
Abstract
Objective
The clinical audiology test battery often involves playing physically simple sounds with questionable ecological value to the listener. In this technical report, we revisit how valid this approach is using an automated, involuntary auditory response; the acoustic reflex threshold (ART).
Design
The ART was estimated four times in each individual in a quasi-random ordering of task conditions. The baseline condition (referred to as Neutral) measured the ART following a standard clinical practice. Three experimental conditions were then used in which a secondary task was performed whilst the reflex was measured: auditory attention, auditory distraction and visual distraction tasks.
Study sample
Thirty-eight participants (27 males) with a mean age of 23 years were tested. All participants were audiometrically healthy.
Results
The ART was elevated when a visual task was performed at the same time as the measurements were taken. Performing an auditory task did not affect the ART.
Conclusions
These data indicate that simple audiometric measures widely used in the clinic, can be affected by central, non-auditory processes even in healthy, normal-hearing volunteers. The role of cognition and attention on auditory responses will become ever more important in the coming years.
Introduction
The acoustic reflex (AR) can be used in clinical settings as a screen for retrocochlear lesions, and to confirm suspected conductive hearing losses (Prasher and Cohen Citation1993). Being a reflex, it is automatic and occurs without the listener needing to make any decision or overtly indicate a response. A loud sound, the elicitor, is played into one ear and this causes the stapedius muscle to contract and stiffen the ossicular chain in both ears, which reduces the amount of energy that is transduced from the outer ear to the inner ear (Gelfand Citation2009). These changes are frequency-dependent and so the spectral content of the elicitor determines the nature of changes in energy transduction by the middle ear.
Patients are instructed to sit still and ignore the sounds heard, but, it has long been known that acoustic reflex thresholds (ARTs) are modulated when performing a secondary task, with elevated ARTs and diminished AR strength when auditory, visual and arithmetic tasks are performed concurrently with measuring reflexes (Bell Citation1966; Durrant and Shallop Citation1969). AR strength is typically defined as supra-threshold growth, and so diminished AR strength is observed as a reduction in this supra-threshold growth function. Klockhoff (Citation1961), Bell (Citation1966) and Durrant and Shallop (Citation1969) all investigated the effect of several different secondary tasks, including auditory and non-auditory tasks of varying complexity, on acoustic reflexes. They found that when performing a secondary task, the ARTs were elevated. This change in ART was primarily driven by whether a secondary task was being performed, rather than the specific modality (auditory or visual) or complexity (i.e. reading from a newspaper or counting backwards in 7s from 100) of the secondary task.
Conversely, Cleaver (Citation1974) demonstrated that the reflex strength was increased when a person closed their eyes. Robinette and Snyder (Citation1982) performed a systematic investigation of how occular muscle tension interacts with measurements of the AR by using conditions of light and darkened rooms in conjunction with the eyes being closed tightly, softly, or by using a visual task stimulus. Closure of the eyes resulted in an enhanced AR (both lower ARTs and increased growth functions), with voluntary muscle tension from tight closure resulting in a greater enhancement. Both passive and active visual tasks, a number manipulation task and vibrotactile stimulation all resulted in suppression of the AR. These enhancements and suppressions of the AR were expressed as both reduced suprathreshold amplitude and elevated thresholds. It seems clear that whilst the perceptual tasks described previously resulted in a reduction in AR strength, there are also physiological mechanisms which result in muscle movement enhancing the AR (Gruters et al. Citation2018; Tasko et al. Citation2022). It may therefore be important to understand how these competing mechanisms function in both the clinic and the real world.
Though AR is a diagnostic tool in the clinic, its evolutionary significance is unknown. Typically it is thought to be protective; to attenuate the amount of high-intensity energy, and perhaps internally generated sound, transmitted through the inner ear (Brask Citation1979; Borg, Counter, and Rosler Citation1984). But this protective element is only obtained for transient loud sounds, not sustained ones. There is much we are still learning about the mechanics of the middle ear (Ugarteburu et al. Citation2022), and it is, therefore, difficult to predict what mechanisms lead to the AR being affected by these central, possibly cognitive factors. There may, therefore, be value in considering the specific instructions given to participants when performing routine, objective auditory assessments. There are also potentially wider implications for the role of attention across the whole audiological test battery (Nixon, Sarant, and Tomlin Citation2019).
