
ABSTRACT
Objectives: The Syrian Civil War forced millions into asylum in neighbouring countries. Refugees/asylum seekers have elevated risk for psychopathology with the most important being post-traumatic stress disorder (PTSD). Subjective experiences and symptoms of the hosting populations which have also experienced similar traumas have received relatively little attention up to now. We aimed to evaluate the effects of Syrian Civil War in terms of psychopathology, traumatic experiences and PTSD on Turkish primary school students living in Suruç which is on the border with Syria and hosts a large population of asylum seekers.
Methods: Two randomly selected schools operating in the district were included in the study. Sociodemographic Data forms, Child Behaviour Checklist (CBCL), Children’s Post-traumatic Reaction Index (CPRI) were used for evaluations. Data were analysed with SPSS 23.0. P was set at 0.05 (two-tailed).
Results: Most common traumatic experiences via parental report were witnessing explosions (26.9%), witnessing injuries of extended family/relatives (21.8%) and witnessing deaths of acquaintances (17.9%). Lifetime traumatic events and lifetime self-injurious behaviour in children via parental report were 26.9% and 19.9%; respectively. Of 156 students (53.2% male) with a mean age of 8.8 years (S.D. = 1.3), 13.5% obtained externalizing scores, 11.0% obtained internalizing scores and 13.5% obtained total scores in the clinical range of CBCL. 98.7% reported PTSD symptoms in moderate and above severity in CPRI. Most common traumatic experiences reported by children included hearing explosions/gunshots (17.3%), damage to residences (17.3%), and witnessing deaths of extended family/ acquaintances (12.8%). Female gender (p = .00), witnessing loss of family members/acquaintances in Syrian Civil War (p = .01) and clinically significant PTSD symptoms in CPRI.
Conclusion: Children in communities hosting Syrian refugees/asylum seekers may also have elevated symptoms of PTSD and female gender may be a risk factor for those symptoms.
Introduction
The Syrian Civil War which has started in 2011 and has been ongoing for the past five years forced millions of Syrians into asylum in neighbouring countries, foremost among them Turkey [Citation1–3]. Almost three million asylum seekers and refugees are registered in Turkey with an additional two million residing in other Middle Eastern and North African countries [Citation2,Citation3]. It is known that refugees and asylum seekers are under elevated risk for various forms of psychopathology with the most important being post-traumatic stress disorder (PTSD) [Citation4]. Existing studies conducted among asylum seekers and refugees residing in Turkey support this view and report the prevalence of PTSD as being 33.5–61.1% among adults and 10.5–49.4% among children [Citation5–10].
The subjective experiences and symptoms of the hosting populations which have also sometimes experienced similar traumas have received relatively little attention up to now [Citation8,Citation11–14]. Some of the Turkish citizens living in Şanlıurfa county have had relatives from their extended families residing in Syria and had witnessed their traumas and/or cared for them. Also, the facts that Turkey signed the Geneva Conventions of 1951 with a geographical limitation (i.e. it does not denote refugee status to asylum seekers from Non-European countries) and that most of the Syrian asylum seekers lived outside of off camps may exacerbate the burden on local communities and infrastructure [Citation3]. Suruc district in Şanlıurfa is one of the most hard-pressed communities in Turkey in this regard and its population was reported to rise from 101.964 in 2012–232.00 in 2015 [Citation15].
As such, this study aimed to evaluate the effects of Syrian Civil War in terms of symptoms of psychopathology, traumatic experiences and clinically significant post-traumatic stress symptoms as a proxy for PTSD on Turkish primary school students living in Suruç. The primary aims were:
To determine the prevalence of psychopathology as assessed by broad-band scales completed by parents and/or teachers.
To determine the rates of post-traumatic stress disorder symptoms as assessed by broad-band scales completed by parents and narrow-band scale completed by children themselves.
To determine the rates of lifetime and Syrian Civil War-related traumatic events in parents and children.
