
Abstract
Background
To describe and explore the risk factors, clinical presentations, timely diagnostic approaches, and management in patients experiencing unscarred uterine rupture with catastrophic hemorrhage.
Methods
We retrospectively analyzed clinical and imaging data from women who encountered postpartum hemorrhage (PPH) and were diagnosed with unscarred uterine rupture within a three-year timeframe (2018-2020). The data were extracted from medical records obtained from a multi-hospital 24-hour emergency PPH transfer system.
Results
Six patients were identified as having unscarred uterine rupture after vaginal delivery. All six women were para 2, with four of them undergoing vacuum-assisted delivery. One patient experienced out-of-hospital cardiac arrest (OHCA), while five patients presented with hypovolemic shock. Abdominopelvic ultrasound revealed a boggy lower uterine segment. Initially, five patients underwent transarterial embolization (TAE) of the internal iliac arteries in an attempt to achieve hemostasis, but this approach proved unsuccessful. Abdominopelvic computed tomography (CT) confirmed the diagnosis of ruptured uterus by demonstrating disrupted myometrium and hemoperitoneum. Immediate exploratory laparotomy followed by life-saving hysterectomy was performed in all cases. The median estimated total blood loss was 2725 mL ± 900 mL (ranging from 1600 mL to 7100 mL). Lower segment lacerations were observed in all patients, with more extensive uterine damage noted in those who underwent vacuum extraction. The length of hospital stay varied between 9 and 38 days.
Conclusion
Instrument-assisted obstetric delivery is a possible contributing factor to unscarred uterine rupture in our study. In specific cases, the use of abdominopelvic CT prior to initiating transarterial embolization (TAE) offers valuable information to complement ultrasound findings. This comprehensive approach helps in accurately identifying the underlying cause of intractable postpartum hemorrhage (PPH). Immediate conversion to laparotomy is essential to explore the intra-abdominal factors causing PPH that cannot be controlled by TAE. The rational etiologies of uterine rupture must be clarified while generating practical guideline in the future.
Introduction
Uterine rupture is a life-threatening obstetric emergency associated with significant fetomaternal mortality and morbidity. In most cases, uterine rupture occurs in the presence of a previous uterine scar, typically from a previous cesarean delivery or myomectomy. Theoretically, an unscarred uterus has a low risk of rupture. An extremely low incidence of unscarred uterine rupture has been reported in previous studies, ranging from 0.28–0.58 per 10,000 deliveries [Citation1–4] to 3.8–5.7 per 10,000 births in developing regions [Citation5,Citation6].
Existing information about unscarred uterine rupture is predominantly derived from case series studies, which provide insights into this obstetric event across various clinical settings [Citation4,Citation5,Citation7–9]. Uterine rupture commonly presents with clinical manifestations such as abdominal pain, acute fetal distress, vaginal bleeding, and hypovolemic shock. Although data on this topic is limited, several potential risk factors for uterine rupture have been proposed. These include induction of labor, having multiple previous pregnancies (grand multiparity), the use of oxytocin to augment labor, obstructive labor, abnormal placental implantation, instrumental vaginal deliveries, the presence of a congenital uterine anomaly, macrosomia(a large fetus), and multiple gestation pregnancies [Citation3,Citation10–13]. In addition to the mentioned risk factors, it is worth noting that unscarred uterine ruptures can also occur without any identifiable predisposing factors [Citation14–16]. These cases highlight the unpredictable nature of this complication and emphasize the importance of considering uterine rupture even in the absence of known risk factors.
Due to rare incidences and unexpected nature of unscarred uterine rupture, physicians may inadvertently overlook or inadequately manage postpartum haemorrhage (PPH) by primarily focusing on more commonly presumed etiologies. Challenges in promptly diagnosing uterine rupture have been documented in the literature [Citation17,Citation18]. Timely recognition of uterine rupture can be difficult due to various factors. The clinical presentation of uterine rupture can be nonspecific and overlap with other obstetric emergencies, making it challenging to differentiate from conditions such as placental abruption or uterine atony. Unscarred uterine rupture is associated with higher maternal mortality, and morbidity, defined as major obstetric hemorrhage or peripartum hysterectomy [Citation19,Citation20]. A delayed correct diagnosis is a major risk factor for high maternal morbidity and poor neonatal outcomes [Citation1,Citation21]. The present study aimed to identify the factors contributing to unscarred gravid uterine rupture. Furthermore, the study aimed to explore the clinical presentations commonly observed in cases of uterine rupture and identify effective diagnostic tools that can facilitate early detection and enable timely surgical intervention. By addressing these objectives, the study sought to enhance our understanding of unscarred uterine rupture and contribute to improved management strategies for this obstetric emergency.
Materials and methods
Patient collection and definition
We retrospectively reviewed the medical records of women with rupture of the unscarred gravid uterus managed at Kaohsiung Chang Gung Memorial Hospital during the 3-year period from January 2018 to December 2020. Our data collection focused on postpartum patients who were transferred to our hospital through a well-established 24-hour emergency transfer system during the study period [Citation22]. An unscarred uterus was defined as a uterus that had not undergone any prior invasive procedures that involved disruption of the myometrium, such as cesarean section or myomectomy. Uterine rupture was categorized into two types: complete and incomplete. A complete uterine rupture was characterized by the complete disruption of uterine wall, resulting in a direct communication between the uterine cavity and peritoneal space. On the other hand, an incomplete uterine rupture, also known as uterine dehiscence, was defined as a laceration in which the uterine serosa remained intact. To ensure accurate confirmation of the diagnosis, we conducted a comprehensive review of all medical charts that contained a code for uterine rupture. The confirmation process involved careful examination of intraoperative findings, as well as a thorough evaluation of pathological examination results.
