
ABSTRACT
Objective: In the present study, we aimed to examine the relationship between the oxidative metabolism with disease severity, sociodemographic, and clinical characteristics in the patients with schizophrenia.
Methods: Seventy-one patients with schizophrenia and 76 healthy volunteers were included in the study. Plasma total antioxidant level (TAL) and total oxidant level (TOL) were analyzed, and oxidative stress index (OSI) was calculated.
Results: There was a statistically significant increase in TOL and OSI and decrease in TAL in the patients with schizophrenia compared to the controls (p < .05). There were positive, mild, statistically significant correlations between TOL, OSI, and Positive and Negative Syndrome Scale-Total scores (p = .01, p = .01, respectively), Positive and Negative Syndrome Scale-Negative scores (p = .002, p = .001, respectively), Positive and Negative Syndrome Scale Global Psychopathology scores (p = .03, p = .03, respectively), and Clinical Global Impression-Severity Scale scores (p = .008, p = .009 respectively). OSI levels were significantly lower in the patients who were on treatment with atypical antipsychotics (AAP) compared to the patients who were on typical antipsychotics (TAP) and combined antipsychotic (CAP) agents (p = .032).
Conclusions: Oxidative stress was higher in schizophrenia patients. The increased severity of negative symptoms was in line with the disruption in oxidative balance. Oxidative stress is quite lower in AAP users compared to the TAP and CAP users. One of the mechanisms underlying the fact that AAPs are more effective on negative symptoms than typical agents may be the positive effect on the oxidative stress.
Introduction
Schizophrenia is a chronic and severe psychiatric illness affecting about 1% of the world’s population and it causes disability [Citation1]. There are researches on many factors exploring etiopathogenesis of schizophrenia, including genetic and biochemical studies [Citation2]. One of the important factors considered to be involved in the pathophysiology of schizophrenia is excessive production of free radical agents [Citation3–5] and failure of antioxidant defense processes [Citation6–8]. Although many studies were conducted on this field, further studies are needed to establish the role of oxidative imbalance in schizophrenia [Citation5]. Cellular oxidative damage is generally caused by free radicals and reactive oxygen species (ROS). Many biochemical processes are involved in low ROS levels [Citation9].
Oxidative stress is the disruption of the balance in the oxidative mechanism as a result of increase in oxidant level and/or decrease in antioxidant level [Citation10]. Several methods have been developed to measure oxidant and antioxidant capacity. Total oxidant level (TOL) and total antioxidant level (TAL) may reflect plasma oxidant and antioxidant status, respectively [Citation11]. Specific metabolites have remained incapable in detecting oxidant and antioxidant capacity. Therefore, we believed that calculation of total oxidant–antioxidant capacity in order to evaluate the relationship between oxidative metabolism and certain disorders may provide us a more global understanding.
Many researchers have carried out studies about the role of oxidative stress on the pathogenesis, progression, and treatment of psychiatric disorders. These studies have found a disruption of the oxidative balance in psychiatric disorders. It was reported that this imbalance is sustained in some psychiatric disorders even during remission while some studies reported recovery in oxidative imbalance after treatment [Citation2,Citation12–16].
There is a growing number of studies on this topic, since toxic radicals are suggested to play a role in the etiology of schizophrenia [Citation17]. The increase in oxidative stress index (OSI) in patients with schizophrenia may play a significant role in pathophysiological disease mechanisms. On the other hand, increased oxidative stress may be a result of pathological processes [Citation3,Citation18–20]. The studies examining the relationship between schizophrenia and total oxidant–antioxidant levels are scarce [Citation21,Citation22]. To our knowledge, there is only one study that analyzed TOL and OSI as well as TAL in schizophrenia [Citation23]. In line with the study conducted by Virit et al., we assessed the relation of total oxidant–antioxidant level and OSI with Positive and Negative Syndrome Scale (PANSS) and Clinical Global Impression-Severity Scale (CGI-S) scores in patients with schizophrenia. The results of the present study were different than those reported by Virit et al. [Citation24] Furthermore, the present study evaluated the relationship between antipsychotic (AP) medications and Oxidative Stress Parameters (OSP) levels. The present study found different results when compared to those of other studies that evaluated the relationship between OSPs and AP [Citation24,Citation25].
