
Abstract
Objective: Research has minimally focussed on the music listening habits and preferred sound volumes among adolescents with severe to profound congenital HL. Listening to music played at loud sound volumes and for a long duration of time could imply risks of worsening the HL. Therefore, it is important to investigate the listening habits in adolescents with HL. The aim of the present study was to describe the use of personal music devices, subjective estimated sound levels, measured sound levels, listening habits, and hearing symptoms in adolescents with severe to profound hearing loss compared with adolescents with normal hearing.
Design: The study was conducted in two steps. First, a questionnaire was given to students with or without hearing loss. In step two, hearing and sound level measurements were made in a subsample from both groups.
Study sample: The study sample were based on 112 seventeen-year-old students with severe to profound hearing loss and 279 adolescents with normal hearing. Hearing thresholds and listening levels was measured on two subsamples based on 29 adolescents with severe to profound hearing loss and 50 adolescents from the group with normal hearing.
Results: The results showed that adolescents with severe to profound hearing loss listened to significantly louder sound levels for longer periods. For both groups, those listening at louder sound levels had poorer hearing thresholds. This finding is especially alarming for subjects with hearing loss. Among those listening above 85 dB per occasion, the sound level ranged between 85.8 dB up to 109 dB for those with hearing loss, whereas the sound level ranged between 85.5 dB and 100 dB for those with normal hearing.
Conclusions: Adolescents with congenital hearing loss used portable music devices in the same manner as adolescents with normal hearing. However, adolescents with hearing loss listened to louder sound volumes most likely to compensate for their hearing loss, which significantly increases the risk of further damage to their hearing. From a hearing rehabilitation perspective it could be concluded that aspect of music listening habits should be focussed in order to prevent noise induced hearing loss among individuals with congenital hearing loss.
Introduction
The use of personal music devices (PMDs) has increased dramatically among adolescents and young adults, causing increased exposure to high sound levels during leisure time activities (Kasper Citation2006). Previous studies have demonstrated both auditory and non-auditory health effects of noise (Basner et al. Citation2014). Audiological problems, such as temporary and permanent hearing threshold shifts (Kim et al. Citation2009) as well as temporary or permanent tinnitus (Meyer-Bish Citation1996; Kim et al. Citation2009) have been reported after acute or long-term exposure to high sound levels when listening to PMD. The increased accessibility of PMDs, the integration of PMDs in cell/smart phones, lower prices and technical improvement regarding sound quality has made the use of these devises extremely common worldwide.
Following regulations for occupational noise exposure in Sweden, the risk for developing music-induced hearing loss can be estimated based on the principle of noise dose or 8 hour equivalent level. This principle means that an 8 hour-long exposure at 85 dB A-weighted sound pressure level noise represents the maximum noise level a person should be exposed to five days a week before being at risk for developing noise-induced HL. For each 3 dB above this limit, the time required to reach maximal noise dose is halved. For example, at 88 dB, the noise dose is reached in 4 hours a day. At 91 dB, the dose is reached in 2 hours (Rydzynski et al. Citation2008). PMDs are capable of producing up to 126 dB sound pressure level output at maximum volume (Breinbauer et al. Citation2012).
Approximately 100 million people within the European Union use PMDs. Among these individuals, it is estimated that approximately 10% listen at levels greater than 85 dB LpAeq (Rydzynski et al. Citation2008). Applying the noise dose principle, approximately 10 million of the users would be at risk for developing noise-induced HL (Rydzynski et al. Citation2008). Identified groups who expose themselves to a higher degree of damaging sound levels include adolescents and young adults, and especially young men with low socio-economic status (Olsen-Widén and Erlandsson Citation2004; Shargorodsky et al. Citation2010). The use of hearing protection as a strategy for lowering the level of noise is a well-known recommendation for industrial workers who are exposed to an equivalent sound level of 85 dB or more for an 8-hour working day. However, the normal PMD listener has the volume at a range between 75 and 100 dB and may listen for 1 to 3 hours a day (Kim et al. Citation2009). Individuals who listen to 15 min of music at 100 dB are exposed to the same levels of loudness as an industrial worker who is exposed to 85 dB for 8 hours. One difference between industrial and leisure time noise exposure, is that industrial workers expose themselves every day for several years to loud noises, whereas the exposure time in leisure activities is less in general.
