
Abstract
Purpose
To determine which factors are relevant when applying for the most appropriate adapted tricycle for people with disabilities.
Methods
Patients participating in a rehabilitation programme and planning to apply for an adapted tricycle were invited to participate in an observational study. Measurements used were watts when pedalling, 6-minute walk test, the Trunk Impairment Scale, 30 s sit-to-stand test, Oxford Scale of muscle strength and range of motion testing. Participants answered questions about important factors for choice of tricycle. Nonparametric correlation tests were performed using SPSS to investigate relevant associations between test results and tricycle type.
Results
The study included 37 participants with a large variety of complex disabilities who applied for 9 different adapted tricycles. Participants ranged in age from 5 to 79 years (M = 24 years, SD = 20), with almost half (49%) under 18 years of age. More than half of the participants (57%) were women. Most participants chose an assistive motor. Participants over 50 years applied for a recumbent tricycle. Answers on questionnaire revealed safety, comfort and mastery as important factors for tricycle choice.
Conclusions
Large variations in personal characteristics and needs indicate that individually tailored assessments are necessary to find the most appropriate tricycle.
Large variations of characteristics and needs among people with disabilities and tricycle types indicate individual-level analyses are necessary to find the most appropriate one.
A large selection of tricycles and support from an experienced professional when testing are success factors for finding the most appropriate tricycle.
Implications for rehabilitation
Introduction
Children, youth and adults benefit from regular physical activity [Citation1–4]. Despite clear national and international recommendations for a physically active lifestyle [Citation1,Citation2,Citation5], people with physical disabilities are far less active than people without disabilities [Citation6,Citation7]. To meet physical activity recommendations, people must find an activity they enjoy [Citation1].
Some people with physical disabilities are prevented from using ordinary activity equipment, such as skis and bikes, but can benefit greatly from adapted activity equipment, including special bikes [Citation7,Citation8]. Such equipment is quite accessible in Norway. Children and youth with significantly reduced function can, with help from a physiotherapist or an occupational therapist, apply for assistive activity equipment [Citation9]. People over 26 years of age must pay a co-payment of 10% or up to NOK 4000 [GBP 350] [Citation10], but funding is limited for this age group and does not meet current demand. If granted, people can borrow equipment from the Norwegian Labour and Welfare Administration (NAV) for as long as they need.
Some research has considered the benefits of using assistive equipment/technology in general [Citation11–15]. However, the lack of information about available assistive equipment is one weakness in the provisioning process [Citation16]. Little research has been conducted in the field of adapted equipment for physical activity [Citation17–20], and no research is found on the procurement of adapted bikes specifically. In this study, a tricycle is the chosen adapted equipment, both because cycling is a very common and useful activity in the general population, and because it is expected that almost everyone can participate. Tricycles are also the most common adapted equipment for activity in Norway [Citation21], and cycling can compensate for reduced walking function among many people with a physical disability. Since each tricycles are tested and adapted to each individual (e.g., with specialized pedals and handlebars, and support for the upper body), we refer to the tricycles as “adapted.” The adaptation makes it possible for the individuals to make the best out of their limited physical function.
In this article, we use the International Classification of Functioning, Disability and Health’s (ICF) definition of activity as “the execution of a task or action by an individual” and participation as “involvement in a life situation” [Citation21]. We are also particularly concerned about the involvement part of participation, which refers to the subjective experience of participation that might include motivation, engagement, persistence and social connection [Citation22].
The project referred to in this article was carried out at Beitostølen and Valnesfjord Healthsports Centres, which are (re)habilitation centres offering secondary rehabilitation to persons with disabilities [Citation23]. The rehabilitation programme is based on the theoretical framework of adapted physical activity [Citation24, p. 85], meaning the activity is adapted to each unique person’s preferences, goals and needs [Citation25]. Adaptation of an activity may include individual instruction, adaptation of environmental factors and, in quite a few cases, the use of assistive devices. Even though the variety of assistive devices is large, the variety of persons using such equipment is even larger. Therefore, the most suitable standardized equipment might need to be tailor-made to each individual. Even Paralympic athletes benefit from individually adapted assistive devices in order to utilize their resources in the best possible way [Citation26]. The people participating in the rehabilitation programs at the Healthsports Centres usually do not have Paralympic ambitions, but they still need individual adaptation of the equipment for optimal performance and thereby experience of mastery. Therefore, a range of assistive devices for activity, in this study tricycles, are available for testing at the Healthsports Centres. At Beitostølen Healthsports Centre, a parents’ programme and courses for local service providers are also offered to enhance the transfer of new skills to enable participation in activities in the local community [Citation27]. The vision at the centre is “activity and participation throughout life” [Citation28], and the philosophy of the (re)habilitation program is to ensure transfer and continued physical activity in the participants’ local environment.
