
Abstract
The origin of the stapes footplate has been controversial for decades, especially regarding involvement of the otic capsule in the development of the footplate. We report two cases of stapes malformation in which the stapes footplate was absent, while the oval window was formed but was covered with mucosal membrane. Both the patients visited our department for long-standing hearing loss, which was due to congenital ossicular anomalies of rare variation, as suggested by intraoperative findings. Through two operated cases, we have also discussed the origin and the mechanisms in the development of the stapes and the oval window. The findings suggest that the formation of the oval window is independent from the development of the stapes footplate. Further reports and accumulation of cases with ossicular malformation are required to develop an appropriate classification of congenital ossicular anomalies based on both developmental mechanisms and analyses of the surgical outcomes.
1. Introduction
Congenital ossicular malformation should be considered as a differential diagnosis while evaluating conductive hearing loss even in adults with a normal tympanic membrane, who have no history of trauma or infection. Hearing outcome is often favorable after surgery for ossicular malformation. However, preoperative diagnosis is challenging due to the diversity and the overlapping nature of the malformations. Development of the ossicles in the middle ear is not fully understood yet and the origin of the stapes is still controversial, especially regarding whether the entire stapes footplate develops from a single source or from distinct sources. We report two cases of stapes malformation where the stapes footplate was absent, while the oval window was formed but was covered with mucosal membrane, providing a clue to understand the origin and the mechanisms in the development of the stapes.
2. Cases reports
Case 1
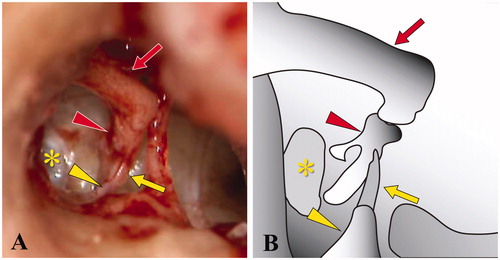
A 28-year-old female patient was referred to our department for long-standing right-sided hearing loss. She had no history of middle ear infection or head injury and did not show any dysmorphic craniofacial features. Pure tone audiometry revealed moderate conductive hearing loss in the right ear with a three-frequency (0.5, 1, and 2 kHz) mean of 42 dB, and a mean air-bone gap of 0.5, 1, and 2 kHz was 26 dB. Impedance audiometry revealed normal tympanic membrane compliance. However, stapedial reflexes were absent on the right side. High-resolution computed tomography (HRCT) of the temporal bones demonstrated that the stapes superstructure of the right side was located inferiorly and was attached to the promontory when compared with the contralateral ear (Figure ). An ossicular anomaly was suspected and exploratory tympanotomy was performed. The stapes superstructure was well formed with two limbs and a head. It was located inferiorly and was attached to the promontory (Figure ). The stapes footplate was not found and the oval window was covered with mucosal membrane (* in Figure ). Ossification of the stapedius tendon was not observed and incudostapedial joint was unremarkable. The malleus and the incus were normally formed in their anatomical positions. The stapes superstructure was removed from the promontory and a small fenestra was made in the oval window. A teflon-wire piston prosthesis (4.25 mm in length and 0.6 mm in diameter) was carefully placed and the fenestra was sealed with connective tissue. Postoperative audiogram revealed auditory restoration with reduction in the air-bone gap from 26 dB to 5 dB.
Figure 1. Preoperative high-resolution computed tomography (CT) of the temporal bones in case 1. (A) Axial CT view shows dislocation of the stapes superstructure from the footplate onto the promontory in the right ear. (B) Coronal view shows the inferiorly displaced stapes in the right. Arrows indicate the stapes superstructure. (C) Axial CT view for the normal left ear. Arrowhead indicates the stapes superstructure.