To evaluate differences in rates of traumatic events and scale scores between genders.
Methods
Participants and procedures
Recent data suggest that approximately 13.0% of children and adolescents worldwide may be affected by mental disorders associated with dysfunction [Citation16]. A priori calculation of sample size with PASSTM 14 Power Analysis and Sample Size Software (NCSS LLC., UT, USA, 2015) yielded 193 participants will be required to evaluate a proportion of 0.13 at 95.0% Confidence Interval at a p-value of 0.05 (two-sided) [Citation17–19]. A priori calculations for t-tests yielded that 210 participants would be required to detect a medium (d = 0.5) effect size at 95% power and a p-value of 0.05 (two-sided) while those for χ2 tests revealed that a sample of 145 would yield 95% power for the same effect size [Citation20].
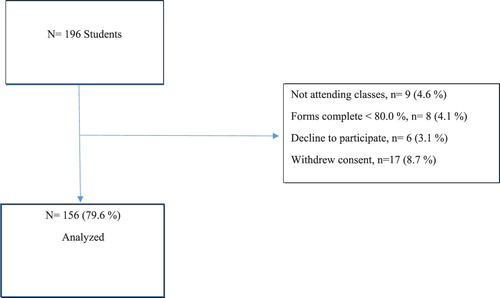
For the 2014–2015 educational year 231.070 primary school students (50.8% male) were reported to receive education in Şanlıurfa county [Citation21]. It was also found that 30.977 students received formal education in the Suruç district within the 2015–2016 educational year and that 30 primary schools operated within the district with each having five classes. Because each class reportedly had an average of 33 students the study universe included 4950 students [Citation22]. Two randomly selected schools (out of 20) operating at the county centre and were representative of the socio-economic status of the parents as well as attendance of Syrian children according to official statistics were included in the study [Citation21]. Within the third to sixth grades of those 196 students were enrolled. Due to student inattendance, incomplete fulfilment and exclusion for various reasons 79.6% of the students (n = 156) could be evaluated. Study flow-chart according to STROBE Statement is provided in [Citation23].
Figure 1. Study flowchart for evaluating the Syrian Civil War’s effects on Turkish school children residing in Suruc.
Institutional Review Board approval prior to commencement of the study was procured from the Ethics Committee of Hasan Kalyoncu University Institute of Social Sciences. Approval to contact children, parents and their teachers was granted by the Suruc Directorate of National Education.
The study was conducted between May and June 2016. Eligible children and their parents were informed of study protocols and aims via telephone and a baseline interview was planned within school hours at the Guidance and Counselling Office. Informed consent from parents and assent of children were procured prior to study evaluations. Afterwards, children completed Post-traumatic Reactions Index for Children (PTRI-C) at the School Guidance Office with the help of the principal investigator. Sociodemographic Survey Forms and parent report forms of Child Behaviour Checklist 4–18 (CBCL-4/18) were completed by parents in a separate room. Families of children with clinically significant symptoms in parent and/or self-reports were provided feedback and referred for further evaluations and treatments to the nearest Child and Adolescent Psychiatry Departments.
Measures
Sociodemographic data form
This form was prepared by the researchers to gather socio-demographic information pertaining to the family and children. The questions in this form include ages, educational and vocational status of parents, monthly income, and housing (own/rent) status. The form also included questions about the effects of Syrian Civil War (i.e. loss of relatives due to conflict, witnessing loss due to conflict, experiencing injury due to conflict, witnessing injury due to conflict, witnessing explosions, experiencing kidnappings of/threats to relatives by conflict parties, experience of change in family economic status due to refugees/asylum seekers, experience of change in education of children due to refugees/asylum seekers, experiencing change in infrastructure of house due to refugees/asylum seekers, damage to housing due to conflict, lifetime traumatic experience of children [war/armed conflict, explosion, earthquake, accident, loss of relatives], lifetime self-injurious behaviours of children). Self-injurious behaviours were operationalized as instances of intentional cutting, burning, hitting, bruising, and scalding of children’s own bodies that were observed by parents.
