
Abstract
Purpose
Assistive technology (AT) is a highly effective intervention to address the capability gap for people living with deafblindness. The My AT Outcomes Framework (MyATOF) is a novel Australian framework founded upon AT process principles and outcomes research. It guides stakeholders to articulate AT use according to 6 dimensions. MyATOF was developed as a data collection and knowledge translation tool. The use case of AT by people with deafblindness in Southern Africa was investigated in this study to determine the applicability of MyATOF dimensions to (a) people with deafblindness and (b) low- and middle-income countries.
Materials and methods
Two online surveys, using the Delphi methodology, were undertaken with key stakeholders including people with deafblindness, family members, researchers, service providers, educators and advocates. An expert panel of 17 completed Phase 1, with 14 completing Phase 2. The WHO 5 Ps AT systems thinking model was used in data analysis.
Results
Respondents affirmed the validity of the dimensions of MyATOF for people with deafblindness in four Southern African countries. In-country barriers and constraints were identified as significantly impacting the capacity of AT users with deafblindness, to realize positive outcomes.
Conclusions
The MyATOF dimensions show promise in their use with persons with deafblindness in Southern Africa, though further research is needed.
The impact of assistive technology and related supports can be evaluated across a number of dimensions including human rights, costs incurred and saved, consumer experience, and service delivery satisfaction.
These dimensions of impact resonate across the two continents investigated to date, with contextual factors being considered.
Variables influencing access to assistive technology across contexts can be understood through the WHO GATE five P’s systems thinking model.
Few tools place data capture and outcomes measurement in the hands of assistive technology users, but indications are that this is of value to consumers.
IMPLICATIONS FOR REHABILITATION
Introduction
People with disability experience disadvantages in socio-economic and employment status and lower overall health status [Citation1,Citation2]. Assistive technology (AT) is a key enabler of improved outcomes for people with disabilities, including those with deafblindness, in all life domains. However, tools are needed to assist people with disabilities to articulate needs, goals, and rights related to the use of AT, and to evaluate and measure AT-related outcomes, in order to make the case for appropriate AT provision.
Assistive technology
AT is an umbrella term for assistive products and related services, the use of which maintains or improves a person’s ability to function and be independent, thus promoting their well-being [Citation3]. When provided effectively, AT can be used to fill the capability gap between a person’s functional capacity and the demands of their environments, enabling people to participate in daily life and work and to achieve the United Nations Sustainable Development Goals [Citation4]. AT represents a hugely impactful yet under-realized intervention and a cost-effective investment for governments [Citation5].
Assistive products include devices, equipment, instruments, and software, designed and produced especially, or available generally on the market. AT services include assessment, product fitting, training, troubleshooting and maintenance support, which are critical to the safe and effective use of products. Accordingly, AT is understood as a complex system requiring policies and markets that can deliver end-to-end products and services [Citation6]. The application of systems thinking within the global AT community has identified five strategic drivers which are critical to realizing the full potential of AT for global citizens. Termed the “5 Ps” and comprising people (that is, AT users and their social networks), policy, products, personnel, and provision, these form the basis of strategic actions by the WHO Global Access to AT (GATE) team [Citation7]. Additional, situational factors of procurement, place, pace, promotion, and partnership have been hypothesized as other critical factors influencing AT outcomes [Citation8].
Assistive technology and deafblindness
Deafblindness is a unique and isolating sensory disability, resulting from the combination of both hearing and vision loss or impairment that significantly affects communication, socialization, mobility and daily living [Citation9]. Deafblind individuals use AT for the vision impaired, for example, long canes for mobility, screen, reading software, and refreshable braille displays [Citation10,Citation11] and AT for the hearing impaired, for example, hearing aids and cochlear implants, as well as human supports, such as sign language interpreters and communication guides (support workers trained specifically to work one-to-one with people with deafblindness) [Citation12,Citation13]. Much of the research on deafblindness and AT focuses on AT for communication and social inclusion ([Citation10,Citation14–17]) which underpin the functioning of people with deafblindness across all life domains and in all contexts. Vibro-tactile or haptic technology and 3D printing are showing early promise for people with deafblindness, however, these technologies are as yet rarely studied [Citation16].
AT, deafblindness and the Southern African Development Community
The Southern African Development Community (SADC) was selected as the focus of this study. Any research into AT and its impacts must be sensitive to context, and the impact of context upon capability [Citation18]. Reasons for selecting the SADC region included the emergence of an active Pan-African AT Community [Citation19]; evidence of strategic thinking about AT systems within the region [Citation20–22]; and the first Deafblind International Conference planned for Africa in 2022 [Citation23].
People with deafblindness have been identified as being at risk of exclusion from the achievement of human rights or implementation of Sustainable Development Goals (SDGs), with approximately 0.2% of the world’s population living with severe deafblindness, and 2% living with “milder forms” of deafblindness [Citation9]. Statistics regarding the prevalence of deafblindness on the African continent are not available, but evidence suggests that in many low- and middle-income countries, only 5–15% of people who require assistive devices receive them [Citation24,Citation25].
Measuring what matters to people living with disability
AT outcomes research can be defined as “systematic investigation aimed at identifying the changes that are produced by AT in the lives of users and their environments” [Citation26]. International calls for the sector-wide collection of AT outcomes data have been made for over two decades yet data is still not routinely collected, and consensus has not been reached on priority dimensions to be measured [Citation27]. That said, extensive scholarly work over several decades has produced a range of psychometrically validated measures, authoritatively reviewed in Federici and Scherer’s AT Assessment Handbook (2017) [Citation28].
Two observations can be made about extant outcome measures which explain the formulation of MyATOF as an alternative “starting point” which provides AT users and stakeholders access to a co-designed, evidence-based and holistic set of outcome dimensions.
Firstly, many AT outcome measurement tools collect partial information, as creating psychometrically valid tools necessitates a focal rather than broad lens [Citation29]. AT outcome measures usually relate to specific products, functional impairments or tasks or specific aspects of consumer experience, for example, predisposition to AT [Citation30]; user satisfaction with AT [Citation31], the psychosocial impact of AT [Citation32]; or assessment for AT with individual products. Some approaches combine these validated measures to obtain a fuller picture across dimensions [Citation33] or offer a comprehensive suite of measures, mediated by professionals [Citation34,Citation35].