The primary research aim was to investigate how secondary tasks, involving some level of cognitive control in either the auditory or non-auditory domain, affect ARTs. Based on the reviewed evidence, the hypothesis was that both auditory and visual tasks will result in an increase in ART. Secondary, exploratory hypotheses focussed on whether the visual task resulted in a larger change in ART (as reported by Bell Citation1966) and whether there is a difference between the two auditory tasks; described as attention and distraction depending on whether the listeners’ attention is directed towards or away from the sounds used to elicit the reflex.
Methods
Participants
A total of 38 participants (27 males) with a mean age of 23 years (S.D. 4 years) were tested. The sample size was chosen based on work within our laboratory which demonstrated that the variability of ARTs measured two hours apart was on average 1 dB (S.D. ± 1.6) and 1.1 dB (S.D. ± 1.5) for a 1000 Hz tonal elicitor and broadband noise elicitor, respectively. An a priori power analysis showed a minimum of 34 participants would allow the detection of a 2 dB shift in threshold (assuming S.D. ±f 4 dB) with 80% power and a two-tailed alpha of 5%. An additional ∼15% were recruited to allow for attrition, given the total cohort size of 38. All participants provided informed, written consent and the study protocol was approved by the University of Manchester Ethical Review Board. Volunteers were enrolled in the study by responding to advertisements placed around the University campus.
Pure tone audiometry
Pure tone audiometry was performed using a GSI Arrow audiometer with TDH-39 headphones and MX41 AR cushions, following the British Society of Audiology Recommended Procedures (BSA Citation2018). Participants were required to have audiometric thresholds of 20 dB HL or better in both ears at the octave frequencies between 250 Hz and 4000 Hz, with any asymmetry 10 dB or less at each frequency. Tympanometry was performed using a GSI Tympstar middle ear analyser, following recommended procedures (BSA Citation2013). Normal tympanograms were also required to permit participation in the study (middle ear pressure from +50 to −50 da Pa, middle ear compliance 0.3–1.6 cm3).
Acoustic reflex measurement
ARs were measured using a GSI Tympstar middle ear analyser. Ipsilateral reflex thresholds were measured from the right ear. The probe tone was 226 Hz tone. The reflex eliciting stimuli were a 1000 Hz pure tone and a broadband noise (BBN), each of 1-second duration. The starting sound level was 70 dB HL for the 1000 Hz tone and 60 dB HL for the BBN. A reflex was defined as a reduction in compliance of at least 0.02 mmho. If no reflex was seen, the level of the elicitor was increased by 2 dB. Once a reflex was identified at a presentation level, an additional elicitor was presented at 2 dB above that presentation level to verify reflex growth (thus establishing the true presence of a reflex) before reducing the presentation level by 10 dB. The 2 dB step-wise increases were then repeated to establish a reliable response. The lowest sound level which produced a reliable response (reliably defined as producing a reflex on each of three consecutive presentations) was recorded as the ART.
Task conditions
The ART was estimated four times in each individual in a quasi-random ordering of task conditions. The four task conditions were as follows:
Neutral (N): the ART was measured according to the standard procedure described above, without a specific task.
Auditory Attention (AA): There were no additional stimuli presented, but participants were instructed to count and report the number of reflex-eliciting stimuli heard in the test ear. In this condition, the attention of the listener was focused on the auditory domain and directed towards the sounds which were integrally involved in measuring the AR.
Auditory Distraction (AD): additional stimuli were presented via a BOSE Sound Link 2 loudspeaker located at eye level, 0 degrees azimuth and 1 metre from the participant. The stimuli were 2000 Hz tone pulses, with a random duration between 0.5 to 4 seconds, and a random inter-pulse interval between 0.5 to 2 seconds. There were 8–12 tones presented in each block before a response was required. The sound level was calibrated using a Bruel and Kjaer sound level metre 2250 and was fixed at a comfortable listening level of 74 dB SPL. Stimuli were detected in the unoccluded left/contralateral ear, and participants reported the number of stimuli heard. In this condition, the listeners’ attention was also focused on the auditory domain, but the stimuli to which the listener had to attend was not involved in eliciting or measuring the reflex. The purpose of this was to ascertain if attending to sounds which are not eliciting a reflex results in a change in the ART.