Child behaviour checklist 4–18 (CBCL- 4/18)
Parent form of the Turkish version of CBCL-4/18 was used to evaluate behaviours of study participants [Citation24]. CBCL-4/18 1991 form was translated to Turkish by Erol and colleagues [Citation25]. Internal reliabilities of internalizing, externalizing and total problem scales at the original study were found as 0.82, 0.81 and 0.88; respectively. Test–retest reliability was found to be 0.70 [Citation26]. CBCL-4/18 was used in multiple studies conducted on Turkish youth in the past and has been found to be valid and reliable [Citation25–28]. In this study internal reliabilities of internalizing, externalizing and total problem scales were found to be 0.87, 0.93 and 0.98; respectively. National median scores for Total Problem Scale Scores were previously found to range from 19 to 26 (6–11 years old vs. 12–18 years old).
Post-traumatic Reactions Index for Children (PTRI-C)
PTRI-C was developed by Pynoos and colleagues to evaluate symptoms of stress after traumatic events [Citation29]. The index includes 20 questions which are scored as five-choice Likert type scales. The Turkish translation and reliability/ validity was established by Erden and colleagues [Citation30]. Cronbach alpha for the whole scale was 0.75 and test–retest reliability was found to be 0.86. The scores from PTRI-C may range from 0 to 100 and similar to the original version scores of 40 and higher denote clinically significant symptoms of Post-traumatic Stress Disorder [Citation30–32]. In this study, Cronbach alpha for the whole scale was found to be 0.78.
Data analysis
Post hoc calculations revealed that a sample of 156 achieved a power of 80.0% to evaluate proportion of 0.13 at 95.0% Confidence Interval at a p-value of 0.05 [Citation17,Citation33,Citation34]. This sample size achieved 96. 3% power for χ2 and 87.3% power for t-tests, respectively [Citation20].
Data were analysed with SPSS 23.0 and with Student’s t-test for independent samples or their non-parametric equivalents. Assumptions of normality were testes with Kolmogorov–Smirnov test. Nominal data were described in numbers and frequencies while quantitative data were summarized either as means and standard deviations (S.D.) or medians and inter-quartile ranges (IQR) depending on normality. Chi-square tests with either Yates’ or Fisher’s corrections were used to evaluate relationships between nominal data. P was set at 0.05 (two-tailed).
Results
The mean age of the study sample was 8.8 years (S.D. = 1.3) with almost equal ratios from both genders (53.2% male). The children were mostly attending fourth (38.5%) and third (27.6%) grades. Mean ages for mothers and fathers were 37.1 (S.D. = 6.0) and 40.8 (S.D. = 6.8) years; respectively. Half of the families resided at the county centre while the rest were living in villages nearby. All of the mothers were housewives while the fathers mostly worked as artisans (67.3%). Mothers had mostly primary school educations (39.7%) or were illiterate (34.6%). Fathers also had limited educations with 32.7% being primary and 25.6% being secondary school graduates. The majority of the families’ income was below the nationally established levels of poverty for the year 2016 (91.7%). Most lived in ramshackle buildings and 75.6% of the children did not have a room of their own.
Most of the parents of children (72.4%) reported that they were negatively affected by Syrian asylum seekers living in Suruc. Subjectively negative experiences of parents were listed as economic (56.4%), infrastructural (48.7%), and educational (39.1%) problems. The most common traumatic experiences related to Syrian Civil War reported by parents of children were witnessing explosions (26.9%), witnessing injuries of extended family/ relatives (21.8%) and witnessing death of acquaintances (17.9%, ).
Table 1. Parent-reported traumatic experiences related to Syrian Civil War in Turkish.schoolchildren residing in Suruc county.