In a recent study among 415 Swedish nine-year-old children, the prevalence of a hearing threshold ≥20 dB HL (HL) at one or several frequencies on one or two ears was 53%. Hearing thresholds at 6 and 8 kHz were increased compared with the low and mid frequencies, indicating that the threshold shifts could be noise induced. In addition, pure-tone audiometry revealed that children who regularly listened with headphones exhibited poorer hearing thresholds (Båsjö et al. Citation2016). Another study among 280 Swedish adolescents found that longer lifetime exposure in years and increased listening frequency were associated with poorer hearing thresholds and self-reported hearing problems (Widén et al. Citation2017). Men also report a higher degree of PMD use. In addition, men listened at higher sound volumes compared with young women. Those adolescents listening at ≥85 dB LAeq, FF and listening every day had poorer mean hearing thresholds, and those who listened for 3 hours or more at every occasion were more likely to report tinnitus (Widén et al. Citation2017).
There is a growing body of research that supports the hypothesis that listening to PMDs at high volumes and for a long period of time in fact increases the risk for developing hearing problems and noise induced HL among adolescents over time (Vogel, Brug, and van der Ploeg Citation2007; Zhao et al. Citation2010). Among clinicians and researchers, there is a growing concern that the noise-induced HL may increase in the future given modern intense listening habits. There are also a number of studies reporting the listening behaviour of adolescents in terms of frequency and preferred sound volumes (Hodgetts, Rieger, and Szarko Citation2007; Kim et al. Citation2009; Vogel et al. Citation2009; Breinbauer et al. Citation2012). However, far less is known about the music listening behaviour among adolescents with severe to profound congenital HL wearing hearing aids.
Recently, technical improvements have been made regarding hearing aid performance for types of sounds other than speech, making it possible for individuals with severe HL to be able to listen to music (Croghan et al. Citation2016). When a hearing aid user is listening to recorded music through PMDs, volume adjustments are available for him or her. The amount of distortion caused by high input levels depends on the sound level of recorded music by the hearing aid user, which is defined as the input chosen listening level (CLL). One way of measuring the CLL is to measure the sound pressure level in the ear canal. This method way of measuring has been used in most of the research addressing CLLs in both listeners with normal hearing (TH) and individuals wearing hearing aids. In a study among 13 adult hearing aid users, the listening levels for recorded music in aided and unaided conditions were investigated. The study revealed that for aided listening, the average CLL was 69.3 dBA (sd = 9.5) at the input to the hearing aid and 80.3 dBA at the tympanic membrane. For unaided listening conditions, the average CLL was 76.9 dBA (sd = 9.9) at the entrance to the ear canal and 77.1 dBA at the tympanic membrane. The amount of audio-industry compression had no significant effect on CLLs (Croghan et al. Citation2016).
To our knowledge, research has minimally focussed on the music listening habits and preferred sound volumes among adolescents with severe to profound HL. Listening to music played at loud sound volumes and for a long duration of time could imply risks of worsening the HL. For these reasons, it is important to investigate the listening habits in adolescents with HL.
Aims of the study
The aim of the study was to describe and compare the listening habits of HI subjects with NH subjects to investigate whether HI subjects are more at risk.
Materials and methods
Sample collection, phases I and II
Data were collected in two phases. In the first phase, data were collected through a questionnaire administered to 112 adolescents with severe to profound HL using hearing aids. These adolescents were recruited from Swedish national upper secondary schools for the deaf and hard of hearing located in a Swedish larger city. All participating students were seventeen years of age. In addition, 279 age-matched adolescents with NH were recruited from other upper secondary schools in Sweden. Thus, the total sample size was 391 participants. In phase two, a subsample was made based on the adolescents’ voluntary participation in an in-depth study where 29 individuals from the group with HL (all air conduction users) and 50 individuals with normal hearing participated. In this phase, hearing thresholds and measured sound volumes were assessed on participants’ PMDs.
Questionnaire used in phase I
The questionnaire included 13 main questions with an additional 10 subquestions regarding headphone listening habits with PMDs and subjective hearing health. This questionnaire has been used in a previous study (Widén et al. Citation2017). The questionnaire was divided into four cluster areas. Cluster 1 contained 3 questions regarding the participants’, sex, age and if they used PMD or not. Cluster 2 addressed history of usage and included three questions (type of portable music player and headphones that were mostly used, age when starting listening). Cluster 3 included 10 questions concerning contemporary use habits (e.g. questions concerning type of portable music player and headphones, period of time (years), the equipment, frequency of use, duration of time, preferred sound level, preferred type of music and listening environments). Cluster 4 included 7 questions that addressed subjective hearing and symptoms, such as the experience of having permanent tinnitus and sound sensitivity. At the end of the information letter, a question regarding voluntary participation in phase II of the study was addressed.