Norway has good support arrangements for obtaining assistive activity equipment and the individualized adaptation is integrated in the assessment and trial process. Still, large variations are seen in how tricycles are chosen and individually adapted and how accurate and tailor-made the adjustments are. Therefore, this study aimed to determine whether specific standardized tests can help therapists and people with disabilities choose the most appropriate adaptive tricycle. A second aim, was to map the participants’ subjective reason for choosing a tricycle, and what characteristics of the tricycle were decisive for their choice.
The Regional Medical Committee for Research Ethics in Norway determined the study fell outside the Health Research Act, and, thus, did not need their approval (ref.: 2018/1349). The Norwegian Centre for Research Data approved the study (ref.: 549301). The identity of the subjects is anonymous in this article.
Materials and methods
Design
The present study applied an observational design.
Participants and inclusion procedures
Participants with disabilities were recruited from Beitostølen and Valnesfjord Healthsports Centres. Inclusion criteria were people who:
planned to apply for a leg-driven tricycle in order to follow up cycling in their local environment
understood Norwegian or English
were able to cooperate with the first author during testing.
Inclusion was independent of age and diagnosis, but the Healthsports Centres do not provide (re)habilitation programmes for children younger than 5 years. Professionals at the Healthsports Centres recruited participants, while the main author informed them about what participation would entail. Participants above 16 years of age provided written informed consent, whereas parents signed for participants below 16 years of age. The participants’ diagnostic and demographic data (age, gender and place of residence) were obtained from their medical records or orally from the participants.
Outcome measures and data collection
The standardized tests were selected based on physical characteristics deemed important for bicycle selection, such as strength, endurance, balance and range of motion. They were conducted by the professionals at the Healthsports Centres. The selection of tricycles consisted of 12 different types. Participants tried two or three of these, based on which ones the participant and professional considered most appropriate.
One test was conducted during tricycle testing:
Vector 3 watt pedals [Citation29] were put on all tricycles during testing, to measure approximate (margin of error ± 1%) maximum power when cycling. Maximum watt scores were used as output scores. A high score indicated the opportunity to create great power in the sitting position of the tricycle in use, and was considered to be positive. Testing of tricycles was conducted on a 400 m flat asphalt pavement (one round per tricycle). Participants tested at least two different tricycles. Two participants tested three tricycles, since the first two did not fit satisfactorily.
Five tests were conducted separately from cycle testing:
6-min walk test [Citation30] tests the distance a person can walk in 6 min on a 30 m flat floor. This test is suitable for measuring endurance and shows good internal consistency. However, the test might show a ceiling effect for people with normal exercise capacity. It was included in the study to determine if the test could separate those who need an assistive motor from those who do not.
The Trunk Impairment Scale, Norwegian version [Citation31] assesses dynamic sitting balance. Total score ranges from 0 (minimal performance) to 16 (perfect performance). This test shows good construct validity, excellent internal consistency and high inter-tester reliability. The test was included in an attempt to separate those who need a low seat with a backrest from those who do not.
The 30-s sit-to-stand test [Citation32] measures lower body power and strength by testing how many times the subject can sit down and stand up in 30 seconds. Although the tool shows good internal consistency, it might have a ceiling effect [Citation30]. This test was included given its ability to measure strength and because the test requires balance skills.
Manual strength test of lower extremity muscle groups with the Oxford Scale [Citation33]. Scale from 0 (paralysis) to 5 (normal). This test is frequently used in clinical practice and shows acceptable specificity, but does not detect accurate muscle weakness [Citation34]. The test was included because of the assumption that muscle power is relevant when choosing a tricycle. Muscle groups tested were dorsal and plantar flexors of the ankle joints, knee flexors, knee extensors, hip flexors and hip extensors.
Range of motion was measured with a goniometer, which is shown to be acceptably reliable [Citation35,Citation36]. The tests were included because of the assumption that the range of motion will affect possible sitting positions and/or need for handlebar close to the body, and thereby tricycle choice. Joints tested and cut off-points for reduced range of motion were: hip flexion 120°, hip extension 10°, knee flexion 140°, knee extension 10°, ankle dorsiflexion with hip and knee in 90° flexion 20°, ankle plantar flexion with hip and knee in 90° flexion 45°, elbow extension 0°, wrist flexion 80° and wrist extension 70°.
