
Abstract
An evaluation of the use of cancer education on the practice of breast self-examination among adult women. The study utilized 90 adult women, their ages ranged from 30 to 50 years of age, with mean age of 38.33. The paticipants were randomly assigned to three groups: experimental group I (EGI), exeprimental group II (EGII) and the control group. The study utilized a 10-item index test of the practice of breast self-examination which was subjected to inter-rater face validity. Paired sample T-test was used to test four hypotheses. The first hypothesis stated that there will be a significant difference between pre-test and post-test exposure to different treatment condition on the practice of breast self-examination was accepted at p < 0.5, the second hypothesis stated that there will be a significant difference between women exposed to written/oral education and pictorial/oral education on the practice of breast self-examination was accepted at p < 0.5, the third hypothesis stated that there will be a significant difference between women exposed to written/oral education and control group on the practice of breast self-examination was accepted at p < 0.5 and the fourth hypothesis stated that there will be a significant difference between women exposed to pictorial/oral education and control group on the practice of breast self-examination was also accepted at p < 0.5. Based on the findings, the researcher recommended that breast cancer sensitization should go along with a pictorial/visual form of educating women on how to practise breast self-examination.
PUBLIC INTEREST STATEMENT
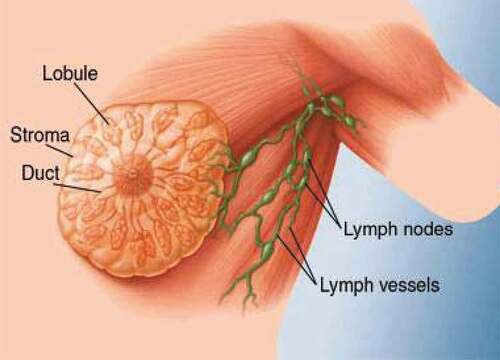
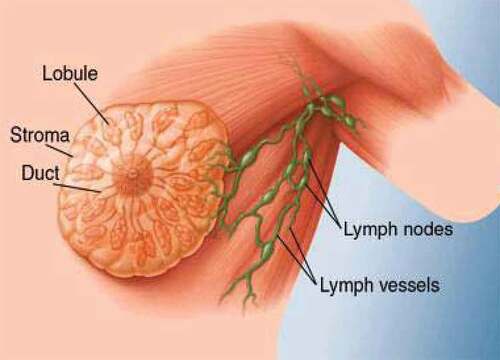
Studies have shown that breast is the most common single site of cancer in women. In Nigeria it is estimated that there being more than one million (1,000,000) women suffering from breast cancer and more than fifty thousand (50,000) deaths per year. Progress has been in recent years in reducing the number of deaths from cancer of the breast, the progress being due mostly to early detection and early treatment. Cancer of the breast tends to spread early to the lymph nodes in the armpit and then to other parts of the body. For this reason the surgeon, in operating for breast cancer, often removes a great deal of tissue in addition to the breast itself—in hope of preventing further spread. Therefore women are counseled to engage in breast self-examination in order to check if there is any lump that may benign or malignant. A surgical operation is usually needed to remove the lump.
1. Introduction
Cancer is a global health problem. It is a leading cause of death and a major burden of disease worldwide (Cancer Fact Sheet, Citation2014a). Each year, tens of millions of people are diagnosed of cancer around the world, and more than half of the patients eventually die from it (Cancer Fact Sheet, Citation2014b). According to Ahmedin et al. (Citation2010), cancer has an estimated worldwide incidence of 10 million new cases per year, 46% of which are in developed countries. According to World Cancer Research Fund international (Citation2013), there are an estimated 14.1 million cancer cases around the world in 2012, of these 7.4 million cases were in women and 6.7 million in men. This number is expected to increase to 24 million by 2035. Cancer has been identified as a leading cause of death in economically developed countries and the second leading cause of death in developing countries. As elderly people are most susceptible to cancer, and the aging population continues to grow in many countries, cancer will remain a major health problem around the globe (Xiaomei & Herbert, Citation2006). The disease burden of cancer is carried more than half by countries and they lack the resources for cancer awareness and prevention; therefore early detection, treatment or palliative options to relieve pain and human suffering is in high demand (Jeffrey, Citation2011).
Breast cancer is a type of cancer originating from breast tissue, most commonly from the inner lining of milk ducts or the lobules that supply the duct with milk, it is the most common malignancy and it is the leading cause of death among women (American Breast Cancer Society, Citation2007).
The primary factors that increase risk of breast cancer in women include lack of practice of breast self-examination, certain inherited genetic mutations, a personal or family history of breast cancer, and biopsy-confirmed hyperplasia. Other factors that increase breast cancer risks include a long menstrual history (menstrual periods that started early and/or ended late in life), obesity after menopause, recent use of oral contraceptives, postmenopausal hormone therapy, never having or had children or having the first child after age 30, ethnicity characteristics, exposure to radiation, or consumption of one or more alcoholic beverages per day. Early detection and prompt treatment offer is the greatest chance of long-term survival (Kanavos, Citation2006).
Table 1. Showing the mean and standard deviation of pretest and posttest exposure on the practice of breast self-examination
Table 2. Showing the mean and standard deviation of within groups and between-group exposure on the practice of breast self-examination
Cancer is more common in women than in men, although men tend to have poorer outcomes due to delays in diagnosis (World Health Organization, Citation2011). The first noticeable symptom of breast cancer is typically a lump that feels different from the rest of the breast tissue and more than 80% of breast cancer cases are discovered when the female feels a lump (Manual of Diagnosis and Therapy 2008).
Breast self-examination (BSE), mammography and clinical breast examination are the secondary preventive methods used for screening in the early detection of breast cancer. Breast self-examination is a step to step approach to examining the breast. Breast self-examination is a self-care practice that is easy, convenient, private, safe, involving no cost and requiring no specific equipment. For breast self-examination, a regular time is best such as 5–7 days during menstruation (counting the first day of the menstruation as day one), when breast tenderness and fullness caused by fluid retention have subsided (Berman, Synder, Kozien and Erb 2008).
