Abstract
Background Skip lesions in Ewing's sarcoma of the bone seem to be rare; to our knowledge only 7 cases have been published in the English medical literature.
Methods We retrospectively reviewed imaging and histological data relating to 235 patients with non-metastatic Ewing's sarcoma of the bone who participated in the cooperative Ewing's sarcoma study (CESS 86 and CESS 91), and we identified 15 patients with a skip lesion at diagnosis.
Results The skip lesion was located in the same bone as the primary tumor in 13 patients, and in an adjacent juxtaarticular bone in 2 cases. The average follow-up was 11 years. Despite aggressive treatment including surgery in all cases, tumor relapse occurred in 9 patients, and 7 of these patients died due to metastatic disease.
Interpretation Skip lesions in patients with otherwise non-metastatic skeletal Ewing's sarcoma may be of the same consequence as the molecular detection of marrow metastases and possibly confer a worse prognosis. Newer imaging modalities (for example PET) and careful staging work-up may indicate that skip metastases in Ewing's sarcoma are more common than previously suspected.
▪
Ewing's sarcoma and malignant peripheral neuroectodermal tumors of bone account for 6–15% of all malignant bone tumors (Jurgens Citation1994). 15–30% of patients present with detectable metastases at the time of diagnosis (Hayes et al. Citation1987, Sundaram et al. Citation1989, Roessner and Jurgens Citation1993, Saifudin et al. Citation2000, Franzius et al. Citation2001). Although they are a well-recognized feature of osteosarcoma, skip lesions appear to be rare in Ewing's sarcoma (Davies et al. Citation1997, Paulussen et al. Citation2001, Schleiermacher et al. Citation2003), and the prognostic implications of skip lesions in Ewing's sarcoma remain unclear. A skip lesion is a separate, histologically proven focus of a neoplasm that has developed within the host bone at the time of diagnosis. It must be separated from the larger primary tumor by an interval of normal bone (Enneking and Kagen Citation1975a, Citationb, Enneking et al. Citation1980, Kissane et al. Citation1983). The discontinuity between the primary lesion and the skip lesion may vary from a few mm to a few cm, but occurs in the same bone. Occasionally, a lesion arises on the opposite side of a joint. We retrospectively reviewed 15 patients with non-metastatic Ewing's sarcoma and a skip lesion.
Patients and methods
We reviewed (retrospectively) 235 patients with non-metastatic Ewing's sarcoma or PNET of the bone, all of whom participated in the cooperative Ewing's sarcoma study trials (CESS 86 and CESS 91) documented in the archives of the cooperative Ewing's sarcoma study center at the University of Münster. The radiographs, MRI scans, CT scans and histology specimens of all 235 patients were reviewed in order to identify patients with a skip lesion. Based on the criteria published by Enneking and Kagen, we found 15 patients with a skip lesion.
Diagnosis
All patients had a diagnostic work-up at presentation based on the CESS protocol. This included radiographs of the affected region, an MRI scan (T1 and T2 weghted, without gadolinium) and/or a CT scan of the affected region, a total body Technitium 99 bone scintigraphic scan, and histology of percutaneous or open biopsy. In addition, radiography and CT scan of the thorax were performed in all patients. At each follow up visit (6, 12 and 24 weeks after surgery, and then yearly), an X-ray of the affected region was done whilst MRI, CT or scintigraphy were done only on indication. In 6 cases, only the biopsies taken from the primary lesion were available, whereas biopsies of the primary tumor and the skip lesion were available in the remaining 9 cases. In 3 of these 9 cases, a second biopsy of the primary tumor and the skip lesion was performed after several cycles of adjuvant chemotherapy, prior to definitive surgery. Retrieved resection specimens in all 15 patients were cut with a band saw in multiple slab sections. Representative slab sections were then cut into thin sections and prepared for routine (hematoxylin and eosin) and immunochemical staining. Besides an assessment of response to preoperative adjuvant therapy, foci of suspected or proven skip lesions were reviewed in detail. In addition, areas between the primary tumor and the skip lesion were dissected, embedded in paraffin and stained to ascertain that they consisted of normal bone.
