
Abstract
A 63-year-old male presented with a trans-scaphoid lunate dislocation after a ten-foot fall. Internal fixation included placement of a dorsal spanning plate (DSP). One-year follow-up yielded a satisfactory outcome. A rigid DSP is a useful tool in acute perilunate injuries to protect internal fixation constructs and help with injury rehabilitation.
Introduction
Perilunate injuries are uncommon wrist pathologies that usually arise in young adults after high-energy trauma, such as falls from significant heights or motor vehicle collisions [Citation1–8]. Despite their severity, diagnosis of these lesions is missed up to 25% of the time [Citation1,Citation3,Citation6–8]. These injuries warrant acute care as they can lead to posttraumatic osteoarthritis, dysfunction of the median nerve, avascular necrosis, chronic carpal instability, or loss of range of motion [Citation1,Citation7–9]. However, even with optimized treatments, 80% of these patients experience some form of functional deficit or arthritic change [Citation7].
Mayfield staging was initially presented in 1980 and detailed the predictable pathomechanical process of sequential ligamentous rupture and joint disruption that occurs in perilunate injury progression () [Citation1,Citation3,Citation4,Citation10,Citation11]. The most severe stage IV perilunate injuries, or lunate dislocations (LD), commonly occur volarly into the space of Poirier [Citation3,Citation6,Citation8,Citation10].
Table 1. Mayfield classification [Citation1,Citation10].
The most accepted initial management principles for perilunate injuries often involve emergent closed reduction, neurovascular monitoring, and definitive surgery within three to five days [Citation1,Citation3–5,Citation11]. Surgery includes open reduction and internal fixation (ORIF) of any bony injuries followed by soft tissue ligamentous repairs as necessary [Citation1,Citation3–5,Citation11]. Popular methods to achieve a stable fixation involve the use of K-wires, screws, or cerclage wires, followed by cast immobilization [Citation4,Citation5].
We propose that in severe wrist trauma, a dorsal spanning plate may be utilized for ligamentous restraint as well as fracture fixation. While previously described, limited literature exists regarding the applicability of dorsal spanning plate (DSP) fixation in perilunate injuries [Citation5,Citation12]. Of note, due to the ambiguity of LDs being referred to interchangeably as perilunate dislocations (PLD) in the literature, this study utilizes the location of the capitate and lunate bones in comparison to the distal radius for nomenclature [Citation6,Citation13]. Malalignment of the capitate is a PLD; while lunate translation is a LD [Citation6,Citation13].
This report illustrates a unique case of a Mayfield Stage IV perilunate injury, or more specifically, a trans-scaphoid volar LD that underwent fixation which included a DSP construct with satisfactory treatment results.
Case presentation
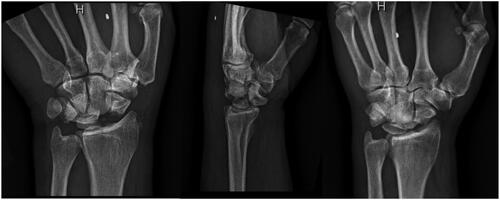
A 63-year-old male with no relevant past medical history presented to the emergency center for left wrist pain after he lost his balance while loading his semi-truck, falling ten feet. On exam he had obvious deformity at the wrist, but intact motor function with thumbs up, OK sign, and 2–3 cross. Pulses were intact, but he reported tingling sensations in the distribution of the radial and median nerves. Radiographic imaging revealed a left trans-scaphoid volar lunate dislocation (). Attempted closed reduction under sedation in the emergency department and a second attempt in the operating room prior to opening were unsuccessful.
Figure 1. Initial presentation of the patient’s left trans-scaphoid lunate dislocation. The classic ‘spilled teacup’ sign can be seen on the lateral view.
ORIF was completed using a dorsal approach. The fourth dorsal compartment was opened and a posterior interosseous nerve neurectomy was performed. The capsule was opened and the joint identified. The lunate was completely volar, as well as a piece of the scaphoid fracture which was lodged in the lunate facet. The scaphoid fragment was dislodged from the lunate facet, and a Freer elevator was used to reduce the lunate. A K-wire was used to provisionally reduce the scaphoid fracture. A Skeletal Dynamics (Miami, FL) cannulated headless compression screw was placed over the K-wire to complete internal fixation of the scaphoid and the K-wire was subsequently removed.
The patient demonstrated an unstable carpus and a scapholunate ligament (SLL) injury causing a dorsal intercalated segment instability (DISI) deformity with the lunate in dorsal tilt. To stabilize the wrist joint, the lunate was pinned to the proximal scaphoid using a 1.55 mm K-wire, then a Skeletal Dynamics (Miami, FL) DSP was placed and secured with three screws both in the third metacarpal and the radius. Carpal positioning in conjunction with the strength provided by the DSP was examined to be adequate for allowing the injured SLL to scar into place. Additional exploration and repair of the SLL was deferred to avoid redundant management. Intraoperative findings also suggested that the DSP was sufficient for stabilization of the lunotriquetral ligament and the interval was not pinned. The final construct consisted of a scaphoid screw, one lunate to scaphoid K-wire, and a DSP ().
