Abstract
Background The Bernese periacetabular osteotomy is used in dysplastic hips to increase the load-bearing area of the hip and to prevent osteoarthritis.The aim of our work was to determine the contact hip stress before and after the osteotomy and to compare the relief of stress with the long-term radiographic and clinical outcome.
Patients and methods We followed 26 dysplastic hips (26 patients) for 7–15 years after the index operation. Clinical evaluation was based on the WOMAC score, osteoarthrosis was evaluated with the Tönnis classification, the angles of lateral (CE) and anterior (VCA) femoral coverage were measured, and biomechanical parameters were studied.
Results Periacetabular osteotomy increased the mean CE from 15° to 37°, and the mean VCA from 22° to 38°. The mean normalized peak contact stress was reduced from 5.2 to 3.0 kPa/N. Four hips required total hip arthroplasty after an average of 4.5 years, 8 hips showed considerable arthrosis progression, and 14 hips had no or mild arthrosis at follow-up. Preoperative WOMAC score, preoperative Tönnis grade and postoperative normalized peak contact stress were the most important predictors of outcome.
Interpretation The Bernese periacetabular osteotomy improves the mechanical status of the hip. Long-term success depends on the grade of arthrosis preoperatively and on the magnitude of operative correction of the contact hip stress.
▪
Hip dysplasia is a structural hip disorder that can lead to degenerative joint disease in early adulthood (Weinstein Citation1987, Murphy et al. Citation1995). The development of secondary arthrosis is thought to be caused by increased contact hip stress due to reduced femoral head coverage (Maxian et al. Citation1995, Michaeli et al. Citation1997) and reorientation of the acetabulum is used to correct acetabular dysplasia in order to prevent progression of arthrosis. Several operative procedures to increase femoral head coverage have been described (Salter Citation1961, LeCoeur Citation1965, Chiari Citation1974, Tönnis Citation1979), but they offer limited correction and the instability of the hemipelvis does not allow immediate weight bearing. Because of such limitations, the ‘Bernese’periacetabular osteotomy was developed in 1984 and published in 1988 (Ganz et al. Citation1988).
The procedure has become widely used because it allows optimal correction with minimal exposure and low complication rate, although the operation is technically demanding with a long learning curve (Søballe Citation2003). Ideally, this procedure would be indicated in younger adults with concentric hip motion, spherical joint surfaces and no secondary arthrosis—but many patients who present with symptomatic hip dysplasia do not meet these criteria (Murphy and Deshmukh Citation2002). Many attempts have thus been made to use additional clinical, radiographic or mechanical factors to carefully select patients who would benefit from the joint preserving surgery (Trousdale and Cabanela Citation2003). Mechanical parameters have also been used in the preoperative planning, in order to determine the optimal degree of correction in different planes and to achieve the subtle balance between improvement of femoral coverage and restriction of range of motion (Srakar et al. Citation1992, Iglič et al.Citation1993b, Hipp et al. Citation1999, Mechlenburg et al. Citation2004).
We evaluated long-term outcome retrospectively in patients with hip dysplasia who had under-gone the Bernese periacetabular osteotomy at the authors’institution. We also investigated preoperative clinical, radiographic and mechanical factors (resultant hip force, contact hip stress) that might help to predict the outcome.
Patients and methods
Study sample
55 consecutive adult patients with residual dysplasia of the acetabulum were treated with the Bernese periacetabular osteotomy at our hospital from 1987 through 1995. In the years 2002–2003, all the patients were invited to participate in a follow-up study and 35 patients responded. Preoperative radiographs were missing for 9 respondents and these patients were excluded from the study. In the excluded group, there were 2 cases of conversion to total hip arthroplasty; the other hips showed no or moderate arthrosis progression. The remaining 26 patients (26 hips)—our study sample—included 22 women and 4 men with a mean age of 34 (18–50) years at the time of the operation. In all 26 hips, the preoperative diagnosis was developmental dysplasia of the hip. The osteotomies were performed by three surgeons. None of the patients had bilateral osteotomy. 4 patients were treated with the Bernese osteotomy on one side and the Chiari osteotomy on the other side, but we included only hips with the Bernese periacetabular osteotomy in the study.
