

ABSTRACT
Introduction
The basophil activation test (BAT) has shown evidence of high sensitivity and high specificity to support the diagnosis of IgE-mediated allergy. It is a functional test that uses live cells analyzed by flow cytometry and thus needs to be performed within 24h of blood collection. BAT has shown to be reproducible and reliable when tested in a clinical diagnostic laboratory with standardized protocols and flow cytometry settings.
Areas covered
In this review, we summarize the evidence to support clinical use of BAT and the next steps required for clinical implementation for an improve clinical care for patients with suspected IgE-mediated food allergy.
Expert opinion
BAT has recently been included in Clinical Guidelines of Food Allergy Diagnosis and its implementation in clinical practice depends largely on availability. Proposed clinical applications of the BAT include: distinction between food allergy and asymptomatic IgE sensitization; determination of food allergic status to peanut, tree nuts and seeds in polysensitized children; evaluation of tolerance to baked egg and baked milk in egg and milk allergic children; identification of patients at high-risk of severe allergic reactions; monitoring for spontaneous resolution of food allergy; confirmation of eligibility for specific treatments of food allergy; prediction and monitoring of response to immunomodulatory treatments.
1. Introduction
The basophil activation test (BAT) is a flow cytometry assay that measures the expression of activation markers (e.g. CD63 and CD203c) on the surface of basophils following stimulation with specific allergens. Its use has gained importance over the last decades as a valid procedure to support the diagnosis of IgE-mediated food allergy. In the recent update of the European Academy of Allergy and Clinical Immunology (EAACI) guidelines on the diagnosis of IgE-mediated food allergy published this year, BAT is, for the first time, listed as one of the recommended tests, and is suggested for patients with a suspected food allergy and equivocal skin prick test (SPT) and specific IgE (sIgE) measurement prior to oral food challenge (OFC) [Citation1.] The BAT is less invasive, safer, and less expensive when compared with OFC. Particularly for BAT to peanut and sesame, there is high certainty of evidence for its use in clinical practice based on a thorough systematic review of the literature and meta-analysis on accuracy of diagnostic tests in food allergy. BAT peanut and sesame demonstrated a moderate sensitivity (86% and 89, respectively) and a high specificity (90% and 93%, respectively), both with low heterogeneity between studies [Citation2]. Furthermore, due to its limited availability, relatively higher cost than SPT and sIgE and the need for flow cytometry and specifically trained laboratory staff, BAT is recommended as a second step in the diagnostic process despite its high diagnostic performance.
In this review, we will discuss the principles of the BAT, the rationale for its use in the diagnosis of IgE-mediated food allergy, its clinical indications, and future steps toward its implementation in clinical practice.
2. General principles of the basophil activation test
IgE-mediated food-induced allergic reactions and anaphylaxis are the result of mast cell and basophil activation and degranulation with the release of vaso-active and inflammatory molecules. Basophils are more readily available cells in the peripheral blood than mast cells and are, therefore, more accessible for testing. The BAT is based on the assessment of blood basophils after stimulation with specific allergens or controls. Activated basophils upregulate various activation markers on their cell surface that can be measured using flow cytometry. The lysosomal-associated membrane protein CD63, located on the membrane of secretory lysosomes inside the basophil and becomes expressed on the plasma membrane as the basophil degranulates, is the most frequently used marker to assess basophil activation [Citation3].
The percentage of CD63 positive basophils increases with increasing concentration of the allergens reaching a plateau at higher concentrations. Many factors can have an impact on the dose-response curve of basophil activation, for instance: the density of epitope-sIgE on the cell surface, the affinity of IgE for the allergen and the intrinsic characteristics of the basophils themselves [Citation4,Citation5]. For this reason, a dose response curve with a broad concentration of allergens is performed to identify the optimal concentration for diagnosis, which is selected for future testing [Citation6]. For each food, the optimal cut off of basophil activation expressed by percentage of CD63-positive basophils and CD203c upregulation (often measured by stimulation index) needs to be established to reach the highest area under the curve (AUC) with a high specificity and acceptable sensitivity [Citation6].
BAT has been strongly correlated with symptoms in patients sensitized to respiratory, venom, and food allergens [Citation7,Citation8]. Its high specificity and retained sensitivity, when compared with other sensitization tests, have led to its increased use not only in research but also in clinical practice, particularly in the diagnosis of food allergy. In food allergy, BAT has high specificity, which contrasts with the lower specificity of SPT and sIgE. For example, BAT has demonstrated up to 100% specificity for peanut allergy [Citation9,Citation10] and for egg allergy [Citation11]. In some studies, BAT has been shown to be useful in differentiating allergic from tolerant to milk and egg among children with AD [Citation12,Citation13,]. Data on the utility of BAT in the diagnosis of allergy to other foods have also shown promising results [Citation7].
