Abstract
Background Iliopsoas impingement is a recurrent complication following THA, caused by muscle friction against a protrusive prosthetic cup.This study was designed to quantify the dimensional variations in acetabular rim proiles, with particular regard to the iliopubic valley, in order to suggest means to prevent iliopsoas impingement.
Material and methods 34 cadaver pelvises were analyzed using a hip navigation system.The morphometric data were processed to plot proiles of all acetabular rims with particular regard to the shape and depth of the psoas valley.
Results The acetabular rim is an asymmetric succession of 3 peaks and 3 troughs.The psoas valley is a salient feature in most pelvises and there is only a weak correlation between its depth (mean 3.8 mm, SD 2.0) and acetabular diameter, anteversion, or inclination.
Interpretation It would be dificult to obviate the anterior overlap of the acetabulum using a hemispheric cup, a fortiori in certain morphotypes, without compromising range of motion or risk of dislocation.The solution for prevention of iliopsoas impingement would be to adapt cup design to acetabular anatomy, which may require different implants for the right and left sides, and hence a doubled inventory.
Ilio-psoas impingement is a recurrent cause of pain following total hip arthroplasty (THA).The syndrome develops as a result of chronic friction of the ilio-psoas muscle against a prosthetic cup that overlaps the iliopubic valley of the acetabulum.Such prosthetic overlap is commonly observed in cases where the implant is too large, insuficiently anteverted, or protrusive due to inadequate reaming.
Ilio-psoas impingement was irst suspected to cause pain in 1975 by Postel, and was later described by Kolmert et al.(Citation1984), Lequesne et al.(Citation1991), and Trousdale et al.(Citation1995).Furthermore, 2 series were reported in France—9 cases by Ala Eddine et al.(Citation2001) and 12 cases by Bricteux et al.(Citation2001).A review of what little literature exists on the syndrome would suggest an incidence of around 5% of all THA (Ala Eddine et al.Citation2001).This igure is dificult to estimate, because the syndrome takes various clinical forms.Most patients develop an early anterior groin pain that can sometimes be cured by iniltration or tenotomy, but it can sometimes take several months before the onset of symptoms.
Iliopsoas impingement can be analyzed using various imaging techniques, starting with standard radiographs—notably in the Arcelin proile, which helps determine whether the implanted cup is oversized (Lequesne et al.Citation1991, Trousdale et al.Citation1995).Ultrasonography (Rezig et al.Citation2004, Wank et al.Citation2004), bursography (Cheung et al.Citation2004), and MRI can all reveal bursitis, whereas CT is considered to be the optimal imaging modality as it highlights the impingement zone (Cyteval et al.Citation2003).Therapeutic attitudes regarding the syndrome have ranged from simple negligence, since symptoms sometimes disappear spontaneously, to surgical revision by iliopsoas tenotomy or even replacement of the prosthetic cup.
An important element in eliciting the syndrome is the anatomical factor, which has never been speciically examined in the literature, although it evidently iniuences the degree of prosthetic overlap.It was only when faced with dificulties in calculating acetabular angles on radiographs that Fabeck et al.(Citation1999) observed the variations in the iliopubic valley, over which the iliopsoas muscle passes to leave the pelvis.The anatomical study of Maruyama et al.(Citation2001) investigated these proile variations and distinguished 4 psoas valley conigurations with the following distribution in the population: 4% straight, 60% curved, 26% angular, and 10% irregular.Acetabular dysplasia, which favors anterior overlap of prosthetic cups, was reported in cases of iliopsoas impingement, affecting 17% in the study of Bricteux et al.(Citation2001) and 50% in Lequesne et al.(Citation1991).To our knowledge, however, no anatomical work has yet been performed to quantify the variations in dimensions of the acetabular rim.
We have quantiied the variations in proile of the acetabular rim with particular regard to the psoas valley, in the belief that a better understanding of acetabular rim morphology will help prevent iliopsoas impingement through improvements in surgical technique or implant design.Our study also employs an innovative imaging technique using a surgical navigation device.We have thus endeavored to assess the repeatability of the method for future use.
Material and methods
34 fresh non-embalmed cadaver pelvises, all free from dysplasia and arthritis, were dissected and cleared of soft tissue.The specimens were from 13 men and 21 women aged 65–88 years.Measurements were taken from each pelvis using a surgical navigation system (Stryker Hip Navigation v.1.1).
