

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Introduction
Opioid analgesic treatment during surgery entails the risk of persistent use. Experiences of childhood adversity have been shown to increase opioid reward in preclinical models, a finding recently extended to healthy humans. We tested whether childhood adversity similarly increased opioid reward, operationalized as drug-induced feeling good and drug liking, in outpatients receiving opioids on the operating table.
Methods
This observational study recruited patients entering a Norwegian hospital for an outpatient surgical procedure. An opioid intravenous opioid analgesic (remifentanil [Minto model, effect-site concentration: 5 ng/ml], or oxycodone [5 mg]) was administered in the minutes before general anesthesia. Verbal numerical ratings of feeling good and anxious were collected 1 min before, and 1–3 min after opioid infusion. Ratings of drug liking, disliking, and feeling high were also collected after infusion. Patients (n = 151) completed measures of childhood adversity at a later date.
Results
Regression analyses revealed a modest yet significant negative association between childhood adversity and post-opioid liking (b = −0.06, p = 0.046) but no significant effect on feeling good (b = 0.01, p = 0.690) after the pre-operative opioid dose. Exploratory analyses showed that more childhood adversity was significantly associated with higher reports of anxiety, depression, loneliness, and pain catastrophising, however not with alcohol or other drug use, or with any other subjective drug effects.
Discussion
Ratings of feeling good and drug liking of medically prescribed opioids given before surgery were not higher after childhood adversity, and previous findings were not conceptually replicated. The discrepancy between current and prior results may be due to the context and stress related to the impending surgery, the short duration of drug exposure, and the relatively limited levels of high childhood adversity in the current sample compared to the original study. Exploratory analysis was consistent with the possibility of a nonlinear relationship between positive opioid effects and childhood adversity scores. Future research should assess the link between childhood adversity, subjective effects, and use of the prescribed opioids after surgery.
1. Introduction
Experiences of childhood adversity (such as abuse, neglect, and household dysfunction) are prevalent among people with opioid use disorders (OUD) (Santo Jr et al. Citation2022; Santo Jr et al. Citation2021). Several mechanisms may underlie this link, including the use of opioids to cope with dysregulated emotion processing (Garland et al. Citation2019), heightened pain sensitivity (Austin and Shanahan Citation2018), increased stress vulnerability (Williams et al. Citation2020), and greater impulsivity (Peck et al. Citation2022) after childhood adversity. Another important mechanism contributing to this link may be an increased sensitivity to opioid reward. In the context of childhood adversity, neurodevelopmental changes to reward and motivation networks may contribute to heightened reward responses to drugs such as opioids, leading to a greater risk of abuse and addiction (Oswald et al. Citation2021).
Preclinical research supports neurobiological changes in reward networks in animals exposed to early adversity, paired with altered drug responses (Levis et al. Citation2021; Vazquez et al. Citation2006; Vazquez et al. Citation2005). Rodents exposed to maternal separation or limited bedding and nesting as infants (both models of early adversity in animals) demonstrated: greater self-administration of opioids, conditioned place-preference for opioid-paired areas (Vazquez et al. Citation2005), resistance to extinction of opioid-seeking behaviors, and faster reinstatement of opioid seeking-behaviors when exposed to cues (Levis et al. Citation2021). This effect has been shown to be stronger for opioids over other drugs such as stimulants or alcohol, indicating an opioid-specific preference after experiences of early adversity (Vazquez et al. Citation2006). There are several potential mechanisms to help explain this heightened reward response after early adversity. Panksepp (Panksepp et al. Citation1980) proposed that opioid drugs mimic the pleasure experienced from caring social bonds by binding to the mu-opioid attachment circuitry, and that exposure to adverse social factors (such as isolation) may increase the desirability of opioids. Accordingly, this may be one explanation for an enhanced pleasure response to opioids among those with limited early experiences of caring social bonds in childhood. However, support for this theory has scarcely been translated from preclinical findings to humans.
A recent translational study measured reward responses to morphine in people with and without experiences of childhood adversity (Carlyle et al. Citation2021). Using a placebo-controlled, double-blind opioid administration design, this study examined subjective and behavioral responses to an intramuscular dose of morphine (0.15 mg/kg) in healthy participants with either severe or no history of childhood abuse and neglect. Individuals with severe childhood adversity rated the effects of morphine as more likeable, felt more euphoric, and reported greater wanting for more drug from 15 min after the morphine administration. The childhood adversity group also rated less disliking, nausea and dizziness from 90 min after the dose compared with the non-adversity group. However, behavioral indices of reward from a progressive ratio paradigm where participants could work for hypothetical rewards (money or more morphine) did not significantly differ between the two groups. These results represent important initial evidence that childhood adversity could enhance the risk of opioid misuse via increased drug reward in humans.
Opioid analgesics such as morphine are critical medicines that are administered to millions of people every year. Rates of persistent use after surgical treatment in the USA are 5–10% (Brummett et al. Citation2017; Howard et al. Citation2023). Known risk factors of persistent opioid use after surgery include conditions such as depression, anxiety and chronic pain (Burcher et al. Citation2018), which are also more frequent in people who experienced childhood adversity. In this study we examined whether childhood adversity increases positive effects of opioids given in a medical context. Positive drug effects are considered a sign of higher abuse liability (Comer et al. Citation2012. As replication and generalization are critical components of the scientific method, it is essential to understand whether the previous findings are generalizable to naturalistic contexts where opioids are frequently administered.