Limitations of BAT are the need for live cells and the necessity to perform the analysis within 24 hours by qualified personnel. Furthermore, around 10% of patients have transient nonresponsive basophils upon stimulation through IgE receptor FcεRI despite normal cell surface IgE, and, as a consequence, show non-interpretable results for BAT [Citation6]. In these patients, a mast cell activation test (MAT) might be an interesting additional cellular assay to be used in the future.
3. Proposed clinical applications of the basophil activation test
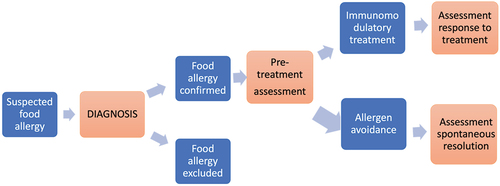
In this section, we discuss possible applications of BAT in clinical practice (). BAT can be useful to support diagnosis and prognosis of food allergy, to monitor for possible spontaneous food allergy resolution and also to confirm eligibility for immunomodulatory treatments and to predict and monitor clinical response to such treatments ().
Table 1. Proposed applications of the basophil activation test in clinical practice.
Figure 1. Proposed integration of the basophil activation test in the clinical pathway of patients with suspected food allergy – the stages of this process that include the basophil activation test are marked in orange.
3.1. Differentiation between food allergy from asymptomatic sensitization
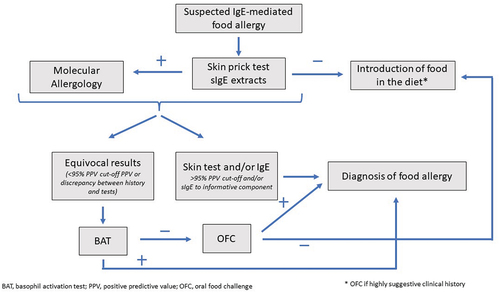
SPT and sIgE, the first-line diagnostic tests following the clinical history, show high sensitivity but low specificity for food allergy diagnosis. Cutoffs with higher specificity have been identified. sIgE measurement to individual allergens has clearly added value in the diagnosis of some food allergies, like peanut, hazelnut, cashew, sesame and peach allergies, but it is not always definite. In fact, most patients still fall in a gray diagnostic area and require a diagnostic OFC. In these situations, BAT, with its high specificity, confers an important advantage compared with SPT and sIgE and can limit the need of OFC. Given BAT’s high specificity, reaching 100% for some food allergies, a positive BAT allows to confirm the diagnosis of food allergy in patients with equivocal SPT and sIgE without the need for a diagnostic OFC. A proposed procedure for diagnosis of food allergy in patients with an immediate reaction after food intake is illustrated in .
Figure 2. Proposed diagnostic procedure in patients with suspected food allergy.
Numerous studies have evaluated the performance of BAT in the diagnosis of food allergy showing high sensitivity and specificity (). Recently, a comprehensive systematic review of the literature with meta-analyses confirmed the high sensitivity and specificity of BAT to support the diagnosis of peanut and sesame seed allergies [Citation2]. BAT can be performed using whole allergen extract or single allergens. The use of single allergens can improve accuracy of diagnosis for some food allergies but carries the risk of missing the potential contribution of other allergens contained in the food. The BAT to peanut as well as to the individual allergens Ara h 2 and the highly similar component Ara h 6 has been shown to discriminate between peanut sensitized but tolerant and peanut allergic patients with similar sIgE levels, reducing the need for OFC [Citation9,Citation14,Citation20]. Similar results were also found for hazelnut allergy where BAT to hazelnut showed higher specificity (97%) than sIgE to individual allergens Cor a 9 (72%) and Cor a 14 (94%) [Citation16].
Table 2. Diagnostic performance of the basophil activation test in different food allergies.
There are clinical scenarios that can be particularly difficult to diagnose with precision and require multiple OFC, such as polysensitization to nuts and seeds and children diagnosed with milk and egg allergies who may tolerate the baked forms of the food.