Adjuvant chemotherapy and radiotherapy
All patients received multiple-agent chemotherapy. Between 1986 and 1990, 5 patients treated according to the CESS 86 protocol received a fourdrug therapy protocol (VAIA), which included vincristine, adriamycin, ifosfamide and actinomycin D. Starting at the end of 1989 through 1992, 10 patients were treated according to the CESS 91 protocol (EVAIA), a five-drug regime including the former four drugs (VAIA) and etoposide. 10 of the 15 patients received adjuvant radiotherapy, preoperatively in 6 patients and postoperatively in 4 patients. 3 of the 6 patients who received preoperative radiotherapy had additional intraoperative local radiation therapy of the resection margins and, in 1 case, of the nearby juxtaarticular skip lesion. Definitive surgery was performed at least 4 weeks after completion of radiation therapy.
Results
15 (8 men) out of 235 patients (6%) with non-metastatic Ewing were found to have a skip lesion as the sole metastatic disease. The mean age at diagnosis was 17 (2–30) years. The average duration of follow-up was 11 (9–12) years.
Diagnosis
The Table shows the location of the primary tumor. The skip lesions could be identified on plain radiographs in only 3 patients, whereas MRI showed the skip lesions in 13 patients before surgery. CT showed the skip lesions in 13 patients, and was not performed in 2 patients. Of the 11 preoperative scintigraphic scans available for review, the skip lesion was demonstrated on 7. In 2 cases with a skip lesion located within 1 cm of the primary tumor, the diagnosis was confirmed only on histology of the resection specimen after definitive surgery. The skip lesion was located in the same bone as the primary tumor in 13 patients (), whereas an adjacent bone was the location of the skip lesion in 2 cases (). Normal signal intensity was noted in the marrow between the primary tumor and the skip lesion, and histology confirmed normal bone tissue between the primary tumor and the skip lesion.
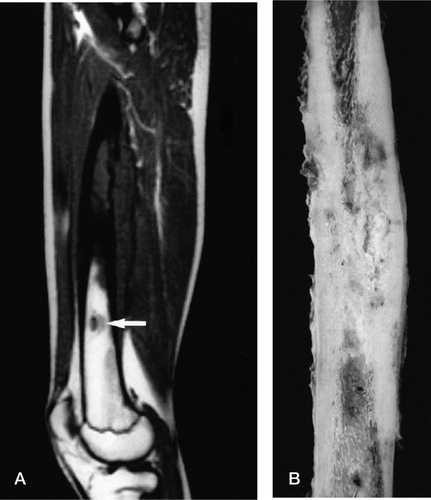
Figure 1. Ewing's sarcoma of the left humerus, demonstrating the primary and skip lesions on both radiographs (A) and MR scan (B).

Figure 2. Ewing's sarcoma of the fibula with a skip lesion on the shaft of the tibia, not evident on conventional radiographs (A) but clearly seen on the MR scan (B).

Clinical data
Surgery
The goal of surgical treatment was a wide enbloc excision of the tumor, including the skip lesion. In 9 patients, the existence of a skip lesion influenced the extent of surgery. In 3 of these 9 cases, one-half of a joint was surgically removed and reconstructed with prosthesis rather than an intercalary allograft reconstruction, preserving the integrity of the joint. In a fourth patient, a subtotal tibia resection (metaphyseal-diaphyseal-metaphyseal) instead of a metaphyseal-diaphyseal resection was performed in order to achieve a wide resection. An allograft and a fibula strut graft bridged the defect. In the fifth and sixth patients, a more extensive resection was necessitated by the existence of a skip lesion. On a 4-year-old boy with a tumor in the proximal two-thirds of the femur, and a skip lesion in the distal inter-condylar region of the same bone, a total femur resection was performed. The other was an 11-year-old boy with a tumor of the proximal fibula and a skip lesion in the shaft of the tibia (). A knee disarticulation was necessary to achieve adequate surgical margins.
Figure 3. A) MR scan of a patient with a proximal femoral Ewing's sarcoma and a distal skip lesion which was not evident on the radiograph.B) Excised femur of the same patient, which has been split into two halves to show the primary and skip lesions.
