
Abstract
Objective: To investigate the association between childhood sensorineural hearing loss (SNHL) and cohabiting/marriage rates in a large Norwegian cohort.
Design: This study is based on data from the School Hearing Investigation in Nord-Trøndelag (SHINT), data from the Nord-Trøndelag Health Study (HUNT), and registry data on marital status from Statistics Norway. Marital status is measured yearly from 1975–2015 (marriage) and 1987–2014 (cohabitation). The association between SNHL and marital status was tested using multinomial logistic regression models estimating odds ratios (OR) and 95% confidence intervals (CI), adjusting for age, sex, and education.
Study sample: The total sample comprised 50,022 participants born between 1940 and 1980. SNHL in SHINT of 41 dB or more was defined as moderate-profound (N = 216), 26–40 dB as mild (N = 294) and 16–25 dB as slight (N = 246).
Results: There was a significant association between any SNHL and cohabitation (OR = .56, 95% CI = 0.43–0.72) and marriage (OR = .50, 95% CI = 0.40–0.62), between mild SNHL and cohabitation (OR = .58, 95% CI = 0.40–0.86) and marriage (OR = .40, 95% CI = 0.29–0.56), and between moderate-profound SNHL and cohabitation (OR = .43, 95% CI = 0.26–0.71) and marriage (OR = .45, 95% CI = 0.31–0.66).
Conclusions: Childhood SNHL reduces the likelihood of cohabitation and marriage.
Introduction
People with a childhood-onset disability have a lower likelihood of getting married than people with no disability (Macinnes Citation2011; Clarke and Mckay Citation2013; Savage and Mcconnell Citation2016;; Tumin Citation2016). Hearing loss may be perceived as a disability due to the impact on communication and interaction with other people. However, many individuals with hearing loss do not consider themselves to be disabled, but rather to be part of a cultural minority that should be recognised and respected (Burke et al. Citation2011; Muñoz-Baell et al. Citation2011; Sutton-Spence and West Citation2011). Whether considered a disability or merely a cultural marker, hearing loss represents a hindrance to interacting with other people. For example, it is not uncommon for people with hearing loss to withdraw from social activities and events (Arlinger Citation2003), which may reduce the chance of meeting a potential partner. In the United States, as well as other countries, there is a tradition of people with profound hearing loss to choose spouses with profound hearing loss (Nance, Liu, and Pandya Citation2000; Nance Citation2003). Furthermore, a study of marital quality among couples in which one or both partners were classified as deaf found that language compatibility and cultural compatibility were considered hallmarks of a successful marriage in deaf-deaf as well as deaf-hearing couples (Mosier Citation1999). This indicates that people with hearing loss prefer a partner who share their language and culture, which may reduce the pool of potential partners. The very few studies that have investigated marriage rates among people with hearing loss seem to reflect this, since marriage rates are lower for this select population, when compared to normally hearing individuals. Barnett and Franks (Citation2002) reported that 49.8% of the prelingually deaf adult population in the United States was married whereas the corresponding number for hearing adults was 66.1%. Deafness in this study was measured by means of self-report and the participants had “bilateral hearing loss that interferes with understanding speech” (Barnett and Franks Citation2002, 106). A Swedish study (Carlsson, Danermark, and Borg Citation2004) investigated marital status among the deaf (defined as early onset profound hearing loss with sign language as the first language) in two different counties and found a similar trend in which a lower percentage of the deaf (35.1% and 37.1%) was married compared to the hearing population (58.8% and 58.5%). Interestingly, despite very similar percentages of married people within the two different counties, the proportion of deaf/deaf and deaf/hearing couples were very different. In Närke county, which was defined as having a strong deaf community with many deaf inhabitants, 99% of deaf married individuals had a deaf spouse. Conversely, in Värmland county, which had a weak deaf community, only 10% of married deaf people had deaf spouses. The authors pointed out that one possible explanation for this might be that a weak deaf community facilitates social integration and contact between deaf and hearing people. They concluded, though, that even with a large deaf community like the one in Närke, marriage rates did not reach the marriage rates of the general population, and that this might be due to cultural and socioeconomic circumstances. To estimate numbers of cohabitations, the authors identified unmarried, deaf women with children living at home, and found a significantly larger proportion of such relationships in Närke compared to the reference group. There was a similar trend in Värmland, but observations were too few to make any inferences.