3.2. Determination of allergic status to tree nuts and seeds in polysensitized children
Cross-sensitization in nut allergic patients can be as high as 50% [Citation21–24]. However, the rate of clinical cross-reactivity, based on OFC, was initially found to be less than 30% [Citation25,Citation26]. These results were, however, based on retrospective studies including small number of patients. In a recent European multicenter prospective study evaluating challenge-proven co-existing peanut, tree-nut and sesame allergies, 60.7% of children had more than one nut or seed allergy, highlighting the importance of testing to all nuts and seeds which are not regularly consumed and tolerated in children with an IgE-mediated allergy to peanut, tree nut or sesame [Citation27]. Clinicians are often confronted with children presenting an IgE-mediated nut allergy with positive SPT and IgE to other nuts that have never been introduced in the diet, at least on a regular basis. Such positive tests can result in unnecessary avoidance of these nuts or, in order to infirm of confirm an allergy, the need of a diagnostic OFC. Although most of these patients tend to get sensitized to more than 4 nuts, most of them will clinically react to 1–2 nuts [Citation28]. Cross-reactivity is particularly high between cashew and pistachio and between walnut and pecan [Citation27,Citation28]. The BAT, used as a second step in the diagnostic process, in patients with equivocal SPT and sIgE to allergen extract and its components, has been shown to reduce the need for OFC by 5% to 15% and the number of positive OFC by 33% to 75% with 0% of false-negative and a diagnostic accuracy of 96% to 100% [Citation15]. Higher basophil activation to walnut has been associated with a higher likelihood of walnut/pecan co-allergy and when performed together with SPT, a sensitivity of 100% for both walnut and pecan allergies and specificities of 90.9% and 93% for walnut and pecan allergies could be reached, respectively [Citation29]. In a recent study with 82 cases of suspected sesame allergy, BAT as a second diagnostic test together with SPT led to correct classification of 91% of patients with only one false negative and four false positive results [Citation30]. Based on these studies, BAT can be considered as a valid second line diagnostic test in polysensitized nuts and seed allergic children prior to considering a diagnostic OFC.
3.3. Evaluation of tolerance to baked egg and baked milk in egg and milk allergic children
Cow’s milk and egg allergies are the most common food allergies worldwide [Citation31,Citation32]. About 60–80% of CM and egg allergic can tolerate the food in their baked form leading to a less restrictive diet and improved quality of life [Citation33]. Furthermore, the baked food may be used for OIT and regular consumption might also accelerate natural resolution [Citation33,Citation34]. To evaluate tolerance of baked goods, OFC is performed in most cases as SPT and sIgE are not reliable predictors of clinical reactivity. In these cases, BAT can be useful prior to evaluating the need of an OFC [Citation35]. In a recent study, BAT was the best diagnostic marker for baked egg allergy, particularly in children aged 2 years or younger and, when performed together with specific IgE, led to a 30% reduction of OFC [Citation36]. A higher basophil activation to milk was also found in children who reacted to baked milk when compared to baked milk-tolerant children and could predict severity of reaction [Citation37].
3.4. Identification of patients at high-risk of severe allergic reactions
Basophil reactivity (i.e. %CD63+ basophils) correlates with the severity of the reaction and its sensitivity (e.g. CD-sens or EC50) with the threshold dose of clinical reactivity [Citation10,Citation38,Citation39]. This initial finding that the BAT can support the identification of patients at risk of severe reactions to peanut was confirmed in a large cohort of well-characterized children participating in the LEAP and related studies and also in a US cohort of peanut allergic patients. In a study analyzing 187 walnut allergic children, an increased basophil activation was associated with severity of reaction and epinephrine use [Citation29]. More recently, in an egg allergy study, BAT was by far the best biomarker for both severe reactions and low threshold of reactivity during double-blind placebo-controlled challenges to baked egg [Citation40]. No demographic or clinical features were statistically significantly different between severity and threshold groups. Nevertheless, BAT distinguished severe from non-severe reactors and identified reactors with low threshold from those with high threshold, suggesting that BAT could help stratify risk of food allergic patients in the future.
3.5. Monitoring for spontaneous resolution of food allergy
An interesting and promising application of BAT is the longitudinal assessment of patients with food allergies that tend to be outgrown over time, such as cow’s milk, egg or wheat allergies, to evaluate possible achievement of tolerance and allow reintroduction of food in the diet. For example, BAT, when performed together with skin testing and sIgE, can diminish the need of OFC to assess possible spontaenous resolution to cow’s milk in milk allergic children [Citation18,Citation41]. In a more recent study, BAT was useful to identify children who had outgrown their egg allergy [Citation36]; however, longitudinal studies assessing the same patients over time are needed to confirm this. Taken together, these data suggest that BAT can be a useful additional tool together with SPT and specific IgE to assess resolution of cow’s milk and egg allergies.
3.6. Confirmation of food allergy for specific treatments
Immunomodulatory treatments for food allergy are being actively researched and some are becoming mainstream practice, such as allergen-specific immunotherapy. Whilst OFC are needed to confirm eligibility in clinical trials, such approach is not practical in the routine setting and may not warrant acceptability by patients and families, particularly if OFC has already been recently performed for diagnosis. It would be useful if a blood test could be used to confirm eligibility. Given its high accuracy in the diagnosis of food allergy, BAT is the most promising test to confirm food allergy without OFC [Citation10].