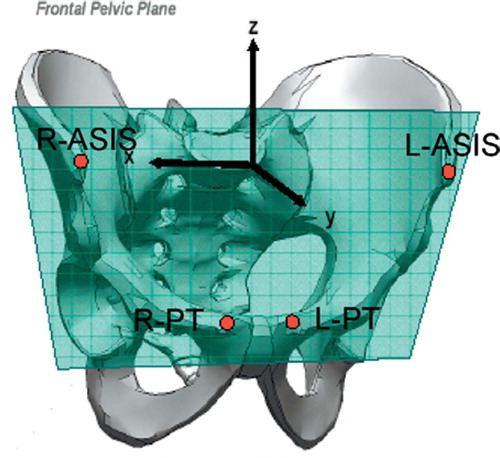
The pelvic tracker was anchored irmly into one of the iliac crests to keep a record of its position and orientation throughout all manipulations.The navigation pointer was then used to digitize four anatomical landmarks on the pelvis, which were then used to calculate the frontal pelvic plane and to deine the pelvic coordinate system, with its origin at the midpoint between the anterior superior iliac spines ().Thereafter, the rotation axis (z) was used to deine anteversion, the circumduction axis (y) for inclination, and the iexion axis (x) for position along the acetabular rim.
Figure 1. The frontal pelvic plane and the pelvic coordinate system as deined by four anatomical landmarks on the pelvis, the anterior superior iliac spines (ASIS) and the pubic tubercles (PT).
The right and left acetabulae were digitized into separate data iles, differentiating between points measured on the articular surface, the cotyloid fossa, or the acetabular rim.The number of points digitized on each acetabular rim was between 60 and 70.The navigation software deduced the acetabular radius and center of rotation from the curvature of the articular surface.It also calculated the anteversion and inclination angles by itting a mean plane to the acetabular rim points using the method of least squares.It is noteworthy that the acetabular notch was not digitized as part of the acetabular rim, as that would have falsiied the estimates of anteversion and inclination.However, 3 distinct anatomical landmarks were recorded to indicate the start, the midpoint, and the end of the acetabular notch: the anterior inferior horn (AIH), the posterior inferior horn (PIH), and the inferior margin of the acetabular notch (IMAN).
The data files of 68 acetabulae were imported into spreadsheets and processed to represent each acetabular rim as a two-dimensional profile ().This was done by treating the acetabular rim coordinates and the center of acetabular rotation as a single data set, then applying the following 3 mathematical manipulations: (i) translation of the data set such that the center of acetabular rotation coincides with the origin of the pelvic coordinate system; (ii) rotation of the data set such that themean acetabular plane coincides with the y-z plane of the pelvic coordinate system; and (iii) transformation of the coordinate system from Cartesian to cylindrical, such that (x, y, z) are expressed as (x, r, θ).
Figure 2. An acetabular rim shown as a two-dimensional profile using cylindrical coordinates.The anatomical landmarks identified on the acetabular rim are the posterior inferior horn (PIH), anterior inferior horn (AIH), and inferior margin of the acetabular notch (IMAN).The depth of the psoas valley is the difference between the average heights of adjacent peaks (P1 and P2) and the height of the central trough (T).
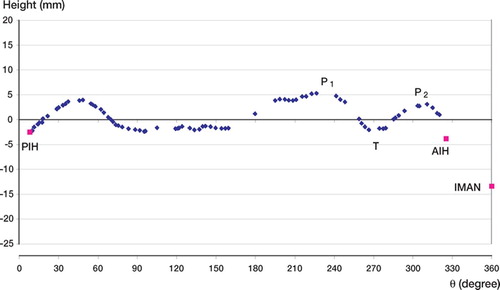
To make all acetabular profiles directly comparable, the inferior margin of the acetabular notch was set at 360° along the θ axis for all acetabulae.The profiles of left acetabulae were mirrored to become superimposable over right acetabulae.The graph of each acetabular rim was observed individually and the shape of its psoas valley was noted.The depth and width of each psoas valley was then calculated from the coordinates of the two adjacent peaks and of its central trough ().
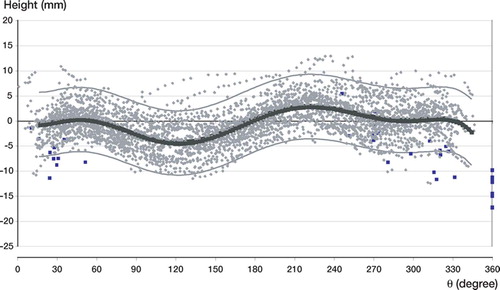
A chart of superposed profiles was produced for all acetabulae and an eighth-order polynomial mean curve was fitted with the 95% confidence band (SigmaPlot 9.0; Systat Software Inc., San Jose`, CA).
Results
The chart of superposed acetabular rim proiles suggests that the acetabular rim follows an asymmetrical succession of three peaks and three troughs ().The eighth-order polynomial it was chosen to represent the average proile, as it admits all 7 extrema almost independently.The individual charts of acetabular proiles reveal the prominence of the psoas valley, the mean depth of which was 3.8 mm (SD 2.0).
