
Abstract
Arthroscopically assisted techniques for the treatment of foveal triangular fibrocartilage complex (TFCC) injuries offer a less invasive option. Reports of the ulnar tunnel technique on a larger patient population are needed. This prospective cohort study of 44 patients aimed to evaluate the clinical and patient-reported outcome after arthroscopic foveal re-attachment using a novel, modified ulnar tunnel technique. Furthermore, preoperative magnetic resonance imaging findings were compared with the findings from the arthroscopic evaluation. History of ulnar sided wrist pain, positive fovea-sign at the clinical examination and positive hook test at the surgery were the main inclusion criteria for the study. Pain, grip strength, wrist motion and patient-reported outcomes were assessed pre-and postoperatively. The follow-up of this study was 31 months (range 18–48). No complications occurred during the surgery. All outcomes improved besides the range of motion, which remained unchanged. Pain on a visual analogue scale was 63 before, and 14 after the surgery (p = .0004). Pre- and postoperative values of Disability of Arm, Shoulder and Hand Questionnaire were 41/6, respectively (p = .007). Grip strength, measured in Kilogram-force were 29 and 36, pre-and postoperatively (p = .0004). Conspicuously, all patients achieved stability. Six patients needed re-operation, three for renewed injury. Thirty-nine of 44 patients scored excellent or good on the satisfaction score. We found the devised method to be with fewer complications and with favourable results compared with other techniques for the treatment of TFCC injuries. Level of evidence: III.
Introduction
Traumatic disruption of the triangular fibrocartilage complex (TFCC) is a common cause of ulnar-sided wrist pain. It is often associated with weakened grip strength, impaired function of the wrist and ‘giving way’ symptoms of the forearm. TFCC injuries are present in up to 90% of displaced distal radius fractures [Citation1] but can also occur after minor wrist trauma.
Initially, Palmer’s classification [Citation2] distinguished traumatic from degenerative TFCC injuries, and traumatic injuries were divided into four different subtypes. Type 1B injuries were considered more suitable for repair than other subtypes, where only debridement was helpful. Later, Atzei’s classification – a more explanatory and clinically relevant classification [Citation3] – further divided type 1B injuries into foveal (proximal), capsular (distal) or combined (complete). Moreover, anatomic studies [Citation4–6] had shown the importance of foveal TFCC attachment as a major stabiliser of the distal radio-ulnar joint (DRUJ).
Most of these injuries heal, but those that do not respond to conservative treatment are treated either by open repair or by arthroscopic surgery techniques. Luchetti et al. [Citation7] compared open and arthroscopic-assisted foveal TFCC repairs and found similar results regarding postoperative pain, Anderson et al. [Citation8] showed comparable results between open and arthroscopic repair of the TFCC. However, increased postoperative nerve pain caused by the ulnar nerve sensory branch was found in the open group, compared with the arthroscopic group. While this difference was not statistically significant, it could be highly clinically relevant. Similarly, a difference was found for the postoperative extensor carpi ulnaris (ECU) tendinitis, favouring the patients treated arthroscopically.
Arthroscopically assisted techniques have recently been developed, offering a less invasive option. Foveal avulsions have been treated either by foveal attachments to an anchor [Citation9–13] or by foveal fixations using the drilling tunnels through the ulnar bone. The drilling of the ulna was performed from proximal to distal, ending just beneath the injured foveal part of the TFCC. This could be achieved either by inserting two parallel K-wires, making a suture placement possible [Citation14,Citation15] or by drilling a single osseous tunnel, thus creating a working portal for the foveal fixation [Citation16–19]. While the parallel ulnar tunnel technique reported some instability problems, both ulnar tunnel techniques used periosteal knots and consequently painful irritation in some patients.
Arthroscopic evaluation represents a gold standard both for the determination of the TFCC injury, as well as for the determination of the injury type. The accuracy of MRI studies for the evaluation of foveal TFCC injuries has been sparely investigated [Citation20,Citation21].
