Abstract
Background Diagnostics of intraarticular lesions is important in the treatment of traumatic anterior shoulder instability.
Patients and methods We studied 30 patients: 26 men and 4 women. For all patients preoperative examinations involved arthrography, CT arthrography, MR arthrography, and 3D-CT.
Results The articular capsule adhered to the margin of the glenoid in only 3 cases. In the remaining 27 patients, the joint capsule was detached, showing medial translation. Hill-Sachs lesions were present in 24 cases. Bankart lesions were detected in all cases, and they extended over 2–5 h. Osseous Bankart lesions were detected in 13 cases. MR arthrography revealed the articular labrum in all cases, but AIGHL in only 16 cases. Bankart lesions were found in all cases. When the patients were divided according to the frequency of dislocation, there was a correlation between both distance of the detached joint capsule and visualization of AIGHL and the frequency of dislocation.
Interpretation From this study, the frequency of dislocation was higher in the patients with severe detachment of the joint capsule, in whom AIGHL could not be visualized by MR arthrography.
▪
The inferior glenohumeral ligament (IGHL), anterior glenoid labrum damage and osseous lesions of the anteroinferior margin of the glenoid play an important role in traumatic anterior shoulder instability. We employed parallel imaging methods for the preoperative evaluation of intraarticular lesions in patients with traumatic anterior shoulder instability. Currently, there is no concensus as to which parameters correlate with the frequency of shoulder dislocation. In this study, we assessed intraarticular lesions by several diagnostic imaging modalities.
Patients and methods
We studied 30 patients (26 men) who had been treated by the arthroscopic Bankart procedure using suture anchors for anterior shoulder instability after an injury (in 25 cases, a sports injury). Mean age at the time of the surgery was 28 (16–39) years.
Of the 30 patients, 5 had a single dislocation but no subsequent signs of subluxation, 10 patients had signs of subluxation but no verified dislocation, and 15 patients with a combination of dislocation and subluxation had an episode of instability before the surgery. Cases in which self-reduction was possible were defined as having subluxation. 10 patients had only subluxations (group A), 11 patients had one or two dislocations (group B), and 9 patients had three or more dislocations (group C). Mean numbers of dislocations were 5 (2–9) in the patients with dislocation alone, and 3 (1–10) in those with a combination of dislocation and sub-luxation.
All patients had a positive anterior apprehension test and the relocation test, but none showed multidirectional instability. The diagnostic imaging procedures for the assessment of intraarticular lesions for all patients included arthrography, CT arthrography (CTA), MR arthrography (MRA), and 3-dimensional CT (3D-CT). The evaluation included 6 parameters: objective evaluation of the glenohumeral ligaments according to the classification established by Hara et al. (Citation1990), the site of the attachment of the anterior part of joint capsule, presence/absence of Hill-Sachs lesions, presence/absence and the range of Bankart lesions, presence/absence of bony Bankart lesions on the anterior margin of the glenoid, and the visualization or non-visualization of the anterior inferior glenohumeral ligament (AIGHL). We compared the involvement of the present findings in the diagnostic imaging studies with the severity of the instability. Statistical analysis between the frequency of dislocation and the 5 parameters evaluated by diagnostic imaging, except the objective evaluation of the glenohumeral ligaments, was done using Welch's t-test or Fisher's exact probability test with a level of significance of less than 0.05.