The aim of the present study was to examine the association of OSPs with sociodemographic and clinical data as well as medications in schizophrenia patients.
Methods
Methods and measurements
The present study is a case-control study and it aims to determine total oxidant and total antioxidant and OSI and compared to the healthy controls.
The study group is composed of patients who were referred to Harran University Hospital’s Psychosis Unit and who were diagnosed with schizophrenia according to DSM-IV diagnosis criteria during routine control. The inclusion criteria were as follows: diagnosis of schizophrenia according to DSM-IV diagnosis criteria, age between 18 and 65 years, being able to read the informed consent form and being able to respond questions after reading the form with the caregiver, being competent to provide informed consent, and absence of other psychiatric conditions.
The exclusion criteria were as follows: being less than 18 years old, presence of an accompanying psychiatric disorder except for schizophrenia, pregnancy, antioxidant agent use (vitamin E and vitamin C), xanthine oxidase inhibitor use (allopurinol and folic acid), presence of a severe neurologic disease (epilepsy, cerebrovascular event, Parkinson’s disease, etc.), presence of severe mental retardation, presence of a remarkable history for severe head trauma, obesity, hypertension, diabetes or other endocrine disorders, current substance-use disorder, or history of substance-use disorder.
The study was approved by the Harran University’s Ethics Committee. The control group is composed of healthy individuals who were matched with the patients in terms of age, gender, and who did not have a history of psychiatric disorder. After providing thorough information to the subjects about the study procedures, all subjects provided written consents for participation in the study in accordance with the Helsinki Declaration [Citation26]. Sociodemographic data and clinical data were recorded for the patients and the control group. Seventy-one patients (55 males and 16 females), who were followed regularly and who met inclusion criteria of the study, and 76 healthy controls (60 males and 16 females) were enrolled. The severity of the symptoms in patients with schizophrenia was assessed by PANSS [Citation27] and CGI-S scales. Simpson–Angus (S-A) scale was used to determine extrapyramidal symptom severity in the patients. Blood samples were drawn between 08:00 and 09:00 a.m. after at least 12 hours of fasting and abstinence from smoking. Blood samples of the patient and control groups were collected from antecubital vein. Blood samples were collected into heparinized blood tubes and kept on ice, and the samples were centrifuged at 3000 rpm for five minutes within six hours to separate the serum and plasma. Serum samples were stored at −80°C for TAL and TOL analysis. TAL and TOL were measured in serum samples at Biochemistry Laboratory of Harran University, Faculty of Medicine and OSI was calculated. The measurements were performed using a fully automated colorimetric method developed by Erel [Citation28].
OSI calculation
OSI was calculated by TOL (mmol H2O2 equiv./l)/TAL (mmol Trolox equiv./l) × 100. Unit: AU (arbitrary unit).
Results
Distribution of the patient and the control groups and their sociodemographic data are shown in .
Table 1. Distribution of the patients and controls according to the gender and sociodemographic data.
Gender distribution did not differ between the groups (p > .062).
The average age at disease onset was 22.3 ± 7.6 years; the average disease period was 12.7 ± 10.6 years. Of these patients, 61.8% had a prior history of hospitalization. The family history for psychiatric disorder was remarkable in 40.2% of the cases. There were no statistically significant differences between the patient and the control groups in terms of family history and oxidative parameters (p > .064).
There were no statistically significant differences in smoking status of the patient and the control group (p > .073). The cigarette smokers accounted for 63.4% (n = 45) of the patients with schizophrenia and 69.7% (n = 53) of the subjects in the control group. The average number of daily cigarettes smoked was 32 ± 11 in patients with schizophrenia and 29.3 ± 10.3 in the control group (p > .068) ().
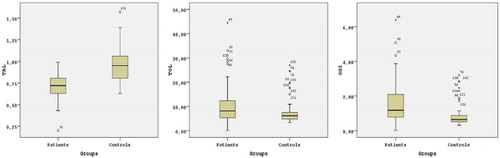
There were statistically significant differences in terms of TAL (p < .001), TOL (p < .002), and OSI (p < .001) levels of the patient and control groups (). This comparison was presented in .
