
Abstract
The heart is generally perceived as the core of emotion, affection, and love. Its universally accepted iconic representation is everywhere these sentiments have to be depicted. However, the question is: where does the popular heart shape comes from? In fact, it is difficult to relate this symbol to the real heart shape. With possible early examples or direct predecessors in the 13th to 14th century, the familiar symbol of the heart representing love developed in the 15th century, and became popular in Europe during the 16th. While performing several coronary total occlusion recanalization procedures, it has become excitingly evident that, during contemporaneous dual injections of both right and left coronary arteries, the iconic shadow of the heart can be effectively observed. The possibility that the evidence of this cardiac shape could already be visible to the eyes of people living at the time of the first iconic appearances of the heart image is difficult to surmise. How could our ancestors connect the iconic form to the real heart shape? In the present article, we discuss how this iconic shape could have been derived from anatomical observations made in the ancient world.
Keywords:
Introduction
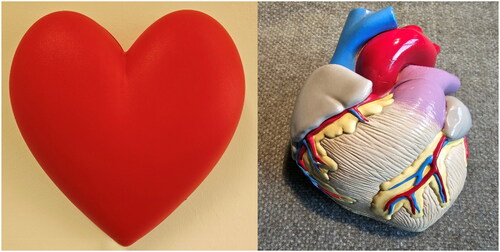
Medical students soon learn that the universally depicted symbol of the heart does not look anything like an actual human heart (). However, no one cares, since the use of the present symbol of the heart is limited to express the idea of the ‘heart’ in its metaphorical sense as the core of emotion, affection, and love. In fact, Greek philosophers considered the heart linked to our strongest emotions, including love. Aristotle is considered the precursor of the ‘cardiocentric’ hypothesis, granting the heart the supremacy in all human processes (Reynolds SWA, n.d). In the 7th century BC the poet Sappho agonised over her own ‘mad heart’ shaking with love (https://www.uh.edu/∼cldue/texts/sappho.html). In the island of Lesbos surrounded by female disciples she wrote passionate poems, like ‘Love shook my heart, Like the wind on the mountain Troubling the oak-trees’ (https://www.poetryintranslation.com/PITBR/Various/Tendsap.php). The relation between emotions and the heart could well be related to emotionally induced activation of the sympatho-adrenal system, inducing physiological increments of heart rate, blood pressure, cardiac contractility, the so called acute stress response that prepares the body to fight or flee (fight or flight reaction). In some cases, in presence of known or unknown pre-existing cardiac conditions, the reaction to a surge of stress hormones due to extreme emotions or even after a good shock (like winning the lottery) could lead to a ‘broken heart’, which is not a metaphorical figure but a real life threatening condition (Adu-Amankwaah, Citation2022).
Figure 1. Left: the popular representation of the human heart. Right: a plastic model of a real human heart from the anterior view. The two forms are only vaguely resembling each other.
The origin of the iconic heart shape
The question is, how did the human heart become transformed into the silhouette we currently use to represent it? One of the theories suggests that the origin of the heart symbol can be traced back to an ancient plant called silphium (https://en.wikipedia.org/wiki/Heart_symbol). Silphium was a species of giant fennel that used to grow on the North African coastline near the Greek colony of Cyrene. The Greeks and Romans used it as a spice, medicine, but also as a form of birth control. There is also speculation of it being modelled after human anatomy of the breasts or buttocks, as well as that of the water lily leaf or ivy (https://tampacardio.com/how-the-heart-shape-got-its-name-and-why-it-looks-nothing-like-the-human-heart/). Somehow the heart symbol reflects the real anatomical contours. The two upper curves of the symbol indicate the presence of two sides of the real organ, by some means responding to anatomical facts.
