Abstract
Background The Weber operation is an anatomical reconstruction of the anterior talofibular ligament with the plantaris tendon. Few long-term studies have been published.
Methods We evaluated 40 ankles in 37 patients (19 women) at an average of 24 years after the procedure.
Results At follow-up, symptoms were present to vary-ing degrees in half of the ankles, but 32 patients were satisfied with the result and approximately two-thirds of the patients had a good or excellent result with the Karlsson and Good scores. Only 3 ankles had secondary arthrotic changes with narrowing (2 patients) or disap-pearance (1 patient) of the joint space.
Interpretation We conclude that the Weber pro-cedure is a good alternative for treatment of chronic anterolateral ankle instability when a direct anatomical reconstruction is not feasible, or has failed.
▪
After nonoperative treatment, residual instability of the ankle occurs in approximately 10–20% of the patients after an injury of the anterior talofibu-lar ligament (ATFL) sometimes combined with a rupture of the calcaneofibular ligament (Kerkhoffs et al. Citation2002). Symptomatic instability persisting for more than 6 months is referred to as chronic ankle instability (Karlsson et al. Citation1997). When stability does not improve, operative treatment is consid-ered.
Reconstruction of the anterolateral ankle liga-ments can be divided in two groups: (1) non-anatomical reconstructions, in which a functional reconstruction is created, usually with the peroneus brevis tendon, and (2) anatomical reconstructions in which the remains of the ligaments themselves are sutured or re-attached to the fibula (Elmslie Citation1934, Evans Citation1953, Broström Citation1966, Chrisman and Snook Citation1969, Bouretz and Duquennoy Citation1975, Watson-Jones Citation1976, Karlsson and Langsinger Citation1992).
In 1969, Weber described a technique using the plantaris tendon for reconstruction of the anterior talofibular ligament () (Weber Citation1966, Weber and Hupfauer Citation1969). Although a tendon graft is used, the Weber procedure approaches the idea of an anatomical reconstruction of the ATFL, since the graft is attached to the original sites of origin and insertion of the ATFL.
Figure 1. Proximal identification of the plantaris tendon medial to the aponeurosis of the gastrocnemius.
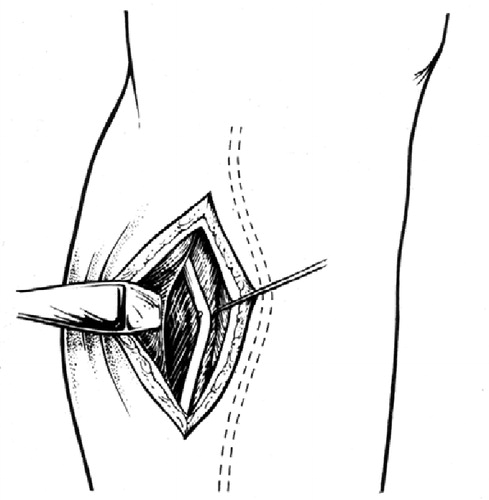
Figure 2. Drill holes are made in the distal fibula (2×) and the talus.
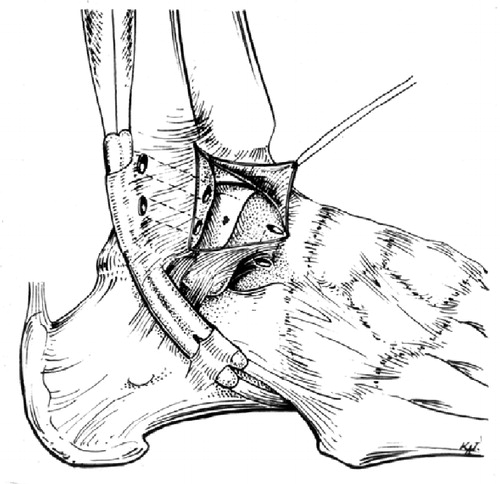
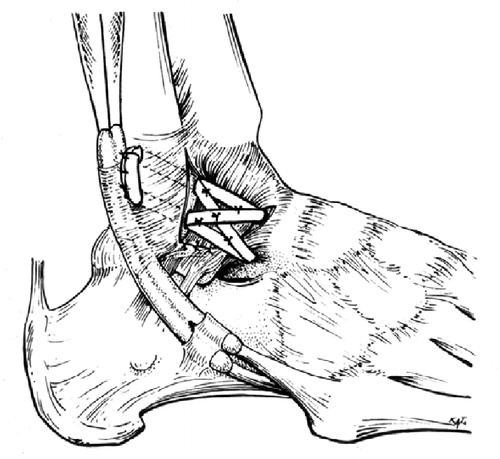
Figure 3. The plantaris tendon is pulled through the drill holes, once or twice in a figure-of-eight and once in a circular configuration. To stimulate the vascularization of the free transplant, the remaining anterolateral ligaments and capsule are integrated into the reconstruction.