Secondly, most tools are not designed to be consumer-directed. Existing approaches to identifying changes regarding AT outcomes are subjective (consumer or AT user-generated) and/or objective (assessed by professionals). Consumer perspectives of AT outcomes have long been discussed and may differ from professional views [Citation36]. Fuhrer et al. classify dimensions of significance as proximal outcomes such as functioning, social participation, vocational productivity, sense of control, and distal outcomes such as environments and assistance costs [Citation26]. Jutai et al. propose the dimensions of device effectiveness, social significance, and subjective well-being [Citation37]. In 2013, Lenker and colleagues conducted a study on consumer perspectives of AT outcomes and at the pilot stage learned, through consumer feedback via their reference group, that “outcomes is a term practitioners and researchers use, created to justify their work…that the term outcomes is not part of the consumer vernacular” [Citation38,p.375]. The term outcomes, and the changes about which it may be important to establish an outcome response, hold different meanings for consumers. Observing that outcomes research methodologies should reflect consumer perspectives, Lenker et al. identified the dimensions that mattered, and the need for research reporting the costs of AT provision; the impact of AT on participation; and the AT service delivery process [Citation38].
MyATOF was devised to capture the AT user’s perspective across relevant dimensions and comprises a series of questions, which summarise information about the AT user’s needs, goals, and context. Data are captured in the areas of (a) supports, (b) valued outcomes, (c) costs and cost offsets, (d) human rights, (e) service delivery pathway, and (f) customer experience. below outlines the operationalization of the six dimensions comprising the Framework.
Table 1. Six dimensions of the MyATOF tool.
Table 2. Panellist demographics.
Data are summarized into report formats, enabling the AT user to inform practitioners and funders regarding a need for specific AT. Since the data fields are benchmarked against international standards and available evidence, MyATOF and its aggregated data set can be used to inform policy, research, and make comparisons around the world.
MyATOF was developed in Australia through an iterative, consultative process, involving a broad range of people with disability, disability professionals including those with experience in deafblindness, and advocates [Citation52–55]. MyATOF has not yet been used with people with deafblindness or outside of Australia, and the aims of this study were to:
determine the relevance and face validity of MyATOF for use with people with deafblindness in the SADC;
refine the tool, if relevant and valid, to increase its relevance and validity in this context;
deepen the understanding of the context of AT provision and use by people with deafblindness in the SADC.
Ethical considerations
Approval to carry out this research was obtained on 28 August 2020 from the Cape Peninsula University of Technology (2020FOBREC785). The Participant Information Sheet confirmed participation in the study was voluntary and anonymous. A small gift voucher was offered to participants who completed all rounds of the Delphi study to thank them for their time and input.
Materials and methods
Study design
Delphi methodology was chosen for this study as the purpose of this approach is to achieve consensus or priorities among an expert panel on a certain topic, where agreement was not previously determined [Citation56]. The Delphi method was also chosen as it integrates elements of both qualitative and quantitative methodologies to address a specific research problem, thus yielding a more holistic view of the research issue [Citation57]. Typically 2 or more rounds of questionnaires are sent to the expert panel until a consensus or clear priorities are reached [Citation56]. In this study, two rounds of electronic surveys using the Qualtrics Platform (www.qualtrics.com) were completed. Participants unable to access the electronic survey had the option of being emailed an MS Word version of the survey. A pilot (n = 2) was conducted during Phase 1 of the survey to confirm accessibility. Junger et al’s [Citation58] recommendations for conducting and reporting on Delphi studies were addressed as follows:
Rationale – the rationale for using the Delphi method is outlined above.
Planning and design – for round one, the consensus was sought regarding the relevance and validity of each question using quantitative analysis, and an understanding of specific contextual issues was sought using qualitative analysis as explained below. For round two, both agreement and prioritization were looked for using quantitative analysis and a deeper understanding of contextual issues was pursued using qualitative analysis, again as outlined below.
Study conduct – the first questionnaire was piloted to check efficacy as reported above. There was no conflict of interest for any of the three researchers, with two researchers being based outside the SADC region and the third researcher having little involvement with the local deafblind community. While high levels of agreement were achieved in both rounds of the study, disagreement on some items in the second round is reported in the results.
Reporting – The purpose of the study and rationale for using the Delphi method is articulated above. The recruitment process for and demographic data of the expert panel are outlined under ‘study population’. The development of the MyATOF, which formed the basis of the first Delphi round is explained in the introductory section titled ‘Measuring what matters to people living with disability’. A detailed description of the data collection and processing analysis are provided in figures and tables below. Limitations and conclusions of the study are made explicit at the end of the paper.
Figure 1. Relevance of MyATOF statements to people with deafblindness and the SADC region.
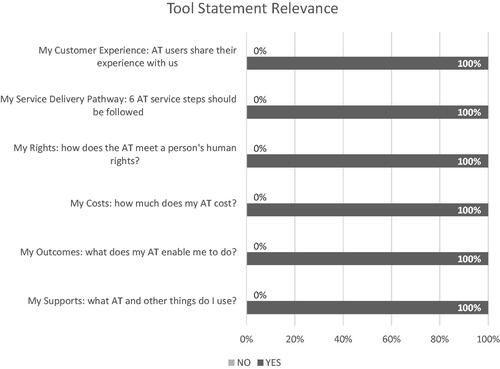
Figure 2. Rating of the importance of sub-themes of the “People” theme.
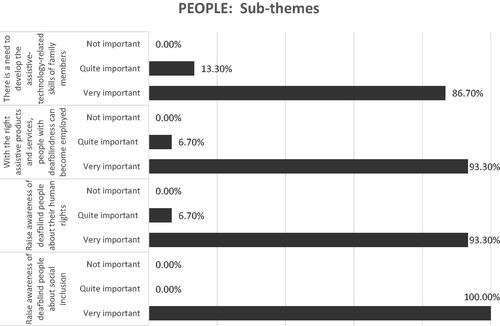
Figure 3. Rating of the importance of sub-themes of the “Policy” theme.
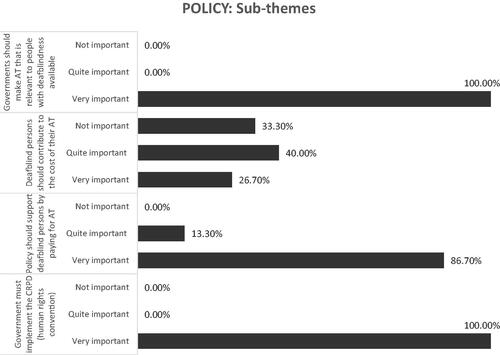
Figure 4. Rating of the importance of sub-themes of the “Products” theme.