Results
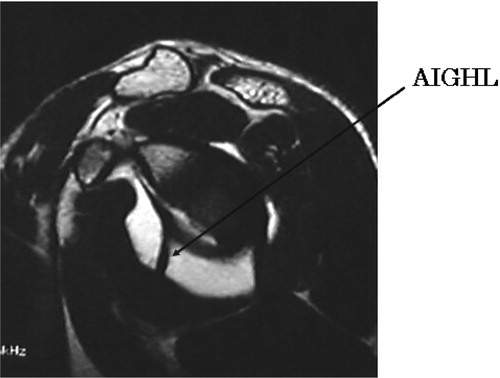
Objective evaluation of the AIGHL according to Hara's classification () revealed that the AIGHL could be visualized obscurely in 27 of the 30 patients, consisting of 14 patients with type III and 13 patients with type IV. Type I, corresponding to normal findings—no loosening of the AIGHL—was found in 1 patient. As for the site of the attachment of the anterior part of the joint capsule, which was determined by CTA, only 3 patients showed type I findings according to Rothman's (Citation1975) classification (which indicated attachment to the anterior margin of the glenoid). In the remaining 27 patients, the joint capsule was detached, showing medial translation by 4.6 (1–11) mm (). The mean rate of this medial translation to the transverse diameter of the scapular glenoid was 0.35 (0–1). The rate was 1.0 in 2 patients, and all of them had had dislocation at least 4 times. Bankart lesions were found in all 30 patients; they covered mean 3.3 (2–5) h on the right side, and 3.4 (2–4) h on the left side. The lesions were located at the 3–5 o'clock position on the right side and at the 7–9 o'clock position on the left side in 28 of the 30 patients. On the other hand, bony Bankart lesions were found in only 13 of the 30 patients, including those in whom the lesions could be identified by 3D-CT, although they could scarcely be identified by plain radiographs and CTA. Hill-Sachs lesions were found in 24 of the 30 patients, although 25% or greater invasion of the bone was not found in any of the patients. shows the AIGHL as visualized in an oblique sagittal section of MRA. It could be identified before the surgery in only 16 patients.
Figure 1. Objective evaluation of the glenohumeral ligament. The tension of the anterior inferior glenohumeral ligament (AIGHL) and medial glenohumeral ligament was evaluated from the internal rotation position to the neutral position of the shoulder. Type III and type IV indicate loosening of the AIGHL. The hollows in the arthrography suggest the tension of the glenohumeral ligament.
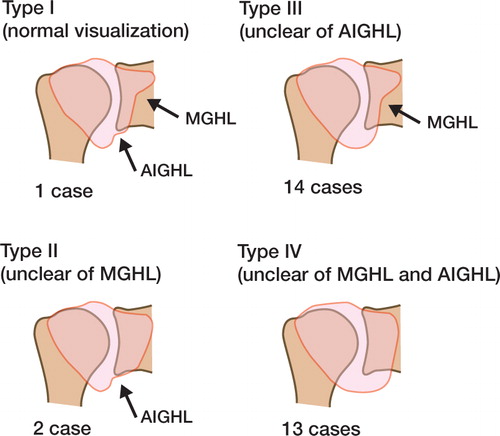
Figure 2. Evaluation of the site of attachment of the joint capsule: The joint capsule is attached to the glenoid labrum, as shown in type 1, in the normal condition. Three types have been described according to the degree of detachment of the joint capsule.
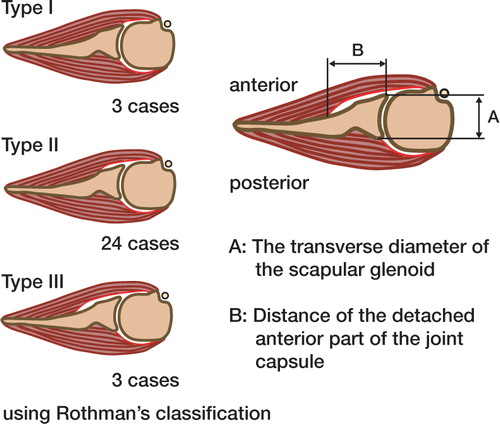
Figure 3. MRA, oblique sagittal section (with visualization of the AIGHL).
AIGHL was identified by arthroscopy in all of the patients. Bankart lesions were found in all patients. All patients showed fibrillation of the articular cartilage on the anterior margin of the glenoid; this was located at the 3–4 o'clock position on the right side and at the 8–9 o'clock position on the left side. However, the type IV SLAP lesion, which was found in 2 patients during the surgery, could not be evaluated by preoperative diagnostic imaging.
Discussion
Various factors are of importance for static stabilization of the glenohumeral joint: articular congruency (the relationship between the angle of inclination of the glenoid and the angle of retroversion of the humeral head), negative intraarticular pressure, the ligaments and joint capsule (glenohumeral ligaments or coracohumeral ligament), and the glenoid labrum. The incidence of Bankart lesions in traumatic anterior shoulder instability has been reported to be 98% by Field et al. (Citation1995) and 87% by Altchek et al. (Citation1993). The incidence of bony Bankart lesions has been reported to be 20% by MacDonald (Citation1962), and the incidence of Hill-Sachs lesions has been reported to be 77% by Pavlov et al. (Citation1985) and 82% by Adams (Citation1948). In the present study, however, the incidences of all of these lesions were equal to those reported by the above authors or higher.