Surgical technique
All operations were performed under epidural anesthesia. In most patients, the epidural catheter was introduced and left in place for 24–48 h postoperatively. Patients were mobilized on the third postoperative day with partial weight bearing (10–20 kg) and the use of crutches. Full weight bearing was allowed after 8–10 weeks. Perioperative antibiotic prophylaxis was used in 5 patients, postoperative indomethacine prophylaxis against heterotropic ossification was used in 10 patients, and postoperative antithrombotic prophylaxis was used in 13 patients.
Clinical, radiographic and mechanical evaluation
The mean follow-up time was 12 (7–15) years. Clinical outcome at follow-up was evaluated with the WOMAC Osteoarthritis Index, with 0 signifying a worst result and 96 a best result (Bellamy et al. Citation1988), and the preoperative values were evaluated retrospectively by the patients. Registered license for use of the original validated version of WOMAC3.1 in the Slovenian language was obtained for this study. We analyzed a set of 5 radiographs for each patient: 3 anterior-posterior (AP) pelvic radiographs (the last preoperative, the first postoperative, and the most recent radiograph at follow-up), and two false profile radiographs (the last preoperative and the first postoperative). The presence and/or progression of hip arthrosis was assessed preoperatively and at follow-up according to the Tönnis (Citation1987) classification, which identifies 4 grades: 0 = no signs of osteoarthritis; 1 = increased sclerosis, slight narrowing of the joint space, no or slight loss of head sphericity; 2 = small cysts, moderate narrowing of the joint space, moderate loss of head sphericity; 3 = large cysts, severe narrowing or obliteration of the joint space, severe deformity of the head. The parameters, measured on preoperative and postoperative AP radiographs, included the lateral center-edge angle of Wiberg and two mechanical parameters: the resultant hip force and the peak stress on the weight-bearing surface. The vertical-center-anterior VCA angle (Lequesne and de Sèze Citation1961) was measured on the preoperative and postoperative false profile radiographs.
The mechanical parameters were estimated from AP pelvic radiographs with a previously developed analytical three-dimensional model (Igličet al. Citation1993a, Citationb, Ipaveč et al. Citation1999, Mavčič et al. Citation2002) that corresponds to the static one-legged stance. The one-legged stance is considered to be the representative position for slow gait, as the most frequent activity in everyday life (McLeish and Charnley Citation1970). The following were measured manually on the AP radiographs (Mavčič et al. Citation2002): the inter-hip distance (l), the pelvic height (H), the pelvic width laterally from the center of the femoral head (C), the coordinates of the insertion point of abductors on the greater trochanter (point coordinates Tx, Tz) in the frontal plane, the average of acetabular and femoral head radius (r) and the Wiberg lateral center-edge angle. The three-dimensional reference coordinates of the muscle attachment points were taken from the paper of Dostal and Andrews (Citation1981), and they were adjusted by linear scaling with regard to the radiographic pelvic parameters for each individual hip. The solution of the vector equations for the equilibria of forces and torques yielded the three components of the resultant hip force (R) and the tensions in the abductor muscles. We computed the peak stress on the weight-bearing surface for every individual hip from known values of the femoral head radius (r), the Wiberg lateral center-edge angle and the resultant hip force, R (Igličet al. Citation1993b, Ipavec et al. Citation1999). The resultant hip force (R), and the peak contact hip stress, pmax, were normalized to the body weight (WB) of each subject (R/WBand pmax/WB), since due to the retrospective nature of the study, the past values of patients’body weights were not available in most cases. Nevertheless, the normalized stress pmax/ WBhas already been acknowledged as the relevant mechanical parameter in previous studies (Brinckmann et al. Citation1981). In radiographic measurements, a uniform magnification factor of 10% was taken into account.
Statistics
We used paired t-test for statistical evaluation of the changes in WOMAC score, the lateral center-edge angle, the vertical center-anterior angle, the normalized resultant hip force and the normalized peak stress. Beforehand, Q-Q plots (with Blom's proportional estimation formula and assigning the mean to ties) were performed for preoperative and postoperative/follow-up values of each parameter, and all data groups were found to correspond sufficiently to the normal distribution.
Results
4 of the hips required conversion to total hip arthroplasty after a mean of 4.5 (2–7) years; all 4 hips had preoperative Tönnis grade 2 or 3. At the time of the index operation, 13 hips had no radio-graphic signs of arthrosis and none of these hips required subsequent total hip arthroplasty.