Visual Distraction (VD): additional stimuli consisted of a black spot, easily visible, which appeared at pseudo-random positions on the computer screen for random durations (0.5–4 seconds) and with a randomly selected inter-presentation-interval from the interval 0.5 to 2 seconds. The stimulus was presented via a MacBook Air laptop, situated 1 metre from the participant at 0 degrees azimuth and eye level. Participants were required to count the number of presentations on this spot. In this condition, the listeners’ attention was explicitly directed away from the auditory domain.
For dual-task experimental conditions (2–4 above) participants were to be excluded if their reported count exceeded ±10 from the true value. No participants were excluded from the data analysis due to this criterion.
Results
The mean ARTs (and 95% confidence intervals) were obtained by averaging across the right ear of all participants, and are shown in . The thresholds for the BBN elicitor were obtained with a sound level around 12 dB lower than those obtained using the 1000 Hz tonal elicitor, which is a well-established finding in the literature (Keefe et al. Citation2017; Causon et al. Citation2020).
Figure 1. Mean ARTs (and 95% confidence intervals) are shown for each of the four conditions for both elicitors. The x-axis labels denote the four conditions: (N) neutral, (AA) auditory attention, (AD) auditory distraction and (VD) visual distraction.
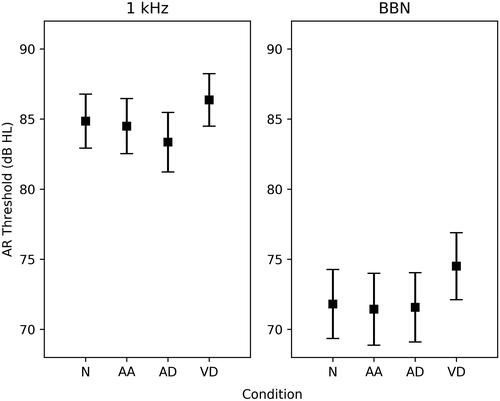
For the 1000 Hz tonal elicitor, the average threshold for the VD condition was 1.5 dB greater than the N condition and 1.9 dB and 3.0 dB greater than the AA and AD conditions, respectively. A one-way repeated measures ANOVA, corrected for a violation of sphericity, revealed a significant effect of condition; F (3, 111) = 15.05, p < 0.001). Post-hoc analyses indicated that the visual distractor condition resulted in significantly higher thresholds compared to all other conditions (p ≤ 0.002).
For the BBN elicitor, the VD condition evoked thresholds which were on average 2.7 dB greater than those in the N condition and 3.1 dB and 2.9 dB greater than AA and AD thresholds, respectively. A one-way repeated measures ANOVA, corrected for a violation of sphericity, revealed a significant effect of condition; F (3,111) = 12.98, p < 0.001. Post-hoc analyses indicated that the VD condition resulted in significantly elevated thresholds compared to all other conditions (p < 0.001).
Discussion
The current experiment aimed to explore the effect of different attentional states on the acoustic reflex threshold. The hypothesis was that performing any task would result in an increase in ARTs. It was of interest to establish the size of these changes with modern electroacoustic bridges, and to observe if there was a difference between what we termed auditory attention and auditory distraction. Contrary to the expected effects, both auditory tasks resulted in no change in ARTs relative to the neutral condition. Only the visual task resulted in a statistically significant elevation of ART.
What is the mechanism for top-down modulation of these “automatic” responses?
It is our view that in order to understand the relevance of how attentional state and secondary tasks might impact hearing, both in the real world and the laboratory, we must understand the mechanism by which modulation of these responses occurs. The attentional state has been shown to affect a number of peripheral auditory responses, such as pure tone hearing thresholds (Heinrich, Ferguson, and Mattys Citation2020), AR magnitude and threshold, evoked otoacoustic emissions (de Boer and Thornton Citation2007) and speech audiometry response times (Lee and Lee Citation2022). Maison and Liberman (Citation2000) provide hypotheses that could explain the role of the top-down efferent system, which projects from the medial oliviocochlear bundle to the outer hair cells of the cochlea. One of these hypotheses is that the system subserves attention and there are two main views; (i) the attentional mechanism is intermodal, and auditory peripheral responses are inhibited during a visual attention task (Hernandez-Peon, Scherrer, and Jouvet Citation1956), and (ii) an auditory attentional filter exists, in which auditory responses are inhibited by directed attention in the auditory domain (Froehlich et al. Citation1990). Our data support the first of these hypotheses; however, it is difficult to reconcile this with the fact that other auditory responses, such as otoacoustic emissions and PTAs have been shown to also be affected by auditory attention tasks.
