
ABSTRACT
This study reports results of a life course study conducted with Inuit in Nunavik to obtain information on the life adversities and cumulative burden of adversity for three groups: those who died by suicide, those who attempted suicide, and those who experienced suicidal ideation but never attempted. The study involved different levels of collaboration between health authorities, front-line health workers and the research team. Results indicate that substance misuse and relational difficulties are most associated with the burden of adversity for those people who died by suicide, while bullying is most associated with the burden of adversity for those people who have made suicide attempts and those who have never made a suicide attempt. Specifically targeting parent–child relations, substance misuse, and bullying may be an important upstream strategy for reducing future suicidality in Nunavik.
Introduction
Historically, Inuit in Canada had a relatively low suicide rate, however, since the 1980s the rate has risen dramatically [Citation1]. Currently, in the four Inuit territories collectively known as Inuit Nunangat rates range from 5 to 25 times the Canadian average [Citation2]. This drastic increase is almost entirely a consequence of suicides amongst youth under 25 years old [Citation3], particularly young males who die by suicide at 40 times the rate of their peers in the rest of Canada [Citation4].
Over the past several decades, community members, clinicians and researchers have been investigating this rise in suicide deaths. Different research approaches and methodologies have uncovered a spectrum of variables involved in suicide vulnerability. For example, anthropology research has identified cultural and societal change and the breakdown of family relationships [Citation5]; geography research has identified climate change and what is known as “ecological grief” [Citation6]; medical and mental health research has identified a host of social and individual risk factors such as presence of depression, physical and psychological abuse, and impulsivity which may have an impact on suicide [Citation7,Citation8].
Researchers have developed conceptual models to better understand the interaction between exogenous factors that influence the susceptibility to suicide behaviours and contextual factors acting as proximal variables [Citation9]. The challenge resides in the integration of multiple risk factors in the investigation of suicide and suicide behaviours [Citation10,Citation11]. To address these challenges, suicide researchers are increasingly turning to the life course approach. Few studies have used a narrative life-course perspective to sequence the biographical events occurring during development. Our research group has been using a retrospective method in which dimensions of interest are identified and mapped onto a participant’s life trajectory [Citation12].
The current article focuses on results from the life-trajectory interviews, which investigated the occurrence of life events, and the severity and the context of these events. The number of adverse events encountered over the life course may be important; therefore, a summary variable of Burden of Adversity is derived from the extensive narrative material. Conceptually, the Burden of Adversity is deemed to reflect the adversity that a given individual bears, during specific age periods. The life course approach has been successfully used with various populations that are at a higher risk for suicide [Citation13,Citation14], including Indigenous people [Citation15,Citation16].
This article reports the findings of a life course study that was undertaken in the Inuit region of Nunavik. The opportunity to conduct this research arose when, following a string of widely reported suicides, the Nunavik Regional Board of Health and Social Services (NRBHSS) commissioned a study to investigate all suicide deaths that occurred between January 2014 and December 2018 in order to make recommendations for targeted suicide prevention strategies.
The aim of this study was to compare the occurrence of events over the life course and the overall burden of adversity for three groups: those who died as a result of suicide, those who attempted suicide, and those who experienced suicidal ideation but never attempted. A better understanding of these differential profiles can aid clinicians and policy makers in developing more targeted suicide prevention interventions.
Methods and materials
Ethics approval
We submitted to research protocol to the Nunavik Nutrition and Health Committee (NNHC) which serves as the regional ethics committee for research related to health, nutrition and contaminants. The committee felt the project should be reviewed by the researcher’s institutional research ethics board. Ethics approval for this study was received from the Research Ethics Board of the Université du Québec en Outaouais and the Douglas Mental Health University Institute. All participants signed a consent form which was available in Inuktituk and in English.