Further knowledge of the ulnar tunnel technique on a larger patient population was needed. Besides, the absence of positive MRI scan findings with the presence of positive clinical and arthroscopic findings is still controversial. The purpose of this study was to evaluate the clinical and patient-reported outcome after arthroscopic TFCC foveal re-attachment by the modified ulnar tunnel technique, using a double-bundle fixation, and without using periosteal knots.
Methods
We treated 44 patients with the modified Iwasaki ulnar tunnel technique for foveal re-attachment of TFCC injury (Atzei Class 3) during April 2013 – September 2019. Overall, 77 patients referred to diagnostic wrist arthroscopy caused by chronic ulnar-sided wrist pain and mild instability of the DRUJ, were assessed clinically and radiographically. Thirty-three patients had to be excluded according to exclusion criteria, leaving 44 patients eligible for inclusion in this study. Mild instability was defined with a soft endpoint during the clinical assessment. The main inclusion criteria for this study was a positive fovea-sign according to Tay et al. [Citation22], and a positive hook test during the arthroscopic evaluation of TFCC injury. The main exclusion criteria for this study were: age under 16 years, acute TFCC injuries (< 3 months), patients with degenerative cartilage changes of the DRUJ (irreparable TFCC), distal or complete (Atzei Class 1 and 2) TFCC injuries and patients with a gross DRUJ instability. All excluded patients’ injury patterns and treatment history are shown in .
Table 1. A consort of 33 patients who were excluded from this study, thus receiving treatment accordingly to their injury pattern. These patients did not present foveal injury on the arthroscopic evaluation (hook test – negative).
Thirty-two patients from our series had preoperative MRI scans with 1.5 Tesla MRI scanners (GE Healthcare, General Electric, USA). The condition for a preoperative MRI scan was ulnar wrist pain and the criteria for a positive finding of a TFCC tear was if any type of TFCC injury was founded on the MRI examination. Negative or uncertain MRI – scan findings before the surgery was not a reason to exclude from this study [Citation20]. For this reason, the final diagnosis, and the indication for the surgical fixation for the foveal TFCC injury, and thereby inclusion in this study was consequently established intraoperatively by the positive hook test [Citation23].
All the relevant demographic data of the included patients are presented in .
Table 2. Demographic data of the included patients.
Time from injury to surgery was 23 months (range 3 − 96 months). Data were recorded prospectively, before the operation and at the follow-up examinations. The patients were followed at 2 and 6 weeks and 3, 6 and 12 months postoperatively, thereafter annually. The prospective evaluation included assessment of pain (VAS score), both in rest and activity, on a scale from 0 to 100, 0 indicating no pain and 100 indicating maximal pain. Grip strength was measured with a Jamar hydraulic hand dynamometer, using level 2 (North Coast Medical, Morgan Hill, USA). Patient-reported functional outcomes were assessed with the Danish, quick version of the Disability of Arm, Shoulder and Hand Questionnaire (qDASH). Range of motion (ROM), including rotation of the wrist, was measured with a goniometer pre-and postoperatively. Patients’ satisfaction and assessment of DRUJ stability were obtained after the treatment, where the planned follow-ups were undertaken. All patients gave signed written consent for the use of their medical data for this study. Approval for the study was granted by the Danish Patients Safety Authority under reference: R-20082124.