We aimed to conceptually replicate the findings from the previous study (Carlyle et al. Citation2021) in generally healthy patients undergoing outpatient surgery. In this observational study, patients were given an intravenous dose of either remifentanil or oxycodone as part of routine care prior to being anesthetized. Both drugs are opioid agonists that are fast-acting and primarily stimulate the µ-opioid receptor subtype and are frequently used both pre- and post-operatively to provide quick and effective pain relief. Patients were asked to give verbal numerical ratings of how good and how anxious they felt immediately before and one minute after opioid infusion, as well as to rate their liking of the effects, disliking of the effects, and feeling high between one and three minutes after. Patients later completed additional state and trait measures. Our primary hypotheses were that patients with greater childhood adversity (higher trauma) would (1) exhibit a larger mood boost (feeling good), and (2) express greater liking of the drug effects after the opioid administration, conceptually replicating the previous findings. The feeling high translation was not deemed as a positive drug effect in the Norwegian population (Eikemo Citation2022), and we did not expect any effect of childhood adversity on disliking or feeling high. Since anxiety is typically higher in people with childhood trauma and opioid use disorder (Evans et al. Citation2020), and anxiety relief has been cited as a motivator for continued opioid use (Rogers et al. Citation2019), we also explored the links between childhood trauma and anxiety pre- and post-drug. Identifying relationships between childhood adversity and opioid drug effects in this pre-operative surgery population has implications for pain management in patients at higher risk of persistent use due to childhood adversity.
2. Methods
2.1. Participants and procedure
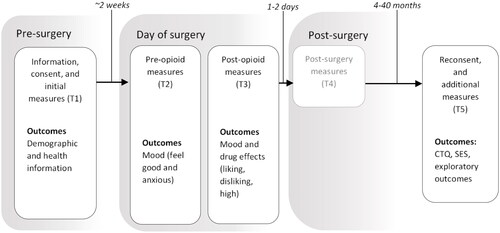
This was an observational study of subjective opioid drug effects in day surgery patients who received a pre-operative opioid analgesic, as part of routine care. The study was part of a broader research project (Eikemo Citation2022; Isabell M. Meier Citation2022) (see for an overall timeline) that recruited 269 generally healthy patients (defined in line with the American Society of Anaesthesiologists’ Physical Status Classification System, ASA I-II; American Society of Anesthesiologists Citation2014) admitted for outpatient surgery at Kongsberg Hospital in Norway between April 2018 to June 2021. Outpatient surgeries were typically minor abdominal, minor gynaecological, minor orthopedic, otorhinolaryngological, or colorectal surgeries. For recruitment, patients were sent a letter approx.two weeks prior to the procedure with information about their upcoming surgery, in addition to the study information sheet, consent form, and some routine clinical questions. All patients provided informed written consent on the morning before the surgery. The study protocol was approved by the internal review board (data protection officer) at Kongsberg Hospital.
Figure 1. Study procedure in the context of the broader research project. T: timepoint for data collection. T4 is in grayscale to indicate that outcomes were collected but are not included within the current study. CTQ: childhood trauma questionnaire, SES: socio-economic status.
Of the initial sample, 220 (82%) were then successfully recontacted by phone and/or email between August 2021 and February 2022 (between 4 and 40 months after the surgery) and agreed to complete the relevant outcomes for this study. A total of 155 (71%) patients completed these additional questionnaires, which was the final sample size for this study. Patients were asked to provide additional consent and subsequently received the questionnaires either electronically by email, or hardcopy by post (depending on the patient’s preference). The email contained a link to the electronic questionnaire form using the University of Oslo’s online data collection software (Nettskjema), and responses were automatically stored on the University of Oslo’s secure data storage server TSD. Hardcopy questionnaires were received and completed by post and registered manually by one of the hospital research personnel. If patients had not completed the questionnaires within one week, they were sent reminders by email. In the rare case of repeated responses, the earliest complete response was used for the analyses. Cases, where the patients responded with the same answer for all questions, were considered invalid and excluded from analyses. The follow-up data collection was approved by the Regional Ethics Committee (Rek Sør-Øst D: 198224).
2.2. Opioid administration and subjective effects
As part of routine care for the surgical procedure, patients were given an intravenous opioid analgesic three to five minutes before being administered the general anesthetic. Patients were informed by the medical personnel that they would be given medication for pain and for sleep while on the operating table. The opioid analgesic was either remifentanil (n = 157, 59%; Minto model, effect site concentration; 5 ng/ml; surgeries conducted Jan 2018-May 2019), or oxycodone (n = 112, 41%; 5 mg; surgeries conducted Nov 2019-June 2021). Both opioids led to comparable subjective intoxication, as reported in the broader research trial (Eikemo Citation2022). Immediately prior to opioid administration, patients were asked by the medical personnel to verbally rate their mood for: (i) how good they felt; and (ii) how anxious they felt, on a scale from 0 (not at all) − 10 (very much) (pre-drug scores). At precisely one minute following the opioid dose, patients were asked to rate their mood again (i-ii), in addition to the subjective opioid effects on a scale from 0-10 for: (iii) how high they felt; (iv) how much they liked any of the effects of the drug; (v) how much they disliked the effects. These ratings took between one and three minutes to complete. The drug effect items are from the Drug Effect Questionnaire (DEQ; Morean et al. Citation2013), a measure frequently used for psychopharmacological research exploring acute drug effects. All patient responses were recorded by pen and paper by the medical personnel.
2.3. Other measures
The primary predictor for childhood adversity was a history of childhood abuse and neglect, which was measured by the Childhood Trauma Questionnaire (CTQ; Bernstein et al. Citation1997). The CTQ is a 28-item measure of experiences of abuse and/or neglect in childhood across five subcategories: emotional and physical abuse, emotional and physical neglect, and sexual abuse. Responses are made on a 5-point Likert-scale (1: never true, 5: very often true), where the total severity score across all subscales is calculated. Another exploratory measure of childhood adversity was the MacArthur Scale of Subjective Social Status in childhood (MSSS; Adler et al. Citation2000), a measure of childhood socioeconomic status (SES) where patients were asked to rate their family’s SES compared to the rest of the Norwegian society when they were young, on a one item scale (0 – low, 10 – high). The families with the highest income, education and most respected jobs were located at the top of the scale, and the families with either no or the lowest ranged education, jobs, and income at the bottom of the scale.