Table 2. Comparison of TAL, TOL, and OSI levels between the patients and controls.
Figure 1. Comparison of TAL, TOL, and OSI levels according to the patients and controls.
OSI average was found to be significantly higher in the smoker and non-smoker subgroups of patients with schizophrenia compared to the control group (p < .05); TAL and TOL averages did not significantly differ according to the smoking status (p > .05). There were no statistically significant correlations between OSPs and number of cigarettes smoked, age at disease onset, disease period, and body mass index (BMI) (p > .058, p > .061, p > .078, and p > .086, respectively).
The distribution of schizophrenia subtypes in our study was as follows: paranoid type, 56.3% (n = 40); disorganized type 9.9% (n = 7); undifferentiated type, 8.5% (n = 6); catatonic type 1.4% (n = 1); and residual type (23.9% (n = 17). There were no statistically significant differences in oxidative parameters between the subtypes of schizophrenia (p > .083).
Furthermore, a statistically significant correlation was not found between OSP and PANSS-Positive (PANSS-P) value (p > .067). Positive, mild, statistically significant correlations were found between TOL and PANSS-Total (PANSS-T), PANSS-Negative (PANSS-N), PANSS-General Psychopathology (PANSS-G), and CGI-S scores. Furthermore, positive, statistically significant correlations were also found between OSI and PANSS-T, PANSS-N, PANSS-G, and CGI-S scores.
Typical AP (TAP) drugs were used by 21.1% (n = 15) of the patients, while 54.9% (n = 39) of the patients were treated with atypical AP (AAP) and 23.9% (n = 17) of the patients used combined APs (CAPs) (typical and atypical).
A statistically significant correlation was not found between OSP and S-A scale score (p > .088).
Discussion
One of the most important findings of the present study is higher TOL and OSI in contrast to lower TAL values in patients with schizophrenia compared to the healthy controls. Elevated level of oxidants was shown in many studies that were conducted previously in patients with schizophrenia and other psychiatric disorders. However, specific oxidant and/or antioxidant levels were explored in most of these studies. Since oxygen free radicals (OFRs) are very reactive and have a short life and low density, it is difficult to detect their values. By considering the fact that this difficulty may cause deficient measurements, measurement of total oxidant and antioxidant levels (TAL and TOL) instead of specific values might provide better results [Citation1,Citation23].
Different opinions were suggested in many studies conducted on oxidative stress in patients with schizophrenia. In general, these studies found elevated levels in the plasma, erythrocytes, platelets, and cerebrospinal fluid [Citation2,Citation15,Citation16,Citation29–37]. There are many study findings which showed elevated oxidant levels in many psychiatric disorders such as bipolar disorder, major depression, and panic disorder besides schizophrenia [Citation14,Citation38–40]. A cause-and-effect relationship between psychiatric disorders and oxidant increase could not be explained completely in all these studies. In other words, whether increased oxidants cause psychiatric disorders or psychiatric disorders cause oxidant increase is not known clearly. However, current data suggest that oxidants may cause psychiatric disorders. The studies show that increase in the oxidant levels may cause damage in cellular constituents and functional molecules [Citation41]. Nowadays, the role of OFRs in the etiopathogenesis of schizophrenia has become one of the most important considerations [Citation4,Citation36,Citation37,Citation42–44]. The present study also supports that hypothesis. Although there are different results derived from previous studies, it is generally expressed that antioxidants are reduced in schizophrenia [Citation8,Citation24,Citation35,Citation40,Citation42,Citation43,Citation45–47]. In the present study, significantly lower plasma TAL levels were found in patients with schizophrenia compared to the controls. Plasma antioxidants have a significant contribution to TAL. Albumin, uric acid, ascorbic acid, bilirubin, and alpha tocopherol in human plasma and blood consist more than 85% of total antioxidant capacity [Citation48]. Determination of total antioxidant capacity serves as an indicator for all antioxidants [Citation24,Citation49]. In line with our study, lower plasma TAL values were reported in patients with schizophrenia in the studies conducted using the same method [Citation24,Citation50,Citation51]. In other words, it may be expressed that antioxidant defense mechanisms against oxidative stress may differ according to the individuals and environmental conditions. TOL was found to be increased in the present study. However, a decrease was found in antioxidant levels, although a reactive increase has been expected. This suggests that patients are under oxidative stress and there is a defect in their defense system against oxidative products or another factor exists in the medium that causes a decrease in antioxidant capacity.