The mean preoperative combined WOMAC score was 66 (96 best), including scores for pain 12 (20 best), stiffness 6 (8 best) and functionality 48 (68 best). The corresponding mean WOMAC score for hips without total hip arthroplasty at follow-up was 63 (12 + 5 + 45) and the change was not statistically significant (p = 0.5).
The osteotomy improved the mean Wiberg lateral center-edge angle from 15° (7–26) preoperatively to 37° (20–68) postoperatively (p < 0.001).
The vertical center-anterior angle of Lequesne and de Sèze (VCA) increased from a preoperative mean of 22° (5–40) to a postoperative mean of 38° (21–56) (p = 0.01). The mean postoperative shift in the center of rotation in the lateral direction was 5 mm (range from medial –14 mm to lateral +22 mm). The mean value of the resultant hip force normalized to the body weight, R/WB, increased from 2.9 (2.5–3.6) preoperatively to 3.3 (2.6–4.1) postoperatively (p < 0.001). The mean value of the peak contact stress normalized to the body weight, pmax/WB, became reduced from 5.2 (2.2–9.6) kPa/N preoperatively to 3.0 (1.9–5.6) kPa/N postoperatively (p < 0.001).
Surgical complications included wound hematoma in 1 hip, and fracture of the acetabulum in 1 hip. There were no postoperative infections or neurological complications. The mean perioperative blood loss was 1.4 (0.3–0.4) L. Pulmonary embolism was diagnosed 14 days after the operation in a 31-year-old female patient who had not received antithrombotic prophylaxis due to the absence of major preoperative risk factors (young age, non-smoker, and no hormonal medications). Anticoagulant therapy was introduced promptly and the patient recovered fully without any sequelae. In 9 patients, the osteosynthetic material was removed 1–3 years after the index operation and 1 patient required removal of periacetabular ossification 3 years after the osteotomy.
In order to clarify the prognostic value of radio-graphic and mechanical parameters, the subjects were stratified in 3 groups according to the clinical outcome: A. patients who required conversion to total hip arthroplasty, B. patients with progression of arthrosis to grade 3 or a reduction in WOMAC score of more than 20 points, and C. the other patients. We found that the average pmax/WB was significantly reduced after the Bernese periacetabular osteotomy in all 3 groups, but the long-term clinical outcome was better in hips with lower preoperative Tönnis grade and lower postoperative pmax/WB ().
Clinical, radiographic and mechanical results for the 26 hips, stratified into 3 subgroups according to clinical outcome
Discussion
The periacetabular osteotomy improved the lateral and anterior coverage of the femoral head and accordingly reduced the normalized peak contact stress in all hips studied. The mechanical results are consistent with previous studies showing contact pressure elevation in dysplastic hips (Hadley et al. Citation1990, Mavčič et al. Citation2002) and contact pressure reduction by simulated acetabular reorientation (Genda et al. Citation1995, Hipp et al. Citation1999). In most cases, the postoperative values were reduced to the level observed in healthy adult hips (Mavčič et al. Citation2004). Although the Bernese periacetabular osteotomy allows medialization of the hip joint in addition to improvement of lateral and anterior coverage (Crockarell et al. Citation1999), most of the hips studied showed lateralization of the center of rotation on the postoperative AP radiographs. Accordingly, the magnitude of the resultant hip force increased in all stratification groups, which is consistent with theoretical predictions of the relationship between the center of rotation and the resultant hip force (). Our clinical results have thus confirmed theoretical predictions (Iglič et al. Citation1993b) that the resultant hip force itself is not an adequate biomechanical parameter for preoperative planning, and that rotational osteotomy can effectively reduce the contact hip stress although the resultant hip force may be slightly increased.
