Abstract
Background Femoral component neck fracture is an uncommon type of failure in total hip arthroplasty. We present a report on 4 retrieved cobalt-chrome femoral components that fractured at the neck, where we investigated the mechanisms of failure.
Methods The 4 retrieved implants were analyzed with regard to their macro- and microstructures and the fracture surfaces were examined using electron microscopy. The medical record of each patient was also examined for any history of complications prior to failure of the implant.
Results These fractures occurred immediately adjacent to the base of the modular head. Skirted modular heads were used in 3 of the 4 failed components. This constructs promotes corrosion. Cyclic fatigue-loading in combination with the material factors of course grain microstructure and extensive carbide precipitation along the grain boundaries were also identified as the cause of implant failure.
Interpretation Our findings suggest that a solution annealing step could be introduced into the manufacturing process to improve the microstructure of the cobalt chrome alloy. We also advise caution in using a skirted modular head in combination with a device of known suboptimum microstructure, for a greater margin of safety.
Fracture of the femoral component is an infrequent but significant complication of total hip arthroplasty. The reported incidence of stem fracture ranges from 0.2% to 11%, with material fatigue being a common mode of failure typically associated with stem loosening (Charnley Citation1975, Ducheyne et al. Citation1975, Galante et al. Citation1975, Collis Citation1977, Wroblewski Citation1982, Amstutz et al. Citation1990, Dall et al. Citation1993).
Stem fracture is a very rare event, particularly with the use of modern high-strength materials including cobalt-chromium alloys. There have been several reports of cobalt chromium stem failures at the neck region distal to the taper (Gilbert et al. Citation1994, Vatani et al, Citation2002), within the modular femoral head (Botti et al. Citation2005), and also in the stem (Della Valle et al. Citation2005). Failure in the femoral neck region has been reported to be due to mechanical properties of the material, corrosion, fatigue, and suboptimal design (Gilbert et al. Citation1994, Vatani et al, Citation2002, Botti et al. Citation2005). In the present case study, we report 4 uncemented Omnifit femoral components (Osteonics, Allandale, NJ) that fractured in an area adjacent to the junction of the modular femoral head/neck. To our knowledge, this is the largest series of femoral component neck fractures of this stem.
Patients and methods
4 patients who underwent uncemented total hip arthroplasty for osteoarthritis of the hip presented with fracture of the femoral component between 1999 and 2005. The time the implants had been in situ ranged from 10 to 17 years. 2 of the patients had had no complications prior to failure of the implant. 1 patient had suffered recurrent dislocations necessitating revision of the acetabular liner and a change of the modular femoral head 3 years after the primary hip replacement. In the other patient, repeated dislocations had been treated with revision of the acetabular liner. This revision procedure was further complicated by infection, which was treated with washouts and antibiotics. This same patient had had 2 further revision procedures for aseptic loosening of the acetabular component prior to failure of the femoral stem ().
Summary and profile of each case
All of the fractured devices were routinely recorded via the Royal Perth Hospital (RPH) Implant Tracking protocol. Similar devices with skirted heads were obtained from the RPH retrieval collection for comparison. Patient records were reviewed during the investigation.
Examination of the fractured stems included identification of the operative failure mechanisms, macroanalysis of the retrieved components by stereomicroscopy (Leica MZ6; Leica, Oberkochen/Wurttemburg, Germany), scanning electron microscopy of the fracture surfaces (Cam-Scan CS3200; CamScan, Cambridge, UK) and microstructural analysis (Leitz Orthoplan; Leica, Oberkochen/Wurttemburg, Germany).
Results
3 of the 4 fractured devices had skirted modular heads. In all cases, the fractures had occurred immediately adjacent to the base of the modular head (). Both surfaces of the taper of head and neck showed evidence of crevices and inter-granular corrosion.
Figure 1. Macrophotograph of fractured stem. Insert shows surface of fracture.