Another important finding of our study is that an increased OSI in patients with schizophrenia. OSI is an index obtained by dividing TOL to TAL and it is used as a general assessment standard related to oxidative stress [Citation52]. Both aspects of the oxidative metabolism as oxidant–antioxidant may be evaluated using OSI. We may observe how antioxidants change according to the oxidant level in the blood by OSI. Decreased antioxidants and/or increased oxidants can cause an increase in OSI. OSI defines an imbalance in support of oxidants between oxidative processes and antioxidant defense systems [Citation53,Citation54]. OSI increase may cause vital disruptions in many physiological mechanisms [Citation45,Citation55,Citation56].
In this present study, TAL was found to be lower in patients with schizophrenia compared to the control group. In response to oxidative stress, compensatory increase is expected in TAL. We think that decreased TAL in schizophrenia patients is a result of diminished compensatory response. Increased oxidative stress is common in schizophrenia and in vivo mechanisms are insufficient to neutralize this condition. OSI levels are reported to be increased in schizophrenia [Citation25,Citation31,Citation46,Citation47,Citation57,Citation58]. May it be oxidative stress and increased OSI or insufficient antioxidant response, and the resulting disruption in the equilibrium between these mechanisms ultimately could cause breakdown of cellular elements and functional compounds [Citation59]. Recovery can be observed in the symptoms to a certain extent by addition of an antioxidant such as N-acetyl cysteine [Citation60,Citation61]. However, further studies are required to evaluate antioxidant therapies in schizophrenia.
Smoking is common among patients with schizophrenia and it is known that smoking affects OSPs [Citation61]. There were no significant differences between the schizophrenia group and the control group in terms of the number of smokers and number of cigarettes smoked. Mean OSI was found to be significantly higher in patients with schizophrenia when compared to the control group (). This finding suggests that OSI is impaired in patients with schizophrenia independently of smoking. In other words, changes in oxidative parameters and OSI elevation are independent from smoking, in line with our study [Citation24,Citation32]. Blood samples were drawn after 12 hours of fasting and abstinence from smoking. According to the previous literature, increased oxidant levels caused by smoking is reversed in 4 hours after smoking [Citation61]. We consider that due to this reversal effect, the present study did not find significant difference between smokers and non-smokers in terms of OSPs.
Table 3. Comparison of oxidative parameters of the patients and controls according to smoking status.
Another finding of the present study is comparison of OSPs, PANSS-T, PANSS subscale scores, and CGI scores. In the present study, significant and positive correlations were found between TOL and PANSS-T, PANSS-N, PANSS-G, and CGI scores. Furthermore, statistically significant and positive correlations were also found between OSI and PANSS-T, PANSS-N, PANSS-G, and CGI scores. No significant correlations were found between TAL and PANSS-T, PANSS subscales and CGI scores (p > .05). Furthermore, there were no statistically significant correlations between PANSS-P and OSPs (TAL, TOL, and OSI) (). TOL and OSI levels increased with increasing PANSS-T, PANSS-N, PANSS-G, and CGI scores that show disease severity. Furthermore, no statistically significant correlations were found between PANSS-P and OSP. It can be speculated that positive symptoms of schizophrenia do not linearly associate with oxidative stress. TAL did not present statistically significant linear association with any of the scale scores. There are contradictory results on this topic in the literature [Citation24,Citation51,Citation62–65]. There are several factors which are responsible for controversial results. These factors include individual experience of disorder, course of illness, medical interventions, co-morbid conditions and medical interventions, and lifestyle. Due to these factors, it is difficult to generalize the results obtained from different studies [Citation65].
Table 4. Correlations between biochemical parameters and PANSS, PANSS-P, PANSS-N, PANSS-G, and CGI-S scores.
