Abstract
Background and purpose Posttraumatic stiffness is a common complication of elbow injury and can result in considerable impairment in daily life. We assessed the outcome in 21 patients treated by a column procedure.
Patients and methods We followed 21 patients (average age 40 (10–76) years, 11 women) for 2 years after surgery for a stiff elbow. Range of motion (ROM) and function (EFA score) were measured preoperatively and at 3,12, and 24 months postoperatively.
Results Before surgery, the mean ROM was 69° (SD 24) and the mean EFA score was 74 (SD 13), which improved significantly to 104° (17) and 91 (6), respectively, after release. There were no significant differences between the postoperative measurements at 3,12, and 24 months. No neurovascular complications were noted; 2 patients developed periarticular ossifications postoperatively.
Interpretation A column procedure results in an increase in motion and functional scores at 2-year follow-up. Outcome at 3 months after treatment is the same as after 2 years.
Posttraumatic stiffness is a common complication of elbow injury and it can result in considerable impairment in daily life. Morrey et al. (Citation1985) stated that an elbow needs a minimal range of motion (ROM) of 100° of flexion/extension and 100° of pronation/supination to function adequately in daily life. Posttraumatic contractures can be classified into extrinsic (extra-articular) or intrinsic (intra-articu-lar) pathology. The exact etiology of contractures is poorly understood; immobilization resulting in adhesions seems to play a role (Trudel et al. Citation1998). Another study showed an increase in myofibro-blasts in the capsule of a posttraumatic elbow (Hildebrand et al. Citation2004).
When a supervised exercise programme and splinting (dynamic or static) fails, surgical treatment is indicated (Green and McCoy Citation1979). Surgical release can be performed using a lateral, a medial, an anterior or a posterior approach.
We assessed the outcome of surgical release using a column procedure in 21 patients.
Patients and methods
Between 2001 and 2004, 21 patients (average age 40 (10–76) years, 11 women) with posttraumatic contractures of the elbow that had resisted nonop-erative treatment were treated by surgical release (). Patients were operated on if they had a flexion contracture of at least 30° or a ROM of less than 100°. The articular surface had to be intact or healed. Patients with ulnaropathy that required release or transfer of the ulnar nerve and patients with calcifications in the medial collateral ligament that needed resection were excluded. All patients were operated on by the same surgeon using a column procedure under regional anesthesia with a long-acting axillary block. The time between surgical intervention and trauma varied from 1 to 28 years.
Table 1. Details of initial injury in the 21 patients
Statistics
Statistical analysis was performed using a paired Student's t-test. Differences were regarded as significant when p < 0.05. A two-tailed test was used in all cases.
Surgical technique and postoperative treatment
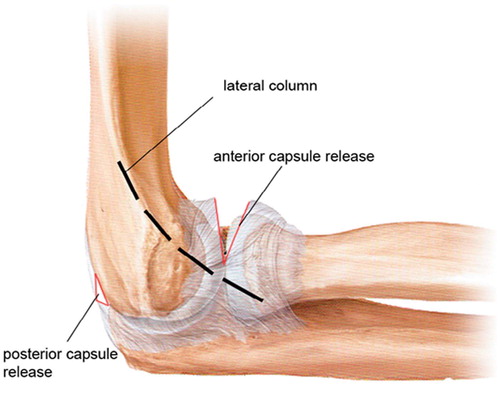
An incision is made supracondylar on the ridge of the humerus () and an arthrotomy is done by releasing the extensor carpi radialis longus. Using an anterior approach, the anterior capsule is released, and the coronoid process and coro-noid fossa are assessed and debrided. The same incision is used for a posterior capsular release. The triceps is elevated from the posterior aspect of the humerus, the posterior aspect of the capsule is released, and the olecranona fossa is cleaned of soft tissue (). Continuous passive motion device (CPM) was started within 2 h of surgery for a minimum of 12 h a day; during the night a dynamic extension splint was used. CPM was used for 48 h; the night splint was used for 3 months. The splint was fully extended. The patients were supervised twice a week by a physiotherapist for 6 months.
Figure 1. Column procedure with anterior and posterior capsule release.
Evaluation took place preoperatively and after 3, 12, and 24 months postoperatively using the visual analog scale (VAS) at rest and with activity, and also the "elbow function assessment" (EFA) (Morrey et al. Citation1985, de Boer et al. Citation1999).
Plain radiography and CT were performed on all patients preoperatively, and plain radiographs in two planes were taken 3 months and 1 year after surgery.
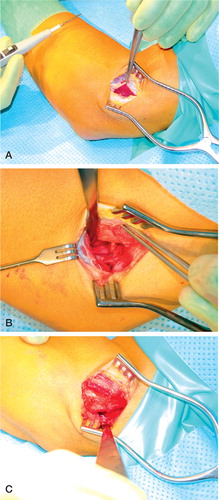
Figure 2. A.The lateral incision. B. Anterior capsule release. C. Posterior capsule release.
Results
There was a statistically significant improvement between the preoperative and postoperative ROM at 3 months from 69° to 104° (p < 0.05) ( and ). The mean EFA score showed a significant improvement, from 74 preoperatively to 91 postoperatively. No significant differences were found between the VAS scores or in the ROM for pro- and supination. The postoperative ROM and EFA scores at 3, 12, and 24 months were similar. 1 patient developed a postoperative contracture which needed another surgical release. The results of the final release were included in this study. No cause for the postoperative contracture could be found. 1 patient had a postoperative superficial infection of the incision wound, which was successfully treated with oral antibiotics. No vascular of neurological complications were noted. Radiographs showed small periarticular ossifications in the anterior capsule of 2 elbows at 1 year after surgery, which were not seen in the preoperative radiographs.