The estimated blood loss was measured by visual estimation of suction canisters, and weighting of blood-soaked gauze, and drapes as determined by the nurse, surgeon or anesthesiology providers. The clinical presentation of haemorrhage was classified according to American college of surgeons (ACS) of acute haemorrhage classification. The grade of blood loss amount was defined by American College of Obstetrician and Gynecologists (ACOG 2010). Grade 0: <500 mL, Grade I: 500–1000 mL, Grade II: > 1000–1500 mL, Grade III: > 1500–2000, and Grade IV: > 2000–3000 mL. Severe blood loss was defined as more than 1500 mL, which leads to hypovolemic shock and disseminated intravascular coagulopathy (DIC) [Citation23–25].
The shock index (SI) is one composite vital sign which may help physician to identify puerperal women with hypovolemic shock [Citation26–28]. The SI was calculated by dividing the heart rate by the systolic blood pressure. In this study, we determined the patients' SI using the vital signs recorded upon their arrival at the triage unit. Additionally, we obtained the post-transarterial embolization (TAE) SI immediately after the TAE procedure. The length of hospitalization was calculated from the day of referral to the day of discharge. To gather comprehensive data for analysis, information on clinical characteristics, risk factors, maternal–fetal outcomes, delivery information, imaging findings, histopathologic reports, and clinical presentations were extracted through an extensive review of medical records. Furthermore, we followed up with the patients through a questionnaire survey conducted via phone calls.
Given the small sample size of only six patients in our study, we utilized descriptive statistics to analyze the data. The institutional review board of Chang Gung Memorial Hospital approved this study (approval no. 202101275B0).
Clinical Management of PPH
Initial assessment on arrival
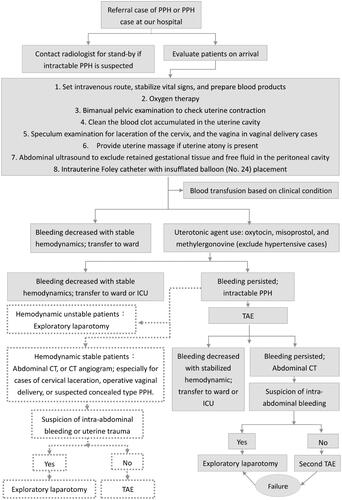
Our study was conducted at a tertiary referral center located in southern Taiwan, which has been offering round-the-clock access to PPH treatment since 2004 [Citation22]. The patients were managed by an interdisciplinary team including specialists in emergency medicine, obstetrics and gynecology, and radiology. An established protocol () was implemented to evaluate patients suspected of having PPH and to identify those with intractable PPH, thereby avoiding the immediate transfer of all patients to the TAE room. When a woman suspected of having PPH arrived at our hospital, our emergency medical staff promptly initiated efforts to stabilize her vital signs. Obstetricians performed pelvic examination, abdominopelvic ultrasound examination, and uterine massage to assess the extent of the hemorrhage. Medical treatments were administered based on the patient's specific condition. These treatments included intravenous infusion of oxytocin, intramuscular administration of methylergonovine in patients without a history of hypertension, and administration of misoprostol suppository. Blood transfusion was performed as necessary, guided by the patient's vital signs, estimated blood loss, and laboratory data.
Figure 1. Flowchart of PPH evaluation and management. CT: computed tomography; ICU, intensive care unit; PPH, postpartum hemorrhage; TAE, transarterial embolization
TAE procedure
Intractable PPH was defined as persistent bleeding despite initial conservative management. In cases of intractable PPH, the patients were assessed by obstetric physicians to determine the appropriate course of action. TAE was considered for patients whose hemodynamic status allowed for the procedure. As per our established protocol [Citation22], the TAE team initiated TAE within 30 min after identifying intractable PPH through routine evaluation procedures. TAE was performed by experienced radiologists with blood product infusion and close monitoring of vital signs. To localize the site of bleeding, the initial step involved performing pelvic angiography. Embolization was performed on either uterine arteries or internal iliac arteries using gel foam cubes, irrespective of active extravasation of contrast medium. Post-TAE pelvic angiography was performed to assess the effectiveness of embolization procedure in controlling the haemorrhage. Thereafter, the patients were transferred to the intensive care unit (ICU) or general ward, depending on the post-TAE hemodynamic status. The decision regarding the appropriate level of care and monitoring was made to ensure the patient's well-being and optimal recovery.
