Abstract
Background and purpose The outcome of clubfoot treatment is the result of several factors such as severity, type of treatment, and measurement instruments. We compared two intervention groups with two assessment procedures.
Patients and methods 16 children were treated consecutively with intensive stretching according to the Copenhagen method and 16 children consecutively with casting according to the Ponseti technique, during their first 2 months of age. The need for surgery was then assessed. At 4 months of age, all children used a dynamic Knee Ankle Foot Orthosis. The Clubfoot Assessment Protocol (CAP) and the Dimeglio Classification System (DCS) were used and compared during treatment and at 2 years of age.
Results According to the CAP (but not the DCS) the casting technique was superior in clubfoot correction, apparent as better mobility and better quality of motion at 2 years of age. These children also required less surgery. The orthotics management functioned well in both groups, with high compliance and maintenance or slight improvement of the clinical status except for morphology. DCS score changed over time but not between the groups. Because of its multidimensional and narrower scoring interval construct, the CAP enabled us to elucidate and evaluate different clinical functions.
Interpretation The casting technique according to Ponseti seems to be the better of the two for clubfoot correction, regarding mobility and quality of motion. The Clubfoot Assessment Protocol (but not the Dimeglio Classification System) was able to reveal differences between the Copenhagen and Ponseti treatment methods.
Treatment of clubfoot is not only a question of initial correction of the deformity; correct surgical decision and orthotic management are important parts of the treatment concept.
A prerequisite for comparison of different treatment protocols is that certain factors such as the initial severity of the deformity and compliance with orthosis treatment are controlled (Dimeglio et al. Citation1995, Ippolito et al. Citation2003, Lehman et al. Citation2003, Dobbs et al. Citation2004, Morcuende et al. Citation2004, Scher et al. Citation2004, Thacker et al. Citation2005). Furthermore, assessment instruments used in clinical studies should have documented reliability and validity, ensuring that these instruments have acceptable methodological quality. Our own literature search on clubfoot instruments using Medline showed that there have been very few studies focusing on reliability and validation (Maffulli et al. Citation1997, Flynn et al. Citation1998, Roye et al. Citation2001, Wainwright et al. Citation2002, Andriesse et al. Citation2005, Celebi et al. Citation2006, Munshi et al. Citation2006, Andriesse et al. Citation2006). This is still an area in need of further development.
The present study is the first part of a longitudinal follow-up of clubfoot treatment with the use of the Clubfoot Assessment Protocol (CAP) (Andriesse et al. Citation2005). The first objective was to compare the 2-year outcome for the Copenhagen stretching method with that for casting techniques according to Ponseti, the treatment period being the first 2 months after birth. The second objective was to evaluate the effects of surgery and orthotic management. The third objective was to compare CAP measurement with the Dimeglio Classification System (DCS).
Patients and methods
Design, subjects, and treatment program
At our department, we had previously treated children with clubfoot according to a modified Copenhagen method (Reimann Citation1962). In January 2001, we started using the casting technique according to Ponseti (Citation1996). To keep research conditions stable, only the first 2-month period of our treatment procedure was changed, which we refer to as phase I: initial correction. Thereafter phase II, maintenance of correction, was started with orthosis treatment. shows a summary of the research design.
Figure 1. Summary of treatment interventions and assessment points.
32 children were included in the study; the last 16 children (6 girls) were treated with the modified Copenhagen method (CPH, 22 feet, 6 bilateral) and the first 16 (4 girls) were treated with the casting technique according to Ponseti (PCT, 23 feet, 7 bilateral). The inclusion criterion was idiopathic congenital clubfoot.
Modified Copenhagen group (CPH-G): During weekdays, daily mobilization (stretching of all shortened soft tissue and manipulation of contract joints) was done by an experienced physiotherapist. This was done by starting with the contract forefoot and systematically working backwards to the hind foot varus, and lastly mobilization of the equinus. Weakened muscles were stimulated manually by triggering spontaneous movement. Parents were trained in a home stretching program to be performed twice a day. The correction obtained was maintained with the use of a splint made of Plexidur (). Total hospital treatment time—excluding travel—was approximately 10 hours a week and the home treatment program was 10 hours a week.
Figure 2. Splint made of Plexidur, which can be remolded as the foot is successively corrected by the stretching and manipulation treatment.

Ponseti casting technique group (PCT-G): During the first 2 weeks of treatment, casts were changed every 5 days, and thereafter once a week until the age of 2 months. The guidelines described by Morcuende et al. (Citation2005) were followed. Total hospital treatment time was 2–4 hours a week.