We evaluated the long-term results of the Weber procedure retrospectively in patients with chronic ankle instability.
Patients and methods
Study design
We performed a retrospective survey of all patients operated on by means of the Weber procedure between 1974 and 1982. All patients were operated by one of the 2 senior authors (ER, RM). The med-ical ethics committee of the hospital approved the study. Evaluation took place between April 2002 and January 2003. Short-term results of largely the same group of patients have been reported by Marti et al. (Citation1977), and later by Raaymakers et al. (Citation1983).
Patients
Between 1974 and 1982, 62 patients (65 ankles) suf-fering from chronic ankle instability with increased laxity of the anterolateral ankle ligaments were operated on. The mean age was 26 (13–57) years at the time of surgery. 30 patients were female and 32 were male. 58 of the 62 patients were sports participants, including international soccer players and ballet dancers.
40 ankles in 37 patients could be reviewed. 4 of these patients did not permit radiographic evalua-tion and 2 patients were interviewed by telephone alone. Of the 25 patients who were lost to follow-up, 4 patients had moved abroad, 2 patients had died and 3 patients were too ill (due to other condi-tions) to come to the hospital for follow-up or to answer questions by telephone. 16 patients could not be traced.
The group of 37 patients that was evaluated con-sisted of 18 male and 19 female patients with 19 right-ankle injuries and 21 left-ankle injuries. The mean duration of complaints before surgery was 4 (0.5–22) years. The average follow-up period was 24 (20–29) years. Mean age at follow-up was 50 (38–73) years.
Surgical technique () (Weber Citation1966, Weber and Hupfauer Citation1969, Magerl and Marti Citation1978)
The plantaris tendon was used, if present. In the early years of this study, the tendon was first identified through an incision near its insertion onto the calcaneus. When present, a second incision was made medial to the gastrocnemius aponeurosis near the junction between the tendon and the muscle. A tendon stripper was inserted distally and advanced upwards to free the tendon from its environment and transect it proximally. Later on in this series, the tendon was first approached through the proximal incision. This modification was made because proximally, its presence is assessed more accurately. Distal fusion with the Achilles tendon sometimes makes the plantaris tendon wrongfully judged to be absent. With the development of a new plantaris tendon stripper including small scissors at the tip, a distal incision was not necessary.
If the plantaris tendon was absent (2 patients), we used the proximal part of the extensor tendon of the third toe. A small distal transverse incision on the dorsum of the foot was made and the third extensor tendon was identified. Through a proxi-mal incision, the extensor tendon was identified at the muscle-tendon junction. The stripper was inserted distally and the tendon cut proximally. In order to protect the surrounding structures on the dorsal side of the foot, we made one or two addi-tional small transverse incisions between the prox-imal and distal incision to guide the stripper safely upwards. To preserve extension of the third toe, the remaining distal extensor tendon was sutured to the extensor tendon of the fourth toe.
Thus, a sufficiently long (plantaris tendon: approximately 30 cm, extensor tendon: approxi-mately 15 cm), strong and nonelastic transplant was easily obtained. The tendon graft was pulled 2 or 3 times through drill holes in the talar neck and distal fibula for 1 or 2 figures-of-eight and one circular configuration, and was finally sutured to itself. To stimulate the vascularization of the free transplant, the remaining anterolateral ligaments and capsule were additionally integrated into the reconstruction, as described earlier (Magerl and Marti Citation1978).
Up to the fifth postoperative day, the ankle was immobilized in a stirrup plaster splint. Afterwards, the patient was allowed to exercise dorsal and plan-tar fiexion. Then a below-the-knee walking cast was applied for an additional 6–8 weeks.
Outcome assessment
We used the following outcome measures for long-term evaluation: Subjective. 1. Instability (yes/no), 2. Persistent pain (yes/no), 3. Persistent swelling (yes/no), 4. Stiffness (yes/no), 5. Limited in work (yes/no), Limited in sport (yes/no), and 6. Satisfaction (10-point numeric rating scale: 1 = completely dissatisfied, 10 = completely satisfied).