Timing of conversion to laparotomy
For patients whose vital sign remained unstable after initial resuscitation, and who were unable to tolerate the TAE procedure, they were promptly transferred to operative room to prepare for exploratory laparotomy. On the other hand, for patients who underwent TAE as a treatment for intractable PPH, the success of the procedure was based on clinical outcomes. TAE was considered clinically successful if there was no need for repeat embolization or surgical intervention to control the bleeding. Following TAE, the patients' condition was re-evaluated to determine the subsequent course of action. Patients who had persistent bleeding and hemodynamic instability after the initial embolization underwent abdominal computed tomography (CT) examination. The purpose of this examination was to guide therapeutic decisions. Secondary embolization or exploratory laparotomy was considered depending on abdominal CT imaging findings and the patient's clinical condition. During laparotomy, several surgical techniques were available for utilization based on intraoperative finding, and the individual patient's condition. These techniques included repairing any uterine lacerations or uterine rupture, placing uterine compression sutures (e.g. B-Lynch, Hayman, Cho, Esike methods), performing bilateral uterine artery ligation (O’Leary sutures), performing bilateral utero-ovarian artery ligation, performing internal iliac artery ligation, or resorting to hysterectomy when necessary [Citation29].
Results
During the study period, a total of six patients were diagnosed with unscarred uterine rupture immediately after vaginal delivery. All patients were referred from five different community hospitals. The average time from delivery to transfer was 124.6 minutes with a range from 41 minutes to 215 minutes. Data on maternal baseline demographics and delivery information are presented in . The mean maternal age among the patients was 34 years (range, 26–40 years). All women were multiparous, and their current pregnancies were full-term singletons. Two patients underwent labor induction using Dinoprostone (Prostaglandin E2). The longest duration of the first stage of labor was 19 hours 40 minutes. One patient had a precipitous labor. Among the patients, four had vaginal deliveries with vacuum assistance. Fetal distress prompted the use of vacuum extraction in one patient, while arrest of the second stage of labor led to its utilization in the other three patients. Additionally, one patient encountered difficulties in placental separation, and another patient experienced shoulder dystocia. The potential contributing factors to uterine rupture are shown in ., highlighting that all patients had more than one risk factors associated with unscarred uterine rupture.
Figure 2. Maternal clinical characteristics and labor course (N = 6)
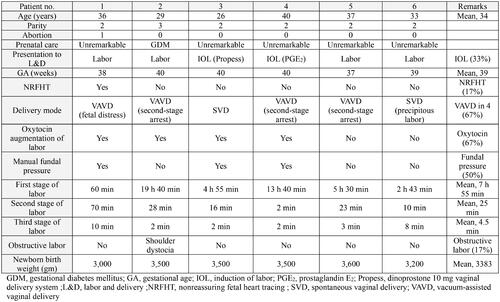
Table 1. Possible contributing factors to uterine rupture in our study population (N = 6)
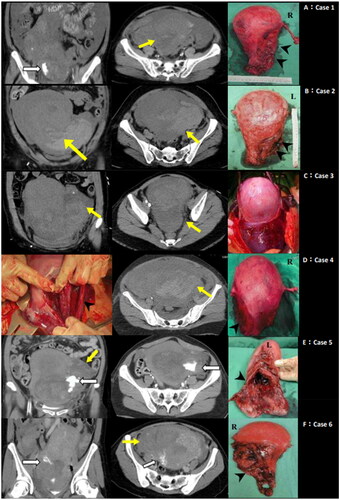
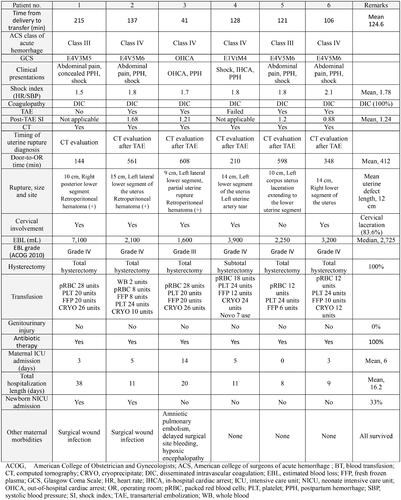
Five of the six patients presented with hypovolemic shock, with a mean SI of 1.78, and ACS class III-IV hemorrhage upon arrival. In terms of mental status, all six patients were lethargic and confused. Notably, the patient in case 3 experienced out-of-hospital cardiac arrest (OHCA) and acute pulmonary embolism, and was resuscitated with venoarterial extracorporeal membrane oxygenation. At the initial evaluation, the mean haemoglobin level was 8.15 g/dL and the mean haematocrit level was 25.5%. All patients were evaluated and managed according to the standard protocol for PPH through collaborative efforts among the emergency department staff and radiologists at our hospital. Five patients presented with active vaginal bleeding, and poor uterine contraction. In one patient (case 1), the presentation was a concealed type of PPH, characterized by minimal vaginal bleeding but progressive abdominal distension and hemodynamic instability. This prompted the arrangement of abdominal CT examination, which revealed uterine rupture and intraperitoneal bleeding. Cervical laceration was observed in five patients, and primary suture repair had been performed prior to their transfer to our hospital in four patients. The emergent abdominopelvic ultrasound examination performed in the emergency department consistently revealed a boggy uterus, except in one patient (case 1) who also exhibited fluid in the pelvis during the initial ultrasound evaluation. All six patients were diagnosed with intractable PPH following failed conservative management of PPH. Initial resuscitation measures, including uterine massage, rapid intravenous fluid challenge, administration of uterotonic agents, and blood transfusion, did not effectively control the bleeding. One patient (case 1) was sent to operative room for exploratory laparotomy. TAE of the internal iliac arteries was attempted in five patients; however, TAE could not be performed in one patient due to uncontrollable hemodynamic deterioration. The TAE procedure was deemed clinically unsuccessful in all patients, necessitating supplementary surgical intervention for achieving hemostasis. The mean post-TAE SI of the four patients was 1.24 (range, 0.88–1.68). Pelvic CT scans were conducted in all six patients, and the findings confirmed the diagnosis of uterine rupture. Five patients had pelvic CT scan after the clinical failure of TAE. Major CT findings included disrupted myometrium, retroperitoneal hematoma, and hemoperitoneum. . displays the pelvic CT images of the six cases, illustrating the pathological features associated with uterine rupture.