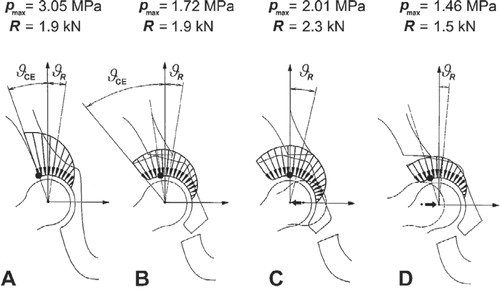
Simulation of the contact stress distribution in the hip joint before and after a periacetabular osteotomy in a single patient. In dysplastic hip, the contact stress increases drastically towards the lateral edge where the peak of the contact stress is located (A). Increase in lateral center-edge angle reduces the magnitude and shifts the location of the peak contact stress, even if the resultant hip force remains unchanged (B). Lateralization or medialization of the periacetabular fragment increases or reduces the peak contact stress due to the change in magnitude/direction of the resultant hip force, even if the lateral center-edge angle is the same (C and D). The location of the peak stress, pmax, on the weight bearing surface is marked with a dot. R denotes the resultant hip force, ϑCEis the lateral center-edge angle of Wiberg, and ϑRis the vertical inclination of the resultant hip force (adapted from Srakar et al. Citation1992, Iglic et al. Citation1993b).
The differences between stratification groups in R/WBand pmax/WBare consistent with the theoretical prediction that increased anterior and lateral femoral coverage and reduced contact hip stress prevent or delay the progression of arthrosis. Hips that later required arthroplasty had less favorable correction of the lateral coverage (CE), anterior (VCA) coverage and smaller operative reduction of the normalized peak contact stress. The 4 hips that later required arthroplasty had considerably higher values of postoperative peak contact stress when compared to the 8 hips with advanced arthrosis, although the postoperative value of CE was similar in both groups. The preoperative WOMAC score and the preoperative Tönnis grade were also important factors for prediction of the outcome. Preoperatively, the group of 4 hips with later arthroplasty already had a mean WOMAC score of 50 and Tönnis grade 2 or 3, while the other 22 patients initially reported scores close to 70 and had Tönnis grades of 0 or 1. In the course of more than 7 years of follow-up, the WOMAC scores have halved in most of the patients with initial Tönnis grade 1, while most of the hips with initial Tönnis grade 0 reported no significant clinical worsening and were eventually classified among the 14 hips with no or mild arthrosis progression. These results correspond well to the degree of patient satisfaction with the index operation. However, radiographic progression of arthrosis for approximately one grade occurred in all groups, and longer follow-up would probably have shown some degree of clinical deterioration in the 14 successful hips also. The average age at operation in patients with no or moderate arthrosis progression was considerably lower than in the other groups, but larger patient series will be required in order to determine whether age is indeed an independent risk factor or it is merely associated with advanced arthrosis.
Previous follow-up studies of the Bernese periacetabular osteotomy have shown results similar to ours. A follow-up study of at least 2 years in 100 hips reported failure in 17 hips, most of which had preoperative arthrosis of grade 2 or 3, and the few failures in grade 0 hips were due to insufficient correction or complications (e.g. nonunion, impingement) (Trumble et al. Citation1999). In a 2–7-year follow-up study, some patients with grade 2 and most patients with preoperative grade 3 arthrosis were converted to total hip arthroplasty, while the remaining patients had stable radiographic status and improved clinical status (Crockarell et al. Citation1999, Murphy et al. Citation1999). Our findings do not corroborate other studies which have reported that after periacetabular osteotomy, radiographic expression of joint degeneration may improve for grade 1 or grade 2 hips (Dagher et al. Citation2003) and that even some dysplastic hips with grade 3 arthrosis may show good clinical results (Murphy and Desmukh Citation2002). It should be noted, however, that in these studies inclusion criteria included sufficient joint congruity on anterior-posterior pelvic radiographs with maximum hip abduction and on false profile views with hip flexion. Some authors have pointed out that hips with asphericity should not be corrected surgically by rotational osteotomy and have the highest risk of failure, irrespective of the degree of arthrosis (Schramm et al. Citation1999).
The average blood loss in our study group was high, and highest in the first patients. None of the operations were performed with hypotensive epidural anesthesia and antifibrinolytic agents (tranexamic acid) were not available at the time. The introduction of these methods in recent years has resulted in a considerable reduction of blood loss (Søballe Citation2003).