All the fractures had started at the superior tensile surface of the neck adjacent to the femoral head stem junction (). Fractography with scanning electron microscopy revealed that the ultimate cause of failure had been initiated by intergranu-lar corrosion, crack growth through fatigue, and catastrophic failure subsequent to tensile overload. Microstructural analysis revealed a course grain structure with grain sizes up to 8 mm in length (ASTM E1 12–96, Citation2004) and the presence of grain boundary carbide precipitates ( and ).
Figure 2. Intergranular cracking on the superior tensile surface of the trunnion. Note the large grains.

Figure 3. Extensive carbide precipitation at the grain boundary.
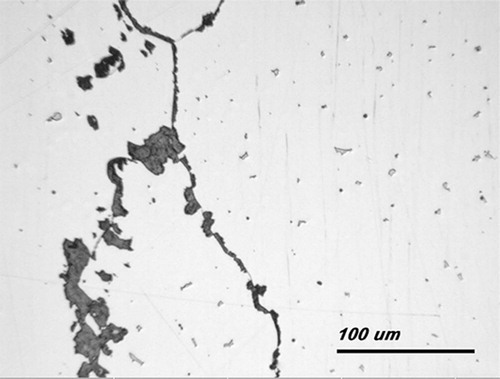
Figure 4. Macrostructure of a cross section taken through the neck of a fractured stem. Note the large grains and the presence of precipitates at the grain boundaries.

Discussion
There have been several case reports of femoral components failing from fracture at the region of the neck caused by corrosion at the morse taper (Gilbert et al. Citation1994), design faults (Vatani et al. Citation2002), laser etching (Lee and Kim Citation2001), or material factors (Aspenberg et al. Citation1987). In addition, patient factors such as weight, body mass index, activity levels, and traumatic incidents have been implicated in failures of this type (Charnley Citation1975, Wroblewski Citation1982, Vatani et al. Citation2002).
In 3 of our 4 cases, the modular femoral heads used were skirted. Inspection of the tapered surfaces revealed intergranular and crevice corrosion. Skirted heads present a geometrical construct that promotes crevice corrosion via a mechanism of oxygen depletion. The microenvironment of the taper interface becomes locally depleted of oxygen and breakdown of the oxide-passive (Cr2O3) layer that imparts corrosion resistance occurs. In our cases, this subsequently led to the initiation of intergranular corrosion. We observed an almost complete network of intergranular cracking on the superior, tensile surface of the trunnion in 3 of the 4 femoral components matched with skirted modular heads. Furthermore, 2 other devices in our retrieval collection of Omnifit stems (n = 53) had advanced intergranular corrosion and fatigue cracking, but they had not fractured and were revised for other reasons prior to catastrophic failure. The remainder of the devices with non-skirted femoral heads in our collection showed varying degrees of corrosion; however, none had advanced intergranular corrosion/cracking. Our finding is consistent with laboratory studies that have shown that head and neck extensions are associated with increased susceptibility to corrosion (Lieberman et al. Citation1994, Brown et al. Citation1995).
Poor microstructures, featuring extensive carbide precipitation at the grain boundaries, have been implicated in the fracture of cobalt-chrome devices (Swarts et al. Citation2001). Carbide distribution is important in the failure of cobalt-chrome stems in at least three ways. Firstly, carbides may act as crack-like discontinuities on the surface of the stem. Secondly, they present an easy crack path. Finally, and most importantly in the present failures, is the concentration of carbon in the carbides—which has an effect on the localized corrosion potential, leading to preferential attack at the grain boundaries and inter-dentritic regions where the carbides precipitate.
Suboptimal macro- and microstructure of the implants also predisposed them to failure. Macro-scopically, we found that the grain size was large. Grain size is a factor that has a direct effect on the fatigue life of an orthopedic device. In general terms, the larger the grain size, the lower the materials yield and fatigue strength. Microscopically, the extensive carbide precipitates along the grain boundaries also predispose the device to failure.
Patient factors may also have contributed to implant failure. 2 of the patients were obese with BMIs greater than 30; however, a recent study (McLaughlin and Lee Citation2006) has demonstrated little clinical or radiographical effect with patients > 30 kg/m2 compared to non-obese patients of < 30 kg/m2. One of our patients had a single revision procedure whilst another had 3 revision procedures where the femoral trunnion may have been damaged. In these cases, it would have been even more important to have an optimum microstructure to resist crack initiation and failure.