In line with several other studies, a significant relation was not found between schizophrenia types and oxidative parameters in the present study [Citation24,Citation33,Citation44]. Furthermore, different data were also obtained in some studies [Citation51,Citation66]. The results of these studies did not reveal a clear relationship between schizophrenia subtypes and specific oxidant and antioxidant enzyme levels. There are supporting and conflicting data. These studies might originate a biological basis for exclusion of subtypes of schizophrenia in DSM-5.
There were no statistically significant linear associations between OSPs and number of cigarettes, BMI, age at disease onset, and disease period. Consistent with the literature, we did not find significant correlation between TAL and age, sex, duration of illness, smoking status, education, and BMI [Citation20,Citation62,Citation66]. These results indicate that oxidative stress is associated directly with the disease.
OSI level was significantly lower in AAP users when compared to TAP and CAP users. Although TOL level was lower in AAP users, there was no significant difference. We did not find any statistically significant differences in TAL level between AP medication groups. Lower TOL and OSI levels in AAP users indicate that AAPs are more reliable in terms of oxidative stress. There were no statistically significant differences between TAP and CAP users (). Although there are diverse opinions, our findings support avoiding TAP and combined pharmacological interventions in order to protect patients against increased oxidative stress. There are conflicting results on this topic. Taneli et al. reported that 6-week AP treatment did not show a significant effect on serum Nitric oxide (NO) levels of patients with schizophrenia [Citation67].
Table 5. Comparison of oxidative parameters according to antipsychotics used for the treatment.
In the study conducted by Gama et al. [Citation25], superoxide dismutase (SOD) activity and tiobarbituric acid reactive substance (TBARS) levels were measured in patients, who used haloperidol and clozapine due to schizophrenia at least for two years. Serum TBARS level was significantly higher in clozapine users when compared to haloperidol users. There was no difference in SOD levels between clozapine and haloperidol users [Citation25]. In a study where AP effects on NO levels were explored in patients with schizophrenia, plasma nitrate levels were higher in patients treated with haloperidol compared to risperidone or olanzapine users. This statistically significant difference found in plasma nitrate levels was between haloperidol and risperidone groups when compared to olanzapine group [Citation65]. No difference was found in OSP levels between TAP, AAP, and CAP users in the study conducted by Virit et al.[Citation24] This study was the first to evaluate the association between AAPs and TAL, TOL, and OSI. There are some differences compared to the present study. These are as follows:
Family history of psychiatric disorder was more remarkable in the present study.
Number of cigarettes smoked was not reported in the study by Virit et al.
In their study, Virit et al. included patients on combined pharmacotherapy with antidepressants, mood stabilizers, and anxiolytics.
Since all differences above might affect OSPs, some of the results may contradict with the data of the present study.
Consequently, oxidative stress is unbalanced in schizophrenia and this condition is usually present with increased oxidation and decreased antioxidants or both. Increase in the severity of negative symptoms was consistent with the disruption in oxidative balance. Oxidative stress is quite lower in AAP users when compared to TAP and CAP users. Better outcomes with AAP in negative symptoms may point out possible positive effects of these drugs on oxidative stress.
Limitations of the study include small sample size. The results suggest there is a clinical benefit from early detection of schizophrenia using serum TOL and TAL. However, further studies are needed to verify this.
In conclusion, in this present study, oxidative stress was found higher in schizophrenia patients. The increased severity of negative symptoms was consistent with the disruption in oxidative balance. Oxidative stress was lower in AAP users compared to TAP and CAP users. This finding might support the idea that one of the mechanisms underlying the fact that AAPs are more effective on negative symptoms than typical agents might have been their positive effect on the oxidative stress. Further studies with larger sample size are needed to replicate our findings.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Jablensky A, Sartorius N, Ernberg G, et al. Schizophrenia: manifestations, incidence and course in different cultures. A world health organization ten-country study. Psychol Med Monogr Suppl. 1992;20:1–97.
- Yanik M, Vural H, Kocyigit A, et al. Is the arginine-nitric oxide pathway involved in the pathogenesis of schizophrenia? Neuropsychobiology. 2003;47(2):61–65.
- Lohr JB. Oxygen radicals and neuropsychiatric illness. Some Speculations. Arch Gen Psychiatry. 1991;48(12):1097–1106.
- Reddy RD, Yao JK. Free radical pathology in schizophrenia: a review. Prostaglandins Leukot Essent Fatty Acids. 1996;55(1–2):33–43.