Figure 3. Superposition of acetabular rim profiles with an eighth-order mean polynomial curve and the 95% confidence bands.
The morphometric data revealed signiicant sexrelated variation in acetabular diameter (p < 0.001), anteversion (p < 0.01), and depth of the psoas valley (p < 0.01) ().Analysis of psoas valley coniguration produced the following distribution: 3% straight, 58% curved, 22% angular, and 17% irregular.The sex-related variations suggested that psoas valley depth could be related to either acetabular diameter or anteversion, and this led us to test for correlation between these 3 variables.By regression analysis, we found only a weak correlation between psoas valley depth and acetabular diameter (R = 0.26, p < 0.01), and between psoas valley depth and anteversion (R = 0.14, p < 0.1).
Table 1. Acetabular morphometric data and sex-related variation
The results reveal some morphometric variation between right and left acetabulae of the same pelvis, the most variable parameter being anteversion, with differences greater than 10° in 12 (35%) pelvises (mean 5.2°, SD 4.3, range 0.5–18).The difference in diameter was greater than 2 mm in 8 (24%) pelvises (mean 1.4 mm, SD 1.6, range 0.1– 6.0) whereas a difference of more than 10° inclination was observed in only 5 (15%) pelvises (mean 3.0°, SD 2.3, range 0.1–8.2).
Discussion
The results of analysis of the psoas valley show that it is a salient feature in most acetabulae, and the morphological distribution we found closely matches that observed by Maruyama et al.(Citation2001).The depth of the psoas valley is greater in men than in women, but the absence of a clear correlation with either acetabular diameter or anteversion suggests that depth might also be related to the musculature of the individual.The unpredictability of psoas valley coniguration might explain the irregular incidence of iliopsoas impingement following THA.
The curvaceous proile of the acetabular rim can be explained from the progressive development of the hip joint, which starts prenatally as early as the embryonic period (Olivier Citation1967, Uthoff 1990, Uthoff and Jarvis 1997).At birth, the pelvis is still partially cartilaginous, most notably the entire iliac crest, the acetabular ioor, and its inferior margin.The acetabulum is still a cartilaginous cup with a triradiate stem, forming an articular surface with a Y-shaped epiphyseal plate between the ilium, ischium, and pubis (Strayer Citation1971, Watanabe Citation1974).Ossiication of the pelvis continues from three primary centers in the innominate bones, and around puberty secondary centers appear in the iliac crest, ischial tuberosity, and pubic symphysis.The epiphyseal plate develops additional centers of ossiication between the eighth and ninth years, with greater growth potential in the iliac center than in the ischial or pubic centers.At puberty these epiphyses expand towards the periphery of the acetabulum, contributing to its depth.An important consideration is that the acetabulum is not formed by ‘digging’ into the pelvis, but rather by outward ossiication of its rim.This process continues until maturity and it ensures that the acetabular rim adapts structure to function (Olivier Citation1967).
The irregularity of the acetabular rim proile makes it dificult to accurately calculate the mean acetabular plane, and hence anteversion and inclination.This presents a source of error in our study because our method used these angles to plot the rim proile.With this in mind, we chose a more localized way to measure depth of the psoas valley, with respect to its two adjacent peaks and the central trough.Another criticism of our method might be our reference to the frontal pelvic plane.We chose to position the pelvis with its anterior superior iliac spines and pubic tubercles in the frontal plane in order to facilitate measurements.In reality, the positioning of the pelvis under the spine in the sagittal plane varies depending on the individual (Zilber et al.Citation2004).It has been demonstrated that the frontal pelvic plane has little or no change in tilt in the supine and in the standing positions, making it a valid reference for acetabular cup implantation (Anda et al.Citation1990, Mayr et al.Citation2005).In any case, the choice of referential merits reproducibility considering the dificulty of orienting the pelvis.
The existence of a valley in the iliopectinal eminence of the acetabulum is not a recent observation, but the function that this valley serves as a passage for the iliopsoas muscle is a relatively new inding (Fabeck et al.Citation1999, Maruyama et al.Citation2001).Our lack of knowledge about the psoas valley is exempliied by the anatomical study of Lazennec et al.(Citation1997), in which they report 11% of pelvises with minor acetabular dysplasia.The study further describes the presence of prominent psoas valleys as “hypoplasia of the anterior acetabular rim that reduces coverage of the femoral head”.It was only while analyzing the dificulty of calculating the anterosuperior angle of the acetabular ceiling that Fabeck et al.(Citation1999) identiied the various shapes of the psoas valley on the iliopectinal eminence.