3.7. Prediction of response to immunomodulatory treatments
Biomarkers able to identify patients who respond to treatment, either before starting and/or during treatment, would be extremely useful in supporting food allergy management. A couple of studies have shown that BAT to Ara h 2 and BAT to peanut could identify as early as 3 months into treatment with peanut OIT patients who were going to reach sustained unresponsiveness as opposed to transient desensitization [Citation42,Citation43]. Over the course of OIT, BAT reduced the response to allergen in active compared to placebo arm in a number of studies of different food allergies [Citation44–46].
The use of biologics targeting the Th2 inflammation has been increasingly evaluated as a possible treatment for food allergy as monotherapy or as an adjunct treatment IT to diminish side effects and increase feasibility of IT in highly reactive patients. In these patients, high basophil activation has been shown to be an interesting biomarker to evaluate patients that might benefit from omalizumab, during OIT or from an adjusted treatment schedule to decrease side effects [Citation47]. Interestingly, other studies have shown that omalizumab induces two types of changes in basophils which have opposite effects on their response to allergen: omalizumab on one hand decreases the density of FcεRI and on the other hand enhances intrinsic basophil sensitivity [Citation48,Citation49]. These changes can both be monitored during the BAT and correlated with clinical outcomes.
3.8. Monitoring of clinical response to immunomodulatory treatments
The BAT has been used in clinical trials as a biomarker to evaluate clinical response in OIT showing immunomodulation of basophil activation throughout treatment, for instance in peanut and egg-allergic patients [Citation42,Citation43,Citation50,Citation51]. A low basophil sensitivity at the start of treatment has been associated with a higher success rate of OIT. An early decrease in basophil response to Ara h 2 has been observed in patients reaching sustained unresponsiveness and a reactivation of basophil response post-OIT in individuals with transient desensitization [Citation42,Citation43]. In a recently published study of 50 cashew allergy children, a significant decrease in basophil activation was shown after 6-months of cashew OIT [Citation52]. Similar results have been published for sesame and walnut [Citation53,Citation54]. In these studies, successful OIT to cashew and walnut led to co-desensitization to pistachio and pecan, respectively. In these patients, BAT might be used to assess cross-desensitization but further studies are needed to confirm this before its use in clinical practice. Based on these data, BAT could be used in clinical practice as a biomarker to select patients who might benefit from OIT, and to guide physicians during treatment in the assessment of possible sustained unresponsiveness and decision to stop treatment.
4. Next steps to bring the basophil activation test to clinical practice
BAT is a functional assay that uses live cells and needs to be performed within 24 hours of blood collection with a standardized and reproducible methodology. BAT requires a simple flow cytometer and qualified laboratory technicians – such flow cytometers are available in clinical diagnostic laboratories that perform routine immunophenotyping, for example for blood cancers or HIV testing. About 10% of individuals have basophils which do not respond to FceRI-mediated signaling and only to stimulants not dependent on the IgE-mediated pathway and for these patients the results of BAT are uninterpretable [Citation11]. Several factors, in particular differences in the analytic and laboratory techniques, can influence the performance of BAT and this can have implications in terms of the diagnostic accuracy of the test [Citation55]. Thus, standardization of laboratory procedures, flow cytometry and data analyses are essential to ensure a reliable and robust clinical use of the test. In a parallel study using samples from children being assessed for possible peanut allergy, BAT to peanut demonstrated a very strong correlation between results tested across two independent laboratories with a very high consistency and narrow intra-CV. This proof-of-concept study confirmed that it is possible to perform a functional assay to a very high-standard with reliable and consistent results and provided confidence in its translation to a clinical diagnostic setting. Automated flow data analysis strategy for flow cytometry could further improve reproducibility and reliability of BAT [Citation56]. An important aspect of implementation OF BAT as a clinical test is to set up external and interlaboratory quality controls, to assure high quality of results and, ultimately, to allow for reimbursement of test costs. Interlaboratory assurance and quality controls are now routinely performed in the U.S.A. and in Europe. Standardization of analysis methods has already improved coherence in the results (CV < 10%) in ten European countries [Citation57].
5. Alternative cellular tests for food allergy
The mast cell activation test (MAT) is an alternative cellular assay that could be used as a complement to BAT, namely, to circumvent the need of fresh blood and results for the 10% of non-responders for whom BAT is uninterpretable. MAT is currently under investigation and has shown interesting results. In the MAT, mast cells grown in the laboratory, either from a mast cell line or from primary mast cells differentiated from haematopoietcic stem cells, are sensitized with patients’ sera and then stimulated with specific allergens or controls and analyzed by flow cytometry for surface expression of activation markers, like CD63. The first study of MAT in the diagnosis of food allergy showed high (98%) specificity in the diagnosis of peanut allergy and that MAT can identify patients who develop severe clinical reactions to peanut during OFC [Citation58]. Recently, MAT has been created using mouse mast cells transfected with a human FceRI allowing for quicker cell culture and high-throughput results but limited expression of FceRI to test samples from either highly atopic highly sensitized patients or patients with low levels of allergen-specific IgE[Citation59].