After the participants had received their tricycles, they, or their parents, answered a questionnaire with two open-ended questions via e-mail: (1) What was decisive for choosing the exact tricycle that was applied for? and (2) What characteristics of the tricycle are important to you?
Data were collected between May 2019 and November 2020.
Statistical analyses
Results were recorded and analyzed using SPSS version 25 (SPSS Inc., Chicago, IL). Descriptive analyses were conducted to reveal frequencies and sample characteristics. Cross-analyses were performed to find relevant associations between test results and tricycle type. Nonparametric correlation tests were performed to determine factors that could predict tricycle choice. Moreover, each test result was analyzed separately to investigate whether the specific test could predict the most appropriate tricycle choice.
Results
Participants
The sample was composed of 37 participants who applied for an adapted tricycle. The participants ranged in age from 5 to 79 years (M = 24 years, SD = 20), of which 18 (49%) were under 18 years of age. More than half of the sample were women (n = 21, 57%). The participants presented a large variety of complex disabilities, including neurological, neuromuscular diseases, Down syndrome and rare syndromes ().
Table 1. Sample characteristics.
Tricycles
The participants applied for nine different tricycles that could be divided into three different categories:
Three tricycles (Sunny (n = 5), Medema (n = 1) and Victoria (n = 1)) with a high seat (> 70 cm for adults) and ordinary handlebars. Two wheels at the back or front.
One tricycle (Easy Rider (n = 9)) with lower (medium) seat (57–63 cm for adults) with backrest. Two wheels at the back.
Five recumbent tricycles (Kettweisel Heinzmann (n = 13), Gekko (n = 4), Scorpion (n = 2), Lepus (n = 1) and Azub (n = 1)) with a low seat (< 57 cm), backrest and alternative handlebar beside the thighs. Two wheels at the back or front.
All tricycles can have an assistive motor if needed, and only two of the participants applied for a tricycle without an assistive motor. The three types of tricycles are shown in . The corresponding colours are used in subsequent figures for ease of identification.
Figure 1. Images of the three tricycle categories. High seat = >70 cm, medium seat = 57–63 cm and low seat = <57 cm.

Outcomes
Spearman’s nonparametric correlation test showed a few weak correlations between personal characteristics and bike type. Higher age (rs = 0.47, p =.004) and longer distance achieved during the 6-min walk test (rs = 0.33, p =.047) were correlated with applying for a tricycle with a lower seat. The same relationship was seen for women (rs = 0.414, p =.011), but only when the tricycles were divided into two categories: high and low (with medium and low in the same category). With these two categories, a correlation was found between higher scores on the 30-s sit-to-stand test and the choice of a tricycle with a high seat (rs = 0.37, p =.024).
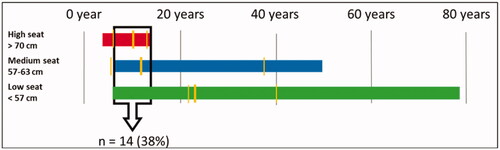
Age
Participants from 8 to 13 years were represented in all three tricycle categories, comprising 38% of the sample (). The results showed that all participants over 50 years (n = 5) applied for a low tricycle, but this tricycle category also contained participants with a wide age range (from 7 to 79 years).
Figure 2. Type of tricycle related to age in years. The thick, vertical, yellow lines represent the medians and the thin yellow lines represent a 95% CI.
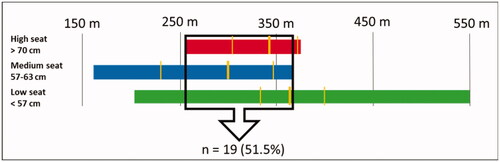
6-min walk test
The 6-min walk test showed that 51.5% of the participants could end up in either of the three tricycle categories (). Also, participants applied for a low tricycle regardless of their score on this test. In other words, participants who scored 200 m and 550 m applied for the same tricycle.
Figure 3. Type of tricycle related to scores on the 6-min walk test in metres (m). The thick, vertical, yellow lines represent the medians and the thin yellow lines indicate a 95% CI.