The choice of other exploratory measures was guided by previous research linking adversity with substance use and mental health. This included an assessment of problematic substance use by both the Alcohol Use Disorders Identification Test (AUDIT; Aasland et al. Citation1990) and the Drug Use Disorders Identification Test (DUDIT; Berman et al. Citation2005), which comprise 10–11 items answered by either 5-point (0 – never, 4 – almost daily) or 3-point (0 – no, 4 – yes, this year) Likert scales. Mental health was measured by the 14-item Hospital Anxiety and Depression scale (HADS; Zigmond and Snaith Citation1983) (4-point Likert response scale: 0 – not at all, 3 – all the time), and loneliness was measured with the Three Item Loneliness Scale (T-ILS; Knapstad et al. Citation2021) (3-point Likert scale; 1: hardly ever, 3: often). Mindfulness was measured by the 15-item Five Facet Mindfulness Questionnaire (FFMQ; Dundas et al. Citation2013) (5-point Likert scale, 1: never, 5: very often). Pain catastrophising was measured by the 13-item Pain Catastrophizing Scale (PCS; Fernandes et al. Citation2012), (5-point Likert scale, 0: not at all, 4: all the time). Total scores were computed for all exploratory outcomes. Demographic data such as age (years), sex (male, female), and weight (kg), were collected, in addition to opioid type (oxycodone, remifentanil), and surgery type (categorical and dummy coded).
2.4. Analyses
Data were analyzed using R v4.1.1 (R Core Team Citation2021). The normality of residuals was assessed using the Shapiro–Wilk and Kolmogorov–Smirnov tests. Bootstrapping using random sampling with replacement (5000 iterations) was used if any of the two tests were significant (p < .01 for the Shapiro–Wilk and p<.05 for the Kolmogorov–Smirnov). The threshold for the Shapiro-Wilk test was adjusted due to overestimates of non-normality in samples when n > 50 (Yap and Sim Citation2011). Outliers (defined as responses >3 standard deviations from the mean) for the CTQ scores were assessed using boxplots. Some extreme values were expected as there is typically a reduction in variation in CTQ scores for the moderate-severe range, however these were retained and reported. Extreme values were not expected for drug effect outcomes as these were bounded between 0 and 10 (11-point integers). Patients with a post-drug rating for a given outcome and a CTQ score were included in that analysis. Missing values were treated as missing. The alpha criterion for significance was p<.05 and p-values were corrected for multiple testing using the Holm-Bonferroni correction.
2.4.1. Primary analyses
Multiple linear regressions were conducted to assess whether the primary predictor variable for childhood adversity (CTQ score) was significantly positively associated with feeling good (H1), and drug liking (H2). Analyses were adjusted for demographic variables (age, sex), weight, opioid type, and surgery type. The analyses for feeling good were adjusted for the pre-drug ratings by entering pre-drug responses as predictors in the regression, as this was also measured before as well as after opioid administration. The regression equation for these analyses were:
where Ŷ is the post-drug score. Surgery type was categorical and dummy coded, where a regression coefficient was obtained for each level of the variable. Pre-drug scores in the regression equation were only relevant for feeling good.
The findings were interpreted as a full conceptual replication if both H1 and H2 were confirmed by a significant positive association between CTQ score and post-drug feeling good and drug liking, or a partial conceptual replication if one of the two were significant. Regression coefficients (betas) were interpreted for effect size. For non-significant findings or significant associations in the opposite direction than hypothesized, we concluded that the conceptual replication was unsuccessful. Because the study was only powered to detect small-medium effect sizes, any null effect was not interpreted as support for no effect. Primary analyses were preregistered as a peer-reviewed, published registered report (Carlyle Citation2022; https://osf.io/7ymts). The data has not been made publicly available due to the sensitive nature regarding health and adversity. The conditions of our ethical approval, and the constraints of Norwegian law, prevent sharing of the data supporting this research with any individual outside the author team.
2.5. Exploratory analyses
2.5.1. Subgroup analyses comparing high childhood adversity with none for ‘feeling good’ and ‘feeling anxious’
The previous study limited recruitment to two groups of participants (people with CTQ scores in the ‘none’ category, and people with a ‘severe’ CTQ score on at least one subscale) which were then compared statistically. In contrast, the current preregistered linear regression tested for a cumulative effect of CTQ, with a linear increase or decrease in positive drug effects with higher CTQ scores. We, therefore, explored (i) the number of patients in this dataset that would qualify for inclusion in the previous study (scoring ‘none’ across all subscales or ‘severe’ on one or more subscales), and (2) whether they showed a similar pattern of drug responses as in the original study. We first visually inspected outcomes in the three subgroups: ‘none’, ‘low-moderate’ on ≥1 subscale, and ‘severe’ on ≥1 subscale. We then used mixed ANOVAs to statistically compare change from ‘pre’ and ‘post’ responses between the ‘none’ and ‘severe’ groups for the two repeated-measures items feeling good and anxious.
2.5.2. Childhood adversity and other subjective drug effects
Other opioid-induced drug effects (disliking and feeling high) were analyzed as outcomes using linear regression models that adjusted for the same variables as the primary analyses. The ‘mediation’ package in R was used to conduct a mediated regression analysis for feeling anxious, since childhood adversity was expected to be associated with higher pre-opioid anxiety, and in turn be associated with a greater reduction in post-opioid anxiety. The feel effects response was dichotomous (yes/no) and analys(Carlyle et al. n.d.)ed using a logistic regression with the same predictors.