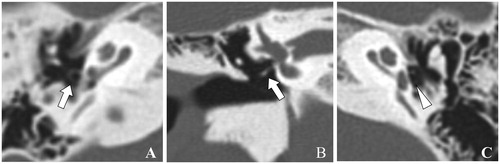
Figure 2. Intraoperative image of the middle ear in case 1. (A) The post-tympanotomy image shows the stapes superstructure attached to the promontory without formation of the stapes footplate. (B) Schema of findings in the ossicular chain and related structures. Red arrow: long process of incus, red arrowhead: stapes superstructure, yellow asterisk: oval window, yellow arrow: tendon of stapedius, and yellow arrowhead: pyramidal eminence
Case 2
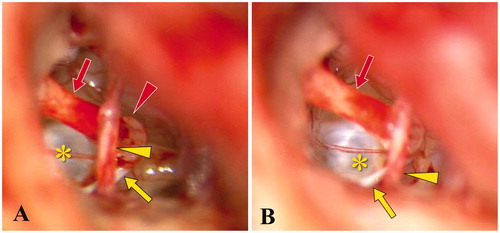
A 24-year-old male patient visited our department for long-standing right-sided hearing loss. He had no history of middle ear infection, head injury, or family history of hearing loss. Pure tone audiometry revealed severe conductive hearing loss with a three-frequency (0.5, 1, and 2 kHz) mean of 72 dB, and a mean air-bone gap of 0.5, 1, and 2 kHz was 57 dB. Tympanometry revealed normal tympanic membrane compliance. Stapedial reflexes were absent on the right side. HRCT of the temporal bones demonstrated that the stapes superstructure of the right side was located inferiorly (arrows in Figure ). HRCT also showed that the stapes footplate was not identifiable (Figure ) and the right oval window showed prominent outward convexity when compared with the contralateral ear (arrowhead in Figure ), suggesting a clue for predicting the absence of the stapes footplate. These findings indicated the existence of ossicular malformation and the patient underwent exploratory tympanotomy. The stapes superstructure was well formed with two limbs and a head. It was located inferiorly and was attached to the promontory (Figure ). The stapes footplate was not formed and the oval window was covered with mucosal membrane (* in Figure Citation4). The round window reflex was observed by pressing the mucosal membrane lying over the oval window. Ossification of the stapedius tendon was not observed. The incudostapedial joint was replaced by mucosal folds between the lenticular process of the incus and the head of stapes (red arrow and red arrowhead, respectively in Figure ). The malleus and the incus were intact and mobile. However, intraoperative inspection gave a bulging appearance of the mucosal membrane lying over the round window, suggesting high pressure of the perilymph which might lead to a gusher when opening the oval window. Therefore, temporalis fascia was placed on the oval window to prevent perilymphatic fistula, followed by the placement of a total ossicular replacement prosthesis of hydroxyapatite onto the temporalis fascia on the oval window. Furthermore, a piece of cartilage was placed onto the prosthesis and fixed to it. The cartilage was designed so that the edge could be placed on the posterior wall of the external canal to stabilize the prosthesis and prevent it from penetrating the membrane or falling into the vestibule. Unfortunately, the patient did not visit for postoperative examination and consequently, hearing could not be evaluated postoperatively.
Figure 3. Preoperative high-resolution computed tomography of the temporal bones in case 2. (A, B) Axial view. Arrows indicate the inferiorly displaced stapes superstructure and arrowhead indicates the oval window portion of the utricle. (C) Coronal view shows the misattachment of the stapes superstructure on the promontory. Arrow indicates the stapes superstructure.