Phase II- measurement of pure tone audiometry and sound levels from PMDs
All students who wanted to participate in the second part with in-depth examinations were contacted via email, SMS or mail, and an appointment was booked at an Audiological Research Centre located in a tertiary hospital. The participants were all given additional written information concerning the second part of the study that clarified the procedure regarding hearing and tympanometry tests and the sound level measurements of the PMDs with their preferred music and listening volumes.
Hearing measurements
Hearing measurements were performed according to standardised methods in a soundproof booth and were conducted by an authorised audiologist according to ISO 8253-1:2010. Otoscopy and tympanometry using Grason-Stadler GSI 33 was performed prior to pure tone audiometry to ensure free passage to the eardrum and a normal middle ear function.
Pure-tone audiometry (hearing thresholds (air conduction) was performed using Astera pure tone audiometer and TDH 39 headphones. The frequencies measured were 0.25, 0.5, 1, 2, 3, 4, 6, and 8 kHz in the −10 to 60 dB HL range. The criteria for normal hearing threshold were set at 0 to 20 dB HL to all but one or more frequencies or according to pure-tone-average (PTA4; 0.5, 1, 2 and 4 kHz) and high-frequency PTA (4, 6 and 8 kHz). Hearing thresholds ≥20 dB HL were considered abnormal. If asymmetry was identified, bone conduction was also measured.
In this second phase, 29 subjects with severe to profound HL and an age-matched reference group of 50 adolescents with normal hearing from phase I participated. All subjects had congenital hearing loss. Specific aetiology is not reported in this study.
Sound level measurements
The sound pressure levels from the PMDs were measured. The music and the personal preferred listening level (PLL) were chosen by the subjects. All measurements were made using the KEMAR manikin described in two previous studies (Kähäri, Åström, and Olsson Citation2011; Widén et al. Citation2017). All adolescents brought their own PMD and headphones. The adolescents were asked to choose a favourite piece and set the volume at the level they typically use. The measurements were made with their right headphone on Kemar’s right ear. When 30 seconds was measured into the song, a 60-second sampling time started. Leq’s 60 sec and Max and Peak levels both linear and A-weighted in 1/3’s octave bands from 20 to 20 kHz (according to IEC 1260) were sampled. Data were recalculated (in real time) to equivalent free- and diffuse sound field and RMS according to ISO-11904-2. Both free field (FF) corrected and uncorrected data are presented. Background noise levels were recorded repeatedly during the day to ensure that this noise was not loud enough to influence the measurements in any manner. Our measurements on preferred listening levels were done in quiet conditions in an anechoic laboratory at Audiological Research Centre at Örebro university hospital. The background noise levels were measured continuously to assure good measuring conditions and the background noises were very low and did not interfere with the chosen listening levels.
Measurement arrangements headphones
KEMAR was equipped with a Brüel & Kjaer 4157 coupler (EC60711) and a Brüel & Kjaer 4192 sound pressure microphone. The microphone was connected via a Brüel & Kjaer 2669 pre-amp to a Brüel & Kjaer 3560B front-end and to a computer with the Brüel & Kjaer computer programme Pulse Labshop. Measuring arrangement for canal phones/earbuds positioned into the right external auditory meatus were presented in (Kähäri, Åström, and Olsson Citation2011; Widén et al. Citation2017).
Statistical analysis
The data were analysed using IBM SPSS (21.0.0.0). Descriptive statistics were used to analyse the results from the hearing thresholds and tympanometry. The hearing thresholds were analysed in regards to ear and headphone listening habits. Differences between the group with NH and the group with HL were analysed with t-test for independent samples regarding measured sound levels and listening habits, such as duration of time. Chi-square tests were used to analyse differences between the group with NH and the group with HL regarding self-reported hearing symptoms and preferred listening level (≥ 85 dB or <85 dB).
Ethics
The study was approved by the regional ethical board (no: 2009/140). Information letters about the project and letters of consent were sent to principals, the school health care departments and teachers for further distribution to students and caregivers. Inclusion criteria for the study were that the adolescents provided informed written consent.