All children started their treatment within 8 days after birth. In both groups, operation (if necessary) was performed at the age of 2 months, followed by over-the-knee castings for 3–5 weeks.
Criteria for surgery and types of intervention were as follows. (1) A remaining isolated equinus position of less than 5° dorsiflexion was treated with percutaneous Achilles tendon lengthening, if necessary in combination with posterior capsulot-omy. (2) A varus-adductus (inversion) component less than 15° mobile into valgus-abduction (eversion) was treated with tibialis posterior lengthening and capsulotomy of the talo-navicular joint. (3) Remaining toe-flexion was treated with lengthening of flexor hallucis longus and/or flexor digito-rum tendon.
The treatment goal for phase I was a foot with at least 15° dorsiflexion and more than 15° eversion.
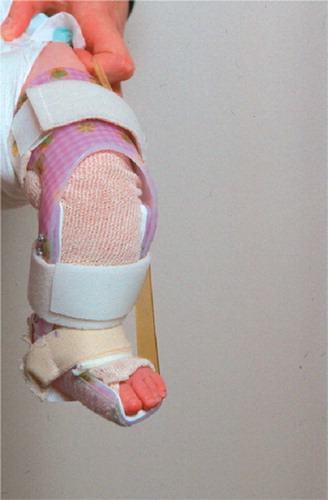
Postoperatively, or at 2 months of age if no operation was needed, the children continued their treatment with an individually made dynamic Knee Ankle Foot Orthosis (KAFO) (). The foot part was positioned in outward rotation, related to the eversion of the foot obtained. The flexed knee part inhibited rotation at the knee and hip level, and fixed the foot in the orthosis. The dynamic construction (hinged ankle joint and elastic band) of the KAFO (and later on the Ankle Foot Orthosis (AFO)) makes it possible to keep the Achilles tendon lightly stretched during the night. The elastic band was kept loose during the day, enabling the foot to move freely in plantar and dorsal flexion. This orthosis was used according to a standardized schedule during the first 2 months of phase II (at least 18 hours a day: the whole night and no more than 2 hours free in the morning and in the afternoon and before bedtime). Regular follow-ups were done by an experienced physiotherapist, to ensure that the parents felt comfortable with using the orthosis and making adjustments. A home program was initiated to keep plantar flexion and toe flexors mobile and to stimulate muscle function and mobility through playful activities. Gradually, based on the muscle function and mobility status of the club-foot and the motor development of the child, use of the orthosis during the day was cut down. By the age of 8 months, all the children used the orthosis for 12 hours at night and during their midday nap. Once the child had achieved a stable independent walk, the KAFO was changed to a dynamic Ankle Foot Orthosis (AFO). Outward rotation of the foot was normally maintained around 15°. Compliance was set to a minimum of 10 hours a night. This was continued until the age of 4 years. Generally, no orthopedic shoes were prescribed.
Figure 3. The dynamic Knee Ankle Foot Orthosis (KAFO, with permission from Scandinavian Orthopaedic Technical Laboratory).
All operating procedures were performed by two experienced pediatric orthopedic surgeons. Stretching and manipulation treatment was done by an experienced physiotherapist. The castings were done by the same pediatric orthopedic surgeons and the physiotherapist. The orthoses were made by two technicians who were well acquainted with clubfoot dynamics.
Assessment instruments
All children in both groups were assessed consecutively and prospectively by the same assessor (HA) when they were newborn (before treatment started), at 1 month, 2 months (preoperatively), 4 months (postoperatively), and at the age of 2 years.
Clubfoot Assessment Protocol (CAP). In previous studies, the CAP has been shown to have moderate-to-good reliability and to be valid for use in follow-up of clubfoot (Andriesse et al. Citation2005, Citation2006).
20 items divided into body/function structures (4 domains) and activity levels (two domains) according to the International Classification of Function, Disability and Health (ICF, World Health Organization Citation2000) form the CAP (). This protocol is intended for use in clinical practice, in research, and in short- and long-term follow-up. The focus is on item and subgroup levels, and total scores are not used.
Table 1. A summary of the Clubfoot Assessment Protocol (CAP)
Dimeglio classification system (DCS). This instrument was originally developed for classification (Dimeglio et al. Citation1995) but it is also often used in follow-up studies (Lehman et al. Citation2003, Dobbs et al. Citation2004, Souchet et al. Citation2004, Zeifang et al. Citation2005). It mainly assesses the mobility of the clubfoot and corresponds to the CAP Mobility I domain. Reliability has been judged to be sufficient (Flynn et al. Citation1998). The DCS consists of 8 items (). One item concerns general muscle function. It focuses on total score and classification: mild, (0–5), moderate (6–10), severe (11–15), and rigid (16–20).