Jenkins (2006) revealed from the findings of his study that places where breast self-examination is widely practised, 70–80% of breast cancer are discovered by patients themselves. Breast self-examination provides a woman with a relatively simple, low-cost method of easy detection of breast cancer that can be performed more frequently than Clinical Breast Examination (CBE) and mammograms. Women who are aware of breast self-examination and perform it regularly are said to be mindful of their breast as they become familiar with any abnormalities (Smeltzer et al., Citation2010).
Breast self-examination is one of the most important steps of identifying breast tumours at an early stage especially the cancerous types (Marinho et al., Citation2010). In developing countries like Nigeria, breast self-examination will most likely be the feasible approach to wide population coverage on the identification of breast tumours rather than mammograms and Clinical Breast Examination (CBE) because it is a cheap and easier method (Park, Citation2007).
According to Hatfield as cited in Allen (Citation2001), education is designed to “develop long-term, organized bodies of knowledge and generic problem-solving skills that will help the learner solve personal problems, both in the present and in the future” (p. 347). Psycho-education is the “process of teaching clients about the nature of the illness, including its etiology, progression, consequences, prognosis, treatment and alternatives (Barker, Citation2003, p. 347). Cancer-education’s goal is to offer education and therapeutic strategies to improve the quality of life for the family while decreasing the possibility of relapse for the patient (Solomon, Citation1996). It also has been described as a “systematic didactic-psychotherapeutic intervention, designed to inform clients and their relatives about their problem and to promote coping (Lincoln et al., Citation2007, p. 233). By strengthening the coping skills, communication and problem-solving abilities of the family, the well-being and adaptability of the individual and family members are expected to improve. Even with limited empirical evidence suggesting the importance of psycho-education, practical application and experience has proven its effectiveness (Creamer & Forbes, Citation2004; Landsverk & Kane, Citation1998).
Cancer-education can be in written form or through verbal communications or pictorial communication to aid in the therapeutic approach. Cancer-education is education used in therapy and it includes discussion and application for the edification of the client’s knowledge regarding the diagnosis, treatment options and techniques for coping (Hornung et al., Citation1996). It is effective in removing myths associated with the diagnosis, providing statistical data, and in describing the symptomology of the diagnosis and also can be effective in reframing of breast-examination audio-visual events. Therefore, this cancer-education can be used for women educating them to practice breast self-examination regularly in order to help in early detection of breast lump, because the practice of breast self-examination is better and cheaper than cure for breast cancer.
Studies have shown that there are relationships between breast cancer and cholesterol. In a study by Danilo and Frank (Citation2012), on cholesterol and breast cancer development. They posited that breast cancer is the most commonly occurring type of cancer in the world. Among the environmental factors believe to be responsible for this phenomenon, cholesterol has recently received considerable attention. Epidemiological studies have provided inconclusive results, indicating that there may be a relationship between abnormal plasma cholesterol levels and breast cancer risk. However, more compelling evidence has been obtained in laboratory studies, and they indicate that cholesterol is capable of regulating proliferation, migration, and signalling pathways in breast cancer. In vivo studies have also indicated that plasma cholesterol levels can regulate tumour growth in mouse models. The recognition of cholesterol as a factor contributing to breast cancer development identifies cholesterol and its metabolism as novel targets for cancer therapy. In another study by Garcia-Estevez and Moreno-Bueno (Citation2019), on updating the role of obesity and cholesterol in breast cancer. They observed that overeating and obesity are intimately related with breast cancer development and recurrence. The interplay between obesity, inflamation, and the tumour microevironment drive tumour expansion, primarily in hormone-sensitive and postmenopausal patients. Lately, the role of leptin and leptin receptor in breast cancer cells has shed light on the role of the adipose environment in breast cancer. Several meta-analyses have provided evidence that obesity carries a 35–40% increased risk of recurrence and death, irresspective of menopausal or hormone receptor status. In this regard, breast cancer prevention requires raising awareness among women for watching their body weight, especially those in menopause. This can be achieved through a low cholesterol/low-saturated fat diet and regular anaerobic exercise. The role of total blood cholesterol for breast cancer development is controversial. Most studies show that high cholesterol levels prior to diagnosis protect against the development of tumours, promoting some authors to advocate the use of statins to lower cholesterol. It is uncertain that total cholesterol makes the most appropriate risk biomarker, with 27-OHC as perhaps a more suitable candidate.
Collectively, clinical studies and meta-analyses support a role for obesity, dietary fat intake and/or cholesterol in the onset and progression of the disease, and practising physicians and dieticians should be proactive in recommending habits such as an appropriate diet and regular physical activity to maintain a healthy weight.
The paper therefore, in the course of this experimental study wants to ascertain the effect of cancer-education on the practice of breast self-examination among adult women of prison officer’s wives association (PROWA) in Umuahia command, Abia State Nigeria.
2. Theoretical framework
2.1. Cognitive theory of memory and learning
The cognitive theory of memory and learning was pioneered by Baddeley and Hitch. They proposed a model of working memory in 1974, in an attempt to describe a more accurate model of short-term memory. The original model of Baddeley & Hitch was composed of three main components; the central executive which acts as supervisory system and controls the flow of information from and to its slave systems: the phonological loop and the visuo-spatial sketchpad. The phonological loop stores verbal content, whereas the visuo-spatial sketchpad caters to visuo-spatial data. Both the slave systems only function as short-term storage centres. In 2000 Baddeley added a third slave system to his model, the episodic buffer.
