
Abstract
Objectives
There are currently no validated hyperacusis questionnaires available in Norway. This study evaluates a new (Norwegian) translation of Khalfa’s Hyperacusis Questionnaire. Another aim was to examine levels of psychological distress in Norwegian hyperacusis patients.
Materials and methods
Seventy-six hyperacusis patients between 21 and 68 years of age completed an online survey on two occasions comprising the Norwegian Hyperacusis Questionnaire (HQ) and Hospital Anxiety and Depression Scale (HADS).
Results
The average scale score for HQ was 25.9 ± 9.0. The HQ scale and subscales had good to excellent internal consistency, except the emotional subscale, which had somewhat lower reliability. The test-retest reliability was moderate to good for the HQ scale and subscales. Fifty-five percent of patients had symptoms of anxiety, while 43% had symptoms of depression.
Conclusion
This preliminary investigation found the Norwegian HQ to be a reliable and valid measure. Patients had more symptoms of anxiety than depression, which is in line with previous findings. Future studies may wish to evaluate the factor structure and measurement invariance of the Norwegian HQ.
Introduction
Clinical hyperacusis is characterised by marked intolerance to ordinary environmental sound while hearing thresholds are quite normal [Citation1]. Hyperacusis affects between 8 and 15% of the population and often co-exists with tinnitus [Citation2,Citation3]. The mechanisms underpinning hyperacusis has been described in different models including the central gain model that suggests hyperacusis is the result of sustained and persistent increase in the central auditory system [Citation4]. Another model suggests that noise-related avoidance and anxiety are modulating factors of the central auditory reaction in hyperacusis [Citation5]. It is unsurprising that persons sensitive or fearful of environmental sounds engage in avoidance behaviours and experience psychiatric comorbidities [Citation6].
While the loudness discomfort level (LDL) is the most commonly used audiometric measure of hyperacusis, the Hyperacusis Questionnaire (HQ) [Citation7] is the most commonly used clinical questionnaire. HQ has been adapted to and validated in several languages [Citation8–14]. Studies generally report acceptable internal consistency (i.e. α ≥ 0.70) although the original study by Khalfa and colleagues [Citation7] report slightly poorer internal reliability. In terms of test-retest reliability, Intra-Class Correlations (ICC) are reported between .73 (Attentional dimension of HQ) and 0.88 (full scale HQ) [Citation8,Citation13]. Bastos and Sanchez [Citation13] report moderate item level test-retest reliability for the majority of items (i.e. Cohen’s Weighted Kappa).
The adaptation and validation of HQ in different languages allows for cross-cultural comparisons of study results. Further, it helps clinicians and other health personnel in different countries by giving them access to sound hyperacusis assessment tools. At present, HQ has not been adapted into Norwegian and therefore not validated using a Norwegian sample. Further, there are no other validated hyperacusis questionnaires available in Norway. This study aims to addresses this important need by validating a Norwegian adaptation of HQ.
Another aim was to evaluate psychological distress in Norwegian patients with self-reported hyperacusis. To this end, patients were administered the Hospital Anxiety and Depression Scale (HADS) [Citation15]. Hyperacusis patients commonly experience psychological distress. For example, a study of 62 Swedish patients with a primary complaint of hyperacusis report based on a short, structured diagnostic interview that as many as 47% of patients had a comorbid anxiety disorder with social phobia being the most common, while 8% suffered from major depression [Citation6]. Others report somewhat higher levels of depression among patients with hyperacusis [Citation16]. When the same Swedish hyperacusis patients completed HQ and HADS there were 31 and 21 patients who meet cut-off (i.e. HADS subscale score ≥8) [Citation15] for anxiety and depression, respectively. Furthermore, there was a significant and positive correlation between the emotional dimension of HQ and the anxiety subscale from HADS [Citation17]. Another study has found significant and positive correlations (i.e. r = 0.31 − 0.48, ps <.01) between both HADS subscales, and the HQ full scale and subscales [Citation8].