Table 2. A summary of the Dimeglio classification scoring system
The raw scores from both instruments were transformed into percentage score (0–100, worst to best possible score).
Surgery and orthoses. Operation type and frequency were registered. Compliance regarding orthosis usage was checked through direct communication with the parents and from the amount of wear and tear on the orthosis.
Statistics
In children with bilateral clubfoot, each foot was used as an independent observation in the statistical analysis. Nonparametric methods were used due to a skewed and asymmetric data distribution (in general) and due to data being based on summarizing ordinal scores. The Mann-Whitney U test was used for between-group comparisons. The Wil-coxon signed rank test was used for within-group comparisons. Median and 95% confidence interval are shown. A p-value of < 0.05 was regarded as statistically significant.
Results
Missing data
In the PCT-G (23 feet), 2 assessments were missing in CAP Morphology and 2 in CAP Muscle function at 2 months. In the CPH-G (22 feet), two assessments were missing in CAP Mobility 2 and four in CAP Muscle function at 2 months, and also 4 in CAP Morphology at 4 months. The item "“.soleus/gastrocnemius” in CAP Muscle function could only be tested properly in 24 of 45 children. This item was therefore excluded in this study.
Surgery
In the PCT-G, 5 feet were not operated, 4 were operated with posteromedial release including Achilles lengthening, and 14 were operated with Achilles lengthening only. In the CPH-G, 2 feet were not operated, 17 were operated with posteromedial release including Achilles lengthening, and 3 had Achilles lengthening only.
Orthosis management
All children complied with the KAFO orthosis treatment. During AFO orthosis treatment, 2 children (1 unilateral and 1 bilateral) in the PCT-G and 1 child (bilateral) in the CPH-G were non-compliant. For the PCT-G, the KAFO foot outward rotation ranged from 25° to 35° and for the CPH-G it ranged from 15° to 25°.
Clinical assessment
At baseline (i.e. shortly after birth), no statistically significant differences were found for the CAP domains Mobility I, Muscle function, Morphology, or the DCS (). CAP Mobility II (length of toe flexors) was worse (p = 0.03) in the PCT-G. Using DCS, the PCT-G (23 feet) had 16 feet classified as moderate (median 9, range 8–10) and 7 as severe (12, range 11–13). The CPH-G (22 feet) had 14 feet classified as moderate (9, range 7–10) and 8 as severe (12, range 12–14). No statistically significant differences were found at baseline between the two treatment groups and their severity classification.
Table 3. The median and 95 % confidence interval (CI) at five different assessment occasions for the Ponseti casting technique group (PCT) and Copenhagen stretchning treatment group (CPH)
At the beginning of the maintenance phase (4 months of age), no statistically significant differences were found between the CPH-G and PCT-G in either the CAP or the DCS ().
Mobility
The CAP Mobility I () showed higher scores (p = 0.02) at 1 month for the PCT-G than for the CPH-G, indicating a faster initials correction effect. Between the first and second month, the CPH-G caught up with the PCT-G and leveled out. The surgical intervention at the age of 2 months had good effect in both groups, shown as a steep incline of scores (p < 0.01 for both groups) at the age of 4 months. Towards the age of 2 years and after the initiation of orthosis treatment, the mobility seemed stable for the CPH-G compared to the situation post-operatively (p = 0.8), but improved for the PCT-G (p = 0.03), causing a difference in mobility between the CPH-G and PCT-G (p = 0.008).
The DCS showed no statistically significant differences in mobility for CPH-G or PCT-G during the first 2 years of treatment (). Both groups showed an increase in mobility after initiation of orthosis (p = 0.001 for both groups).
CAP Mobility II (toe flexors) had a lower score (p = 0.03) at baseline for the PCT-G, which changed during treatment into a better score for this group at the age of 2 months (p = 0.02) (). Improvement was also seen after surgical intervention in the CPH-G at the age of 4 months (p = 0.05) (). During orthosis treatment, no change was seen up to 2 years of age.
Muscle function
Muscle function (evertor muscles) in the PCT-G improved faster during the first 2 months, and showed a better status than the children in the CPH-G at the age of two months (p = 0.05). After surgical intervention at the age of 4 months, the muscle function in the CPH-G had leveled out (p = 0.5). After beginning orthosis, improvement was seen for the CPH-G towards the age of two years, thus leveling out the difference between the two groups.