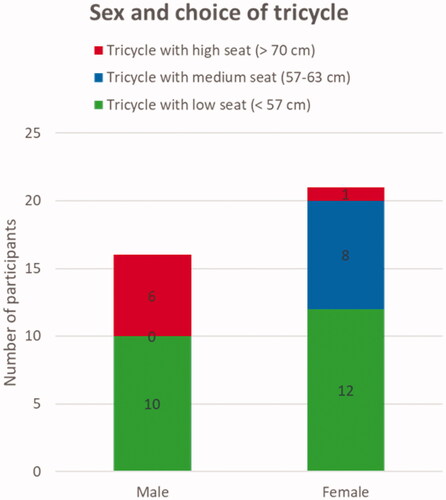
Sex
Sex was correlated with tricycle choice, but only when the categories “medium” and “low” were merged, where more women applied for low tricycles. When three categories were kept, the same trend did not appear. Specifically, men were represented in the “high” and “low” category but were absent in the “medium” category ().
Figure 4. Choice of tricycle based on sex.
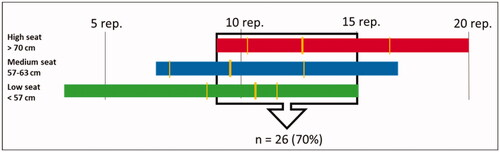
30-s sit-to-stand test
For the 30-s sit-to-stand test, the number of participants in the same “window” was 70% (). Participants who scored in the wide range of 7–20 applied for a high tricycle. Still, there is a trend of participants with lower scores applying for a tricycle with a low seat and those with higher scores applying a high seat tricycle.
Figure 5. Type of tricycle related to scores (repetitions) on the 30-s sit-to-stand test. The thick, vertical, yellow lines represent the medians and the thin yellow lines indicate the 95% CI.
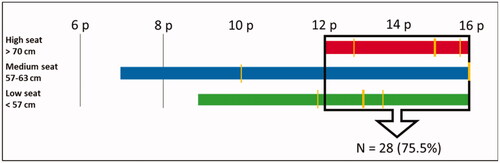
Trunk impairment scale
For the Trunk Impairment Scale, 75.5% of the participants scored within the same “window” (). Participants with scores between 12 and 16 applied for a tricycle from any of the three categories.
Figure 6. Type of tricycle related to scores on the Trunk Impairment Scale (0–16 points). The thick, vertical, yellow lines represent the medians and the thin yellow lines indicate a 95% CI.
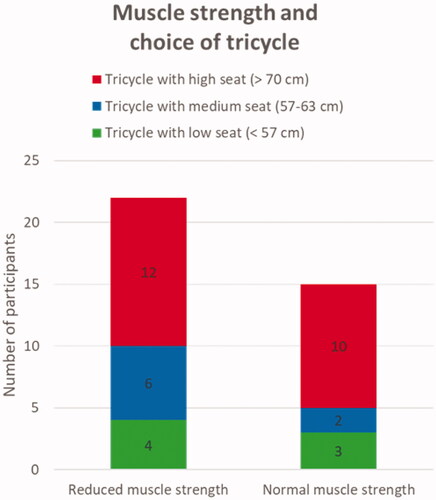
Oxford scale
Participants both with reduced and normal muscle strength applied for tricycles in all three categories (). In the “medium” category, three times as many with reduced muscle strength applied compared to those with normal muscle strength. However, the total number of participants in this subgroup is small (n = 8).
Figure 7. Type of tricycle related to muscle strength as measured with the Oxford Grading Scale for manual muscle testing. Reduced = 0–4 of 5, normal = 5 of 5.
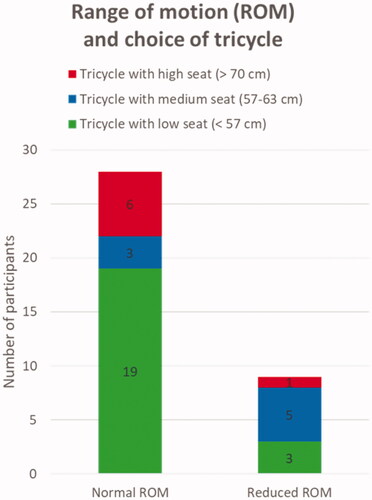
Range of motion
Participants with a reduced range of motion in either of the tested joints applied for tricycles from all three categories. The total number of applicants with a reduced range of motion in their joints was low, which also means that the number in each tricycle category was low. Only one participant with reduced range of motion applied for a high tricycle, but many participants with a normal range of motion applied for tricycles in both the high and low tricycle categories, with fewer in the medium category ().