Figure 3. Abdominal computed tomography images and intraoperative findings in our study (N = 6). Each case is dipicted in panel A to F. A: Contrast extravasation (white arrow), and myometrium disruption with intraperitoneal hematoma formation (yellow arrow) observed on contrast-enhanced abdominal computed tomography. This corresponds to the location of uterine rupture site (black arrowhead). B : Abdominal computed tomography following trans-arterial embolization displaying myometrium disruption with intraperitoneal hematoma formation (yellow arrow) consistent with the uterine rupture site (black arrowhead). C : Contrast-enhanced abdominal computed tomography following trans-arterial embolization, revealing myometrium disruption with concealed subserosal hematoma formation (yellow arrow) leading to engorgement of the lower uterine segment. D: Abdominal computed tomography after failure of attempted trans-arterial embolization, demostrating myometrial disruption and intraperitoneal hematoma (yellow arrow) in line with the uterine rupture site. Also indicating direct uterine vessel injury after operative vaginal delivery (black arrowhead). E: Contrast extravasation (white arrow), and myometrial disruption with intraperitoneal hematoma formation (yellow arrow) on contrast-enhanced abdominal computed tomography, corresponding to the uterine rupture site (black arrowhead). (L, left; R, right)
During exploratory laparotomy, vertical lacerations on uterine lower segment were identified in all six patients. In five patients, these lacerations extended inferiorly to involve the lateral cervix. One patient exhibited a partial uterine rupture with a concealed hematoma in the subserosal space of the uterus. The remaining five patients had complete uterine rupture with laceration lengths ranging from 9 to 15 cm. Among those who had undergone vacuum-assisted delivery, more extensive uterine damage was observed. Cases of vacuum-assisted delivery showed direct tearing of the uterine vessels and superior extension of the laceration to the uterine corpus. The characteristics of the laceration sites are summarized in , and in . Repairing fragile, and congestive tissue of ruptured gravid uterus under current haemorrhaging could posed high risk of maternal mortality, so emergent life-saving hysterectomy was performed in all six patients (subtotal hysterectomy in one patient). The decision to perform hysterectomy was driven by the severity of the uterine rupture, the ongoing hemorrhage, and the potential risks associated with attempting uterine repair in such critical circumstances. The histopathological result of the cervix, and uterus described uterine laceration, and the endometrium exhibited decidualization. None of the six cases showed evidence of placenta accrete spectrum. The mean time of arrival to the operating room was 412 min (range, 144–598 min). The median estimated total blood loss was 2725 mL± 900 mL (range, 1600–7100 mL). All six patients experienced significant blood loss, classified as grade III-IV according to the blood loss scale. Five women required admission to the ICU, with the maximum duration stay being 14 days. Two patients needed prolonged hospitalization lasting more than 14 days. Following the major surgery, all six patient had a five-day course of antibiotic therapy. Two patients developed surgical wound infections as a postoperative complication. There was no major complication associated with TAE procedure. In the case of patient 3, surgical site bleeding occurred on day 4 after hysterectomy, necessitating a hemostatic second-look laparotomy to control the bleeding.
Table 2. Site of uterine rupture among patients with unscarred uterus in our study (N = 6)
The clinical presentations and maternal–neonatal outcomes of the six patients are summarized in , providing an overview of the maternal and neonatal status. Among the neonates, two neonates were admitted to the neonatal ICU. One neonate was admitted due to fetal distress as indicated by low Apgar score 1 at 1 minutes, and 1 at 5 minutes. The other neonate was admitted due to suspected brachial plexus injury. All six mothers survived the ordeal. One mother who experienced OHCA developed hypoxic encephalopathy-related psychotic symptoms two months after the event. The remaining five women had a smooth recovery without neurologic sequelae. Notably, there were no cases of postpartum permanent hypopituitarism observed in this study.
Figure 4. Clinical maternal presentations and outcome, and perinatal morbidities (N = 6)
Discussion
Rupture of an unscarred gravid uterus is a critical emergency. In the present study, we observed that all six patients experienced hemorrhagic shock, and DIC, and in some cases, even cardiac arrest. It is important to note that the risk of amniotic fluid embolism is elevated in cases of uterine rupture due to the injury inflicted upon the uterine myometrium and venous sinuses [Citation30,Citation31]. Remarkably, one of our patients experienced uterine rupture complicated by a pulmonary amniotic embolism, further highlighting the severity and potential complications associated with this obstetric event.