Morphology
After 1 and 2 months of treatment, the PCT-G showed higher scores (p = 0.001 and 0.05, respectively) than the CPH-G. After surgical intervention and at the age of 4 months, the CPH-G status increased almost significantly (p = 0.05), leveling out with the PCT-G. During orthosis treatment, a decrease of the scores was noticeable in both groups (p = 0.05 for PCT-G, p = 0.02 for CPH-G) and no difference was found between these two groups at the age of 2 years (p = 0.4).
Quality of motion
Assessment of motion quality is not appropriate before the age of 2 years. At this age, a better quality of motion (running and walking) was seen in the PCT-G relative to the CPH-G (p = 0.03). This implies fewer problems with intoeing, initial contact in stance, lateral loading, and toe-off.
Discussion
The serial casting according to the Ponseti technique showed better results than the intensive stretching according to the Copenhagen method, as measured with the CAP. There were better outcomes in 3 of 4 CAP domains preoperatively and at 2 months of age, and less invasive surgery was needed. At the age of 2 years, the scores for mobility and quality of motion assessed by the CAP were in favor of the PCT-G.
The DCS showed change over time for both groups, but was not sensitive enough to reveal differences between the groups.
It seems confusing that preoperatively there was no significant difference in CAP Mobility I () and at the same time more surgery was needed in the CPH-G. Analysis of the individual scores showed that the items dorsal flexion, hindfoot varus/ valgus, and foot abduction differed systematically between the groups. In contrast to the PCT-G, the CPH-G had higher scores on dorsal flexion and lower scores on abduction and varus/valgus. This explains the similar scores in CAP Mobility 1, concomitant with the more extensive surgery required in the CPH-G. These mobility results are mainly caused by the fact that the Copenhagen stretching treatment concentrates more on the dorsal flexion compared to the Ponseti casting technique, and less on overcorrection of foot eversion.
In spite of the intensive manual stimulation of muscles in the CPH-G, this did not result in better function. It seems that increased mobility had a greater effect on muscle function. At 2 years, quality of motion (running and walking) was significantly better for the PCT-treated children. Two possible explanations may be that the motion difference is caused by better mobility or by the fact that the proprioceptive nerve system is intact because of less disturbance from surgery.
Several recent studies have shown that the Ponseti treatment gives a faster treatment effect and less surgical interventions (Herzenberg et al. Citation2002, Ippolito et al. Citation2003, Lehman at al. Citation2003, Morcuende et al. Citation2004, 2005, Segev et al. Citation2005). Our study confirms these observations. Less pain, better mobility, and higher function are seen in the long-term outcome (Cooper and Dietz Citation1995, Ippolito et al. Citation2003, Dobbs et al. Citation2006) as compared to extensive soft tissue release (Aronson and Puskarich Citation1990). In the future, we hope to evaluate these two groups in an extended prospective study in which external factors such as severity at baseline, surgery, and orthotic management are controlled and performed with properly tested assessment tools.
The orthotics management functioned well in both groups, with high compliance and maintenance of–or slight improvement in–the clinical status except for CAP Morphology. Problems have been reported concerning acceptance of the Foot Abduction Orthosis (FAO) used in the Ponseti method (Lehman et al. Citation2003, Dobbs et al. Citation2004, Thacker et al. Citation2005, Abdelgawad et al. Citation2007). Non-compliance with orthotics management increases the risk of recurrences (Lehman et al. Citation2003, Dobbs et al. Citation2004, Morcuende et al. Citation2004, Thacker et al. Citation2005, Abdelgawad et al. Citation2007).
Our KAFO/AFO management maintained or improved most of the mobility function items at the age of 2 years in both treatment groups. The difference found at 2 years for CAP Mobility I was caused by a decrease in plantar flexion in the CPH-G. Herzenberg et al. (Citation2002) showed the same tendency in clubfeet operated with extensive surgery. Dorsiflexion increased in both groups, however, improving the scoring for the PCT-G. The DCS does not contain plantar flexion, which resulted in improvement in both groups. Thacker et al. (Citation2005) showed the same tendency for improvement of mobility after initiation of the FAO in their compliant group. Miura et al. (Citation2005), who included a control group, also showed that hinged ankle-foot orthoses had a positive effect on ankle function without loss of correction.