6. Conclusion
An accurate diagnosis and active management of food allergy are of utmost importance to improve clinical care and quality of life of food allergic patients and their families. The BAT has demonstrated high specificity and ability to reduce the need of diagnostic OFC and reach higher accuracy of diagnosis compared with current tests. BAT shows very good diagnostic accuracy for peanut and sesame with low heterogenicity among studies and promising results for other food allergies. BAT to foods other than peanut or sesame were, however, not included in the recommendations of the recent EAACI food allergy guidelines due to insufficient number of studies in the systematic review to be able to complete meta-analyses. In addition to supporting food allergy diagnosis, BAT can be useful to confirm eligibility for and monitor response during immunomodulatory treatments. The availability of BAT in routine clinical practice requires standardization of the assay, external quality assurance of results and provision of the test to practicing clinicians and is likely to have clinical impact.
7. Expert opinion
An accurate diagnosis of IgE-mediated food allergy remains challenging in daily practice. In patients with a highly suggestive clinical history of immediate reactions after ingesting a specific food, evidence of allergen-specific SPT and IgEs can be sufficient to confirm the diagnosis. Conversely, in patients with no history of an allergic reaction, undetectable SPT and specific IgE rule out food allergy. However, in many other commonly encountered situations (for example, of patients with a unclear history of reaction or a primary avoidance of the food due to multiple (cross-) sensitizations), the lack of specificity of SPT and specific IgE leads to the need for multiple OFC to confirm or exclude a food allergy.
The BAT has shown to have a particularly high specificity for most foods and can reduce the need for diagnostic OFC in patients with an equivocal diagnosis, following history an SPT/specific IgE. BAT is now proposed as a recommended test to support the diagnosis of IgE-mediated food allergy in the recently updated EAACI Guidelines for the Diagnosis of IgE-mediated food allergy1. BAT is considered to be particularly useful in cases that remain equivocal after first-line tests prior to OFC. The meta-analyses supporting the new guidelines was done for BAT to peanut and BAT to sesame, with very good diagnostic performance and low heterogeneity between studies2.
The promising results for BAT’s use in other situations encountered in clinical practice, particularly its use for monitoring natural resolution of food allergy and clinical response to IT, still need to be confirmed by further studies but represent a potentially important application of BAT in clinical practice. Additional effort is now needed to increase BAT’s availability in laboratories around the globe and ensure excellent standardization and quality assurance to allow reliable and consistent results for its use in clinical practice. By raising awareness among experts in the field of laboratory medicine, we believe that implementing BAT in clinical practice will strongly improve diagnosis and management of food allergic patients.
Article highlights
The basophil activation test (BAT) is a functional test that uses live cells and assesses whether basophils degranulate following stimulation with allergen and controls.
The BAT takes into account various elements of an allergic reaction (allergen, cells, quantity and quality of IgE and other antibodies) and is more precise than measuring IgE levels to support the diagnosis of IgE-mediated food allergy.
BAT can be useful to confirm the diagnosis and identify allergic patients at high-risk of developing severe reactions and/or reacting to low doses of the allergen.
BAT can also help confirm indication of allergen-specific treatment and assessing clinical response to such treatment.
Changes in BAT over time may be helpful in assessing for possible spontaneous resolution of food allergy.
Availability of BAT and 10% individuals with non-responder basophils are limiting its use in clinical practice; however, these barriers need to be overcome, especially after the recent inclusion of BAT as a recommended test for food allergy in clinical guidelines.
Declaration of interest
A Santos reports grants from Medical Research Council (MR/M008517/1; MC/PC/18052; MR/T032081/1), Food Allergy Research and Education (FARE), the Immune Tolerance Network/National Institute of Allergy and Infectious Diseases (NIAID, NIH), Asthma UK (AUK-BC-2015-01), BBSRC, Rosetrees Trust and the NIHR through the Biomedical Research Centre (BRC) award to Guy’s and St Thomas’ NHS Foundation Trust, during the conduct of the study; personal fees from Thermo Scientific, Nutricia, Infomed, Novartis, Allergy Therapeutics, Buhlmann, as well as research support from Buhlmann and Thermo Fisher Scientific through a collaboration agreement with King’s College London. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Additional information
Funding
References
- Santos AF, Riggioni C, Agache I, et al. EAACI guidelines on the diagnosis of IgE-mediated food allergy. Allergy. 2023;78(12):3057–3076. doi: 10.1111/all.15902
- Riggioni C, Ricci C, Moya B, et al. Systematic review and meta-analyses on the accuracy of diagnostic tests for IgE-mediated food allergy. Allergy. 2023;79(2):324–352. doi: 10.1111/all.15939
- Knol EF, Mul FP, Jansen H, et al. Monitoring human basophil activation via CD63 monoclonal antibody 435. J Allergy Clin Immunol. 1991;88:328–338. doi: 10.1016/0091-6749(91)90094-5
- Prussin C, Metcalfe DD. 5. IgE, mast cells, basophils, and eosinophils. J Allergy Clin Immunol. 2006;117:S450–456. doi: 10.1016/j.jaci.2005.11.016
- Kabashima K, Nakashima C, Nonomura Y, et al. Biomarkers for evaluation of mast cell and basophil activation. Immunol Rev. 2018;282(1):114–120. doi: 10.1111/imr.12639
- Santos AF, Alpan O, Hoffmann H-J. Basophil activation test: mechanisms and considerations for use in clinical trials and clinical practice. Allergy. 2021;76(8):2420–2432.