Results
Description of use habits of PMDs
Almost all (N = 102/112) (91%) of the adolescents with severe to profound HL and NH adolescents (N = 272/279) (97.1%) listened to music with a PMD. The average starting time for using PMDs was at 13.30 years for NH group (sd = 2.1) and 12.44 years for the group with HL (sd = 2.5). This difference were statistical significant (t = 2.98; df = 140.858; p < .01). More adolescents with HL (N = 94, 92%) listened every day or several times per week compared with adolescents with NH (n = 241, 88.6%). The mean listening time was 45 minutes longer (2 hours 45 minutes, range: 0.5–12 hours) at every occasion for adolescents with HL compared with adolescents with NH (mean listening time 2 hours, range: 0.5–12 hours) In addition, 54.3% of adolescents with HL listened for 0.5 to 2 hours at every session, whereas 45.7% listened for 3 hours or more. In the group with NH, 80% of the adolescents listened for 0.5 to 2 hours at every session, whereas 20.0% listened for 3 hours or more.
The most commonly used type of headphones was canal phones (HL group = 43.2% versus NH group = 49.4%). Among adolescents with HL, 33% used regular earbuds, and 17% used headphones closed ear muffs. Most adolescents with NH used either regular earbuds (38%) or canal phones (49%), and the remaining 13% used regular headphones with muffs. Almost all (99%) of the respondents reported using PMDs during some type of transportation, such as when travelling by bus, train, car, walking, and biking. The same pattern was reported in the NH group. In the HL group, 33.3% used their portable music player during school hours, and 29% used their portable music player while sleeping. Approximately 45% of the adolescents with NH used their portable music player during school hours, and 21% reported use while sleeping. No significant differences were observed between the groups regarding subjective assessment of sound volume (25, 50, 75 or 100 percentages = maximal sound volume). Most used a subjective 75 or 50% of maximum volume.
Comparisons between adolescents with severe to profound HL (n = 112) and adolescents with NH (n = 279) regarding hearing symptoms
Significant differences were found concerning subjective hearing symptoms between the NH and HL groups. Significantly more (χ2 = 10.65; df = 1; p < .01) subjects with HL reported permanent tinnitus (19%) compared with NH subjects (7%). Further, sound sensitivity was reported by significantly more respondents (χ2 = 12.90; df = 1; p <.001) in the HL group (21%) compared with the NH groups (8%). Finally, significant differences were noted in reports of sound fatigue (χ2 = 8.70; df = 1; p < .01) where more individuals with HL reported sound fatigue (17%) compared with persons with NH (7%).
Description of pure tone average values for the HL group and PMDs with or without a hearing aid
Out of 29 adolescents with HL, 27 adolescents used a hearing aid: 23 bilaterally and 4 monaurally. PTA4 values (0.5, 1, 2 and 4 kHz) for this group were 52 dB HL for the right vs. 61 dB HL for the left ear. Two students did not use a hearing aid because they had normal hearing function on one ear and profound HL in the other ear. Out of 29 adolescents with HL, 5 used the tele coil setting and a tele loop system or a microphone when listening to music via their hearing aid. Five individuals used ear buds, and 17 adolescents used ear canal phones while listening to music. Two individuals used their personal hearing aid in combination with ear muffs.
Comparisons between adolescents with HL (n = 29) and adolescents with NH (n = 50) regarding measured preferred sound levels when listening to music with a PMD
Comparisons were made between adolescents with HL (n = 29) and adolescents with NH (n = 50) concerning preferred sound levels on their PMDs (). Those adolescents with HL who typically used a loop system or ear cuffs when listening to music used their personal hearing aids when the sound volumes in their PMDs were tested. Whereas those who typically used canal phones or ear buds when listening to music did not. When comparing the HL group with the NH group regarding sound levels (dB LAeq,FF), significant differences were noted (t = −2.40; df = 47.24; p < .05). The average sound level for the NH group was 75.8 dB LAeq,FF compared with 83.1 dB LAeq, FF for the HL group. Among the 14 adolescents with HL that listened at levels greater than 85 dB, the sound level ranged between 85,8 dB and 109 dB. Among the 10 adolescents with NH, the range was 85.5 dB to 100 dB.
Table 1. Comparisons between adolescents with NH and adolescents with HL regarding PMD sound levels.
Regarding listening habits, significant differences were observed concerning the reported duration of time measured in hours per occasion (t = −2.84; df = 123,14; p < .01). The mean time in the NH group was m = 1.98; sd = 1.91 (or 119 minutes per occasion) compared with the HL group m = 2.77, sd = 2.28 (or 166 minutes per occasion). Significant differences were also observed between the groups regarding the frequency of persons listening less than 85 dB and those listening at 85 dB or higher (χ2 = 6.94; df = 1; p < .01). In the NH group, 10 participants (20%) listened to music in their PMDs at 85 dB or louder, whereas 14 participants from the HL groups (48%) listened at 85 dB or higher on their PMDs.
presents means and standard deviations for right and left ear for adolescents with hearing impairment or normal hearing distributed on those listening below 85dBA and those listening at 85dBA or louder.