Baddeley & Hitch’s argument for the distinction of two domain-specific slave systems in the older model was derived from experimental findings with dual-task paradigms. Performance of two simultaneous tasks requiring the use of two separate perceptual domains (i.e. a visual and a verbal task) is nearly as efficient as performance of the tasks individually. In contrast, when a person tries to carry out two tasks simultaneously that use the same perceptual domain, performance is less efficient than when performing the tasks individually.
Baddeley and Hitch (Citation1974) also developed an alternative model of short-term memory which they called working memory. Baddeley and Hitch (Citation1974) argue that the picture of short-term memory (STM) provided by the Multi-Store Model is far too simple. According to the Multi-Store Model, STM holds limited amounts of information for short periods of time with relatively little processing. It is a unitary system. This means it is a single system (or store) without any subsystems. Working Memory is not a unitary store. Working memory is short-term memory. Instead of all information going into one single store, there are different systems for different types of information. Working memory consists of a central executive that controls and coordinates the operation of two subsystems: the phonological loop and the visuo-spatial sketch pad. Central executive drives the whole system (e.g., the boss of working memory) and allocates data to the subsystems. It also deals with cognitive tasks such as mental arithmetic and problem solving. Visuo-Spatial Sketchpad stores and processes information in a visual or spatial form. The VSS is used for navigation. The phonological loop is the part working memory that deals with spoken and written materials. It can be used to remember a phone number. It consists of two parts: Phonological Store (inner ear) linked to speech perception and holds information in speech-based form (i.e. spoken words) for 1–2 seconds. Articulatory control process (inner voice) linked to speech production. Used to rehearse and store verbal information from the phonological store.
This theoretical entities interact together to ensure the assimilation of vital information in form of aiding in learning of some tips drawn from cancer education and the practice of the breast self-examination among adult women in Nigeria. This paper is anchored on this theory for an exposition of vital knowledge that will assist a greater population a handy techniques of breast examination for onward detection of lumps that may cancerous in future.
3. Statement of the problem
The increase of breast cancer has caused myriad of havoc on women in our society. This is because women do not practice breast self-examination and they report breast cancer cases at an advanced stage in hospitals. Therefore, it has been a problem that has silently kept people in their shell until the breast cancer condition exacerbates into advanced stage. Being anxious of the outcome of the result after the practice of breast self-examination may discourage the practise of breast self-examination but breast lump is better identify at early stage than at advanced stage.
Furthermore, lack of skills to practice breast self-examination may discourage the practise of breast self-examination thereby encouraging late detection of breast cancer which may eventually lead to death. But the other way round, which is early detection and prompt treatment offer the greatest chance of long-term survival.
Kanavos (Citation2006) noted that breast cancer remains one of the leading causes of morbidity and mortality worldwide, its increase has caused myriad of havoc on women in our society and much of its burden occurs in the developing world. The global cost and socio-economic impact cannot be overemphasized. Available statistics has shown that breast cancer killed 5.6 million women in 2013 worldwide and there is an indication that the figure could be double by 2030 (World Health Organization, Citation2013). It is possible that this high mortality rate may stem from poor awareness or negative awareness or lack of the skills to practice breast self-examination and consequently late identification and intervention in cancer cases in general population.
As observed by Institution of Human Virology, (IHVN) Abuja, Nigeria (Citation2012), Nigeria has a substantial increase in the incidence of breast cancer. This increase therefore necessitated the researcher’s experimental study on the effect of cancer-education on the practice of breast self-examination among adult women of prison officer’s wives’ association (PROWA) in Umuahia command, Abia State, Nigeria. It also wishes to find answer to the following questions:
Would there be any significant difference between pre- and post-exposure to different treatment conditions on the practice of breast self-examination?
Would there be any significant difference between women who are exposed to written/oral education and those who are exposed to pictorial/oral education on the practice of breast self-examination?
Would there be any significant difference between women who are exposed to written/oral education and control group on the practise of breast self-examination?
Would there be any significant difference between women who are exposed to pictorial/oral education and control group on the practise of breast self-examination?
4. Purpose of the study
The main purpose of this experimental study is to examine the effect of cancer-education on the practice of breast self-examination among adult women of prison officer’s wives association (PROWA) in Umuahia command, Abia State, Nigeria.
5. Hypotheses
There will be a significant difference between pre and post-exposure to different treatment conditions on the practice of breast self-examination.
There will be a statistical difference between women exposed to written/oral education and pictorial/oral education on the practice of breast self-examination.
There will be a statistical difference between women exposed to written/oral education and control group on the practise of breast self-examination.
There will be a statistical difference between women exposed to pictorial/oral education and control group on the practise of breast self-examination.
6. Method
6.1. Participants
A total of ninety (90) women, who were prison officer’s wives and are between the ages of 30 and 50 years (Mean = 38, SD = 5.93) participated in the study. Biographic data show that all the participants are married, have at least OND and at least two (2) children. These participants were randomly assigned to the different treatment conditions using simple random sampling and were purposively drawn from the population of one hundred and twenty women (120) women.
7. Instrument
The major instrument of the study is a ten (10) item index test of the practice of breast self-examination. The instrument was designed to obtain information on the variable of the study. The test was made up of two sections: The section A part of the test was used in the experiment to elicited whether the women have knowledge of breast self-examination or have ever practised breast self-examination and the bio-data inclusion criteria such as age, marital status, years of marriage, number of children, academic qualification, do you have the knowledge of BSE and have you ever practised BSE? The section B of the test includes all the cancer-educational materials about the practice of breast self-examination to elicit whether learning has taken place or not.
8. Validity and reliability of instrument
The validity of the instrument was tested using some senior resident doctors and nurses in Nnamdi Azikiwe University Teaching Hospital (NAUTH) Nnewi who are vast in the area of breast self-examination. The test which contained 10 items was given to the resident doctors, clinical psychologist and nurses to judge the appropriateness, and the whole 10 items were found to have 95% inter-rater agreement among the resident doctors and nurses. Consequently, the 10 items were used for the experiment.