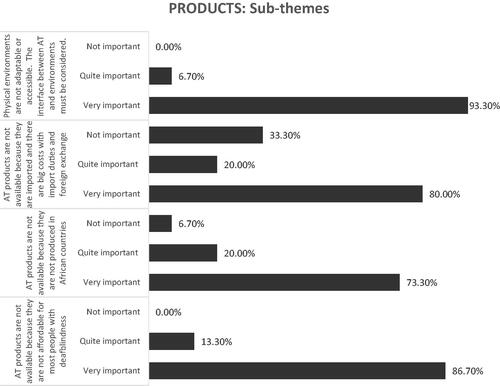
Figure 5. Rating of the importance of sub-themes of the “Provision” theme.
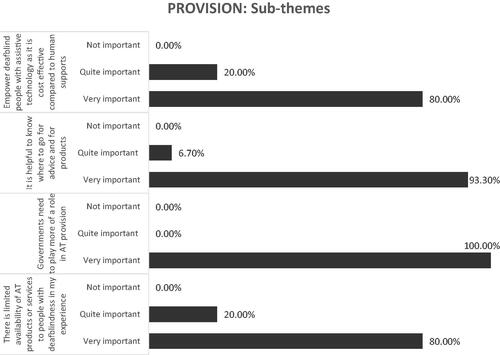
Figure 6. Rating of the importance of sub-themes of the “Personnel” theme.
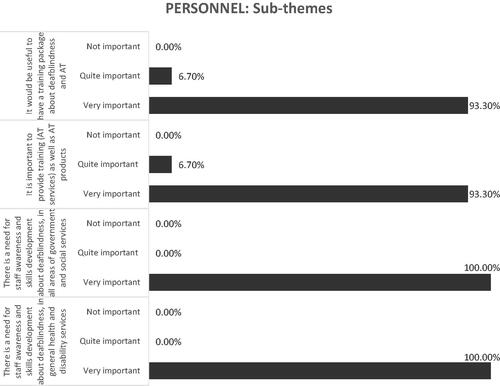
Table 3. Summary of Phase 2 data sub-themes.
Setting
Southern African Development Community (SADC), established in 1992, is a regional economic community, consisting of 16 low- and middle-income Member States [Citation59].
Study population
A heterogeneous e-Delphi expert panel, representing the diverse stakeholder group across the field of deafblindness in the SADC was selected. The criteria of eligibility to participate in the study were:
people with deafblindness over 18 years;
family members of people with deafblindness;
educators with a minimum of 3 years experience working in deafblindness;
researchers with a minimum of 3 years experience working in the field of deafblindness;
service providers with a minimum of 3 years experience working in the field of deafblindness;
representatives from advocacy groups who had a minimum of 3 years experience in working with people with deafblindness.
provides an overview of the demographics of the panelists.
Sampling method
Purposive and snowball sampling were undertaken to develop a list of potential participants for the Delphi expert panel. Selection occurred over 3 weeks (between mid-September and end-October 2020). An email advertisement was circulated to 96 identified stakeholders. Twenty-nine people from 10 countries within the SADC region, of the 96 stakeholders originally identified, agreed to participate and were emailed Participant Information Sheets, a link to the online survey, and the option to obtain an accessible MS Word version of the survey. Three reminders were issued to these 29 potential participants, with only 17 participants (representing 4 countries) responding and completing Delphi Phase 1. Of the 17 participants who completed Phase 1, 15 completed Phase 2 (representing 4 countries). The invitation to complete Phase 2 was provided to the Delphi panel with a 3-week completion period, including two email reminders. The full Delphi questionnaire is available upon request.
Data collection
Participants were asked to look at all MyATOF dimensions and state whether they perceived them to be (a) relevant to people with deafblindness, and (b) relevant to the SADC context. Participants were invited to provide additional comments about each section of the framework. Participants were anonymous to each other and the researchers giving equal opportunity and weighting to the ideas of each panel member [Citation56]. Qualtrics online survey software provided a secure and accessible platform to capture consent and survey responses. Three participants requested MS Word copies of the survey and returned these to the first author who uploaded the responses manually to Qualtrics.
Data analysis
Both quantitative and qualitative analyses were undertaken with the data from each Delphi round. Phase 1 responses were downloaded into a CSV file, with duplicates (n = 3) removed. The third author tabulated the quantitative data. The second author conducted an initial, thematic analysis of the qualitative responses using the first four steps outlined by Braun and Clarke [Citation60], transcription (not required for this study), reading and data familiarisation, coding, and searching for themes. Given the specific nature of the comments made by participants, an inductive approach was taken to determine broader themes reflected by the data. The themes arising from the initial analysis of comments made by participants in response to the questions in Phase 1 were reviewed by all authors (stage 4 of Braun and Clarke’s process for thematic analysis [Citation60]. The third author identified consistency between the themes emerging from the data and the WHO 5Ps. for example mapping the themes of the cost and lack of availability of AT, as barriers captured by Products, and Policy. Completion of the final two steps of the thematic analysis outlined by Braun and Clarke comprised defining and naming themes (completed by the third author) and finalizing the analysis (undertaken by all three authors, ensuring all the data was consistent with the 5Ps and determining sub-themes for each) [Citation60]. Phase 2 involved asking participants to rate (in order to prioritize) the importance of these themes derived from Phase 1. Participants were invited to provide additional comments (beyond responding to the individual questions). Phase 2 results were downloaded to a CSV file. The second author undertook an analysis of the qualitative data, using the existing themes from Phase 1 and expanding existing sub-themes or adding new sub-themes if the existing themes did not adequately capture new ideas emerging from the Phase 2 data. These expanded as well as the new themes were reviewed by authors one and three. Some further modifications were made until consensus was reached by all three authors.
Results
The quantitative and qualitative data from each of the two Delphi phases are presented overleaf. Considerable consistency was observed in both phases, apart from two sub-themes in the second phase. From the qualitative data, key issues were identified to be addressed regarding AT provision to people with deafblindness in the SADC region.
Phase 1 results
Overwhelmingly, 100% of the 17 participants in the Delphi panel, agreed that the set of questions in each section of MyATOF were relevant both to people with deafblindness and the SADC context. See for results of the quantitative data collection during Phase 1.
A summary of the qualitative data for each tool is presented below, followed by the 20 sub-themes organized against 5 key themes, which were consistent with the WHO 5 Ps [Citation8].
Tool A – My supports: What AT and other things do I use?