2.5.3. Associations with mental health, alcohol and other drug use, and related constructs
Other exploratory analyses included Pearson’s correlations to assess associations between the predictors and outcomes with: Socioeconomic status, alcohol and other drug use, mental health, and loneliness. Spearman’s Rho correlations were used for non-parametric data. Any group-based analyses were conducted using analyses of variance (ANOVA). The alpha level for exploratory analyses was not corrected for multiple testing as they were considered hypothesis-generating (Bender and Lange Citation2001).
2.6. Level of bias and control
As a registered prospective analysis (Carlyle et al. Citation2022; https://osf.io/7ymts), we designated a Level 2 bias control because the wider dataset (n = 269) was acquired and partially observed as part of the broader research project (Eikemo Citation2022). However, the main predictor, CTQ scores, and the exploratory variables were not accessed or observed prior to in-principle acceptance, nor did any of the authors know which individuals made up the subset of participants (n = 155, 71%) that provided data for the current analysis. Steps to reduce bias included: (i) the submission of the pre-specified analysis script to provide transparency on the analytical plan and contingencies before this data was observed; (ii) using the Holm-Bonferroni alpha correction on the confirmatory tests; (iii) ensuring the lead authors of the manuscript responsible for analysis had limited exposure to the data that was already accessed as part of the broader research project.
3. Results
3.1. Sample descriptives
Patients were aged 48 years on average (SD = 14.0), 52% were female, and self-reported socioeconomic status was relatively high (M = 7.0, SD = 1.2; maximum of 10) (). The most common surgical procedure was abdominal surgery (n = 66, 44%), followed by minor gynaecological surgery (n = 32, 21%). Remifentanil was the pre-operative opioid analgesic delivered in 55% of the patients, and oxycodone for the remaining 45%. Overall, 80% of the patients reported that they felt the effect of the opioid when asked one minute after injection. For the five CTQ subscales, 11% of patients scored in the severe range for one or more subscale, which was most commonly emotional abuse (6%), while 52% scored in the none range across all five subscales. A subset of patients reported anxiety (15% scored as mild or higher), depression (<2% scored as mild or higher), risky alcohol use (10%) and other risky drug use (6%). Of the originally reported 155 patients, 4 (3%) were identified as duplicate cases, leading to a final sample of 151 patients.
Table 1. Sample Descriptives for Patients (n = 151) Involved in This Study.
3.2. Childhood adversity and post-drug feeling good and liking (hypotheses 1-2)
In the tests of the preregistered hypotheses, regression analyses indicated a modest yet significant effect of childhood adversity on post-opioid liking (b = −0.06, 95%CIs [−0.11 – −0.01], p = 0.046; Holm-Bonferroni corrected, ), indicating a negative association between total CTQ score and liking () when adjusting for opioid type, age, sex, weight, and operation category. As the CTQ total score is the sum of 25 items answered on a 1 to 5-point Likert scale (range 25-125), an average 1 Likert unit increase across all items would equate to a 25-point increase in the CTQ total score. Thus, for each average 1 Likert unit increase on the CTQ, we would expect a decrease in 1.5 numeric rating scale (NRS) units of liking. The regression analyses also showed a significant effect of surgery type, with patients undergoing minor gynaecological surgery reporting significantly less liking than patients undergoing minor abdominal surgeries (b = −2.28, 95%CIs [-3.91 – −0.64], p = .014).
Figure 2. Overlay of scatter plot and regression line (with the shaded 95% confidence interval band) for the effect of childhood adversity on post-opioid a) liking of the effects and b) feeling good. There was a modest yet significant effect of childhood adversity (CTQ total score) on post-opioid liking (b = –0.06, p = 0.046) where an average 1 Likert unit increase across all of the CTQ items (rated on a 1–5 Likert scale) led to a significant –1.5 NRS unit decrease in liking. There were no significant effects of CTQ total score on feeling good (b = 0.01, p = 0.690). While the range of the CTQ total score is 25–125, the maximum score did not exceed 72 in this patient population. The red dotted vertical lines crossing the x-axis are to visually illustrate total scores with an average 1 Likert unit difference for the CTQ items (equivalent to a 25-point difference in the CTQ total score), starting from the lowest total score. The regression lines and respective models adjusted for age, sex, weight, opioid type, and surgery type. As these variables were mean-centred prior to plotting, the regression line reflects predicted liking and feel-good averaged across gender, drug, age, and weight for an individual that is undergoing the most common surgery (minor abdominal surgery).
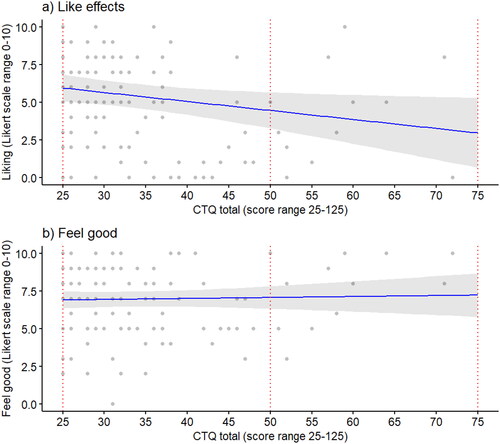
Table 2. Regression model estimates for post-drug liking and feeling good.