9. Procedure
Before conducting the experiment, a formal permission was obtained from the Deputy Controller of Prisons, who was in charge of the Umuahia Prison Command in Abia State Nigeria, and from the chair-woman of the prison officer’s wives association (PROWA). The researchers met her on one of their bi-monthly meetings, during which the researchers/experimenters introduced themselves formally to the association.
At the end of the meeting, they were given a baseline questionnaire to ascertain those who have the knowledge of breast self-examination nor have ever practised breast self-examination. Out of 120 women present in the meeting, only 20 women were familiar with the knowledge of breast self-examination and other 100 women who have no knowledge of breast self-examination were subsequently invited for a workshop after their second bi-monthly meeting but out of the 100 women only 90 women availed themselves. Purposive sampling technique was used to select the participants and the participants were assigned to different groups using simple random sampling technique, after which a pre-test was given to all the participants. Before the experiment took off, the nitty-gritty of the exercise was explained to all the participants.
The experimental group I and group II were exposed to a standard lecture on the practice of breast self-examination (BSE) using written/oral explanations and pictorial/oral explanations respectively while the control group was not exposed to any stimuli. At the end of the exposure, the experimenters re-administered the (posttest) to the three different groups—(experimental group I, experimental group II and control group) to ascertain its after-effects.
10. Design and statistics
This is an experimental study. Between-group randomized pretest-posttest design was adopted by the experimenter. Based on the research design, paired sample T-test was used as the statistical tool to test the hypotheses of the study.
11. Result
Results from the table show that there is a significant difference between pretest and posttest exposure to different treatment conditions on the practice of breast self-examination.
12. Discussion
The study examined the possibility of using copious forms of education or teaching in managing the practise of breast self-examination. The participants were thought about the knowledge and practice of breast self-examination using different medium (written/oral and pictorial/oral) and were assessed after some duration to know the effect of the teaching. With the literature review, the psychological and social factors that are responsible for lack of the practice of breast self-examination were elucidated. From the summary of table, it was discovered that experimental group II participants (those thought using pictorial/oral cues) were more responsive to treatment. This is not to say that experimental group I participants (those thought using written/oral method) are not. It is just that pictorial/oral method of teaching influenced the practice of breast self-examination.
The prediction of the first hypothesis that there will be a significant difference between pre-test and post-test exposure to different treatment conditions on the practice of breast self-examination was found to be significant at p < 0.5. From the tables of result, it can be observed that the treatment had a significant effect on the post-test score. This may suggest that the treatment influenced the post-test score in order words learning has taken place.
The above finding is in line with the postulations of difference authorities for instance, in the theory of learning that states that learning is a relatively permanent change in behaviour that occurs as the result of prior experience or practice. In order words there is a change in behaviour due to new experience and practice. The women gained a new knowledge and therefore the behaviour change was observed.
The prediction of the second hypothesis that there will be a statistical difference between women exposed to written/oral education and pictorial/oral education on the practice of breast self-examination was found to be significant at p < 0.5. From the tables of result, it can be observed that the treatment had a significant effect on all groups except the control group. This may suggest that the treatment is applicable to a broad spectrum of breast self-examination practice.
The above finding is in line with the postulations of different authorities for instance, in the observational theory of learning, pioneered by Albert Bandura in 1965, in the area of learning. He emphasized the role of observation in bringing about learning which involves the use of observational skills in acquiring new behaviours or modifying the existing one. It is also in line with Baddeley theory of working memory (1997) that the visuo-spatial sketch pad (inner eye) deals with visual and spatial information. Visual information refers to what things look like. It is likely that the visuo-spatial sketch pad plays an important role in helping us keep track of where we are in relation to other objects as we move through our environment and the sketch pad also displays and manipulates visual and spatial information held in long-term memory.
The prediction of the third hypothesis that there will be a statistical difference between women exposed to written/oral education and control group on the practise of breast self-examination was found to be significant at p < 0.5. This signifies that the treatment had more effect on the women exposed to written/oral education than the control group. Based on the above assertion it could be deduced that this finding is consistent with Fleming (Citation1995) theory of learning which states that auditory learners’ best learn through listening, lectures, discussion, tapes etc.
The prediction of the fourth hypothesis that there will be a statistical difference between women exposed to pictorial/oral education and control group on the practise of breast self-examination was found to be significant at p < 0.5. The above finding is in line with the postulation of different authorities for instance, in the theory of visual perception by McLeod (Citation2007), which states that perception begins with the stimulus itself and it is carried out in one direction from the retina to the visual cortex with each successive stage in the visual pathway carrying out ever more complex analysis of the input.
Furthermore, the analysis of the experiment has been able to demonstrate that pictorial form of learning breast self-examination enhances the knowledge and practice of breast self-examination. With the administration of the treatment, there was a significant increase among the participants in experimental group II as against experimental group I in their knowledge and practice of breast self-examination. Also this study was able to demonstrate that pictorial form of learning the practice of breast self-examination is useful when applied along with breast cancer awareness and sensitization, this is because it was also observed that participants who were thought using pictorial/oral cues benefitted more from the knowledge and practice of breast self-examination.
13. Implication of the study
This experimental study has shown the effect of cancer education on the practice of breast self-examination among adult women. The study implied that adult women learnt more about the practice of breast self-examination through pictorial/oral method of learning. However, more effort should be made to include pictorial/oral teaching in sensitizing people to practice breast self-examination.
The findings from this study will encourage women to practise breast self-examination, so as to detect breast cancer or abnormalities easily and to initiate prompt treatment because early detection and prompt treatment offer the greatest chance of long-term survival.