Figure 8. Type of tricycle related to the range of motion (ROM) in legs and arms as measured with a goniometer. Reduced ROM = reduced in at least one joint.
Power output
About two-thirds (60%) of the participants applied for the tricycle with a higher power output. For those subjects, the mean power output was 52.5% (SD = 51.3, range = 2–155%) higher than the tricycle not selected. Forty per cent of the participants applied for the tricycle with a lower power output. For those subjects, the mean power output was 21.1% (SD = 20.9, range = 2–80%) lower than the tricycle not selected.
Participants’ reasons for choice of tricycle
Seventeen participants (46%) answered the two open-ended questions regarding reasons for choice of tricycle. The feeling of being safe, the ability to master cycling and comfortable sitting position were reported to be the main reasons for choosing the exact tricycle over the others (see ). Other important characteristics of a tricycle were reported to be that stability, and an assistive motor with sufficient battery capacity to assist in steep uphills (see ). Self-reported reasons for choice of tricycles are presented in .
Table 2. Participants’ reasons for choice of tricycle (n = 17).
Discussion
It is known that many people with disabilities struggle to reach the recommended amount of physical activity. For quite a few, cycling is a motivating and feasible way of being physically active [Citation8,Citation18,Citation20]. Norway has a well-developed nationwide system that gives people good access to adaptive activity equipment. Still, some have limited access because funding is limited for those over 26 years of age and some might have difficulties managing the co-payment. Therefore, opportunities to participate in cycling might be different within a group of people with physical disabilities.
For those with the opportunity to access an adapted tricycle, it is important to find an appropriate one. However, knowledge of how to select an adapted tricycle varies among local therapists within Norway [Citation17]. The selection of tricycles is large and ever increasing. The 37 participants in this study applied for a total of nine different tricycles, each of which is available with different opportunities for adjustments. Given that people applying for an adapted tricycle present with a wide variation in functional abilities, it is beneficial they have a wide choice in products. However, the complexity of finding a suitable tricycle for each unique individual is challenging, which sets requirements for the professional and the person with a disability to find the most suitable bike.
Some people with disabilities might need a tandem tricycle, especially those with visual impairment or severe physical impairment. However, we chose not to include people who applied for a tandem tricycle, because then the adaptation is not only focussed on the person with disability but also to the companion who contribute with some or all the propulsion.
The findings in this study suggest that age, gender and result on the 6-min walk test might be associated with the choice of a well-adapted tricycle. Still, none of the mentioned tests could alone predict the most appropriate type of tricycle for a specific person with a complex disability.
Age
Age had the highest correlation to bike type. One-third of the participants were in an age category where all three bike types were represented (i.e., 8–13 years), meaning that younger cyclists could end up on either of the tricycles. It seems clear that adults did not apply for tricycles with high seats. All participants over the age of 50 applied for the recumbent bikes. Even though there are many different tricycles in the recumbent category, and multiple aspects need to be considered to conclude which tricycle is the most appropriate, results from this study suggest that people over 50 years reasonably can start by testing a type of recumbent tricycle.
6-min-walk test
The results from the 6-min walk test suggest that many people with disabilities, regardless of endurance capacity, might benefit from using a low tricycle. One of the reasons why this test was included in the study was the assumption that it might separate those who needed an assistive motor from those who did not. However, only two participants applied for a tricycle without an assistive motor. This test could not separate between those who benefitted from an assistive motor and those who did not need one. The results from this study show that most people with disabilities benefit from a tricycle with an assistive motor. Many people with disabilities have lower endurance capacity than the general population [Citation37] and might benefit from an assistive motor to be able to follow friends and family when cycling. For many people, this social aspect might be the most important reason to cycle. The assistive motor might be the factor that enables them to be involved in social cycling activities [Citation22]. Also, a trend among Norwegians, in general, is to buy ordinary two-wheeled bikes with an assistive motor for transportation to work and leisure activities. Riding a tricycle with an assistive motor enables people with disabilities to follow this trend.
Sex
Although no men applied for the medium tricycle, it is likely they would also find a medium tricycle appropriate because they fit on both higher and lower tricycles. This result may be different with a larger sample size.
30-s sit-to-stand test
This test demands both strength in lower extremities and balance [Citation32], which are factors that might affect the choice of bike type. As seen in , there was a slight trend, that those with higher scores on this test applied for a tricycle with a high seat. Despite this trend, the percentage of participants who scored in the same “window,” and thereby applied for either of the three tricycle categories, was as much as 70%. A “cut off point,” that separated the three categories was not observed, which means that completing this test did not seem to help people with disabilities or their therapists chose the most appropriate tricycle.