For post-opioid feeling good, there was no significant effect of CTQ score (0.25 NRS units of change in feel good, per average increase in 1 Likert unit of the CTQ; b = 0.01, 95%CIs [- 0.03 − 0.04], p = 0.690; Holm-Bonferroni corrected ). The only significant predictor for post-opioid feeling good was pre-opioid feeling good (0.71 NRS units of change in post-opioid feel good, per average increase in 1 NRS unit of pre-opioid feel good; b = 0.71, 95%CIs [0.55 − 0.87], p <.001). Residuals for feeling good regression deviated from normality, however, bootstrapped estimates did not differ significantly from the original model. No other predictors were significantly associated with the two outcomes. Both regression outcomes are presented in .
3.3. Exploratory subgroup analyses comparing high childhood adversity with none for ‘feeling good’ and ‘feeling anxious’
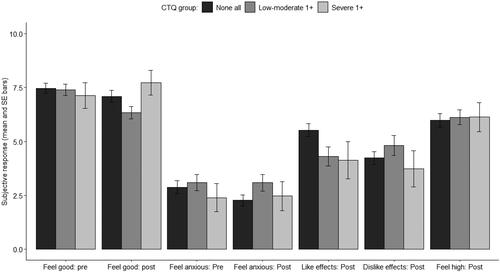
Seventy-two patients scored in the ‘none’ range for all CTQ subscales (50%); 56 patients scored in the ‘low’ and ‘moderate’ ranges on one or more subscales (39%); and 15 patients rated scored in the ‘severe’ range for at least one subscale (11%). After visual inspection of group means for subjective drug effects (), we noted that none of the 15 patients with ‘severe’ CTQ scores reported a reduction in feel-good after opioid injection, whereas the overall group mean was reduced by 0.4 points. While the positive mean change in feeling good scores for the severe group is consistent with the original study results, post-hoc exploratory ANOVA’s comparing the interaction between group (‘none’, ‘severe’) and time (pre, post) did not yield a significant interaction effect for feeling good (F(1,89) = 3.45, p = .067), nor any significant main effects. The ANOVA of anxiety ratings did not show any significant interaction effects (F(1,87) = 1.69, p = .202). These were exploratory analyses that were not included in the registered report. Additional data and figures comparing these groups are available in SM2, including scatterplots where visual inspection did not indicate a clear linear or nonlinear pattern. SM2 also contains demographic variables between this and the previous sample, in addition, to mean differences and confidence intervals for each of the drug effects ().
Figure 3. Subjective opioid effects (feeling good, feeling anxious, and drug-specific effects for liking, disliking, and feeling high post-opioid) stratified by group: (i) patients that scored in the ‘none’ category across all CTQ subscales (n = 76), (ii) patients that scored in the ‘low’ or ‘moderate’ category for one or more (denoted as ‘1+’ in the figure legend) of the CTQ subscales, but never in the severe category (n = 52), and (iii) patients that scored severe on one or more (1+) subscales (n = 15). Error bars represent standard errors.
3.4. Exploratory regressions for other subjective drug effects
For other subjective drug effects not relevant to the conceptual replication, exploratory regression models indicated no significant effects of childhood adversity on feeling high (-0.09 units of change in feeling high, per average increase in 1 Likert unit of the CTQ; b < −0.01, 95%CIs [–0.05 − 0.04], p = .87), disliking (0.1 units of change in disliking, per average increase of 1 Likert unit of the CTQ; b = 0.01, 95%CIs [– 0.04 − 0.06], p = .760), or feel effects (logistic regression; OR = 0.99, 95%CIs [0.93 − 1.07], p = .773) (full model estimates are in SM1). Childhood adversity was not significantly associated with greater pre- (b < 0.00, 95%CIs [–0.05 − 0.05], p = .965) or post-opioid anxiety (b = 0.03, 95%CIs [–0.02 − 0.07], p = .206).
3.5. Exploratory correlations with mental health, alcohol and other drug use, and related constructs
displays the exploratory correlations between the main predictor (childhood adversity) and theoretically-related exploratory variables. CTQ score was negatively associated with childhood socioeconomic status (SES; rs = −0.30, p<.001), and to a lesser degree with adulthood SES (rs = −0.14, p = .12). CTQ was also associated with higher anxiety (rs = 0.29, p <.001), depression (rs = 0.26, p = .002), loneliness (rs = 0.20, p = .021), and pain catastrophising (rs = 0.23, p = .005). Other significant associations were also found between the exploratory variables and post-drug effects (). Correlations between drug effects are reported in SM3.
Table 3. Correlation matrix for exploratory variables (total scores) with post-drug effects.
4. Discussion
We aimed to conceptually replicate the findings of increased subjective pleasure and liking of opioids after childhood adversity (Carlyle et al. Citation2021) in patients administered an intravenous opioid before undergoing surgery. Our analyses did not support the hypothesis that cumulatively more experiences of childhood adversity would heighten ratings of drug liking and feeling good after opioid injection in day surgery patients on the operating table (N = 151). Rather, the findings indicated an inverse relationship: Patients with higher levels of childhood adversity reported significantly less liking of the effects. Exploratory subgroup analysis restricted to patients matching the groups included in the original study (‘none’ or ‘severe’ in at least one CTQ domain) showed a non-significant pattern of change in feeling good that was consistent with the original study, allowing for a non-linear effect of childhood adversity that should be examined with greater sample sizes. Childhood adversity scores were linearly associated with higher anxiety, depression, loneliness, and pain catastrophising, in line with previous literature (Furuya and Wang Citation2023; Pieritz et al. Citation2015; Van Assche et al. Citation2020), including the study we aimed to conceptually replicate (Carlyle et al. Citation2021).
