
Abstract
Seriously ill or immunocompromised children are at increased risk of invasive fungal infections, particularly candidemia. Candida albicans and Candida parapsilosis are the two most frequent causes of candidemia in pediatric patients. Candidemia in children is associated with high morbidity and mortality, increased length of hospital stays, and higher healthcare costs. Early effective antifungal therapy is the key to improved outcomes. Risk factors for candidemia may be used to identify patients suitable for empiric therapy. Such risk factors include prolonged stay in an intensive care unit, immunosuppression, prior bacterial infection, and recent surgery, as well as the use of a central venous catheter, mechanical ventilation, and/or total parenteral nutrition. Recent guidelines from the Infectious Diseases Society of America recommend consideration of fluconazole or an echinocandin for empiric therapy in suitable candidates, with a preference for an echinocandin in patients with moderate-to-severe disease, recent azole exposure, or high risk of Candida glabrata or Candida krusei infection. Fluconazole or an echinocandin is also preferred initial therapy for non-neutropenic candidemia, depending on disease severity and other characteristics. The guidelines recommend treatment with an echinocandin or lipid formulation of amphotericin B for most patients with neutropenic candidemia, although fluconazole is identified as an alternative for less critically ill patients without recent azole exposure. Risk factors for candidemia – and, hence, criteria for prophylaxis – are less well established in older children than in neonates. Further research is needed to better establish criteria for antifungal prophylaxis in children at high risk for candidemia.
Introduction
Invasive fungal infections are a considerable source of morbidity, mortality, increased length of hospital stays, and high healthcare costs in critically ill or immunocompromised childrenCitation1,Citation2. Most invasive fungal infections in children occur in the hospital setting, and most are caused by Candida spp.Citation1,Citation3. A recent prospective study of pediatric nosocomial bloodstream infections (BSIs) determined that Candida spp. were the third most common microbial cause of BSIs overall (9.4% of isolates), and the most common fungal causeCitation4. The most frequent causes of nosocomial BSI were bacteria: coagulase-negative staphylococci (43.3%) and enterococci (9.4%).
Anatomic and physiologic differences between pediatric and adult patients alter susceptibility to infection by different Candida spp. and approaches to antifungal treatment, including issues relating to drug toxicity, pharmacokinetics, and dosing. There is also much less data to guide decision making in children with invasive fungal infections than in adults with similar infections. The objective of this paper is to provide a general review of invasive candidiasis, and particularly candidemia, in pediatric patients other than neonates, including risk factors, incidence, species distribution, and antifungal therapy. One of the accompanying pieces in this supplement, by Dr. David Kaufman, focuses on invasive candidiasis in neonates. As in that piece, a case-study-centered approach will be used to advance the discussion of various issues of interest. The material here is based on an expert roundtable presentation, and as such, is not meant to be an exhaustive review of the topic.
Risk factors for pediatric candidemia and empiric therapy
Case study: pediatric patient presenting with nosocomial bloodstream infection
A 3-year-old boy is treated in the intensive care unit (ICU) for 2 weeks for multiple medical problems, including short gut syndrome, failure to thrive, gastrointestinal surgery, and problems related to prematurity. He is currently receiving total parenteral nutrition and has a central venous catheter (CVC) in place. He recently received a course of broad-spectrum antibiotics for a catheter-associated bacterial BSI. He now presents with new-onset fever and hypotension. Blood cultures are obtained, and a new round of broad-spectrum antibiotic therapy is initiated pending culture results. The patient is not neutropenic.
This case study presents a young pediatric patient with a number of risk factors for invasive infection or BSI, and a recent history of treatment for a bacterial BSI. The patient now presents with signs of new-onset sepsis. Empiric antibacterial therapy is once again initiated. One of the questions posed by this case is whether the patient has risk factors for fungal infection and should also be considered for empiric antifungal therapy.
Risk factors for invasive candidiasis
Risk factors for fungal infection in pediatric patients are generally similar to those in adult patients. Factors present in the case study that have been linked with increased risk of invasive candidiasis/candidemia in pediatric patients include prolonged stay in an ICU, prior bacterial infection, use of a CVC, and total parenteral nutrition (hyperalimentation)Citation1,Citation3,Citation5. Immunosuppression (related to malignancy and its treatment, transplantation immunosuppressive therapy, or other factors) has also been linked with increased risk of invasive candidiasisCitation3. Additional factors associated with elevated risk of invasive candidiasis include use of mechanical ventilation (endotracheal intubation), dialysis, extended vancomycin use, and recent surgeryCitation1,Citation3,Citation6.