This study will motivate health-care practitioners, all the women groups, prison officer’s wives association (PROWA), governmental and non-governmental agencies, etc., in the society to disseminate positive information concerning knowledge of breast self-examination and its practice in a way that will encourage the practice of breast self-examination even to the door post of the adult women especially those in rural areas.
It will help to reduce the high mortality and morbidity rate that occur due to breast cancer, this is because the practice of breast self-examintion is better and cheaper than cure for breast cancer.
14. Recommendations/conclusion
The experiemental study has showed the effect of cancer education on the practice of breast self-examination. Therefore based on the findings, the researcher recommended that breast cancer sensitization should go along with a pictorial/visual form of educating women on how to practise breast self-examination.
The researcher also recommends that Government should play a pivotal role in advocacy especially through the ministry of women affairs for more active participation of the government for enlightenment campaign in prevention of breast cancer through the practice of breast self-examination. Furthermore, the role of traditional and religious rulers cannot be over-emphasized as they are paramount in the drive especially at the grass root for more awareness and enlightenment for breast self-examination against breast cancer. The researchers concluded that pictorial/visual form of cancer education positively affected the practice of breast self-examination among adult women.
Cover image
Source: Author.
Acknowledgements
The researchers of this study wish to acknowledge with appreciation, the efforts of the individuals; like the Comptroller of the Prison service in Umuahia Command Abia State, Nigeria for being magnanimous enough in approving that the study will be conducted among the Prison Officers Wives’ Association (PROWA) under his command. The researchers appreciate the participants, in persons of the wives of the prison personnel for giving their consent to participate in this study. We say a big thanks to all of them. We also appreciate all the researchers who painstakingly took part in this study. They worked tirelessly in great measure in the process of this research in collecting data, and in writing up this beautiful manuscript. We are highly indebted to all people that contributed in one or the other for the successful outcome of this study. Finally, we sincerely hope that this manuscript will be peer-reviewed and published in the journal of Cogent Psychology.
Additional information
Funding
Notes on contributors

Cynthia Nwanneka Udeze
The authors of this paper are Clinical Psychologists and Lecturers in the Department of Psychology, Faculty of Social Sciences, Nnamdi Azikiwe University, Awka Anambra State Nigeria. Our key research activities are in the area of psychotic disorders, health Psychology, psycho-oncology and sexual deviations. The research reported in this paper are topical issues relating to breast cancer. Statistics have shown that breast cancer is among the frontline killer diseases in Africa and Nigeria in particular. About 50,000 women die of breast cancer related diseases annually. Therefore educating women on the regular practice of breast examination becomes essential in the early detection of traceable lumps in the breast which may be benign or malignant. When a lump is benign in a woman’s breast, it means that the lump has not posed any serious danger in woman’s body and it can be easily removed through surgical operation. But when the lump is malignant, it means that cancer cells has invaded most tissues of the breast.
References
- Ahmedin, G., Melissa, M. C., & Desantis, C., (2010). Global patterns of cancer incidence and mortality rates and trends. Retrieved March 12, 2014, from. http://www.cebp.aacrjournals.org/content/19/8/1893.full
- Allen, J. (2001). Traumatic Relationships and Serious Mental Disorders. John Wiley & Sons, Ltd.
- American Breast Cancer Society (2007). Cancer facts and figures 2007. Retrieved September 17, 2014, from. http://www.cancer.org.com
- Authier, J. (1977). The psych-education model: Definition, contemporary roots and contemporary roots and content. Canadian Counsellor, 12, 15–20.
- Baddeley, A. D., & Hitch, G. (1974). Working memory. In G. H. Bower (Ed.), The psychology of learning and motivation: Advances in research and theory (Vol. 8, pp. 47–89). Academic Press.
- Barker, R. L. (2003). The social work dictionary. NASW Press.
- Cancer Fact Sheet. (2014a). (a) Key Facts. Retrieved Feb, 23, 2014, from http:www.who.int/mediacentre/factsheets/fs297/en
- Cancer Fact Sheet. (2014b). (b) Cancer. Retrieved Feb 17, 2014, from http://www.who.int/mediacentre/factsheets/fs297/en
- Colom, F., & Lam, D. (2005). Psycho-education: Improving outcomes in bipolar disorder. European, Psychiatry, 20,359-364.
- Creamer, M., & Forbes, D. (2004). Treatment of posttraumatic stress disorder in military and veteran populations. Psychotherapy: Theory, Research, Practice, Training, 41(4), 388–398.
- Danilo, C., & Frank, P. G. (2012). Cholesterol and breast cancer development. Current Opinion in Pharmacology, 12(6), 677–682. PubMed. 10.1016j. Coph.2012.07.009
- Dollard, I., & Miller, N. (1950). Personality and psychotherapy. NY: McGraw-Hill.
- Doyle, J. (2005). Prevention and Early Intervention. Retrieved March 23, 2008, from http://www.emq.org/press/docs/Prevention%20and%20Early%20Intervention%20Issue%201%20-%20Overview.pdf
- Edwards, J., & McGorry, P. (2002). Implementing Early Intervention in Psychosis: A Guide to Establishing Early Psychosis Services. Martin Dunitz.
- Fatima, D. (2009). Knowledge, Attitude and Practice of Breast Self-Examination among Nurses and Teachers in Aydin Turkey. Journal of Medical Science, 3, 112–545. Retrieved 19 January, 2013. http://www.ehow.com
- Fleming, N. D. (1995). I’m different, not dumb: Modes of presentation (VARK) in the tertiary classroom. Higher education: blending tradition and technology: proceedings of the 1995 Annual Conference of the Higher Education and Research Development Society of Australasia (HERDSA).
- Fung, C., & Fry, A. (1998). The Role of Community Mental Health Nurses in Educating Clients and Families about Schizophrenia. Australian and New Zealand Journal of Mental Health Nursing, 8, 162–175.