Operative technique
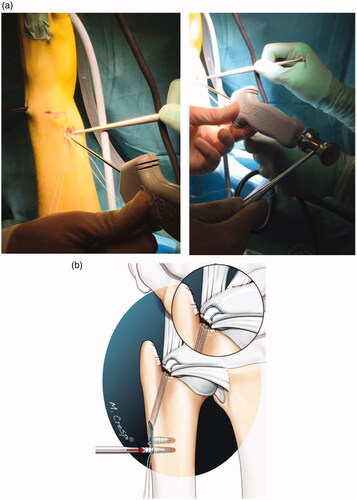
The operative technique follows to some extent the description of Iwasaki and Minami [Citation24]. The original technique described drilling the osseous tunnel (2.9 mm in diameter), outside-in through distal ulna, ending in the dorso-ulnar part of the TFCC complex. Single, 2-0 non-absorbable suture (Prolene, Ethicon, Somerville, USA) was used for the foveal stitch and was thereafter pulled out and tied into the ulnar periosteum. The postoperative bleeding from the cancellous bone tunnel enhanced the healing of the foveal re-attachment, thus securing firm and stable fixation. We modified this technique ensuring easier instrumentalisation, enabling double suture placement and avoiding using knots on the ulnar periosteal bone. The modification of the original technique included drilling a 3.2-mm bony tunnel by cannulated drill, over the inserted 1.2-mm K-wire, which was installed either using a C-Ring guide (Arthrex, Naples, USA) or by using free-hand placement. For the foveal suture, two FiberWire or FiberStick (Arthrex, Naples, USA) were used and pulled out using Micro SutureLasso Straight (Arthrex, Naples, USA) (). Double fixation with 2.5 mm × 8 mm. Mini PushLock PEEK Suture Anchors (Arthrex, Naples, USA) was used, after loosening the tension on the wrist arthroscopy traction tower, and in the forearm in neutral rotation. Two additional (2.5 mm in diameter, approximately 8–10 mm in length) bony canals were then drilled proximally from the working tunnel in the ulna, using the same, proximally extended skin incision. Knotless fixation under direct visualisation was then performed. While pulling the sutures in opposite direction, proper tension of the foveal reconstruction was ensured, and the final fixation was performed using a light hammer (). All the operative procedures were conducted by a single surgeon in the lateral infra-clavicular regional anaesthesia, using 3/4 wrist arthroscopy portal as an instrumentation portal and 6 R as a working portal.
All patients were immobilised for 2 weeks in a modified sugar tong splint including the elbow with the limitation of the forearm rotation, and thereafter by a removable orthosis with limited rotation for further 4 weeks. Hand therapy included gradually movement- and weight-increasing exercises. Full weight-bearing activities were allowed at 3 months, postoperatively. Contact sports and heavy, full weight-bearing activities without orthosis were allowed at 6 months.
Figure 1. (a) Intra-operative picture of the preoperative drawing, the guide-wire placement, and the 3.2 mm cannulated drill. NOTE: striped lines are depicting the patient’s ulna, while the tipped, bold line is the guide for the free-hand guide-wire placement. (b) Intra-articular guide-wire placement.
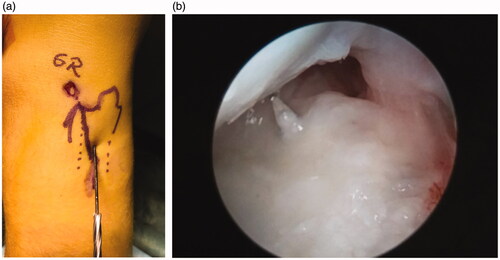
Figure 2. (a) The placement of the Micro SutureLasso Straight through the ulnar tunnel and the grasper through the 6 R arthroscopic portal. (b) The grasper is pulling the wire-loop from the SutureLasso.
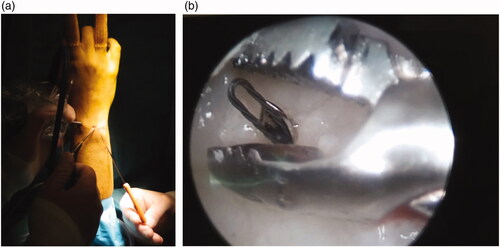
Figure 3. (a) The placement of two transosseous FiberWire sutures through the foveal aspect of the TFCC complex. The wire-loop is pulled out of the joint, through a 6 R arthroscopic portal using a grasper. (b) Then, the wire-loop is fed by the suture to be retracted back throughout the working tunnel.