Table 2. Mean and standard deviations for right and left ear for adolescents with hearing impairment and normal hearing distributed on those listening below 85 dBA and those listening at 85 dBA or louder.
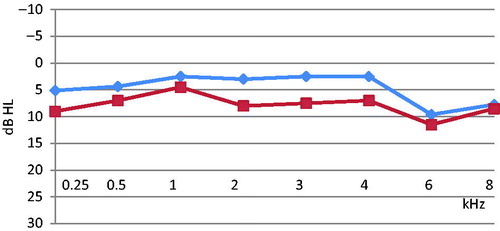
The following results will be presented for the right and the left ear separately. For adolescents with HL () and those with NH (), the result indicates that persons who listened at ≥85 dB had poorer hearing thresholds at most frequencies compared with those who listened at ≤85 dB for the left ear. For the HL group, the differences were most pronounced at 6 kHz (20 dB) and 8 kHz (17 dB). For the group with NH, participants who listened at ≤85 dB and those who listened at ≥85 dB showed a notch at 6 Hz (10–12 dB). Out of 50 adolescents with NH, 7 (14%) had a hearing threshold greater than 20 dB HL at 6 kHz at the right ear.
Figure 1. Right ear hearing thresholds for 29 adolescents with HL who preferred two different PMP listening levels: no 15: ≤85 dB (diamonds) and no 14: ≥85 dB (squares).
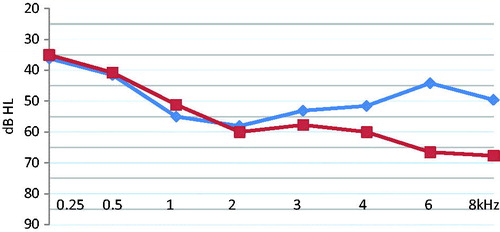
Figure 2. Right hearing thresholds for 50 adolescents with NH who preferred two different PMP listening levels: no 40: ≤85 dB (diamonds) and no 10: ≥85 dB (squares).
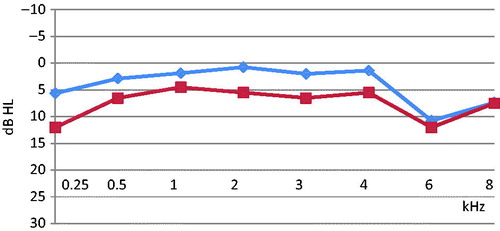
Those adolescents with HL () who listened at ≥85 dB exhibited poorer hearing thresholds at all frequencies (approximately 15 dB from 0.25 kHz up to 3 kHz). At 4 kHz, the difference increases between the groups. At 6 kHz, the difference is 20 dB. At 8 kHz, a 30-dB difference is noted between those who listen at ≥85 dB in compared with those who listen at ≤85 dB. Among adolescents with NH (), those who listen above 85 dB in general have poorer hearing thresholds (approximately 5 dB). Those who listen at ≤85 dB and those who listen at ≥85 dB have a tendency to exhibit a notch at 6 kHz (12–13 dB). Out of 50 adolescents, 10 (20%) had a hearing threshold greater than 20 dB HL at 6 kHz in the left ear.
Figure 3. Left hearing thresholds for 29 adolescents with HL who preferred two different PMP listening levels: no 15: ≤85 dB (diamonds) and no 14: ≥85 dB (squares).
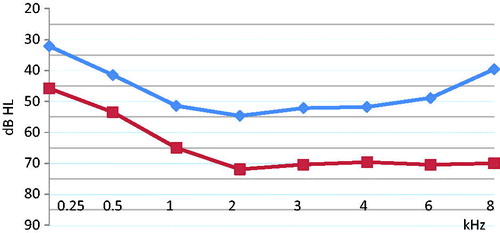
Figure 4. Left hearing thresholds for 50 adolescents with NH who preferred two different PMP listening levels: no 40: ≤85 dB (diamonds) and no 10: ≥85 dB (squares).