- Garcia-Estevez, L., & Moreno-Bueno, G. (2019). Updating the role of Obesity and Cholesterol in breast cancer. Breast Cancer Research, 21(1), 35. Article number. https://doi.org/10.1186/s13058-019-1124-1
- Health and Human Development Programs (HHD). (2008). EDC’s Health and Human Development Programs (HHD) Focuses on Mental Health. Retrieved 04/08, 2008, from http://www.hhd.org/mental-health/
- Hornung, W. P., Kieserg, A., Feldmann, R., & Buchkremer, G. (1996). Psycho-educational Training for Schizophrenic patients: Background. Procedure and Empirical Findings, 29, 257–268.
- Institute of Psychiatry. (2006). Early intervention. Retrieved March 25, 2008, from http://www.mentalhealthcare.org.uk/content/?id=13
- Institution of Human Virology, (IHVN) Abuja, Nigeria. (2012). Cancer–incidence in-Nigeria. A-Report-from-population-Based-cancer-registries. CancerEpidemiology, 36(5), 271–278. www.researchgate.net/publication/225057898-cancer-incidence-in-Nigeria-from-population-based-cancer-registries
- Jeffrey, L. S., (2011). The Global burden of cancer. Retrieved March 20, 2014 from www.hiffingtonpost.com
- Kanavos, P. (2006). Annals of Oncology: The rising burden of cancer in developing world. Retrieved May 5, 2014 from http.//www.annocoxforadjournals.org/content/17/supple8/viii5abtract
- Kirkegaard, S. A. (1944). The Concept of Dread (2 ed.). Princeton University Press.
- Landsverk, S., & Kane, C. (1998). Antonovsky’s Sense of Coherence: Theoretical Basis of Psychoeducation In Schizophrenia. Mental Health Nursing, 19(5), 419–431. https://doi.org/10.1080/016128498248872
- Lincoln, T. M., Wilhelm, K., & Nestoriuc, Y. (2007). Effectiveness of Psychoeducation for Relapse, Symptoms, Knowledge, Adherence and Functioning in Psychotic Disorders: A Meta-Analysis. Schizophrenia Research, 96(1–3), 232–245. https://doi.org/10.1016/j.schres.2007.07.022
- Mahmoodi, M. H. (2002). The Breast Journal Volume 8, Issue 4, pages 222-225, July 2002. Copyright 1999-2015 John Wiley & Sons, Inc. All Right Reserved.
- Marinho, L. A., Costa-gurgel, M. S., Cecalti, J. G., & Osis, M. J. (2010). Knowledge, Attitude and Practice of Breast Self-Examintaion in Health Centres. Revista De Saúde Pública, 37(5), 576–582. Retrieved 15 March, 2013, from http://www.joint.com.org
- McLeod, S. A. (2007).Visualperceptiontheory. www.simplypsychology.org/perception-theories
- Meyerowitz, B. E., & Chaiken, S. (1987, March). The effect of message framing on breast self-examination attitudes, intentions, and behavior.. Journal of Personality and Social Psychology, 52(3), 500–510. https://doi.org/10.1037/0022-3514.52.3.500
- Morse, W. C. (2004). Psycho-educational Perspective Overview. University of Michigan - a transcript of spoken commentary. Retrieved 10 March 2006 from http://www.coe.missouri.edu/~vrcbd/pdf/PSYPERSP.PDF
- Norman, P., & Hoyle, S. (2004). The Theory of Planned Behavior and Breast Self-Examination: Distinguishing Between Perceived Control and Self-Efficacy. Journal of Applied Social Psychology, 34(4), 694–708. https://doi.org/10.1111/j.1559-1816.2004.tb02565.x
- Panksepp, J. (1982). Towards a general psychobiological theory of emotions. Behavioral and Brain Sciences, 5(3), 407–422. https://doi.org/10.1017/S0140525X00012759
- Panksepp, J. (1991). Affective neuroscience: A conceptual framework for the neurobiological study of emotions. In K. T. Strongman (Ed.), International Review Of Studies On Emotion (Vol. 1). Wiley.
- Park, K. (2007). Park’s textbook of prevention and social medicine (19th ed). Banarsidas Bhanot publishers, Jabalpur.
- Paterson, K., Jones, J., Dagg, B., Scanlon, K., & Raphael, B. (2001). Getting in early: A framework for early intervention and prevention in mental health for young people in New South wales. New South Wales Public Health Bulletin, 12(5), 137. https://doi.org/10.1071/NB01042
- Pratt, S. I., Rosenberg, S., & Mueser, K. T. (2005). Evaluation of a PTSD psycho-education program for psychiatric inpatients. Journal of Mental Health, 14(2), 121–127. https://doi.org/10.1080/09638230500066356
- Rogers, C. (1980). Carl Rogers theory in client centered therapy; its current practice and implications. Houghton Mifflin.
- Rosenstock, M., Strecher, V. J., & Beck, M. H. (1994). The health belief model and HIV risk behaviour change in preventing AIDS. In R. J. D. Clement (Ed.), Theories and methods of behavioural interventions (pp. 5–24).
- Rushton, C. H. (2008). A framework for integrating pediatric palliative care: Being with dying. Journal of Pediatric, 20 (5), 311–325. American Association of colleges of Nursing Education: the next Decade. Washington, D.C: Author
- Smeltzer, S., Bare, B., Hinkle, J., & Cheever, K. (2010). Brunner & suddarth’s textbook of medical-surgical nursing (12th ed.). Lippincott Williams & Wilking.
- Solomon, P. (1996). Moving from psycho-education for families of adults with serious mental illness. Psychiatric Services, 47(12), 1364–1370.
- Staats, A. W., & Eifert, G. H. (1990). The paradigmatic behaviourism theory of emotions basis for unification. Clinical Psychology Review, 10(5), 539–566. https://doi.org/10.1016/0272-7358(90)90096-S
- Sullivan, H. S. (1953). The interpersonal theory of psychiatry. Norton.