Figure 3. Range of motion (flexion-extension), showing a significant improvement 3 months after surgery. The functional outcome did not improve further after 1 and 2 years. The line in the box is the medial score; the box itself represents the standard deviation.
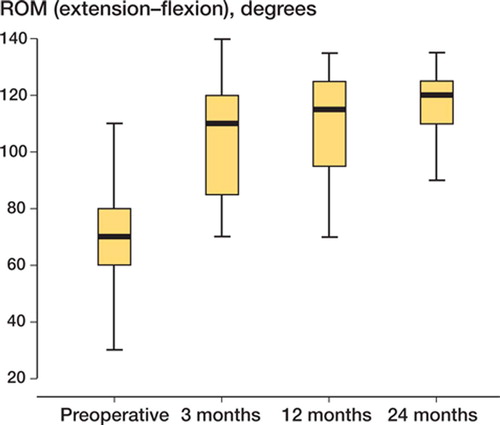
Table 2. Outcome
Discussion
Surgical release is indicated in stiff elbows when nonoperative treatment has failed and function is severely impaired. Previous reports of the results of surgical release have shown an overall improvement in ROM (Green and McCoy Citation1979, Mansat and Morrey Citation1998, Bruno et al. Citation2002, Park et al. Citation2004). Mansat and Morrey treated 38 elbows using a limited lateral approach to the anterior and posterior aspects of the capsule. The mean preoperative arc of flexion was 49°. At an average of 3 years postoperatively, the mean arc of flexion was 94°. The mean total gain was 45°. Marti et al. (Citation2002) performed a capsulectomy using a lateral approach on 23 elbows, and an additional medial approach was used on 24 elbows to excise ulnar adhesions and perform a more extensive capsulectomy. They achieved an improvement in ROM from 45° to 99°. Our results compare favorably with these reports.
Different surgical approaches have been described. The choice of type of approach is based on many factors such as the site of any previous incision, the presence of neuropathy, and the location of periarticular ossifications and intra-articu-lar deformities. The column procedure was first described by Mansat and Morrey in Citation1998. The advantage of this approach is the ability to see and treat both the anterior and posterior ulnohumeral and radiocapitellar joint through one incision, with preservation of the collateral ligaments. One disadvantage is that patients with an ulnar neuropathy or calcifications in the medial collateral ligament cannot be treated using one single incision; in those cases, a medial approach is preferred. The disadvantage of a medial approach is the risk of injury of the ulnar nerve (Cohen et al. Citation1998).
The rehabilitation program we used was rather aggressive in comparison to other studies. Some authors have mentioned continuous passive motion and dynamic splinting as risk factors for development of periarticular ossifications (Park Citation2004). In our series, 2 patients had minimal periarticular ossifications—in both cases without symptoms.
The ROM was similar at 3, 12, and 24 months. Prolongation of physiotherapy after 3 months did not improve the functional outcome, and it can probably be reduced after 3 months.
The column procedure is a simple and safe procedure for posttraumatic stiffness of the elbow joint, with good functional outcome after 2 years. Postoperative rehabilitation is important, especially during the first 3 months after surgery.
Acknowledgments
No competing interests declared.
Contributions of authors
UG: scored the patients postoperatively, wrote the manuscript, and prepared the tables and figures. DE: scored the patients preoperatively and performed all the surgery; she also edited parts of the manuscript.
- Bruno R J, Lee M L, Strauch R J, Rosenwasser M P. Post-traumatic elbow stiffness: evaluation and management. J Am Acad Orthop Surg 2002; 10: 106–16
- Cohen M S, Hastings H. Post-traumatic contracture of the elbow Operative release using a lateral collateral ligament sparing approach. J Bone Joint Surg (Br) 1998; 80: 805–12
- de Boer Y A, van den Ende C H, Eygendaal D, Jolie I M, Hazes J M, Rozing P M. Clinical reliability and validity of elbow functional assessment in rheumatoid arthritis. J Rheumatol 1999; 26: 1909–17
- Green D P, McCoy H. Turnbuckle orthotic correction of elbow-flexion contractures after acute injuries. J Bone Joint Surg (Am) 1979; 61: 1092–5
- Hildebrand K A, Zhang M, van Snellenberg W, King G J, Hart D A. Myofibroblast numbers are elevated in human elbow capsules after trauma. Clin Orthop 2004, 419: 189–97
- Mansat P, Morrey B F. The column procedure: A limited lateral approach for extrinsic contracture of the elbow. J Bone Joint Surg (Am) 1998; 80: 1603–15
- Marti R K, Kerkhoffs G M, Maas M, Blankevoort L. Progressive surgical release of a posttraumatic stiff elbow Technique and outcome after 2–18 years in 46 patients. Acta Orthop Scand 2002; 73: 144–50
- Morrey B F, An K N. Functional evaluation of the elbow. The elbow and its disoders, B F Morrey. W.B. Saunders, Philedelphia 1985; 73–91
- Park M J, Kim H G, Lee J Y. Surgical treatment of posttraumatic stiffness of the elbow. J Bone Joint Surg (Br) 2004; 86: 1158–62
- Trudel G, Jabi M, Uhthoff H K. Intraarticular tissue proliferation after immobility: methods of assessment and preliminary results in rat knee joints. J Rheumatol 1998; 25: 945–50