Discussion
Numerous studies have reported the listening behaviour of adolescents with NH in terms of frequency and preferred sound volumes (Hodgetts, Rieger, and Szarko Citation2007; Peng, Tao, and Huang Citation2007; Kim et al. Citation2009; Kumar et al. Citation2009; Vogel et al. Citation2009; Breinbauer et al. Citation2012). However, to our knowledge, few studies are available concerning adolescents with HL and their PMD listening habits and preferred sound volumes. In this study, we conclude that adolescents with HL exhibit approximately the same behavioural pattern regarding listening habits as adolescents with NH in the sense that they tend to do the same activities. However, significant differences were also identified. For instance, more adolescents with HL listened to music every day or several times a week with longer exposure times for each session. Among adolescents with HL, approximately 46% listened for 3 hours or more compared with 20% among adolescents with NH. In addition, adolescents with HL reported that they started listening to headphones earlier in life compared to adolescents with NH. This finding indicates significantly more extensive listening habits among adolescents with HL, which may imply an increased risk of more pronounced hearing loss due to music exposure from PMDs. However, we can only speculate about why these differences exist. One suggestion to explanation is that the data for the adolescents with HL was collected among students who studied at the Swedish national upper secondary schools for the deaf and hard of hearing. Many of these adolescents don’t live at home together with their parents. Instead they live together with their peers in student accommodations. This could imply that a special culture develops where more extensive music listening becomes normative for the behaviour. Adolescents are in a phase in life were the creation of their own identity becomes important, where symbols such as music style and clothing is a way of create a sense of belonging to a group and to be accepted by others. Since adolescents with normal hearing listens to music and uses headphones, this behaviour is naturally adapted by adolescents with HL. Maybe music listening among adolescents with HL could be regarded in terms of a normalisation process and a way to fit in and be regarded as normal as possible by others in mainstream society. Another explanation could be that the results indicate that adolescents with HL report more tinnitus compared to the group with NH. Listening to music could be a way of masking the tinnitus sound e.g. while falling to sleep.
Regarding the adolescents’ choice of type of headphones, the group of adolescents with HL used the same products as adolescents with NH with one exception. Two out of 50 (4%) of those with NH used occluding earmuffs, whereas 5 adolescents (17%) among the HL group used this type. Only three adolescents with HL used a hearing aided loop system, which was an unexpected result. Instead of combining their hearing aid with a loop system, most participants choose to turn off their hearing aid and instead use regular canal headphones or ear buds and turning up the sound volume on their PMDs to hear the music. This finding is most likely the reason why the group with HL listened at much higher sound volumes compared with those with normal hearing. If this behaviour continues over time, it will increase the risk of hearing loss progression. Given that the study population is relatively young and they are a vulnerable group, this is indeed an alarming result potentially implying that adolescents with hearing loss subject their hearing to even greater risk compared with adolescents with normal hearing.
Almost everyone used their PMDs during transportation, such as bus, car, train, biking and walking. Our measurements on sound levels were done in quiet conditions in an anechoic laboratory. Background noise levels were measured continuously to assure good measuring conditions. However listening to music during transportation where there is background noise would most likely make the listening levels to become louder. Using PMDs when biking or walking in traffic implies a clear risk given that music at a loud volume masks traffic noises, which could serve as a warning signal. Studies on music listening in ear buds and walking or cycling behaviour clearly indicate that auditory stop signals is often missed when persons listened to music (De Waard, Edlinger, and Brookhuis Citation2011; Stavrinos, Byington, and Schwebel Citation2011). This hazardous behaviour may be even more dangerous for people with a hearing loss.
Adolescents with normal hearing used their PMDs during school hours more than those with hearing loss (45/33%), whereas the opposite trend was observed during sleep (21/29%). This finding could arguably be explained by the fact that 19% of the adolescents with hearing loss reported permanent tinnitus compared with 7% among those with normal hearing. One interpretation could therefore be that the PMD for some might be used to mask tinnitus while going to sleep. When comparing hearing symptoms, significantly more adolescents with hearing loss reported sound sensitivity and sound fatigue compared with adolescents with normal hearing. The result is somewhat ambiguous when considering that these adolescents at the same time being the ones listening to louder volumes instead of avoiding them. A suggestion to interpretation could be that this group uses music as a way to screen off disturbing sounds. A common complaint is that hearing aids often attenuate background noise. Hence music could be used as a way of escaping disturbing background noises.