This study strictly adhered to the principles of collaborative research [Citation17] and the Canadian Institutes of Health Research Guideline for Health Research Involving Aboriginal People [Citation18]. For example, all aspects of the study were designed in collaboration with the local steering committee, which was comprised of community members, members of local town councils, the staff of the NRBHSS, and front-line health workers, who included Suicide-Prevention Liaison Workers (SPLW), and the Community Liaison Wellness Workers (CLWW). Local leaders in each community were also consulted prior to data collection to ensure that locally relevant cultural issues were addressed, and that the research proceeded in a safe and respectful manner.
The discussions with the steering committee raised a number of concerns regarding the recruitment and interview process, which led to some changes in the research methodology. For example, the use of long-structured questionnaires on mental health raised a lot of negative feedback for the committee who felt that it was not congruent with the narrative culture of Inuit. Thus, data collection used a narrative interview on life trajectory using a calendar method, which was used in a prior study in Nunavut [Citation15]. Similarly, the committee felt that bereaved individuals were already vulnerable and could potentially be retraumatized by participating in the research. Thus, research data for those who died by suicide were retrieved solely by the coroner’s files and medical reports. All knowledge produced by this study was co-owned by the research team and the local partnering organisation, and was presented to stakeholders and community members prior to publication.
Study design
The study design is a comparative study between three groups: individuals who died as a result of suicide, individuals who have attempted suicide during their life course, and individuals who have never attempted suicide.
Recruitment
Recruitment procedures were determined in collaboration with a steering committee. In the course of this research, for those who died by suicide in the 14 communities, the research team proceeded to analyse the information based on the content retrieved from the coroner’s reports and the medical reports of the deceased. In each case, authorisation was obtained from the Director of Public Health (DSP) and the Director of Archives to review the medical reports.
As for the other two groups, those who have made a suicide attempt, and those who have never made a suicide attempt, recruitment was conducted in the six Nunavik communities where the suicide rates were highest. Recruitment followed two strategies. First, key resource contacts in the community read recruitment messages over the local FM radio, either alone or accompanied by a member of the research team. Second, snowball sampling was used whereby participants were recruited through word of mouth. Participants received a 25 USD gift certificate for their participation.
We solicited all those interested to participate in the study. According to what was revealed during the interview, participants were assigned to either the group who have made a suicide attempt or the group who have never made a suicide attempt only after the interview process was finished.
Interviews
The interview schedule was developed in collaboration with the steering committee to ensure that it was culturally appropriate and sensitive to local ethical issues. Interviews lasted between 1 and 3.5 hours and took place in an office of the partnering organisation, in a community or municipal office, or in participant’s homes. Interviews were conducted in English or Inuktitut depending on the respondent’s preference. Inuktitut interviews were conducted with a local interpreter.
The data for those who have made a suicide attempt and those who have never attempted suicide was collected through interviews and a review of medical records. Interviews followed the life trajectory calendar, a semi-structured interview technique designed to investigate the occurrence of life events and the cumulative burden of adversity over the life course. This approach serves to simultaneously record sequence and to investigate event characteristics. It has been used in several previous studies [Citation12,Citation14].
The life trajectory calendar is used to map the events that mark an individual’s life in eight spheres of life: 1) place of residence and change of household, 2) parent–child relationship and early adverse events, 3) emotional–romantic relationships, 4) personal family life of adult, 5) episodes of personal difficulty, 6) academic and professional life, 7) losses/separations/departures and other adversity, 8) help seeking/services and drug utilisation.
In the life trajectory calendar, questions concerning events occurring in different spheres of life (family environment, social relations, school and work context, etc.) are used to probe informants for narrative details. With the help of a drawn circle representing the life course, used as a memory anchor, for each period of life (infancy, childhood, young adult, adulthood) the interviewers identify when events occurred, whether they were situational or permanent and determine their duration, intensity, frequency and context. Questions included: What were the events you experienced when you were a small child? and Tell me about the difficulties that you experienced during this period. Common adversities that were not brought up by the participant were then probed. For example, if the respondent did not bring up early issues of domestic violence, the interviewer would ask: Some participants have discussed how there was a lot of physical violence in their household growing up. What was it like in your household? The goal of the interview was to document sufficient details about the individuals’ life events and its trajectory to allow trained evaluators to assess the key characteristics of each event, such as duration, frequency, and severity.
