Abstract
Background and purpose Doctor's delay in diagnosing Ewing sarcoma is often long. We examined the initial symptoms of Ewing sarcoma of the rib to find characteristics that could help to shorten the delay in diagnosis and hopefully influence the prognosis.
Patients and methods We examined the records from the first visit for symptoms related to Ewing sarcoma of the rib in 26 consecutive patients, all of whom were < 30 years of age and had been diagnosed between 1981 and 2000. All patients had a minimum of 5 years follow-up.
Results A tumor was suspected at the first visit in only 5 of the 26 patients; pleurisy was the most common misdiagnosis. 23 patients complained of pain, localized or pleuritic, and 11 had a palpable mass. 15 of the 26 patients had chest radiographs taken at the first visit, but a tumor was suspected in only 4 cases. The most common radiographic finding was pleural effusion— diagnosed in 10 of the 15 patients. 23 patients were operated. It is noteworthy that in 6 patients no tumor was suspected before surgery. 12 patients died from the Ewing sarcoma. Median survival was 2.4 years. Doctor's delay was median 3.0 (0–10) months, but it exceeded 7 months in 4 patients. Patient's delay was 2.5 (0–10) months.
Interpretation The most important clinical finding in Ewing sarcoma of the rib was a palpable mass and pleural effusion. Both findings are rare in this age group and should be thoroughly investigated.
Ewing sarcoma is preferentially located in the long bones or in the pelvis, the ribs being the third most frequent site (making up 10–15% of all cases) (Gladish et al. Citation2002). Ewing sarcoma is the most frequent chest wall tumor in children and adolescents (Saenz et al. Citation2000).
Primary malignant bone tumors are so rare that most physicians will only meet a few patients with symptoms from an undiagnosed tumor during their entire professional career.
There have been numerous articles on the treatment and prognosis of Ewing sarcoma, but only a few have concentrated on the initial symptoms. Once the patient has been referred to a sarcoma center for diagnosis and treatment, he or she—or his or her parent—may have a blurred recollection of when and how the disease started.
We examined the initial symptoms and physical findings in Ewing sarcoma of the rib as described in the report from the patient's first visit to a physician.
Patients and methods
All patients with Ewing sarcoma of the rib diagnosed in Sweden from 1981 through 2000 were identified from the National Swedish Cancer Register. The study was limited to patients who were less than 30 years of age.
Files from the clinic where the tumor diagnosis was initially made were used to obtain information on when and where the patient first consulted a doctor for symptoms that could be related to the primary bone malignancy. Records from these earlier visits were requested in order to examine the medical file from the very first visit, for symptoms that could be related to the disease.
The following data were registered from the first medical visit: pain, pleuritic pain, localized thoracic pain, pain at night, duration of pain, swelling, history of trauma, dyspnoea, cough, periods of fever, and physical signs such as palpable mass, tenderness, and diminished breath sounds. The initial diagnosis, treatment, and findings at the chest radiograph were also registered.
Patient's delay was defined as the period from when symptoms were first noted until the first visit to a doctor, and doctor's delay was defined as the period from the first visit until the time that the diagnosis of Ewing sarcoma was established. Analysis of variance was used for statistical analysis and the significance level was set at p < 0.05. Kaplan-Meier analysis was used to calculate survival.
Results
From January 1, 1981 through December 31, 2000, 26 patients (16 male) with Ewing sarcoma of the rib were diagnosed in Sweden. The median age of the patients was 16 (6–26) years. Pertinent data could be obtained for all patients. There was no difference in distribution of tumor location between left and right ribs ().
Figure 1. Distribution of the 26 different Ewing sarcomas of the rib.
Reasons for consulting a doctor
17 patients consulted their doctor about thoracic pain and 6 had discovered a palpable mass in the thorax. In 2 cases the main reason was dyspnea, and 1 tumor was diagnosed accidentally.
15 patients had first consulted a general practitioner for symptoms related to the tumor, 10 consulted the emergency ward, and 1 case was discovered accidentally.
Symptoms
22 patients complained about intermittent localized thoracic pain and 10 also had pain of pleuritic nature. Only 1 patient reported pain at night. At the first visit, as many as 11 patients had noted a mass. General symptoms such as intermittent fever were reported by 11 patients and 5 complained of dyspnea. Trauma to the chest wall—occurring at about the same time as when the symptoms started—was reported by 5 patients.
Physical findings at the first medical visit
The physical examination yielded abnormal findings in 21 cases. In 11 patients the doctor noted a mass. Tenderness was found in 11 patients. Diminished breathing sounds were noted in 6 cases.