Previous studies have extensively reviewed the potential risk factors associated with unscarred uterine rupture [Citation1,Citation5,Citation10]. In our study, most of the patients presented with more than one risk factor for unscarred uterine rupture, as indicated in . The signs and symptoms of uterine rupture are often nonspecific, and can resemble those of uterine atony, which is a common cause of primary PPH in 75-90% of cases. Cervical laceration was observed in five patients (83.3%) in our study, and despite primary suture repair being performed at the community hospital prior to referral, persistent hemorrhage was evident. This finding aligns with previous research indicating a higher prevalence of cervical involvement in cases of unscarred uterine rupture [Citation3]. A high index of suspicion for uterine rupture is warranted when cervical laceration is identified and initial suturing repair fails to achieve hemostasis. Regarding obstetric practice, all six cases were multiparous women, 67% underwent vacuum extraction during delivery, 50% experienced fundal pressure maneuvers, and 67% received oxytocin augmentation. It is worth noting that uterine fundal pressure maneuvers and excessive oxytocin augmentation have been associated with uterine rupture, and adverse perinatal outcome, as reported in a population-based study conducted in Japan [Citation32]. Sequential operative vaginal delivery has also been linked to an increased risk of severe obstetric trauma, primarily in nulliparous women [Citation33,Citation34]. Factors such as fetal head position, instrument type, sequential use of instruments, practice volume of the obstetrician, and indications of operative vaginal delivery have been highlighted in the literature as potential contributors to the risk of obstetric trauma [Citation35,Citation36]. Although rare, the possibility of iatrogenic rupture cannot be excluded in our cases. It is crucial to acknowledge that rupture of an unscarred uterus, while uncommon, can lead to catastrophic obstetric outcomes. The incidence of this complication should decrease with ongoing improvement in obstetric practice [Citation37].
As a leading cause of maternal mortality, current guidelines for its prevention and management of PPH are well- established [Citation28,Citation38]. However, the lack of a standard approach to clarify the underlying causes of intractable PPH highlights the need for better evidence-based practices in managing this condition. Ultrasonography has emerged as a first-line tool in the assessment of women with PPH due to its advantages of non-invasive nature, availability, and absence of ionizing radiation [Citation39–41]. In the context of uterine rupture, ultrasound findings often include fluid accumulation or a mass lesion in the abdominal cavity [Citation40,Citation42]. In our study, five out of six patients did not exhibit free fluid in the pelvis on the initial ultrasound scan. We hypothesized that the presence of blood clot over the myometrial defect in lower uterine segment resulted in a transient uterine tamponade effect. Concealed hematomas formed in the broad ligament, retroperitoneum and subserosal space of the uterus may contributed to the ultrasound appearance of a boggy uterus. The visualization of free fluid in abdomino-pelvic cavity may have occurred as uterine bleeding progressed. While abdominopelvic ultrasound can detect some indirect signs of uterine rupture, it may not directly depict uterine wall defects. These inconclusive imaging findings can pose a dilemma for physicians when making decisions about the management of intractable PPH.
As abdominopelvic ultrasound examination yields inconclusive results, further advanced imaging studies using multidetector CT and magnetic resonance imaging play a crucial role in providing valuable information regarding the localization and characteristics of PPH [Citation17,Citation43,Citation44]. The American College of Radiology Appropriateness Criteria recommend appropriate use of contrast-enhanced CT and CT angiogram of the abdomen and pelvis to identify the source of bleeding, particularly in cases of suspected intra-abdominal hemorrhage when active hemorrhage persists despite conventional medical or embolization treatment [Citation43,Citation44]. The diagnosis of uterine rupture was confirmed using pelvic CT in all six patients in the present study. The CT findings of uterine rupture include a focal low-attenuation defect over the disrupted uterine wall and the presence of hemoperitoneum. Additionally, hidden retroperitoneal hematoma can be visualized on CT, which is useful in in evaluating PPH associated with lower genital tract injury, especially following instrument-assisted vaginal delivery [Citation17,Citation18,Citation43,Citation44]. By providing detailed anatomical information, CT imaging aids in the accurate diagnosis and management of cases involving uterine rupture.
Angiographic arterial embolization, first described by Brown et al. [Citation45], has emerged as an effective, safe, and fertility-preserving alternative to hemostatic hysterectomy for managing patients with intractable PPH [Citation22,Citation43,Citation46]. While TAE has no absolute contraindication, it is crucial to promptly address traumatic factors such as uterine rupture and genital tract laceration before considering TAE [Citation47]. The post-TAE SI is a significant indicator which is associated with the clinical success or failure of TAE, with a cut-off value of 0.8 being utilized [Citation48]. In our study, four patients treated with TAE, and the mean post-TAE SI of these patients was 1.24 (range, 0.88–1.68), indicating a high likelihood of TAE failure. It is important to recognize that simple TAE alone may not effectively control obstetric hemorrhage resulting from a ruptured gravid uterus, and it may potentially delay the time to surgical intervention. In our study, the mean time from arrival to the operating room was 412 minutes, emphasizing the need for timely recognition of unscarred uterine rupture to optimize patients’ outcomes.