Trunk impairment scale
The Trunk Impairment Scale was included in the study with the assumption that people with a lower sitting balance would benefit from a low and wide seat with a backrest. This assumption was confirmed to some extent, since all participants applying for the high tricycle scored high on the Trunk Impairment Scale. Yet, these test results could not predict tricycle choice, since many participants with high scores also applied for the two other tricycle categories. The result suggests that a low tricycle also is relevant for several people with good sitting balance. The reasons for this relevance might partly be explained by characteristics of the low tricycles that the high ones do not have, such as (Citation1) the possibility of shock absorption for less back pain and thereby better comfort, and (Citation2) a lower centre of gravity that allows higher speed in turns with a higher level of safety.
Oxford scale
No pattern was observed concerning whether participants with low muscle power chose bike types with a specific angle between seat and pedals. Since muscles have different prerequisites for generating power in different positions [Citation38], a hypothesis before conducting the study was that people with reduced muscle strength in their legs would prefer one specific bike type. The tricycles with backrests provide support to their back when pedalling, creating a counterforce, which might give an advantage when creating power; however, this hypothesis was not confirmed.
Range of motion
To suggest that range of motion can predict tricycle choice, a trend of reduced range of motion should have been observed as people chose a tricycle with a higher or lower seat compared to the centre of the pedals. Such trend was not seen in this study. Therapists should not base the choice of higher or lower seat on reduced or not reduced range of motion. It seems that all three tricycles categories can fit for people with reduced range of motion in their lower extremities. However, two participants with reduced range of motion in their arms applied for a medium and a low tricycle, which have the handlebar closer to the seat than the high tricycle.
Power output
The power output factor seemed to have a larger influence on tricycle choice as the difference between power output scores on the tested tricycles increased. It might be that when differences in power output measures were small, other factors were more relevant for tricycle choice. When the difference was larger, and the cyclists could feel a noticeable difference, they were more likely to choose the tricycle on which they managed to pedal with the most power output.
Participants’ reasons for choice of tricycle
Comfort was not surprisingly, reported to be important for choice of tricycle. In addition, the participants highlighted the importance of an assistive motor that could help them reach to the places they want. Norway is a country with varied terrain, steep hills and scattered settlements, which means that many, including people without disabilities, benefit from an assistive motor. The feeling of safety was also reported to be important. Safety seemed partly to be about having a stable tricycle with low risk of falling, but also about having a tricycle that was easy to manoeuvre and to have breaks that were easy to reach and use. The feeling of mastery was also highlighted as important for the choice of tricycle. This factor is reported to be crucial for sustaining physical activity [Citation39,Citation40], and should therefore be considered as one of the most relevant factors in order to ensure sustained cycling activity.
Overall interpretation of the results
Evaluation of these results might suggest that relevant factors for choosing a well-adapted tricycle are even more complex than the factors tested in this study (i.e., strength, endurance, balance and range of motion). However, people over the age of 50 ended up applying for a recumbent tricycle and young people with good sitting balance tended to apply for a tricycle with a high seat. Many other aspects can be relevant, including other physical skills, local environment, pain, motivation, preferences and self-image [Citation18,Citation19,Citation39]. The answers on the questionnaire supported that safety, comfortable sitting position and the ability to master the tricycle had great importance. In addition, almost all participants benefitted from an assistive motor.
The intended use of the tricycle is crucial; for instance, a different type might be required if the tricycle is primarily meant for transport in the local community versus outdoor life in the forest. At Beitostølen Healthsports Centre, experience-based procedures for testing and adaptation of tricycles have been developed over the years. Professionals use strategies from the theoretical framework of adapted physical activity [Citation27]; adapting the preferred activity to the athlete with the use of adaptive equipment when they plan to apply for a tricycle together with the cyclist. Years of experience with the adaptation of different bikes to different people in different environments is key to success. Cooperation with the cyclist, and colleagues when necessary, in addition to multiple testing over several days, results in a well-adapted tricycle. The factors that are relevant for each person vary and seem to require an individually tailored adaptation process. We found no clear pattern of which factors are most significant for which person in this study, indicating individual combinations of factors are crucial. This might indicate that consulting with an experienced professional who can determine the most relevant factors for each person is valuable for selecting the most appropriate tricycle. However, more research is needed to determine the most crucial factors for choosing and adapting appropriate adaptive tricycles to increase therapists’ knowledge and ability to help clients effectively.