Objective. 1. Manual anterior drawer test (yes/no, positive: injured compared to noninjured side). 2. Stress radiographs (a. talar tilt (TT): positive: > 10° or difference injured/noninjured side > + 6°, b. Anterior talar translation (ATT): positive: > 4 mm or difference injured/noninjured side > +3 mm) (Krips et al. Citation2000). 4. Limited range of motion (ROM, yes/no, limitation dorsi- or plantarflexion injured ankle compared to noninjured ankle > 5°), and 4. Degree of arthrosis (grade 0: normal; grade I: osteophytes without joint space narrowing; grade II: joint space narrowing with or without osteophytes; grade III: (sub-) total disappearance or deformation of the joint space) (van Dijk et al. Citation1997).
Ankle scores. 1. Good score (range: 0–12: Activ-ity level (0–3), Pain (0–3), Swelling (0–3), Func-tional Instability (0–3); Excellent: 0; Good: 1; Fair: 2–6; Poor: < 6) (Good and Jones Citation1975). 2. Karls-son score (Ranging 0–100: Instability (0–25); Pain (0–20); Swelling (0–10); Stiffness (0–5); Activities (0–15); Stair climbing (0–10); Running (0–10); Support (0–5): Excellent: 91–100, Good: 81–91, Fair: 61–80, Poor: < 60) (Karlsson and Petersen Citation1991).
Data analysis
Unless clearly stated differently, patients were ana-lyzed—not ankles. In patients with two affected ankles, the side with the worst score was used for analysis. Means with 95% CI are given where appro-priate. All other results are given as the number of patients/ankles with the condition compared to the total population/number of ankles, or compared to the number of patients/ankles analyzed for the condition. Difference between ROM, radiographic TT, ATT and degree of arthrosis of the affected and unaffected side were analyzed statistically, using a non-parametric test for related samples (Wilcoxon signed rank test). Patients with both sides affected were excluded from this comparison.
Results (Table)
1 patient required a revision operation 6 years after the initial procedure because of recurrence of instability and increased mechanical laxity. The secondary direct anatomical reconstruction led to full recovery.
Patient demographics and follow-up results (37 patients, 40 ankles)
Subjective results
At follow-up, there was subjective instability in 11 patients (11 ankles), pain in 11 patients (11 ankles), swelling in 16 patients (16 ankles), and 6 patients (6 ankles) experienced stiffness. One or more of the symptoms were present in 20 patients (20 ankles). 3 patients were limited in work or activities of daily living, and 14 patients were limited in sports activity. At follow-up, mean satisfaction (10-point scale, 37 patients) was 7.9 (95% CI: 7.3–8.5). 32 of the 37 patients (35 ankles) rated 6 or higher.
Objective results
Physical examination. There was a positive manual anterior drawer test in 6 of the 38 ankles, whereas a limited range of motion was also found in 6 ankles. There was no statistically significant difference between the mean ROM of the affected and the unaffected ankles.
Stress radiographs. Stress radiographs were taken of 34 ankles in 31 patients. Mean TT of the injured ankle was 3.9° (95% CI: 2.6–5.3) com-pared to 3.0° (95% CI: 1.7–4.3) in the uninjured ankle. The mean ATT of the injured leg was 3.0 mm (95% CI: 2.5–3.5) compared to 3.2 mm (95% CI: 2.4-–3.5) in the uninjured leg. 5 patients had a positive TT, and 6 patients had a positive ATT. 9 patients had a positive TT and/or ATT. There was no statistically significant difference between the mean TT or ATT of the affected and the unaffected ankles.
Osteoarthrosis (OA). 10 patients had no osteoar-throtic changes of the injured ankle at follow-up. 21 patients had OA of grade I, 2 patients had grade II and 1 patient had grade III. Of the uninjured ankles, 13 patients had no OA changes at follow-up. 20 patients had grade I, no patients had grade II, and 1 patient underwent fusion of the talotibial joint because of posttraumatic OA (not caused by chronic ankle instability). There was no statisti-cally significant difference between the degree of OA in the affected and the unaffected ankles.
Ankle scores. The mean Karlsson score at follow-up was 85 points (95% CI: 80–90). 23 of the 37 patients achieved a good or excellent result accord-ing to the Karlsson score (4 patients scored poor), and 25 of the 37 patients had a good or excellent result according to the Good score (no patient scored poor).