Our study had some limitations that should be acknowledged. First, owing to the rarity of unscarred uterine rupture, and this is a single-institution study, so the number of cases included in our study is limited. Second, the retrospective nature of our study had inherent limitation. The absence of control group made it difficult to elucidate definite risk factors for unscarred uterine rupture. Another limitation of our study is that the detailed delivery information regarding the duration, and the sequential attempts for vacuum extraction, and the experience of referral obstetrician are not available in datum collection afterwards. Some cases of unscarred uterine rupture may have been transferred to other tertiary hospitals in which the details were not accessible for data collection. Consequently, the incidence of unscarred uterine rupture during the study period was unobtainable. Unscarred uterine rupture was not among the expected diagnoses in our initial assessment. This can be attributed to the rarity of this condition and a lack of awareness among physicians. As a result, physicians tend to manage PPH by focusing on more common etiologies based on the PPH management protocol at our hospital. The lesson learned from these six cases of unscarred gravid uterine rupture was that unclear diagnoses may lead to delayed appropriate treatment for intractable PPH. Delayed diagnosis of unscarred ruptured uterus following vaginal delivery significantly increases the risk of peripartum hysterectomy [Citation18,Citation33]. By incorporating advanced image study, and radiologic intervention, we aimed to optimize the management protocol for intractable PPH, and improve the understanding of its etiology in clinical practice. The modification for the order of CT scan arrangement is illustrated in dotted line in . In selective patients whose hemodynamic status can undergo transportation, and examination, we propose to perform CT in order to evaluate the extent of genital tract injury prior to TAE. This approach aims to identify the specific characteristics of PPH, especially in patients with predisposing factors for uterine rupture, such as operative vaginal delivery, cervical laceration with failed hemostasis after primary repair, or suspicion of concealed type PPH. In addition to the benefits mentioned, a CT examination prior to TAE can play a crucial role in precisely locating the bleeding site and guiding further angiographic intervention. This approach can help reduce the overall radiation burden during TAE procedures [Citation17]. Patients who require operative hemostasis may greatly benefit from a CT examination as it can provide valuable information about the extent of damage, which allows more precise surgical planning. Besides advanced image study, it is important for physician to closely monitor serial clinical changes, hemodynamic status, laboratory studies, and utilize diagnostic tools such as culdocentesis and abdominal ultrasound in the management of intractable PPH [Citation49]. We want to emphasize the importance of prompt life-saving surgical intervention in postpartum patients with an unstable condition after initial resuscitation. In settings with limited access to radiologic interventions, such as in developing regions with low-resource settings, immediate exploratory laparotomy should be arranged for unstable patients with intractable PPH. Timely surgical intervention is crucial in preventing further complications and improving patient outcomes.
Conclusion
We observed that instrument-assisted obstetric delivery and cervical injury potentially predispose patients to a risk of unscarred uterine rupture following vaginal delivery in our study. CT imaging is a valuable tool in complementing ultrasound findings to clarify the cause of intractable PPH. In selective patients, we recommend the inclusion of abdominopelvic CT as part of the diagnostic workup before initiating TAE. This helps evaluate the extent of genital tract injury, and guides further treatment options. Immediate conversion to laparotomy is necessary to explore the intra-abdominal etiology of PPH uncontrollable with TAE. The rational etiologies of uterine rupture must be clarified to improve management strategies while generating practical guideline in the future.
Ethics approval and consent to participate
The institutional review board of Chang Gung Memorial Hospital approved this study (approval no. 202101275B0). The institutional review board of Chang Gung Memorial Hospital approves the waiver of the participants' consent. All methods were carried out in accordance with relevant guidelines and regulations.
Consent for publication
Not applicable.
Authors' contributions
Conception & supervision: F.T.K; Interpretation or Analysis of Data: L.Y.C., F.T.K. Preparation of the manuscript: L.Y.C. Patient recriutment, data collection and revision for important Intellectual Content: F.T.K, L.L.T, T.H.Y, Y.J.L, Y.W.C, T.Y.H
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, F.T.K, upon reasonable request.All data generated or analysed during this study are included in this published article.
Additional information
Funding
References
- Gibbins KJ, Weber T, Holmgren CM, et al. Maternal and fetal morbidity associated with uterine rupture of the unscarred uterus. Am J Obstet Gynecol. 2015 ;213(3):382 e1-6. doi: 10.1016/j.ajog.2015.05.048.
- Justus Hofmeyr G, Say L, Metin Gülmezoglu A. Systematic review: WHO systematic review of maternal mortality and morbidity: the prevalence of uterine rupture. BJOG: Int. J. Obstet. Gynaecol. 2005;112(9):1221–1228. doi: 10.1111/j.1471-0528.2005.00725.x.
- Ofir K, Sheiner E, Levy A, et al. Uterine rupture: differences between a scarred and an unscarred uterus. Am J Obstet Gynecol. 2004;191(2):425–429. doi: 10.1016/j.ajog.2004.01.026.
- Mulot S, Thibon P, Rikelman S, et al. Rupture utérine sur utérus non cicatriciel: à propos de 10 cas. Gynecol Obst Fert Se. 2018 ;46(10):692–695. doi: 10.1016/j.gofs.2018.09.007.
- Vernekar M, Rajib R. Unscarred uterine rupture: A retrospective analysis. J Obstet Gynaecol India. 2016 ;66(Suppl 1):51–54. doi: 10.1007/s13224-015-0769-7.
- Batra K, Gaikwad HS, Gutgutia I, et al. Determinants of rupture of the unscarred uterus and the related feto-maternal outcome: current scenario in a low-income country. Trop Doct. 2015 ;46(2):69–73. doi: 10.1177/0049475515598464.
- Wang YL, Su TH. Obstetric uterine rupture of the unscarred uterus: a twenty-year clinical analysis. Gynecol Obstet Invest. 2006;62(3):131–135. doi: 10.1159/000093031.