As for the pathology of the glenoid labrum-AIGHL complex, which has been recognized in recent years to be important, various reports have been published. For example, Uhtoff et al. (Citation1985) reported that the joint capsule was derived from the neck of the scapula, and not from the glenoid labrum, in one-fifth of the cases autopsied in their study; Rowe et al. (Citation1961) reported that Hill-Sachs lesions were not involved in anterior instability of the shoulder if the anterior soft tissue integrity was maintained; Townley (Citation1950) and Speer et al. (Citation1994) reported that instability is not induced by resection of the glenoid labrum alone or detachment from the glenoid alone; Schwartz et al. (Citation1988) emphasized the high probability of the ligament being involved in the instability, because instability can be induced by excision of the AIGHL alone. In our study, the AIGHL was visualized in all shoulders, but the ligament was visualized obscurely even by arthrography in at least 90% of the shoulders, suggesting loosening of the AIGHL.
We also compared the findings of the diagnostic imaging studies with the severity of the instability. In , a statistical analysis between the frequency of dislocation and the five parameters evaluated by diagnostic imaging is shown. The patients were divided according to the frequency of dislocation into group A in which the frequency was 0, group B in which the frequency was 1 or 2, and group C in which the frequency was 3 or more. Two parameters, namely, the distance of the detached joint capsule and the presence/absence of visualization of the AIGHL, showed a correlation with the frequency of dislocation (). The results indicate that the patients with marked detachment of the joint capsule, in which the AIGHL was scarcely visualized by MRA, tended to have an increased frequency of dislocation. In some cases, patients with a traumatic dislocation of the shoulder also had pathological alterations in the glenohumeral joint, similarly to those with no history of complete dislocation, but instability of the shoulder. It remains unclear whether the pathological imaging findings are a cause or an effect of the severity of the instability.
Table 1. Correlations between the frequency of dislocation and the presence of various intraarticular lesions
Table 2. Statistical analysis of data between the groups
- Adams J C. Recurrent dislocation of the shoulder. J Bone Joint Surg (Br) 1948; 30: 26–38
- Altchek D W, Dines D M. The surgical treatment of anterior instability: selective capsular repair. Oper Tech Sports Med 1993; 1: 285–92
- Field L D, Warren R F, O'Brien S J, Aitchek D W, Wickiewicz T L. Isolated closure of rotator interval defects for shoulder instability. J Sports Med 1995; 23: 557–63
- Hara M, Takeshita M, Midorikawa K, Iwamoto H, Takagishi N. A study of shoulder joint anterior capsular mechanism arthrographically. The Shoulder Joint 1990; 14: 236–9, (in Japanese)
- MacDonald F R. Intra-articular fractures in recurrent dislocation of the shoulder. J Can Assoc Radiol 1962; 13: 1–8
- Pavlov H, Warren R F, Weiss C B, Jr, Dines D M. The roentgenographic evaluation of anterior shoulder instability. Clin Orthop 1985, 194: 153–8
- Rothman R H. Anatomical consideration in glenohumeral joint. Orthop Clin North Am 1975; 6: 341–52
- Rowe C R, Sakellarides H T. Factors related to recurrence of anterior dislocations of the shoulder. Cin Orthop 1961, 20: 40–8
- Schwartz R E, O'Brien S J, Warren R F, Torzilli P A. Capsular restraints to anterior-posterior motion of the shoulder. Orthop Trans 1988; 12: 727
- Speer K P, Deng X, Borrero S, Torzilli P A, Altchek D A, Warren R F. Biomechanical evaluation of a simulated Bankart lesion. J Bone Joint Surg (Am) 1994; 76: 1819–26
- Townley C O. The capsular mechanism in recurrent dislocation of the shoulder. J Bone Joint Surg (Am) 1950; 32: 370–80
- Uhtoff H K, Piscopo M. Anterior capsular redundancy of the shoulder. Congenital or traumatic? An embryological study. J Bone Joint Surg (Am) 1985; 67: 363–6