Discussion
10–20% of patients sustaining an acute ankle inversion trauma suffer from residual chronic anterolateral ankle instability, often accompanied by disabling symptoms such as pain and swelling (Karlsson et al. Citation1997). Van Dijk et al. (Citation1996) found (osteo-) chondral lesions in 20 of 30 patients who underwent arthroscopy after a primary acute ankle inversion trauma. Harrington (Citation1979) and Taga et al. (Citation1993) found a correlation between the duration of chronic ankle instability and degenerative changes in the ankle joint.
When nonoperative treatment of recurrent sprains fails and increased laxity of the anterolateral ligaments is present, surgery may be considered. A choice must be made between an anatomical reconstruction, e.g. the Weber procedure, and a nonanatomical procedure, in which a peroneal tendon is used for reconstruction (Elmslie Citation1934, Evans Citation1953, Broström Citation1966, Weber Citation1966, Weber and Hupfauer Citation1969, Chrisman and Snook Citation1969, Bouretz and Duquennoy Citation1975, Watson-Jones Citation1976). A major disadvantage of using a peroneal tendon is that its attribution to functional stability of the ankle is partially sacrificed (St. Pierre et al. Citation1984). Of the 3 best-known procedures, the Evans, Watson-Jones and the Chrisman-Snook reconstructions, the latter seems to provide the best results—but is also the most complex (Snook et al. Citation1985). The outcome after the Evans and Watson-Jones procedures deteriorates in the long term with recurrent instability, pain and limited subtalar movement (van der Rijt and Evans Citation1984, Karlsson et al. Citation1988). Comparative studies have shown better long-term results for anatomical reconstructions, for both subjective and objective outcome measures (Krips et al. Citation2000, Citation2001, Citation2002). The results of a randomized controlled trial by Hennrikus et al. (Citation1996) comparing the Chrisman-Snook with a direct anatomical reconstruction showed similar results for stability after an average of almost 2.5 years of follow-up, but a worse functional outcome (Sefton score) and more complications in the Chrisman-Snook population.
The disadvantages of procedures using a pero-neus tendon inspired Weber to develop a new tech-nique, using the plantaris tendon for an anatomical reconstruction of the ATFL (Weber Citation1966, Weber and Hupfauer Citation1969). Several authors have reported their experience with the Weber procedure, or have, as in this study, added technical modifications. Marti et al. (Citation1977), Magerl and Marti (Citation1978), and later Raaymakers et al. (Citation1983) reported good-to-excellent results in about four-fifths of the patients after an average of 2–3 years follow-up. The stud-ies by Marti et al. (Citation1977) and Raaymakers et al. (Citation1983) evaluated mainly the same population as presented in this study.
Anderson (Citation1985), followed by Palladino et al. (Citation1991), Segesser and Goesele (Citation1996), and Hin-termann and Renggli (Citation1999), modified the Weber procedure by additionally reconstructing the CFL with the same tendon graft. According to the vari-ant of Anderson and Palladino, the plantaris tendon remains attached to its distal insertion and is led to the anterolateral ankle ligaments by a drill hole through the calcaneus. All 4 groups reported good short- to long-term results (range 4 months to 18 years). However, it is questionable whether addi-tional reconstruction of the CFL is always neces-sary, since the ATFL is the most important pas-sive stabilizer against inversion injury and is most often the only damaged ligament (Broström Citation1966, Colville et al. Citation1990). Segesser and Goesele (Citation1996) actually compared a plantaris reconstruction with and without reconstruction of the CFL. Although not randomized, short-term results—mainly return to work and sport—were better in the CFL group, but long-term results were equal in both groups. Still, in selected cases with obvious damage to the CFL, additional reconstruction of this ligament might be considered.
Compared to reconstructions with a pero-neal tendon, Brunner and Gaechter (Citation1991) found better results for reconstructions with the plantaris tendon (128 versus 52 (plantaris) patients). Huy et al. (Citation1985) found better subjective results for the Watson-Jones tenodesis compared to the Weber procedure, but this was in a much smaller series of 39 patients (25 Watson-Jones vs 14 plantaris).
We used the original technique described by Weber (Citation1966) and Weber et al. (Citation1969) (-) combined with integration of the remnants of the ligaments and capsule for better vascularization of the free transplant (); a modification described by Magerl and Marti (Citation1978). Segesser and Goesele (Citation1996) and Hintermann and Renggli (Citation1999) used a similar modification, although they described it merely as reinforcement.
We used the extensor tendon of the third toe as tendon graft in 2 patients, because of the absence of the plantaris tendon. This method has also been reported previously, with good results (Takashi et al. Citation2003).