There is a large void in the literature when it comes to marriage rates among people with hearing loss. The aim of the present study was to help fill this knowledge gap by investigating rates of marriages and cohabitations among people with childhood sensorineural hearing loss (SNHL) in Norway. Whereas the abovementioned studies focussed on people with severe hearing loss (defined as deaf) only, the present study distinguishes between slight, mild, and moderate-profound hearing loss. To our knowledge, this is the first study to examine marriage rates and cohabitation rates in a large cohort with different degrees of hearing loss. Norway has a Western culture; hence we expect our results to resemble those from Sweden and the United States (Barnett and Franks Citation2002; Carlsson, Danermark, and Borg Citation2004).
Materials and methods
Sample
The present study is based on data from the School Hearing Investigation in Nord-Trøndelag (SHINT), and registry data on marital status from Statistics Norway to investigate the association between childhood hearing loss and marriage in adulthood. The sample includes 50,022 individuals and is restricted to participants with given consent from one of the three waves of the Nord-Trøndelag Health Study (HUNT, i.e. HUNT 1, 2 or 3). The SHINT and the HUNT studies were carried out in Nord-Trøndelag County, which has about 135,000 inhabitants. Please see for an overview of the participant flow. Further details are presented in the following.
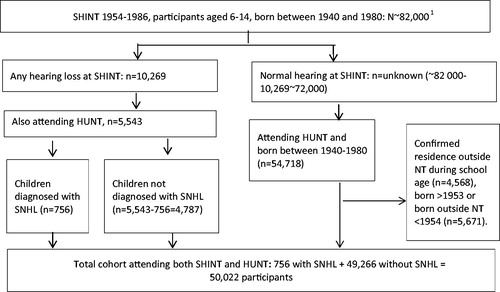
Figure 1. Flow chart of participants from the baseline childhood study (the School Hearing Investigation in Nord-Trøndelag; SHINT) and the age-matched control group study (the Norwegian Health Study; HUNT). 1Children born in Nord Trøndelag between 1940–1980 = 81,920.
The SHINT study
Between 1954 and 1986, every pupil in the first, fourth and/or seventh grade in regular primary school in Nord-Trøndelag County participated in an audiometric screening. The screening took place in a quiet location on the school premises and was performed by a health nurse or a trained hearing assistant. Air-conduction thresholds were obtained by means of pure tone audiometry at 0.25, 0.5, 1, 2, 4, and 8 kHz using Amplivox type 70 or Amplivox model 51 screening audiometers following the international standard at all times. Pupils were registered with hearing loss if they had thresholds of 20 dB or greater at three or more frequencies in the same ear and/or a threshold of 30 dB or more at one or more frequencies. No records were made for pupils without hearing loss. This means that the exact number of participants is unknown. We do know, however, that the children who participated in the SHINT were born between 1940 and 1980, and we know that a total of 81,920 children were born in Nord-Trøndelag in this period. It is likely that most of these children participated in the screening at some point, either at one, two or all three time points. A total of 10,269 children tested positive for hearing loss at the screening and were invited to have their hearing further tested with a full examination by an Ear- Nose- and Throat (ENT) specialist at one of the 14 out-patient clinics in Nord-Trøndelag. Questionnaire data regarding the children’s ear problems were also collected from the parents. The visit at the ENT specialist’s office included new puretone audiometry thresholds with both air- and bone-conduction as well as a complete medical examination including family and medical history. The ENT specialists at the time mainly used clinical Amplivox Model 81 audiometers with supra-aural earphones (Fabritius Citation1968). The ENT specialist recorded findings and hearing disorder diagnoses (for example, SNHL, otitis media, etc.), and we based our sample on these diagnoses. To ensure correct classification, the children underwent at least one ENT examination and sometimes more, depending on the diagnosis. The SHINT was led by the late otolaryngologist Hans Fabritius. He defined SNHL as a hearing loss in which the air-conduction thresholds followed those of the bone-conduction. The maximum accepted air-bone gap was omitted from the definition of SNHL. Fabritius and his team were renowned for their diligent work, so there is reason to believe that the high attendance rate of 97% between 1954 and 1962 persisted (Fabritius Citation1968).