Use of a vascular access device or CVC appears to be a particularly important risk factor. A recent Australian study reported that candidemia was attributed to a vascular access device in 70% of infected children, which was an even higher percentage than in neonates (58%) or adults (44%) with a vascular access deviceCitation7. Another recent study used multivariate regression analysis to identify use of CVCs as an independent risk factor for colonization with Candida spp. in children aged 1 month to 14 years in a pediatric ICU for longer than 5 daysCitation8. Ninety percent of the children in the study who developed candidemia were colonized with Candida, 15% with the same species. presents the results from a study presented at the 2009 annual Society for Healthcare Epidemiology of America (SHEA) meeting of risk factors for candidemia in the pediatric ICUCitation6. Presence of a CVC, total parenteral nutrition, use of antibiotics, and immunosuppression (underlying malignancy) were significant risk factors.
Table 1. Risk factors for candidemia in the pediatric ICU.
Some risk factors for invasive candidiasis may coexist. For example, increased stay in an ICU often means prolonged use of a CVC, mechanical ventilation, and/or total parenteral nutrition, all well-documented risk factors. In the recent study presented at the annual SHEA meeting, the median length of ICU stay for pediatric patients who developed candidemia was 35 days compared with 2.2 days for the ICU cohort that did not develop candidemia – again illustrating the relationship between prolonged ICU stay and risk of developing candidemiaCitation6.
In addition to being present in blood (candidemia), Candida infection can disseminate to end organs, including brain, lungs, liver, heart, kidneys, eyes, and spleen. Disseminated disease is generally considered to be more serious than BSI and to require longer antifungal therapy. A 2004 study by Zaoutis and colleagues reported that persistent candidemia (>3 days) with a CVC in place (odds ratio [OR] = 3.0; 95% confidence interval [CI] = 1.2–7.8; p = 0.02) and immunosuppression (OR = 2.9; 95% CI = 1.2–7.0; p = 0.02) were independent risk factors for disseminated disease in children with candidemiaCitation9. Another recent study of pediatric patients in Turkey reported that disseminated candidiasis was an independent risk factor for candidemia-related death (OR = 8.1, p = 0.01)Citation10.
Other variables reported in the Turkish study to be independent risk factors for mortality in pediatric patients with candidemia included stay in the ICU (OR = 8.1, p = 0.001), prolonged antibiotic therapy (OR = 5.2, p = 0.014), use of total parenteral nutrition (OR = 4.4, p = 0.038), and mechanical ventilation (OR = 4.9, p = 0.01)Citation10. Similarly, Zaoutis and coworkers identified location in the pediatric ICU at the time of infection (hazard ratio [HR] = 6.3; 95% CI = 1.6–24.3) and presence of an arterial catheter (HR = 2.4; 95% CI = 1.1–5.8) as independent risk factors for mortality in children with candidemiaCitation11. More recently, Pasqualotto and colleagues used multivariate analysis to identify failure to remove the CVC as an independent risk factor for early mortality among pediatric patients with candidemiaCitation12. Clearly, many of the risk factors for development of invasive candidiasis/candidemia are also risk factors for mortality in patients with candidemia.
Empiric treatment of suspected invasive candidiasis in non-neutropenic pediatric patients
In the case study, the 3-year-old child has several risk factors for invasive candidiasis/candidemia and infection-related mortality. The question then becomes: should this patient be considered for empiric antifungal therapy? The 2009 guidelines for candidiasis management from the Infectious Diseases Society of America (IDSA) state that “empirical antifungal therapy should be considered for critically ill patients with risk factors for invasive candidiasis and no other known cause of fever, and it should be based on clinical assessment of risk factors, serologic markers for invasive candidiasis, and/or culture data from nonsterile sites…”Citation13. The guidelines further advise that the same therapeutic approach should be followed for children as adults, with attention to differences in dosing regimens. While there is no information concerning culture data from nonsterile sites or serologic markers for disease for the case here, the patient has the other characteristics listed and, hence, should be considered for empiric antifungal therapy.
