Abstract
Background Most fractures of the proximal femur are easily diagnosed by conventional radiography. When the images are judged to be negative or equivocal and a clinical suspicion of fracture persists, another approach is to use magnetic resonance imaging (MRI) to help reach a diagnosis.
Methods In a prospective study running from November 1998 to December 2001, we registered all patients being examined by MRI who had had a negative or equivocal radiograph and where there was continued clinical suspicion of hip fracture.
Results 100 consecutive patients (67 women) were included, with an average age of 80 (37–100) years. The MRI examinations corresponded to 4% of the 2,350 patients admitted with hip trauma during the study period. 46 patients had a femoral neck or intertrochanteric fracture on MRI. 27 patients had other fractures. 18 had other findings on MRI, and 10 were interpreted as being negative, although one of these was a false negative. In a separate interobserver analysis, two experienced radiologists agreed on the diagnoses in 19/23 cases (kappa value 0.78). They agreed with a less experienced radiologist in 17/23 and 19/23 cases, respectively (kappa values 0.66 and 0.76).
Interpretation MRI is a useful tool for demonstration of occult hip fractures. In the absence of a hip fracture, another explanation for the patient’s pain and disability will often be given.
Most fractures of the proximal femur are easily diagnosed by conventional radiography. In cases where the images are negative or equivocal, and a continued clinical suspicion of fracture exists, magnetic resonance imaging (MRI) may be a useful tool in the diagnosis. The ability of MRI to detect occult fractures has been described for several locations, among them wrist, carpal bones, knee and hip (Ohashi et al. Citation1997, Brossmann et al. Citation1999, Rogers Citation2001). MRI has been in use in the detection of hip fractures for more than a decade (Deutsch et al. Citation1989). We have recently made MRI our standard diagnostic modality for occult hip fracture. We assessed the role of MRI in clinical decision-making, both in the surgical management and the conservative management of patients with a clinically suspected hip fracture, where there have been negative or equivocal plain films.
Patients and methods
In this prospective study, we registered all patients examined with MRI due to suspicion of a proximal femoral fracture in the period from November 1998 to December 2001. There were 100 patients (67 women) with a mean age of 80 (37–100)years. All patients with a clinical suspicion of hip fracture were examined with a conventional anteroposterior radiograph of the pelvis and a lateral view of the affected hip. When there was a negative or equivocal radiograph but continued clinical suspicion of hip fracture, the patients were also examined with MRI. Coronal STIR and T1-weighted series of the pelvis were made on a Philips Gyroscan Intera, with a 1.5 Tesla magnet. The procedure took less than 10 min (MRI time). A fracture was visualized as a linear low-density signal on T1 weighting, surrounded by an area of intermediate density. A high signal area surrounding the fracture on STIR aided in the diagnosis. The T1 weighting is specific for this indication, and has a better signal-to-noise ratio and anatomical resolution than with the T2-weighted images. STIR images are highly sensitive in detecting posttraumatic changes in both bone and soft tissue, but they are less specific than T1. T2 images may also be used for this purpose, but require more MRI time and give little additional information (Ingari et al. Citation1996, Resnick and Kang Citation1997, Schultz et al. Citation1999). In the intertrochanteric area, we registered a complete fracture when the linear black signal on T1 crossed more than half the width of the bone; otherwise it was registered as a partial fracture. Other findings and diagnoses on MRI were also registered. All images were read by one of three musculoskeletal radiologists. The charts and images of all patients were reviewed at least 1 year after the initial radiographic examination. The total numbers of hip traumas and hip fractures were calculated from the hospital database. 23 MRI series were randomly selected for an interobserver analysis involving two experienced musculoskeletal radiologists (A and B) and one radiologist (C) starting his training in musculosk-eletal radiology.
A conventional radiograph interpreted as being negative. In retrospect, it may be possible to see an irregularity in the proximal cortex of the femoral neck.

A T1 weighted image with a subcapital femoral neck fracture as a black line with a somewhat vertical progression through the femoral neck.
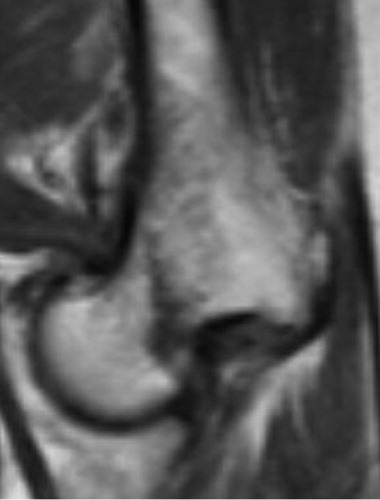
An STIR image showing high signal areas surrounding the fracture (white and light gray) and extending towards the lesser trochanter, indicating a recent trauma.