Comparisons between subjects with hearing loss compared with normal hearing subjects regarding preferred sound levels indicated that adolescents with hearing loss listened to sound levels much louder. Twice as many with hearing loss (48/20%) listened at sound levels of 85 dB LAeq,FF or greater, and the result also revealed poorer hearing thresholds for both subjects with normal hearing and those with hearing loss. These results must be interpreted with some caution. Among those with normal hearing, the results might indicate that listening at 85 dB or higher might provide repeated temporary threshold shifts (TTS) resulting in a small but possible progressive permanent threshold shift (PTS). This notion is further stressed by the fact that a notch configuration at 6 kHz was observed, where 20% of the group with normal hearing had a hearing threshold greater than 20 dB HL. This finding could imply an early stage of noise-induced HL. Among the group of adolescents with hearing loss, the configuration was somewhat different. In the left ear, a difference in measured hearing thresholds was observed when comparing those listening at 85 dB LAeq,FF or above with those listening at less than 85 dB LAeq,FF. This finding was true at all frequencies (0.5–8 kHz) ranging between 10 to 30 dB. In the right ear, a difference was observed mainly between 4 and 8 kHz with a 25 dB at 6 kHz. The results indicate that those listening at 85 dB LAeq,FF or higher are those individuals with the poorest hearing thresholds. It is likely that these subjects in this group in the near or more distant future will be candidates for cochlear implants. When comparing right and left ear for the group with congenital hearing loss, we can observe a difference in configuration between left and right ear. The reason for this is difficult to speculate about in this small sample, but we believe that some of the congenital hearing losses could be mixed with some middle ear problems that might affect the results. Among those with hearing loss, approximately half (14/29) listened at levels between 85 and 109 dB. Among those with normal hearing, 10/50 listened at levels between 85 and 100 dB. This result indicates that there is a subgroup of adolescents who listens at very high sound levels, which could lead to future noise-induced hearing loss.
This study raises other questions regarding risks associated with the use of PMDs, such as when biking or walking in traffic areas while listening to PMDs. Other risks include the development of other noise-induced auditory symptoms, such as tinnitus, noise sensitivity and auditory sound fatigue, symptoms that were found in this study. Many studies have been focussing occupational noise exposure among adults; however, less is known about children and adolescents leisure time noise exposure and long-term consequences to the hearing. One important difference between occupational noise exposure and leisure time noise exposure is that for example industrial workers expose themselves every day for several years to loud noises, whereas the exposure time in leisure activities is less in general”. On the other hand, our study indicates that headphone use starts early in life during late childhood and early adolescence. It could be argued from a life time noise exposure perspective, that leisure time noise exposure is merely one contributing factor among others, e.g. occupational noise later in life, which all together increases the risk for developing noise induced hearing loss and other hearing impairments over time.
Conclusions
Adolescents with hearing loss used PDMs in the same manner as adolescents with normal hearing. Adolescents with hearing loss listened to louder sound volumes to compensate for their hearing loss, which significantly increases the risk of more severe hearing loss. This study shows that along with preventive actions among adolescents with normal hearing, there is also an urgent need of longitudinal studies on listening habits, sound levels and exposure time to determine potential risks associated with PMDs and long-term health consequences for both adolescents with NH and adolescents with HL.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Båsjö, S., C. Möller, S. Widén, G. Jutengren, and K. Kähäri. 2016. “Hearing Thresholds, Tinnitus, and Headphone Listening Habits in Nine-Year-Old Children.” International Journal of Audiology 55 (10): 587–596. doi:10.1080/14992027.2016.1190871.
- Basner, M., W. Babisch, A. Davis, M. Brink, C. Clark, S. Janssen, and S. Stansfeld. 2014. “Auditory and Non-Auditory Effects of Noise on Health.” Lancet (London, England) 383 (9925): 1325–1332. doi:10.1016/S0140-6736(13)61613-X.
- Breinbauer, H. A., J. L. Anabalón, D. Gutierrez, R. Cárcamo, C. Olivares, and J. Caro. 2012. “Output Capabilities of Personal Music Players and Assessment of Preferred Listening Levels of Test Subjects: Outlining Recommendations for Preventing Music-Induced HL.” Laryngoscope 122 (11): 2549–2555. doi:10.1002/lary.23596.
- Croghan, N. B. H., A. M. Swanberg, M. C. Anderson, and K. H. Arehart. 2016. “Chosen Listening Levels for Music with and without the Use of Hearing Aids.” American Journal of Audiology 25 (3): 161–166. doi:10.1044/2016_AJA-15-0078.