Our study has several potential limitations. The main limitation is the small number of hips studied (26) and the small number of conversions to total hip arthroplasty (4). We could not analyze the predictive value of preoperative CT or MRI, since these two imaging techniques were not used in our institution before 1995. The preoperative WOMAC scores were reported by the patients retrospectively. The relatively simple biomechanical model enabled evaluation of peak stress in one static body position only, and did not permit comparison of kinetic and kinematic parameters. Nevertheless, some authors have argued that contact hip stresses for similar but different activities from the midstance of gait can be predicted from linear regression equations (Hipp et al. Citation1999). In our model the femoral head was considered to be a perfect sphere, which may correspond to Tönnis grade 0 and grade 1 hips. However, dysplastic hips in advanced stages of arthrosis have incongruent femoral heads with reduced joint space width, which leads to radio-graphic overestimation of the femoral head radius and the Wiberg lateral center-edge angle, and therefore results in underestimation of the peak contact stress. It is therefore reasonable to expect that incorporation of joint congruity assessment in the mechanical model would result in even higher values of peak contact hip stress in dysplastic hips and thus improve the predictive value of these mechanical parameters. Nevertheless, considering that most adult body weight values lie between 500 and 1,500 N, the results of the estimated peak contact hip stress in our study (range of the normalized values 2.2–9.6 kPa/N preoperatively and 1.9–5.6 kPa/N postoperatively) lie within an order of magnitude of the peak contact hip stress measured with an instrumented partial hip endoprosthesis in vivo (6.7 MPa), estimated with cadaveric specimens in vitro (7.7–8.8 MPa), or computed with the finite element models (Hodge et al. Citation1986, von Eisenhart-Rothe et al. Citation1999, Brand et al. Citation2001).
Our findings are consistent with the hypothesis that long-lasting high contact stress results in early hip arthrosis (Ganz et al. Citation1988). Achievement of the main goal of the operation—reduction of contact stress—which was based on this hypothesis has been shown quantitatively here. This indicates that peak contact hip stress postoperatively may be a better predictive factor of clinical outcome than the lateral center-edge angle alone, and may be a useful tool for improvement of surgical planning.
The authors are grateful to the senior orthopedic surgeons France Vrevc and the late Prof. France Srakar for help, teaching and guidance.
No competing interests declared.
- Bellamy N, Buchanan W W, Goldsmith C H, Campbell J, Stitt L W. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol 1988; 15: 1833–40
- Brand R A, Iglič A, Kralj-Iglič V. Contact stress in the human hip, implications for disease and treatment. Hip Int 2001; 11: 117–26
- Brinckmann P, Frobin W, Hierholzer E. Stress on the articular surface of the hip joint in healthy adults and person with idiopathic osteoarthrosis of the hip joint. J Biomech 1981; 14: 149–56
- Chiari K. Medial displacement osteotomy of the pelvis. Clin Orthop 1974; 98: 55–71
- Crockarell J, Jr, Trousdale R T, Cabanela M E, Berry D J. Early experience and results with the periacetabular osteotomy. The Mayo Clinic experience. Clin Orthop 1999, 363: 45–53
- Dagher F, Ghanem I, Abiad R, Haykal G, Kharrat K, Phares A. Bernese periacetabular osteotomy for the treatment of the degenerative dysplasic hip. Rev Chir Orthop Reparatrice Appar Mot 2003; 89: 125–33
- Dostal W F, Andrews J G. A three-dimensional biomechanical model of hip musculature. J Biomech 1981; 14: 803–12
- Ganz R, Klaue K, Vinh T S, Mast J W. A new periacetabular osteotomy for the treatment of hip dysplasia. Technique and preliminary results. Clin Orthop 1988, 232: 26–36
- Genda E, Konishi N, Hasegawa Y, Miura T. A computer simulation study of normal and abnormal hip joint contact pressure. Arch Orthop Trauma Surg 1995; 114: 202–6