Results
There were no differences in age and sex between those who were proven to have a fracture and those who were not. 51 patients were admitted on the day of their injury. 42 patients were admitted on average 3 (1–14) days after injury. 3 patients were diagnosed as outpatients, and for 4 patients no date of injury could be established. For the patients who were admitted, there was an average of 2 days between examination by conventional radiography and the MRI examination. The MRI examinations constituted 4% of the total of 2,350 patients who were admitted because of hip trauma during the registration period. Of these 2,350 patients, 1,818 had hip fractures, 157 had stable pelvic fracture and in 375 patients no fracture was found.
At conventional radiography, the most serious injury was recorded for each patient (). 52 radiographs were negative, 41 raised the suspicion of a fracture, 7 patients had severe osteoarthrosis making interpretation difficult, and 1 radiograph was interpreted as possible osteolysis. The MRI diagnoses of the patients with negative radiographs (n = 52) were complete fracture in 34 cases (65%), another specific diagnosis in 10 cases, while 6 remained negative, although one later proved to be a false negative. 21 of these 52 patients were operated. Patients with suspected fracture on radiographs and patients with a fracture of the greater trochanter (n = 41) were diagnosed by MRI to have complete fractures in 35 cases, of which 23 were operated. 8 patients had severe osteoarthrosis, making interpretation of the conventional radiographs difficult. 7 of these were initially interpreted as negative for fracture by conventional radiography, and one was interpreted as a suspected femoral neck fracture. None of these 8 patients had complete fractures by MRI. In 1, how-ever, there seemed to be a subcapital skeletal injury to the femoral neck, involving about one-third of the diameter, which was interpreted as a partial fracture of the femoral neck. In total, 44 of the 46 patients diagnosed with a femoral neck fracture or an intertrochanteric fracture were operated.
Table 1. Crosstable giving diagnoses after conventional radiography and the corresponding diagnoses after magnetic resonance imaging
In 1 patient, a large tumor surrounding one of the ovaries was found on MRI, in addition to a femoral neck fracture. The patient died before this finding could be investigated further. 1 patient with a negative conventional radiograph and negative by MRI was readmitted after 4 days with a dislocated femoral neck fracture without having sustained a new trauma, and without having been mobilized in the nursery home. This MRI result was consequently the only false negative found.
It seemed to be possible to divide the 10 patients who were shown to have an isolated fracture of the greater trochanter on MRI into two subgroups based on the MRI findings. In one subgroup (consisting of 7 patients), the anterior portion of the greater trochanter was mainly involved, with changes in the gluteus medius muscle. In the other subgroup (consisting of 3 patients), loosening of the posterior portion of the greater trochanter and laxity in the gluteus minimus muscle was found. 9 of these patients had sustained a low-energy fall with direct trauma to the hip 0–5 days before admission. For 1 patient, no date of trauma could be established.
We classified the MRI examinations retrospectively as to whether they were of decisive importance for further treatment. In 43 cases, the MRI results directly dictated the treatment. In 30 cases, MRI led to operative treatment of a proximal femoral fracture. In 13 cases, the MRI examination enabled us to institute further investigations or nonoperative treatment essential to the patient, which would probably have been delayed without the MRI scan. 2 of these patients were diagnosed with previously unrecognized malignant disease and were transferred to other departments for further investigation and treatment. 2 had proximal femoral fractures that were treated conservatively due to serious medical conditions, and both healed uneventfully. 1 had a fracture of the acetabulum and was instructed to avoid weight bearing on the affected side for a limited period. In 1 case, a diagnosis of femoral neck fracture was given on conventional radiography by the radiologist, but the surgeon was not convinced and requested an MRI, which showed no fracture. Unnecessary surgery was probably avoided in this case. The remaining 7 had radiographs with suspicion of a fracture of the proximal femur, but the MRI investigations were negative and conservative management could be instituted.
Interobserver variability
The kappa value between radiologists A and B was 0.78 (SE 0.10). Between A and C, the kappa value was 0.66 (SE 0.12), and between B and C it was 0.76 (SE 0.11). There were 4 discrepancies in the interpretations between radiologists A and B (). In 3 cases, radiologist A diagnosed an isolated fracture of the greater trochanter whereas radiologist B found a fracture with intertrochanteric extension. 2 of these patients underwent surgery for fractures with intertrochanteric extension while hospitalized, and the third was treated conservatively with fracture of the greater trochanter as the diagnosis. In one case, radiologist A diagnosed severe osteoarthrosis, and radiologist B a femoral neck fracture with severe osteoarthrosis. The original interpretation of this examination was a partial femoral neck fracture, as noted above. The patient was treated nonoperatively with gradual improvement of pain and walking ability. The less experienced radiologist C interpreted the 3 MRIs in which A and B found pelvic and acetabular fractures, as negative. Apart from that, radiologist C only disagreed with either one of the other two radiologists in the 4 examinations where radiologists A and B also had different interpretations.
