Abstract
Background Classification of fractures is crucial in decision making and planning of acetabular surgery. Transverse fractures with secondary vertical fracture lines—which constitute either a large posterio-superior fragment (floating dome) or an inverse T with the posterior ileum attached to the axial skeleton—have not been described in detail in the literature.
Methods All acetabular fractures at Ullevål University Hospital have been recorded prospectively since 1993 and classified according to Judet/Letournel.
Results In 10/449 fractures (2%) there was a transverse fracture line through the acetabulum, with an additional vertical fracture line ascending either to the iliac crest or the SI-joint. In 6 of these fractures the vertical line started within the acetabulum, and the posterior part of the ileum with part of the articular surface was attached to the axial skeleton. In 4 fractures the vertical fracture line started posterior to the joint, constituting a very large posterio-superior fragment without any articular surface (a floating dome).
Interpretation Open reduction and internal fixation of inverse T-fractures and transverse fractures with a floating dome require different surgical approaches. The latter can be treated through a single approach alone, while the inverse T-fracture may require extensile or combined approaches for adequate reduction and fixation.
▪
Fracture classification is essential in order to obtain information about treatment options, for prognosis, and in comparing results of treatment.
In acetabular fracture surgery, the fracture lines transverse a complex 3-dimensional pelvis and a comprehensive classification system is decisive in preoperative planning (Jimenez and Vrahas Citation1997). In complex fractures anatomic reduction is important for preservation of hip function (Matta Citation1996, Mears et al. Citation2003).
There are two comprehensive classification methods for acetabular fractures: the classification of Judet/Letournel (Letournel and Judet Citation1993) and the AO classification (OTA Citation1996). The classification system most widely used was presented by Judet/Letournel in 1964 (Judet et al. Citation1964) and improved later on. It has shown high inter- and intra-observer reliability (Beaule et al. Citation2003). The classification has 10 main categories and subgroups which cover the transitional forms.
In the transverse category, there are transitional groups with a secondary vertical fracture line which constitutes either a floating dome (a very large posterio-superior fragment extending to the crest), or an inverse T with the posterior ileum attached to the axial skeleton. These fractures have been described previously, but the inverse T-fracture has not been discussed to any great extent in the literature.
Methods
Since 1993, acetabular fractures admitted or referred to Ullevål University Hospital have been recorded prospectively according to a protocol developed by the senior author (OR). All radiographs taken at admission and through follow-up are collected and archived. At admission, anterior-posterior (a-p) and oblique radiographs are taken and a CT-scan of the pelvis is performed. At follow-up, only a-p and oblique views are taken. All fractures have been classified initially by the experienced pelvic surgeons treating the patient and re-evaluated later on by the authors. The Judet/Letournel classification is used. Data from the operations and follow-ups at 3, 6 and 12 months and at 2, 5, 7–8 and 10 years are recorded. The data in this study were taken from the patient records made during their hospital stay in the period 1993 through 2003.
Fracture lines
Results
Among the 449 fractures in 443 patients during the inclusion period, 10 fractures (2.2%) were classified according Judet/Letournel as transverse fractures with a secondary vertical fracture line. 6 fractures were classified as inverse T-fractures and 4 fractures were classified as transverse fractures with a floating dome (large posterio-superior fragment).
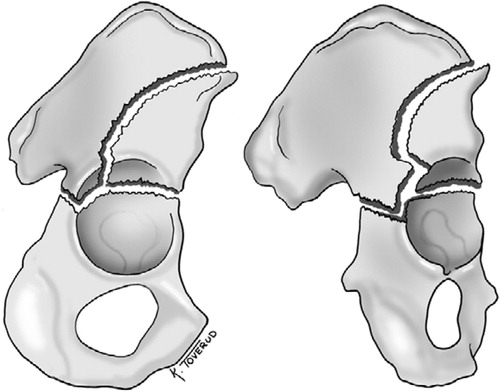
In the inverse T-fractures (, and ) the additional vertical line stretched upwards from the horizontal line either to the iliac crest (5 patients) or to the sacroiliac joint (1 patient, no. 5; see Table). The transverse fracture was rather oblique and no fracture lines involved the obturator foramen. The part of the ileum attached to the axial skeleton reached the posterior part of the acetabular joint and had a segment with articular cartilage ( and , arrow B).