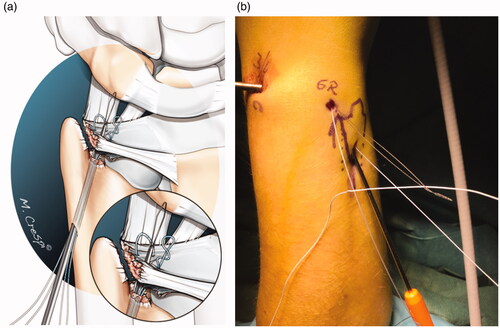
Figure 4. (a) Final fixation into the 2.5-mm predrilled bony canals in the ulna. Knotless fixation of the foveal TFCC reconstruction using 2.5 mm × 8 mm. Mini PushLock PEEK Suture Anchors using a hammer. Note: During this procedure, the tension on the arthroscopy traction tower must be lowered. (b) The final, knotless fixation of the fovea only TFCC injury.
Statistics
A non-parametric Wilcoxon’s signed-rank test was used for comparing data not normally distributed (qDASH scores), and the paired parametric Welch t-test was used for normally distributed data (pain and VAS scores, range of motion, and grip strength). Significance was set at a p-value of less than .05.
Results
The study included 44 patients. Mean follow-up was 31 months (range 18–48). Mean preoperative pain score (VAS score in activity) was 63 (SD 15), which decreased to 14 (SD 18) (p = .0004). Grip strength also improved significantly, from mean 29 (SD 11) preoperatively, to 36 (SD 10) postoperatively (p = .0004). Median q-DASH score was 41 (IQR 31–43), which improved to 6 (IQR 2–22) (p = .007) (). The range of motion including the rotation of the forearm remained unchanged after the surgical treatment. None of the patients experienced intra- or postoperative complications, fractures of the ulna, infections or neurological disorders concerning the surgical treatment. Twenty-nine patients had preoperative MR scans. Eleven patients, out of 29, had a positive MR scan confirming a foveal injury ().
Table 3. Clinical and functional results for pain, grip strength, patient-reported functional outcome and range of motion, preoperatively and after the last follow-up.
All 44 patients from the study achieved full stability of the DRUJ, after the operative treatment for a foveal TFCC injury. Six patients from this cohort needed re-operation. However, three patients with a renewed TFCC injury needed revision surgery for foveal re-fixation. One patient, a 26-year-old cook discontinued the orthosis early and went to work. A 30-year-old male, detained in the state prison was attacked by other prisoners, thus sustaining instability and pain. Finally, a 46-year-old man was diagnosed with throat cancer, 6 months after the primary TFCC procedure. In the chemo- and radiation-therapy period, he regained instability and pain of the TFCC. All three patients underwent re-fixation with the same surgical technique. They achieved full DRUJ stability and a good clinical and functional result, after the renewed foveal TFCC re-attachment procedure.
Three further patients required renewed surgical treatment. One 44-year-old male was successfully treated with an outside-in suture for the distal, Atzei Class 1 injury. A 22-year-old male was re-operated twice with arthroscopic debridement, caused by a new, central TFCC defect (Palmer 1 A type), solving the ulnar pain, but not solving the clicking problem. A 34-year-old male underwent a synovectomy, without improvement of pain symptoms, despite achieving stability.
Finally, one female, 61-year-old patient with a complex, intra-articular distal radius fracture, awaits ulnar head prosthesis, for the development of DRUJ osteoarthritis.
Altogether, 5 out of 44 patients had fair or poor satisfaction scores, leaving 39 patients (89%) with excellent or good satisfaction scores after the last follow-up.
Discussion
In this study, we reported results of a novel, arthroscopically assisted, modified ulnar tunnel technique for foveal fixation after chronic TFCC injuries. This method of the reattachment of the foveal TFCC uses double-bundle FiberWire suture and knotless fixation, not endangering the sensory nerves or tendons, thus securing safe and stable reconstruction with fewer complications and favourable results.
