

ABSTRACT
Introduction
Antibiotics are life-saving drugs but irrational/inappropriate use leads to the emergence of antibiotic-resistant bacterial superbugs, making their treatment extremely challenging. Increasing antimicrobial resistance (AMR) among bacterial pathogens is becoming a serious public health concern globally. If ignorance persists, there would not be any antibiotics available to treat even a common bacterial infection in future.
Area covered
This article intends to collate and discuss the potential of 4D’s (right Drug, Dose, Duration, and De-escalation of therapy) approach to tackle the emerging problem of AMR. For this, we searched PubMed, Google Scholar, Medline, and clinicaltrials.gov databases primarily using keywords ‘optimal antibiotic therapy,’ ‘antimicrobial resistance,’ ‘higher versus lower dose antibiotic treatment,’ ‘shorter versus longer duration antibiotic treatment,’ ‘de-escalation study’, and ‘antimicrobial stewardship measures’ and based on the findings, form and expressed our opinion.
Expert opinion
More efforts are needed for developing diagnostics for rapid, accurate, point-of-care, and cost-effective pathogen identification and antimicrobial susceptibility testing (AST) to facilitate rational use of antibiotics. Current dosing and duration of therapies also need to be redefined to maximize their impact. Furthermore, de-escalation approaches should be developed and encouraged in the clinic. This altogether will minimize selection pressure on the pathogens and reduce emergence of AMR.
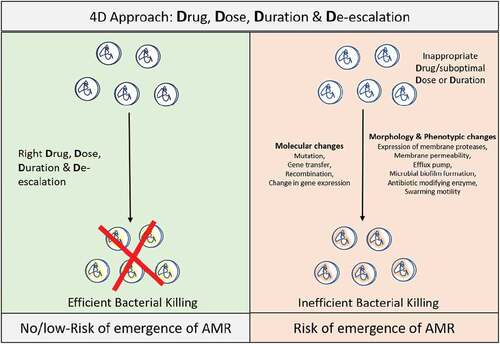
Graphical Abstract
Article highlights
Rapidly emerging antibiotic-resistant bacterial superbugs are becoming a global threat; whereas the rate of new antibiotic development is very slow. Hence, the world may soon enter into the post-antibiotic era where even a common infection may be life threatening.
To save the existing last resort of antibiotics, rational drug use (RDU), which requires 1) accurate diagnosis, 2) regulated antimicrobial dispensing, and 3) right 4D’s (Drug, Dose, Duration and De-escalation of therapy), may be an optimal approach.
Rapid, accurate, non/minimally-invasive, point-of-care and cost-effective diagnostics for pathogen identification and AST may help in choosing the right drug. However, no such diagnostic is currently available and this contributes to the inappropriate use of antibiotics.
Clinical studies have demonstrated that an optimal dose for a shorter duration can also be similarly efficacious as a higher dose for a longer duration. However, such limited studies have merely been able to impact the current treatment practices. More clinical trials and united efforts are required to redefine the treatment approaches for current clinical scenarios.
Antibiotic de-escalation (i.e. use of narrow-spectrum antibiotics, promoting monotherapy and using antibiotic cycling) may help in reducing the selection pressure on bacterial pathogens and hence the emergence of AMR. However, more clinical evidence is required for the development of such approaches.
Awareness, educational programs, and a worldwide policy may be developed and implemented to maximize the benefits of the 4D approach to combat the problem of AMR.
Acknowledgments
We are grateful to Prof. Pramod Kumar Garg (Executive Director), Mr. M.V. Santo (Head Administration), Shrikant Kumar (Technical officer-MCTR), Shailesh Kumar and Manoj Kumar (Lab Technicians-MCTR) of Translational Health Science and Technology Institute Faridabad, India for their support.
Abbreviations
| 4D | = | Right Drug, Dose and Duration of therapy, and the De-escalation |
| AMR | = | Antimicrobial-resistant |
| CARAT | = | Council for Appropriate and Rational Antibiotic Therapy |
| KPC | = | Carbapenem-resistant Klebsiella pneumoniae |
| MRSA | = | Methicillin-resistant Staphylococcus aureus |
| CD | = | Clostridioides difficile |
| RDU | = | Rational Drug Use |
| AST | = | Antimicrobial Susceptibility Testing |
| PK | = | Pharmacokinetic |
| PD | = | Pharmacodynamic |
| AI | = | Artificial intelligence |
| MDR | = | Multi drug resistant |
| ICU | = | Intensive Care Unit |
| PCR | = | Polymerase Chain Reaction |
| LFA | = | Lateral Flow Assays |
| NAAT | = | Nucleic Acid Amplification Test |
| MALDI-TOF | = | Matrix Assisted Laser Desorption Ionization Time of Flight |
| MIC | = | Minimum Inhibitory Concentration |
| ADME | = | Absorption, Distribution, Metabolism and Excretion. |
| UTI | = | Urinary tract infection |
| CAP | = | Community Acquired Pneumonia |
| DSS | = | Decision Support Systems |
| EMR | = | Electronic Medical Records |
| WAAW | = | World Antimicrobial Awareness Week |
| WHO | = | World Health Organization |
| POC | = | Point of Care |
| ESBL | = | Extended spectrum beta-lactamase |
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or material discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or mending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Author contributions
All authors have substantially contributed to the conception, design of the review article and interpretation of the relevant literature. Dr. Archana Angrup helped in improving its quality and readability.