Initial diagnosis
A tumor was suspected at the first visit in only 5 cases. Pleurisy was the most common misdiagnosis— being the initial diagnosis in 11 patients. In 6 patients, a rib fracture or muscle strain was the initial diagnosis. Other initial diagnoses were constipation, fibrocystic tumor of the breast, and acute abdomen.
Radiographic examination
15 patients had a chest radiograph taken at their first medical visit. A tumor was suspected by the radiologist in only 4 cases. 4 radiographs were interpreted as being normal and the remaining 6 were inconclusive. Pleural effusion was noted in 10 of the 15 radiographic examinations. The size of effusion detected ranged from 2 cm in decubitus to almost complete ().
Figure 2. Large Ewing sarcoma of the rib showing pleural effusion on the left side. Destruction of costa 4 sin.

Delay
Median patient's delay was 2.5 (0–10) months and median doctor's delay was 3.0 (0–10) months. Both patient's and doctor's delay were longer for males than for females, the difference being almost statistically significant for patient's delay (13 weeks as compared to 7 weeks; p < 0.06). Doctor's delay was shorter for those reporting fever or a palpable mass at the first visit (). 4 patients had a doctor's delay longer than 7 months, however, and all 4 had recurrent disease after treatment.
Table 1. Doctor's delay in diagnosis
Treatment and outcome
Treatment of Ewing sarcoma is often confined to sarcoma centers. In Sweden there are 5 such centers. Not all of the patients in our study were treated at sarcoma centers, however, and surgery was performed at as many as 11 different hospitals. The Scandinavian Sarcoma Group has protocols for the treatment of Ewing sarcoma, and of those patients who were not treated at a sarcoma center, many followed an SSG protocol.
23 patients underwent surgery. It is noteworthy that in 6 patients a Ewing sarcoma was not suspected prior to surgery. In these 6 cases, the main provisional diagnosis was infection, pleura empyema, or a subphrenic abscess, and the surgical procedure resulted in excisional biopsy or an intralesional surgical procedure. 14 of the patients who underwent surgery were treated preoperatively with chemotherapy. The chemotherapy started after fine-needle or core-needle biopsy indicated a malignant tumor. Two patients were treated with an inadequate chemotherapy regimen due to a wrong preoperative diagnosis of lymphoma after fine-needle biopsy. The surgical margin was classified into 3 different categories: wide, marginal, and intralesional (). During the operative procedure, the affected rib was resected—often including the adjacent ribs. In 8 patients the defect in the thorax wall was reconstructed with Mesh net. 3 patients were only treated with chemotherapy and radiotherapy. The chemotherapy regimens were SSG IV (1980–1989) and SSG IX (1990–1999) (www.ssg-org.net).
Table 2. Surgical margins
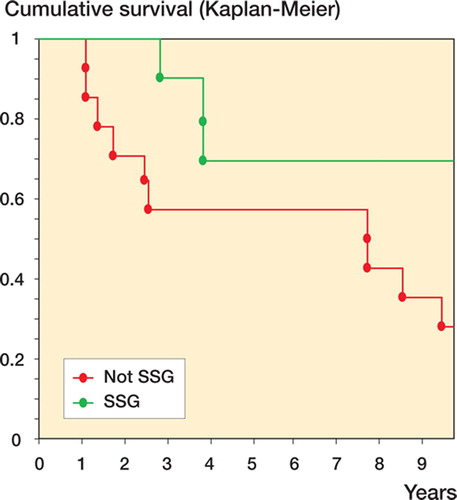
12 patients died from the disease. Except for 1 patient, who lived 8 years, all died within 4 years of diagnosis. 5 patients had metastasis already at the time of diagnosis. For these patients, doctor's delay was longer (mean 4.8 months as opposed to 2.8 months), but the difference was not statistically significant (p = 0.09). 14 patients had relapse of the Ewing sarcoma—as local recurrence, metastasis, or both. 3 of these patients were salvaged. Mean survival of the patients who relapsed was 1.7 years. Survival of those treated according to SSG regimens was longer (p = 0.05) ().
Figure 3. Survival analysis of patients treated and not treated according to the SSG regimen.
. Doctor's delay in diagnosis Symptom Delay (weeks) P-value Fever Yes, n = 11 8 0.05 No, n = 15 16 Palpable mass Yes, n = 11 7 0.06 No, n = 15 14 . Surgical margins Hospital Margin Wide Marginal Intralesional Sarcoma center 4 4 1 Other 2 6 6 Acta Orthopaedica 2007; 78 (6): 840–844 843
Discussion
Chest pain is the predominant initial symptom of Ewing sarcoma of the rib; it is found in the majority of patients (Saenz et al Citation2000). In our study it was reported by 9 of 10 patients. Chest pain in children and adolescents leads to consideration of a number of differential diagnoses. Musculoskeletal causes are common, and often related to trauma. Other non-traumatic diagnoses associated with chest pain are pneumothorax, pleurisy, myocarditis, pericarditis, and pleurodynia (Kocis Citation1999). Pain at night was reported by only 1 patient—a symptom often considered typical of bone malignancies.