- Santos AF, Shreffler WG. Road map for the clinical application of the basophil activation test in food allergy. Clin Exp Allergy. 2017;47(9):1115–1124. doi: 10.1111/cea.12964
- Hemmings O, Kwok M, McKendry R, et al. Basophil activation test: old and new applications in allergy. Curr Allergy Asthma Rep. 2018;18(12):77. doi: 10.1007/s11882-018-0831-5
- Santos AF, Douiri A, Bécares N, et al. Basophil activation test discriminates between allergy and tolerance in peanut-sensitized children. J Allergy Clin Immunol. 2014;134(3):645–652. doi: 10.1016/j.jaci.2014.04.039
- Santos AF, Du Toit G, O’Rourke C, et al. Biomarkers of severity and threshold of allergic reactions during oral peanut challenges. J Allergy Clin Immunol. 2020;146:344–355.
- Ocmant A, Mulier S, Hanssens L, et al. Basophil activation tests for the diagnosis of food allergy in children. Clin Exp Allergy. 2009;39(8):1234–1245. doi: 10.1111/j.1365-2222.2009.03292.x
- Kim YH, Kim YS, Park Y, et al. Investigation of basophil activation test for diagnosing milk and egg allergy in younger children. J Clin Med. 2020;9(12):3942. doi: 10.3390/jcm9123942
- Licari A, D’Auria E, De Amici M, et al. The role of basophil activation test and component-resolved diagnostics in the workup of egg allergy in children at low risk for severe allergic reactions: a real-life study. Pediatr Allergy Immunol. 2023;34(8):e14012. doi: 10.1111/pai.14012
- Glaumann S, Nopp A, Johansson SGO, et al. Basophil allergen threshold sensitivity, CD-sens, IgE-sensitization and DBPCFC in peanut-sensitized children. Allergy. 2012;67(2):242–247. doi: 10.1111/j.1398-9995.2011.02754.x
- Santos AF, Bergmann M, Brough HA, et al. Basophil activation test reduces oral food challenges to nuts and sesame. J Allergy Clin Immunol Pract. 2021;9(5):2016–2027.e6. doi: 10.1016/j.jaip.2020.12.039
- Brandström J, Nopp A, Johansson SGO, et al. Basophil allergen threshold sensitivity and component-resolved diagnostics improve hazelnut allergy diagnosis. Clin Exp Allergy. 2015;45(9):1412–1418. doi: 10.1111/cea.12515
- Sato S, Tachimoto H, Shukuya A, et al. Basophil activation marker CD203c is useful in the diagnosis of hen’s egg and cow’s milk allergies in children. Int Arch Allergy Immunol. 2010;Suppl 152(Suppl. 1):54–61. doi: 10.1159/000312126
- Rubio A, Vivinus-Nébot M, Bourrier T, et al. Benefit of the basophil activation test in deciding when to reintroduce cow’s milk in allergic children. Allergy. 2011;66(1):92–100. doi: 10.1111/j.1398-9995.2010.02432.x
- Tokuda R, Nagao M, Hiraguchi Y, et al. Antigen-induced expression of CD203c on basophils predicts IgE-mediated wheat allergy. Allergol Int. 2009;58(2):193–199. doi: 10.2332/allergolint.08-OA-0023
- van Erp FC, Knol EF, Pontoppidan B, et al. The IgE and basophil responses to ara h 2 and ara h 6 are good predictors of peanut allergy in children. J Allergy Clin Immunol. 2017;139:358–360.e8. doi: 10.1016/j.jaci.2016.06.041
- Sicherer SH, Furlong TJ, Muñoz-Furlong A, et al. A voluntary registry for peanut and tree nut allergy: characteristics of the first 5149 registrants. J Allergy Clin Immunol. 2001;108(1):128–132. doi: 10.1067/mai.2001.115755
- Maloney JM, Rudengren M, Ahlstedt S, et al. The use of serum-specific IgE measurements for the diagnosis of peanut, tree nut, and seed allergy. J Allergy Clin Immunol. 2008;122(1):145–151. doi: 10.1016/j.jaci.2008.04.014
- Hourihane JO, Dean TP, Warner JO. Peanut allergy in relation to heredity, maternal diet, and other atopic diseases: results of a questionnaire survey, skin prick testing, and food challenges. BMJ. 1996;313(7056):518–521. doi: 10.1136/bmj.313.7056.518
- Ewan PW. Clinical study of peanut and nut allergy in 62 consecutive patients: new features and associations. BMJ. 1996;312(7038):1074–1078. doi: 10.1136/bmj.312.7038.1074