Prompts included examples of AT supports [Citation39] as follows: hearing amplification (e.g., hearing aids); low technology magnifiers (e.g., magnifying glass); high technology magnifiers (e.g., closed-circuit television); mobility products (e.g., long cane); visual or tactile alert devices and systems; screen enlargement software; screen reading software; refreshable braille displays; visual or tactile labels; human supports (e.g., interpreter, intervenor, communication guide, technology trainer, support worker, personal assistant); and environmental supports (e.g., large signs, braille signage, tactile ground surface indicators, audible traffic lights, and other audible signals).
In their responses, the panellists described the use of AT as enabling the achievement of outcomes and endorsed and expanded the sub-set of products suggested for deafblindness, noting that “Assistive technologies have played a pivotal role in helping the deafblind” (Panellist 21/3). Barriers include lack of access, appropriateness, training, availability, knowledge and family commitment and high cost, for example, “the inclusion of assistive technologies for the deafblind come[s] with financial obligations and still there has no[t] been commitments towards making the environment adaptable for the inst[a]llation of assistive technologies” (Panellist 21/3). These themes relate to the “Products” and “People” principles of the WHO 5 Ps.
Tool B – My outcomes: What does my AT enable me to do?
Prompts included the WHO activity and participation domains, suggesting that AT enables participation in mobility; self-care; communication; managing general tasks and demands (such as handling money, paying bills, organizing the day); managing domestic life (such as cooking, washing clothes, cleaning the home); learning and applying knowledge (e.g., remembering, writing, reading); relationships with others; an educational life (learning); an economic life (working, volunteering); a civic life (being part of the community); recreation and leisure; a spiritual life (able to worship); and political life (able to vote in person) [Citation7,Citation24].
Panellists endorsed the broad spectrum presented, with statements such as “everything is captured here” (Panellist 16/11) and identified an array of outcomes that are possible but yet not achieved in their country owing to a perceived lack of awareness of deafblindness in society, the need for knowledge/training in AT to assist interpreting guides to improve access, and the need for vocational guidance. One panellist (6/14) noted that “In most cases, deafblind do not have access to AT, making their lives difficult and unbearable”.
Tool C – My costs: How much does my AT cost? How much does my AT save?
Prompts provided definitions of costs (the price of the AT and any costs involved in set-up and maintenance); cost savings (including money that could be saved by the user or the government, by using AT. For example, a user might not need to purchase another piece of equipment or might need less support work hours); and downstream cost savings (avoiding costs in the future by investing in AT now. For example, if AT supports a user’s health, independence and safety, this might save visits to the doctor or to hospital).
Panellists identified costs as a major barrier because of “prohibitive AT costs” (Panellist 6/14) and noted that “AT is only available to those who can afford it. Government is not set-up for … ATs” (Panellist 5/0). A range of actions was proposed, including subsidies, import duties, and in-country production, which might address these issues in part. Solutions required action in the Policy and Products areas of the WHO GATE’s agenda.
Tool D – My Rights: How does AT meet a person’s human rights?
Prompts included a list of rights from the United Nations Convention on the Rights of Persons with Disabilities [Citation45] (Article 4: General obligations; Article 5: Equality and non-discrimination; Article 9: Accessibility; Article 19: Living independently and being included in the community; Article 20: Personal mobility; Article 21: Freedom of expression and opinion, and access to information; Article 24: Education; Article 25: Health; Article 26: Habilitation and rehabilitation; Article 27: Work and employment; Article 29: Participation in political and public life; Article 30: Participation in cultural life, recreation, leisure and sport; other articles of relevance).
Panellists described a lack of realization of rights, for example, “normally, deafblind persons rights are not made possible, for example, the right to education, independent mobility, participation in society, etc.” (Panellist 6/14). Lack of knowledge regarding basic human rights was linked to advocacy: “It is vital for the deafblind persons to be familiar with UNCRPD because it is an advocating tool for full inclusion and availability of accessible services” (Panellist 11/0). Roles for government and civil society (such as private companies) were identified: “Government is also not ready to implement most of these rights” (Panellist 5/0). The themes in the data about lack of implementation and lack of knowledge of rights, related to the “Policy” and “People” principles of the WHO 5 Ps.
Tool E – The AT Service Delivery Pathway
The pathway has been conceptualized as initiation, assessment, trial and solution selection, procurement, implementation (delivery/setup/trial), follow-up, and review [Citation50,Citation61].
Panellists endorsed the notion of a service delivery process, noting that “if one step is skipped the clients [might] be given wrong AT” (Panellist 20/06). Panellists suggested that services could be provided at various levels of skill and noted that there was no service delivery model of this kind in Africa, with one panellist stating that these steps were “currently not possible in Africa” (Panellist 6/14). These findings related to the “Provision” principle of the WHO 5 Ps.
Tool F – Customer experience
Based on the following prompts, drawn from the experience of Australian AT users [Citation51], panellists said they wanted:
the best combination of devices, personal care, and environmental design;
access to sufficient funding for good quality and long-lasting devices;
funding to meet AT needs in every area of life, based on a holistic assessment of needs, so that each product works well and does not interfere with other supports;
consideration of AT needs across people’s lifespan and as needs change;
support throughout the process of obtaining AT, including product trial, training, and maintenance;
access to resources when needed;
active involvement in decision-making;
consideration of personal preferences and identity so that AT is chosen to suit lifestyle and participation.
Rather than responses about being a consumer, this section elicited comments regarding inclusion, rights, and expertise, which are precursors to having a positive customer experience. Panellists identified the scarcity of AT and specific design features that would contribute to participation and inclusion; a lack of services: “In Africa there is hardly any existence of specialised services for deafblind persons” (Panellist 19/0); and the human right that: “Deafblindness must be treated equal like everyone” (Panellist 9/4). Aspirations included the hope that “deafblind persons in [the] African continent should also take part in ensuring full inclusion, participation, budgeting, and implementation of AT-related services” (Panellist 11/0). The themes related to the “Personnel” principle of the WHO 5 Ps.
See in the section below for the Phase 2 data for the five key themes and sub-themes identified in Phase 1.
Phase 2 results
In the Phase 2 survey, panel members were invited to identify the level of importance that each of the 20 sub-themes, derived from the Phase 1 data, held for addressing the assistive technology needs of people with deafblindness in the SADC region.
shows the responses of the panellists to the themes, derived from the Phase 1 data, regarding their importance in furthering AT outcomes for people with deafblindness in the SADC region. Of the six themes, which all participants counted as very important, “Governments need to play more of a role in AT provision” was reiterated frequently in the comments of the Delphi panel, for example, “I would suggest that government[s] in Africa need to play a big role and en[s]ure that more AT are provided in Africa” (Panellist 16/11).