Figure 1. The inverse T-fracture in 75° (A) and 150° (B) oblique view. Notice the ileum attached to the axial skeleton and with articular cartilage stretching into the joint posteriorly.
In 1 patient (no. 2), the vertical fracture line divided and stretched both to the anterior superior iliac spine and to the crest. In 1 patient (no. 3), the vertical line was incomplete at the iliac crest, even though there was significant dislocation where the vertical and horizontal lines met. In 1 patient (no. 4), there was a straddle fracture in the anterior pelvic ring and though the obturator foramen was involved in front, the anterior pelvic fracture was not connected to the acetabular fracture system. There were separate posterior wall fractures in 2 patients (nos. 2 and 4).
In addition to the 6 inverse T-fractures, there were 4 fractures classified as transverse fractures with a large posterio-superior fragment extending to the iliac crest in accordance with the Judet/Letournel classification ( and , ). The fracture lines followed principally the same pattern, and in 1 patient (no. 7, Table) the transverse fracture line stretched from the ileopubic eminence through the acetabulum as a juxta-tectal fracture and running backwards inferiorly. Then the fracture line crossed the tuberischial line in the middle between the major sciatic notch and the sciatic spine. The extraarticular fracture line ran upwards from the transverse fracture and ischial corpus just anterior to the tuberischial line to the crest just above the anterio-superior iliac spine. In addition to the main fracture system, one of the patients had an almost undetectable, undislocated fissure through the incisura acetabuli into the obturator foramen without any fissures in the ischial corpus, sciatic rami or pubic bones.
Figure 2. The transverse fracture with a floating acetabular dome in 75° (A) and 150° (B) oblique view. The acetabular dome is neither connected to the axial skeleton of the ileum nor to the ischium or the pubic bone.
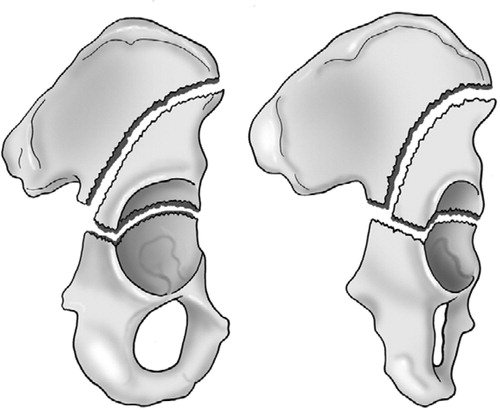
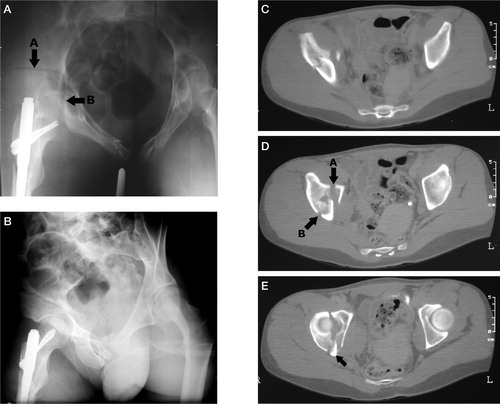
Figure 3. Patient no. 2 with an inverse T-fracture. In panel A, arrow A points to the vertical fracture line which divides and ascends to the crest and ant. sup. iliac spine. Arrow B points to the transverse fracture line. The axial scan in panel B shows the vertical fracture line which is also marked by arrow B in panel C. In this panel, arrow A marks the start of the transverse fracture. The posterior wall fragment is pointed out in panel D, and in panel E the distal end of the ileum with articular cartilage connected to the axial skeleton is marked with an arrow. Panel F shows the posterior wall fragment and there are no fracture lines involving the foramen obturatum.