- Couch C, Franxman T, Greenhawt M. Characteristics of tree nut challenges in tree nut allergic and tree nut sensitized individuals. Ann Allergy Asthma Immunol. 2017;118(5):591–596.e3. doi: 10.1016/j.anai.2017.02.010
- Ball H, Luyt D, Bravin K, et al. Single nut or total nut avoidance in nut allergic children: outcome of nut challenges to guide exclusion diets. Pediatr Allergy Immunol. 2011;22(8):808–812. doi: 10.1111/j.1399-3038.2011.01191.x
- Brough HA, Caubet J-C, Mazon A, et al. Defining challenge-proven coexistent nut and sesame seed allergy: a prospective multicenter European study. J Allergy Clin Immunol. 2020;145(4):1231–1239. doi: 10.1016/j.jaci.2019.09.036
- Elizur A, Appel MY, Nachshon L, et al. NUT Co reactivity - ACquiring knowledge for elimination recommendations (NUT CRACKER) study. Allergy. 2018;73(3):593–601. doi: 10.1111/all.13353
- Goldberg MR, Appel MY, Nega R, et al. A prospective validation of the NUT CRACKER diagnostic algorithm for walnut and pecan allergy with prediction of severity. J Allergy Clin Immunol Pract. 2021;9(1):265–274.e6. doi: 10.1016/j.jaip.2020.09.041
- Appel MY, Nachshon L, Elizur A, et al. Evaluation of the basophil activation test and skin prick testing for the diagnosis of sesame food allergy. Clin Exp Allergy. 2018;48(8):1025–1034. doi: 10.1111/cea.13174
- Hill DA, Grundmeier RW, Ram G, et al. The epidemiologic characteristics of healthcare provider-diagnosed eczema, asthma, allergic rhinitis, and food allergy in children: a retrospective cohort study. BMC Pediatr. 2016;16(1):133. doi: 10.1186/s12887-016-0673-z
- Sicherer SH, Sampson HA. Food allergy: epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133:291–307. quiz 308. doi: 10.1016/j.jaci.2013.11.020
- Leonard SA. Baked egg and milk exposure as immunotherapy in food allergy. Curr Allergy Asthma Rep. 2016;16(4):32. doi: 10.1007/s11882-016-0604-y
- Dantzer J, Dunlop J, Psoter KJ, et al. Efficacy and safety of baked milk oral immunotherapy in children with severe milk allergy: a randomized, double-blind, placebo-controlled phase 2 trial. J Allergy Clin Immunol. 2022;149(4):1383–1391.e17. doi: 10.1016/j.jaci.2021.10.023
- D’Auria E, Venter C. Precision medicine in cow’s milk allergy. Curr Opin Allergy Clin Immunol. 2020;20(3):233–241. doi: 10.1097/ACI.0000000000000640
- Krawiec M, Radulovic S, Foong R-X, et al. Diagnostic utility of allergy tests to predict baked egg and lightly cooked egg allergies compared to double-blind placebo-controlled food challenges. Allergy. 2023;78(9):2510–2522. doi: 10.1111/all.15797
- Ford LS, Bloom KA, Nowak-Węgrzyn AH, et al. Basophil reactivity, wheal size, and immunoglobulin levels distinguish degrees of cow’s milk tolerance. J Allergy Clin Immunol. 2013;131:180–186.e1–3. doi: 10.1016/j.jaci.2012.06.003
- Santos AF, Du Toit G, Douiri A, et al. Distinct parameters of the basophil activation test reflect the severity and threshold of allergic reactions to peanut. J Allergy Clin Immunol. 2015;135(1):179–186. doi: 10.1016/j.jaci.2014.09.001
- Chinthrajah RS, Purington N, Andorf S, et al. Development of a tool predicting severity of allergic reaction during peanut challenge. Ann Allergy Asthma Immunol. 2018;121(1):69–76.e2. doi: 10.1016/j.anai.2018.04.020
- Radulovic S, Foong R-X, Bartha I, et al. Basophil activation test as predictor of severity and threshold of allergic reactions to egg. Allergy. 2023;79(2):419–431. doi: 10.1111/all.15875
- Ruinemans-Koerts J, Schmidt-Hieltjes Y, Jansen A, et al. The basophil activation test reduces the need for a food challenge test in children suspected of IgE-mediated cow’s milk allergy. Clin Exp Allergy. 2019;49(3):350–356. doi: 10.1111/cea.13307