Six of the 20 sub-themes were viewed as being very important by all members of the Delphi panel:
Raise awareness of deafblind people about social inclusion.
Government must implement the CRPD (human rights conventions).
Governments should make AT that is relevant to people with deafblindness available.
Governments need to play more of a role in AT provision.
There is a need for staff awareness about deafblindness and skills development in general health and disability services.
There is a need for staff awareness about deafblindness and skills development in all areas of government and social services.
Most of the sub-themes were viewed as being very important by more than two-thirds of the Delphi panel, with the remaining members viewing them as quite important.
Only the following two sub-themes were viewed as being not important by some members of the Delphi panel:
Deafblind persons should contribute to the cost of their AT (5 participants indicated “not important”).
AT products are not available because they are not produced in African countries (1 participant indicated “not important”).
Additional comments were added by panellists to the Phase 2 questionnaire. Most comments reiterated existing sub-themes, but some new themes emerged, and some existing themes were extended. New and extended sub-themes, that emerged from comments submitted during the Delphi Phase 2, have been described below.
Theme 1: people
In their responses (refer to ), panellists identified the key role of stakeholders, their awareness, knowledge, and exposure, in realizing the potential of using assistive products to achieve the quality of life, productivity, access to opportunities, and enabling people to “follow our dreams to fulfil our passion and enrich others lives” (Panellist 15/17). Systemic barriers, such as lack of access to information, inadequate or ineffective policy and legislation, and lack of availability in early childhood settings and schools were identified.
Based on the data from Phase 2, the fourth sub-theme was extended to “There is a need to develop the assistive-technology-related skills of family members and support networks” and an additional theme was identified: ‘The value of peer support’.
Theme 2: policy
Policy was regarded as being a highly relevant aspect of access to AT, with panellists identifying the impact of policies upon costs and financial access (refer to ). Some policy solutions were offered to legislate the right to AT and to enforce compliance, for example, “AT should be legalised and a mandatory requirement for all public and private institutions” as well as social protection (Panellist 21/3); affordability: “Not all can manage to contribute something towards AT as most of them come from very poor families” (20/06); and nuanced inclusion of people with deafblindness in general policy. Civil society, as well as government, were regarded as duty holders to enact better policies, and organizations for people with disabilities should prioritize the matter in their advocacy work (6/14). There was strong concurrence by panellists on all themes except the question of who should pay for AT.
Two new themes were identified: “The need for policies about AT to have an implementation plan and to be actioned”, and that: “People with deafblindness themselves should be involved in the process of developing AT policies”.
Theme 3: products
Broad agreement was evident across themes, with panellists noting that AT products play a critical role: “Braille and Assistive Listening Technology are the most important methods (refer to ). Deafblind people can experience the world of sound” (Panellist 15/17). “AT products should indeed be affordable and reliably supplied” (Panellist 12/10). Panellists were divided over whether AT is best produced locally or whether import barriers should be lifted, with suggestions including both lowering of taxes and increasing design and production in Africa: “Governments must waive all import excise and customs duties on AT products…. Governments must facilitate local design and manufacture of AT products which adequately meet the needs of their respective deafblind communities” (Panellist 7/16).
A fifth theme was identified also that: “AT needs to be user-friendly/easy to use, and durable”.
Theme 4: provision
The comments submitted by panellists were consistent with original themes and with the WHO. Data from Phase 1 and Phase 2 (refer to ) indicated the relevance of the AT service delivery steps, which constitute “good practice” in AT provision, that is, awareness: “More awareness raising on assistive technology available and on what deafblind community unique needs are” (Panellist 8/12); advice, education, maintenance: “Having places where [to] get advice on how to use and care [for] AT” (Panellist 20/6); and provision, all underpinned by the fundamentals of rights: “Primary health and government must come on board with the provision of assistive technology” (Panellist 8/12); and enabling attitudes: “There is need to combat negative beliefs about AT provisions, such as AT provisions are a budget constraint” (Panellist 21/3).
The second sub-theme was extended to: “Governments need to play more of a role in AT provision (noting roles undertaken by civil society including large corporates, donors, advocacy groups)”, and a new sub-theme was added: “There is a need for strategies and processes to ensure AT provision in rural areas”.
Theme 5: personnel
A very high level of concurrence with the themes was noted. The panellists provided a clear picture of the pivotal role of personnel in enabling AT access and use (refer to ). A need for targeted education at vocational and higher education levels was identified repeatedly: “AT training must be offered to institutions and NGOs that provide services to deafblind learners, adults and their families/caregivers” (Panellist 7/16).
A blueprint for addressing this was offered: “DeafBlind South Africa [has] a dream of establishing a development centre for the deafblind community, family and caregivers to provide the distribution and skilled training on assistive technology as well as living skills training, central social services, occupational therapy service and counselling services. It is a whole one-stop package we would like to provide to the DeafBlind community – but infrastructure costs is our greatest stumbling block due to a lack of funding!” (Panellist 8/12).
From the data provided in Phase 2, the fourth sub-theme was extended to: “It would be useful to have a training package about deafblindness and AT and training packages available at tertiary student and workforce levels”, and a fifth theme emerged as: “[A] need for cultural/religious awareness and sensitivity to age of client”.
Discussion
The discussion of the findings of this study has been presented according to the three aims of the study.
How relevant and valid is MyATOF for use with people with deafblindness in the SADC region?
This study found the MyATOF dimensions to be relevant and hold face validity, suitable for use with people with deafblindness in the four countries represented, namely, Malawi, South Africa, Zambia and Zimbabwe. The dimensions (supports, outcomes, costs, rights, and service delivery) were recognizable to the panellists, and strongly related to the issues that the panellists faced. A powerful theme of AT under-realization or unavailability pervaded the Delphi responses. This was consistent with the Australian experience, where AT users noted that they might not have the supports required to realize potential outcomes fully or to meet their human rights fully [Citation53,Citation54]. Similarly, service-delivery contexts might not provide a satisfactory service-delivery outcome or customer experience. However, the data collected from Africa suggested a far higher level of under-realization, particularly in the latter dimension of customer experience.
While all fourteen countries in the SADC region were targeted during the recruitment phase of this study, panellists represented only four countries, so it is not possible to extrapolate to the whole SADC region.
What refinements to MyATOF might be required to increase its relevance and validity in this context?
The data from the Delphi study revealed underlying issues in AT systems within four countries within Southern Africa, which influence the capacity of people with deafblindness to realize their potential to participate fully in AT as measured by MyATOF. Analysis using the systems lens of WHO 5 P’s has illuminated the forcefield of supply network and social policy issues which underpin the realization of rights and outcomes for people using AT. Based upon these findings, MyATOF does not require refinement in its dimensions or granularity. Nevertheless, foregrounding a person’s context will be considered in the next iteration of the framework, that is, specifying and naming the impact of systems upon an individual.