The CAP Morphology domain had deteriorated close to the age of 2 years in both groups. Analysis of this domain at the item level showed that this decrease was mainly caused by an increase in the tibial rotation score. Earlier studies have shown that there is a variation in leg torsion in children with clubfoot (Cuevas de Alba et al. Citation1998, Reikeras et al. Citation2001), which is important in order to be able to distinguish from other causes of in-toeing. Ponseti's FAO is set to a recommended 70° of outward rotation, in contrast to our KAFO's 25° in the PCT-G. It should, however, be pointed out that in the FAO, part of the rotation might be compensated for at the level of the hip and knee joint–which is not the case in the KAFO. Whether the amount of outward rotation of the orthosis influences tibial rotation and increases out-toeing is still an unanswered question.
The CAP appears to be more sensitive to differences than the DCS. This is partly caused by the scaling construct of the instruments, with wider intervals in the DCS. This enhances reliability but reduces sensitivity to change. The interval construct of the CAP is weighted and based on its clinical relevance. Thus, the findings are also clinically valid. The minimal detectable change related to subjective, patient-rated change is another step to be made in the development of the CAP. Furthermore, the CAP's multidimensional construct and the use of domain scores rather then a total score provides us with more detailed clinical information. An instrument that is more sensitive to change means that less numbers are needed in studies and more subtle but relevant details for treatment evaluation can be extracted.
Our study has some limitations. The children included in the PCT-G were the first cohort to be treated at our department. The results of the PCT-G could perhaps have been even better than shown with this material if we had had more experience.
The main argument against the validity of the study is that the assessor was not blinded and even took active part in treatment. However, the assessment procedure was standardized and there was no particular interest in achieving any specific result.
Randomized controlled trial studies in children born with clubfoot are difficult to perform. A thorough database of our own with standardized assessment procedures had been started years before we changed our clubfoot treatment in 2001. This made it possible for us to check baseline status between the two study groups. The referral process and catchment areas were not changed during the study. Together with keeping external conditions stable and follow-ups at the same standard age, we kept research conditions as stable as possible.
The feet of children with bilateral clubfeet were used as independent observations in the statistical analysis. There is a risk that there may be some correlation between the results from different feet of the same patient, causing overestimation or underestimation of the treatment effect. As both treatment groups had almost equal distribution of unilateral and bilateral clubfeet (6 and 7, respectively) and orthosis compliance, we consider that this statistical problem would have had a minor effect on the outcome. Lastly, the risk of type II error exists due to low numbers, and this must be taken into account.
In conclusion, the casting technique according to Ponseti appears to be the method of choice in clubfoot correction, in terms of mobility and quality of motion. The Clubfoot Assessment Protocol (but not the Dimeglio classification system instrument) made it possible to evaluate and compare interventions. Future studies should focus on the orthosis construct, its clinical effects, and factors influencing compliance.
The study was supported by the Medical Faculty of Lund University, Sweden. Special thanks to Per-Erik Isberg, Department of Statistics, Lund University, for statistical advice.
No competing interests declared.
Contributions of authors
HA designed the study, collected and analyzed data, and wrote the draft manuscript. GH also designed the study and revised the manuscript.
- Abdelgawad A A, Lehman W B, van Boss H J, Scher D M, Sala D A. Treatment of idiopathic clubfoot using the Ponseti method: minimum 2-year follow-up. J Pediatr Orthop B 2007; 16(2)98–105
- Andriesse H, Hägglund G, Jarnlo G B. The clubfoot assessment protocol (CAP); description and reliability of a structured multi-level instrument for follow-up. BMC Musculoskeletal Disorders 2005; 6: 40