More specifically, the guidelines recommend empiric treatment with fluconazole or an echinocandin for suspected invasive candidiasis in non-neutropenic patientsCitation13. An echinocandin is preferred in non-neutropenic patients with moderate-to-severe disease, recent exposure to an azole, or who are at high risk of infection due to Candida glabrata or Candida krusei. Recent azole exposure increases the likelihood of infection with an azole-resistant species, and azoles show less activity against C. glabrata or C. krusei than against other Candida spp. Amphotericin B deoxycholate (AmB-d) or a lipid formulation of AmB (LFAmB) are suitable alternatives for non-neutropenic patients with suspected invasive candidiasis if there is intolerance to or limited availability of other antifungals. Caspofungin is the only echinocandin currently approved by the US Food and Drug Administration (FDA) for use in pediatric patients. However, there is growing evidence supporting the use of micafungin in pediatric patients with non-neutropenic invasive candidiasisCitation14–18, some of it coming out while the 2009 IDSA guidelines were being compiled or after its publication. At this time, there is only very limited pharmacokinetic or clinical data concerning anidulafungin therapy in pediatric patientsCitation15.
For suspected invasive candidiasis in neutropenic patients, the 2009 IDSA guidelines recommend LFAmB, an echinocandin, or voriconazole, and cite fluconazole, itraconazole, and AmB-d as alternatives, noting there is a greater risk of toxicity with AmB-d than with LFAmBCitation13. The guidelines also state that azoles should not be used for empiric therapy in patients who received an azole for prophylaxis.
Other epidemiologic features of pediatric candidiasis
Case (continued): blood culture results
Empiric antifungal therapy was considered but not initiated while awaiting blood culture results. The patient’s blood culture results were subsequently received and were positive for a Candida spp. and, more specifically, Candida parapsilosis.
Incidence of candidemia and fungal sepsis
As suspected based on signs and symptoms and the presence of various risk factors for candidemia, the blood culture results for the case study indicate infection with a Candida spp. As discussed earlier, Candida is the third most common microorganism causing nosocomial BSI in pediatric patients, accounting for roughly 9% of all causesCitation4. Furthermore, Candida spp. are the most common cause of invasive fungal infection, followed by Aspergillus sppCitation1. However, it should be noted that diagnosis of candidemia by blood culture is slow and insensitive, although it is the current gold standard.
Based on a review of 10,319,418 cases of sepsis observed in US acute-care hospitals from 1979 through 2000, the rate of sepsis from any cause increased by 8.7% over this approximate 20-year period, while the incidence of sepsis due to fungal organisms increased by 207%Citation19. Presumably a similar increase of fungal sepsis is observed in pediatric and adult patients. A study of adults and children hospitalized in the US in 2000 demonstrated a similar frequency of candidemia in pediatric and adult patients (43 cases vs. 30 cases per 100,000 admissions, respectively), although there were more adult than pediatric admissions (8949 vs. 1118)Citation2. Abelson and colleagues reported that the rate of fungemia (85% due to Candida spp.) at a tertiary care US hospital increased by 91% from the 1991-through-1996 period to the 1997-through-2001 period (mean of 6.8 vs. 13.0 cases)Citation20.
Mortality and healthcare costs associated with candidemia
The rate of increase in fungal sepsis is particularly noteworthy considering the severe outcomes associated with fungal sepsis or candidemia. Watson and coworkers reported that fungal sepsis was associated with the second highest case fatality (13.0%) in children older than 1 year and up to 19 years old in 1995, just behind pneumococcal sepsis (14.5%)Citation21. The rate was higher in children aged 1 to 10 years (16.8%) or 11 to 19 years (11.6%) than in those younger than 1 year (10.8%). Similarly, Zaoutis and colleagues used large databases for adult (n = 8949) and pediatric (n = 1118) hospitalized patients in the US to demonstrate that pediatric patients (median age 1 year; range 0–7 years) with a diagnosis of candidemia had a 10% higher rate of mortality (95% CI = 6.2–13.8) compared with matched candidemia-unexposed hospitalized patientsCitation2. Wisplinghoff and colleagues reported that the crude mortality rate with monomicrobial BSI was second highest for those involving Candida spp. (19.6%), behind only Pseudomonas aeruginosa BSI (28.7%)Citation4. The mean age of patients in this study was 2 ± 4 years (range 0–24 years), with half of the patients younger than 1 year.