Table 2. MRI diagnoses given by radiologist A and B (both experienced musculoskeletal radiologists) in 23 randomly selected examinations. Differences in interpretation are marked with red
Discussion
Our study demonstrates that easy access to MRI aids the diagnostic work associated with suspected proximal femoral fractures, and can lead to changes of treatment. In our hospital, nondislocated femoral neck and intertrochanteric fractures are treated operatively in order to shorten hospital stay and rehabilitation time, to avoid complications related to prolonged immobilization and because a secondary dislocation or nonunion worsens the prognosis (Parker Citation1992, Cserhati et al. Citation1996, Pathak et al. Citation1997, Raaymakers Citation2002, Parker et al. Citation2004). About half of the patients in our series underwent surgery as a consequence of the MRI examinations. For 30 of them, we judge that the MRI examination was decisive for their treatment. Furthermore, for most patients without a fracture, an explanation for their hip pain was possible after the MRI examination, enabling an individualized plan of treatment and rehabilitation to be established without delay.
Ingari and coworkers (Citation1996) induced non-dislocated fractures in cadaveric femora. In their study, the black lines on T1 weighting were found—and confirmed by histology—to represent trabecular impaction in the absence of bleeding and edema. They concluded that the low signal band was a direct visualization of the fracture itself, thereby strengthening the assumption that there was no need to delay in the MRI examination after injury to await secondary changes in order to make the diagnosis. MRI results are, however, investigator-related to some extent. This can be illustrated by the fact that we presented the one false-negative MRI examination in our series to a senior radiologist (RT) 2 years after the original reading, and this time he interpreted it as a fracture. This error of judgment probably results from paying too much attention to the STIR sequence, which showed limited changes. The existence of a learning curve may also be an important consideration, as this was one of our first MRI examinations performed on this indication. We believe that the T1 sequence is essential for a fracture diagnosis.
A higher rate of intertrochanteric fracture extensions has been found previously when using MRI to investigate isolated fractures of the greater trochanter (diagnosed on plain films) in greater depth () (Schulz et al. Citation1999, Craig et al. Citation2000, Omura et al. Citation2000). In adults, these fractures are probably wrongly interpreted usually as avulsion fractures—even if they result from the same mechanism of trauma as most hip fractures, a direct blow to the greater trochanter (Merlino and Nixon Citation1969). Thus, if a fracture of the greater trochanter is demonstrated on plain films, one should reexamine these patients clinically and follow them closely during mobilization, as an undisplaced intertrochanteric fracture may be present. The finding of an isolated fracture of the greater trochanter, however, is probably not in itself an indication for MRI.
Partial or incomplete fractures of the femoral neck on MRI are rare. Apart from the one with severe osteoarthrosis, all fractures of the femoral neck were clearly visualized through the entire femoral neck on the T1 weighted sequence. In the intertrochanteric area, however, the presence of a fracture line from the greater trochanter towards the lesser trochanter, but not always breaching the medial cortex, is known to occur (Schultz et al. Citation1999). In our department, we treat fractures of less than half the bone width nonoperatively. We usually operate fractures with a further coronal extension because they are unstable, resulting in large stress on the medial cortex. Based on the clinical consequences, we have used the same distinction in the MRI diagnoses, and only fractures with intertrochanteric extension not crossing the midline are registered as incomplete fractures. As a definition, this may seem arbitrary. A more anatomically correct definition of complete fractures, including mandatory crossing of both cortices by the fracture line, would be less functional for us in the clinical context.
Various other methods have been described for diagnosis of occult proximal femoral fractures. These include CT scans, conventional tomography, repeated radiographs and other methods (Egund et al. Citation1990, Alba and Youngberg Citation1992, Strange-Vognsen et al. Citation1992, Sanville et al. Citation1994, Conway et al. Citation1996, File et al. Citation1998, Helland et al. Citation2000). Scintigraphy, another well-established method of detecting occult fractures of the proximal femur, has the disadvantage of being dependent on the timing of the examination, and has a lower sensitivity and specificity than MRI. Scintigraphy would also be less reliable in very old patients and patients with circulatory disturbances (Lewis et al. Citation1991, Evans et al. Citation1994, Pandey et al. 1998). MRI may reduce the length of stay in hospital by expediting definitive treatment sooner, and may thus be more cost-effective (Quinn and McCarthy Citation1993, Rizzo et al. Citation1993, Rubin et al. Citation1998). Our experience with the use of MRI is similar to those of previous authors who mainly presented smaller studies with a lower percentage of fractures—including the finding that in the absence of a fracture of the proximal femur another explanation for the patient’s symptoms will be offered (Feldman et al. Citation1994, Guanche et al. Citation1994, Haramati et al. Citation1994, Bogost et al. Citation1995, May et al. Citation1996, Stiris and Lilleas Citation1997, Pandey et al. Citation1998, Oka and Monu Citation2004).