The parents reported that 26.9% of their children experienced life-threatening traumatic events during their lifetime. Almost one-fifth (19.9%) reported self-injurious behaviours in their children within their life-time. The children reported their traumatic experiences as witnessing explosions/gunshots (17.3%), damage to house (17.3%), witnessing deaths of relatives/acquaintances (12.8%) and being injured themselves (8.3%). Median numbers of self-reported traumatic events for lifetime of children were 5.0 (IQR = 4.0).
Among the whole sample 13.5% obtained externalizing scores, 11.0% obtained internalizing scores and 13.5% obtained total scores in clinical range of the CBCL (). The corresponding rates for attention problems and thought problems were 3.2% and 7.1%; respectively. Almost 8% of children (7.7%) scored in the clinical range for delinquent behaviours while 1.3% scored in this range for aggressive behaviours. Clinically significant anxiety/depression, somatic complaints, social problems and social withdrawal were reported in 0.6%, 3.2%, 6.4% and 7.1%; respectively.
Table 2. T scores in parent reports of Child Behaviour Checklist for 4–18 years old children according to gender.
No difference between genders could be found in terms of clinically significant CBCL 4/18 scores. Significantly higher lifetime and Syrian Civil War-related traumatic experiences were reported in children with clinically significant somatic complaints (Mann–Whitney U test, Z=−2.1, p = .03 and Z=−2.4, p = .02; respectively). Children with clinically significant delinquent behaviours experience significantly higher indicators of poverty (Z=−2.5, p = .01). Mean T scores for Post-traumatic Stress Problems Subscale of CBCL-4/18 for males and females were found to be 54.4 (S.D. = 1.4) and 37.2 (S.D. = 0.0); respectively. When a cut-off of 70 or higher was used nine children (5.8% of the whole sample, 77.8% male) demonstrated PTS Problems at clinical range according to parental reports ().
Mean score for PTRI- C in the study sample was 41.0 (S.D. = 9.9) with girls having significantly higher scores (49.7 vs. 33.4, Student’s t-test, p < .0001). It was previously reported that children with scores of 25 or higher in PTRI-C may have significant symptoms of PTSD and that scores of 40 and above may correspond to a clinical diagnosis of PTSD [Citation30–32]. When those criteria are applied rate of moderate–severe PTSD symptoms was found to be 98.7% while 48.1% of the sample may have symptoms corresponding to a clinical diagnosis.
Bivariate analyses revealed relationships between female gender (p = .00, Fisher’s exact test, Phi = 0.9), parental report of loss of family member/acquaintances in Syrian Civil War (p = .01, Fisher’s exact test, Phi = 0.22) and clinically significant PTSD symptoms in CPTS-RI. There was also a trend level association between clinical levels of social withdrawal in P-CBCL-4/18 and clinically significant PTSD symptoms in CPTS-RI (p = .06, Fisher’s exact test, Phi = 0.17).
Conclusions
In this cross-sectional study we evaluated a sample of Turkish school children residing in a community with a large influx of Syrian asylum seekers and refugees and attending third to sixth grades of two schools located at the district centre in terms of life-time traumatic experiences, traumatic experiences pertaining to Syrian Civil War, life-time self-injurious behaviour, parent and self-reported PTSD symptoms and psychopathology as reported by parents and teachers. As a result, we found that most of the children and their families lived in poverty and that their living conditions were inadequate. Most of the parents had negative perceptions of hosting asylum seekers/refugees and one-fourth to one-fifth reported trauma-related to Syrian Civil War. Almost one-fourth of parents reported lifetime psychological trauma in their children while one-fifth reported that their offspring displayed self-injurious behaviours. Up to 17.3% of children reported witnessing explosions/gunshots during the conflict and damaged houses. Among the whole sample 13.5% obtained externalizing scores, 11.0% obtained internalizing scores and 13.5% obtained total scores in clinical range of the CBCL completed by parents. Clinically significant PTSD symptoms were found in 5.8% of children via parental and 48.1% via self-report scales.