The HUNT studies
The HUNT studies were large general health surveys that comprised the entire adult population in Nord-Trøndelag County. HUNT 1 was carried out in 1984–1986 (about 75,000 participants, response rate about 90%), HUNT 2 in 1995–1997 (70,000, 70%), and HUNT 3 in 2006–2008 (60,000, 56%). In the present study, we link data from the SHINT with data from the HUNT studies in order to obtain a matched control group. Out of the 10,269 children that tested positive for hearing loss at the screening in the SHINT, 5543 also participated in HUNT 1, 2 or 3. As mentioned above, the exact number of participants in the SHINT is unknown. However, it is likely that many of the 81,920 children who were born in Nord-Trøndelag between 1940 and 1980 participated in the SHINT, and we know that 10,269 of these children tested positive for hearing loss at the screening This means that about 72,000 children (82,000 − 10,269) most likely had no hearing loss. Many of the children who did not test positive for hearing loss in the SHINT probably also participated in the HUNT. Therefore, we use those HUNT participants who did not screen positive for hearing loss in the SHINT and who were born in the same period as the SHINT participants as our control group (N = 54,414). For participants born 1954 and later, we have information of residence during primary school age; for participants born before 1954, we have information of residence at birth. We excluded those born 1954 and later with confirmed residence outside Nord-Trøndelag during primary school age (N = 5671) and those born before 1953 with confirmed residence outside Nord-Trøndelag at birth (4568), resulting in 50,022 controls.
The final sample
For the purpose of the present study, children diagnosed with SNHL in the SHINT were selected as our case group. Altogether, 216 people were classified with moderate-profound SNHL, 294 with mild SNHL, and 246 with slight SNHL (see further details under “measures”). The final sample is thus comprised of 756 people with any degree of SNHL and 49,266 controls; in total, 50,022 people.
Measures
Childhood SNHL (predictor)
Hearing was measured in the SHINT by pure-tone audiometry at 0.25, 0.5, 1, 2, 4, and 8 kHz. The range for registered hearing levels (HL) was 20−100 dB. HLs below 20 dB were not registered, and HLs of 100 dB or more were registered as “100 dB HL”. In the present study, we used the last audiogram from the ENT examination to estimate the bilateral pure-tone average (PTA) as the average over hearing thresholds of 0.5, 1, 2, and 4 kHz over both ears. We defined moderate-profound hearing loss as PTA of 41–100 dB HL (moderate, severe, and profound hearing loss were placed in the same category in order to ensure sufficient group size for the analyses), mild hearing loss as PTA 26–40 dB HL and slight hearing loss as PTA 16–25 dB HL.
Partner status (outcome)
Data on cohabitation and marriage were available from Statistics Norway yearly from 1987–2014 and 1975–2015, respectively.
Control variables
A number of variables may confound the association between hearing loss and partner status. We controlled for age, sex and education. Education is also a potential mediator.
Treatment of missing values
Since no records were made for children with normal hearing in the SHINT, values below 20 dB were missing for many frequencies. Therefore, we replaced the missing value for each frequency with the frequency specific mean values of the scores below 20 dB from the original sample (N = 10,269).
Data on the outcome variable of partner status from Statistics Norway are regarded as complete. Participants with missing data on education (0.2%) were excluded from our analyses.
Design and statistical analyses
This study applies a longitudinal cohort design, investigating the association between childhood SNHL at baseline starting in 1954 and partner status in adulthood registered yearly from 1975 to 2015.
First, we explored partner status among people with SNHL descriptively. Second, we tested the association between SNHL and partner status using multinomial logistic regression models estimating odds ratios (ORs) and 95% confidence intervals (95% CIs). All statistical tests were run using Stata (StataCorp. Citation2017) to perform two-tailed analyses calculated at a 95% confidence interval (p < 0.05). The first model tested the association between SNHL and partner status, whereas the second model tested the same association adjusted for control variables.
Results
Descriptive statistics on SNHL, partner status, as well as mean age (measured in 2015) are presented in . In general, marriage rates are lower among people with hearing loss than among people without hearing loss, whereas cohabitation rates are actually slightly higher among people with hearing loss. A total of 647 people with hearing loss were cohabiting or married, corresponding to 85.6%, whereas, a total of 45,781 people without hearing loss were cohabiting or married, corresponding to 92.9%.
Table 1. SNHL, partner status and age.
The results from the multinomial logistic regression analyses are presented in . There is an overall, significant association between any hearing loss and cohabiting/being married (Model 1), respectively, in which people with hearing loss have .56 times lower odds of cohabiting and .50 times lower odds of being married, compared to people with normal hearing. People with mild hearing loss have significantly lower odds of cohabiting (.58) or being married (.40) compared to people with normal hearing. Similarly, people with moderate-profound hearing loss also have significantly lower odds of cohabiting (.43) or being married (.45) compared to people with normal hearing.