- Mahadik SP, Mukherjee S. Free radical pathology and antioxidant defense in schizophrenia: a review. Schizophr Res. 1996;19(1):1–17.
- Yao JK, Reddy R, McElhinny LG, et al. Effects of haloperidol on antioxidant defense system enzymes in schizophrenia. J Psychiatr Res. 1998;32(6):385–391.
- Zhang XY, Zhou DF, Cao LY, et al. Elevated blood superoxide dismutase in neuroleptic-free schizophrenia: association with positive symptoms. Psychiatry Res. 2003;117(1):85–88.
- McCreadie RG, MacDonald E, Wiles D, et al. The nithsdale schizophrenia surveys. XIV: Plasma lipid peroxide and serum vitamin E levels in patients with and without tardive dyskinesia, and in normal subjects. Br J Psychiatry. 1995;167(5):610–617.
- Valko M, Leibfritz D, Moncol J, et al. Free radicals and antioxidants in normal physiological functions and human disease. Int J Biochem Cell Biol. 2007;39(1):44–84.
- Valko M, Rhodes CJ, Moncol J, et al. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem Biol Interact. 2006;160(1):1–40.
- McGue M, Gottesman II. The genetic epidemiology of schizophrenia and the design of linkage studies. Eur Arch Psychiatry Clin Neurosci. 1991;240(3):174–181.
- Savas HA, Gergerlioglu HS, Armutcu F, et al. Elevated serum nitric oxide and superoxide dismutase in euthymic bipolar patients: impact of past episodes. World J Biol Psychiatry. 2006;7(1):51–55.
- Gergerlioglu HS, Savas HA, Bulbul F, et al. Changes in nitric oxide level and superoxide dismutase activity during antimanic treatment. Prog Neuropsychopharmacol Biol Psychiatry. 2007;31(3):697–702.
- Herken H, Gurel A, Selek S, et al. Adenosine deaminase, nitric oxide, superoxide dismutase, and xanthine oxidase in patients with major depression: impact of antidepressant treatment. Arch Med Res. 2007;38(2):247–252.
- Herken H, Akyol O, Yilmaz HR, et al. Nitric oxide, adenosine deaminase, xanthine oxidase and superoxide dismutase in patients with panic disorder: alterations by antidepressant treatment. Hum Psychopharmacol. 2006;21(1):53–59.
- Sogut S, Zoroglu SS, Ozyurt H, et al. Changes in nitric oxide levels and antioxidant enzyme activities may have a role in the pathophysiological mechanisms involved in autism. Clin Chim Acta. 2003;331(1–2):111–117.
- Hoffer A, Osmond H, Smythies J. Schizophrenia; a new approach. II. Result of a year’s research. J Ment Sci. 1954;100(418):29–45.
- Halliwell B. Free radicals, antioxidants, and human disease: curiosity, cause, or consequence? Lancet. 1994;344(8924):721–724.
- Yao JK, Reddy RD, van Kammen DP. Oxidative damage and schizophrenia: an overview of the evidence and its therapeutic implications. CNS Drugs. 2001;15(4):287–310.
- Reddy R, Keshavan M, Yao JK. Reduced plasma antioxidants in first-episode patients with schizophrenia. Schizophr Res. 2003;62(3):205–212.
- Uranova NA, Casanova MF, DeVaughn NM, et al. Ultrastructural alterations of synaptic contacts and astrocytes in postmortem caudate nucleus of schizophrenic patients. Schizophr Res. 1996;22(1):81–83.
- Lieberman JA. Is schizophrenia a neurodegenerative disorder? A clinical and neurobiological perspective. Biol Psychiatry. 1999;46(6):729–739.
- Southorn PA, Powis G. Free radicals in medicine. I. Chemical nature and biologic reactions. Mayo Clin Proc. 1988;63(4):381–389.
- Virit O, Altindag A, Yumru M, et al. A defect in the antioxidant defense system in schizophrenia. Neuropsychobiology. 2009;60(2):87–93.