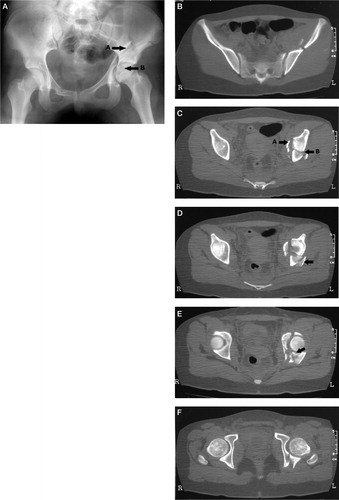
Figure 4. The inverse T-fracture of patient no. 4 is shown in panel A, and arrow A marks the vertical fracture line. Arrow B marks the transverse fracture line. On the oblique iliac view in panel B, the arrow points to the attached ileum with articular cartilage stretching into the joint posteriorly. In panel C, the vertical fracture is shown and both the vertical (A) and transverse (B) fracture lines are pointed out in panel D. The scan also shows comminution with an additional fragment marked C between the attached and unattached ileum. The posterior wall fragment is marked A in panel E and the arrow B points to attached ileum with articular cartilage. The most distal part of the attached ileum is marked in panel F. There are no fracture lines into the foramen obturatum.
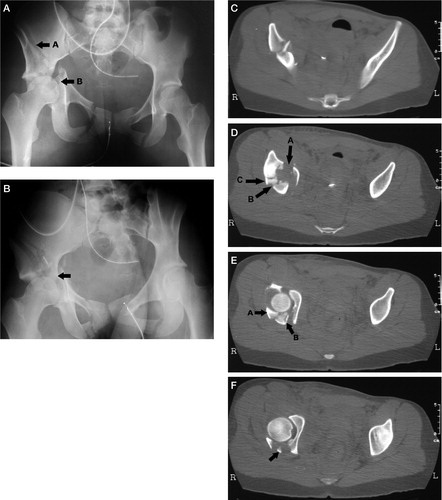
Figure 5. The transverse fracture with a floating acetabular dome is shown. In panel A with the pelvis inlet view, arrow A points to the vertical fracture line. Arrow B marks the transverse fracture line. (The inlet view is not part of standard radiographic examination of acetabular fractures.) In panel B, the iliac view clearly shows the vertical fracture line. The vertical line is also obvious on the axial CT-scan shown in panel C. Arrow A in panel D points to the start of the transverse fracture and arrow B shows the vertical fracture line. The scan is just proximal to the dome. In panel E, the arrow points to ileum connected to the IS-joint. No part of the acetabulum is attached to the axial skeleton.
1 patient with inverse T (no. 5, Table) died on the day of admission due to concomitant head trauma. Patient no. 6, aged 73 years, had osteoporotic bone stock, minor fracture dislocation, and was treated nonoperatively. The other 4 patients were treated with simultaneous double approaches. The anterior (ilieoinguinal) and posterior (Kocher-Langenbeck) approaches were used in 3 of the 4 operated patients with inverse T. The fourth patient (no. 1) was treated through a posterior incision combined with the proximal part of the ilieoinguinal approach. In the same period, only 9 of 151 complex acetabular fractures were treated using simultaneous anterior and posterior approaches.
Patient no. 3 was initially operated on through an anterior incision and later reoperated using both anterior and posterior approaches, due to unacceptable dislocation in the posterior column and inadequate screw positioning. The unacceptable posterior dislocation was not recognized during the first procedure.
1 patient with large posterio-superior fragment was treated nonoperatively due to alcohol abuse. The 3 others were operated using the anterior approach for the acetabular fractures with additional incisions in 2 cases due to pelvic ring fractures.