Procedure and analysis
The research interviews were conducted in a conversational mode, with open-ended questions, allowing the participants to discuss events (adversities and protective factors) that occurred during their life. For each file, a clinical vignette was drafted detailing the events the participant reported.
The analysis procedure followed three strategies. First, all these events were placed in a temporal sequence (infancy, childhood, young adult, adult). These events were then compiled into an SPSS data file and analysed to identify those which were most prevalent.
Secondly, to map out the burden of adversity over the life course, all the available data pertaining to the individual’s life course were integrated into the clinical vignettes. The vignettes were reviewed by members of the research team who gave each period of life (0–4 years, 5–9 years, etc.) a score between 1 and 6, which is a summary variable corresponding to the total burden of adversity. The score of 1 to 6 for each period of life (infancy, childhood, youth, young adulthood, adult life), represents the total burden of adversity that the person experienced during each period. The score of 1 indicates a low adversity burden and higher protective factors, while a rating of 6 indicates significant adversity with little protection. Therefore, the higher the burden, the higher the curve. This consensus method has been described elsewhere [Citation12, Citation19].
To map out the curves of the total burden of adversity over time, Growth Modeling (software Mplus Version 7 for Mac) was used to examine the separate group variation in burden of adversity within age periods described earlier and generate a set of continuous growth factors, which are the intercept, slope and quadratic term.
Results
Socio-demographic variables
In total, 133 individual cases were studied. This included 63 cases of those who died by suicide, 23 cases of those who have attempted suicide, and 47 cases of those who have had suicidal ideation but never attempted suicide. 84% of individuals who died by suicide were men, while nearly 70% of those who have attempted suicide and those who have not attempted suicide were women. The age at death, including men and women, averaged around 25 years, approximately 37 years for individuals who have attempted suicide and 42 years for those who have never attempted suicide.
Major social and health adversities over the life course
Results indicated in identifies the presence of adversities across the life course. Among the group of people who died after a suicide, it indicates a decrease in a total number of people, as the age of death created losses of individuals in this group. Results show a number of different adversities between people who died as a result of suicide and those who made a suicide attempt such as: bullying, which was more important in the group of suicide attempt; and the presence of mental health difficulties and relational difficulties with spouse, which was more important in the suicide group.
Table 1. Major social and health adversities over the life course
The comparison of adversities between people who died after a suicide and those who never attempted a suicide generated the most variables starting with discipline/neglect/tension in parent–child relations at a very early age, mental health problems, legal difficulties, relational difficulties, relational difficulties with spouse more often observed for the group of people who died after a suicide. Bullying was a variable reported by people who never attempted suicide.
As for the comparison between those who made a suicide attempt and those who never attempted suicide, results indicate that relational difficulties were more important for the suicide attempt group only for the period between 15 and 19 years old.
Discipline/neglect/tension in parent–child relationship was important among the three groups, increasing from the period between 0 and 4 years to 15–19 years old. Results on sexual and physical violence are mostly reported by people who made a suicide attempt followed by those who never made an attempt especially between the age periods between 5 and 15 years old. The results in regards to sexual and physical violence among the group of people who died as a result of suicide were not reported in the coroner’s file or medical files, and therefore may have been underreported.
Being a victim of bullying was another important adversity. Approximately 40% of those who attempted suicide and 50% of those who have never attempted suicide reported being bullied during school age, and were most often reported by women. Although it is not reported in the medical records or coroner’s reports of those who died by suicide, it is not excluded that bullying could also have been a variable that was present in their lives. Finally, relational difficulties, especially relational difficulties with spouse, were often identified among those who died as a result of suicide.
Mental health difficulties current and lifetime
The most important mental health difficulty is substance misuse (see , ), which affected approximately 70% of cases in all three groups. Results from the coroner’s file regarding toxicological analyses performed at the time of death highlight the association between suicide and substance misuse. Of the 63 individuals who died by suicide, 43 had poly-substance intoxication, 31 had alcohol intoxication, and 21 had drug intoxication.