It is necessary to determine if the mechanism affecting all peripheral auditory responses is the same, and if so the extent to which it is domain specific. The best way to do this is to collect a number of baseline peripheral auditory responses in a single cohort of listeners and measure the extent to which these are inhibited by auditory and non-auditory attentional demands.
Is the effect size too small to be of interest or value?
The magnitude of change in ART was ∼3 dB for the broadband elicitor, which is consistent with previous studies (Robinette and Snyder Citation1982). As noted by Robinette and Snyder (Citation1982), a change of this size is easy to dismiss as negligible and/or irrelevant; however, 14% their participants showed changes in ART greater than 10 dB. In our experiment, 4 (10%) participants showed changes of 8 dB or greater. It is still not clear whether there is any possible clinical, or real-world, a consequence for a change in the threshold of this size in a small percentage of people.
We certainly make no strong claims at the moment that this effect size is important. However, it must be acknowledged that many studies in this area: a) use well-controlled clinical settings for these measurements, and b) typically test healthy, normal-hearing listeners. Heinrich, Ferguson, and Mattys (Citation2020) showed an effect of cognitive load on pure tone hearing thresholds in older listeners but not younger listeners. It is conceivable that the effect of a secondary task would be larger in listeners with elevated pure-tone hearing thresholds and that the effect may be exacerbated in older listeners. It may also be the case that the effect is more pronounced in a real-world environment, which is less predictable. It is our view that further work involving a wider range of participant demographics and more ecologically valid experimental paradigms is needed before the effect can be dismissed as too small to be of clinical importance.
Potential implications for the clinic and the laboratory
It is desirable that clinical tests are accurate and reliable, in order to obtain the best evaluation of hearing health in a patient. There are some relatively straightforward extrapolations from these data which may have some clinical relevance. Cleaver (Citation1974) showed that tightly closing the eyes increases the reflex magnitude. Indeed though we attribute the changes in ART on the visual distraction condition to attention, it could also be related to the muscular movement of the eyes. This would be a good candidate for future study, investigating how visual attention tasks with and without significant eye movements affect the AR. As noted earlier, the size of the effect may well be larger in listeners’ with hearing loss and with increased age. It may well be that the attention of a patient in the clinic needs controlling better. There may also be diagnostic and screening functions for the reflex beyond its current uses, for example in understanding how well central gain mechanisms are functioning (Brotherton et al. Citation2017), or as a compliment to speech-in-noise testing (de Andrade et al. Citation2011). But to unlock the utility of these approaches, the mechanistic processes underlying the reflex must be full characterised.
AR is also a very popular research tool to study sub-clinical hearing changes in the field of cochlear synaptopathy. The reflex has been shown to be nearly absent in listeners with tinnitus, possibly due to a lack of cochlear synapses (Wojtczak, Beim, and Oxenham Citation2017). It has also been shown in animal models that a reduced ART is a reliable indicator of an auditory system that has lost a significant number of cochlear synapses due to noise exposure (Valero et al. Citation2018). Recently several studies have used the acoustic reflex to further explore the possible role the AR has in elucidating cochlear synaptopathy in human listeners (Bharadwaj et al. Citation2019; Mepani et al. Citation2019). However the data presented here, in addition to historic literature on the effect secondary tasks have on the AR, highlight how the nature of the AR may not translate analogously across different species.
Our primary aim in revisiting this topic was not specifically to quantify the magnitude of the threshold shift, but to establish which types of measures and tasks makes sense to pursue further. It is clear from the experimental results presented here that the AR is affected by a visual attention task, consistent with an intermodal attentional hypothesis pertaining to the efferent projections from the medial oliviocochlear bundle to the cochlea. Our primary long-term goal is to understand what mechanisms underpin this change in ART and what clinical and real-world relevance it may have. This must be done across a range of different peripheral auditory responses in order to build up a coherent account of the mechanistic processes involved.