- De Waard, D.,. K. Edlinger, and K. Brookhuis. 2011. “Effects of Listening to Music, and of Using Handlheld and Handsfree Telephone on Cykling Behaviour.” Transportation Research Part F: Traffic Behaviour and Psychology 14 (6): 626–637. doi:10.1016/j.trf.2011.07.001.
- Hodgetts, W. E., J. M. Rieger, and A. Szarko. 2007. “The Effects of Listening Environment and Earphone Style on Preferred Listening Levels of Normal Hearing Adults Using MP3 Player. Ear & Hearing.” Ear and Hearing 28 (3): 290–297. doi:10.1097/AUD.0b013e3180479399.
- Kähäri, K. R., T. Åslund, and J. Olsson. 2011. “Portable Music Players – Preferred Sound Levels and Listening Habits among Adolescents.” Noise and Health 13 (50): 9–15. doi:10.4103/1463-1741.73994.
- Kasper, C. A. 2006. The Simple Guide to Optimum Health for the MP3 Generation. New York: Craig A. Kasper, Au D.
- Kim, M. G., S. M. Hong, H. J. Shim, Y. D. Kim, C. I. Cha, and S. G. Yeo. 2009. “Hearing Threshold of Korean Adolescents Associated with the Use of Personal Music Players.” Yonsei Medical Journal 50 (6): 771–776. doi:10.3349/ymj.2009.50.6.771.
- Kumar, A., K. Mathew, S. A. Alexander, and C. Kiran. 2009. “Output Sound Pressure Levels of Personal Music Systems and Their Effect on Hearing.” Noise and Health 11 (44): 132–140. doi:10.4103/1463-1741.53357
- Meyer-Bisch, C. 1996. “Epidemiological Evaluation on Hearing Damage Related to Strongly Amplified Music (Personal Cassette Players, Discotheques, Rock Concerts) –High Definition Audiometric Survey on 1364 Subjects.” International Journal of Audiology 35 (3): 121–142.
- Olsen-Widén, S. E., and S. I. Erlandsson. 2004. “The Influence of Socio-Economic Status on Adolescent Attitude to Social Noise and Hearing Protection.” Noise and Health 7 (25): 59–70.
- Peng, J. H., Z. Z. Tao, and Z. W. Huang. 2007. “Risk of Damage to Hearing from Personal Listening Devices in Young Adults.” The Journal of Otolaryngology 36 (3): 181–185. doi:10.2310/7070.2007.0032
- Rydzynski, K., T. Jung, Y. Cazals, A. Davis, A. Hygge, D. Prasher, P. Ravazzani, A. Śliwińska-Kowalska, and H. Verschuure. 2008. SCENIHR (Scientific Committee on emerging and Newly-Identified Health Risks). Scientific opinion on the potential health risks of exposure to noise from personal music plyers and mobile phones including a music playing function. September 23, 2008. Available at: http://ec.europa.eu/health/opinion/en/hearing-loss-personal-music-player-mp3.
- Shargorodsky, J., S. G. Curhan, G. C. Curhan, and R. Eavey. 2010. “Change in Prevalence of HL in US Adolescents.” Journal of American Medical Association 304 (7): 772–778. doi:10.1001/jama.2010.1124
- Stavrinos, S.,. K. Byington, and D. Schwebel. 2011. “Distracted Walking: Cell Phones Increase Injury Risk for College Pedestrians.” Journal of Safety Research 42 (2): 101–107. doi:10.1016/j.jsr.2011.01.004
- Vogel, I., J. Brug, C. P. B. van der Ploeg, and H. Raat. 2007. “ Young Peoples Exposure to Loud Music: A Summary of the Literature.” American Journal of Preventive Medicine 33 (2): 124–133. doi:10.1016/j.amepre.2007.03.016
- Vogel, I., H. Verschuure, C. P. B. van der Ploeg, J. Brug, and H. Raat. 2009. “Adolescents and MP3 Players: To Many Risks, Too Few Precautions.” Pediatrics 123 (6): e953–e958. doi:10.1542/peds.2008-3179
- Widén, S. E., S. Båsjö, C. Möller, and K. Kähäri. 2017. “Headphone Listening Habits and Hearing Thresholds in Swedish Adolescents.” Noise and Health 19 (88): 125–132. doi:10.4103/nah.NAH_65_16
- Zhao, F., K. C. Manchaiah, D. French, and S. M. Price. 2010. “Music Exposure and Hearing Disorders: An Overview.” International Journal of Audiology 49 (1): 54–64. doi:10.3109/14992020903202520