The present preliminary study aims to provide the first-ever validated hyperacusis questionnaire in Norway by validating a Norwegian adaptation of Khalfa’s Hyperacusis Questionnaire using a test-retest design. A second aim was to evaluate psychological distress in Norwegian patients with self-reported hyperacusis.
Materials and methods
Participants and procedure
The sample comprised 76 patients (87% females) with self-reported hyperacusis, who were on average 47 years of age. Patients were recruited through two Norwegian audiology-themed closed Facebook-groups with approximately 800 and 6500 members, respectively. Patients completed an online survey comprising background questions (i.e. age, gender, and patient email address), HADS and the Norwegian adaptation of HQ on two occasions. Patients had to answer in the affirmative to the question: Do sounds make you feel unwell or cause you physical pain? in order to participate in the study and as a way of assessing self-reported hyperacusis or other symptoms of decreased sound tolerance. The data were collected during February and March 2019. The Norwegian Centre of Research Data approved the methods of this study.
Measures and statistical analyses
The Hyperacusis Questionnaire (HQ) [Citation7] is comprised of 14 items (HQ-T), which patients rate on a scale from 0 (response corresponding to “No”) to 3 (response corresponding to “Yes, a lot”). Items are divided into three dimensions (i.e. subscales): Attentional dimension (HQ-A; items 1 − 4), Social dimension (HQ-S; items 5 − 10), and Emotional dimension (HQ-E; items 11 − 14). A cut-off score >28 represents strong auditory hypersensitivity, although some suggest this cut-off is too high and propose a lower cut-off [Citation11,Citation14]. HQ was adapted to Norwegian using the Translation, Review, Adjudication, Pretesting and Documentation (TRAPD) approach. TRAPD is a team approach where team members (i.e. translators) work both independently and together to develop an adaptation of a questionnaire into a target language and culture (for a detailed description, see [Citation18]). A schematic overview of the approach is presented in .
Figure 1. Schematic representation of the TRAPD approach from Harkness [Citation18].
![Figure 1. Schematic representation of the TRAPD approach from Harkness [Citation18].](/cms/asset/0f14cecf-720f-43b3-aa27-120e7204a0d3/ihbc_a_1943775_f0001_b.jpg)
The Hospital Anxiety and Depression Scale (HADS) [Citation15] is comprised of 14 items (HADS-T) with seven items tapping anxiety (HADS-A) and depression (HADS-D), respectively. Items are rated on a 4-point scale and scores are summed to create a total scale score and subscale scores, respectively. HADS has previously been adapted and extensively used in Norway. The Norwegian HADS demonstrates good psychometric properties [Citation15].
Data analyses were performed using the R software environment for statistical computing and graphics [Citation19]. Internal consistency was evaluated using Cronbach’s coefficient alpha (α) [Citation20] and ordinal alpha (Oα). Item-level test-retest reliability was evaluated using Cohen’s Weighted Kappa (Kw) and scale-level test-retest reliability was evaluated with Intra-Class Correlations (ICC) using a two-way mixed model with absolute agreement. The following criteria were applied for interpreting Kw: 0.21 < Kw < 0.40 = fair agreement, 0.41 < Kw < 0.60 = moderate agreement, 0.61 < Kw < 0.80 = substantial agreement and 0.81 < Kw < 1.00 = almost perfect agreement [Citation21] and for scale and subscale reliability: 0.51 < ICC <0.75 = acceptable reliability with, 0.76 < ICC <90 = good reliability with and ICC >0.90 = excellent reliability [Citation22].
Results
Descriptive statistics and HQ and HADS correlations
The average HQ-T score was 25.87 ± 9.09 and 30 patients (39.4%) met Khalfa’s cut-off for strong auditory hypersensitivity. They had an average HQ-T score of 35.03 ± 3.69. The average HADS-T score was 14.13 ± 6.87 and 42 (55.3%) and 33 (43.4%) patients met cut-off for anxiety (10.64 ± 2.42) and depression (9.88 ± 1.93), respectively, with HADS subscale scores ≥8. HQ and HADS correlations were all significant (ps<.001). See and .
Figure 2. HQ total scale (HQ-T) score distribution (N = 76).