Strengths and limitations
Although the sample of this study was sufficient for an observational study, the large number of bike categories limited our ability to identify potential associations. However, a larger sample may not produce clear trends given the wide range of tricycles and people. There might be, and most likely are, relevant factors for choosing the best tricycle that are not included in this study. Still, the study includes a large variety of factors and a diversity of disabilities, which strengthen the transferability of the results to other contexts. Further, the study has been conducted in a country with a well-developed system for procuring adapted tricycles, which prevents socio-economic bias of the participants.
Conclusions
None of the conducted standardized tests could predict the right adaptive tricycle for each person alone. Participants over the age of 50 applied for one of the five recumbent tricycles, and only young participants with good sitting balance ended up with a tricycle with a high seat. Most participants benefitted from, and, therefore, chose, a tricycle with an assistive motor. Safety, comfort and mastery were stated as important factors when choosing the most appropriate tricycle. Large variations among people with disabilities, bike types and possible adjustments indicate individual-level analyses are necessary to find the most appropriate tricycle.
Acknowledgements
The authors thank all participants and parents of participating children as well as the professionals who contributed to the recruitment process.
Disclosure statement
The authors report no conflict of interest.
Additional information
Funding
References
- O'Donovan G, Blazevich AJ, Boreham C, et al. The ABC of physical activity for health: a consensus statement from the British Association of Sport and Exercise Sciences. J Sports Sci. 2010;28(6):573–591.
- World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization; 2010.
- Blair SN, Morris JN. Healthy hearts—and the universal benefits of being physically active: physical activity and health. Ann Epidemiol. 2009;19(4):253–256.
- Janssen I, LeBlanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. 2010;7(1):40.
- Helsedirektoratet. Anbefalinger om kosthold, ernaering og fysisk aktivitet. [Recommendations on diet, nutrition and physical activity]. Oslo, Norwegian; 2014.
- Rimmer JH, Riley B, Wang E, et al. Physical activity participation among persons with disabilities: barriers and facilitators. Am J Prev Med. 2004;26(5):419–425.
- Bedell G, Coster W, Law M, et al. Community participation, supports, and barriers of school-age children with and without disabilities. Arch Phys Med Rehabil. 2013;94(2):315–323.
- Gjessing B, Jahnsen RB, Strand LI, et al. Adaptation for participation! Children’s experiences with use of assistive devices in activities. Disabil Rehabil: Assist Technol. 2018;13(8):803–808.
- Arbeidsdepartementet. NOU 2010:5. Aktiv deltakelse. likeverd og inkludering. Et helhetlig hjelpemiddeltilbud. [Active participation, equality and inclusion. A comprehensive system for assistive technology]. Oslo, Norwegian: Arbeidsdepartementet; 2010.
- NAV. Rundskriv til § 10-7 bokstav a – Aktivitetshjelpemidler til personer over 26 år. [Circular to § 10-7 letter a – assistive activity technology for persons over 26 years of age]. Oslo, Norwegian: NAV; 2015.
- Kurtze N, Hem K-G, Svardal ÅS, et al. Utrednings-og forskningsprosjekt om hjelpemiddelformidling, tilrettelegging og rehabilitering som fag-og forskningsfelt. [Study and research project on assistive technology, adaptation and rehabilitation as a discipline and research field]. Oslo, Norwegian; 2009.
- Scherer MJ, Glueckauf R. Assessing the benefits of assistive technologies for activities and participation. Rehabil Psychol. 2005;50(2):132–141.
- Østensjø S, Carlberg EB, Vøllestad NK. The use and impact of assistive devices and other environmental modifications on everyday activities and care in young children with cerebral palsy. Disabil Rehabil. 2005;27(14):849–861.
- Øien I, Fallang B, Østensjø S. Everyday use of assistive technology devices in school settings. Disabil Rehabil: Assist Technol. 2016;11(8):630–635.
- Ravneberg B, Söderström S. Disability, society and assistive technology. New York (NY): Taylor & Francis; 2017.
- Arbeids- og sosialdepartementet. Gjennomgang av hjelpemiddelformidlingen. Samhandling og organisering av hjelpemiddelområdet. [Review of the distribution of assistive technology. Interaction and organization of the assistive technology area]. Oslo, Norwegian: Arbeids- og sosialdepartementet; 2017.