In our sample, there were no significant differences between genders for CBCL scores. Studies conducted in countries with various cultures, including Turkey, have reported that males displayed elevated levels of externalizing symptoms when evaluated with CBCL [Citation24–28]. Our results do not support those observations. The lack of gender differences in our sample for externalizing disorders as measured by CBCL may be due to sampling and/or reporting bias. The parents may have limited opportunities to observe behavioural problems of their children and addition of teacher reports may have changed our results. Because parents received support from the principal investigator for completion of forms, limited literacy may not be an explanation for our findings. Further studies on similar samples may benefit from gathering information from multiple informants.
Girls are known to report elevated rates of internalizing and PTSD symptoms in self-report scales and in accordance with those observations mean scores female children in PTRI-C in our sample were significantly higher [Citation16,Citation29–32]. Concordance of internalizing symptoms with parent reports are known to be limited and similar to those observations parents in our study reported lower rates of PTSD symptoms among their children with no significant difference between genders [Citation16,Citation24–32].
Previous studies conducted on Syrian children with refugee/asylum seeker status living in Turkey have reported rates of clinically significant psychopathology (including PTSD) as 10.5–49.4% among children [Citation5–10]. There are no studies to determine the prevalence of PTSD on nationally representative samples of Turkish schoolchildren with existing studies focusing on traumatized populations [Citation28–32]. In the National Comorbidity Survey Replication- Adolescent Supplement (NCSR-A) conducted in the US lifetime rate of PTSD was found to be 5.0% in adolescents with a female preponderance (8.0% vs. 2.3%) [Citation35,Citation36]. However, the rate of PTSD in younger children is not known. Risk factors for PTSD in youth include exposure variables related to trauma, female gender, previous traumatic experiences, preexisting psychopathology, parental psychopathology and low social supports [Citation35,Citation36]. Our results suggest that post-traumatic stress symptoms may be prevalent among hosting populations and be associated with female gender, life-time trauma exposure and loss.
The rate of clinically significant PTSD symptoms and psychopathologies as evaluated by CBCL were similar to those reported previously. The similarity in rates of clinically significant psychopathology between our sample of Turkish youth and those reported previously for Syrian youth may be explained by the geographical proximity of Suruc to the Turkish–Syrian border and by the fact that children in our sample have relatives living in Syria. That is; geographical, cultural and social proximity of the traumatic experiences pertaining to the Syrian Civil War may have affected children in our sample.
Our findings should be evaluated within their limitations. Firstly, the cross-sectional design of our study precludes hypotheses on causality. Secondly, the rates of non-retention and attrition were high. Analysis revealed that those with missing data were poorer and had less educated parents suggesting that even among our sample of disadvantaged youth, the results may not be generalizable to those with elevated risk factors for psychopathology. Thirdly, the dependence on parental and self-report scales for determining psychopathology and lack of structured clinical evaluations of children may reduce reliability. Fourth, self- and parental- reports may be subject to recall, desirability and reporting bias. Fifth, the findings may not be generalized to students attending schools outside the county centre. Despite those limitations, our results suggest that children in communities hosting Syrian refugees/asylum seekers may also have elevated symptoms of PTSD and that female gender may be a risk factor for those symptoms. The subjective experiences and symptoms of the hosting populations which have also sometimes experienced similar traumas have received relatively little attention up to now and should be further studied.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Ali Evren Tufan http://orcid.org/0000-0001-5207-6240
Notes
* This study was conducted as Dissertation Study of Sinem Tabur for the degree of Masters in Clinical Psychology at the Department of Psychology of Hasan Kalyoncu University Institute of Social Sciences. Parts of the study were previously presented as “The Effects of Syrian Civil War on Turkish Primary School Students: Prevalence and Predictors of Psychopathology, Traumatic Experiences and Post -Traumatic Stress Symptoms: A Field Study from Suruç” at the 17th International ESCAP Congress (07.09.2017–07.11.2017, Switzerland). The study has not been presented before in full and is not currently under consideration for publication at another journal. All of the authors have contributed to the study and confirm the integrity of the research process and data.