Nevertheless it is difficult to relate this symbol to the real heart shape. Since the times of the ancient Egypt, doctors living in Alexandria were performing autopsies. Five hundred years later, Galen produced anatomical reports which remained uncontested until 1543, when printed descriptions and illustrations of human dissections were published in the seminal work ‘De humani corporis fabrica’ by Andreas Vesalius. To understand the human anatomy better, and to improve their skills, the artists Leonardo da Vinci and Michelangelo also performed autopsies. Therefore, our ancestors had already a clear notion of the real anatomical features of the heart, which was clearly depicted in the anatomical books available at the times and representing the real shape. Indeed, the combination of the heart icon and its use within the heart metaphor was developed in the Middle Ages, although the shape had been used in many ancient epigraphy monuments and texts. With possible early examples or direct predecessors in the 13th to 14th century, the familiar symbol of the heart representing love developed in the 15th century, and became popular in Europe during the 16th (Vinken, Citation2001). However, the question is: where does the popular heart shape come from? In the present report we describe the serendipitous observation that the iconic heart shape could really derive from the real heart shape.
Cardiac catheterisation
Modern diagnostic cardiac catheterisation was introduced by André Cournand and Dickinson Richards in the early 1940s, and selective coronary angiography was described by Mason Sones in the early 1960s (Sones & Shirey, Citation1962). Coronary angiography is a minimally invasive procedure to access the coronary circulation using a catheter. It is performed for both diagnostic and interventional (treatment) purposes. Soon after, Charles Dotter and Melvin Judkins, in Portland, Oregon, begun to develop percutaneous transluminal coronary angioplasty (PTCA) using a wire and coaxial Teflon catheters to ‘unclog arteries, improving symptoms and peripheral blood flow’ (https://thoracickey.com/history-of-coronary-balloon-angioplasty-and-current-indications/#bib5) but for the lack of financial support they were not able to develop the technique further. However, the PTCA technique was refined by other investigators and finally, in 1974, Andreas Grüentzig, a young German radiologist, developed a double-lumen catheter at the distal end of which was a distensible balloon made of polyvinylchloride (Grüntzig & Hopff, Citation1974). When inflated, the balloon exerted circumferential pressure on the plaque and determined dilatation and, subsequentely, patency of the dilated vessel. The PTCA approach was first adopted to dilate vessels with discrete narrowings, stenoses, but with the continuos development of materials and techniques it has been progressively employed also to recanalize completely occluded vessels, coronary total occlusions (CTO). CTO in coronary artery is recognised by a significant atherosclerotic plaque burden within the artery, resulting in complete occlusion of the vessel and absence of any antegrade flow beyond the coronary occlusion. The introduction of enhanced guidewires, microcatheters combined with novel specialised devices and techniques has reduced the number of unapproachable CTO (Amsavelu et al., Citation2016). Most operators first approach CTO with the same floppy guidewires used for PTCA in non-occluded lesions. CTOs which cannot be crossed with floppy wires, can be encountered with different dedicated wires. In some cases, CTO cannot be crossed with an antegrade approach but the true lumen can be penetrated from a retrograde direction (via epicardial or septal collateral vessel or a bypass graft that connects with the distal vessel). In the retrograde approach, the guidewire reaches the distal cap of the occluded vessel through collateral vessels. As compared to proximal cap, distal cap is usually less resistant which makes penetration easier (Dave, Citation2016). Understanding the course of the guidewire is critical both for enhancing the likelihood of success and for minimising the risk for complications. This is accomplished in all cases using dual coronary injection, showing the path of collateral vessels filling the occluded artery beyond the occlusion. Dual contemporaneous coronary injection allows the operator to properly visualise the anatomy and correctly enter the distal true lumen: at this point, the micro-catheter is advanced past the occlusion, and the guidewire can be utilised as an antegrade way, permitting balloon and stent positioning in the culprit area.