The interobserver agreement between the two experienced radiologists A and B was good according to the guidelines of Altman (Citation1997) as was the agreement between radiologists B and C. The agreement between radiologists A and the less experienced radiologist C seemed to be somewhat poorer, but was still acceptable. The disagreements of interpretation between the experienced radiologists occurred in a patient with disturbing pathological signals on MRI due to traumatized severe osteoarthritis. The other area of difficulty was to separate a fracture of the greater trochanter from a fracture with an intertrochanteric extension. The good agreement, at least regarding diagnoses in the proximal femur, between the less experienced radiologist and the two more experienced ones may indicate that MRI used for this purpose may also be useful in departments performing smaller numbers of examinations than we do. The lack of fracture diagnoses on the part of radiologist C in areas away from the proximal femur may have been due to his experience.
One weakness of the present study was that no formal protocol for referral to MRI during the study period was applied. Furthermore, false-positive examinations will not be disclosed with the present design: the fracture itself is not exposed during surgical treatment, and at follow up the absence of a visible fracture or signs of healing will not be conclusive. Thus, this patient series reflects the routine use of MRI in the detection of occult hip fractures. For practical reasons, it is not possible to perform MRI scans on all patients with hip pain after trauma who have negative conventional radiographs. Therefore, one probably has to accept that hip fractures might be overlooked occasionally. With careful clinical examination and liberal use of MRI, however, it should be possible to keep this number to a minimum. To provide the best service for our patients, and to avoid unnecessary hospital stay and delay in surgery, MRI should be performed as soon as possible after inconclusive radiography. During planning of radiology resources, one should take into account that about 4% of hip trauma patients will need an emergency MRI scan. Despite a negative or equivocal conventional radiograph, but with a clinical suspicion of fracture, almost half of such patients had a fracture in need of operative treatment as diagnosed by MRI. In almost all the remaining cases, another explanation for the patient’s pain and disability could be given, thus offering a guide for further treatment.
We thank radiologists Sølve Sesseng and Johan Castberg Hellund for help with the interobserver variability study, and Kåre Osnes for assisting with kappa statistics.
No competing interests declared.
- Alba E, Youngberg R. Occult fractures of the femoral neck. Am J Emerg Med 1992; 10(1)64–8
- Altman D G. Interrater agreement. Practical statistics for medical research. Chapman & Hall, London 1997; 403–9
- Bogost G A, Lizerbram E K. Crues III JV MR imaging in evaluation of suspected hip fracture: frequency of unsuspected bone and soft-tissue injury. Radiology 1995; 197: 263–7
- Brossmann J, Biederer J, Heller M. MR imaging of musculoskeletal trauma to the pelvis and the lower limb. Eur Radiol 1999; 9(2)183–91
- Conway W F, Totty W G, McEnery K W. CT and MR imaging of the hip. Radiology 1996; 198(2)297–307
- Craig J G, Moed B R, Eyler W R, van Holsbeeck M. Fractures of the greater trochanter: intertrochanteric extension shown by MR imaging. Skeletal Radiol 2000; 29(10)572–6
- Cserhati P, Kazar G, Manninger J, Fekete K, Frenyo S. Non-operative or operative treatment for undisplaced femoral neck fractures: a comparative study of 122 non-operative and 125 operatively treated cases. Injury 1996; 27(8)583–8
- Deutsch A L, Mink J H, Waxman A D. Occult fractures of the proximal femur: MR imaging. Radiology 1989; 170(1 Pt 1)113–6
- Egund N, Nilsson L T, Wingstrand H, Strömqvist B, Pettersson H. CT scans and lipohaemarthrosis in hip fractures. J Bone Joint Surg Br 1990; 72(3)379–82