- Gama CS, Salvador M, Andreazza AC, et al. Elevated serum superoxide dismutase and thiobarbituric acid reactive substances in schizophrenia: a study of patients treated with haloperidol or clozapine. Prog Neuropsychopharmacol Biol Psychiatry. 2006;30(3):512–515.
- JR S. Neurology and neuropathology of schizophrenia, in schizophrenia as a brain disease. New York: Oxford University Press; 1987.
- Weinberger DR. From neuropathology to neurodevelopment. Lancet. 1995;346(8974):552–557.
- Erel O. A novel automated direct measurement method for total antioxidant capacity using a new generation, more stable ABTS radical cation. Clin Biochem. 2004;37(4):277–285.
- Dawson VL, Dawson TM. Nitric oxide actions in neurochemistry. Neurochem Int. 1996;29(2):97–110.
- Karson CN, Griffin WS, Mrak RE, et al. Nitric oxide synthase (NOS) in schizophrenia: increases in cerebellar vermis. Mol Chem Neuropathol. 1996;27(3):275–284.
- Akyol O, Herken H, Uz E, et al. The indices of endogenous oxidative and antioxidative processes in plasma from schizophrenic patients. The possible role of oxidant/antioxidant imbalance. Prog Neuropsychopharmacol Biol Psychiatry. 2002;26(5):995–1005.
- Derin D, Yazici A, Erkoc S. The investigation of free radical metabolism and antioxidant defense systems elements in patients with schizophrenic disorder. Klinik Psikofarmakoloji Bulteni/Bull Clin Psychopharmacol. 2001;11(3):174–182. Turkish.
- Zoroglu SS, Herken H, Yurekli M, et al. The possible pathophysiological role of plasma nitric oxide and adrenomedullin in schizophrenia. J Psychiatr Res. 2002;36(5):309–315.
- Zoroglu SS, Yurekli M, Meram I, et al. Pathophysiological role of nitric oxide and adrenomedullin in autism. Cell Biochem Funct. 2003;21(1):55–60.
- Bulut M, Selek S, Gergerlioglu HS, et al. Malondialdehyde levels in adult attention-deficit hyperactivity disorder. J Psychiatry Neurosci. 2007;32(6):435–438.
- Kanofsky JD, Sandyk R. Antioxidants in the treatment of schizophrenia. Int J Neurosci. 1991;62(1–2):97–100.
- Mahadik SP, Evans D, Lal H. Oxidative stress and role of antioxidant and omega-3 essential fatty acid supplementation in schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2001;25(3):463–493.
- Selek S, Savas HA, Gergerlioglu HS, et al. The course of nitric oxide and superoxide dismutase during treatment of bipolar depressive episode. J Affect Disord. 2008;107(1–3):89–94.
- Savas HA, Herken H, Yurekli M, et al. Possible role of nitric oxide and adrenomedullin in bipolar affective disorder. Neuropsychobiology. 2002;45(2):57–61.
- Yu YW, Chen TJ, Wang YC, et al. Association analysis for neuronal nitric oxide synthase gene polymorphism with major depression and fluoxetine response. Neuropsychobiology. 2003;47(3):137–140.
- Akyol O, Zoroglu SS, Armutcu F, et al. Nitric oxide as a physiopathological factor in neuropsychiatric disorders. In Vivo. 2004;18(3):377–390.
- Akyol O, Yanik M, Elyas H, et al. Association between Ala-9Val polymorphism of Mn-SOD gene and schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2005;29(1):123–131.
- Mahadik SP, Scheffer RE. Oxidative injury and potential use of antioxidants in schizophrenia. Prostaglandins Leukot Essent Fatty Acids. 1996;55(1-2):45–54.
- Herken H, Uz E, Ozyurt H, et al. Evidence that the activities of erythrocyte free radical scavenging enzymes and the products of lipid peroxidation are increased in different forms of schizophrenia. Mol Psychiatry. 2001;6(1):66–73.
- Berg D, Youdim MB, Riederer P. Redox imbalance. Cell Tissue Res. 2004;318(1):201–213.
- Albayrak Y, Unsal C, Beyazyuz M, et al. Reduced total antioxidant level and increased oxidative stress in patients with deficit schizophrenia: a preliminary study. Prog Neuropsychopharmacol Biol Psychiatry. 2013;45:144–149.
