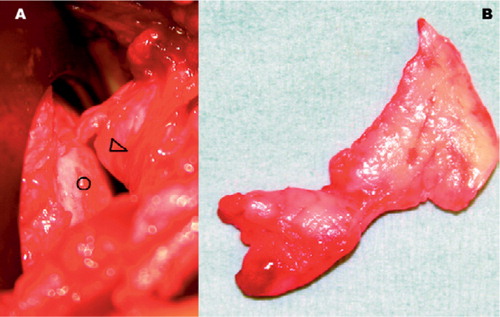
A 52-year-old active, obese (height 191 cm, weight 110 kg) but otherwise healthy woman fell while descending stairs and sustained an anterior shoulder dislocation with a displaced fracture of the greater tuberosity. Gentle manipulation under general anesthesia reduced the dislocation. Immediate post-reduction radiographs () were interpreted as showing a congruent glenohumeral joint and satisfactory position of the tuberosity fracture fragment. However, a close review of the radiographs on the following day raised the suspicion that the glenohumeral space was somewhat wider than expected. MRI confirmed a widened articular space and showed soft tissue between the humeral head and glenoid (). Surgical exploration revealed a large, meniscus-like labrum turned into the articular space (thereby obscuring the glenoid surface), and after its removal the glenoid surface became visible. The fragment of labrum measured 4 × 3 × 1 cm, and was totally detached from the 2 o'clock to 5 o'clock position on the anterior glenoid margin in the fashion of a bucket-handle tear (). Two screws were inserted, fixing the tuberosity in situ. 6 months postoperatively, the patient had a good range of both active and passive motion and her shoulder was pain-free and stable.
Figure 1. Anterior-posterior view and axillary view, immediately following closed reductio
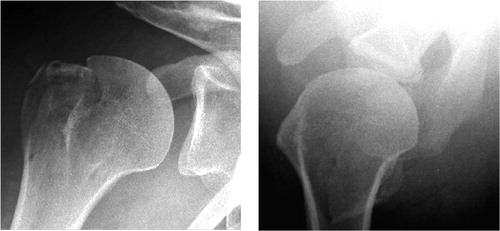
Figure 2. A and B: T1-weighted images; coronal view (A), axial view (B). C and D: T2-weighted images (soft tissue can be seen at tip of arrowhead); coronal view (C), axial view (D).
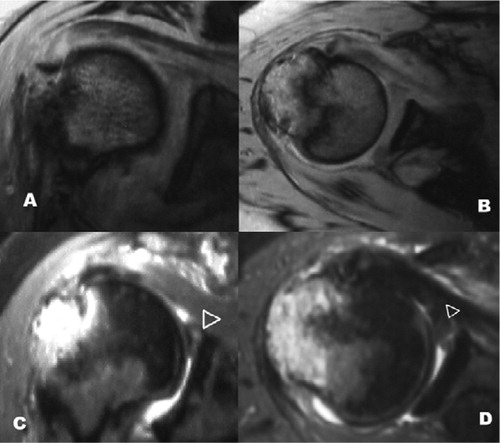
Figure 3. Intraoperative photographs. A: detached labrum (arrowhead) between humeral head (open circle) and glenoid, obscuring the glenoid surface. B: specimen of excised labrum.
Discussion
Irreducible anterior dislocations of the shoulder have been well described (Razemon Citation1961, Lam Citation1966, Kuhnen and Groves Citation1979, Vichard et al. Citation1981, Seradge and Orme Citation1982, Tietjen Citation1982, Oni Citation1983, Bridle and Ferris Citation1990, Inao et al. Citation1990, Ilahi Citation1998, Davies et al. Citation2000, Mihata et al. Citation2000), with responsible factors including (1) impaction of the humeral head on the glenoid rim (Herbert Citation1946), (2) held by a tightly stretched subscapularis (Lam Citation1966, Kuhnen and Groves Citation1979, Ilahi Citation1998), and (3) interposition of a surrounding structure including rotator cuff (Vichard et al. Citation1981, Tietjen Citation1982), biceps tendon (Cubbins et al. Citation1934, Seradge and Orme Citation1982, Freeland and Higgins Citation1985, Inao et al. Citation1990), torn labrum (Seradge and Orme Citation1982), subscapularis (Bridle and Ferris Citation1990), a fracture fragment of the greater tuberosity (Oni Citation1983, Davies et al. Citation2000), or a displaced fragment of the anterior glenoid rim (Mihata et al. Citation2000). However, the entity we have presented has been rarely mentioned in the literature. We have termed this “pseudoreduction” of a shoulder dislocation to alert one to the possibility that a single post-reduction AP radiograph may not be sufficient to show that the shoulder joint is concentrically reduced.
A literature search has failed to reveal any study which clearly defines what constitutes a normal gap (distance) between the humeral head and the glenoid, and in what shoulder position this gap width would be best judged (with regard to abduction and rotation in an anterior-posterior view, for example). Asymmetry of the joint space may be a subtle finding, but if one aspect of the joint space is wider than the other the shoulder is not concentrically reduced, which demands further diagnostic studies and most likely an open reduction with removal of any interposed structure(s) blocking reduction.
- Bridle S H, Ferris B D. Irreducible acute anterior dislocation of the shoulder: interposed scapularis. J Bone Joint Surg (Br) 1990; 72(6)1078–9
- Cubbins W, Callahan J, Scuderi C. The reduction of old or irreducible dislocations of the shoulder joint. Surg, Gynec Obstet 1934; LVIII: 129–35
- Davies M B, Rajasekhar C, Bhamra M S. Irreducible anterior shoulder dislocation: the greater tuberosity Hill-Sachs lesion. Injury 2000; 31(6)470–1
- Freeland A E, Higgins R W. Anterior shoulder dislocation with posterior displacement of the long head of the biceps tendon. Arthrographic findings. A case report. Orthopedics 1985; 8(4)468–9
- Herbert J. Luxation irréductible d'emblée de l'épaule et fractures tubérositaires. Rev d'orthop 1946; 32: 63–7
- Ilahi O A. Irreducible anterior shoulder dislocation with fracture of the greater tuberosity. Am J Orthop 1998; 27(8)576–8
- Inao S, Hirayama T, Takemitsu Y. Irreducible acute anterior dislocation of the shoulder: interposed bicipital tendon. J Bone Joint Surg (Br) 1990; 72(6)1079–80
- Kuhnen W, Groves R J. Irreducible acute anterior dislocation of the shoulder: case report. Clin Orthop 1979, 139: 167–8
- Lam S. Irreducible anterior dislocation of the shoulder. J Bone and Joint Surg (Br) 1966; 48: 132–3
- Mihata T, Doi M, Abe M. Irreducible acute anterior dislocation of the shoulder caused by interposed fragment of the anterior glenoid rim. J Orthop Sci 2000; 5(4)404–6
- Oni O O. Irreducible acute anterior dislocation of the shoulder due to a loose fragment from an associated fracture of the greater tuberosity. Injury 1983; 15(2)138
- Razemon J P. Irreducible dislocations of the shoulder. Apropos of 3 cases. Acta Orthop Belg 1961; 27: 239–46
- Seradge H, Orme G. Acute irreducible anterior dislocation of the shoulder. J Trauma 1982; 22(4)330–2
- Tietjen R. Occult glenohumeral interposition of a torn rotator cuff. A case report. J Bone Joint Surg (Am) 1982; 64(3)458–9
- Vichard P, Bellanger P, Watelet F. Irreducible shoulder dislocation caused by interposition of the rotator cuff. Apropos of 2 cases. Acta Orthop Belg 1981; 47(1)113–22