- Taylor, R. C., Lemon, P., & Lyne, P. (2010). Fundamentals of nursing: The art and science of nuring care (7th ed.). Lippincott, Williams & Wilkins.
- Walsh, A. C. (2007). Watsons’ clinical nursing and related sciences (7th ed.). Elsevier Limited.
- Wood, M. M., Brendtro, L. K., Fecser, F. A., & Nichols, P. (1999). Psychoeducation: An idea whose time has come. The Council for Exceptional Children.
- World Cancer Research Fund international (2013). Stopping cancer before it starts. http://www.wcrf.org/cancer-statistics/world-cancer-statistics.php
- World Health Organization. (2011). Screening for Breast Cancer. http://www.who.int/cancer/detection/breastcancer/en/onSeptember,2013
- World Health Organization. (2013). Nigeria has the highest cancer death rate in Africa WHO. Retrieved May 12, 2014, from. http://www.naji.com/23850.html
- Xiaomei, M., & Herbert, Y. (2006). Global burden of cancer. Yale Journal of Biology and Medicine, 79(3–4), 85–94. http://www.ncbi.nlm,nih.gov/pmc/article/pmc19947991
- Zuckerman, M., & Lubin, B. (1965). Manual for the Multiple Adjective Checklists. Edits.
Appendix I
GROUP I LECTURE/TREATMENT
Aetiology of cancer
Cancer is the abnormal, uncontrollable, continuous growth of cells which will inevitably lead to the formation of a tumour. Breast cancer is a malignant tumour that has developed from cells in the breast.
Cancer is not contagious. It is suggested that every living organism has some inactive cancer-causing genes called proto-oncogenes. Normal body cells grow, divide to make new cells and die in an orderly way. During the early years of a person’s life, normal cells divide faster to allow the person to grow. After the person becomes an adult, most cells divide only to replace worn-out or dying cells or to repair injured parts. However, sometimes this orderly process goes wrong. The genetic materials (deoxyribonucleic acid which is a substance storing genetic information) of a cell can become damaged or changed, producing mutations that affect normal cell growth and division; this is because the damaged DNA is caused by aberrations that happen while the normal cell is reproducing. When this happens, cells do not die when they should and new cells form when the body does not need them. The extra cells may form mass of tissue called tumour. These physical and chemical agents which induce cancer growth are called carcinogens (American Cancer Association, 2014).
Its Progression
Not all tumours are cancerous; tumours can be benign or malignant. Benign tumours refer to tumours that can grow very large and exert pressure on healthy organs and tissues but they cannot grow or invade other tissues. Because they cannot invade, they also cannot spread to other parts of the body. Benign tumours are typically slow-growing. They often have well-defined borders, so surgical removal can be an effective treatment.
In malignant tumours, the cell structure is significantly different from that of normal cells. Malignant tumours tend to grow faster and can be more invasive than benign tumours. Malignant tumours are life-threatening.
The spread of cancer from one part of the body to another is called metastasis. Most cancers are named from the organ or type of cell in which they start. For example, cancer that begins in the breast is called breast cancer; cancer that begins in the colon is called colon cancer and so on. No matter where a cancer may spread, it is always named after the place where it started. For example, breast cancer that spread to the liver is called metastatic breast cancer, not liver cancer. Likewise, prostate cancer that has spread to the bone is called metastatic prostate cancer, not bone cancer. Some cancers do not form tumours for example; leukaemia is a cancer of the bone marrow and blood.
Clinical Signs and Symptoms of Breast Cancer include
A lump in the breast—the most common first sign.
Pain is more often a symptom of a non-cancerous (benign) condition, but should be checked by a doctor.
A lump in the armpit (axilla), sometimes small, hard lumps in the armpit may be a sign that breast cancer has spread to the lymph nodes. Although these lumps are often painless, they may be tender.
Changes in breast shape or size
Skin changes, the skin of the breast may become dimpled or puckered. A thickening and dimpling of the skin is sometimes called orange peel skin. Redness, swelling and increased warmth (signs that look like an infection) may be a sign of inflammatory breast cancer.
Nipple changes, some people’s nipples are always pointed inward (inverted). Normal nipples that suddenly become inverted should be checked by a doctor.
Discharge from nipple can be caused by many conditions, most of which are non-cancerous (benign). Discharge from one nipple may be a sign of breast cancer, especially if it appears without squeezing the nipple (is spontaneous) and is blood-stained.
Crusting, ulcers or scaling on the nipple may be a sign of some rare types of breast cancer, such as Paget disease of the nipple.
Late signs and symptoms occur as the cancer grows larger or spreads to other parts of the body, including other organs such as bone pain, nausea, loss of appetite, weight loss, jaundice, buildup of fluid around the lungs (pleural effusion), shortness of breath, cough, headache, double vision, and muscle weakness.
Its Consequences
There are copious consequences of breast cancer but tiredness (fatigue) is the most common side effect for people having chemotherapy. It may continue for some months after the treatment ends. How quickly one get back to normal will depend on her general health, and the amount of treatment she had previously.
Other side effects of chemotherapy can include
Feeling sick (nausea) and being sick
Hair loss or thinning
A sore mouth
Taste and appetite changes
Diarrhoea
Sore eyes—they may feel as if they have grit in them
Changes to periods (menstrual cycle)
Constipation etc.
Pertinently, all these can be avoided and ameliorated through the practice of breast self-examination which is a self-care practice that is easy, convenient, private, safe, involving no cost and requiring no specific equipment. Monthly breast self-examination can play an important role in the early detection of breast cancer resulting in greater chance of cure for cancer or less complex treatment and increase chances of survival. The importance of breast self-examination is to become aware of your breast and be able to detect any breast abnormality. The practice of breast self-examination is better than the cure for breast cancer and reduces mortality and mobility rate.