Serendipitous evidence of the correspondence of the iconic with real heart shape
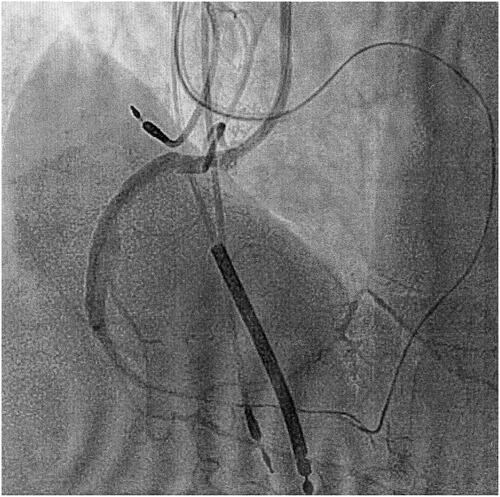
While performing several CTO recanalization procedures, it has become excitingly evident that during contemporaneous dual injections of both right and left coronary arteries, the iconic shadow of the heart can be effectively observed (). These images are regularly obtained during coronary angiography performed during recanalization of a CTO. By injecting at the same time both right and left coronary arteries, the entire coronary arterial circulation can be visualised. Contemporaneous visualisation of the right and left coronary trees form the exact shape of what we have been used to recognise as ‘the human heart’. However, the possibility that the evidence of this cardiac shape could already be visible to the eyes of people living at the time of the first iconic appearances of the heart image is difficult to surmise. How could they connect the iconic form to the real heart shape?
Figure 2. Appearance of the iconic shadow of the heart immediately after injection of the contrast dye in the right coronary artery, while the path of the left coronary system is evidenced by the path of the microcatheter previously deployed in a context of a retrograde approach (left anterior oblique projection 30°). These images are regularly obtained at coronary angiography performed during recanalization of a CTO. Contemporaneous visualisation of the right and left coronary trees form the exact shape of what we have been used to recognise as ‘the human heart’.
Coronary circulation casts
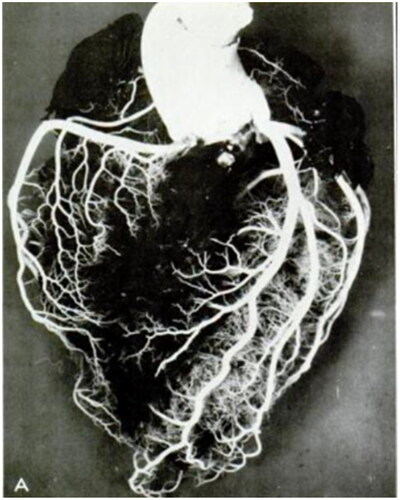
Going back to the ancient world, we reckon that since Erasistratus and Herophilus, we had a detailed account of the vascular system based on a systematic anatomical and functional distinction between veins and arteries (Reverón, Citation2014). However, these observations were not yet sufficient to admit a possible knowledge of the potential trueness of the popularly recognised shape of the heart. The anatomical patterns of the coronary arterial system were first investigated and reported through post-mortem injection and casts by the mid 1950s (Baroldi et al., Citation1954; Baroldi & Scomazzoni, Citation1967; James, Citation1965). By injecting plastic substances into the aorta under pressure, ranging from 130 to 200 mmHg, the obtained coronary circulation casts resembled the iconic shape of the heart (). These examples are the first reported images of coronary circulation casts, but it cannot be excluded that previous anatomists, scientists, artists could have done the same procedure, eventually with less sophisticated materials, and obtained similar shapes. From which, consequentially, the iconic form of the heart could be derived. In the old ages, anatomical studies were often performed by artists, who subsequentely could reproduce their ‘scientific’ observations into pictorial art. It is therefore likely that the replicated iconic shape of the heart could be derived from information obtained by inspections of real cardiac organs, probably aided by plaster moulds after injection of the coronary ostia. This hypothesis cannot be substantiated by coronary artery anatomical casts appearing before those relatively recent mentioned above. However, this appears as the most plausible hypothesis to explain the exact correspondence of our images with the old standing archetipal image of the heart.
Figure 3. Anterior surface of the heart, after injection of plastic materials (Geon Latex 576 and Neoprene 842A). The obtained vascular cast clearly resembles the iconic shape of the heart. Reproduced from Baroldi G, Scomazzoni G. Coronary Circulation in the Normal and Pathological Heart. Washington, DC: Office of the Surgeon General, Department of the Army; 1967.