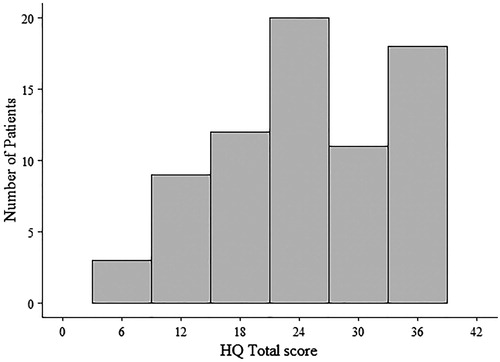
Table 1. Means, standard deviations, and Pearson correlations for Hyperacusis Questionnaire (HQ) and Hospital Anxiety and Depression Scale (HADS) at first testing occasion (N = 76).
Psychometric evaluation of HQ
HQ inter-item correlations (within subscales) ranged from 0.06 (Item 11 with Item 12) to 0.84 (Item 3 with Item 4). Five correlations fell below 0.30. The scale reliability of HQ-T was excellent, while the internal reliability for HQ-A and HQ-S was good. HQ-E had somewhat lower internal reliability. The internal reliability of HQ-S increased to 0.87 if Item 5 was deleted and HQ-E increased (substantially) to 0.81 if Item 11 was deleted. Ordinal alphas were generally a little higher.
The percentage of hyperacusis patients who responded the same on both occasions ranged from 45.9% (Item 11) to 73.8% (Item 5), while the percentage of patients who had ≤1-point difference between occasions was above 86.9% for all items. Cohen’s Weighted Kappa values ranged from 0.39 (Item 11) to 0.68 (Item 10), with all items, except Item 11 and Item 13, achieving a moderate level of agreement between the two testing occasions (i.e. Kw > 0.40). Thus, patients’ responses on HQ was stable across time. HQ scale and subscale test-retest reliability was good for the most part (see rightmost column).
Discussion
The average HQ-T score in the present study was substantially higher than the original study by Khalfa and colleagues (15.00 ± 6.7) [Citation7]. Our result is more in line with Shabana et al. [Citation10], who report an average total score of 20 ± 7.9 and 28.9 ± 5.3 in their two samples of hyperacusis patients without and with comorbid tinnitus. An obvious explanation for these discrepant results is the differing samples; Khalfa used a general population sample where study participation did not necessitate a complaint of hyperacusis, whereas participants in our and Shabana’s studies all had a complaint of hyperacusis. While Shabana et al. report a lower HQ-T score in hyperacusis patients relative to hyperacusis patients with comorbid tinnitus, our HQ-T average score, which is somewhere in between. This may likely reflect that some of our patients had comorbid tinnitus (something we did not ask patients about specifically) and these patients may have scored higher on HQ. It nonetheless suggests that it is important to test for both conditions, not just because they often co-exist [Citation2,Citation3], but because comorbid tinnitus may “inflate” scores on HQ.
In terms of the psychometric properties of the Norwegian HQ, we found similarly to the Japanese, Italian, Portuguese, and Dutch validation studies of HQ [Citation11–14] that internal reliability was near excellent for HQ-T and good for HQ-A and HQ-S, while reliability was somewhat lower for HQ-E. Ordinal alphas were slightly higher. When we inspected inter-item correlations within subscales and the impact of item deletion on the subscale coefficient alpha, we found that Item 11 (“Do noises or particular sounds bother you more in a quiet place than in a slightly noisy room?”) was the most problematic item. It correlated weakly with all other subscale items and if deleted from the HQ-E subscale, internal consistency improved markedly. While the HQ was carefully adapted into Norwegian using a thorough and established translation procedure, we cannot be absolutely certain that the lower scale correlation has to do with the (poor or unclear) Norwegian translation of the item. This uncertainly lies within all cross-cultural questionnaire adaptations, even when rigorous translation procedures are used. However, we think it is more likely that Item 11 is measuring something slightly different to the other items in the subscale. While Item 11 does have an emotional element (i.e. bother you) and ought to fit with the emotional dimension of HQ, the item seems to be more about the place where one is bothered (i.e. a quiet place than in a slightly noisy room) than on the emotional aspect per se. We speculate that this could be a reason for the low correlation with other subscale items and seems also to explain the item’s low factor loading in Khalfa’s original study. The ICCs were good for all HQ subscales, except HQ-E, which had moderate test-retest reliability. These results are similar to Bastos et al. [Citation13] and Müller et al. [Citation8], although we note that the latter study used a sample of tinnitus patients, where only a proportion (17.7%) had a complaint of hyperacusis. Although it was not an aim of the present study, we checked the test-retest reliability of HADS, as no other Norwegian studies have previously reported on this, and found that the total scale as well as the two subscales had good test-retest reliability (i.e. all ICCs >0.80). Together these results suggest stability of HQ and HADS scores across time. This is particularly relevant for clinicians who may follow patients through a treatment phase as HQ and HADS are reliable tools that can be used through patients’ treatment trajectory.