An analysis of the panellists’ countries of origin demonstrated differences between economic status [Citation18] which could have influenced the responses received. Malawi is considered to be a low-income country, remaining one of the poorest countries in the world; Zambia, with its stalled economy, along with Zimbabwe, currently in an economic crisis, are both classified as lower-middle-income countries; and South Africa is considered to be an upper-middle-income country, despite having one of the highest inequality rates in the world.
Common responses, received from panellists outside South Africa, referred to the need for cogent AT policy, access to AT (free or at low cost or through donations), local manufacturing to reduce costs and increase access, the need for social protection, organizations of persons with disability (OPDs) to advocate for AT, and that AT that is provided/made available is context relevant. Panellists from South Africa, on the other hand, highlighted the need for legislation, focusing on the human rights element and the provision of AT through resource centres and new supply chains. There was also an expressed need concerning training in AT across all levels of education, that is, primary, secondary and post-secondary. These differences could be ascribed to varying country contexts, including economic, social and political disparities. Further specific research is required to better understand commonalities and differences between countries in Africa.
What has been learned about the context of AT provision and use by people with deafblindness in the SADC region?
Findings and implementation priorities from the data have been presented according to the WHO 5 P’s [Citation7]:
People
The WHO proposes the following principles related to AT People (users and families). Involving users and their families in all interventions is crucial. A user-centred approach is critical to make sure that users’ needs are addressed when developing policies and provision of services. Services should not just be accessible physically, but also appropriate culturally and tailored to users’ needs [Citation7].
The panellists concurred, noting that the circle of support for people with deafblindness includes teachers and communication partners, and calling for a societal attitudinal change towards a focus on abilities, not disabilities.
Policy
In terms of AT Policy, the WHO proposes that countries should develop national policy and programmes to ensure everyone, everywhere can access assistive products. The WHO is building assistive technology assessment toolkits and guidance on financing mechanisms to ensure the sustainability of service provision and universal access, as well as producing guidance also on the implementation of a Priority Assistive Products List with minimum standards, appropriate training, and service provision [Citation7].
The top priorities of the panellists included: laws to ensure access to AT to support learning and independence; governments to implement their commitments to policy and be held accountable; and governments to fund AT to increase access and to provide social protection. Panellists called specifically for people with deafblindness to be consulted and involved with the development of AT-related policies, and that access to AT should be assured through governments as well as the private sector, while organizations of people with disabilities should prioritize advocacy for improved AT policies.
Products
The WHO promotes a range of strategies to strengthen product availability including the WHO Priority Assistive Products List [Citation62]. This encourages countries to develop a list of national priority products and is a guide to enhance production, procurement and service provision, to develop reimbursement policies and to shape markets [Citation7].
The panellists agreed with the sub-set of AT for deafblindness presented in this research, noting several additional products (e.g., Job Access Without Speech (JAWS) screen reading software) and focussing on supply network issues. Congruent with the WHO view of market-shaping referred to above, top priorities included removal of import barriers and taxes, and enhanced local manufacturing to reduce costs and ensure availability; also, high-quality and fit-for-purpose products, utilization of alternate funding pathways and innovative supply options such as refurbishment and redistribution of AT products.
Provision
The WHO suggests that AT service provision should include universal access and should enable early intervention. People should be able to access assistive products for all their functional needs from a single point. The WHO is developing guidance on innovative models of service provision around the globe. Fundamental components include (a) health systems that make service provision for assistive products, and (b) networks of specialist referral centres connected to primary healthcare infrastructure [Citation7].
The panellists supported the call for universal access and early intervention. The specific specialist set of skills for working with deafblindness reinforced the notion of single points of service, possibly with prioritized access to information, for example, resource centres. Other priorities included knowing what is available, trialling products, and guidance on care and maintenance. A business case for investment in AT by governments was proposed, with a focus on services and support in rural, not only urban, areas and, with the aim of realizing human rights, safety, security, independence, and access to information.
Personnel
AT Personnel, as defined by WHO, must be available and accessible to AT users and possess skills in culturally safe assessment and prescription, fitting and user training, follow-up, maintenance and repairs. A WHO Assistive Products Training Package is underway to develop skills in providing AT to support countries in building the capacity of their community-level workforce [Citation7].
The panellists concurred on the need for widespread training for people with deafblindness and their families and extends to civil society and professionals. A point that differed from the WHO stance, specific to deafblindness, was the need for specific training of personnel in deafblindness, in particular, deafblind communication methods. Further, panellists called for AT service provision to be included in relevant curricula, for example, in all health sciences fields with a focus on vocational education and the need for continuous professional development (CPD). Further priorities outlined were training of service providers and other individuals working with people with deafblindness and for information related to AT products to be accessible (in multiple languages) and comprehensible.
Strengths and limitations
MyATOF is a data capture and storytelling tool under development, without the psychometric properties of formal AT outcome measures. It does not replace formal outcome measurement but, as a consumer-focussed, whole-of-system approach, it fills a gap in capturing and systematizing experiential knowledge.
All key stakeholder groups were represented on the Delphi panel, however, only 4 of the 14 countries in the SADC region were represented in the data from the second survey. While the data were consistent, it is necessary to seek data from other SADC countries in future studies in order to better understand the situation within the whole region.
Implications and recommendations
Researchers must consider the context in which they are situated to capture the impact of socio-political and economic systems on the AT user [Citation63,Citation64]. This study indicated that supports, outcomes, costs, rights, service delivery steps and customer experiences (dimensions captured with MyATOF framework) are relevant to people with deafblindness in 4 countries in the SADC region. It identified that stakeholders see MyATOF dimensions as relevant to express the realities of life for AT users and to raise awareness of the potential outcomes of AT and its current undersupply. In Australia, AT users utilize the self-reports generated by the MyATOF online tool to support discussions between AT users and AT funders within existing AT service delivery frameworks or use their data to lobby for the improvement of systemic AT issues such as inequitable funding. Furthermore, this study suggests that considerable work is required to improve systemic access to AT in the Southern African context. Local stakeholders may, like their Australian counterparts, choose to tell their stories of “rights met and unmet” using these 6 dimensions and to engage in systemic advocacy and empowerment initiatives to alert relevant duty bearers to improve services, systems and therefore outcomes.