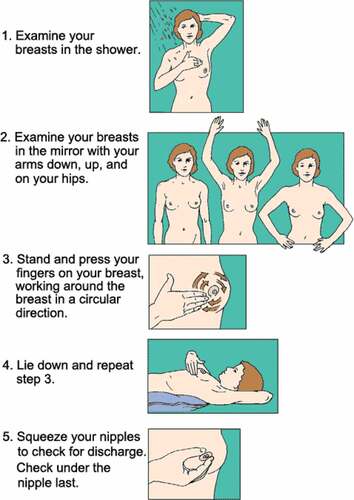
It involves inspection and palpation of the breast which includes five key steps of detecting any breast lumps.
Step 1: Remove your cloth, stand in front of the mirror and keep your arms at your side, then look at your breast carefully. Raise your arms and flex the muscle of your chest and look at your breast contour. Then keep your hands on your hips, bend forwards toward the mirror and examine again.
Step 2: Then look at your breast and check for dimpling of the skin, swelling, changes in the contour and the way the nipple looks. Remember that it is possible for one breast to be larger than the other in size.
Step 3: Then with your first few finger pads of the hand, press on to your breasts. Check the whole breasts as well as the armpits. Use a circular motion, a wedge pattern or an up or down motion while checking for lumps. Check breasts and use the same methods every month.
Step 4: Squeeze your nipple gently and check for discharge. If there is any discharge then report to your doctor about it, in order to find out the cause.
Step 5: Then lie down and examine both breasts. When you are examining the right breast, put a pillow below your right shoulder and place your fingertips, check the right breast and armpit with firm movement. Do the same for the left breast. The examination should always be carried out with the pad of the fingers and not the hand. After examination of both breasts, the client should turn on her side in oblique position and with hand raised over head; this is to allow for a more thorough examination of the outer quadrants of the breast particularly in the larger breast (Walsh, Citation2007). Any discharge from the nipple except in pregnancy and lactation is an abnormality and the best time to do breast self-examination is 5–7 days during menstruation and repeated the same day of every month.
Appendix II
GROUP II LECTURE/TREATMENT
Cancer is the abnormal, uncontrollable, continuous growth of cells which will inevitably lead to the formation of a tumour. Breast cancer is a malignant tumour that has developed from cells in the breast though it can be prevented through the practice of breast self-examination. It is a self-care practice that is easy, convenient, private, safe, involving no cost and requiring no specific equipment. Monthly breast self-examination can play an important role in the early detection of breast cancer resulting in greater chance of cure and less complex treatment.
This can be practised by adopting the following steps.
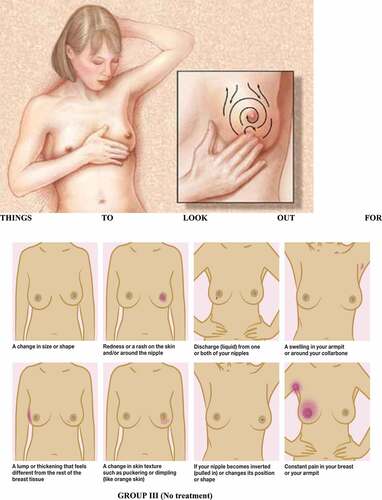
GROUP III (No treatment)
A TEST
This test is to be used to assess the knowledge and practice of breast self-examination (BSE) among adult women.
You are assured of confidentiality in this interaction, as your sincere responses to the questions below will make this study a success. The information given will be used solely for research purposes.
SECTION A: Please tick the appropriate box.
Age of last birthday: 30–34 [], 35–39[], 40–44[], 45–50[].
Marital status—Married [], Divorced [], Widow [].
Duration of Marriage- 6 months [], 1 year [], 2 years and above [].
No of children—None [], 1 child [], 2 and above [].
Academic Qualification-SSCE [], OND/HND [], B.Sc. [].
Have you heard of breast self-examination Yes [], No [].
Have you ever practised breast self-examination Yes [], No [].
SECTION B: RESPONDENT’S KNOWLEDGE AND PRACTISE OF BREAST SELF-EXAMINATION.
Please indicate your agreement with each statement by circling one of the four alternatives besides each statement, thus:
The practice of BSE is a screening method that involves
Inspection of the breast.
Palpation of the breast.
Touching of the breast.
Inspection and palpation of the breast.
The practice of BSE involves
Two key steps of detecting any breast lump.
Three key steps of detecting any breast lump.
Four key steps of detecting any breast lump.
Five key steps of detecting any breast lump.
The practice of BSE involves palpation of breast using
One finger pad of the hand.
Two finger pads of the hand.
Three finger pads of the hand.
First few finger pads of the hand.
The best time to do BSE is
Day 2 to day 7 during menstruation.
Day 3 to day 5 during menstruation.
Day 4 to day 5 during menstruation.
Day 5 to day 7 during menstruation.
BSE should be practised
Every week and repeated the same day of every week.
Every month and repeated the same day of every month.
Every 2 months and repeated the same day of every 2 months.
Every 3 months and repeated the same day of every 3 months.
The best place to usually carry out BSE
Is in front of the mirror.
Lying on a bed in the room.
In the bathroom.
Combination of the above.
The importance of BSE
Is to become aware of your breast.
Is to become aware of your body.
Is to become aware of any abnormality.
Is to become aware of your breast and be able to detect any breast abnormality.
The best means to learn the practice of BSE is
Learning through verbal teaching.
Learning through pictorial cues.
Learning by self.
Learning by practice.
The practice of breast self-examination
Reduces mortality rate.
Reduces breast cancer cases.
Reduces morbidity rate.
Reduces morbidity and mortality rate.
The practice of BSE is better than
Cure for breast pain.
Cure for breast lump.
Cure for breast cancer.