Conclusions
We found mean ARTs to be elevated during a visual attention task by ∼ 3 dB, but not by auditory attention/distraction tasks.
The mechanism whereby visual attention affects automatic peripheral auditory responses remains unclear.
Future work should cover a range of peripheral auditory responses in the same individuals and ascertain if the true effect size is larger in the real world than in the laboratory.
Basic and translational research studies which use the AR as a quantitative response measure (for instance when studying deprivation, synaptopathy, central gain etc.) may benefit from controlling these aspects of attentional influence.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bell, D. W. 1966. Effects of task performance upon the acoustic reflex. Unpublished Ph.D diss., University of Southern California.
- Bharadwaj, H. M., A. R. Mai, J. M. Simpson, I. Choi, M. G. Heinz and B. G. Shinn-Cunningham. 2019. “Non-invasive assays of cochlear synaptopathy – Candidates and Considerations.” Neuroscience 407: 53–66. doi:10.1016/j.neuroscience.2019.02.031.
- Borg, E., S. A. Counter, and G. Rosler. 1984. “Theories of middle ear function.” In The Acoustic Reflex: Basic Principles and Clinical Applications, edited by Silman S, 63–99. Orlando FL: Academic Press.
- Brask, T. 1979. “The noise protection effect of the stapedius reflex.” Acta oto-Laryngologica. Supplementum 360: 116–117. doi:10.3109/00016487809123490.
- British Society of Audiology 2018. Pure-tone air-conduction and bone-conduction threshold audiometry with and without masking. Recommended Procedure. British Society of Audiology, Reading, UK.
- British Society of Audiology. 2013. Tympanometry. Recommended. Procedure. British Society of Audiology, Reading UK.
- Brotherton, H., C. J. Plack, R. Schaette, and K. J. Munro. 2017. “Using acoustic reflex threshold, auditory brainstem response and loudness judgments to investigate changes in neural gain following acute unilateral deprivation in normal hearing adults.” Hearing Research 345: 88–95. doi:10.1016/j.heares.2017.01.009.
- Causon, A., K. J. Munro, C. J. Plack, and G. Prendergast. 2020. “The role of the clinically obtained acoustic reflex as a research tool for subclinical hearing pathologies.” Trends in Hearing 24:2331216520972860. doi:10.1177/2331216520972860.
- Cleaver, V. C. G. 1974. “The effects of mental set on the acoustic reflex.” M.Sc. diss., University of Southampton, England.
- de Andrade, K. C. L., E. D. Camboim, I. d A. Soares, M. V. d S. Peixoto, S. C. Neto, and P. d L. Menezes. 2011. “The importance of acoustic reflex for communication.” American Journal of Otolaryngology 32 (3): 221–227. doi:10.1016/j.amjoto.2010.02.002.
- de Boer, J., and A. R. Thornton. 2007. “Effect of subject task on contralateral suppression of click evoked otoacoustic emissions.” Hearing Research 233 (1–2): 117–123. doi:10.1016/j.heares.2007.08.002.
- Durrant, J. D., and J. K. Shallop. 1969. “Effects of Differing States of Attention on Acoustic Reflex Activity and Temporary Threshold Shift.” The Journal of the Acoustical Society of America 46 (4): 907–913. doi:10.1121/1.1911809.
- Froehlich, P., L. Collet, J. M. Chanal, and A. Morgon. 1990. “Variability of the Influence of a Visual Task on the Active Micromechanical Properties of the Cochlea.” Brain Research 508 (2): 286–288. doi:10.1016/0006-8993(90)90408-4.
- Gelfand, S. A. 2009. “The acoustic reflex.” In: Katz J, Medwetsky L, Burkard R & Hood L (eds.) Handbook of Clinical Audiology. Philadelphia, PA: Wolters Kluwer, 189–221.
- Gruters, K. G., D. L. K. Murphy, C. D. Jenson, D. W. Smith, C. A. Shera, and J. M. Groh. 2018. “The Eardrums Move when the Eyes move: A Multisensory Effect on the Mechanics of Hearing.” Proceedings of the National Academy of Sciences of the United States of America 115 (6): E1309–E1318. doi:10.1073/pnas.1717948115.