- Hadley N A, Brown T D, Weinstein S L. The effects of contact pressure elevations and aseptic necrosis on the long-term outcome of congenital hip dislocation. J Orthop Res 1990; 8: 504–13
- Hipp J A, Sugano N, Millis M B, Murphy S B. Planning acetabular redirection osteotomies based on joint contact pressures. Clin Orthop 1999, 364: 134–43
- Hodge W A, Fijan R S, Carlson C E, Burgess R G, Harris W H, Mann R W. Contact pressures in the human hip joint measured in vivo. Proc Natl Acad Sci USA 1986; 83: 2879–83
- Iglič A, Srakar F, Antolič V. Influence of the pelvic shape on the biomechanical status of the hip. Clin Biomech 1993a; 8: 223–4
- Iglič A, Kralj-Iglič V, Antolič V, Srakar F, Stanič U. Effect of the periacetabular osteotomy on the stress on the human hip joint articular surgace. IEEE Trans Rehab Engr 1993b; 1: 207–12
- Ipaveč M, Brand R A, Pedersen D R, Mavčič B, Kralj-Iglič V, Iglič A. Mathematical modelling of stress in the hip during gait. J Biomech 1999; 32: 1229–35
- LeCoeur P. Corrections des défauts d’orientation de l’articulation coxofémorale par ostéotomie de l’isthme iliaque. Rev Chir Orthop 1965; 51: 211–2
- Lequesne M, de Sèze S. Le faux profil du bassin: Nouvelle incidence radiographique pour l’étude de la hanche: Son utilité dans les dysplasies et les différentes coxopathies. Rev Rhum Mal Osteoartic 1961; 28: 643–52
- Mavčič B, Pompe B, Antolič V, Daniel M, Iglič A, Kralj-Iglič V. Mathematical estimation of stress distribution in normal and dysplastic human hips. J Orthop Res 2002; 20: 1025–30
- Mavčič B, Slivnik T, Antolič V, Iglič A, Kralj-Iglič V. Hip contact stress is related to the development of hip pathology with increasing age. Clin Biomech 2004; 19: 939–43
- Maxian T A, Brown T D, Weinstein S L. Chronic stress tolerance levels for human articular cartilage: two nonuniform contact models applied to long term follow up of CDH. J Biomech 1995; 28: 159–66
- McLeish R D, Charnley J. Abduction forces in the one-legged stance. J Biomech 1970; 3: 191–209
- Mechlenburg I, Nyengaard J R, Romer L, Soballe K. Changes in load-bearing area after Ganz periacetabular osteotomy evaluated by multislice CT scanning and stereology. Acta Orthop Scand 2004; 75: 147–53
- Michaeli D A, Murphy S B, Hipp J A. Comparison of predicted and measured contact pressures in normal and dysplastic hips. Med Eng Phys 1997; 19: 180–6
- Murphy S B, Ganz R, Muller M E. The prognosis in untreated dysplasia of the hip. A study of radiographic factors that predict the outcome. J Bone Joint Surg (Am) 1995; 77: 985–9
- Murphy S B, Millis M B, Hall J E. Surgical correction of acetabular dysplasia in the adult. A Boston experience. Clin Orthop 1999, 363: 38–44
- Murphy S, Deshmukh R. Periacetabular osteotomy: preoperative radiographic predictors of outcome. Clin Orthop 2002, 405: 168–74
- Salter R B. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg (Br) 1961; 43: 518–39
- Schramm M, Pitto R P, Bar K, Meyer M, Rohm E, Hohmann D. Prophylaxis of secondary osteoarthrosis with spherical osteotomy in residual acetabular dysplasia. Analysis of predictive factors of success. Arch Orthop Trauma Surg 1999; 119: 418–22
- Søballe K. Pelvic osteotomy for acetabular dysplasia. Acta Orthop Scand 2003; 74: 117–8
- Srakar F, Iglič A, Antolič V, Herman S. Computer simulation of the periacetabular osteotomy. Acta Orthop Scand 1992; 63: 411–2
- Tönnis D. Eine neue Form der Hüftpfannenschwenkung durch Dreifachosteotomie zur Ermöglichung späterer Hüftprothesenversorgung. Orthop Praxis 1979; 15: 1003–5
- Tönnis D. Congenital dysplasia and dislocation of the hip in children and adults. Springer, New York 1987
- Trousdale R T, Cabanela M E. Lessons learned after more than 250 periacetabular osteotomies. Acta Orthop Scand 2003; 74: 119–26
- Trumble S J, Mayo K A, Mast J W. The periacetabular osteotomy. Minimum 2 year followup in more than 100 hips. Clin Orthop 1999, 363: 54–63
- Weinstein S L. Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop 1987, 225: 62–76
- von Eisenhart-Rothe R, Witte H, Steinlechner M, Muller-Gerbl M, Putz R, Eckstein F. Quantitative Bestimmung der Druckverteilung im Hüftgelenk während des Gangzyklus. Unfallchirurg 1999; 102: 625–31