Comparing different, arthroscopically assisted surgical methods in the treatment of foveal TFCC injuries is a difficult task as comparative studies are sparse and randomised control trials do not exist in the literature. Various reports of different arthroscopic techniques presented generally good clinical and functional results with few complications. Nakamura et al. [Citation14] introduced an arthroscopically assisted technique using two separate 1.2-mm osseous tunnels. In a study of 25 wrists from 24 patients, the authors found seven patients had moderate to severe DRUJ instability and six patients had recurrent or severe pain. In total 67% of patients reported good or excellent satisfaction scores. Shinohara et al. [Citation15], using a similar technique, found two out of eleven patients had mild DRUJ instability at the final follow-up, and three patients had skin irritation at the ulnar neck caused by the suture knot. Altogether, 92% of the satisfaction scores were excellent or good. Iwasaki et al. [Citation16] followed 12 patients after foveal repair using a 2.9 mm, osseous ulnar tunnel and a single 2-0 non-absorbable, Prolene suture. The suture was then tied onto the ulnar periosteum, proximal to the entrance of the osseous tunnel. Although pain decreased significantly, five patients experienced mild pain and one patient experienced moderate pain, postoperatively. Two patients experienced irritation at the ulna. Grip strength and DASH improved significantly. All patients achieved full stability of the DRUJ joint and reported excellent or good satisfaction scores. Atzei et al. [Citation9], reported results after foveal attachments with an anchor placed through the distal foveal portal. Sutures were tied on the radiocarpal and volar surface of the TFCC, using a sliding knot and a knot pusher through the same portal in 75 patients. In total, 48 of these patients (64%) were available for follow-up evaluation. Pain improved significantly but remained moderate in four patients and severe in one. DRUJ instability resolved in 44 out of 48 patients. Wrist ROM and grip strength increased, Modified Mayo Wrist Score and DASH scores improved significantly. Five patients reported transient neuropraxia of the sensory branch of the ulnar nerve. Similar results were reported for the anchor technique in the study by Kim et al. [Citation25], regardless of the presence of positive ulnar variance in most of the cases. A total of 80% of patients reported good or excellent scores for satisfaction.
A recent systematic review [Citation26] of both peripheral and foveal TFCC tears revealed that transosseous suture repairs achieved improved outcomes compared with suture anchors, in terms of DASH and pain scores, whereas PRWE scores and grip strength were higher in the group treated with suture anchors.
The results of our study are consistent with those of Iwasaki et al. [Citation16]. All patients achieved full stability of the DRUJ joint. Although 6 out of 44 patients needed renewed surgery in our cohort, three of the patients needed re-fixation for reasons unrelated to the method. These patients achieved full stability and improved clinical and functional scores after re-fixation with the same surgical technique. Only one of the patients from our cohort experienced irritation at the site of suture fixation, perhaps because our technique avoids using knots. In comparison with a study by Atzei et al. [Citation9], even only being transient, neuropraxia of the sensory branch of the ulnar nerve was present in 5 out of 48 patients in their study. We used a transosseous tunnel for the approach to the TFCC fovea, thus not coming in the vicinity of the sensory branch of the ulnar nerve. In comparing with the technique with two 1.2-mm parallel tunnels through the ulna and a single foveal suture, studies [Citation14,Citation15] reported some instability issues. In our study, placing a double, foveal FibreWire suture inside the ulnar tunnel ensured all patients’ sealed and stable fixation of the foveal TFCC re-attachment. We believe that the 3.2-mm drill hole used in this technique debrided sufficiently the degenerative fibrous tissue around the injury site, stimulating bleeding from the bone marrow, thus enhancing stable healing of the reconstruction.