There are many possible explanations for the lack of replication of the previously reported association between childhood adversity and positive opioid effects. Impending surgery is a stressful situation, whereas participants in the previous study volunteered for a drug experiment designed to limit stress. The preexisting stress experienced as part of surgery may limit or alter the subjective effects of opioids, in line with the ‘state-dependent’ perspective of opioids on behavior (Loseth et al. Citation2014). Different psychological responses to the acute stress of surgery in patients with greater childhood adversities could have contributed to lower opioid liking e.g. an increased desire to remain in control. Note that the reported inverse effect on liking is modest, with a 0.6-point reduction in liking of the pre-surgical opioid injection per 10 percentage point increase in childhood adversity. Demographic differences between this patient sample and the prior study sample, such as older age and higher body weight (kg), may have contributed to different drug effects. The present data also deviate substantially from the original study in the timing of drug effects measures. Here, responses were given between 1–3 min after a substantial intravenous dose of remifentanil or oxycodone. In contrast, after intramuscular morphine or saline (placebo) in the previous study, greater positive effects were found after the first measure (at 15 min), whereas significantly reduced nausea and dizziness emerged after 90 min in people with childhood adversity. It is conceivable that the impact of childhood adversity on positive subjective effects may become more pronounced after a longer duration of time following the dose. In healthy people, a biphasic pattern has been described where initial positive responses to opioids are followed by increasing ratings of nausea, dizziness and higher disliking of the drug effects (Gorka et al. Citation2014; Zacny et al. Citation1997).
While this observational study had enough variation in childhood adversity to explore the research question, exploratory subgroup analyses were limited by the small number of patients that scored as severe on one or more subscales for childhood adversity. Mean differences and confidence intervals for post-opioid liking and feeling good were not comparable to the previous study. Curvilinear effects of childhood adversity have been reported for related areas of research, for example when assessing stress-related resilience: Primates exposed to some early adversity demonstrate greater indications of stress resilience compared to primates with either none or high levels of early adversity (Yuan et al. Citation2021). Observational work in humans similarly reports that children who experience some adversity demonstrate lower biological markers of stress reactivity than children with none or high adversity (Shakiba et al. Citation2020), and some adversity has been linked to the better adult quality of life (Höltge et al. Citation2019). A large amount of evidence supporting a ‘dose-like’ cumulative effect of childhood adversity for poor physical and mental health outcomes has also been reported however (Hamby et al. Citation2021; Zarse et al. Citation2019).
Similar to the previous study, the current sample varied on other important characteristics associated with childhood adversity that may be relevant to subjective drug effects, including loneliness, socioeconomic status, and mental health, all of which are known risk factors associated with persistent opioid use (Adewumi et al. Citation2021; Sullivan Citation2018; Vyas et al. Citation2021). The findings support a linear relationship between childhood adversity scores and these health-related measures. Exploratory correlations indicated the potential importance of loneliness and anxiety on subjective opioid effects; future research should aim to better understand and address the impacts of these factors. The lack of significant association between childhood adversity with problematic alcohol and other drug use could be due to low levels of use overall in this patient sample. Scores for hazardous alcohol use using the AUDIT in the current sample were almost two points lower than the Norwegian general population-based sample for that age group (an average of 4.5 for people aged 36–55; Mathiesen et al. Citation2013), however, drug use scores by the DUDIT were in line with the Swedish findings from the general population (3% scoring >2) (Berman et al. Citation2005).
The study had several limitations. The limited number of patients with high levels of childhood adversity was expected given the sample size. The data provides important insights on the impact of lower and moderate levels of childhood adversity, with clinical relevance since patients exposed to opioids are more likely to have experienced lower levels of childhood adversity. The data may also reflect some selection bias where patients with more childhood adversity were less likely to respond. Furthermore, follow-up questionnaires for exploratory outcomes were collected later than the surgery and the state measures may not reflect the time of surgery. Lastly, this study only aimed to conceptually replicate the prior findings using subjective responses as an early indicator of risk for persistent use. Future research should assess the link between childhood adversity, subjective effects, and use of the prescribed opioids after surgery.
To conclude, this study did not conceptually replicate findings for increased subjective pleasure to opioids given before surgery in people with greater histories of childhood adversity. This study found some support for the inverse: people with greater childhood adversity reported less liking of the opioid effects. This effect was predominantly driven by patients with lower to moderate levels of childhood adversity as there were limited numbers of patients with high levels; however, the effects of moderate childhood trauma are still important to understand given the greater prevalence of lower levels of adversity at a population level. Exploratory associations between childhood adversity and more loneliness, anxiety, pain catastrophising, and lower SES may support clinically targeting these as risk factors for persistent use, and help to curb the increase of prescribed opioid-related deaths in Norway (Gjersing and Amundsen Citation2022) and internationally (Martins et al. Citation2015). Opioids are the cornerstone of surgical care, and understanding the specific early risk factors for persistent use is critical for developing more individualized and supportive approaches to prescribing opioid analgesics, while ensuring necessary pain treatment for all patients.
Author contributions
ME, SL, MK, and MC conceptualized this study, while ME, SL, and GE conceptualized the broader research trial. MK, IMM, KB, and ENJ conducted the data curation. MC and MK conducted the formal analyses, supported by ME and MT. SL acquired the funding as part of the broader trial. MC and MKK completed data visualization. MC, MK, ME and SL wrote the original draft. IMM, MT, KB, ENJ, and GE reviewed and edited. MC and MK contributed equally and share the first authorship.
Open Scholarship

This article has earned the Center for Open Science badges for Open Materials and Preregistered. The materials are openly accessible at https://osf.io/2sp9z and https://doi.org/10.17605/OSF.IO/XR2VB.
Disclosure statement
No potential conflict of interest was reported by the author(s)
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Aasland OG, Amundsen A, Bovim G, Fauske S, Morland J. 1990. Identification of patients at risk of alcohol related damage. Tidsskr nor Laegeforen. 110(12):1523–1527.