According to our results, the Weber procedure appears to prevent arthrotic changes in patients with chronic ankle instability and with increased ligament laxity. Only 1 patient underwent a second reconstruction because of persistent instability. The high rate of subjective symptoms (20 of the 37 patients) that we found at follow-up does not correlate with the low rate of degenerative changes, the high rate of patient satisfaction (32 of the 37 patients) and the high rate of good or excellent results according to the Karlsson and Good scores. One explanation may be the lack of differentiation between mild and severe symptoms. Even minor, non-limiting complaints were scored and contributed to the high percentage of symptoms at follow-up. Although we used another score, our findings are similar to the 74% good-to-excellent results reported in the study by Raaymakers et al. (Citation1983).
The strength of our study is the long follow-up period. One weakness is the number of patients lost to follow-up, due to the length of the follow-up period and the large proportion of international sports and ballet participants. A second weakness in our study was the non-comparative design. In general, the results of the Weber procedure seem not to be as good as a direct anatomical reconstruc-tion, but appear to be superior to the outcome of an Evans procedure.
One theoretical disadvantage, which the Weber procedure has in common with other (tendon) graft reconstructions, is the additional risk of donor site morbidity (St. Pierre et al. Citation1984). We did not review postoperative complications, but a low rate of complications was reported in the study by Raaymakers et al. (Citation1983). Additionally, the com-parative studies of Krips et al. (Citation2000, Citation2001, Citation2002) showed no significant difference in postoperative complications between anatomical reconstructions and tenodeses.
Author contributions
JdV: protocol development, patient evaluation, writing of manuscript.
PS: protocol development, patient evaluation, writing of manuscript.
ER: operating on patients, protocol development, review of manuscript.
RM: operating on patients, protocol development, review of manuscript.
No competing interests declared.
- Anderson M E. Reconstruction of the lateral ligaments of the ankle using the plantaris tendon. J Bone Joint Surg (Am) 1985; 67: 930–4
- Bouretz J C, Duquennoy A. Operative treatment. Surgical technic. Rev Chir Orthop Reparatrice Appar Mot 1975; 61: 154–6, (Suppl 2)
- Broström L. Sprained ankles. VI. Surgical treatment of chronic ligament ruptures. Acta Chir Scand 1966; 132: 551–65
- Brunner R, Gaechter A. Repair of fibular ligaments: com-parison of reconstructive techniques using plantaris and peroneal tendons. Foot Ankle 1991; 11: 359–67
- Chrisman O D, Snook G A. Reconstruction of lateral ankle ligament tears of the ankle. J Bone Joint Surg (Am) 1969; 51: 904–12
- Colville M R, Marder R A, Boyle J J, Zarins B. Strain measurement in lateral ankle ligaments. Am J Sports Med 1990; 18: 196–200
- Elmslie R C. Recurrent subluxation of the ankle joint. Ann Surg 1934; 100: 364–7
- Evans L D. Recurrent instability of the ankle. A method of surgical treatment. Proc Roy Soc Med 1953; 46: 343–4
- Good C J, Jones M A, Lingstone B N. Reconstruction of the lateral ligament of the ankle. Injury 1975; 7: 63–5
- Harrington K D. Degenerative arthritis of the ankle second-ary to long-standing lateral ligament instability. J Bone Joint Surg (Am) 1979; 61: 354–61
- Hennrikus W L, Mapes R C, Lyons P M, Lapoint J M. Out-comes of the Chrisman-Snook and modified-Brostrom procedures for chronic lateral ankle instability. A prospec-tive, randomized comparison. Am J Sports Med 1996; 24: 400–4
- Hintermann B, Renggli P. Anatomische Rekonstruktion der lateralen Sprunggelenkbänder mit der Plantarissehne zur Behandlung der chronischen Instabilität. Orthopäde 1999; 28: 778–84
- Huy J, Schaap E J, Tonino A J. Comparison of the Watson-Jones with the Weber Technique of reconstruction of the ankle ligaments long after injury. Acta Orthop Scand 1985; 56: 517