The surgical treatment of foveal TFCC injuries may be challenging, particularly for the group of patients with high physical demands, either because of their profession or their sports or leisure activities. Dunn et al. [Citation12] reported favourable results with an arthroscopically assisted, knotless anchor technique developed by Geissler [Citation13]. Fifteen patients, all military personnel, were followed for a mean of 3.8 years and 93% were able to remain on active duty, one patient required secondary surgery. Several patients from our study were involved in sports and heavy-working activities that made significant demands on their wrist and DRUJ function. Six patients were involved in vigorous catcher sports activities (e.g. tennis and squash), and one patient was a passionate climber. They all resumed their sporting activities after the surgery. Although, a young female boxer, on the way to a semi-professional career, was unable to continue boxing at the elite level. In our study, all the patients with heavy-working demands returned to their previous jobs.
As Morley et al. [Citation20] stated, a negative MRI examination does not exclude TFCC injury. Nozaki et al. [Citation21] investigated the usefulness of high-resolution 3 T MRI for the evaluation of TFCC injuries using Palmer Classification. They found a statistically significant difference for Type 1 A, Type 1 C and Type 1 D, compared with a group of healthy wrists. This difference was not detected for Type 1B TFCC injuries, where foveal TFCC injuries belong. The study had a limited number of asymptomatic subjects involved as controls, and the results were not compared with arthroscopy findings. Recently, Magnetic Resonance Arthrography has been introduced showing improved results towards plain MRI. This method is time-consuming and therefore more expensive. In our series, 29 patients had preoperative MRI scans of which 18 showed no signs of TFCC injury. Further studies, correlating the high-resolution MRI findings with the findings of surgery are necessary. Until then, wrist and DRUJ arthroscopy remains the golden-standard methods in both diagnosing the type of TFCC injury, and in defining the treatment method.
A strength of our study is that it was designed and performed as a prospective cohort study with preoperative clinical data and systematical follow-up examinations. This study also had some limitations. First, the patients were not randomised at inclusion but were selected using treatment criteria. Although great efforts have been made to avoid it, there may have been selection bias. Nevertheless, we used the hook test as a major instrument for inclusion and it is recently found to have 100% sensibility and 97% specificity in defining foveal TFCC injuries [Citation23]. Second, this patient cohort lacks a control group. For example, a group of individuals who had another surgical or conservative treatment or no treatment at all, for their TFCC injury. Third, not all the patients underwent preoperative MRI investigations of the wrist, perhaps due to organisational problems at our institution during a certain time of the study. While the results are fully valid, the report of the MRI findings could have been more accurate.
In summary, this study reports significant improvements in pain reduction, grip strength and patient-reported function, for the patients with foveal TFCC tears treated arthroscopically with the modified ulnar tunnel technique. The findings present notable good stability, good satisfaction scores and a low complication rate.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Scheer JH, Adolfsson LE. Patterns of triangular fibrocartilage complex (TFCC) injury associated with severely dorsally displaced extra-articular distal radius fractures. Injury. 2012;43(6):926–932.
- Palmer AK. Triangular fibrocartilage complex lesions: a classification. J Hand Surg Am. 1989;14(4):594–606.
- Atzei A, Luchetti R. Foveal TFCC tear classification and treatment. Hand Clin. 2011;27(3):263–272.
- Haugstvedt JR, Berger RA, Nakamura T, et al. Relative contributions of the ulnar attachments of the triangular fibrocartilage complex to the dynamic stability of the distal radioulnar joint. J Hand Surg Am. 2006;31(3):445–451.
- Kleinman WB. Stability of the distal radioulna joint: biomechanics, pathophysiology, physical diagnosis, and restoration of function what we have learned in 25 years. J Hand Surg Am. 2007;32(7):1086–1106.
- Nakamura T, Yabe Y. Histological anatomy of the triangular fibrocartilage complex of the human wrist. Ann Anat. 2000;182(6):567–572.
- Luchetti R, Atzei A, Cozzolino R, et al. Comparison between open and arthroscopic-assisted foveal triangular fibrocartilage complex repair for post-traumatic distal radio-ulnar joint instability. J Hand Surg Br Eur Vol. 2014;39(8):845–855.
- Anderson ML, Larson AN, Moran SL, et al. Clinical comparison of arthroscopic versus open repair of triangular fibrocartilage complex tears. J Hand Surg Am. 2008;33(5):675–682.