In addition to mortality, pediatric candidemia has also been linked with longer hospital stays and increased costs, and relatively greater increases than seen in adult patients with candidemia. For example, in the study just mentioned by Zaoutis and coworkers, candidemia in pediatric patients was also associated with a mean 21.1-day increase in length of hospital stay (95% CI = 14.1–27.8) and a mean increase in total per-patient hospital charges of $92,266 (95% CI = $65,058–$119,474). The comparable numbers in adult patients were a mean 10.1-day increase in length of stay (95% CI = 8.9–11.3 days) and mean increase in total per-patient hospital charges of $39,331 (95% CI = $33,604–$45,602)Citation2. However, other studies suggest that roughly 30% to 40% of the increases in hospitalization and costs are incurred by very low birth weight neonatesCitation21. Nonetheless, these findings underscore the importance of finding ways to optimize the prevention or treatment of invasive candidiasis in pediatric patients.
Invasive candidiasis and species distribution
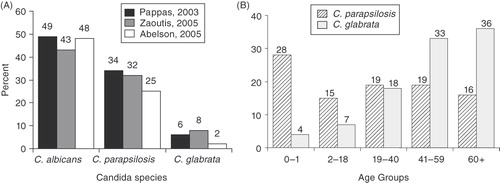
In the case study, the argument was made that an empiric antifungal should be considered. Assuming a decision was made to pursue empiric therapy, the next question is: what species is most likely to be the cause of a fungal infection in a 3-year-old child with the identified risk factors? As illustrated in albicans and C. parapsilosis are the first and second most common species causing invasive candidiasis/candidemia in pediatric patientsCitation20,Citation22,Citation23. As people age and become adults, C. glabrata becomes the second most common non-albicans cause of invasive candidiasis or candidemia, replacing C. parapsilosis ()Citation24.
Figure 1. (A) Species distribution for all pediatric patients with invasive candidiasis (Abelson, 2005Citation20; Pappas, 2003Citation22; Zaoutis, 2005Citation23). (B) Species distribution by age group (Malani, 2001Citation24).
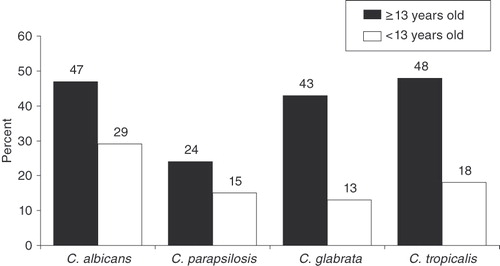
The distribution of Candida spp. in candidemia is important, in part, because some species seem to be associated with better outcomes compared with others. For example, in both adult and pediatric patients, candidemia due to C. parapsilosis is associated with lower mortality rates than cases involving C. albicans. illustrates this findingCitation22. In this study, C. parapsilosis related candidemia was also associated with lower mortality rates compared with Candida tropicalis or C. glabrata related candidemia in adults. With respect to younger patients (<13 years old), there probably were not enough patients with C. glabrata or C. tropicalis candidemia to draw any firm conclusions. The other conclusion that can be drawn from is that crude mortality rates seem to be generally lower in younger (pediatric) than older (adult) patients with candidemia regardless of the Candida spp. involved.
Figure 2. Mortality associated with selected Candida spp. among younger (<13 years old; n = 144) and older (≥13 years old; n = 1447) patients with candidemiaCitation22.
Management of pediatric candidiasis
Case (continued): initiating antifungal therapy
The patient is initiated on caspofungin therapy (a single 70-mg/mCitation2 loading dose on day 1, followed by 50 mg/mCitation2 daily on subsequent days). Daily blood cultures are planned to document the clearance of candidemia and to monitor the effectiveness of therapy.
Antifungal treatment of candidemia in non-neutropenic patients
The laboratory findings for the case study indicate that the child has candidemia due to C. parapsilosis infection. A decision is made to administer caspofungin at the usual pediatric dose: 70 mg/mCitation2 on day 1, followed by 50 mg/mCitation2 thereafter, 12 mg/kg daily. Caspofungin is chosen, instead of fluconazole, because the symptoms of hypotension and fever are indicative of moderate-to-severe disease. This approach is consistent with recommendations from the 2009 IDSA guidelines for the management of candidiasisCitation13.