Finally, we found evidence of comorbid anxiety and depression in our sample of Norwegian patients with self-reported hyperacusis. Specifically, we observed significant and positive correlations between HQ and HADS, and 42 and 33 patients met cut-off for anxiety and depression, respectively. These results are in line with previous studies [Citation8,Citation16,Citation17] and indicate that Norwegian patients with self-reported hyperacusis have similar psychological complaints as patients from other countries. Relatedly, we highlight that prior to patient rehabilitation; it is important to establish if the patient has only hyperacusis or tinnitus, or whether the two conditions co-exist as rehabilitation differs because of this. Specifically, the recommendation is to focus on the patient’s hyperacusis first, as this may not only alleviate hyperacusis, but also the annoyance of tinnitus and associated psychiatric and somatic complaints [Citation23]. We recommend the Norwegian HQ for use by researchers, and clinicians in Norway prior to tests of pure-tone audiometry and LDL measures. We encourage researchers to replicate and extend our validation of the Norwegian HQ using a larger sample recruited from a hospital or clinical setting, and focussing on the factor structure of HQ and measurement invariance evaluations.
Methodological considerations/limitations
One may level a criticism at the recruitment approach and the distribution of HQ and HADS online. For example, it may be argued that people who actively engage with online groups (such as the Facebook groups used for recruitment purposes in the present study) are more motivated generally. However, online recruitment has been advantageous in reaching patients with acute tinnitus and long-time sufferers [Citation24] and we believe a parallel may be drawn to the case of hyperacusis, although this has not yet been empirically tested. Further, the online distribution of HQ and HADS has been successfully demonstrated [Citation2]. Another related criticism is that we relied on the patients to self-report a complaint of hyperacusis by use of a questionnaire. However, hyperacusis is a subjective self-reported condition [Citation25] and even using a clinical measure such as LDL to diagnose hyperacusis, patients self-report the discomfort of sounds. Another possibility is to use a structured clinical interview, but unfortunately, we did not have the opportunity to use this in the present study. We nonetheless suggest that future studies may like to use this; alternatively, open-ended questions could be added to gather more information from the patients if recruited online.
Supplemental Material
Download MS Word (14 KB)Acknowledgements
We are grateful to all the patients who participated in this project and we extend our gratitude to the Facebook group administrators who let us advertise the study on their closed Facebook groups. We also wish to thank Eirin Svoldal for assisting with the translation of the Hyperacusis Questionnaire into Norwegian. The authors were all affiliated with the Department of Special Needs Education at University of Oslo at the time of the research. Linda Larsen is now affiliated with the Norwegian Institute of Public Health, Terese Stople Gjendem with the Hearing Centre at Sola, Karina Svevad with Pedogogical-Psychological Service at Indre Østfold, and Guri Engernes Nielsen with the University of Oslo, HEAR Clinic, and Linderud Educational Audiology Centre in Oslo. The authors received no financial support for the project.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Vernon JA. Pathophysiology of tinnitus: a special case–hyperacusis and proposed treatment. Am J Otol. 1987;8(3):201–202.
- Andersson G, Lindvall N, Hursti T, et al. Hypersensitivity to sound (hyperacusis): a prevalence study conducted via the Internet and post. Int J Audiol. 2002;41(8):545–554.