Conclusion
While contexts differ, AT users globally, including those with deafblindness, share common, unifying, human experiences and aspirations. In MyATOF these are conceptualized as supports, outcomes, costs, rights, service delivery steps and customer experiences, and are operationalized using available taxonomies and evidence. The results of the Delphi process undertaken with deafblind stakeholders across 4 countries in the SADC region support the face validity of the framework dimensions. Analysis of the data suggested that the experience of accessing AT and achieving participation outcomes is extremely challenging, and the evidence generated could be clearly mapped onto an AT systems view based on the WHO 5 Ps model. This is a critical point, as the achievement of individual outcomes must be viewed in the context of systemic barriers. From a human rights perspective, it appears that tools such as those offered by MyATOF have the potential to enable the collection of individualized data and self-advocacy and to contribute to the systemic advocacy necessary for the realization of rights. It is hoped that the MyATOF platform contributes to the state of the art in AT research by guiding consumers and their AT practitioners to report the outcomes of their AT solutions across a range of impact areas.
Acknowledgements
The authors wish to thank Deafblind International for providing financial support through a competitive grant through the African Research Initiative to undertake this project.
Disclosure statement
No potential conflict of interest was reported by the author(s). The views expressed in the submitted article are the authors’ own and not an official position of their institutions or the funder.
Data availability statement
Data from the two Delphi rounds are available from the first author upon request. Further information on the MyATOF Framework is available from the third author upon request.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Groce N, Kett M, Lang R, et al. Disability and poverty: the need for a more nuanced understanding of implications for development policy and practice. Third World Quarterly. 2011;32(8):1493–1513.
- Hosseinpoor AR, Stewart Williams JA, Gautam J, et al. Socioeconomic inequality in disability among adults: a multicountry study using the world health survey. Am J Public Health. 2013;103(7):1278–1286.
- Khasnabis C, Mirza Z, MacLachlan M. Opening the GATE to inclusion for people with disabilities. The Lancet. 2015;386(10010):2229–2230.
- Borg J, Östergren P, Larsson S, et al. Assistive technology use is associated with reduced capability poverty: a cross-sectional study in Bangladesh. Disabil Rehabil Assist Technol. 2012;7(2):112–121.
- Tebbutt E, Brodmann R, Borg J, et al. Assistive products and the sustainable development goals (SDGs). Global Health. 2016;12(1):1–6.
- MacLachlan M, McVeigh J, Cooke M, et al. Intersections between systems thinking and market shaping for assistive technology: the SMART (Systems-Market for assistive and related technologies) thinking matrix. IJERPH. 2018;15(12):2627.
- World Health Organisation. Policy brief: access to assistive technology. Geneva (Switzerland): WHO; 2020.
- MacLachlan M, Scherer M. Systems thinking for assistive technology: a commentary on the GREAT summit. Disabil Rehabil Assist Technol. 2018;13(5):492–496.
- World Federation of the Deafblind. At risk of exclusion from CRPD and SDGs implementation: inequality and persons with deafblindness. Geneva (Switzerland): World Federation of the Deafblind; 2018.
- Cantin S, De Abreu Cybis W, Trudeau S, et al. Assessment of a communication assistive technology for individuals with deafblindness: a case study. JDBSC. 2019;5(1):73–95.
- Cantin S, de Abreu Cybis W, Durocher N. Setup by a person with deafblindness of a face-to-face communication assistive technology based on generally available applications. Disability and Rehabilitation: Assistive Technology. 2020;1–7. DOI:10.1080/17483107.2020.1751315
- Wittorff MM. Communication guide support for Western Australians with deafblindness: a pilot project. Perth (Australia): Curtin University; 2014; p. 214.
- Raanes E, Berge SS. Sign language interpreters use of haptic signs in interpreted meetings with deafblind persons. Journal of Pragmatics. 2017;107:91–104.
- Hatakeyama T, Watanabe T, Takahashi K, et al. Development of communication assistive technology for persons with Deaf-Blindness and physical limitation. Stud Health Technol Inform. 2015;217:974–979.
- Dyzel V, Oosterom-Calo R, Worm M, et al. Assistive technology to promote communication and social interaction for people with deafblindness: a systematic review. Front Educ. 2020;164.
- Wittich W, Granberg S, Wahlqvist M, et al. Device abandonment in deafblindness: a scoping review of the intersection of functionality and usability through the international classification of functioning, disability and health lens. BMJ Open. 2021;11(1):e044873.
- Perfect E, Jaiswal A, Davies TC. Systematic review: Investigating the effectiveness of assistive technology to enable internet access for individuals with deafblindness. Assist Technol. 2019;31(5):276–285.
- The World Bank. Inclusion matters - the foundation for shared prosperity. Washington (DC): World Bank; 2013.
- Layton N, Bell D, Buning ME, et al. Opening the GATE: systems thinking from the global assistive technology alliance. Disabil Rehabil Assist Technol. 2020; 2020/07/0315(5):484–490.
- Matter RA, Eide AH. Access to assistive technology in two Southern African countries. BMC Health Serv Res. 2018;18(1):792. DOI:10.1186/s12913-018-3605-9
- Matter R. What works to increase access to assistive technology in Southern Africa. Cape Town (South Africa): University of Cape Town; 2020.
- Visagie S, Scheffler E, Seymour N, et al. Assistive technology service delivery in South Africa: conceptualising a systems approach. In: Kathard H, Padarath A, Galvaan R, editors. South African health review. Durban (South Africa): Health Systems Trust; 2020.
- Deafblind Australia. What is deafblindness Australia [Internet]. Burswood (Australia): Deafblind Australia; 2021 [cited 2021 January 30]. Available from: https://www.deafblind.org.au/deafblind-information/what-is-deafblindness/
- World Health Organisation. World report on disability. Geneva (Switzerland): World Health Organisation; 2011.
- Matter R, Harniss M, Oderud T, et al. Assistive technology in resource-limited environments: a scoping review. Disabil Rehabil Assist Technol. 2017; 2017/02/1712(2):105–114.
- Fuhrer MJ, Jutai JW, Scherer MJ, et al. A framework for the conceptual modelling of assistive technology device outcomes. Disabil Rehabil. 2003;25(22):1243–1251.
- Smith R, Scherer M, Layton N. Committing to AT outcomes and synthesizing practice, research and policy. In: Layton N, Borg J, editors. Global perspectives on assistive technology: proceedings of the GReAT Consultation 2019. Geneva (Switzerland): World Health Organization; 2019. p. 196–217.
- Federici S, Scherer M, editors. Assistive technology assessment handbook. Boca Raton (FL): CRC Press; 2017.