- Karlsson J, Lansinger O. Lateral instability of the ankle joint. Clin Orthop 1992, 276: 253–61
- Karlsson J, Petersen L. Evaluation of ankle function: The use of a scoring scale. Foot 1991; 1: 15–9
- Karlsson J, Bergsten T, Lansinger O, Peterson L. Lateral instability of the ankle treated by the Evans procedure. A long-term clinical and radiological follow-up. J Bone Joint Surg (Br) 1988; 70: 476–80
- Karlsson J, Eriksson B I, Bergsten T, Rudholm O, Swärd L. Comparison of two anatomic reconstrions for chronic lat-eral instability of the ankle joint. Am J Sports Med 1997; 25: 48–53
- Kerkhoffs G M M J, Handoll H H, de Bie R, Rowe B H, Struijs P A A. Surgical versus conservative treatment for acute injuries of the lateral ligament complex of the ankle in adults. Cochrane Database Syst Rev 2002, 3, CD000380
- Krips R, van Dijk C N, Halasi T, Lehtonen H, Moyen B, Lan-zetta A, Farkas T, Karlsson J. Anatomical reconstruction versus tenodesis for the treatment of chronic anterolateral instability of the ankle joint: a 2- to 10-year follow-up, multicenter study. Knee Surg Sports Traumatol Arthrosc 2000; 8: 173–9
- Krips R, van Dijk C N, Halasi P T, Lehtonen H, Corradini C, Moyen B, Karlsson J. Long-term outcome of anatomi-cal reconstruction versus tenodesis for the treatment of chronic anterolateral instability of the ankle joint: a multi-center study. Foot Ankle Int 2001; 22: 415–21
- Krips R, Brandsson S, Swensson C, van Dijk C N, Karlsson J. Anatomical reconstruction and Evans tenodesis of the lateral ligaments of the ankle. Clinical and radiological findings after follow-up for 15 to 30 years. J Bone Joint Surg (Br) 2002; 84: 232–6
- Magerl F, Marti R K. Fibulotalare Bandplastik mit der Plan-tarissehne. Hefte Unfallheilkunde 1978; 133: 169–74
- Marti R K, Reichen A, Oberhammer L, Raaymakers E. Talo-fibular tendon graft for recurrent instability of the ankle joint. In: Injuries of the ligaments and their repair. Chapchal George. Georg Thieme Verlag, Stuttgart 1977; 219–22
- Palladino S J, Smith S B, Jackson J L. Plantaris tendon reconstruction of the lateral ankle ligaments. J Foot Surg 1991; 30: 406–13
- Raaymakers E, Postma J, van Gulik Th, Marti R. Sport-verletzungen und Sportschäden. Chapchal George. Georg Thieme Verlag, Stuttgart 1983; 223–6
- Segesser B, Goesele A. Fibuläre Bandplastik mit Planta-rissehne nach Weber, modifiziert nach Segesser. Sportverl Sportschäd 1996; 10: 88–93
- Snook G A, Chrisman O D, Wilson T C. Long-term results of the Chrisman-Snook operation for reconstruction of the lateral ligaments of the ankle. J Bone Joint Surg (Am) 1985; 67: 1–7
- St. Pierre R K, Andrews L, Allman F, Jr., Fleming L L. The Cybex II evaluation of lateral ankle ligamentous recon-structions. Am J Sports Med 1984; 12: 52–6
- Taga I, Shino K, Inoue M, Nakata K, Maeda A. Articular cartilage lesions in ankles with lateral ligament injury. An arthroscopic study. Am J Sports Med 1993; 21(1)20–6
- Takahashi T, Nakahira M, Kaho K, Kawakami T. Anatomi-cal reconstruction for chronic lateral ligament injury of the ankle using pedicle tendon of the extensor digitorum longus. Arch Orthop Trauma Surg. 2003; 123: 175–9
- van der Rijt A J, Evans G A. The long-term results of Watson-Jones tenodesis. J Bone Joint Surg (Br) 1984; 66: 371–5
- van Dijk C N, Bossuyt P M.M, Marti R K. Medial ankle pain after lateral ligament rupture. J Bone Joint Surg (Br) 1996; 78: 562–7
- van Dijk C N, Tol J L, Verheyen C P.M. A prospective study of prognostic factors concerning the outcome of arthroscopic surgery for anterior ankle impingement. Am J Sports Med 1997; 25: 737–45
- Watson-Jones R. Fractures and joint injuries. Fifth ed. Churchill Livingstone, Edinburgh 1976; 2: 1114–6
- Weber B G. Die Verletzungen des oberen Sprunggelenkes. Huber, Bern 1966
- Weber B G, Hupfauer W. Zur Behandlung der frischen fibularen Bandruptur und der chronische fibularen Bandinsuf-fizienz. Arch Orthop Unfall-Chir 1969; 65: 251–7