- Bergem S. Knowledge among important actors in the field of adaptive equipment for young people with disabilities. Disabil Rehabil: Assist Technol. 2020;15(1):109–118.
- Pedersen H, Söderström S, Kermit P. The fact that I can be in front of others, I am used to being a bit behind”: how assistive activity technology affects participation in everyday life. Disabil Rehabil: Assist Technol. 2021;16(1):83–89.
- Pedersen H, Söderström S, Kermit P. Assistive activity technology as symbolic expressions of the self. TAD. 2019;31(3):129–140.
- Pickering DM, Horrocks L, Visser K, et al. Adapted bikes–what children and young people with cerebral palsy told us about their participation in adapted dynamic cycling. Disabil Rehabil: Assist Technol. 2013;8(1):30–37.
- World Health Organization. International classification of functioning, disability and health. Geneva: ICF; 2001.
- Imms C, Granlund M, Wilson PH, et al. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. 2017;59(1):16–25.
- Røe C, Dalen H, Lein M, et al. Comprehensive rehabilitation at Beitostølen Healthsports Centre: influence on mental and physical functioning. J Rehabil Med. 2008;40(6):410–417.
- Sherill C. Adapted physical activity, recreation and sport. 6th ed. New York (NY): McGraw-Hill; 2004.
- Morisbak I, Standal Ø. Rehabilitering med tilpasset fysisk aktivitet som hovedvirkemiddel. [Rehabilitation with adapted physical activity as the main tool]. In: Kissow A-M, Therkildesen B, editors. Kroppen som deltager. Idraet og bevaegelse i rehabiliteringen. Roskilde, Norwegian: Handicapidraettens Videncenter; 2006. p. 146–156.
- Severin AC, Danielsen J, Falck Erichsen J, et al. Case report: adjusting seat and backrest angle improves performance in an elite paralympic rower. Front Sports Act Living. 2021;3:15.
- Willis CE, Reid S, Elliott C, et al. It’s important that we learn too’: empowering parents to facilitate participation in physical activity for children and youth with disabilities. Scand J Occup Ther. 2019;26(2):135–148.
- Beitostølen Healthsports Center. 2019. Beitostølen, Norway. Available from: https://www.bhss.no/media/2937/engelsk-brosjyre_lang_2019.pdf.
- Garmin. Vector 3. 2020. Available from: https://buy.garmin.com/nb-NO/NO/p/573589.
- Bennell K, Dobson F, Hinman R. Measures of physical performance assessments: *Self‐Paced Walk Test (SPWT), Stair Climb Test (SCT), Six‐Minute Walk Test (6MWT), Chair Stand Test (CST), Timed Up & Go (TUG), Sock Test, Lift and Carry Test (LCT), and Car Task. Arthritis Care Res. 2011;63(S11):S350–S370.
- Gjelsvik B, Breivik K, Verheyden G, et al. The Trunk Impairment Scale–modified to ordinal scales in the Norwegian version. Disabil Rehabil. 2012;34(16):1385–1395.
- TopEndSports. Chair Stand Test. Available from: https://www.topendsports.com/testing/tests/chair-stand.htm.
- Physiopedia. The Oxford Scale. Available from: https://www.physio-pedia.com/Muscle_Strength.
- Bohannon RW. Manual muscle testing: does it meet the standards of an adequate screening test? Clin Rehabil. 2005;19(6):662–667.
- Milanese S, Gordon S, Buettner P, et al. Reliability and concurrent validity of knee angle measurement: smart phone app versus universal goniometer used by experienced and novice clinicians. Manual Ther. 2014;19(6):569–574.
- Mullaney MJ, McHugh MP, Johnson CP, et al. Reliability of shoulder range of motion comparing a goniometer to a digital level. Physiother Theory Pract. 2010;26(5):327–333.
- Voelker R. Adults with disabilities need physical activity too. JAMA. 2014;123.
- Arnold EM, Hamner SR, Seth A, et al. How muscle fiber lengths and velocities affect muscle force generation as humans walk and run at different speeds. J Exp Biol. 2013;216(11):2150–2160.
- Saebu M, Sørensen M. Factors associated with physical activity among young adults with a disability. Scand J Med Sci Sports. 2011;21(5):730–738.
- Bandura A. Social foundations of thought and action. In: Bandura A, editor. The health psychology reader. Englewood Cliffs (NJ): Prentice-Hall; 2002; p. 94.