However, it should be noted that pediatric data are much more sparse than for adult patients, for dosing, individual treatment effectiveness, and comparisons between treatments. This is particularly the case for newer agents, including LFAmB and the echinocandins (particularly anidulafungin). Hence, many of the recommendations for management of pediatric candidiasis are based largely on expert opinion and experience in the absence of abundant data from published clinical trials. Also, results from additional pediatric research has become available and published since the publication of the 2009 IDSA guidelines. These potential shortcomings of the 2009 IDSA guidelines should be kept in mind when considering pediatric recommendations from the guidelines.
According to 2009 IDSA guidelines, fluconazole (12 mg/kg daily for pediatric patients) or an echinocandin is recommended as initial treatment for candidemia in non-neutropenic patientsCitation13. Moreover, the guidelines state that an echinocandin is preferred in patients with moderate-to-severe disease or recent azole exposure, and fluconazole for less critically ill patients with no recent azole exposureCitation13. For patients initially started with an echinocandin, the IDSA guidelines recommend transition to fluconazole, if the patient is clinically stable and has isolates likely to be susceptible to fluconazole (and hence no recent azole exposure). Echinocandins are fungicidal against Candida spp., whereas fluconazole and other azoles are fungistatic against the most clinically relevant Candida spp.Citation25, which may be part of the reason for preferring an echinocandin in more critically ill patients.
With respect to specific pathogen causes of candidemia, the guidelines recommend treatment with fluconazole for C. parapsilosis infectionCitation13. Echinocandin treatment is de-emphasized because some studies have reported higher echinocandin minimum inhibitory concentrations (MICs) for C. parapsilosis than other Candida spp., suggesting this pathogen may be somewhat less responsive to echinocandin therapy, although several clinical trials did not show this to be the caseCitation13,Citation26. For patients initially treated with an echinocandin (e.g., prior to documentation of C. parapsilosis infection), echinocandin therapy may continue, provided the patient is clinically improved and follow-up cultures are negative for the pathogenCitation13.
For patients infected with C. glabrata, the 2009 guidelines state a preference for echinocandin treatment, without transition to fluconazole or voriconazole unless there is confirmation of isolate susceptibilityCitation13. This is because all available azoles (fluconazole, itraconazole, voriconazole, and posaconazole) exhibit less activity against C. glabrata (and C. krusei) than other Candida spp. In particular, C. glabrata is more likely to exhibit dose-dependent susceptibility or resistance to voriconazole than to echinocandins, and while active against C. krusei, voriconazole requires more frequent administration and demonstrates less predictable pharmacokinetics than echinocandins. For its part, posaconazole demonstrates in vitro activity against both C. glabrata and C. krusei, but it is not available as an intravenous formulation and there are relatively few data to support its use among patients with candidemia. However, for patients who initially received fluconazole or voriconazole and are clinically improved with negative follow-up culture results, it is reasonable to continue azole treatment to completionCitation13.
AmB-d or LFAmB are alternative therapies if there is intolerance or limited availability of other antifungal agentsCitation13. Transition from initial treatment with AmB-d or LFAmB to fluconazole is recommended for all clinically stable patients with isolates likely to be susceptible to fluconazole.
In terms of duration of antifungal therapy, the IDSA guidelines state that treatment should be continued for 2 weeks after documented clearance of Candida from the bloodstream and resolution of candidemia-related symptoms, provided there is no evidence of metastatic complications, that is, disseminated diseaseCitation13. In practice, this typically means about 2 to 3 weeks of treatment: a few days to clear the infection and then for 2 weeks afterwards. Treatment shifts to longer durations for patients with disseminated disease.
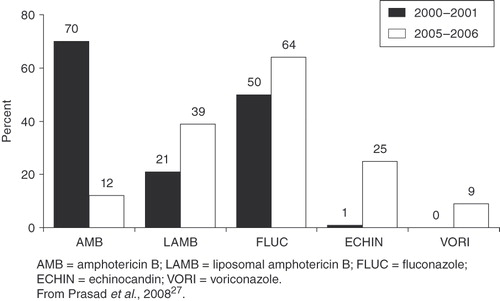
illustrates trends in antifungal therapy for pediatric invasive candidiasis/fungal infections, based on a retrospective analysis of data collected in the Pediatric Health Information System database from 25 US children’s hospitalsCitation27. There has been a general shift away from AmB-d treatment to greater use of LFAmB and echinocandin, and, to a lesser degree, fluconazole and voriconazole. It should be noted that these trends are based on a total of 62,842 pediatric patients who received antifungal therapy for fungal infections, a relatively limited database.