References
- Hinnebusch R. Syria: from ‘authoritarian upgrading’ to revolution? Int Aff. 2012;88(1):95–113. doi: 10.1111/j.1468-2346.2012.01059.x
- Icduygu A. Syrian refugees in Turkey: the long road ahead. Washington (DC): Migration Policy Institute; 2015. Available from: http://www.migrationpolicy.org/sites/default/files/publications/TCM-Protection-Syria.pdf
- Icduygu A, Millet E. Syrian refugees in Turkey: insecure lives in an environment of pseudo-integration. Working Paper No:13 of Istanbul Policy Institute of the Sabancı University, Istanbul; 2016. Available from: http://www.iai.it/sites/default/files/gte_wp_13.pdf
- Tufan AE, Alkin M, Bosgelmez S. Post-traumatic stress disorder among asylum seekers and refugees in Istanbul may be predicted by torture and loss due to violence. Nord J Psychiatry. 2013;67(3):219–224. doi: 10.3109/08039488.2012.732113
- Alpak G, Unal A, Bulbul F, et al. Post- traumatic stress disorder among Syrian refugees in Turkey: a cross- sectional study. Int J Psychiatry Clin Pract. 2015;19(1):45–50. doi: 10.3109/13651501.2014.961930
- Ceri V, Özlü-Erkilic Z, Özer Ü, et al. Psychiatric symptoms and disorders among Yazidi children and adolescents immediately after forced migration following ISIS attacks. Neuropsychiatr. 2016;30(3):145–150. doi: 10.1007/s40211-016-0195-9
- Gormez V, Kilic HN, Orengul AC, et al. Psychopathology and associated risk factors among forcibly displaced Syrian children and adolescents. J Immigr Minor Health. 2018;20(3):529–535. doi: 10.1007/s10903-017-0680-7
- Marwa KI. Psychosocial Sequels of Syrian conflict. J Psychiatry. 2016;19:355. doi: 10.4172/2378-5756.1000355
- Nasıroğlu S, Çeri V. Posttraumatic stress and depression in Yazidi refugees. Neuropsychiatr Dis Treat. 2016;12:2941–2948. doi: 10.2147/NDT.S119506
- Yalin Sapmaz S, Uzel Tanriverdi B, Ozturk M, et al. Immigration-related mental health disorders in refugees 5–18 years old living in Turkey. Neuropsychiatr Dis Treat. 2017;13:2813–2821. doi: 10.2147/NDT.S150592
- Chemali Z, Borba CPC, Johnson K, et al. Humanitarian space and well-being: effectiveness of training on a psychosocial intervention for host community-refugee interaction. Med Confl Surv. 2017;33(2):141–161. doi: 10.1080/13623699.2017.1323303
- Elsafti AM, van Berlaer G, Al Safadi M, et al. Children in the Syrian Civil War: the familial, educational, and public health impact of ongoing violence. Disaster Med Public Health Prep. 2016;10(6):874–882. doi: 10.1017/dmp.2016.165
- Ozer S, Sirin S, Oppedal B. Bahçeşehir study of Syrian refugee children in Turkey. Oslo: Norwegian Institute of Public Health; 2012. Available from: https://www.fhi.no/globalassets/migrering/dokumenter/pdf/bahcesehir-study-report3.pdf
- Sirin SR, Rogers-Sirin L. The educational and mental health needs of Syrian refugee children. Washington (DC): Migration Policy Institute; 2015. Available from: http://www.migrationpolicy.org/sites/default/files/publications/FCD-Sirin-Rogers-FINAL.pdf
- Leylak A, Şulul Ö. Suruç’un nüfusu patladı [The population of Suruç has exploded]. Hürriyet Daily 2014. Available from: http://www.hurriyet.com.tr/surucun-nufusu-patladi-27258856
- Polanczyk GV, Salum GA, Sugaya LS, et al. Annual research review: a meta-analysis of the world-wide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. 2015;56:345–365. doi: 10.1111/jcpp.12381
- PASS 14 power analysis and sample size software. Kaysville (UT): NCSS, LLC; 2015. Available from: http://ncss.com/software/pass.