The seventh and eighth patients, in whom only the primary tumor was radically excised (even though the skip lesion was diagnosed before surgery), received intraoperative after-loading radiotherapy of the resection margin and, in 1 case, of the juxtaarticular skip lesion. Both patients responded well to preoperative chemotherapy and radiotherapy. An intercalary allograft reconstruction was used in both cases. In the nineth patient, intralesional resection of the primary tumor involving the proximal femur and a wide excision of a distal skip lesion was combined with intraoperative radiotherapy. The hip joint could be preserved and reconstruction was performed using an intercalary allograft instead of proximal femur endoprosthesis. In 6 patients, the existence and location of the skip lesion did not have a significant influence on the type and extent of surgery. The skip lesions were not only located within 4 cm of the primary tumor, but also within the diaphysis of a long bone.
Tumor relapse
There were 9 cases of tumor relapse, with only 1 being a local recurrence. Of the remaining 8 patients, 5 had skeletal metastasis, 4 of whom died due to metastastic disease at a follow-up duration of 9 months and 1, 3 and 8 years, respectively. 1 patient had pulmonary, lymph node and skeletal metastasis, and subsequently succumbed to the disease 5 years after diagnosis. Of the remaining 2 patients, one had bone and lymph node metastasis, and the other had lung and mediastinal metastasis. Both had died at 1 and 4 years of follow-up, respectively
Discussion
Our study represents the largest group of patients with Ewing's sarcoma and a skip lesion as sole metastatic disease. MRI and CT allowed diagnosis of the skip lesion in 13 of 15 cases. We found that in many cases, a skip lesion influences the choice and extent of the surgical excision and reconstruction. Although the number of patients is too small to make definitive statements with regard to survival in this subgroup, it is still important to note that despite aggressive treatment (including surgery in all cases), metastases occurred in 8 of 15 patients. This is higher than the 35% rate of metastatic disease reported by Paulussen et al. (Citation2001) in 301 patients with localized Ewing's sarcoma of the bone. Our findings suggest that survival in patients with skip lesions may be worse than would be expected in non-metastatic Ewing's sarcoma (Paulussen et al. Citation2001).
The occurrence of skip lesion in Ewing's sarcoma is rare. Previous studies (Saifudin et al. Citation2000, Paulussen et al. Citation2001) have failed to give a detailed account of the treatment, event-free survival and mortality of this patient population. Also, previous large studies on the Ewing's sarcoma family of tumors have not mentioned the occurrence of skip lesions—illustrating the extreme rarity (Saifudin et al. Citation2000, Ferrari et al. Citation2001, Paulussen et al. Citation2001, Bacci et al. Citation2002, Citation2003). Recent studies have indicated that micrometastases present at diagnosis, but undetectable by conventional methods, can be demonstrated by RT-PCR with a sensitivity of 83% in bone marrow (Athale et al. Citation2001). Patients with localized disease but with bone marrow micro-metastases have a poorer disease-free survival (53%) than patients with strictly localized disease (80%) (Athale et al. Citation2001). The significance of skip lesions has been extensively reviewed in another childhood malignancy, osteosarcoma. Osteosarcoma patients with a skip lesion as the sole metastatic disease have a higher risk of development of distant metastasis and have a poorer prognosis than patients with non-metastatic osteosarcoma.
Newer imaging modalities such as proton emission tomograms (PET) and careful staging work-up may show that skip metastases in Ewing's sarcoma are more common than previously suspected. The need to differentiate suspected skip lesions from other osseous pathologies requires, whenever possible, a biopsy of the primary tumor as well as the skip lesion. For strictly localized Ewing's sarcoma of the bone, local excision with chemotherapy can be curative. The potential implications for patient prognosis with Ewing's sarcoma and a skip lesion as the sole metastatic disease remain unknown. We therefore suggest that these patients should be considered as a separate group.
The authors wish to acknowledge the assistance of Professor H. Jurgens and Dr. M. Paulussen of the Department of Orthopaedics, Westfalischen Wilhelms University, Münster, Germany, in the preparation of this manuscript.
No competing interests declared.