- Adewumi AD, Maravilla JC, Alati R, Hollingworth SA, Hu X, Loveday B, Connor JP. 2021. Duration of opioid use and association with socioeconomic status, daily dose and formulation: a two-decade population study in Queensland, Australia. Int J Clin Pharm. 43(2):340–350.
- Adler NE, Epel ES, Castellazzo G, Ickovics JR. 2000. Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychol. 19(6):586–592.
- American Society of Anesthesiologists. 2014. ASA Physical Status Classification System. Retrieved July 1, 2022 from https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system.
- Austin AE, Shanahan ME. 2018. Association of childhood abuse and neglect with prescription opioid misuse: examination of mediation by adolescent depressive symptoms and pain. Children and Youth Services Review. 86:84–93.
- Bender R, Lange S. 2001. Adjusting for multiple testing—when and how? J Clin Epidemiol. 54(4):343–349.
- Berman AH, Bergman H, Palmstierna T, Schlyter F. 2005. Evaluation of the drug use disorders identification test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. Eur Addict Res. 11(1):22–31.
- Bernstein DP, Ahluvalia T, Pogge D, Handelsman L. 1997. Validity of the childhood trauma questionnaire in an adolescent psychiatric population. J Am Acad Child Adolesc Psychiatry. 36(3):340–348.
- Brummett CM, Waljee JF, Goesling J, Moser S, Lin P, Englesbe MJ, Bohnert ASB, Kheterpal S, Nallamothu BK. 2017. New persistent opioid use after minor and major surgical procedures in us adults. JAMA Surg. 152(6):e170504-e170504.
- Burcher KM, Suprun A, Smith A. 2018. Risk factors for opioid use disorders in adult postsurgical patients. Cureus, 10(5):e2611. doi:10.7759/cureus.2611.
- Carlyle M, Broomby R, Simpson G, Hannon R, Fawaz L, Mollaahmetoglu OM, Drain J, Mostazir M, Morgan CJ. 2021. A randomised, double‐blind study investigating the relationship between early childhood trauma and the rewarding effects of morphine. Addict Biol. 26(6):e13047.
- Carlyle M, Kvande M, Leknes S, Meier I, Buen K, Jensen EN, Ernst G, Eikemo M. 2022. Does childhood adversity alter opioid drug reward? A conceptual replication in outpatients before surgery, in principle acceptance of Version 4 by Peer Community in Registered Reports. doi:10.17605/OSF.IO/7YMTS.
- Comer SD, Zacny JP, Dworkin RH, Turk DC, Bigelow GE, Foltin RW, Jasinski DR, Sellers EM, Adams EH, Balster R, et al. 2012. Core outcome measures for opioid abuse liability laboratory assessment studies in humans: IMMPACT recommendations. PAIN. 153(12):2315–2324.
- Dundas I, Vøllestad J, Binder PE, Sivertsen B. 2013. The five factor mindfulness questionnaire in Norway. Scand J Psychol. 54(3):250–260.
- Eikemo M, Meier IM, Løseth GE, Trøstheim M, Ørstavik N, Jensen EN, … Leknes S. 2022. Do opioid analgesics improve subjective well-being? A prospective observational study of acute opioid effects before surgery. PsyArXiv Preprints. 1-19. doi:10.31234/osf.io/pq7dh.
- Evans EA, Goff SL, Upchurch DM, Grella CE. 2020. Childhood adversity and mental health comorbidity in men and women with opioid use disorders. Addict Behav. 102:106149.
- Fernandes L, Storheim K, Lochting I, Grotle M. 2012. Cross-cultural adaptation and validation of the Norwegian pain catastrophizing scale in patients with low back pain. BMC Musculoskelet Disord. 13(1):1–9.
- Furuya S, Wang J. 2023. The long shadow: early life adversity and later life loneliness in the United States. J Gerontol B Psychol Sci Soc Sci. 78(2):370–382.
- Garland EL, Reese SE, Bedford CE, Baker AK. 2019. Adverse childhood experiences predict autonomic indices of emotion dysregulation and negative emotional cue-elicited craving among female opioid-treated chronic pain patients. Dev Psychopathol. 31(3):1101–1110.
- Gjersing L, Amundsen E. 2022. Increasing trend in accidental pharmaceutical opioid overdose deaths and diverging overdose death correlates following the opioid prescription policy liberalization in Norway 2010–2018. Int J Drug Policy. 108:103785.
- Gorka SM, Fitzgerald DA, de Wit H, Angstadt M, Phan KL. 2014. Opioid modulation of resting-state anterior cingulate cortex functional connectivity. J Psychopharmacol. 28(12):1115–1124.
- Hamby S, Elm JH, Howell KH, Merrick MT. 2021. Recognizing the cumulative burden of childhood adversities transforms science and practice for trauma and resilience. Am Psychol. 76(2):230–242.
- Holm S. 1979. A simple sequential rejective method procedure. Scand J Stat. 6:65–70.
- Howard R, Brown CS, Lai YL, Gunaseelan V, Brummett CM, Englesbe M, Waljee J, Bicket MC. 2023. Postoperative opioid prescribing and new persistent opioid use: the risk of excessive prescribing. Ann Surg. 277(6):e1225-e1231. doi:10.1097/SLA.0000000000005392.
- Höltge J, Mc Gee SL, Thoma MV. 2019. The curvilinear relationship of early-life adversity and successful aging: the mediating role of mental health. Aging Ment Health. 23(5):608–617.