Figure 4. Schema and intraoperative microscopic view of the middle ear in case 2. (A, B) The post-tympanotomy images show the inferiorly located stapes superstructure attached to the promontory. Red arrow: long process of incus, red arrowhead: head of stapes, yellow asterisk: oval window, yellow arrow: tendon of stapedius, and yellow arrowhead: chorda tympani nerve
3. Discussion
Various classification systems have been proposed for congenital middle ear malformation and Cremers’ classification is the most widely accepted classification [Citation1]. Teunissen and Cremers [Citation1] classified congenital anomalies of the middle ear into four main categories based on the different surgical reconstructive techniques according to the surgical findings in 144 operated ears. Particularly, class 2 anomalies include stapes ankylosis with another concomitant ossicular chain anomaly and class 4 anomalies include aplasia or severe dysplasia of the oval window. Park [Citation2] classified congenital anomalies of the middle ear into five types, modifying the previously published Cremers’ classification. He subdivided the main categories into different morphological subcategories. However, both the cases in the present study demonstrated aplasia of the stapes footplate and normal development of the oval window with the stapes superstructure attached to the promontory. These two cases could not be clearly classified into any category according to Cremers’ classification or Park’s classification. The type of middle ear malformation observed in the present cases has not been described in the literature related to case series with relatively large number of middle ear malformations [Citation2,Citation3]. Since stapes malformation is the most common isolated middle ear malformation, we believe that the type of middle ear anomaly observed in the present study is extremely rare. Further accumulation of cases from multi-center studies is required to develop an appropriate classification of congenital middle ear anomalies based on developmental mechanisms and analyses of the surgical outcomes.
The origin of the stapes footplate has been controversial for decades, especially regarding the involvement of the otic capsule in the development of the footplate. In humans, some histological studies on embryos have indicated that the head of malleus and the body of incus are originated from the first branchial arch, while the handle of malleus, the long process of incus, and most of the stapes are originated from the second arch (the dual-arch interpretation) [Citation4]. In contrast, the classical interpretation has been revived, indicating that the incus and the malleus are derived from the first arch and the stapes is derived from the second arch [Citation5]. Most of the previous works presume that the footplate has two origins: the tympanic side derived from the stapedial ring of the second branchial arch and the vestibular side derived from the lamina stapedialis of the otic capsule [Citation6]. According to the theory, the medial border of the stapedial ring comes in contact with a depression in the lateral wall of the otic capsule, which is referred to as the lamina stapedialis and gives rise to the future oval window. The medial border of the stapedial ring fuses with the lamina stapedialis to form the stapes footplate. However, later studies reported that there was no evidence of stapes development from two separate anlages and concluded that formation of the stapes is completely independent of the otic capsule [Citation7]. It was also reported that the stapedial anlage is a unique formation with two distinct superior and inferior parts in the cranial end of the second branchial arch, which give rise to the base and the superstructure of the stapes, respectively.
Yang [Citation8] reviewed 41 articles with 662 cases published between 2000 and 2017 and reported that only 17 out of 189 cases with atresia of the oval window or a fixed stapes footplate demonstrated normal stapes superstructure. In a study of 97 ears with a missing oval window, no cases showed normal stapes, suggesting that the defects in the stapes were closely correlated with the absence of the oval window [Citation9]. These findings indicate that the development of the stapes superstructure is correlated with the formation of the stapes footplate and the oval window. The two cases in the present series support the theory that the development of the stapes footplate takes place independently from the development of the otic capsule. On the other hand, Henriques [Citation10] reported a case of ossicular malformation with isolated misplacement of the stapes superstructure attached to the promontory with an osseous footplate in the oval window and an absence of the stapedial tendon. Whittemore [Citation11] also reported a case of a 12-year-old boy with the stapes crura attached to the promontory and the stapes head connected to the stapedial tendon, while the stapes footplate was located in the oval window and was mobile. Kanona [Citation12] reported an unusual case of progressive conductive hearing loss with a lack of connection between the stapes superstructure and the footplate, which was fixed with an absent stapedius tendon. The location of the stapes superstructure is missing in the report. These reports suggest that the footplate and the stapes superstructure have dual origins. However, these cases do not completely confirm the theory that the footplate, at least in part, originates from the otic capsule. To date, it is not clear whether the otic capsule is the source of a part of the stapes footplate or whether it has also been interpreted as the source of signals that induce the formation of the part of the footplate without contribution from the mesoderm itself.