- Padurariu M, Ciobica A, Dobrin I, et al. Evaluation of antioxidant enzymes activities and lipid peroxidation in schizophrenic patients treated with typical and atypical antipsychotics. Neurosci Lett. 2010;479(3):317–320.
- Yao JK, Reddy R, McElhinny LG, et al. Reduced status of plasma total antioxidant capacity in schizophrenia. Schizophr Res. 1998;32(1):1–8.
- Selek S, Herken H, Bulut M, et al. Oxidative imbalance in obsessive compulsive disorder patients: a total evaluation of oxidant-antioxidant status. Prog Neuropsychopharmacol Biol Psychiatry. 2008;32(2):487–491.
- Zhang XY, Zhou DF, Shen YC, et al. Effects of risperidone and haloperidol on superoxide dismutase and nitric oxide in schizophrenia. Neuropharmacology. 2012;62(5–6):1928–1934.
- Ustundag B, Atmaca M, Kirtas O, et al. Total antioxidant response in patients with schizophrenia. Psychiatry Clin Neurosci. 2006;60(4):458–464.
- Aycicek A, Erel O, Kocyigit A. Decreased total antioxidant capacity and increased oxidative stress in passive smoker infants and their mothers. Pediatr Int. 2005;47(6):635–639.
- Yao JK, Keshavan MS. Antioxidants, redox signaling, and pathophysiology in schizophrenia: an integrative view. Antioxid Redox Signal. 2011;15(7):2011–2035.
- Lohr JB, Kuczenski R, Niculescu AB. Oxidative mechanisms and tardive dyskinesia. CNS Drugs. 2003;17(1):47–62.
- Kohen R, Nyska A. Oxidation of biological systems: oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol Pathol. 2002;30(6):620–650.
- Qing H, Xu H, Wei Z, et al. The ability of atypical antipsychotic drugs vs. haloperidol to protect PC12 cells against MPP+-induced apoptosis. Eur J Neurosci. 2003;17(8):1563–1570.
- Zhang XY, Zhou DF, Cao LY, et al. Blood superoxide dismutase level in schizophrenic patients with tardive dyskinesia: association with dyskinetic movements. Schizophr Res. 2003;62(3):245–250.
- Srivastava N, Barthwal MK, Dalal PK, et al. Nitrite content and antioxidant enzyme levels in the blood of schizophrenia patients. Psychopharmacology (Berl). 2001;158(2):140–145.
- Obata T. Dopamine efflux by MPTP and hydroxyl radical generation. J Neural Transm (Vienna). 2002;109(9):1159–1180.
- Bulut M, Savas HA, Altindag A, et al. Beneficial effects of N-acetylcysteine in treatment resistant schizophrenia. World J Biol Psychiatry. 2009;10(4 Pt 2):626–628.
- Miller ER, Appel LJ, Jiang L, et al. Association between cigarette smoking and lipidperoxidation in a controlled feding study. Circulation. 1997;96(4):1097–1101.
- Li XF, Zheng YL, Xiu MH, et al. Reduced plasma total antioxidant status in first-episode drug-naive patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2011;35(4):1064–1067.
- Yao JK, Reddy R, Van Kammen DP. Reduced level of plasma antioxidant uric acid in schizophrenia. Psychiatry Res. 1998;80(1):29–39.
- Nakano Y, Yoshimura R, Nakano H, et al. Association between plasma nitric oxide metabolites levels and negative symptoms of schizophrenia: a pilot study. Hum Psychopharmacol. 2010;25(2):139–144.
- Minutolo G, Petralia A, Dipasquale S, et al. Nitric oxide in patients with schizophrenia: the relationship with the severity of illness and the antipsychotic treatment. Expert Opin Pharmacother. 2012;13(14):1989–1997.
- Zhang XY, Tan YL, Cao LY, et al. Antioxidant enzymes and lipid peroxidation in different forms of schizophrenia treated with typical and atypical antipsychotics. Schizophr Res. 2006;81(2–3):291–300.
- Taneli F, Pirildar S, Akdeniz F, et al. Serum nitric oxide metabolite levels and the effect of antipsychotic therapy in schizophrenia. Arch Med Res. 2004;35(5):401–405.