- Patil SU, Steinbrecher J, Calatroni A, et al. Early decrease in basophil sensitivity to ara h 2 precedes sustained unresponsiveness after peanut oral immunotherapy. J Allergy Clin Immunol. 2019;144(5):1310–1319.e4. doi: 10.1016/j.jaci.2019.07.028
- Tsai M, Mukai K, Chinthrajah RS, et al. Sustained successful peanut oral immunotherapy associated with low basophil activation and peanut-specific IgE. J Allergy Clin Immunol. 2020;145(3):885–896.e6. doi: 10.1016/j.jaci.2019.10.038
- Burks AW, Jones SM, Wood RA, et al. Oral immunotherapy for treatment of egg allergy in children. N Engl J Med. 2012;367(3):233–243. doi: 10.1056/NEJMoa1200435
- Jones SM, Pons L, Roberts JL, et al. Clinical efficacy and immune regulation with peanut oral immunotherapy. J Allergy Clin Immunol. 2009;124:292–300.e97. doi: 10.1016/j.jaci.2009.05.022
- Jones SM, Kim EH, Nadeau KC, et al. Efficacy and safety of oral immunotherapy in children aged 1-3 years with peanut allergy (the immune tolerance network IMPACT trial): a randomised placebo-controlled study. Lancet. 2022;399:359–371. doi: 10.1016/S0140-6736(21)02390-4
- Frischmeyer-Guerrerio PA, Masilamani M, Gu W, et al. Mechanistic correlates of clinical responses to omalizumab in the setting of oral immunotherapy for milk allergy. J Allergy Clin Immunol. 2017;140(4):1043–1053.e8. doi: 10.1016/j.jaci.2017.03.028
- Macglashan DW, Saini SS. Omalizumab increases the intrinsic sensitivity of human basophils to IgE-mediated stimulation. J Allergy Clin Immunol. 2013;132:906–911.e1–4. doi: 10.1016/j.jaci.2013.04.056
- MacGlashan DW, Savage JH, Wood RA, et al. Suppression of the basophil response to allergen during treatment with omalizumab is dependent on 2 competing factors. J Allergy Clin Immunol. 2012;130(5):1130–1135.e5. doi: 10.1016/j.jaci.2012.05.038
- Chinthrajah RS, Purington N, Andorf S, et al. Sustained outcomes in oral immunotherapy for peanut allergy (POISED study): a large, randomised, double-blind, placebo-controlled, phase 2 study. Lancet. 2019;394(10207):1437–1449. doi: 10.1016/S0140-6736(19)31793-3
- Vila L, Moreno A, Gamboa PM, et al. Decrease in antigen-specific CD63 basophil expression is associated with the development of tolerance to egg by SOTI in children. Pediatr Allergy Immunol. 2013;24(5):463–468. doi: 10.1111/pai.12070
- Elizur A, Appel MY, Nachshon L, et al. Cashew oral immunotherapy for desensitizing cashew-pistachio allergy (NUT CRACKER study). Allergy. 2022;77(6):1863–1872. doi: 10.1111/all.15212
- Nachshon L, Goldberg MR, Levy MB, et al. Efficacy and safety of sesame oral immunotherapy-A real-world, single-center study. J Allergy Clin Immunol Pract. 2019;7:2775–2781.e2. doi: 10.1016/j.jaip.2019.05.031
- Elizur A, Appel MY, Nachshon L, et al. Walnut oral immunotherapy for desensitisation of walnut and additional tree nut allergies (nut CRACKER): a single-centre, prospective cohort study. Lancet Child Adolesc Health. 2019;3(5):312–321. doi: 10.1016/S2352-4642(19)30029-X
- Santos AF, Lack G. Basophil activation test: food challenge in a test tube or specialist research tool? Clin Transl Allergy. 2016;6(1):10. doi: 10.1186/s13601-016-0098-7
- Patil SU, Calatroni A, Schneider M, et al. Data-driven programmatic approach to analysis of basophil activation tests. Cytometry B Clin Cytom. 2018;94(4):667–673. doi: 10.1002/cyto.b.21537
- Pascal M, Nopp A, Mayorga C. Building confidence in the basophil activation test: standardization and external quality assurance -an EAACI task force. Allergy. 2020;75:115–116.
- Santos AF, Couto-Francisco N, Bécares N, et al. A novel human mast cell activation test for peanut allergy. J Allergy Clin Immunol. 2018;142(2):689–691.e9. doi: 10.1016/j.jaci.2018.03.011
- Zbären N, Brigger D, Bachmann D, et al. A novel functional mast cell assay for the detection of allergies. J Allergy Clin Immunol. 2022;149(3):1018–1030.e11. doi: 10.1016/j.jaci.2021.08.006