- Heinrich, A., M. A. Ferguson, and S. L. Mattys. 2020. “Effects of Cognitive Load on Pure-tone Audiometry Thresholds in Younger and Older Adults.” Ear and Hearing 41 (4): 907–917. doi:10.1097/AUD.0000000000000812.
- Hernandez-Peon, R., H. Scherrer, and M. Jouvet. 1956. “Modification of electric activity in cochlear nucleus during attention in unanesthetized cats.” Science 24 ( 123): 331–332. doi: 10.1126/science.123.3191.331.
- Keefe, D. H., M. P. Feeney, L. L. Hunter, and D. F. Fitzpatrick. 2017. “Aural Acoustic Stapedius-Muscle Reflex Threshold Procedures to Test Human Infants and Adults.” Journal of the Association for Research in Otolaryngology : JARO 18 (1): 65–88. doi:10.1007/s10162-016-0599-z.
- Klockhoff, I. 1961. “Middle Ear Muscle Reflexes in Man. A Clinical and Experimental Study with Special Reference to Diagnostic Problems in Hearing Impairment.” Acta Otolaryngol Suppl 164: 1–92.
- Lee, S. J., and S. Lee. 2022. “Clinical utility of response time in speech audiometry in elderly with mild cognitive impairment”, International Journal of Audiology 1–6. doi:10.1080/14992027.2022.2047234.
- Maison, S. F., and M. C. Liberman. 2000. “Predicting Vulnerability to Acoustic Injury with a Noninvasive Assay of Olivocochlear Reflex Strength.” The Journal of Neuroscience : The Official Journal of the Society for Neuroscience 20 (12): 4701–4707. doi:10.1523/JNEUROSCI.20-12-04701.2000.
- Mepani, A. M., S. A. Kirk, K. E. Hancock, K. Bennett, V. de Gruttola, M. C. Liberman, and S. F. Maison. 2019. “Middle Ear Muscle Reflex and Word Recognition in “Normal-Hearing” Adults: Evidence for Cochlear Synaptopathy?” Ear and Hearing 41: 25–38. doi: 10.1097/AUD.0000000000000804.
- Nixon, G. K., J. Z. Sarant, and D. Tomlin. 2019. “Peripheral and Central Hearing Impairment and their Relationship with Cognition: A Review.” International Journal of Audiology 58 (9): 541–552. doi:10.1080/14992027.2019.1591644.
- Prasher, D., and M. Cohen. 1993. “Effectiveness of Acoustic Reflex Threshold Criteria in the Diagnosis of Retrocochlear Pathology.” Scandinavian Audiology 22 (1): 11–18. doi:10.3109/01050399309046013.
- Robinette, M. S., and K. S. Snyder. 1982. “Effect of Eye Closure, Mental Concentration, and Nonauditory Sensory Stimulation on the Threshold and Magnitude of the Acoustic Reflex.” Ear and Hearing 3 (4): 220–226. doi:10.1097/00003446-198207000-00007.
- Tasko, S. M., K. K. Deiters, G. A. Flamme, M. V. Smith, W. J. Murphy, H. G. Jones, N. T. Greene, and W. A. Ahroon. 2022. “Effects of Unilateral Eye Closure on Middle Ear Muscle Contractions.” Hearing research 424: 108594. doi:10.1016/j.heares.2022.108594.
- Ugarteburu, M., R. H. Withnell, L. Cardoso, A. Carriero, and C. P. Richter. 2022. “Mammalian Middle Ear Mechanics: A review.” Frontiers in Bioengineering and Biotechnology 10: 10:983510. doi:10.3389/fbioe.2022.983510.
- Valero, M. D., K. E. Hancock, S. F. Maison, and M. C. Liberman. 2018. “Effects of Cochlear Synaptopathy on Middle-ear Muscle Reflexes in Unanesthetized Mice.” Hearing Research 363: 109–118. doi:10.1016/j.heares.2018.03.012.
- Wojtczak, M., J. A. Beim, and A. J. Oxenham. 2017. “Weak Middle-Ear-Muscle Reflex in Humans with Noise-Induced Tinnitus and Normal Hearing May Reflect Cochlear Synaptopathy.” eNeuro 27 4(6). doi:10.1523/ENEURO.0363-17.2017.