Figure 2. Left wrist status post DSP, headless compression screw, and single pin fixation.

At four weeks, the K-wire was removed in clinic. At eight weeks, radiographic imaging demonstrated increased callus formation, bony remodeling, and good alignment of the scaphoid with the implants intact. At three months, the patient underwent DSP removal with extensor tendon tenolysis of the second, third, and fourth digits due to adhesions present on the noted tendons (). Intraoperative passive motion at that time demonstrated 35 degrees of flexion and 40 degrees of extension. One month later at the four-month follow-up visit, the patient demonstrated limited wrist flexion and extension, lacking about 20 degrees in each direction from normal. Grip strength was 100 lbs (45.35 kg) on the right, and 30 lbs (13.61 kg) on the left. At the patient’s request, he was released to full duty work as a truck driver at this time. At nine months, the patient had stopped attending physical therapy appointments and demonstrated a continued lack of 20 degrees in wrist flexion and extension. Continued range of motion exercises were strongly encouraged at this time. At 13 months, the patient had been working full duty, and left upper extremity exam demonstrated 50 degrees of flexion, 40 degrees of extension, 60 lbs (27.22 kg) of grip strength, 23 lbs (10.43 kg) on key pinch (). In comparison, the contralateral extremity demonstrated 50 degrees of flexion, 50 degrees of extension, 80 lbs (36.28 kg) of grip strength, and 22 lbs (9.98 kg) of key pinch strength.
Figure 3. 3-month follow-up after removal of DSP fixation.

Figure 4. 13-month follow-up after removal of DSP fixation.

Discussion
There is no consensus on the management of perilunate injuries. Described interventions encompass utilizing closed reduction and percutaneous pinning, ORIF and ligamentous repair, arthroscopy, external fixation, proximal row carpectomy, or wrist arthrodesis depending on the acuity and severity of the injury [Citation1,Citation2,Citation4,Citation5,Citation7,Citation8,Citation11,Citation14–16]. Yet even with these treatments, perilunate injuries lead to long term sequelae such as pain, stiffness or posttraumatic arthritis in up to 80% of patients [Citation7]. The patient in this report had a trans-scaphoid volar LD that underwent ORIF with DSP placement. We turned towards using a DSP over other popular carpal fixation methods, such as diamond K-wire pinning, as we theorized the additional strength provided by the plate would allow the SLL to scar down [Citation17]. The stronger construct would promote better healing by better positioning the carpus and take stress off the fixation of the scaphoid and lunate.
The use of temporary DSP fixation in carpal injuries is not novel, however limited literature exists regarding its use in perilunate management. In their proof of concept study, Nguyen et al. described DSP fixation for PLDs as ‘not inferior’ to ORIF with cast immobilization [Citation5]. However, the population studied largely consisted of polytrauma patients in which DSP fixation occurred in a delayed fashion at 19 ± 36 days after the inciting event in comparison to ORIF with casting occurring within 3 ± 5 days [Citation5]. Persistent unreduced dislocations generally warrant salvage procedures to achieve satisfactory outcomes, although recent studies have debated this [Citation3,Citation8,Citation16]. DSP use in PLDs in the more acute setting has yet to be reported. Acute management of perilunate injuries is paramount as tissue distortion, scarring, ligament contraction, and vascular supply disruption can affect fixation success and the ability to perform ligamentous repair [Citation1,Citation8,Citation15,Citation16,Citation18]. In our report, the patient presented with an isolated upper extremity injury and underwent definitive fixation within 24 h.
In their case series, Gjeluci et al. presented five patients with trans-scaphoid LDs, one of which was treated with bilateral proximal row carpectomy stabilized with DSPs [Citation15]. Kastanis et al. described a similar case to ours with the presentation of a trans-scaphoid volar lunate dislocation, but with a more extreme migration of the lunate [Citation9]. After undergoing ORIF and application of an external dynamic wrist fixator for neutralization, the patient demonstrated similar functional results as our patient [Citation9]. The outcomes of our case reinforce that when used in a true acute setting, DSP constructs are an additional tool for hand surgeons to utilize for immobilization in perilunate injuries with the benefits of promoting early rehabilitation and weightbearing.