Table 2. Multinomial logistic regression with SNHL as predictor of partner status.
Discussion
The present study investigated rates of marriage and cohabitation among people with childhood SNHL in Norway. The results showed that childhood SNHL reduce the likelihood of marriage and cohabitation later in life for people with mild or moderate-profound hearing loss, but not for people with slight hearing loss.
The marriage rate observed in our sample was 67.9% in the SNHL case group, which is higher than corresponding numbers from previous American and Swedish studies (Barnett and Franks Citation2002; Carlsson, Danermark, and Borg Citation2004), in which 49.8% and 35.1–37.1% of people with hearing loss were married, respectively. One explanation might be that the group of people with hearing loss in our study is heterogenous with respect to degree of hearing loss, including slight, mild and moderate-profound hearing loss, whereas, the study population in the other two studies were prelingually deaf (United States) and (mostly prelingually) deaf (Sweden). It is possible that the marriage rates in those studies had been somewhat higher if they had included people with mild and slight hearing losses as well. However, the difference in marriage rate between people with and without hearing loss is similar within each country.
In our study, cohabitation rates are slightly higher among people with hearing loss than among people without hearing loss. This supports the trend reported by Carlsson et al. (Citation2004), who found a significantly larger number of cohabitations among unmarried, deaf women compared to the hearing population. However, the results from the multinomial logistic regression analyses in our study show that people with mild or moderate-profound hearing loss as well as people in the group “any hearing loss” have significantly lower odds of cohabiting or marrying compared to people with normal hearing. This is in line with the results from the previously mentioned studies from Sweden and United States (Barnett and Franks Citation2002; Carlsson, Danermark, and Borg Citation2004).
There was no difference between people with slight hearing loss and people with no hearing loss in our study when it comes to cohabiting or marrying. This suggests that there might be a tipping point, in which mild as well as the more severe hearing losses impose a greater hindrance on cohabitation and marriage than a slight hearing loss does. This may be taken as support for research showing that people with a childhood-onset disability tend to be less likely to get married than people with no disability (Macinnes Citation2011; Clarke and Mckay Citation2013; Savage and Mcconnell Citation2016; Tumin Citation2016).
A hearing loss greater than 30 dB in the better hearing ear in children is considered disabling (WHO. Citation2019). In the present study, we defined slight hearing loss as 16–25 dB HL, mild hearing loss as 26–40 dB HL, and moderate-profound hearing loss as 41–100 dB HL. From a disability perspective it makes sense, then, that a slight hearing loss does not represent a disability in terms of building a relationship that eventually leads to cohabitation or marriage. Mild and moderate-profound hearing losses, on the other hand, seem to impede the forming of marriage/cohabiting relationships. From a cultural perspective, however, an alternative explanation could be that people with more severe hearing losses prefer partners who share their language and/or culture, significantly reducing the number of potential partners. Cultural and socioeconomic circumstances have been suggested as explanations for lower marriage rates previously, for example by Carlsson et al. (Citation2004).
In an earlier paper, we studied the association between childhood SNHL and highest obtained education in adulthood (Idstad and Engdahl Citation2019). We found that people with SNHL were about half as likely to complete higher education as people with normal hearing. In the present study, we included education as a control variable in order to adjust for a potential effect on cohabitation/marriage rates. Since we detected a significant association between SNHL and cohabitation/marriage rates after controlling for education, this provides evidence that the effect of SNHL goes beyond that of education.
The present study has several strengths. It is based on data from a large cohort covering an entire county, and the participants are followed for several decades. SNHL is measured by means of pure tone audiometry, often described as a gold standard for hearing loss assessment, and thorough examination by an ENT Specialist. However, our results should be viewed in the context of some limitations. Although the participants had their hearing tested in their childhood, we do not know whether the hearing loss is prelingual or if it occurred during primary school. Furthermore, it would have been interesting to know whether the people with hearing loss in our study that cohabit or are married have partners who also have a hearing loss. This information would have enabled comparison of the results from this study to those from the Swedish study (Carlsson, Danermark, and Borg Citation2004) not only on cohabitation and marriage rates per se, but also on the partner’s hearing status. Finally, we do not have data on whether participants were fitted with Cochlear implants or used hearing aids. This would obviously affect communication, which in turn might affect the forming and building of romantic relationships that could lead to cohabitation and marriage.