Figure 3. Trends in antifungal therapy for invasive candidiasis.
Antifungal treatment of candidemia in neutropenic patients
While the case study reviewed here involves a child with non-neutropenic candidemia, many patients encountered in the pediatric ICU exhibit neutropenic candidemia, including those immunosuppressed due to cancer chemotherapy. What would be the recommended treatment for a young child, similar to the one here, with neutropenic candidemia?
The 2009 IDSA guidelines recommend treatment with an echinocandin or LFAmB for most patients with neutropenic candidemiaCitation13. As mentioned, at this time caspofungin is the only echinocandin approved by the FDA for the treatment of invasive candidiasis in pediatric patients, specifically those aged 3 months and older. There is growing experience with other echinocandins in children and neonates28–32. Anidulafungin has been studied in children 2–17 years of age and should be dosed at 1.5 mg/kg/day32. Micafungin has been studied in children and neonates; children should be treated with 2–4 mg/kg daily, but neonates may require as much as 10–12 mg/kg daily to achieve therapeutic concentrations33. Data for each of the echinocandins suggest safety and efficacy in the pediatric population. Caspofungin, but not micafungin or anidulafungin, has been evaluated as treatment for pediatric febrile neutropeniaCitation15. Taken together with the fact that caspofungin is the only FDA approved echinocandin for pediatric patients with invasive candidiasis, it remains the treatment of choice among this drug class for pediatric patients with febrile neutropenia due to Candida spp. infection. For this patient population, caspofungin should be administered as a single 70-mg/mCitation2 loading dose on day 1, followed by 50 mg/mCitation2 daily thereafter. The pharmacokinetics of AmB-d appear to be similar in neonates and adults; few studies have examined the use of LFAmB in neonates or childrenCitation13.
For patients who are less critically ill and without recent azole exposure, the guidelines recommend fluconazole (12 mg/kg/d) as an alternative to an echinocandin or LFAmBCitation13. The reason an echinocandin or LFAmB is recommended over fluconazole or other azoles in more critically ill patients probably has to do (at least in part) with the fact that echinocandins and LFAmB are fungicidal agents, whereas azoles are usually fungistatic. Voriconazole (7 mg/kg every 12 hours allowed for children up to approximately 12 years of age) is recommended in situations where coverage of molds (e.g., Aspergillus spp.) as well as Candida spp. is desiredCitation13.
For non-albicans spp., an echinocandin is preferred for candidemia due to C. glabrataCitation13. LFAmB is considered an effective but less attractive alternative, due to higher cost and the potential for toxicity, and fluconazole or voriconazole may be continued in patients already receiving these agents who are clinically improved with negative follow-up culture results. An echinocandin, LFAmB, or voriconazole is recommended for candidemia due to C. krusei, and fluconazole or LFAmB is considered preferred initial therapy for infections due to C. parapsilosis. For non-neutropenic patients, treatment with an echinocandin may be continued to completion in those already receiving a member of this class for neutropenic candidemia due to C. parapsilosis and who are clinically stable and with negative follow-up culture results.
The recommended duration of therapy for neutropenic patients with candidemia is generally similar to that for non-neutropenic patients with candidemia, if there is no evidence of persistent fungemia or metastatic complications: 2 weeks after documented clearance of Candida from the bloodstream, resolution of symptoms attributable to candidemia, and resolution of neutropeniaCitation13.
Infectious Diseases Society of America recommendations for intravenous catheter removal
In addition to antifungal therapy, the IDSA guidelines also recommend removal of intravenous catheters from patients with candidemia when feasible, particularly those who are not neutropenicCitation13. Studies involving adults or neonates with candidemia have demonstrated that catheter removal is associated with shorter duration of candidemia and reduced mortality (reviewed in Pappas et al., 200913), but there is less evidence involving older children with candidemia. A 2004 study by Zaoutis and coworkers reported that “persistently positive blood cultures for Candida with a CVC in place” was a significant independent risk factor for disseminated candidiasis in children with a median age of 3.5 years (range: 0.6–14.3) (OR = 3.0; 95% CI = 1.2–7.8; p = 0.02)Citation9. Persistent candidemia (>3 days), regardless of catheter status, was not associated with dissemination.