Conclusion
Despite a universal appreciation, the traditional heart symbol has been traditionally considered a dummy. The contemporaneous injection of a contrast dye in both coronary arteries does provide evidence of an image superimposable to the popular heart icon. The hypothesis is that previous scientists had already obtained a similar form, probably by injecting with plaster the coronary arteries during autopsies and then transposing the obtained structure into drawings. However, further studies from medical historians are necessary to better investigate and eventually confirm this speculation.
Copyright agreement
The Corresponding Author has the right to grant on behalf of all authors and does grant on behalf of all authors, an exclusive licence on a worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be published in BMJ editions and any other BMJPGL products and sublicences such use and exploit all subsidiary rights, as set out in our licence.
Transparency declaration
The lead author affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Disclosure statement
All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years, no other relationships or activities that could appear to have influenced the submitted work.
References
- Adu-Amankwaah, J. (2022). “Happy heart” versus “broken heart” syndrome: The 2 faces of Takotsubo syndrome: Similarities and differences. JACC. Heart Failure, 10(7), 467–469. https://doi.org/10.1016/j.jchf.2022.02.016
- Amsavelu, S., Carlino, M., & Brilakis, E. S. (2016). Carlino to the rescue: Use of intralesion contrast injection for bailout antegrade and retrograde crossing of complex chronic total occlusions. Catheterization and Cardiovascular Interventions: Official Journal of the Society for Cardiac Angiography & Interventions, 87(6), 1118–1123. https://doi.org/10.1002/ccd.26418
- Baroldi, G., & Scomazzoni, G. (1967). Coronary circulation in the normal and pathological heart. Office of the Surgeon General, Department of the Army.
- Baroldi, G., Mantero, O., & Scomazzoni, G. (1954). Su di una nuova metodica di studio del circolo coronarico mediante sostanze plastiche [New method of the study of coronary circulation obtained with the aid of plastic substances]. Policlinico Prat, 61, 745–749. Italian.
- Dave, B. (2016). Recanalization of chronic total occlusion lesions: A critical appraisal of current devices and techniques. Journal of Clinical and Diagnostic Research: Jcdr, 10(9), OE01–OE07. https://doi.org/10.7860/JCDR/2016/21853.8396
- Grüntzig, A., & Hopff, H. (1974). Perkutane Rekanalisation chronischer arterieller mit einem neuen Dilatationskatheter. Deutsche Medizinische Wochenschrift (1946), 99(49), 2502–2510, 2511. https://doi.org/10.1055/s-0028-1108161
- https://en.wikipedia.org/wiki/Heart_symbol
- https://tampacardio.com/how-the-heart-shape-got-its-name-and-why-it-looks-nothing-like-the-human-heart/
- https://thoracickey.com/history-of-coronary-balloon-angioplasty-and-current-indications/#bib5
- https://www.poetryintranslation.com/PITBR/Various/Tendsap.php
- https://www.uh.edu/∼cldue/texts/sappho.html
- James, T. N. (1965). Anatomy of the coronary arteries in health and disease. Circulation, 32(6), 1020–1033. https://doi.org/10.1161/01.cir.32.6.1020
- Reverón, R. R. (2014). Herophilus and Erasistratus, pioneers of human anatomical dissection. Vesalius: Acta Internationales Historiae Medicinae, 20(1), 55–58.
- Reynolds SWA. (n.d.)The historical struggle for dominance between the heart, liver, and brain. The Proceedings of the 16th Annual History of Medicine Days, March 30th and 31st, 2007 Health Sciences Centre,. http://hdl.handle.net/1880/47541 conference proceedings.
- Sones, F. M., & Shirey, E. K. (1962). Cine coronary arteriography. Modern Concepts of Cardiovascular Disease, 31, 735–738.
- Vinken, P. (2001). How the heart was held in medieval art. Lancet (London, England), 358(9299), 2155–2157. https://doi.org/10.1016/S0140-6736(01)07224-5