Table 2. Mental health difficulties among the three groups
Table 3. Trajectory parameters
Summary of variables associated with the burden of adversity
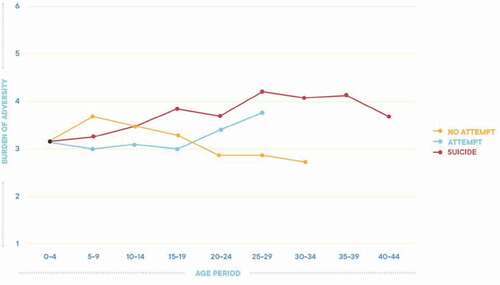
and indicate that no differences were found in the prevalence of adversity during the first 4 years of life for any of the three groups. The trajectory in red, representing the burden of adversity of those who died as a result of suicide, reveals a burden that is present from the beginning of life and that increases throughout the life course compared to the trajectory of the other two groups. The trajectory in green, that of the people who made a suicide attempt, depicts a life course whose adversity is high from the beginning of life and remains stable until the age of 15–19, and then increases in the early twenties, corresponding to the median age at which suicide attempts occur. However, the blue trajectory of people who have not made a suicide attempt remains stable throughout the life course.
Figure 1. Lifetime burden of adversity for each group
Discussion
Over the last 20 years, research from a variety of fields has focused on identifying variables that are most associated with Inuit suicide vulnerability [Citation5,Citation7,Citation8]. By using a life course approach, this study adds to the identification of variables associated with Inuit suicide, but importantly it also quantifies the burden that these variables represent across the life course. In so doing, this study is able to identify a number of significant variables that distinguish between those who died by suicide, those who attempted suicide, and those who had suicidal ideation but never attempted, which, if targeted, may have the greatest impact on reducing future suicide behaviours.
This study points to the importance of more distal and proximal adversities. Distal factors identified by early adversity in regards to neglect/discipline/tension in parent–child relationships were reported by an important number of participants in all groups. Sexual and physical violences were reported by 13% of those who made a suicide attempt and 10% of those who never made an attempt. These results may be underreported by participants as the results found in this study are lower than those reported by Chachamovich and colleagues in the Nunavut study [Citation7]. The possibility of under-reporting is discussed in the limitations. Likewise, the data source used to identify the events and adversities among the group of people that were deceased by suicide, namely, the coroner’s files and medical reports, may also under-report distal factors such as violence and neglect.
Substance misuse is identified as a distal and proximal risk factor and was most commonly reported in the files of those who died by suicide (77.8%) and likewise for those who made a suicide attempt (56% during lifetime) and those who never made a suicide attempt (68% during lifetime). Substance misuse is a well-known risk factor for suicide vulnerability and is present in between 40% and 60% of people who die by suicide [Citation20–22]. Proximally, substance misuse can increase inhibition and impulsiveness, impair judgement, and ease the distress associated with committing the suicidal act [Citation23]. In fact, alcohol intoxication has been found to increase the risk of suicide by 90% compared to abstinence [Citation24]. Distally, substance misuse also contributes to myriad other risk factors for suicide vulnerability. For example, substance misuse leads to higher rates of family dysfunction and domestic violence [Citation25]. When it occurs amongst parents, substance misuse can increase the risk of childhood traumas, including neglect, and serious physical, sexual, and emotional abuse [Citation26]. Substance misuse is also a significant contributing factor for mental health problems, including mood disorders and personality disorders [Citation27]. The results for this study suggest an important link between early substance misuse and ongoing substance misuse, creating relational difficulties with friends and family, relational difficulties with a spouse and in many cases legal difficulties such as arrest, incarceration and imprisonment.
