
Abstract
Angiosarcoma of the thyroid gland is a very rare and aggressive mesenchymal tumor with destructive behavior, characterized by high mortality rates. We presented the cyto-histopathological findings of an angiosarcoma case of primarily thyroid origin. A 39-year-old female patient was presented with thyroid tumor appeared as hemorrhagic, non-encapsulated, with focal cystic nodules. Histological appearance of the tumor included vascular-like spaces lined with large epithelioid cells staining positively with factor VIII, CD31. These vascular-like spaces contained erythrocytes. Retrospective cytology showed that malignant endothelial cells were arranged in loosely cohesive clusters. These cells had abundant cytoplasm, distinct nucleoli, irregular contoured and hyperchromatic oval nuclei. This is one of rare cases of primary thyroid angiosarcoma with sufficient cytological material, showing macroscopic and histopathological findings with liquid-based cytology. For the diagnosis of thyroid primary angiosarcoma in aspiration, cytological findings should be evaluated with immunohistochemical methods or, if possible, together with histopathological findings.
Background
Thyroid angiosarcomas, which constitute less than 1% of all sarcomas, are rare malignant mesenchymal tumors with aggressive and destructive characteristics [Citation1–4]. Patients have commonly presented with various symptoms including a lesion on the neck, dyspnea, hoarseness, and dysphagia due to the rapid growth of the tumor. In many cases, systemic metastasis has been indicated at the time of diagnosis, commonly with a tendency of metastasizing to local regional lymph nodes and the lungs [Citation2–6]. The angiosarcoma in the thyroid originates from the vascularity of the gland; histopathologically recognized by atypical endothelial cells. Thus, it resembles to anaplastic cancer in addition to pseudoangiosarcomatous appearance, so it is difficult to classify the tumor, resulting in misdiagnosis [Citation1–4].
Anaplastic thyroid carcinoma-like appearance may be encountered in cytological smears, and it may be difficult to obtain cells from fine needle aspiration for diagnosis. In Turkey, only two case reports with thyroid angiosarcoma in which cytological material can be obtained were presented and these cases are rarely encountered in the literature [Citation4–7].
In this study, the radiological, cytological and morphological findings of the case, which was diagnosed as ‘poorly differentiated malignant tumor metastasis’ by fine needle aspiration cytology prepared with the ThinPrep method, and ‘primary thyroid angiosarcoma’ in the histopathological examination after total thyroidectomy, were presented together.
Case report
A 39-year-old female patient applied to our clinic for a mass on her neck that existed for a long time but showed progressive enlargement for a few months with labored breathing. During physical examination, a nodule in approximately 2 cm diameter and several lymph nodes were detected on the area of thyroid tissue on the neck. Ultrasonography performed for the neck showed a nodule, the largest in 2 cm diameter and several cervical lymph nodes; the thyroid was observed to push the trachea to the right side; thus, computer tomography (CT) was requested. In CT of neck, the thyroid gland was detected as enlarged (Figure ); some nodules, the largest in 2.5 cm diameter including calcifications were remarkable on the right lobe (Figure ). Many lymph nodes were detected as the largest in approximately 14 × 10 mm dimensions on inferior of the thyroid and a pressure was also monitored right to the trachea on the submandibular region.
Figure 1. Non-contrast computed tomography demonstrates irregular growth in the thyroid lobes (curved arrow) and a nodule containing calcification foci in the right thyroid lobe (straight arrow); (a) axial, (b) sagittal, and (c) coronal planes of CT.