Discussion
In the well-recognized Judet/Letournel classification (Letournel and Judet Citation1993), there are 10 main categories and 52 subgroups that cover the transitional types of acetabular fractures. In their book (Letournel and Judet Citation1993), the authors discussed the inverse T-fracture, but could not recognize any such fractures in their clinical material complying with the qualifications. Their series is from the start of the era of CT-scanning. According to Judet and Letournel, an inverse T-fracture would have the main characteristics of an articular fragment attached to the posterior part of the iliac wing. As shown in and , and and , the fractures in our material comply with their definition of an inverse T-shaped fracture and demonstrate segments with articular cartilage being attached to the posterior ileum.
Judet and Letournel also discuss a fracture entity with a secondary vertical fracture line constituting a very large posterio-superior fragment. The fractures are classified as a transitional form with no segment of articular cartilage attached to the iliac fragment connected to the axial skeleton. This type of fracture is identical to 4 of the transitional fractures in our series. The entire dome is neither connected to the axial skeleton nor to the ischiopubic fragment. A more precise and more easily understandable name for this fracture is a transverse fracture with a floating acetabular dome.
The AO classification of acetabular fractures (OTA Citation1996) builds upon the general AO philosophy of fracture classification and on the Judet/Letournel classification. It can be pointed out that the inverse T-fracture is a B3.1 or B3.2 in the AO classification. However, then the main characteristics of the fracture with an undisturbed obturator foramen and a vertical fracture line stretching either to the iliac crest or the sacroiliac joint is missed. Important information needed in preoperative planning will thus be concealed.
Harris et al. (Citation2004) proposed a new CT-based classification system for simplicity and to avoid ambiguity. In this system, both the inverse T-fracture and the fracture with floating dome will be type IIB, a two-column fracture with superior extension. The classification system does not reveal differences between the fracture types.
One of the distinctive characteristics of the inverse T-fracture, of significant surgical relevance, is that a segment of the articular surface is attached to the posterior part of the iliac wing and the axial skeleton. This segment should be the starting point for the internal fixation. In these fractures, perfect reduction of the posterior column is difficult and may even be impossible to achieve using an anterior approach. On the other hand, dislocation of the anterior column and the anterior part of the iliac wing requires an anterior approach. Simultaneous anterior and posterior approaches were used in the 4 operated inverse T-fractures, while this was only used in 9 of all 151 surgically treated complex fractures in the same period of time. When treating the inverse T-fracture, one should be prepared to expose both the posterior column from behind and the anterior column either by the use of an extensile incision or combined anterior and posterior approaches.
- Beaule P E, Dorey F J, Matta J M. Letournel classification for acetabular fractures. Assessment of interobserver and intraobserver reliability. J Bone Joint Surg (Am) 2003; 85(9)1704–9
- Harris J H, Jr., Coupe K J, Lee J S, Trotscher T. Acetabular fractures revisited: part 2, a new CT-based classification. AJR Am J Roentgenol 2004; 182(6)1367–75
- Jimenez M, Vrahas M. Surgical approaches to the acetabulum. Orthop Clin North Am 1997; 28(3)419–34
- Judet R, Judet J, Letournel E. Fractures of the acetabulum: Classification and surgical approaches for open reduction. J Bone Joint Surg (Am) 1964; 46: 1615–46, Preliminary report
- Letournel E, Judet R. Fractures of the acetabulum. Springer-Verlag, New York, London, Berlin, Heidelberg 1993
- Matta J M. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg (Am) 1996; 78(11)1632–45
- Mears D C, Velyvis J H, Chang C P. Displaced acetabular fractures managed operatively: indicators of outcome. Clin Orthop 2003, 407: 173–86
- OTA Fracture and dislocation compendium. Orthopaedic Trauma Association Committee for Coding and Classification. J Orthop Trauma (Suppl 1) 1996; 10: v–ix; 1–154