The most important adversity for those who attempted suicide and those who never attempted suicide was being a victim of bullying. Bullying may have been present among those who died after a suicide, but not reported in medical files or coroner’s files. Bullying is implicated in low self-esteem, social isolation and can result in negative feeling states such as sadness, frustration, confusion, guilt, and shame, which are implicated in suicide vulnerability, especially amongst youth [Citation28].
While the identification of alcohol misuse and bullying are not innovative, the sheer numbers of individuals suffering from these problems must be a concern for health authorities.
Other distal factors related to early adversity contribute to the development of other adversities, some of which have been identified in this study. For example, dysfunctional parent–child relationships are implicated in academic difficulties, externalising behaviours [Citation29,Citation30], romantic break-ups [Citation31], and difficulties with social relationships [Citation32,Citation33].
The findings of this study point to several different strategies that policy makers can consider to reduce future suicides in Nunavik. The first is to target the distal variables related to early adversity [Citation34,Citation35], such as child neglect and dysfunctional parent–child relationships. Reducing the burden of childhood adversity would disrupt the trajectory that leads to suicide vulnerability. While feasible, this strategy involves targeting social determinants, such as poverty, equity, and intergenerational trauma, which would require long-term implementation and extensive financial resources [Citation36]. Another strategy, which could be implemented simultaneously in a localised setting, is to specifically target substance misuse and bullying. Such interventions could be incorporated into social and educational/academic services throughout the life cycle in order to change behaviours as earlier as possible.
For example, in 2016, Inuit Tapiriit Kanatami (ITK), the national representational organisation for Canada’s Inuit, launched the National Inuit Suicide Prevention Strategy (NISPS), which seeks to coordinate suicide prevention efforts at the national, regional, and community level, and provide financial support for existing community and regional efforts to prevent suicide [Citation2]. The NISPS lists bullying and substance misuse amongst other important risk factors for Inuit suicide and offers direction for how these risk factors should be addressed. For example, to address childhood adversities, such as bullying, the NISPS recommends supporting “programs and approaches that build resilience and skills for coping in children and youth” [Citation2, p. 28]. Likewise, to address mental health issues, which include substance misuse, it recommends increasing access to “a full range of culturally relevant mental wellness services at the community level” [Citation2, p. 28].
In a recent report, the NISPS Working Group identified 96 promising interventions (e.g. resources, programmes, services) related to suicide prevention in Inuit Nunangat that could be supported by the NISPS [Citation2]. This includes 10 initiatives in Nunavik. Though not targeted specifically, substance misuse and bullying fall under the purview of many of these initiatives. For example, issues of bullying are addressed in the Good Touch Bad Touch programme. Similarly, Brighter Futures focuses in part on mental wellness, which includes issues of substance misuse. Challenges arise because many of the initiatives identified by the NISPS Working Group have not been formally evaluated, making it difficult to glean best practices.
Other initiatives from the around the world have shown to lower rates of bullying and substance misuses in Indigenous communities. While these programs are diverse, they tend to share a common approach, which combines universal strategies directed towards the general population, with individualised strategies targeting high-risk individuals. A good example is the Community Mobile Treatment (CMT) program, a substance misuse initiative from Western Canada. This program starts with an extensive multi-year public outreach campaign to raise awareness about the dangers of substance misuse and the benefits of treatment. This campaign is delivered through the local media, townhall meetings, and public health messaging. This is followed by a month-long clinical intervention, which is delivered to substance misusers by a mobile treatment team consisting of social workers and local health workers. The program ends with 6 months of aftercare provided by community volunteers. Evaluations show that during the CMT intervention as many as 75% of community members received treatment, and a 75% abstinence rate remains 6 months after the intervention finishes [Citation37].
Another example is the Mt Theo anti-petrol sniffing program, which was created by the Australian aboriginal community of Yuendemu. In this program, a community-wide educational campaign is first undertaken to raise awareness about petrol sniffing and the treatments that are available. Next, with the permission of their family, individuals caught sniffing petrol are sent out of the community to an outstation (Mt. Theo) where they receive a month-long clinical intervention, provided by local elders and mental health professionals. Upon returning from Mt. Theo community volunteers provide ongoing aftercare support. Following this model, over the course of a decade, Yuendemu was able to completely eliminate petrol sniffing in the community. The program has now expanded to include other forms of substance misuse and is funded by the Australian government[Citation38].