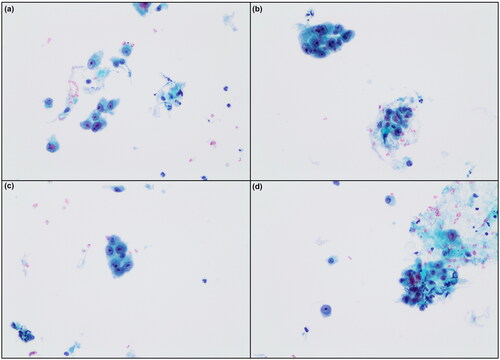
FNAC had been performed to the case on another clinic and the smears had been evaluated in another pathology laboratory. Smears from the liquid-based cytology were reported as ‘metastatic poorly differentiated malignant neoplasm. FNAC smears of the case prepared by ThinPrep method, requested from the other institute (Figure ), indicated the malignant endothelial cells were arranged in loosely cohesive clusters admixed with erythrocytes and neutrophils. These irregular contoured cells had abundant cytoplasm, hyperchromatic oval nuclei and distinct nucleoli (Figure ).
Figure 2. (a–d) FNAC of the case. Malignant endothelial cells are arranged in loosely cohesive clusters admixed with erythrocytes (E) (Papanicolau ×200).
This case re-applied to our clinic for surgery; considering the clinical findings, total thyroidectomy was performed in the first place with a suspicious for ‘poorly differentiated thyroid carcinoma’. During surgery, a tumor was macroscopically detected that infiltrated into the right recurrent nerve. The right lobe of total thyroidectomy material was measured as 7.5 × 4.5 × 4 cm and left lobe was 4.5 × 2×1.5 cm in dimension but the right vocal cord of the case became paralytic. The macroscopic sections of right lobe had cystic and hemorrhagic nodules with irregular inner surface, the largest in 2.5 cm length (Figure ). In other sides of the right lobe and in macroscopic sections of left lobe, there were local calcified nodules and heterogenic appearance in brown-beige colors (Figure ).
The sections from formalin fixed and paraffin-embedded tissues in 2.5 µm thickness were stained with H&E (Figure ). Microscopically, the malign differentiated neoplasm invading the thyroid parenchyma was detected with hemorrhagic and necrotic regions and many anastomosing vascular canals (Figure ). These partly rudimentary cleft-like vascular canals were surrounded with polygonal shaped and mostly epithelioid-like cells constituting local cordons with abundant cytoplasm, dense hyperchromatic nucleus located eccentric and clear eosinophilic nucleoli. In these cells, pleomorphism and high mitotic activity were significant. Many erythrocytes were observed around proliferated cells and inside vascular canals (Figure ). There were sarcoma metastases in 3 of the 11 dissected left cervical lymph nodes.
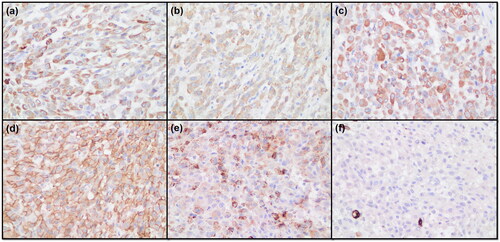
Immunohistochemical analysis confirmed the diagnosis of angiosarcoma with positive staining for factor VIII, CD31, vimentin, laminin, pan-cytokeratin and negative staining for CD34, thyroglobulin, calcitonin, type IV collagen, p53 and actin (Figure ) (Figure ). Ki-67 proliferation index was 60% in the sarcoma component. Besides a large number of nodules with hyperplastic appearance around the parenchyma of the thyroid, some lymphocytic inflammation composing lymphoid aggregates was remarkable (Figure ).
Figure 3. (a) Macroscopic image of a section from thyroid of the primary angiosarcoma case. A number of enlarged nodules are detected in different sizes, some of which are cystic formations. (b–c–d) Histopathological image of the case. Atypical cells with hyperchromatic nuclei and vascular channels containing erythrocytes are prominent (H&E, ×110, ×200, ×400).