The mechanism of failure for all of these implants was tensile overload with crack propagation caused by fatigue crack initiation via a combined crevice/ intergranular corrosion mechanism. A suboptimum microstructure contributed to ultimate failure.
This report is the largest series of fractures in the neck region of uncemented cobalt-alloy femoral components that we are aware of. In light of our findings, attention should be paid to the manufacturing process—as we believe that the structure of the device could be improved by introducing a solution-annealing step that would help to prevent intergranular carbide precipitation. We also advise caution when using a skirted head in combination with a device of suboptimal microstructure.
No competing interests declared.
Contributions of authors
LL: data collection and review, manuscript writing and preparation, and review of the literature. KS: Initiator of project and supervisor. AK: Failure analysis of implants, metallurgical analysis, and manuscript writing. ES: Laboratory analysis of implants and preparation of digital illustrations.
- Amstutz H C, Yao J, Markolf K, Dorey F. Stem fracture incidence in Trapezoidal-28 stainless steel hip arthroplasty. Clin Orthop 1990, 256: 105–14
- Aspenberg P, Kolmert L, Person L, Onnerfalt R. Fracture of hip prosthesis due to inadequate welding. Acta Orthop Scand 1987; 58: 479–82
- ASTM E1 12–96 (2004). Standard test methods for determining average grain size. 2004
- Botti T, Gent J, Martell J, Manning D. Trunion fracture of a fully porous-coated femoral stem. J Arthroplasty 2005; 20(7)943–5
- Brown S, Flemming C, Kawalec J. Fretting corrosion accelerates crevice corrosion of modular hip tapers. J Appl Biomater 1995; 6: 19–26
- Charnley J. Fracture of femoral prostheses in total hip replacement. A clinical study. Clin Orthop 1975, 111: 105–20
- Collis D K. Femoral stem failure in total hip replacement. J Bone Joint Surg (Am) 1977; 8: 1033–41
- Dall D M, Learmonth I D, Solomon M I, Miles A W, Davenport J M. Fracture and loosening of Charnley femoral stems. J Bone Joint Surg (Br) 1993; 75: 259–65
- Della Valle A, Becksac B, Anderson J. Late fatigue fracture of a modern cemented forged cobalt chrome stem for total hip arthroplasty. J Arthroplasty 2005; 20(8)1084–8
- Ducheyne P, De Meester P, Aernoudt E, Martens M, Mulier J C. Fatigue failure of the femoral component of Charnley and Charnley-Muller type total hip prostheses. J Biomed Mater Res Symp 1975; 6: 199–219
- Galante J O, Rostoker W, Doyle J M. Failed femoral stems in total hip prostheses. J Bone Joint Surg (A) 1975; 57: 230–6
- Gilbert J, Buckley C, Jacobs J. Intergranular corrosion-fatigue failure of cobalt-alloy femoral stems. A failure analysis of two implants. J Bone Joint Surg (Am) 1994; 76: 110–115
- Lee G W, Kim H T. Early fatigue failures of cemented, forged, cobalt-chromium femoral stems at the neck-shoulder junction. J Arthroplasty 2001; 16: 236
- Lieberman J, Rimnac C, Garvin K. An analysis of the head-neck taper interface in retrieved hip prostheses. Clin Orthop 1994, 300: 162–7
- McLaughlin J R, Lee K R. The outcome of total hip replacement in obese and non-obese patients at 10- to 18-years. J Bone Joint Surg (Br) 2006; 88: 1286–92
- Swarts E, Miller S, Keogh C V. Lim G, Beaver R. Fractured Whiteside Ortholoc II knee components. J Arthroplasty 2001; 16(7)927–34
- Vatani N, Comando D, Acuna J. Faulty design increases the risk of neck fracture in a hip prosthesis. Acta Orthop Scand 2002; 73(5)513–7
- Wroblewski B M. Fractured stem in total hip replacement. Acta Orthop Scand 1982; 53: 279–84