- Isabell M. Meier ME, Trøstheim M, Buen K, Jensen EN, Karlsen SG, Reme SE, Berna C, Leknes S, Ernst G. 2022. Factors associated with use of opioid rescue medication after surgery. PsyArXiv Preprints. 1–21.
- Knapstad M, Sivertsen B, Knudsen AK, Smith ORF, Aarø LE, Lønning KJ, Skogen JC. 2021. Trends in self-reported psychological distress among college and university students from 2010 to 2018. Psychol Med. 51(3):470–478.
- Levis SC, Bentzley BS, Molet J, Bolton JL, Perrone CR, Baram TZ, Mahler SV. 2021. On the early life origins of vulnerability to opioid addiction. Mol Psychiatry. 26(8):4409–4416.
- Loseth GE, Ellingsen D-M, Leknes S. 2014. State-dependent μ-opioid modulation of social motivation. Front Behav Neurosci. 8:430.
- Martins SS, Sampson L, Cerdá M, Galea S. 2015. Worldwide prevalence and trends in unintentional drug overdose: a systematic review of the literature. Am J Public Health. 105(11):e29–e49.
- Mathiesen EF, Nome S, Richter J, Eisemann M. 2013. Alcohol use patterns in a Norwegian general population-based sample with special reference to socio-demographic variables. J Public Health. 21(3):241–249.
- Morean ME, de Wit H, King AC, Sofuoglu M, Rueger SY, O'Malley SS. 2013. The drug effects questionnaire: psychometric support across three drug types. Psychopharmacology (Berl). 227(1):177–192.
- Oswald LM, Dunn KE, Seminowicz DA, Storr CL. 2021. Early life stress and risks for opioid misuse: review of data supporting neurobiological underpinnings. JPM. 11(4):315.
- Panksepp J, Herman BH, Vilberg T, Bishop P, DeEskinazi FG. 1980. Endogenous opioids and social behavior. Neurosci Biobehav Rev. 4(4):473–487.
- Peck KR, Nighbor TD, Price M. 2022. Examining associations between impulsivity, opioid use disorder, and posttraumatic stress disorder: the additive relation between disorders. Exp Clin Psychopharmacol. 30(5):486–493.
- Pieritz K, Rief W, Euteneuer F. 2015. Childhood adversities and laboratory pain perception. Neuropsychiatr Dis Treat. 11:2109–2116.
- R Core Team. 2021. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL: https://www.R-project.org/. In (Version Version 4.1.1)
- Rogers AH, Kauffman BY, Bakhshaie J, McHugh RK, Ditre JW, Zvolensky MJ. 2019. Anxiety sensitivity and opioid misuse among opioid-using adults with chronic pain. Am J Drug Alcohol Abuse. 45(5):470–478.
- Santo T, Jr, Campbell G, Gisev N, Degenhardt L. 2022. Exposure to childhood trauma increases risk of opioid use disorder among people prescribed opioids for chronic non-cancer pain. Drug Alcohol Depend. 230:109199.
- Santo T, Jr, Campbell G, Gisev N, Tran LT, Colledge S, Di Tanna GL, Degenhardt L. 2021. Prevalence of childhood maltreatment among people with opioid use disorder: a systematic review and meta-analysis. Drug Alcohol Depend. 219:108459.
- Shakiba N, Ellis BJ, Bush NR, Boyce WT. 2020. Biological sensitivity to context: a test of the hypothesized U-shaped relation between early adversity and stress responsivity. Dev Psychopathol. 32(2):641–660.
- Sullivan MD. 2018. Depression effects on long-term prescription opioid use, abuse, and addiction. Clin J Pain. 34(9):878–884.
- Van Assche L, Van de Ven L, Vandenbulcke M, Luyten P. 2020. Ghosts from the past? The association between childhood interpersonal trauma, attachment and anxiety and depression in late life. Aging Ment Health. 24(6):898–905.
- Vazquez V, Giros B, Daugé V. 2006. Maternal deprivation specifically enhances vulnerability to opiate dependence. Behav Pharmacol. 17(8):715–724.
- Vazquez V, Penit-Soria J, Durand C, Besson MJ, Giros B, Daugé V. 2005. Maternal deprivation increases vulnerability to morphine dependence and disturbs the enkephalinergic system in adulthood. J Neurosci. 25(18):4453–4462.
- Vyas MV, Watt JA, Yu AY, Straus SE, Kapral MK. 2021. The association between loneliness and medication use in older adults. Age Ageing. 50(2):587–591.
- Williams JR, Cole V, Girdler S, Cromeens MG. 2020. Exploring stress, cognitive, and affective mechanisms of the relationship between interpersonal trauma and opioid misuse. PLoS One. 15(5):e0233185.
- Yap BW, Sim CH. 2011. Comparisons of various types of normality tests. J Stat Comput Simul. 81(12):2141–2155.
- Yuan R, Nechvatal JM, Buckmaster CL, Ayash S, Parker KJ, Schatzberg AF, Lyons DM, Menon V. 2021. Long-term effects of intermittent early life stress on primate prefrontal–subcortical functional connectivity. Neuropsychopharmacology. 46(7):1348–1356.
- Zacny JP, Conley K, Galinkin J. 1997. Comparing the subjective, psychomotor and physiological effects of intravenous buprenorphine and morphine in healthy volunteers. J Pharmacol Exp Ther. 282(3):1187–1197.
- Zarse EM, Neff MR, Yoder R, Hulvershorn L, Chambers JE, Chambers RA. 2019. The adverse childhood experiences questionnaire: two decades of research on childhood trauma as a primary cause of adult mental illness, addiction, and medical diseases. Cogent Medicine. 6(1):1581447.
- Zigmond AS, Snaith RP. 1983. The hospital anxiety and depression scale. Acta Psychiatr Scand. 67(6):361–370.