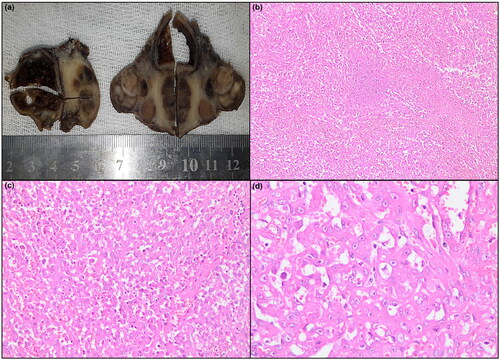
Figure 4. Immunohistochemical images of the case. (a) Positive staining of cytoplasmic granules for pan-cytokeratin (×400). (b) Positive staining of the cytoplasm for laminin (×400). (c) Positive staining of cytoplasm for vimentin (×400). (d) Positive staining of cytoplasm for CD31 (×400). (e) Positive granular staining of the cytoplasm for factor VIII (×400). (f) Negative staining for CD34 (×400).
Discussion
Being very rare mesenchymal tumor of the thyroid, primary angiosarcoma has been observed mostly in Alp zones of Europe [Citation4,Citation6,Citation8]. Clinical symptoms of the disease, as in this case, are anaplastic findings resembling to carcinoma. These tumors have highly similar macroscopic and microscopic appearance with soft tissue angiosarcomas [Citation2,Citation7]. Yet, the current case is an unusual example of the angiosarcoma in the thyroid gland in a young female patient, who was initially diagnosed as ‘undifferentiated thyroid carcinoma’ in an external clinic and then as ‘primary thyroid angiosarcoma’ in our clinic based on histopathological and immunohistochemical analysis.
The diagnosis of angiosarcoma is challenging for surgeons and pathologists and is one of the most debated vascular pathologies of the thyroid [Citation2,Citation4]. However, now it is clearly acknowledged that the distinction between malign neoplastic angiosarcoma in thyroid and anaplastic or undifferentiated carcinoma in thyroid can be performed by histopathology and immunohistochemistry. Moreover, liquid-based cytology with ThinPrep method can facilitate the differential diagnosis of malign vascular tumor in the thyroid. In the present case, the diagnosis was determined not only by macroscopic and histopathological analysis but also immunohistochemical staining and cytopathology which exhibited true primary angiosarcoma.
FNAC with acellular smears can generally limit the diagnosis of sarcoma and so inconclusive in defining the correct histotype [Citation2,Citation9–12]. We are unable to develop a consistent overall cytopathologic picture from the provided findings. Numerous cytologic characteristics have been reported, frequently varying based on the tumor’s degree of differentiation. The cellularity of classical angiosarcomas varied (half had few cells), they had a hemorrhagic background, spindle-shaped, round, epithelioid to oval, isolated or clustered cells, and erythrophagocytosis [Citation13]. Luckily, our retrospective evaluation of FNA smears of this case showed swollen spindle-shaped atypical endothelial cells constituting rare vascular canals in the thyroid, associated with angiosarcoma. However, only application of an immunohistochemical stains including endothelial markers (more than one) in addition to the conventional epithelial, melanocytic, lymphoid, and myogenic markers, allows defining the correct histological type on a needle biopsy. Factor VIII, CD31, laminin, vimentin are the most sensitive and useful endothelial markers, as they were at least positive in this case, whereas vascular marker such as CD34 is always negative [Citation2,Citation9]. In keeping with the literature, epithelial markers were found as positively expressed in our case for factor VIII, CD31, vimentin, laminin and pancytokeratin but other markers were negative for CD34, thyroglobulin, calcitonin, type IV collagen, p53 and actin. Additionally, cases that are positive for factor VIII, CD31, pancytokeratin are determined to be epithelioid angiosarcoma and should also be taken into consideration [Citation11]. Moreover, positive factor VIII, CD31, pancytokeratin staining was observed in this angiosarcoma case. To sum up, a thyroid angiosarcoma can be detected by the expression of endothelial markers in combination with absence of expression of thyroglobulin, calcitonin, type IV collagen, p53 and SMA [Citation14,Citation15].