- Chang Y-H. Uterine rupture over 11 years: a retrospective descriptive study. Aust N Z J Obstet Gynaecol. 2020;60(5):709–713. doi: 10.1111/ajo.13133.
- Vuong ADB, Nguyen XT, Nguyen PN. Placenta accreta spectrum on an unscarred uterus in the third-trimester pregnancy: two rare cases at Tu Du Hospital in Vietnam. Int J Surg Case Rep. 2022;99:107603. doi: 10.1016/j.ijscr.2022.107603.
- Thisted DL, Mortensen LH, Krebs L. Uterine rupture without previous caesarean delivery: a population-based cohort study. Eur J Obstet Gynecol Reprod Biol. 2015 ;195:151–155. doi: 10.1016/j.ejogrb.2015.10.013.
- Al-Zirqi I, Daltveit AK, Forsén L, et al. Risk factors for complete uterine rupture. Am J Obstet Gynecol. 2017;216(2):165.e1–165.e8. doi: 10.1016/j.ajog.2016.10.017.
- Hochler H, Wainstock T, Lipschuetz M, et al. Grandmultiparity, maternal age, and the risk for uterine rupture—A multicenter cohort study. Acta Obstet Gynecol Scand. 2020;99(2):267–273. doi: 10.1111/aogs.13725.
- Sturzenegger K, Schäffer L, Zimmermann R, et al. Risk factors of uterine rupture with a special interest to uterine fundal pressure. J. Perinat. Med. 2017;45(3):309–313. doi: 10.1515/jpm-2016-0023.
- You SH, Chang YL, Yen CF. Rupture of the scarred and unscarred gravid uterus: outcomes and risk factors analysis. Taiwan J Obstet Gynecol. 2018 ;57(2):248–254. doi: 10.1016/j.tjog.2018.02.014.
- Uccella S, Cromi A, Bogani G, et al. Spontaneous prelabor uterine rupture in a primigravida: a case report and review of the literature. Am J Obstet Gynecol. 2011 ;205(5):e6–e8. doi: 10.1016/j.ajog.2011.08.013.
- Guèye M, Mbaye M, Ndiaye-Guèye MD, et al. Spontaneous uterine rupture of an unscarred uterus before labour. Case Rep. Obstet. Gynecol. 2012;2012:598356. doi: 10.1155/2012/598356.
- Lee NK, Kim S, Lee JW, et al. Postpartum hemorrhage: clinical and radiologic aspects. Eur J Radiol. 2010 ;74(1):50–59. doi: 10.1016/j.ejrad.2009.04.062.
- Has R, Topuz S, Kalelioglu I, et al. Imaging features of postpartum uterine rupture: a case report. Abdom Imaging. 2008 ;33(1):101–103. doi: 10.1007/s00261-007-9206-4.
- McEvoy A, Corbett GA, Nolan C, et al. Outcomes of uterine rupture in the setting of the unscarred compared with the scarred uterus. Obstet Gynecol. 2023;141(4):854–856. doi: 10.1097/AOG.0000000000005108.
- Amikam U, Hochberg A, Abramov S, et al. Risk factors for maternal complications following uterine rupture: a 12-year single-center experience. Arch Gynecol Obstet. 2023. doi: 10.1007/s00404-023-07061-1.
- Rottenstreich M, Rotem R, Hirsch A, et al. Delayed diagnosis of intrapartum uterine rupture – maternal and neonatal consequences. J Matern Fetal Neonatal Med. 2021 ;34(5):708–713. doi: 10.1080/14767058.2019.1613366.
- Cheng HH, Tsang LL, Hsu TY, et al. Transcatheter arterial embolization as first-line rescue in intractable primary postpartum hemorrhage: assessment, outcome, and subsequent fertility. J Formos Med Assoc. 2017 ;116(5):380–387. doi: 10.1016/j.jfma.2016.06.011.
- Bonnar J. Massive obstetric haemorrhage. Best Pract Res Clin Obstet Gynaecol. 2000 ;14(1):1–18. doi: 10.1053/beog.1999.0060.
- Thi Pham XT, Bao Vuong AD, Vuong LN, et al. A novel approach in the management of placenta accreta spectrum disorders: a single-center multidisciplinary surgical experience at Tu Du Hospital in Vietnam. Taiwan J Obstet Gynecol. 2023;62(1):22–30. doi: 10.1016/j.tjog.2022.09.003.
- Schwickert A, van Beekhuizen HJ, Bertholdt C, et al. Association of peripartum management and high maternal blood loss at cesarean delivery for placenta accreta spectrum (PAS): A multinational database study. Acta Obstet Gynecol Scand. 2021;100(S1):29–40. doi: 10.1111/aogs.14103.
- Pacagnella RC, Borovac-Pinheiro A. Assessing and managing hypovolemic shock in puerperal women. Best Pract Res Clin Obstet Gynaecol. 2019 2019/11/01/;61:89–105. doi: 10.1016/j.bpobgyn.2019.05.012.
- Kohn JR, Dildy GA, Eppes CS. Shock index and delta-shock index are superior to existing maternal early warning criteria to identify postpartum hemorrhage and need for intervention. J Matern Fetal Neonatal Med. 2019;32(8):1238–1244. doi: 10.1080/14767058.2017.1402882.