- Andriesse H, Roos E M, Hägglund G, Jarnlo G B. Validity and responsiveness of the Clubfoot Assessment Protocol (CAP). A methodological study. BMC Musculoskeletal Disorders 2006; 7: 28
- Aronson J, Puskarich C L. Deformity and disability from treated clubfoot. J Pediatr Orthop 1990; 10(1)109–19
- Celebi L, Mratli H H, Aksahin E, Yagmurlu M F, Bicimo-glu A. Bensahel et al. and the International Clubfoot Study Group evaluation of treated clubfoot: assessment of interobserver and intraobserver reliability. J Pediatr Orthop B 2006; 15(1)34–6
- Cooper D M, Dietz F R. Treatment of idiopathic clubfoot. A thirty-year follow-up note. J Bone Joint Surg (Am) 1995; 77(10)1477–89
- Cuevas de Alba C, Guille J T, Bowen J R, Harcke H T. Computed tomography for femoral and tibial torsion in children with clubfoot. Clin Orthop 1998, 353: 203–9
- Dimeglio A, Bensahel H, Souchet P, Mazeau P, Bonnet F. Classification of clubfoot. J Pediatr Orthop 1995; 4: 129–36
- Dobbs M B, Rudzki J R, Purcell D B, Welton T, Porter K R, Gurnett C A. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic club-feet. J Bone Joint Surg (Am) 2004; 86(1)22–7
- Dobbs M B, Nunley R, Schoenecker P L. Long-term follow-up of patients with clubfeet treated with extensive soft-tissue release. J Bone Joint Surg (Am) 2006; 88: 986–96
- Flynn J M, Donoho M, Mackenzie W G. An independent assessment of two clubfoot classification systems. J Pedi-atr Orthop 1998; 18: 323–7
- Herzenberg J E, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop 2002; 22(4)517–21
- Ippolito E, Farsetti P, Caterini R, Tudisco C. Long-term comparative results in patients with congenital clubfoot treated with two different protocols. J Bone Joint Surg (Am) 2003; 85(7)1286–94
- Lehman W B, Mohaideen A, Madan S, Atar D, Feldman D S, Scher D. A method for the early evaluation of the Ponseti (Iowa) technique for the treatment of idiopathic clubfoot. J Pediatr Orthop B 2003; 12(2)133–40
- Maffulli N, Ken ward M G, Irwin A S, Porter R W. Assessment of late results of surgery in talipes equino-varus: a reliability study. Eur J Pediatr 1997; 156(4)317–9
- Miura Y, Kamegaya M, Saisu T, Mariya H. Effect of postoperative early ankle motion exercise using hinged ankle-foot orthoses in clubfoot. J Pediatr Orthop 2005; 25(4)529–32
- Morcuende J A, Dolan L A, Dietz F R, Ponseti, IV. Radical reduction in the rate of extensive corrective surgery using the Ponseti method. Pediatrics 2004; 113(2)376–80
- Morcuende J A, Abbasi D, Dolan L A, Ponseti V. Results of an accelerated Ponseti protocol for clubfoot. J Pediatr Orthop 2005; 25(5)623–6
- Munshi S, Varghese R A, Joseph B. Evaluation of outcome of treatment of congenital clubfoot. J Pediatr Orthop 2006; 26(5)664–72
- Ponseti I V. Congenital clubfoot. University Press, Oxford 1996
- Reikeras O, Kristiansen L P, Gunderson R, Steen H. Reduced tibial torsion in congenital clubfoot. Acta Orthop Scand 2001; 72(1)53–6
- Reimann I. Congenital idiopathic clubfoot. University of Copenhagen, Copenhagen 1962
- Roye B D, Vitale M G, Gelijns A C, Roye D P, Jr. Patient-based outcomes after clubfoot surgery. J Pediatric Orthop 2001; 21: 42–9
- Scher D M, Feldman D S, Van Bosse H J, Sala D A, Lehman W B. Predicting the need for tenotomy in the Ponseti method for correction of clubfeet. J Pediatr Orthop 2004; 24(4)349–52
- Segev E, Keret D, Lokiec F, Yavor A, Wientroub S, Ezra E, Hayek S. Early experience with the Ponseti method for the treatment of congenital idiopathic clubfoot. Isr Med Assoc J 2005; 7(5)307–10
- Souchet P, Bensahel H, Theman-Noel C, Pennecot G, Csu-koyi Z. Functional treatment of clubfoot: a new series of 350 idiopathic clubfeet with long term follow-up. J Pediatr Orthop B 2004; 13(3)189–96
- Thacker M M, Scher D M, Sala D A, van Bosse H J, Feldman D S, Lehman W B. Use of the foot abduction orthosis following Ponseti casts: is it essential?. J Pediatr Orthop 2005; 25(2)225–8
- Wainwright A M, Auld T, Benson M K, Theologis T N. The classification of congenital talipes equinovarus. J Bone Joint Surg (Br) 2002; 84: 1020–4
- World Health Organization: Classification, assessment, surveys and terminology team. ICIDH. Geneva Switzerland. Prefinal draft 2000. Full version
- Zeifang F, Carstens C, Schneider S, Thomsen M. Continuous passive motion versus immobilisation in a cast after surgical treatment of idiopathic clubfoot in infants. A prospective, blinded, randomised, clinical study. J Bone Joint Surg (Br) 2005; 87(12)1663–5