with no public transport and a poor road network, people must spend around 4–6 US dollars to reach health facilities [Citation2]. This could be one of the primary reasons for low vaccine uptake despite being provided free of cost. VMV has overcome this issue by making the COVID-19 vaccine accessible to this underprivileged population.
The use of HSAs to conduct community-based COVID-19 vaccinations in Malawi was a game changer as it increased vaccine availability, accessibility, and acceptability at the community level. The strong partnership and trust between HSAs and their communities were essential for convincing community leaders and people to accept the messages and vaccinations related to COVID-19. Various studies have shown that advocacy by community health workers (like VMV strategy), community and religious leaders, and community champions is crucial to improving vaccine uptake as it is essential for increased trust and confidence in the vaccination program [Citation16,Citation17].
A systematic review for low‐ and middle‐income countries suggested that, compared to a status quo implementation, paying for performance increases the availability and commitment of health workers to offer the services [Citation18]. The availability of incentives assisted in making the HSAs available to provide the services and have creative ways of mobilizing more people in their communities to take the COVID-19 vaccinations (like in the VMV strategy). However, sustainability measures need to be considered since these monetary incentives were mostly donated by partners. It will likely be challenging to reach the COVID-19 vaccination targets (in the absence of donors) using routine and non-incentivized COVID-19 vaccine delivery mode.
5. Conclusions
Door-to-door vaccination involving HSAs benefitted the COVID-19 vaccination program in rural and difficult-to-reach areas of Malawi by ensuring accessibility, availability, and acceptability.
5.1 Recommendation
The outcome, regarding the benefit, could be used as an advocacy tool to encourage the government to integrate mobile outreach with primary health care in the country. As the difficult-to-reach area continues to exist, marginalized populations of this area are vulnerable to preventable disease. Therefore, planning must be done at respective levels to ensure the sustainability of these outreach programs.
5.2. Limitations
Although this strategy improved COVID-19 vaccine coverage, a cost-benefit analysis of the intervention should be conducted.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or material discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or mending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Data sharing
Data will be made available on request to the corresponding author.
Ethics
This study was exempted from the scientific and ethical review by National Health Sciences Research Committee, Malawi, given data evaluation from the ministry (MED/4/36c dated 21 November 2022).
Author contributions
GS, MNC, LS, PON, BL, KCM, TD, and JP were involved in the implementation and monitoring of the project. LS, SS, and KJ were involved in data analysis. SS, LS, KJ, and KD initially drafted the manuscript. GS, LS, and KD edited the manuscript. All authors have reviewed and approved the final manuscript.
Additional information
Funding
References
- Anderson RM, Vegvari C, Hollingsworth TD, et al. The SARS-CoV-2 pandemic: remaining uncertainties in our understanding of the epidemiology and transmission dynamics of the virus, and challenges to be overcome. Interface Focus. 2021;11(6):20210008.
- Sethy G, Chisema M, Sharma L, et al. COVID-19 vaccine express strategy in Malawi: an effort to reach the un-reach. Vaccine. 2022;40(35):5089–5094.
- Malawi marks one year of COVID-19. vaccination 828,080 people receive full dose. https://www.afro.who.int/countries/malawi/news/malawi-marks-one-year-covid-19-vaccination-828-080-people-receive-full-dose. Cited 2022 Mar 11
- http://www.nsomalawi.mw/index.php?%20option=com_content&view=article&id=136%3Amalawi-table-30-population-by-age-and-sex. Accessed 21 Dec 2010
- 2018. Malawi population and housing census main report. Cited May 2019. https://malawi.unfpa.org/sites/default/files/resource-pdf/2018%20Malawi%20Population%20and%20Housing%20Census%20Main%20Report%20%281%29.pdf
- Uddin MJ, Saha NC, Islam Z, et al. Improving low coverage of child immunization in rural hard-to-reach areas of Bangladesh: findings from a project using multiple interventions. Vaccine. 2012;30(2):168–179.
- Patel AR, Nowalk MP. Expanding immunization coverage in rural India: a review of the evidence for the role of community health workers. Vaccine. 2010;28(3):604–613.
- Bawa S, Shuaib F, Saidu M, et al. Conduct of vaccination in hard-to-reach areas to address potential polio reservoir areas, 2014–2015. BMC Public Health. 2018;18(Suppl4):1312.
- Shikuku DN, Muganda M, Amunga SO, et al. Door-to-door immunization strategy for improving access and utilization of immunization Services in Hard-to-Reach Areas: a case of Migori County, Kenya. BMC Public Health. 2019;19(1):1064.
- World Health Organization. Microplanning for immunization service delivery using the Reaching Every District (RED) strategy. Geneva: WHO; 2009. Cited 2019 Aug 7. https://apps.who.int/iris/bitstream/handle/10665/70450/WHO_IVB_09.11_eng.pdf
- Alfred K, Tabu S, Paul KM, et al. Utilization of essential immunization services among children under five years old in Kacheliba division, Pokot County. Kenya: DSpace Repository for Moi University School of Public Health; 2014. Cited 2014 Nov 11. http://ir.mu.ac.ke:8080/xmlui/handle/123456789/939.
- Lott BE, Okusanya BO, Anderson EJ, et al. Interventions to increase uptake of Human Papillomavirus (HPV) vaccination in minority populations: a systematic review. Prev Med Rep. 2020;19:101163.
- Peterson P, McNabb P, Maddali SR, et al. Engaging communities to reach immigrant and minority populations: the Minnesota Immunization Networking Initiative (MINI), 2006–2017. 433021. 2019;134(3):241–248.
- Rani U, Darabaner E, Seserman M, et al. Public education interventions and uptake of human papillomavirus vaccine: a systematic review. J Public Health Manag Pract. 2022;28(1):E307–15.
- Hutchins SS, Fiscella K, Levine RS, et al. Protection of racial/ethnic minority populations during an influenza pandemic. Am J Public Health. 2009;99(Suppl 2):S261–70.
- Frew PM, Saint-Victor DS, Owens LE, et al. Socioecological and message framing factors influencing maternal influenza immunization among minority women. Vaccine. 2014;32(15):1736–1744.
- Greenfield LS, Page LC, Kay M, et al. Strategies for increasing adolescent immunizations in diverse ethnic communities. J Adolesc Health. 2015;56(5):S47–53.
- Diaconu K, Falconer J, Verbel A, et al. Paying for performance to improve the delivery of health interventions in low- and middle-income countries. Cochrane Database Syst Rev. 2021;5(5):CD007899.