- Atzei A, Luchetti R, Braidotti F. Arthroscopic foveal repair of the triangular fibrocartilage complex. J Wrist Surg. 2015;4(1):22–30.
- Auzias P, Camus EJ, Moungondo F, et al. Arthroscopic-assisted 6U approach for foveal reattachment of triangular fibrocartilage complex with an anchor: clinical and radiographic outcomes at 4 years’ mean follow-up. Hand Surg Rehabil. 2020;39(3):193–200.
- Chou KH, Sarris IK, Sotereanos DG. Suture anchor repair of ulnar-sided triangular fibrocartilage complex tears. J Hand Surg Br Eur Vol. 2003;28(6):546–550.
- Dunn J, Polmear M, Daniels C, et al. Arthroscopically assisted transosseous triangular fibrocartilage complex foveal tear repair in the United States military. J Hand Surg Glob Online. 2019;1(2):79–84.
- Geissler WB. Arthroscopic knotless peripheral ulnar-sided TFCC repair. Hand Clin. 2011;27(3):273–279.
- Nakamura T, Sato K, Okazaki M, et al. Repair of foveal detachment of the triangular fibrocartilage complex: open and arthroscopic transosseous techniques. Hand Clin. 2011;27(3):281–290.
- Shinohara T, Tatebe M, Okui N, et al. Arthroscopically assisted repair of triangular fibrocartilage complex foveal tears. J Hand Surg Am. 2013;38(2):271–277.
- Iwasaki N, Nishida K, Motomiya M, et al. Arthroscopic-assisted repair of avulsed triangular fibrocartilage complex to the fovea of the ulnar head: a 2- to 4-year follow-up study. Arthroscopy. 2011;27(10):1371–1378.
- Jegal M, Heo K, Kim JP. Arthroscopic trans-osseous suture of peripheral triangular fibrocartilage complex tear. J Hand Surg Asian Pac Vol. 2016;21(3):300–306.
- Jung HS, Song KS, Yoon BI, et al. Clinical outcomes and factors influencing these outcome measures result in success after arthroscopic transosseous triangular fibrocartilage complex foveal repair. Arthroscopy. 2019;35(8):2322–2330.
- Park JH, Park JW. Arthroscopic transosseous repair for both proximal and distal components of peripheral triangular fibrocartilage complex tear. Indian J Orthop. 2018;52(6):596–601.
- Morley J, Bidwell J, Bransby-Zachary M. A comparison of the findings of wrist arthroscopy and magnetic resonance imaging in the investigation of wrist pain. J Hand Surg Br. 2001;26(6):544–546.
- Nozaki T, Rafijah G, Yang L, et al. High-resolution 3 T MRI of traumatic and degenerative triangular fibrocartilage complex (TFCC) abnormalities using Palmer and Outerbridge classifications. Clin Radiol. 2017;72(10):904.e1–904.e10. e1
- Tay SC, Tomita K, Berger RA. The “ulnar fovea sign” for defining ulnar wrist pain: an analysis of sensitivity and specificity. J Hand Surg Am. 2007;32(4):438–444.
- Atzei A, Luchetti R, Carletti D, et al. The hook test is more accurate than the trampoline test to detect foveal tears of the triangular fibrocartilage complex of the wrist. Arthroscopy. 2021;37(6):1800–1807.
- Iwasaki N, Minami A. Arthroscopically assisted reattachment of avulsed triangular fibrocartilage complex to the fovea of the ulnar head. J Hand Surg Am. 2009;34(7):1323–1326.
- Kim B, Yoon HK, Nho JH, et al. Arthroscopically assisted reconstruction of triangular fibrocartilage complex foveal avulsion in the ulnar variance-positive patient. Arthroscopy. 2013;29(11):1762–1768.
- Liu EH, Suen K, Tham SK, et al. Surgical repair of triangular fibrocartilage complex tears: a systematic review. J Wrist Surg. 2021;10(1):70–83.