In conclusion, our study suggests that SNHL reduces the likelihood of cohabitation and marriage. More studies are needed to better understand the underlying mechanisms. Future research should include information on both partners’ degree of hearing loss, preferences regarding language and culture, and use of hearing aids and Cochlear implants.
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, NTNU), Nord-Trøndelag County Council and the Norwegian Institute of Public Health. The authors also thank our colleagues in Nord-Trøndelag involved in the School Hearing Investigation.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of the study are available from the HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, NTNU) upon application. Restrictions apply to the availability of these data, which were used under licence for this study.
Additional information
Funding
References
- Arlinger, S. 2003. “Negative Consequences of Uncorrected Hearing Loss—A Review.” International Journal of Audiology 42 (Sup 2): 17–20. doi:10.3109/14992020309074639.
- Barnett, S., and P. Franks. 2002. “Health Care Utilization and Adults Who Are Deaf: Relationship with Age at Onset of Deafness.” Health Services Research 37 (1): 103–118. doi:10.1111/1475-6773.99106.
- Burke, T. B., P. Kushalnagar, G. Mathur, D. J. Napoli, C. Rathmann, and K. Vangilder. 2011. “Language Needs of Deaf and Hard-of-Hearing Infants and Children: Information for Spiritual Leaders and Communities.” Journal of Religion, Disability and Health 15 (3): 272–295. doi:10.1080/15228967.2011.590644.
- Carlsson, P., B. Danermark, and E. Borg. 2004. “Marital Status and Birthrate of Deaf People in Two Swedish Counties: The Impact of Social Environment in Terms of Deaf Community.” American Annals of the Deaf 149 (5): 415–427. doi:10.1353/aad.2005.0010.
- Clarke, H., and S. Mckay. 2013. “Disability, Partnership and Parenting.” Disability and Society 29 (4): 543–555. doi:10.1080/09687599.2013.831745.
- Fabritius, H. F. 1968. “Hearing Investigations of School Children in North Trøndelag County.” Journal of Oslo City Hospital 18: 5–44.
- Idstad, M., and B. Engdahl. 2019. “Childhood Sensorineural Hearing Loss and Educational Attainment in Adulthood: Results from the HUNT Study.” Ear and Hearing 40 (6): 1359–1367. doi:10.1097/AUD.0000000000000716.
- Macinnes, M. D. 2011. “Altar-Bound? The Effect of Disability on the Hazard of Entry into a First Marriage.” International Journal of Sociology 41 (1): 87–103. doi:10.2753/IJS0020-7659410105.
- Mosier, A. G. 1999. Marital Quality in Deaf-Deaf and Deaf-Hearing Marriages. Ann Arbor, MI: U.M.I.
- Muñoz-Baell, I. M., M. T. Ruiz-Cantero, C. Álvarez-Dardet, E. Ferreiro-Lago, and E. Aroca-Fernández. 2011. “Comunidades Sordas: ¿Pacientes o Ciudadanas? [Deaf Communities: Patients or Citizens?].” Gaceta Sanitaria 25 (1): 72–78. doi:10.1016/j.gaceta.2010.09.020.
- Nance, W. E. 2003. “The Genetics of Deafness.” Mental Retardation and Developmental Disabilities Research Reviews 9 (2): 109–119. doi:10.1002/mrdd.10067.
- Nance, W. E., X. Liu, and A. Pandya. 2000. “Relation Between Choice of Partner and High Frequency of Connexin-26 Deafness.” The Lancet 356 (9228): 500–501. doi:10.1016/S0140-6736(00)02565-4.
- Savage, A., and D. Mcconnell. 2016. “The Marital Status of Disabled Women in Canada: A Population-Based Analysis.” Scandinavian Journal of Disability Research 18 (4): 295–303. doi:10.1080/15017419.2015.1081616.
- StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC.
- Sutton-Spence, R., and D. West. 2011. “Negotiating the Legacy of Hearingness.” Qualitative Inquiry 17 (5): 422–432. doi:10.1177/1077800411405428.
- Tumin, D. 2016. “Marriage Trends among Americans with Childhood-Onset Disabilities, 1997–2013.” Disability and Health Journal 9 (4): 713–718. doi:10.1016/j.dhjo.2016.05.004.
- WHO. 2019. https://www.who.int/news-room/fact-sheets/detail/deafness-and-hearing-loss.