To our knowledge, there are no anti-bullying interventions designed specifically for work with Indigenous populations. However, KiVa is a school-based program that has been shown to work well with Indigenous students [Citation39]. This program also uses a combination of universal and individualised strategies. It starts with a general educational campaign about the dangers of bullying, how to recognise bullying, and how to stop bullying if it is encountered, which is directed towards all students in the school, their parents, teachers, and school administrators. Next, individualised strategies target specific high-risk groups such as perpetrators and victims of bullying. Targeted strategies include one-on-one counselling and computer-simulated learning opportunities. Evaluations have found that the KiVa program lowers bullying by 60%. It also increases empathy towards victimised peers, self-efficacy amongst bystanders to stop bullying, enjoyment of school for bullied youth, and reduces anxiety, depression, and negative peer perceptions amongst all students [Citation40].
Universal strategies should be directed towards all community members as both substance misuse and bullying may have a direct or indirect effect on all age groups. However, the results of this study suggest that in order to have the greatest impact on future suicide vulnerability, substance misuse interventions should target young adults before they become future parents. Substance misuse in households contributes to suicide vulnerability in children, and youth are most vulnerable to developing patterns of substance misuse. Likewise, education on anti-bullying should start in an early school setting, should be implemented continuously over the school years, and be modulated throughout the developmental process.
Limitations
This study has a number of limitations. First, there was a limited number of participants. Despite tailoring recruitment strategies to the local context, and the researcher’s efforts to make themselves available to answer questions about the research, the study did not attract a high number of respondents. This is likely due to stigma surrounding suicide; the difficulty of talking about suicide; the lack of trust of Southern researchers; and finally, a suspicion that participation in research may not make a difference in policy changes.
Next, the recruitment process was complex and delicate, and the different procedures had to be weighed against culturally accepted practices. For example, the recruitment period corresponded with a spike in suicides across Nunavik, and the steering committee was not comfortable with the recruitment of bereaved family members and close friends to participate in this research, even if researchers had extensive experience in regards to this type of research interview [Citation14,Citation16,Citation21]. Therefore, research data for those who died by suicide were retrieved solely from medical files and coroner’s reports, which may not have documented or detailed important events that may have occurred in the deceased’s life especially in regards to the specific distal sphere like sexual and physical violence.
Similarly, it is possible that some events such as early physical and sexual violence may have been under-reported by some participants. Again, if this did occur, it would likely be a result of the sensitive nature of these topics, sensibility to social judgement and mistrust in regards to the way the results could be presented and interpreted. One of the interviewers was also male, which may have made some participants less likely to share information about past sexual trauma.
The data on mental health were mostly identified through self-report and medical files and was not identified with the use of the Structured Clinical Interview for DSM Disorders (SCID). This is why we do not refer to a mental health diagnosis, but we use the term mental health problems. These results are not as robust as they could have been with the use of the SCID questionnaire. But this study was not planned as a psychological autopsy study and the aim was not to identify the presence of mental health disorders in the months before the suicide occurred. Rather, this study implemented a life trajectory methodology, which sought to identify psychosocial risk factors, periods during which these factors appeared over the life course and period during which the burden of adversity was most important.
Results from this study should be interpreted in light of these limitations. However, it is important that the strengths of this study are considered as well. First and foremost, the collaborative work with local partners and the originality of the method contributed to widely positive appreciation from our partners and from individuals who participants in this research.
Conclusion
Despite these limitations, this study provides a good example of a collaboration between researchers, mental health administrators and community members to investigate a delicate event such as suicide and to work and learn from one another. Suicide is an important health problem, and talking about suicide is difficult, not because community members are denying the problem, but rather because talking about the lives lost, while not having a specific strategy creates deep feelings of despair and powerlessness. It is therefore important that recommendations from this study regarding alcohol misuse and bullying be implemented rapidly and incorporated into social and educational/academic services, and for which the rates of suicide behaviours be monitored in order to verify if these strategies have an impact on reducing suicides and suicide behaviours.