For the purpose of elucidation of stapes footplate development, Thompson et al. [Citation13] produced transgenic reporter mice to distinguish cells of neural crest origin from those of mesodermal origin. Consequently, they confirmed that the stapes footplate is of dual origin and that the stapes superstructure or the parts of mesodermal origin are needed for the development of the stapes footplate. They also argued that the stapedial ring was necessary for the correct development of the oval window after initiation but not needed for the initiation itself. These observations are supported by the reports that the oval window is present as a small opening in the otic capsule in mice even when the stapes is absent [Citation14,Citation15]. In the present cases, the stapes superstructure was attached to the promontory and the stapes footplate was absent, while the oval window was formed and covered with mucosal membrane. These findings indicate that the development of the stapes footplate is tightly associated with that of the otic capsule and the stapes superstructure. However, the positioning of the oval window is independent of the formation of the stapes footplate.
4. Conclusion
We have discussed two cases having a stapes anomaly with absence of the stapes footplate and a patent oval window covered with mucosal membrane. The crura were attached to the promontory and the stapedius tendon was present, connecting the stapes superstructure and the pyramidal eminence in both the cases. These findings suggest that the formation of the oval window is independent from the development of the stapes footplate.
Informed consent
The patients have provided written informed consent forms to publication of clinical information about them, and the identities of the patients have been protected. This study was conducted in accordance with the ethical standards in the Declaration of Helsinki of 1975 and its amendments or comparable ethical standards.
Acknowledgements
The authors thank Dr. Sho Koyasu, Department of Radiology, Kyoto University Hospital, for a critical discussion.
Disclosure statement
The authors report no conflict of interest.
References
- Teunissen EB, Cremers WR. Classification of congenital middle ear anomalies. Report on 144 ears. Ann Otol Rhinol Laryngol. 1993;102:606–612.
- Park K, Choung YH. Isolated congenital ossicular anomalies. Acta Otolaryngol. 2009;129:419–422.
- Nandapalan V, Tos M. Isolated congenital stapes ankylosis: an embryologic survey and literature review. Am J Otol. 2000;21:71–80.
- Anson BJ, Hanson JS, Richany SF. Early embryology of the auditory ossicles and associated structures in relation to certain anomalies observed clinically. Ann Otol Rhinol Laryngol. 1960;69:427–447.
- Burford CM, Mason MJ. Early development of the malleus and incus in humans. J Anat. 2016;229:857–870.
- Louryan S, Vanmuylder N, Résimont S. Ectopic stapes: a case report with embryologic correlations. Surg Radiol Anat. 2003;25:342–344.
- Rodríguez-Vázquez JF. Development of the stapes and associated structures in human embryos. J Anat. 2005;207:165–173.
- Yang F, Liu Y. Reporting and description for congenital middle ear malformations to facilitate surgical management. Ann Otol Rhinol Laryngol. 2018;127:717–725.
- Su Y, Yuan H, Song YS, et al. Congenital middle ear abnormalities with absence of the oval window: diagnosis, surgery, and audiometric outcomes. Otol Neurotol. 2014;35:1191–1195.
- Henriques V, Teles R, Sousa A, et al. Abnormal congenital location of stapes’ superstructure: clinical and embryological implications. Case Rep Otolaryngol. 2016;2016:2598962.
- Whittemore Jr KR, Dargie JM, Dornan BK. Crural attachment to promontory case report: implications for stapes development. Am J Otolaryngol. 2013;34:366–368.
- Kanona H, Virk JS, Kumar G, et al. A rare stapes abnormality. Case Rep Otolaryngol. 2015;2015:387642.
- Thompson H, Ohazama A, Sharpe PT, Tucker AS. The origin of the stapes and relationship to the otic capsule and oval window. Dev Dyn. 2012;241:1396–1404.
- Kanzler B, Foreman RK, Labosky PA, et al. BMP signaling is essential for development of skeletogenic and neurogenic cranial neural crest. Development. 2000;127:1095–1104.
- Mallo M. Retinoic acid disturbs mouse middle ear development in a stage-dependent fashion. Dev Biol. 1997;184:175–186.