The IDSA guidelines strongly recommend intravenous catheter removal for non-neutropenic patients with candidemia, and state that intravenous catheter removal should be considered for neutropenic patients with candidemiaCitation13. The evidence for the benefits of catheter removal (in neonates and adults) is strongest for non-neutropenic patients. The situation in neutropenic patients is less straightforward because disseminated disease is more common, and it is often difficult to distinguish whether the source of candidemia is catheter- or gastrointestinal-related. In addition, catheter removal in neutropenic patients more often creates substantial intravenous access difficulties.
Conclusions
Candidemia is a serious condition associated with high morbidity and mortality and elevated healthcare costs in pediatric patients. Children at highest risk are those with prolonged ICU stay, reduced immune function, prior bacterial infection, and recent surgery, as well as use of a CVC, total parenteral nutrition, mechanical ventilation, and/or dialysis. Similar risk factors are associated with increased risk of death due to candidemia. Treatment recommendations are similar for pediatric and adult patients, taking into consideration the need for dose modifications with certain antifungal agents in pediatric patients. Empiric therapy with fluconazole or an echinocandin should be considered in patients at high-risk for candidemia and signs or symptoms consistent with such a diagnosis. Fluconazole or an echinocandin are also recommended as initial treatment for documented candidemia in non-neutropenic patients. Treatment with an LFAmB or caspofungin is recommended for most patients with neutropenic candidemia. Treatment modifications may be warranted based on disease severity, the Candida spp. involved, and prior azole use. Early treatment with optimal antifungal therapy is required to improve outcomes in pediatric patients with candidemia.
Transparency
Declaration of funding
This activity is supported by an educational grant from Merck & Co., Inc.
Declaration of financial/other relationships
T.Z. has disclosed that he has performed contracted research for Merck and has received fees for non-CME services from Cephalon.
Some peer reviewers receive honoraria from CMRO for their review work. Peer reviewer 1 has disclosed that he/she has received research grants from Children’s Cancer Foundation of Baltimore and is on speakers bureaus of Enzon Pharmaceuticals and Sigma Tau Pharmaceuticals. Peer reviewer 2 has no relevant financial relationships to disclose.
Acknowledgment
The authors of this supplement thank Global Education Exchange, LLC, for editorial support.
References
- Marodi L, Johnston RB Jr. Invasive Candida species disease in infants and children: occurrence, risk factors, management, and innate host defense mechanisms. Curr Opin Pediatr 2007;19:693-7
- Zaoutis TE, Argon J, Chu J, et al. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Clin Infect Dis 2005;41:1232-9
- Filioti J, Spiroglou K, Panteliadis CP, et al. Invasive candidiasis in pediatric intensive care patients: epidemiology, risk factors, management, and outcome. Intensive Care Med 2007;33:1272-83
- Wisplinghoff H, Seifert H, Tallent SM, et al. Nosocomial bloodstream infections in pediatric patients in United States hospitals: epidemiology, clinical features and susceptibilities. Pediatr Infect Dis J 2003;22:686-91
- MacDonald L, Baker C, Chenoweth C. Risk factors for candidemia in a children’s hospital. Clin Infect Dis 1998;26:642-5
- Zaoutis T, Prasad P, Localio RA, et al. Risk factors for candidemia in the pediatric intensive care unit. Abstracts of the Society for Healthcare Epidemiology of America annual meeting, San Diego, CA [Abstract 503; platform presentation]. 2009
- Blyth CC, Chen SC, Slavin MA, et al. Not just little adults: candidemia epidemiology, molecular characterization, and antifungal susceptibility in neonatal and pediatric patients. Pediatrics 2009;123:1360-8