Acknowlegements
We would like to acknowledge a number of people who participated in this effort including Valerie Lock, Geneviève Pellerin, Michael O’Leary, Jessica Tooma, and Mae Ningiuruvik.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Hicks J, Bjerregaard P, Berman M. The transition from the historical Inuit suicide pattern to the present Inuit suicide pattern. In: editors, Beavon D, White J, Wingert S, et al. Aboriginal policy research moving forward, making a difference. Vol. 4. Toronto: Thompson Educational Publishing Canada; 2007:39-46.
- Inuit Tapiriit Kanatami, National Inuit Suicide Prevention Strategy. Retrieved Apr 11, 2020 from: https://www.itk.ca/wp-content/uploads/2016/07/ITK-National-Inuit-Suicide-Prevention-Strategy-2016.pdf
- Chachamovich E, Haggarty J, Cargo M, et al. A psychological autopsy study of suicide among Inuit in Nunavut: methodological and ethical considerations, feasibility and acceptability. Int J Circumpolar Health. 2013;72(1):20078.
- Nunavut Suicides by Region, Sex, Age Group and Ethnicity, 1999 to 2009. Available online: http://www.eia.gov.nu.ca/stats/historical.html (accessed on 2020 Oct 26).
- Kral MJ, Idlout L. It’s all in the family: wellbeing among Inuit in arctic Canada. In: Happiness across cultures. Dordrecht: Springer; 2012. p. 387–10.
- Willox AC, Harper SL, Ford JD, et al. Climate change and mental health: an exploratory case study from Rigolet, Nunatsiavut, Canada, edited by Selin, H & Davey, G. Clim Change. 2013;121(2):255–270.
- Chachamovich E, Kirmayer LJ, Haggarty JM, et al. Suicide among Inuit: results from a large, epidemiologically representative follow-back study in Nunavut. Can J Psychiatry. 2015;60(6):268–275.
- Crawford A. “The trauma experienced by generations past having an effect in their descendants”: narrative and historical trauma among Inuit in Nunavut, Canada. Transcult Psychiatry. 2014;51(3):339–369.
- Gunnell D, Lewis G. Studying suicide from the life course perspective: implications for prevention. Br J Psychiatry. 2005;187(3):206–208.
- Barraclough BM, Bunch J, Nelson B, et al. A hundred cases of suicide: clinical aspects. Br J Psychiatry. 1974;125(587):355–373.
- Kim CD, Lesage A, Seguin M, et al. Patterns of co-morbidity in male suicide completers. Psychol Med. 2003;33(7):1299–1309.
- Séguin M, Beauchamp G, Robert M, et al. Developmental model of suicide trajectories. Br J Psychiatry. 2014;205(2):120–126.
- Andronicos M, Beauchamp G, Robert M, et al. Male gamblers–suicide victims and living controls: comparison of adversity over the life course. Int Gambl Stud. 2016;16(1):140–155.
- Séguin M, Renaud J, Lesage A, et al. Youth and young adult suicide: a study of life trajectory. J Psychiatr Res. 2011;45(7):863–870.
- Affleck W, Chachamovich E, Chawky N, et al. Suicide amongst the Inuit of Nunavut: an exploration of life trajectories. Int J Environ Res Public Health. 2020;17(6):1812.
- Pettingell SL, Bearinger LH, Skay CL, et al. Protecting urban American Indian young people from suicide. Am J Health Behav. 2008;32(5):465–476.
- Macaulay AC, Delormier T, McComber AM, et al. Participatory research with native community of Kahnawake creates innovative code of research ethics. Can J Public Health. 1998;89(2):105–108.
- Canadian Institutes for Health Research. CIHR guidelines for health research involving aboriginal people. Ottawa, ON: Canadian Institutes for Health Research. 2007.