- Athale U H, Shurtleff S A, Jenkins J J, Poquette C A, Tan M, Dovoning J A, Pappo A S. Use of RT-PCR for the diagnosis and staging of alveolar rhabdomyosarcoma, Ewing sarcoma family of tumours, and desmoplastic small round cell tumour. J Pediat Hematol Oncol 2001; 23: 99–104
- Bacci G, Mercuri M, Longhi A, Bertoni F, Barhieri E, Donati L, Giacomini S, Bacchini P, Forni C, Ferrari S. Neoadjuvant chemotherapy for Ewing's sarcoma of bone: recent experience at the Rizzoli Orthopaedic Institute. Eur J Cancer 2002; 38: 2243–51
- Bacci G, Ferrari S, Mercuri M, Longhi A, Giacomini S, Forni C, Bertoni F, Monfrini M, Barbieri E, Lari S, Donati D. Multimodal therapy for the treatment of nonmetastatic Ewing sarcoma of the pelvis. J Pediat Hematol Oncol 2003; 25: 118–124
- Davies A M, Makwana N K, Grimer R J, Carter S R. Skip metastases in Ewing's sarcoma: a report of three cases. Skeletal Radiol 1997; 26: 379–84
- Enneking W F, Kagan A. “Skip” metastases in osteosarcoma. Cancer 1975a; 36: 2192–205
- Enneking W F, Kagan A. The implications of “skip” metastases in osteosarcoma. Clin Orthop 1975b, 111: 33–41
- Enneking W F, Spanier S S, Goodman M A. A system for the surgical staging of musculoskeletal sarcoma. Clin Orthop 1980, 153: 106–20
- Ferrari S, Bertoni F, Mercuri M, Sottili S, Versari M, Bacci G. Ewing's sarcoma of bone: relationship between clinical characteristics and staging. Oncology Reports 2001; 8: 553–6
- Franzius C, Daldrup-Link H E, Sciuk J, Rummeny E J, Bielack S, Jungens H, Schoher O. FDG-PET for detection of pulmonary metastases from malignant primary bone tumors: comparison with spiral C. T. Ann Oncol 2001; 12: 479–86
- Hayes F A, Thomson E I, Parvey L, Rao B, Kun L, Parham D, Hutsu H O. Metastatic Ewing's sarcoma: remission induction and survival. J Clin Oncol 1987; 5: 1199–204
- Jurgens H F. Ewing's sarcoma and peripheral primitive neuroectodermal tumor. Curr Opin Oncol 1994; 6: 391–6
- Kissane J M, Askin F B, Foulkes M, Stratton L B, Shirley S F. Ewing's sarcoma of bone: clinicopathologic aspects of 303 cases from the Intergroup Ewing's Sarcoma Study. Hum Pathol 1983; 14: 773–9
- Paulussen M, Ahrens S, Dunst J, Winkelmann W, Exner G U, Kotz R, Amann G, Dockham-Dwomiczak B, Harms D, Muller-Weihrich S, Welte K, Komhuber B, Janka-Scaub G, Gabel U, Trennery Voute P A, Woulack A, Gadner H, Iwigens H. Localized Ewing tumor of bone: Final results of the Cooperative Ewing's Sarcoma Study CESS 86. J Clin Oncol 2001; 19: 1818–29
- Roessner A, Jurgens H. Round cell tumours of bone. Pathol Res Pract 1993; 189: 11–136
- Saifudin A, Whelan J, Pringle J A, Cannon S R. Malignant round cell tumours of bone: atypical clinical and imaging features. Skeletal Radiol 2000; 29: 646–51
- Schleiermacher G, Peter M, Oberlin O, Philip T, Rubie H, Mechinaud F, Sommelet-Olive D, Landman, Parter J, Bours D, Michon J, Dalattre O. Increased risk of systemic relapses associated with bone marrow micrometastasis and circulating tumor cells in localized Ewing tumor. J Clin Oncol 2003; 21: 85–91
- Sundaram M, Merenda G, McGuire M M. A skip lesion in association with Ewing sarcoma. J Bone Joint Surg (Am) 1989; 71: 764–8, Report of a case