- Baguley DM, Andersson G. Hyperacusis: mechanisms, diagnosis, and therapies. San Diego (CA): Plural Publishing; 2007.
- Auerbach BD, Rodrigues PV, Salvi RJ. Central gain control in tinnitus and hyperacusis. Front Neurol. 2014;5:206. DOI:10.3389/fneur.2014.00206.
- Blaesing L, Kroener-Herwig B. Self-reported and behavioral sound avoidance in tinnitus and hyperacusis subjects, and association with anxiety ratings. Int J Audiol. 2012;51(8):611–617.
- Jüris L, Andersson G, Larsen HC, et al. Psychiatric comorbidity and personality traits in patients with hyperacusis. Int J Audiol. 2013;52(4):230–235.
- Khalfa S, Dubal S, Veuillet E, et al. Psychometric normalization of a Hyperacusis Questionnaire. ORL J Otorhinolaryngol Relat Spec. 2002;64(6):436–442.
- Müller K, Edvall NK, Idrizbegovic E, et al. Validation of online versions of Tinnitus Questionnaires translated into Swedish. Front Aging Neurosci. 2016;8:272. DOI:10.3389/fnagi.2016.00272.
- Wallén MB, Hasson D, Theorell T, et al. The correlation between the hyperacusis questionnaire and uncomfortable loudness levels is dependent on emotional exhaustion. Int J Audiol. 2012;51(10):722–729.
- Shabana MI, Selim MH, El Refaie A, et al. Assessment of hyperacusis in Egyptian patients: evaluation of the Arabic version of the Khalfa Questionnaire. Audiol Med. 2011;9(4):127–134.
- Oishi N, Yamada H, Kanzaki S, et al. Assessment of hyperacusis with a newly produced Japanese version of the Khalfa Hyperacusis Questionnaire. Acta Otolaryngol. 2017;137(9):957–961.
- Fioretti A, Tortorella F, Masedu F, et al. Validity of the Italian version of Khalfa’s Questionnaire on hyperacusis. Acta Otorhinolaryngol Ital. 2015;35(2):110–115.
- Bastos S, Sanchez TG. Validation of the Portuguese version of Hyperacusis Questionnaire and comparison of diagnostic skills with loudness discomfort levels. Otolaryngol Res Rev. 2017;1(1):49–54.
- Meeus OM, Spaepen M, De Ridder D, et al. Correlation between hyperacusis measurements in daily ENT practice. Int J Audiol. 2010;49(1):7–13.
- Bjelland I, Dahl AA, Haug TT, et al. The validity of the Hospital Anxiety and Depression Scale: an updated literature review. J Psychosom Res. 2002;52(2):69–77.
- Paulin J, Andersson L, Nordin S. Characteristics of hyperacusis in the general population. Noise Health. 2016;18(83):178–184.
- Jüris L, Ekselius L, Andersson G, et al. The Hyperacusis Questionnaire, loudness discomfort levels, and the Hospital Anxiety and Depression Scale: a cross-sectional study. Hearing Balance Commun. 2013;11(2):72–79.
- Harkness J. Questionnaire translation. In: Harkness J, van de Vijver FJR, Mohler P, editors. Cross-cultural survey methods. Hoboken (NJ): Wiley. 2003; p. 35–56.
- R Core Team. R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria; 2019. Available from: https://www.R-project.org/.
- Cohen J. Weighted kappa: nominal scale agreement provision for scaled disagreement or partial credit. Psychol Bull. 1968;70(4):213–220.
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163.
- Jastreboff PJ, Jastreboff MM. Tinnitus retraining therapy (TRT) as a method for treatment of tinnitus and hyperacusis patients. J Am Acad Audiol. 2000;11(3):162–177.
- Probst T, Pryss RC, Langguth B, et al. Outpatient tinnitus clinic, self-help web platform, or mobile application to recruit tinnitus study samples? Front Aging Neurosci. 2017;9:113.
- Baguley DM, Hoare DJ. Hyperacusis: major research questions. Hno. 2018;66(5):358–363.