As in a previous report of Ewing sarcoma of the rib, a palpable mass was an important clinical feature found in 8 of 20 patients (Saenz et al Citation2000). Half of the patients in our study had a palpable mass in the chest wall as early as the first visit, which, in most cases, led to early diagnosis.
Generally, 20–30% of Ewing sarcoma patients experience fever (Grier Citation1997). In our study, at least half of the patients with Ewing sarcoma of the rib had a history of fever. Since respiratory symptoms are common, it is not surprising that pleurisy appears to be a common misdiagnosis. However, in our study the clinical course often diverged from what would be expected of respiratory infections; the patients did not improve clinically as expected, and therefore consulted the doctor again.
A pleural effusion, detected in 10 of 15 radiographs in our study, is an uncommon radiological finding in young patients with chest pain. In a prospective study of chest pain in children, pleural effusion was seen in only 1 of 137 radiographs (Selbst et al. Citation1988). Thus, pleural effusion in a child should certainly be followed up.
In a previous study of primary Ewing sarcoma of the rib, Levine and Levine (Citation1983) concluded that “chest radiography usually demonstrates a rib lesion, often with an adjacent extra pleural, soft tissue mass”. In our series, however, a tumor was suspected in only 4 of the 15 radiographs taken at the first visit. In 4 patients, the chest radiographs were considered normal. The doctor might hesitate to order new radiographs shortly after the first examination has been interpreted as being normal.
Both patient's and doctor's delay were around 2–3 months, which is consistent with the findings of previous studies (Pollock et al Citation1991). The extent to which delay influences outcome is controversial, but is an important issue—not least in claims of malpractice (Spurgeon et al. Citation2000). In our study 5 patients had metastasis at the time of diagnosis, and 4 of these died from the Ewing sarcoma. Doctor's delay tended to be longer in these 5 patients, but the difference was not significant.
Doctor's delay exceeded 7 months for 4 patients. None of these individuals had had a chest radiograph at the first visit, and all of them had recurrent disease. In 2, there was local recurrence, and the other 2 developed metastases. The initial course of Ewing sarcoma of the rib was not steadily progressive— and in some cases intermittent—thereby misleading both doctor and patient and resulting in a longer delay. Besides delay, misdiagnosis by the doctor is also an issue. In Sweden, centralization of centers for the treatment of sarcoma is widely accepted by the medical community. The finding that many patients were operated outwith a center was due to the fact that the correct diagnosis was not made preoperatively. Thus, wide surgical mar gins were more frequent for those operated in sarcoma centers than in those treated in the other 11 hospitals.
In contrast to most published reports of Ewing sarcoma of the rib, this was a population-based study covering all patients diagnosed in Sweden over a 20-year period. Initial symptoms of Ewing sarcoma of the rib were chest pain. The most important clinical finding was a palpable mass and pleural effusion—findings that must always be followed up. Primary bone malignancies are rare; thus, centralization not only of treatment but also of the diagnostic process might give a more favorable prognosis.
Contributions of authors
The study was initiated by BW and TW. BW collected the patient data and wrote the first manuscript draft. All authors contributed to data analysis and writing of the final manuscript.
- Gladish G W, Sabloff B M, Munden R F. Primary thoracic sarcomas. Radiographics 2002; 22: 621–37
- Grier H E. The Ewing family of tumors: Ewing's sarcoma and primitive neuroectodermal tumors. Pediatric Clin North Am 1997; 44: 991–1004
- Kocis K C. Chest pain in pediatrics. Pediatric Clin North Am 1999; 46: 189–203
- Levine E, Levine C. Ewing tumor of the rib: radiologic findings and computed tomography contribution. Skeletal Radiol 1983; 9: 227–33
- Pollock B H, Krischer J P, Vietti T J. Interval between symptom onset and diagnosis of pediatric solid tumors. Journal of Pediatrics 1991; 119: 725–32
- Saenz N C, Hass D J, Meyers P, Wollner N, Gollamudi S, Bains M, LaQuaglia M P. Pediatric chest wall Ewing's sarcoma. J Pediatr Surg 2000; 35: 550–5
- Selbst S M, Ruddy R M, Clark B J, Henretig F M, Santulli T, Jr. Pediatric chest pain: a prospective study. Pediatrics 1988; 82: 319–23
- Spurgeon P, Barwell F, Kerr D. Waiting time for patients in England after general practioners’ referrals: retrospective national survey. BMJ 2000; 320: 838–39