Anaplastic thyroid carcinoma should be included in your differential diagnosis in thyroid aspiration where a pleomorphism and necrotic background are common. The term ‘high-grade pleomorphic, epithelial-derived malignancy with epithelial and spindle features’ refers to anaplastic thyroid cancer (ATC). Although the cellularity of cytological samples varies, most FNA patients are either moderately or highly cellular. ATC’s cyto-morphological characteristics include spindle- or epithelioid-shaped cells, as well as certain multinucleate large, plasmacytoid, or rhabdoid cell morphologies that are present against a background of tumor diathesis. Enlarged and pleomorphic nuclei with prominent irregular nucleoli, parachromatin clearance, and coarse chromatin clumping are observed in tumor cells. There may be widespread inflammation, necrotic backdrop, and both normal and aberrant mitotic figures. Osteoclast-like large cells are less prevalent than other cell patterns, despite the giant cell variety being a well-known morphologic pattern. TTF-1 and thyroglobulin generally result in negative ATC results. Over 50% of cases, particularly those with epithelioid morphology, maintain PAX-8, and cytokeratin positive indicates that ATC is epithelial in nature. A substantial fraction of ATC cases exhibits overexpression of P53, beta-catenin, and cyclin-D1. A subgroup of ATC exhibits negative results for epithelial markers, particularly those with spindled cytomorphology. A TP53 mutation is among the most common genetic changes [Citation16]. However, unlike carcinoma, angiosarcomas express the vascular markers ERG, CD34, and CD31, which would help to support the diagnosis like present case.
There have only been 60 histologically verified cases of primary angiosarcoma of the thyroid gland described in the English literature as of 2021, making it an extremely rare form of cancer [Citation17,Citation18]. Our case supports the peak incidence reported in the current data, which occurs in the seventh decade of life and is primarily observed in females [Citation17]. There are only three case reports from Turkey according to the English literature [Citation4,Citation6,Citation7]. Cytological material could be obtained from only two of these patients [Citation6,Citation7]. The micrographs of the bone marrow aspiration of one of these patients with bone marrow metastases were presented in the study [Citation7]. However, the cytological micrographs were not shared in the other study. In the third case report, the fine needle aspiration materials were insufficient for diagnosis [Citation4]. Therefore, our study is the third study achieved to obtain sufficient cytological material among the case reports from Turkey. And also, to the best of our knowledge, this is one of rare cases of primary angiosarcoma of the thyroid and showing macroscopic and histopathological findings with liquid-based cytopathology prepared by ThinPrep Pap test.
Angiosarcoma of the thyroid is a type of head and neck neoplasm with a poor prognosis, which morphologically resembles a soft tissue sarcoma, and exhibits epithelial and endothelial differentiation. In addition, cytopathology can be valuable but not sufficient in the diagnosis; however, histochemical investigation of a variety of markers is required for the differential diagnosis of angiosarcoma, such as CD31, CD34, factor VIII, vimentin and pancytokeratin. As a result, considering the FNA findings of the malign tumors in the thyroid, angiosarcoma should also be considered and be included in the differential diagnosis of thyroid tumors.
Ethical approval
This study was conducted according to the Helsinki principles, the patient signed the consent for the participation and nothing offensive was done against the patient’s privacy. Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the editor of this journal.
Informed consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Authors’ contribution
BYB drafted the manuscript; BYB, IC, TY, ATE, IK collected all medical reports of the patients, BYB, IC revised the manuscript critically. All authors read and approved the final manuscript.
Acknowledgements
The study was presented as a poster at the 27th National Pathology Congress held in Antalya, Turkey.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Bala NM, Simões P, Aragüés JM, et al. Non-alpine primary thyroid angiosarcoma. Arch Endocrinol Metab. 2022;66(3):425–428.
- Saoud C, Lam H, Callegari F, et al. Cytopathology of mesenchymal tumors of the thyroid gland: analysis of 12 cases from multinational institutions with review of the literature. J Am Soc Cytopathol. 2023;12(6):436–450. doi: 10.1016/j.jasc.2023.09.004.