- Fleiss JL, Levin B, Paik MC. Statistical methods for rates and proportions. 3rd ed. New York: John Wiley & Sons; 2003.
- Newcombe RG. Two-sided confidence intervals for the single proportion: comparison of seven methods. Stat Med. 1998;17:857–872. doi: 10.1002/(SICI)1097-0258(19980430)17:8<857::AID-SIM777>3.0.CO;2-E
- Faul F, Erdfelder E, Lang AG, et al. G*power 3: a flexible statistical power analysis program for the social, behavioral and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi: 10.3758/BF03193146
- National Educational Statistics- Formal Education 2014/15. Ministry of National Education Directorate for Strategy Development. Publication of the Program for Official Statistics. Ankara. 2015.
- Anonymous. Available from: http://suruc.meb.gov.tr/</authors, 2015.
- The PLOS Medicine Editors. Observational studies: Getting Clear about Transparency. PLoS Med. 2014;11(8):e1001711. doi: 10.1371/journal.pmed.1001711
- Achenbach TM, Ruffle TM. The child behavior checklist and related forms for assessing behavioral/emotional problems and competencies. Pediatr Rev. 2000;21(8):265–271. doi: 10.1542/pir.21-8-265
- Erol N, Kılıç C, Ulusoy M, et al. Turkey Mental Health Profile Report. General Directorate of the Health Project of Ministry of Health of Republic of Turkey. Ankara; 1998.
- Erol N, Simsek Z. Child and youth behavior checklists manual for school age. Ankara: Mentis Press; 2010.
- Erol N, Simsek Z, Öner Ö, et al. Epidemiology of attention problems among Turkish children and adolescents: A national study. J Atten Disord. 2008;11(5):538–545. doi: 10.1177/1087054707311214
- Erol N, Simsek Z, Öner Ö, et al. Effects of internal displacement and resettlement on children: mental health problems reported by parents, teachers and youth. Europ Psychiatry. 2005;39:243–246.
- Pynoos RS, Goenjian A, Tashjian M, et al. Post-traumatic stress reactions in children after the 1988 Armenian earthquake. Brit J Psychiatry. 1993;163(2):239–247. doi: 10.1192/bjp.163.2.239
- Erden G, Kılıç EZ, Uslu Rİ, et al. Turkish reliability and validity study of the children’s post-traumatic stress Reactions scale. J Child Adolesc Ment Health. 1999;6(3):143–149. [Turkish].
- Laor N, Wolmer L, Kora M, et al. Posttraumatic, dissociative and grief symptoms in Turkish children exposed to the 1999 earthquakes. J Nerv Ment Dis. 2002;35(3):286–287.
- Kiliç EZ, Rİ U, Erden G, et al. Factors maintaining symptoms of post-traumatic stress disorder in children. Crisis. 1999;7(2):1–8. [Turkish].
- Machin D, Campbell M, Fayers P, et al. Sample size tables for clinical studies. 2nd ed. Malden (MA): Blackwell Science; 1997.
- Ryan TP. Sample size determination and power. Hoboken (NJ): John Wiley & Sons; 2013.
- Kessler R, et al. Prevalence, persistence and sociodemographic correlates of DSM-IV disorders in the national comorbidity survey replication- adolescent sample. Arch Gen Psychiatry. 2012;69:372–380. doi: 10.1001/archgenpsychiatry.2011.160
- Anonymous. Practice parameters for the assessment and treatment of children and adolescents with posttraumatic stress disorder. J Am Acad Child Adolesc Psychiatry. 2010;49:414–430.