Furthermore, DSP implants promote many more reasons to be considered in surgical interventions. Wahl et al. examined 13 patients managed for radiocarpal dislocations with DSPs and found comparable outcomes to previous reports in the literature [Citation12]. The authors noted that DSP usage provides the advantage of being a reduced infection risk compared to other stabilization methods and avoids larger surgical trauma to the wrist [Citation12]. Through immobilization of the carpus to protect internal fixation, simpler hygiene than with casting, and early weight-bearing during rehabilitation, the benefits of temporary fixation through the use of a DSP cannot be overlooked [Citation5].
Conclusion
A rigid dorsal spanning plate construct can be a useful tool in acute perilunate injuries which allows for protection and immobilization of internal fixation constructs to help with early injury rehabilitation.
Consent
The patient agreed and provided written informed consent to publication of their data. A copy of the written consent is available for review by the editor-in-chief of the journal.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Access to the data supporting the case report is restricted due to the Health Insurance Portability and Accountability Act. Deidentified data can be provided by the authors upon request.
Additional information
Funding
References
- Goodman AD, Harris AP, Gil JA, et al. Evaluation, management, and outcomes of lunate and perilunate dislocations. Orthopedics. 2019;42(1):1–5. doi:10.3928/01477447-20181102-05.
- Liu B, Chen SL, Zhu J, et al. Arthroscopic management of perilunate injuries. Hand Clin. 2017;33(4):709–715. doi:10.1016/j.hcl.2017.06.002.
- Fisher ND, Bi AS, De Tolla JE. Perilunate dislocations: current treatment options. JBJS Rev. 2022;10(9):1–9. doi:10.2106/jbjs.Rvw.22.00106.
- Garner M, Rudran B, Khan A, et al. Lunate dislocations: anatomy, diagnosis and management. Br J Hosp Med. 2021;82(7):1–10. doi:10.12968/hmed.2021.0025.
- Nguyen DM, Boden AL, Allen MK, et al. Dorsal spanning plate for perilunate dislocations. J Wrist Surg. 2022;11(1):16–20. doi:10.1055/s-0041-1729634.
- Ramponi DR, Good AE. Perilunate and lunate dislocations. Adv Emerg Nurs J. 2023;45(2):119–122. doi:10.1097/tme.0000000000000453.
- Garçon C, Degeorge B, Coulet B, et al. Perilunate dislocation and fracture dislocation of the wrist: outcomes and long-term prognostic factors. Orthop Traumatol Surg Res. 2022;108(5):103332. doi:10.1016/j.otsr.2022.103332.
- Alonso-Tejero D, Luengo-Alonso G, Jiménez-Díaz V, et al. Chronic isolated dorsal dislocation of the lunate. A rare presentation of carpal instability. Strategies Trauma Limb Reconstr. 2022;17(1):59–62. doi:10.5005/jp-journals-10080-1543.
- Kastanis G, Velivasakis G, Pantouvaki A, et al. An unusual localization of lunate in a transcaphoid volar lunate dislocation: current concepts. Case Rep Orthop. 2019;2019:7207856. doi:10.1155/2019/7207856.
- Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg Am. 1980;5(3):226–241. doi:10.1016/s0363-5023(80)80007-4.
- Kinghorn A, Finlayson G, Faulkner A, et al. Perilunate injuries: current aspects of management. Injury. 2021;52(10):2760–2767. doi:10.1016/j.injury.2021.09.012.
- Wahl EP, Lauder AS, Pidgeon TS, et al. Dorsal wrist spanning plate fixation for treatment of radiocarpal fracture-dislocations. Hand (N Y). 2021;16(6):834–842. doi:10.1177/1558944719893068.
- De Jonge MC, Assink J, Vanhoenacker FM. Acute bony injuries of hand and wrist. Semin Musculoskelet Radiol. 2021;25(2):277–293. doi:10.1055/s-0041-1729151.
- Kim JP, Lee JS, Park MJ. Arthroscopic treatment of perilunate dislocations and fracture dislocations. J Wrist Surg. 2015;4(2):81–87. doi:10.1055/s-0035-1550160.
- Gjeluci A, Raskind A, Dwan B, et al. Trans-scaphoid lunate dislocation: a case series. Radiol Case Rep. 2022;17(3):514–520. doi:10.1016/j.radcr.2021.11.033.
- Kang SH, Park HW, Im JH, et al. A novel surgical technique for neglected volar dislocation of the lunate: cases report and literature review. Orthop Surg. 2023;15(7):1920–1925. doi:10.1111/os.13760.
- Özyürekoğlu T, Acar MA. Treatment of acute perilunate dislocation or fracture dislocation using dorsal approach and diamond-shaped kirschner-wire fixation. Jt Dis Relat Surg. 2021;32(1):42–50. doi:10.5606/ehc.2021.74838.
- Wu K, Athwal GS, Ross D. Total scapholunate extrusion into the forearm in a transscaphoid, transcapitate perilunate fracture dislocation: a case report. JBJS Case Connect. 2020;10(3):e1900534. doi:10.2106/jbjs.Cc.19.00534.