- Petronella P, Scorzelli M, Luise R, et al. Primary thyroid angiosarcoma: an unusual localization. World J Surg Oncol. 2012;10(1):73. doi: 10.1186/1477-7819-10-73.
- Altinay S, Ozen A, Namal E, et al. Electron microscopic analysis of an angiosarcoma of the thyroid from a non-Alpine endemic goiter region: a case report and brief review of the literature. Oncol Lett. 2014;8(5):2117–2121. doi: 10.3892/ol.2014.2470.
- Gouveia P, Silva C, Magalhães F, et al. Non-Alpine thyroid angiosarcoma. Int J Surg Case Rep. 2013;4(5):524–527. doi: 10.1016/j.ijscr.2013.02.005.
- Bayır Ö, Yılmazer D, Ersoy R, et al. An extremely rare case of thyroid malignancy from the non-Alpine region: angiosarcoma. Int J Surg Case Rep. 2016;19:92–96. doi: 10.1016/j.ijscr.2015.12.028.
- Yilmazlar T, Kirdak T, Adim S, et al. A case of hemangiosarcoma in thyroid with severe anemia due to bone marrow metastasis. Endocr J. 2005;52(1):57–59. doi: 10.1507/endocrj.52.57.
- Tanda F, Massarelli G, Bosincu L, et al. Angiosarcoma of the thyroid: a light, electron microscopic and histoimmunological study. Hum Pathol. 1988;19(6):742–745. doi: 10.1016/s0046-8177(88)80183-7.
- Collini P, Barisella M, Renne SL, et al. Epithelioid angiosarcoma of the thyroid gland without distant metastases at diagnosis: report of six cases with a long follow-up. Virchows Arch. 2016;469(2):223–232. doi: 10.1007/s00428-016-1964-3.
- Lepe M, Hui Y, Pisharodi L, et al. Primary diagnosis of angiosarcoma by fine needle aspiration: lessons learned from 3 cases. Diagn Cytopathol. 2018;46(4):349–354. doi: 10.1002/dc.23853.
- Isa NM, James DT, Saw TH, et al. Primary angiosarcoma of the thyroid gland with recurrence diagnosed by fine needle aspiration: a case report. Diagn Cytopathol. 2009;37(6):427–432. doi: 10.1002/dc.21065.
- Eusebi V, Carcangiu ML, Dina R, et al. Keratin-positive epithelioid angiosarcoma of thyroid. A report of four cases. Am J Surg Pathol. 1990;14(8):737–747. doi: 10.1097/00000478-199008000-00004.
- Klijanienko J, Caillaud JM, Lagacé R, et al. Cytohistologic correlations in angiosarcoma including classic and epithelioid variants: Institut Curie’s experience. Diagn Cytopathol. 2003;29(3):140–145. doi: 10.1002/dc.10335.
- Marina M, Corcione L, Serra MF, et al. Primary epithelioid angiosarcoma of the thyroid in a patient occupationally exposed to radiations. Front Endocrinol. 2018;9:577. doi: 10.3389/fendo.2018.00577.
- Chan JK. Newly available antibodies with practical applications in surgical pathology. Int J Surg Pathol. 2013;21(6):553–572. doi: 10.1177/1066896913507601.
- Rossi ED, Faquin WC, Pantanowitz L. Cytologic features of aggressive variants of follicular-derived thyroid carcinoma. Cancer Cytopathol. 2019;127(7):432–446. doi: 10.1002/cncy.22136.
- Huang SH, Wu SC. Primary angiosarcoma of the thyroid in an Asian woman: a case report with review of the literature. Case Rep Pathol. 2020;2020:9068506. 31 doi: 10.1155/2020/9068506.
- Negură I, Bădescu MC, Rezuş C, et al. Morphology and one immunohistochemical marker are enough for diagnosis of primary thyroid angiosarcoma. Arch Clin Cases. 2021;8(1):7–13. doi: 10.22551/2021.30.0801.10178.