Unlike the majority of prosthetic cups, the acetabular rim is not planar.It is therefore dificult to obviate the anterior overlap of the acetabular rim with a hemispherical implant.The degree of prosthetic overlap depends largely on the individual’s acetabular morphology and on the dimensions of their psoas valley.We believe that it would be advantageous to adapt the design of prosthetic cups to reproduce acetabular rim morphology.This would necessitate cups with asymmetrically curved rim proiles, and might require different implants for right and left sides.This solution has its economic limitations as it would double the implant inventory, but it would most likely reduce the incidence of iliopsoas impingement without compromising range of motion or increasing the risk of dislocation.
Contributions of authors
EV: Team leader, literature review and manuscript preparation.MS: Data processing, statistical analysis and manuscript preparation.ND and JLM: Support with data processing and use of navigation equipment.MN: Data collection on cadaver specimens.
Stryker provided navigation equipment for measurements as well as support for data processing and statistical analysis.
- Ala Eddine T, Remy F, Chantelot C, Giraud F, Migaud H, Duquennoy A. Anterior iliopsoas impingement after total hip arthroplasty: diagnosis and conservative treatment in 9 cases. Rev Chir Orthop Reparatrice Appar Mot 2001; 87(8)815–9
- Anda S, Svenningsen S, Grontvedt T, Benum P. Pelvic inclination and spatial orientation of the acetabulum. A radiographic.computed tomographic and clinical investigation. Acta Radiol 1990; 31(4)389–94
- Bricteux S, Beguin L, Fessy M H. Iliopsoas impingement in 12 patients with a total hip arthroplasty. Rev Chir Orthop Reparatrice Appar Mot 2001; 87(8)820–5
- Cheung Y M, Gupte C M, Beverly M J. Iliopsoas bursitis following total hip replacement. Arch Orthop Trauma Surg 2004; 124(10)720–3
- Cyteval C, Sarrabere M P, Cottin A, Assi C, Morcos L, Maury P, Taourel P. Iliopsoas impingement on the acetabular component: radiologic and computed tomography indings of a rare hip prosthesis complication in eight cases. J Comput Assist Tomogr 2003; 27(2)183–8
- Fabeck L, Farrokh D, Descamps P Y, Tolley M, Krallis P, Delince P. Analysis of the acetabulum anterior cover. J Radiol 1999; 80(12)1636–41
- Kolmert L, Persson B M, Herrlin K, Ekelund L. Ileopectineal bursitis following total hip replacement. Acta Orthop Scand 1984; 55(1)63–5
- Lazennec J Y, Laudet C G, Guerin-Surville H, Roy-Camille R, Saillant G. Dynamic anatomy of the acetabulum: an experimental approach and surgical implications. Surg Radiol Anat 1997; 19(1)23–30
- Lequesne M, Dang N, Montagne P, Lemoine A, Witvoet J. Coniict between psoas and total hip prosthesis. Rev Rhum Mal Osteoartic 1991; 58(9)559–64
- Maruyama M, Feinberg J R, Capello W N, D'Antonio J A. The Frank Stinchield Award: Morphologic features of the acetabulum and femur: anteversion angle and implant positioning. Clin Orthop 2001, 393: 52–65
- Mayr E, Kessler O, Prassl A, Rachbauer F, Krismer M, Nogler M. The frontal pelvic plane provides a valid reference system for implantation of the acetabular cup: spatial orientation of the pelvis in different positions. Acta Orthop 2005; 76(6)848–53
- Olivier G. Comparative embryology of the hip bone in primates. Z Morphol Anthropol 1967; 58(3)213–29
- Postel M. Painful prosthesis.I. Possible causes. Rev Chir Orthop Reparatrice Appar Mot 1975; 61(Suppl 2)57–61
- Rezig R, Copercini M, Montet X, Martinoli C, Bianchi S. Ultrasound diagnosis of anterior iliopsoas impingement in total hip replacement. Skeletal Radiol 2004; 33(2)112–6
- Strayer L M, Jr. Embryology of he human hip joint. Clin Orthop 1971, 74: 221–40
- Trousdale R T, Cabanela M E, Berry D J. Anterior iliopsoas impingement after total hip arthroplasty. J Arthroplasty 1995; 10(4)546–9
- Uhthoff H K. Embryology of the human hip with special reference to the development of the labra. Z Orthop Ihre Grenzgeb 1990; 128(4)341–3
- Uhthoff H K, Jarvis J. Embryology of the human hip. Orthopade 1997; 26(1)2–6
- Wank R, Miller T T, Shapiro J F. Sonographically guided injection of anesthetic for iliopsoas tendinopathy after total hip arthroplasty. J Clin Ultrasound 2004; 32(7)354–7
- Watanabe R S. Embryology of the human hip. Clin Orthop 1974, 98: 8–26
- Zilber S, Lazennec J Y, Gorin M, Saillant G. Variations of caudal.central.and cranial acetabular anteversion according to the tilt of the pelvis. Surg Radiol Anat 2004; 26(6)462–5