- Borovac-Pinheiro A, Pacagnella RC, Cecatti JG, et al. Postpartum hemorrhage: new insights for definition and diagnosis. Am J Obstet Gynecol. 2018 2018/08/01/;219(2):162–168. doi: 10.1016/j.ajog.2018.04.013.
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum Hemorrhage. N Engl J Med. 2021;384(17):1635–1645. doi: 10.1056/NEJMra1513247.
- Josey WE, Patterson WM, Wood HE, et al. Hypofibrinogenemia and presumptive amniotic fluid embolism associated with rupture of the uterus. Am J Obstet Gynecol. 1961 1961/07/01/;82(1):172–176. doi: 10.1016/S0002-9378(16)36112-9.
- Conde-Agudelo A, Romero R. Amniotic fluid embolism: an evidence-based review. Am J Obstet Gynecol. 2009;201(5):445.e1–445.13. doi: 10.1016/j.ajog.2009.04.052.
- Hasegawa J, Ikeda T, Toyokawa S, et al. Obstetric factors associated with uterine rupture in mothers who deliver infants with cerebral palsy. J Matern Fetal Neonatal Med. 2021;34(5):663–669. doi: 10.1080/14767058.2019.1611775.
- Muraca GM, Lisonkova S, Skoll A, et al. Ecological association between operative vaginal delivery and obstetric and birth trauma. CMAJ. 2018;190(24):E734–E741. doi: 10.1503/cmaj.171076.
- Panelli DM, Leonard SA, Joudi N, et al. Severe maternal and neonatal morbidity after attempted operative vaginal delivery. Am J Obstet Gynecol MFM. 2021;3(3) doi: 10.1016/j.ajogmf.2021.100339.
- Ducarme G, Hamel J-F, Bouet P-E, et al. Maternal and neonatal morbidity after attempted operative vaginal delivery according to fetal head station. Obstet Gynecol. 2015;126(3). doi: 10.1097/AOG.0000000000001000.
- Yamasato K, Kimata C, Chern I, et al. Complications of operative vaginal delivery and provider volume and experience. J Matern Fetal Neonatal Med. 2021;34(21):3568–3573. doi: 10.1080/14767058.2019.1688293.
- Turner MJ. Uterine rupture. Best Pract Res Clin Obstet Gynaecol. 2002;16(1):69–79. doi: 10.1053/beog.2001.0256.
- Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet Gynecol. 2017;130(4):e168–e186. doi: 10.1097/aog.0000000000002351.
- Lousquy R, Morel O, Soyer P, et al. Routine use of abdominopelvic ultrasonography in severe postpartum hemorrhage: retrospective evaluation in 125 patients. Am J Obstet Gynecol. 2011;204(3):232 e1–6. doi: 10.1016/j.ajog.2010.10.003.
- Oba T, Hasegawa J, Sekizawa A. Postpartum ultrasound: postpartum assessment using ultrasonography. J Matern Fetal Neonatal Med. 2017;30(14):1726–1729. doi: 10.1080/14767058.2016.1223034.
- Easter SR, Hameed AB, Shamshirsaz A, et al. Point of care maternal ultrasound in obstetrics. Am J Obstet Gynecol. 2023;228(5):509.e1–509.e13. doi: 10.1016/j.ajog.2022.09.036.
- Tauchi M, Hasegawa J, Oba T, et al. A case of uterine rupture diagnosed based on routine focused assessment with sonography for obstetrics. J Med Ultrason (2001). 2016;43(1):129–131. doi: 10.1007/s10396-015-0662-0.
- Sierra A, Burrel M, Sebastia C, et al. Utility of multidetector CT in severe postpartum hemorrhage. RadioGraphics. 2012;32(5):1463–1481. doi: 10.1148/rg.325115113.
- Uyeda JW, George E, Reinhold C, et al. ACR Appropriateness criteria® postpartum hemorrhage. J Am Coll Radiol. 2020;17(11, Supplement):S459–S471. doi: 10.1016/j.jacr.2020.09.011.
- Brown Bj Fau - Heaston DK, Heaston Dk Fau - Poulson AM, Poulson Am Fau - Gabert HA, et al. Uncontrollable postpartum bleeding: a new approach to hemostasis through angiographic arterial embolization. (0029-7844 (Print)).
- Deux J-F, Bazot M, Le Blanche AF, et al. Is Selective embolization of uterine arteries a safe alternative to hysterectomy in patients with postpartum hemorrhage? AJR Am J Roentgenol. 2001;177(1):145–149. doi: 10.2214/ajr.177.1.1770145.
- Chen C, Lee SM, Kim JW, et al. Recent update of embolization of postpartum hemorrhage. Korean J Radiol. 2018;19(4):585–596. doi: 10.3348/kjr.2018.19.4.585.
- Fu CJ, Irama W, Wong YC, et al. Transarterial embolization for postpartum hemorrhage: lessons learned. Acta radiol. 2018;59(12):1451–1457. doi: 10.1177/0284185118769691.
- Vuong ADB, Pham TH, Nguyen XT, et al. Spontaneous hemoperitoneum in the second and third trimester of pregnancy: two uncommon case reports at Tu Du Hospital, in Vietnam and a literature review. Int J Emerg Med. 2023;16(1):26. doi: 10.1186/s12245-023-00498-w.