- Dijkers M. When the best is the enemy of the good: the nature of research evidence used in systematic reviews and guidelines. Austin (TX): NCDDR Task Force on Systematic Review and Guidelines; 2009.
- Federici S, Scherer MJ, Ehrlich-Jones L. Measurement characteristics and clinical utility of the assistive technology device predisposition assessment (ATD PA) among mixed patient populations. Archives of Physical Medicine and Rehabilitation. 2021;102(4):805–806.
- Demers L, Weiss-Lambrou R, Ska B. The Quebec user evaluation of satisfaction with assistive technology (QUEST 2.0) An overview and recent progress. TAD. 2002;14(3):101–105.
- Day H, Jutai J. Measuring the psychosocial impact of assistive devices: the PIADS. Canadian Journal of Rehabilitation. 1996; 9(2):159–168.
- Andrich R. Tracking individual assistive technology interventions and measuring their outcomes. In: Miesenberger K, Fels D, Archambault D, Peňáz P, Zagler W, editors. Computers helping people with special needs. Cham (Switzerland): Springer; 2018.
- Wessels R, Persson J, Lorentsen O, et al. IPPA: individually prioritised problem assessment. TAD. 2002;14(3):141–145.
- Scherer MJ. Living in the state of stuck: how assistive technology impacts on the lives of people with disabilities. 4th ed. Brookline (MA): Brookline Books; 2005.
- Wessels RD, de Witte L, van den Heuvel W. Measuring effectiveness of and satisfaction with assistive devices from a user perspective: an exploration of the literature. TAD. 2004;16(2):83–90.
- Jutai J, Fuhrer MJ, Demers L, et al. Toward a taxonomy of assistive technology device outcomes. American Journal of Physical Medicine and Rehabilitation. 2005;84(4):294–302.
- Lenker J, Harris F, Taugher M, et al. Consumer perspectives on assistive technology outcomes. Disabil Rehabil Assist Technol. 2013;8(5):373–380.
- ISO. ISO 9999 Assistive products for persons with disability — Classification and terminology. 2016.
- NED. Australia's National Equipment Database. 2021. [cited 2021 Sep 18]. Available from: https://www.askned.com.au/
- World Health Organization. International classification of functioning, disability and health: ICF. Geneva (Switzerland): World Health Organization; 2020.
- Layton N, Shih S. Economic pathway analysis for assistive technology: a pilot study from Australia. Paper presented at the RESNA Annual Conference; 2018 August 3; Arlington, VA.
- Layton N, Irlam C. Assistive technology for older Australians: rapid evidence review and economic pathway analysis. Canberra (Australia): National Aged Care Alliance; 2018.
- Carter R, Vos T, Moodie M, et al. Priority setting in health: origins, description and application of the Australian Assessing Cost-Effectiveness initiative. Expert Rev Pharmacoecon Outcomes Res. 2008;8(6):593–617.
- United Nations. Convention on the rights of persons with disabilities and optional protocol. Geneva (Switzerland): United Nations; 2006.
- Watchorn V, Layton N. Advocacy via human rights legislation - the application to assistive technology and accessible environments. Australian Journal of Human Rights. 2011;17(1):117–138.
- Desideri L, Salatino C, Pigini L, et al. Using a standard procedure to assess assistive technology service delivery outcomes: a proposal from the Italian network of independent assistive technology centres. In: Layton N, Borg J, editors. Global perspectives on assistive technology: proceedings of the GReAT Consultation 2019. Geneva (Switzerland): WHO; 2019.
- Dijcks BPJ, Wessels RD, de Vlieger SLM, et al. KWAZO, a new instrument to assess the quality of service delivery in assistive technology provision. Disability and Rehabilitation. 2006; 2006/01/0128(15):909–914.
- Larsson Ranada Å, Lidström H. Satisfaction with assistive technology device in relation to the service delivery process-A systematic review. Assist Technol. 2019;31(2):82–97.
- AAATE. Excellence in the process of AT provision. Linz (Austria): Johannes Kepler University; 2018.
- De Jonge D, Layton N, Vicary F, et al. Motivations and incentives: exploring assistive technology service delivery from the perspectives of multiple stakeholders. In: Yih-Kuen J, Ray G, editors. RESNA 2015: new frontiers in assistive technology. Denver (CO): RESNA; 2015.
- Layton N, Volkert A, Joyce R. ARATA/AFDO/OTA Breakfast Forum on Assistive Technology. Australian Assistive Technology Conference; 2018 November 15; Melbourne, Australia.
- Layton N, Noonan M, O’Connor J. My assistive technology outcomes framework – a collaborative tool for AT users and their practitioners. Melbourne (Australia): AOPA; 2019.
- Layton N, Thomson C, Noonan M. Consumer-defined outcomes: applying the assistive technology outcomes framework applied to wheeled mobility and seating. Melbourne (Australia): Oceania Seating Symposium; 2019.
- Layton N, Doyle L, Volkert A. My Outcomes Framework: synthesising the evidence on valued outcomes into a set of user-led and policy-relevant tools. Paper presented at the Occupational Therapy Australia 28th National Conference and Exhibition; 2019 July 10; Sydney, Australia.
- Keeney S, Hasson F, McKenna H. The Delphi technique in nursing and health research. Chichester (UK): Wiley-Blackwell; 2011. p. 1–17.
- Ogbeifun E, Agwa-Ejon J, Mbohwa C, editors. The Delphi technique: a credible research methodology. Paper presented at the 2016 International Conference on Industrial Engineering and Operations Management; 2016 March 8–10; Kuala Lumpur, Malaysia.
- Jünger S, Payne SA, Brine J, et al. Guidance on conducting and REporting DElphi studies (CREDES) in palliative care: Recommendations based on a methodological systematic review. Palliat Med. 2017; 2017/09/0131(8):684–706.
- Southern African Development Community - Towards a common future. 2012. [cited 2021 Sep 1]. Available from: https://www.sadc.int/about-sadc
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
- Renzo A, Niels-Erik M, Evert-Jan H, et al. Service delivery systems for assistive technology in Europe: an AAAT E/EAST IN position paper. Technol Disabil. 2013;25(3):127–146.
- World Health Organisation. Priority assistive products list. Geneva (Switzerland): World Health Organisation; 2017.
- Boisselle A, Grajo L. They said: a global perspective on access to assistive technology. The Open J Occup Ther. 2018;6(3):2.
- Berghs M. Practices and discourses of ubuntu: Implications for an African model of disability? Afr J Disabil. 2017;6:292.