- Singhi S, Rao DS, Chakrabarti A. Candida colonization and candidemia in a pediatric intensive care unit. Pediatr Crit Care Med 2008;9:91-5
- Zaoutis TE, Greves HM, Lautenbach E, et al. Risk factors for disseminated candidiasis in children with candidemia. Pediatr Infect Dis J 2004;23:635-41
- Celebi S, Hacimustafaoglu M, Ozdemir O, et al. Nosocomial candidaemia in children: results of a 9-year study. Mycoses 2008;51:248-57
- Zaoutis TE, Coffin SE, Chu JH, et al. Risk factors for mortality in children with candidemia. Pediatr Infect Dis J 2005;24:736-9
- Pasqualotto AC, de Moraes AB, Zanini RR, et al. Analysis of independent risk factors for death among pediatric patients with candidemia and a central venous catheter in place. Infect Control Hosp Epidemiol 2007;28:799-804
- Pappas PG, Kauffman CA, Andes D, et al. Clinical practice guidelines for the management of candidiasis: 2009 update by the Infectious Diseases Society of America. Clin Infect Dis 2009;48:503-35
- Benjamin DK Jr, Smith PB, Arrieta A, et al. Safety and pharmacokinetics of repeat-dose micafungin in young infants. Clin Pharmacol Ther 2010;87:93-9
- VandenBussche HL, Van Loo DA. A clinical review of echinocandins in pediatric patients. Ann Pharmacother 2010;44:166-77
- Ikeda F, Saika T, Sato Y, et al. Antifungal activity of micafungin against Candida and Aspergillus spp. isolated from pediatric patients in Japan. Med Mycol 2009;47:145-8
- Kawaguchi C, Arai I, Yasuhara H, et al. Efficacy of micafungin in treating four premature infants with candidiasis. Pediatr Int 2009;51:220-4
- Smith PB, Walsh TJ, Hope W, et al. Pharmacokinetics of an elevated dosage of micafungin in premature neonates. Ped Infect Dis J 2009;28:412-15
- Martin GS, Mannino DM, Eaton S, et al. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med 2003;348:1546-54
- Abelson JA, Moore T, Bruckner D, et al. Frequency of fungemia in hospitalized pediatric inpatients over 11 years at a tertiary care institution. Pediatrics 2005;116:61-7
- Watson RS, Carcillo JA, Linde-Zwirble WT, et al. The epidemiology of severe sepsis in children in the United States. Am J Respir Crit Care Med 2003;167:695-701
- Pappas PG, Rex JH, Lee J, et al. A prospective observational study of candidemia: epidemiology, therapy, and influences on mortality in hospitalized adult and pediatric patients. Clin Infect Dis 2003;37:634-43
- Zaoutis TE, Foraker E, McGowan KL, et al. Antifungal susceptibility of Candida spp. isolated from pediatric patients: a survey of 4 children’s hospitals. Diagn Microbiol Infect Dis 2005;52:295-8
- Malani PN, Bradley SF, Little RS, et al. Trends in species causing fungaemia in a tertiary care medical centre over 12 years. Mycoses 2001;44:446-9
- Fisher BT, Zaoutis TE. Treatment of invasive candidiasis in immunocompromised pediatric patients. Paediatr Drugs 2008;10:281-98
- Trofa D, Gacser A, Nosanchuk JD. Candida parapsilosis, an emerging fungal pathogen. Clin Microbiol Rev 2008;21:606-25
- Prasad PA, Coffin SE, Leckerman KH, et al. Pediatric antifungal utilization: new drugs, new trends. Pediatr Infect Dis J 2008;27:1083-8
- Walsh TJ. Echinocandins—an advance in the primary treatment of invasive candidiasis. N Engl J Med 2002;347:2070-2
- Steinbach WJ, Benjamin DK. New antifungal agents under development in children and neonates. Curr Opin Infect Dis 2005;18:484-9
- Seibel NL, Schwartz C, Arrieta A, et al. Safety, tolerability, and pharmacokinetics of Micafungin (FK463) in febrile neutropenic pediatric patients. Antimicrob Agents Chemother 2005;49:3317-24
- Heresi GP, Gerstmann DR, Reed MD, et al. The pharmacokinetics and safety of micafungin, a novel echinocandin, in premature infants. Pediatr Infect Dis J 2006;25:1110-5
- Benjamin DK Jr, Driscoll T, Seibel NL, et al. Safety and pharmacokinetics of intravenous anidulafungin in children with neutropenia at high risk for invasive fungal infections. Antimicrob Agents Chemother 2006;50:632-8
- Smith PB, Walsh TJ, Hope W, et al. Pharmacokinetics of an elevated dosage of micafungin in premature neonates. Pediatr Infect Dis J 2009;28:412-5