- Séguin M, Lesage A, Chawky N, et al. Suicide cases in new brunswick from april 2002 to may 2003: the importance of better recognizing substance and mood disorder comorbidity. Can J Psychiatry. 2006;51(9):581–586.
- Cheng AT, Chen TH, Chen CC, et al. Psychosocial and psychiatric risk factors for suicide: case-control psychological autopsy study. Br J Psychiatry. 2000;177(4):360–365.
- Norström T, Rossow I. Alcohol consumption as a risk factor for suicidal behavior: a systematic review of associations at the individual and at the population level. Arch Suicide Res. 2016;20(4):489–506.
- Pompili M, Serafini G, Innamorati M, et al. Substance abuse and suicide risk among adolescents. Eur Arch Psychiatry Clin Neurosci. 2012;262(6):469–485.
- Sher L. Alcohol consumption and suicide. QJM. 2006;99(1):57–61.
- Hufford MR. Alcohol and suicidal behavior. Clin Psychol Rev. 2001;21(5):797–811.
- Orford J, Copello A, Velleman R, et al. Family members affected by a close relative’s addiction: the stress-strain-coping-support model. Drugs: Education, Prevention and Policy. 2010;17(sup1):36–43.
- Straussner SL, Fewell CH. A review of recent literature on the impact of parental substance use disorders on children and the provision of effective services. Curr Opin Psychiatry. 2018;31(4):363–367.
- Klomek AB, Marrocco F, Kleinman M, et al. Bullying, depression, and suicidality in adolescents. J Am Acad Child Adolesc Psychiatry. 2007;46(1):40–49.
- Hawker DS, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. J Child Psychol Psychiatry Allied Disciplines. 2000;41(4):441–455.
- Nikulina V, Widom CS, Czaja S. The role of childhood neglect and childhood poverty in predicting mental health, academic achievement and crime in adulthood. Am J Community Psychol. 2011;48(3–4):309–321.
- Kendall-Tackett KA, Eckenrode J. The effects of neglect on academic achievement and disciplinary problems: a developmental perspective. Child Abuse Negl. 1996;20(3):161–169.
- Dubowitz H, Papas MA, Black MM, et al. Child neglect: outcomes in high-risk urban preschoolers. Pediatrics. 2002;109(6):1100–1107.
- Manly JT, Oshri A, Lynch M, et al. Child neglect and the development of externalizing behavior problems: associations with maternal drug dependence and neighborhood crime. Child Maltreat. 2013;18(1):17–29.
- Selby EA, Braithwaite SR, Joiner Jr TE, et al. Features of borderline personality disorder, perceived childhood emotional invalidation, and dysfunction within current romantic relationships. J Family Psychol. 2008;22(6):885.
- Berzenski SR. Distinct emotion regulation skills explain psychopathology and problems in social relationships following childhood emotional abuse and neglect. Dev Psychopathol. 2018;1:14.
- Young JC, Widom CS. Long-term effects of child abuse and neglect on emotion processing in adulthood. Child Abuse Negl. 2014;38(8):1369–1381.
- Krysinska K, Batterham PJ, Tye M, et al. Best strategies for reducing the suicide rate in Australia. Aust N Z J Psychiatry. 2016;50(2):115–118.
- Wiebe J, Huebert KM. Community mobile treatment. What it is and how it works. J Subst Abuse Treat. 1996;13(1):23–31.
- Preuss K, Brown JN. Stopping petrol sniffing in remote aboriginal Australia: key elements of the Mt Theo program. Drug Alcohol Rev. 2006;25(3):189–193.
- Green VA, Woods L, Wegerhoff D, et al. An evaluation of the KiVa anti-bullying program in New Zealand. Int J Bullying Prev. 2020;2(3):225-237.
- Salmivalli C, Poskiparta E. KiVa antibullying program: overview of evaluation studies based on a randomized controlled trial and national rollout in Finland. Int J Conflict Violence (IJCV). 2012;6(2):293–301.