- Evans P D, Wilson C, Lyons K. Comparison of MRI with bone scanning for suspected hip fracture in elderly patients. J Bone Joint Surg Br 1994; 76(1)158–9
- Feldman F, Staron R, Zwass A, Rubin S, Haramati N. MR imaging: its role in detecting occult fractures. Skeletal Radiol 1994; 23(6)439–44
- File P, Wood J P, Kreplick L W. Diagnosis of hip fracture by the auscultatory percussion technique. Am J Emerg Med 1998; 16(2)173–6
- Guanche C A, Kozin S H, Levy A S, Brody L A. The use of MRI in the diagnosis of occult hip fractures in the elderly: a preliminary review. Orthopedics 1994; 17(4)327–30
- Haramati N, Staron R B, Barax C, Feldman F. Magnetic resonance imaging of occult fractures of the proximal femur. Skeletal Radiol 1994; 23(1)19–22
- Helland E B, Tollefsen I, Reksten G. Radiographic diagnosis of the occult hip fracture: experience in 16 patients. Acta Orthop Scand 2000; 71(6)639–41
- Ingari J V, Smith D K, Aufdemorte T B, Yaszemski M J. Anatomic significance of magnetic resonance imaging findings in hip fracture. Clin Orthop 1996, 332: 209–14
- Lewis S L, Rees J I, Thomas G V, Williams L A. Pitfalls of bone scintigraphy in suspected hip fractures. Br J Radiol 1991; 64(761)403–8
- May D A, Purins J L, Smith D K. MR imaging of occult traumatic fractures and muscular injuries of the hip and pelvis in elderly patients. AJR Am J Roentgenol 1996; 166(5)1075–8
- Merlino A F, Nixon J E. Isolated fractures of the greater trochanter. Int Surg 1969; 52(2)117–24
- Ohashi K, Brandser E A, el-Khoury G Y. Role of MR imaging in acute injuries to the appendicular skeleton. Radiol Clin North Am 1997; 35(3)591–613
- Oka M, Monu J U. Prevalence and patterns of occult hip fractures and mimics revealed by MRI. AJR Am J Roentgenol 2004; 182(2)283–8
- Omura T, Takahashi M, Koide Y, Ohishi T, Yamanashi A, Kushida K, Inoue T. Evaluation of isolated fractures of the greater trochanter with magnetic resonance imaging. Arch Orthop Trauma Surg 2000; 120(3–4)195–7
- Pandey R, McNally E, Ali A, Bulstrode C. The role of MRI in the diagnosis of occult hip fractures. Injury 1998; 29(1)61–3
- Parker M J. Missed hip fractures. Arch Emerg Med 1992; 9: 23–7
- Parker M J, Handoll H H G, Bhargara A. Conservative versus operative treatment for hip fractures (Cochrane review). The Cochrane Library. John Wiley & Sons, Ltd, ChichesterUK 2004, Issue 1,
- Pathak G, Parker M J, Pryor G A. Delayed diagnosis of femoral neck fractures. Injury 1997; 28(4)299–301
- Quinn S F, McCarthy J L. Prospective evaluation of patients with suspected hip fracture and indeterminate radiographs: use of T1-weighted MR images. Radiology 1993; 187(2)469–71
- Raaymakers E L. The non-operative treatment of impacted femoral neck fractures. Injury 2002; 33(Suppl 3)C8–14
- Resnick D, Kang H S. Hip and femur. Occult fractures. The internal derangement of joints. Emphasis on MR imaging, D Resnick, H S Kang. WB Saunders, Philadelphia 1997; 520–5
- Rizzo P F, Gould E S, Lyden J P, Asnis S E. Diagnosis of occult fractures about the hip. Magnetic resonance imaging compared with bone-scanning. J Bone Joint Surg (Am) 1993; 75(3)395–401
- Rogers L F. What is the role of MR imaging in acute skeletal trauma. AJR Am J Roentgenol 2001; 177(6)1245
- Rubin S J, Marquardt J D, Gottlieb R H, Meyers S P, Totterman S M, O'Mara R E. Magnetic resonance imaging: a cost-effective alternative to bone scintigraphy in the evaluation of patients with suspected hip fractures. Skeletal Radiol 1998; 27(4)199–204
- Sanville P, Nicholson D A, Driscoll P A. ABC of emergency radiology. The hip. BMJ 1994 19; 308(6927)524–9
- Schultz E, Miller T T, Boruchov S D, Schmell E B, Toledano B. Incomplete intertrochanteric fractures: imaging features and clinical management. Radiology 1999; 211(1)237–40
- Stiris M G, Lilleas F G. MR findings in cases of suspected impacted fracture of the femoral neck. Acta Radiol 1997; 38(5)863–6
- Strange-Vognsen H H, Neergaard K, Schantz K. CT scan compared to tomography in suspected hip fracture. Arch Orthop Trauma Surg 1992; 111(2)124–5